
Contents
What is histoplasmosis
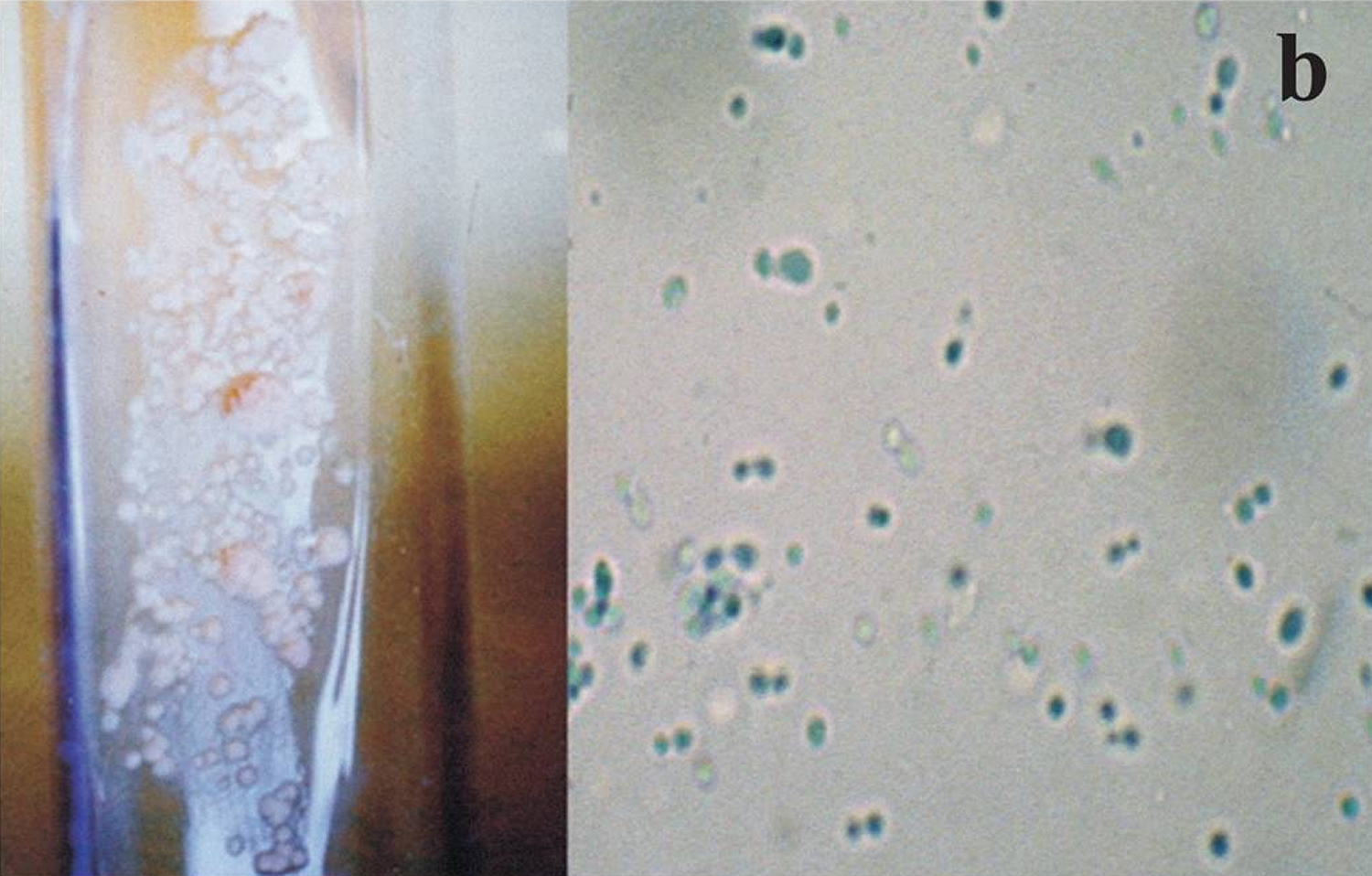
Histoplasmosis is an infection caused by a fungus called Histoplasma capsulatum (a dimorphic fungus). There are two varieties of the pathogen, Histoplasma capsulatum var. capsulatum and Histoplasma capsulatum var. duboisii that cause disease in humans 1. Histoplasma capsulatum var. capsulatum is the causative agent of classical histoplasmosis 2. Less commom, Histoplasma capsulatum var. duboisii is the etiologic cause for African histoplasmosis 3. The Histoplasma capsulatum fungus grows as a mold in the soil and when its microconidia are inhaled, causes infection and grows as a yeast in the host tissues (see Figures 1 and 2).
Histoplasmosis mainly affects the lungs with most patients often showing minimal (self-limiting flu-like illness) or no symptoms. Histoplasma capsulatum fungus lives in the environment, particularly in soil that contains large amounts of bird and bat droppings. The fungus has been found in the droppings of domestic birds, such as chickens, starlings and other birds that often nest around the house. The histoplasmosis fungus thrives in damp soil that’s rich in organic material, especially the droppings from birds and bats. For that reason, it’s particularly common in chicken and pigeon coops, old barns, caves and parks.
An estimated 40 million people in the United States have been infected with Histoplasma capsulatum, with 500,000 new cases occurring each year 4.
Even if you’ve had histoplasmosis in the past, you can still get the infection again. However, if you contract histoplasmosis again, the illness will likely be milder than the initial infection.
Figure 1. Histoplasma capsulatum fungus – mold form (culture and microscopy)
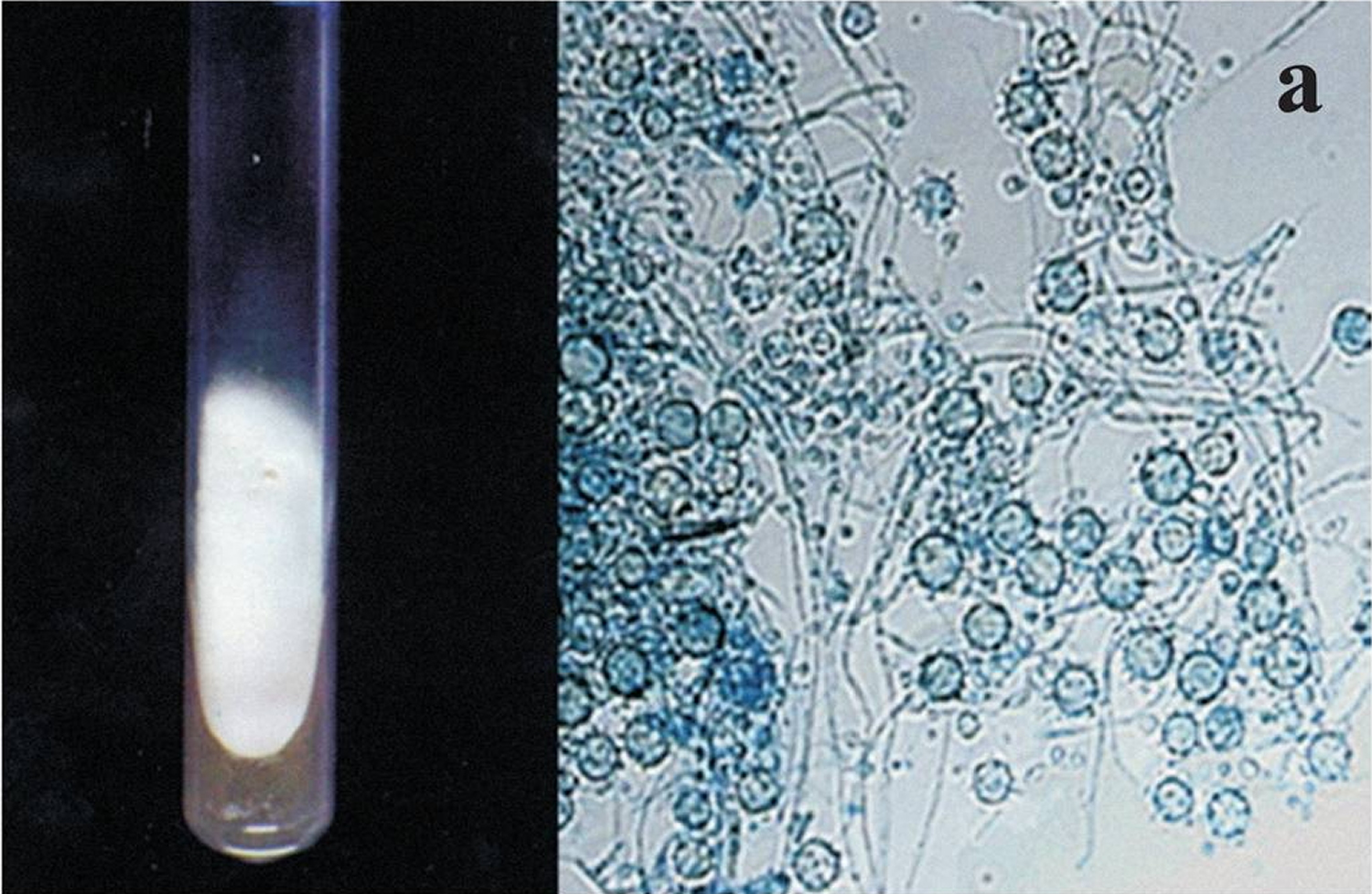
Figure 2. Histoplasma capsulatum fungus – yeast form at 37° C (98.6 °F) culture and microscopy
Histoplasmosis is a common disease throughout the world, occurring in temperate and tropical climates such as parts of the USA, Africa and Australasia. In the United States, Histoplasma mainly lives in the central and eastern states, the region often referred to as the “Histo Belt”, includes Arkansas, Kentucky, Tennessee, West Virginia as well as other areas of southeastern and central US, especially areas around the Ohio and Mississippi River valleys 5. The Histoplasma capsulatum fungus also lives in parts of Central and South America 6, Africa 7, Asia 8, and Australia 9. In certain areas up to 90% of the adult population are infected with histoplasmosis 10, 11.
