Contents
What is hydrocele
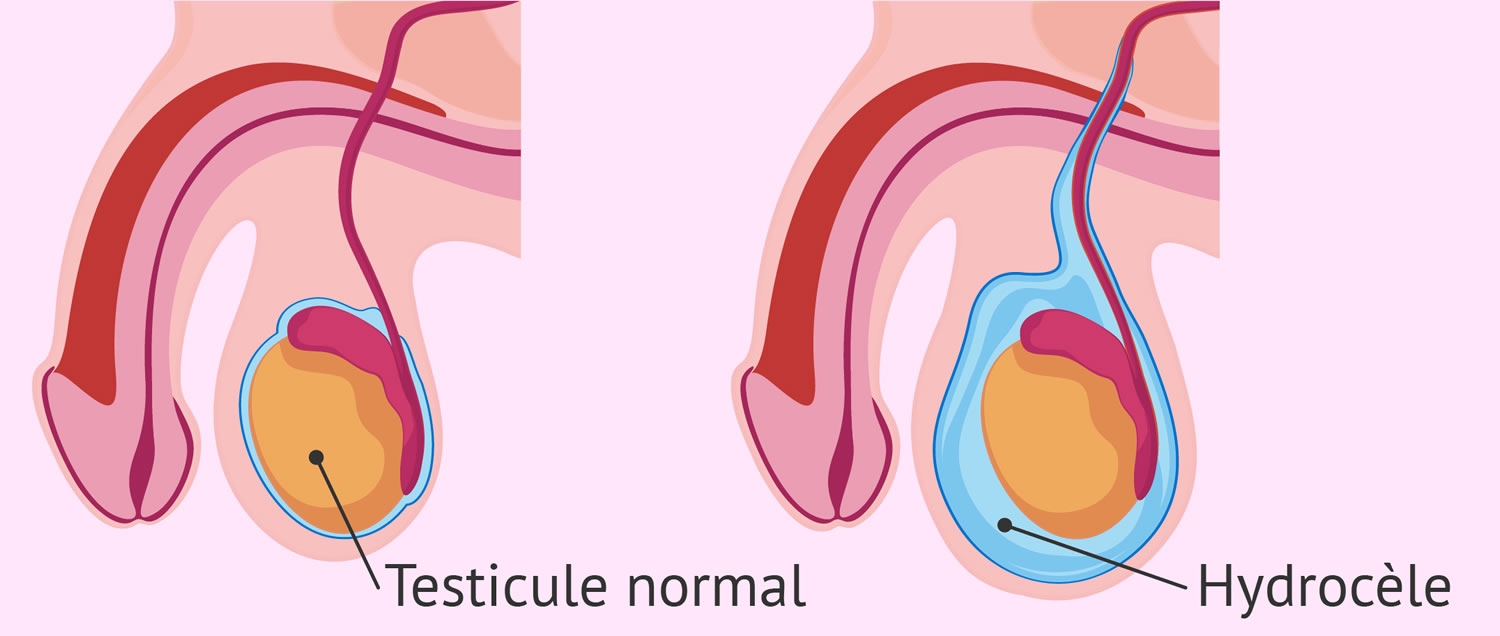
Hydroceles are common cystic scrotal abnormalities, described as a fluid‐filled collection around the testicles, between the visceral and parietal layers of the tunica vaginalis of the scrotum. Hydrocoeles are responsible for most painless scrotal swellings 1. Hydrocele is common in newborns and usually disappears without treatment by age 1. Older boys and adult men can develop a hydrocele due to inflammation or injury within the scrotum. The typical hydrocele is observed at or shortly after birth as a unilateral or bilateral swelling in the scrotum, which may fluctuate in size 2. The scrotum appears enlarged with fluid; it may be very tense, is usually non-tender and is often, bluish in color. The inguinal canal is normal. Although most hydroceles will transilluminate, a fluid- or gas-filled bowel may transilluminate as well, especially in infants. Elective referral to a pediatric surgeon is advised.
During a baby’s development in the womb, the testicles descend from the abdomen through a tube into the scrotum. Hydroceles occur when this tube does not close. Fluid drains from the abdomen through the open tube and gets trapped in the scrotum. This causes the scrotum to swell.
Most hydroceles go away a few months after birth. Sometimes, a hydrocele may occur with an inguinal hernia.
Hydroceles may also be caused by:
- Buildup of the normal fluid around the testicle. This may occur because the body makes too much of the fluid or it does not drain well. (This type of hydrocele is more common in older men.)
- Swelling or injury of the testicle or epididymis
The recommended management of a hydrocele is observation during the first one to two years of a child’s life, unless the diagnosis of a hernia cannot be excluded. Hydroceles that persist or appear beyond that age are unlikely to resolve spontaneously and should, therefore, undergo elective surgical repair.
See your doctor if you or your child experiences scrotal swelling. It’s important to rule out other causes of the swelling that might require treatment. For example, a hydrocele might be associated with a weak point in the abdominal wall that allows a loop of intestine to extend into the scrotum (inguinal hernia).
