Contents
Gallbladder cancer
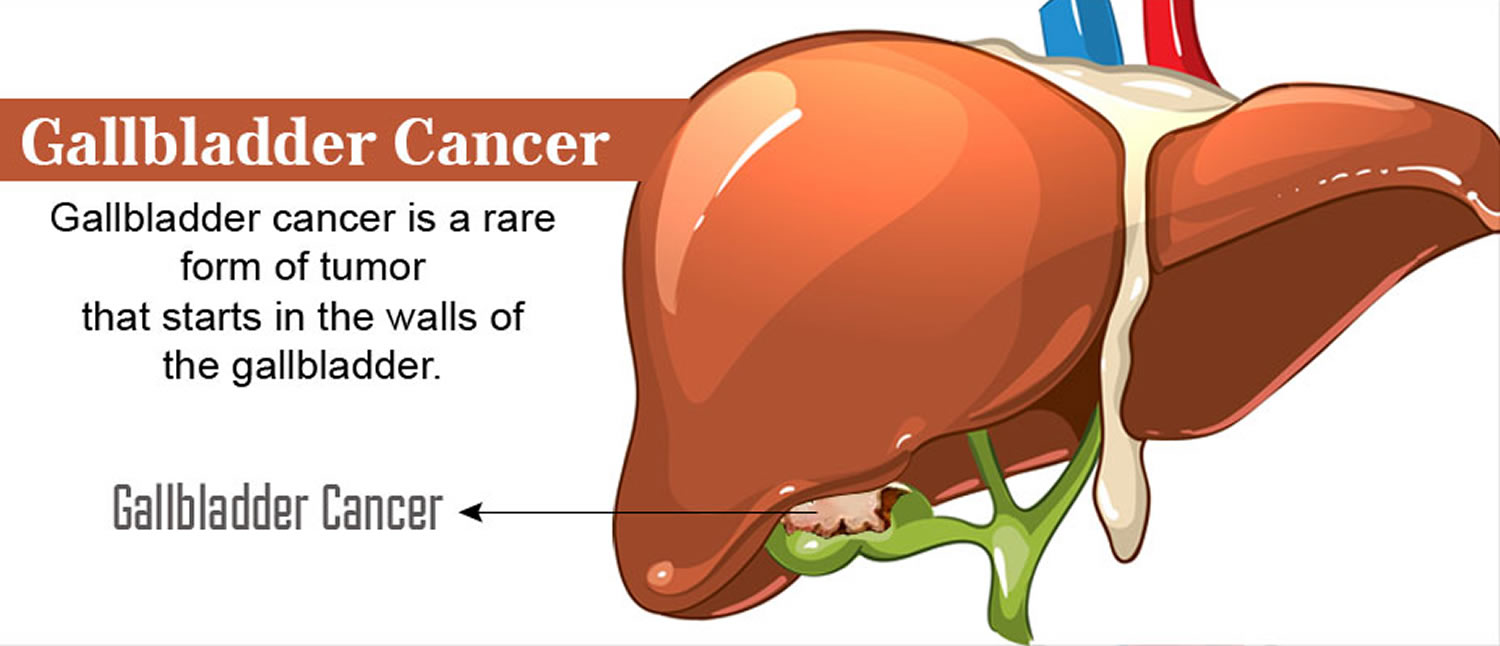
Gallbladder cancer is a rare cancer that begins in the gallbladder.
The American Cancer Society’s estimates for cancer of the gallbladder and nearby large bile ducts in the United States for 2018 are 1:
- About 12,190 new cases diagnosed: 5,450 in men and 6,740 in women
- About 3,790 deaths from these cancers: 1,530 in men and 2,260 in women
Of these new cases, a little less than 4 in 10 will be gallbladder cancers.
Gallbladder cancer is not usually found until it has become advanced and causes symptoms. Only about 1 of 5 gallbladder cancers is found in the early stages, when the cancer has not yet spread beyond the gallbladder.
The chances of survival for patients with gallbladder cancer depend to a large extent on how advanced it is when it is found.
Your gallbladder is a small, pear-shaped organ on the right side of your abdomen, just beneath your liver (see Figure 1 to 4). The gallbladder stores bile, a digestive fluid produced by your liver.
Gallbladder cancer is uncommon. When gallbladder cancer is discovered at its earliest stages, the chance for a cure is very good. But most gallbladder cancers are discovered at a late stage, when the prognosis is often very poor.
Gallbladder cancer is difficult to diagnose because it often causes no specific signs or symptoms. Also, the relatively hidden nature of the gallbladder makes it easier for gallbladder cancer to grow without being detected.
The Gallbladder
The gallbladder is a pear-shaped sac in a depression on the liver’s under surface. The gallbladder is lined with epithelial cells and has a strong layer of smooth muscle in its wall. The gallbladder stores bile between meals, reabsorbs water to concentrate bile, and contracts to release bile into the small intestine. The gallbladder connects to the cystic duct, which in turn joins the common hepatic duct (Figure 2).
The common hepatic duct and cystic duct join to form the bile duct (common bile duct). It leads to the duodenum where the hepatopancreatic sphincter guards its exit (Figure 3). Because this sphincter normally remains contracted, bile collects in the bile duct. It backs up into the cystic duct and flows into the gallbladder, where it is stored.
The gallbladder is helpful, but you do not need it to live. Many people have their gallbladders removed and go on to live normal lives.
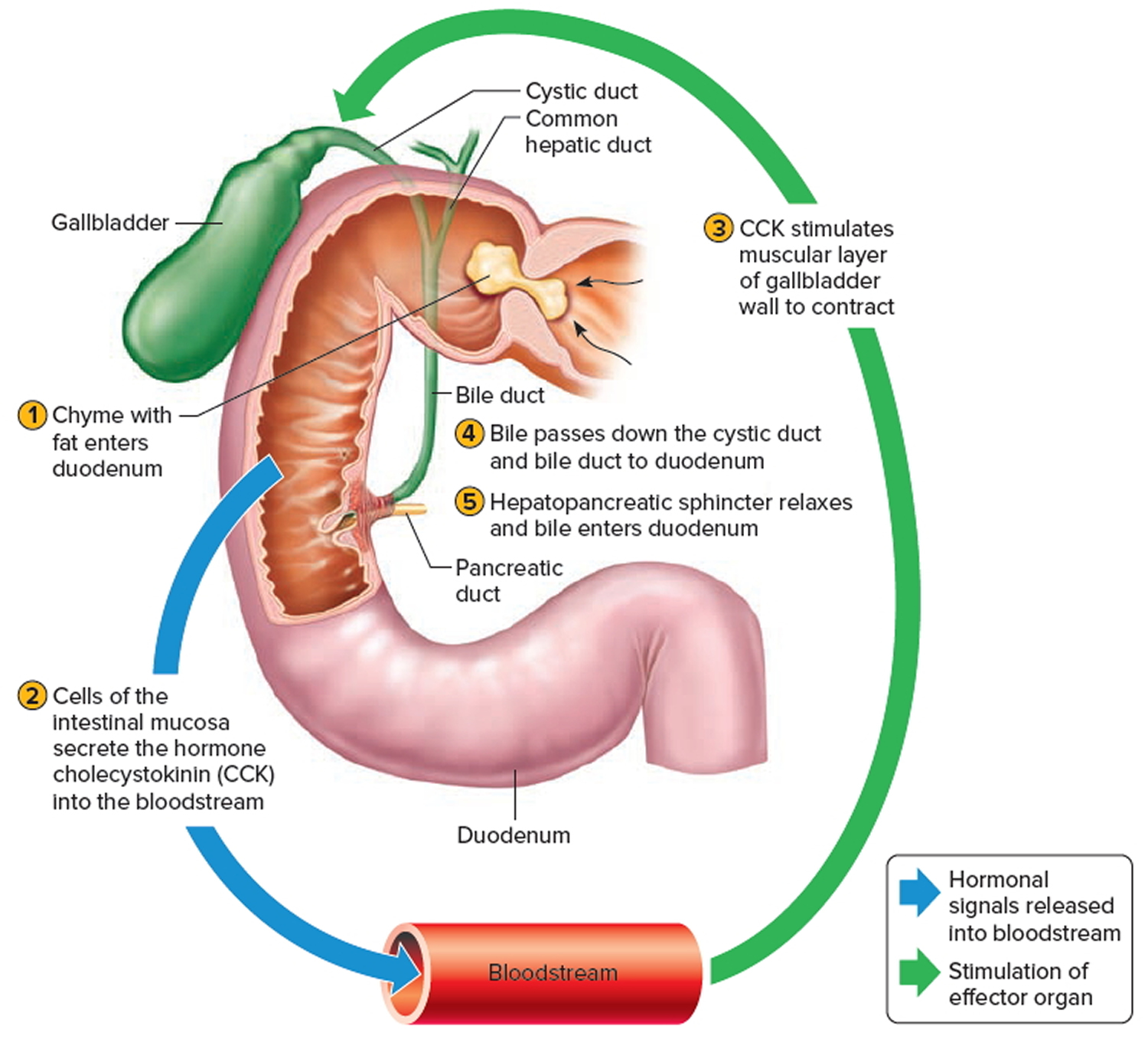
Gallbladder function
Following a meal, the mixing movements of the stomach wall aid in producing a semifluid paste of food particles and gastric juice called chyme.
