Contents
- What causes hormonal acne
- How Hormones Influence Acne
- Hormonal acne treatment for Women
- Hormonal Therapy for Acne in Women
What causes hormonal acne
What causes acne ? Surprisingly, the common medical answer is that the exact cause of acne is unknown 1. This humble answer appreciates the complexities of the processes that take place in your body. However, it does not mean that doctors don’t understand anything about acne. On the contrary, doctors and scientists have a good grasp of most of the pieces of the puzzle that result in acne, and as a result, the effectiveness of acne medication has improved significantly in recent years.
Acne is the most common skin problem that doctors and skin doctors see. In fact, it affects nearly everyone and most commonly teenagers. While acne is not a life-threatening disease, it is a very visible skin problem that can cause embarrassment and social anxiety. As is the case with many skin diseases, there is a social and psychological element that must be taken into consideration. In particular, it is most prevalent in teenagers, who are often very sensitive to these problems. Severe acne can also result in permanent scars if they are not treated carefully, and thus, concerns about acne should be taken seriously.
Teenagers are the age group most commonly thought to struggle the most with acne, but dermatologists are finding that late-onset or adult-onset acne is becoming increasingly common in women in their 20s, 30s, 40s and even 50s 2.
- A study examining the prevalence of acne in adults over age 20 found that acne affects more than 50 percent of women between the ages of 20-29 and more than 25 percent of women between the ages of 40-49.
- The study found a disproportionate number of adult women were affected by acne compared to similar-aged men.
- A 2011 clinical study examining photos of women from age 10-70 for visible signs of acne found that 45 percent of women aged 21-30 had clinical acne, 26 percent of women aged 31-40 had clinical acne, and 12 percent of women aged 41-50 had clinical acne.
Although there is no one single cure that works in all patients with acne, doctors can recommend patient-specific treatment regimens to control acne and minimize future breakouts. In women, hormonal therapies are commonly used to treat acne safely and effectively.
With acne, it’s important for patients to understand that there are no quick fixes and none of the therapies used to treat acne work overnight (like many acne quick fix scams that’s been marketed online). Furthermore, patients need to be consistent when using their acne medications and realize that they may not see the full effects of their treatment regimen for eight to 10 weeks — and in many case, some type of maintenance therapy is required for long-term clearance of acne.
Types of Acne
Comedones
Comedones, more commonly known as blackheads and whiteheads are yellow or black bumps. Blackheads in particular, on first appearance, resemble dirt. They are caused by blocked pores, and the color is the result of oxidized sebum, which is the natural oil that occurs in the glands. It is not, as commonly believed, a result of poor hygiene.
Papules
Papules, which are commonly known as zits or pimples, occur when comedones become inflamed. They tend to be larger in size, and will often be sensitive to touch, causing pain or discomfort when pressure is applied to it.
Nodules
Nodules are large bumps which originate in the deeper levels of the skin. This type of lesion occurs in those with severe acne. As nodules affect the deeper layers of the skin, they often result in permanent scarring.
How Hormones Influence Acne
Primary causes of acne
- Excess sebum, or oil gland, production (influenced by hormones).
- Skin cells that shed become abnormally sticky and accumulate, or clog up, in the hair follicle (influenced by hormones).
- Increased number of the acne-causing bacterium Propionbacterium acnes, or P. acnes.
- Skin inflammation.
The role of androgens
- Androgens, the male hormones present in both men and women, can contribute to acne flares by overstimulating the oil glands and altering the development of skin cells that line hair follicles in the skin.
- The majority of women with acne have normal androgen levels, but hormonal testing is recommended for females who have acne accompanied by excess facial or body hair, deepening voice, or irregular or infrequent menstrual periods.
