Contents
What is keratoconus
Keratoconus is an eye condition that is characterized by a progressive thinning of the central zone of the cornea. This condition is the most common corneal dystrophy in the U.S., affecting 1 in every 2,000 Americans. However better screening techniques indicate that it may be as high as 1 in 500 persons. The onset of keratoconus can be anywhere between the ages of 8 and 45. Keratoconus is more prevalent in teenagers and adults in their 20s. Keratoconus tends to be more aggressive when diagnosed in adolescence. Progression usually continues until the age of about 40 years. Because it affects people from puberty onward, it can have a significant impact on a person’s education, work, social and family life if not treated correctly.
Keratoconus is when the middle of the cornea thins and gradually bulges outward, forming a rounded cone shape. These corneal abnormalities, which worsen over time, can lead to changes the cornea’s refractive power, producing moderate to severe distortion (irregular astigmatism) and nearsightedness (myopia), blurred vision that cannot be improved with corrective lenses and vision loss. Keratoconus may also cause swelling and a sight-impairing scarring of the tissue.
With keratoconus, try to avoid rubbing your eyes. This can damage thin corneal tissue and make your symptoms worse. If you have itchy eyes that cause you to rub, speak to your ophthalmologist about medicines to control your allergies.
Other corneal changes typical of keratoconus that can be seen during an eye exam include iron deposits in the cornea that form a yellow-to-brownish ring, called the Fleischer ring, surrounding the colored part of the eye (iris). Affected individuals may also develop Vogt’s striae, which are thin, vertical, white lines in the tissue at the back of the cornea.
Keratoconus may affect only one eye at first, but eventually the corneas of both eyes become misshapen, although they might not be affected with the same severity. Studies show that keratoconus occurs in one eye only in a very small percentage of cases (<1%) – and in those cases keratoconus may be present in the other eye but undetectable. As keratoconus worsens, people with this condition can develop corneal scarring, often caused by exposure of the abnormally thin cornea to prolonged contact lens use or excessive eye rubbing.
The eye changes characteristic of keratoconus typically begin in adolescence and slowly worsen until mid-adulthood at which point the shape of the cornea remains stable. People of African American and Latino heritage have 50 percent higher chance than whites of contracting keratoconus. And people with Asian heritage have a 39 percent lower rate of keratoconus eye disease.
Keratoconus rarely leads to permanent vision loss. However, the changes to the cornea make it impossible for the eye to focus without eyeglasses or contact lenses.
Keratoconus can be dangerous if laser vision correction surgery (laser-assisted-in-situ keratomileusis [LASIK] or photo refractive keratectomy [PRK]) is performed on the eye, because it can make the condition worse. Anyone who has even a small degree of keratoconus should not have laser vision correction surgery, unless recommended by the doctor in very specific circumstances.
Does keratoconus cause blindness?
Keratoconus does not cause blindness, except in the rare circumstances of a failed corneal transplant that cannot be treated. In those circumstances the other eye usually retains good quality vision and allows normal functioning. However, severe keratoconus can lead to a significant vision impairment resulting in legal blindness. Legal blindness means that the best vision that can be obtained by any correction is the largest letter on the standard eye chart. This is substantially reduced vision and well below the legal limit for driving.
I’ve been told my cornea is very thin, can my cornea perforate?
Even a very thin cornea can still be quite robust. A very thin cornea is usually not the reason why a decision is made to proceed to a corneal graft. Often a very thin cornea has significant scarring or distortion that results in very poor vision quality and the need for better vision results in a corneal graft. Perforation is extremely rare and is an ocular emergency. It requires immediate treatment by an ophthalmologist or at an eye clinic at a hospital. Perforation is treated by stitches or a special glue and bandage contact lens or corneal surgery. A corneal graft is usually required after corneal perforation.
Does pregnancy affect the progression of keratoconus?
Keratoconus often develops in teenage years and occasionally develops during pregnancy or advances during pregnancy. These times are associated with elevated hormone levels; however there is no evidence of a causal relationship.
Can progression in keratoconus be halted or reversed?