A baby’s hydrocele typically disappears on its own. But if your baby’s hydrocele doesn’t disappear after a year or if it enlarges, ask your child’s doctor to examine the hydrocele again.
Get immediate medical treatment if you or your child develops sudden, severe scrotal pain or swelling, especially within several hours of an injury to the scrotum. These signs and symptoms can occur with a number of conditions, including blocked blood flow in a twisted testicle (testicular torsion). Testicular torsion must be treated within hours of the beginning of signs and symptoms to save the testicle.
Although most hydroceles do not require therapeutic intervention, there are two approaches for treatment of hydrocoeles: surgical open hydrocoelectomy and aspiration followed by sclerotherapy. Surgical open hydrocelectomy is considered to be the current therapeutic standard 3. An alternative approach is percutaneous aspiration followed by sclerotherapy. Aspiration without sclerotherapy carries a significant risk of hydrocele recurrence 4. Aspiration and sclerotherapy for the management of hydroceles involves aspirating the hydrocele and then injecting a sclerosing solution into the hydrocele sac. This solution fuses the visceral and parietal layers of the tunica vaginalis, obliterating the potential space for reformation of the hydrocele 5.
Postoperative complications as well as cost and time to work resumption were less in the aspiration and sclerotherapy group; however the recurrence rate was higher. The cure rate in short-term follow-up was similar between the two groups – aspiration and sclerotherapy group and open surgery group.
A hydrocele usually isn’t painful or harmful and might not need any treatment. But if you have scrotal swelling, see your doctor to rule out other causes.
Figure 1. Testis (normal)
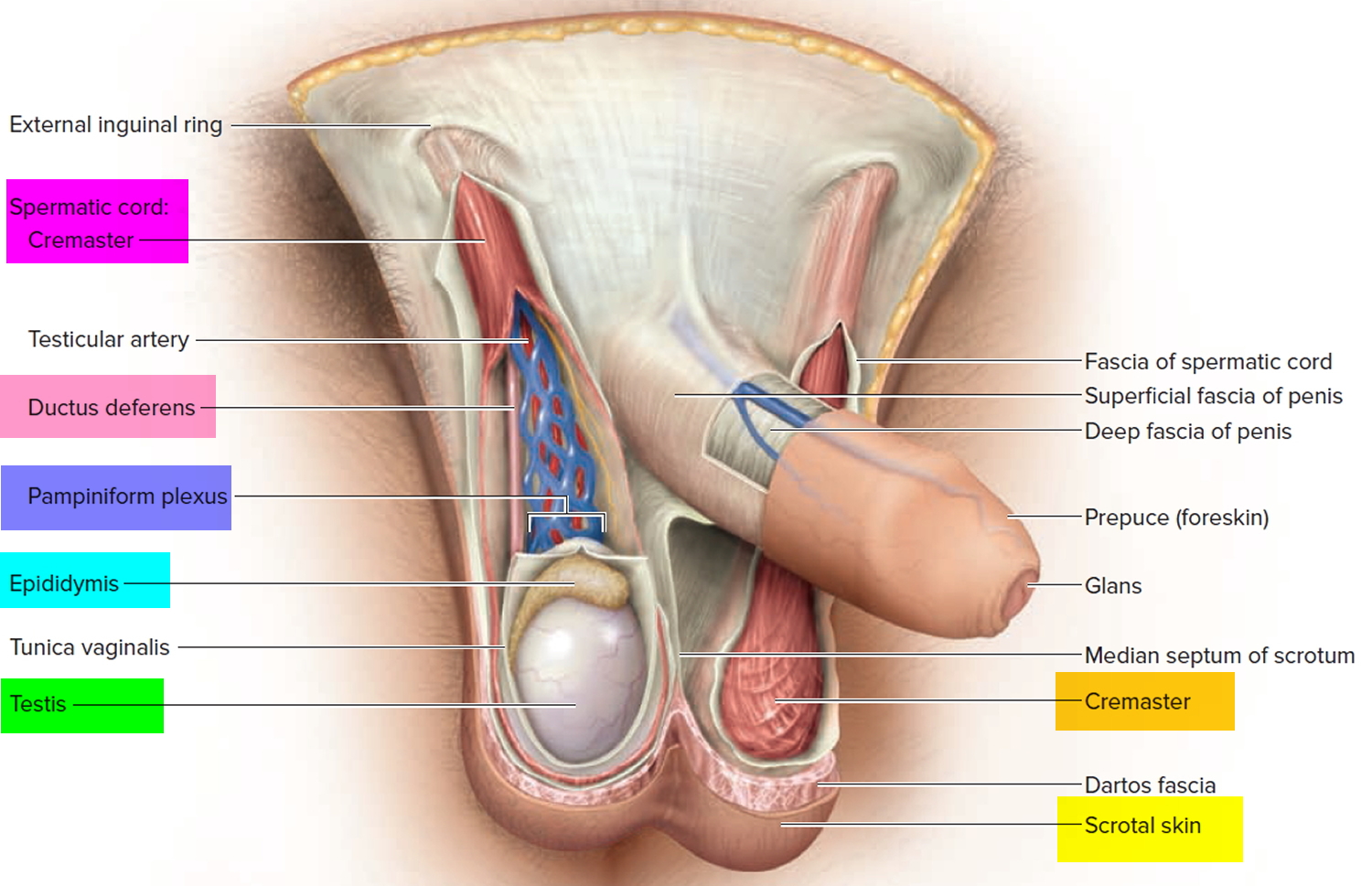 Figure 3. Testicle anatomy (normal)
Figure 3. Testicle anatomy (normal)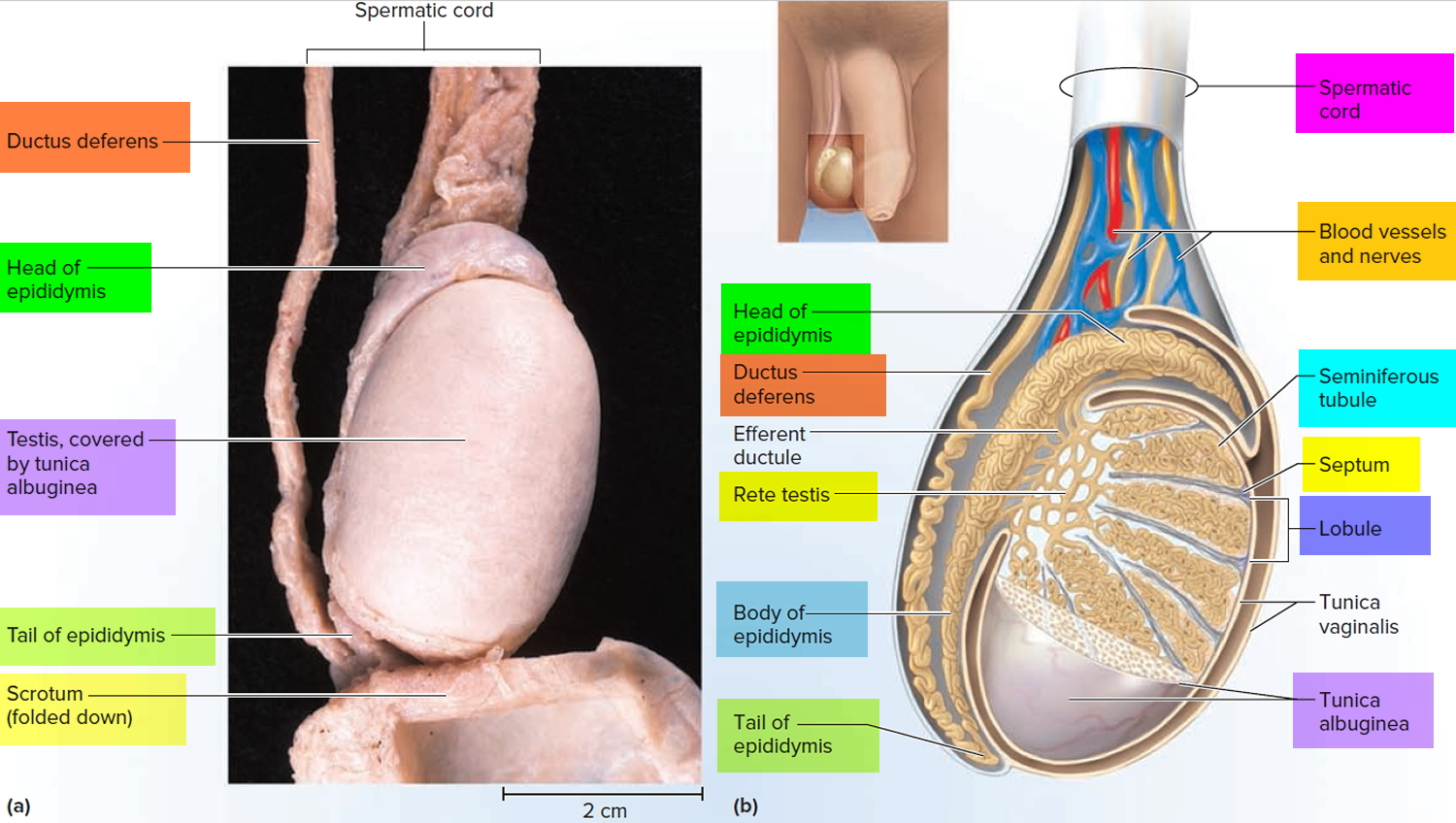
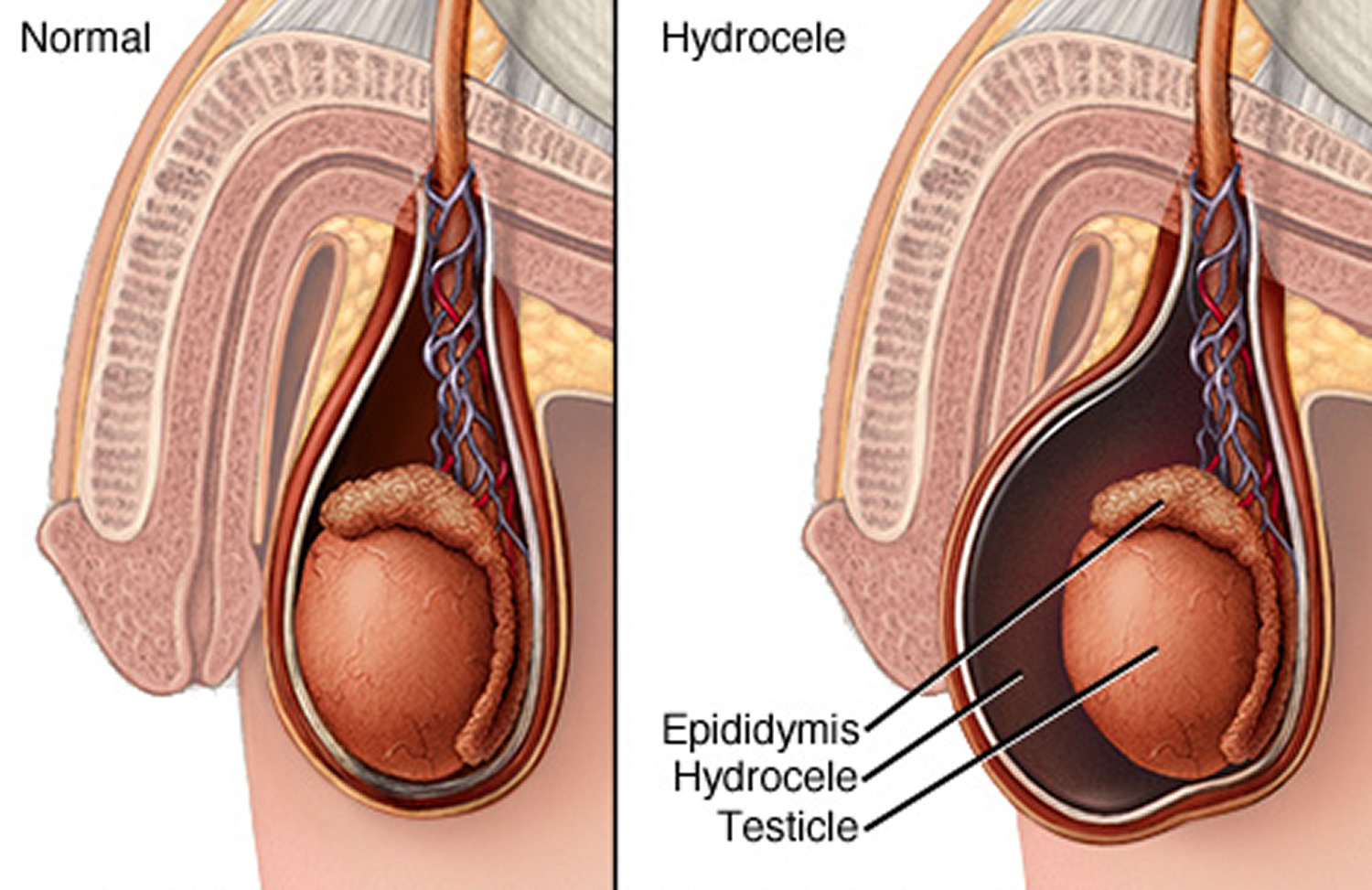
Figure 3. Hydrocele
See a doctor if you have:
- a lump in your testicles
- swollen testicles
- a change in the shape of your testicles
- a change in the way your testicles feel
- one testicle that’s become bigger than the other
- aching or discomfort in your testicles that doesn’t go away
Lumps in the testicles can be a sign of testicular cancer. This is easier to treat if it’s found early.
Pain in the scrotum or testicles is an emergency. If you have pain and your scrotum is enlarged, seek medical help right away to prevent the loss of the testicle.
Go to the emergency room if you get sudden, unbearable pain in your testicles or tummy
This could be caused by your testicle becoming twisted, which needs to be treated in hospital as soon as possible.
Hydrocele hernia
A infant inguinal hernia is usually a protrusion of intra-abdominal contents through a patent processus vaginalis. The processus vaginalis is an outpouching of the peritoneum through the internal inguinal ring, which normally closes spontaneously following testicular descent. Incomplete obliteration of the processus vaginalis may result in an abnormal communication between the abdominal cavity and the inguinal region. The congenital hernia of infancy and childhood is not a ‘rupture’ or a muscle weakness, and it should not be referred to as such.
Hernias occur in 1% to 4% of all infants; the incidence may reach 30% in premature infants (depending on the child’s gestational age at birth). One third of all children with hernias present before six months of age 6.
Most hernias occur in males, with a male to female ratio of 6:1. Correct recognition and initiation of the proper therapeutic route are essential for an excellent outcome, which should approach 100% success.
