Contents
- What is hypertrophic cardiomyopathy
What is hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy is an inherited disease of your heart muscle, where the muscle wall (myocardium) of your heart becomes thickened. Hypertrophic cardiomyopathy is caused by a change or mutation in one or more genes and is passed on through families. Each child of someone with hypertrophic cardiomyopathy has a 50 per cent chance of inheriting the condition. Most often diagnosed during infancy or adolescence, hypertrophic cardiomyopathy is the second most common form of heart muscle disease and comprises about 35–40% of cardiomyopathies in children.
In familial hypertrophic cardiomyopathy the thickening usually occurs in the interventricular septum, which is the muscular wall that separates the lower left chamber of the heart (the left ventricle) from the lower right chamber (the right ventricle). In some people, thickening of the interventricular septum impedes the flow of oxygen-rich blood from the heart, which may lead to an abnormal heart sound during a heartbeat (heart murmur) and other signs and symptoms of the condition. Other affected individuals do not have physical obstruction of blood flow, but the pumping of blood is less efficient, which can also lead to symptoms of the condition. Cardiac hypertrophy often begins in adolescence or young adulthood, although it can develop at any time throughout life.
The symptoms of familial hypertrophic cardiomyopathy are variable, even within the same family. Many affected individuals have no symptoms. Other people with familial hypertrophic cardiomyopathy may experience chest pain; shortness of breath, especially with physical exertion; a sensation of fluttering or pounding in the chest (palpitations); lightheadedness; dizziness; and fainting.
While most people with familial hypertrophic cardiomyopathy are symptom-free or have only mild symptoms, this condition can have serious consequences. It can cause abnormal heart rhythms (arrhythmias) that may be life threatening. People with familial hypertrophic cardiomyopathy have an increased risk of sudden death, even if they have no other symptoms of the condition. A small number of affected individuals develop potentially fatal heart failure, which may require heart transplantation.
Hypertrophic cardiomyopathy is very common and can affect people of any age. Hypertrophic cardiomyopathy affects men and women equally.
About 1 in 500 of the US population has familial hypertrophic cardiomyopathy, although most people who have hypertrophic cardiomyopathy have few, if any, symptoms. Hypertrophic cardiomyopathy affects up to 500,000 people in the United States. with children under age 12 accounting for less than 10% of all cases. According to the Pediatric Cardiomyopathy Registry, Hypertrophic cardiomyopathy occurs at a rate of five per 1 million children. Familial hypertrophic cardiomyopathy is the most common genetic heart disease in the United States.
If you have hypertrophic cardiomyopathy, the muscular wall of your heart – the myocardium – becomes thickened without an obvious cause, making the heart muscle stiff. Usually the ventricles, the lower chambers of the heart, and septum (the wall that separates the left and right side of the heart) thicken. The thickened areas create narrowing or blockages in the ventricles (hypertrophic obstructive cardiomyopathy), making it harder for the heart to pump blood. Hypertrophic cardiomyopathy also can cause stiffness of the ventricles, changes in the mitral valve, and cellular changes in the heart tissue. Hypertrophic cardiomyopathy also can affect the heart’s mitral valve, causing blood to leak backward through the valve.
Sometimes, the thickened heart muscle doesn’t block blood flow out of the left ventricle. This is referred to as non-obstructive hypertrophic cardiomyopathy. In both obstructive and non-obstructive hypertrophic cardiomyopathy, the thickened muscle makes the inside of the left ventricle smaller, so it holds less blood. The walls of the ventricle may stiffen, and as a result, the ventricle is less able to relax and fill with blood. This thickening makes it harder for your heart to pump blood out of your heart and around your body. This can raise blood pressure in the ventricles and the blood vessels of the lungs. Changes also occur to the cells in the damaged heart muscle, which may disrupt the heart’s electrical signals and lead to arrhythmias.
How thick your muscle is and how much of your muscle is affected, varies from one person to another. The left ventricle (one of your heart’s four chambers) is almost always affected, and in some people the muscle of the right ventricle also thickens.
Hypertrophic cardiomyopathy often goes undiagnosed because many people with the disease have few, if any, symptoms and can lead normal lives with no significant problems. However, in a small number of people with hypertrophic cardiomyopathy, the thickened heart muscle can cause shortness of breath, chest pain, an inability to exercise or problems in the heart’s electrical system, resulting in life-threatening abnormal heart rhythms (arrhythmias).
