Contents
What is gastroparesis
Gastroparesis long-term (chronic) condition where the stomach can’t empty itself in the normal way. Gastroparesis is also known as delayed gastric emptying, where food passes through your stomach into your small intestine more slowly than usual. Gastroparesis is caused by muscle or nerve damage and results in symptoms such as bloating and belching.
Normally, the muscles of the stomach, which are controlled by the vagus nerve, contract to break up food and move it through the gastrointestinal (GI) tract. The gastrointestinal tract is a series of hollow organs joined in a long, twisting tube from the mouth to the anus. The movement of muscles in the gastrointestinal tract, along with the release of hormones and enzymes, allows for the digestion of food. Gastroparesis is thought to be the result of a problem or damage to the vagus nerve caused by illness or injury and the stomach muscles stop working normally. Food then moves slowly from the stomach to the small intestine or stops moving altogether.
In many cases of gastroparesis, there’s no obvious cause. This is known as idiopathic gastroparesis. Women are more likely to develop gastroparesis than are men.
Certain medications, such as opioid pain relievers, some antidepressants, and high blood pressure and allergy medications, can lead to slow gastric emptying and cause similar symptoms. For people who already have gastroparesis, these medications may make their condition worse.
Gastroparesis can interfere with normal digestion, cause nausea and vomiting, and cause problems with blood sugar levels and nutrition. The cause of gastroparesis is usually unknown. Sometimes it’s a complication of diabetes, and some people develop gastroparesis after surgery. Although there’s no cure for gastroparesis, changes to your diet, along with medication, can offer some relief.
Figure 1. Stomach
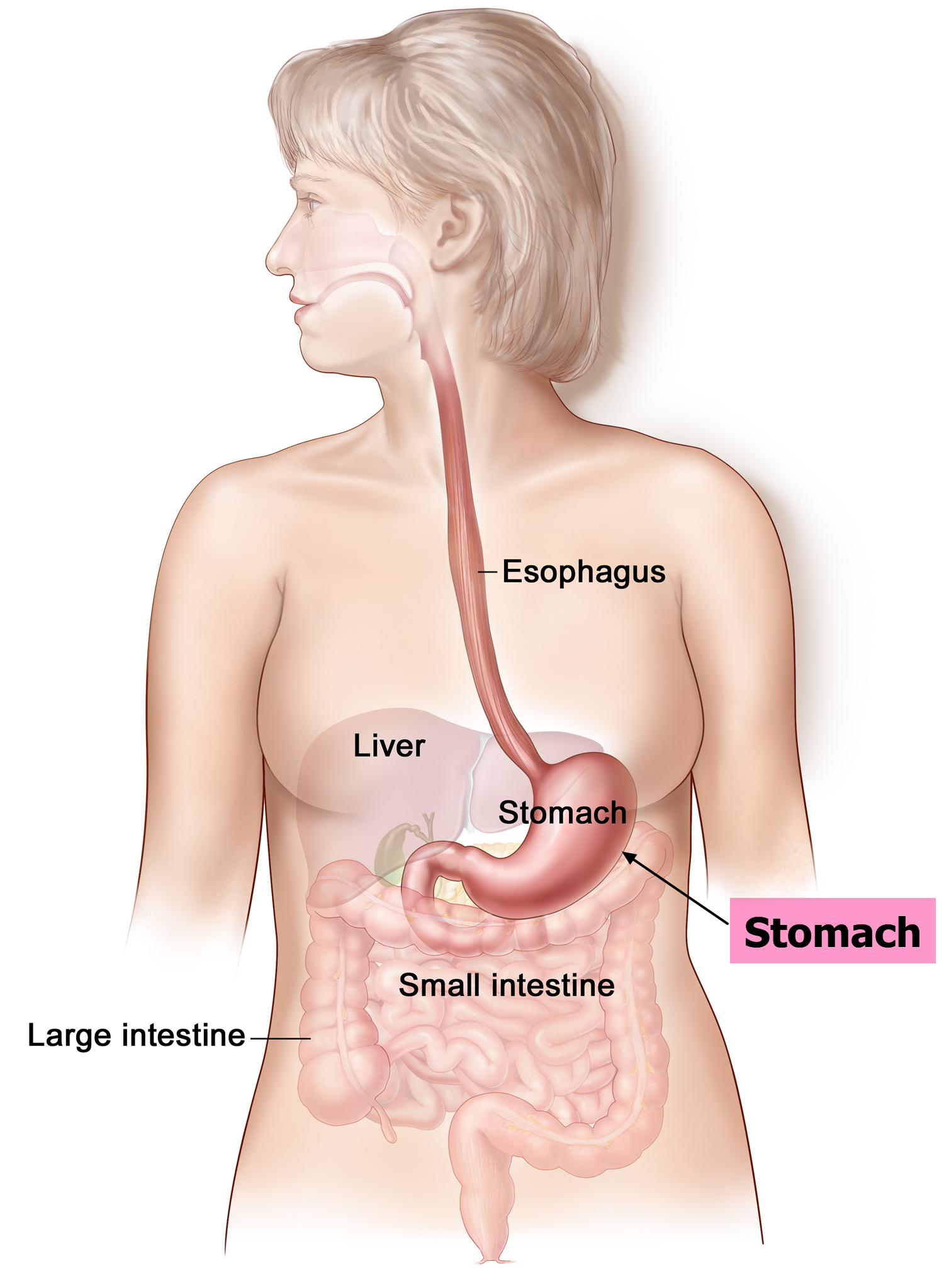 Figure 2. Gastroparesis
Figure 2. Gastroparesis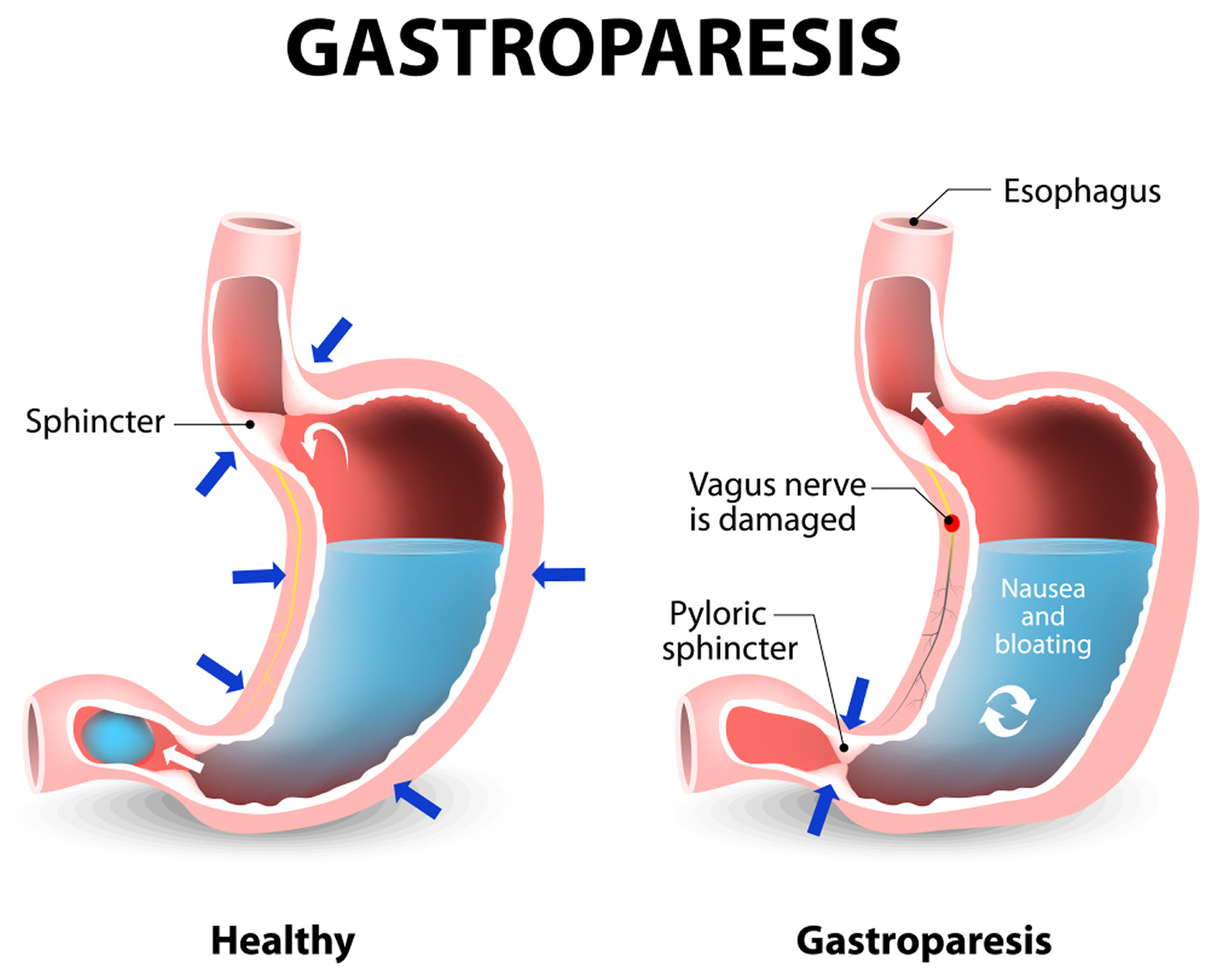
Gastroparesis causes
What causes gastroparesis
Most people diagnosed with gastroparesis have idiopathic gastroparesis, which means a health care provider cannot identify the cause, even with medical tests. Gastroparesis may also be caused by a disruption of nerve signals to the stomach. Gastroparesis is also a common complication of diabetes. People with diabetes have high levels of blood glucose, also called blood sugar. Over time, high blood glucose levels can damage the vagus nerve.
The vagus nerve helps manage the complex processes in your digestive tract, including signaling the muscles in your stomach to contract and push food into the small intestine. A damaged vagus nerve can’t send signals normally to your stomach muscles. This may cause food to remain in your stomach longer, rather than move normally into your small intestine to be digested.
The vagus nerve can be damaged by diseases, such as diabetes, or by surgery to the stomach or small intestine.
Other identifiable causes of gastroparesis include intestinal surgery and nervous system diseases such as Parkinson’s disease or multiple sclerosis. For reasons that are still unclear, gastroparesis is more commonly found in women than in men.
