
Contents
What is Hunter syndrome
Hunter syndrome also known as Mucopolysaccharidosis type II or Iduronate sulfatase deficiency, is a very rare inherited genetic disorder caused by a lack of the enzyme iduronate sulfatase (I2S enzyme). Without this enzyme, mucopolysaccharides build up in various body tissues, causing damage. Hunter syndrome affects many different parts of the body and occurs almost exclusively in males. Hunter syndrome occurs in approximately 1 in 100,000 to 1 in 170,000 males. The early-onset, severe form of the disease begins shortly after age 2. A late-onset, mild form causes less severe symptoms to appear later in life.
Hunter syndrome (mucopolysaccharidosis type II) is a progressively debilitating disorder; however, the rate of progression varies among affected individuals.
At birth, individuals with Hunter syndrome do not display any features of the condition. Between ages 2 and 4, they develop full lips, large rounded cheeks, a broad nose, and an enlarged tongue (macroglossia). The vocal cords also enlarge, which results in a deep, hoarse voice. Narrowing of the airway causes frequent upper respiratory infections and short pauses in breathing during sleep (sleep apnea). As the disorder progresses, individuals need medical assistance to keep their airway open.
Many other organs and tissues are affected in Hunter syndrome. Individuals with this disorder often have a large head (macrocephaly), a buildup of fluid in the brain (hydrocephalus), an enlarged liver and spleen (hepatosplenomegaly), and a soft out-pouching around the belly-button (umbilical hernia) or lower abdomen (inguinal hernia). People with Hunter syndrome usually have thick skin that is not very stretchy. Some affected individuals also have distinctive white skin growths that look like pebbles. Most people with this disorder develop hearing loss and have recurrent ear infections. Some individuals with Hunter syndrome develop problems with the light-sensitive tissue in the back of the eye (retina) and have reduced vision. Carpal tunnel syndrome commonly occurs in children with this disorder and is characterized by numbness, tingling, and weakness in the hand and fingers. Narrowing of the spinal canal (spinal stenosis) in the neck can compress and damage the spinal cord. The heart is also significantly affected by Hunter syndrome, and many individuals develop heart valve problems. Heart valve abnormalities can cause the heart to become enlarged (ventricular hypertrophy) and can eventually lead to heart failure.
Children with Hunter syndrome grow steadily until about age 5, and then their growth slows and they develop short stature. Individuals with this condition have joint deformities (contractures) that significantly affect mobility. Most people with Hunter syndrome also have dysostosis multiplex, which refers to multiple skeletal abnormalities seen on x-ray. Dysostosis multiplex includes a generalized thickening of most long bones, particularly the ribs.
There are two types of Hunter syndrome, called the severe and mild types. While both types affect many different organs and tissues as described above, people with severe Hunter syndrome also experience a decline in intellectual function and a more rapid disease progression. Individuals with the severe form begin to lose basic functional skills (developmentally regress) between the ages of 6 and 8.
Hunter syndrome life expectancy
People with the early-onset (severe) form usually live for 10 – 20 years. People with the late-onset (mild) form usually live 20 – 60 years.
Individuals with mild Hunter syndrome also have a shortened lifespan, but they typically live into adulthood and their intelligence is not affected. Heart disease and airway obstruction are major causes of death in people with both types of Hunter syndrome.
Hunter syndrome possible complications
A variety of complications can occur with Hunter syndrome depending on the type and severity of the disease. Complications can affect the lungs, heart, joints, connective tissue, and brain and nervous system.
- Airway obstruction
- Carpal tunnel syndrome
- Hearing loss that gets worse over time
- Loss of ability to complete daily living activities
- Joint stiffness that leads to contractures
- Mental function that gets worse over time
Respiratory complications
An enlarged tongue, thickened gums, and thickening of the nasal passages and windpipe (trachea) make breathing difficult. Children often have chronic ear and sinus infections, respiratory infections, and pneumonia.
Sleep apnea, a condition in which breathing is intermittently interrupted during sleep, is often present because of airway constriction.