It is rare, but some people with hypertrophic cardiomyopathy can have sudden cardiac arrest during very vigorous physical activity. The physical activity can trigger dangerous arrhythmias. Ask your doctor what types and amounts of physical activity are safe for you.
Other Names for Hypertrophic Cardiomyopathy
- Asymmetric septal hypertrophy
- Familial hypertrophic cardiomyopathy
- Hypertrophic nonobstructive cardiomyopathy
- Hypertrophic obstructive cardiomyopathy
- Idiopathic hypertrophic subaortic stenosis
How serious is hypertrophic cardiomyopathy?
Most people with hypertrophic cardiomyopathy will be able to live a full, normal life. Some people don’t even have symptoms and don’t need treatment.
But that doesn’t mean the condition can’t be serious. Hypertrophic cardiomyopathy is the most common cause of sudden unexpected death in childhood and in young athletes.
The main heart chambers can become stiff, leading to back pressure on the smaller collecting chambers. This can sometimes worsen the symptoms of heart failure and lead to abnormal heart rhythms (atrial fibrillation).
Blood flow from the heart may become reduced or restricted (known as obstructive hypertrophic cardiomyopathy).
Also, the mitral heart valve can become leaky (mitral regurgitation), causing blood to leak backwards.
These heart changes can cause dizziness, chest pain, shortness of breath and temporary loss of consciousness.
You’ll also be at greater risk of developing endocarditis (a heart infection).
If you have severe hypertrophic cardiomyopathy, you’ll need to see your doctor regularly so your condition can be monitored.
Your doctor will advise about the level and amount of exercise you can do and sensible lifestyle changes to make.
Human Heart
The heart is a specialized muscle that contracts regularly and continuously, pumping blood to the body and the lungs. It has four chambers – two at the top (the atria), and two at the bottom (the ventricles). See the Figures 1 to 3 below.