People can get histoplasmosis after breathing in the microscopic fungal spores from the air, often after participating in activities that disturb the soil. Although most people who breathe in the spores don’t get sick, those who do may have a fever, cough, and fatigue. Many people who get histoplasmosis will get better on their own without medication, but in some people, such as those who have weakened immune systems, the infection can become severe.
Humans and animals such as dogs, rats and cats may become infected. The disease is not transmitted from human-to-human or animal-to-human.
Infants, young children, and older persons, particularly those with chronic lung disease are at increased risk for severe disease. Sometimes the disease may spread from the lungs to other organs (disseminated histoplasmosis). This is more commonly found in people with immunodeficiency such as those with cancer or acquired immune deficiency syndrome (AIDS). Up to 25% of people infected with human immunodeficiency virus (HIV) will develop disseminated histoplasmosis, with considerable morbidity and mortality 10.
Where does Histoplasma live?
Histoplasma, the fungus that causes histoplasmosis, lives throughout the world, but it’s most common in North America and Central America. In the United States, Histoplasma mainly lives in soil in the central and eastern states, particularly areas around the Ohio and Mississippi River Valleys 5, but it can likely live in other parts of the U.S. as well 12. The fungus also lives in parts of Central and South America 6, Africa 7, Asia 8, and Australia 9.
Histoplasma grows best in soil that contains bird or bat droppings. Bats can get histoplasmosis and spread the fungus in their droppings 13.
This map shows the approximate areas (called “endemic areas”) where Histoplasma is known to live or is suspected to live in the U.S. Much of what’s known about where the fungus lives in the U.S. is based on studies performed in the late 1940s and early 1950s. Infection outside endemic areas and atypical presentations represent a diagnostic challenge.
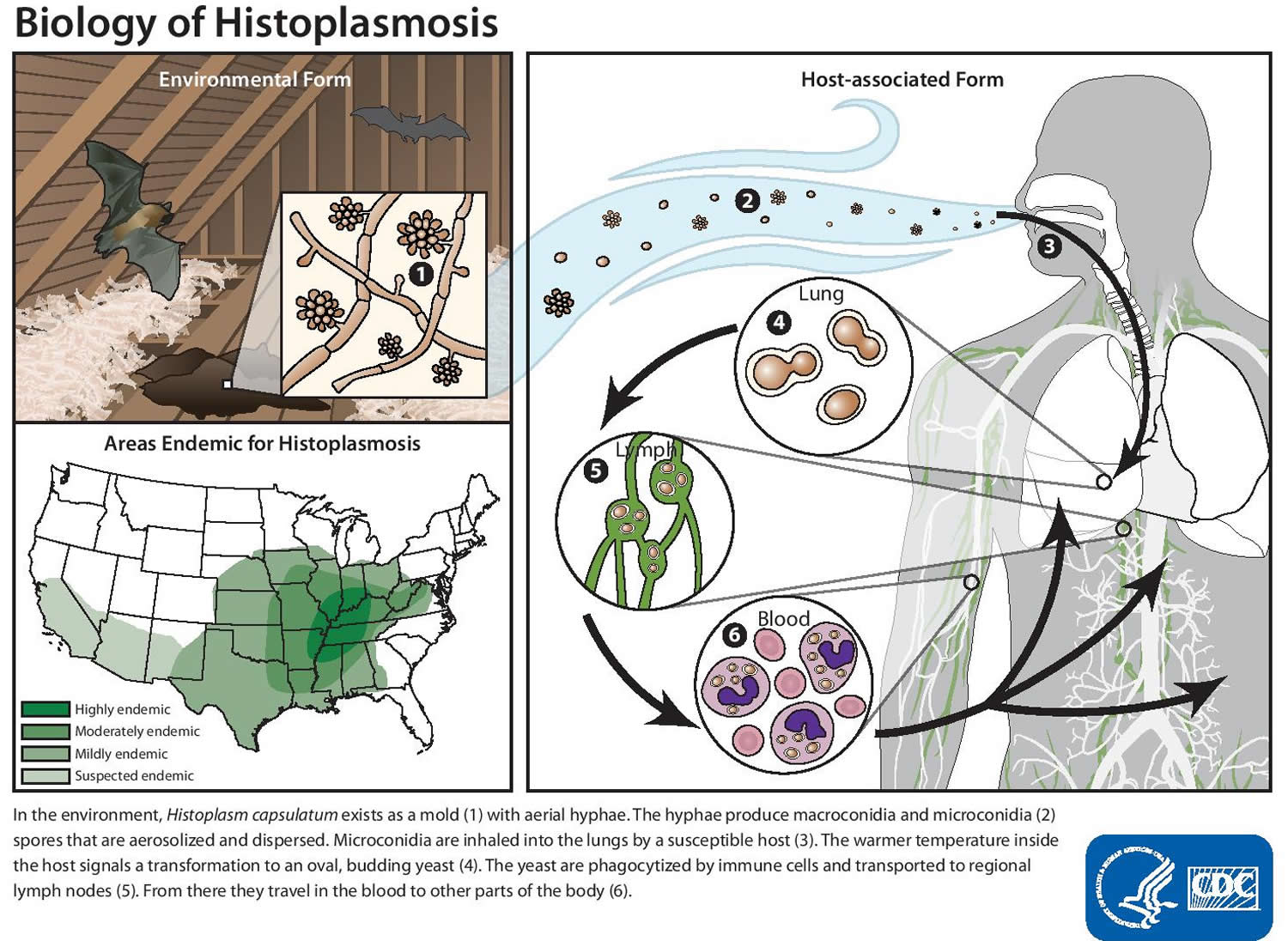
Figure 3. Histoplasmosis life cycle
Risk factors for developing histoplasmosis
The chances of developing histoplasmosis symptoms increase with the number of spores you inhale. Professions with a higher likelihood of spore exposure include:
- Farmers
- Pest control workers
- Poultry keepers
- Construction workers
- Roofers
- Landscapers and gardeners
- Cave explorers
Who gets histoplasmosis?
Anyone can get histoplasmosis if they’ve been in an area where Histoplasma lives in the environment. Histoplasmosis is often associated with activities that disturb soil, particularly soil that contains bird or bat droppings. Certain groups of people are at higher risk for developing the severe forms of histoplasmosis:
People who have weakened immune systems, for example, people who:
- Have HIV/AIDS 14
- Have had an organ transplant 15
- Are taking medications such as corticosteroids or TNF-inhibitors 16
- Infants 17
- Adults aged 55 and older 18
Is histoplasmosis contagious?
No. Histoplasmosis can’t spread from the lungs between people or between people and animals. However, in extremely rare cases, the infection can be passed through an organ transplant with an infected organ 19.
I’m worried that Histoplasma is in the soil or in bird/bat droppings near my home. Can someone test the environment to find out if the fungus is there?
No, in this situation, testing the environment for Histoplasma isn’t likely to be useful because the fungus is thought to be common in the environment in certain areas. A soil sample that tests positive for Histoplasma doesn’t necessarily mean that it’s a source of infection, and a sample that tests negative doesn’t necessarily mean that the fungus isn’t there. Also, there are no commercially-available tests to detect Histoplasma in the environment. Testing environmental samples for Histoplasma is currently only done for scientific research. If there are bird or bat droppings near your home, you should have it cleaned up, if possible. If it’s not possible to clean up, try not to disturb it.
If I’ve already had histoplasmosis, could I get it again?
It’s possible for someone who’s already had histoplasmosis to get it again, but the body’s immune system usually provides some partial protection so that the infection is less severe the second time. In people who have weakened immune systems, histoplasmosis can remain hidden in the body for months or years and then cause symptoms later (also called a relapse of infection) 20.
Can my pets get histoplasmosis?
Yes. Pets, particularly cats, can get histoplasmosis, but it is not contagious between animals and people 21. Histoplasmosis in cats and dogs is similar to histoplasmosis in humans. Like humans, many cats and dogs that are exposed to Histoplasma never get sick. Cats and dogs that do develop symptoms often have symptoms that include coughing, lack of energy, and weight loss. The fungus that causes histoplasmosis grows well in soil that contains bird droppings, but birds don’t appear to be able to get histoplasmosis. If you’re concerned about your pet’s risk of getting histoplasmosis or if you think that your pet has histoplasmosis, please talk to a veterinarian.
Histoplasmosis complications
Histoplasmosis can cause a number of serious complications, even in otherwise healthy people. For infants, older adults and people with compromised immune systems, the potential problems are often life-threatening. Complications can include:
- Acute respiratory distress syndrome (ARDS). Histoplasmosis can damage lungs to the point that the air sacs begin filling with fluid. This prevents efficient air exchange and can deplete oxygen levels in the blood.
- Heart problems. Inflammation of the pericardium, the sac that surrounds your heart, is called pericarditis. When the fluid in this sac increases, it can interfere with the heart’s ability to pump blood efficiently.
- Adrenal insufficiency. Histoplasmosis can harm your adrenal glands, which produce hormones that give instructions to virtually every organ and tissue in your body.
- Meningitis. In some cases, histoplasmosis can cause meningitis, an infection and inflammation of the membranes surrounding your brain and spinal cord.
