Contents
What is gallbladder pain ?
The liver produces bile, a greenish yellow, thick, sticky fluid. Bile aids digestion by making cholesterol, fats, and fat-soluble vitamins easier to absorb from the intestine. Bile also helps eliminate certain waste products (mainly bilirubin and excess cholesterol) and by-products of drugs from the body.
The biliary tract consists of small tubes (ducts) that carry bile from the liver to the gallbladder and then to the small intestine. The gallbladder is a small, pear-shaped sac located beneath the liver. The gallbladder stores bile between meals, reabsorbs water to concentrate bile, and contracts to release bile into the small intestine. The gallbladder connects to the cystic duct, which in turn joins the common hepatic duct (Figure 1 and 2). When bile is needed, as when people eat, the gallbladder contracts, pushing bile through the bile ducts into the small intestine.
The flow of bile can be blocked by the following 1:
- Gallstones that pass out of the gallbladder into the ducts
- Injury to the bile ducts during gallbladder surgery
- Narrowing of the bile ducts caused by factors such as AIDS-related infections and primary sclerosing cholangitis
- Disorders of the pancreas, which can narrow the bile ducts that pass through the pancreas
- Tumors in the pancreas, gallbladder, or bile ducts
- Infestation by parasites (in Asia)
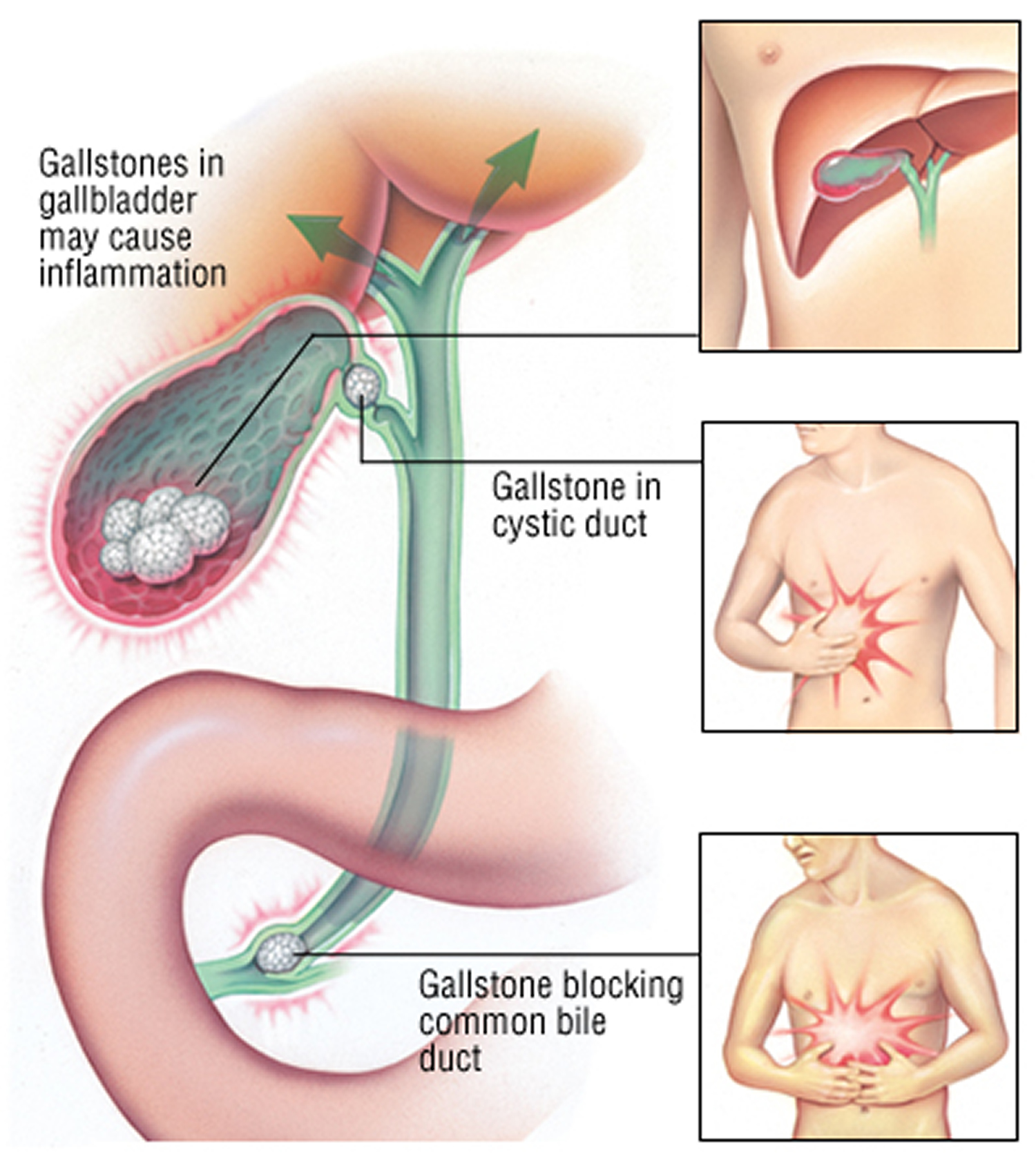
If the bile ducts are blocked, the gallbladder may become inflamed (cholecystitis).
Over 95 percent of cholecystitis is caused by gallbladder stones.
Gallbladder pain is commonly caused by a gallstone blocking the cystic duct, the tube through which bile travels into and out of the gallbladder 2. When a stone (gallstone) blocks this duct, bile builds up, causing irritation and pressure in the gallbladder. This can lead to swelling and infection of the gallbladder, a medical condition called cholecystitis.
However, gallbladder pain without gallstones (acalculous biliary pain) can also occur.
Cholecystitis can lead to a number of serious complications, including:
- Infection within the gallbladder. If bile builds up within your gallbladder, causing cholecystitis, the bile may become infected.
- Death of gallbladder tissue. Untreated cholecystitis can cause tissue in the gallbladder to die, which in turn can lead to a tear in the gallbladder, or it may cause your gallbladder to burst.
- Torn gallbladder. A tear in your gallbladder may result from gallbladder enlargement or infection.
Make an appointment with your doctor if you have signs or symptoms that worry you. If your doctor suspects you have cholecystitis, he or she may either refer you to a doctor who specializes in the digestive system (gastroenterologist) or send you to a hospital.
Acute cholecystitis
Acute cholecystitis begins suddenly, resulting in severe, steady pain in the upper abdomen. The pain usually lasts more than 6 hours. At least 95% of people with acute cholecystitis have gallstones 3. The inflammation almost always begins without infection, although infection may follow later. Inflammation may cause the gallbladder to fill with fluid and its walls to thicken.
Rarely, a form of acute cholecystitis without gallstones (acalculous cholecystitis) occurs 3. However, the gallbladder may contain sludge (microscopic particles of materials similar to those in gallstones). Acalculous cholecystitis is more serious than other types of cholecystitis. It tends to occur after the following:
- Major surgery
- Critical illnesses such as serious injuries, severe burns, or a bloodstream infection (sepsis)
- Intravenous feedings for a long time
- Fasting for a long time
- A deficiency in the immune system
Acute acalculous cholecystitis can occur in young children, perhaps developing from a viral or another infection.
Some people are more at risk for gallstones. Risk factors include:
- Being female
- Pregnancy
- Hormone therapy
- Older age
- Being Native American or Hispanic
- Obesity
- Losing or gaining weight rapidly
- Diabetes
Sometimes the bile duct becomes blocked temporarily. When this occurs repeatedly, it can lead to chronic cholecystitis. This is swelling and irritation that continues over time. Eventually, the gallbladder becomes thick and hard. It does not store and release bile as well as it did.
Prevention of acute cholecystitis
Removing the gallbladder and gallstones will prevent further attacks.
Symptoms of acute cholecystitis
The main symptom is pain in the upper right side or upper middle of your belly that begins suddenly that usually lasts at least 30 minutes (usually lasts more than 6 hours). You may feel:
- Sharp, cramping, or dull pain
- Steady pain
- Pain that spreads to your back or below your right shoulder blade
Other symptoms that may occur include:
- Clay-colored stools
- Fever
- Nausea and vomiting
- Yellowing of skin and whites of the eyes (jaundice)
Acute cholecystitis diagnosis
Your health care provider will perform a physical exam and ask about your symptoms. During the physical exam, you will likely have pain when the provider touches your belly.