Figure 1. Acne formation
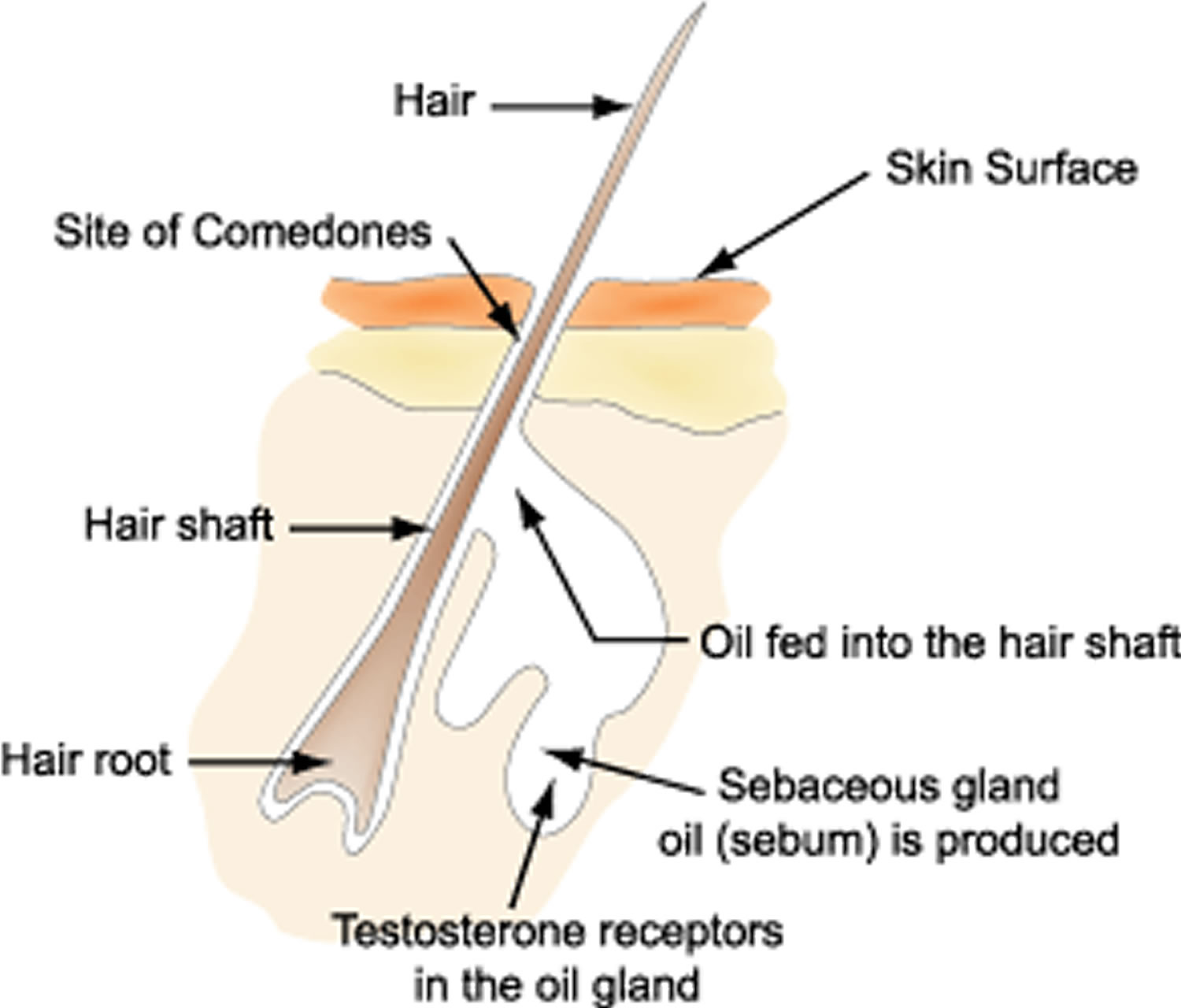
Figure 2. Skin structure

Acne formation involves complex hormonal, bacterial, and inflammatory processes that intertwine with each other. Larger amounts of sebum (skin oil) are produced, and the composition of the oil also changes. Scales are produced on the walls of the hair follicle which build up and block the pore. This process produces comedones – blackheads and whiteheads.
Acne bacteria proliferate in the oil rich environment, and release chemicals which attract white cells from the blood which produce inflammation. This results in papules-zits or pimples on the skin. Severe inflammation can result in the expansion of the pores and the surrounding skin can also become inflamed. This process results in larger lumps called nodules.
When excessive inflammation damages the collagen producing cells, it results in scarring. When collagen production is reduced, they present as depressed scars, while increased collagen production will result in scars that present as thickened skin.
As can be seen in Figure 1 above, the key factors that cause and aggravate acne are androgenic hormones (which produce excess oil), acne bacteria, and inflammation of the oil gland. Anything that aggravates one of the three factors generally results in the worsening of acne. Acne medication aims to control one or more of these factors in order to control acne.