Histoplasmosis complication can also include pericarditis, broncholithiasis, pulmonary nodules, mediastinal granuloma, or mediastinal fibrosis 16, 22. In persons who develop progressive, chronic, or disseminated disease, symptoms may persist for months or longer. Mortality is high in HIV-infected persons who develop disseminated histoplasmosis.
Ocular histoplasmosis
Histoplasmosis, even mild cases, can later cause a serious eye disease called ocular histoplasmosis syndrome, a leading cause of vision loss in Americans ages 20 to 40. Ocular histoplasmosis syndrome is a clinical entity that is characterized by small, round, discrete, macular or mid peripheral atrophic (punched out) chorioretinal lesions (histo spots), peripapillary scarring, choroidal neovascularization and the absence of anterior uveitis and vitritis 23. Diagnosis of this disorder is based upon characteristic clinical findings and a positive histoplasmin skin test or residence in an endemic region for Histoplasma capsulatum. There is no active systemic disease during diagnosis of ocular histoplasmosis syndrome. Disciform scarring and macular choroidal neovascularization secondary to ocular histoplasmosis syndrome is a well-known complication which leads to loss of visual acuity or visual disturbance. Without therapy, the visual prognosis in these patients is unfavorable. Submacular surgery, radiation, steroids, photodynamic therapy, and most recently anti-vascular endothelial growth factor therapy are current therapeutic options for this condition.
How does histoplasmosis cause ocular histoplasmosis syndrome?
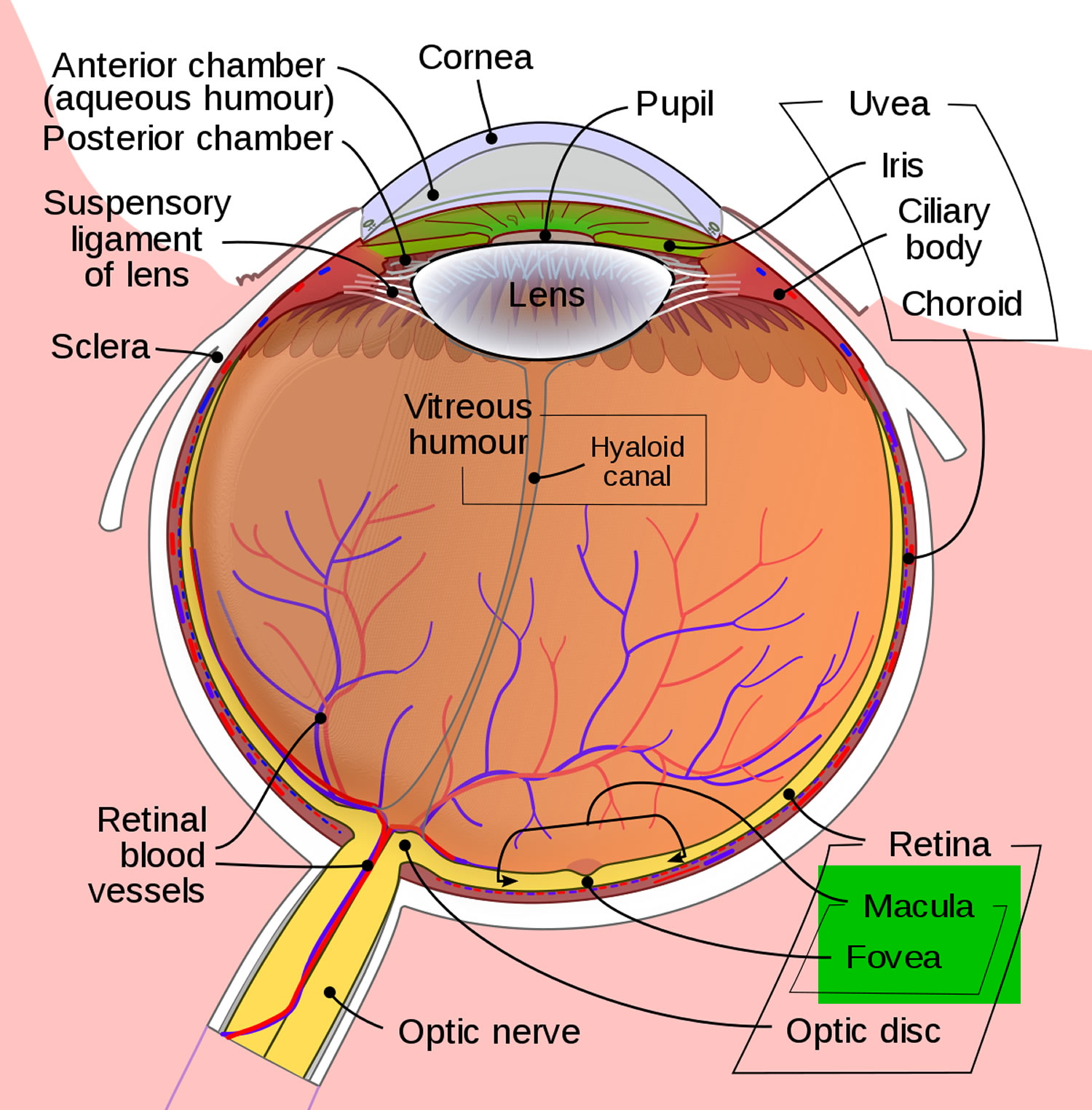
Scientists believe that Histoplasma capsulatum spores spread from the lungs to the eye, lodging in the choroid, a layer of blood vessels that provides blood and nutrients to the retina. The retina is the light-sensitive layer of tissue that lines the back of the eye. Scientists have not yet been able to detect any trace of the Histoplasma capsulatum fungus in the eyes of patients with ocular histoplasmosis syndrome. Nevertheless, there is good reason to suspect the Histoplasma organism as the cause of ocular histoplasmosis syndrome.
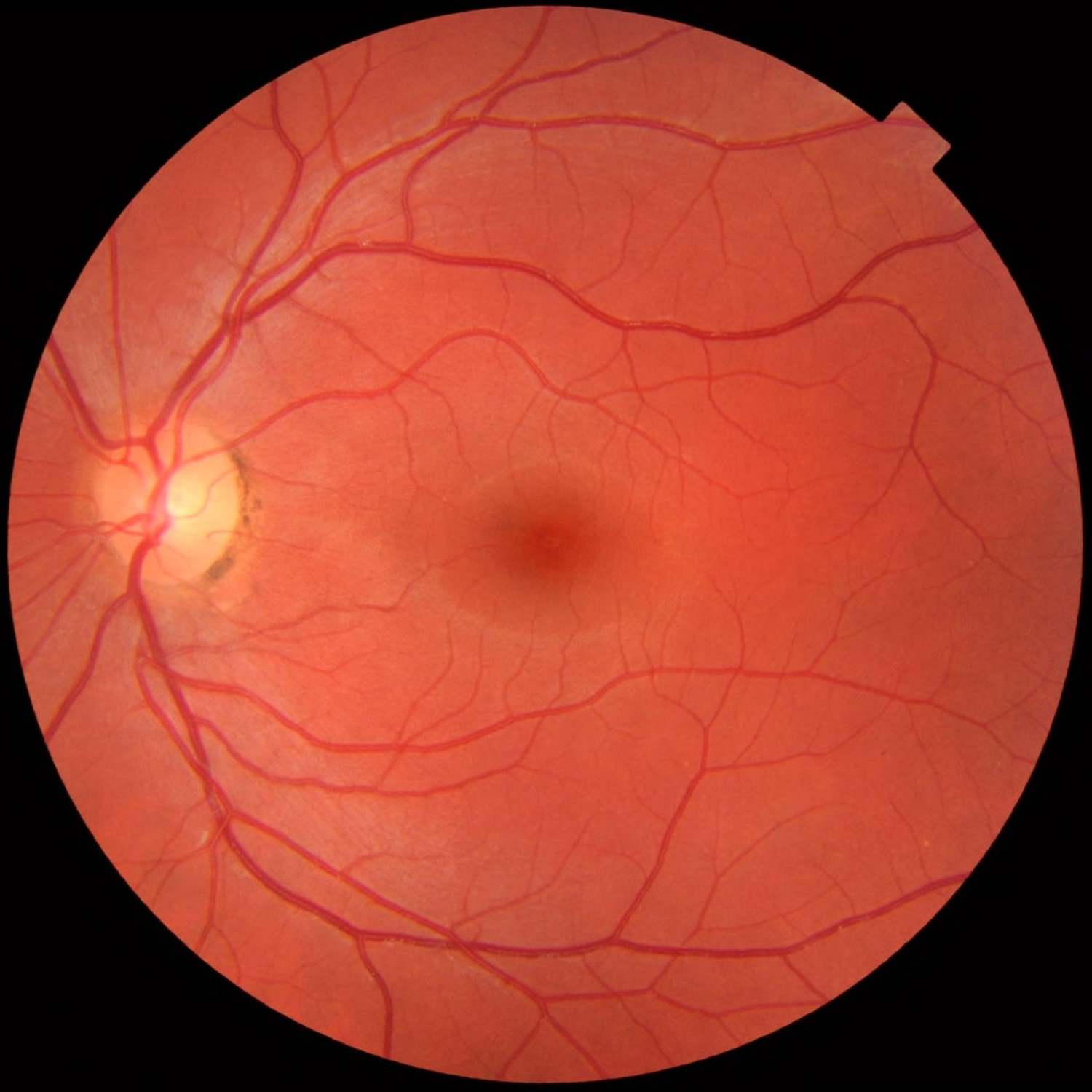