As chyme enters the duodenum (the proximal portion of the small intestine), accessory organs—the pancreas, liver, and gallbladder—add their secretions.
Bile is a yellowish-green liquid continuously secreted from hepatic (liver) cells. In addition to water, bile contains bile salts, bile pigments (bilirubin and biliverdin), cholesterol, and electrolytes. Of these, bile salts are the most abundant and are the only bile components that have a digestive function.
Bile pigments are breakdown products of hemoglobin from red blood cells and are normally secreted in the bile.
Normally bile does not enter the duodenum until cholecystokinin stimulates the gallbladder to contract. Proteins and fats in chyme in the duodenum stimulate
the intestinal wall to release cholecystokinin. Cholecystokinin travels via the bloodstream to the pancreas also, where it stimulate the pancreas to release its pancreatic juice that has a high concentration of digestive enzymes.
The hepatopancreatic sphincter usually remains contracted until a peristaltic wave in the duodenal wall approaches it. Then the sphincter relaxes, and bile is squirted into the duodenum (see Figure 4).
Note: Cholecystokinin produced by the intestinal wall cells, in response to proteins and fats in the small intestine, decreases secretory activity of gastric glands and inhibits gastric motility; stimulates pancreas to secrete fluid with a high digestive enzyme concentration and stimulates gallbladder to contract and release bile.
Figure 1. Gallbladder location
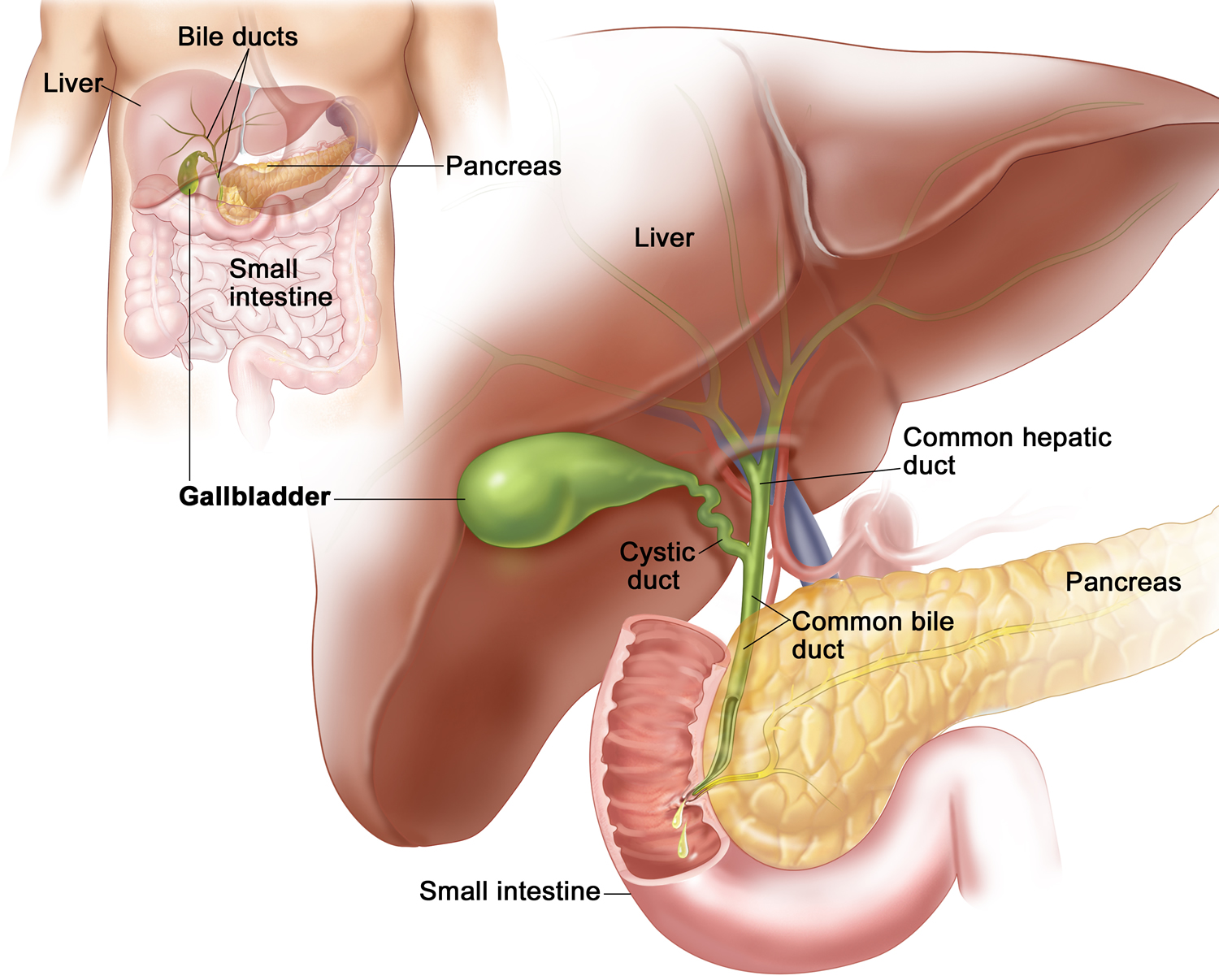
Figure 2. Gallbladder anatomy
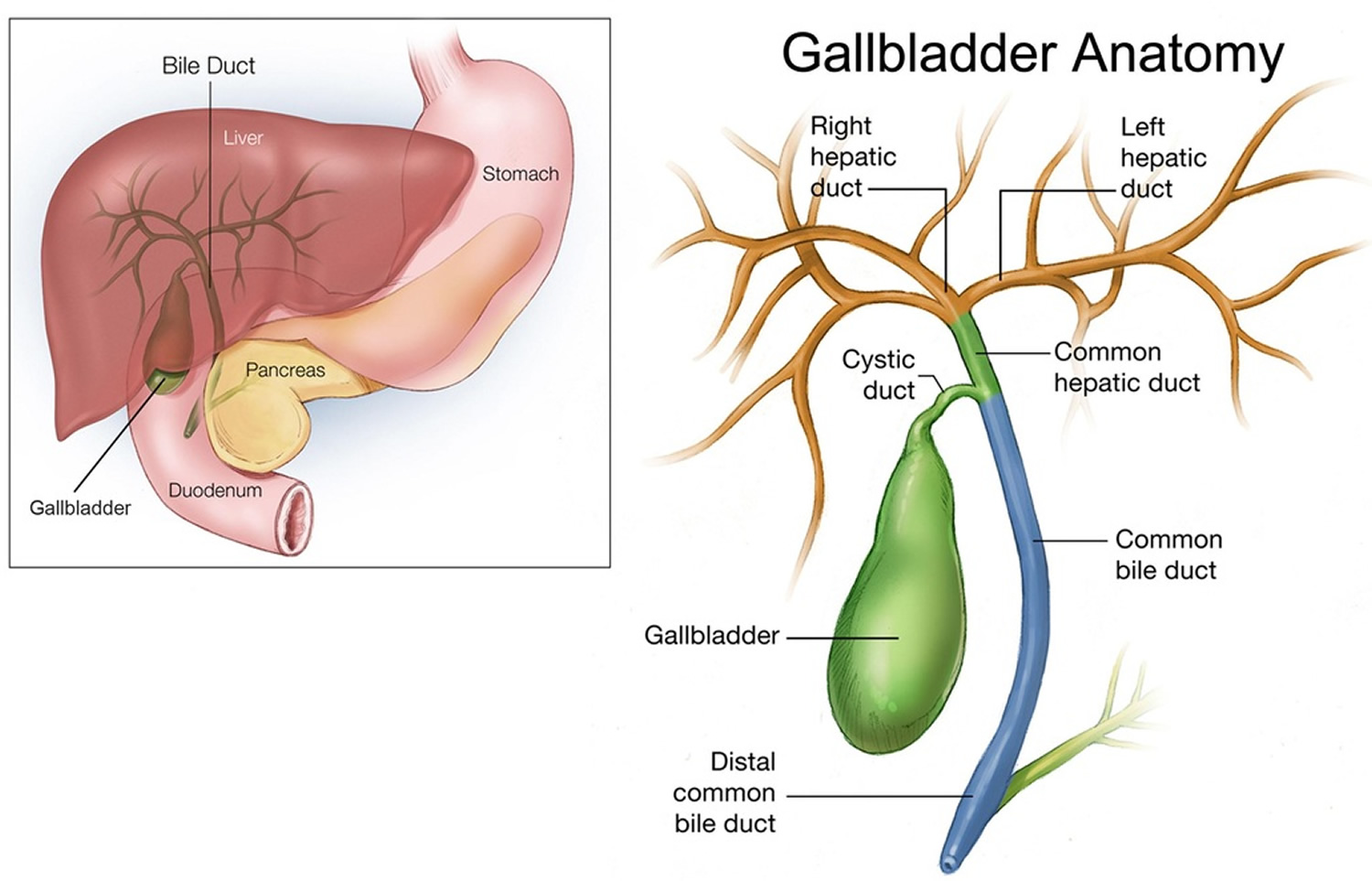
Figure 3. The common bile duct is closely associated with the pancreatic duct and the duodenum
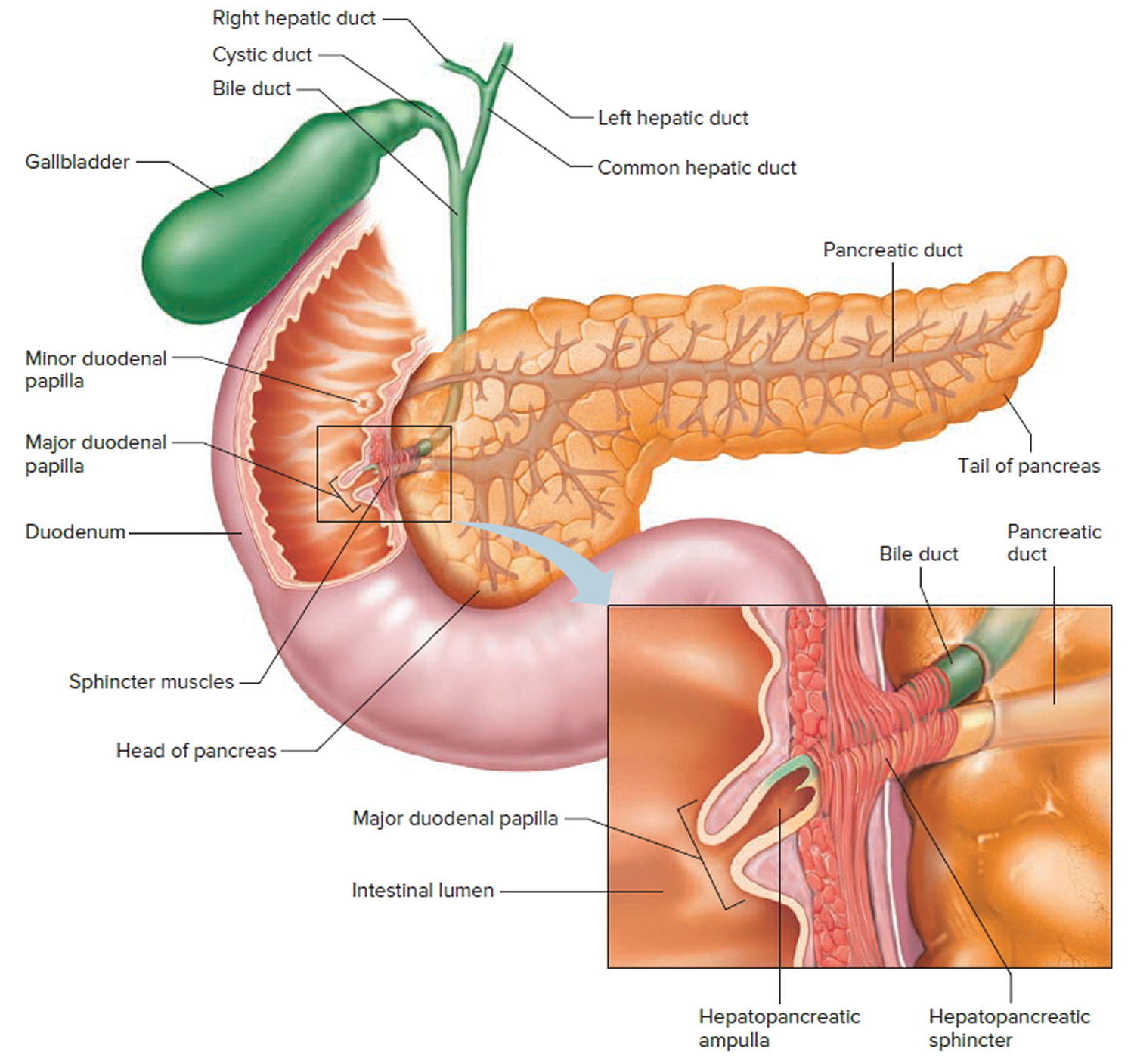
Figure 4. Fatty chyme entering the duodenum stimulates the gallbladder to release bile
 Types of gallbladder cancers
Types of gallbladder cancers
