Contents
- What is a growth plate fracture
What is a growth plate fracture
The bones of children and adults share many of the same risks for injury. But because they are still growing, a child’s bones are also subject to a unique injury called a growth plate fracture. Growth plates are areas of cartilage located near the ends of bones (see Figures 1 and 2). Because they are the last portion of a child’s bones to harden (ossify), growth plates are particularly vulnerable to fracture. Growth plates are the softest and weakest sections of the skeleton — sometimes even weaker than surrounding ligaments and tendons. An injury that might cause a joint sprain for an adult can cause a growth plate fracture in a child.
Most growth plate fractures occur in the long bones of the fingers. They are also common in the outer bone of the forearm (radius) and lower bones of the leg (the tibia and fibula).
Growth plate injuries are more likely to occur:
- In growing children and teens. When your child or teen injures a joint, they are more likely to fracture the growth plate. A similar injury in an adult is would cause a sprain.
- Growth plate fractures occur twice as often in boys as in girls. A girl’s body matures at an earlier age than boys. As a result, girls’ bones finish growing sooner. When the growth plates finish growing, they are replaced by stronger, solid bone.
- Growth plate injuries often occur in children and teens who participate in competitive sports or activities such as:
- Football.
- Basketball.
- Gymnastics.
- Biking.
- Sledding.
- Skiing.
- Skateboarding.
Fractures can result from a single traumatic event, such as a fall or automobile accident, or from chronic stress and overuse. Most growth plate fractures occur in the long bones of the fingers (phalanges) and the outer bone of the forearm (radius). They are also common in the lower bones of the leg (the tibia and fibula).
Approximately 15% to 30% of all childhood fractures are growth plate fractures. Because the growth plate helps determine the future length and shape of the mature bone. Growth plate fractures often need immediate treatment because they can affect how the bone will grow. An improperly treated growth plate fracture could result in a fractured bone ending up more crooked or shorter than its opposite limb. With proper treatment, most growth plate fractures heal without complications. If not treated properly, it could result in a limb that is crooked or unequal in length when compared to its opposite limb. Fortunately, serious problems are rare. With proper treatment, most growth plate fractures heal without complications.
What is the growth plate
All long bones have an area called the epiphysis, which is the rounded end of the bone. The long, middle part (or shaft) of the bone is the diaphysis; the area where the bone gets wider at its end is the metaphysis.
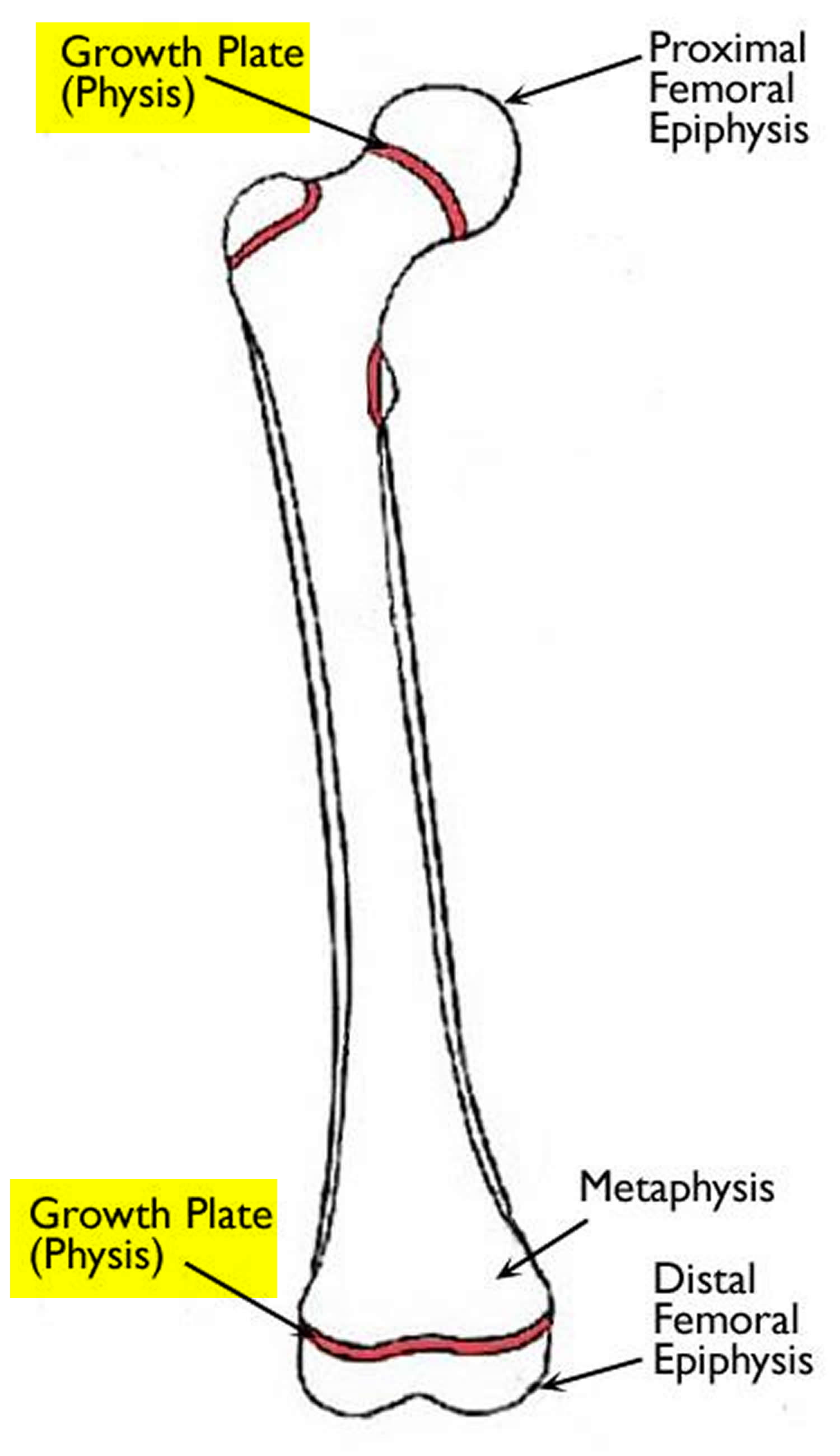
In growing kids, growth plates sit between the metaphysis and the epiphysis. Growth plates are found in the long bones of the body—the bones that are longer than they are wide. Examples of long bones include the femur (thighbone), the radius and ulna in the forearm, as well as the metacarpal bones in the hands. Growth plates are at the end of long bones, and grow in length. They’re made up of cartilage, a rubbery, flexible material (the nose, for instance, is made of cartilage).
