
Contents
- What is hemoglobin
- How is hemoglobin test used?
- Why get your hemoglobin tested?
- Normal hemoglobin levels
- What are Red blood cells
- What are Hemoglobin abnormalities?
- Low hemoglobin
- High hemoglobin levels
- Hemoglobin a1c
What is hemoglobin
Hemoglobin (Hb or Hgb) is the iron-containing protein found in all red blood cells (RBCs) that gives red blood cells their characteristic red color and it carries oxygen (O2) throughout the body. Hemoglobin enables red blood cells to bind to oxygen in the lungs and carry oxygen to tissues and organs throughout your body. Hemoglobin also helps transport a small portion of carbon dioxide (CO2), a product of cell metabolism, from tissues and organs to the lungs, where it is exhaled 1. Under normal circumstances, adult blood contains 4 types of hemoglobin: oxygenated hemoglobin or oxyhemoglobin, hemoglobin that contains no oxygen (reduced hemoglobin) or deoxyhemoglobin, hemoglobin transporting carbon dioxide or carboxyhemoglobin, and oxidized hemoglobin or methemoglobin. The last 2 are usually found in small amounts in blood.
Hemoglobin is made up of heme, which is the iron-containing portion, and globin chains, which are proteins. The globin protein consists of chains of amino acids, the “building blocks” of proteins. One portion of hemoglobin called heme is the molecule with iron at the center (see Figure 1). Another portion is made of up four protein chains called globins. Depending on their structure, the globin chains are designated as alpha (α), beta (ß), delta (δ), and gamma (γ). Each of the four globin chains holds a heme group containing one iron atom. .
Not all hemoglobin is the same. Different types of hemoglobin are classified according to the type of globin chains they contain. The type of globin chains present is important in hemoglobin’s ability to transport oxygen.
Normal hemoglobin types include:
- Hemoglobin A (Hb A) – this is the predominant type of hemoglobin (Hb) in adults, makes up about 95%-98% of hemoglobin found in adults; Hb A contains two alpha (α) protein chains and two beta (ß) protein chains.
- Hemoglobin A2 (Hb A2) – makes up about 2-3.5% of hemoglobin (Hb) found in adults; it has two alpha (α) and two delta (δ) protein chains.
- Hemoglobin F (Hb F, fetal hemoglobin) – makes up to 1%-2% of hemoglobin (Hb) found in adults; it has two alpha (α) and two gamma (γ) protein chains. Hemoglobin F (Hb F, fetal hemoglobin) is the primary hemoglobin produced by a developing baby (fetus) during pregnancy. Its production usually falls to a low level within a year after after birth and reaches adult level within 1-2 years.
For hemoglobin (Hb), there are four genes in your DNA that code for the alpha (α) globin chains and two genes (each) for the beta (β), delta (δ), and gamma (γ) globin chains. Globin polypeptides are synthesized from separate α-like and β-like globin gene clusters located on human chromosomes 16 and 11, respectively. Since everyone inherits a set of chromosomes from each parent, each person inherits two alpha globulin genes and one beta globulin gene from each parent. A person may inherit mutations in either the alpha or beta globin genes.
The hemoglobin test measures the amount of hemoglobin in a person’s sample of blood. Serum free hemoglobin is a blood test that measures the level of free hemoglobin in the liquid part of the blood (the serum). Free hemoglobin is the hemoglobin outside of the red blood cells. Most of the hemoglobin is found inside the red blood cells, not in the serum. A hemoglobin level can be performed alone or with a hematocrit, a test that measures the proportion of blood that is made up of red blood cells, to quickly evaluate an individual’s red blood cells. Red blood cells, which make up about 40% (ranging 37-49%) of the blood’s volume, are produced in the bone marrow and are released into the bloodstream when they are, or nearly are, mature. The typical lifespan of an red blood cell is 120 days, and the bone marrow must continually produce new red blood cells to replace those that age and degrade or are lost through bleeding.
Several diseases and conditions can affect red blood cells and consequently the level of hemoglobin in the blood. In general, the hemoglobin level and hematocrit rise when the number of red blood cells increases. The hemoglobin level and hematocrit fall to less than normal when there is a drop in production of red blood cells by the bone marrow, an increase in the destruction of red blood cells, or if blood is lost due to bleeding. A drop in the red blood cell count, hemoglobin and hematocrit can result in anemia, a condition in which tissues and organs in the body do not get enough oxygen, causing fatigue and weakness. If too many red blood cells are produced, polycythemia results and the blood can become thickened, causing sluggish blood flow and related problems.
Since a hemoglobin level is often performed as part of a complete blood count (CBC), results from other components are taken into consideration. A rise or drop in the hemoglobin level must be interpreted in conjunction with other parameters, such as red blood cell count, hematocrit, reticulocyte count, and/or red blood cell indices. Age, sex, and race are other factors to be considered.
The hemoglobin test is a common test and is almost always done as part of a complete blood count (CBC). Reasons or conditions for ordering the hemoglobin test include:
- Symptoms such as fatigue, poor health, or unexplained weight loss
- Signs of bleeding
- Before and after major surgery
- During pregnancy
- Chronic kidney disease or many other chronic medical problems
- Monitoring of anemia and its cause
- Monitoring during treatment for cancer
- Monitoring medicines that may cause anemia or low blood counts
In general, hemoglobin mirrors the results of the red blood cell count and hematocrit.
- A recent blood transfusion can affect a person’s hemoglobin level.
- Hemoglobin decreases slightly during normal pregnancy.
Low hemoglobin with low red blood cell count and low hematocrit indicates anemia. Some causes include:
- Excessive loss of blood from, for example, severe trauma or chronic bleeding from sites such as the digestive tract (e.g., ulcers, polyps, colon cancer), the bladder or uterus (in women, heavy menstrual bleeding, for example)
- Nutritional deficiencies such as iron, folate or B12 deficiency
- Damage to the bone marrow from, for example, a toxin, radiation or chemotherapy, infection or drugs
- Bone marrow disorders such as aplastic anemia, myelodysplastic syndrome, or cancers such as leukemia, lymphoma, multiple myeloma, or other cancers that spread to the marrow
- Kidney failure—severe and chronic kidney diseases lead to decreased production of erythropoietin, a hormone produced by the kidneys that stimulates red blood cell production by the bone marrow.
- Chronic inflammatory diseases or conditions
- Decreased hemoglobin production (e.g., thalassemia)
- Excessive destruction of red blood cells, for example, hemolytic anemia caused by autoimmunity or defects in the red blood cell itself; the defects could be hemoglobinopathy (e.g., sickle cell anemia), abnormalities in the red blood cell membrane (e.g., hereditary spherocytosis) or red blood cell enzyme (e.g., G6PD deficiency).
High hemoglobin with a high red blood cell count and high hematocrit indicates polycythemia. Some causes include:
- Lung (pulmonary) disease—if someone is unable to breathe in and absorb sufficient oxygen, the body tries to compensate by producing more red blood cells.
- Congenital heart disease—in some forms, there is an abnormal connection between the two sides of the heart, leading to reduced oxygen levels in the blood. The body tries to compensate by producing more red blood cells.
- Kidney tumors that produce excess erythropoietin
- Smoking—heavy smokers have higher hemoglobin levels than nonsmokers.
- Genetic causes (altered oxygen sensing, abnormality in hemoglobin oxygen release)
- Living at high altitudes (a compensation for decreased oxygen in the air)
- Dehydration—as the volume of fluid in the blood drops, the hemoglobin artificially rises.
