Contents
- What is irritable bowel syndrome (IBS)
What is irritable bowel syndrome (IBS)
Irritable bowel syndrome also called IBS is a common, long-term condition that affects the functioning of your large intestine 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. Irritable bowel syndrome (IBS) is a functional disorder of the intestine but is now called disorder of gut–brain interaction (DGBI), because there is no sign of the disease that can be seen or measured, but the large intestine is not functioning normally 12. The main symptoms of irritable bowel syndrome (IBS) are abdominal pain, stomach cramps or discomfort that is often relieved by passing wind or feces, stomach bloating and chronic diarrhea or constipation. Some people go back and forth between diarrhea and constipation 12. In addition, IBS is often associated with other somatic comorbidities such as pain syndromes, overactive bladder and migraine; psychiatric conditions including depression and anxiety and visceral sensitivity 13. Although IBS can cause a great deal of discomfort, it does not harm the intestines.
IBS symptoms vary between individuals and affect some people more severely than others. They tend to come and go in periods lasting a few days to a few months at a time, often during times of stress or after eating certain foods.
These symptoms can be embarrassing, inconvenient and distressing. Fortunately, IBS does not cause permanent damage to your bowel and it does not cause other serious diseases like bowel cancer.
Irritable bowel syndrome (IBS) is common, occurring in about one in five Americans and up to 8–12% of the population worldwide 8, 14, 15, 16. Studies have estimated the prevalence in the United States is somewhere between 15% and 20% of the entire population. IBS is seen in similar frequencies in other countries around the world. Irritable bowel syndrome (IBS) affects about twice as many women as men and is most often found in people younger than 45 years. It usually begins in late adolescence or early adult life between 20 and 30 years of age and rarely appears for the first time after the age of 50.
Based on questionnaire data, women are 1.5 to 3.0 times more likely to have IBS, reflecting a prevalence in women of 14% and in men of 8.9% 13, 14. However, based on healthcare system utilization, women are up to 2 to 2.5 times more likely to see a healthcare provider for their symptoms 17. The reason why women are more commonly affected by irritable bowel syndrome is not completely understood. It does not seem to be merely due to hormonal differences between men and women. Rather it seems to be due to differences in how women and men process sensations from the intestines, both in the intestinal nervous system ( “enteric nervous system”) as well as the brain and spinal cord (“central nervous system”) 18. The frequency of IBS seems to be the same across racial, ethnic and national boundaries.
Despite the fact that irritable bowel syndrome is so common, most people with IBS do not see a doctor for their symptoms 18. It is estimated that only 1 in 4 people with IBS see a doctor (and thus become a patient with IBS). Reasons why some people chose to see a doctor and others do not are not completely understood. Interestingly severity of gastrointestinal symptoms from IBS alone does not seem to be the major driving factor. Rather the impact of IBS on the patient’s ability to function on a day-to-day basis while having IBS symptoms, the stress from having IBS, and concerns about other diseases that they might have are some of the more frequent reasons patients see their doctor for IBS like symptoms.
Studies have shown that that when compared to patients with no medical problems, patients with diabetes, gastroesophageal reflux disease (GERD), as well as individuals who have no gastro intestinal disorders, patients with IBS had significantly higher degrees of impairment in their quality of life. By this is meant their physical functioning, their ability to participate in the activities of daily living, their level of emotional distress, their sexual functioning and all the other components that go into a happy and healthy normal life without disease. This is the true impact of IBS and is an important reason that it deserves serious attention from the medical community. IBS is also a costly disease, not only in terms of money spent for health care but also money lost because patients cannot work while they have symptoms. It is estimated that IBS patients because of their inability to participate in work activities, school activities, etc. lose $30 to $90 billion per year in productivity. After the common cold, IBS is the second most frequent reason people take days off from work in the United States. This makes IBS a very important issue for public health and the society in general, which clearly needs to be addressed by the medical community.
The exact cause of irritable bowel syndrome (IBS) remains incompletely understood, but is probably multifactorial and complex 14. A unifying theme is that the symptoms of IBS result from disordered communication between your gut and your brain, which clinically presents as increased internal organ perception and altered bowel habits 14. Scientific evidence has identified alterations in central (brain) and peripheral (gut) mechanisms in IBS and the bidirectional communication between the brain and the gut. Significant mechanisms linked to IBS include a gut motility disturbance, visceral hypersensitivity, altered mucosal and immune function, altered gut microbiota, and altered central nervous system (brain and spinal cord) processing 14. Other less reproducible mechanisms may include genetic associations, alterations in gastrointestinal microbiota, and disturbances in mucosal and immune function 19.
Irritable bowel syndrome (IBS) is best defined by what it is NOT!
- IBS is NOT an anatomical or structural defect.
- IBS is NOT an identifiable physical or chemical disorder.
- IBS is NOT a cancer and will not cause cancer.
- IBS will NOT cause other gastrointestinal diseases.
Patients suffering from IBS should not be worried about it leading to other serious diseases. The major problem with IBS is not because it causes death or serious disease, but because it changes the quality of life for the patient.
IBS is diagnosed based on symptoms, and a distinction is made between the following subtypes of IBS:
- IBS-D: Diarrhea predominant
- IBS-C: Constipation predominant
- IBS with mixed bowel habits (IBS-M): Alternating, or mixed, between constipation and diarrhea
- IBS-PI: Post Infectious IBS
- PDV-IBS: Post Diverticulitis IBS
- IBS unclassified (IBS-U): Patients who meet diagnostic criteria for IBS but whose bowel habits cannot be accurately categorized into 1 of the 3 groups above should be categorized as having IBS unclassified.
Classifying patients with IBS into specific subtypes based on predominant bowel habits is useful as it helps focus treatment on the predominant, and often, the most bothersome symptom. For clinical trials, or when appropriate in clinical settings, subjects should complete a 14-day bowel diary to most accurately categorize IBS subtypes. Bristol stool types 1 and 2 or types 6 and 7 are considered abnormal 20.
The diagnosis of IBS is based on symptoms ranging from the Manning criteria to the Rome criteria, and the most widely used diagnostic criteria are the Rome IV 21. Rome IV diagnostic criteria defined irritable bowel syndrome (IBS) as a functional bowel disorder in which recurrent abdominal pain is associated with defecation or a change in bowel habits. Disordered bowel habits are typically present (i.e., constipation, diarrhea or a mix of constipation and diarrhea), as are symptoms of abdominal bloating or distension. Symptom onset should occur at least 6 months prior to diagnosis and symptoms should be present during the last 3 months 22.
IBS Rome IV Diagnostic Criteria – recurrent abdominal pain, on average, at least 1 day per week in the last 3 months, associated with 2 or more of the following criteria 22:
- Related to defecation.
- Associated with a change in the frequency of stool.
- Associated with a change in the form (appearance) of stool.
These criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis.
According to Vijayvargiya et al 23, fecal bile acids and fecal fat are potential biomarkers for IBS-D (IBS with diarrhea predominant) and IBS-C (IBS with constipation predominant). Total fecal bile acids, chenodeoxycholic acid, cholic acid, and primary bile acids were significantly higher in patients with IBS-D (IBS with diarrhea predominant) than in healthy patients or patients with IBS-C (IBS with constipation predominant). In contrast, deoxycholic acid and combined deoxycholic acid and chenodeoxycholic acid (secretory) bile acids were significantly lower in patients with IBS-C than in healthy control and patients with IBS-D. Combining fasting serum 7α-hydroxy-4-cholesten-3-one and primary bile acids or fecal bile acid concentrations in stool samples is a simple, low-cost diagnostic for bile acid diarrhea. Circulating resolvin D1 (RvD1) and C-reactive protein (CRP) are inflammatory markers in patients with IBS-C; patients with IBS-C have higher CRP and lower resolvin D1 (RvD1) concentrations than healthy control 24. Furthermore, radiopaque markers and radionuclide scanning can be used to assess transit function, and rectal sensation to balloon distension can be used to assess visceral hypersensitivity 25. All of the ancillary tests listed above can be used to further identify the cause and guide medication use if the first-line medication is ineffective.
Irritable bowel syndrome is not associated with serious medical consequences. People with IBS tend to live long and in some studies, somewhat longer than individuals who do not have IBS. IBS is not associated with other serious GI diseases, such as inflammatory bowel disease (Crohn’s disease or ulcerative colitis) or colon cancer. The presence of IBS does not put extra stress on the other organs in the body such as the heart, liver or kidneys. Overall the prognosis for irritable bowel syndrome is excellent.
A subset of irritable bowel syndrome (IBS) sufferers may have co-morbidities with other digestive health disorders namely; GERD (gastroesophageal reflux disease) / Heartburn, Dyspepsia, Chronic Constipation, Chronic Abdominal Pain, Fibromyalgia, Pelvic pain or perhaps Crohn’s Disease and Ulcerative Colitis, known collectively as Inflammatory Bowel Disease (IBD). For instance, 29% of gastroesophageal reflux disease (GERD) patients have Chronic Constipation. Diagnosis can shift from one motility disorder to another over time; however, co-morbidity in IBS may be due to a general amplification of symptom reporting and physician consultation rather than a direct association.
Doctors may treat irritable bowel syndrome (IBS) by recommending changes in what you eat and other lifestyle changes, medicines, probiotics, and mental health therapies. You may have to try a few treatments to see what works best for you. Your doctor can help you find the right treatment plan. A research study illustrated that patient education in diet, exercise, and stress management showed significant improvement in pain and symptoms at 1 and 6 months of treatment. An educational approach and appropriate use of medications should be components of a physician-based IBS treatment plan.
See your doctor if you have a persistent change in bowel habits or other signs or symptoms of IBS. They may indicate a more serious condition, such as colon cancer. More-serious signs and symptoms include:
- Weight loss
- Diarrhea at night
- Rectal bleeding
- Iron deficiency anemia
- Unexplained vomiting
- Difficulty swallowing
- Persistent pain that isn’t relieved by passing gas or a bowel movement
There is no specific test for IBS. Your doctor may run tests to be sure you don’t have other diseases. These tests may include stool sampling tests, blood tests, and x-rays. Your doctor may also do a test called a sigmoidoscopy or colonoscopy. Most people diagnosed with IBS can control their symptoms with diet, stress management, probiotics, and medicine.
No one knows the exact cause of IBS.
The main feature of IBS is abdominal pain associated with a change in bowel habits.
Symptoms to look for include:
- Recurring episodes of diarrhea or constipation
- Symptoms that alternate between diarrhea and constipation
- Bloating
- Pain or discomfort that is relieved by passing wind or going to the toilet and opening your bowels
- Symptoms are more common in women and may be worse around menstruation or at times of stress.
IBS does not cause bleeding from the back passage.
If you have irritable bowel syndrome (IBS) , then an episode can be triggered by an infection, food intolerance or particular medicines.
Irritable bowel syndrome (IBS) often occurs at times of emotional stress.
The condition is often lifelong, although it may improve over several years. Talking with your doctor about your problem is the first helpful step, because we all fear the unknown.
Who is more likely to develop IBS?
Women are up to two times more likely than men to develop IBS 26. People younger than age 50 are more likely to develop IBS than people older than age 50 27.
Factors that can increase your chance of having IBS include:
- having a family member with IBS
- a history of stressful or difficult life events, such as abuse, in childhood
- having a severe infection in your digestive tract.
What other health problems do people with IBS have?
People with IBS often have other health problems, including 26, 13, 1, 2, 28:
- certain conditions that involve chronic pain, such as fibromyalgia, chronic fatigue syndrome and chronic pelvic pain
- certain digestive diseases, such as dyspepsia and gastroesophageal reflux disease
- certain mental disorders, such as anxiety, depression, and somatic symptom disorder.
Is there a cure for IBS?
At the present time there isn’t a cure for IBS. But, most people manage symptoms by avoiding triggers and taking medications when necessary.
What are there different types of IBS?
According to the Rome IV criteria, there are 4 main types of IBS are based on different patterns of changes in your bowel movements or abnormal bowel movements 29. Sometimes, it is important for your doctor to know which type of IBS you have. Some medicines work only for some types of IBS or make other types worse. Your doctor might diagnose IBS even if your bowel movement pattern does not fit one particular type.
Many people with IBS have normal bowel movements on some days and abnormal bowel movements on other days.
- IBS with constipation (IBS-C). With IBS-C, on days when you have at least one abnormal bowel movement more than a quarter (>25%) of your stools are hard or lumpy and less than a quarter (<25%) of your stools are loose or watery.
- IBS with diarrhea (IBS-D). In IBS-D, on days when you have at least one abnormal bowel movement more than a quarter (>25%) of your stools are loose or watery and less than a quarter (<25%) of your stools are hard or lumpy.
- IBS with mixed bowel habits (IBS-M). In IBS-M, on days when you have at least one abnormal bowel movement more than a quarter (>25%) of your stools are hard or lumpy and more than a quarter (>25%) of your stools are loose or watery.
- IBS unclassified (IBS-U): Patients who meet diagnostic criteria for IBS but whose bowel habits cannot be accurately categorized into 1 of the 3 groups above should be categorized as having IBS unclassified.
Irritable bowel syndrome causes
The exact cause of irritable bowel syndrome is not known. However, tremendous advances in our understanding of this common and disabling disorder have been made in the last 10 years. Abnormal motility in terms of the bowel moving too fast (which causes diarrhea) or too slow (which causes constipation) is certainly part of this syndrome. However, this represents only one part of a complicated disease. The symptoms of pain, incomplete emptying of the bowels, and bloating cannot be blamed only on abnormal gastrointestinal motility. Over the last 20 years a number of very well done scientific studies have demonstrated that individuals with IBS tend to have higher levels of sensitivity in the intestines compared to individuals who do not have IBS.