Most long bones in the body have at least two growth plates, including one at each end. Growth plates are located between the widened part of the shaft of the bone (the metaphysis) and the end of the bone (the epiphysis). The long bones of the body do not grow from the center outward. Instead, growth occurs at each end of the bone around the growth plate.
When a child’s bones are done growing (called reaching skeletal maturity), the growth plates ossify (harden) and the epiphysis fuses with the metaphysis, forming one complete bone. When a bone ceases to grow in length at about ages 14–24, the cartilage in the growth plate (epiphyseal growth plate) is replaced by bone; the resulting bony structure is known as the epiphyseal line.
Girls tend to reach skeletal maturity earlier than boys. Their growth plates usually close around ages 13 to 15, while boys’ growth plates close later, at around ages 15 to 17. Before growth is complete, the growth plates are at risk for fractures (breaks). An adult whose bones have finished growing might simply pull a muscle or a tendon after a fall. But in a child, that same fall could injure the growth plate.
Figure 1. Growth plate (an epiphyseal plate)
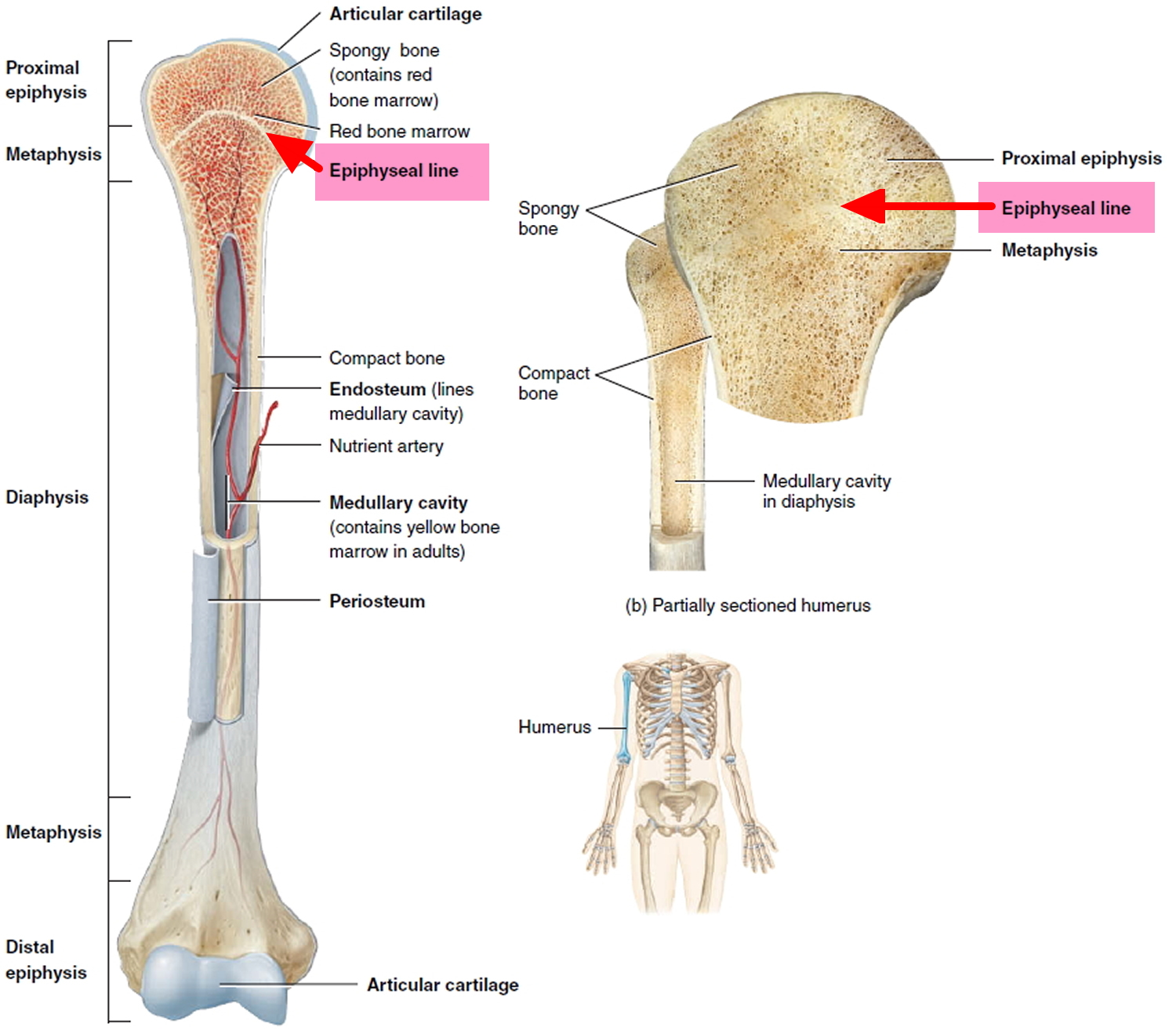
Figure 2. Growth plate (thigh bone or femur)
Growth Plate Fractures Classification
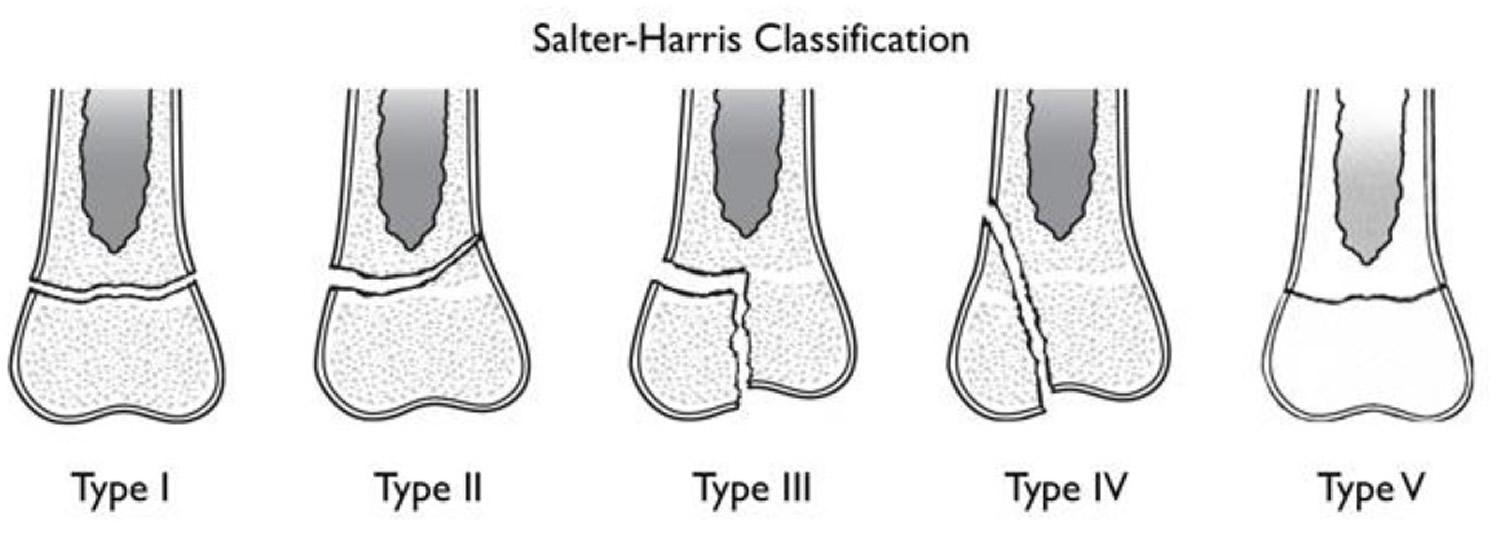
Several classification systems have been developed that categorize the different types of growth plate fractures. Perhaps the most widely used by doctors is the Salter-Harris system. The Salter-Harris classification was proposed by Salter and Harris in 1963 1 and remains the most widely used system for describing growth plate fractures.
Conveniently the Salter-Harris types can be remembered by the mnemonic SALTR and SMACK.
SALTR
- S: slipped (type I)
- A: above (type II)
- L: lower (type III)
- T: through or transverse or together (type IV)
- R: ruined or rammed (type V)
SMACK
- S: slipped (type I)
- M: metaphyseal (type II)
- A: articular-epiphyseal (type III)
- C: complete-metaphysis and epiphysis (type IV)
- K: krushed! (type V)