- Polycythemia vera—a rare disease in which the body produces excess red blood cells inappropriately
Figure 1. Red blood cell hemoglobin
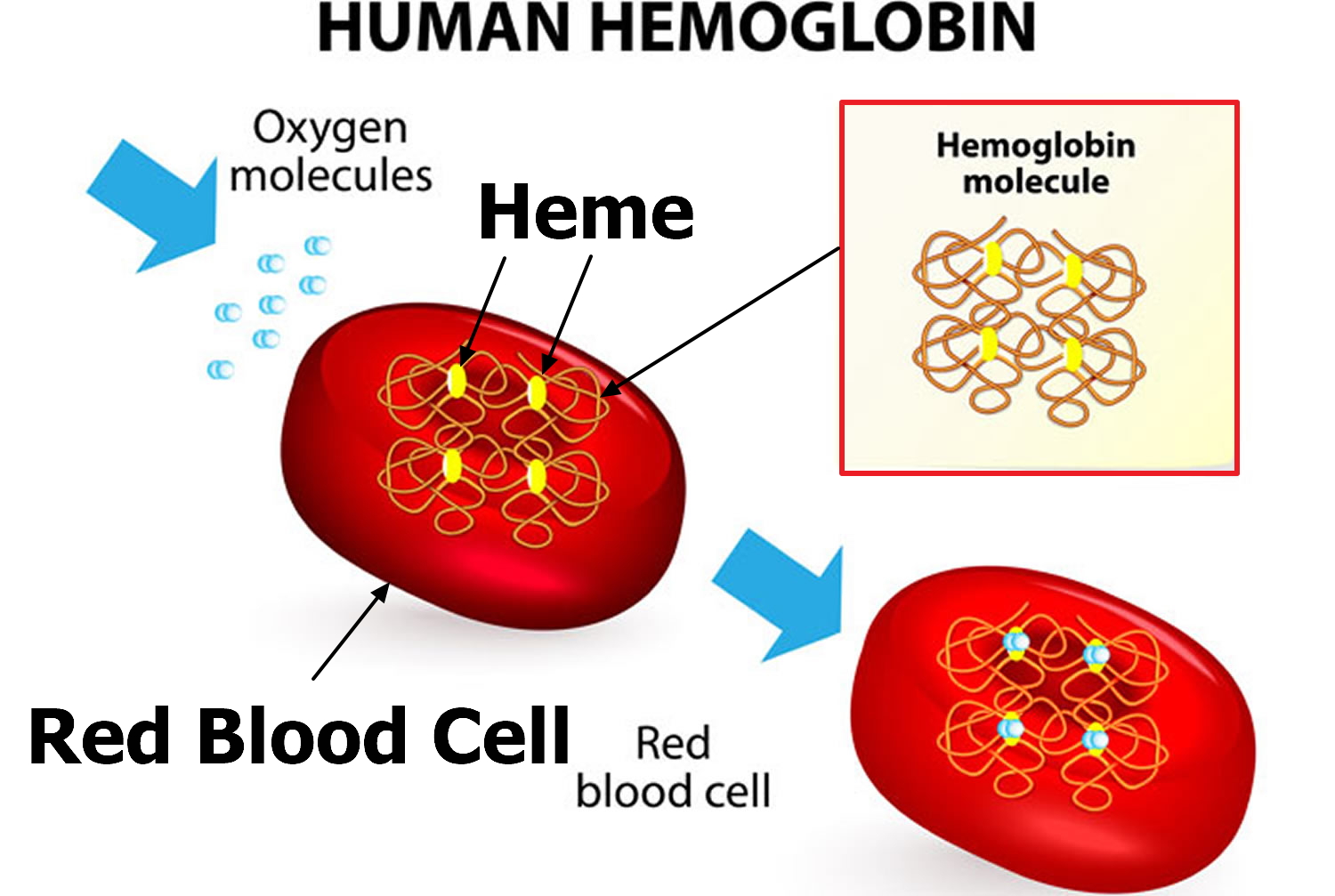
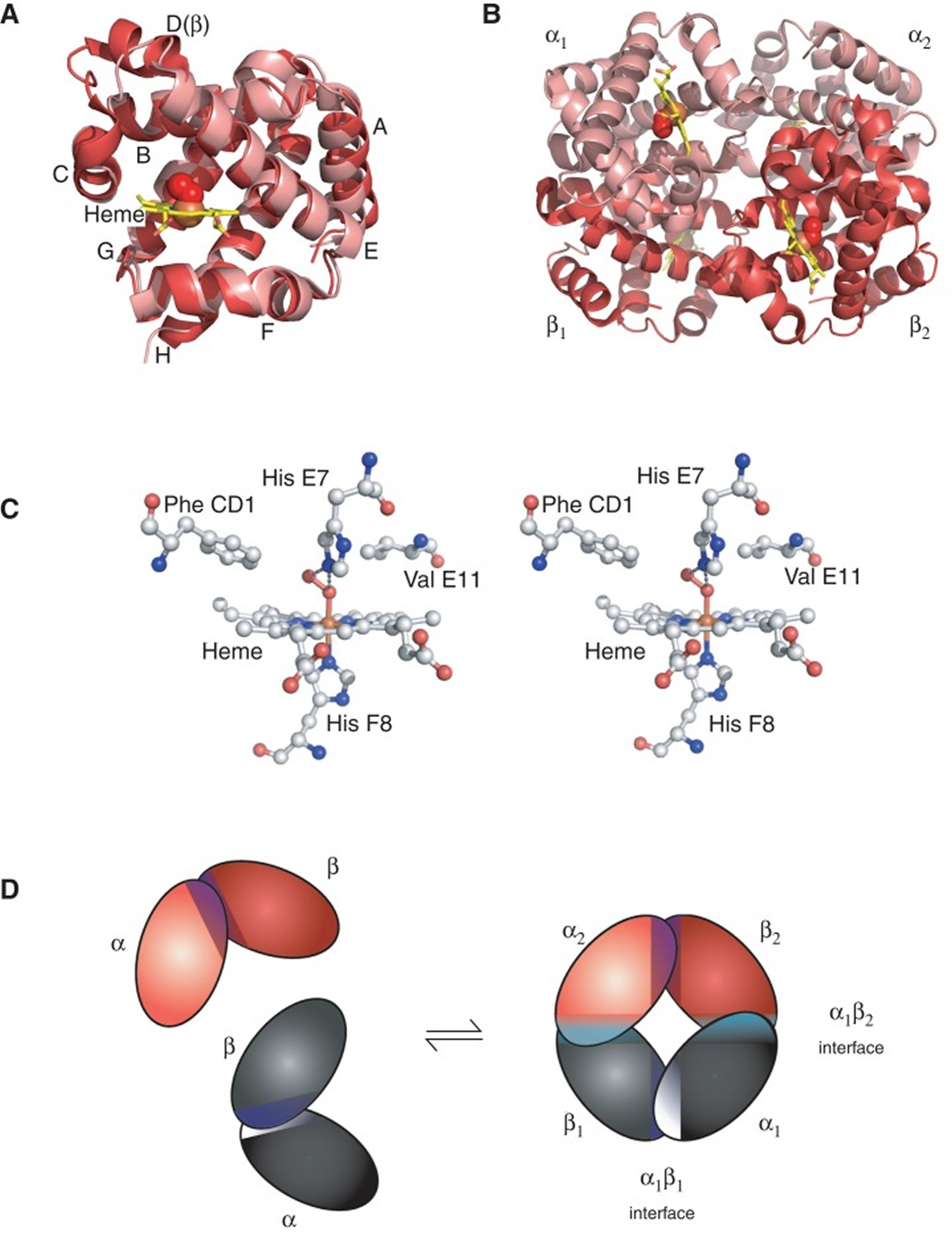
Figure 2. Structure of hemoglobin
 Footnotes:
Footnotes:The structure of hemoglobin (Hb). (A) The α (pink) and β (red) hemoglobin (Hb) subunits have conserved α-helical folds. Helices are labeled A–H from the amino terminus. The α subunit lacks helix D. (B) The high O2 affinity R state quaternary structure of hemoglobin (Hb) with O2 (red spheres) bound at all four heme sites (protoporphyrin-IX as yellow sticks, with central iron atom as orange sphere). (C) Stereo (wall-eye) diagram of the heme pocket of β showing the proximal (F8) and distal (E7) histidines and selected residues in the distal heme pocket that influence ligand binding and autoxidation. (D) hemoglobin (Hb) tetramer is assembled from two identical αβ dimers (shown in red and gray for clarity). In the tetramer, each subunit makes contact with the unlike chain through a high affinity dimerization α1β1 interface and a lower affinity α1β2 dimer–tetramer interface (cyan).
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm or by a fingerstick (for children and adults) or heelstick (for newborns).
Is any test preparation needed to ensure the quality of the sample?
If your blood sample is being tested only for hemoglobin, you can eat and drink normally before the test. If your blood sample will be used for other tests, you may need to fast for a certain amount of time before the sample is taken. Your doctor will give you specific instructions.
Are there warning signs for abnormally low hemoglobin levels?
Some warning signs are fatigue, fainting, pale skin (pallor), and shortness of breath.
Can I test my hemoglobin at home?
Yes, there are some home tests currently available that have been approved by the U.S. Food and Drug Administration (FDA). Home testing offers many benefits, but it’s also important to recognize the potential tradeoffs between quality and convenience and to take steps to protect yourself against the possibility of false results, and your own lack of training. Talk to your doctor about this type of testing and consult her about any questions or concerns you may have.
Is anyone at greater risk of abnormal hemoglobin levels?
Women of childbearing age tend to have lower hemoglobin levels than men due to loss of iron and blood during menstrual periods and increased need for iron during pregnancy. Others who are at greater risk of a low hemoglobin level (anemia) include people with poor nutrition and diets low in iron or vitamins, people who have undergone surgery or have been severely injured, people with chronic conditions such as kidney disease, cancer, HIV/AIDS, inflammatory bowel disease, chronic infection or chronic inflammatory conditions (e.g., rheumatoid arthritis). Someone who has family members with a genetic cause of anemia, such as sickle cell or thalassemia, also has a higher risk of having the condition and a higher risk of anemia.
Can a healthy diet and nutrition help keep optimal hemoglobin levels?
Yes, to the extent that if you eat a well-balanced diet, you can prevent anemia due to a lack of iron, vitamin B12, or folate in the foods you eat. Sometimes use of a supplement is recommended if you are at risk of a vitamin deficiency. However, the most common cause of vitamin B12 deficiency is malabsorption, and the most common cause of iron deficiency is bleeding. These conditions and other red blood cell problems that are caused by diseases other than nutritional deficiencies cannot be corrected by diet.
How is hemoglobin test used?
The hemoglobin test is often used to check for anemia, usually along with a hematocrit or as part of a complete blood count (CBC). The test may be used to screen for, diagnose, or monitor a number of conditions and diseases that affect red blood cells (RBCs) and/or the amount of hemoglobin in blood. Hemoglobin is the iron-containing protein found in all red blood cells that enables red blood cells to bind to oxygen in the lungs and carry it to tissues and organs throughout the body.
A hemoglobin test may be used to:
- Check your overall health. Your doctor may test your hemoglobin as part of a complete blood count during a routine medical examination to monitor your general health and to screen for a variety of disorders, diagnose, and measure the severity of anemia (low red blood cells, hemoglobin and hematocrit) or polycythemia (high red blood cells, hemoglobin and hematocrit).
- Diagnose a medical condition. Your doctor may suggest a hemoglobin test if you’re experiencing weakness, fatigue, shortness of breath or dizziness. These signs and symptoms may point to anemia or polycythemia vera. A hemoglobin test may help diagnose these or other medical conditions.
- Monitor a medical condition. If you’ve been diagnosed with anemia or polycythemia vera, your doctor may use a hemoglobin test to monitor your condition and guide treatment.
- Help make decisions about blood transfusions or other treatments if the anemia is severe.
Some conditions affect red blood cell production in the bone marrow and may cause an increase or decrease in the number of mature red blood cells released into the blood circulation. Other conditions may affect the lifespan of red blood cells in the circulation. If there is increased destruction of red blood cells (hemolysis) or loss of red blood cells through bleeding and/or the bone marrow is not able to produce new ones fast enough, then the overall number of red blood cells and hemoglobin will drop, resulting in anemia.
This test can indicate if there is a problem with red blood cell production and/or lifespan, but it cannot determine the underlying cause. In addition to the full CBC, some other tests that may be performed at the same time or as follow up to establish a cause include a blood smear, reticulocyte count, iron studies, vitamin B12 and folate levels, and in more severe conditions, a bone marrow examination.
Why get your hemoglobin tested?
The hemoglobin test is a common test and is almost always done as part of a complete blood count (CBC) to evaluate the hemoglobin content of your blood as part of a general health checkup; to screen for and help diagnose conditions that affect red blood cells (RBCs); if you have anemia (low hemoglobin) or polycythemia (high hemoglobin), to assess the severity of these conditions and to monitor response to treatment.
Reasons or conditions for ordering the hemoglobin test include:
- Symptoms such as fatigue, poor health, or unexplained weight loss
- Signs of bleeding
- Before and after major surgery
- During pregnancy
- Chronic kidney disease or many other chronic medical problems
- Monitoring of anemia and its cause
- Monitoring during treatment for cancer
- Monitoring medicines that may cause anemia or low blood counts
When is hemoglobin test ordered?