Your provider may order the following blood tests:
- Amylase and lipase
- Bilirubin
- Complete blood count (CBC)
- Liver function tests
Imaging tests can show gallstones or inflammation. You may have one of these tests:
- Abdominal ultrasound
- Abdominal CT scan
- Abdominal x-ray
- Oral cholecystogram
- Gallbladder radionuclide scan
Treatment for acute cholecystitis
If you have severe belly pain, seek medical attention right away.
In the emergency room, you’ll be given fluids through a vein. You also may be given antibiotics to fight infection.
Cholecystitis may clear up on its own. However, if you have gallstones, you will probably need surgery to remove your gallbladder.
Nonsurgical treatment includes:
- Antibiotics you take at home to fight infection
- Low-fat healthy diet (if you are able to eat). Diets high in fat and low in fiber may increase the risk of gallstones. To reduce your risk of gallstones, choose a diet high in fruits, vegetables and whole grains.
- Pain medicines
- Lose weight slowly. Rapid weight loss can increase the risk of gallstones. If you need to lose weight, aim to lose 1 or 2 pounds (0.5 to about 1 kilogram) a week.
- Maintain a healthy weight. Being overweight increase the risk of gallstones. To achieve a healthy weight, reduce calories and increase the physical activity. Maintain a healthy weight by continuing to eat well and exercise.
Hospitalization
If you’re diagnosed with cholecystitis, you’ll likely be hospitalized. Your doctor will work to control your signs and symptoms and to control the inflammation in your gallbladder. Treatments may include:
- Fasting. You may not be allowed to eat or drink at first in order to take stress off your inflamed gallbladder. So that you don’t become dehydrated, you may receive fluids through a vein in your arm.
- Antibiotics to fight infection. If your gallbladder is infected, your doctor likely will recommend antibiotics.
- Pain medications. These can help control pain until the inflammation in your gallbladder is relieved.
Your symptoms are likely to subside in a day or two.
You may need emergency surgery if you have complications such as:
- Gallbladder gangrene (tissue death)
- Perforation (a hole that forms in the wall of the gallbladder)
- Pancreatitis (inflamed pancreas)
- Persistent bile duct blockage
- Inflammation of the common bile duct
If you are very ill, a tube may be placed through your belly into your gallbladder to drain it. Once you feel better, you may have surgery.
Outlook (Prognosis) for acute cholecystitis
Most people who have surgery to remove their gallbladder recover completely.
Possible Complications of acute cholecystitis
Untreated, cholecystitis may lead to any of the following health problems:
- Empyema (pus in the gallbladder)
- Gangrene
- Injury to the bile ducts draining the liver (may occur after gallbladder surgery)
- Pancreatitis
- Perforation
- Peritonitis (inflammation of the lining of the abdomen)
Figure 1. Gallbladder location
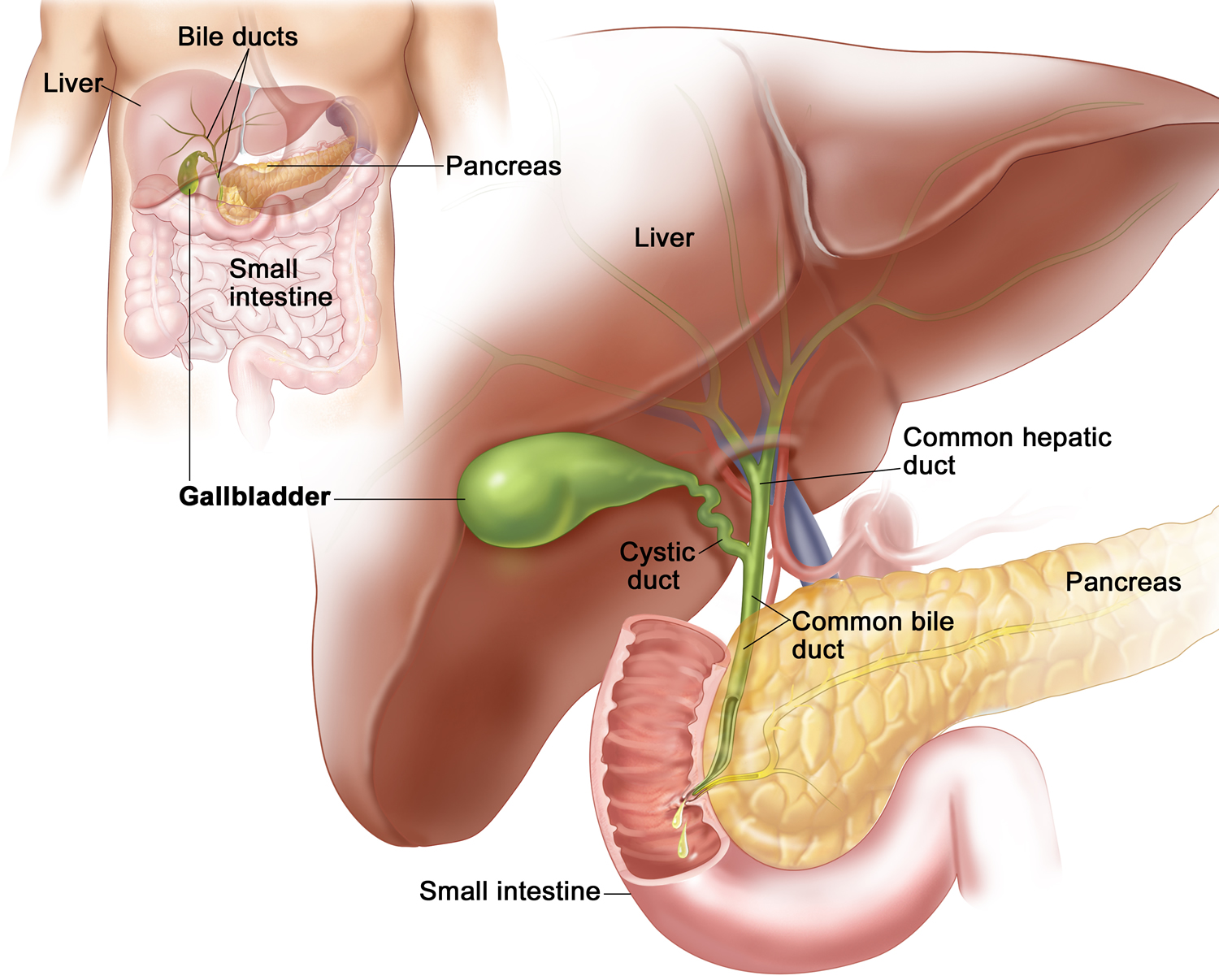
Figure 2. Gallbladder anatomy
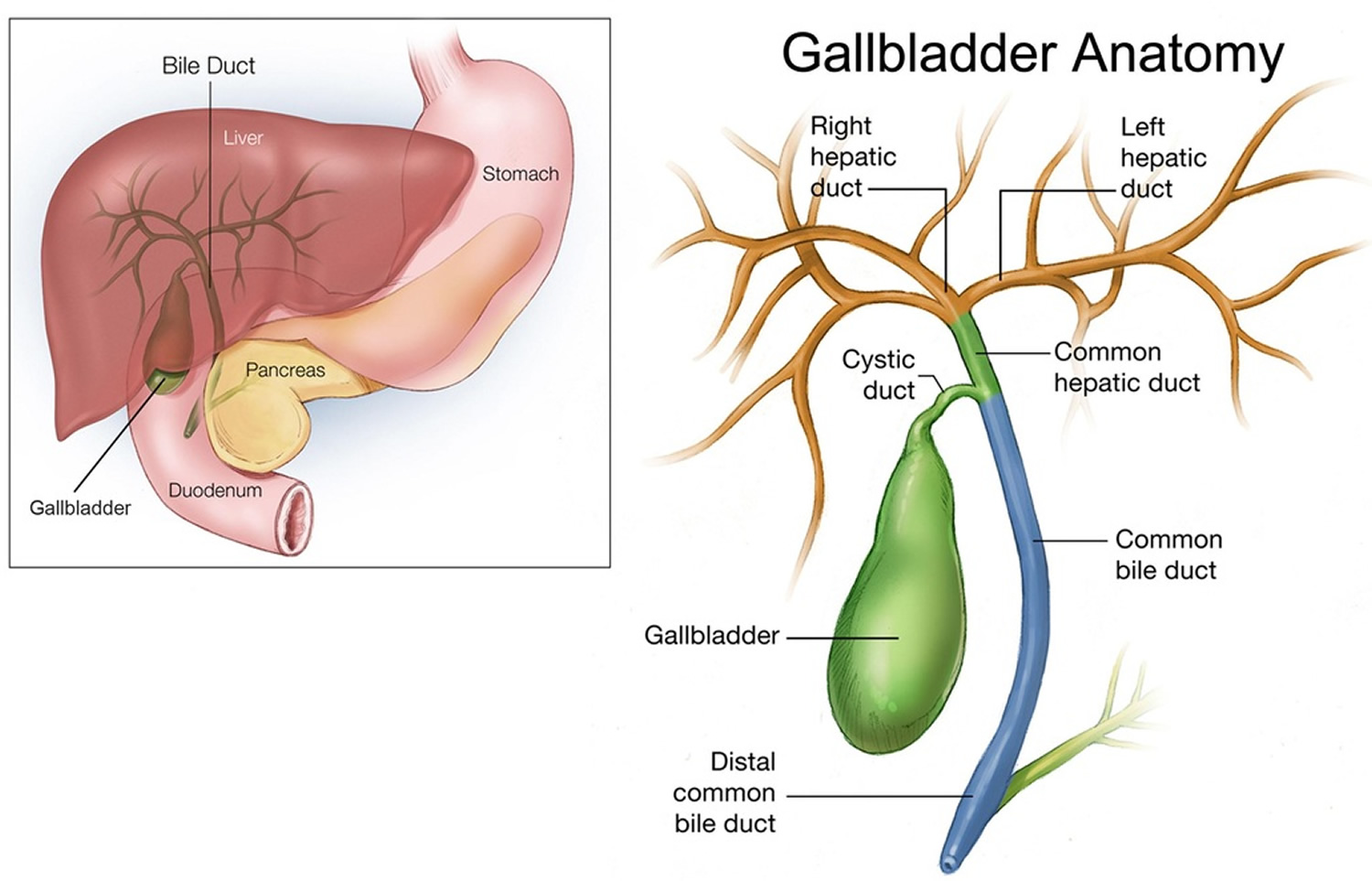
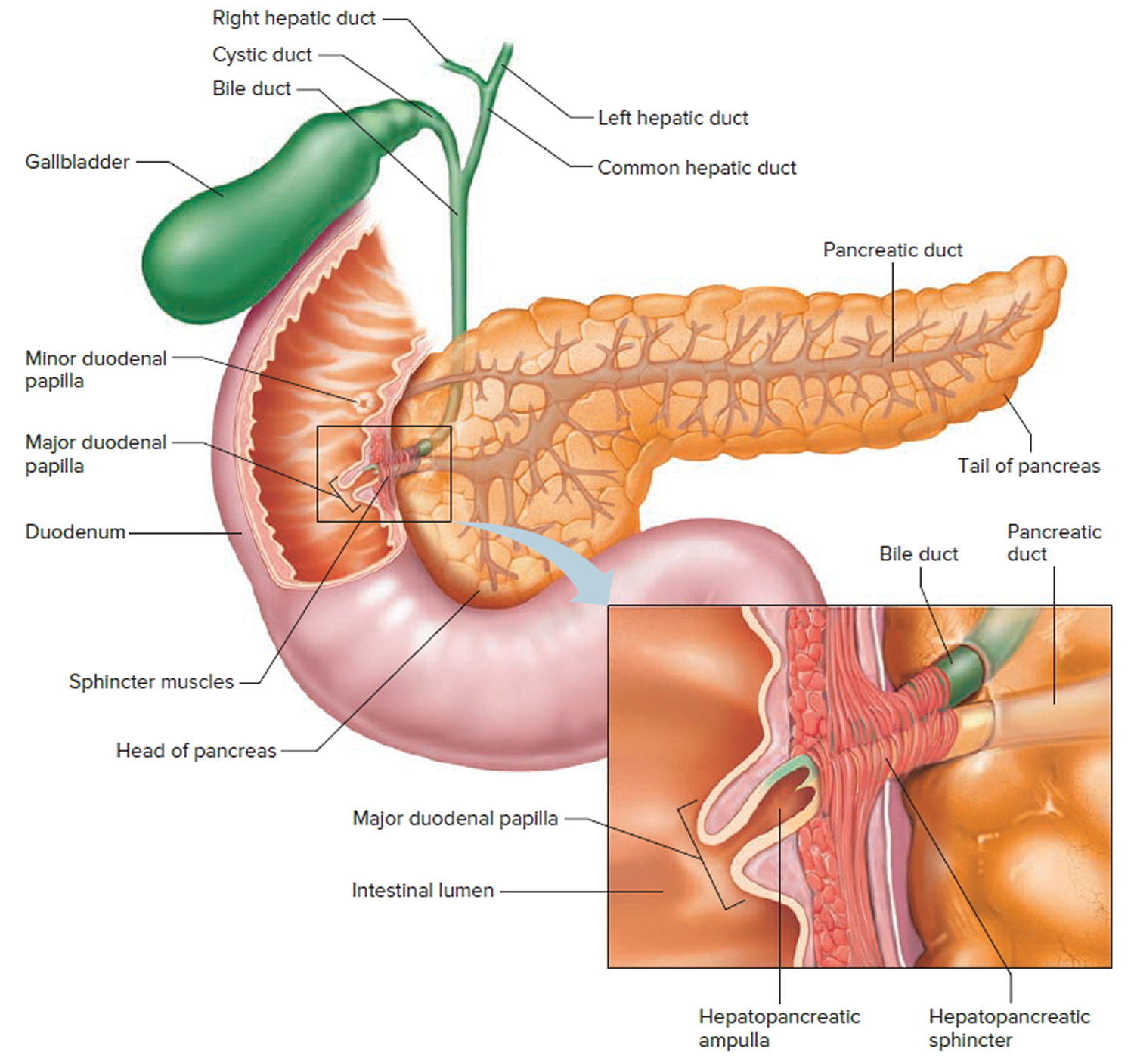
Figure 3. The common bile duct is closely associated with the pancreatic duct and the duodenum
What are gallstones ?
Gallstones are solid clumps of cholesterol crystals or pigment material that form in the gallbladder. Gallstones can range in size from a grain of sand to a golf ball. The gallbladder can develop a single large gallstone, hundreds of tiny stones, or both small and large stones. Gallstones can cause sudden pain in the upper right abdomen. This pain, called a gallbladder attack or biliary colic, occurs when gallstones block the ducts of the biliary tract.
In the United States, more than 80% of gallstones contain cholesterol as their major component 4. Over the past two decades, much has been learned about the epidemiology of this condition and its risk factors.
Figure 4. Gallstones
How are gallstones formed ?
Imbalances in the substances that make up bile cause gallstones. Gallstones may form if bile contains too much cholesterol, too much bilirubin, or not enough bile salts. Scientists do not fully understand why these imbalances occur. Gallstones also may form if the gallbladder does not empty completely or often enough.
When there is too much of these bile components, they precipitate and form solid crystals. These clump together forming gallstones also known as cholelithiasis 5.
Are all gallstones the same ?
No. There are two different types of gallstones, depending on what component of the bile has solidified. Also, the stones can vary in size ranging from tiny, sand-like particles less than one millimeter in diameter to ping pong ball-like particles more than four centimeters in diameter. Almost 90 percent of gallstones are composed of cholesterol. The remainder consist of pigment material (bilirubin). The reason for the formation of pigment stones is not yet fully understood. However, some people with blood disorders such as sickle cell anemia are at risk for developing pigment stones.
Who is at risk for developing gallstones ?
Certain people have a higher risk of developing gallstones than others 6:
- Women are more likely to develop gallstones than men. Extra estrogen can increase cholesterol levels in bile and decrease gallbladder contractions, which may cause gallstones to form. Women may have extra estrogen due to pregnancy, hormone replacement therapy, or birth control pills.