In the last 10 years, we found and identified certain chemicals present in the intestines, which send signals from nerve endings from the intestines to the brain, and also from the brain to the intestines. These chemicals are called “neuro transmitters” and work as messengers between nerve endings to carry signals in both directions between the brain and gut. This is very important because it has led to the development of new drugs. Some of these drugs are currently available. Others are being developed, as we better understand how these chemical ‘neuro transmitters’ work. One of the major neuro transmitters involved in sensation of pain in the gut as well as playing a key role in motility activity of the gut is serotonin. This chemical also known by its chemical abbreviation 5-HT. However, serotonin is only one of a large number of neuro transmitters that are present in the gut. As scientists identify more and more of these substances and better understand their actions, they may be able to further supplement the arsenal of medications that will influence these neuro transmitters and thus help relieve the symptoms of IBS. Clearly the future is quite bright both for better understanding this perplexing and disabling disorder as well as using this knowledge to make newer and better treatments for IBS.
The precise cause of IBS isn’t known. Certain problems are more common in people with IBS. Experts think these problems may play a role in causing IBS. These problems include 30, 31, 32, 33, 34, 35, 36, 37:
- Muscle contractions in the intestine. The walls of the intestines are lined with layers of muscle that contract as they move food through your digestive tract. Contractions that are stronger and last longer than normal can cause gas, bloating and diarrhea. Weak intestinal contractions can slow food passage and lead to hard, dry stools.
- Nervous system. Abnormalities in the nerves in your digestive system may cause you to experience greater than normal discomfort when your abdomen stretches from gas or stool. Poorly coordinated signals between the brain and the intestines can cause your body to overreact to changes that normally occur in the digestive process, resulting in pain, diarrhea or constipation.
- Inflammation in the intestines. Some people with IBS have an increased number of immune-system cells in their intestines. This immune-system response is associated with pain and diarrhea.
- Severe infection. IBS can develop after a severe bout of diarrhea (gastroenteritis) caused by bacteria or a virus. IBS might also be associated with a surplus of bacteria in the intestines (bacterial overgrowth).
- Changes in bacteria in the gut (microflora). Microflora are the “good” bacteria that reside in the intestines and play a key role in health. Research indicates that microflora in people with IBS might differ from microflora in healthy people.
- Early-life stress. People exposed to stressful events such as physical or sexual abuse, especially in childhood, tend to have more symptoms of IBS.
- Certain mental disorders, such as depression, anxiety, and somatic symptom disorder.
- Food intolerances or food sensitivities, in which certain foods cause digestive symptoms
Research suggests that genes may make some people more likely to develop IBS.
Triggers for Irritable bowel syndrome (IBS)
Symptoms of IBS can be triggered by:
- Food. The role of food allergy or intolerance in IBS isn’t fully understood. A true food allergy rarely causes IBS. But many people have worse IBS symptoms when they eat or drink certain foods or beverages, including wheat, dairy products, citrus fruits, beans, cabbage, milk and carbonated drinks.
- Stress. Most people with IBS experience worse or more frequent signs and symptoms during periods of increased stress. But while stress may aggravate symptoms, it doesn’t cause them.
- Hormones. Women are twice as likely to have IBS, which might indicate that hormonal changes play a role. Many women find that signs and symptoms are worse during or around their menstrual periods.
Risk factors for Irritable bowel syndrome (IBS)
Many people have occasional signs and symptoms of IBS. But you’re more likely to have IBS if you 38, 39, 40:
- Are young. IBS occurs more frequently in people under age 50.
- Are female. In the United States, IBS is more common among women. Estrogen therapy before or after menopause also is a risk factor for IBS.
- Have a family history of IBS. Genes may play a role, as may shared factors in a family’s environment or a combination of genes and environment.
- Have anxiety, depression or other mental health issues. Anxiety, depression and other mental health issues are associated with IBS. A history of sexual, physical or emotional abuse also might be a risk factor.
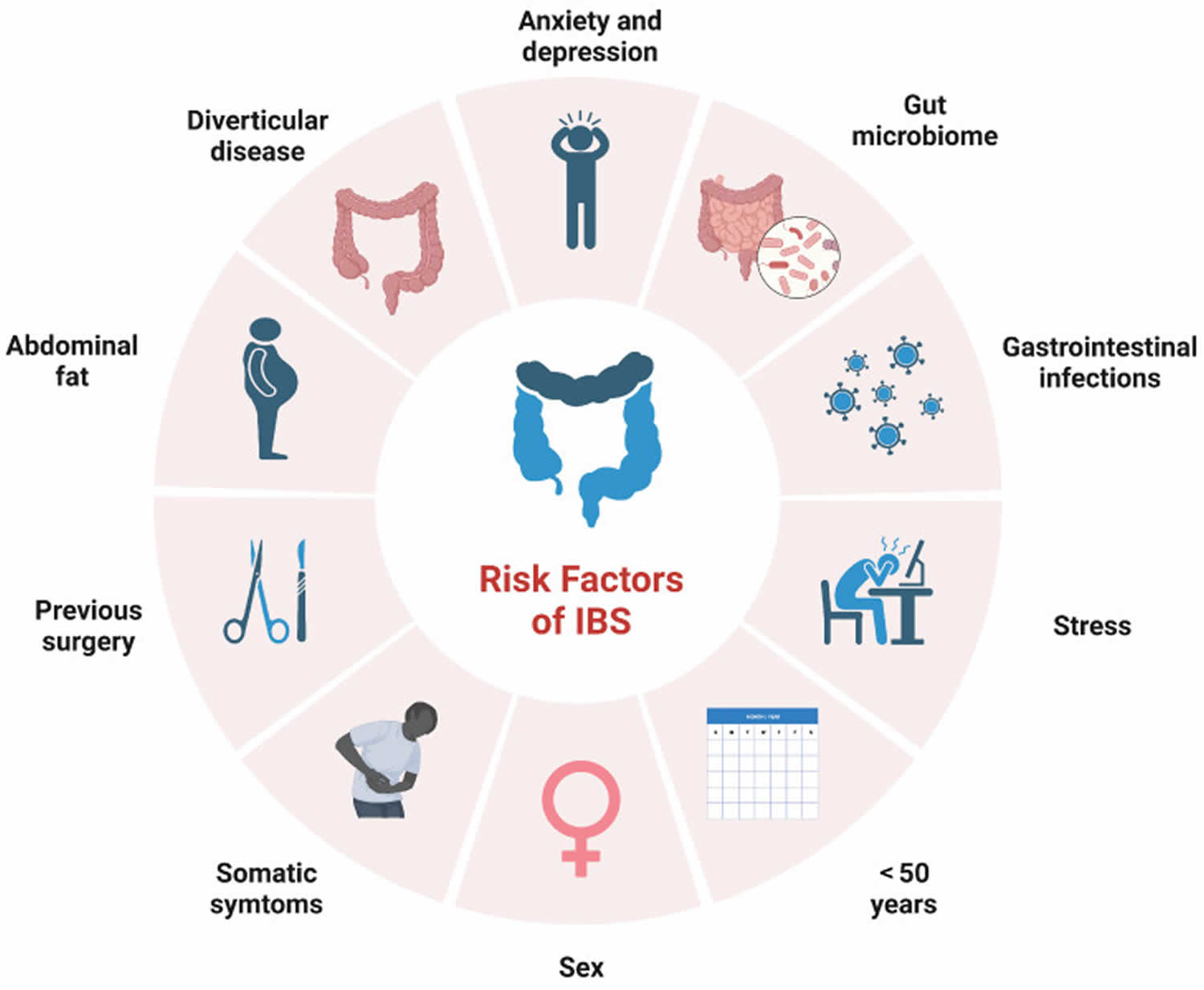
Figure 1. Risk factors in irritable bowel syndrome (IBS)
Irritable bowel syndrome (IBS) prevention
Finding ways to deal with stress may help prevent or ease symptoms of IBS. Consider trying:
- Counseling. A counselor can help you learn to modify or change your responses to stress. Studies have shown that psychotherapy can provide significant and long-lasting reduction of symptoms.
- Biofeedback. Electrical sensors help you receive information (feedback) on your body’s functions. The feedback helps you focus on making subtle changes, such as relaxing certain muscles, to ease symptoms.
- Progressive relaxation exercises. These exercises help you relax muscles in your body, one by one. Start by tightening the muscles in your feet, then concentrate on slowly letting all of the tension go. Next, tighten and relax your calves. Continue until the muscles in your body, including those in your eyes and scalp, are relaxed.
- Mindfulness training. This stress-reduction technique helps you focus on being in the moment and letting go of worries and distractions.
Irritable bowel syndrome symptoms
The most common symptoms of irritable bowel syndrome (IBS) are pain in your abdomen, often related to your bowel movements, and changes in your bowel movements. These changes may be diarrhea, constipation, or both, depending on what type of IBS you have.
The signs and symptoms of IBS include:
- Abdominal pain, cramping or bloating that is usually worse after eating and typically relieved or partially relieved by passing a bowel movement
- Excess gas
- Diarrhea or constipation — sometimes alternating bouts of diarrhea and constipation
- Mucus in the stool
IBS symptoms can include:
- sensation of incomplete evacuation
- farting (flatulence)
- passing mucus in the stool
- tiredness and a lack of energy
- feeling sick (nausea)
- backache
- problems peeing, like needing to pee often, sudden urges to pee, and feeling like you cannot fully empty your bladder
- not always being able to control when you poop (bowel incontinence)
Most people with IBS experience times when the signs and symptoms are worse (flare-ups) and times when they improve or even disappear completely.
Women with IBS often have more symptoms during their periods.
The signs and symptoms may be triggered by food or drink such as alcohol, caffeine, certain foods, such as spicy or fatty food, stress and anxiety.
Irritable bowel syndrome (IBS) complications
Chronic constipation or diarrhea can cause hemorrhoids.
In addition, IBS is associated with:
- Poor quality of life. Many people with moderate to severe IBS report poor quality of life. Research indicates that people with IBS miss three times as many days from work as do those without bowel symptoms.
- Mood disorders. Experiencing the signs and symptoms of IBS can lead to depression or anxiety. Depression and anxiety also can make IBS worse.
Irritable bowel syndrome (IBS) Diagnosis
There’s no test to definitively diagnose IBS. Your doctor is likely to start with a complete medical history, physical exam and tests to rule out other conditions. If you have IBS with diarrhea, you likely will be tested for gluten intolerance (celiac disease).
After other conditions have been ruled out, your doctor is likely to use one of these sets of diagnostic criteria for IBS:
- Rome criteria. These criteria include abdominal pain and discomfort lasting on average at least one day a week in the last three months, associated with at least two of these factors: Pain and discomfort are related to defecation, the frequency of defecation is altered, or stool consistency is altered.
- Manning criteria. These criteria focus on pain relieved by passing stool and on having incomplete bowel movements, mucus in the stool and changes in stool consistency. The more symptoms you have, the greater the likelihood of IBS.
- Type of IBS. For the purpose of treatment, IBS can be divided into three types, based on your symptoms: constipation-predominant, diarrhea-predominant or mixed.
Your doctor will also likely assess whether you have other signs or symptoms that might suggest another, more serious, condition. These signs and symptoms include:
- Onset of signs and symptoms after age 50
- Weight loss
- Rectal bleeding
- Fever
- Nausea or recurrent vomiting
- Abdominal pain, especially if it’s not completely relieved by a bowel movement, or occurs at night
- Diarrhea that is persistent or awakens you from sleep
- Anemia related to low iron
If you have these signs or symptoms, or if an initial treatment for IBS doesn’t work, you’ll likely need additional tests.
What tests do doctors use to diagnose IBS?
Your doctor may recommend several tests, including stool studies to check for infection or problems with your intestine’s ability to take in the nutrients from food (malabsorption). You may also have a number of other tests to rule out other causes for your symptoms.
Diagnostic procedures and imaging tests can include:
- Flexible sigmoidoscopy. Your doctor examines the lower part of your colon (sigmoid) with a flexible, lighted tube (sigmoidoscope).
- Colonoscopy. Your doctor uses a small, flexible tube to examine the entire length of your colon.
- Upper endoscopy. A long, flexible tube is inserted down your throat and into your esophagus, which is the tube connecting your mouth and stomach. A camera on the end of the tube provides a view of your upper digestive tract. During an endoscopy, a tissue sample called a biopsy may be collected. A sample of fluid may be collected to look for overgrowth of bacteria. This test may be recommended if celiac disease is suspected.
- X-ray or CT scan. These tests produce images of your abdomen and pelvis that might allow your doctor to rule out other causes of your symptoms, especially if you have abdominal pain. Your doctor might fill your large intestine with a liquid (barium) to make any problems more visible on X-ray. This barium test is sometimes called a lower GI series.
Laboratory tests can include:
- Lactose intolerance tests. Lactase is an enzyme you need to digest the sugar found in dairy products. If you don’t produce lactase, you may have problems similar to those caused by IBS, including abdominal pain, gas and diarrhea. Your doctor may order a breath test or ask you to remove milk and milk products from your diet for several weeks.
- Breath test for bacterial overgrowth. A breath test also can determine if you have bacterial overgrowth in your small intestine. Bacterial overgrowth is more common among people who have had bowel surgery or who have diabetes or some other disease that slows down digestion.