The hemoglobin test may be ordered during a general health examination or when a person has signs and symptoms of a condition affecting red blood cells such as anemia or polycythemia.
Some signs and symptoms of anemia include:
- Weakness or fatigue
- Lack of energy
- Fainting
- Paleness (pallor)
- Shortness of breath
Some signs and symptoms of polycythemia include:
- Disturbed vision
- Dizziness
- Headache
- Flushing
- Enlarged spleen
This test may be performed several times or on a regular basis when someone has been diagnosed with ongoing bleeding problems or chronic anemias or polycythemia to determine the effectiveness of treatment. It may also be ordered routinely for people undergoing treatment for cancer that is known to affect the bone marrow.
Normal hemoglobin levels
Normal hemoglobin results for adults vary, but in general are:
- Male: 13.8 to 17.2 grams per deciliter (g/dL) or 138 to 172 grams per liter (g/L)
- Female: 12.1 to 15.1 g/dL or 121 to 151 g/L
Normal hemoglobin results for children vary, but in general are:
- Newborn: 14 to 24 g/dL or 140 to 240 g/L
- Infant: 9.5 to 13 g/dL or 95 to 130 g/L
The normal hemoglobin ranges above are common measurements for results of the hemoglobin test and is almost always done as part of a complete blood count (CBC) tests. Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your health care provider about the meaning of your specific test results.
Plasma or serum hemoglobin in someone who does not have hemolytic anemia may contain up to 5 milligrams per deciliter (mg/dL) or 0.05 grams per liter (g/L) hemoglobin.
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or may test different samples. Talk to your health care provider about the meaning of your specific test results.
A higher-than-normal level of serum hemoglobin (free hemoglobin) may indicate:
- A hemolytic anemia
- Condition in which red blood cells break down when the body is exposed to certain drugs or the stress of infection (G6PD deficiency)
- Low red blood cell count due to red blood cells breaking down sooner than normal
- Blood disorder in which red blood cells are destroyed when they go from cold to warm temperatures (paroxysmal cold hemoglobinuria)
- Sickle cell anemia
- Disorder in which there is excessive breakdown of hemoglobin (thalassemia)
- Transfusion reaction
What are Red blood cells
Blood transports a variety of materials between interior body cells and those that exchange substances with the external environment. In this way, blood helps maintain stable internal environmental conditions. Blood is composed of formed elements suspended in a fluid extracellular matrix called blood plasma. The “formed elements” include red blood cells, white blood cells, and cell fragments called platelets. Most blood cells form in red marrow within the hollow parts of certain long bones.
Most blood samples are roughly 37% to 49% red blood cells by volume – adult females is 38–46% (average = 42%) and for adult males, it
is 40–54% (average = 47). This percentage is called the hematocrit. The white blood cells and platelets account for less than 1% of blood volume. The remaining blood sample, about 55%, is the plasma, a clear, straw-colored liquid. Blood plasma is a complex mixture of water, gases, amino acids, proteins, carbohydrates, lipids, vitamins, hormones, electrolytes, and cellular wastes (see Figure 1).
Blood volume varies with body size, percent adipose tissue, and changes in fluid and electrolyte concentrations. An average-size adult has a blood volume of about 5 liters (5.3 quarts), 4–5 liters in a female and 5–6 liters in a male.
Red blood cell (also called erythrocyte) is biconcave disc without a nucleus. This biconcave shape is an adaptation for transporting the gases oxygen and carbon dioxide. It increases the surface area through which oxygen and carbon dioxide can diffuse into and out of the cell. The characteristic shape of a red blood cell also places the cell membrane closer to oxygen-carrying hemoglobin (Figure 5) molecules in the cell reducing the distance for diffusion.
Each red blood cell is about one-third hemoglobin by volume. This protein imparts the color of blood. When hemoglobin binds oxygen, the resulting oxyhemoglobin is bright red, and when oxygen is released, the resulting deoxyhemoglobin is darker.
Prolonged oxygen deficiency (hypoxia) causes cyanosis, in which the skin and mucous membranes appear bluish due to an abnormally high blood concentration of deoxyhemoglobin in the superficial blood vessels. Exposure to low temperature may also result in cyanosis by constricting superficial blood vessels. This response to environmental change slows skin blood flow. As a result, more oxygen than usual is removed from the blood flowing through the vessels, increasing the concentration of deoxyhemoglobin.
Note: Blood is a complex mixture of formed elements in a liquid extracellular matrix, called blood plasma. Note that water and proteins account for 99% of the blood plasma.
Figure 2. Blood composition


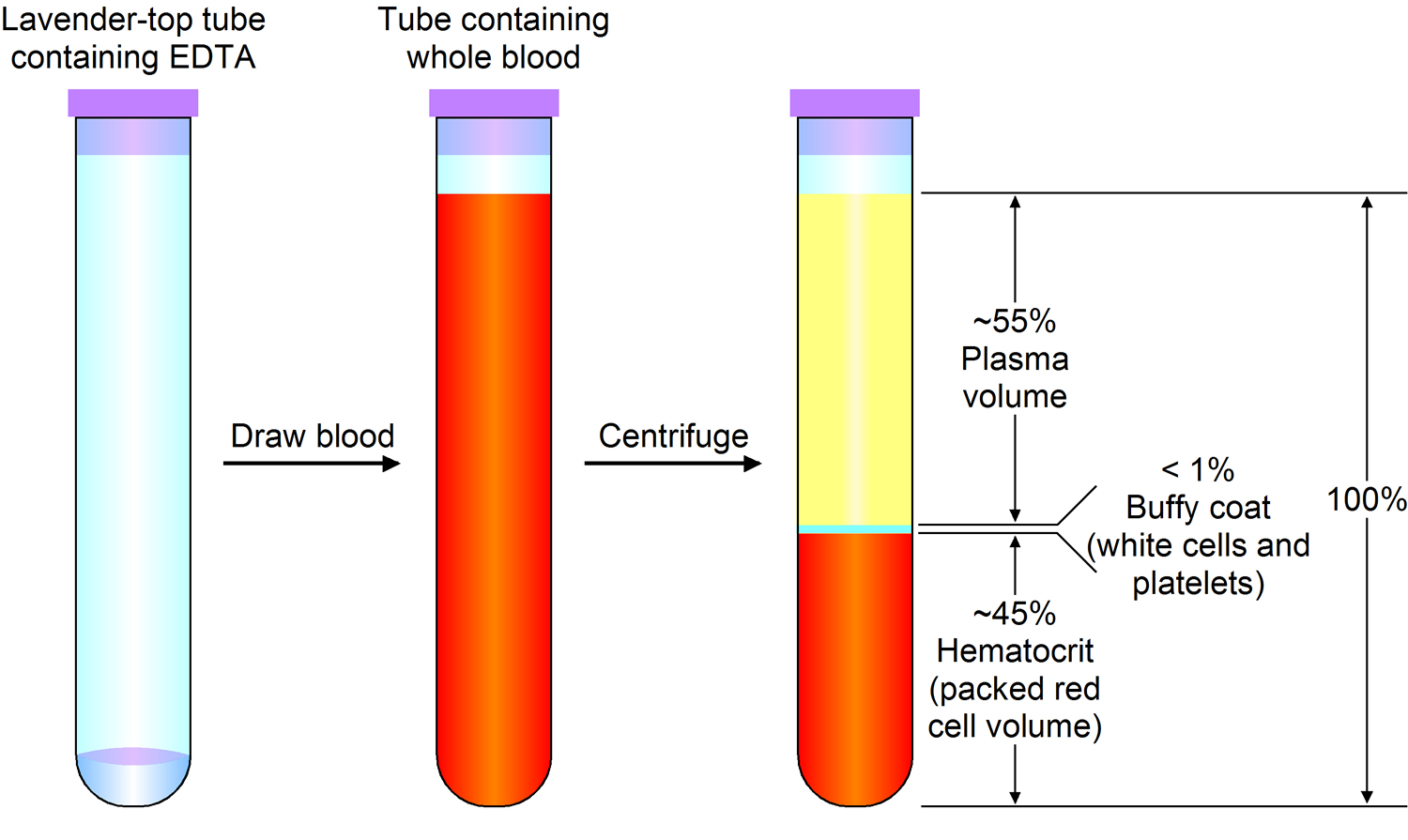
Note: Blood consists of a liquid portion called plasma and a solid portion (the formed elements) that includes red blood cells, white blood cells, and platelets. When blood components are separated by centrifugation, the white blood cells and platelets form a thin layer, called the “buffy coat,” between the plasma and the red blood cells, which accounts for about 1% of the total blood volume. Blood cells and platelets can be seen under a light microscope when a blood sample is smeared onto a glass slide.