The heart is made up of three layers:
- the endocardium
- the myocardium
- the pericardium.
The endocardium is a thin layer on the inside of the heart, lining the chambers and valves. The myocardium is the thick, muscular layer of the heart that contracts and squeezes the blood out of the heart. It’s this layer that is affected by cardiomyopathy. The pericardium is a thin, double layer that forms a protective sac around the outside of the heart. It contains a small amount of fluid – called pericardial fluid – which acts as a lubricant when the heart is contracting.
The pumping action of the heart is caused by a flow of electricity through the heart that repeats itself in a cycle. This is normally triggered by the heart’s natural pacemaker, the SA node (sino-atrial node), which is in the right atrium (see Figure 4 below). The SA node sends out regular electrical impulses, which make the atria contract and pump blood into the ventricles. The electrical impulse then passes to the ventricles through a form of ‘junction box’ called the AV node (atrio-ventricular node). This causes the ventricles to contract and pump blood out of the heart. The blood from the right ventricle goes through the pulmonary artery to the lungs, and the blood from the left ventricle goes through the aorta and then around the body.
Figure 1. The anatomy of the heart
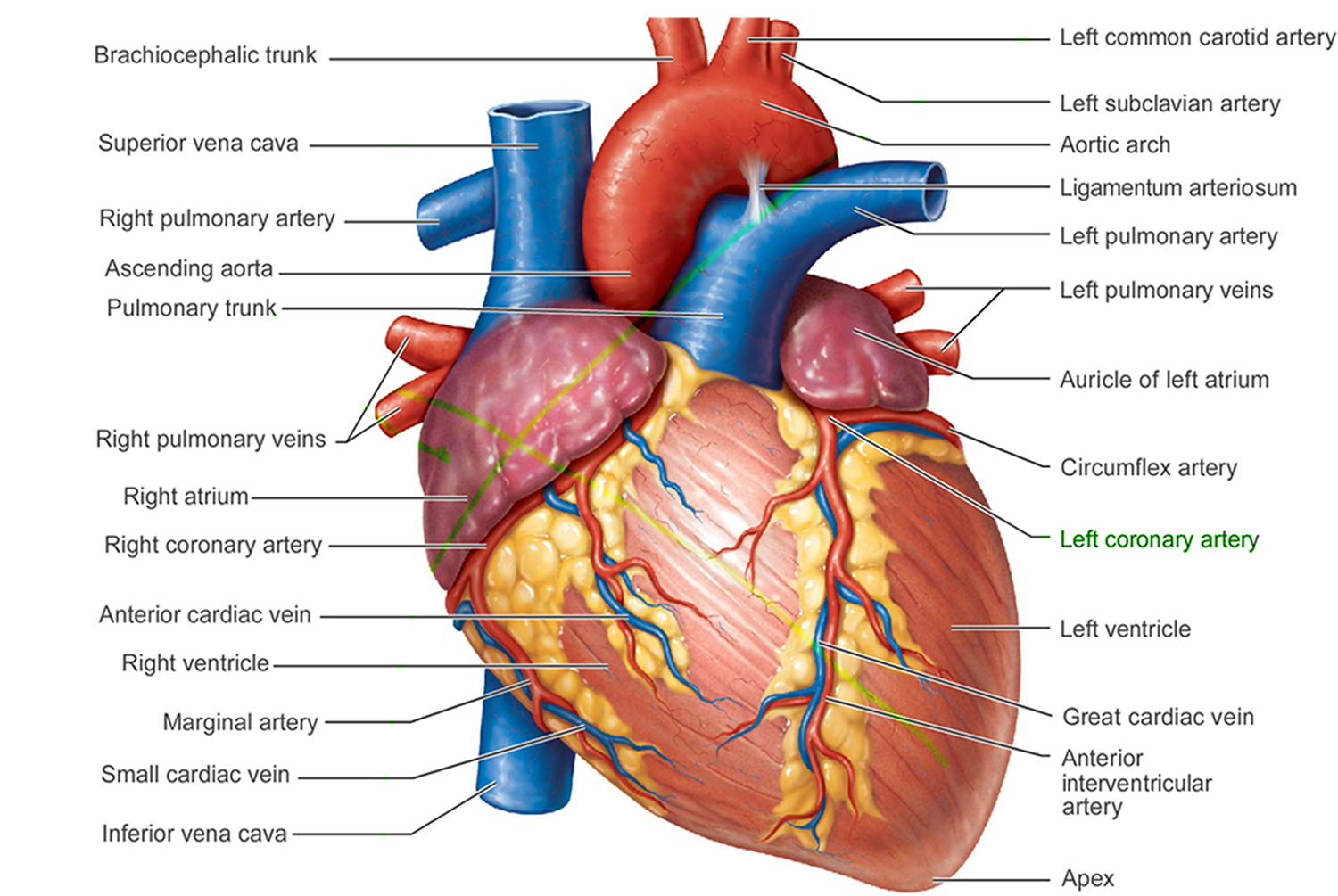
Figure 2. The anatomy of the heart chambers
 Figure 3. Normal heart blood flow
Figure 3. Normal heart blood flow Figure 4. The heart’s electrical system
Figure 4. The heart’s electrical system
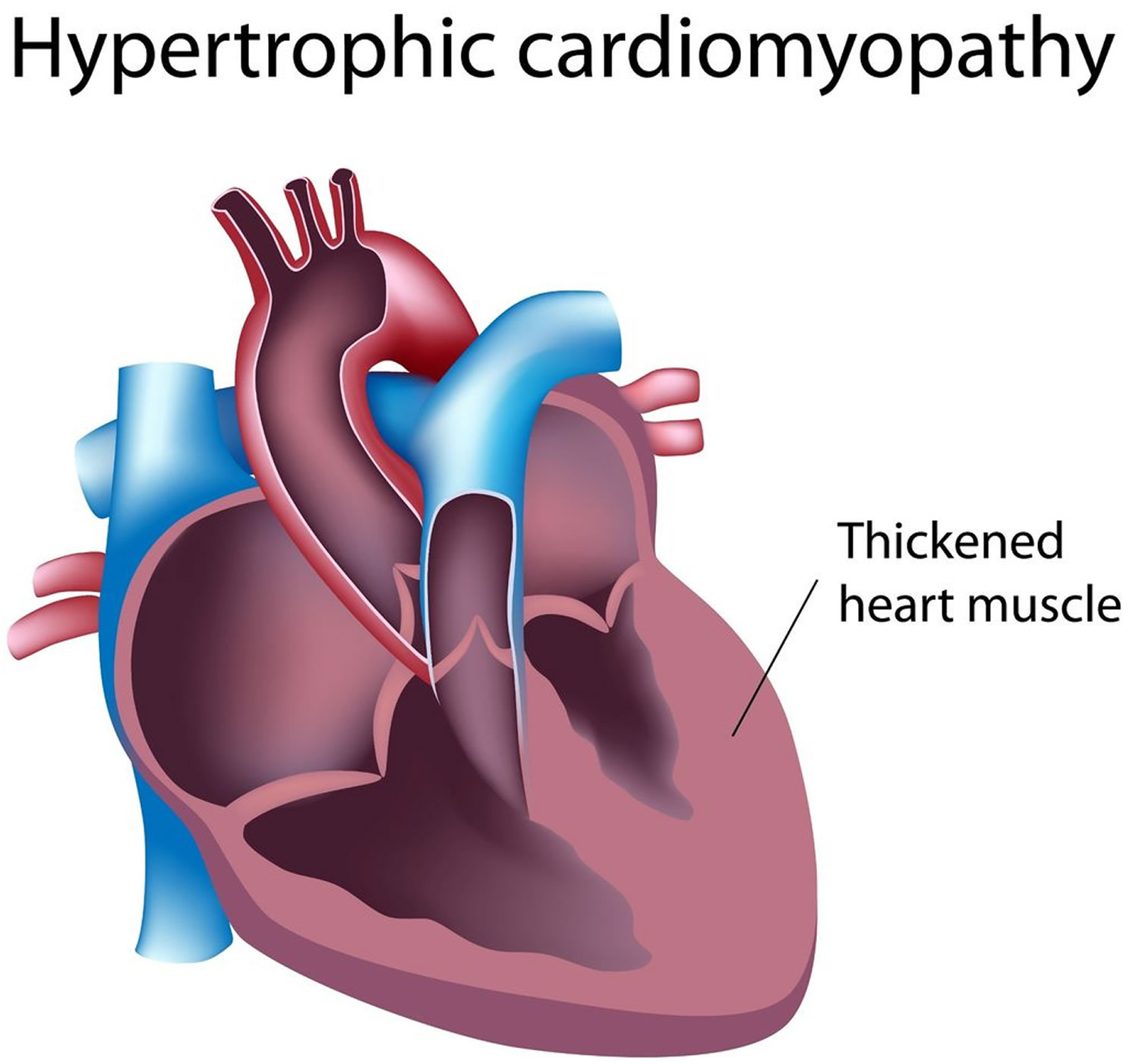
 Figure 5. Hypertrophic cardiomyopathy
Figure 5. Hypertrophic cardiomyopathy
 Hypertrophic cardiomyopathy causes
Hypertrophic cardiomyopathy causes
Hypertrophic cardiomyopathy usually is inherited. It’s caused by a change in some of the genes in heart muscle proteins. Hypertrophic cardiomyopathy also can develop over time because of high blood pressure or aging. Diseases such as diabetes or thyroid disease can cause hypertrophic cardiomyopathy. However, the cause of the disease isn’t known.