Figure 4. Ocular histoplasmosis — digital fundus image of patient with ocular histoplasmosis syndrome – chorioretinal lesions inferiorly in left eye. Lesions in the left eye are more prominent than those in the right eye. There is a yellowish lesion just inferonasal to foveal center of the left eye
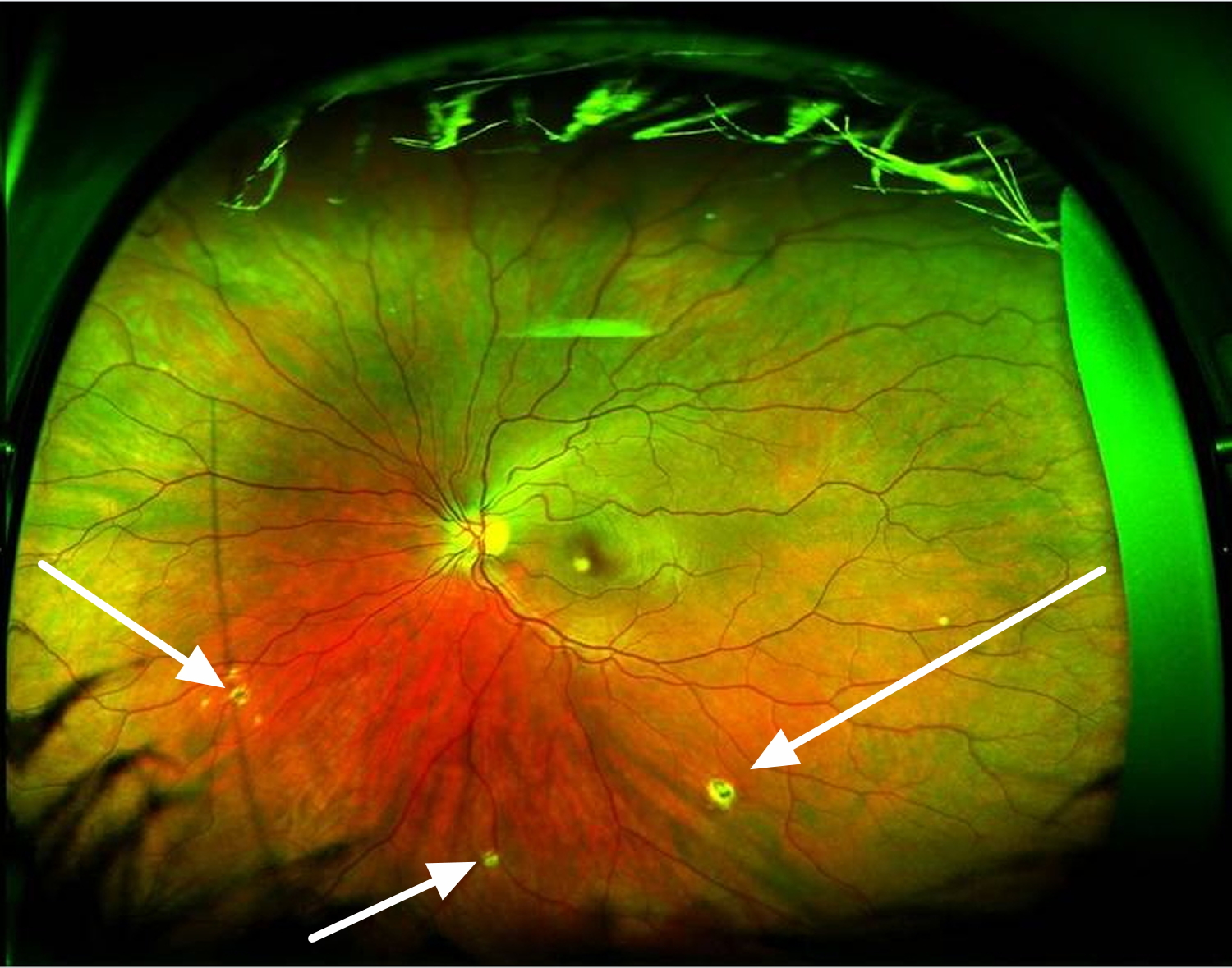
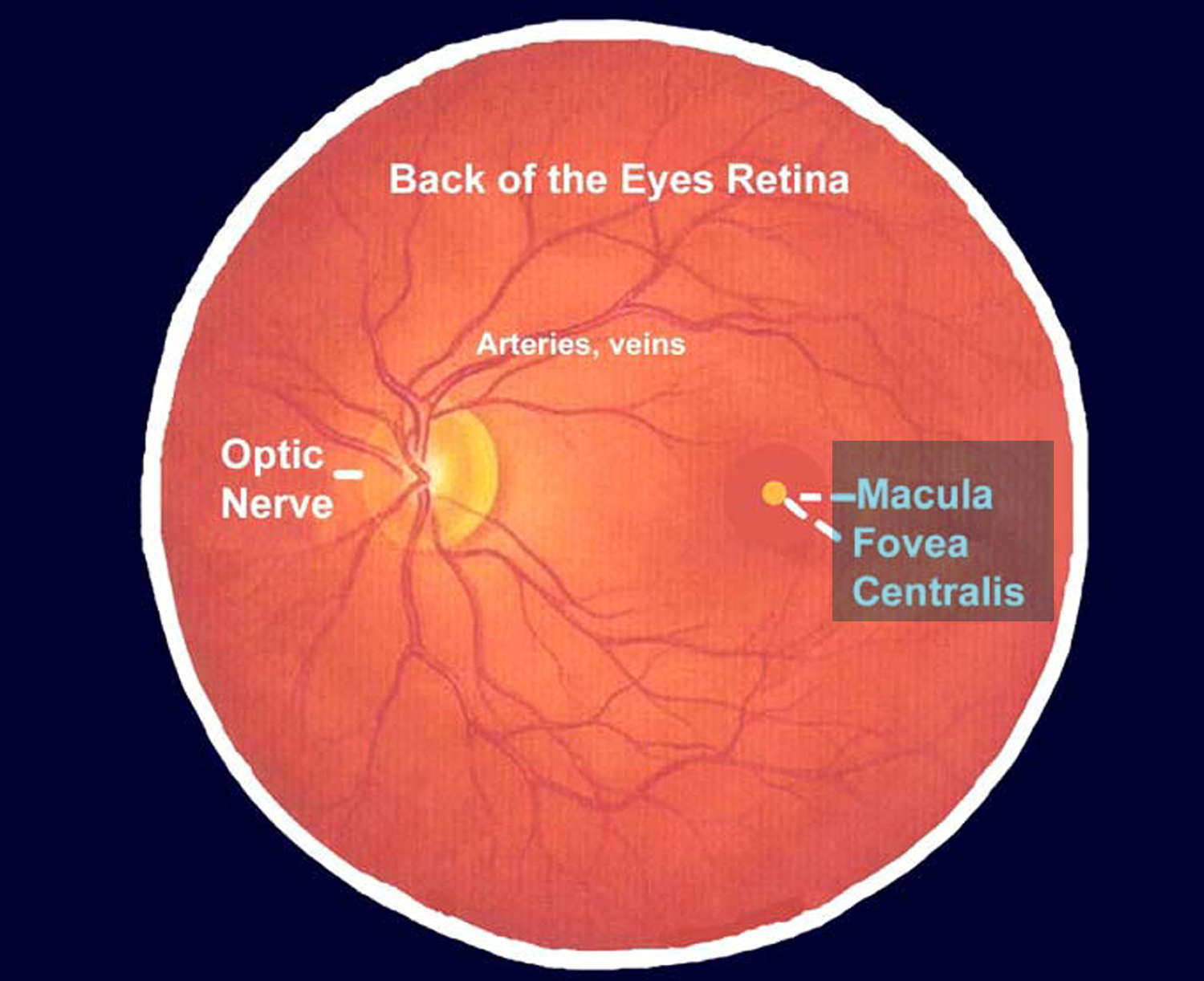
Figure 5. Normal macula and retina (left eye)
How does ocular histoplasmosis syndrome develop?
Ocular histoplasmosis syndrome develops when fragile, abnormal blood vessels grow underneath the retina. These abnormal blood vessels form a lesion known as choroidal neovascularization. If left untreated, the choroidal neovascularization lesion can turn into scar tissue and replace the normal retinal tissue in the macula. The macula is the central part of the retina that provides the sharp, central vision that allows you to read a newspaper or drive a car. When this scar tissue forms, visual messages from the retina to the brain are affected, and vision loss results.
Vision is also impaired when these abnormal blood vessels leak fluid and blood into the macula. If these abnormal blood vessels grow toward the center of the macula, they may affect a tiny depression called the fovea. The fovea is the region of the retina with the highest concentration of special retinal nerve cells, called cones, that produce sharp, daytime vision. Damage to the fovea and the cones can severely impair, and even destroy, this straight-ahead vision. Early treatment of ocular histoplasmosis syndrome is essential; if the abnormal blood vessels have affected the fovea, controlling the disease will be more difficult. Since ocular histoplasmosis syndrome rarely affects side, or peripheral vision, the disease does not cause total blindness.
Who is at risk for ocular histoplasmosis syndrome?
Although only a tiny fraction of the people infected with the Histoplasma fungus ever develops ocular histoplasmosis syndrome, any person who has had histoplasmosis should be alert for any changes in vision similar to those described above. Studies have shown the ocular histoplasmosis syndrome patients usually test positive for previous exposure to histoplasmosis.