About 9 out of 10 gallbladder cancers are adenocarcinomas. An adenocarcinoma is a cancer that starts in cells with gland-like properties that line many internal and external surfaces of the body (including the inside the digestive system).
Papillary adenocarcinoma or just papillary cancer is a type of gallbladder adenocarcinoma that deserves special mention. When seen under a microscope, the cells in these gallbladder cancers are arranged in finger-like projections. In general, papillary cancers are not as likely to grow into the liver or nearby lymph nodes. They tend to have a better prognosis (outlook) than most other kinds of gallbladder adenocarcinomas. About 6% of all gallbladder cancers are papillary adenocarcinomas.
Other types of cancer, such as adenosquamous carcinomas, squamous cell carcinomas, small cell carcinomas, and sarcomas, can develop in the gallbladder, but these are uncommon.
Gallbladder Adenocarcinoma
This is the most common type of gallbladder cancer. More than 90 out of every 100 gallbladder cancers (9%) are adenocarcinomas. The cancer starts in gland cells in the gallbladder lining. These gland cells normally produce mucus (thick fluid).
There are three types of adenocarcinomas of the gallbladder. You might hear your doctor talking about 2:
- Non papillary adenocarcinoma
- Papillary adenocarcinoma
- Mucinous adenocarcinoma
Only about 6 out of every 100 gallbladder cancers (6%) are papillary adenocarcinomas. They develop in the tissues that hold the gallbladder in place (connective tissues). This type of gallbladder cancer is less likely to spread to the liver and nearby lymph nodes. It tends to have a better outlook than most other types of gallbladder cancer.
With mucinous adenocarcinomas, the cancer cells are often in pools of mucus. Only about 1 or 2 out of every 100 gallbladder cancers (1 or 2%) are mucinous adenocarcinoma.
Gallbladder Squamous cell cancer
Squamous cell cancers develop from the skin like cells that form the lining of the gallbladder, along with the gland cells. They are treated in the same way as adenocarcinomas.