Aggravating Factors For Acne
The points below are well documented factors that cause or aggravate existing acne. While there is great individual variability, these are factors that have been well documented in acne studies. While complete avoidance is not a reasonable possibility all the time, minimizing them can help you reduce the chance of flare-ups.
- Excessive cleansing-aggravates inflammation
- Squeezing or popping pimples-aggravates inflammation
- Oily cosmetic products-promotes acne bacteria proliferation by clogging the pores
- Use of drugs such as anabolic steroids-promotes excessive androgenic hormones
- Sweating
Possible factors that may aggravate acne
The points below have been not been established as aggravating factors in controlled medical studies, but there is an abundance of anecdotal evidence that supports possible connections. These may be minor factors. As acne is a complex process with a lot of individual variability, it can be difficult to establish causal relationships in a controlled study, as there are many factors to take into consideration. Small sample size is also a big hurdle for factors that only affect a small percentage of the population. Our suggestion is to not be paranoid, but if you know that these factors do affect you negatively, it would be wise to avoid them as much as possible.
- Certain types of foods (individual dependent)
- Chronic stress
- Certain sunscreens and moisturizers
Here are some tips to help prevent acne breakouts and clear them up as fast as possible:
- Wash your face twice a day (no more) with warm water and a mild soap made for people with acne. Gently massage your face with circular motions. Don’t scrub. Overwashing and scrubbing can cause skin to become irritated. After cleansing, the American Academy of Dermatology recommends applying an over-the-counter (no prescription needed) lotion containing benzoyl peroxide.
- Remove your makeup before you go to sleep. When buying makeup, make sure you choose brands that say “noncomedogenic” or “nonacnegenic” on the label. And even if a product is labeled nonacnegenic or noncomedogenic, you should stop using it and talk to your doctor if you notice that it’s irritating your skin or seems to cause breakouts. Throw away old makeup that smells or looks different from when you first bought it.
- Don’t pop pimples. It’s tempting, but here’s why you shouldn’t: Popping pimples can push infected material further into the skin, leading to more swelling and redness, and even scarring. If you notice a pimple coming before a big event, like the prom, a dermatologist can often treat it for you with less risk of scarring or infection.
- Avoid touching your face with your fingers or leaning your face on objects that collect sebum and skin residue like your phone. Touching your face can spread the bacteria that cause pores to become inflamed and irritated. To keep bacteria at bay, wash your hands before applying anything to your face, such as treatment creams or makeup.
- Protect your skin from the sun. It may seem like a tan masks acne, but it’s only temporary. A tan may worsen your acne, not improve it. Tanning also causes damage to skin that will eventually lead to wrinkles and increase your risk of skin cancer.
- If you wear glasses or sunglasses, make sure you clean them frequently to keep oil from clogging the pores around your eyes and nose.
- Keep hair clean and out of your face to prevent additional dirt and oil from clogging your pores.
- If you get acne on your body, try not to wear tight clothes. They don’t allow skin to breathe and may cause irritation. Scarves, headbands, and caps can collect dirt and oil, too.
Do certain foods cause acne ?
Some studies suggest there is a link between the food we eat and acne. It is very difficult to study the role of diet and acne.
Acne is reported to be less common in people that have a diet with lower glycemic index, e.g., natives from Kitava and Papua New Guinea, the Ache people of Paraguay, Inuits and rural residents of Kenya, Zambia and Bantu. These people tend to become sexually mature at a later age than in the cities where higher glycemic index foods are consumed. Early puberty is associated with earlier onset and more severe acne that tends to peak at the time of full maturity (age 16 to 18).
Several studies, criticised for their quality, have shown benefits in acne from a low-glycemic, low-protein, low-fat and low-dairy diet. The reasons for these benefits are thought to relate to the effects of these foods on insulin and insulin-like growth factor-1 (IGF-1).
Insulin induces male hormones (androgens), glucocorticoids and growth factors. These provoke keratinisation (scaling) of the hair follicle and sebum production. An increase in sebum production and keratinisation is a factor in the appearance of acne.
Foods that increase insulin production
Foods that increase insulin levels have a high glycemic index. The glycemic index is a measurement of how carbohydrates have an effect on our blood sugar levels. When we eat foods with a high glycaemic index, such as white bread and baked goods, our blood sugar level rises. This increases the amount of insulin produced in our body.