Collagen cross-linking is a relatively new treatment that has been shown to slow or halt progression in keratoconus. The procedure involves using riboflavin (vitamin B2) and ultraviolet light (UVA) to significantly increase the corneal rigidity or stiffness. The treatment promotes greater cross-links between the sheets of collagen in the stroma. During the procedure, the eye is anaesthetised and the epithelium is removed, then riboflavin drops are applied regularly through the procedure and the eye is exposed to UV radiation for 30 minutes. This technique has been shown to be safe for the cornea and internal eye structures and few long-term problems have been reported to date.
Other protocols which leave the epithelium in place have been shown to be less effective than the epithelium-off method.
Does keratoconus occur in families?
Some cases of keratoconus have a hereditary component; however its occurrence is sporadic. Some 20% of patients with keratoconus have relatives with keratoconus. Consequently, even if both parents have keratoconus they are unlikely to have children with keratoconus. In some cases there is a familial association and then it is likely that keratoconus follows a dominant type of transmission.
Because there is a genetic predisposition and evidence of higher rates of keratoconus in relatives of patients with keratoconus, it is important that there is regular screening for keratoconus in relatives of patients with keratoconus. This is to ensure early detection of progressive keratoconus before there is any significant deterioration of vision.
In marriages between first or second cousins there is a fourfold increase in the risk of keratoconus.
What about relatives of people with keratoconus?
Recent research has shown that 33% of relatives of people with keratoconus have subtle abnormalities of the cornea, such as a slightly thinner cornea or having a slightly asymmetrical corneal shape. These subtle changes do not indicate keratoconus. These relatives have otherwise normal eyes and the corneal abnormalities do not affect their vision. The subtle changes in the cornea can only be detected by using special instruments – pachymeter and topographer (see below – detection methods). These corneal abnormalities are stable, as only a small proportion of these relatives (20%) are likely to develop to full keratoconus.
Relatives of people with keratoconus may have a higher risk of developing irregularities in the corneal shape following laser refractive surgery to correct myopia or astigmatism. This is more likely in LASIK laser treatment that requires a thin corneal flap to be cut across the front of the cornea before the cornea is reshaped and thinned by the laser. Laser treatment that does not require a corneal flap (PRK – photorefractive keratectomy) is safer in these eyes. It is important that relatives of people with keratoconus who are considering laser refractive surgery, advise the practitioner so that comprehensive measurements can be made.
Cornea Anatomy
Although the cornea may look clear and seem to lack substance, it is a highly organized tissue. Unlike most tissues in the body, the cornea contains no blood vessels to nourish or protect it against infection. Instead, the cornea receives its nourishment from tears and the aqueous humor (a fluid in the front part of the eye that lies behind the cornea).
The tissues of the cornea are arranged in three basic layers, with two thinner layers, or membranes, between them. Each of these five layers has an important function. These layers are:
Epithelium
The epithelium is the cornea’s outermost layer and consists of 10% thickness of the cornea with the highest concentration of nerves in the body, very sensitive, 5-6 cells thick, heals very quickly.
Its primary functions are to:
- block the passage into the eye of foreign material, such as dust, water, and bacteria; and
- provide a smooth surface to absorb oxygen and nutrients from tears, which are then distributed to the other layers of the cornea.
The epithelium is filled with thousands of tiny nerve endings, which is why your eye may hurt when it is rubbed or scratched. The part of the epithelium that epithelial cells anchor and organize themselves to is called the basement membrane.
Bowman’s membrane
The next layer behind the basement membrane of the epithelium is a transparent film of tissue called Bowman’s layer, composed of protein fibers called collagen. If injured, Bowman’s layer can form a scar as it heals. If these scars are large and centrally located, they may cause vision loss.
Stroma
Behind Bowman’s layer is the stroma, which is the thickest layer of the cornea (90% thickness of the cornea). It is composed primarily of water and collagen. Collagen gives the cornea its strength, elasticity, and form. The unique shape, arrangement, and spacing of collagen proteins are essential in producing the cornea’s light-conducting transparency.
Descemet’s Membrane
Behind the stroma is Descemet’s membrane, a thin but strong film of tissue that serves as a protective barrier against infection and injuries. Descemet’s membrane is composed of collagen fibers that are different from those of the stroma, and are made by cells in the endothelial layer of the cornea (see above). Descemet’s membrane repairs itself easily after injury.
