Contents
- Hypertriglyceridemia
- Table 1. Hypertriglyceridemia definition
- What’s the difference between triglycerides and cholesterol?
- Hypertriglyceridemia causes
- Hypertriglyceridemia pathophysiology
- Hypertriglyceridemia symptoms
- Hypertriglyceridemia diagnosis
- Hypertriglyceridemia treatment
- Hypertriglyceridemia prognosis
Hypertriglyceridemia
Hypertriglyceridemia also called elevated plasma triglyceride concentration, refers to a fasting plasma triglyceride above 150 to 199 mg/dL (1.7 to 2.2 mmol/L) in adults, typically above the 95th percentile for age and sex, although additional quantitative or qualitative lipoprotein abnormalities can also be present 1, 2. Triglycerides are a type of fat called lipid that circulate in your blood. Triglycerides are the most common type of fat in your body. Triglycerides come from foods, especially butter, oils, and other fats you eat. Triglycerides also come from extra calories your body does not need right away. Unused calories (energy you don’t need right away) are stored as triglycerides in fat cells, thus triglycerides is a major source of energy for your body. When your body needs energy, it releases the triglycerides. In between meals, triglycerides are released from fat tissue to be used as an energy source for your body. Most triglycerides are carried in the blood by lipoproteins called very low-density lipoproteins (VLDL). Some triglycerides are important for good health. However, high triglyceride levels in your blood or hypertriglyceridemia can raise your risk of heart disease and stroke. How severe hypertriglyceridemia is can vary based on sex, age, hormone use, and dietary factors. Hypertriglyceridemia can result from a variety of causes. Mild to moderate hypertriglyceridemia occurs commonly as part of the metabolic syndrome, can be the result of multiple genetic mutations in an individual or family and can be secondary to several diseases and drugs 3. High smoking rates, excessive drinking, and high prevalence of obesity and abdominal obesity in middle-aged men appear to contribute to elevated triglycerides levels 4, 5. On the other hand, decreased metabolic effects of estrogen around menopause and the increased visceral adiposity (fat around your abdomen) could be related to increasing hypertriglyceridemia prevalence in older-aged women 6. Among medical conditions contributing to hypertriglyceridemia, obesity and uncontrolled diabetes mellitus are the most common causes 7. Obesity and diabetes are commonly characterized by insulin resistance, and elevated triglycerides worsen atherosclerosis in people with insulin resistance 8. Due to the increased intake of processed food, excess nutrients, and the increase in sedentary lifestyle, obesity prevalence has increased substantially over the last couple of decades worldwide 9. The prevalence of hypertriglyceridemia is increasing among youth and adolescents due to increasing rates of obesity and diabetes mellitus 10.
The National Health Survey in China 11, the US 12, Russia 13 and Thailand 14 reported the prevalence of hypertriglyceridemia (fasting plasma Triglyceride ≥ 150 mg/dL) among adults aged 20 years, accounting for 13.1, 25.9, 29.2 and 36.0%, respectively. The incidence of hypertriglyceridemia is higher among Mexican-Americans as compared to white Americans and lowest in African-Americans 15.
Your doctor will usually check for high triglycerides as part of a cholesterol test, which is sometimes called a lipid panel or lipid profile. You’ll have to fast before blood can be drawn for an accurate triglyceride measurement.
For adults, triglyceride levels results are categorized as follows:
- Normal: Less than 150 mg/dL (less than 1.7 mmol/L)
- Mild high: 150 to 199 mg/dL (1.7-2.2 mmol/L)
- Moderate high: 200 to 999 mg/dL (2.3-11.3 mmol/L)
- Severe high: 1,000 to 1,999 mg/dL (11.3-22.6 mmol/L)
- Very severe: Greater than 2,000 mg/dL (more than 22.6 mmol/L)
Note: For improved metabolic health and protection to the heart and blood vessels, the American Heart Association now recommends an optimum fasting triglyceride level of 100 mg/dL (1.12 mmol/L). This puts an even stronger emphasis on lifestyle change which has been the recommended therapy for mildly elevated triglycerides. However, the American Heart Association does not recommend people use drug therapy to achieve this optimal level because there has not been adequate study to show that drug therapy to lower triglycerides to this level is helpful. Many people will be able to reduce their triglycerides as well as other metabolic risk factors such as elevated blood sugar and elevated blood pressure with diet, weight loss and increased physical activity.
For children, teens and young adults:
- From newborn to age 9
- Acceptable: Less than 75 mg/dL (0.85 mmol/L)
- Borderline high: 75-99 mg/dL (0.85-1.12 mmol/L)
- High: Greater than 100 mg/dL (1.13 mmol/L)
- For ages 10-19 years
- Acceptable: Less than 90 mg/dL (1.02 mmol/L)
- Borderline high: 90-129 mg/dL (1.02-1.46 mmol/L)
- High: Greater than 130 mg/dL (1.47 mmol/L)
- For young adults older than 19
- Acceptable: Less than 115 mg/dL (1.30 mmol/L)
- Borderline high: 115-149 mg/dL (1.30-1.68 mmol/L)
- High: Greater than 150 mg/dL (1.7 mmol/L)
When triglycerides are very high (greater than 1000 mg/dL (11.30 mmol/L)), there is a risk of developing pancreatitis in children and adults. Treatment to lower triglycerides should be started as soon as possible.
Note: These values are based on fasting triglyceride levels.
Serum triglycerides are higher in men than in women 16. Serum triglycerides increase with age in both genders. In youth and adolescents, with increasing obesity rates, the prevalence of hypertriglyceridemia is increasing as well. In the National Health and Nutrition Examination Survey 1999 through 2004, about a third of participants had serum triglycerides above 150 mg/dL 16. In subjects aged 60 years or older, prevalence was 42%. Two percent of subjects with hypertriglyceridemia had triglycerides of more than 500 mg/dL. The incidence of hypertriglyceridemia also varies by race, with a higher incidence in Hispanic-Americans and Asian-Indians, and lower incidence in African-Americans who generally have lower triglyceride levels.
The serum triglyceride level reflects the concentration of the triglyceride-rich lipoproteins (VLDL and chylomicrons). VLDL (very-low-density lipoprotein) and chylomicrons become relatively cholesterol-enriched once the triglyceride core is hydrolyzed at peripheral tissues. It appears that remnant triglyceride-rich lipoproteins, as opposed to very large triglyceride-rich lipoproteins, may be atherogenic. Although triglyceride itself is not found in atherosclerotic plaques, it is thought that the cholesterol content of triglyceride-rich lipoproteins may contribute to plaque development. Also, the lipolysis of triglyceride-rich lipoproteins produces free fatty acids, lysolecithin, and other reactive lipids that may have pro-inflammatory and pro-coagulant effects.
The plasma level of triglyceride is a well-established independent biomarker of cardiovascular disease risk 17 and triglyceride-rich lipoproteins have atherogenic properties. Triglyceride predicts cardiovascular disease in a wide range of circumstances. Its association with cardiovascular disease risk is partly attenuated by adjustment for HDL cholesterol, with which it is moderately correlated 18.
Genetic variation associated with lifelong low triglyceride levels is associated with a lower incidence of cardiovascular disease 19. Triglyceride is carried primarily within large lipoproteins, chylomicrons, and VLDL (very low density lipoprotein), which are also rich in cholesterol and like LDL can enter the arterial wall and stimulate atherosclerosis. These triglyceride-rich lipoproteins carry various atherogenic proteins such as apolipoprotein C-III, itself associated with atherosclerosis and cardiovascular disease 20.
Replacing 1% of daily energy intake from saturated fat with polyunsaturated or monounsaturated fat lowers triglyceride by 0.9 or 0.4 mg/dL 21 perhaps more in those with hypertriglyceridemia 22.
Replacing the 1% saturated fat with 1% carbohydrates raises serum triglycerides by ≈1 mg/dL. Dietary carbohydrates raise plasma triglyceride levels by increasing the production by the liver of triglycerides and subsequent incorporation into VLDL (very low density lipoprotein) 22. The magnitude that dietary carbohydrates increase plasma triglyceride is similar whether the carbohydrate has a high or low glycemic index 23.
Most often, having high triglycerides has no warning signs or symptoms. Levels above 150mg/dl (1.7 mmol/L) may raise your risk for heart disease. A triglyceride level of 150 mg/dL (1.7 mmol/L) or higher is also a risk factor for metabolic syndrome. Above 2,000 mg/dL (22.58 mmol/L) poses a high risk for pancreatitis [inflammation of the pancreas]. Triglycerides are the most common type of fat in your body and triglycerides store excess energy (calories) from your diet, thus triglycerides is a major source of energy for your body. Triglycerides is stored in your body’s fat (adipose) cells and is also found in foods such as dairy products, meat and cooking oils. Some triglycerides circulate in your blood to provide fuel for muscles to work. After a person eats, an increased level of triglycerides is found in the blood as the body converts the excess calories (energy you don’t need right away) into fat. Triglycerides move via the blood from the gut to adipose (fat) tissue for storage. In between meals, triglycerides are released from fat tissue to be used as an energy source for your body. Most triglycerides are carried in the blood by lipoproteins called very low-density lipoproteins (VLDL).
If you are diabetic and your blood sugar (glucose) is out of control, your triglycerides may be very high.
Certain drugs such as corticosteroids, protease inhibitors for HIV, beta blockers, and estrogens can increase blood triglyceride levels.
Triglycerides change dramatically in response to meals, increasing as much as 5 to 10 times higher than fasting levels just a few hours after eating. Even fasting levels vary considerably day to day. Therefore, modest changes in fasting triglycerides measured on different days are not considered to be abnormal.
Normal triglyceride levels vary by age and sex. Triglycerides normally increase with age.
Also, many people with high triglycerides have other lipid problems or other risk factors for heart disease. A high triglyceride level is one part of the metabolic syndrome, a cluster of risk factors that increase the risk for heart disease and diabetes. People with high triglycerides often have a high total cholesterol level, including a high LDL (bad) cholesterol level and a low HDL (good) cholesterol level. Many people with heart disease or diabetes also have high triglyceride levels.
The management of hypertriglyceridemia is by a multidisciplinary team that includes an endocrinologist, gastroenterologist, internist, primary care provider, nurse practitioner and a cardiologist. Appropriate management of the patient with hypertriglyceridemia requires knowledge of the likely cause of the hypertriglyceridemia, in order to prevent its complications. Although current guidelines agree that a triglyceride level of less than 150 mg/dL is desirable, the number varies in definitions of hypertriglyceridemia and recommendations concerning management. Besides pharmacological therapy the key is lifestyle changes. This includes dietary changes, for example, the reducing your carbohydrate intake, avoidance of sugar-sweetened beverages and processed carbohydrates, along with exercise and weight loss, is the foundation in managing hypertriglyceridemia. Weight loss of 5% to 10% can reduce triglycerides by about 20%, and regular aerobic exercise can reduce triglycerides by 10% to 20%. Even with all the controversy surrounding dietary fat, a mono-unsaturated fatty acid rich Mediterranean-type diet has been shown in many studies to reduce postprandial (after meal) lipemia (high blood fat). In the setting of triglyceride levels above 500 mg/dL, dietary fat restriction becomes important to avoid post prandial rise in chylomicrons to levels that increase risk of pancreatitis. Addressing the underlying cause and secondary contributors is important. Quitting alcohol, and improving glycemic control in patients with diabetes, is effective in improving secondary components of hypertriglyceridemia. In patients with triglycerides of more than 500 mg/dL, the primary goal is to reduce triglycerides levels to triglycerides the risk of pancreatitis. In patients with mild to moderate elevations in triglycerides (200 mg/dL to 500 mg/dL), the focus should be on preventing cardiovascular disease. For cardiovascular risk reduction, the goal should be to reduce non-HDL cholesterol level down to 30 mg/dL above LDL goal. Those who remain compliant with lifestyle changes and medications have a good outcome with fewer complications 24.