In the United States, the highest incidence of histoplasmosis occurs in a region often referred to as the “Histo Belt,” where up to 90 percent of the adult population has been infected by histoplasmosis. This region includes all of Arkansas, Kentucky, Missouri, Tennessee, and West Virginia as well as large portions of Alabama, Illinois, Indiana, Iowa, Kansas, Louisiana, Maryland, Mississippi, Nebraska, Ohio, Oklahoma, Texas, and Virginia. Since most cases of histoplasmosis are undiagnosed, anyone who has ever lived in an area known to have a high rate of histoplasmosis should consider having their eyes examined for histo spots.
Ocular histoplasmosis syndrome symptoms
Ocular histoplasmosis syndrome usually has no symptoms in its early stages; the initial ocular histoplasmosis syndrome infection usually subsides without the need for treatment. This is true for other Histoplasma fungus infections; in fact, often the only evidence that the inflammation ever occurred are tiny scars called “histo spots,” which remain at the infection sites. Histo spots do not generally affect vision, but for reasons that are still not well understood, they can result in complications years–sometimes even decades–after the original eye infection. Histo spots have been associated with the growth of the abnormal blood vessels underneath the retina.
In later stages, ocular histoplasmosis syndrome symptoms may appear if the abnormal blood vessels cause changes in vision. For example, straight lines may appear crooked or wavy, or a blind spot may appear in the field of vision. Because these symptoms indicate that ocular histoplasmosis syndrome has already progressed enough to affect vision, anyone who has been exposed to histoplasmosis and perceives even slight changes in vision should consult an eye care professional.
Ocular histoplasmosis syndrome diagnosis
An eye care professional will usually diagnose ocular histoplasmosis syndrome if a careful eye examination reveals two conditions: (1) The presence of histo spots, which indicate previous exposure to the histo fungus spores; and (2) Swelling of the retina, which signals the growth of new, abnormal blood vessels. To confirm the diagnosis, a dilated eye examination must be performed. This means that the pupils are enlarged temporarily with special drops, allowing the eye care professional to better examine the retina.
If fluid, blood, or abnormal blood vessels are present, an eye care professional may want to perform a diagnostic procedure called fluorescein angiography. In this procedure, a dye, injected into the patient’s arm, travels to the blood vessels of the retina. The dye allows a better view of the choroidal neovascularization lesion, and photographs can document the location and extent to which it has spread. Particular attention is paid to how close the abnormal blood vessels are to the fovea.
Ocular histoplasmosis syndrome treatment
The only proven treatment for ocular histoplasmosis syndrome is a form of laser surgery called photocoagulation. A small, powerful beam of light destroys the fragile, abnormal blood vessels, as well as a small amount of the overlying retinal tissue. Although the destruction of retinal tissue during the procedure can itself cause some loss of vision, this is done in the hope of protecting the fovea and preserving the finely-tuned vision it provides.
How effective is laser surgery?
Controlled clinical trials, sponsored by the National Eye Institute, have shown that photocoagulation can reduce future vision loss from ocular histoplasmosis syndrome by more than half. The treatment is most effective when:
- The choroidal neovascularization has not grown into the center of the fovea, where it can affect vision.
- The eye care professional is able to identify and destroy the entire area of choroidal neovascularization.
Does laser surgery restore lost vision?
Laser photocoagulation usually does not restore lost vision. However, it does reduce the chance of further choroidal neovascularization growth and any resulting vision loss.
Does laser surgery cure ocular histoplasmosis syndrome?
No. ocular histoplasmosis syndrome cannot be cured. Once contracted, ocular histoplasmosis syndrome remains a threat to a person’s sight for their lifetime.
People with ocular histoplasmosis syndrome who experience one bout of abnormal blood vessel growth may have recurrent choroidal neovascularization. Each recurrence can damage vision and may require additional laser therapy. It is crucial to detect and treat ocular histoplasmosis syndrome as early as possible before it causes significant visual impairment.
Is there a simple way to check for signs of ocular histoplasmosis syndrome damage to the macula?
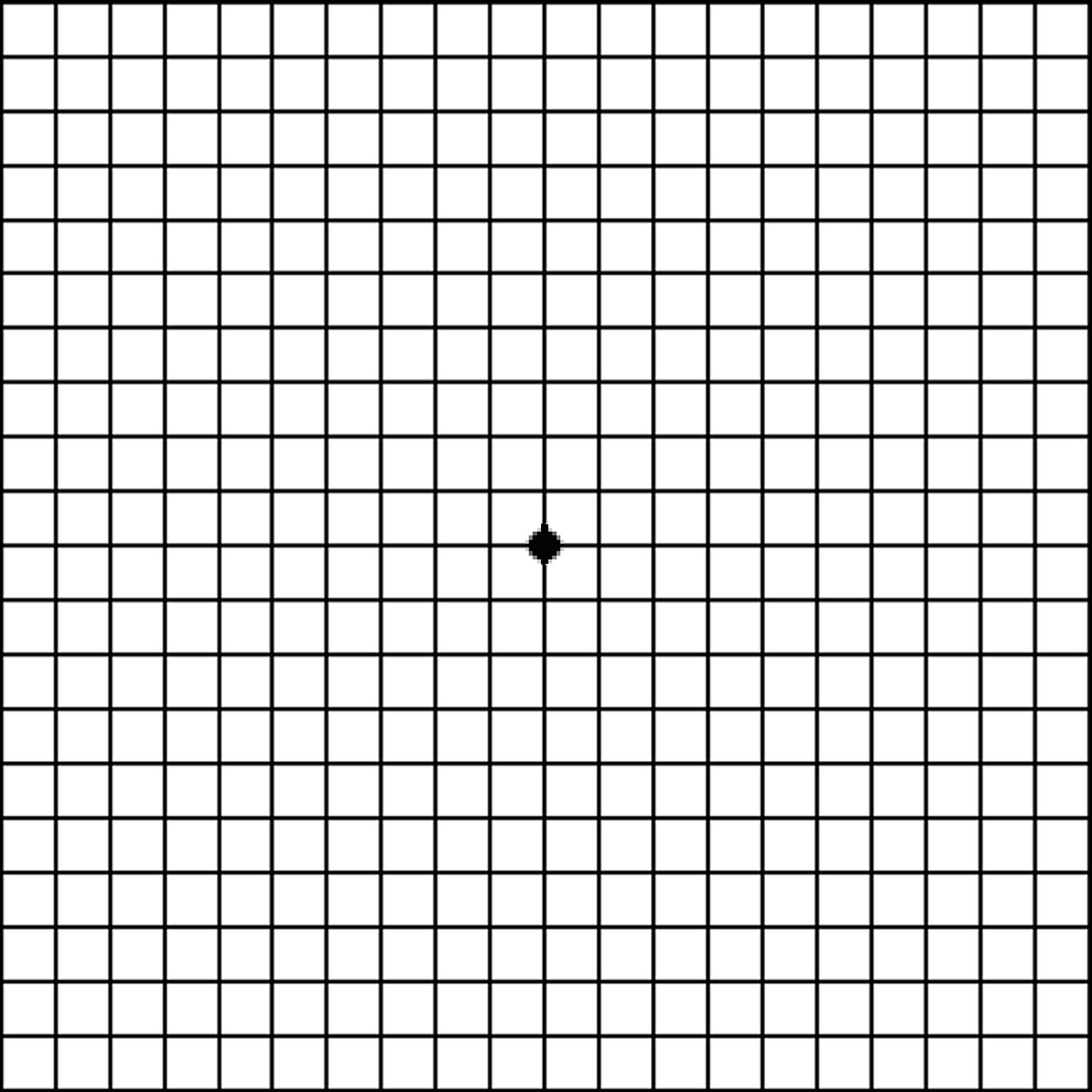
Yes. A person can check for signs of damage to the macula by looking at a printed pattern called an Amsler grid. If the macula has been damaged, the vertical and horizontal lines of the grid may appear curved, or a blank spot may seem to appear.
Many eye care professionals advise patients who have received treatment for ocular histoplasmosis syndrome, as well as those with histo spots, to check their vision daily with the Amsler grid one eye at a time. Patients with ocular histoplasmosis syndrome in one eye are likely to develop it in the other.
How To Perform Amsler Grid Test
This test helps detect macular degeneration. If you normally wear glasses for reading, wear them for this test. If you wear bifocals, look through the bottom reading portion.
Do the test with each eye separately, first the right and then the left. Hold the test grid right in front of you, 14 inches (35centimeters) away from your eye. Look at the dot in the center of the grid, not at the grid pattern.
While looking at the dot, you will see the rest of the grid in your peripheral vision. All the lines, both vertical and horizontal, should appear straight and unbroken. They should meet at all the crossing points with no missing areas. If any lines appear distorted or broken, note their location on the grid using a pen or pencil.
Figure 6. Amsler grid
What help is available for people who have already lost significant vision from ocular histoplasmosis syndrome?
Scientists and engineers have developed many useful devices to help people with severe visual impairment in both eyes. These devices, called low vision aids, use special lenses or electronics to create enlarged visual images. An eye care professional can suggest sources that provide information on counseling, training, and special services for people with low vision. Many organizations for people who are blind also serve those with low vision.
Disseminated histoplasmosis
Disseminated histoplasmosis is more likely to occur in immunosuppressed persons – HIV/AIDS 14, organ transplant 16, or use of immunosuppressive medications 15, infants 17 or adults age 55 years and older 18.