Familial hypertrophic cardiomyopathy is caused by mutations in any of several genes. The genes most commonly responsible are the MYH7, MYBPC3, TNNT2, and TNNI3 genes. Other genes that have not yet been identified may also be responsible for familial hypertrophic cardiomyopathy 1.
The proteins produced from the genes associated with familial hypertrophic cardiomyopathy play important roles in contraction of the heart muscle by forming muscle cell structures called sarcomeres. Sarcomeres, which are the basic units of muscle contraction, are made up of thick and thin protein filaments. The overlapping thick and thin filaments attach to each other and release, which allows the filaments to move relative to one another so that muscles can contract. In the heart, regular contractions of cardiac muscle pump blood to the rest of the body.
The protein produced from the MYH7 gene, called cardiac beta (β)-myosin heavy chain, is the major component of the thick filament in sarcomeres. The protein produced from the MYBPC3 gene, cardiac myosin binding protein C, associates with the thick filament, providing structural support and helping to regulate muscle contractions.
The TNNT2 and TNNI3 genes provide instructions for making cardiac troponin T and cardiac troponin I, respectively, which are two of the three proteins that make up the troponin protein complex found in cardiac muscle cells. The troponin complex associates with the thin filament of sarcomeres. It controls muscle contraction and relaxation by regulating the interaction of the thick and thin filaments.
While it is unclear exactly how mutations in these genes cause familial hypertrophic cardiomyopathy, they are thought to lead to abnormal structure or function of sarcomeres, or reduce the amount of proteins made. When the function of sarcomeres is impaired, normal heart muscle contractions are disrupted 1.