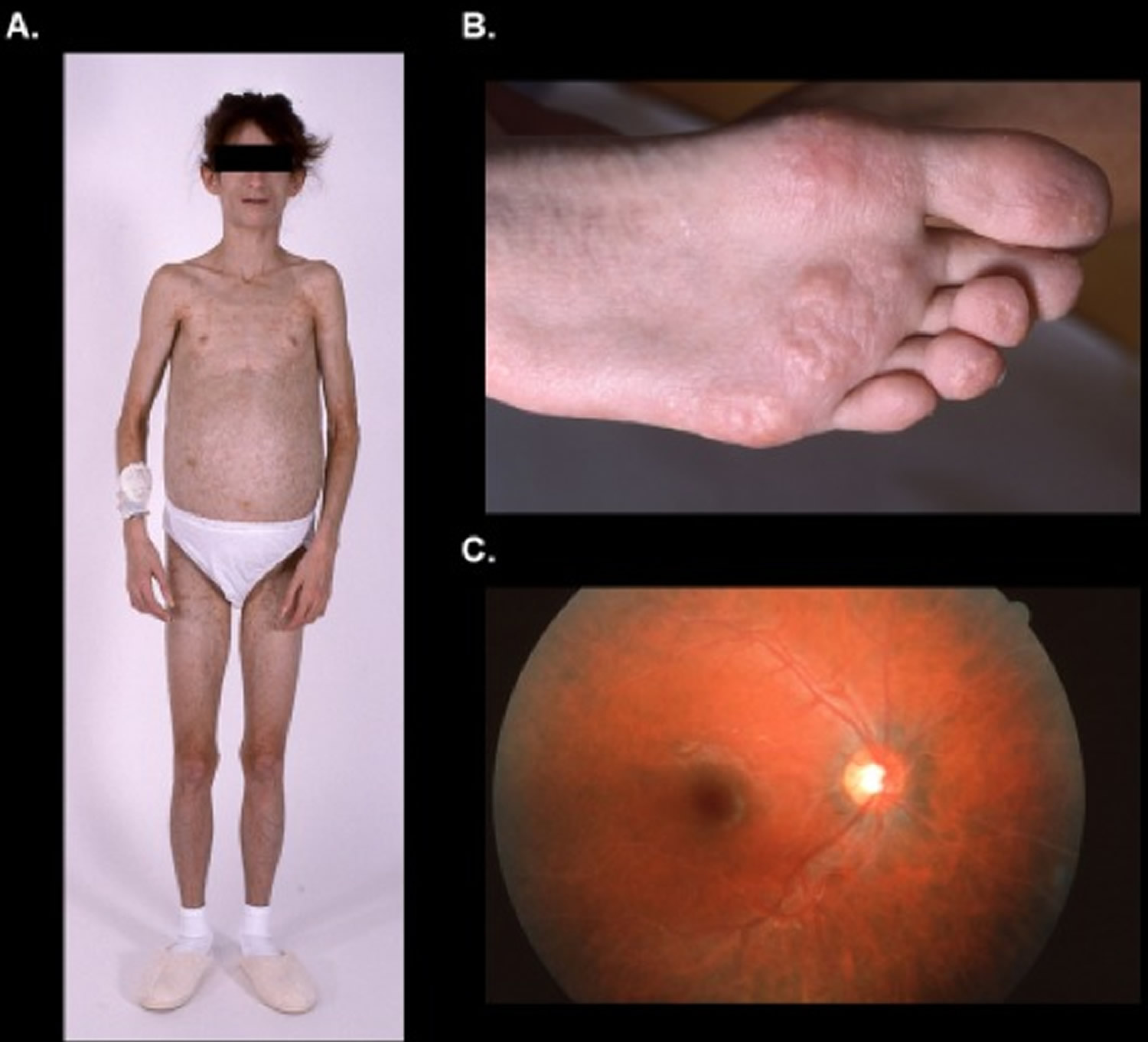
Figure 1. Hypertriglyceridemia
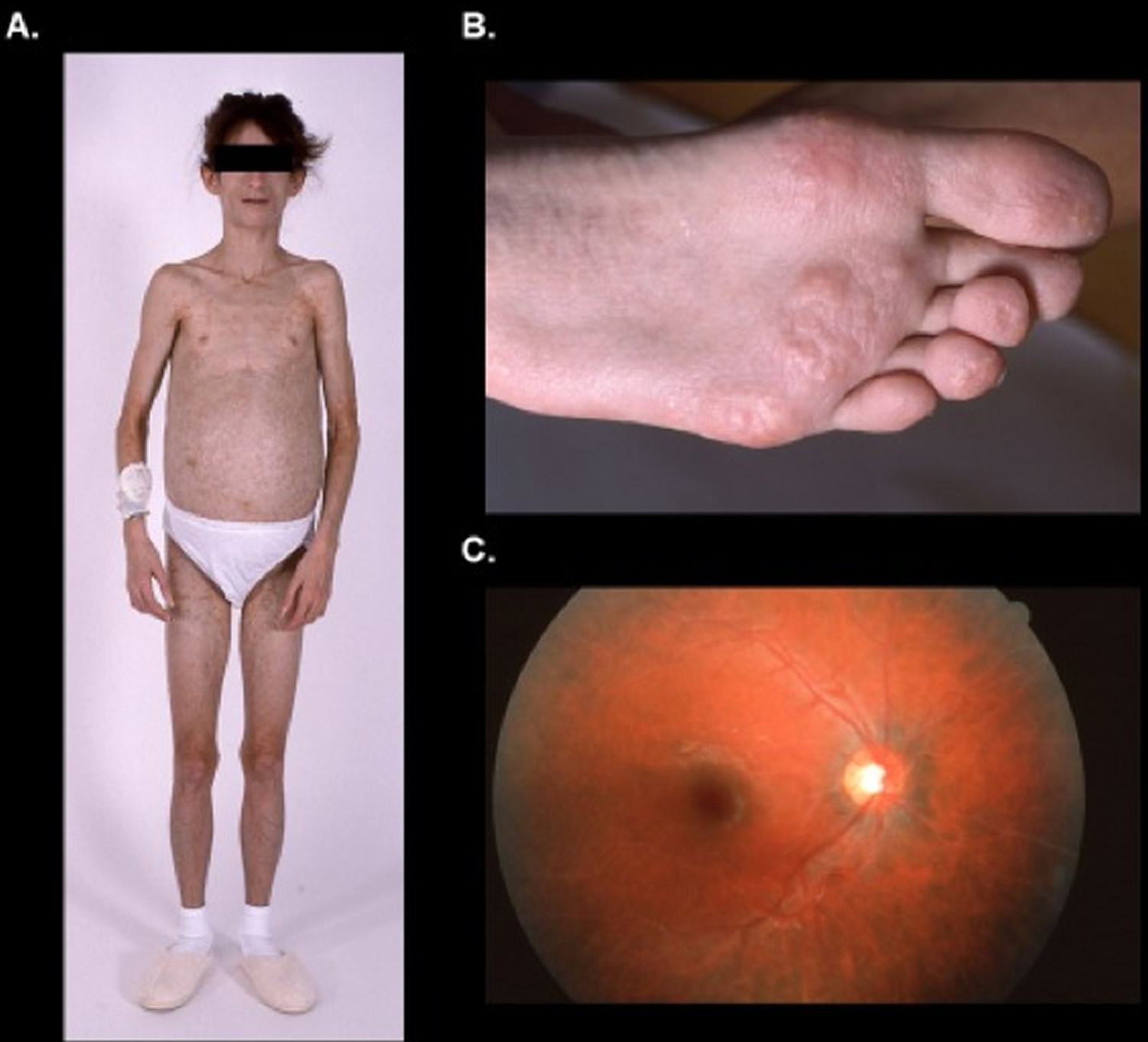
Footnote: (A) Generalized lack of subcutaneous fat, (B) eruptive xanthomas, and (C) lipemia retinalis secondary to severe hypertriglyceridemia in a patient with heterozygous LMNA p.T10I pathogenic mutation.
[Source 25 ]Figure 2. Eruptive xanthomas

Footnote: (Panels A and B) Eruptive xanthomas associated with hypertriglyceridemia and new-onset type 2 diabetes. A previously healthy, 38-year-old man with a family history of early cerebrovascular accidents presented with a sudden eruption of pink papules with creamy-colored centers on his arms and upper torso. He was otherwise asymptomatic and had no abdominal pain. The results of laboratory tests performed while the patient was fasting included a total cholesterol level of 1268 mg per deciliter (32.8 mmol per liter), a total triglyceride level of 8869 mg per deciliter (100.1 mmol per liter), a glucose level of 241 mg per deciliter (13.4 mmol per liter), and a glycosylated hemoglobin value of 13.4 percent. Triglyceride-lowering therapy with gemfibrozil was initiated to enhance lipoprotein lipase activity, and insulin therapy was initiated to treat the hyperglycemia. Twenty-four hours later, his total triglyceride level was 6466 mg per deciliter (73.0 mmol per liter). At follow-up visits three and five months later, the patient’s eruptive xanthomas had decreased in size and number. After eight months of treatment with gemfibrozil, glyburide, and glucophage, his total cholesterol level was 218 mg per deciliter (5.6 mmol per liter), his total triglyceride level was 302 mg per deciliter (3.4 mmol per liter), and his glycosylated hemoglobin value was 8.3 percent; the eruptive xanthomas had completely resolved.