Endothelium
The endothelium is the thin, innermost layer of the cornea. Endothelial cells are important in keeping the cornea clear. Normally, fluid leaks slowly from inside the eye into the stroma. The endothelium’s primary task is to pump this excess fluid out of the stroma. Without this pumping action, the stroma would swell with water and become thick and opaque.
In a healthy eye, a perfect balance is maintained between the fluid moving into the cornea and the fluid pumping out of the cornea. Unlike the cells in Descemet’s membrane, endothelial cells that have been destroyed by disease or trauma are not repaired or replaced by the body.
Figure 1. Cornea (human eye)
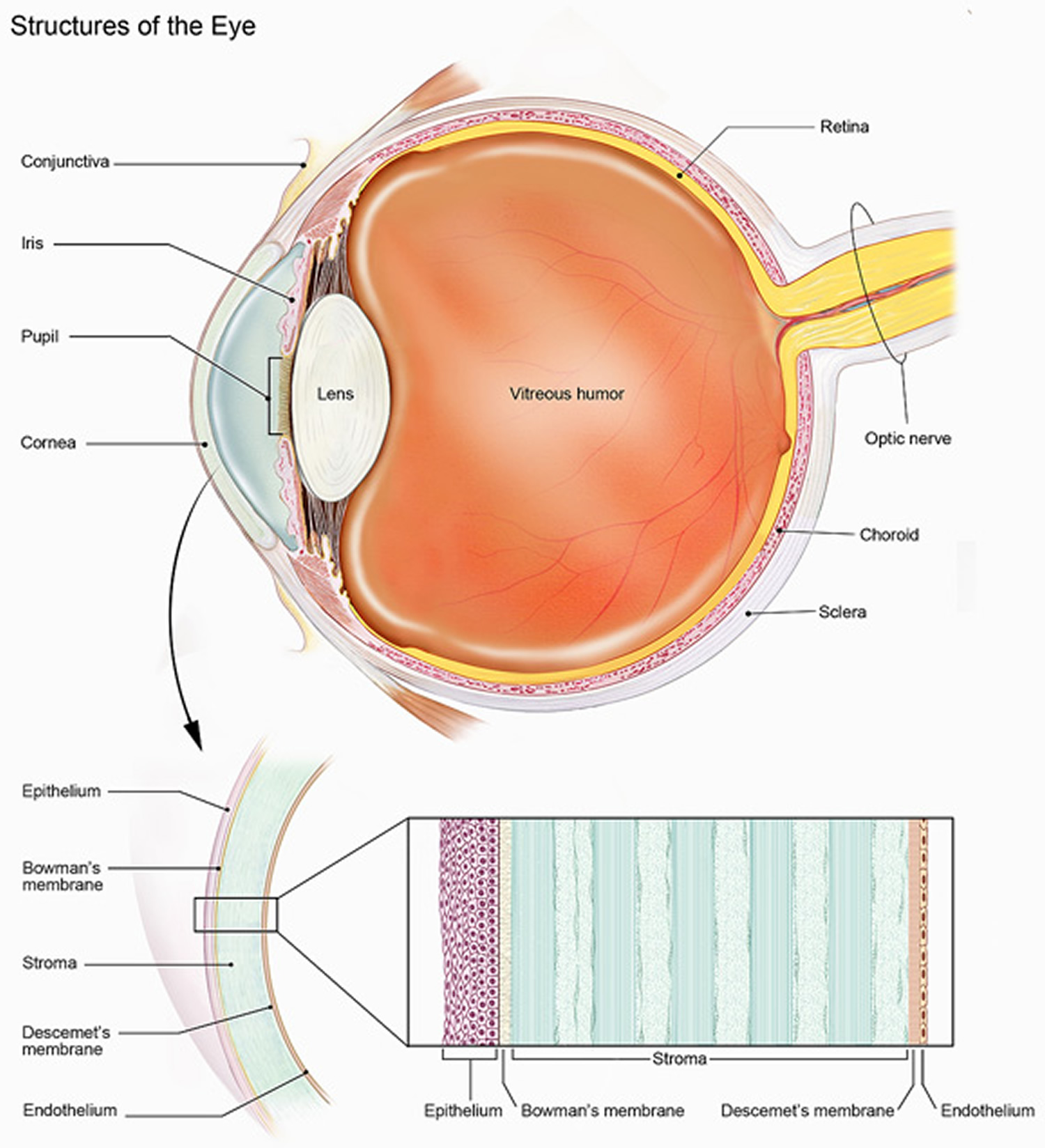 Figure 2. Keratoconus
Figure 2. Keratoconus
What does the cornea do?