Gallbladder Adenosquamous cancer
Adenosquamous carcinomas are cancers that have both squamous cancer cells and glandular cancer cells. Your doctor might call this a mixed histology. These cancers are treated in the same way as adenocarcinomas.
Gallbladder Small cell cancer
Small cell carcinomas are also called oat cell carcinomas. This is because the cancer cells have a distinctive oat like shape.
Gallbladder Sarcoma
Sarcoma is the name for a cancer that affects the supportive or protecting tissues of the body, also called the connective tissues. Muscles, blood vessels and nerves are all connective tissues. So a cancer that begins in the muscle layer of the gallbladder is called a sarcoma.
Gallbladder Neuroendocrine tumour
Neuroendocrine tumours are rare cancers that grow from hormone producing tissues, usually in the digestive system. The most common type of neuroendocrine tumour is called carcinoid. Carcinoid tumours tend to grow slowly. They might not cause any symptoms for several years.
Lymphoma and melanoma
These are extremely rare types of gallbladder cancer. They are not necessarily treated in the same way as the other types. For example, lymphomas tend to respond well to chemotherapy and radiotherapy. So it is very unlikely that you would have surgery to treat a lymphoma.
Gallbladder cancer causes
The exact cause of gallbladder cancer isn’t known, but certain things are thought to increase your chances of developing it.
Researchers have found several risk factors that make a person more likely to develop gallbladder cancer. Scientists are also beginning to understand how some of these risk factors might lead to gallbladder cancer.
Chronic gallbladder inflammation is a common link among many of the risk factors for gallbladder cancer. For example, when someone has gallstones, the gallbladder may release bile more slowly. This means that cells in the gallbladder are exposed to the chemicals in bile for longer than usual. This could lead to irritation and inflammation.
In another example, abnormalities in the ducts that carry fluids from the gallbladder and pancreas to the small intestine might allow juices from the pancreas to flow backward (reflux) into the gallbladder and bile ducts. This reflux of pancreatic juices might inflame and stimulate growth of the cells lining the gallbladder and bile ducts, which might increase the risk of gallbladder cancer.
Scientists are starting to understand how risk factors such as inflammation might lead to certain changes in the DNA of cells, making them grow abnormally and form cancers. DNA is the chemical in each of our cells that makes up your genes (the instructions for how your cells function). You usually look like your parents because they are the source of your DNA. But DNA affects more than how you look.
Some genes control when cells grow, divide into new cells, and die. Genes that help cells grow, divide, and stay alive are called oncogenes. Genes that slow down cell division or cause cells to die at the right time are called tumor suppressor genes. Cancers can be caused by DNA changes (mutations) that turn on oncogenes or turn off tumor suppressor genes. Changes in several different genes are usually needed for a cell to become cancerous.
Some people inherit DNA mutations from their parents that greatly increase their risk for certain cancers. But inherited gene mutations are not thought to cause very many gallbladder cancers.
Gene mutations related to gallbladder cancers are usually acquired during life rather than being inherited. For example, acquired changes in the TP53 tumor suppressor gene are found in many cases of gallbladder cancer. Other genes that may play a role in gallbladder cancers include KRAS, BRAF, CDKN2, and HER2. Some of the gene changes that lead to gallbladder cancer might be caused by chronic inflammation. But sometimes what causes these changes is not known. Many gene changes might just be random events that sometimes happen inside a cell, without having an outside cause.
Risk Factors for Gallbladder Cancer
A risk factor is anything that affects your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking, can be changed. Others, like a person’s age or family history, can’t be changed.
But having a risk factor, or even several risk factors, does not mean that a person will get the disease. And many people who get the disease may have few or no known risk factors.
Scientists have found several risk factors that make a person more likely to develop gallbladder cancer. Many of these are related in some way to chronic inflammation (irritation and swelling) in the gallbladder.
Gallstones
Gallstones are the most common risk factor for gallbladder cancer. Gallstones are pebble-like collections of cholesterol and other substances that form in the gallbladder and can cause chronic inflammation. At least 3 out of 4 people with gallbladder cancer have gallstones when they are diagnosed. But gallstones are very common, and gallbladder cancer is quite rare, especially in the United States. Most people with gallstones never develop gallbladder cancer.
Porcelain gallbladder
Porcelain gallbladder is a condition in which the wall of the gallbladder becomes covered with calcium deposits. It sometimes occurs after long-term inflammation of the gallbladder (cholecystitis), which can be caused by gallstones. People with this condition have a higher risk of developing gallbladder cancer (possibly because both conditions can be related to inflammation).
Female gender
In the United States, gallbladder cancer occurs more than twice as often in women. Gallstones and gallbladder inflammation are important risk factors for gallbladder cancer and are also much more common in women than men.
Obesity
Patients with gallbladder cancer are more often overweight or obese than people without this disease. Being overweight causes changes in hormones in the body, particularly for women. It could be this change in the body’s hormone balance that increases the risk of gallbladder cancer. Obesity is also a risk factor for gallstones, which might help explain this link.
Diabetes
You might have an increased risk of gallbladder cancer or cancer of the bile duct if you have diabetes.
Older age
Gallbladder cancer is seen mainly in older people, but younger people can develop it as well. The average age of people when they are diagnosed is 72. More than 2 out of 3 people with gallbladder cancer are 65 or older when it is found.
Ethnicity and geography
In the United States, the risk of developing gallbladder cancer is highest among Mexican Americans and Native Americans. They are also more likely to have gallstones than members of other ethnic and racial groups. The risk is lowest among African Americans. Worldwide, gallbladder cancer is much more common in India, Pakistan, and Central European and South American countries than it is in the United States.
Areas of the world where gallbladder cancer is significantly high are:
- Latin America
- Asia
- Eastern and Central Europe
Low rates of gallbladder cancer are found in:
- western countries such as UK, USA, Australia, Canada and New Zealand
- western and Mediterranean European countries
Choledochal cysts
Choledochal cysts are bile-filled sacs that are connected to the common bile duct, the tube that carries bile from the liver and gallbladder to the small intestine. (Choledochal means having to do with the common bile duct.) The cysts can grow large over time and may contain as much as 1 to 2 quarts of bile. The cells lining the sac often have areas of pre-cancerous changes, which increase a person’s risk for gallbladder cancer.
Abnormalities of the bile ducts
The pancreas is another organ that releases fluids through a duct into the small intestine to help digestion. This duct normally meets up with the common bile duct just as it enters the small intestine. Some people have an abnormality where these ducts meet that lets juice from the pancreas reflux (flow backward) into the bile ducts. This backward flow also prevents the bile from being emptied through the bile ducts as quickly as normal. People with these abnormalities are at higher risk of gallbladder cancer. Scientists are not sure if the increased risk is due to the action of the pancreatic juice or is possibly due to the ducts being exposed longer to damaging substances in the bile itself.
Gallbladder polyps
A gallbladder polyp is a growth that bulges from the surface of the inner gallbladder wall. Some polyps are formed by cholesterol deposits in the gallbladder wall. Others may be small tumors (either cancerous or benign) or may be caused by inflammation. Polyps larger than 1 centimeter (almost a half inch) are more likely to be cancer, so doctors often recommend removing the gallbladder in patients with gallbladder polyps that size or larger.
Gallstones and gallbladder inflammation
Gallstones and inflammation of the gallbladder (cholecystitis) are the most common risk factors for gallbladder cancer.
Gallstones are hard lumps, like little rocks, that form in the gallbladder. They are mostly cholesterol, mixed with other substances found in bile. About 6 to 8 out of 10 people with gallbladder cancer (60% to 80%) have gallstones or an inflamed gallbladder when they are diagnosed.
One study has shown that a family history of gallstones doubles the risk of gallbladder cancer, and that people with a family history of gallstones who also have gallstones themselves have almost 60 times the normal risk of gallbladder cancer.
Gallstones are very common but gallbladder cancer is very rare. Most people with an inflamed gallbladder or gallstones do not get gallbladder cancer.
Primary sclerosing cholangitis
In primary sclerosing cholangitis, there is inflammation and scarring of the bile ducts. People with this disease have an increased risk of cancer of the gallbladder and bile ducts. Many people with primary sclerosing cholangitis also have ulcerative colitis, a type of inflammatory bowel disease.