[Source 26 ]Figure 3. Triglyceride
Figure 4. Triglyceride (TG) lipoprotein metabolism
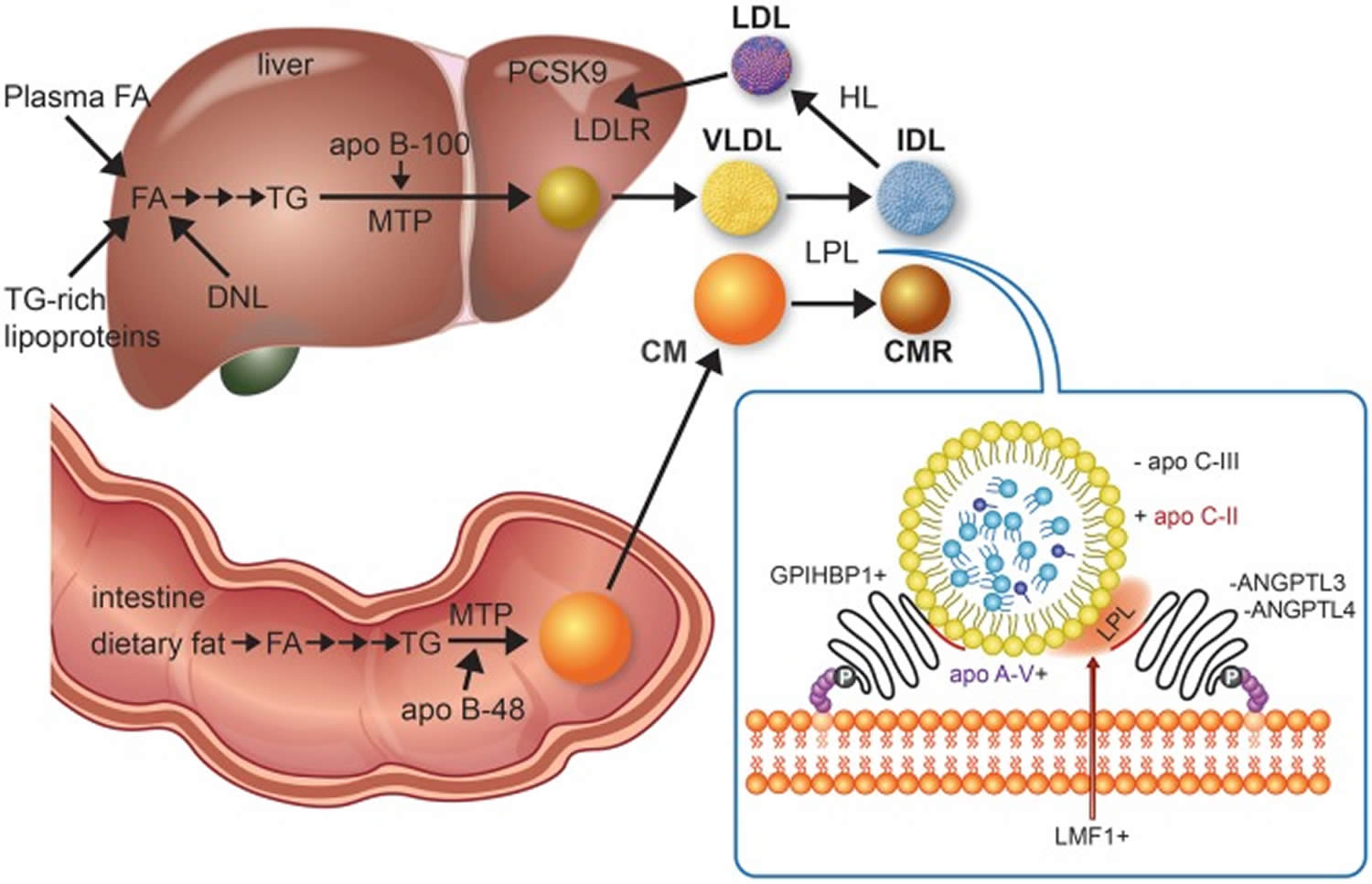
Footnotes: Triglyceride-rich lipoproteins (TRLs), such as chylomicron (CM), very low-density lipoprotein (VLDL), and their remnant particles assembly begins with triglyceride synthesis, which derive from fatty acids in the intestine from the diet or in the liver taken up from plasma, fatty acids released from lysosomes after breakdown of endocytosed triglyceride-rich lipoproteins, and fatty acids generated from glucose by de novo lipogenesis. Plasma triglyceride levels are regulated by the balance of synthesis, lipoprotein lipase (LPL)-mediated hydrolysis, and hepatic remnant clearance 27. Microsomal triglyceride transfer protein unites triglyceride, cholesterol, and phospholipids, with tissue-specific isoforms of apolipoprotein (apo) B, i.e. small B-48, shortened as a result of RNA editing in enterocytes and full-length B-100 in hepatocytes, forming chylomicrons and very-low-density lipoprotein, respectively. Chylomicrons formation also requires Sar1 homolog B GTPase (SAR1B gene product, not shown). Chylomicrons enter plasma indirectly through lymphatics while very-low-density lipoprotein is secreted directly into the circulation. Hydrolysis of circulating chylomicrons and very-low-density lipoprotein by lipoprotein lipase releases free fatty acids and produce chylomicron remnant clearance and intermediate-density lipoprotein particles, respectively. Chylomicrons remnant clearance by the liver (not shown) requires apo E, as apo B-48 does not have the low-density lipoprotein receptor binding domain. Intermediate-density lipoprotein can also be removed by the liver (not shown) with apo B-100 and apo E both acting as ligands for the low-density lipoprotein receptor. Intermediate-density lipoprotein can be further lipolyzed by lipoprotein lipase and also remodelled by hepatic lipase to generate low-density lipoprotein, which is cleared by the low-density lipoprotein receptor, whose activity is reduced by proprotein convertase subtilisin kexin 9. The inset depicts lipoprotein lipase activity on a triglyceride-rich lipoprotein particle as well as several interacting proteins at the endothelial surface that affect lipoprotein lipase activity. A plus sign indicates enhancement or stimulation of lipolysis, whereas a minus sign indicates inhibition. Lipase maturation factor 1 (LMF1) is a chaperone protein that ensures that lipoprotein lipase attains functionality and is properly secreted from adipose cells or myocytes. Glycosylphosphatidylinositol-anchored high-density lipoprotein binding protein-1 (GPIHBP1) is necessary for transcytosis of lipoprotein lipase across the endothelium of capillaries in adipose and muscle tissues as well as tethering lipoprotein lipase to the endothelium, thereby stabilizing it. Apo C-II activates lipoprotein lipase, while apo A-V is a stabilizing cofactor. Lipolysis is reduced by apo C-III, which is a component of triglyceride-rich lipoproteins, and by angiopoietin-like proteins 3 and 4 (ANGPTL3 and ANGPTL4), which both operate near the endothelium. Volanesorsen and AKCEA-APOCIII-LRx reduce triglyceride by targeting apo C-III, while evinacumab and IONIS-ANGPTL3-LRx lower triglyceride by targeting ANGPTL3. Peroxisome proliferator-activated receptors (not shown), particularly alpha and delta types, form a regulatory network that influences several of the above target molecules.
[Source 28 ]Figure 5. Hypertriglyceridemia diagnostic and treatment algorithm
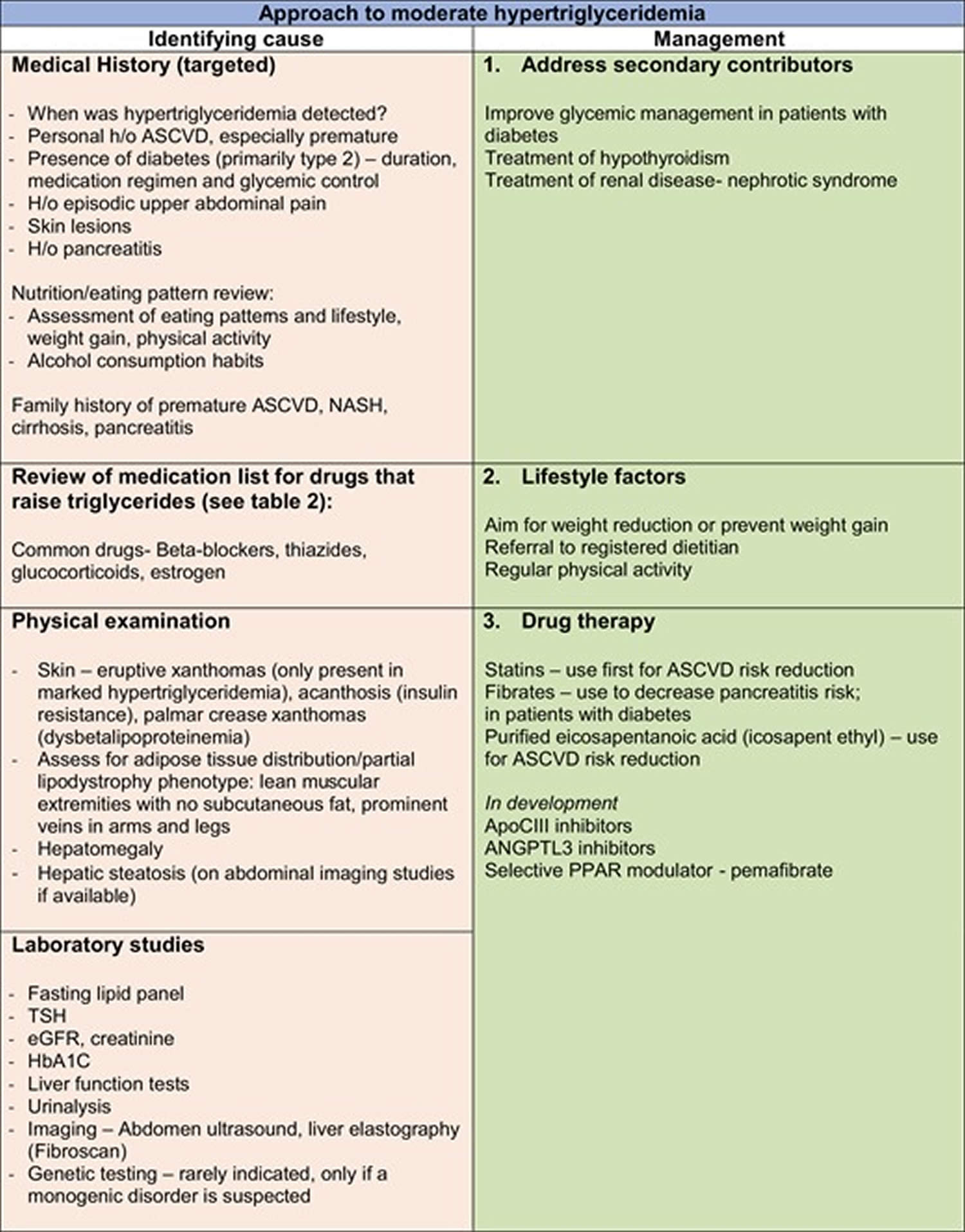
Table 1. Hypertriglyceridemia definition
| Guideline | Classification | Triglyceride Levels |
|---|---|---|
| National Cholesterol Education Program Adult Treatment Panel (NCEP/ ATP III) 30 American Heart Association 15 National Lipid Association 31 |
|
|
| The Endocrine Society 32 |
|
|
| European Society of Cardiology/European Atherosclerosis Society 33 |
|
|
| Hegele et al 34 |
|
|
What’s the difference between triglycerides and cholesterol?
Triglycerides and cholesterol are different types of lipids that circulate in your blood:
- Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. Triglycerides store unused calories and provide your body with energy. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. Triglycerides are fats that provide energy for your muscles. If you eat foods with a lot of saturated fat or carbohydrates, you will raise your triglyceride levels. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels. Elevated triglycerides levels are thought to lead to a greater risk of heart disease, but scientists do not agree that high triglycerides alone are a risk factor for heart disease. Normal triglyceride levels vary by age and sex. People with high triglycerides often have a high total cholesterol level, including a high LDL (bad) cholesterol level and a low HDL (good) cholesterol level. Many people with metabolic syndrome or diabetes also have high triglyceride levels. Extremely high triglyceride levels (more than 1000 mg/dL) can lead to abdominal pain and a life-threatening disorder of the pancreas called pancreatitis. Factors that can contribute to elevated triglyceride levels:
- Overweight or obesity
- Insulin resistance or metabolic syndrome
- Diabetes mellitus, especially with poor glucose control
- Alcohol consumption, especially in excess
- Excess sugar intake, especially from processed foods
- High saturated fat intake
- Hypothyroidism
- Chronic kidney disease
- Physical inactivity
- Pregnancy (especially in the third trimester)
- Inflammatory diseases (such as rheumatoid arthritis, systemic lupus erythematosus
- Some medications may also increase triglycerides.
- Cholesterol is a waxy, fat-like substance that’s found in all the cells in your body. Cholesterol is produced by your body and also found in some foods. Your body needs some cholesterol to make hormones, vitamin D and substances that help you digest foods. Cholesterol comes from two sources. Your liver makes all of the cholesterol your body needs to form cell membranes and to make certain hormones. Cholesterol is also found in foods from animal sources, such as egg yolks, meat, and cheese, which is called dietary cholesterol. Although we often blame the cholesterol found in foods that we eat for raising blood cholesterol, the main culprit is actually saturated fat. Foods rich in saturated fat include butter fat in milk products, fat from red meat, and tropical oils such as coconut oil. Cholesterol travels to cells through your bloodstream in special carriers called lipoproteins. Two of the most important lipoproteins are low-density lipoprotein (LDL) and high-density lipoprotein (HDL).
- There are different types of cholesterol:
- HDL stands for high-density lipoprotein or HDL-C (high-density lipoprotein cholesterol). HDL is sometimes called “good cholesterol” because it carries harmful cholesterol from other parts of your body including your arteries back to your liver. Your liver then removes the cholesterol from your body and helps protect you from heart attack and stroke. A healthy HDL-cholesterol level may protect against heart attack and stroke. If you have low HDL levels, you have a greater heart disease risk, even if your total cholesterol is below 200 mg/dL. Your doctor will evaluate your HDL and other cholesterol levels and other factors to assess your risk for heart attack or stroke. People with high blood triglycerides usually also have lower levels of HDL. Genetic factors, Type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do, because the female hormone estrogen raises HDL, but this can change after menopause.