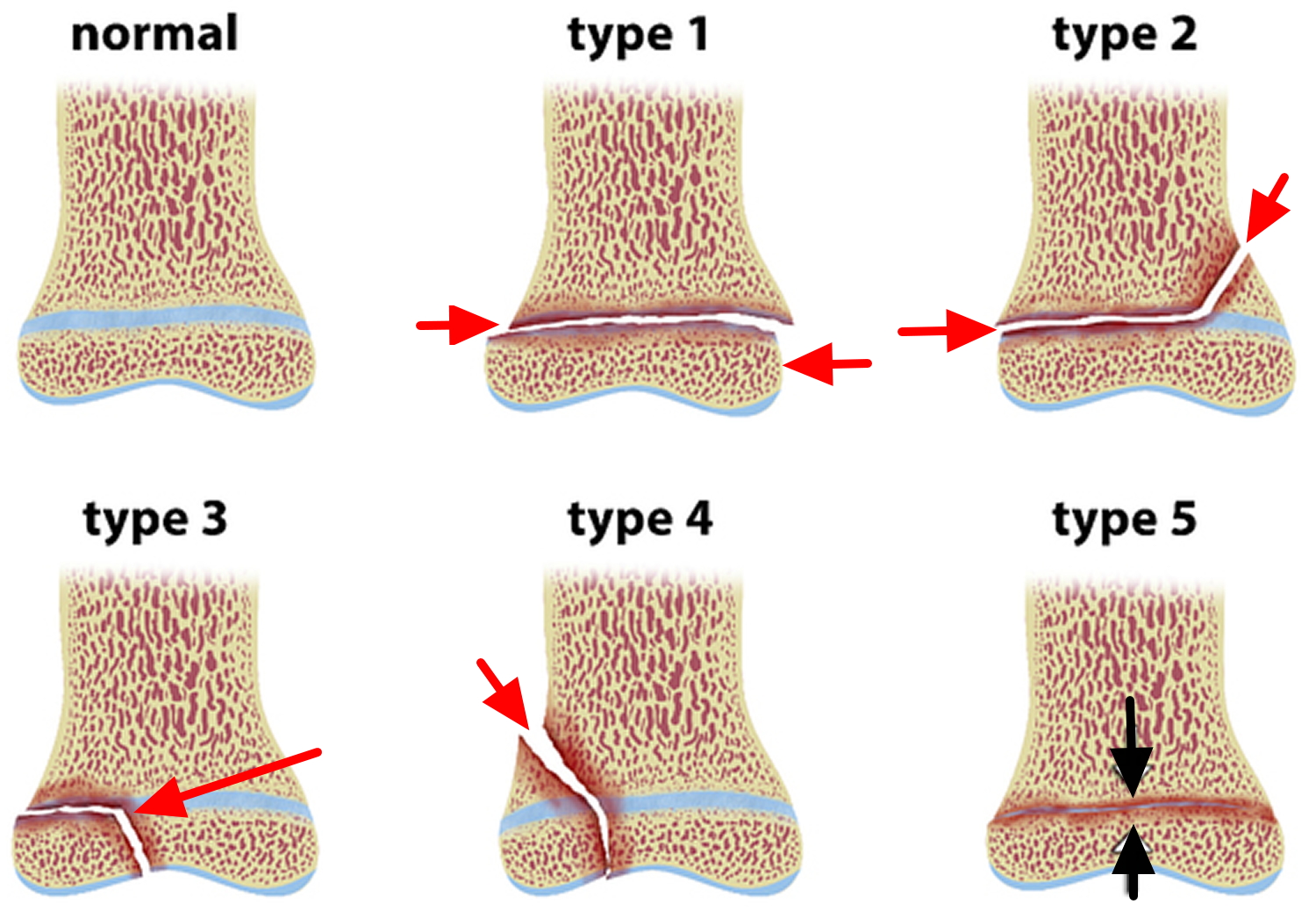
Figure 3. Salter-Harris growth plate fracture classification
Type I Growth Plate Fractures
These fractures break through the bone at the growth plate, separating the bone end from the bone shaft and completely disrupting the growth plate.
- Slipped
- 5-7% of all growth plate fractures
- Fracture through the growth plate and happens when the epiphysis is completely separated from the end of the bone, through the deep layer of the growth plate. The growth plate remains attached to the epiphysis.
- Cannot occur if the growth plate is fused 2
- Good prognosis. The doctor may have to put or set the fracture back into place if it is significantly displaced. Type I injuries generally require a cast to protect the plate as it heals. Unless there is damage to the blood supply to the growth plate, the likelihood that the bone will grow normally is excellent.
Figure 4. Growth plate fracture finger (Salter-Harris type I fracture of the head of humerus – fracture through the growth plate of the fifth distal phalanx with mild dorsal displacement and palmar angulation)