Although cow’s milk has a low glycemic index, it contains androgens, oestrogen, progesterone and glucocorticoids, which also provoke keratinisation and sebum production. Milk also contains amino acids (eg arginine, leucine, and phenylalanine) that produce insulin when combined with carbohydrates. Other components of milk that might induce comedones include whey proteins and iodine.
Caffeine, theobromine, and serotonin found in chocolate may also increase insulin production.
Food containing fatty acids
Fatty acids are needed to form sebum. Studies show that some monounsaturated fatty-acids, such as sapienic acid and some vegetable oils, can increase sebum production. However, the essential fatty acids linoleic, linolenic and gamma linolenic acid can unblock the follicles and reduce sebum production.
Suitable food if you have acne
Some people with acne have reported improvement in their skin when they follow a low-glycemic index diet and increase their consumption of whole grains, fresh fruits and vegetables, fish, olive oil, garlic, while keeping their wine consumption moderate.
It’s a good idea to drink less milk and eat less of high glycemic index foods such as sugar, biscuits, cakes, ice creams and bottled drinks. Reducing your intake of meat and amino acid supplements may also help.
Seek medical help if you are concerned about your skin, as changing diet does not always help.
Hormonal acne treatment for Women
Factors to consider
- Therapy must be tailored to the patient’s specific type and severity of acne: mild, moderate or severe.
- Pregnancy considerations must be taken into account when prescribing acne medications because several oral and topical medications should not be used when trying to conceive or during pregnancy.
- Adult women may be more likely to have dry skin as they get older, and topical acne medications may cause more skin irritation in patients with dry skin.
- Some adult women with acne also may show signs of rosacea (another common skin condition characterized by redness and inflammation), which would make some topical acne medications harder to tolerate.
Topical retinoids
In acne patients of any age, dermatologists consider topical retinoids (medications that contain vitamin A derivatives) first-line therapy by for mild-to-moderate inflammatory acne accompanied by blackheads and whiteheads.
Topical retinoids also are the preferred therapy for overall long-term prevention of new acne.
Hormonal Therapy for Acne in Women
Hormonal therapy can be used whether or not hormonal abnormalities have been demonstrated.
Progesterone-only oral contraceptives are not effective in the management of androgen-mediated skin conditions.
Combined oral contraceptives contain two hormones, ethinyloestrodiol 20–35 mcg (an oestrogen) and a progesterone. They prevent pregnancy by suppressing ovulation and changing cervical mucus. There are various kinds of progesterone, which may be androgenic in nature and thus unsuitable for those androgen-mediated skin conditions (particularly levonorgesterol and norgestrel). Anti-androgenic or minimally androgenic progesterones (see below) are indicated in these women.
- The progestational antiandrogen-containing contraceptives, i.e., 2mg cyproterone acetate and 0.35ìg ethinyl estradiol (Diane-35®), or 3.0mg drospirenone and 0.030mg ethinyl estradiol (Yasmin®) work best. The side-effect profile is similar to other oral contraceptive pills.
Their effect in hyperandrogenism is to reduce production of androgens by the ovaries, by the adrenals and at the receptor level in the skin. They also decrease circulating testosterone by increasing sex hormone binding globulin (SHBG).
Combined oral contraceptives are available as 21-day and 28-day packs; start on Day 1 (conventionally, day 1 is the first day of menstruation) and take one a day for 21 days. Then have a 7-day break (21-day pack) or take the placebo tablets for a week (28-day pack) before starting the cycle again. During this time, you can expect a withdrawal bleed (a period).
Combined oral contraceptives can increase the risk of thromboembolism (blood clots blocking blood vessels), especially in those with an inherited tendency (“thrombophilia”), or who smoke.
- Combination oral contraceptives (also known as “the pill”) have been found to effectively clear acne in women either when used alone or in conjunction with an anti-androgen medication, such as spironolactone.
- Many different oral contraceptives have been shown to be effective in treating acne. Oral contraceptives approved by the U.S. Food and Drug Administration (FDA) for the treatment of hormonal acne contain ethinyl estradiol plus either the progestin norgestimate, norethindrone acetate or drospirenone.