- LDL stands for low-density lipoprotein or LDL-C (low-density lipoprotein cholesterol). LDL is sometimes called “bad cholesterol” because a high LDL level leads to the buildup of plaque in your arteries. LDL is the most important lipid for predicting your heart disease risk. Low-density lipoprotein (LDL or ‘bad’) cholesterol can join with fats and other substances to build up (also known as plaque) in the inner walls of your arteries, which starts a disease process called atherosclerosis. The arteries can become clogged and narrow, and blood flow is reduced. When plaque builds up in your coronary arteries that supply blood to your heart, you are at greater risk of having a heart attack. Since LDL is the bad kind of cholesterol, a low LDL level is considered good for your heart health. A diet high in saturated and trans fat is unhealthy because it tends to raise LDL cholesterol levels. Your LDL levels may be high if you eat a diet with a lot of saturated fat, cholesterol, or both. Sometimes, an under-active thyroid called hypothyroidism may also increase LDL levels.
- VLDL stands for very low-density lipoprotein or VLDL-C (very low-density lipoprotein cholesterol). Some people also call VLDL a “bad cholesterol” because it too contributes to the buildup of plaque in your arteries. But VLDL and LDL are different; VLDL mainly carries triglycerides and LDL mainly carries cholesterol. VLDL particles are released into the blood by the liver and circulate in the bloodstream, ultimately being converted into LDL as they lose triglyceride, having carried it to other parts of the body. According to the National Heart, Lung and Blood Institute’s National Cholesterol Education Program Guidelines ATP III, there is growing evidence that VLDL plays an important role in atherogenesis, in which plaques form on the interior walls of arteries, narrowing these passageways and restricting blood flow, which can lead to heart disease and increase the risk of stroke. Currently, direct measurement of VLDL cholesterol requires specialized testing. However, since VLDL-C contains most of the circulating triglyceride (if a person is fasting) and since the composition of the different particles is relatively constant, it is possible to estimate the amount of VLDL-C based on the triglyceride value. To estimate VLDL-C, divide the triglyceride value by 5 if the value is in mg/dL or divide by 2.2 if the value is in mmol/L. In most cases, this formula provides a good estimate of VLDL-C. However, this formula becomes less accurate with increased triglyceride levels when, for example, a person has not fasted before having blood drawn. The calculation is not valid when the triglyceride level is greater than 400 mg/dl (4.5 mmol/L) because other lipoproteins are usually present. In this situation, VLDL-C may be measured directly using specialized testing.
- High cholesterol usually has no symptoms. You can find out the levels of these in your blood and also your total cholesterol level with a cholesterol or lipid profile blood test. If you are concerned about your cholesterol level, talk to your doctor. You will need to stop eating for 10 to 12 hours before a cholesterol or lipid profile blood test, and the only liquid you may drink is water.
According to the National Heart, Lung and Blood Institute, a person’s first cholesterol screening should occur between the ages of 9 and 11 and then be repeated every five years after that 36. The National Heart, Lung and Blood Institute recommends that cholesterol screenings occur every 1 to 2 years for men ages 45 to 65 and for women ages 55 to 65. People over 65 should receive cholesterol tests annually 36. More-frequent cholesterol testing might be needed if your initial cholesterol test results were abnormal or if you already have coronary artery disease, you’re taking cholesterol-lowering medications or you’re at higher risk of coronary artery disease because you:
- Have a family history of high cholesterol or heart attacks
- Are overweight
- Are physically inactive
- Have diabetes
- Eat an unhealthy diet
- Smoke cigarettes
People undergoing treatment for high cholesterol require regular cholesterol testing to monitor the effectiveness of their treatments.
Your doctor can best help you understand what your specific test results mean for your health. Some doctors may set a specific target level when prescribing medication to lower cholesterol. Factors like diet, age, smoking, physical activity, weight, sex, genetics, medicines, and other medical conditions can all affect your LDL cholesterol level.
Lifestyle changes such as exercising and eating a healthy diet are the first line of defense against high cholesterol. But, if you’ve made these important lifestyle changes and your cholesterol levels remain high, your doctor might recommend medication.
Hypertriglyceridemia causes
Elevated triglycerides can be caused by several factors. Hypertriglyceridemia in many cases is multifactorial, resulting from the combination of genetic factors and other causes of increased production and or impaired clearance of triglyceride-rich lipoproteins 37, 28.
Several factors can contribute to high triglyceride level, including:
- Being overweight, or obesity
- Physical inactivity
- Cigarette smoking
- Excess alcohol consumption
- A diet very high in carbohydrates (more than 60 percent of total calories)
- Sometimes underlying diseases or genetic disorders can also cause high triglyceride levels.
These factors can be addressed with lifestyle changes.
Genetic causes
The primary disorders predominantly causing high triglyceride are 38:
- Familial hypertriglyceridemia. Familial hypertriglyceridemia is a common autosomal dominant inherited disorder characterized by increased plasma concentration of very-low-density lipoprotein (VLDL) (type 4 lipoprotein pattern), typically with low LDL (low-density lipoprotein) and HDL (high-density lipoprotein) 38. Usually asymptomatic but in the setting of secondary contributors to hypertriglyceridemia, can present with chylomicronemia syndrome and pancreatitis. Moderate elevations of triglycerides usually occur during early adulthood, and a triad of obesity, hyperglycemia, and hyperinsulinemia can be seen in affected individuals. In individuals with moderate elevation in plasma triglycerides associated with a normal cholesterol level, the possibility of familial hypertriglyceridemia should be suspected 38. Although patients with familial hypertriglyceridemia usually have moderate elevation of plasma triglycerides, whenever conditions known to elevate triglyceride, such as diabetes mellitus or alcohol or oral contraceptive consumption, concurrently occur, they may develop a profound hypertriglyceridemia and a mixed hyperlipidemia (type 5 lipoprotein pattern). An increased incidence of atherosclerosis has been reported. Hypertension and hyperuricemia have also been frequently observed. Familial hypertriglyceridemia is not associated with premature cardiovascular disease.
- Familial combined hyperlipidemia. Elevated VLDL (very-low-density lipoprotein) and or LDL (low-density lipoprotein), the phenotype can vary from isolated hypertriglyceridemia to isolated hypercholesterolemia. Regardless of phenotype, increased apo-B concentration is seen and is used to distinguish from familial hypertriglyceridemia. Associated with premature cardiovascular disease.
- Congenital deficiency of lipoprotein lipase. Congenital lipoprotein lipase deficiency is a rare autosomal recessive disorder secondary to absence or severe diminution in the activity of lipoprotein lipase. Affected individuals are homozygous for a mutation that prevents normal expression of lipoprotein lipase activity. The parents, although clinically normal, are obligate heterozygotes. This enzymatic disorder is reflected in a massive accumulation of chylomicrons in the plasma without elevation of very-low-density lipoprotein (VLDL) (type 1 lipoprotein pattern). Triglycerides may reach levels of 2000 to 10,000 mg/dl. This disorder usually appears in childhood with recurrent bouts of abdominal pain secondary to pancreatitis. Another characteristic feature of the disorder is the occurrence of eruptive xanthomas, predominantly in the buttocks and other pressure-sensitive areas of the body, attributed to the deposition of chylomicron triglycerides in histiocytes. The elevation in chylomicrons may also cause a lipemic serum, a picture of lipemia retinalis, and hepatosplenomegaly. The diagnosis is suspected by the presence of a lipemic plasma in a young patient who has fasted for 12 hours. Overnight incubation of a test tube of such plasma in a refrigeration at 4°C demonstrates a visible white layer at the top of the tube. Failure of lipoprotein lipase levels to increase after an infusion of heparin confirms the diagnosis. The occurrence of accelerated atherosclerosis is not reported in this condition.
- Apoprotein CII deficiency. Apoprotein CII deficiency is a rare autosomal recessive disorder caused by absence of apoprotein CII, a required co-factor for the activity of lipoprotein lipase. The ensuing functional deficiency in this enzyme leads to a clinical picture similar to that described above for congenital lipoprotein lipase deficiency. However, in contrast to what occurs in the latter disorder, affected individuals are diagnosed at later age and rarely present eruptive xanthomas. The usual presentation is also with recurrent abdominal pains secondary to acute pancreatitis. At times the diagnosis is made by chance discovery of a milky serum. Due to the inherent defect in this condition, in which lipoprotein lipase is not activated, both chylomicrons and very-low-density lipoprotein (VLDL) are elevated in the blood causing a type 1 or type 5 lipoprotein pattern.
- Familial dysbetalipoproteinemias (type III hyperlipoproteinemia). Familial dysbetalipoproteinemia, also called familial type 3 hyperlipoproteinemia, is a condition inherited through a single gene mechanism whose clinical presentation requires the presence of other genetic or environmental factors. Elevation of both plasma cholesterol and triglycerides occurs because of accumulation of remnant very-low-density lipoprotein (VLDL) particles in the plasma. The metabolic defect in most patients occurs in apolipoprotein E. This has three common alleles, designated E2, E3, and E4. Patients with this disorder have only apolipoprotein E2 in very-low-density lipoprotein (VLDL), which is less effective in facilitating clearance of remnants than E3 or E4. The condition occurs only in individuals who are homozygous for E2, that is, those with an E2/E2 genotype. Clinical evidence of hyperlipoproteinemia usually appears after the second decade. The characteristic clinical findings are xanthoma striata palmaris and tuberous and tuberoeruptive xanthomas over the elbows and knees. The disorder is associated with severe atherosclerosis of the coronary arteries, abdominal aorta, and peripheral arteries. The diagnosis is facilitated by encountering a broad beta band on lipoprotein electrophoresis. Confirmation can be obtained in specialized laboratories either by measuring the chemical composition of the VLDL fraction after ultracentrifugation of the plasma or by determining for the E2 allele after isoelectric focusing of remnant proteins.
Severe hypertriglyceridemia with plasma triglyceride levels >1000-1500 mg/dL can result from 3 groups of conditions 3:
- Rare mutations in the lipoprotein lipase (LPL) complex, where it is termed the familial chylomicronemia syndrome,
- The co-existence of genetic and secondary forms of hypertriglyceridemia, termed the multifactorial chylomicronemia syndrome, which is a much more common cause of severe hypertriglyceridemia, and
- Familial partial lipodystrophy.
Other causes
- Diet with high positive energy-intake balance and high fat or high glycemic index (eating high GI foods)
- Obesity and associated insulin-resistant states
- Metabolic syndrome
- Diabetes mellitus, more frequently in type 2 diabetes mellitus
- Excessive alcohol intake (hypertriglyceridemia risk increases with > 2 and > 1 drink(s) per day in men and women, respectively)
- Endocrine conditions: Hypothyroidism (underactive thyroid): predominant dyslipidemia is increase in LDL, but hypertriglyceridemia can also occur, Cushings syndrome,
- Acromegaly
- Drug-induced: thiazides, beta blockers, oral estrogens, tamoxifen, oral contraceptives (birth control pills), corticosteroids, oral estrogen, atypical antipsychotics, second-generation antipsychotic agents (such as clozapine and olanzapine), cyclophosphamide, L-asparaginase, protease inhibitors, isotretinoin, bile acid binding resins, anti-retroviral protease inhibitors, immunosuppressive agents: sirolimus (mTOR inhibitors)
- Pregnancy (particularly in the third trimester): triglyceride levels in the third trimester can increase by 200% or more from pre-pregnancy levels. In the setting of underlying primary or secondary disorders of hypertriglyceridemia, this can result in pancreatitis.
- HIV
- Kidney disease: nephrotic syndrome, proteinuria, glomerulonephritis, uremia or chronic kidney disease
- Critical illness: sepsis
- Autoimmune conditions: Juvenile dermatomyositis, systemic lupus erythematosis (SLE)
- Inherited and congenital lipodystrophies
- Paraproteinemia
Hypertriglyceridemia pathophysiology
Triglycerides are carried in the circulation by triglyceride-rich lipoproteins (TRLs) such as chylomicron (CM) and very low-density lipoprotein (VLDL) 15. Chylomicrons are released from the small intestines and carry a significantly high percentage of triglyceride. The triglyceride rich chylomicrons undergo hydrolysis in peripheral tissues. Due to the lipolysis, free fatty acids (FFA) are released 15.The free fatty acids (FFA) is taken by muscle cells, where they are a source of energy. In adipose tissue, the free fatty acids (FFA) is stored as an inactive fuel 15.