The cornea acts as a barrier against dirt, germs, and other particles that can harm the eye. The cornea shares this protective task with the eyelids and eye sockets, tears, and the sclera (white part of the eye). The cornea also plays a key role in vision by helping focus the light that comes into the eye. The cornea is responsible for 65-75 percent of the eye’s total focusing power.
The cornea and lens of the eye are built to focus light on the retina, which is the light-sensitive tissue at the back of the eye. When light strikes the cornea, it bends—or refracts—the incoming light onto the lens. The lens refocuses that light onto the retina, which starts the translation of light into vision. The retina converts light into electrical impulses that travel through the optic nerve to the brain, which interprets them as images.
The refractive process the eye uses is similar to the way a camera takes a picture. The cornea and lens in the eye act as the camera lens. The retina is like the film (in older cameras), or the image sensor (in digital cameras). If the image is not focused properly, the retina makes a blurry image.
The cornea also serves as a filter that screens out damaging ultraviolet (UV) light from the sun. Without this protection, the lens and the retina would be exposed to injury from UV rays.
Keratoconus Stages
Keratoconus advances at varying rates and differently in each eye. Progression is generally more rapid, the earlier the age of onset. Keratoconus causes increasing blurriness and shortsightedness in vision, light sensitivity and halos and ghosting around light sources. Progression usually occurs to an age of around 40-45 years and then tends to stabilize. However some progression may be experienced by persons 50 or older. On average, the most significant progression occurs in the first 15-20 years after the time of onset.
Corneal collagen crosslinking, a procedure designed to harden the cornea and halt progression, is widely offered to patients today to prevent progression to the advanced and severe stages of keratoconus. It is hoped that in the future, crosslinking will significantly reduce rates of corneal transplantation and the difficulty of fitting contact lenses to keratoconus patients.
Early keratoconus
Forme Fruste keratoconus has only very slight corneal distortion; it has little or no effect on the quality of vision and exhibits minimal or no progression. Spectacles are usually successful in correcting the myopia and astigmatism and give adequate vision. Soft contact lenses, spherical or with a toric correction, can be a good option for general use or just for sporting activities.
Moderate keratoconus
Corneal distortion increases and corneal changes typical of keratoconus can be observed. As the vision quality with spectacles decreases, rigid gas permeable contact lenses become the option for better quality vision.
The rigid gas permeable contact lens covers the corneal irregularity with a regular hard surface and neutralises 90% of the corneal distortion. The focussing power of the contact lens can also compensate for any myopia, hyperopia and astigmatism resulting in better contrast, substantially reduced ghosting and flaring and overall much clearer vision.
Rigid gas permeable lenses are available in many diameters form 8.0mm up to 20.0mm in a miniscleral form. Hybrid lenses – RGP centre with a soft surround – can also give excellent vision with good comfort and stability. A new form of soft lens (KeraSoft) may also be effective in some cases.
Emergency spectacles can still be very useful as a back-up if an eye irritation arises or with lost lenses, even though the vision may not be 100%. Regular reviews are also essential to check that there has been no progression of the keratoconus, to check that the rigid gas permeable contact lenses are still fitting well, are in good condition, that the vision is stable and that the eye is healthy.
Advanced keratoconus
Substantial corneal distortion with moderate keratoconic corneal changes, slight to moderate corneal scarring present. Contact lens fitting as for moderate keratoconus except that there may be greater changes in the rigid gas permeable contact lens design, often using much steeper inside curvatures to maintain an appropriate fitting. Large miniscleral or scleral rigid gas permeable contact lenses may also be useful in unusually shaped corneae as they vault the cornea and improve stability and comfort.