Dissemination of Histoplasma capsulatum is common in the early stages of this fungal infection 24. Symptomatic acute dissemination develops in immunocompromised patients can affect nearly any part of your body, including your mouth, liver, central nervous system, skin and adrenal glands. If untreated, disseminated histoplasmosis is usually fatal 25. Disseminated histoplasmosis presents with a febrile illness that can be complicated by severe sepsis, acute respiratory distress syndrome, and disseminated intravascular coagulopathy. On the other hand, chronic progressive disseminated histoplasmosis is typically reported in middle-aged and elderly men who are not immunosuppressed 26. They present with a wasting syndrome, long-standing fever, and night sweats. The infection may involve multiple organ systems, including the gastrointestinal tract (with resulting ulceration), adrenal glands (precipitating adrenal insufficiency), the reticuloendothelial system (causing hepatosplenomegaly), bone marrow (leading to pancytopenia), the central nervous system, and the lungs. On rare occasions, progressive disseminated histoplasmosis has been associated with hypercalcemia, and this is attributed to increased 1, 25 dihydroxyvitamin D production from the fungal granulomas 27.
In the literature, approximately two-thirds of patients with chronic disseminated histoplasmosis present with oropharyngeal or laryngeal involvement, which is almost invariably the clinical feature that leads to the diagnosis 28. In addition, adrenal involvement has been found in over half of all patients with disseminated histoplasmosis, the lesions being more commonly found in the zona reticularis; this could be due to the presence of higher downstream concentrations of cortisol, en route from secretion to the medullary central venous system 28. Cutaneous lesions of disseminated histoplasmosis are infrequent, being most commonly found in individuals who are infected with HIV 29.
Figure 7. Disseminated histoplasmosis brain
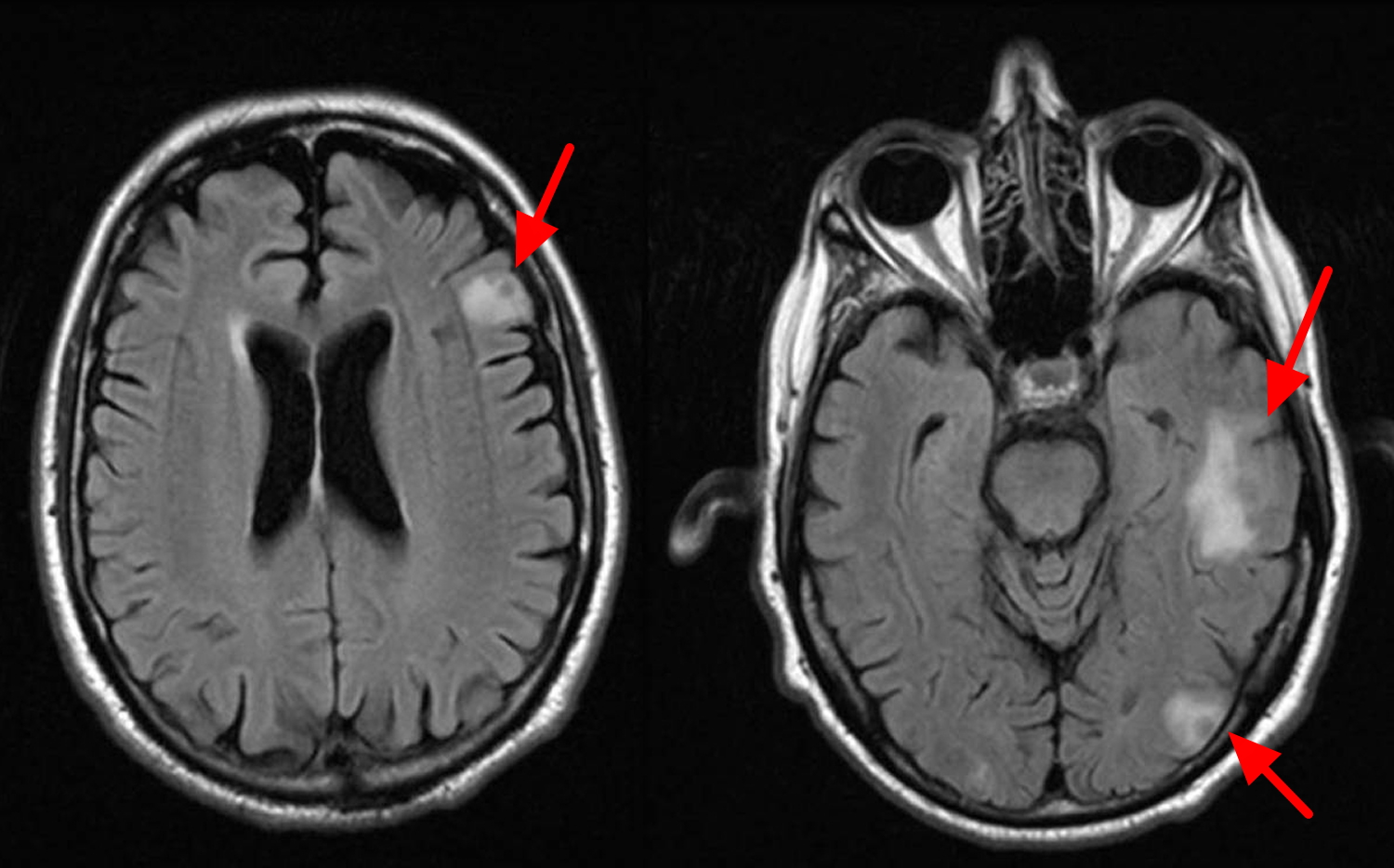
Figure 8. Histoplasmosis lung

Histoplasmosis prevention
It can be difficult to avoid breathing in Histoplasma in areas where it’s common in the environment. In areas where Histoplasma is known to live, people who have weakened immune systems (for example, by HIV/AIDS, an organ transplant, or medications such as corticosteroids or TNF-inhibitors) should avoid doing activities that are known to be associated with getting histoplasmosis, including 30:
- Disturbing material (for example, digging in soil or chopping wood) where there are bird or bat droppings
- Cleaning chicken coops
- Exploring caves
- Cleaning, remodeling, or tearing down old buildings
Large amounts of bird or bat droppings should be cleaned up by professional companies that specialize in the removal of hazardous waste.
- Spray contaminated surfaces. Before you dig soil or work in an area that could harbor the fungus that causes histoplasmosis, spray it thoroughly with water. This can help prevent spores from being released into the air. Spraying chicken coops and barns before cleaning them also can reduce your risk.
- Use an effective face mask. Wear a respirator mask. Consult the National Institute for Occupational Safety and Health to determine which type of mask will provide adequate protection for your level of exposure.
Histoplasmosis symptoms
Most people who are exposed to the fungus Histoplasma never have symptoms. Other people may have flu-like symptoms that usually go away on their own.
Symptoms of histoplasmosis (1%) may appear between 3 and 17 days after a person breathes in the fungal spores. Acute pulmonary histoplasmosis is often self-limiting; symptoms include fever, malaise, cough, headache, chest pain, chills, and myalgias. Persons with a history of pulmonary disease can develop chronic pulmonary histoplasmosis. Immunosuppressed persons are at risk for developing disseminated histoplasmosis.
Symptoms of histoplasmosis include 31:
- Fever
- Cough
- Fatigue (extreme tiredness)
- Chills
- Headache
- Chest pain
- Body aches
For most people, the symptoms of histoplasmosis will go away within a few weeks to a month 20. However, some people have symptoms that last longer than this, especially if the infection becomes severe.
In some people, usually those who have weakened immune systems, histoplasmosis can develop into a long-term lung infection, or it can spread from the lungs to other parts of the body, such as the central nervous system (the brain and spinal cord) 32.
There are several clinical presentations of histoplasmosis.
| Presentation | Features |
|---|---|
| Acute pulmonary histoplasmosis (lung disease) |
|
| Chronic pulmonary histoplasmosis |
|
| Progressive disseminated histoplasmosis |
|
| Ocular histoplasmosis syndrome (eye disease) |
|
Cutaneous features of histoplasmosis
Skin lesions of histoplasmosis are varied and can be caused by an immune reaction to an acute pulmonary infection (the lesions do not have the fungus in them) or as a manifestation of disseminated histoplasmosis (the lesions are infected). Cutaneous manifestations are reported to occur in 10% to 25% of AIDS patients with disseminated histoplasmosis.
- Erythema nodosum presents with painful red plaques on the shins. This is due to an immunologic reaction and organisms cannot be obtained from this site.
- Erythema multiforme is a target or bull’s eye type of skin reaction. This too is an immunologic reaction and organisms cannot be obtained from this site.
- Skin lesions appearing as papules, pustules and nodules may be found throughout the body and are caused by the fungus spreading to infect the skin. Biopsy of lesions often shows presence of the fungus.