When compared to very large triglyceride-rich lipoproteins, the remnant triglyceride-rich lipoproteins can be atherogenic 39. Even though triglyceride particles are not found in atherosclerotic plaques, the cholesterol content (especially the LDL particles) of triglyceride-rich lipoproteins plays a role in plaque formation 40. In addition, the lipolysis of triglyceride-rich lipoproteins produces free fatty acids, lysolecithin, and other reactive lipids that may have pro-inflammatory and pro-coagulant effects 41.
The release of excess free fatty acids and lysolecithin from chylomicrons in pancreatic capillaries is linked to the causation of pancreatitis. Hyperviscosity from increased chylomicrons leads to acidosis and ischemia in the capillary beds. This leads to the activation of pancreatic lipases, lipolysis, and release of toxic free fatty acids (FFA), which cause inflammation, cytotoxic injury, and pancreatitis 41. The risk of pancreatitis correlates with the level of triglycerides and markedly increases with levels above 500 mg/dL 41. In most instances, pancreatitis can be prevented by keeping triglyceride levels below 250 mg/dL to 500 mg/dL.
Hypertriglyceridemia symptoms
Usually, most people with hypertriglyceridemia or high triglyceride levels, have no symptoms and the only means of discovering a high triglyceride level is with blood tests. However, in rare cases, a person may have an extremely high level of triglycerides (well above 1000 mg/dL) sustained over time and the individual may experience repeated bouts of acute pancreatitis. Some of the signs and symptoms include pain in the upper half of the stomach area that develops suddenly and then gradually gets worse, fever, nausea, vomiting, and sometimes jaundice. A person with severely high levels may also develop lesions on the skin called xanthomas. These typically appear as several small, round, solid, yellow bumps mostly on the back, chest, buttocks, shoulders and thighs.
The mechanisms leading to pancreatitis are not clear. It is suspected to be related to release of excess free fatty acids and lysolecithin from chylomicrons exceeding the binding capacity of albumin in pancreatic capillaries. The unbound free fatty acids are thought to form micellar structures with detergent properties, causing injury and ischemia leading to pancreatitis. Risk of pancreatitis markedly increases with triglycerides levels above 200 mg/dL and in most cases can be prevented by keeping triglycerides levels below 250 mg/dL to 500 mg/dL.
Mild to moderate hypertriglyceridemia is associated with an increased risk of premature cardiovascular disease (CVD), while severe hypertriglyceridemia can lead to pancreatitis and other features of the chylomicronemia syndrome, as well as an increased risk of premature cardiovascular disease. Severe hypertriglyceridemia is the third leading cause of pancreatitis in the United States. Patients can fluctuate between hypertriglyceridemic states: given an appropriate metabolic stress, mild or moderate hypertriglyceridemia can deteriorate into severe hypertriglyceridemia 42.
Hypertriglyceridemia diagnosis
The diagnosis of hypertriglyceridemia should be made based on a fasting lipid panel with recommended length of the fast of 12 hours. An important point in the setting of triglycerides higher than 400 mg/dL, the Friedewald equation which is commonly used to calculate LDL-cholesterol (bad choletserol) levels, underestimates LDL-cholesterol (bad choletserol) levels. In this setting, it is best to rely on calculation of non-HDL-cholesterol levels (total cholesterol minus HDL “good” cholesterol) or obtain direct LDL-cholesterol (bad choletserol) levels when available.
Regarding utility of advanced lipoprotein testing, measurement of LDL size or density is not recommended for prevention of cardiovascular events. Apo B and Lp(a) may have utility for assessment of cardiovascular risk in the setting of hypertriglyceridemia. Although effective therapies exist for Apo B lowering, there is no evidence-based therapy for Lp(a) lowering in the prevention of atherosclerotic cardiovascular disease events, although niacin and estrogen have been shown to lower levels of Lp(a). Lp(a) has strong familial inheritance and association with premature cardiovascular disease, thus aggressive LDL lowering is recommended when Lp(a) is high.
Hepatic steatosis, commonly associated with insulin resistance states and hypertriglyceridemia, can be associated with elevation of aminotransferases on hepatic function panel (commonly alanine aminotransferase (ALT) elevation) and should be evaluated radiologically with ultrasound as an initial step.
Hypertriglyceridemia treatment
The goal of treatment is to lower your triglycerides. Patients with very severe high triglycerides should try to lower their triglycerides below 1,000 mg/dL (11.3 mmol/L), to reduce their risk for pancreatitis.
For many people, high triglycerides are caused by another disorder, such as diabetes, obesity, renal failure, or alcoholism. With these conditions, the strategy is to treat the primary cause. When high triglycerides are not caused by another disorder, they are often seen together with high cholesterol and treatment is directed toward lowering both cholesterol and triglycerides. Lifestyle changes, such as a healthy diet and increased exercise, are usually the primary strategy for lowering levels. If these fail, lipid-lowering medications such as statins are generally recommended.
If you are diagnosed with high blood triglycerides, your doctor may recommend that you make heart-healthy lifestyle changes 32:
- Choose heart-healthy foods. Eat more high-fiber foods from plants. Choose 100% whole grains, whole fruits and vegetables.
- Get regular physical activity. Aim for at least 30 minutes of physical activity on most or all days of the week. Regular exercise can lower triglycerides and boost “good” cholesterol. Try to incorporate more physical activity into your daily tasks — for example, climb the stairs at work or take a walk during breaks.
- Lose weight. If you have mild to moderate hypertriglyceridemia, focus on cutting calories. Extra calories are converted to triglycerides and stored as fat. Reducing your calories will reduce triglycerides.
- Manage stress.
- Quit smoking.
- Get enough good quality sleep.
- Limit alcohol. Alcohol is high in calories and sugar and has a particularly potent effect on triglycerides. If your blood triglyceride levels are considered very high, your doctor may tell you not to drink alcohol.
If healthy lifestyle changes aren’t enough to control high triglycerides, your doctor might recommend a few different types of medicines to control or lower your triglyceride levels 32:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. These cholesterol-lowering medications may be recommended if you also have poor cholesterol numbers or a history of blocked arteries or diabetes. Examples of statins include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor).
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can also be used to remove triglycerides from the blood when paired with a healthy diet. Ezetimibe can be used with a statin drug. If statins don’t reduce cholesterol enough, doctors often suggest adding ezetimibe.
- Fibrates. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Fibrates have been shown to markedly reduce triglyceride levels by 50% and beyond. Drugs like fenofibrate and gemfibrozil help activate lipoprotein lipase (LPL) through PPAR-alpha leading to further breakdown of triglycerides. However, fibrates aren’t used if you have severe kidney or liver disease. Furthermore, caution must be noted during polypharmacy. A combination of fibrates with statins can increase the risk of statin side effects 43, 44. This is theorized to be a result of CYP-3A4 inhibition via fibrates. If combined therapy is required, exercise caution and consider statin therapy that is not primarily metabolized through CYP-3A4 (pravastatin) 44.
- Fish oil also known as omega-3 fatty acids. Fish oil or omega-3 fatty acid can help lower your triglycerides. Fish oil has shown a significant reduction of both VLDL and triglyceride levels 45. Triglyceride lowering by fish oil omega-3 fatty acids are mediated primarily via eicosopentanoic acid (EPA) and docosahexaenoic acid (DHA), which result in variable, dose-dependent, and modest lowering of triglycerides through chylomicron clearance 46. To achieve triglyceride reduction of 20% to 50%, administration of 3 to 4 g/day of omega-3 fish oil is required. Omega-3 preparations are available by prescription and readily available as over-the-counter (OTC) supplements with variable quantities/purity of EPA and DHA. A generic version of purified EPA alone is also available. Both prescription and OTC supplements can lower triglycerides. Prescription fish oil preparations such as Lovaza, contain more-active omega-3 fatty acids than many nonprescription supplements. Fish oil taken at high levels can interfere with blood clotting and cause gastrointestinal symptoms, so talk to your doctor before taking any supplements.
- Niacin also called nicotinic acid or vitamin B3. Niacin can lower your triglycerides and low-density lipoprotein (LDL) cholesterol the “bad” cholesterol. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. Niacin (nicotinic acid) can decrease plasma triglycerides by up to 40% 47. Niacin decreases adipose tissue lipolysis and free fatty acid delivery to the liver with resultant reduced hepatic VLDL synthesis. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins. Talk to your doctor before taking over-the-counter niacin because it can interact with other medications and cause significant side effects.
More than one medicine may be necessary to treat very high levels of triglycerides. If your doctor prescribes medication to lower your triglycerides, take the medication as prescribed. And remember the significance of the healthy lifestyle changes you’ve made. Medications can help — but lifestyle matters, too.
First-line therapy for acute hypertriglyceridemia pancreatitis includes intravenous (IV) fluids and fasting. Pancreatitis can be a life-threatening condition and may require admission to an intensive care unit. Identifying and treating the underlying cause is important. Also, low-dose IV insulin infusion (as low as 1 unit/hour) is effective through suppression of lipolysis and decreased hepatic triglyceride assembly. With IV insulin infusion, concomitant glucose infusion may be needed in the absence of hyperglycemia to prevent hypoglycemia. Heparin causes a release of LpL from the capillary endothelial surface and may reduce triglyceride levels rapidly, but is short-acting and so not commonly used. Plasmapheresis is an option, when available, for extremely high triglyceride levels but the cost is limiting, the risk of infection is a concern, and the effect is also short-lived. On discharge from the hospital, to decrease recurrence of pancreatitis, lifestyle change, treatment of the underlying cause, use of fibrate therapy to keep triglyceride levels below 500 mg/dL and ideally less than 150 mg/dL, has benefit 48.
Lifestyle changes
If you have mild to moderate hypertriglyceridemia, focus on cutting calories. Extra calories are converted to triglycerides and stored as fat. Reducing your calories will reduce triglycerides.
Lose weight
The first step for lowering triglycerides is to lose weight if you are overweight, exercise often, and eat a healthy diet low in saturated (bad) fat and sugar. Also, limit the amount of refined, processed grains you eat, such as white bread, rice, and pasta. Follow your doctor’s advice about limiting intake of alcohol, which
raises triglycerides in some people.
Exercise
Be active for at least 30 minutes a day. A good starting goal is at least 150 minutes a week, but if you don’t want to sweat the numbers, just move more!
Regular physical activity strengthens your heart and reduces your ‘bad’ cholesterol. Being active helps increase your ‘good’ HDL cholesterol while helping your body move the ‘bad’ non-HDL cholesterol to your liver where it will be disposed of.
You don’t have to join a gym or take up a sport, just look for chances to move more every day. Staying active is great way to keep your heart healthy.
Stop smoking
Quitting smoking can help to lower your cholesterol and improve your heart health. Smoking stops ‘good’ cholesterol doing its job of getting rid of your ‘bad’ cholesterol. Speak to your doctor about how to stop smoking as soon as you can. Not smoking will really help you avoid heart disease.
Limit how much alcohol you drink
Alcohol is high in calories and sugar and has a particularly potent effect on triglycerides. If you have severe hypertriglyceridemia, avoid drinking any alcohol.