Severe keratoconus
Dramatic corneal distortion, substantial corneal scarring and thinning. Often there is poor vision with rigid gas permeable contact lenses, substantially reduced contact lens tolerance and usually very difficult to fit an acceptable rigid gas permeable contact lens. Referral to an experienced corneal surgeon is recommended for consideration of a corneal transplant.
Keratoconus causes
The cause of keratoconus is largely unknown. Some studies have found that keratoconus runs in families, and that it happens more often in people who have certain medical conditions. But in most cases, there is no eye injury or disease that explains why the eye starts to change. Patients with keratoconus tend to rub their eyes a lot, which may cause the condition to develop more rapidly.
Some cases of keratoconus have a hereditary component and studies indicate that about 20% of keratoconus patients have affected relatives. If there is no evidence of keratoconus in successive generations of a family, there is less than a 1 in 10 chance of the children of a person with keratoconus also having the condition.
Things that may increase your chance of developing keratoconus also include having allergic conditions, such as asthma and eczema or having other genetic diseases such as retinitis pigmentosa, Trisomy 21 (Down’s Syndrome), Marfan’s Syndrome and Ehlers-Danlos Syndrome.
Keratoconus is often associated with atopic diseases (hayfever, eczema, allergies, asthma etc) which can result in people having itchy eyes. Excessive and vigorous eye rubbing can break down the fibres of the cornea and has therefore been implicated as a causative factor or a trigger to progressive keratoconus in persons having a genetic disposition to the disease.
Some studies point to keratoconic corneas lacking structural fibrils that maintain the stability of the cornea, leading to a thinning and weakening of the cornea.
Oxidative stress may also be linked to the development of keratoconus. Under this theory, keratoconic corneas are unable to eliminate free radicals and self repair resulting structural damage like a normal cornea. This weakens the bonds in the cornea.
Other conditions that can also cause thinning of the cornea
These conditions are rare:
- Keratoglobus – Keratoglobus causes thinning over the entire cornea resulting in an enlarged, globular shaped cornea.
- Pellucid marginal degeneration – Pellucid marginal degeneration causes thinning of a peripheral narrow (1-2 mm) band of the inferior cornea.
- Posterior keratoconus – Posterior keratoconus causes a non-progressive thinning of the inner surface of the cornea, while the curvature of the front surface of the cornea remains normal. Posterior keratoconus is a separate condition to keratoconus.
Keratoconus symptoms
The main symptoms of keratoconus are the following:
- The vision in one or both eyes gradually gets worse, usually in late adolescence.
- The person has double vision when looking with just one eye, even with glasses on.
- Bright lights look like they have halos around them.
- Increased sensitivity to bright light and glare, which can cause problems with night driving.
- A need for frequent changes in eyeglass prescriptions.
- Sudden worsening or clouding of vision.
Someone with keratoconus will notice that his or her vision slowly becomes distorted. The change can end at any time, or it can continue for several years. In most people who have keratoconus, both eyes are eventually affected.
Keratoconus complications
In some situations, your cornea may swell quickly and cause sudden reduced vision and scarring of the cornea. This is caused by a condition in which the inside lining of your cornea breaks down, allowing fluid to enter the cornea (hydrops).
In advanced keratoconus, your cornea may become scarred, particularly where the cone forms. A scarred cornea causes worsening vision problems and may require corneal transplant surgery.
What is hydrops?
Hydrops is an uncommon complication from advanced keratoconus. A tear in Descemet’s membrane (next to the endothelium) allows a sudden inflow of aqueous fluid from the inside of the eye into the stroma. This results in the dry stromal layers absorbing lots of fluid causing a sudden onset of blurred and very foggy vision and a visible white spot visible on the cornea. This is like a dry sponge that expands rapidly when dropped into water. Contact lenses should not be worn during active corneal hydrops due to the increase risk of corneal ulceration and corneal perforation. The stromal fluid is usually cleared over six to eight weeks without any specific treatment and so the corneal haze reduces. Unfortunately once the cornea has healed; it may result in corneal scarring and permanently reduced vision. Some patients who have corneal hydrops need to have a corneal graft to restore their vision.