- Upper endoscopy. A long, flexible tube is inserted down your throat and into the tube connecting your mouth and stomach (esophagus). A camera on the end of the tube allows the doctor to inspect your upper digestive tract and obtain a tissue sample (biopsy) from your small intestine and fluid to look for overgrowth of bacteria. Your doctor might recommend endoscopy if celiac disease is suspected.
- Stool tests. Your stool might be examined for bacteria or parasites, or a digestive liquid produced in your liver (bile acid), if you have chronic diarrhea. Bile acid is a digestive liquid produced in the liver. Stool studies also can check to see if the intestine has trouble taking in nutrients. This is a condition known as malabsorption.
IBS Rome IV Diagnostic Criteria
Recurrent abdominal pain, on average, at least 1 day per week in the last 3 months, associated with 2 or more of the following criteria 22:
- Related to defecation.
- Associated with a change in the frequency of stool.
- Associated with a change in the form (appearance) of stool.
These criteria fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis.
IBS subtypes diagnostic criteria
Predominant bowel habits are based on stool form on days with at least one abnormal bowel movement 22:
- IBS with constipation predominant (IBS-C): More than one-fourth (25%) of bowel movements with Bristol stool form types 1 or 2 and less than one-fourth (25%) of bowel movements with Bristol stool form types 6 or 7. Alternative for epidemiology or clinical practice: Patient reports that abnormal bowel movements are usually constipation (like type 1 or 2 in the picture of Bristol Stool Form Scale [BSFS] below).
- IBS with diarrhea predominant (IBS-D): more than one-fourth (25%) of bowel movements with Bristol stool form types 6 or 7 and less than one-fourth (25%) of bowel movements with Bristol stool form types 1 or 2. Alternative for epidemiology or clinical practice: Patient reports that abnormal bowel movements are usually diarrhea (like type 6 or 7 in the picture of Bristol Stool Form Scale [BSFS] below).
- IBS with mixed bowel habits (IBS-M): more than one-fourth (25%) of bowel movements with Bristol stool form types 1 or 2 and more than one-fourth (25%) of bowel movements with Bristol stool form types 6 or 7. Alternative for epidemiology or clinical practice: Patient reports that abnormal bowel movements are usually both constipation and diarrhea (more than one-fourth of all the abnormal bowel movements were constipation and more than one-fourth were diarrhea, using picture of Bristol Stool Form Scale [BSFS] below).
- IBS unclassified (IBS-U): Patients who meet diagnostic criteria for IBS but whose bowel habits cannot be accurately categorized into 1 of the 3 groups above should be categorized as having IBS unclassified.
The Bristol stool form scale (BSFS) was developed in the 1990s in the Bristol Royal Infirmary in England 20. The authors described 7 types of stool (see Figure 2 below):
- Type 1: Separate hard lumps, like nuts (hard to pass)
- Type 2: Sausage-shaped, but lumpy
- Type 3: Like a sausage but with cracks on its surface
- Type 4: Like a sausage or snake, smooth and soft
- Type 5: Soft blobs with clear cut edges (passed easily)
- Type 6: Fluffy pieces with ragged edges, a mushy stool
- Type 7: Watery, no solid pieces, entirely liquid
The authors classified stool types 1 and 2 as being associated with constipation, while stool types 6 and 7 were associated with diarrhea and stool type 5 to some degree 20. Stool types 3 and 4 were considered normal stools. The BSFS is a convenient way for patients to describe their bowel habits, and is routinely used in clinical trials. In addition, at the two extremes (Bristol stool types 1 and 2 or types 6 and 7), the stool form serves as a rough surrogate marker of colon transit 20. Patients with IBS with constipation predominant (IBS-C) have >25% of their bowel movements associated with BSFS 1 or 2, while those with IBS with diarrhea predominant (IBS-D) have >25% of their bowel movements associated with BSFS 6 or 7. Those with the mixed subtype of alternating constipation and diarrhea (IBS-M) have >25% of their bowel movements associated with BSFS 1 or 2 and >25% of their bowel movements associated with BSFS 6 or 7.
For clinical trials, or when appropriate in clinical settings, subjects should complete a 14-day bowel diary to most accurately categorize IBS subtypes. Bristol stool types 1 and 2 or types 6 and 7 are considered abnormal 20.
IBS subtypes related to bowel habit abnormalities (IBS-C, IBS-D, and IBS-M) can only be confidently established when the patient is evaluated off medications used to treat bowel habit abnormalities.
Figure 2. Bristol Stool Form Scale
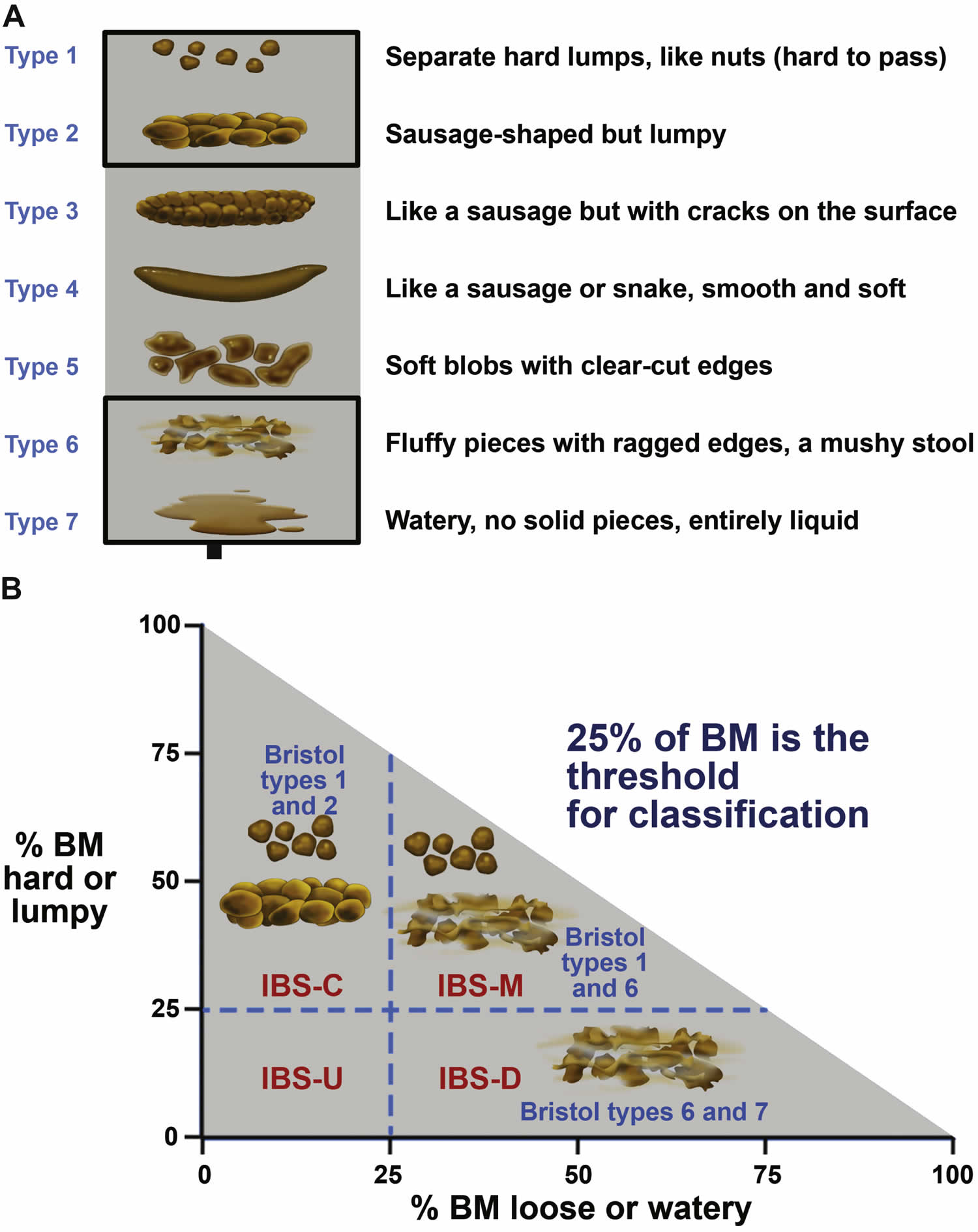
Footnotes: (A) The Bristol Stool Form Scale (BSFS) is a useful tool to evaluate bowel habit. The Bristol Stool Form Scale (BSFS) has been shown to be a reliable surrogate marker for colonic transit 41. (B) IBS subtypes should be established according to stool consistency, using the Bristol Stool Form Scale (BSFS). IBS subtyping is more accurate when patients have at least 4 days of abnormal bowel habits per month. Bowel habit subtypes should be based on Bristol Stool Form Scale (BSFS) for days with abnormal bowel habits.
[Source 22 ]Irritable bowel syndrome treatment
Treatment of IBS focuses on relieving symptoms so that you can live as normally as possible.
Stressful life experiences can worsen IBS symptoms and it is important you seek advise for stress reduction from your primary care clinician if you are having difficulty dealing with the stress.
Mild signs and symptoms can often be controlled by managing stress and by making changes in your diet and lifestyle. Try to:
- Avoid foods that trigger your symptoms
- Eat high-fiber foods. Fiber may improve constipation in IBS because it makes stool soft and easier to pass. The Dietary Guidelines for Americans recommends that adults should get 22 to 34 grams of fiber a day 42. To help your body get used to more fiber, add foods with fiber to your diet a little at a time. Too much fiber at once can cause gas, which can trigger IBS symptoms. Adding fiber to your diet slowly, by 2 to 3 grams a day, may help prevent gas and bloating.
- Two types of fiber are:
- Soluble fiber, which is found in beans, fruit, and oat products. Research suggests that soluble fiber is more helpful in relieving IBS symptoms.
- Insoluble fiber, which is found in whole-grain products and vegetables
- Two types of fiber are:
- Drink plenty of fluids
- Exercise regularly
- Get enough sleep.
Your doctor might suggest that you ELIMINATE or AVOID from your diet:
- High-gas foods. If you experience bloating or gas, you might avoid items such as carbonated and alcoholic beverages, caffeine, raw fruit, and certain vegetables, such as cabbage, broccoli and cauliflower.
- Gluten. Research shows that some people with IBS report improvement in diarrhea symptoms if they stop eating gluten (wheat, barley and rye) even if they don’t have celiac disease.
- FODMAPs. Some people are sensitive to certain carbohydrates such as fructose, fructans, lactose and others, known as FODMAPs — fermentable oligo-, di-, and monosaccharides and polyols. FODMAPs are found in certain grains, vegetables, fruits and dairy products. Your IBS symptoms might ease if you follow a strict low-FODMAP diet and then reintroduce foods one at a time. Examples of foods that contain FODMAPs include:
- fruits such as apples, apricots, blackberries, cherries, mango, nectarines, pears, plums, and watermelon, or juice containing any of these fruits.
- canned fruit in natural fruit juice, or large amounts of fruit juice or dried fruit.
- vegetables such as artichokes, asparagus, beans, cabbage, cauliflower, garlic and garlic salts, lentils, mushrooms, onions, and sugar snap or snow peas.
- dairy products such as milk, milk products, soft cheeses, yogurt, custard, and ice cream.
- wheat and rye products.
- honey and foods with high-fructose corn syrup.
- products, including candy and gum, with sweeteners ending in “–ol,” such as sorbitol, mannitol, xylitol, and maltitol.
Your doctor may suggest that you try the low FODMAP diet for a few weeks to see if it helps with your symptoms. If your symptoms improve, your doctor may recommend slowly adding foods that contain FODMAPs back into your diet. You may be able to eat some foods with FODMAPs without having IBS symptoms.
A dietitian can help you with these diet changes.
If your problems are moderate or severe, your doctor might suggest counseling — especially if you have depression or if stress tends to worsen your symptoms.
In addition, based on your symptoms your doctor might suggest medications such as:
- Fiber supplements. Taking a supplement such as psyllium (Metamucil) with fluids may help control constipation.
- Laxatives. If fiber doesn’t help constipation, nonprescription laxatives, such as magnesium hydroxide oral (Milk of Magnesia) or polyethylene glycol (Miralax), may be recommended.
- Anti-diarrheal medications. Over-the-counter medications, such as loperamide (Imodium), can help control diarrhea. Your doctor might also prescribe a bile acid binder, such as cholestyramine (Prevalite), colestipol (Colestid) or colesevelam (Welchol). Bile acid binders can cause bloating.
- Anticholinergic medications. Medications such as dicyclomine (Bentyl) can help relieve painful bowel spasms. They are sometimes prescribed for people who have bouts of diarrhea. These medications are generally safe but can cause constipation, dry mouth and blurred vision.
- Tricyclic antidepressants. This type of medication can help relieve depression as well as inhibit the activity of neurons that control the intestines to help reduce pain. If you have diarrhea and abdominal pain without depression, your doctor may suggest a lower than normal dose of imipramine (Tofranil), desipramine (Norpramine) or nortriptyline (Pamelor). Side effects — which might be reduced if you take the medication at bedtime — can include drowsiness, blurred vision, dizziness and dry mouth.
- SSRI antidepressants. Selective serotonin reuptake inhibitor (SSRI) antidepressants, such as fluoxetine (Prozac, Sarafem) or paroxetine (Paxil), may help if you’re depressed and have pain and constipation.
- Pain medications. Pregabalin (Lyrica) or gabapentin (Neurontin) might ease severe pain or bloating.