Figure 5. Shoulder growth plate fracture (Salter-Harris type I fracture of the head of humerus – complete slip of the humeral epiphysis)

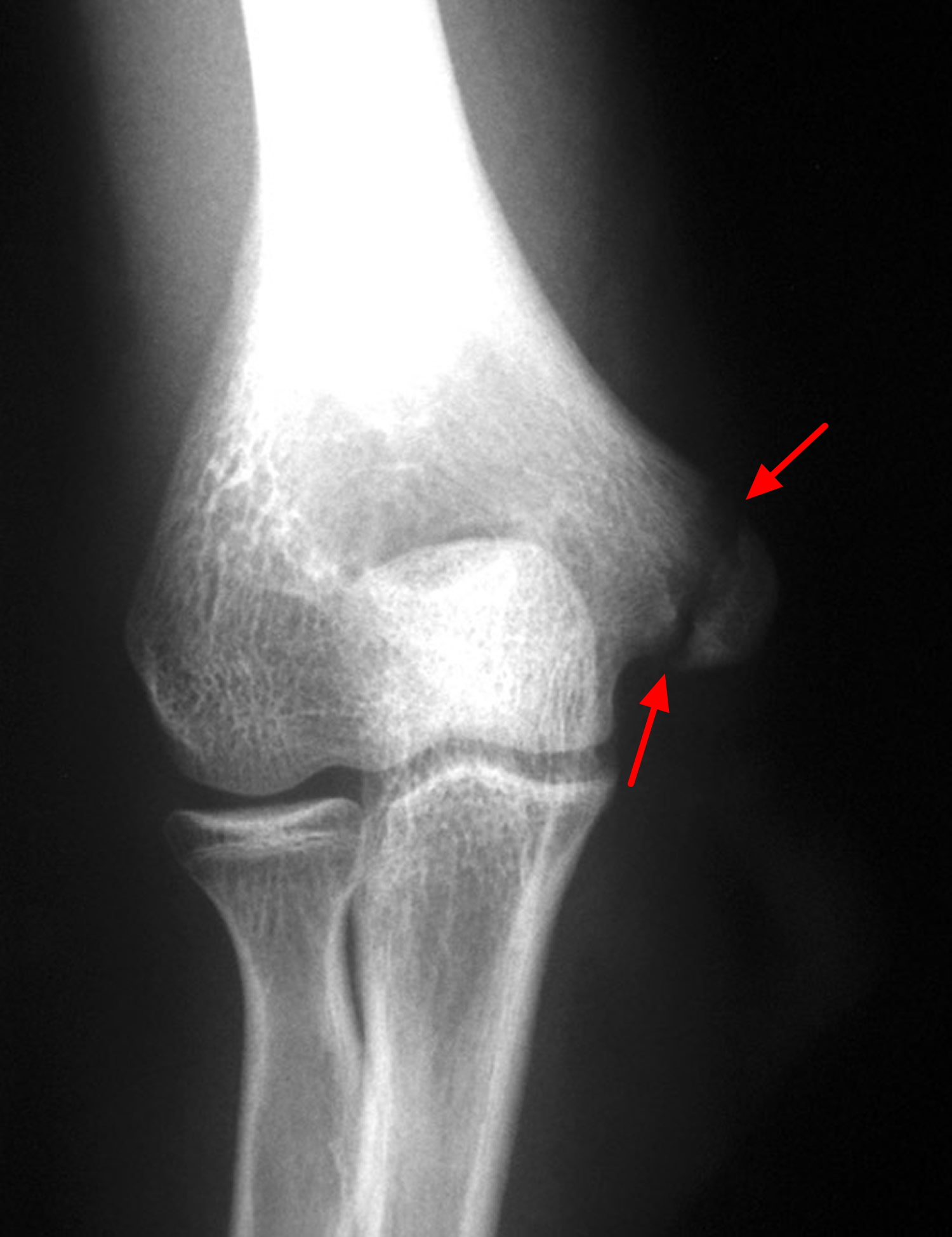
Figure 6. Growth plate fracture elbow (Salter-Harris type I fracture of the medial epicondyle of humerus)
Type II Growth Plate Fractures
These fractures break through part of the bone at the growth plate and crack through the bone shaft, as well. This is the most common type of growth plate fracture.
- Above
- ~75% (by far the most common) of all growth plate fractures
- Fracture passes across most of the growth plate and up through the metaphysis, but not through the epiphysis.
- Good prognosis. Type II fractures may need the doctor to set the bones and immobilize the injury. However, this type of injury can heal quickly younger children and the doctor may not need to set the bone back into position. If this is the case, the injury heals and strengthens with time.