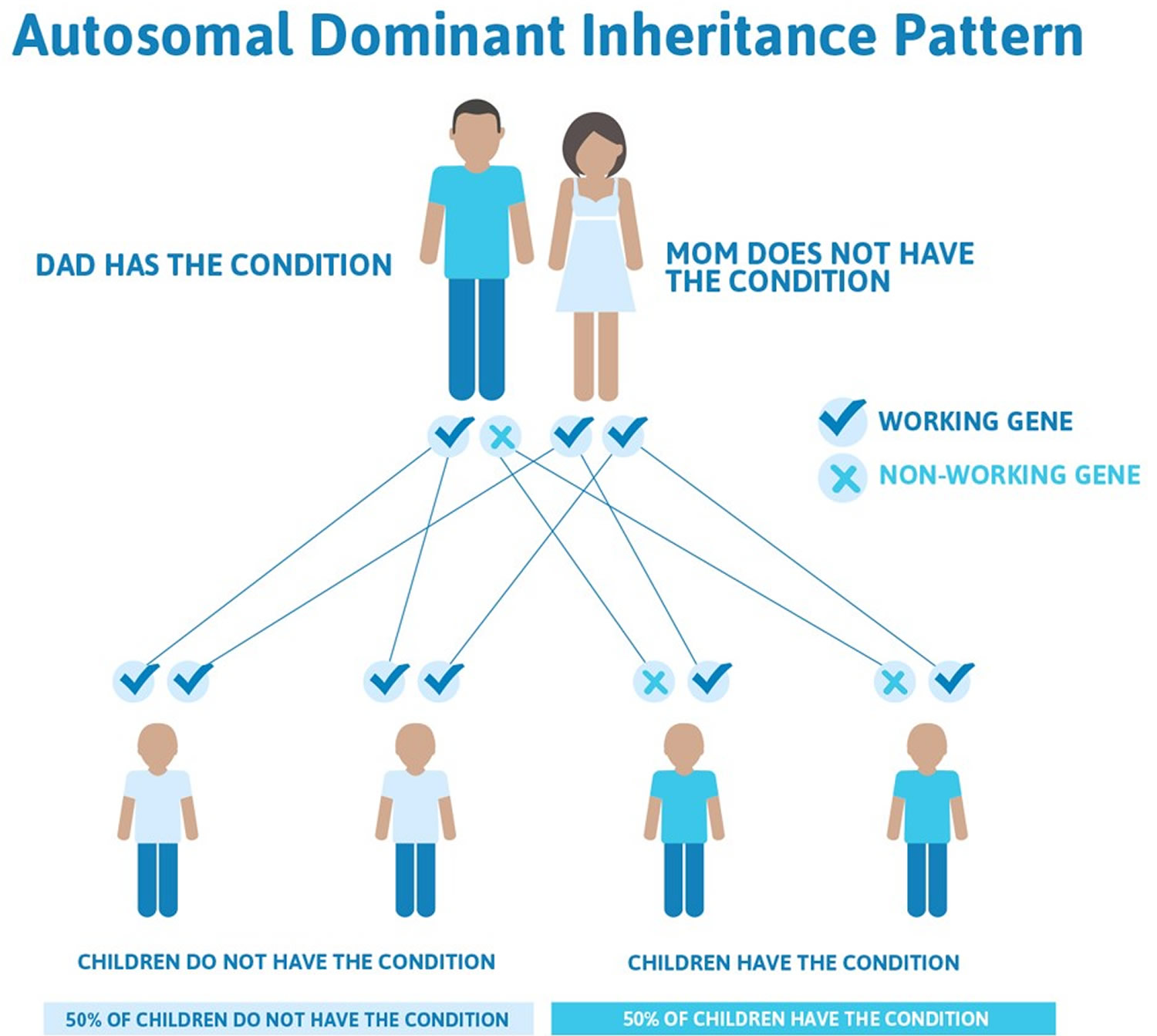
Familial hypertrophic cardiomyopathy is inherited in an autosomal dominant manner. This means that having only one changed (mutated) copy of the responsible gene in each cell is enough to cause features of the condition. When a person with an autosomal dominant condition has children, each child has a 50% (1 in 2) chance to inherit the mutated copy of the gene. First-degree relatives — parents, children or siblings — of a person with hypertrophic cardiomyopathy should ask their doctors about screening for the disease.
In rare cases, a person with familial hypertrophic cardiomyopathy has a mutation in both copies of the responsible gene, which leads to more severe signs and symptoms.
Figure 6. Familial hypertrophic cardiomyopathy autosomal dominant inheritance pattern
Hypertrophic cardiomyopathy symptoms
Signs and symptoms of hypertrophic cardiomyopathy may include one or more of the following:
- Shortness of breath, especially during exercise
- Chest pain, especially during exercise
- Palpitations – sensation of rapid, fluttering or pounding heartbeats
- Light headedness and fainting, especially during or just after exercise or exertion
- Heart murmur, which a doctor might detect while listening to your heart
You may find that you never have any serious problems related to your condition, and with treatment, your symptoms should be controlled. However some people may find that their symptoms worsen or become harder to control in later life.