IBS medication
Medications approved for certain people with IBS include:
- Alosetron (Lotronex). Alosetron is designed to relax the colon and slow the movement of waste through the lower bowel. Alosetron can be prescribed only by doctors enrolled in a special program, is intended for severe cases of diarrhea-predominant IBS in women who haven’t responded to other treatments, and isn’t approved for use by men. It has been linked to rare but important side effects, so it should only be considered when other treatments aren’t successful.
- Eluxadoline (Viberzi). Eluxadoline can ease diarrhea by reducing muscle contractions and fluid secretion in the intestine, and increasing muscle tone in the rectum. Side effects can include nausea, abdominal pain and mild constipation. Eluxadoline has also been associated with pancreatitis, which can be serious and more common in certain individuals.
- Rifaximin (Xifaxan). This antibiotic can decrease bacterial overgrowth and diarrhea.
- Lubiprostone (Amitiza). Lubiprostone can increase fluid secretion in your small intestine to help with the passage of stool. It’s approved for women who have IBS with constipation, and is generally prescribed only for women with severe symptoms that haven’t responded to other treatments.
- Linaclotide (Linzess). Linaclotide also can increase fluid secretion in your small intestine to help you pass stool. Linaclotide can cause diarrhea, but taking the medication 30 to 60 minutes before eating might help.
Potential future treatments
Researchers are investigating new treatments for IBS. Serum-derived bovine immunoglobulin/protein isolate (SBI), a nutritional therapy, has shown some promise as a treatment for IBS with diarrhea.
Studies also show that, in people who have IBS with diarrhea, a specially coated tablet that slowly releases peppermint oil in the small intestine (enteric-coated peppermint oil) eases bloating, urgency, abdominal pain and pain while passing stool. It isn’t clear how enteric-coated peppermint oil might affect IBS, so ask your doctor before using it.
Researchers are investigating new treatments for IBS, such as fecal microbiota transplantation (FMT). Considered investigational at this time, fecal microbiota transplantation (FMT) restores healthy intestinal bacteria by placing another person’s processed stool into the colon of a person affected by IBS. Clinical trials to study fecal transplants are currently underway.
Lifestyle and home remedies
Simple changes in your diet and lifestyle often provide relief from IBS. Your body will need time to respond to these changes. Try to:
- Experiment with fiber. Fiber helps reduce constipation but also can worsen gas and cramping. Try slowly increasing the amount of fiber in your diet over a period of weeks with foods such as whole grains, fruits, vegetables and beans. A fiber supplement might cause less gas and bloating than fiber-rich foods.
- Avoid problem foods. Eliminate foods that trigger your symptoms.
- Drink plenty of water. Drink at least eight 8-ounce glasses of water a day (2 liters). Water keeps your gastrointestinal tract lubricated and can help treat or prevent constipation.
- Limit dairy products, like cheese and milk. Lactose intolerance is more common in people with IBS. If you cut back on dairy, make sure to eat nondairy foods rich in calcium, like broccoli, spinach or salmon.
- Limit foods that can make you gassy. Foods like beans, brussels sprouts and cabbage are notorious for causing gas, but carbonated sodas and even chewing gum can make you gassy. Reduce these foods to go easier on your gut.
- Avoid gluten. People with IBS — even those without celiac disease — tend to be more sensitive to gluten. If you opt for a gluten-free diet, work with your doctor and dietitian to ensure you’re getting enough of the key vitamins and minerals (like fiber, iron and calcium) often found in foods with gluten.
- Eat at regular times. Don’t skip meals, and try to eat at about the same time each day to help regulate bowel function. If you have diarrhea, you may find that eating small, frequent meals makes you feel better. But if you’re constipated, eating larger amounts of high-fiber foods may help move food through your intestines.
- Exercise regularly. Exercise helps relieve depression and stress, stimulates normal contractions of your intestines, and can help you feel better about yourself. Aim for 150 minutes of moderate exercise weekly. This is about 30 minutes a day, five days a week.
- Try relaxation techniques. Daily yoga, meditation and other de-stressing techniques can help calm an overtaxed nervous system and a “nervous gut”. Sometimes, a behavioral therapist can help.
- Get enough sleep. Aim for seven to nine hours of quality sleep each night. Go to bed at the same time each night. A good night’s rest is one of the most powerful de-stressors available. Reach out to your doctor if you’re having trouble sleeping.
Many people with IBS benefit from seeing a therapist. Therapy can help you get a handle on stress and conditions such as anxiety and depression that contribute to IBS. Some people find relief through:
- Cognitive behavioral therapy (CBT). Cognitive behavioral therapy (CBT) is a type of psychotherapy (talk therapy) that helps people learn to challenge negative thoughts and behaviors. It can help with a variety of mental health conditions such as depression and anxiety, and emotional concerns, and PTSD. CBT can also help manage nonpsychological health conditions, such as insomnia and chronic pain. Mental health professionals, including psychologists, therapists and counselors, use CBT to treat or manage mental health conditions and emotional concerns. It’s one of the most common and best-studied forms of psychotherapy.
- Hypnotherapy. Hypnotherapy is a psychological therapy that uses hypnosis to treat mental and physical health conditions. Hypnosis allows you to be more open to suggestions about making healthful changes in your perceptions, sensations, emotions, memories, thoughts or behaviors. It can also help change habits. A trained, certified hypnotist or hypnotherapist will guide you.
- Biofeedback. Biofeedback is a type of mind-body technique that helps you take control of certain involuntary bodily functions, such as your heart rate, breathing patterns and muscle responses. There are several types of biofeedback therapy. It can help manage conditions like chronic pain, anxiety and incontinence. During biofeedback, you’re connected to electrical pads and a healthcare provider uses noninvasive monitoring equipment and instruments to measure your body’s involuntary functions. Based on feedback from the instruments, your healthcare provider suggests how you can create voluntary (conscious) changes for these mostly involuntary functions. With education and practice, you can learn to make those bodily changes without equipment.
Bloating, cramps and farting remedies
- eat oats (such as porridge) regularly
- eat up to 1 tablespoon of linseeds (whole or ground) a day
- avoid foods that are hard to digest (like cabbage, broccoli, cauliflower, brussels sprouts, beans, onions and dried fruit)
- avoid products containing a sweetener called sorbitol
- ask your pharmacist about medicines that can help, like Buscopan or peppermint oil
Diarrhea remedies
- cut down on high-fiber foods like wholegrain foods (such as brown bread and brown rice), nuts and seeds
- avoid products containing a sweetener called sorbitol
- ask your pharmacist about medicines that can help, like Imodium (loperamide)
Constipation remedies
- drink plenty of water to help make your stool softer
- increase how much soluble fiber you eat – good foods include oats, pulses, carrots, peeled potatoes and linseeds (whole or ground)
- ask your pharmacist about medicines that can help (laxatives), like Metamucil or Citrucel.
Alternative medicine
The role of alternative therapies in relieving IBS symptoms is unclear. Ask your doctor before starting any of these treatments. Alternative therapies include:
- Hypnosis. A trained professional teaches you how to enter a relaxed state and then guides you in relaxing your abdominal muscles. Hypnosis may reduce abdominal pain and bloating. Several studies support the long-term effectiveness of hypnosis for IBS.
- Mindfulness training. Mindfulness is the act of being intensely aware of what you’re sensing and feeling at every moment, without interpretation or judgment. Research indicates that mindfulness can ease symptoms of IBS.
- Acupuncture. Researchers have found that acupuncture may help improve symptoms for people with IBS.
- Peppermint. Peppermint is a natural antispasmodic that relaxes smooth muscles in the intestines. It might provide short-term relief of IBS symptoms, but study results have been inconsistent.
- Probiotics. Probiotics are “good” bacteria that normally live in your intestines and are found in certain foods, such as yogurt, and in dietary supplements. Recent studies suggest that certain probiotics may relieve IBS symptoms, such as abdominal pain, bloating and diarrhea.
- Stress reduction. Yoga or meditation can help relieve stress. You can take classes or practice at home using books or videos.
IBS treatment guidelines
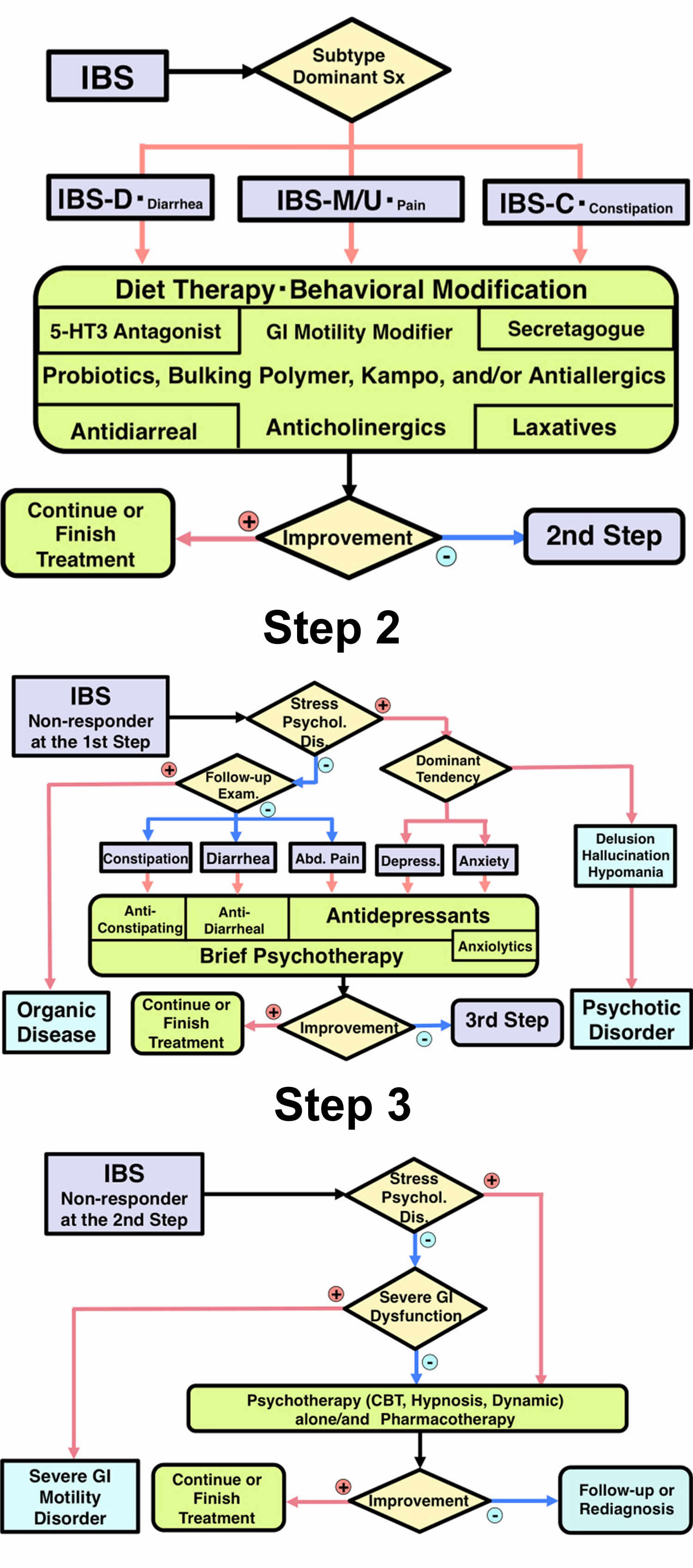
Patients diagnosed with IBS are initially treated with step 1 therapy (see Figure 3 below). Dietary therapy such as the low FODMAP diet and behavioral modification including exercise are indicated regardless of IBS subtype 43, 44, 45, 46, 47. Most patients need medications in addition to lifestyle modifications. Probiotics 48, bulking polymers 49, 50 and gastrointestinal motility modifiers 51, 52, 53 can be prescribed regardless of IBS subtype. For patients with IBS-D or with diarrhea as the main feature, 5-hydroxytryptamine 3 (type 3 serotonin receptor antagonists) should be used 54, 55, 56, 57, 58. For intractable cases, antidiarrheal agents including loperamide 59, 60, 61 or eluxadoline 62, 63 and bile acid sequestrants 64, 65 are the next in line for IBS-D. Intestinal secretagogues (gastrointestinal epithelium modifiers) 66, 67, 68 are indicated for cases with IBS-C or constipation as the main feature. Laxatives 69, 70, 71 except for long-term use of anthraquinones 72, 73, bile acids 74 and ileal bile acid transporter inhibitors 75, 76 are the next in line for IBS-C. In IBS-M, IBS-U, or abdominal pain-dominant cases, anticholinergic agents can be used 77, 78, 79. In some cases, kampo 80, 81, 82, anti-allergic agents 83, 84, antibiotics 85, 86, 87, 88, or peppermint oil 89, 90, 91, 92 may be administered. After treatment with step 1 for 4 weeks, non-responders will advance to step 2.