Keratoconus diagnosis
To diagnose keratoconus, your eye doctor (ophthalmologist) will review your medical and family history and conduct an eye exam. He or she may conduct other tests to determine more details regarding the shape of your cornea.
Tests to diagnose keratoconus include:
- Eye refraction. In this test your eye doctor uses special equipment that measures your eyes to check for vision problems. He or she may ask you to look through a device that contains wheels of different lenses (phoropter) to help judge which combination gives you the sharpest vision. Some doctors may use a hand-held instrument (retinoscope) to evaluate your eyes.
- Slit-lamp examination. In this test your doctor directs a vertical beam of light on the surface of your eye and uses a low-powered microscope to view your eye. He or she evaluates the shape of your cornea and looks for other potential problems in your eye. The doctor may repeat the test after you’ve had eyedrops applied to dilate your pupils. This helps with viewing the back of your eye.
- Keratometry. In this test your eye doctor focuses a circle of light on your cornea and measures the reflection to determine the basic shape of your cornea.
- Computerized corneal mapping. Special photographic tests, such as optical coherence tomography and corneal topography, record images of your cornea to create a detailed shape map of your cornea’s surface. The tests can also measure the thickness of your cornea.
Keratoconus treatment
There are several methods for treating keratoconus, depending on how severe the condition is and how quickly the condition is progressing. In the early stages of the disease, vision can be corrected with normal eyeglasses or soft contact lenses. For most people, the cornea will become stable after a few years. If you have this type, you likely won’t experience severe vision problems or require further treatment.
As keratoconus gets worse, vision may no longer be correctable with eyeglasses because of the amount of irregular astigmatism, and so the patient may need to be fit with a special type of hard contact lens.
For some patients, the disease may advance to a stage at which they do not have acceptable vision even with glasses or contact lenses. At this point, the doctor may recommend a cornea transplant, which is a surgical procedure to replace the cornea with a cornea from a donor.
Keratoconus contact lenses
- Eyeglasses or soft contact lenses. Glasses or soft contact lenses can correct blurry or distorted vision in early keratoconus. But people frequently need to change their prescription for eyeglasses or contacts as the shape of their corneas change.
- Hard contact lenses. Hard (rigid gas permeable) contact lenses are often the next step in treating progressing keratoconus. Hard lenses may feel uncomfortable at first, but many people adjust to wearing them and they can provide excellent vision. This type of lens can be made to fit your corneas.
- Piggyback lenses. If rigid lenses are uncomfortable, your doctor may recommend “piggybacking” a hard contact lens on top of a soft one.
- Hybrid lenses. These contact lenses have a rigid center with a softer ring around the outside for increased comfort. People who can’t tolerate hard contact lenses may prefer hybrid lenses.
- Scleral lenses. These lenses are useful for very irregular shape changes in your cornea in advanced keratoconus. Instead of resting on the cornea like traditional contact lenses do, scleral lenses sit on the white part of the eye (sclera) and vault over the cornea without touching it.
If you’re using rigid or scleral contact lenses, make sure to have them fitted by an eye doctor with experience in treating keratoconus. You’ll also need to have regular checkups to determine whether the fitting remains satisfactory. An ill-fitting lens can damage your cornea.
Can wearing rigid gas permeable contact lenses “cure” my keratoconus by flattening out my irregular cornea?
No. Rigid gas permeable contact lenses improve vision by covering the irregular cornea with the regular focussing surface of the contact lens. The lens fitting is carefully designed to lightly rest on the corneal surface to allow all day wearing times and maximum comfort. Fitting a substantially flatter than recommended contact lens curve can significantly flatten the corneal shape, especially in a thin keratoconic cornea, however the corneal irregularity that causes poor quality vision is still present. Also the effect is only temporary and after removing the lens, the cornea gradually returns to its previous irregular shape.
Can wearing rigid gas permeable lenses make my keratoconus worse?
No and Yes.