Most children present with a history of intermittent swelling in the inguinal region, which in males, may extend to the scrotum. The presence of a mass or thickening in the inguinal canal, or at the level of the internal inguinal ring is diagnostic. The swelling is usually nontender and readily reducible with gentle pressure.
Figure 4. Inguinal hernia
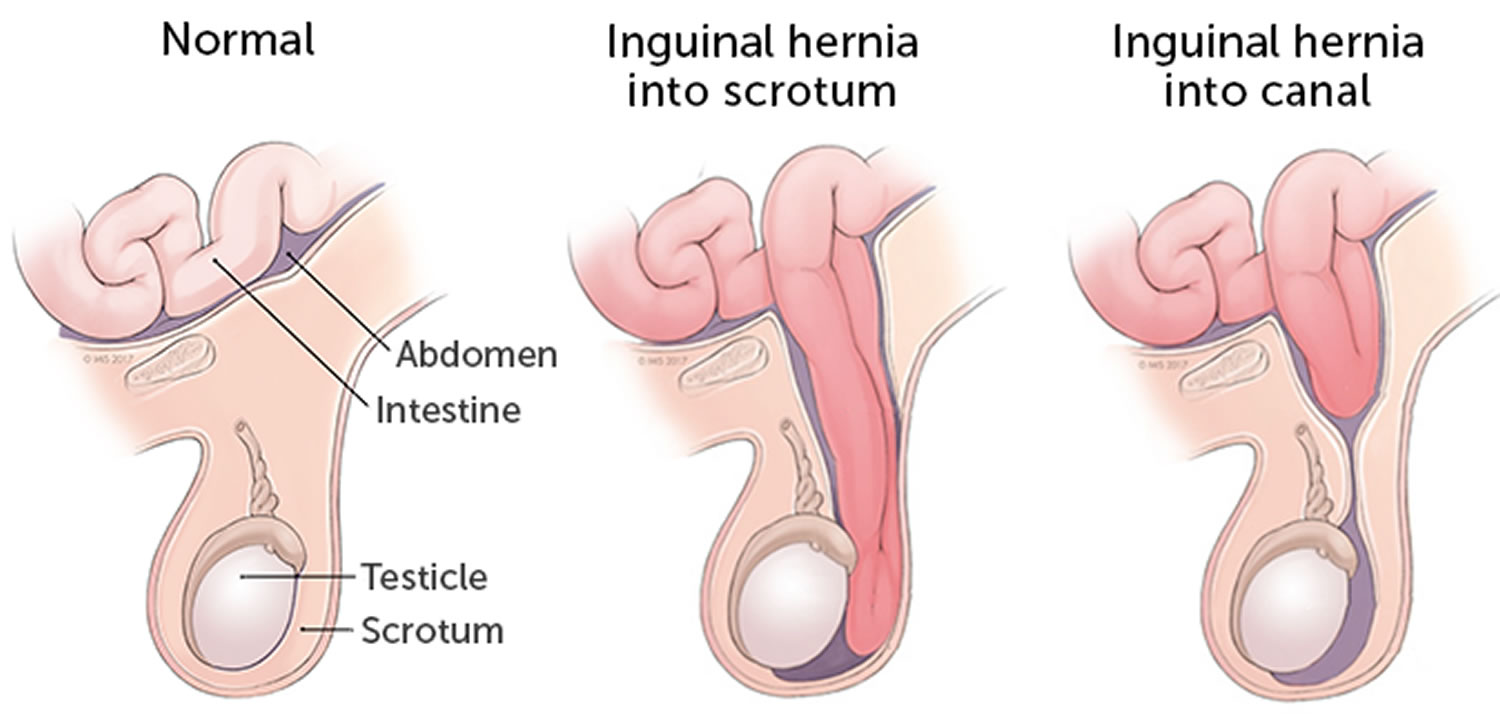
Inguinal hernia symptoms
Most inguinal hernias are diagnosed by either a parent who notices a bulge when a child is straining or crying, or by a physician during a routine physical examination. Some discomfort may be present because many infants with hernias are ‘fussy’; the discomfort resolves after repair. In males, it is important to verify that the testicle is in the scrotum; the bulge of an undescended or retractile testicle may mimic an inguinal hernia.
The differential diagnosis for uncomplicated inguinal hernias includes hydrocele and lymphadenopathy. In these cases, however, the inguinal canal will feel entirely normal 7.
Inguinal hernia treatment
A pediatric inguinal hernia will not close spontaneously, and it must be repaired. While repair is not a surgical emergency, prompt referral to a pediatric surgeon is recommended.
Most inguinal hernia repairs in full term, healthy infants and older children may be performed electively in an outpatient setting soon after the diagnosis is made. Infants younger than one year of age, particularly former preterm infants, are at greater risk for an incarcerated hernia. Repairs in preterm infants should be carried out as soon as it is convenient, preferably within one week of diagnosis. After surgery, overnight hospitalization may be necessary to monitor postoperative apnea in preterm infants and children with special needs (e.g, with a ventriculo-peritoneal shunt, cardiopulmonary disease) 8.