The area of heart muscle that is affected by hypertrophic cardiomyopathy and the amount of stiffening that occurs will determine how the symptoms affect you.
For some people, a number of other conditions can develop as a result of having hypertrophic cardiomyopathy. These may include abnormal heart rhythms, or arrythmias, including heart block and endocarditis.
Hypertrophic cardiomyopathy life expectancy
Research has shown that, with proper treatment and follow-up, most people with hypertrophic cardiomyopathy live a normal life.
However, because there is a very small risk of getting a life-threatening abnormal heart rhythm, a small number of people with hypertrophic cardiomyopathy are at risk of sudden cardiac death. It’s important to discuss this risk with your doctor, who may offer medication or advise that you need to have an implantable cardioverter defibrillator (ICD) fitted if you are at an increased risk.
The overall annual mortality from sudden death is 3-5% in adults and at least 6% in children and young adults. However, severity of disease and prognosis varies widely according to the genetic features involved. Certain genes are associated with a worse prognosis.
You may have to make some small changes to your lifestyle, such as avoiding competitive sports, but you should be able to continue to work and drive a car, for example.
However, you will not be able to drive a commercial passenger vehicle and you may have to reconsider manual jobs which involve strenuous activity.
Hypertrophic cardiomyopathy complications
Many people with hypertrophic cardiomyopathy don’t experience significant health problems. But some people experience complications, including:
- Atrial fibrillation. Thickened heart muscle, as well as the abnormal structure of heart cells, can disrupt the normal functioning of the heart’s electrical system, resulting in fast or irregular heartbeats. Atrial fibrillation can also increase your risk of developing blood clots, which can travel to your brain and cause a stroke.
- Sudden cardiac death. Ventricular tachycardia and ventricular fibrillation can cause sudden cardiac death. People with hypertrophic cardiomyopathy have an increased risk of sudden cardiac death, although such deaths are rare. Sudden cardiac death is estimated to occur in about 1 percent of people with HCM each year. Hypertrophic cardiomyopathy can cause heart-related sudden death in people of all ages, but the condition most often causes sudden cardiac death in people under the age of 30.
- Obstructed blood flow. In many people, the thickened heart muscle obstructs the blood flow leaving the heart. Obstructed blood flow can cause shortness of breath with exertion, chest pain, dizziness and fainting spells.
- Dilated cardiomyopathy. Over time, thickened heart muscle may become weak and ineffective in a very small percentage of people with HCM. The ventricle becomes enlarged (dilated), and its pumping ability becomes less forceful.
- Mitral valve problems. The thickened heart muscle can leave a smaller space for blood to flow, causing blood to rush through your heart valves more quickly and forcefully. This increased force can prevent the valve between your heart’s left atrium and left ventricle (mitral valve) from closing properly. As a result, blood can leak backward into the left atrium (mitral valve regurgitation), possibly leading to worsening symptoms.
- Heart failure. The thickened heart muscle can eventually become too stiff to effectively fill with blood. As a result, your heart can’t pump enough blood to meet your body’s needs.
Hypertrophic cardiomyopathy prevention
Because hypertrophic cardiomyopathy is inherited, it can’t be prevented. But it’s important to identify the condition as early as possible to guide treatment and prevent complications.
Preventing sudden death
Implantation of a cardioverter-defibrillator has been shown to help prevent sudden cardiac death, which occurs in about 1 percent of people with hypertrophic cardiomyopathy.
Unfortunately, because many people with hypertrophic cardiomyopathy don’t realize they have it, there are instances where the first sign of a problem is sudden cardiac death. These cases can happen in seemingly healthy young people, including high school athletes and other young, active adults. News of these types of deaths generates understandable attention because they’re so unexpected, but parents should be aware these deaths are quite rare.
Still, doctors trained in heart abnormalities generally recommend that people with hypertrophic cardiomyopathy not participate in most competitive sports with the possible exception of some low-intensity sports. Discuss specific recommendations with your cardiologist.
Hypertrophic cardiomyopathy diagnosis
Your doctor may review your medical and family history, discuss your signs and symptoms, and conduct a physical examination. Your doctor may order several tests to diagnose hypertrophic cardiomyopathy.
The most common tests for hypertrophic cardiomyopathy are:
- ECG – this records the electrical activity of your heart.
- Echocardiogram – this shows the pumping action of your heart.