- People over age 40 are more likely to develop gallstones than younger people.
- People with a family history of gallstones have a higher risk.
- American Indians have genetic factors that increase the amount of cholesterol in their bile. In fact, American Indians have the highest rate of gallstones in the United States—almost 65 percent of women and 30 percent of men have gallstones.
- Mexican Americans are at higher risk of developing gallstones.
Other factors that affect a person’s risk of gallstones include 6:
- Obesity. People who are obese, especially women, have increased risk of developing gallstones. Obesity increases the amount of cholesterol in bile, which can cause stone formation.
- Rapid weight loss. As the body breaks down fat during prolonged fasting and rapid weight loss, the liver secretes extra cholesterol into bile. Rapid weight loss can also prevent the gallbladder from emptying properly. Low-calorie diets and bariatric surgery—surgery that limits the amount of food a person can eat or digest—lead to rapid weight loss and increased risk of gallstones.
- Diet. Research suggests diets high in calories and refined carbohydrates and low in fiber increase the risk of gallstones. Refined carbohydrates are grains processed to remove bran and germ, which contain nutrients and fiber. Examples of refined carbohydrates include white bread and white rice.
- Certain intestinal diseases. Diseases that affect normal absorption of nutrients, such as Crohn’s disease, are associated with gallstones.
- Metabolic syndrome, diabetes, and insulin resistance. These conditions increase the risk of gallstones. Metabolic syndrome also increases the risk of gallstone complications. Metabolic syndrome is a group of traits and medical conditions linked to being overweight or obese that puts people at risk for heart disease and type 2 diabetes.
Pigment stones tend to develop in people who have:
- Cirrhosis of the liver—a condition in which the liver slowly deteriorates and malfunctions due to chronic, or long lasting, injury
- Infections in the bile ducts
- Severe hemolytic anemias—conditions in which red blood cells are continuously broken down, such as sickle cell anemia.
Prevention of gallstones
Factors related to eating, diet, and nutrition that increase the risk of gallstones include:
- obesity
- rapid weight loss
- diets high in calories and refined carbohydrates and low in fiber
Because obesity is a risk factor, people should aim to maintain an ideal body weight through proper diet and nutrition. Otherwise there is no specific diet for gallstone disease. Very obese individuals who are attempting drastic weight reduction are at risk for developing gallstones. They should lose weight under medical supervision.
Ursodiol can help prevent gallstones in people who rapidly lose weight through low-calorie diets or bariatric surgery. People should talk with their health care provider or dietitian about what diet is right for them.
What symptoms are associated with gallstones ?
Patients with symptomatic gallstones experience severe abdominal pain, and may suffer further complications such as jaundice (yellowing of the skin and eyes), and inflammation of the gallbladder, bile ducts, liver or pancreas. However, about 80 percent of people who have gallstones have no symptoms. These people are said to have so-called “silent” gallstones with no associated pain. Silent gallstones do not interfere with the function of the gallbladder, liver, or pancreas. Gas and indigestion are not specific symptoms of gallstones or gallbladder disease.
If gallstones block the bile ducts, pressure increases in the gallbladder, causing a gallbladder attack. The pain usually lasts from 1 to several hours 7. Gallbladder attacks often follow heavy meals, and they usually occur in the evening or during the night.
Gallbladder attacks usually stop when gallstones move and no longer block the bile ducts. However, if any of the bile ducts remain blocked for more than a few hours, complications can occur. Complications include inflammation, or swelling, of the gallbladder and severe damage or infection of the gallbladder, bile ducts, or liver.
A gallstone that becomes lodged in the common bile duct near the duodenum and blocks the pancreatic duct can cause gallstone pancreatitis—inflammation of the pancreas.
Left untreated, blockages of the bile ducts or pancreatic duct can be fatal.
People with any of the following symptoms during or after a gallbladder attack should see a health care provider immediately 8:
- Abdominal pain lasting more than 5 hours
- Nausea and vomiting
- Fever—even a low-grade fever—or chills
- Yellowish color of the skin or whites of the eyes, called jaundice
- Tea-colored urine and light-colored stools
These symptoms may be signs of serious infection or inflammation of the gallbladder, liver, or pancreas.
How are gallstones diagnosed ?
A health care provider will usually order an ultrasound exam to diagnose gallstones. Other imaging tests may also be used.
Ultrasound exam
Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. A specially trained technician performs the procedure in a health care provider’s office, outpatient center, or hospital, and a radiologist—a doctor who specializes in medical imaging—interprets the images. Anesthesia is not needed. If gallstones are present, they will be visible in the image. Ultrasound is the most accurate method to detect gallstones.
Computerized tomography (CT) scan
A CT scan is an x ray that produces pictures of the body. A CT scan may include the injection of a special dye, called contrast medium. CT scans use a combination of x rays and computer technology to create three-dimensional (3-D) images. CT scans require the person to lie on a table that slides into a tunnel-shaped device where the x rays are taken. An x-ray technician performs the procedure in an outpatient center or hospital, and a radiologist interprets the images. Anesthesia is not needed. CT scans can show gallstones or complications, such as infection and blockage of the gallbladder or bile ducts. However, CT scans can miss gallstones that are present.
Magnetic resonance imaging (MRI)
MRI machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues without using x rays. A specially trained technician performs the procedure in an outpatient center or hospital, and a radiologist interprets the images. Anesthesia is not needed, though people with a fear of confined spaces may receive light sedation. An MRI may include the injection of contrast medium. With most MRI machines, the person lies on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some newer machines allow the person to lie in a more open space. MRIs can show gallstones in the ducts of the biliary system.
Cholescintigraphy
Cholescintigraphy—also called a hydroxyl iminodiacetic acid scan, HIDA scan, or hepatobiliary scan—uses an unharmful radioactive material to produce pictures of the biliary system. In cholescintigraphy, the person lies on an exam table and a health care provider injects a small amount of unharmful radioactive material into a vein in the person’s arm. The health care provider may also inject a substance that causes the gallbladder to contract. A special camera takes pictures of the radioactive material as it moves through the biliary system. A specially trained technician performs the procedure in an outpatient center or hospital, and a radiologist interprets the images. Anesthesia is not needed. Cholescintigraphy is used to diagnose abnormal contractions of the gallbladder or obstruction of the bile ducts.
Endoscopic retrograde cholangiopancreatography (ERCP)
ERCP uses an x ray to look into the bile and pancreatic ducts. After lightly sedating the person, the health care provider inserts an endoscope—a small, flexible tube with a light and a camera on the end—through the mouth into the duodenum and bile ducts. The endoscope is connected to a computer and video monitor. The health care provider injects contrast medium through the tube into the bile ducts, which makes the ducts show up on the monitor. The health care provider performs the procedure in an outpatient center or hospital. ERCP helps the health care provider locate the affected bile duct and the gallstone. The stone is captured in a tiny basket attached to the endoscope and removed. This test is more invasive than other tests and is used selectively.
Health care providers also use blood tests to look for signs of infection or inflammation of the bile ducts, gallbladder, pancreas, or liver. A blood test involves drawing blood at a health care provider’s office or commercial facility and sending the sample to a lab for analysis.
Gallstone symptoms may be similar to those of other conditions, such as appendicitis, ulcers, pancreatitis, and gastroesophageal reflux disease.
Sometimes, silent gallstones are found when a person does not have any symptoms. For example, a health care provider may notice gallstones when performing ultrasound for a different reason.
How are gallstones treated ?
If gallstones are not causing symptoms, treatment is usually not needed. However, if a person has a gallbladder attack or other symptoms, a health care provider will usually recommend treatment. A person may be referred to a gastroenterologist—a doctor who specializes in digestive diseases—for treatment. If a person has had one gallbladder attack, more episodes will likely follow.
The usual treatment for gallstones is surgery to remove the gallbladder. If a person cannot undergo surgery, nonsurgical treatments may be used to dissolve cholesterol gallstones. A health care provider may use ERCP to remove stones in people who cannot undergo surgery or to remove stones from the common bile duct in people who are about to have gallbladder removal surgery.
Surgery
Surgery to remove the gallbladder, called cholecystectomy, is one of the most common operations performed on adults in the United States.