- These oral contraceptives work together to alter levels and activity of hormones that can trigger acne.
- Patients must be carefully screened before using any hormonal therapy for acne because there are numerous contraindications (or factors that increase the risks of a particular medication). Contraindications for use of oral conceptive pills include, but are not limited to:
- Personal history of breast cancer.
- Heart attack, stroke or blood clots.
- Uncontrolled high blood pressure.
- Abnormal vaginal bleeding.
- Patients also need to be monitored regularly while using hormonal therapies.
The combined oral contraceptive may be unsuitable if the patient:
- Has had a previous blood clot (thrombosis, embolism or ‘DVT’)
- Has high blood pressure (hypertension) or heart disease
- Smokes
- Is significantly overweight (obese)
- Has recently undergone surgery or trauma or is immobile
- Is undertaking long distance air travel (4 hours or more)
- Has a family member aged less than 50 years who has had blood clots or high blood pressure
Many of these women can instead use progesterone-only contraceptive pills while they are being treated with spironolactone or cyproterone.
Oral contraceptives can sometimes aggravate migraine and are inadvisable in those with significant liver disease. They may occasionally increase the risk of certain uncommon forms of breast cancer. They must not be taken in pregnancy.
On the other hand, the combined oral contraceptive reduces the risk of ovarian and endometrial cancer, benign breast disease, ectopic pregnancy, painful periods, iron deficiency anemia and pelvic inflammatory disease.
Combined oral contraceptives with anti-androgenic components have advantages
- They regulate the menstrual cycle in the majority of women
- Lighter, less painful periods occur in the majority of women
- Iron deficiency anaemia is less common because of less bleeding
- Increased “good” HDL cholesterol may protect against atherosclerosis (hardened arteries predisposing to heart disease)
- A decrease in the number and size of ovarian cysts occurs in polycystic ovarian syndrome
- Sebum production is reduced by 30%, resulting in worthwhile improvement in 80% of those with seborrhoea
- Acne usually improves by 40-50% by the third cycle and by 80-90% by the ninth cycle.
- More than 40% of women with facial hair (hirsutism) find it improves within 9 months, and many get worthwhile reduction in hair growth elsewhere as well.
Studies have demonstrated that the skin condition continues to improve even after the medication has been taken for a year. Combined oral contraceptives can usually be taken safely for many years.
Unfortunately, the skin condition tends to deteriorate again within a few months after the medication has been stopped.
New forms of oral contraceptive are introduced from time to time, to increase efficacy and reduce side effects.
Oral contraceptives
Oral contraceptives (OCs) have been used for many years by dermatologists as a treatment option for women with acne. The onset of acne is triggered by the production of androgens. Oral contraceptives inhibit ovulation, thereby resulting in the prevention of androgen production. The lower serum androgen levels reduce sebum secretion, which consequentially exerts an antiacne effect. Oral contraceptives (OCs) that are indicated for use in acne are effective across the spectrum of disease severity:
- in mild acne as an adjunct to topical therapy for female patients desiring contraception
- in moderate acne as a form of systemic therapy
- in severe acne
- as a primary form of therapy (e.g., ethinyl estradiol/ cyproterone acetate)
- as one of two preferred forms of contraception for women treated with systemic isotretinoin.
These preparations have evolved to include less estrogen and incorporate progestins with less intrinsic androgenicity in order to reduce the potential risk of thromboembolic events, hepatic tumors, hypertension, altered glucose metabolism, and rare androgenic side-effects such as acne, hirsutism, and weight gain.
Four hormonal preparations are presently approved for the treatment of acne.
- All contain estrogen and progestins
- with minimal androgenicity
- ethinyl estradiol/ norgestimate (Ortho Tri-Cyclen®)
- ethinyl estradiol/ levonorgestrel (Alesse®)
- with anti-androgenic potential
- ethinyl estradiol/ drospirenone (Yasmin®)
- ethinyl estradiol/ cyproterone acetate (Diane-35®)
- with minimal androgenicity
- All have demonstrated efficacy in the treatment of acne and long-term safety profiles.
Ethinyl Estradiol 0.030mg/ Drospirenone 3mg (Yasmin®)
Drospirenone is a novel progestogen derived from spironolactone, which is an antiandrogen.
- Drospirenone 3mg combined with 0.030mg ethinyl estradiol (Yasmin®)
- Recently approved for the treatment of moderate acne.