Hypertriglyceridemia diet
What you eat and drink affects your triglyceride and cholesterol levels. No randomized clinical trial evidence for any specific dietary recommendations for mild to moderate triglyceride exists. The key principle of making changes to eating patterns is to reduce net caloric intake. Replacing refined carbohydrates with complex carbohydrates, limiting dietary saturated fat, avoiding trans fats, and inclusion of mono- or polyunsaturated fats are reasonable approaches 49. Intermittent fasting may decrease triglycerides more than standard hypocaloric diets, but evidence is inconsistent in studies 50, 51. Very low carbohydrate or ketogenic diets also appear to consistently lower triglycerides in patients with mild to moderate hypertriglyceridemia 52; additionally, in some individuals who follow such eating patterns, marked LDL cholesterol elevations can occur 29. In the online “ketogenic world” these individuals are referred to as “lean-mass hyper-responders” 53. Such responses may be related to the higher fat (especially saturated fat) consumption and resultant downregulation of cell surface LDL receptors. Such diets are hard to maintain and cannot be recommended especially in patients with moderate hypertriglyceridemia who have strong history of atherosclerotic cardiovascular disease 54 or in patients with predisposition to marked hypertriglyceridemia with pancreatitis 52.
If you have high triglyceride levels, your doctor may recommend following a heart healthy diet. A heart-healthy diet focuses on plant-based foods, including fruits, vegetables and whole grains while limiting saturated fats, trans fats, salt and sugar. Saturated fats such as those in meat, butter, cheese and other full-fat dairy products can raise your total cholesterol. Decreasing your consumption of saturated fats to less than 7% of your total daily calorie intake can reduce your LDL cholesterol by 8% to 10%. Trans fats sometimes listed on food labels as “partially hydrogenated vegetable oil”, are often used in margarines and store-bought cookies, crackers and cakes. Trans fats raise overall cholesterol levels. The Food and Drug Administration (FDA) banned the use of partially hydrogenated vegetable oils in processed foods sold after January 1, 2020.
Eat a healthy balanced diet
Eating more fruit, vegetables and wholegrain is better than eating foods high in saturated fat and sugar. Eating a healthy, balanced diet low in saturated fats can also reduce your level of LDL “bad” cholesterol.
Avoid or cut down on the following foods, which are high in saturated fat:
- fatty cuts of meat and meat products, such as sausages and pies
- butter, ghee and lard
- cream, soured cream, crème fraîche and ice cream
- cheese, particularly hard cheese
- cakes and biscuits
- milk chocolate
- coconut oil, coconut cream and palm oil
Choose healthier healthy monounsaturated and polyunsaturated fats such as:
- olive, rapeseed or sunflower oils and spreads
- vegetable oil spreads
- nuts
- seeds
- oily fish.
Choose more wholegrains and foods that are high in soluble fiber as this can help lower cholesterol such as:
- oats
- beans
- pulses
- lentils
- nuts
- fruits and vegetables.
Oatmeal, oat bran and high-fiber foods
Oatmeal has soluble fiber, which reduces your low-density lipoprotein (LDL) cholesterol, the “bad” cholesterol. Soluble fiber is also found in such foods as kidney beans, Brussels sprouts, apples and pears. Soluble fiber can reduce the absorption of cholesterol into your bloodstream. Five to 10 grams or more of soluble fiber a day decreases your LDL cholesterol.
One serving of a breakfast cereal with oatmeal or oat bran provides 3 to 4 grams of fiber. If you add fruit, such as a banana or berries, you’ll get even more fiber.
Omega-3 fatty acids
Fatty fish has high levels of omega-3 fatty acids consisting of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) can lower triglycerides 55. However, too much omega-3 fatty acids can contribute to obesity. These polyunsaturated (good) fats are found in oily fish such as salmon, mackerel and tuna. Omega-3 fatty acids is also found in avocados. In high doses, omega-3 fatty acids (EPA and DHA) can treat high triglycerides. For people with a high triglyceride level, at least 2 portions of oily fish a week is thought to be beneficial.
You can get high doses of omega-3 fatty acids in a fish oil supplement or by prescription. However, there’s no evidence that taking omega-3 fatty acid supplements has the same benefit. Side effects of omega-3 supplements are usually mild. They include unpleasant taste, bad breath, bad-smelling sweat, headache, and gastrointestinal symptoms such as heartburn, nausea, and diarrhea.
According to National Cholesterol Education Program (NCEP) Expert Panel on Treatment of High Blood Cholesterol In Adults (NCEP ATP III) guidelines, omega-3 fatty acids are recommended for patients with moderate to severe hypertriglyceridemia [7]. At a dose of 4 grams/day, omega-3 fatty acids can lower TG by 20%–30% in patients with TG levels 200–500 mg/dL 30. Plasma triglyceride reductions of 50%–60% have been demonstrated among patients receiving 6 grams/day of omega-3 fatty acids 56. The triglyceride-lowering effectiveness is related to baseline triglyceride values 57. Lower doses of omega-3 fatty acids (1 to 2 g/day) have also demonstrated significant reductions in cardiovascular mortality 58 and morbidity 59. Therefore, omega-3 fatty acids remain an important option in the management of hypertriglyceridemia 2.
Triglycerides-lowering medication
Besides lifestyle changes, you may also need drug treatment. There are several different types of cholesterol-lowering medication that work in different ways 60, 61, 62, 63, 64. Your doctor can advise you about the most suitable type of treatment, and may also prescribe medication to lower high blood pressure (hypertension) if it affects you.
For mildly or moderately high triglycerides, your doctor may prescribe one of these types of drugs:
Note: It is unclear if fibrates and niacin prevent heart attacks and strokes.
If your triglycerides are above 1,000 mg/dL, though, the first choice of medicine is a fibrate. You may need a statin, too, but experts advise against treatment with statins alone if your high triglycerides are severe or very severe. Fibrates are better than statins at lowering triglycerides. However, people with liver disease or gallbladder disease should not take fibrates.
Talk to your doctor about the risks and benefits of all these drugs. Medications do not cure the problem of high triglycerides, so you will need to take them long term. However, weight loss and other lifestyle changes can lower high trigylcerides enough to eliminate the need for medication.
Table 2. Hypertriglyceridemia medications
| Fibrates | Omega 3 fish oil |
|---|---|
| Gemfibrozil Doses: 300 mg, 600 mg taken twice daily | Omega -3 fatty acids (Epanova) 850 mg polyunsaturated fatty acids, including eicosapentanoic acid (EPA) and docosahexanoic acid (DHA) |
| Fenofibrate Micronizeda 43, 130 mg or 67, 134, 200 mg | Omega 3 ethyl esters (Lovaza, Omacor) 375 mg DHA and 465 mg EPA |
| Bezafibrate (not available in the United States) 200 mg twice daily or 400 mg extended release once daily | Icosapent ethyl (Vascepa) EPA only—0.5 or 1 g |
Fibrates
Fibrates, which greatly lower triglycerides and sometimes raise HDL (good) cholesterol. In the U.S., these prescription drugs include gemfibrozil and fenofibrate.
Fibrates help to slow or halt the build-up of cholesterol in the arteries to reduce the risk of heart problems. They are given to people who have high cholesterol levels because they have a raised level of triglycerides in their blood.
Fibrates are first-line medications for triglyceride lowering with a decrease of 30% to 50% with concomitant increase in HDL-C. Fibrates decrease VLDL production, increase catabolism of TGRL through increased fatty acid oxidation, increased LpL synthesis, and reduced apoC-III. The effect on LDL-C can be variable in that with high triglyceride levels, LDL-C can increase but can decrease with mildly elevated hypertriglyceridemia. Dose adjustment is required with renal insufficiency, and pre-existing liver and gallbladder disease are contraindications. In the setting of concomitant statin use, fenofibrate is the preferred fibrate as gemfibrozil is associated with a higher risk of myositis. Due to protein binding, fenofibrate has an interaction with warfarin and requires close monitoring. Treatment triglyceride goal of less than 500 mg/dL is recommended to decrease the risk of recurrent pancreatitis. Concerning cardiovascular disease reduction, secondary analysis and meta-analysis of cardiovascular disease trials have shown the consistent reduction in cardiovascular disease in subgroups with baseline triglycerides below 200 and low HDL. Other potential benefits include the reduction in retinopathy and albuminuria in patients with diabetes.
Niacin (vitamin B3)
Niacin (vitamin B3) at doses of 1,000 to 3,000 mg per day, lowers triglycerides and LDL cholesterol and raises HDL cholesterol. These doses apply to immediate-release (released into the body right away) niacin, available by prescription or as a supplement.
The dose of sustained-release (released into the body over time) niacin, which is only available as a supplement, shouldn’t exceed 2,000 mg per day because of the risk of liver damage.
Niacin reduces triglyceride by about 15% to 40%, decreasing triglyceride synthesis through inhibition of liver DGAT 2, and decreasing lipolysis by inhibiting hormone-sensitive lipase. With recent clinical trials not showing any cardiovascular disease benefit when used with statins, the use of niacin has declined. Flushing is a common side effect that can be reduced by concomitant aspirin use and starting with a low dose at bedtime and slow-dose titration. Complications include hepatotoxicity, impaired glucose tolerance, and hyperuricemia. Niacin is contraindicated in patients with active peptic ulcer disease.
Omega-3 fatty acids
Omega-3 fatty acids, which are FDA-indicated for treatment of severe and very severe hypertriglyceridemia (greater than 1000 mg/dL), reduce triglycerides by 20% to 50% at 3 g to 4 g/day of eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA). Higher baseline triglycerides are associated with greater triglyceride lowering. As triglyceride lowering is dose-related, and over the counter dietary fish oil supplements contain variable amounts of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), it is important to look at the nutrition label and instruct patients to ingest 3 gm to 4 gm per day of omega-3 fatty acids. Fishy taste and gastrointestinal discomfort can occur with such high doses of over-the-counter omega-3 fatty acid, and change to available FDA-approved prescription omega-3 fatty acid may be beneficial. Increased conversion of VLDL to LDL can lead to a rise in levels of low-density lipoprotein cholesterol (LDL-C) but has not been shown with the eicosapentaenoic acid (EPA)-only prescription product. No studies have shown cardiovascular disease benefit in patients with hypertriglyceridemia on high dose omega-3 fatty acid. Recent trials have failed to demonstrate that lowering triglyceride with omega-3 fatty acid in statin-treated patients with hypertriglyceridemia can reduce cardiovascular risk. A diet rich in omega-3 fatty acids is associated with cardiovascular health benefits.
Statins
Your doctor may add a statin to your other drug treatment. Though statins mainly lower LDL cholesterol, they also can decrease triglycerides. Some studies show that statins reduce the risk of heart attacks and strokes.
Statins block the enzyme (HMG-CoA reductase, the rate-limiting step in cholesterol biosynthesis) in your liver that helps to make cholesterol. This leads to a reduction in your blood cholesterol level.
You’ll usually be started on a medication called atorvastatin. Other statins include simvastatin and rosuvastatin.
When someone has side effects from using a statin, it’s described as having an “intolerance” to it. Side effects of statins include headaches, muscle pain and stomach problems, such as indigestion, diarrhea or constipation.
Statins will only be prescribed to people who continue to be at high risk of heart disease, because they need to be taken for life. Cholesterol levels start to rise again once you stop taking them.
Statins lower triglyceride by about 10% to 30% in a dose-dependent manner and can be used as monotherapy in triglyceride levels of more than 500 m/dL when indicated to decrease cardiovascular risk.
Ezetimibe
Ezetimibe is an intestinal cholesterol absorption inhibitor whose primary target is the NPC1L1 intestinal cholesterol transporter. Ezetimibe might be a useful adjunct therapy in patients with hypertriglyceridemia. For instance, patients on a combination of fenofibrate 160 mg plus ezetimibe vs. fenofibrate alone had significantly greater triglyceride reductions 65. Ezetimibe can also be used to remove triglycerides from the blood when paired with a healthy diet.
Aspirin
In some cases, a low daily dose of aspirin may be prescribed, depending on your age (usually over 40 years old) and other risk factors.
Low-dose aspirin can help to prevent blood clots forming, particularly for someone who’s had a heart attack, has established vascular disease, or a high risk of developing cardiovascular disease.
You may also be advised to have periodic blood tests to ensure your liver is functioning well.