Cardiac complications
Thickening of heart tissue can cause improper closing of heart valves. As a result, the heart and other parts of the body don’t receive blood efficiently. As the disease progresses, these conditions often become worse and typically result in heart failure.
The thickening of tissue can also cause narrowing of the aorta (coarctation) and other blood vessels. This in turn can result in high blood pressure (hypertension) and narrowing of arteries in the lungs (pulmonary hypertension).
Skeletal and connective tissue complications
The storage of undigested complex sugar molecules in connective tissues results in abnormalities in bones, joints and ligaments. This reduces your child’s growth, causing pain and physical malformations and making it difficult for him or her to move.
Joint stiffness is caused by swelling of joint connective tissues and abnormalities of cartilage and bones. If your child is in pain, he or she will likely move less, which can lead to more stiffness and pain.
The group of abnormalities typically seen in the bones of people with Hunter syndrome is called dysostosis multiplex. Children with these abnormalities can develop irregularly shaped vertebrae and spines (kyphoscoliosis), ribs, arms, fingers, legs, and pelvises.
Their skulls may press down on or fuse with their upper spines. These complications cause many people with Hunter syndrome to be abnormally short. Those with milder cases may reach normal or near-normal height.
Hernias (inguinal and umbilical) are common in Hunter syndrome. A hernia occurs when soft tissue, usually part of the intestine, pokes through a weak spot or tear in the lower abdominal wall.
Hernias associated with Hunter syndrome can become quite large and are often one of the first signs of the disorder. Enlargement of the liver and spleen (hepatosplenomegaly) may increase pressure in the abdomen, causing a hernia.
Brain and nervous system complications
A variety of neurological complications may be present and continue to develop in children with Hunter syndrome.
Many neurological problems are caused by buildup of excess fluids in your child’s brain (hydrocephalus). Pressure from these fluids can cause other problems that may affect your child’s eyes, ears and other sensory organs, which can cause severe headaches, interfere with vision or hearing and change your child’s mental state.
Your child also may develop a condition in which the membranes that surround the spinal cord may become thick and scarred (hypertrophic cervical pachymeningitis). This causes pressure and compression of the upper spinal cord. As a result, your child may develop fatigue in his or her legs and gradually weaken and become less physically active.
Other disorders, such as carpal tunnel syndrome, can result from nerve compression that happens because of bone deformities and storage of complex sugar molecules in tissues.
Abnormal behavior can develop in children with more-severe cases of Hunter syndrome. Often your child’s mental development will become affected between the ages of 2 and 6. Some children are hyperactive and have trouble paying attention or following directions. Your child may also behave aggressively and seem unable to sense danger. As your child’s overall physical functioning declines, these behavior problems tend to become less severe.
Seizures also may occur in children with Hunter syndrome.
Longer recovery from other illnesses
Recovery times from normal childhood illnesses may be longer for children with Hunter syndrome. As a result, be sure to take general preventive measures — for example, get your child a flu shot and ensure your child receives all necessary vaccinations.
Hunter syndrome causes
Mutations in the IDS gene cause Hunter syndrome. The IDS gene provides instructions for producing the I2S enzyme (iduronate sulfatase), which is involved in the breakdown of large sugar molecules called glycosaminoglycans (GAGs). Glycosaminoglycans were originally called mucopolysaccharides, which is where this condition gets its name. Mutations in the IDS gene reduce or completely eliminate the function of the I2S enzyme (iduronate sulfatase). Lack of I2S enzyme (iduronate sulfatase) activity leads to the accumulation of glycosaminoglycans within cells, specifically inside the lysosomes. Lysosomes are compartments in the cell that digest and recycle different types of molecules. Conditions that cause molecules to build up inside the lysosomes, including Hunter syndrome, are called lysosomal storage disorders. The accumulation of glycosaminoglycans increases the size of the lysosomes, which is why many tissues and organs are enlarged in this disorder. Researchers believe that the glycosaminoglycans may also interfere with the functions of other proteins inside the lysosomes and disrupt the movement of molecules inside the cell.