Figure 9. Histoplasmosis rash (Erythema nodosum)
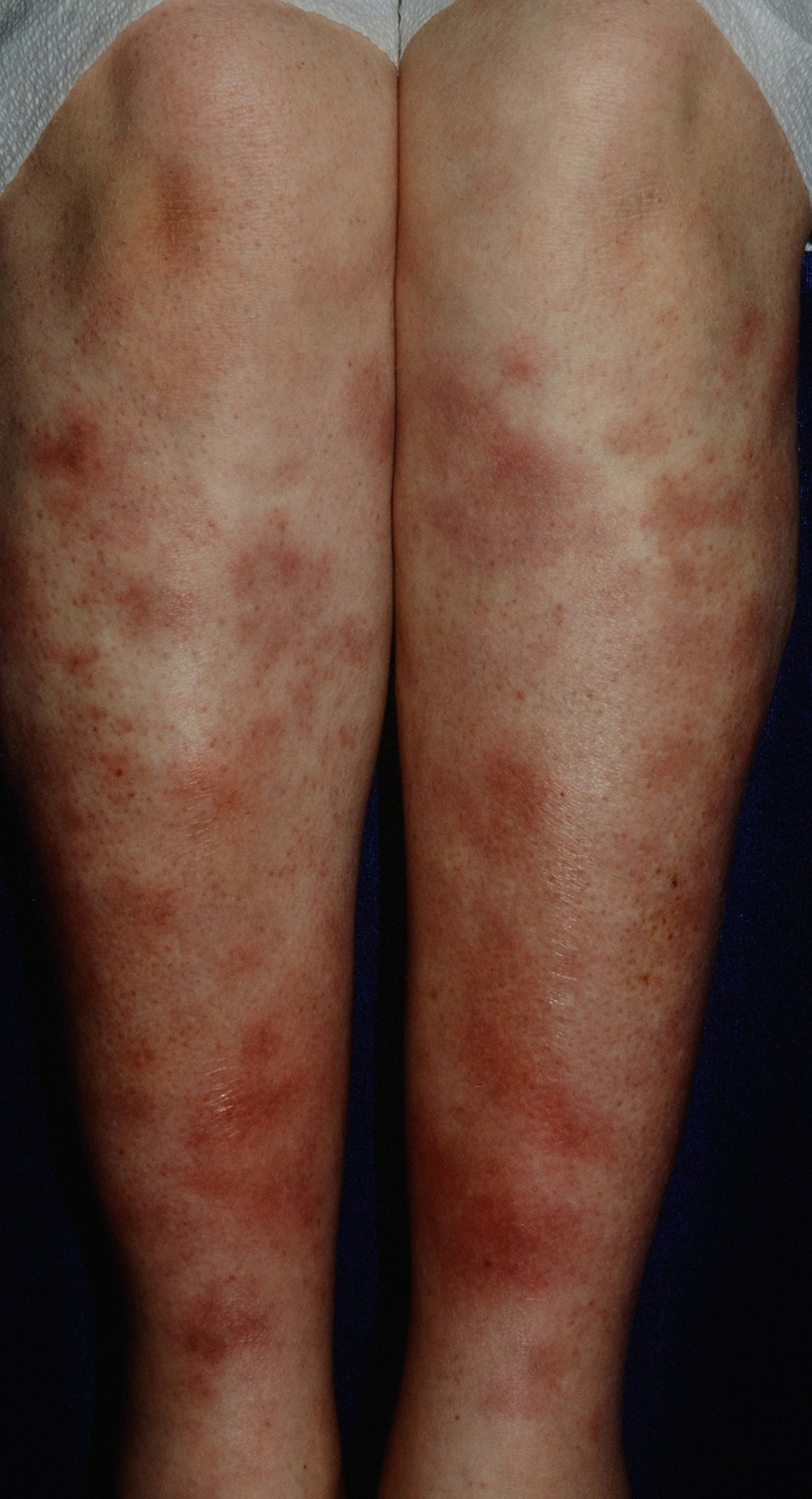
Figure 10. Histoplasmosis rash (Erythema multiforme)

Histoplasmosis diagnosis
Healthcare providers rely on your medical and travel history, symptoms, physical examinations, and laboratory tests to diagnose histoplasmosis. The most common way that healthcare providers test for histoplasmosis is by taking a blood sample or a urine sample and sending it to a laboratory.
Healthcare providers may do imaging tests such as chest x-rays or CT scans of your lungs. They may also collect a sample of fluid from your respiratory tract or perform a tissue biopsy, in which a small sample of affected tissue is taken from the body and examined under a microscope. Laboratories may also see if Histoplasma will grow from body fluids or tissues (this is called a culture).
Culture is the gold standard for diagnosing histoplasmosis but is limited by a two- to four-week incubation period and decreased sensitivity to self-limited disease 33. This method of diagnosis is not practical in cases of severe disease where delayed treatment may prove to be fatal.
Laboratory and radiological studies are performed to confirm the diagnosis of histoplasmosis.
- Sputum cultures – positive yields found in 10-15% of patients with acute pulmonary histoplasmosis and 60% in patients with chronic pulmonary histoplasmosis
- Blood cultures – positive results found in 50-90% of patients with progressive disseminated histoplasmosis
- Serologic testing may indicate spreading of the disease
- Chest x-ray and CT scanning
- Tissue biopsy may show characteristic histopathology.
Antigen detection: Enzyme immunoassay (EIA) is typically performed on urine and/or serum, but can also be used on cerebrospinal fluid or bronchoalveolar lavage fluid. Sensitivity is generally higher in urine than in serum, particularly for HIV-infected persons with disseminated histoplasmosis.
Antibody tests: Because development of antibodies to Histoplasma can take two to six weeks, antibody tests are not as useful as antigen detection tests in diagnosing acute histoplasmosis or in immunosuppressed persons, who may not mount a strong immune response.
- Immunodiffusion (ID): Tests for the presence of H (indicates chronic or severe acute infection) and M (develops within weeks of acute infection and can persist for months to years after the infection has resolved) precipitin bands; ~80% sensitivity.
- Complement Fixation (CF): Complement-fixing antibodies may take up to 6 weeks to appear after infection. CF is more sensitive but less specific than immunodiffusion.
Culture: can be performed on tissue and body fluids, but may take up to 6 weeks to become positive; most useful in the diagnosis of the severe forms of histoplasmosis.
Microscopy: for detection of budding yeast in tissue or respiratory secretions; low sensitivity.
Polymerase Chain Reaction (PCR): PCR for detection of Histoplasma directly from clinical specimens is still experimental, but promising.
How long will it take to get my test results?
It depends on the type of test. Results from a blood test or a urine test will usually be available in a few days. If your healthcare provider sends a sample to a laboratory to be cultured, the results could take a couple of weeks.
Histoplasmosis treatment
Most people infected with acute pulmonary histoplasmosis that have normal immune systems and who are not experiencing any symptoms of the disease will recover spontaneously without any treatment. Otherwise healthy patients with mild symptoms need to be monitored. Patients with prolonged or severe pulmonary symptoms may need treatment with antifungal therapy. All cases of chronic pulmonary and disseminated histoplasmosis need to be treated with antifungal medications.
The antifungals ketoconazole and itraconazole are the drugs of choice to treat mildly symptomatic or prolonged acute pulmonary histoplasmosis. They are also useful in treating cutaneous or rheumatologic manifestations of the disease in patients with weakened immune systems. Depending on the severity of the infection and the person’s immune status, the course of treatment can range from 3 months to 1 year.
Table 1. Treatment Recommendations for Patients with Histoplasmosis
| Type of histoplasmosis | Treatment of severe manifestations | Treatment of moderate or mild manifestations |
|---|---|---|
Acute pulmonary | Amphotericin B (Fungizone IV), 0.7 mg per kg per day* with corticosteroids† (prednisone [Deltasone], 60 mg daily for 2 weeks), then itraconazole (Sporanox), 200 mg once or twice daily* for 12 weeks | Symptoms less than four weeks: none |
Symptoms more than four weeks: itraconazole, 200 mg once or twice daily for six to 12 weeks | ||
Chronic pulmonary | Amphotericin B,‡ then itraconazole for 12 to 24 months | Itraconazole for 12 to 24 months |
Disseminated (in patients without AIDS) | Amphotericin B, 0.7 to 1.0 mg per kg per day,‡ then itraconazole for six to 18 months§ | Itraconazole for six to 18 months |
Disseminated (in patients with AIDS) | Induction: amphotericin B,‡ then itraconazole, 200 mg twice daily, to complete a 12-week course | Induction: itraconazole, 200 mg three times daily for three days, then twice daily to complete a 12-week course |
Maintenance: itraconazole for life | ||
Maintenance: itraconazole for life | ||
Granulomatous mediastinitis | Amphotericin B, then itraconazole for six to 12 months; also consider corticosteroids and/or surgical resection∥ | Itraconazole for six to 12 months |
Pericarditis | Corticosteroids¶ and/or pericardial drainage | NSAIDs for two to 12 weeks |
Rheumatologic | NSAIDs for two to 12 weeks | NSAIDs for two to 12 weeks |
AIDS = acquired immunodeficiency syndrome; NSAIDs = nonsteroidal anti-inflammatory drugs.
*—Unless otherwise specified.
†—Effectiveness of corticosteroid therapy is controversial.
‡—If amphotericin B is used for the entire course of treatment, dosage is 35 mg per kg over three to four months.
§—Therapy should continue until Histoplasma antigen concentrations are less than 4 units in urine and serum.
∥—Corticosteroids may be considered in patients with major airway obstruction; surgical resection should be reserved for patients who remain symptomatic and continue to demonstrate obstruction of major mediastinal structures, despite antifungal therapy.
¶—If corticosteroids are administered, concurrent antifungal therapy is recommended.
Amphotericin B is the drug of choice for severe cases of acute pulmonary histoplasmosis, chronic pulmonary histoplasmosis and all forms of disseminated histoplasmosis. Chronic progressive disseminated disease may run a long course that lasts for years with long asymptomatic periods interspersed. Acute progressive disseminated disease may need life long treatment with antifungals to prevent relapses. Amphotericin B (Fungizone IV) is considered the treatment of choice in severe or disseminated disease 35. A decrease in fever occurs within a week of treatment in the majority of patients 35. Treatment can usually be changed to itraconazole (Sporanox) within three to 14 days, which is desirable because amphotericin is associated with toxicity and requires intravenous administration 35. Nephrotoxicity, the most serious adverse effect, is manifested by azotemia or hypokalemia requiring potassium supplementation 36. Normocytic anemia can also occur but, like azotemia, usually resolves after discontinuation of the medication 36.