Hypertriglyceridemia prognosis
Patients with hyperlipidemia are at extremely high risk of developing premature coronary artery disease (coronary heart disease) (30%) 66. If the disease is inadequately managed, the prognosis is poor, especially if other cardiovascular risk factors are present. If the patient complies with lipid-lowering therapy, dietary modification, and lifestyle modification and if therapy is successful, outcome is improved significantly.
Cardiovascular disease
Hypertriglyceridemia is correlated with an increased risk of cardiovascular disease (CVD), particularly in the setting of low high-density lipoprotein (HDL) cholesterol levels and/or elevated low-density lipoprotein (LDL) cholesterol levels. When low HDL cholesterol levels are controlled for, some studies demonstrate that elevated triglycerides do not correlate with risk of cardiovascular disease. Others suggest that high triglyceride levels are an independent risk factor.
Because metabolism of the triglyceride-rich lipoproteins (chylomicrons, very low-density lipoprotein [VLDL]) and metabolism of HDL are interdependent and because triglycerides are very labile, the independent impact of hypertriglyceridemia on cardiovascular disease risk is difficult to confirm. However, randomized clinical trials using triglyceride-lowering medications have demonstrated decreased coronary events in both the primary and secondary coronary prevention populations.
An understanding of lipoprotein catabolism provides an explanation for the absence of increased risk of cardiovascular disease in patients with the most severe form of hypertriglyceridemia, type I hyperlipoproteinemia. The atherogenicity correlated with elevated triglyceride levels is thought to be secondary to increased levels of chylomicron and VLDL remnants. Remnants are smaller, richer in cholesterol, and more readily taken up by macrophages, which are converted to plaque-forming foam cells. The chylomicrons in patients with type I disease cannot be converted to remnants and, therefore, should not be atherogenic.
Using data from the National Health and Nutrition Examination Survey (2007-2014), Fan et al 67 estimated that in adult statin users with triglyceride levels in the range between greater than 150 and 500 mg/dL, the mean 10-year risk of atherosclerotic cardiovascular disease is 11.3-19.1%, while in non–statin users falling within the same parameters, the mean 10-year risk is 6.0-15.6%.
Pancreatitis
Extreme elevations of triglycerides, usually well above 1000 mg/dL, may cause acute pancreatitis and all the sequelae of that condition. A study by Pedersen et al 68 indicated that even nonfasting mild to moderate hypertriglyceridemia (177 mg/dL or above) raises the risk for acute pancreatitis; the investigators found, for example, the multivariable adjusted hazard ratio for acute pancreatitis to be 2.3 for persons with triglyceride levels of 177-265 mg/dL. However, many patients tolerate triglycerides of 4000 mg/dL or higher without developing symptoms 69.
The National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) guidelines 70 indicate that triglycerides are so labile that a level between 500 and 1000 mg/dL may in certain settings increase dramatically and should be a target of treatment even before ensuring that the LDL goal is reached. Thus, these guidelines stipulate that if triglycerides are 500 mg/dL or greater, the initial management should be to lower the triglycerides to prevent pancreatitis. Only when the triglyceride level is below 500 should LDL-lowering be addressed.
The risk of recurrent pancreatitis secondary to hypertriglyceridemia can be avoided entirely by ensuring that levels are maintained well below 700 mg/dL. Because triglyceride levels are so labile, simply moderating levels to less than 1000 mg/dL does not decrease risk substantially, because the slightest metabolic imbalance or dietary indiscretion may push levels several hundred points higher.
Chylomicronemia syndrome
The chylomicronemia syndrome 71, 72 is an often unrecognized and less severe condition than pancreatitis that is usually caused by triglyceride levels greater than 1000 mg/dL. Recurrent episodes of ill-defined abdominal pain that may be accompanied by nausea and vomiting are the most common presenting symptom, but chest pain and dyspnea may sometimes occur. A papular rash may be present on the trunk, thighs, and buttocks, which resolves with treatment. Amylase and lipase are minimally, if at all, elevated. Symptoms resolve when triglyceride levels decrease well below 1000 mg/dL.
Type 2 diabetes
A prospective study by Lee et al 73 indicated that a patient’s risk for developing type 2 diabetes increases with the number of exposures the individual has to hypertriglyceridemia. The investigators looked at individuals with no history of type 2 diabetes, in whom 4 consecutive annual health checkups had been performed. Compared with those who had no hypertriglyceridemia exposures, those with 1, 2, 3, or 4 exposures had multivariable-adjusted hazard ratios for incident diabetes of 1.674, 2.192, 2.637, and 3.715, respectively 73. The study’s follow-up period was 6.53 years 73.
Rheumatoid arthritis
Using the National Health and Nutrition Examination Survey (NHANES) database (2007-2010), a study by Shand et al 74 indicated that in patients with either hypertriglyceridemia or obesity, the added presence of depression increases the risk for developing rheumatoid arthritis. The investigators reported that the “synergistic effect” of hypertriglyceridemia and depression was particularly strong when the patient’s C-reactive protein level was between 1 and 3 mg/L. However, the presence of hypertriglyceridemia and obesity together was not associated with a greater likelihood of arthritis 74.
- Monogenic dyslipidemias: window on determinants of plasma lipoprotein metabolism. Hegele RA. Am J Hum Genet. 2001 Dec; 69(6):1161-77.[↩]
- Brahm A, Hegele RA. Hypertriglyceridemia. Nutrients. 2013 Mar 22;5(3):981-1001. doi: 10.3390/nu5030981[↩][↩]
- Chait A, Subramanian S. Hypertriglyceridemia: Pathophysiology, Role of Genetics, Consequences, and Treatment. 2019 Apr 23. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK326743[↩][↩]
- Grønbaek M. The positive and negative health effects of alcohol- and the public health implications. J Intern Med. 2009 Apr;265(4):407-20. doi: 10.1111/j.1365-2796.2009.02082.x[↩]
- Luo WS, Chen F, Ji JM, Guo ZR. Interaction of tobacco smoking and alcohol consumption with obesity on cardiovascular disease in a Chinese cohort. Coron Artery Dis. 2020 Jun;31(4):372-377. doi: 10.1097/MCA.0000000000000837[↩]
- Heidari R, Sadeghi M, Talaei M, Rabiei K, Mohammadifard N, Sarrafzadegan N. Metabolic syndrome in menopausal transition: Isfahan Healthy Heart Program, a population based study. Diabetol Metab Syndr. 2010 Oct 5;2:59. doi: 10.1186/1758-5996-2-59[↩]
- Subramanian S, Chait A. Hypertriglyceridemia secondary to obesity and diabetes. Biochim Biophys Acta. 2012 May;1821(5):819-25. doi: 10.1016/j.bbalip.2011.10.003[↩]
- De Man FH, Cabezas MC, Van Barlingen HH, Erkelens DW, de Bruin TW. Triglyceride-rich lipoproteins in non-insulin-dependent diabetes mellitus: post-prandial metabolism and relation to premature atherosclerosis. Eur J Clin Invest. 1996 Feb;26(2):89-108. doi: 10.1046/j.1365-2362.1996.114256.x[↩]
- Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019 May;15(5):288-298. doi: 10.1038/s41574-019-0176-8[↩]
- Karanchi H, Muppidi V, Wyne K. Hypertriglyceridemia. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459368[↩]
- Joint committee for guideline revision. 2016 Chinese guidelines for the management of dyslipidemia in adults. J Geriatr Cardiol. 2018 Jan;15(1):1-29. doi: 10.11909/j.issn.1671-5411.2018.01.011[↩]
- Fan W, Philip S, Granowitz C, Toth PP, Wong ND. Prevalence of US Adults with Triglycerides ≥ 150 mg/dl: NHANES 2007-2014. Cardiol Ther. 2020 Jun;9(1):207-213. doi: 10.1007/s40119-020-00170-x[↩]
- Karpov Y, Khomitskaya Y. PROMETHEUS: an observational, cross-sectional, retrospective study of hypertriglyceridemia in Russia. Cardiovasc Diabetol. 2015 Aug 25;14:115. doi: 10.1186/s12933-015-0268-2[↩]
- Aekplakorn W. Thai National Health Examination VI (NHES VI) 2019.[↩]
- Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, Goldberg AC, Howard WJ, Jacobson MS, Kris-Etherton PM, Lennie TA, Levi M, Mazzone T, Pennathur S; American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011 May 24;123(20):2292-333. doi: 10.1161/CIR.0b013e3182160726[↩][↩][↩][↩][↩]
- Karanchi H, Wyne K. Hypertriglyceridemia. [Updated 2019 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459368 [↩][↩]
- Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, et. al. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292–2333. doi: 10.1161/CIR.0b013e3182160726.[↩]
- Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, Boekholdt SM, Khaw KT, Gudnason V. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation. 2007;115:450–458. doi: 10.1161/CIRCULATIONAHA.106.637793.[↩]
- TG and HDL Working Group of the Exome Sequencing Project, National Heart, Lung, and Blood Institute. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med.2014;371:22–31.[↩]
- Wyler von Ballmoos MC, Haring B, Sacks FM. The risk of cardiovascular events with increased apolipoprotein CIII: a systematic review and meta-analysis. J Clin Lipidol. 2015;9:498–510. doi: 10.1016/j.jacl.2015.05.002.[↩]
- Mensink RP. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis. Geneva, Switzerland: World Health Organization; 2016.[↩]
- Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, Goldberg AC, Howard WJ, Jacobson MS, Kris-Etherton PM, Lennie TA, Levi M, Mazzone T, Pennathur S; on behalf of the American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292–2333. doi: 10.1161/CIR.0b013e3182160726.[↩][↩]
- Sacks FM, Carey VJ, Anderson CA, Miller ER 3rd, Copeland T, Charleston J, Harshfield BJ, Laranjo N, McCarron P, Swain J, White K, Yee K, Appel LJ. Effects of high vs low glycemic index ofdietary carbohydrate on cardiovascular disease risk factors andinsulin sensitivity: the OmniCarb randomized clinical trial. JAMA.2014;312:2531–2541. doi: 10.1001/jama.2014.16658.[↩]
- Generoso G, Janovsky CCPS, Bittencourt MS. Triglycerides and triglyceride-rich lipoproteins in the development and progression of atherosclerosis. Curr Opin Endocrinol Diabetes Obes. 2019 Apr;26(2):109-116.[↩]
- Akinci B, Sahinoz M, Oral E. Lipodystrophy Syndromes: Presentation and Treatment. [Updated 2018 Apr 24]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Figure 6, [Generalized lack of subcutaneous fat…]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513130/figure/lipodystrophy_f_lipodystrophy_etx-obesity-new-ch15-fig6[↩]