Known causes of gastroparesis include:
- Poorly controlled type 1 diabetes or type 2 diabetes
- A complication of some types of surgery – such as weight loss (bariatric) surgery or removal of part of the stomach (gastrectomy)
Other possible causes include:
- Medication – such as opioid painkillers like morphine and some antidepressants
- Parkinson’s disease – a condition in which part of the brain becomes progressively damaged over many years
- Scleroderma – an uncommon disease that results in hard, thickened areas of skin, and sometimes problems with internal organs and blood vessels
- Amyloidosis – a group of rare but serious diseases caused by deposits of abnormal protein in tissues and organs throughout the body
Risk factors for gastroparesis
Risk factors for gastroparesis include:
- Diabetes
- Gastrectomy (surgery to remove part of the stomach)
- Scleroderma (a connective tissue disease)
- Use of medicine that blocks certain nerve signals (anticholinergic medicine)
- Abdominal or esophageal surgery
- Infection, usually a virus
- Certain medications that slow the rate of stomach emptying, such as narcotic pain medications
- Nervous system diseases, such as Parkinson’s disease or multiple sclerosis
- Hypothyroidism (low thyroid)
Gastroparesis complications
Ongoing nausea and vomiting may cause:
- Dehydration
- Electrolyte imbalances
- Malnutrition due to poor absorption of nutrients or a low calorie intake
- Gastro-esophageal reflux disease (GERD) – where stomach acid leaks out of your stomach and into your gullet. GERD can lead to esophagitis— irritation of the esophagus.