There is significant controversy concerning contralateral inguinal exploration. While a contralateral patent process is found in about 40% of children, the actual risk of a metachronous (occurring or starting at different times) hernia is estimated to be 10% to 15%, with reports ranging from 1% to 34% 6. Consequently, opinions vary widely between performing contralateral exploration in all females and young males or only in cases when a contralateral hernia is clinically suspected.
Few complications should occur following elective hernia repairs. In addition to the usual wound infections and bleeding problems, specific complications may include hernia recurrence, testicular atrophy and injury to the vas deferens (all of the above occur in less than 1% of children). Scrotal swelling is frequent in small infants, with resolution occurring by six months after surgery.
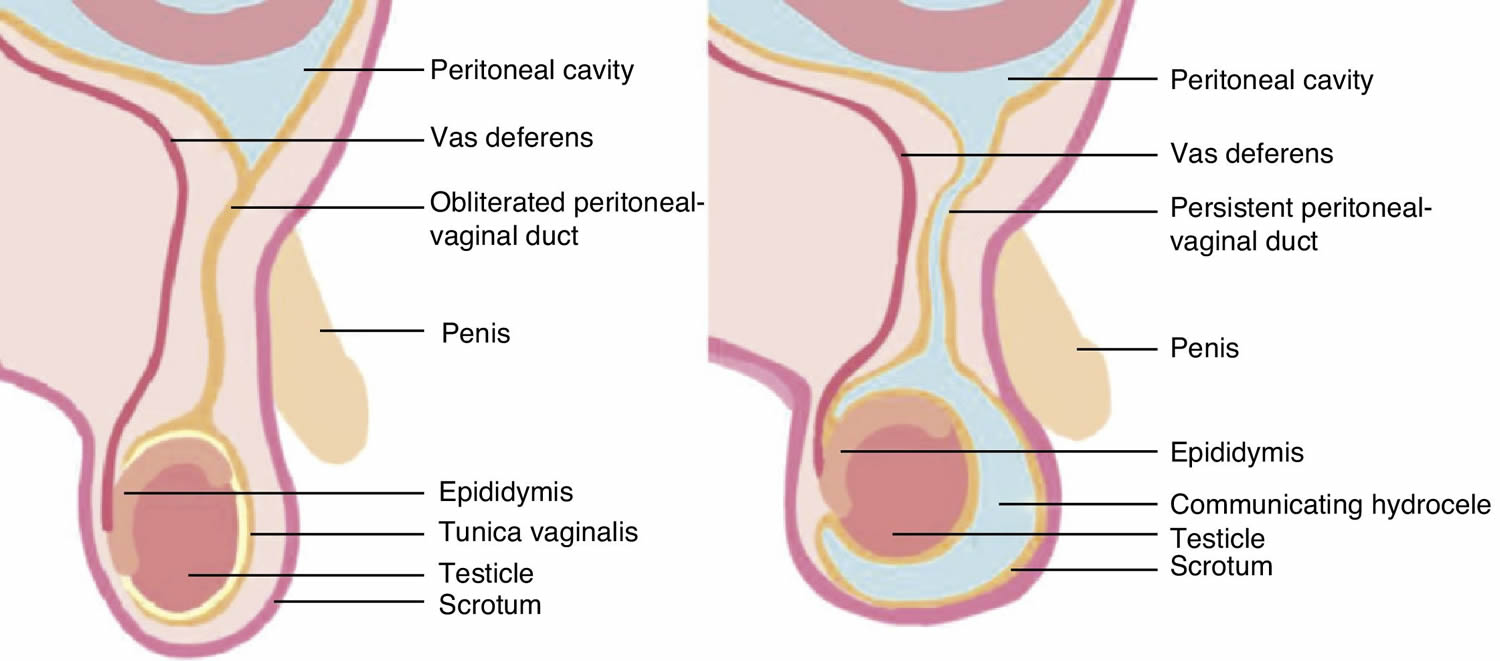
Communicating hydrocele
If the opening between the abdominal cavity and the scrotum has not closed properly and completely, abdominal fluid will pass into the sac around the testis, causing a mass called a communicating hydrocele. As many as half of all newborn boys have this problem; however, it usually disappears within one year without any treatment. Although most common in newborns, hydroceles also can develop later in childhood, most often with a hernia.
If your son has a hydrocele, he probably will not complain, but you or he will notice that one side of his scrotum is swollen. In an infant or young boy, this swelling decreases at night or when he is resting or lying down. When he gets more active or is crying, it increases, then subsides when he quiets again. Your pediatrician may make the final diagnosis by shining a bright light through the scrotum, to show the fluid surrounding the testicle. Your doctor also may request an ultrasound examination of the scrotum if it is very swollen or hard.
If your baby is born with a hydrocele, your pediatrician will examine it at each regular checkup until around one year of age. During this time your child should not feel any discomfort in the scrotum or the surrounding area. But if it seems to be tender in this area or he has unexplained discomfort, nausea, or vomiting, call the doctor at once. These are signs that a piece of intestine may have entered the scrotal area along with abdominal fluid. If this occurs and the intestine gets trapped in the scrotum, your child may require immediate surgery to release the trapped intestine and close the opening between the abdominal wall and the scrotum.