Step 2 therapy begins with an evaluation of the role of psychosocial stress and co-morbid psychiatric diagnosis in each patient 93. In patients with less influence from psychosocial factors, follow-up examinations and/or further gastrointestinal tract or other organ system examination 94, 95, 96, 97, 98 should be performed to rule out organic gastrointestinal or systemic disease. After confirmation of the accurate diagnosis of IBS, gastrointestinal agents that were not prescribed in step 1 therapy are indicated. Anti-constipation agents for constipation, anti-diarrheal agents for diarrhea, and antidepressants for abdominal pain are recommended. Antidepressants are indicated for IBS patients with depression. For IBS patients with anxiety, anxiolytic antidepressants are indicated 99. In these patients, anxiolytic drugs should mainly be prescribed from among 5-HT1A (serotonin) agonists 100 or, if necessary, benzodiazepine derivatives and only for short durations 101. In some cases, brief psychotherapy 102 can be added to manage psychosocial stress and negative emotion. If patients have delusion, hallucination, or hypomanic episodes, psychotic disorders should be suspected 11. Therefore, early collaboration with psychiatrists is indicated. The effect of step 2 therapy is evaluated for 4 weeks. Non-responders will proceed to step 3.
Step 3 therapy begins with a repeat evaluation of the role of psychosocial stress or psychopathology in each patient. If negative, gastrointestinal imaging or motility examination is indicated to determine coexisting pathophysiology of IBS such as mild lower gastrointestinal tract dysmotility or visceral hypersensitivity and/or to rule out severe gastrointestinal motility disorders. The majority of IBS patients usually have stress-related pathophysiology. A combination of gastrointestinal agents, psychopharmacological treatments and/or specific psychotherapy, particularly cognitive behavior therapy or hypnotherapy, will be helpful in these cases. If patients do not respond to this level either, re-diagnosis or careful observation is required.
Figure 3. IBS treatment algorithm
Living with IBS
Living with IBS can be challenging because symptoms come and go throughout your life. Treatment often involves trial and error. But the good news is that nearly everyone with IBS can find a treatment that helps them over time.
Usually, changing the foods you eat and your activity levels improve symptoms with time. You may need some patience as you figure out your triggers and take steps to avoid them. Your symptoms may not completely disappear. But, after a few weeks or months, you should notice a significant improvement in how you feel.
IBS Diet
There is no ‘one size fits all’ diet for IBS. However, dietary changes can often relieve IBS symptoms.
It may help to keep a food diary so you can identify any foods that make your symptoms worse.
It can also help to modify the amount and type of fiber in your diet:
- If you have IBS with constipation, it can help to eat more soluble fiber and drink more water
- If you have IBS with diarrhea, it can help to cut down on insoluble fiber.
In some cases, avoiding a particular food or food group might help – examples include gluten, caffeine, alcohol, spicy foods, high fat foods or foods that cause excessive bloating such as beans, lentils or certain vegetables.
In past years IBS was treated from the perspective that it was a “motility disorder”. The use of fiber supplementation to improve intestinal motility or movement was a common recommendation. While some studies have questioned whether fiber supplementation alone is helpful for the treatment of IBS and its symptoms, there are other good reasons to consume a high fiber diet. High fiber diets are associated with lower blood sugar, lower cholesterol as well as a lower tendency to form diverticula or outpouchings of the colon. Moreover, some patients with IBS report having a good result with a high fiber diet. Certainly every patient should include at least 25 grams of fiber in their diet every day.
What is FODMAP?
Australian researchers have recently developed a special diet that may help control IBS symptoms in some people. It’s called the FODMAP diet, and it involves restricting your intake of certain dietary carbohydrates (sugars) that are poorly absorbed by the bowel.
Before making any major changes to your diet it is a good idea to talk to your doctor or a dietitian.
FODMAP stands for “Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols“. A diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) – low FODMAP diet. Since ingestion of FODMAPs increases the delivery of readily fermentable substrates and water to the distal small intestine and colon—which results in luminal distention and gas—the reduction of FODMAPs in a patient’s diet may improve functional gastrointestinal symptoms 103.
These fermentable short-chain carbohydrates are prevalent in the diet.
- Oligosaccharides: fructans and galactooligosaccharides (GOS)
- Disaccharides: lactose
- Monosaccharides: fructose
- Polyols: sorbitol and mannitol
Researchers suggest that the small intestine does not absorb FODMAPs very well. They increase the amount of fluid in the bowel. They also create more gas. That’s because bacteria in the colon they are easily fermented by colonic bacteria. The increased fluid and gas in the bowel leads to bloating and changes in the speed with which food is digested. This results in gas, pain and diarrhea. Eating less of these types of carbohydrates should decrease these symptoms.
As FODMAPs are poorly absorbed during the digestive process, they may pass to the large intestine (colon), where they are rapidly fermented by the bacteria that normally live in the colon. This makes chemicals called short chain fatty acids, as well as gas. This, in turn, leads to changes in the acidity and types of bacteria in the colon. The colon expands, which can lead to pain, bloating, and changes in bowel habits.
- Diets rich in FODMAPs may increase symptoms in patients with functional gut disorders (FGD) or irritable bowel syndrome (IBS). However, the FODMAPs themselves are not the root of the problem. For that reason, patients may need to include other options to treat their symptoms. This may include medicine, exercise, meditation, hypnotherapy, etc.
So far, studies have shown that a low FODMAP diet has a beneficial effect in a majority of patients with Irritable Bowel Syndrome (IBS) symptoms 104. One study even found that 76% of Irritable Bowel Syndrome (IBS) patients following the diet reported improvement with their symptoms. Probiotics also have great potential in the management of Irritable Bowel Syndrome (IBS); however, it is still unclear which strains and doses are the most beneficial. Further research is needed on the effect of different fibers or combinations of fibers, in Irritable Bowel Syndrome (IBS).
Low Fodmap Diet
FODMAP stands for Fermentable, Oligo-, Di-, Mono-saccharides And Polyols. FODMAPs are short-chain carbohydrates (sugars) that are highly fermentable (to ferment, is to go through a chemical change that results in alcohol) and poorly absorbed during digestion 105. The acronym FODMAPs was created to describe poorly absorbed, short-chain carbohydrates that can lead to excessive fluid and gas accumulation, resulting in bloating, abdominal pain, and distention (Figure 4).
The Low FODMAP diet was developed by researchers at Monash University more than five years ago, in Australia, by Susan Shepherd and Peter Gibson. This diet eliminates certain foods to improve the symptoms of functional gut disorders (FGD). Irritable bowel syndrome (IBS), a type of FGD, may be helped by this diet. IBS is the most commonly diagnosed gastrointestinal condition and over half of patients with IBS associate a trigger in their symptoms with eating a meal 106. The Monash team, led by Professor Peter Gibson, provided the first evidence that a Low FODMAP diet improves IBS symptoms. Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder affecting one in seven Australian adults and approximately 35 million Americans are impacted by IBS including many in Europe and many in Asian countries. IBS is characterised by chronic and relapsing symptoms; lower abdominal pain and discomfort, bloating, wind, distension and altered bowel habit (ranging from diarrhoea to constipation) but with no abnormal pathology. The diagnosis of IBS should be made by a medical practitioner.
FODMAPs are found in a wide variety of foods, including those containing lactose, fructose in excess of glucose, fructans, galacto-oligosaccharides, and polyols (sorbitol, mannitol, xylitol, and maltitol). All FODMAPs have poor absorption and rapid fermentation, and they are comprised of small, osmotically active molecules. FODMAPs are poorly absorbed for a number of reasons, including the absence of luminal enzymes capable of hydrolyzing the glycosidic bonds contained in carbohydrates, the absence or low activity of brush border enzymes (eg, lactase), or the presence of low-capacity epithelial transporters (fructose, glucose transporter 2 [GLUT-2], and glucose transporter 5 [GLUT-5]). Fructose, which is an important FODMAP in the Western diet, is absorbed across villous epithelium through low-capacity, carrier-mediated diffusion involving GLUT-5. The absorption of free fructose is markedly enhanced in the presence of glucose via GLUT-2. Therefore, if fructose is present in excess of glucose, the risk of fructose malabsorption is increased. In addition, some molecules, such as polyols, are too large for simple diffusion. The fermentation rate is determined by the chain length of the carbohydrate 107.
For example, oligosaccharides are rapidly fermented, compared to polysaccharides. Fermentation results in the production of carbon dioxide, hydrogen, and/or methane gas. Finally, small, osmotically active molecules draw more water and other liquid into the small bowel. Given these properties, a diet low in FODMAPs has become a potential therapy for IBS patients.
When FODMAPs reach the colon (large intestine), bacteria ferment these sugars, turning them into gas and chemicals. This stretches the walls of the colon, causing abdominal bloating, distension, and pain or cramping in many people. Other symptoms, such as diarrhea, constipation, and nausea, are also common side effects of FODMAP carbohydrates. Not everyone has the same reaction to FODMAPs. Ethnicity, genetics, and environmental factors (such as an individual’s microbiome, motility, immune system, and sensory system) may play a part in your body’s ability to tolerate these carbohydrates.
Figure 4. FODMAPs in your gut
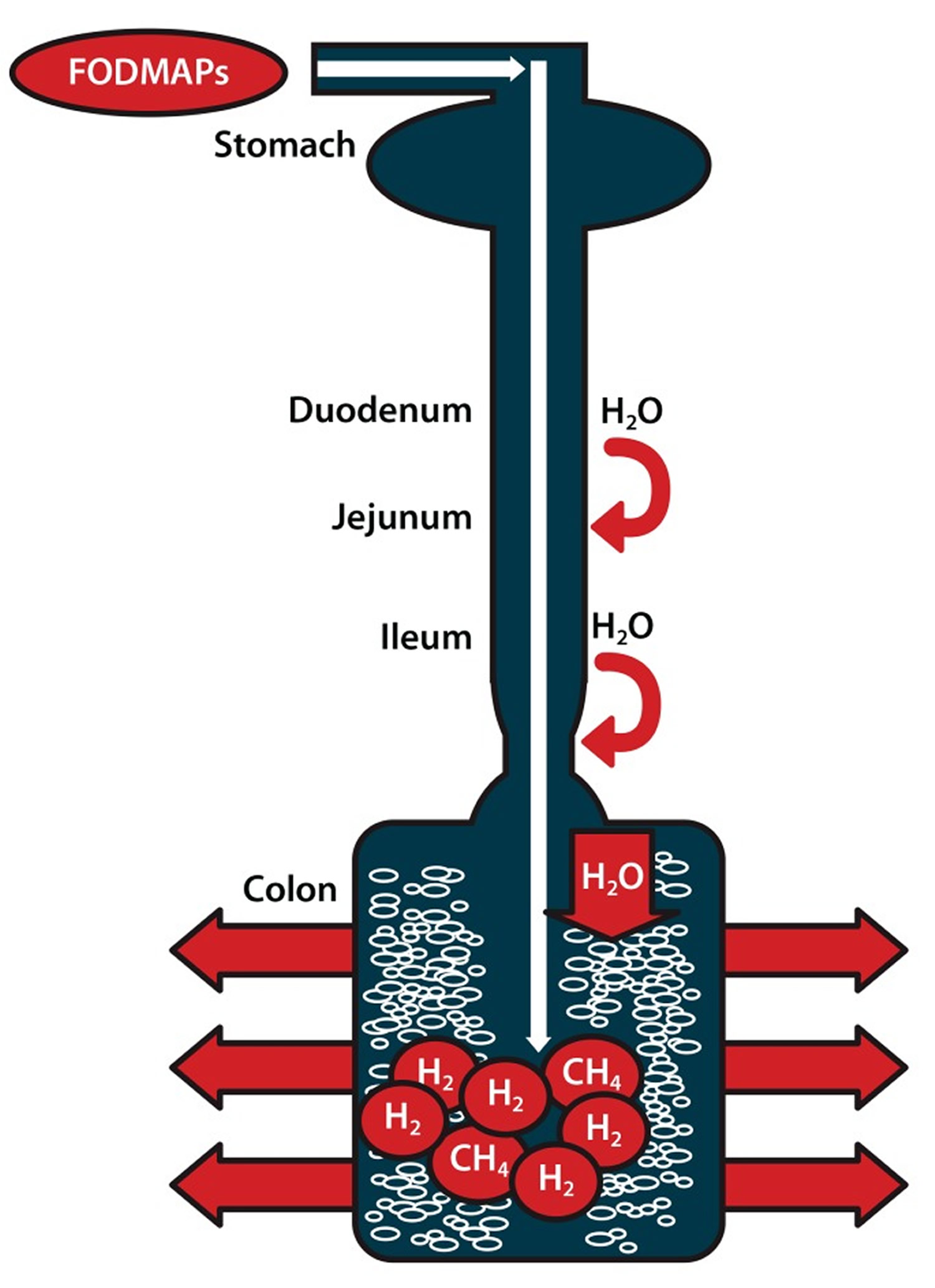
Note: Ingested fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) are poorly absorbed in the small intestine. Their small molecular size results in an osmotic effect, drawing water (H20) through to the large intestine. FODMAPs are then fermented by colonic microflora, producing hydrogen (H2) and/or methane gas (CH4). The increase in fluid and gas leads to diarrhea, bloating, flatulence, abdominal pain, and distension.
[Source 103]When is a Low-FODMAP diet recommended?
Despite limited data, implementation of a low-FODMAP diet should be considered in patients with IBS, particularly those in whom food is a trigger for symptoms.
Eliminating or restricting FODMAPs from the diet may greatly improve symptoms of functional gut disorders (FGD). In Australia, a Low-FODMAP diet is the main treatment for irritable bowel syndrome (IBS). It was adopted by their National Therapeutic Guidelines. The Low-FODMAP diet can be adjusted to meet personal food and lifestyle preferences. Following a personally developed Low-FODMAP plan does not cure IBS, but it may lead to drug-free management of symptoms and better quality of life. As with any diet, it is important to discuss with your doctor and working with a gastrointestinal trained dietician is also useful.