The gallbladder is not an essential organ, which means a person can live normally without a gallbladder. Once the gallbladder is removed, bile flows out of the liver through the hepatic and common bile ducts and directly into the duodenum, instead of being stored in the gallbladder.
Surgeons perform two types of cholecystectomy:
Laparoscopic cholecystectomy. In a laparoscopic cholecystectomy, the surgeon makes several tiny incisions in the abdomen and inserts a laparoscope—a thin tube with a tiny video camera attached. The camera sends a magnified image from inside the body to a video monitor, giving the surgeon a close-up view of organs and tissues. While watching the monitor, the surgeon uses instruments to carefully separate the gallbladder from the liver, bile ducts, and other structures. Then the surgeon removes the gallbladder through one of the small incisions. Patients usually receive general anesthesia.
Most cholecystectomies are performed with laparoscopy. Many laparoscopic cholecystectomies are performed on an outpatient basis, meaning the person is able to go home the same day. Normal physical activity can usually be resumed in about a week 9.
Open cholecystectomy. An open cholecystectomy is performed when the gallbladder is severely inflamed, infected, or scarred from other operations. In most of these cases, open cholecystectomy is planned from the start. However, a surgeon may perform an open cholecystectomy when problems occur during a laparoscopic cholecystectomy. In these cases, the surgeon must switch to open cholecystectomy as a safety measure for the patient.
To perform an open cholecystectomy, the surgeon creates an incision about 4 to 6 inches long in the abdomen to remove the gallbladder 10. Patients usually receive general anesthesia. Recovery from open cholecystectomy may require some people to stay in the hospital for up to a week. Normal physical activity can usually be resumed after about a month 9.
A small number of people have softer and more frequent stools after gallbladder removal because bile flows into the duodenum more often. Changes in bowel habits are usually temporary; however, they should be discussed with a health care provider.
Though complications from gallbladder surgery are rare, the most common complication is injury to the bile ducts. An injured common bile duct can leak bile and cause a painful and possibly dangerous infection. One or more additional operations may be needed to repair the bile ducts. Bile duct injuries occur in less than 1 percent of cholecystectomies 11.
Nonsurgical Treatments for Cholesterol Gallstones
Nonsurgical treatments are used only in special situations, such as when a person with cholesterol stones has a serious medical condition that prevents surgery. Gallstones often recur within 5 years after nonsurgical treatment 12.
Two types of nonsurgical treatments can be used to dissolve cholesterol gallstones:
Oral dissolution therapy. Ursodiol (Actigall) and chenodiol (Chenix) are medications that contain bile acids that can dissolve gallstones. These medications are most effective in dissolving small cholesterol stones. Months or years of treatment may be needed to dissolve all stones.
Shock wave lithotripsy. A machine called a lithotripter is used to crush the gallstone. The lithotripter generates shock waves that pass through the person’s body to break the gallstone into smaller pieces. This procedure is used only rarely and may be used along with ursodiol.
Acalculous cholecystitis
Acalculous cholecystitis a rare form of acute cholecystitis without gallstones, typically causes sudden, excruciating pain in the upper abdomen in people with no previous symptoms or other evidence of a gallbladder disorder. The inflammation is often very severe and can lead to gangrene or rupture of the gallbladder.
People with acalculous cholecystitis tend to be very ill. For example, they may be in the intensive care unit for another reason and have many other symptoms. Also, because these people are so ill, they may not be able to communicate very clearly. For these reasons, acalculous cholecystitis may be overlooked at first.
The only symptoms may be a swollen (distended), tender abdomen or a fever with no known cause. If untreated, acalculous cholecystitis results in death for 65% of people 3.
Acalculous cholecystitis is more serious than other types of cholecystitis. It tends to occur after the following:
- Major surgery
- Critical illnesses such as serious injuries, severe burns, or a bloodstream infection (sepsis)
- Intravenous feedings for a long time
- Fasting for a long time
- A deficiency in the immune system
Acute acalculous cholecystitis can occur in young children, perhaps developing from a viral or another infection.
Acalculous biliary pain is most common among young women.
This disorder may develop when bile (produced by the gallbladder) does not pass through the ducts into the small intestine as it usually does. Passage of bile may be slowed or blocked because 13:
- Gallstones, which may be too small to be detected by ultrasonography, are present.
- For unknown reasons, the gallbladder does not empty normally.
- The biliary tract or small intestine is overly sensitive.
- The ring-shaped muscle between the common bile and pancreatic ducts and small intestine (sphincter of Oddi) malfunctions.
- Gallstones may have blocked the ducts, then passed through before they were detected.
Some people with acalculous biliary pain eventually develop other unexplained (functional) disorders of the digestive tract.
Doctors suspect this disorder if people have biliary pain but ultrasonography shows no stones 13.
The best way to confirm the diagnosis is unclear 13. Usually, cholescintigraphy, a type of radionuclide imaging, is done after people are given a drug that causes the gallbladder to contract. If the gallbladder does not fully contract, removing the gallbladder may cause symptoms to resolve.
Surgical removal of the gallbladder (cholecystectomy) is usually done using a flexible viewing tube called a laparoscope. After small incisions are made in the abdomen, the laparoscope and surgical instruments are inserted through the incisions. Doctors then use instruments to remove the gallbladder.
Cholecystectomy may also cause symptoms to resolve if they were caused by gallstones that are too small to be detected by ultrasonography.
What are gallbladder polyps ?
Gallbladder polyps are growths that protrude from the lining of the inside of the gallbladder. Polyps can be cancerous, but they rarely are 14. About 95 percent of gallbladder polyps are benign 14.
In the majority of patients, diagnosis of gallbladder polyps is an incidental finding of a routine abdominal ultrasound or following cholecystectomy for gallstones or biliary colic 15.
The size of a gallbladder polyp can help predict whether it’s cancerous (malignant) or noncancerous (benign).
Small gallbladder polyps that are less than 1/2 inch — about 10 millimeters (mm) — in diameter are unlikely to be cancerous and generally don’t require treatment 14. However, for these polyps, your doctor may suggest follow-up examinations to look for changes that may be an indication of cancer. This can be done using standard abdominal ultrasound or endoscopic ultrasound.
Gallbladder polyps larger than 1/2 inch (about 10 mm) in diameter are more likely to be cancerous or turn into cancer over time, and those larger than 3/4 inch (18 mm) in diameter may pose a significant risk of being malignant 14. Treatment of larger gallbladder polyps includes surgical removal of the gallbladder (cholecystectomy). Again, malignant polyps are extremely rare. Only about 5 percent of gallbladder polyps are cancerous 14.
Gallbladder cancer is a rather uncommon disease, but when it gives symptoms it has usually reached an incurable stage. Therefore, every attempt must be made to find the asymptomatic stages and look for premalignant gallbladder polyps 15.
Your doctor may also recommend cholecystectomy if you have a gallbladder polyp of any size accompanied with gallstones.
Types of gallbladder polyps
Benign gallbladder polyps are subdivided into: pseudotumors (cholesterol polyps, inflammatory polyps; cholesterolosis and hyperplasia), epithelial tumors (adenomas) and mesenchymatous tumors (fibroma, lipoma, and hemangioma).
Malignant gallbladder polyps are gallbladder carcinomas. The poor prognosis of gallbladder carcinoma patients means it is important to differentiate between benign polyps and malignant or premalignant polyps 16.
Incidence of gallbladder polyps
The prevalence of gallbladder polyps was reported as 4.3–6.9%. Polypoid gallbladder lesions include a variety of pathologic types. Although there are some differences according to reports, the prevalence of polypoid lesions of the gall bladder are reported in 2–12% of cholecystectomy specimens, probably dependent on indications for cholecystectomy 17.
Age and gender seem to be notable factors for incidence of gallbladder polyps. In a study of 1558 patients with gallbladder polyps, the age at the time of diagnosis was 49 years 18. In the majority of publications in which the ratio is calculated, the incidence is more prevalent in men 19. The sex ratio and age at the time of diagnosis of gallbladder polyps was 1.15 to 1 (male to female) 20.
Risk factors for gallbladder polyps
Polyps of gall bladder are tumor-like lesions of this organ. Little has been known about factors associated with the occurrence of gallbladder polyps. The formation of gallbladder polyps is however associated with fat metabolism. Relationship between gallbladder polyps and family history of some diseases suggests to perform some genetic studies 21.