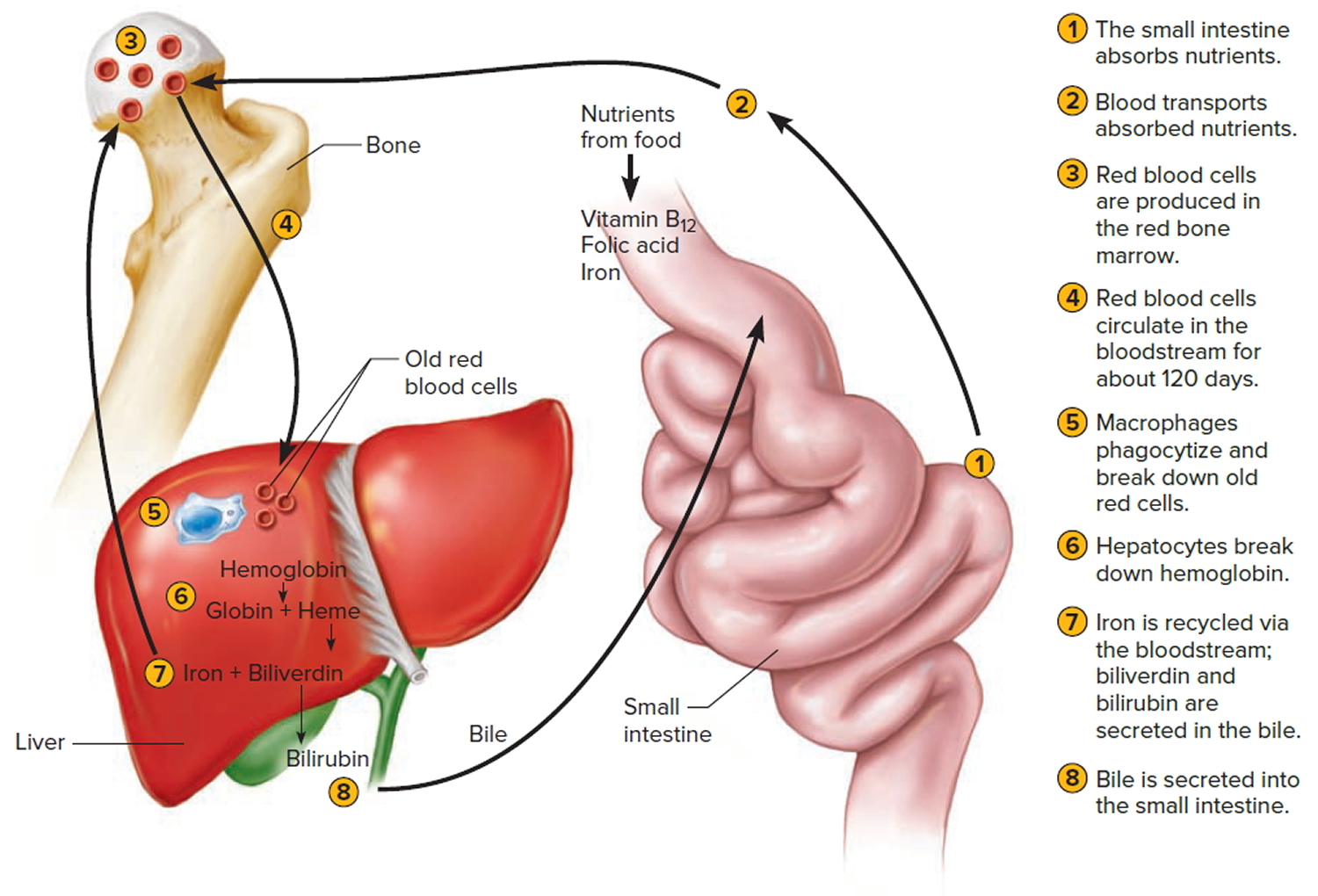
Figure 3. Lifecycle of a red blood cell
What are Hemoglobin abnormalities?
A hemoglobin abnormality is a variant form of hemoglobin that is often inherited and may cause a blood disorder (hemoglobinopathy).
Genetic changes (mutations) in the globin genes cause alterations in the globin protein, resulting in structurally altered hemoglobin, such as hemoglobin S, which causes sickle cell, or a decrease in globin chain production (thalassemia). In thalassemia, the reduced production of one of the globin chains upsets the balance of alpha to beta chains and causes abnormal hemoglobin to form (alpha thalassemia) or causes an increase of minor hemoglobin components, such as Hb A2 or Hb F (beta thalassemia).
Four genes code for the alpha globin chains, and two genes (each) code for the beta, delta, and gamma globin chains. Mutations may occur in either the alpha or beta globin genes. The most common alpha-chain-related condition is alpha thalassemia. The severity of this condition depends on the number of genes affected.
Mutations in the beta gene are mostly inherited in an autosomal recessive fashion. This means that the person must have two altered gene copies, one from each parent, to have a hemoglobin variant-related disease. If one normal beta gene and one abnormal beta gene are inherited, the person is heterozygous for the abnormal hemoglobin, known as a carrier. The abnormal gene can be passed on to any children, but it generally does not cause symptoms or significant health concerns in the carrier.
If two abnormal beta genes of the same type are inherited, the person is homozygous. The person would produce the associated hemoglobin variant and may have some associated symptoms and potential for complications. The severity of the condition depends on the genetic mutation and varies from person to person. A copy of the abnormal beta gene would be passed on to any children.
If two abnormal beta genes of different types are inherited, the person is “doubly heterozygous” or “compound heterozygous.” The affected person would typically have symptoms related to one or both of the hemoglobin variants that he or she produces. One of the abnormal beta genes would be passed on to children.
Red blood cells containing abnormal hemoglobin may not carry oxygen efficiently and may be broken down by the body sooner than usual (a shortened survival), resulting in hemolytic anemia. Several hundred hemoglobin variants have been documented, but only a few are common and clinically significant. Some of the most common hemoglobin variants include hemoglobin S, the primary hemoglobin in people with sickle cell disease that causes the red blood cell to become misshapen (sickle), decreasing the cell’s survival; hemoglobin C, which can cause a minor amount of hemolytic anemia; and hemoglobin E, which may cause no symptoms or generally mild symptoms.
Hemoglobin variants
Several hundred abnormal forms of hemoglobin (variants) have been identified, but only a few are common and clinically significant.
Common hemoglobin variants
- Hemoglobin S (Hb S): this is the primary hemoglobin in people with sickle cell disease (also known as sickle cell anemia). Approximately 1 in 375 African American babies are born with sickle cell disease, and about 100,000 Americans live with the disorder, according to the Centers for Disease Control and Prevention. Those with hemoglobin S (Hb S) disease have two abnormal beta chains and two normal alpha chains. The presence of hemoglobin S causes the red blood cell to deform and assume a sickle shape when exposed to decreased amounts of oxygen (such as might happen when someone exercises or has infection in the lungs). Sickled red blood cells are rigid and can block small blood vessels, causing pain, impaired circulation, and decreased oxygen delivery, as well as shortened red cell survival. A single beta (βS) copy (known as sickle cell trait, which is present in approximately 8% of African Americans) typically does not cause significant symptoms unless it is combined with another hemoglobin mutation, such as that causing hemoglobin C (Hb C) or beta thalassemia.
- Hemoglobin C (Hb C): about 2-3% of African Americans in the United States are heterozygotes for hemoglobin C (have one copy, known as hemoglobin C trait) and are often asymptomatic. Hemoglobin C disease (seen in homozygotes, those with two copies) is rare (0.02% of African Americans) and relatively mild. It usually causes a minor amount of hemolytic anemia and a mild to moderate enlargement of the spleen.
- Hemoglobin E (Hb E): Hemoglobin E is one of the most common beta chain hemoglobin variants in the world. It is very prevalent in Southeast Asia, especially in Cambodia, Laos, and Thailand, and in individuals of Southeast Asian descent. People who are homozygous for hemoglobin E (Hb E) (have two copies of βE) generally have a mild hemolytic anemia, microcytic red blood cells, and a mild enlargement of the spleen. A single copy of the hemoglobin E gene does not cause symptoms unless it is combined with another mutation, such as the one for beta thalassemia trait.
Less common hemoglobin variants
There are many other variants. Some are silent – causing no signs or symptoms – while others affect the functionality and/or stability of the hemoglobin molecule. Examples of other variants include: Hemoglobin D, Hemoglobin G, Hemoglobin J, Hemoglobin M, and Hemoglobin Constant Spring caused by a mutation in the alpha globin gene that results in an abnormally long alpha (α) chain and an unstable hemoglobin molecule. Additional examples include:
- Hemoglobin F (Hb F): Hb F is the primary hemoglobin produced by the fetus, and its role is to transport oxygen efficiently in a low oxygen environment. Production of Hb F decreases sharply after birth and reaches adult levels by 1-2 years of age. Hb F may be elevated in several congenital disorders. Levels can be normal to significantly increased in beta thalassemia and are frequently increased in individuals with sickle cell anemia and in sickle cell-beta thalassemia. Individuals with sickle cell disease and increased Hb F often have a milder disease, as the F hemoglobin inhibits sickling of the red cells. Hb F levels are also increased in a rare condition called hereditary persistence of fetal hemoglobin. This is a group of inherited disorders in which Hb F levels are increased without the signs or clinical features of thalassemia. Different ethnic groups have different mutations causing hereditary persistence of fetal hemoglobin. Hb F can also be increased in some acquired conditions involving impaired red blood cell production. Some leukemias and other myeloproliferative neoplasms are also associated with mild elevation in Hb F.
- Hemoglobin H (Hb H): Hb H is an abnormal hemoglobin that occurs in some cases of alpha thalassemia. It is composed of four beta (β) globin chains and is produced due to a severe shortage of alpha (α) chains. Although each of the beta (β) globin chains is normal, the tetramer of 4 beta chains does not function normally. It has an increased affinity for oxygen, holding onto it instead of releasing it to the tissues and cells. Hemoglobin H is also associated with significant breakdown of red blood cells (hemolysis) as it is unstable and tends to form solid structures within red blood cells. Serious medical problems are not common in people with hemoglobin H disease, though they often have anemia.
- Hemoglobin Barts (Hb Barts): Hb Barts develops in fetuses with alpha thalassemia. It is formed of four gamma (γ) protein chains when there is a shortage of alpha chains, in a manner similar to the formation of Hemoglobin H. If a small amount of Hb Barts is detected, it usually disappears shortly after birth due to dwindling gamma chain production. These children have one or two alpha gene deletions and are silent carriers or have the alpha thalassemia trait. If a child has a large amount of Hb Barts, he or she usually has hemoglobin H disease and a three-gene deletion. Fetuses with four-gene deletions have hydrops fetalis and usually do not survive without blood transfusions and bone marrow transplants.
A person can also inherit two different abnormal genes, one from each parent. This is known as being compound heterozygous or doubly heterozygous. Several different clinically significant combinations are listed below.
- Hemoglobin SC disease: inheritance of one beta S gene and one beta C gene results in Hemoglobin SC disease. These individuals have a mild hemolytic anemia and moderate enlargement of the spleen. Persons with Hb SC disease may develop the same vaso-occulsive (blood vessel-blocking) complications as seen in sickle cell anemia, but most cases are less severe.
- Sickle Cell – Hemoglobin D disease: individuals with sickle cell – Hb D disease have inherited one copy of hemoglobin S and one of hemoglobin D-Los Angeles (or D-Punjab) genes. These people may have occasional sickle crises and moderate hemolytic anemia.
- Hemoglobin E – beta thalassemia: individuals who are doubly heterozygous for hemoglobin E and beta thalassemia have an anemia that can vary in severity, from mild (or asymptomatic) to severe, dependent on the beta thalassemia mutation(s) present.
- Hemoglobin S – beta thalassemia: sickle cell – beta thalassemia varies in severity, depending on the beta thalassemia mutation inherited. Some mutations result in decreased beta globin production (beta+) while others completely eliminate it (beta0). Sickle cell – beta+ thalassemia tends to be less severe than sickle cell – beta0 thalassemia. People with sickle cell – beta0 thalassemia tend to have more irreversibly sickled cells, more frequent vaso-occlusive problems, and more severe anemia than those with sickle cell – beta+ thalassemia. It is often difficult to distinguish between sickle cell disease and sickle cell – beta0 thalassemia.