- Exercise test – in this test, an ECG is recorded while you’re on a treadmill or an exercise bike, to see how your heart works when it’s more active.
- MRI scan – creates detailed images of your internal organs, such as your heart.
- Echocardiogram. Your doctor is likely to recommend an imaging test called an echocardiogram to diagnose hypertrophic cardiomyopathy. This test allows your doctor to see whether your heart muscle is abnormally thick, your blood flow is obstructed and your heart valves are moving normally.In a transthoracic echocardiogram, a device (transducer) is pressed firmly against your skin. The transducer aims an ultrasound beam through your chest to your heart, producing moving images of the working of the heart.Doctors may sometimes conduct another type of echocardiogram called a transesophageal echocardiogram. In this test, a flexible tube containing a transducer is guided down your throat and into the tube connecting your mouth and stomach (esophagus). From there, the transducer can obtain more-detailed images of your heart. This test may be recommended if it’s difficult to get a clear picture of your heart with a standard echocardiogram or if the doctor wants to further examine your mitral valve. This test is done in very few people with hypertrophic cardiomyopathy.
Additional tests might be ordered to look for other effects of hypertrophic cardiomyopathy and help your doctor determine the most appropriate treatment for your condition. These tests include:
- Electrocardiogram (ECG). Wires (electrodes) attached to adhesive pads on your skin measure electrical impulses from your heart. An ECG can detect enlarged chambers of your heart and abnormal heart rhythms.
- Treadmill stress test. Your heart rhythm, blood pressure and breathing are monitored while you walk on a treadmill. Your doctor may recommend a treadmill stress test to evaluate symptoms, determine your exercise capacity and determine if exercise provokes abnormal heart rhythms.Treadmill stress tests are sometimes performed with echocardiography if you have symptoms of HCM, but a resting echocardiogram doesn’t show obstructed blood flow. Treadmill stress tests are commonly used in people with hypertrophic cardiomyopathy.
- Holter monitor. You may wear a portable ECG that records your heart’s activity continuously over one to two days. This test is often done in people with hypertrophic cardiomyopathy.
- Cardiac MRI. A cardiac MRI uses magnetic fields and radio waves to create images of your heart. Cardiac MRI is often used in addition to echocardiograms to evaluate people with hypertrophic cardiomyopathy.
- Cardiac catheterization. In this procedure, a catheter is inserted into a blood vessel, usually in your neck or groin area. The catheter is then carefully threaded to your heart chambers under guidance of an X-ray machine.In addition to measuring pressures in your heart, cardiac catheterization is used to obtain X-ray images (angiograms) of your heart and blood vessels. A dye is injected through the catheter to help visualize your heart and blood vessels. This test is rarely used to diagnose hypertrophic cardiomyopathy.
Genetic testing for hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy is an inherited heart condition, which means that it’s passed on through families. If your doctor thinks that you have hypertrophic cardiomyopathy, you may be offered a genetic test to identify a faulty gene that may be causing your condition.
If you’re found to have a faulty gene, your specialist may ask for your help in identifying close relatives – such as parents, siblings or children – who may have also inherited this gene.
Being tested as soon as possible means that your treatment can start as quickly as possible, which will reduce your risk of developing life-threatening abnormal heart rhythms.
- Genetic testing. Genetic tests may not provide a definitive answer because the genetic causes of hypertrophic cardiomyopathy aren’t fully understood. Only about 50 percent of families with hypertrophic cardiomyopathy have a currently detectable mutation, and some insurance companies may not cover genetic testing.However, if an abnormal gene is detected in your family, then other family members can learn if they are at risk of hypertrophic cardiomyopathy through genetic testing. Consultation with a genetic counselor is recommended to help you determine whether genetic testing is a good option for you.
- Echocardiogram. If genetic testing isn’t done, or if the results aren’t helpful, then your doctor may recommend echocardiograms on a regular basis if you have a family member with hypertrophic cardiomyopathy. Adolescents and competitive athletes should be screened once a year. Adults who don’t compete in athletics should be screened every five years.
Hypertrophic cardiomyopathy treatment
At present there is no cure for hypertrophic cardiomyopathy, but treatments are available to help control your symptoms and prevent complications. Your treatment will depend on how your heart is affected and what symptoms you have.
The goal of hypertrophic cardiomyopathy treatment is to relieve symptoms and prevent sudden cardiac death in people at high risk. Specific treatment varies depending on the severity of your symptoms. Your doctor will discuss with you the most appropriate treatment for your condition.