No – The “perfect fitting” contact lens will have even pressure across the central area of the cornea with enough lift at the edge to allow the lens to move freely and also permit adequate tear flow under the lens. As a keratoconic cornea has an irregular shape, “a perfect fitting” is often impossible to achieve. The final contact lens shape often has to become a compromise of trying to minimise any areas of hard pressure. The more advanced the keratoconus the more difficult this to achieve. A well-fitted lens, even with very advanced keratoconus will not cause an increase in the rate of keratoconic changes in the cornea. Occasionally a lens has to be fitted flatter than recommended to preserve adequate vision and these eyes need to be monitored regularly to ensure the contact lens fitting does not increase corneal scarring.
Yes – Flat fitting lenses with excessive pressure on the elevated and thin cornea have been associated with increased rates of corneal scarring. This situation can arise from a practitioner prescribing an inappropriate contact lens shape. It also can occur when there has been a significant increase in the corneal curvature over time and the patient continues to wear a contact lens design that was fitted when the cornea was flatter. The result is often a lens that is highly unstable and can pop out, even a few times per day. This type of lens also has intense central pressure on the thin cornea. If this lens is worn for months or years, scarring in the cornea can often be seen in the area of hard pressure. Reduced vision from excessive corneal scarring is one of the major causes why patients finally agree to have a corneal transplant. Sometimes it can be difficult to determine with certainty if the contact lens fitting has caused the scarring or the scarring would have occurred anyway with the natural progression of the keratoconus. Certainly all experienced practitioners will try and minimize the central pressure of the contact lens on the cornea, to preserve vision and avoid any increase in corneal scarring. It also emphasizes the need for regular reviews, usually every 6 – 12 months, to make sure that the contact lens fitting is still as good as possible.
Should I see a specialist contact lens fitter for keratoconus?
Absolutely yes. Poorly fitted contact lenses often lead to three undesirable outcomes.
- Uncomfortable contact lenses can convince patients that rigid gas permeable contact lenses are always uncomfortable and they may resist future attempts to accept them as a solution for better vision.
- Patients unable to tolerate an uncomfortable rigid gas permeable contact lens may stop wearing lenses and attempt to function with poor vision. This can seriously impact on their ability to study, work and engage in sporting activities. It can create unnecessary hardship and even endanger themselves and those around them, e.g. driving without lenses when they have an endorsed license, operating dangerous equipment or increased risk of falls and household accidents etc. Inability to function normally, often leads to loss of self-confidence and depression.
- Frustration with the unreliability of rigid gas permeable contact lenses, patients may seek unnecessary surgical solutions (INTACS, corneal transplant).
Keratoconus surgery
You may need surgery if you have corneal scarring, extreme thinning of your cornea, poor vision with the strongest prescription lenses or an inability to wear any type of contact lenses. Several surgeries are available, depending on the location of the bulging cone and the severity of your condition.
Two treatments for keratoconus that have recently been approved by the Food and Drug Administration are implantable ring segments (often referred to as INTACS) and corneal cross linking:
- Implantable ring segments (Intrastromal Corneal Ring Segments [INTACS]) are small curved devices that are inserted into the cornea to improve vision or make it easier to fit a patient with contact lenses. In this procedure, which is performed under local anesthesia (the patient’s eye is numbed), the doctor creates pockets in the cornea and inserts the rings into these pockets. The rings help to flatten the cornea and partially reverse the cone shape caused by the keratoconus.
- Corneal cross linking uses a special type of ultraviolet light treatment that may slow or stop the keratoconus from getting worse in patients who are in the earlier stages of the disease. In this procedure, the patient also receives local anesthesia (the eye is numbed). Drops of riboflavin (vitamin B2) are put into the eye for up to 30 minutes. The eye is then exposed to an ultraviolet light for up to 30 minutes. The corneal crosslinking procedure is designed to increase the amount of collagen “crosslinks” in the cornea, which can help keep the cornea from steepening.
Not all patients with keratoconus are candidates for these treatments. Your doctor can help to decide which, if any, of these treatments may help you.
Keratoconus cross linking
Corneal collagen crosslinking is a relatively new procedure that aims to strengthen the cornea in order to slow or halt progression in keratoconus. It achieves this through a chemical reaction using a combination of riboflavin (vitamin B2) and ultraviolet (UVA) light to strengthen the crosslinks between the collagen fibres within the stroma layer of the cornea.