Industrial and environmental chemicals
It is not clear if exposure to certain chemicals in the workplace or the environment increases the risk of gallbladder cancer. This is hard to study because this cancer is not common. Some studies in lab animals have suggested that chemical compounds called nitrosamines may increase the risk of gallbladder cancer. Other studies have found that gallbladder cancer might occur more in workers in the rubber and textile industries than in the general public. More research is needed in this area to confirm or refute these possible links.
Typhoid
People chronically infected with salmonella (the bacterium that causes typhoid) and those who are carriers of the disease are more likely to get gallbladder cancer than those not infected. This is probably because the infection can cause gallbladder inflammation. But typhoid is rare in the United States.
A few small studies show that Helicobacter pylori bacteria might also increase the risk of gallbladder cancer. More research needs to be done to confirm this link.
Family history
Most gallbladder cancers are not found in people with a family history of the disease. A history of gallbladder cancer in the family seems to increase a person’s chances of developing this cancer.
People are 5 times more likely to develop gallbladder cancer if they have one of the following:
- any family history of gallstone disease
- a first degree relative (a parent, sibling or child) with gallbladder cancer
Because gallbladder cancer is so rare, this is still a very small risk.
Smoking
People who smoke increase their risk of gallbladder cancer by nearly 5 times (20%).
Alcohol
Drinking alcohol can increase your risk of gallbladder cancer. Heavy drinkers are more at risk of developing gallbladder than moderate drinkers. And the less you drink, the lower your risk of gallbladder cancer.
Number of children (parity)
For women the risk of gallbladder cancer increases with each child they have. Because gallbladder cancer is rare this is still a small risk.
Gallbladder cancer signs and symptoms
Gallbladder cancer doesn’t usually cause symptoms in its early stages. So by the time you know it’s there, it might be at a more advanced stage than some other types of cancer. At diagnosis, gallbladder cancer has often spread outside the gallbladder itself to areas nearby.
It can be difficult for doctors to feel if your gallbladder is swollen or tender when they examine you. The gallbladder lies behind other organs deep inside your body, so it can be difficult to feel. Many early stage cancers of the gallbladder are found by chance. For example, when someone is having their gallbladder taken out to treat gallstones.
You may get a number of symptoms with gallbladder cancer. Most of these happen in the later stages of the disease.
Other illnesses apart from gallbladder cancer can also cause these symptoms. Even so, it is important that you see your doctor. Whatever is causing your symptoms needs treating.
Some of the more common symptoms of gallbladder cancer are:
Abdominal (belly) pain
Most people with gallbladder cancer will have abdominal pain. Some people describe it as a dragging feeling. If the cancer or gallstones block the bile duct, you will have a sharper pain. Most often this is in the upper right part of the belly.
Nausea and/or vomiting
People with gallbladder cancer sometimes have vomiting as a symptom. This is very common in the later stages of gallbladder cancer.
Over half the people diagnosed with gallbladder cancer will feel or be sick quite often at some stage of their illness. This is usually fairly easy to control with anti sickness drugs.
Jaundice
Jaundice is a yellowing of the skin and the white part of the eyes. If the cancer grows large enough to block the bile ducts, bile from the liver can’t drain into the intestines. This can cause bilirubin (a chemical in bile that gives it a yellow color) to build up in the blood and settle in different parts of the body. This can often be seen in the skin and eyes.
The symptoms can include:
- yellowing skin and whites of the eyes
- severe itching in some people
- darkened urine
- pale colored stools (bowel movements)
The bile salts make your skin and the whites of your eyes look yellow, and your skin itch (doctors call this itching pruritis). They also make your urine darker than normal. Because the bile is not passing into your bowel, your stools will be much paler than normal.
Nearly half the people diagnosed with gallbladder cancer have jaundice. This is often a sign that the cancer is in its later stages.
Remember – having jaundice does not always mean you have cancer. A viral infection of the liver (hepatitis) is a much more common cause of jaundice than gallbladder cancer.
Lumps in the belly
If the cancer blocks the bile ducts, the gallbladder can swell to larger than normal. Gallbladder cancer can also spread to nearby parts of the liver. These can sometimes be felt by the doctor as lumps on the right side of the belly. They can also be detected by imaging tests such as an ultrasound.
Other symptoms
Less common symptoms of gallbladder cancer include:
- Loss of appetite
- Weight loss
- Swelling in the abdomen (belly)
- Fever
- Itchy skin
- Dark urine
- Light-colored or greasy stools
Gallbladder cancer is not common, and these symptoms and signs are more likely to be caused by something other than gallbladder cancer. For example, people with gallstones also have many of these symptoms. There are many far more common causes of abdominal pain than gallbladder cancer. And viral hepatitis (infection of the liver) is a much more common cause of jaundice. Still, if you have any of these problems, it’s important to see your doctor right away so the cause can be found and treated, if needed.
Can Gallbladder Cancer Be Found Early?
Gallbladder cancer is hard to find early. The gallbladder is deep inside the body, so early tumors can’t be seen or felt during routine physical exams. There are no blood tests or other tests that can reliably detect gallbladder cancers early enough to be useful as screening tests. (Screening is testing for cancer in people without any symptoms.) Because of this, most gallbladder cancers are found only after the cancer has grown enough to cause signs or symptoms.
Still, some gallbladder cancers are found before they have spread to other tissues and organs. Many of these early cancers are found unexpectedly when a person’s gallbladder is removed because of gallstones. When the gallbladder is looked at in the lab after it is removed, small cancers or pre-cancers that did not cause any symptoms are sometimes found.
Gallbladder Cancer Diagnosis
Some gallbladder cancers are found after the gallbladder has been removed to treat gallstones or chronic (long-term) inflammation. Gallbladders removed for those reasons are always looked at under a microscope to see if they contain cancer cells.
Most gallbladder cancers, though, are not found until a person goes to a doctor because they have symptoms.
Medical history and physical exam
If you have any signs or symptoms that suggest you might have gallbladder cancer, your doctor will want to take a complete medical history to check for risk factors and to learn more about your symptoms.
Your doctor will examine you to look for signs of gallbladder cancer and other health problems. The exam will focus mostly on the abdomen to check for any lumps, tenderness, or buildup of fluid. The skin and the white part of the eyes will be checked for jaundice (a yellowish color). Sometimes, cancer of the gallbladder spreads to lymph nodes, causing a lump that can be felt beneath the skin. Lymph nodes above the collarbone and in several other locations may be examined carefully.
If symptoms and/or the physical exam suggest you might have gallbladder cancer, other tests will be done. These might include lab tests, imaging tests, and other procedures.
Blood tests
Tests of liver and gallbladder function
Your doctor may order lab tests to find out how much bilirubin is in the blood. Bilirubin is the chemical that gives the bile its yellow color. Problems in the gallbladder, bile ducts, or liver can raise the blood level of bilirubin. A high bilirubin level tells the doctor that there may be gallbladder, bile duct, or liver problems.
The doctor may also order tests for other substances in your blood, such as albumin, alkaline phosphatase, AST, ALT, and GGT, which can also be abnormal if you have liver, bile duct, or gallbladder disease. These are sometimes referred to as liver function tests.
Tumor markers
CEA and CA 19-9 are tumor markers (proteins found in the blood when certain cancers are present). High levels of these substances are often (but not always) found in people with gallbladder cancer. Usually the blood levels of these markers are high only when the cancer is in an advanced stage. These markers are not specific for gallbladder cancer – that is, other cancers or even some other health conditions can cause high levels.
These tests can sometimes be useful after a person is diagnosed with gallbladder cancer. If the levels of these markers are found to be high, they can be followed over time to help tell how well treatment is working.
Imaging tests
Imaging tests use x-rays, magnetic fields, or sound waves to create pictures of the inside of your body. Imaging tests can be done for a number of reasons, including:
- To look for suspicious areas that might be cancer
- To help a doctor guide a biopsy needle into a suspicious area to take a sample
- To learn how far cancer has spread
- To help guide certain types of treatments
- To help determine if treatment is working
- To look for signs of the cancer coming back after treatment
People who have (or might have) gallbladder cancer may have one or more of the following tests.