Figure 7. Growth plate fracture wrist (Salter-Harris type II fracture – posteriorly displaced fracture passing across the growth plate and through the metaphysis of distal radius)

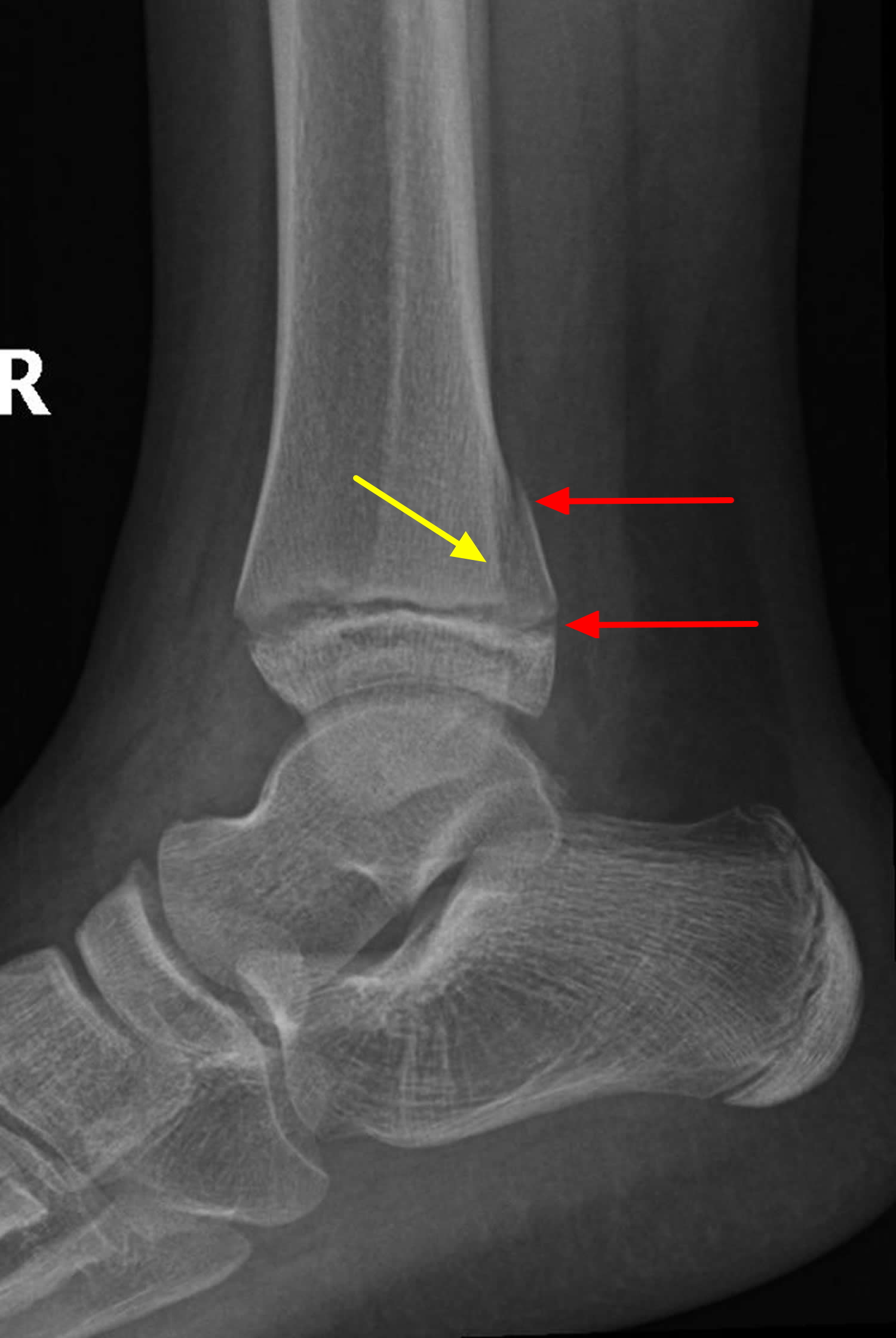
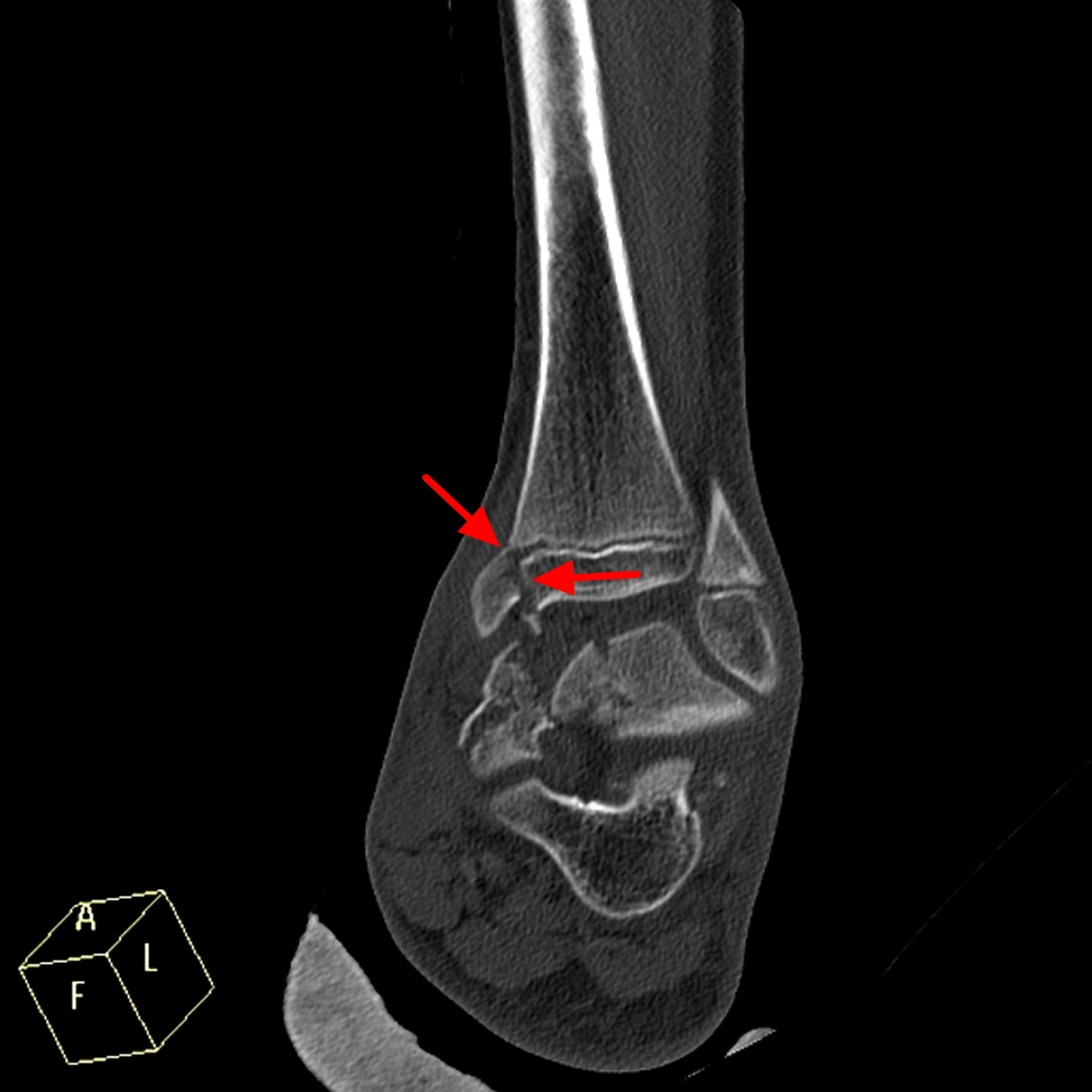
Figure 8. Tibial growth plate fracture (Salter-Harris type II fracture)
Type III Growth Plate Fractures
These fractures cross through a portion of the growth plate and break off a piece of the bone end. This type of fracture is more common in older children.
- Lower
- 7-10% of all growth plate fractures. When this type of fracture occurs, it is usually at the lower end the long bones of the lower leg.
- Fractures run through growth plate leading to a separation of epiphysis and growth plate from the metaphysis.
- Poorer prognosis as the proliferative and reserve zones are interrupted. Surgery is sometimes necessary to restore the joint surface to normal. The outlook or prognosis for growth is good if the blood supply to the separated portion of the epiphysis is still intact and if the joint surface heals in a normal position.