Itraconazole is an effective treatment in mild or moderate cases of disseminated histoplasmosis, as well as in acute and chronic pulmonary disease 35. Although itraconazole is not as rapid-acting as amphotericin, it has the advantage of being well tolerated even in long-term use.4,15 Most side effects, including headache, dizziness, and gastrointestinal symptoms, are transient 36. Biliary excretion eliminates the need for adjusting dosages in patients with renal disease 36.
Abnormal results on liver function tests are possible, but levels typically return to normal on completion of therapy. The risk of hepatitis is rare 36. Careful monitoring and assessment of the risks and benefits are recommended to prevent unnecessary discontinuation of this drug.
Fluconazole (Diflucan) is less effective than amphotericin B or itraconazole in the treatment of histoplasmosis 37 and is associated with more relapses 38. Unlike itraconazole, fluconazole enters the cerebrospinal fluid 39. Therefore, fluconazole therapy is reserved for use in patients with mild to moderate disease who cannot take itraconazole 38 and patients with meningitis 39.
- Guimarães AJ, Nosanchuk JD, Zancopé-Oliveira RM. Diagnosis of Histoplasmosis. Braz J Microbiol. 2006;37:1–13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2863343/[↩]
- Bradsher RW. Histoplasmosis and blastomycosis. Clin Infect Dis. 1996;22(Suppl 2):S102–111. https://www.ncbi.nlm.nih.gov/pubmed/8722836[↩]
- Kwon-Chung KJ. Perfect state (Emmonsiella capsulata) of the fungus causing large-form African histoplasmosis. Mycologia. 1975;67(5):980–990. https://www.ncbi.nlm.nih.gov/pubmed/1196334[↩]
- Springston JP. The birds. Occup Health Saf. 1998;67:86–9.[↩]
- Manos NE, Ferebee SH, Kerschbaum WF. Geographic variation in the prevalence of histoplasmin sensitivity. Dis Chest. 1956 Jun;29(6):649-68.[↩][↩]
- Colombo AL, Tobon A, Restrepo A, Queiroz-Telles F, Nucci M. Epidemiology of endemic systemic fungal infections in Latin America. Med Mycol. 2011 Nov;49(8):785-98.[↩][↩]
- Loulergue P, Bastides F, Baudouin V, Chandenier J, Mariani-Kurkdjian P, Dupont B, et al. Literature review and case histories of Histoplasma capsulatum var. duboisii infections in HIV-infected patients. Emerg Infect Dis. 2007 Nov;13(11):1647-52.[↩][↩]
- Chakrabarti A, Slavin MA. Endemic fungal infections in the Asia-Pacific region. Med Mycol. 2011 May;49(4):337-44.[↩][↩]
- McLeod DS, Mortimer RH, Perry-Keene DA, Allworth A, Woods ML, Perry-Keene J, et al. Histoplasmosis in Australia: report of 16 cases and literature review. Medicine. 2011 Jan;90(1):61-8.[↩][↩]
- Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007;86(3):162–169. https://www.ncbi.nlm.nih.gov/pubmed/17505255[↩][↩]
- Guimarães AJ, Nosanchuk JD, Zancopé-Oliveira RM. DIAGNOSIS OF HISTOPLASMOSIS. Brazilian journal of microbiology : [publication of the Brazilian Society for Microbiology]. 2006;37(1):1-13. doi:10.1590/S1517-83822006000100001. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2863343/[↩]
- CDC. Histoplasmosis in a state where it is not known to be endemic–Montana, 2012-2013. MMWR. 2013 Oct 25;62(42):834-7.[↩]
- DiSalvo A. The role of bats in the ecology of Histoplasma capsulatum. In: Ajello L CE, Furcolow ML, editors. Histoplasmosis: proceedings of the second national conference; 1971; Springfield, IL; 1971. p. 149–61.[↩]
- Marukutira T, Huprikar S, Azie N, Quan SP, Meier-Kriesche HU, Horn DL. Clinical characteristics and outcomes in 303 HIV-infected patients with invasive fungal infections: data from the Prospective Antifungal Therapy Alliance registry, a multicenter, observational study. HIV/AIDS. 2014;6:39-47.[↩][↩]
- Cuellar-Rodriguez J, Avery RK, Lard M, Budev M, Gordon SM, Shrestha NK, et al. Histoplasmosis in solid organ transplant recipients: 10 years of experience at a large transplant center in an endemic area. Clin Infect Dis. 2009 Sep 1;49(5):710-6.[↩][↩]
- McKinsey DS, McKinsey JP. Pulmonary histoplasmosis. Semin Respir Crit Care Med. 2011 Dec;32(6):735-44.[↩][↩][↩]
- Odio CM, Navarrete M, Carrillo JM, Mora L, Carranza A. Disseminated histoplasmosis in infants. Ped Infect Dis J. 1999 Dec;18(12):1065-8.[↩][↩]
- Wheat LJ, Slama TG, Norton JA, Kohler RB, Eitzen HE, French ML, et al. Risk factors for disseminated or fatal histoplasmosis. Analysis of a large urban outbreak. Ann Intern Med. 1982 Feb;96(2):159-63.[↩][↩]
- Roy M, Park BJ, Chiller TM. Donor-Derived Fungal Infections in Transplant Patients. Curr Fungal Infect Rep. 2010;4:219-28.[↩]
- Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med. 2004 Apr;25(2):129-44.[↩][↩]
- Bromel C, Sykes JE. Histoplasmosis in dogs and cats. Clinical techniques in small animal practice. 2005 Nov;20(4):227-32.[↩]
- Kauffman CA. Histoplasmosis: a clinical and laboratory update. Clin Microbiol Rev. 2007 Jan;20(1):115-32.[↩]
- Yılmaz T, Dikci S, Genç O, Mutlu K. Multiple Intravitreal Ranibizumab Injections for Persistant Choroidal Neovascularization Associated with Presumed Ocular Histoplasmosis Syndrome. Turkish Journal of Ophthalmology. 2017;47(2):115-118. doi:10.4274/tjo.82956. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5384118/[↩]
- Kauffman CA. Histoplasmosis. Clin Chest Med. 2009;30(2):217–225. v. https://www.ncbi.nlm.nih.gov/pubmed/19375629[↩]
- Knox KS, Hage CA. Histoplasmosis. Proc Am Thorac Soc. 2010;7(3):169–172. https://www.atsjournals.org/doi/full/10.1513/pats.200907-069AL[↩]
- Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007;86(3):162–169. https://journals.lww.com/md-journal/fulltext/2007/05000/Systemic_Histoplasmosis__A_15_Year_Retrospective.4.aspx[↩]
- Chalhoub E, Elhomsy G, Brake M. Hypercalcemia in histoplasmosis aggravated with antifungal treatment. J Med Liban. 2012;60(3):165–168. https://www.ncbi.nlm.nih.gov/pubmed/23198458[↩]
- Goodwin RA, Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980;59(1):1–33. https://www.ncbi.nlm.nih.gov/pubmed/7356773[↩][↩]
- Wheat LJ, Kauffman CA. Histoplasmosis. Infect Dis Clin North Am. 2003;17(1):1-19, vii. http://dx.doi.org/10.1016/S0891-5520(02)00039-9 https://www.ncbi.nlm.nih.gov/pubmed/12751258[↩]
- Kaplan JE, Benson C, Holmes KK, Brooks JT, Pau A, Masur H, et al. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR. 2009 Apr 10;58(RR-4):1-207.[↩]
- Cano MV, Hajjeh RA. The epidemiology of histoplasmosis: a review. Semin Respir Infect. 2001 Jun;16(2):109-18.[↩]
- Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine. 2007 May;86(3):162-9.[↩]
- Gomez BL, Figueroa JI, Hamilton AJ, Ortiz BL, Robledo MA, Restrepo A, et al. Development of a novel antigen detection test for histoplasmosis. J Clin Microbiol. 1997;35:2618–22.[↩]
- Wheat J, Sarosi G, McKinsey D, Hamill R, Bradsher R, Johnson P, et al. Practice guidelines for the management of patients with histoplasmosis. Infectious Diseases Society of America. Clin Infect Dis 2000;30:690.[↩]
- Wheat J. Histoplasmosis. Experience during outbreaks in Indianapolis and review of the literature. Medicine. 1997;76:339–54.[↩][↩][↩][↩]
- Walsh TJ, Gonzalez C, Lyman CA, Chanock SJ, Pizzo PA. Invasive fungal infections in children: recent advances in diagnosis and treatment. Adv Pediatr Infect Dis. 1996;11:187–290.[↩][↩][↩][↩][↩]
- Bradsher RW. Histoplasmosis and blastomycosis. Clin Infect Dis. 1996;22(suppl 2):S102–11.[↩]
- McKinsey DS, Kauffman CA, Pappas PG, Cloud GA, Girard WM, Sharkey PK, et al. Fluconazole therapy for histoplasmosis. The National Institute of Allergy and Infectious Diseases Mycoses Study Group. Clin Infect Dis. 1996;23:996–1001.[↩][↩]
- Wheat J, Sarosi G, McKinsey D, Hamill R, Bradsher R, Johnson P, et al. Practice guidelines for the management of patients with histoplasmosis. Infectious Diseases Society of America. Clin Infect Dis. 2000;30:688–95.[↩][↩]





{kind=link}