- Nayak KR, Daly RG. Images in clinical medicine. Eruptive xanthomas associated with hypertriglyceridemia and new-onset diabetes mellitus. N Engl J Med. 2004 Mar 18;350(12):1235. doi: 10.1056/NEJMicm030676[↩]
- Hassing HC, Surendran RP, Mooij HL, Stroes ES, Nieuwdorp M, Dallinga-Thie GM. Pathophysiology of hypertriglyceridemia. Biochim Biophys Acta. 2012 May;1821(5):826-32. doi: 10.1016/j.bbalip.2011.11.010[↩]
- Laufs U, Parhofer KG, Ginsberg HN, Hegele RA. Clinical review on triglycerides. Eur Heart J. 2020 Jan 1;41(1):99-109c. doi: 10.1093/eurheartj/ehz785[↩][↩]
- Savitha Subramanian, Approach to the Patient With Moderate Hypertriglyceridemia, The Journal of Clinical Endocrinology & Metabolism, Volume 107, Issue 6, June 2022, Pages 1686–1697, https://doi.org/10.1210/clinem/dgac085[↩][↩][↩]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001 May 16;285(19):2486-97. doi: 10.1001/jama.285.19.2486[↩][↩]
- Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, Wilson DP, Brown WV. National lipid association recommendations for patient-centered management of dyslipidemia: part 1–full report. J Clin Lipidol. 2015 Mar-Apr;9(2):129-69. doi: 10.1016/j.jacl.2015.02.003[↩]
- Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Sacks F, Murad MH, Stalenhoef AF; Endocrine society. Evaluation and treatment of hypertriglyceridemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012 Sep;97(9):2969-89. doi: 10.1210/jc.2011-3213. Erratum in: J Clin Endocrinol Metab. 2015 Dec;100(12):4685. doi: 10.1210/jc.2015-3649[↩][↩][↩]
- Authors/Task Force Members:; Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, Hoes AW, Jennings CS, Landmesser U, Pedersen TR, Reiner Ž, Riccardi G, Taskinen MR, Tokgozoglu L, Verschuren WM, Vlachopoulos C, Wood DA, Zamorano JL. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016 Oct;253:281-344. doi: 10.1016/j.atherosclerosis.2016.08.018[↩]
- Hegele RA, Ginsberg HN, Chapman MJ, Nordestgaard BG, Kuivenhoven JA, Averna M, Borén J, Bruckert E, Catapano AL, Descamps OS, Hovingh GK, Humphries SE, Kovanen PT, Masana L, Pajukanta P, Parhofer KG, Raal FJ, Ray KK, Santos RD, Stalenhoef AF, Stroes E, Taskinen MR, Tybjærg-Hansen A, Watts GF, Wiklund O; European Atherosclerosis Society Consensus Panel. The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management. Lancet Diabetes Endocrinol. 2014 Aug;2(8):655-66. doi: 10.1016/S2213-8587(13)70191-8[↩]
- Subramanian S. Hypertriglyceridemia: Pathophysiology, Role of Genetics, Consequences, and Treatment. [Updated 2024 Jan 8]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK326743[↩]
- Blood Cholesterol Diagnosis. https://www.nhlbi.nih.gov/health/blood-cholesterol/diagnosis[↩][↩]
- Schaefer EJ, Geller AS, Endress G. The biochemical and genetic diagnosis of lipid disorders. Curr. Opin. Lipidol. 2019 Apr;30(2):56-62.[↩]
- Cox RA, García-Palmieri MR. Cholesterol, Triglycerides, and Associated Lipoproteins. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 31. Available from: https://www.ncbi.nlm.nih.gov/books/NBK351[↩][↩][↩]
- Ginsberg HN. New perspectives on atherogenesis: role of abnormal triglyceride-rich lipoprotein metabolism. Circulation. 2002 Oct 15;106(16):2137-42. doi: 10.1161/01.cir.0000035280.64322.31[↩]
- Kwiterovich PO Jr. Clinical relevance of the biochemical, metabolic, and genetic factors that influence low-density lipoprotein heterogeneity. Am J Cardiol. 2002 Oct 17;90(8A):30i-47i. doi: 10.1016/s0002-9149(02)02749-2[↩]
- Karalis DG. A Review of Clinical Practice Guidelines for the Management of Hypertriglyceridemia: A Focus on High Dose Omega-3 Fatty Acids. Adv Ther. 2017 Feb;34(2):300-323. doi: 10.1007/s12325-016-0462-y[↩][↩][↩]
- Yuan G, Al-Shali KZ, Hegele RA. Hypertriglyceridemia: its etiology, effects and treatment. CMAJ. 2007;176(8):1113–1120. doi:10.1503/cmaj.060963 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1839776[↩]
- Brunzell JD. Clinical practice. Hypertriglyceridemia. N Engl J Med. 2007 Sep 6;357(10):1009-17. doi: 10.1056/NEJMcp070061[↩]
- Athyros VG, Papageorgiou AA, Hatzikonstandinou HA, Didangelos TP, Carina MV, Kranitsas DF, Kontopoulos AG. Safety and efficacy of long-term statin-fibrate combinations in patients with refractory familial combined hyperlipidemia. Am J Cardiol. 1997 Sep 1;80(5):608-13. doi: 10.1016/s0002-9149(97)00430-x[↩][↩]
- Pradhan A, Bhandari M, Vishwakarma P, Sethi R. Triglycerides and Cardiovascular Outcomes-Can We REDUCE-IT ? Int J Angiol. 2020 Mar;29(1):2-11. doi: 10.1055/s-0040-1701639[↩]
- Park Y, Harris WS. Omega-3 fatty acid supplementation accelerates chylomicron triglyceride clearance. J Lipid Res. 2003 Mar;44(3):455-63. doi: 10.1194/jlr.M200282-JLR200[↩]
- Kamanna VS, Kashyap ML. Mechanism of action of niacin. Am J Cardiol. 2008 Apr 17;101(8A):20B-26B. doi: 10.1016/j.amjcard.2008.02.029[↩]
- Lv YB, Mao C, Gao X, Yin ZX, Kraus VB, Yuan JQ, Zhang J, Luo JS, Zeng Y, Shi XM. Triglycerides Paradox Among the Oldest Old: “The Lower the Better?”. J Am Geriatr Soc. 2019 Jan 10[↩]
- De Natale C, Annuzzi G, Bozzetto L, Mazzarella R, Costabile G, Ciano O, Riccardi G, Rivellese AA. Effects of a plant-based high-carbohydrate/high-fiber diet versus high-monounsaturated fat/low-carbohydrate diet on postprandial lipids in type 2 diabetic patients. Diabetes Care. 2009 Dec;32(12):2168-73. doi: 10.2337/dc09-0266[↩]
- Meng H, Zhu L, Kord-Varkaneh H, O Santos H, Tinsley GM, Fu P. Effects of intermittent fasting and energy-restricted diets on lipid profile: A systematic review and meta-analysis. Nutrition. 2020 Sep;77:110801. doi: 10.1016/j.nut.2020.110801[↩]
- Yang F, Liu C, Liu X, Pan X, Li X, Tian L, Sun J, Yang S, Zhao R, An N, Yang X, Gao Y, Xing Y. Effect of Epidemic Intermittent Fasting on Cardiometabolic Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Nutr. 2021 Oct 18;8:669325. doi: 10.3389/fnut.2021.669325[↩]
- Kirkpatrick CF, Bolick JP, Kris-Etherton PM, Sikand G, Aspry KE, Soffer DE, Willard KE, Maki KC. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J Clin Lipidol. 2019 Sep-Oct;13(5):689-711.e1. doi: 10.1016/j.jacl.2019.08.003[↩][↩]
- Goldberg IJ, Ibrahim N, Bredefeld C, Foo S, Lim V, Gutman D, Huggins LA, Hegele RA. Ketogenic diets, not for everyone. J Clin Lipidol. 2021 Jan-Feb;15(1):61-67. doi: 10.1016/j.jacl.2020.10.005[↩]
- Seidelmann SB, Claggett B, Cheng S, Henglin M, Shah A, Steffen LM, Folsom AR, Rimm EB, Willett WC, Solomon SD. Dietary carbohydrate intake and mortality: a prospective cohort study and meta-analysis. Lancet Public Health. 2018 Sep;3(9):e419-e428. doi: 10.1016/S2468-2667(18)30135-X[↩]
- Davidson M.H. Mechanisms for the hypotriglyceridemic effect of marine omega-3 fatty acids. Am. J. Cardiol. 2006;98:27i–33i. doi: 10.1016/j.amjcard.2005.12.024[↩]
- Dallongeville J., Boulet L., Davignon J., Lussier-Cacan S. Fish oil supplementation reduces beta-very low density lipoprotein in type III dysbetalipoproteinemia. Arterioscler. Thromb. 1991;11:864–871. doi: 10.1161/01.ATV.11.4.864[↩]
- Skulas-Ray A.C., West S.G., Davidson M.H., Kris-Etherton P.M. Omega-3 fatty acid concentrates in the treatment of moderate hypertriglyceridemia. Expert Opin. Pharmacother. 2008;9:1237–1248. doi: 10.1517/14656566.9.7.1237[↩]
- Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet. 1999 Aug 7;354(9177):447-55. Erratum in: Lancet 2001 Feb 24;357(9256):642. Erratum in: Lancet. 2007 Jan 13;369(9556):106.[↩]
- Yokoyama M., Origasa H., Matsuzaki M., Matsuzawa Y., Saito Y., Ishikawa Y., Oikawa S., Sasaki J., Hishida H., Itakura H., et al. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): A randomised open-label, blinded endpoint analysis. Lancet. 2007;369:1090–1098. doi: 10.1016/S0140-6736(07)60527-3[↩]
- Jacobson TA, Ito MK, Maki KC, et al. National Lipid Association recommendations for patient-centered management of dyslipidemia: part 1—full report. J Clin Lipidol. 2015;9:129–169. doi: 10.1016/j.jacl.2015.02.003[↩]
- Jacobson TA, Maki KC, Orringer CE, et al. National Lipid Association recommendations for patient-centered management of dyslipidemia: part 2. J Clin Lipidol. 2015;9:S1–S122. doi: 10.1016/j.jacl.2015.09.002[↩]
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2889–2934. doi: 10.1016/j.jacc.2013.11.002[↩]
- Miller M, Cannon CP, Murphy SA, Qin J, Ray KK, Braunwald E. Impact of triglyceride levels beyond low-density lipoprotein cholesterol after acute coronary syndrome in the PROVE IT-TIMI 22 trial. J Am Coll Cardiol. 2008;51:724–730. doi: 10.1016/j.jacc.2007.10.038[↩]
- Faergeman O, Holme I, Fayyad R, et al. Plasma triglycerides and cardiovascular events in the treating to new targets and incremental decrease in end-points through aggressive lipid lowering trials of statins in patients with coronary artery disease. Am J Cardiol. 2009;104:459–463. doi: 10.1016/j.amjcard.2009.04.008[↩]
- McKenney JM, Farnier M, Lo KW, Bays HE, Perevozkaya I, Carlson G, Davies MJ, Mitchel YB, Gumbiner B. Safety and efficacy of long-term co-administration of fenofibrate and ezetimibe in patients with mixed hyperlipidemia. J Am Coll Cardiol. 2006 Apr 18;47(8):1584-7. doi: 10.1016/j.jacc.2005.11.072[↩]
- Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA. 1986 Nov 28. 256(20):2823-8.[↩]
- Fan W, Philip S, Granowitz C, Toth PP, Wong ND. Hypertriglyceridemia in statin-treated US adults: the National Health and Nutrition Examination Survey. J Clin Lipidol. 2019 Jan – Feb. 13 (1):100-8.[↩]
- Pedersen SB, Langsted A, Nordestgaard BG. Nonfasting Mild-to-Moderate Hypertriglyceridemia and Risk of Acute Pancreatitis. JAMA Intern Med. 2016 Dec 1. 176 (12):1834-42.[↩]
- Athyros VG, Giouleme OI, Nikolaidis NL, Vasiliadis TV, Bouloukos VI, Kontopoulos AG, et al. Long-term follow-up of patients with acute hypertriglyceridemia-induced pancreatitis. J Clin Gastroenterol. 2002 Apr. 34(4):472-5.[↩]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001 May 16. 285(19):2486-97.[↩]
- Brunzell JD, Bierman EL. Chylomicronemia syndrome. Interaction of genetic and acquired hypertriglyceridemia. Med Clin North Am. 1982 Mar;66(2):455-68. doi: 10.1016/s0025-7125(16)31430-4[↩]
- Chait A, Brunzell JD. Chylomicronemia syndrome. Adv Intern Med. 1992. 37:249-73.[↩]
- Lee MK, Han K, Kim B, Kim JD, Jung Kim M, Kim B, Heo J, Ahn J, Sohn SY, Lee JH. Cumulative exposure to hypertriglyceridemia and risk of type 2 diabetes in young adults. Diabetes Res Clin Pract. 2024 Feb;208:111109. doi: 10.1016/j.diabres.2024.111109[↩][↩][↩]
- Shand G, Fuller DT, Lufkin L, Lovelett C, Pal N, Mondal S, Sur S. A stronger association of depression with rheumatoid arthritis in presence of obesity and hypertriglyceridemia. Front Epidemiol. 2023 Dec 15;3:1216497. doi: 10.3389/fepid.2023.1216497[↩][↩]





{kind=link}