In contrast to the well-known risk factors for gallstones, attempts to identify risk factors for developing gallbladder polyps have not shown any consistent relationship between formation of polyps and age, gender, obesity, or medical conditions such as diabetes. There is some literature to suggest an inverse relationship between gallbladder polyps and stones. It is hypothesized that polyps either mechanically disrupt the formation of stones or that polyps are harder to diagnose radiographically when stones are present 22.
Patients with congenital polyposis syndromes such as Peutz-Jeghers and Gardner syndrome can also develop gallbladder polyps. A large retrospective analysis of risk factors for gallbladder polyps in the Chinese population identified chronic hepatitis B as a risk factor 22.
Proposed patient risk factors for malignant gallbladder polyps include age greater than 60, presence of gallstones, and primary sclerosing cholangitis. Polyp risk characteristics include a size greater than 6 mm, solitary, and sessile 22.
Gallbladder polyps symptoms
The presenting symptoms of polypoid lesions of the gallbladder are nonspecific and vague, and in many cases asymptomatic. For such reason, polypoid lesions of the gallbladder are often detected incidentally 23. However, there are some patients with gallbladder polyps which may suffer nausea, vomiting, and occasional pain in the right hypochondrium, due to intermittent obstructions caused by small fragments of cholesterol that become detached from the gallbladder mucosa. There are descriptions of polyps that protrude greatly obstructing the cystic canal or the primary biliary ducts, causing acute cholecystitis or obstructive jaundice, but these are very rare complications 24.
Polyps are sometimes identified on transabdominal ultrasounds done for right upper quadrant pain. In the absence of other findings, the gallbladder polyp may be considered a source of biliary colic. If any symptoms are caused, most commonly right upper quadrant pain, nausea, dyspepsia, and jaundice are seen. However, most of the patients have gallstones; it is unclear whether the polyps were primarily driving the symptoms. There was no difference in presenting symptoms between patients with benign versus malignant polyps. In a large retrospective analysis found to have gallbladder polyps on abdominal ultrasound, 64% of these polyps were diagnosed during a work-up of unrelated illness. Twenty-three percent had abdominal symptoms, and 13% had elevated liver function tests. Cholesterol polyps may detach and behave clinically as a gallstone, causing biliary colic, obstruction, or even pancreatitis. There are also reports of gallbladder polyps causing acalculous cholecystitis or even massive hemobilia 22.
Symptoms may be associated with pseudo-polyps such as a cholesterol polyp, inflammatory or hyperplastic polyp, which include indigestion, right upper quadrant pain, and discomfort, cholecystitis or gallbladder stone 25. Metabolic syndrome has a close relationship with the development of cholesterol polyps 25.
Primary sclerosing cholangitis
Primary sclerosing cholangitis is inflammation with progressive scarring and narrowing of the bile ducts in and outside the liver 26. Eventually, the bile ducts become blocked and then obliterated. Cirrhosis, liver failure, and sometimes bile duct cancer develop.
- Symptoms begin gradually and include worsening fatigue, itchiness, and, later, jaundice.
- An imaging test can confirm the diagnosis.
- Treatment focuses on relieving symptoms, but liver transplantation can prolong life.
In primary sclerosing cholangitis, scarring worsens, eventually becoming severe (cirrhosis). The scar tissue narrows and blocks the bile ducts. As a result, bile salts, which help the body absorb fats, are not secreted normally. The disorder resembles primary biliary cirrhosis except that it affects the bile ducts outside the liver as well as those in the liver. The cause is not known but is likely to be autoimmune (when the immune system attacks the body’s own tissues).
Primary sclerosing cholangitis most often affects young men at an average age of 40. It commonly occurs in people with inflammatory bowel disease, especially ulcerative colitis. It tends to occur in families, suggesting that genes may be involved. An infection or injury of the bile ducts may trigger the disorder in people who have genes that make them susceptible to the disorder. The bile ducts may be injured during an endoscopic procedure, such as placement of tubes (stents) intended to keep the bile ducts open.
Primary sclerosing cholangitis is one of the risk factors for malignancy in a gallbladder polyp. Any gallbladder polyp, regardless of size, in a patient with primary sclerosing cholangitis should be considered for cholecystectomy 15. Solitary sessile polyps greater than 10 mm in patients over age 50 should be considered for cholecystectomy, particularly in patients with cholelithiasis and primary sclerosing cholangitis 27. Although gallbladder polyps are common and are usually benign in the general population, they are often malignant in primary sclerosing cholangitis. Therefore, regardless of size, any gallbladder polyps in a patient with primary sclerosing cholangitis should be considered for cholecystectomy 28. If a cholecystectomy is not performed, careful follow-up is warranted 29.
Symptoms of primary sclerosing cholangitis
Symptoms usually begin gradually with worsening fatigue and itchiness. Jaundice (yellowish discoloration of the skin and whites of the eyes) tends to develop later.
Inflammation and recurring infection of the bile ducts (bacterial cholangitis) sometimes occur. Bacterial cholangitis causes attacks of pain in the upper abdomen, jaundice, and fever.
Because bile salts are not secreted normally, people may be unable to absorb enough fats and fat-soluble vitamins (A, D, E, and K). Such impaired bile secretion results in osteoporosis, easy bruising and bleeding, and stools that are greasy and foul-smelling (steatorrhea). Gallstones and bile duct stones develop in about three fourths of people with primary sclerosing cholangitis. The liver and spleen may enlarge.
As the disorder progresses, symptoms of cirrhosis develop. Advanced cirrhosis causes the following:
- Increased blood pressure in the vein that carries blood from the intestines to the liver (portal hypertension)
- Accumulation of fluid in the abdominal cavity (ascites)
- Liver failure, which can be fatal
Some people have no symptoms until the disorder is advanced and cirrhosis is present. Symptoms may not appear for up to 10 years.
Cancer of the bile ducts (cholangiocarcinoma) develops in 10 to 15% of people with primary sclerosing cholangitis.
Usually, primary sclerosing cholangitis worsens gradually. Liver failure occurs about 12 years after the disorder is diagnosed.
Diagnosis of primary sclerosing cholangitis
- Liver function tests
- Ultrasonography, followed by other imaging tests
The disorder may be suspected when results of liver function tests, done as part of an annual physical examination or for some unrelated reason, are abnormal. Then, ultrasonography is typically done first to check for blockage of bile ducts outside the liver.
Tests that can confirm the diagnosis include the following:
- Magnetic resonance cholangiopancreatography (MRCP): Magnetic resonance imaging (MRI) is used to obtain images of the bile ducts and the pancreatic duct. This test helps confirm primary sclerosing cholangitis and rule out other causes of bile duct obstruction.
- Endoscopic retrograde cholangiopancreatography (ERCP): X-rays are taken after a radiopaque contrast agent, which is visible on x-rays, is injected into the bile ducts through an endoscope (see Figure: Understanding Endoscopic Retrograde Cholangiopancreatography). ERCP is less desirable than MRCP because ERCP is more invasive and requires injection of a contrast agent. However, ERCP can also sometimes be used to treat the disorder.
Blood tests and ERCP may be done regularly to check for cancer of the bile ducts.
Treatment of primary sclerosing cholangitis
- Treatment of symptoms and complications
- Sometimes liver transplantation
If people have no symptoms, no treatment is required. But twice a year, they need to have a physical examination and blood tests to monitor the progression of the disorder.
The drug ursodeoxycholic acid may help relieve itching. Recurring bacterial cholangitis is treated with antibiotics. ERCP is done as needed to widen (dilate) the blocked ducts. Sometimes tubes to keep the ducts open (stents) are inserted temporarily.
Liver transplantation is the only treatment that prolongs life. It can cure some types of this otherwise fatal disorder. People with cirrhosis that causes serious complications or those with recurrent bacterial cholangitis may require liver transplantation.
If cancer of the bile ducts develops and surgery to remove the cancer is not possible, stents may be passed through an endoscope and placed in bile ducts that are blocked by the cancer. These stents open the ducts.
Tumors of the Bile Ducts and Gallbladder
Cancer of the bile ducts (cholangiocarcinoma) is rare 30. It can originate anywhere in the bile ducts, particularly in those outside of the liver. Being older or having primary sclerosing cholangitis increases the risk of developing this cancer.