Hemoglobin Abnormalities Signs and Symptoms
Signs and symptoms associated with hemoglobin variants can vary in type and severity depending on the variant present and whether an individual has one variant or a combination. Some are the result of an increase in the breakdown (hemolysis) of red blood cells and a shortened red blood cell survival, leading to anemia. Some examples include:
- Weakness, fatigue
- Lack of energy
- Jaundice
- Pale skin (pallor)
Some serious signs and symptoms include:
- Episodes of severe pain
- Shortness of breath
- Enlarged spleen
- Growth problems in children
- Upper abdomen pain (due to stone formation in gallbladder)
Hemoglobin Abnormalities Diagnosis
Testing for hemoglobin abnormalities (variants) is done:
- To screen for common and clinically significant hemoglobin variants in newborns. In all states, this has become a standard part of newborn screening. Infants with variants such as Hb S can benefit from early detection and treatment.
- As part of prenatal screening, on high-risk women including those with an ethnic background associated with a higher prevalence of hemoglobin variants (such as those of African descent) and those with affected family members. Screening may also be done in conjunction with genetic counseling prior to pregnancy to determine possible carrier status of potential parents.
- To identify variants in asymptomatic parents with an affected child.
- To identify hemoglobin variants in those with symptoms of unexplained anemia, with red blood cells (RBCs) that are small and/or paler than normal (microcytosis and hypochromia). It may also be ordered as part of an anemia investigation, or when someone has signs and symptoms associated with hemoglobin variants.
Laboratory tests
Laboratory testing for hemoglobin variants is an exploration of the “normalness” of an individual’s red blood cells, an evaluation of the hemoglobin inside the red blood cells, and/or an analysis of relevant gene mutations. Each test provides a piece of the puzzle, giving the clinician important information about the hemoglobins that may be present. Testing typically includes:
- CBC (complete blood count): The complete blood count is a snapshot of the cells circulating in the blood. Among other things, the complete blood count will tell the doctor how many red blood cells are present, how much hemoglobin is in them, and give the doctor an evaluation of the average size of the red blood cells present. Mean corpuscular volume (MCV) is a measurement of the size of the red blood cells. A low MCV is often the first indication of thalassemia. If the MCV is low and iron-deficiency has been ruled out, the person may be a carrier of the thalassemia trait or have a hemoglobin variant that results in smaller than normal red blood cells (for example, Hb E).
- Blood smear (also called a peripheral smear): In this test, a trained laboratorian looks under the microscope at a thin layer of blood on a slide treated with a special stain. The number and type of white blood cells, red blood cells, and platelets can be evaluated to see if they are normal and mature. With a hemoglobinopathy, the red blood cells may be:
- Smaller than normal (microcytic)
- Paler than normal (hypochromic)
- Varying in size (anisocytosis) and shape (poikilocytosis, e.g., sickle-shaped cells)
- Having a nucleus (nucleated red blood cell, not normal in a mature red blood cell) or crystal (e.g., C crystal)
- Having uneven hemoglobin distribution (producing “target cells” that look like a bull’s-eye under the microscope).
The greater the percentage of abnormal-looking red blood cells, the greater the likelihood of an underlying disorder.
- Hemoglobinopathy evaluation: These tests identify the type, and measure the relative amount, of the different types of hemoglobin present in an individual’s red blood cells. Most of the common variants can be identified using one of these tests or a combination. The relative amounts of any variant hemoglobin detected can help diagnose combinations of hemoglobin variants and thalassemia (compound heterozygotes).
- Genetic testing: These tests are used to investigate deletions and mutations in the alpha and beta globin-producing genes. Family studies can be done to evaluate carrier status and the types of mutations present in other family members. Genetic testing is not routinely done but can be used to help confirm hemoglobin variants, thalassemia, and to determine carrier status.
Hemoglobin Abnormalities Treatment
Hemoglobin variants are rarely cured. The main goals in treating hemoglobin variants include relieving pain, minimizing complications and organ damage, and preventing infections. Children with sickle cell disease should have regular childhood vaccinations and influenza vaccination.
Treatment during a sickle cell crisis may involve hospitalization and supportive care, including drinking lots of fluids and taking pain medication. Sometimes blood transfusions are needed to treat severe anemia. Antibiotics are needed if sickle crisis is triggered by infection (e.g., pneumonia).
Individuals with hemoglobin variants can minimize crises by avoiding or managing situations likely to trigger episodes. These situations include overexertion, dehydration, extreme temperatures, altitude changes, smoking, and stress.
Drugs that increase hemoglobin F are available. These drugs (e.g., hydroxyurea) relieve some symptoms, but research into safer and more effective therapy continues. L-glutamine has been approved for use to reduce severe complications of sickle cell anemia. Bone marrow or stem cells transplants from a family member with normal hemoglobin are known to cure sickle cell disease. These treatments are risky and has severe side effects, so they remain rare. Gene therapy to correct the mutated gene is beginning to show promise in small trials, but it will require much more research before it is considered for widespread use.
Low hemoglobin
Low hemoglobin levels may be due to:
- Anemia caused by red blood cells dying earlier than normal (hemolytic anemia)
- Anemia (various types)
- Bleeding from digestive tract or bladder, heavy menstrual periods
- Chronic kidney disease
- Bone marrow being unable to produce new red blood cells. This may be due to leukemia, other cancers, drug toxicity, radiation therapy, infection, or bone marrow disorders
- Poor nutrition (including low level of iron, folate, vitamin B12, or vitamin B6)
- Low level of iron, folate, vitamin B12, or vitamin B6
- Other chronic illness, such as rheumatoid arthritis
Anemia is a condition in which your blood has a lower than normal number of red blood cells 2.
- Anemia is diagnosed when a blood test shows a hemoglobin value of less than 13.5 gm/dl in a man or less than 12.0 gm/dl in a woman.
Anemia also can occur if your red blood cells don’t contain enough hemoglobin. Hemoglobin is an iron-rich protein that gives blood its red color. This protein helps red blood cells carry oxygen from the lungs to the rest of the body.
Anemia has three main causes 2:
- Blood loss,
- Lack of red blood cell production, or
- High rates of red blood cell destruction.
These causes might be the result of diseases, conditions, or other factors.
If you have anemia, your body doesn’t get enough oxygen-rich blood. As a result, you may appear pale, feel tired or weak. You also may have other symptoms, such as shortness of breath, dizziness, or headaches.
Severe or long-lasting anemia can damage your heart, brain, and other organs in your body. Very severe anemia may even cause death 2.
Many types of anemia can be mild, short term, and easily treated. You can even prevent some types with a healthy diet. Other types can be treated with dietary supplements.
However, certain types of anemia can be severe, long lasting, and even life threatening if not diagnosed and treated.
If you have signs or symptoms of anemia, see your doctor to find out whether you have the condition. Treatment will depend on the cause of the anemia and how severe it is.
There are many types of anemia with specific causes and traits.
Some of these include:
- Aplastic anemia
- Blood loss anemia
- Cooley’s anemia
- Diamond-Blackfan anemia
- Fanconi anemia
- Folate- or folic acid-deficiency anemia
- Hemolytic anemia
- Iron-deficiency anemia
- Pernicious anemia
- Sickle cell anemia
- Thalassemias; Cooley’s anemia is another name for beta thalassemia major
Common types of anemia
Iron-deficiency anemia is the most common type of anemia. It happens when you do not have enough iron in your body. Iron deficiency is usually due to blood loss but may occasionally be due to poor absorption of iron. Pregnancy and childbirth consume a great deal of iron and thus can result in pregnancy-related anemia. People who have had gastric bypass surgery for weight loss or other reasons may also be iron deficient due to poor absorption.
Vitamin-deficiency anemia may result from low levels of vitamin B12 or folate (folic acid), usually due to poor dietary intake. Pernicious anemia is a condition in which vitamin B12 cannot be absorbed in the gastrointestinal tract.
Anemia and Pregnancy – your body goes through significant changes when you become pregnant. The amount of blood in your body increases by about 20-30 percent, which increases the supply of iron and vitamins that the body needs to make hemoglobin. Many women lack the sufficient amount of iron needed for the second and third trimesters. When your body needs more iron than it has available, you can become anemic. Mild anemia is normal during pregnancy due to an increase in blood volume. More severe anemia, however, can put your baby at higher risk for anemia later in infancy. In addition, if you are significantly anemic during your first two trimesters, you are at greater risk for having a pre-term delivery or low-birth-weight baby. Being anemic also burdens the mother by increasing the risk of blood loss during labor and making it more difficult to fight infections.
Good nutrition is the best way to prevent anemia if you are pregnant or trying to become pregnant. Eating foods high in iron content (such as dark green leafy vegetables, red meat, fortified cereals, eggs, and peanuts) can help ensure that you maintain the supply of iron your body needs to function properly. Your obstetrician will also prescribe vitamins to ensure that you have enough iron and folic acid. Make sure you get at least 27 mg of iron each day. If you do become anemic during your pregnancy, it can usually be treated by taking iron supplements.
Ask your doctor about your risk for anemia and make sure you are tested at your first prenatal visit. You also may want to get tested four to six weeks after delivery. Depending on your condition, your doctor may refer you to a hematologist, a doctor who specializes in blood conditions.
Aplastic anemia is a rare bone marrow failure disorder in which the bone marrow stops making enough blood cells (red blood cells, white blood cells, and platelets). This occurs as a result of destruction or deficiency of blood-forming stem cells in your bone marrow, in particular when the body’s own immune system attacks the stem cells. However, the few blood cells the marrow does make are normal. Viral infections, ionizing radiation, and exposure to toxic chemicals or drugs can also result in aplastic anemia.
Hemolytic anemia occurs when red blood cells are broken up in the bloodstream or in the spleen. Hemolytic anemia may be due to mechanical causes (leaky heart valves or aneurysms), infections, autoimmune disorders, or congenital abnormalities in the red blood cell. Inherited abnormalities may affect the hemoglobin or the red blood cell structure or function. Examples of inherited hemolytic anemias include some types of thalassemia and low levels of enzymes such as glucose-6 phosphate dehydrogenase deficiency. The treatment will depend on the cause.
Sickle cell anemia is an inherited hemolytic anemia in which the hemoglobin protein is abnormal, causing the red blood cells to be rigid and clog the circulation because they are unable to flow through small blood vessels.