- Unpredictable blood sugar levels – this is a particular risk in people with diabetes. These variations in blood sugar make diabetes worse. In turn, poor control of blood sugar levels makes gastroparesis worse.
- Undigested food that hardens and remains in your stomach. Undigested food in your stomach can harden into a solid mass called a bezoar. Bezoars can cause nausea, obstruction, and vomiting and may be life-threatening if they prevent food from passing into your small intestine. Bezoars, can also interfere with absorption of some medications in pill form.
- Decreased quality of life, including work absences due to severe symptoms. An acute flare-up of symptoms can make it difficult to work and keep up with other responsibilities.
People with diabetes may have serious complications from poor blood sugar control.
Gastroparesis symptoms
The most common symptoms of gastroparesis are nausea, a feeling of fullness after eating only a small amount of food, and vomiting undigested food—sometimes several hours after a meal.
Symptoms of gastroparesis may include:
- Abdominal distention or bloating
- Hypoglycemia (in people with diabetes)
- Nausea
- Premature abdominal fullness after meals
- Weight loss without trying
- Vomiting
- Abdominal pain
- Loss of appetite
- Weight loss
- Tummy (abdominal) pain or discomfort
- Heartburn
These symptoms can be mild or severe, and tend to come and go.
Symptoms may be aggravated by eating greasy or rich foods, large quantities of foods with fiber—such as raw fruits and vegetables—or drinking beverages high in fat or carbonation. Symptoms may be mild or severe, and they can occur frequently in some people and less often in others. The symptoms of gastroparesis may also vary in intensity over time in the same individual. Sometimes gastroparesis is difficult to diagnose because people experience a range of symptoms similar to those of other diseases.
Gastroparesis diagnosis
Gastroparesis is diagnosed through a physical exam, medical history, blood tests, tests to rule out blockage or structural problems in the GI tract, and gastric emptying tests. Tests may also identify a nutritional disorder or underlying disease. To rule out any blockage or other structural problems, the health care provider may perform one or more of the following tests:
- Esophagogastroduodenoscopy (EGD) – a thin, flexible tube (endoscope) is passed down your throat and into your stomach to examine the esophagus, stomach, and duodenum —the first part of the small intestine lining and rule out other possible causes. The test is performed at a hospital or outpatient center by a gastroenterologist—a doctor who specializes in digestive diseases. The endoscope is carefully fed down the esophagus and into the stomach and duodenum. A small camera mounted on the endoscope transmits a video image to a monitor, allowing close examination of the intestinal lining. A person may receive a liquid anesthetic that is gargled or sprayed on the back of the throat. An intravenous (IV) needle is placed in a vein in the arm if general anesthesia is given. The test may show blockage or large bezoars—solid collections of food, mucus, vegetable fiber, hair, or other material that cannot be digested in the stomach—that are sometimes softened, dissolved, or broken up during an upper GI endoscopy.
- Upper GI series. An upper GI series may be done to look at the small intestine. The test is performed at a hospital or outpatient center by an x-ray technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging. Anesthesia is not needed. No eating or drinking is allowed for 8 hours before the procedure, if possible. If the person has diabetes, a health care provider may give different instructions about fasting before the test. During the procedure, the person will stand or sit in front of an x-ray machine and drink barium, a chalky liquid. Barium coats the small intestine, making signs of gastroparesis show up more clearly on x rays. Gastroparesis is likely if the x ray shows food in the stomach after fasting. A person may experience bloating and nausea for a short time after the test. For several days afterward, barium liquid in the GI tract causes stools to be white or light colored. A health care provider will give the person specific instructions about eating and drinking after the test.