If the hydrocele persists beyond one year without causing pain, a similar surgical procedure may be recommended. In this operation, the excess fluid is removed and the opening into the abdominal cavity closed.
Figure 5. Communicating hydrocele
Hydrocele causes
Hydroceles are either congenital or acquired, and can present in any age group, from neonates to the elderly 9. Accumulation of fluid resulting from communication between the tunica vaginalis and the peritoneal cavity leads to formation of congenital hydroceles. Acquired hydroceles are most commonly idiopathic, although they can occur secondary to intrascrotal infections, regional or systemic diseases, inguinal or scrotal surgery, or neoplasms 10. The prevalence of idiopathic hydrocele in adult male population is unclear but some experts reported the incidence of hydrocele to be 1% in adult male population in USA 11.
Hydrocele in infants
A hydrocele can develop before birth. Normally, the testicles descend from the developing baby’s abdominal cavity into the scrotum. A sac accompanies each testicle, allowing fluid to surround the testicles. Usually, each sac closes and the fluid is absorbed.
Sometimes, the fluid remains after the sac closes (noncommunicating hydrocele). The fluid is usually absorbed gradually within the first year of life. But occasionally, the sac remains open (communicating hydrocele). The sac can change size or if the scrotal sac is compressed, fluid can flow back into the abdomen. Communicating hydroceles are often associated with inguinal hernia.
Hydrocele in adults
A hydrocele can develop as a result of injury or inflammation within the scrotum. Inflammation might be caused by an infection in the testicle or in the small, coiled tube at the back of each testicle (epididymitis).
Risk factors for hydrocele
Most hydroceles are present at birth. At least 5 percent of newborn boys have a hydrocele. Babies who are born prematurely have a higher risk of having a hydrocele.
Risk factors for developing a hydrocele later in life include:
- Injury or inflammation to the scrotum
- Infection, including a sexually transmitted infection (STI)
Hydrocele symptoms
Usually, the only indication of a hydrocele is a painless round-oval shaped swelling of one or both testicles, which feels like a water balloon. A hydrocele may occur on one or both sides. However, the right side is more commonly involved.
The scrotum is swollen, but not painful to the touch. Often, the testicle cannot be felt because of the fluid around it. The size of the fluid-filled sac can sometimes be increased and decreased by putting pressure on the abdomen or the scrotum.
If the size of the fluid collection changes, it is more likely to be due to an inguinal hernia.
Hydroceles can be easily seen by shining a flashlight through the swollen part of the scrotum. If the scrotum is full of clear fluid, the scrotum will light up.
Adult men with a hydrocele might experience discomfort from the heaviness of a swollen scrotum. Pain generally increases with the size of the inflammation. Sometimes, the swollen area might be smaller in the morning and larger later in the day.
Hydrocele complications
A hydrocele typically isn’t dangerous and usually doesn’t affect fertility. But a hydrocele might be associated with an underlying testicular condition that can cause serious complications, including:
- Infection or tumor. Either might reduce sperm production or function.
- Inguinal hernia. The loop of intestine trapped in the abdominal wall can lead to life-threatening complications.
Hydrocele diagnosis
Your doctor will start with a physical exam. It’s likely to include:
- Checking for tenderness in an enlarged scrotum.
- Applying pressure to the abdomen and scrotum to check for inguinal hernia.
- Shining a light through the scrotum (transillumination). If you or your child has a hydrocele, transillumination will show clear fluid surrounding the testicle.
After that, your doctor might recommend:
- Blood and urine tests to help determine if you or your child has an infection, such as epididymitis
- Ultrasound to help rule out hernia, testicular tumor or other causes of scrotal swelling
- CT scan to confirm the diagnosis.
Hydrocele treatment
In baby boys, a hydrocele sometimes disappears on its own, but not in adults. Most hydroceles in infants will go away by the time they are 2 years old. But for males of any age, it’s important for a doctor to evaluate a hydrocele because it can be associated with an underlying testicular condition. Hydroceles from an inguinal hernia should be fixed with surgery as soon as possible.
A hydrocele that doesn’t disappear on its own might need to be surgically removed, typically as an outpatient procedure. The surgery to remove a hydrocele (hydrocelectomy) can be done under general or regional anesthesia. An incision is made in the scrotum or lower abdomen to remove the hydrocele. If a hydrocele is found during surgery to repair an inguinal hernia, the surgeon might remove the hydrocele even if it’s causing no discomfort.
After hydrocelectomy, you might need a tube to drain fluid and a bulky dressing for a few days. Your doctor is likely to recommend a follow-up examination because a hydrocele might recur.
Hydrocele repair
Hydrocele repair is surgery to correct the swelling of the scrotum that occurs when you have a hydrocele. Baby boys sometimes have a hydrocele at birth. Hydroceles also occur in older boys and men. Sometimes they form when there is also a hernia (an abnormal bulging of tissue) present. Hydroceles are fairly common.