Figure 9. Tibial growth plate fracture (Salter-Harris type III fracture – comminuted fracture of the talus extending to ankle joint with fracture of growth plate of lower end of tibia. Also evident is fracture lateral margin of navicular bone.)
Type IV Growth Plate Fractures
These fractures break through the bone shaft, the growth plate, and the end of the bone.
- Through or transverse or together – the fractures run through the growth plate, metaphysis, and epiphysis.
- Intra-articular
- 10% of all growth plate fractures. This injury occurs most commonly at the end of the humerus (the upper arm bone) near the elbow.
- Fracture plane passes directly through the metaphysis, growth plate and down through the epiphysis
- Poor prognosis as the proliferative and reserve zones are interrupted. Doctors frequent need to perform surgery to restore the joint surface to normal and to perfectly align the growth plate. If perfect alignment isn’t achieved and maintained during healing, prognosis for growth is poor, and angulation (bending) of the bone may occur.
Figure 10. Metatarsal head growth plate fracture (Salter-Harris type IV fracture – intraarticular fracture involving the left 3rd metatarsal head with step depression of the dominant metatarsal head fragment of up to 2mm)

Figure 11. Hip growth plate fracture (triradiate cartilage fracture)

Type V Growth Plate Fractures
These fractures occur due to a crushing injury to the growth plate from a compression force. They are rare fractures.
- Ruined or rammed
- Uncommon <1% for growth plate fracture. However, when it happens, it is most likely to occur at the knee or ankle.
- Crushing type injury does not displace the growth plate but damages it by direct compression
- Worst prognosis because premature stunting of growth almost always occurs.
Type VI growth plate fractures
Type VI fractures are included in a newer classification, called the Peterson classification. This injury happens when a portion of the epiphysis, growth plate, and metaphysis are missing. This usually occurs with open wounds or compound fractures. A type VI growth plate injury often involves lawn mowers, farm machinery, snowmobiles, or gunshot wounds. All children or teens with a type VI fracture require surgery, and most require additional reconstructive or corrective surgery. Bone growth is almost always stunted.
Growth plate fracture complications
Most growth plate fractures heal with no complications. But the following factors can increase the risk of crooked, accelerated or stunted bone growth.
- Severity of the injury. If the growth plate has been shifted, shattered or crushed, the risk of limb deformity is greater.
- Age of the child. Younger children have more years of growth ahead of them, so if the growth plate is permanently damaged, there is more chance of deformity developing. If a child is almost done growing, permanent damage to the growth plate may cause only minimal deformity.
- Location of the injury. The growth plates around the knee are more sensitive to injury. A growth plate fracture at the knee can cause the leg to be shorter, longer or crooked if the growth plate has permanent damage. Growth plate injuries around the wrist and shoulder usually heal without problems.
Although most growth plate fractures heal without any lasting effect, complications can occur.
Rarely, a bony bridge will form across the fracture line, stunting the growth of the bone or causing the bone to curve. If this occurs, your doctor may perform a procedure to remove the bony bar and insert fat or other materials to prevent it from reforming.
In other cases, a growth plate fracture may actually stimulate growth so that the injured bone ends up longer than its opposite, uninjured limb. If this occurs, surgery can help achieve a more even length.
What effect could growth plate arrest have on my child?
Growth arrest may affect the angle of bone growth and overall height of a child. When a body part with two parallel bones, like the wrist, experiences growth arrest, each bone needs to be examined separately. If one bone stops growing, there is risk that the parallel bone might continue to grow and surpass it, making the wrist grow at an angle. Also, if one leg were to stop growing because of a growth arrest, the legs could end up being different lengths. Orthopedic surgeons can usually prevent angled bone growth or unequal bone growth with early treatment.
Usually, an orthopedist can determine whether a child’s bones have stopped growing within the first three to six months after the injury. If the bone has stopped growing, then your child’s doctor will decide whether or not to stunt the bone that matches it. For example, if one of your child’s thigh bones stops growing, the doctor will then decide whether or not to stop the growth of the other thigh bone, so that your child’s legs will be the same length.
If the bone has continued to heal and grow after treatment, then your child may not require more follow-up care.
- Older children have already done most of their growing, and therefore the consequences can be less substantial.
- Younger children’s bones have more growing to do, and therefore if a bone stops growing, the consequences could be more severe.
Most people are concerned with how growth arrest may affect their child’s height. Since height is determined by multiple growth plates in the hips, knees and ankles, having growth arrest in just one of these areas may not ultimately impact a child’s height significantly.
Growth plate fracture prognosis
Most growth plate fractures heal without any lasting effect. However, some children experience complications. The most frequent complication of a growth plate fracture is premature arrest or a stop of bone growth. Whether your child experiences an arrest in growth depends on the type of treatment your child received and the following factors:
- Severity of the injury. If your child’s injury causes the blood supply to the epiphysis to be cut off, growth can be stunted. If the growth plate is shifted, shattered, or crushed, the growth plate may close prematurely, forming a bony bridge or “bar.” The risk of growth arrest is higher in this setting. An open injury in which the skin is broken carries the risk of infection, which could destroy the growth plate.
- Age of your child. In a younger child, the bones have a great deal of growing to do; therefore, growth arrest can be more serious, and closer surveillance is needed. It is also true, however, that younger bones have a greater ability to heal.
- Which growth plate is injured. Some growth plates, such as those in the region of the knee, are more involved in extensive bone growth than others.