Anemia caused by other diseases – Some diseases can affect the body’s ability to make red blood cells. For example, some patients with kidney disease develop anemia because the kidneys are not making enough of the hormone erythropoietin to signal the bone marrow to make new or more red blood cells. Chemotherapy used to treat various cancers often impairs the body’s ability to make new red blood cells, and anemia often results from this treatment.
Low hemoglobin causes
The three main causes of anemia are:
- Blood loss. Excessive loss of blood from, for example, severe trauma or chronic bleeding from sites such as the digestive tract (e.g., ulcers, polyps, colon cancer), the bladder or uterus (in women, heavy menstrual bleeding, for example)
- Lack of red blood cell production.
- High rates of red blood cell destruction. Excessive destruction of red blood cells, for example, hemolytic anemia caused by autoimmunity or defects in the red blood cell itself; the defects could be hemoglobinopathy (e.g., sickle cell anemia), abnormalities in the red blood cell membrane (e.g., hereditary spherocytosis) or red blood cell enzyme (e.g., G6PD deficiency).
For some people, the condition is caused by more than one of these factors.
Blood Loss
Blood loss is the most common cause of anemia, especially iron-deficiency anemia. Blood loss can be short term or persist over time.
Heavy menstrual periods or bleeding in the digestive or urinary tract can cause blood loss. Surgery, trauma, or cancer also can cause blood loss.
If a lot of blood is lost, the body may lose enough red blood cells to cause anemia.
Lack of Red Blood Cell Production
Both acquired and inherited conditions and factors can prevent your body from making enough red blood cells. “Acquired” means you aren’t born with the condition, but you develop it. “Inherited” means your parents passed the gene for the condition on to you. For example, Thalassemia is a group of inherited blood disorders that can be passed from parents to their children and affect the amount and type of hemoglobin the body produces. People with thalassemia have one or more genetic mutations that they have inherited and that result in a decreased production of normal hemoglobin. When the body doesn’t make enough normal hemoglobin, red blood cells do not function properly and oxygen delivery suffers. This can lead to anemia with signs and symptoms that can range from mild to severe, depending on the type of thalassemia that a person has. Examples of signs and symptoms include weakness, fatigue, and pale skin (pallor). With thalassemias, mutations in one or more of the globin genes cause a reduction in the amount of the particular globin chain produced. This can upset the balance of alpha to beta chains, resulting in unusual forms of hemoglobin or an increase in the amount of normally minor hemoglobin, such as Hb A2 or Hb F. The thalassemias are usually classified by the type of globin chain whose synthesis is decreased. For example, the most common alpha chain-related condition is called alpha thalassemia. The severity of this condition depends on the number of genes affected.
Acquired conditions and factors that can lead to anemia include poor diet, abnormal hormone levels, some chronic (ongoing) diseases, and pregnancy.
Aplastic anemia also can prevent your body from making enough red blood cells. This condition can be acquired or inherited.
Nutritional deficiencies
A diet that lacks iron, folic acid (folate), or vitamin B12 can prevent your body from making enough red blood cells. Your body also needs small amounts of vitamin C, riboflavin, and copper to make red blood cells.
Conditions that make it hard for your body to absorb nutrients also can prevent your body from making enough red blood cells.
Hormones
Your body needs the hormone erythropoietin to make red blood cells. This hormone stimulates the bone marrow to make these cells. A low level of this hormone can lead to anemia.
Diseases and Disease Treatments
Chronic diseases, like kidney disease and cancer, can make it hard for your body to make enough red blood cells.
Some cancer treatments may damage the bone marrow or damage the red blood cells’ ability to carry oxygen. If the bone marrow is damaged, it can’t make red blood cells fast enough to replace the ones that die or are destroyed.
People who have HIV/AIDS may develop anemia due to infections or medicines used to treat their diseases.
Pregnancy
Anemia can occur during pregnancy due to low levels of iron and folic acid and changes in the blood.
During the first 6 months of pregnancy, the fluid portion of a woman’s blood (the plasma) increases faster than the number of red blood cells. This dilutes the blood and can lead to anemia.
Aplastic Anemia
Some infants are born without the ability to make enough red blood cells. This condition is called aplastic anemia. Infants and children who have aplastic anemia often need blood transfusions to increase the number of red blood cells in their blood.
Acquired conditions or factors, such as certain medicines, toxins, and infectious diseases, also can cause aplastic anemia.
High Rates of Red Blood Cell Destruction
Both acquired and inherited conditions and factors can cause your body to destroy too many red blood cells. One example of an acquired condition is an enlarged or diseased spleen.
The spleen is an organ that removes wornout red blood cells from the body. If the spleen is enlarged or diseased, it may remove more red blood cells than normal, causing anemia.
Examples of inherited conditions that can cause your body to destroy too many red blood cells include sickle cell anemia, thalassemias, and lack of certain enzymes. These conditions create defects in the red blood cells that cause them to die faster than healthy red blood cells.
Hemolytic anemia is another example of a condition in which your body destroys too many red blood cells. Inherited or acquired conditions or factors can cause hemolytic anemia. Examples include immune disorders, infections, certain medicines, or reactions to blood transfusions.
Who is at Risk for Anemia ?
Anemia is a common condition. It occurs in all age, racial, and ethnic groups. Both men and women can have anemia. However, women of childbearing age are at higher risk for the condition because of blood loss from menstruation.
Many people are at risk for anemia because of poor diet, intestinal disorders, chronic diseases, infections, and other conditions. Women who are menstruating or pregnant and people with chronic medical conditions are most at risk for this disease. The risk of anemia increases as people grow older.
Anemia can develop during pregnancy due to low levels of iron and folic acid (folate) and changes in the blood. During the first 6 months of pregnancy, the fluid portion of a woman’s blood (the plasma) increases faster than the number of red blood cells. This dilutes the blood and can lead to anemia.
During the first year of life, some babies are at risk for anemia because of iron deficiency. At-risk infants include those who are born too early and infants who are fed breast milk only or formula that isn’t fortified with iron. These infants can develop iron deficiency by 6 months of age.
Infants between 1 and 2 years of age also are at risk for anemia. They may not get enough iron in their diets, especially if they drink a lot of cow’s milk. Cow’s milk is low in the iron needed for growth.
Drinking too much cow’s milk may keep an infant or toddler from eating enough iron-rich foods or absorbing enough iron from foods.
Older adults also are at increased risk for anemia. Researchers continue to study how the condition affects older adults. Many of these people have other medical conditions as well.
Major Risk Factors
Factors that raise your risk for anemia include:
- A diet that is low in iron, vitamins, or minerals
- Blood loss from surgery or an injury
- Long-term or serious illnesses, such as kidney disease, cancer, diabetes, rheumatoid arthritis, HIV/AIDS, inflammatory bowel disease (including Crohn’s disease), liver disease, heart failure, and thyroid disease
- Long-term infections
- A family history of inherited anemia, such as sickle cell anemia or thalassemia
If you have any of the following chronic conditions, you might be at greater risk for developing anemia:
- Rheumatoid arthritis or other autoimmune disease
- Kidney disease
- Cancer
- Liver disease
- Thyroid disease
- Inflammatory bowel disease (Crohn disease or ulcerative colitis)
Is Anemia Preventable?
While many types of anemia cannot be prevented, eating healthy foods can help you avoid both iron-and vitamin-deficiency anemia. Foods to include in your diet include those with high levels of iron (beef, dark green leafy vegetables, dried fruits, and nuts), vitamin B-12 (meat and dairy), and folic acid (citrus juices, dark green leafy vegetables, legumes, and fortified cereals). A daily multivitamin will also help prevent nutritional anemias; however, older adults should not take iron supplementsfor iron-deficiencyanemia unless instructed by their physicians.
Anemia Prevention
Eat a vitamin-rich diet
Many types of anemia can’t be prevented. But iron deficiency anemia and vitamin deficiency anemias can be avoided by having a diet that includes a variety of vitamins and nutrients, including:
- Iron. Iron-rich foods include beef and other meats, beans, lentils, iron-fortified cereals, dark green leafy vegetables, and dried fruit.
- Folate. This nutrient, and its synthetic form folic acid, can be found in fruits and fruit juices, dark green leafy vegetables, green peas, kidney beans, peanuts, and enriched grain products, such as bread, cereal, pasta and rice.
- Vitamin B-12. Foods rich in vitamin B-12 include meat, dairy products, and fortified cereal and soy products.
- Vitamin C. Foods rich in vitamin C include citrus fruits and juices, peppers, broccoli, tomatoes, melons and strawberries. These items help increase iron absorption.
Consider a multivitamin
If you’re concerned about getting enough vitamins from the food you eat, ask your doctor whether a multivitamin may be right for you.
Consider genetic counseling
If you have a family history of an inherited anemia, such as sickle cell anemia or thalassemia, talk to your doctor and possibly a genetic counselor about your risk and what risks you may pass on to your children.
Prevent malaria
Anemia can be a complication of malaria. If you plan on traveling to a place where malaria is common, talk with your doctor beforehand about taking preventive drugs. In areas where malaria is common, prevention involves reducing exposure to mosquitoes, for example, by using bed nets treated with insecticide.
Risk factors for anemia
These factors place you at increased risk of anemia:
- A diet lacking in certain vitamins. Having a diet that is consistently low in iron, vitamin B-12 and folate increases your risk of anemia.
- Intestinal disorders. Having an intestinal disorder that affects the absorption of nutrients in your small intestine — such as Crohn’s disease and celiac disease — puts you at risk of anemia.
- Menstruation. In general, women who haven’t experienced menopause have a greater risk of iron deficiency anemia than do men and postmenopausal women. That’s because menstruation causes the loss of red blood cells.
- Pregnancy. If you’re pregnant and aren’t taking a multivitamin with folic acid, you’re at an increased risk of anemia.
- Chronic conditions. If you have cancer, kidney failure or another chronic condition, you may be at risk of anemia of chronic disease. These conditions can lead to a shortage of red blood cells. Slow, chronic blood loss from an ulcer or other source within your body can deplete your body’s store of iron, leading to iron deficiency anemia.
- Family history. If your family has a history of an inherited anemia, such as sickle cell anemia, you also may be at increased risk of the condition.
- Other factors. A history of certain infections, blood diseases and autoimmune disorders, alcoholism, exposure to toxic chemicals, and the use of some medications can affect red blood cell production and lead to anemia.
- Age. People over age 65 are at increased risk of anemia.