You may need:
- Medicines – to help control your blood pressure, abnormal heart rhythms or other symptoms you may have
- A Pacemaker – to control your heart rate
- An implantable cardioverter defibrillator (ICD) – if you are at risk of having a life threatening abnormal heart rhythm.
- Medications. You may be given medications to relax the heart muscle and to slow the heart rate so that the heart can pump more efficiently. Your doctor may recommend beta blockers such as metoprolol (Lopressor, Toprol), propranolol (Inderal, Innopran) or atenolol (Tenormin), calcium channel blockers such as verapamil (Verelan, Calan, Covera) or diltiazem (Cardizem, Tiazac, Dilacor), or medications to control your heart rhythm such as amiodarone (Pacerone) or disopyramide (Norpace).If you have atrial fibrillation, your doctor may prescribe blood thinners such as warfarin (Coumadin, Jantoven), dabigatran (Pradaxa), rivaroxaban (Xarelto) or apixaban (Eliquis) to reduce your risk of blood clots.
- Septal myectomy. A septal myectomy is an open-heart procedure in which the surgeon removes part of the thickened, overgrown septum between the ventricles. Removing part of this overgrown muscle improves blood flow and reduces mitral regurgitation.Surgeons may conduct this procedure using different approaches, depending on the location of the thickened heart muscle. In one type of septal myectomy called apical myectomy, surgeons remove thickened heart muscle from near the tip of the heart. Surgeons may sometimes perform mitral valve repair at the same time as a myectomy.A septal myectomy may be recommended if medications don’t relieve your symptoms. Most people who have a myectomy have no further symptoms. Septal myectomy is available only in medical centers that specialize in the treatment of hypertrophic cardiomyopathy.
- Septal ablation. In septal ablation, a small portion of the thickened heart muscle is destroyed by injecting alcohol through a long, thin tube (catheter) into the artery supplying blood to that area. This procedure may improve your symptoms. Possible complications with this procedure include heart block — a disruption of the heart’s electrical system — which requires implantation of a pacemaker.
- Implantable cardioverter-defibrillator (ICD). Doctors may recommend an ICD if you have life-threatening heart rhythm disorders (arrhythmias) such as ventricular tachycardia or ventricular fibrillation. An ICD is a small device that continuously monitors your heartbeat. It’s implanted in your chest like a pacemaker.If a life-threatening arrhythmia occurs, the ICD delivers precisely calibrated electrical shocks to restore a normal heart rhythm. Your doctor may recommend an ICD if you have hypertrophic cardiomyopathy and you’re at high risk of sudden cardiac death because of abnormal heart rhythms.
Lifestyle and home remedies
Lifestyle changes can reduce your risk of complications related to hypertrophic cardiomyopathy. Your doctor may recommend lifestyle changes, including:
- Getting physical activity. Competitive sports are generally not recommended for people with hypertrophic cardiomyopathy. Many people with hypertrophic cardiomyopathy may be able to participate in low- to moderate-intensity exercise as part of a healthy lifestyle. Ask your doctor for guidance.
- Eating a healthy diet. A healthy diet is an important part of maintaining your heart health.
- Maintaining a healthy weight. Maintaining a healthy weight will prevent excessive stress on your heart and reduce health risks associated with surgery or other procedures.
- Reducing alcohol use. If you have symptoms or a history of rhythms provoked by alcohol, ask your doctor for guidance about safe levels of alcohol use. Drinking too much alcohol can trigger irregular heart rhythms and can lead to increased blockage of blood flow in your heart.
- Taking your medications. Make sure to take your medications as prescribed.
- Having regular medical appointments. Your doctor may recommend regular follow-up appointments to evaluate your condition. Let your doctor know if you have any new or worse symptoms.
Pregnancy
Women who have hypertrophic cardiomyopathy can generally have normal pregnancies. However, if you have symptoms and complications of hypertrophic cardiomyopathy, your doctor may recommend that you see a doctor experienced in caring for women with high-risk conditions during your pregnancy.
Coping and support
Being diagnosed with hypertrophic cardiomyopathy can cause a range of difficult emotions. Like many people with this condition, you may experience feelings of grief, fear and anger. These responses are appropriate to the lifestyle changes that come with your diagnosis.
To cope with your condition:
- Reduce your stress. Find ways to reduce your stress.
- Get support. Get support from your friends and family.
- Follow lifestyle changes your doctor recommends. Making healthy lifestyle changes, such as eating a healthy diet and maintaining a healthy weight, can help you cope with living with your condition.





{kind=link}