Ultrasound. Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. The procedure is performed in a health care provider’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist; anesthesia is not needed. The images can show whether gallbladder disease and pancreatitis could be the cause of a person’s digestive symptoms, rather than gastroparesis. - Gastric emptying scintigraphy. The test involves eating a bland meal—such as eggs or an egg substitute—that contains a small amount of radioactive material. The test is performed in a radiology center or hospital by a specially trained technician and interpreted by a radiologist; anesthesia is not needed. An external camera scans the abdomen to show where the radioactive material is located. The radiologist is then able to measure the rate of gastric emptying at 1, 2, 3, and 4 hours after the meal. If more than 10 percent of the meal is still in the stomach at 4 hours, the diagnosis of gastroparesis is confirmed.
- Wireless capsule test or Smartpill– you swallow a small, electronic device that sends information about how fast it moves through your digestive tract to a recording device. The SmartPill test is available at specialized outpatient centers. The images are interpreted by a radiologist. The device is swallowed and moves through the entire digestive tract, sending information to a cell-phone-sized receiver worn around the person’s waist or neck. The recorded information provides a detailed record of how quickly food travels through each part of the digestive tract.
- Gastric emptying breath test. With this test, the person eats a special test meal that includes a natural material with a special type of carbon in it. Then, breath samples are taken over a period of several hours to measure the amount of the material in the exhaled breath. The results allow the health care provider to calculate how fast the stomach is emptying.
Gastroparesis treatment
Gastroparesis can’t usually be cured, but dietary changes and medical treatment can help you control the condition.
People with diabetes should always control their blood sugar levels. Better control of blood sugar level may improve symptoms of gastroparesis. Eating small and more frequent meals and soft foods may also help relieve some symptoms.
Gastroparesis diet
Here’s a brief list of foods recommended for people with gastroparesis (your dietitian can give you a more comprehensive list):
Starches
- White bread and rolls and “light” whole-wheat bread without nuts or seeds
- Plain or egg bagels
- English muffins
- Flour or corn tortillas
- Pancakes
- Puffed wheat and rice cereals
- Cream of wheat or rice
- White crackers
- Potatoes, white or sweet (no skin)
- Baked french fries
- Rice
- Pasta
Protein
- Lean beef, veal and pork (not fried)
- Chicken or turkey (no skin and not fried)
- Crab, lobster, shrimp, clams, scallops, oysters
- Tuna (packed in water)
- Cottage cheese
- Eggs
- Tofu
- Strained meat baby food
Fruits and vegetables
- Baby food vegetables and fruits
- Tomato sauce, paste, puree, juice
- Carrots (cooked)
- Beets (cooked)
- Mushrooms (cooked)
- Vegetable juice
- Vegetable broth
- Fruit juices and drinks
- Applesauce
- Bananas
- Peaches and pears (canned)
Dairy
- Milk, if tolerated
- Yogurt (without fruit pieces)
- Custard and pudding
- Frozen yogurt
You may find these tips helpful:
- instead of three meals a day, try smaller, more frequent meals – this means there’s less food in your stomach and it will be easier to pass through your system
- try soft and liquid foods – these are easier to digest
- eat well-cooked fruits and vegetables rather than raw fruits and vegetables
- chew food well before swallowing
- drink non-fizzy liquids with each meal
- try soups and pureed foods if liquids are easier for you to swallow
- drink about 34 to 51 ounces (1 to 1.5 liters) of water a day
- exercise gently after you eat, such as going for a walk
- avoid carbonated drinks, alcohol and smoking
- try to avoid lying down for 2 hours after a meal
- take a multivitamin daily
It may also help to avoid certain foods that are hard to digest – such as apples with their skin on, or high-fiber foods like oranges and broccoli – as well as foods high in fat, which can also slow down digestion. People with gastroparesis should minimize their intake of large portions of these foods because the undigested parts may remain in the stomach too long. Sometimes, the undigested parts form bezoars.