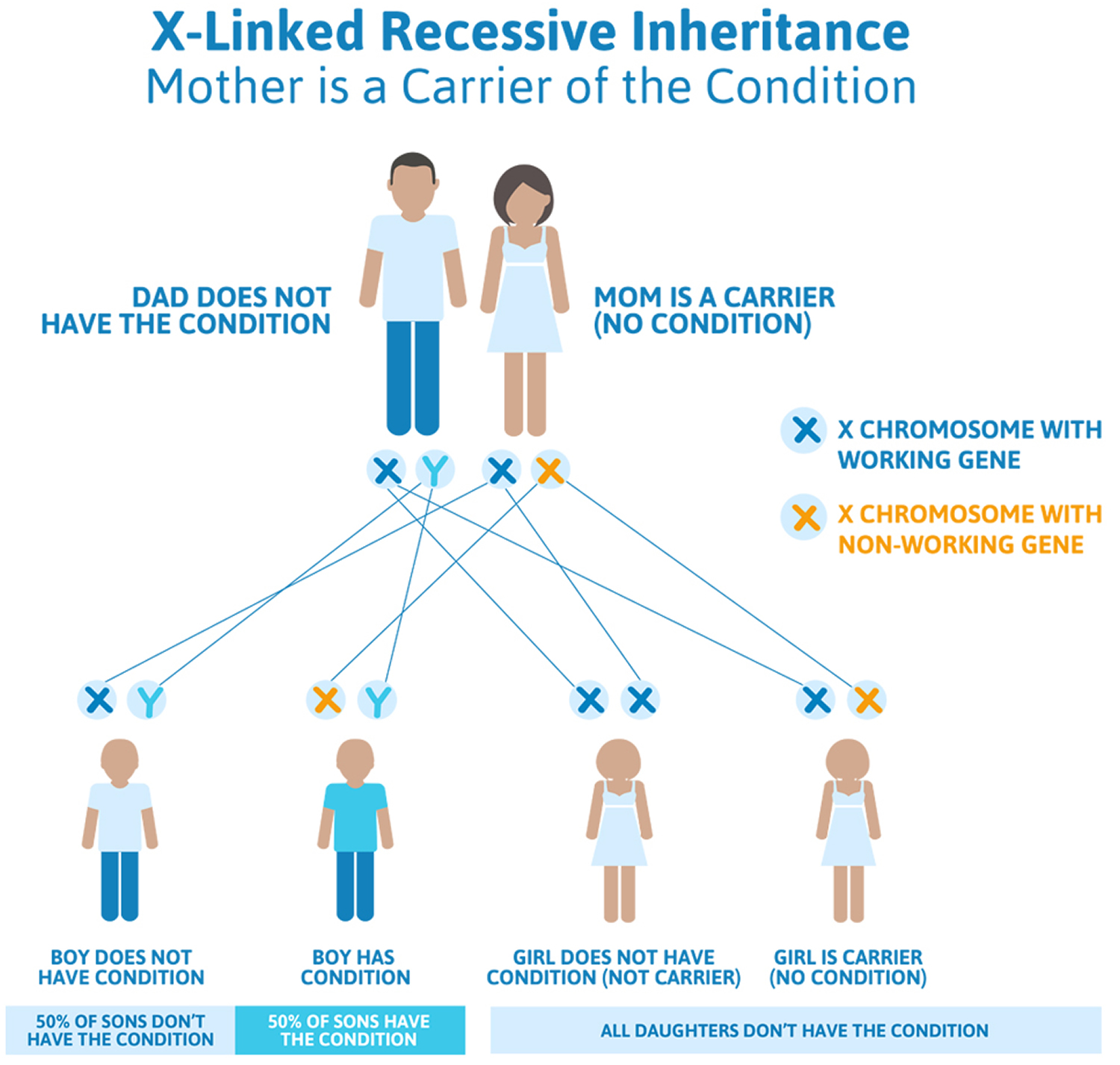
Hunter syndrome is inherited in an X-linked recessive pattern (see Figure 1). The gene associated with this condition is located on the X chromosome, which is one of the two sex chromosomes. In males (who have only one X chromosome), one altered copy of the gene in each cell is sufficient to cause the condition. In females (who have two X chromosomes), a mutation would have to occur in both copies of the gene to cause the disorder. Because it is unlikely that females will have two altered copies of this gene, males are affected by X-linked recessive disorders much more frequently than females. A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons.