Ultrasound
For this test, a small instrument called a transducer gives off sound waves and picks up their echoes as they bounce off organs inside the body. The echoes are converted by a computer into an image on a screen. The patterns of echoes can help find tumors and show how far they have grown into nearby areas.
- Abdominal ultrasound: This is often the first imaging test done in people who have symptoms (such as jaundice or pain in the right upper part of their abdomen) that might be caused by gallbladder problems. This is an easy test to have done, and it uses no radiation. You simply lie on a table while the doctor or ultrasound technician moves the transducer (which is shaped like a wand) along the skin over the right upper abdomen. Usually, the skin is first lubricated with gel.
- Endoscopic or laparoscopic ultrasound: In these techniques, the doctor puts the ultrasound transducer inside the body and closer to the gallbladder, which gives more detailed images than a standard ultrasound. The transducer is on the end of a thin, lighted tube that has an attached viewing device. The tube is either passed through the mouth, down through the stomach, and near the gallbladder area (endoscopic ultrasound) or through a small surgical cut in the belly (laparoscopic ultrasound). If there is a tumor, ultrasound might help the doctor tell if and how far it has invaded the gallbladder wall, which helps in planning for surgery. Ultrasound may be able to show if nearby lymph nodes are enlarged, which can be a sign that cancer has reached them.
Ultrasound can also be used to guide a needle into a suspicious lymph node so that cells can be removed (biopsied) and viewed under a microscope. This is known as an ultrasound-guided needle biopsy.
Computed tomography (CT) scan
The CT scan uses x-rays to make detailed cross-sectional images of your body. Instead of taking one picture, like a regular x-ray, a CT scanner takes many pictures as it rotates around you while you lie on a table. A computer then combines these into images of slices of the part of your body that is being studied.
A CT scanner has been described as a large donut, with a narrow table that slides in and out of the middle opening. You will need to lie still on the table while the scan is being done. CT scans take longer than regular x-rays, and you might feel a bit confined by the ring while the pictures are being taken.
Before any pictures are taken, you might be asked to drink 1 to 2 pints of a liquid called oral contrast. This helps outline the intestine so that certain areas are not mistaken for tumors. You might also need an IV (intravenous) line through which a different kind of contrast dye (IV contrast) is injected. This helps better outline structures throughout your body.
The injection can cause some flushing (redness and warm feeling). Some people are allergic and get hives or, rarely, more serious reactions like trouble breathing and low blood pressure. Be sure to tell the doctor if you have any allergies or have ever had a reaction to any contrast material used for x-rays.
CT scans can have several uses for gallbladder cancer:
- They are often used to help diagnose gallbladder cancer by showing tumors in the area.
- They can help stage the cancer (find out how far it has spread). CT scans can show the organs near the gallbladder (especially the liver), as well as lymph nodes and distant organs the cancer might have spread to.
- A type of CT known as CT angiography can be used to look at the blood vessels near the gallbladder. This can help determine if surgery is a treatment option.
- CT scans can also be used to guide a biopsy needle into a suspected tumor or metastasis. For this procedure, called a CT-guided needle biopsy, you remain on the CT scanning table, while the doctor advances a biopsy needle through the skin and toward the mass. CT scans are repeated until the needle is within the mass. A biopsy sample is then removed and looked at under a microscope.
Magnetic resonance imaging (MRI) scan
Like CT scans, MRI scans provide detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays. A contrast material called gadolinium may be injected into a vein before the scan to better see details.
MRI scans provide a great deal of detail and can be very helpful in looking at the gallbladder and nearby bile ducts and other organs. Sometimes they can help tell a benign tumor from a cancerous one.
Special types of MRI scans can also be used in people who may have gallbladder cancer:
- MR cholangiopancreatography (MRCP), which can be used to look at the bile ducts, is described below in the section on cholangiography.
- MR angiography (MRA), which looks at blood vessels, is mentioned below in the next section on angiography.
MRI scans can be a little more uncomfortable than CT scans. They take longer, often up to an hour. You may have to lie inside a narrow tube, which is confining and can upset people who have a fear of enclosed spaces. Special, more open MRI machines can sometimes be used instead. The MRI machine also makes buzzing and clicking noises that might be disturbing. Some places will provide earplugs to help block this noise out.
Cholangiography
A cholangiogram is an imaging test that looks at the bile ducts to see if they are blocked, narrowed, or dilated. This can help show if someone might have a tumor that is blocking a duct. It can also be used to help plan surgery. There are several types of cholangiograms, each of which has different pros and cons.
- Magnetic resonance cholangiopancreatography (MRCP): This is a non-invasive way to take images of the bile ducts using the same type of machine used for standard MRI scans. It does not require use of a contrast agent and is not invasive, unlike other types of cholangiograms. Because it is non-invasive, doctors often use MRCP if the purpose of the test is just to image the bile ducts. But this test can’t be used to get biopsy samples of tumors or to place stents (small tubes) in the ducts to keep them open.
- Endoscopic retrograde cholangiopancreatography (ERCP): In this procedure, a doctor passes a long, flexible tube (endoscope) down the throat, through the esophagus and stomach and into the first part of the small intestine. This is usually done while you are sedated (given medicine to make you sleepy). A small catheter (tube) is passed from the end of the endoscope and into the common bile duct. A small amount of contrast dye is injected through the tube to help outline the bile ducts and pancreatic duct as x-rays are taken. The images can show narrowing or blockage of these ducts.
This test is more invasive than MRCP, but the advantage is that the doctor can also take samples of cells or fluid to look at under a microscope. ERCP can also be used to place a stent (a small tube) into a duct to help keep it open.
- Percutaneous transhepatic cholangiography (PTC): In this procedure, the doctor places a thin, hollow needle through the skin of the belly and into a bile duct within the liver. You will get medicine through an IV line to make you sleepy before the test. A local anesthetic is also used to numb the area before inserting the needle. A contrast dye is then injected through the needle, and x-rays are taken as it passes through the bile ducts. As with ERCP, this approach can also be used to take samples of fluid or tissues or to place a stent into a duct to help keep it open. Because it is more invasive (and might cause more pain), PTC is not usually used unless ERCP has already been tried or can’t be done for some reason.
Angiography
Angiography or an angiogram is an x-ray test used to look at blood vessels. For this test, a small amount of contrast dye is injected into an artery to outline blood vessels while x-ray images are taken. The images show if blood flow in an area is blocked or affected by a tumor, and any abnormal blood vessels in the area. The test can also show if a gallbladder cancer has grown through the walls of certain blood vessels. This information is used to help surgeons decide whether a cancer can be removed and to help plan the operation.
X-ray angiography can be uncomfortable because the doctor has to put a small catheter (a flexible hollow tube) into the artery leading to the gallbladder to inject the dye. Usually the catheter is put into an artery in your inner thigh and threaded up into the artery supplying the gallbladder. A local anesthetic is often used to numb the area before inserting the catheter. Then the dye is injected quickly to outline all the vessels while the x-rays are being taken.
Angiography can also be done with a CT scanner (CT angiography) or an MRI scanner (MR angiography). These techniques are now used more often because they can give information about the blood vessels near the gallbladder without the need for a catheter in the artery. You may still need an IV line so that contrast dye can be injected into the bloodstream during the imaging.
Laparoscopy
Laparoscopy is a type of minor surgery. The doctor inserts a thin tube with a light and a small video camera on the end (a laparoscope) through a small incision (cut) in the front of the abdomen to look at the gallbladder, liver, and other organs. (Sometimes more than one cut is made.) This procedure is done in the operating room while you are under general anesthesia (in a deep sleep).
Laparoscopy can help doctors plan surgery or other treatments, and can help determine the stage (extent) of the cancer. If needed, doctors can also insert instruments through the incisions to remove biopsy samples, which are then looked at under a microscope to make or confirm the diagnosis of cancer.
Laparoscopy is often used to remove the gallbladder to treat gallstones or chronic inflammation of the gallbladder. This operation is called a laparoscopic cholecystectomy. If gallbladder cancer is found or suspected during that operation, surgeons usually convert the operation to an open cholecystectomy (removal of the gallbladder through a larger cut in the abdomen). The open method lets the surgeon see more and may lower the chance of releasing cancer cells into the abdomen when the gallbladder is removed. The use of the open procedure depends on the size of the cancer and whether surgery can remove all the cancer.