A number of studies suggest that limiting FODMAPs in the diet leads to improved symptoms in one-half to two-thirds of patients who follow this diet. Many patients see improvement in 1-2 weeks, though some may need to wait up to 4 weeks. Bloating and abdominal pain are the most likely symptoms to improve. Diarrhea is more likely to improve than constipation. If there is no improvement after 4 weeks, it is likely not worth continuing this diet.
A Low-FODMAP diet is not recommended for people without gastrointestinal symptoms. Also, if your IBS symptoms improve on the Low-FODMAP diet, you should eventually re-introduce FODMAPs, one at a time, to identify foods that trigger symptoms and those that do not. This will allow a more diverse diet. Keeping a personal food diary may help simplify this process
Implementation of a low-FODMAP diet is best done with the help of a dietician during a one-to-one consultation so that the dietician can understand the patient’s symptoms; this process also ensures that any diet modifications are individualized and still provide a balanced diet. A diet history should be taken to determine the composition of FODMAPs in an individuals diet. Education can then be tailored appropriately rather than focusing on FODMAPs that may never be consumed. Lists of food substitutions can help patients understand what they can and cannot eat (Table 1) 108. For good symptom control, individuals should restrict their total FODMAP load for 6-8 weeks. After this time, the diet may be modified to be less restrictive based on symptom response.
However, there are also several limitations to low-FODMAP diets. Most foods do not list their FODMAP content. In addition, the cutoff levels for FODMAP content are not clearly defined. When this diet was first examined, cutoff values were proposed based on foods that patients identified to be triggers for their symptoms. Foods and beverages with the following amounts of FODMAPs were considered to have risk for inducing symptoms: more than 0.5 g of fructose in excess of glucose per 100 g, more than 3 g of fructose in an average serving quantity regardless of glucose amount, and more than 0.2 g of fructans per serving 108. Although a low-FODMAP diet has been shown to be helpful in patients with IBS or other functional bowel disorders, further randomized controlled trials should be conducted.
Table 1. Foods High in Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs) and Suitable Alternatives
| FODMAP | Foods high in FODMAPs | Suitable alternatives low in FODMAPs |
|---|---|---|
| Excess fructose | Fruits: apple, clingstone peach, mango, nashi pear, pear, sugar snap pea, tinned fruit in natural juice, watermelon | Fruits: banana, blueberry, cantaloupe, carambola, durian, grape, grapefruit, honeydew melon, kiwi, lemon, lime, orange, passion fruit, pawpaw, raspberry, strawberry, tangelo |
| Honey sweeteners: fructose, high-fructose corn syrup | Honey substitutes: golden syrup, maple syrup | |
| Large total fructose dose: concentrated fruit sources, large servings of fruit, dried fruit, fruit juice | Sweeteners: any sweeteners except polyols | |
| Lactose | Milk: regular and low-fat cow, goat, and sheep milk; ice cream | Milk: lactose-free milk, rice milk Ice cream substitutes: gelato, sorbet |
| Yogurts: regular and low-fat yogurts | Yogurts: lactose-free yogurts | |
| Cheeses: soft and fresh cheeses | Cheeses: hard cheeses | |
| Oligosaccharides (fructans and/or galactans) | Vegetables: artichoke, asparagus, beetroot, broccoli, Brussels sprout, cabbage, fennel, garlic, leek, okra, onion, pea, shallot | Vegetables: bamboo shoot, bok choy, capsicum, carrot, celery, chives, choko, choy sum, corn, eggplant, green bean, lettuce, parsnip, pumpkin, silverbeet, spring onion (green part only) |
| Cereals: rye and wheat cereals when eaten in large amounts (eg, biscuit, bread, couscous, cracker, pasta) | Onion/garlic substitutes: garlic-infused oil | |
| Legumes: baked bean, chickpea, lentil, red kidney bean | Cereals: gluten-free and spelt bread/cereal products | |
| Fruits: custard apple, persimmon, rambutan, watermelon, white peach | Fruit: tomato | |
| Polyols | Fruits: apple, apricot, avocado, cherry, longon, lychee, nashi pear, nectarine, peach, pear, plum, prune, watermelon | Fruits: banana, blueberry, cantaloupe, carambola, durian, grape, grapefruit, honeydew melon, kiwi, lemon, lime, orange, passion fruit, pawpaw, raspberry |
| Vegetables: cauliflower, mushroom, snow pea | ||
| Sweeteners: isomalt, maltitol, mannitol, sorbitol, xylitol, and other sweeteners ending in “-ol” | Sweeteners: glucose, sugar (sucrose), other artificial sweeteners not ending in “-ol” |
FODMAP Food List
Table 2. FODMAP Food List
| Food | Avoid | Suitable |
|---|---|---|
| Lactose | Dairy whey and high-lactose containing milks such as cow, goat, sheep, chocolate, buttermilk, and condensed milk, and whipped cream. Ice cream, cow’s milk-based yogurt, brie, cottage cheese, ricotta, and sour cream. | Gelato or sorbet (though watch fructose content) and lactose-free yogurts. Aged hard cheeses tend to be easier to tolerate. Cheddar, Colby, parmesan, and mozzarella. Greek yogurt. Limit: Butter, margarine, sour cream, half and half, cream cheese, Swiss cheese, goat cheese, feta cheese, cheddar, parmesan, and mozzarella contain lactose, although at lower amounts. |
| Non-Dairy Milk Alternatives | Soy milk contains galactans and should be avoided as well, coconut milk, soy products, hummus, beans, and lentils. | Lactose- free or lactaid milk, rice milk, almond milk, almond butter, and cashew milk. |
| Fructose / Sweeteners | Honey, agave, apples, cherries, dates, guava, honeydew melon, lychee, mandarin oranges, mangoes, peaches, pears, persimmons, star fruit, canned fruit in natural juices, dried fruits and less ripe fruits, corn syrup, high fructose sweeteners, coconut milk, fruit pastes (i.e. chutney, plum sauce, barbeque sauce, ketchup), rosé wine, port, and sherry | Maple syrup, jams, marmalades, vegemite, table sugar, bananas, blackberries, blueberries, boysenberries, cranberries, grapefruit, kiwis, kumquats, lemons, limes, passion fruit, raspberries, and strawberries. Limit: grapes, oranges, papaya, pineapple, and watermelon. |
| Fructans | ||
| Starches | Bread, pasta, semolina, flour tortillas, wheat-based bread and breadcrumbs. Wheat-based cereals, crackers, cookies, cakes, pasta, and pastries. Beer. | Corn breads, gluten- free breads, pastas, cereals, as well as corn flakes, oatmeal, potato-based breads, rice-based noodles and breads, and wheat-free rye bread. |
| Fruit | Grapes, mangoes, peaches, persimmon, pineapple, watermelon, and bananas. | Grapefruit, lemons, limes, papaya, raspberries, strawberries, and blueberries. |
| Vegetables | Artichokes, asparagus, beets, broccoli, Brussel sprouts, cabbage, chicory, garlic, leeks, lettuce, okra, onions, radicchio, scallions, shallots, snow peas, and zucchini. | Bean sprouts, bell peppers, bok choy, carrots, celery, chives, cucumber, eggplant, potatoes, pumpkin, radishes, spinach, tomatoes, turnips, winter squash, and garlic-infused oil. |
| Galactans | Plant based proteins such as beans, black-eyed peas, chick peas, kidney beans, lentils, lima beans, pinto beans, soy products, broccoli, Brussel sprouts, cabbage, green beans, and yellow beans. | Eggs, nuts, quinoa, seeds, bean sprouts, bell peppers, bok choy, carrots, celery, chives, cucumbers, eggplant, potatoes, pumpkin, radish, spinach, and tomatoes. |
| Artificial Sweeteners | Sorbitol, mannitol, isomaltose, malitol, xylitol, polydextrose, hydrogenated starch | Aspartame, sucralose, saccharin. Commonly found in various gum and candy as well. |
| Polyols | ||
| Fruit | Apples, apricots, avocados, cherries, lychee, nectarines, peaches, pears, plums, and watermelon. | Bananas, blueberries, grapefruit, kiwi, lemons, limes, passion fruit, raspberries, cantaloupe, honeydew, and strawberries |
| Vegetables | Artichoke, asparagus, brussel sprouts, cabbage, cauliflower, green beans mushrooms, snow peas sprouts, and summer squash. | Bean sprouts, bell peppers, bok choy, carrots, celery, chives, cucumbers, eggplant, kale, lettuce, potatoes, pumpkin, radishes, spinach, tomatoes, winter squash, yams, and zucchini. |
Eat Less Of These Foods
Lactose
- Cow’s milk, yogurt, pudding, custard, ice cream, cottage cheese, ricotta cheese and mascarpone
Fructose
- Fruits, such as apples, pears, peaches, cherries, mangoes, pears and watermelon
- Sweeteners, such as honey and agave nectar
- Products with high fructose corn syrup
Fructans
- Vegetables, such as artichokes, asparagus, Brussels sprouts, broccoli, beetroot, garlic and onions
- Grains such as wheat and rye
- Added fiber, such as inulin
Oligosaccharides (fructans and/or galactans)
- Chickpeas, lentils, kidney beans and soy products
- Vegetables, such as broccoli
Polyols
- Fruits, such as apples, apricots, blackberries, cherries, nectarines, pears, peaches, plums and watermelon
- Vegetables, such as cauliflower, mushrooms and snow peas
- Sweeteners, such as sorbitol, mannitol, xylitol, maltitol and isomalt found in sugar-free gum and mints, and cough medicines and drops
Eat More Of These Foods
- Dairy: Lactose-free milk, rice milk, almond milk, coconut milk, lactose-free yogurt; hard cheeses such as feta and brie
- Fruit: Bananas, blueberries, cantaloupe, grapefruit, honeydew, kiwi, lemon, lime, oranges and strawberries
- Vegetables: Bamboo shoots, bean sprouts, bok choy, carrots, chives, cucumbers, eggplant, ginger, lettuce, olives, parsnips, potatoes, spring onions and turnips
- Protein: Beef, pork, chicken, fish, eggs and tofu
- Nuts/seeds (limit to 10-15 each): Almonds, macadamia, peanuts, pine nuts and walnuts
- Grain: Oat, oat bran, rice bran, gluten-free pasta, such as rice, corn, quinoa, white rice, corn flour and quinoa
The idea behind the low FODMAPs diet is to only limit the problematic foods in a category — not all of them. (After all, they do have health benefits.) You may tolerate some foods better than others.
Meet with a registered dietician if you are considering this diet. It’s important to make sure your eating plan is safe and healthy. He or she will have you eliminate FODMAPs from your diet. Then you gradually add the carbohydrates back in one at a time and monitor your symptoms. A food diary and symptom chart may be helpful tools.