- Competitively binds to androgen receptors.
- Inhibits 5á-reductase activity, which results in the down regulation of sebum production.
- Reduces androgen biosynthesis.
- For anti-mineralocorticoid activity, the dose equivalence for drospirenone 3mg is spironolactone 25mg.
- Efficacy for treating acne vulgaris was evaluated in a randomized controlled trial with ethinyl estradiol 0.035mg/ cyproterone acetate 2mg as the active comparator 3.
- 125 subjects aged 16-35 years with mild-to-moderate facial acne treated for 9 cycles
- Median reduction in total facial acne lesions:
- 62% for ethinyl estradiol 0.030mg/ drospirenone 3mg (Yasmin®)
- 59% for ethinyl estradiol 0.035mg/cyproterone acetate 2mg (Diane-35®)
- Both formulations were effective for treatment of acne and well tolerated
- Adverse events were mild-to-moderate in intensity and typical of those associated with oral contraceptives.
Ethinyl Estradiol/ Norgestimate (Ortho Tri-Cyclen®)
- Ethinyl estradiol 0.035mg with norgestimate in increasing doses, 0.180mg/ 0.215mg/ 0.250mg
- Norgestimate has low intrinsic androgenicity with low binding affinity for androgen receptors. It is strongly selective and avidly bound to progesterone receptor sites. This combination estrogen and progestin preparation produces a synergistic effect which enhances regulation of hormonal levels.
- Shown to be efficacious in moderate facial acne in two randomized placebo-controlled trials involving 324 subjects over 6 cycles 4; 5.
- Inflammatory lesions were reduced by 56%, noninflammatory lesions by 41%, and 32% achieved excellent improvement using investigator global assessment scores 5.
Ethinyl Estradiol/ Levonorgestrel (Alesse®)
- Ethinyl estradiol 0.020mg and levonorgestrel 100ìg
- Shown to be efficacious for moderate facial acne in two randomized placebo-controlled trials 6.
- A compilation of both studies showed 721 women treated for 6 cycles.
- Significant improvements seen:
- Reduction in acne counts:
- 32%–47% inflammatory
- 13%–25% noninflammatory
- 23%–40% total lesions.
- Reduction in acne counts:
- Investigator global assessment scores were rated as clear to almost clear in 48%-58% of subjects.
Ethinyl Estradiol/ Cyproterone Acetate (Diane-35®)
The combination of ethinyl estradiol 0.035mg and cyproterone acetate 2mg has been available as a hormonal treatment for acne in Canada since 1998.
- Cyproterone acetate is an analogue of hydroxyprogesterone and has progestational activity.
- It also acts as a potent antiandrogen:
- by inhibiting gonadotropin secretion.
- by competitive inhibition of testosterone and dihydrotestosterone (DHT) binding to the androgen receptor.
Efficacious in mild-to-moderate facial acne based on smaller trials with variable study designs and parameters, which produced data that could not be combined for meta analysis 7.
Cyproterone acetate
Higher doses of cyproterone acetate are indicated for more severe cases of androgenetic skin conditions. It is effective for 70% of those with hirsutism.
Several different regimes are prescribed with doses ranging from 25 to 200 mg daily. Prior to the menopause, the medication is usually combined with cyproterone acetate/ethinyloestradiol or other oral contraceptive agent:
- To regulate menstrual cycle irregularities caused by the high dose cyproterone
- To prevent pregnancy; there are concerns that cyproterone could harm a male fetus by “feminising” it.
One system is to take the high dose cyproterone for the first ten days of the cycle.
Postmenopausal women and women who have had a hysterectomy can take cyproterone every day. It may be advisable to have a 7-day break every month. They may also take spironolactone.
Occasional significant side effects include:
- Liver disturbance
- Tiredness and depression
- Weight increase
Ethinyl Estradiol/ Cyproterone Acetate (Diane-35®) should be discontinued in the following circumstances:
- Severe migraine (headache, visual disturbance, numb feelings)
- Any form of thrombosis (such as heart attack, stroke) or increased blood pressure
- In case of immobility (including due to surgery) or trauma (eg bad sprains)
- If an increase in number or severity of epileptic seizures occurs, or liver disease arises during treatment
- Pregnancy
As with other oral contraceptives, minor side effects may arise, especially in the first few weeks. These include:
- Breast tenderness (20%) and increase in bra size
- “Spotting” (irregular mild bleeding between periods) occurs in 10% of women in the first month, but only affects 3% by the sixth month. Rarely, periods may stop altogether (amenorrhoea). If you have spotting (bleeding in between periods), see your doctor. He or she may advise you to take the active medication continuously for 3 months or more. This is quite safe and often prevents unwanted bleeding.