Complications of anemia
Left untreated, anemia can cause many health problems, such as:
- Severe fatigue. When anemia is severe enough, you may be so tired that you can’t complete everyday tasks.
- Pregnancy complications. Pregnant women with folate deficiency anemia may be more likely to experience complications, such as premature birth.
- Heart problems. Anemia can lead to a rapid or irregular heartbeat (arrhythmia). When you’re anemic your heart must pump more blood to compensate for the lack of oxygen in the blood. This can lead to an enlarged heart or heart failure.
- Death. Some inherited anemias, such as sickle cell anemia, can be serious and lead to life-threatening complications. Losing a lot of blood quickly results in acute, severe anemia and can be fatal.
Low hemoglobin symptoms
When you have anemia, your body lacks oxygen, so you may experience one or more of the following symptoms:
- Weakness or fatigue
- Lack of energy
- Fainting
- Paleness (pallor)
- Shortness of breath
- Dizziness
- Fast or irregular heartbeat
- Pounding or “whooshing” in your ears
- Headache
- Cold hands or feet
- Pale or yellow skin
- Chest pain
The signs and symptoms of anemia can easily be overlooked. In fact, many people do not even realize that they have anemia until it is identified in a blood test.
How to increase hemoglobin
The treatment for anemia depends on what causes it. Talk with your doctor if you believe you may be at risk for anemia. Your doctor will determine your best course of treatment and, depending on your condition, may refer you to a hematologist, a doctor who specializes in blood disorders.
Iron-deficiency anemia is almost always due to blood loss. If you have iron-deficiency anemia, your doctor may order tests to determine if you are losing blood from your stomach or bowels.
- Iron deficiency anemia. Treatment for this form of anemia usually involves taking iron supplements and making changes to your diet. If the underlying cause of iron deficiency is loss of blood — other than from menstruation — the source of the bleeding must be located and stopped. This may involve surgery.
Vitamin deficiency anemias. Nutritional anemias, such as folate or B-12 deficiency, may result from poor diet or from an inability to absorb vitamins in the gastrointestinal tract. Treatment for folic acid and B-12 deficiency involves dietary supplements and increasing these nutrients in your diet. Treatment varies from changing your diet to taking dietary supplements.
- If your digestive system has trouble absorbing vitamin B-12 from the food you eat, you may need vitamin B-12 shots. At first, you may receive the shots every other day. Eventually, you’ll need shots just once a month, which may continue for life, depending on your situation.
Anemia of chronic disease. There’s no specific treatment for this type of anemia. Doctors focus on treating the underlying disease. Treatment of the underlying disease will often improve the anemia. Under some circumstances, such as chronic kidney disease, your doctor may prescribe medication such as erythropoietin injections to stimulate your bone marrow to produce more red blood cells. If symptoms become severe, a blood transfusion or injections of synthetic erythropoietin, a hormone normally produced by your kidneys, may help stimulate red blood cell production and ease fatigue.
Aplastic anemia. Aplastic anemia occurs if your bone marrow stops producing red blood cells. Aplastic anemia may be due to primary bone marrow failure, myelodysplasia (a condition in which the bone marrow produces abnormal red blood cells that do not mature properly), or occasionally as a side effect of some medications. If you appear to have a form of aplastic anemia, your doctor may refer you to a hematologist for a bone marrow biopsy to determine the cause of the anemia. Anemias associated with bone marrow disease. Treatment of these various diseases can include medication, chemotherapy or bone marrow transplantation. Treatment for this anemia may include blood transfusions to boost levels of red blood cells. You may need a bone marrow transplant if your bone marrow is diseased and can’t make healthy blood cells.
Hemolytic anemias. Hemolytic anemia occurs when red blood cells are destroyed in the blood stream. This may be due to mechanical factors (a leaky heart valve or aneurysm), infection, or an autoimmune disease. The cause can often be identified by special blood tests and by looking at the red blood cells under a microscope. Managing hemolytic anemias includes avoiding suspect medications, treating related infections and taking drugs that suppress your immune system, which may be attacking your red blood cells. The treatment will depend upon the cause and may include referral to a heart or vascular specialist, antibiotics, or drugs that suppress the immune system.
Depending on the severity of your anemia, a blood transfusion or plasmapheresis may be necessary. Plasmapheresis is a type of blood-filtering procedure. In certain cases, removal of the spleen can be helpful.
Sickle cell anemia. Treatment for this anemia may include the administration of oxygen, pain-relieving drugs, and oral and intravenous fluids to reduce pain and prevent complications. Doctors also may recommend blood transfusions, folic acid supplements and antibiotics.
A bone marrow transplant may be an effective treatment in some circumstances. A cancer drug called hydroxyurea (Droxia, Hydrea) also is used to treat sickle cell anemia.
Thalassemia. This anemia may be treated with blood transfusions, folic acid supplements, medication, removal of the spleen (splenectomy), or a blood and bone marrow stem cell transplant.
High hemoglobin levels
Higher than normal hemoglobin level is most often caused by low oxygen levels in the blood (hypoxia), present over a long period of time. Common reasons include:
- Certain birth defects of the heart that are present at birth (congenital heart disease)
- Failure of the right side of the heart (cor pulmonale)
- Severe chronic obstructive pulmonary disease (COPD)
- Scarring or thickening of the lungs (pulmonary fibrosis) and other severe lung disorders
Other reasons for high hemoglobin level includes:
- A rare bone marrow disease that leads to an abnormal increase in the number of blood cells (polycythemia vera)
- The body having too little water and fluids (dehydration)
High hemoglobin with a high red blood cell count and high hematocrit indicates polycythemia. Some causes include:
- Lung (pulmonary) disease—if someone is unable to breathe in and absorb sufficient oxygen, the body tries to compensate by producing more red blood cells.
- Congenital heart disease—in some forms, there is an abnormal connection between the two sides of the heart, leading to reduced oxygen levels in the blood. The body tries to compensate by producing more red blood cells.
- Kidney tumors that produce excess erythropoietin
- Smoking—heavy smokers have higher hemoglobin levels than nonsmokers.
- Genetic causes (altered oxygen sensing, abnormality in hemoglobin oxygen release)
- Living at high altitudes (a compensation for decreased oxygen in the air)
- Dehydration—as the volume of fluid in the blood drops, the hemoglobin artificially rises.
- Polycythemia vera—a rare disease in which the body produces excess red blood cells inappropriately
Hemoglobin a1c
Hemoglobin A1c, also called A1c or glycosylated hemoglobin, is hemoglobin with glucose attached. The hemoglobin A1c test evaluates the average amount of glucose in your blood over the last 2 to 3 months by measuring the percentage of glycated (glycosylated) hemoglobin.
Hemoglobin is an oxygen-transporting protein found inside red blood cells (RBCs). There are several types of normal hemoglobin, but the predominant form – about 95-98% – is hemoglobin A. As glucose circulates in the blood, some of it spontaneously binds to hemoglobin A. When glucose molecules combine with hemoglobin A in the bloodstream, the resulting molecule is called hemoglobin A1c.
The more glucose in the bloodstream over a given amount of time, the more hemoglobin A molecules become hemoglobin A1c molecules. And of course, with diabetes, you want to keep that level of glucose as normal as possible. The proportion of hemoglobin A1c molecules in the blood is measured by an A1c test—that’s why it’s reported as a percentage. An hemoglobin A1c of 7 means that 7 percent of the hemoglobin has glucose stuck to it.
The higher the level of glucose in the blood, the more glycated hemoglobin is formed. Once the glucose binds to the hemoglobin, it remains there for the life of the red blood cell – normally about 120 days. The predominant form of glycated hemoglobin is referred to as hemoglobin A1c. Hemoglobin A1c is produced on a daily basis and slowly cleared from the blood as older red blood cells die and younger red blood cells (with non-glycated hemoglobin) take their place.
Hemoglobin A1c test may be used to screen for and diagnose diabetes or risk of developing diabetes. Standards of medical care in diabetes from the American Diabetes Association state that diabetes may be diagnosed based on hemoglobin A1c criteria or plasma glucose criteria, either the fasting plasma glucose (FPG) or the 2-hour plasma glucose value after a 75-g oral glucose tolerance test (OGTT).
Hemoglobin A1c test is also used to monitor treatment for someone who has been diagnosed with diabetes. It helps to evaluate how well the person’s glucose levels have been controlled by treatment over time. For monitoring purposes, a hemoglobin A1c of less than 7% indicates good glucose control and a lower risk of diabetic complications for the majority of diabetics.
However, the American Diabetes Association and the European Association for the Study of Diabetes recommend that the management of glucose control in type 2 diabetes be more “patient-centered.” Data from recent studies have shown that low blood sugar (hypoglycemia) can cause complications and that people with risk of severe hypoglycemia, disease duration, underlying health conditions, established vascular complications, and a limited life expectancy do not necessarily benefit from having a stringent goal of less than 7% for their hemoglobin A1c. It is recommend that people work closely with their healthcare provider to select a goal that reflects each person’s individual health status and that balances risks and benefits.
When is hemoglobin A1c ordered?
Screening and diagnosis
A1c may be ordered as part of a health checkup or when someone is suspected of having diabetes because of classical signs or symptoms of increased blood glucose levels (hyperglycemia) such as:
- Increased thirst and drinking fluids
- Increased urination
- Increased appetite
- Fatigue
- Blurred vision
- Slow-healing infections
The hemoglobin A1c test may also be considered in adults who are overweight with the following additional risk factors:
- Physical inactivity
- First-degree relative (sibling or parent) with diabetes
- High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander)
- High blood pressure (hypertension)
- Abnormal lipid profile (low HDL cholesterol and/or high triglycerides)
- Women with polycystic ovary syndrome
- History of cardiovascular diseases
- Other clinical conditions associated with insulin resistance
The American Diabetes Association recommends to begin A1c testing at age 45 for overweight or obese people; if the result is normal, the testing should be repeated at a minimum of 3-year intervals, with consideration of more frequent testing depending on initial results and risk status.
People who are not diagnosed with diabetes but are determined to be at increased risk for diabetes (prediabetes) should have hemoglobin A1c testing yearly.
Monitoring
Depending on the type of diabetes that a person has, how well that person’s diabetes is controlled, and on the healthcare provider’s recommendations, the A1c test may be measured 2 to 4 times each year. The American Diabetes Association recommends hemoglobin A1c testing for diabetics at least twice a year if they are meeting treatment goals and under stable glycemic control. When someone is first diagnosed with diabetes or if control is not good, hemoglobin A1c may be ordered quarterly.