It is currently the only procedure available that can slow or halt progressive keratoconus. Crosslinking may result in a slight flattening of the cornea, leading to small improvements in vision in certain cases. However patients should not expect a reversal in existing vision loss from crosslinking nor should it be considered a cure for keratoconus.
Most patients in America with keratoconus are being treated today with crosslinking after being monitored for progression for a period of 3 to 6 months.
Crosslinking should be done to only one eye at a time unless there are exceptional circumstances. Usually the worst eye (the one progressing fastest) is done first.
Crosslinking cannot be performed on patients:
- if their cornea is too thin (generally less than 350-400 microns)
- with an active ocular disease other than keratoconus
- with herpes simplex keratitis, a corneal infection caused by the herpes simplex virus (cold sore)
- who are pregnant
- with active, uncontrolled eye allergies
- with corneal scarring that significantly affects their vision
A variety of protocols are being used to perform crosslinking.
The most widely adopted and extensively studied remains the Dresden protocol. Under the protocol, the epithelium (outer) layer of the cornea is removed. The eye is then soaked in riboflavin drops for about 30 minutes. Riboflavin acts a photosensitiser to create the reaction with the ultraviolet light and absorbs it to protect the endothelium layer of the cornea and the back of the eye from UV damage during the procedure. The cornea is then irradiated with ultraviolet A light for about 30 minutes. Riboflavin drops are inserted regularly during that stage.
Other protocols being adopted today include the epithelium-on method which leaves the epithelium intact to lower the risk of infection and reduce the post-operative pain and healing period for the patient. Accelerated crosslinking involves the use of a stronger UVA source to deliver the same crosslinking effect in a shorter period of time.
Crosslinking under the Dresden protocol appears to be safe and has a success rate of around 70-90% in stabilizing keratoconus, depending on the patient. Younger patients generally have more aggressive keratoconus and may progress again after a period of stabilization. There is less evidence on the safety and efficacy of the other protocols at this time.
Crosslinking is also being done in combination with other procedures including laser refractive surgery and intracorneal rings.
Crosslinking and children
Corneal collagen crosslinking is used less frequently in children and has been studied less than in adults. That being said some studies have performed corneal collagen crosslinking in children as young as 9 years old and have not found safety of the procedure to be any different from adults. However, how long CXL will last in children and side effects of the procedure are more uncertain than in adults. Although several studies have shown corneal collagen crosslinking to stop progression in a similar way to adults, some have found it is less effective with 1 in 4 children progressing despite corneal collagen crosslinking.
Complications of corneal collagen crosslinking
Complications include hazing of vision which generally resolves within 12 months, corneal swelling (sometimes permanent), infections and sterile infiltrates or white spots on the cornea.
Haze in the cornea is by the most common of these complications and 9 in every 100 patients still are experiencing haze that affects their vision after 12 months, according to some studies.
In about 3 out of every 100 patients having crosslinking, these complications will cause a worsening in vision. In the rare cases in which scarring occurs, vision can be restored only by replacing the entire cornea via corneal transplantation. This is a major operation with more risks, long recovery and the chance of rejection at any time.
Cornea transplant
Many patients with keratoconus will never need a cornea transplant. Newer treatments like corneal cross-linking may be effective in slowing or stopping keratoconus in patients who are in less advanced stages.
In cases in which vision can no longer be corrected with glasses or contact lenses, surgery may be recommended.
If you have corneal scarring or extreme thinning, you’ll likely need a cornea transplant (keratoplasty).
- Lamellar keratoplasty is a partial-thickness transplant, in which only a section of the cornea’s surface is replaced.
- Penetrating keratoplasty is a full-cornea transplant. In this procedure, doctors remove a full-thickness portion of your central cornea and replace it with donor tissue.
- A deep anterior lamellar keratoplasty (DALK) preserves the inside lining of the cornea (endothelium). It helps avoid rejection of this critical inside lining that can occur with a full-thickness transplant.
Recovery after keratoplasty can take up to one year, and you may need to continue wearing rigid contact lenses to have clear vision. Full improvement of vision may occur several years after your transplant.
Cornea transplant for keratoconus generally is very successful, but possible complications include graft rejection, poor vision, astigmatism, inability to wear contact lenses and infection.





{kind=link}