A woman who is a carrier of an X-linked recessive disorder has a 25 percent chance of having an unaffected son, a 25 percent chance of having an affected son, a 25 percent chance of having an unaffected daughter and a 25 percent chance of having an unaffected daughter who is also a carrier.
Figure 1. Hunter syndrome X-linked recessive inheritance pattern
Risk factors for developing Hunter syndrome
There are two major risk factors for developing Hunter syndrome:
- Family history. Hunter syndrome is caused by a defective chromosome, and a child must inherit the defective chromosome to develop the disease. Hunter syndrome is what’s known as an X-linked recessive disease. This means that women carry the defective disease-causing X chromosome and can pass it on, but women aren’t affected by the disease themselves.
- Sex. Hunter syndrome nearly always occurs in males. Girls are far less at risk of developing this disease because they inherit two X chromosomes. If one of the X chromosomes is defective, their normal X chromosome can provide a functioning gene. If the X chromosome of a male is defective, however, there isn’t another normal X chromosome to compensate for the problem.
Hunter syndrome prevention
Hunter syndrome is a genetic disorder. Talk to your doctor or a genetic counselor if you’re thinking about having children and you or any members of your family have a genetic disorder or a family history of genetic disorders.
If you think you might be a carrier, genetic tests are available. If you already have a child with Hunter syndrome, you may wish to seek the advice of a doctor or genetic counselor before you have more children.
Hunter syndrome symptoms
Hunter syndrome symptoms vary and range from mild to severe. Symptoms aren’t present at birth, but often begin around ages 2 to 4.
Juvenile form (early-onset, severe form):
- Aggressive behavior
- Hyperactivity
- Mental function gets worse over time
- Severe intellectual disability
- Spasticity
Late (mild) form:
- Mild to no mental deficiency
Both forms:
- Carpal tunnel syndrome
- Coarse features of the face
- Deafness (gets worse over time)
- Increased hair (hypertrichosis)
- Joint stiffness
- Large head (macrocephaly)
Signs of Hunter syndrome include:
- Thickening of the lips
- White skin growths that resemble pebbles
- A protruding tongue
- A broad nose and flared nostrils
- A deep, hoarse voice
- Abnormal bone size or shape and other skeletal irregularities
- Abnormal retina (back of the eye)
- Decreased iduronate sulfatase enzyme in blood serum or cells
- Heart murmur and leaky heart valves
- Enlarged liver (hepatomegaly)
- Enlarged spleen (splenomegaly)
- A distended abdomen, as a result of enlarged internal organs
- Diarrhea
- Inguinal hernia
- Joint contractures
- Spasticity
- Stunted growth
- Delayed development, such as late walking or talking
Hunter syndrome diagnosis
Babies born with Hunter syndrome almost always appear healthy at birth. Changes in facial features are often the first noticeable sign that something’s not right.
Blood, urine or tissue samples can be checked for the deficient enzyme or for excess amounts of the complex sugar molecules associated with this disorder. A genetic analysis can confirm the diagnosis.
Because Hunter syndrome progresses slowly and its signs and symptoms overlap with a number of other disorders, definitive diagnosis may take some time.
Prenatal testing
Prenatal testing of the fluid that surrounds the baby (amniocentesis) or of a tissue sample from the placenta (chorionic villus sampling) can verify if your unborn child carries a copy of the defective gene or is affected with the disorder.
Hunter syndrome treatment
The U.S. Food and Drug Administration has approved the first treatment for Hunter syndrome. The medicine, called idursulfase (Elaprase), is given through a vein (intravenously). Talk to your doctor for more information.
Bone marrow transplant has been tried for the early-onset form, but the results can vary.
Each health problem should be treated separately.
Because there’s no cure for Hunter syndrome, treatment focuses on managing signs, symptoms and complications to provide some relief for your child as the disease progresses.