- Nausea, loss of appetite and bloating
- Headaches
- Increased appetite and weight increase (uncommon)
- Mood changes including depression and reduced libido
- Melasma (facial pigmentation)
- Hair loss (it is more common for hair fall to occur when the medication has been discontinued however)
- Acne.
Anti-androgen therapy
Anti-androgen therapy refers to medication taken by women to counteract the effect of male sex hormones such as testosterone on the skin.
- Anti-androgens are not suitable for skin problems in men.
What are anti-androgens used for ?
Anti-androgen medications are used to treat signs of hyperandrogenism, including the following skin and hair disorders:
- Acne
- Seborrhoea
- Hirsutism
- Female pattern hair loss
- Hidradenitis suppurativa
How does anti-androgen therapy work ?
Anti-androgen therapy may:
- Block androgen receptor
- Reduce adrenal androgen production
- Reduce ovarian androgen production
- Reduce pituitary production of prolactin
- Inhibit 5-alpha reductase (this enzyme acts in the skin to increase dihyroxytestosterone)
- Reduce insulin resistance
Which drugs have anti-androgenic action ?
Androgen receptor blockers act on the sebaceous gland and base of the hair follicle. They include:
- Oral contraceptive (birth control pill) containing ethinylestrodiol (oestrogen) and an antiandrogenic progesterone. These include cyproterone acetate (co-cyprindiol or Diane™-35, Estelle™ 35 and Ginet-84™), drospirenone (Yasmin™, Yaz™) or dienogest (Valette™).
- Other low-dose combined oral contraceptives with minimal androgen effect. These contain ethinylestrodiol and desorgestrel, gestodene or norgestimate.
- Spironolactone 25-200 mg daily (Aldactone™, Spirotone™, Spiractin™), which is most useful in women over the age of 30 years.
- Cyproterone acetate 50 to 200 mg (Androcur™, Procur™, Siterone™ – available on prescription). This powerful anti-androgen is usually taken on days 1 to 10 of the menstrual cycle (conventionally, day 1 is the first day of menstruation).
Spironolactone and cyproterone may be effectively combined with cyproterone acetate/ethinyloestradiol or other oral contraceptive agent, partly because they cause menstrual irregularities and partly to prevent pregnancy. The combined treatment is not necessary in post-menopausal women.
What are the clinical effects of anti-androgen therapy ?
In acne, the effects of anti-androgens include:
- Reduced sebum production
- Reduced comedone formation
They can be combined with other topical and oral treatments for acne.
Spironolactone
Spironolactone is a potassium-sparing medication used as a diuretic medication for heart failure, liver disease and high blood pressure. However, it has also been found useful for hirsutism, acne and seborrhoea because it has anti-androgenic properties. Spironolactone mainly works by blocking androgen receptors.
Spironolactone (Aldactone®), at a dose of 100mg daily, works well as an antiandrogen, but must be used in combination with oral contraceptives in women of childbearing age.
Side-effects for Spironolactone are rare but may include menstrual irregularities, breast tenderness, dizziness, and fatigue. Hypokalemia is extremely rare in patients who are not taking concurrent diuretics.
The dose of spironolactone is usually slowly increased from 25 to 200 mg daily, taken at night. It is sometimes prescribed cyclically to reduce menstrual irregularities, eg, for 3 weeks out of every 4 weeks or days 5–21 of the menstrual cycle. It may take six or more months to see improvement in the skin condition.
Side effects of spironolactone include:
- Nausea, diarrhoea, gastrointestinal bleeding
- Drowsiness (possibly due to high blood potassium levels)
- Headache and dizziness
- Menstrual cycle irregularities including increased frequency of menstruation, bleeding in the middle of the month or stopping periods altogether (amenorrhoea)
- Breast pain
Potassium, other electrolytes and creatinine levels in the blood are often monitored. This is especially necessary in older women, if high doses are prescribed, in patients taking other medicines (due to drug interactions) and in those with heart or kidney problems. Spironolactone should not be taken in pregnancy or during lactation.