Biopsy
During a biopsy, the doctor removes a tissue sample to be looked at under a microscope to see if cancer (or some other disease) is present. For most types of cancer, a biopsy is needed for a diagnosis. Biopsies are also used to help find out how far the cancer has spread. This is important when determining the best treatment options.
But a biopsy may not always be done before surgery to remove a gallbladder tumor. Doctors are often concerned that sticking a needle into the tumor or otherwise disturbing it without completely removing it might allow cancer cells to spread to other areas.
If imaging tests (ultrasound, CT or MRI scans, cholangiography, etc.) suggest there is a tumor in the gallbladder and there are no obvious signs of distant spread, the doctor may decide to proceed directly to surgery and to treat it as a gallbladder cancer. In these cases, the gallbladder tissue is looked at under a microscope after the gallbladder is removed.
In other cases, a doctor may feel that a biopsy of a suspicious area in the gallbladder is the best way to know for certain if it is cancer. For example, imaging tests may show that a tumor has spread or grown too large to be removed completely by surgery. Unfortunately, many gallbladder cancers are not removable by the time they are first found.
Types of biopsies
There are several ways to take biopsy samples of the gallbladder.
If cholangiography (ERCP or PTC) is being done, a sample of bile may be collected during the procedure to look for cancer cells within the fluid.
As noted earlier, biopsy specimens can be taken during laparoscopy. This lets the doctor see the surface of the gallbladder and nearby areas and take samples of suspicious areas.
If the cancer appears to be too advanced for surgery, a needle biopsy may be done to confirm the diagnosis and help guide treatment. For this test, a thin, hollow needle is inserted through the skin and into the tumor without making a surgical incision. (The skin is numbed first with a local anesthetic.) The needle is usually guided into place using ultrasound or CT scans. When the images show that the needle is in the tumor, a sample is drawn into the needle and sent to the lab to be viewed under a microscope.
In most cases, this is done as a fine needle aspiration (FNA) biopsy, which uses a very thin needle attached to a syringe to suck out (aspirate) a sample of cells. If this isn’t successful, a core needle biopsy, which uses a slightly larger needle to get a bigger sample, may be done. Doctors don’t usually do a core needle biopsy first because it has a higher chance of spreading cancer cells.
Gallbladder cancer staging
After someone is diagnosed with gallbladder cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and how best to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
The earliest stage gallbladder cancers are called stage 0 (a very early cancer called carcinoma in situ), and then range from stages I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Nearly all gallbladder cancers start in the epithelium (the inside wall of the gallbladder). Over time they grow through the various layers toward the outside of the gallbladder. They may also grow to fill some or all the space inside the gallbladder at the same time.
How is the gallbladder cancer stage determined?
The staging system most often used for gallbladder cancer is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
The extent (size) of the tumor (T): How far has the cancer grown into the wall of the gallbladder? Has the cancer grown through the gallbladder wall into nearby organs such as the liver?
Histologically, the wall of the gallbladder has fewer layers than the wall of the alimentary canal:
- The epithelium, consisting of a simple columnar epithelium, a thin sheet of cells closest to the inside of the gallbladde. The columnar cells of the
lining epithelium concentrate the bile by absorbing some of its water and ions. - The lamina propria, , a thin layer of loose connective tissue (the epithelium plus the lamina propria form the mucosa)
- The muscularis, a layer of one layer of smooth muscle tissue that helps the gallbladder contract, squirting its bile into the bile duct
- The perimuscular (“around the muscle”) fibrous tissue, another layer of connective tissue
- A thick outer layer of connective tissue that is covered by a serosa, the outer covering of the gallbladder that comes from the peritoneum, which is the lining of the abdominal cavity wherever it is not in direct contact with the liver.
The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes and if so, how many?
The spread (metastasis) to distant sites (M): Has the cancer spread to distant organs such as the liver, peritoneum [the lining of the abdominal cavity], or the lungs)?
The system described below is the most recent American Joint Committee on Cancer (AJCC) system effective January 2018. This system is used to stage cancers of the gallbladder as well as cancers that start in the cystic duct (the tube that carries bile away from the gallbladder).
Figure 5. Gallbladder microscopic anatomy
The staging system below uses the pathologic stage (also called the surgical stage) which is determined by examining tissue removed during an operation. Sometimes, if surgery is not possible right away or at all, the cancer will be given a clinical stage instead. This is based on the results of a physical exam, biopsy, and imaging tests. The clinical stage will be used to help plan treatment. Sometimes, though, the cancer has spread further than the clinical stage estimates, and may not predict the patient’s outlook as accurately as a pathologic stage.
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
Cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Gallbladder Cancer Staging
| AJCC Stage | Stage grouping | Stage description* |
| 0 | Tis N0 M0 | Cancer cells are only found in the epithelium (the inner layer of the gallbladder) and have not grown into deeper layers of the gallbladder. This is also known as carcinoma in situ (Tis). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| I | T1 N0 M0 | The tumor has grown into the lamina propria or the muscle layer (muscularis) (T1). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IIA | T2a N0 M0 | The cancer has grown through the muscle layer into the fibrous tissue on the side of the peritoneum (the lining of the abdominal cavity) (T2a). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IIB | T2b N0 M0 | The cancer has grown through the muscle layer into the fibrous tissue on the side of the liver without invading the liver (T2b). It has not yet spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IIIA | T3 N0 M0 | The cancer has grown through the serosa (the outermost covering of the gallbladder) and/or it has grown from the gallbladder directly into the liver and/or a nearby structure such as the stomach, duodenum (first part of the small intestine), colon, pancreas, or bile ducts outside the liver (T3). It has not yet spread to nearby lymph nodes (N0) or to distant sites (M0). |
| IIIB | T1-3 N1 M0 | The cancer has not grown directly into the liver or nearby organs such as the stomach, duodenum, colon, pancreas or bile ducts (T1 to T3), but it has spread to no more than 3 nearby lymph nodes (N1). It has not spread to distant sites (M0). |
| IVA | T4 N0 or N1 M0 | The tumor has grown into one of the main blood vessels leading into the liver (portal vein or hepatic artery) or it has grown into 2 or more structures outside of the liver (T4). It has not spread to nearby lymph nodes (N0) or might have spread to no more than 3 nearby lymph nodes (N1). It has not spread to distant sites (M0). |
| IVB | Any T N2 M0 | The primary tumor may or may not have grown outside the gallbladder. The cancer has spread to 4 or more nearby lymph nodes (N2). It has not spread to distant sites (M0). |
| OR | ||
| Any T Any N M1 | The primary tumor may or may not have grown outside the gallbladder. The cancer may or may not have spread to nearby lymph nodes. Cancer has spread to distant sites such as the liver, peritoneum (the lining of the abdominal cavity), or the lungs (M1). | |
* The following additional categories are not listed on the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- T0: No evidence of a primary tumor.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
Other Prognostic Factors
Besides your stage, there are other factors that can affect your prognosis (outlook).
Grade
The grade describes how closely the cancer looks like normal tissue when seen under a microscope.
The scale used for grading gallbladder cancer is from 1 to 3.
- Grade 1 (G1) means the cancer looks much like normal gallbladder tissue.
- Grade 3 (G3) means the cancer looks very abnormal.
- Grade 2 (G2) falls somewhere in between.
Low-grade cancers (G1) tend to grow and spread more slowly than high-grade (G3) cancers. Most of the time, the outlook is better for Grade 1 and Grade 2 cancers than it is for Grade 3 cancers of the same stage for gallbladder cancer.
Subtype
The specific type of gallbladder cancer you have can influence your outlook. Rare cancer types such as squamous and adenosquamous carcinomas of the gallbladder tend to have a worse prognosis (outlook) than adenocarcinomas. Papillary carcinomas tend to have a favorable prognosis.
Lymphovascular Invasion
If cancer cells are seen in small blood vessels (vascular) or lymph vessels (lymphatics) under the microscope, it is called lymphovascular invasion. When cancer is growing in these vessels, there is an increased risk that it has spread outside the gallbladder. Gallbladder cancers with lymphovascular invasion tend to have a poor prognosis.
Extent of Resection
Whether the entire gallbladder tumor can be removed with surgery can influence your outlook. Cancers that can be removed completely by surgery tend to have a better outlook than those cancers that cannot.