When a person has severe symptoms, a liquid or puréed diet may be prescribed. As liquids tend to empty more quickly from the stomach, some people may find a puréed diet helps improve symptoms. Puréed fresh or cooked fruits and vegetables can be incorporated into shakes and soups. A health care provider may recommend a dietitian to help a person plan meals that minimize symptoms and ensure all nutritional needs are met.
When the most extreme cases of gastroparesis lead to severe nausea, vomiting, and dehydration, urgent care may be required at a medical facility where IV fluids can be given.
Advice for people with diabetes
Having gastroparesis means your food is being absorbed slowly and at unpredictable times. If you also have diabetes, this can lead to wide swings in blood sugar levels.
The nerves to the stomach can be damaged by high levels of blood glucose, so it’s important to keep your blood glucose levels under control if you have diabetes.
An elevated blood glucose level directly interferes with normal stomach emptying, so good blood glucose control in people with diabetes is important. However, gastroparesis can make blood glucose control difficult. When food that has been delayed in the stomach finally enters the small intestine and is absorbed, blood glucose levels rise. Gastric emptying is unpredictable with gastroparesis, causing a person’s blood glucose levels to be erratic and difficult to control.
The primary treatment goals for gastroparesis related to diabetes are to improve gastric emptying and regain control of blood glucose levels. In addition to the dietary changes and treatments already described, a health care provider will likely adjust the person’s insulin regimen.
To better control blood glucose, people with diabetes and gastroparesis may need to:
- take insulin more often or change the type of insulin they take
- take insulin after meals, instead of before
- check blood glucose levels frequently after eating and administer insulin when necessary
A health care provider will give specific instructions for taking insulin based on the individual’s needs and the severity of gastroparesis.
In some cases, the dietitian may suggest eating several liquid or puréed meals a day until gastroparesis symptoms improve and blood glucose levels are more stable.
Gastroparesis medications
Several prescription medications are available to treat gastroparesis. A combination of medications may be used to find the most effective treatment.
Medicines that may help include:
- Cholinergic drugs, which act on acetylcholine nerve receptors
- Metoclopramide (Reglan). This medication stimulates stomach muscle contractions to help with gastric emptying. Metoclopramide also helps reduce nausea and vomiting. The medication is taken 20 to 30 minutes before meals and at bedtime. Possible side effects of metoclopramide include fatigue, sleepiness, and depression. Currently, this is the only medication approved by the FDA for treatment of gastroparesis. However, the FDA has placed a black box warning on this medication because of rare reports of it causing an irreversible neurologic side effect called tardive dyskinesia—a disorder that affects movement.
- Erythromycin. This antibiotic, prescribed at low doses, may improve gastric emptying. Like metaclopramide, erythromycin works by increasing the contractions that move food through the stomach. Possible side effects of erythromycin include nausea, vomiting, and abdominal cramps.
- Serotonin antagonist drugs, which act on serotonin receptors
However, the evidence that these medications relieve the symptoms of gastroparesis is relatively limited and they can cause a number of side effects. Your doctor should discuss the potential risks and benefits with you.
Gastric Electrical Stimulation
If dietary changes and medication don’t improve your symptoms, a relatively new treatment called gastroelectrical stimulation may be tried.
Gastroelectrical stimulation involves surgically implanting a battery-operated device under the skin of your abdomen.
The procedure may be performed at a hospital or outpatient center by a gastroenterologist. General anesthesia may be required.
Two leads attached to this device are fixed to the muscles of your lower stomach. They deliver electrical impulses to help stimulate the muscles involved in controlling the passage of food through your stomach. The device is turned on using a handheld external control.
The effectiveness of this treatment can vary considerably. Not everyone will respond to it, and for many of those who do the effect will largely wear off within 12 months. This means electrical stimulation isn’t suitable for everyone with the condition.