- Napolitano M, Fasulo E, Ungaro F, Massimino L, Sinagra E, Danese S, Mandarino FV. Gut Dysbiosis in Irritable Bowel Syndrome: A Narrative Review on Correlation with Disease Subtypes and Novel Therapeutic Implications. Microorganisms. 2023 Sep 22;11(10):2369. doi: 10.3390/microorganisms11102369[↩][↩][↩]
- Staudacher HM, Black CJ, Teasdale SB, Mikocka-Walus A, Keefer L. Irritable bowel syndrome and mental health comorbidity – approach to multidisciplinary management. Nat Rev Gastroenterol Hepatol. 2023 Sep;20(9):582-596. doi: 10.1038/s41575-023-00794-z[↩][↩]
- Nabi MY, Nauhria S, Reel M, Londono S, Vasireddi A, Elmiry M, Ramdass PVAK. Endometriosis and irritable bowel syndrome: A systematic review and meta-analyses. Front Med (Lausanne). 2022 Jul 25;9:914356. doi: 10.3389/fmed.2022.914356[↩]
- Chlebicz-Wójcik A, Śliżewska K. Probiotics, Prebiotics, and Synbiotics in the Irritable Bowel Syndrome Treatment: A Review. Biomolecules. 2021 Aug 4;11(8):1154. doi: 10.3390/biom11081154[↩]
- Shin A, Kashyap PC. Multi-omics for biomarker approaches in the diagnostic evaluation and management of abdominal pain and irritable bowel syndrome: what lies ahead. Gut Microbes. 2023 Jan-Dec;15(1):2195792. doi: 10.1080/19490976.2023.2195792[↩]
- Wu Y, Li Y, Zheng Q, Li L. The Efficacy of Probiotics, Prebiotics, Synbiotics, and Fecal Microbiota Transplantation in Irritable Bowel Syndrome: A Systematic Review and Network Meta-Analysis. Nutrients. 2024 Jul 2;16(13):2114. doi: 10.3390/nu16132114[↩]
- Ghoshal UC, Sachdeva S, Pratap N, Karyampudi A, Mustafa U, Abraham P, Bhatt CB, Chakravartty K, Chaudhuri S, Goyal O, Makharia GK, Panigrahi MK, Parida PK, Patwari S, Sainani R, Sadasivan S, Srinivas M, Upadhyay R, Venkataraman J. Indian consensus statements on irritable bowel syndrome in adults: A guideline by the Indian Neurogastroenterology and Motility Association and jointly supported by the Indian Society of Gastroenterology. Indian J Gastroenterol. 2023 Apr;42(2):249-273. doi: 10.1007/s12664-022-01333-5[↩]
- Huang KY, Wang FY, Lv M, Ma XX, Tang XD, Lv L. Irritable bowel syndrome: Epidemiology, overlap disorders, pathophysiology and treatment. World J Gastroenterol. 2023 Jul 14;29(26):4120-4135. doi: 10.3748/wjg.v29.i26.4120[↩][↩]
- García Mansilla MJ, Rodríguez Sojo MJ, Lista AR, Ayala Mosqueda CV, Ruiz Malagón AJ, Gálvez J, Rodríguez Nogales A, Rodríguez Sánchez MJ. Exploring Gut Microbiota Imbalance in Irritable Bowel Syndrome: Potential Therapeutic Effects of Probiotics and Their Metabolites. Nutrients. 2024 Dec 31;17(1):155. doi: 10.3390/nu17010155[↩]
- Gwee KA, Ghoshal UC, Chen M. Irritable bowel syndrome in Asia: pathogenesis, natural history, epidemiology, and management. J Gastroenterol Hepatol. 2018;33:99–110. doi: 10.1111/jgh.13987[↩]
- Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology. 2021 Jan;160(1):99-114.e3. https://www.gastrojournal.org/article/S0016-5085(20)30487-X/fulltext[↩][↩]
- Irritable Bowel Syndrome. http://s3.gi.org/patients/cgp/pdf/ibs.pdf[↩][↩]
- Enck P, Aziz Q, Barbara G, Farmer AD, Fukudo S, Mayer EA, Niesler B, Quigley EM, Rajilić-Stojanović M, Schemann M, Schwille-Kiuntke J, Simren M, Zipfel S, Spiller RC. Irritable bowel syndrome. Nat Rev Dis Primers. 2016 Mar 24;2:16014. doi: 10.1038/nrdp.2016.14[↩][↩][↩]
- Ford AC, Sperber AD, Corsetti M, Camilleri M. Irritable bowel syndrome. Lancet. 2020 Nov 21;396(10263):1675-1688. https://eprints.whiterose.ac.uk/166983/3/THELANCET-D-20-00123R3%20CLEAN.pdf[↩][↩][↩][↩][↩]
- Lacy BE, Patel NK. Rome Criteria and a Diagnostic Approach to Irritable Bowel Syndrome. J Clin Med. 2017 Oct 26;6(11):99. doi: 10.3390/jcm6110099[↩]
- Sperber AD, Dumitrascu D, Fukudo S, Gerson C, Ghoshal UC, Gwee KA, Hungin APS, Kang JY, Minhu C, Schmulson M, Bolotin A, Friger M, Freud T, Whitehead W. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: a Rome Foundation working team literature review. Gut. 2017 Jun;66(6):1075-1082. doi: 10.1136/gutjnl-2015-311240[↩]
- Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Grant Thompson W, et al. U. S. Householder survey of functional gastrointestinal disorders. Dig Dis Sci. 1993;38:1569–80. doi: 10.1007/BF01303162[↩]
- IRRITABLE BOWEL SYNDROME. http://s3.gi.org/patients/gihealth/pdf/ibs.pdf[↩][↩]
- Eijsbouts C, Zheng T, Kennedy NA, Bonfiglio F, Anderson CA, Moutsianas L, et al. Genome-wide analysis of 53,400 people with irritable bowel syndrome highlights shared genetic pathways with mood and anxiety disorders. Nat Genet. 2021;53:1543–52. doi: 10.1038/s41588-021-00950-8[↩]
- Lewis S.J., Heaton K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997;32:920–924. doi: 10.3109/00365529709011203[↩][↩][↩][↩][↩]
- Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel Disorders. Gastroenterology. 2016 doi: 10.1053/j.gastro.2016.02.031[↩]
- Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel Disorders. Gastroenterology. 2016 Feb 18:S0016-5085(16)00222-5. https://www.gastrojournal.org/article/S0016-5085(16)00222-5/fulltext[↩][↩][↩][↩][↩]
- Vijayvargiya P, Camilleri M, Burton D, Busciglio I, Lueke A, Donato LJ. Bile and fat excretion are biomarkers of clinically significant diarrhoea and constipation in irritable bowel syndrome. Aliment Pharmacol Ther. 2019;49:744–758. doi: 10.1111/apt.15106[↩]
- Karatay E, Utku ÖG. Serum resolvin D1 levels as a marker of inflammation in constipation dominant irritable bowel syndrome. Turk J Gastroenterol. 2020;31:113–119. doi: 10.5152/tjg.2020.19751[↩]
- Camilleri M, Boeckxstaens G. Irritable bowel syndrome: treatment based on pathophysiology and biomarkers. Gut. 2023;72:590–599. doi: 10.1136/gutjnl-2022-328515[↩]
- Chey WD, Kurlander J, Eswaran S. Irritable bowel syndrome: a clinical review. JAMA. 2015 Mar 3;313(9):949-58. doi: 10.1001/jama.2015.0954[↩][↩]
- Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel Disorders. Gastroenterology. 2016 Feb 18:S0016-5085(16)00222-5. doi: 10.1053/j.gastro.2016.02.031[↩]
- Mayer EA, Ryu HJ, Bhatt RR. The neurobiology of irritable bowel syndrome. Mol Psychiatry. 2023 Apr;28(4):1451-1465. doi: 10.1038/s41380-023-01972-w[↩]
- Drossman DA, Hasler WL. Rome IV-Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology. 2016 May;150(6):1257-61. https://www.gastrojournal.org/article/S0016-5085(16)30048-8/fulltext[↩]
- Ford A.C., Sperber A.D., Corsetti M., Camilleri M. Irritable Bowel Syndrome. Lancet. 2020;396:1675–1688. doi: 10.1016/S0140-6736(20)31548-8[↩]
- Enck P., Aziz Q., Barbara G., Farmer A.D., Fukudo S., Mayer E.A., Niesler B., Quigley E.M.M., Rajilić-Stojanović M., Schemann M., et al. Irritable Bowel Syndrome. Nat. Rev. Dis. Primers. 2016;2:16014. doi: 10.1038/nrdp.2016.14[↩]
- Osadchiy V., Martin C.R., Mayer E.A. The Gut-Brain Axis and the Microbiome: Mechanisms and Clinical Implications. Clin. Gastroenterol. Hepatol. 2019;17:322–332. doi: 10.1016/j.cgh.2018.10.002[↩]
- Zamani M., Alizadeh-Tabari S., Zamani V. Systematic Review with Meta-Analysis: The Prevalence of Anxiety and Depression in Patients with Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2019;50:132–143. doi: 10.1111/apt.15325[↩]
- Erdrich S., Hawrelak J.A., Myers S.P., Harnett J.E. A Systematic Review of the Association between Fibromyalgia and Functional Gastrointestinal Disorders. Ther. Adv. Gastroenterol. 2020;13:175628482097740. doi: 10.1177/1756284820977402[↩]
- Kleykamp B.A., Ferguson M.C., McNicol E., Bixho I., Arnold L.M., Edwards R.R., Fillingim R., Grol-Prokopczyk H., Turk D.C., Dworkin R.H. The Prevalence of Psychiatric and Chronic Pain Comorbidities in Fibromyalgia: An ACTTION Systematic Review. Semin. Arthritis Rheum. 2021;51:166–174. doi: 10.1016/j.semarthrit.2020.10.006[↩]
- Gholamnezhad F., Qeisari A., Shahriarirad R. Gastroesophageal Reflux Disease Incidence among Male Patients with Irritable Bowel Syndrome: A Cross-sectional Study in Southern Iran. JGH Open. 2023;7:152–156. doi: 10.1002/jgh3.12867[↩]
- Ng Q.X., Soh A.Y.S., Loke W., Lim D.Y., Yeo W.-S. The Role of Inflammation in Irritable Bowel Syndrome (IBS) J. Inflamm. Res. 2018;11:345–349. doi: 10.2147/JIR.S174982[↩]
- Lovell R.M., Ford A.C. Global Prevalence of and Risk Factors for Irritable Bowel Syndrome: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2012;10:712–721.e4. doi: 10.1016/j.cgh.2012.02.029[↩]
- Zia J.K., Lenhart A., Yang P.-L., Heitkemper M.M., Baker J., Keefer L., Saps M., Cuff C., Hungria G., Videlock E.J., et al. Risk Factors for Abdominal Pain-Related Disorders of Gut-Brain Interaction in Adults and Children: A Systematic Review. Gastroenterology. 2022;163:995–1023.e3. doi: 10.1053/j.gastro.2022.06.028[↩]
- Agnello M., Carroll L.N., Imam N., Pino R., Palmer C., Varas I., Greene C., Hitschfeld M., Gupta S., Almonacid D.E., et al. Gut Microbiome Composition and Risk Factors in a Large Cross-Sectional IBS Cohort. BMJ Open Gastroenterol. 2020;7:e000345. doi: 10.1136/bmjgast-2019-000345[↩]
- Patel P, Bercik P, Morgan DG, Bolino C, Pintos-Sanchez MI, Moayyedi P, Ford AC. Prevalence of organic disease at colonoscopy in patients with symptoms compatible with irritable bowel syndrome: cross-sectional survey. Scand J Gastroenterol. 2015 Jul;50(7):816-23. doi: 10.3109/00365521.2015.1007079[↩]
- Dietary Guidelines for Americans. https://www.dietaryguidelines.gov/[↩]
- Staudacher HM, Whelan K, Irving PM, et al. Comparison of symptom response following advice for a diet low in fermentable carbohydrates (FODMAPs) versus standard dietary advice in patients with irritable bowel syndrome. J Hum Nutr Diet. 2011;24:487–495. doi: 10.1111/j.1365-277X.2011.01162.x[↩]
- Böhn L, Störsrud S, Liljebo T, et al. Diet low in FODMAPs reduces symptoms of irritable bowel syndrome as well as traditional dietary advice: a randomized controlled trial. Gastroenterology. 2015;149(1399–1407):e2. doi: 10.1053/j.gastro.2015.07.054[↩]
- Johannesson E, Simren M, Strid H, et al. Physical activity improves symptoms in irritable bowel syndrome: a randomized controlled trial. Am J Gastroenterol. 2011;106:915–922. doi: 10.1038/ajg.2010.480[↩]
- Johannesson E, Ringström G, Abrahamsson H, et al. Intervention to increase physical activity in irritable bowel syndrome shows long-term positive effects. World J Gastroenterol. 2015;21:600–608. doi: 10.3748/wjg.v21.i2.600[↩]
- Zhou C, Zhao E, Li Y, et al. Exercise therapy of patients with irritable bowel syndrome: a systematic review of randomized controlled trials. Neurogastroenterol Motil. 2019;31:e13461. doi: 10.1111/nmo.13461[↩]
- Ford AC, Harris LA, Jacy BE, et al. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther. 2018;48:1044–1060. doi: 10.1111/apt.15001[↩]
- Toskes PP, Connery KL, Ritchey TW. Calcium polycarbophil compared with placebo in irritable bowel syndrome. Aliment Pharmacol Ther. 1993;7:87–92. doi: 10.1111/j.1365-2036.1993.tb00074.x[↩]
- Masamune K, Miwa T, Fukutomi H, et al. Phase III trial of calcium polycarbophil in patients with irritable bowel syndrome: double-blind, randomized, controlled trial comparing trimebutine maleate. Yakuri-to-Chiryou. 1998;26:967–996.[↩]
- Lee HT, Kim BJ. Tromebutine as a modulator of gastrointestinal motility. Arch Pharm Res. 2011;34:861–864. doi: 10.1007/s12272-011-0600-7[↩]
- Kang SH, Jeen YT, Koo JS, et al. Efficacy of fenoverine and trimebutine in the management of irritable bowel syndrome: multicenter randomized double-blind non-inferiority clinical study. Korean J Gastroenterol. 2013;62:278–287. doi: 10.4166/kjg.2013.62.5.278[↩]
- Karabulut GS, Beser OF, Erginoz E, et al. The incidence of irritable bowel syndrome in children using the Rome III criteria and the effect of trimebutine treatment. J Neurogastroenterol Motil. 2013;19:90–93. doi: 10.5056/jnm.2013.19.1.90[↩]
- Black CJ, Burr NE, Camilleri M, et al. Efficacy of pharmacological therapies in patients with IBS with diarrhoea or mixed stool pattern: systematic review and network meta-analysis. Gut. 2019;69:74–82. doi: 10.1136/gutjnl-2018-318160[↩]
- Zheng Y, Yu T, Tang Y, et al. Efficacy and safety of 5-hydroxytryptamine 3 receptor antagonists in irritable bowel syndrome: a systematic review and meta-analysis of randomized controlled trials. PLoS ONE. 2017;12:e0172846. doi: 10.1371/journal.pone.0172846[↩]