- Serum potassium should be ≤5.0mmol/L and renal function should be normal before starting spironolactone.
- Monitor potassium and creatinine after one week on spironolactone, monthly for the first 3 months and then 2 to 4 times each year
Spironolactone is prohibited in athletic competition (requires therapeutic use exemption).
Hormonal acne natural treatment
Some natural treatments may be helpful in reducing acne inflammation and breakouts:
Topical treatments
- Tea tree oil. Gels containing at least 5 percent tea tree oil may be as effective as lotions containing 5 percent benzoyl peroxide, although tea tree oil might work more slowly. Possible side effects include minor itching, burning, redness and dryness. Tea tree oil should be used only topically.
- Bovine cartilage. Creams containing 5 percent bovine cartilage, applied to the affected skin twice a day, may be effective in reducing acne.
Oral treatments
- Zinc. The mineral zinc plays a role in wound healing and reduces inflammation, which may help improve acne. It may cause a metallic taste, bloating and diarrhea.
- Brewer’s yeast. A specific strain of brewer’s yeast, called Hansen CBS, seems to help decrease acne when taken orally. It may cause gas (flatulence).
Talk with your doctor about the pros and cons of specific treatments before you try them.
Table 1 summarizes other therapies that are used in the treatment of acne, with varying levels of evidence to support their use.
Table 1. Miscellaneous Therapies for the Treatment of Acne
| Therapy | Evidence |
|---|---|
| Acupuncture | Ah-shi acupuncture is no better than general acupuncture treatment |
| Avoidance of chocolate or sugar consumption | No evidence of effectiveness |
| Biofeedback | May enhance response to medical treatment for acne |
| Chemical peel (glycolic/salicylic acid) | No studies of effectiveness |
| Comedo removal | May help with treatment-resistant comedones and provide short-term reductions in the number of noninflammatory lesions |
| Intralesional steroids | May improve individual large cystic lesions |
| Microdermabrasion | No evidence of effectiveness |
| Tea tree (Melaleuca alternifolia) oil | Effective for total lesion reduction of papules, pustules, and comedones in mild to moderate acne |
- What Causes Acne? http://www.acneguide.ca/basics/acne/what_causes_acne.html[↩]
- Hormonal factors key to understanding acne in women. https://www.aad.org/media/news-releases/hormonal-factors-key-to-understanding-acne-in-women[↩]
- van Vloten WA, et al. Cutis 69(4 Suppl):2-15; 2002 Apr[↩]
- Lucky AW, et al. J Am Acad Dermatol 37(5 Pt 1):746-54;1997 Nov[↩]
- Redmond GP, et al. Obstet Gynecol 89(4): 615-22;1997 Apr[↩][↩]
- Leyden J, et al. J Am Acad Dermatol 47(3):399-409 (2002 Sep); Thiboutot D, et al. Fertil Steril 76(3):461-8; 2001 Sep[↩]
- Tan J. J Cutan Med Surg 8(Suppl 4):11-5;2004 Dec[↩]
- Strauss JS, Krowchuk DP, Leyden JJ, American Academy of Dermatology/American Academy of Dermatology Association, et al. Guidelines of care for acne vulgaris management. J Am Acad Dermatol. 2007;56(4):651–663.[↩]
- Karimipour DJ, Karimipour G, Orringer JS. Microdermabrasion: an evidence-based review. Plast Reconstr Surg. 2010;125(1):372–377.[↩]
- Magin P, Pond D, Smith W, Watson A. A systematic review of the evidence for ‘myths and misconceptions’ in acne management: diet, face-washing and sunlight. Fam Pract. 2005;22(1):62–70.[↩]
- Son BK, Yun Y, Choi IH. Efficacy of ah shi point acupuncture on acne vulgaris. Acupunct Med. 2010;28(3):126–129.[↩]
- Enshaieh S, Jooya A, Siadat AH, Iraji F. The efficacy of 5% topical tea tree oil gel in mild to moderate acne vulgaris: a randomized, double-blind placebo-controlled study. Indian J Dermatol Venereol Leprol. 2007;73(1):22–25.[↩]





{kind=link}