Your surgeon may recommend hydrocele repair if the hydrocele:
- Becomes too large
- Causes problems with blood flow
- Is infected
- Is painful or uncomfortable
The repair may also be done if there is a hernia associated with the problem.
Surgery to repair a hydrocele is often done at an outpatient clinic. General anesthesia is used so you will be asleep and pain-free during the procedure.
In a baby or child:
- The surgeon makes a small surgical cut in the fold of the groin, and then drains the fluid. The sac (hydrocele) holding the fluid may be removed. The surgeon strengthens the muscle wall with stitches. This is called a hernia repair.
- Sometimes the surgeon uses a laparoscope to do this procedure. A laparoscope is a tiny camera that the surgeon inserts into the area through a small surgical cut. The camera is attached to a video monitor. The surgeon makes the repair with small instruments that are inserted through other small surgical cuts.
In adults:
The cut is most often made on the scrotum. The surgeon then drains the fluid after removing part of the hydrocele sac.
Needle drainage of the fluid is not done very often because the problem will always come back.
Risks of hydrocele surgery
Risks for any anesthesia are:
- Allergic reactions to medicines
- Breathing problems
Risks for any surgery are:
- Bleeding
- Infection
- Blood clots
- Recurrence of the hydrocele
- Injury to the scrotum
- Loss of the testicle
- Long-term (chronic) pain
- Continuous swelling
Before the hydrocele repair
Always tell your health care provider what drugs you are taking, even drugs, supplements, or herbs you bought without a prescription. Also tell your provider if you have any drug allergies or if you have had bleeding problems in the past.
Several days before surgery, adults may be asked to stop taking aspirin or other drugs that affect blood clotting. These include ibuprofen (Motrin, Advil), naproxen (Naprosyn, Aleve), some herbal supplements, and others.
You or your child may be asked to stop eating and drinking at least 6 hours before the procedure.
Take the medicines you have been told to take with a small sip of water.
After the hydrocele repair
Recovery is quick in most cases. Most people can go home a few hours after surgery. Children should limit activity and get extra rest in the first few days after surgery. In most cases, normal activity can start again in about 4 to 7 days.
Hydrocele repair outlook (prognosis)
The success rate for hydrocele repair is very high. The long-term outlook is excellent. However, another hydrocele may form over time, or if there was also a hernia present.
- Micallef M, Torreggiani WC, Hurley M, Dinsmore WW, Hogan B. The ultrasound investigation of scrotal swelling. International Journal of STD and AIDS 2000;11(5):297-302. https://www.ncbi.nlm.nih.gov/pubmed/10824938[↩]
- Sonnino RE. Hydroceles. In: Reece R, editor. Manual of Emergency Pediatrics. 4th edn. Philadelphia: WB Saunders Company; 1992. p. 261.[↩]
- Beiko DT, Kim D, Morales A. Aspiration and sclerotherapy versus hydrocelectomy for treatment of hydroceles. Urology 2003;61(4):708-12. https://www.ncbi.nlm.nih.gov/pubmed/12670550[↩]
- Roosen JU, Larsen T, Iversen E, Berg JB. A comparison of aspiration, antazoline sclerotherapy and surgery in the treatment of hydrocele. British Journal of Urology 1991;68(4):404-6. https://www.ncbi.nlm.nih.gov/pubmed/1933162 [↩]
- Shan CJ, Lucon AM, Arap S. Comparative study of sclerotherapy with phenol and surgical treatment for hydrocele. Journal of Urology 2003;169(3):1056-9. https://www.ncbi.nlm.nih.gov/pubmed/12576845[↩]
- Lloyd DA, Rintal RJ. Inguinal hernia and hydrocele. In: O’Neill JA, Rowe MI, Grosfeld JL, Fonkalsrud EW, Coran AG, editors. Pediatric Surgery. 5th edn. St Louis: Mosby; 1998. pp. 1071–86.[↩][↩]
- Rescorla FJ. Hernias and umbilicus. Surgery of Infants and Children: Scientific Principles and Practice. In: Oldham K, Colombani P, Foglia R, editors. Philadelphia: Lippincott-Raven Publishers; 1997. pp. 1069–76.[↩]
- Steward DJ. Preterm infants are more prone to complications following minor surgery than are term infants. Anesthesiology. 1982;56:304–6. https://www.ncbi.nlm.nih.gov/pubmed/7065438[↩]
- Epstein A, Novicki D. Management of hydroceles. American Urological Association (AUA) Update Series 1988; Vol. VII lesson 19:145-9.[↩]
- Rubenstein RA, Dogra VS, Seftel AD, Resnick MI. Benign intrascrotal lesions. Journal of Urology 2004;171(5):1762-72.[↩]
- Rudkin SE, Kazzi AA. Hydrocele in emergency medicine. http://emedicine.medscape.com/article/777386-overview[↩]





{kind=link}