- Type of fracture. Of the six fracture types described earlier, types IV, V, and VI are the most serious.
If your child experiences an arrest in bone growth, they could have one limb shorter than the uninjured limb. If only part of the growth plate is injured, growth may be lopsided and the limb may become crooked.
Growth plate injuries at the knee have the greatest risk of complications. Nerve and blood vessel damage occurs most frequently there. Injuries to the knee have a much higher incidence of premature growth arrest and crooked growth.
Growth plate fractures must be watched carefully to ensure proper long-term results. Regular follow-up visits to the doctor should continue for at least a year after the fracture to make sure that the growth plate is growing appropriately.
More complicated fractures, as well as fractures to the thighbone (femur) and shinbone (tibia), may require follow-up visits until the child reaches skeletal maturity.
Growth plate fracture causes
Growth plate injuries happen for many reasons. Growth plate fractures are often caused by a single event, such as a fall or car accident. They can also occur gradually as a result of repetitive stress on the bone, which may occur when a child overtrains in a sports activity.
Sometimes growth plate injuries happen when your child overuses a certain part of the body. For example:
- Gymnasts who practice for hours on the uneven bars.
- Long-distance runners.
- Baseball pitchers perfecting their curve balls.
Although many growth plate injuries are caused by accidents that occur during play or athletic activity, growth plates are also susceptible to other disorders that can alter their normal growth and development. Other possible causes of growth plate injuries include the following:
- Bone infections.
- Child abuse.
- Injury from extreme cold (for example, frostbite).
- Radiation and medications.
- Neurological disorders.
- Genetics.
- Metabolic disease.
All children who are still growing are at risk for growth plate injuries, but there are certain factors that may make them more likely to occur:
- Growth plate fractures occur twice as often in boys as in girls, because girls finish growing earlier than boys.
- One-third of all growth plate fractures occur during participation in competitive sports such as football, basketball, or gymnastics.
- About 20% of all growth plate fractures occur during participation in recreational activities such as biking, sledding, skiing, or skateboarding.
- The incidence of growth plate fractures peaks in adolescence.
Risk factors for growth plate fracture
Growth plate fractures occur twice as often in boys as in girls, because girls finish growing earlier than do boys. By the age of 12, most girls’ growth plates have already matured and been replaced with solid bone.
Growth plate fracture symptoms
Most growth plate fractures occur in bones of the fingers, forearm and lower leg.
Signs and symptoms of a growth plate fracture may include:
- Pain and tenderness, particularly in response to pressure on the growth plate
- Inability to move the affected area or to put weight or pressure on the limb
- Warmth and swelling at the end of a bone, near a joint
Growth plate fracture diagnosis
Because growth plates haven’t hardened into solid bone, they are difficult to interpret on X-rays. Doctors may ask for X-rays of both the injured limb and the opposite limb so that they can be compared.
Sometimes a growth plate fracture cannot be seen on X-ray. If the child is tender over the area of the growth plate, your doctor may recommend a cast or a splint to protect the limb. X-rays are taken again in three to four weeks and, if there was a fracture, new bone healing will typically be seen at that time.
For more-serious injuries, scans that can visualize soft tissue — such as magnetic resonance imaging (MRI), computerized tomography (CT) or ultrasound — may be ordered.
Growth plate fracture treatment
Treatment for growth plate fractures depends on several factors, including:
- Which bone is injured
- The type of fracture
- How much the broken ends of the bone are out of alignment (displaced)
- The age and health of the child
- Any associated injuries
Nonsurgical Treatment
Many growth plate fractures can heal successfully when treated with immobilization. The least serious fractures usually require only a cast or a splint. A cast is applied to the injured area and the child limits some types of activity.
Doctors most often use cast immobilization when the broken fragments of bone are not significantly out of place. A cast will protect the bones and hold them in proper position while they heal.
Surgical Treatment
If the fracture crosses the growth plate or goes into the joint and is not well-aligned, surgery may be necessary.
If the bone fragments are displaced and the fracture is unstable, surgery may be necessary.
Growth plates that are surgically realigned may have a better chance of recovering and growing again than do growth plates that are left in a poor position.
The most common operation used to treat fractures is called open reduction and internal fixation.
During the procedure, the bone fragments are first repositioned into their normal alignment (called a reduction). The bones are then fixed into place with special implants like screws or wires, or by attaching metal plates to the outer surface of the bone.
A cast is often applied to protect and immobilize the injured area while it heals.
Growth plate fracture healing time
A child’s bones heal quickly, but a growth plate fracture can still take several weeks to heal. If cast immobilization is used, the length of time the cast is worn will vary depending on the severity of the fracture.
After the bone heals, your doctor may recommend specific exercises to strengthen the muscles that support the injured area of bone and improve the range of motion of the joint.
At the time of injury, it’s difficult to tell if a growth plate has permanent damage. Your doctor may recommend checking X-rays for several years after the fracture to make sure the growth plate is growing appropriately. Depending on the location and severity of the fracture, your child may need follow-up visits until his or her bones have finished growing.
- Salter R, Harris WR. Injuries Involving the Epiphyseal Plate. J Bone Joint Surg Am 1963. 45 (3) 587-622.[↩]
- Little JT, Klionsky NB, Chaturvedi A et-al. Pediatric distal forearm and wrist injury: an imaging review. Radiographics. 2014;34 (2): 472-90. doi:10.1148/rg.342135073 http://pubs.rsna.org/doi/10.1148/rg.342135073[↩]





{kind=link}