Cancer of the gallbladder is also rare 30. Nearly everyone with gallbladder cancer has gallstones. Many people live only a few months after this cancer develops. This cancer is more common among American Indians, people with large gallstones, and people with a extensive scarring of the gallbladder, which can occur in severe chronic cholecystitis.
Polyps, which are noncancerous (benign) outgrowths of tissue, may develop in the gallbladder. They rarely cause symptoms or require treatment. They are found in about 5% of people during ultrasonography.
Sometimes cancers can block the flow of bile, but most blockages are caused by gallstones. Even less often, cancer can spread (metastasize) from elsewhere in the body to adjacent structures or nearby lymph nodes, causing blockage. Noncancerous tumors in bile ducts also cause blockages.
Symptoms of Tumors of the Bile Ducts and Gallbladder
Symptoms of bile duct cancer typically begin at age 50 to 70. Early symptoms include the following:
- Worsening jaundice (yellowish discoloration of the skin and whites of the eyes)
- Abdominal discomfort
- Loss of appetite
- Weight loss
- Itchiness
Symptoms gradually worsen. Abdominal pain may become increasingly severe and constant. The pain is usually caused by blockage of the bile ducts. The stool may become pale. People feel tired and uncomfortable. They may feel a mass in their abdomen.
Gallbladder cancer causes similar symptoms.
Most gallbladder polyps cause no symptoms.
Diagnosis of Tumors of the Bile Ducts and Gallbladder
- Ultrasonography, followed by other imaging tests
- Sometimes endoscopic retrograde cholangiopancreatography (ERCP) or taking a tissue sample
Doctors suspect bile duct or gallbladder cancer when a bile duct is blocked and no other cause is identified. Bile duct cancer is suspected especially in people with primary sclerosing cholangitis. If people have primary sclerosing cholangitis, blood tests to measure substances secreted by tumors (tumor markers) are done periodically to check for this cancer.
The diagnosis is confirmed by imaging tests. Usually, ultrasonography is done first. Sometimes computed tomography (CT) is done, but results are often not conclusive. CT cholangiography (CT of the bile ducts done after a radiopaque contrast agent is injected into a vein) or magnetic resonance cholangiopancreatography (MRCP) is usually necessary.
If results of imaging tests are unclear, endoscopic retrograde cholangiopancreatography (ERCP) is done. In this procedure, a flexible viewing tube (endoscope) is inserted through the mouth and into the small intestine. A thin tube (catheter) is inserted through the endoscope, and a radiopaque contrast agent, which is visible on x-rays, is injected through the catheter into the bile ducts. Then x-rays are taken to detect any abnormalities. This procedure enables doctors to obtain images and a tissue sample for examination under a microscope (see Figure: Understanding Endoscopic Retrograde Cholangiopancreatography).
If these tests suggest a tumor but are not conclusive, doctors take a tissue sample by inserting a thin needle through the skin into the area thought to be abnormal. Ultrasonography or CT is used to guide the needle.
To determine how extensive the cancer is, doctors may have to make a large incision and directly examine the area (a procedure called open laparotomy).
Treatment of Tumors of the Bile Ducts and Gallbladder
- Insertion of stents into blocked bile ducts
- Sometimes surgery to remove tumor
Most bile duct and gallbladder cancers are fatal, but treatment can help control symptoms.
Tubes (stents) inserted into a duct allow bile to flow past the blockage. This procedure helps control pain and relieves itchiness. Stents can be inserted during ERCP.
Surgery to remove a cancerous tumor may be done, but usually the tumor cannot be completely removed. Chemotherapy and radiation therapy for cholangiocarcinoma are being studied. If tumors have spread from other parts of the body (metastasized), chemotherapy may provide some symptom relief but does not dramatically improve survival.
Very early gallbladder cancer that is found during surgery for gallstones can often be cured by removing the gallbladder.
Narrowing of the Bile Ducts Due to AIDS
People with AIDS tend to develop certain unusual infections because their immune system is weakened 31. Such infections are called opportunistic infections because they take advantage of a weakened immune system. These infections can cause the bile ducts to narrow—a disorder called AIDS cholangiopathy. Usually, the ducts eventually become inflamed and scarred.
Before drugs to treat HIV infection (antiretroviral therapy) were widely used, AIDS cholangiopathy developed in about one fourth of people with AIDS.
The disorder causes pain in the upper right and upper middle parts of the abdomen. If the infection affects the small intestine, people also have diarrhea. A few people have fever and jaundice (a yellowish discoloration of the skin and whites of the eyes).
Diagnosis of narrowing of the bile ducts due to AIDS
Endoscopic retrograde cholangiopancreatography (ERCP) or ultrasonography
Endoscopic retrograde cholangiopancreatography (ERCP) may be done to confirm the diagnosis because it enables doctors to take a sample of infected tissue for examination under a microscope. Then doctors can identify the organism causing the infection. During ERCP, doctors can also widen (dilate) the narrowed bile ducts and thus relieve symptoms. For ERCP, a flexible viewing tube (endoscope) with surgical attachments is passed through the mouth, down the esophagus, through the stomach, and into the small intestine (see Figure: Understanding Endoscopic Retrograde Cholangiopancreatography). A thin catheter is passed through the endoscope, through the ring-shaped muscle between the common bile and pancreatic ducts and small intestine (sphincter of Oddi), and up into the common bile duct. A radiopaque contrast agent, which is visible on x-rays, is then injected through the catheter into the bile ducts, and x-rays are taken to detect any abnormalities.
Alternatively, ultrasonography may be done to help confirm the diagnosis. It is less invasive and is very accurate.
Blood tests to determine how well the liver is functioning and whether it is damaged (liver function tests) are usually also done. The results can support the diagnosis.
Treatment of narrowing of the bile ducts due to AIDS
- Surgery
- Antimicrobial drugs
During ERCP, a surgical instrument is passed through the endoscope and used to cut the sphincter of Oddi—a procedure called endoscopic sphincterotomy. Cutting the sphincter of Oddi allows bile to pass into the small intestine. This procedure helps relieve pain, jaundice, and inflammation. If only one part of a duct is narrowed, a tube may be passed through the endoscope and placed in the affected spot to widen it.
Antimicrobial drugs are given to treat the infection.
Chronic cholecystitis
Chronic cholecystitis is gallbladder inflammation that has lasted a long time. It almost always results from gallstones and from prior attacks of acute cholecystitis. Chronic cholecystitis is characterized by repeated attacks of pain (biliary colic) that occur when gallstones periodically block the cystic duct.
In chronic cholecystitis, the gallbladder is damaged by repeated attacks of acute inflammation, usually due to gallstones, and may become thick-walled, scarred, and small. The gallstones may block the opening of the gallbladder into the cystic duct or block the cystic duct itself. The gallbladder usually also contains sludge. If scarring is extensive, calcium may be deposited in the walls of the gallbladder, causing them to harden (called porcelain gallbladder).
Causes of chronic cholecystitis
Most of the time, chronic cholecystitis is caused by repeated attacks of acute (sudden) cholecystitis. Most of these attacks are caused by gallstones in the gallbladder.
These attacks cause the walls of the gallbladder to thicken. The gallbladder begins to shrink. Over time, the gallbladder is less able to concentrate, store, and release bile.
The disease occurs more often in women than in men. It is more common after age 40.
Symptoms of chronic cholecystitis
Acute cholecystitis is a painful condition that leads to chronic cholecystitis. It is not clear whether chronic cholecystitis causes any symptoms.
Symptoms of acute cholecystis can include:
- Sharp, cramping, or dull pain in upper right or upper middle of your belly
- Steady pain lasting about 30 minutes
- Pain that spreads to your back or below your right shoulder blade
- Clay-colored stools
- Fever
- Nausea and vomiting
- Yellowing of skin and whites of the eyes (jaundice)
Diagnosis of chronic cholecystitis
Your health care provider may order the following blood tests:
- Amylase and lipase. To diagnose diseases of the pancreas.
- Complete blood count (CBC)
- Liver function tests. To evaluate how well the liver is working.