- Andresen V, Montori VM, Keller J, et al. Effects of 5-hydroxytryptamine (serotonin) type 3 antagonists on symptom relief and constipation in nonconstipated irritable bowel syndrome: a systematic review and meta-analysis of randomized controlled trials. Clin Gastroenterol Hepatol. 2008;6:545–555. doi: 10.1016/j.cgh.2007.12.015[↩]
- Cremonini F, Nicandro JP, Atkinson V, et al. Randomised clinical trial: alosetron improves quality of life and reduces restriction of daily activities in women with severe diarrhoea-predominant IBS. Aliment Pharmacol Ther. 2012;36:437–448. doi: 10.1111/j.1365-2036.2012.05208.x[↩]
- Chey WD, Chey WY, Heath AT, et al. Long-term safety and efficacy of alosetron in women with severe diarrhea-predominant irritable bowel syndrome. Am J Gastroenterol. 2004;99:2195–2203. doi: 10.1111/j.1572-0241.2004.30509.x[↩]
- Lavö B, Stenstam M, Nielsen AL. Loperamide in treatment of irritable bowel syndrome: a double-blind placebo controlled study. Scand J Gastroenterol Suppl. 1987;130:77–80. doi: 10.3109/00365528709091003[↩]
- Hovdenak N. Loperamide treatment of the irritable bowel syndrome. Scand J Gastroenterol Suppl. 1987;130:81–84. doi: 10.3109/00365528709091004[↩]
- Efskind PS, Bernklev T, Vatn MH. A double-blind placebo-controlled trial with loperamide in irritable bowel syndrome. Scand J Gastroenterol. 1996;31:463–468. doi: 10.3109/00365529609006766[↩]
- Dove LS, Lembo A, Randall CW, et al. Eluxadoline benefits patients with irritable bowel syndrome with diarrhea in a phase 2 study. Gastroenterology. 2013;145:329–338. doi: 10.1053/j.gastro.2013.04.006[↩]
- Lembo AJ, Lacy BE, Zuckerman MJ, et al. Eluxadoline for irritable bowel syndrome with diarrhea. N Engl J Med. 2016;374:242–253. doi: 10.1056/NEJMoa1505180[↩]
- Fernández-Bañares F, Rosinach M, Piqueras M, et al. Randomised clinical trial: colestyramine vs. hydroxypropyl cellulose in patients with functional chronic watery diarrhoea. Aliment Pharmacol Ther. 2015;41:1132–1140. doi: 10.1111/apt.13193[↩]
- Camilleri M, Acosta A, Busciglio I, et al. Effect of colesevelam on faecal bile acids and bowel functions in diarrhoea-predominant irritable bowel syndrome. Aliment Pharmacol Ther. 2015;41:438–448. doi: 10.1111/apt.13065[↩]
- Li F, Fu T, Tong WD, et al. Lubiprostone is effective in the treatment of chronic idiopathic constipation and irritable bowel syndrome: a systematic review and meta-analysis of randomized controlled trials. Mayo Clin Proc. 2016;91:456–468. doi: 10.1016/j.mayocp.2016.01.015[↩]
- Black CJ, Burr NE, Quigley EMM, et al. Efficacy of secretagogues in patients with irritable bowel syndrome with constipation: systematic review and network meta-analysis. Gastroenterology. 2018;155:1753–1763. doi: 10.1053/j.gastro.2018.08.021[↩]
- Shah ED, Kim HM, Schoenfeld P. Efficacy and tolerability of guanylate cyclase-C agonists for irritable bowel syndrome with constipation and chronic idiopathic constipation: a systematic review and meta-analysis. Am J Gastroenterol. 2018;113:329–338. doi: 10.1038/ajg.2017.495[↩]
- Nyberg C, Hendel J, Nielsen OH. The safety of osmotically acting cathartics in colonic cleansing. Nat Rev Gastroenterol Hepatol. 2010;7:557–564. doi: 10.1038/nrgastro.2010.136[↩]
- Chapman RW, Stanghellini V, Geraint M, et al. Randomized clinical trial: macrogol/PEG 3350 plus electrolytes for treatment of patients with constipation associated with irritable bowel syndrome. Am J Gastroenterol. 2013;108:1508–1515. doi: 10.1038/ajg.2013.197[↩]
- Kamm MA, Mueller-Lissner S, Wald A, et al. Oral bisacodyl is effective and well-tolerated in patients with chronic constipation. Clin Gastroenterol Hepatol. 2011;9:577–583. doi: 10.1016/j.cgh.2011.03.026[↩]
- Wald A. Is chronic use of stimulant laxatives harmful to the colon? J Clin Gastroenterol. 2003;36:386–389. doi: 10.1097/00004836-200305000-00004[↩]
- Alsalimy N, Madi L, Awaisu A. Efficacy and safety of laxatives for chronic constipation in long-term care settings: a systematic review. J Clin Pharm Ther. 2018;43:595–605. doi: 10.1111/jcpt.12721[↩]
- Rao AS, Wong BS, Camilleri M, et al. Chenodeoxycholate in females with irritable bowel syndrome-constipation: a pharmacodynamic and pharmacogenetic analysis. Gastroenterology. 2010;139:1549–1558. doi: 10.1053/j.gastro.2010.07.052[↩]
- Nakajima A, Seki M, Taniguchi S, et al. Safety and efficacy of elobixibat for chronic constipation: results from a randomised, double-blind, placebo-controlled, phase 3 trial and an open-label, single-arm, phase 3 trial. Lancet Gastroenterol Hepatol. 2018;3:537–547. doi: 10.1016/S2468-1253(18)30123-7[↩]
- Nakajima A, Taniguchi S, Kurosu S, et al. Efficacy, long-term safety, and impact on quality of life of elobixibat in more severe constipation: post hoc analyses of two phase 3 trials in Japan. Neurogastroenterol Motil. 2019;31:e13571. doi: 10.1111/nmo.13571[↩]
- Poynard T, Naveau S, Mory B, et al. Meta-analysis of smooth muscle relaxants in the treatment of irritable bowel syndrome. Aliment Pharmacol Ther. 1994;8:499–510. doi: 10.1111/j.1365-2036.1994.tb00322.x[↩]
- Ford AC, Talley NJ, Spiegel BM, et al. Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: a systematic review and meta-analysis. BMJ. 2009;337:e2313. doi: 10.1136/bmj.a2313[↩]
- Khalif IL, Quigley EM, Makarchuk PA, Golovenko OV, Podmarenkova LF, Dzhanayev YA. Interactions between symptoms and motor and visceral sensory responses of irritable bowel syndrome patients to spasmolytics (antispasmodics). J Gastrointestin Liver Dis. 2009 Mar;18(1):17-22. https://www.jgld.ro/jgld/index.php/jgld/article/view/2009.1.2/991[↩]
- Oka T, Okumi H, Nishida S, Ito T, Morikiyo S, Kimura Y, Murakami M. JOPM-EBM working team effects of kampo on functional gastrointestinal disorders. Biopsycho Soc Med. 2014;8:5. doi: 10.1186/1751-0759-8-5[↩]
- Manabe N, Camilleri M, Rao A, et al. Effect of daikenchuto (TU-100) on gastrointestinal and colonic transit in humans. Am J Physiol Gastrointest Liver Physiol. 2010;298:G970–975. doi: 10.1152/ajpgi.00043.2010[↩]
- Bizen A. Clinical efficacy of of hange-shashin-to in diarrhea-predominant irritable bowel syndrome patients with psychological stress: an open-label study Igaku-to- Yakugaku. Med Pharma. 2012;68:127–133.[↩]
- Stefanini GF, Saggioro A, Alvisi V, et al. Oral cromolyn sodium in comparison with elimination diet in the irritable bowel syndrome, diarrheic type. Multicenter study of 428 patients. Scand J Gastroenterol. 1995;30:535–541. doi: 10.3109/00365529509089786[↩]
- Wouters MM, Balemans D, Van Wanrooy S, et al. Histamine receptor H1-mediated sensitization of TRPV1 mediates visceral hypersensitivity and symptoms in patients with irritable bowel syndrome. Gastroenterology. 2016;150:875–887. doi: 10.1053/j.gastro.2015.12.034[↩]
- Pimentel M, Park S, Mirocha J, et al. The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial. Ann Intern Med. 2006;145:557–563. doi: 10.7326/0003-4819-145-8-200610170-00004[↩]
- Pimentel M. An evidence-based treatment algorithm for IBS based on a bacterial/SIBO hypothesis: part 2. Am J Gastroenterol. 2010;105:1227–1230. doi: 10.1038/ajg.2010.125[↩]
- Pimentel M, Lembo A, Chey WD, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation. N Engl J Med. 2011;364:22–32. doi: 10.1056/NEJMoa1004409[↩]
- Menees SB, Maneerattannaporn M, Kim HM, Chey WD. The efficacy and safety of rifaximin for the irritable bowel syndrome: a systematic review and meta-analysis. Am J Gastroenterol. 2012;107:28–35. doi: 10.1038/ajg.2011.355[↩]
- Cappello G, Spezzaferro M, Grossi L, et al. Peppermint oil (Mintoil) in the treatment of irritable bowel syndrome: a prospective double blind placebo-controlled randomized trial. Dig Liver Dis. 2007;39:530–536. doi: 10.1016/j.dld.2007.02.006[↩]
- Khanna R, MacDonald JK, Levesque BG. Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis. J Clin Gastroenterol. 2014;48:505–512. doi: 10.1097/MCG.0b013e3182a88357[↩]
- Moayyedi P, Andrews CN, MacQueen G, et al. Canadian Association of gastroenterology clinical practice guideline for the management of irritable bowel syndrome (IBS) J Can Assoc Gastroenterol. 2019;2:6–29. doi: 10.1093/jcag/gwy071[↩]
- Alammar N, Wang L, Saberi B, et al. The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data. BMC Complement Altern Med. 2019;19:21. doi: 10.1186/s12906-018-2409-0[↩]
- Fukudo S, Okumura T, Inamori M, Okuyama Y, Kanazawa M, Kamiya T, Sato K, Shiotani A, Naito Y, Fujikawa Y, Hokari R, Masaoka T, Fujimoto K, Kaneko H, Torii A, Matsueda K, Miwa H, Enomoto N, Shimosegawa T, Koike K. Evidence-based clinical practice guidelines for irritable bowel syndrome 2020. J Gastroenterol. 2021 Mar;56(3):193-217. doi: 10.1007/s00535-020-01746-z. Erratum in: J Gastroenterol. 2023 Nov;58(11):1165. doi: 10.1007/s00535-023-02044-0[↩][↩]
- Kim ES, Cheon JH, Park JJ, et al. Colonoscopy as an adjunctive method for the diagnosis of irritable bowel syndrome: focus on pain perception. J Gastroenterol Hepatol. 2010;25:1232–1238. doi: 10.1111/j.1440-1746.2010.06338.x[↩]
- Güçlü M, Pourbagher A, Serin E, et al. Ultrasonographic evaluation of gallbladder functions in patients with irritable bowel syndrome. J Gastroenterol Hepatol. 2006;21:1309–1312. doi: 10.1111/j.1440-1746.2006.04136.x[↩]
- Fukunaga M, Ishimura N, Fukuyama C, et al. Celiac disease in non-clinical populations of Japan. J Gastroenterol. 2018;53:208–214. doi: 10.1007/s00535-017-1339-9[↩]
- Smalley W, Falck-Ytter C, Carrasco-Labra A, et al. AGA clinical practice guidelines on the laboratory evaluation of functional diarrhea and diarrhea-predominant irritable bowel syndrome in adults (IBS-D) Gastroenterology. 2019;157:851–854. doi: 10.1053/j.gastro.2019.07.004[↩]
- Ford AC, Chey WD, Talley NJ, et al. Yield of diagnostic tests for celiac disease in individuals with symptoms suggestive of irritable bowel syndrome: systematic review and meta-analysis. Arch Intern Med. 2009;169:651–658. doi: 10.1001/archinternmed.2009.22[↩]
- Ford AC, Lacy BE, Harris LA, et al. Effect of antidepressants and psychological therapies in irritable bowel syndrome: an updated systematic review and meta-analysis. Am J Gastroenterol. 2019;114:21–39. doi: 10.1038/s41395-018-0222-5[↩]
- Lan L, Chen YL, Zhang H, et al. Efficacy of tandospirone in patients with irritable bowel syndrome-diarrhea and anxiety. World J Gastroenterol. 2014;20:11422–11428. doi: 10.3748/wjg.v20.i32.11422[↩]
- Pace F, Maurano A, Ciacci C, et al. Octatropine methyl bromide and diazepam combination (Valpinax) in patients with irritable bowel syndrome: a multicentre, randomized, placebo-controlled trial. Eur Rev Med Pharmacol Sci. 2010;14:155–162.[↩]
- Moss-Morris R, McAlpine L, Didsbury LP, et al. A randomized controlled trial of a cognitive behavioural therapy-based self-management intervention for irritable bowel syndrome in primary care. Psychol Med. 2010;40:85–94. doi: 10.1017/S0033291709990195[↩]
- Magge S, Lembo A. Low-FODMAP Diet for Treatment of Irritable Bowel Syndrome. Gastroenterology & Hepatology. 2012;8(11):739-745. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3966170/[↩][↩]
- Irritable bowel syndrome and diet: where are we in 2018 ? Current Opinion in Clinical Nutrition & Metabolic Care: November 2017 – Volume 20 – Issue 6 – p 456–463. http://journals.lww.com/co-clinicalnutrition/Abstract/2017/11000/Irritable_bowel_syndrome_and_diet___where_are_we.6.aspx[↩]
- Low-FODMAP Diet. American College of Gastroenterology. http://patients.gi.org/topics/low-fodmap-diet/[↩]
- Low FODMAP diet for Irritable Bowel Syndrome. Monash University. https://www.monash.edu/medicine/ccs/gastroenterology/fodmap[↩]
- Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. Gibson PR, Shepherd SJ. J Gastroenterol Hepatol. 2010 Feb; 25(2):252-8. https://www.ncbi.nlm.nih.gov/pubmed/20136989/[↩]
- Gibson PR, Barrett JS. Clinical ramifications of malabsorption of fructose and other short-chain carbohydrates. Practical Gastroenterology. 2007;31:51–65.[↩][↩][↩]





{kind=link}