How is hemoglobin A1c used?
Screening and diagnosis
The hemoglobin A1c test may be used to screen for and diagnose diabetes and prediabetes in adults.
The hemoglobin A1c test, however, should not be used for screening for cystic fibrosis-related diabetes, for diagnosis of gestational diabetes in pregnant women, or for diagnosis of diabetes in children and adolescence, people who have had recent severe bleeding or blood transfusions, those with chronic kidney or liver disease, or people with blood disorders such as iron-deficiency anemia, vitamin B12 deficiency anemia, and some hemoglobin variants (e.g., patients with sickle cell disease or thalassemia). In these cases, a fasting plasma glucose or oral glucose tolerance test should be used for screening or diagnosing diabetes.
Only hemoglobin A1c tests that have been referenced to an accepted laboratory method (National Glycohemoglobin Standardization Program certified) should be used for diagnostic or screening purposes. Currently, point-of-care tests, such as those that may be used at a doctor’s office or a patient’s bedside, are not accurate enough for use in diagnosis but can be used to monitor treatment (lifestyle and drug therapies).
Monitoring
The hemoglobin A1c test is also used to monitor the glucose control of diabetics over time. The goal of those with diabetes is to keep their blood glucose levels as close to normal as possible. This helps to minimize the complications caused by chronically elevated glucose levels, such as progressive damage to body organs like the kidneys, eyes, cardiovascular system, and nerves. The A1c test result gives a picture of the average amount of glucose in the blood over the last 2-3 months. This can help diabetics and their healthcare providers know if the measures that are being taken to control their diabetes are successful or need to be adjusted.
Hemoglobin A1c is frequently used to help newly diagnosed diabetics determine how elevated their uncontrolled blood glucose levels have been over the last 2-3 months. The test may be ordered several times while control is being achieved, and then at least twice a year to verify that good control is being maintained.
What Hemoglobin A1c test result mean?
In screening and diagnosis, some results that may be seen include:
- Normal (no diabetes): Less than 5.7%. A nondiabetic person will have an hemoglobin A1c result less than 5.7% (39 mmol/mol).
- Diabetes: hemoglobin A1c level is 6.5% (48 mmol/mol) or higher.
- Pre-diabetes (increased risk of developing diabetes in the future): 5.7% to 6.4% hemoglobin A1c (39-46 mmol/mol)
For monitoring glucose control, hemoglobin A1c is currently reported as a percentage and, for most diabetics, it is recommended that they aim to keep their hemoglobin A1c below 7%. The closer diabetics can keep their A1c to the American Diabetes Association’s therapeutic goal of less than 7% without experiencing excessive low blood glucose (hypoglycemia), the better their diabetes is in control. As the hemoglobin A1c increases, so does the risk of complications.
An individual with type 2 diabetes, however, may have an A1c goal selected by the person and his or her healthcare provider. The goal may depend on several factors, such as length of time since diagnosis, the presence of other diseases as well as diabetes complications (e.g., vision impairment or loss, kidney damage), risk of complications from hypoglycemia, limited life expectancy, and whether or not the person has a support system and healthcare resources readily available.
For example, a person with heart disease who has lived with type 2 diabetes for many years without diabetic complications may have a higher hemoglobin A1c target (e.g., 7.5%-8.0%) set by their healthcare provider, while someone who is otherwise healthy and just diagnosed may have a lower target (e.g., 6.0%-6.5%) as long as low blood sugar is not a significant risk.
The hemoglobin A1c test report also may include the result expressed in SI units (mmol/mol) and an estimated Average Glucose (eAG), which is a calculated result based on the hemoglobin A1c levels.
The purpose of reporting estimated Average Glucose (eAG) is to help a person relate hemoglobin A1c results to everyday glucose monitoring levels and to laboratory glucose tests. The formula for eAG converts percentage A1c to units of mg/dL or mmol/L. By making Hemoglobin A1c easier to equate with day-to-day blood glucose readings might just promote more blood glucose testing and improve glucose control, many experts believe.
| Here’s how the Hemoglobin A1c relates to the eAG | |
| Hemoglobin A1c (%) | eAG (mg/dl) |
| 5 | 97 |
| 5.5 | 111 |
| 6 | 126 |
| 6.5 | 140 |
| 7 | 154 |
| 7.5 | 169 |
| 8 | 183 |
| 8.5 | 197 |
| 9 | 212 |
| 9.5 | 226 |
| 10 | 240 |
| 10.5 | 255 |
| 11 | 269 |
| 11.5 | 283 |
| 12 | 298 |
It should be noted that the eAG is still an evaluation of a person’s glucose over the last couple of months. It will not match up exactly to any one daily glucose test result.
How is estimated Average Glucose (eAG) calculated?
The A1c-Derived Average Glucose formula that is used to calculate the eAG from your hemoglobin A1c (A1c) result is:
- 28.7 X A1c (%) – 46.7 = eAG (milligrams/deciliter, mg/dL)
An example of this is an A1c of 6%. The calculation for this would be:
- 28.7 X 6 – 46.7 = 126 mg/dL
for an estimated average glucose of 126 mg/dL.
What this means is that for every one percent that your A1c goes up, it is equivalent to your average glucose going up by about 29 mg/dL.
What abnormal hemoglobin A1c results mean?
An abnormal result means that you have had a high blood sugar level over a period of weeks to months.
If your hemoglobin A1c is above 6.5% and you do not already have diabetes, you may be diagnosed with diabetes.
If your hemoglobin A1c level is above 7% and you have diabetes, it often means that your blood sugar is not well controlled. You and your provider should determine your target hemoglobin A1c.
The higher your hemoglobin A1c, the higher the risk that you will develop problems such as:
- Eye disease
- Heart disease
- Kidney disease
- Nerve damage
- Stroke
If your hemoglobin A1c stays high, talk to your provider about how to best manage your blood sugar.
Is there anything else I should know about the Hemoglobin A1c test?
The hemoglobin A1c test will not reflect temporary, acute blood glucose increases or decreases, or good control that has been achieved in the last 3-4 weeks. The glucose swings of someone who has “brittle” diabetes will also not be reflected in the Hemoglobin A1c.
If an individual has a hemoglobin variant, such as sickle cell hemoglobin (hemoglobin S), that person will have a decreased amount of hemoglobin A. This may limit the usefulness of the hemoglobin A1c test in diagnosing and/or monitoring this person’s diabetes, depending on the method used.
If a person has anemia, hemolysis, or heavy bleeding, hemoglobin A1c test results may be falsely low. If someone is iron-deficient, the hemoglobin A1c level may be increased.
If a person receives erythropoietin therapy or has had a recent blood transfusion, the hemoglobin A1c may be inaccurate and may not accurately reflect glucose control for 2-3 months.
Why are my hemoglobin A1c and blood glucose different?
Beyond the difference in units used to report them, the hemoglobin A1c represents an average over time while your blood glucose reflects what is happening in your body now. Your blood glucose will capture the changes in your blood sugar that occur on a daily basis, the highs and the lows. Each blood glucose is a snapshot and each is different. The hemoglobin A1c is an indication that “in general” your glucose has been elevated over the last few months or “in general” it has been normal. It is inherently not as sensitive as a blood glucose. However, if your day-to-day glucose control is stable (good or bad), then both the A1c and blood glucose should reflect this. It is important to remember the time lag associated with the hemoglobin A1c. Good glucose control for the past 2-3 weeks will not significantly affect the A1c result for several more weeks.
In addition to this, it is also important to remember that glycated hemoglobin and blood glucose are two different but related things. For unknown reasons, some peoples’ hemoglobin A1c may not accurately reflect their average blood glucose.
Is hemoglobin A1c reported the same way around the world?
For monitoring purposes, the way that the hemoglobin A1c is reported is in the process of changing. Traditionally, in the United States, the hemoglobin A1c has been reported as a percentage, and the American Diabetes Association has recommended that people with diabetes strive to keep their hemoglobin A1c below 7%. While this is still generally true, more than a decade of national and international efforts to improve and standardize the hemoglobin A1c test and its reporting led to the release of a consensus statement in 2007 (and an update in 2010) by the American Diabetes Association, the European Association for the Study of Diabetes, the International Federation of Clinical Chemistry and Laboratory Medicine, the International Society for Pediatric and Adolescent Diabetes, and the International Diabetes Federation. These joint statements and the completion of a study called ADAG (A1c-Derived Average Glucose) that further examined the relationship between blood glucose concentrations and A1c led to a recommendation that A1c be reported worldwide in two ways:
- As a percentage (based upon National Glycohemoglobin Standardization Program (NGSP) derived units) and
- In SI (Système International) units (mmol/mol)
An estimated Average Glucose (eAG) based upon a formula developed from the ADAG study with either mg/dL or mmol/l as units that continue to be recognized by the American Diabetes Association and the American Association for Clinical Chemistry in the 2015 ADA Diabetes Care Position Statement may also be reported.
What this means for diabetics and health practitioners in the U.S. is that hemoglobin A1c results will be reported as a percentage but may in addition to this be reported as mmol/mol and, in some cases, also as an eAG with the same type of units (mg/dL) as are reported by home glucose monitors and laboratory results.
How is the sample collected for hemoglobin A1c testing?
A blood sample is obtained by inserting a needle into a vein in the arm or a drop of blood is taken from a finger by pricking it with a small, pointed lancet.
A blood sample is needed. Two methods are available:
- Blood drawn from a vein. This is done at a lab.
- Finger stick. This can be done in your health care provider’s office. Or you may be prescribed a kit that you can use at home.
Is hemoglobin A1c test preparation needed to ensure the quality of the sample?
No special preparation is needed. The food you have recently eaten does not affect the A1C test, so you do not need to fast to prepare for this blood test.
Is there a home test for hemoglobin A1c?
Yes. If you have already been diagnosed with diabetes, a home test may be used to help monitor your glucose control over time. However, a home test (point-of-care test) is not recommended for screening or diagnosing the disease.
- Thom CS, Dickson CF, Gell DA, Weiss MJ. Hemoglobin Variants: Biochemical Properties and Clinical Correlates. Cold Spring Harbor Perspectives in Medicine. 2013;3(3):a011858. doi:10.1101/cshperspect.a011858. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3579210/[↩]
- Anemia. National Heart, Lung and Blood Institute. https://www.nhlbi.nih.gov/health/health-topics/topics/anemia[↩][↩][↩]





{kind=link}