- Relief for respiratory complications. Removal of tonsils and adenoids can open up your child’s airway and help relieve sleep apnea. But as the disease progresses, tissues continue to thicken and these problems can come back.Breathing devices that use air pressure to keep the airway open — such as continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP) devices — can help with upper airway obstructions and sleep apnea. Keeping your child’s airway open can also help avoid low blood oxygen levels.
- Addressing heart complications. Your child’s doctor will want to watch closely for cardiovascular complications, such as high blood pressure, heart murmur and leaky heart valves. If your child has severe cardiovascular problems, your doctor may recommend surgery to replace heart valves.
- Treatment for skeletal and connective tissue problems. Because most children with Hunter syndrome don’t heal well and often have complications after surgery, options are limited for addressing skeletal and connective tissue complications. For example, surgery to stabilize the spine using internal hardware is difficult when bones are fragile.Your child’s joint flexibility can be improved with physical therapy, which helps address stiffness and maintain function. However, physical therapy can’t stop the progressive decline of joint motion. Your child may eventually need to use a wheelchair because of pain and limited stamina.
Surgery can repair hernias, but because of weakness in connective tissues, results usually aren’t ideal. The procedure often needs to be repeated. One option is to manage your child’s hernias with supportive trusses rather than surgery because of the risks of anesthesia and surgery.
- Managing neurological complications. Problems associated with the buildup of fluid and tissue around the brain and spinal cord are difficult to address because of the inherent risks in treating these parts of the body.Your child’s doctor may recommend surgery to drain excess fluids or remove built-up tissue. If your child has seizures, your doctor may prescribe anticonvulsant medications.
- Managing behavioral problems. If your child develops abnormal behavior as a result of Hunter syndrome, providing a safe home environment is one of the most important ways you can manage this challenge.Treating behavior problems with medications has had limited success because most medications have side effects that can make other complications of the disease, such as respiratory problems, even worse.
- Addressing sleep issues. The sleep patterns of a child with Hunter syndrome become more and more disorganized. Medications including sedatives and especially melatonin can improve sleep.Keeping a strict bedtime schedule and making sure your child sleeps in a well-darkened room also can help. In addition, creating a safe environment in your child’s bedroom — putting the mattress on the floor, padding the walls, removing all hard furniture, placing only soft, safe toys in the room — may help you rest easier if you know your child has less opportunity for injury.
Emerging treatments
Some treatments that are in their early stages of development have had some success by slowing the disease’s progress and lessening its severity.
- Enzyme therapy. This treatment uses man-made or genetically engineered enzymes to replace your child’s missing or defective enzymes and ease the disease symptoms. This treatment is given once a week through an intravenous (IV) line.Given early enough, enzyme replacement therapy may delay or prevent some of the symptoms of Hunter syndrome. It’s unclear, however, if the improvements seen with this therapy are significant enough to raise quality of life for people with the disease. In addition, benefits in thinking and intelligence haven’t been seen with enzyme replacement therapy.
Serious allergic reactions can occur during enzyme replacement therapy. Other possible side effects include headache, fever, skin reactions and high blood pressure. Side effects tend to lessen over time, however.
- Gene therapy. Replacing the chromosome responsible for producing the missing enzyme could theoretically cure Hunter syndrome, but much more research is needed before this therapy will be available.
Coping and support
Joining a support group for parents of children with Hunter syndrome can be a great way to obtain practical information, daily living strategies and encouragement from other parents in similar situations to your own. Ask your doctor if there’s a group in your area.
The intense supervision that may be needed for your child can cause you and other caregivers to become physically, mentally and emotionally exhausted. If respite care is available, take advantage of it so that you can have a break and be more effective in the long run to meet the day-to-day challenges of caring for your child.
Check with your county and state for resources that may be available to you as a parent of a child with special needs.
Letting others know
Due to a narrow airway, people with Hunter syndrome often have difficulty receiving a breathing tube (being intubated) during general anesthesia. You may wish to note this on child care or school forms so that emergency personnel can be alerted to this fact, in case your child has an emergency and you’re not there. An experienced anesthesia specialist (anesthesiologist) should perform the intubation of a person with Hunter syndrome.





{kind=link}