There’s also a small chance of this procedure leading to complications that would require removing the device, such as:
- infection
- the device dislodging and moving
- a hole forming in your stomach wall
Other treatments may include:
- Botulinum toxin (Botox) injected into the outlet of the stomach (pylorus)
- Surgical procedure that creates an opening between the stomach and small intestine to allow food to move through the digestive tract more easily (gastroenterostomy).
Botulinum toxin
More severe cases of gastroparesis may occasionally be treated by injecting botulinum toxin into the valve between your stomach and small intestine.
This relaxes the valve and keeps it open for a longer period of time so food can pass through.
The injection is given through an endoscope, which is passed down your throat and into your stomach.
This is a fairly new treatment and some studies have found it may not be very effective, so it’s not recommended by all doctors.
Botox is supposed to help keep the pylorus open for longer periods of time and improve symptoms of gastroparesis. Although some initial research trials showed modest improvement in gastroparesis symptoms and the rate of gastric emptying following the injections, other studies have failed to show the same degree of effectiveness of the Botox injections 1.
A feeding tube
If you have extremely severe gastroparesis that isn’t improved with dietary changes and medication, you may benefit from a feeding tube.
Many different types of temporary and permanent feeding tube are available.
A temporary feeding tube called a nasojejunal tube may be offered to you first, which is inserted through your nose to pass nutrients directly into your small intestine.
A feeding tube can also be inserted into your bowel surgically through a cut (incision) made in your abdomen. This is known as a jejunostomy.
Liquid food containing nutrients can be fed through the tube, which goes straight to your bowel to be absorbed, bypassing your stomach.
Speak to your doctor about the risks and benefits of each type of feeding tube.
An alternative feeding method for severe gastroparesis is intravenous (parenteral) nutrition, where liquid nutrients are passed straight into your bloodstream through a catheter fed into a large vein. This approach is a less preferable alternative to a jejunostomy and is usually a temporary treatment to get through a difficult period of gastroparesis.
Gastroparesis surgery
Some people may benefit from having an operation to insert a tube into the stomach through the abdomen. This tube can be periodically opened to release gas and relieve bloating.
A surgical procedure may be recommended as a last resort to either:
- create a new opening between your stomach and small intestine (gastroenterostomy)
- connect your stomach directly to the second part of your small intestine, called the jejunum (gastrojejunostomy)
These procedures may reduce your symptoms by allowing food to move through your stomach more easily.
Your doctor can explain whether any procedures are suitable for you, and can discuss the possible risks involved.
Alternative medicine
There is some evidence that certain alternative treatments can be helpful to people with gastroparesis, although more studies are needed. Some treatments that look promising include:
- Acupuncture and electroacupuncture. Acupuncture involves the insertion of extremely thin needles through your skin at strategic points on your body. During electroacupuncture, a small electrical current is passed through the needles. Studies have shown these treatments to ease gastroparesis symptoms more than a sham treatment.
- STW 5 (Iberogast). This herbal formula from Germany contains nine different herbal extracts. It hasn’t been shown to speed up gastric emptying, but was slightly better at easing digestive symptoms than a placebo.
- Rikkunshito. This Japanese herbal formula also contains nine herbs. It may help reduce abdominal pain and the feeling of post-meal fullness.
- Cannabis. There aren’t any published clinical trials on cannabis and gastroparesis. However, cannabis — commonly known as marijuana — is thought to ease nausea and other digestive complaints. Derivatives of cannabis have been used by people who have cancer in the past, but there are better FDA-approved medications available to control nausea now. Because cannabis is often smoked, there’s concern about possible addiction and harm, similar to what occurs with tobacco smoke. In addition, daily users of marijuana (cannabis) may develop a condition that mimics the symptoms of gastroparesis called cannabis hyperemesis syndrome. Symptoms can include nausea, vomiting and abdominal pain. Quitting cannabis may help.
- Bai Y, Xu MJ, Yang X, et al. A systematic review on intrapyloric botulinum toxin injection for gastroparesis. Digestion. 2010;81(1):27–34.[↩]





{kind=link}