Tests that reveal gallstones or inflammation in the gallbladder include:
- Abdominal CT scan
- Abdominal ultrasound
- Gallbladder scan (HIDA scan)
- Oral cholecystogram
Treatment of chronic cholecystitis
Surgery is the most common treatment. Surgery to remove the gallbladder is called cholecystectomy.
Laparoscopic cholecystectomy is most often done. This surgery uses smaller surgical cuts, which result in a faster recovery. Many people are able to go home from the hospital on the same day as surgery, or the next morning.
Open cholecystectomy requires a larger cut in the upper-right part of the abdomen.
If you are too ill to have surgery because of other diseases or conditions, the gallstones may be dissolved with medicine you take by mouth. However, this may take 2 years or longer to work. The stones may return after treatment.
Outlook (Prognosis) of chronic cholecystitis
Cholecystectomy is a common procedure with a low risk.
- Overview of Gallbladder and Bile Duct Disorders. Merck Manual. http://www.merckmanuals.com/home/liver-and-gallbladder-disorders/gallbladder-and-bile-duct-disorders/overview-of-gallbladder-and-bile-duct-disorders[↩]
- Acute cholecystitis. Medline Plus. https://medlineplus.gov/ency/article/000264.htm[↩]
- Cholecystitis. Merck Manual. http://www.merckmanuals.com/home/liver-and-gallbladder-disorders/gallbladder-and-bile-duct-disorders/cholecystitis[↩][↩][↩]
- Surgical and Nonsurgical Management of Gallstones. Am Fam Physician. 2014 May 15;89(10):795-802. http://www.aafp.org/afp/2014/0515/p795.html[↩]
- Gallstones. American College of Gastroenterology. http://s3.gi.org/patients/cgp/pdf/gallstones.pdf[↩]
- Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut and Liver. 2012;6(2):172–187.[↩][↩]
- Heuman DM. Cholelithiasis. http://emedicine.medscape.com/article/175667-overview#showall[↩]
- Gallstones. National Institute of Diabetes and Digestive and Kidney Diseases. https://www.niddk.nih.gov/health-information/digestive-diseases/gallstones[↩]
- Sherwinter DA. Laparoscopic cholecystectomy. http://emedicine.medscape.com/article/1582292-overview[↩][↩]
- Hope WW. Open cholecystectomy. http://emedicine.medscape.com/article/1582261-overview[↩]
- Sahajpal AK, Chow SC, Dixon E, Greig PD, Gallinger S, Wei AC. Bile duct injuries associated with laparoscopic cholecystectomy: timing of repair and long-term outcomes. Archives of Surgery. 2010;145(8):757–763.[↩]
- Portincasa P, Ciaula AD, Bonfrate L, Wang DQ. Therapy of gallstone disease: what it was, what it is, what it will be. World Journal of Gastrointestinal Pharmacology and Therapeutics. 2012;3(2):7–20.[↩]
- Biliary Pain Without Gallstones. Merck Manual. http://www.merckmanuals.com/home/liver-and-gallbladder-disorders/gallbladder-and-bile-duct-disorders/biliary-pain-without-gallstones[↩][↩][↩]
- Gallbladder polyps: Can they be cancerous ? Mayo Clinic. http://www.mayoclinic.org/gallbladder-polyps/expert-answers/faq-20058450[↩][↩][↩][↩][↩]
- Andrén-Sandberg Å. Diagnosis and Management of Gallbladder Polyps. North American Journal of Medical Sciences. 2012;4(5):203-211. doi:10.4103/1947-2714.95897. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3359430/[↩][↩][↩]
- [Gallbladder polyps: how should they be treated and when?]. Matos AS, Baptista HN, Pinheiro C, Martinho F. Rev Assoc Med Bras (1992). 2010 May-Jun; 56(3):318-21. https://www.ncbi.nlm.nih.gov/pubmed/20676540/[↩]
- Clinicopathologic features of polypoid lesions of the gallbladder and risk factors of gallbladder cancer. Kwon W, Jang JY, Lee SE, Hwang DW, Kim SW. J Korean Med Sci. 2009 Jun; 24(3):481-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2698196/[↩]
- Long-term follow up of gallbladder polyps. Park JY, Hong SP, Kim YJ, Kim HJ, Kim HM, Cho JH, Park SW, Song SY, Chung JB, Bang S. J Gastroenterol Hepatol. 2009 Feb; 24(2):219-22. https://www.ncbi.nlm.nih.gov/pubmed/19054258/[↩]
- [Prevalence and risk factors of gallbladder polyp in adults living in Daegu and Gyeongbuk provinces]. Kim SY, Lee HS, Lee YS, Chung KW, Jang BK, Chung WJ, Park KS, Cho KB, Hwang JS. Korean J Gastroenterol. 2006 Nov; 48(5):344-50. https://www.ncbi.nlm.nih.gov/pubmed/17132923/[↩]
- Pre-operative predictive factors for gallbladder cholesterol polyps using conventional diagnostic imaging. Choi JH, Yun JW, Kim YS, Lee EA, Hwang ST, Cho YK, Kim HJ, Park JH, Park DI, Sohn CI, Jeon WK, Kim BI, Kim HO, Shin JH. World J Gastroenterol. 2008 Nov 28; 14(44):6831-4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2773878/[↩]
- Cantürk Z, Sentürk O, Cantürk NZ, Anik YA. Prevalence and risk factors for gall bladder polyps. East Afr Med J. 2007;84:336–41. https://www.ncbi.nlm.nih.gov/pubmed/17886428[↩]
- Gallahan WC, Conway JD. Diagnosis and management of gallbladder polyps. Gastroenterol Clin North Am. 2010;39:359–67. https://www.ncbi.nlm.nih.gov/pubmed/20478491[↩][↩][↩][↩]
- Zielinski MD, Atwell TD, Davis PW, Kendrick ML, Que FG. Comparison of surgically resected polypoid lesions of the gallbladder to their pre-operative ultrasound characteristics. J Gastrointest Surg. 2009;13:19–25. https://www.ncbi.nlm.nih.gov/pubmed/18972168[↩]
- Matos AS, Baptista HN, Pinheiro C, Martinho F. Gallbladder polyps: How should they be treated and when? Rev Assoc Med Bras. 2010;56:318–21. https://www.ncbi.nlm.nih.gov/pubmed/20676540[↩]
- Yang LP, Yang ZL, Tan XG, Miao XY. Expression of annexin A1 (ANXA1) and A2 (ANXA2) and its significance in benign and malignant lesions of gallbladder. Zhonghua Zhong Liu Za Zhi. 2010;32:595–9. https://www.ncbi.nlm.nih.gov/pubmed/21122411[↩][↩]
- Primary Sclerosing Cholangitis. Merck Manual. http://www.merckmanuals.com/home/liver-and-gallbladder-disorders/gallbladder-and-bile-duct-disorders/primary-sclerosing-cholangitis[↩]
- Kimura K, Fujita N, Noda Y, Kobayashi G, Ito K. Differential diagnosis of large-sized pedunculated polypoid lesions of the gallbladder by endoscopic ultrasonography: A prospective study. J Gastroenterol. 2001;36:619–22. https://www.ncbi.nlm.nih.gov/pubmed/11578066[↩]
- Leung UC, Wong PY, Roberts RH, Koea JB. Gall bladder polyps in sclerosing cholangitis: Does the 1-cm rule apply? ANZ J Surg. 2007;77:355–7. https://www.ncbi.nlm.nih.gov/pubmed/17497975[↩]
- Buckles DC, Lindor KD, Larusso NF, Petrovic LM, Gores GJ. In primary sclerosing cholangitis, gallbladder polyps are frequently malignant. Am J Gastroenterol. 2002;97:1138–42. https://www.ncbi.nlm.nih.gov/pubmed/12014717[↩]
- Tumors of the Bile Ducts and Gallbladder. Merck Manual. http://www.merckmanuals.com/home/liver-and-gallbladder-disorders/gallbladder-and-bile-duct-disorders/tumors-of-the-bile-ducts-and-gallbladder[↩][↩]
- Narrowing of the Bile Ducts Due to AIDS. Merck Manual. http://www.merckmanuals.com/home/liver-and-gallbladder-disorders/gallbladder-and-bile-duct-disorders/narrowing-of-the-bile-ducts-due-to-aids[↩]





{kind=link}