- Resectable cancers are those that doctors believe can be removed completely by surgery.
- Unresectable cancers have spread too far or are in too difficult a place to be removed entirely by surgery.
Unfortunately, only a small portion of gallbladder cancers are resectable when they are first found.
Gallbladder cancer survival rate
To get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. Although the numbers below are among the most current we have available, improvements in treatment since then may result in a better outlook for people now being diagnosed with gallbladder cancer.
The rates below are based on the stage of the cancer at the time of diagnosis. When looking at survival rates, it’s important to understand that the statistics may be different for cancers that have come back or progressed during treatment. Still, the stage of a cancer does not change over time, even if the cancer progresses. A cancer that comes back or spreads is still referred to by the stage it was given when it was first found and diagnosed, but more information is added to explain the current extent of the cancer. (And of course, the treatment plan is adjusted based on the change in cancer status.)
The numbers below come from the American College of Surgeons/American Cancer Society National Cancer Data Base as published in the AJCC Cancer Staging Manual in 2010 and are based on more than 10,000 patients diagnosed with gallbladder cancer from 1989 to 1996.
Table 2. Gallbladder cancer survival rate
| Stage | 5-Year Survival Rate |
| 0 | 80% |
| I | 50% |
| II | 28% |
| IIIA | 8% |
| IIIB | 7% |
| IVA | 4% |
| IVB | 2% |
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen with any particular person. Many other factors can also affect a person’s outlook, such as their age and overall health, and how well the cancer responds to treatment. Even when taking these other factors into account, survival rates are at best rough estimates. Your doctor can tell you how the numbers above apply to you, as he or she knows your situation best.
Gallbladder cancer treatment
What gallbladder cancer treatment options are available to you will depend on the stage of your cancer, your overall health and your preferences.
The initial goal of treatment is to remove the gallbladder cancer, but when that isn’t possible, other therapies may help control the spread of the disease and keep you as comfortable as possible.
After gallbladder cancer is found and staged, your cancer care team will discuss your treatment options with you. The doctors on this team may include:
- A surgeon or a surgical oncologist (a surgeon who specializes in cancer treatment)
- A radiation oncologist: a doctor who uses radiation to treat cancer
- A medical oncologist: a doctor who uses chemotherapy and other medicines to treat cancer
- A gastroenterologist (GI doctor): a doctor who treats diseases of the digestive system
It’s important to discuss all of your treatment options, including their goals and possible side effects, with your doctors to help make the decision that best fits your needs. It’s also very important to ask questions if there is anything you’re not sure about.
The main types of treatments for gallbladder cancer include:
- Surgery
- Radiation therapy
- Chemotherapy
- Palliative therapy
Your treatment plan will depend on the stage of your cancer and other factors.
Surgery for early-stage gallbladder cancer
Surgery may be an option if you have an early-stage gallbladder cancer. Options include:
- Surgery to remove the gallbladder. Early gallbladder cancer that is confined to the gallbladder is treated with an operation to remove the gallbladder (cholecystectomy).
- Surgery to remove the gallbladder and a portion of the liver. Gallbladder cancer that extends beyond the gallbladder and into the liver is sometimes treated with surgery to remove the gallbladder, as well as portions of the liver and bile ducts that surround the gallbladder.
- Removal of the gallbladder and surrounding tissues (radical resection)
If the cancer has spread outside your gallbladder to nearby lymph nodes, your surgeon will do an even bigger operation. The surgeon will remove:
- the gallbladder
- a small part of the liver close to the gallbladder
- the common bile duct
- part or all of a fibrous strap (a ligament) that connects your liver and intestines
- the lymph nodes from around nearby organs such as the liver, stomach, intestines and pancreas
- tissue surrounding the site of any previous keyhole surgery to the gallbladder
Surgery to remove nearby organs affected by the cancer
If your surgeon thinks the cancer has spread to other organs in your body, you may need to have them removed. This can include taking out:
- your pancreas
- your duodenum (the beginning of your small bowel)
- a larger part of your liver
- any other parts of organs that contain cancer cells, for example your stomach or part of your bowel
Operations to remove other organs
You may have other organs taken out during your gallbladder operation. These operations can include:
- Gastrojejunostomy
In a gastrojejunostomy, your surgeon takes out your gallbladder, bile ducts and duodenum and reconnects your stomach to your small bowel (intestine).
- Liver (hepatic) resection
Hepatic resection means taking out part of your liver. Your surgeon may do this if the cancer has spread from your gallbladder to part of your liver. It is only usually possible to do this if the cancer is small and when there are no major blood vessels affected by the cancer.
- Hepatic lobectomy
A hepatic lobectomy means removing a lobe of the liver. If you have no medical problems with your liver (such as cirrhosis) it is possible for the liver to grow back and work normally after surgery.
It is important that your liver function is carefully checked before you have surgery. As the liver is such a vital organ, your doctors need to know that the remaining part of your liver can work well enough after your operation. If you have cirrhosis, your liver may not work well enough for your body to cope. Liver failure after surgery is much more likely in people who have cirrhosis.
- Hepatopancreatoduodenectomy
Hepatopancreatoduodenectomy means taking out your pancreas, duodenum and some liver tissue.
- Pancreatoduodenectomy
Pancreatoduodenectomy is also known as a Whipple’s or Kausch-Whipple’s operation. This means removing:
- part of your pancreas
- your duodenum (the first part of your small bowel)
- part of your stomach
- your gallbladder and part of your bile duct
Large bowel resection
Large bowel resection means taking out part of the large bowel (colon). This will be done if there are signs that the cancer has spread to your large bowel. The affected part of the bowel is cut out and the two ends rejoined.
It’s not clear whether additional treatments after successful surgery can increase the chances that your gallbladder cancer won’t return. Some studies have found this to be the case, so in some instances, your doctor may recommend chemotherapy, radiation therapy or a combination of both after surgery.
Discuss the potential benefits and risks of additional treatment with your doctor to determine what’s right for you.
Treatments for late-stage gallbladder cancer
Surgery can’t cure gallbladder cancer that has spread to other areas of the body. Instead, doctors use treatments that may relieve signs and symptoms of cancer and make you as comfortable as possible.
Options may include:
- Chemotherapy. Chemotherapy is a drug treatment that uses chemicals to kill cancer cells.
- Radiation therapy. Radiation uses high-powered beams of energy, such as X-rays and protons, to kill cancer cells.
- Clinical trials. Clinical trials are studies testing experimental or new medications to treat gallbladder cancer. Talk to your doctor to see whether you’re eligible to participate in a clinical trial.
Procedures to relieve blocked bile ducts
Advanced gallbladder cancer can cause blockages in the bile ducts, causing further complications. Procedures to relieve blockages may help. For instance, surgeons can place a hollow metal tube (stent) in a duct to hold it open or surgically reroute bile ducts around the blockage (biliary bypass).
Coping and support
Learning you have any life-threatening illness can be devastating. And coping with a diagnosis of gallbladder cancer can be especially difficult because the disease often carries a poor prognosis. Some ideas for learning to cope with gallbladder cancer include:
Ask questions about gallbladder cancer. Write down questions you have about your cancer. Ask these questions at your next appointment. Also ask your doctor for reliable sources where you can get more information.
Knowing more about your gallbladder cancer and your treatment options may make you more comfortable when it comes to making decisions about your care.
Stay connected to friends and family. Your cancer diagnosis can be stressful for friends and family, too. Try to keep them involved in your life.
Your friends and family will likely ask if there’s anything they can do to help you. Think of tasks you might like help with, such as caring for your home if you have to stay in the hospital or just being there when you want to talk.
You may find comfort in the support of a caring group of your friends and family.
Find someone to talk with. Find someone you can talk to who has experience with people facing a life-threatening illness. Consult a counselor, medical social worker, clergy member or a support group for people with cancer.
Write down your medical wishes. Take steps to ensure that your wishes are known and respected.
Ask your doctor about advance directives, which allow you to indicate what types of treatment you’d want in the event you can’t communicate your wishes.
Also ask about designating a medical power of attorney, which is someone you designate to make your choices for you if you can’t communicate.





{kind=link}