Contents
- Kidney
- Kidney problems
- Symptoms of kidney disease
- Risk factors for kidney disease
- Diagnosis of kidney disease
- Prevention of kidney disease
- Treatment for kidney disease
- Types of kidney diseases
- Acute kidney injury
- Chronic kidney disease
- Kidney Cancer
- Kidney Stones
- Kidney Infections
- Kidney Cysts
- Kidney transplant
- What is a “preemptive” or “early” transplant ?
- Who can get a kidney transplant ?
- What if you’re older or have other health problems ?
- How will you pay for a transplant ?
- Getting a Transplant
- How does the evaluation process work ?
- What does the kidney transplant operation involve ?
- What are anti-rejection medicines ?
- After Your Kidney Transplant
- What if your body tries to reject the new kidney ?
- How often do rejection episodes happen ?
- When can you return to work ?
- Will your sex life be affected ?
- Will you need to follow a special diet ?
- Finding a Kidney
Kidney
The paired kidneys are reddish, kidney bean–shaped organs located just above the waist between the peritoneum and the posterior wall of the abdomen. Because their position is posterior to the peritoneum of the abdominal cavity, the organs are said to be retroperitoneal (Figure 1). The kidneys are located between the levels of the last thoracic vertebrae T12 and third lumbar (L3) vertebrae, a position where they are partially protected by ribs 11 and 12. If these lower ribs are fractured, they can puncture the kidneys and cause significant, even life-threatening damage. The right kidney is slightly lower than the left (see Figure 1) because the liver occupies considerable space on the right side superior to the kidney.
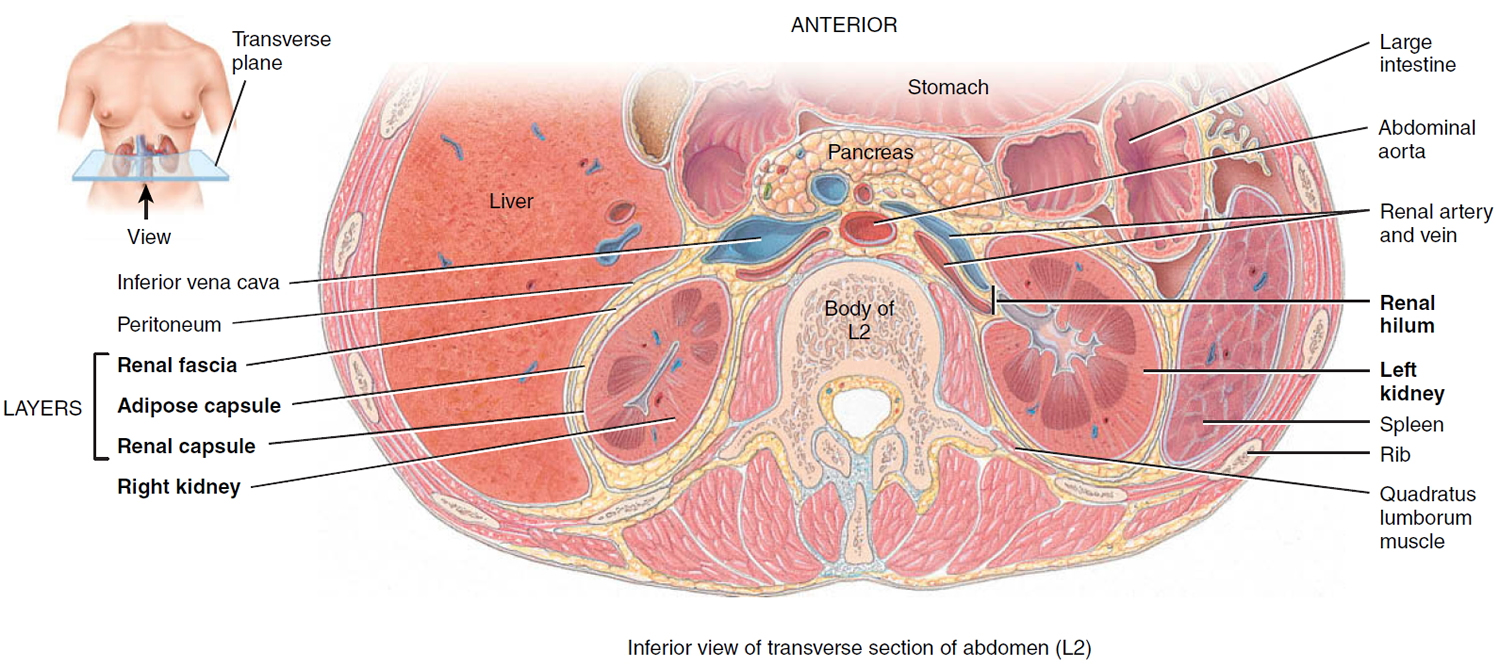
A typical adult kidney is 10–12 cm (4–5 in.) long, 5–7 cm (2–3 in.) wide, and 3 cm (1 in.) thick—about the size of a bar of bath soap—and weighs about 135–150 g (4.5–5 oz). The concave medial border of each kidney faces the vertebral column (see Figure 2). Near the center of the concave border is an indentation called the renal hilum, through which the ureter emerges from the kidney along with blood vessels, lymphatic vessels, and nerves.
Three layers of tissue surround each kidney. The deep layer, the renal capsule, is a smooth, transparent sheet of dense irregular connective tissue that is continuous with the outer coat of the ureter. It serves as a barrier against trauma and helps maintain the shape of the kidney. The middle layer, the adipose capsule, is a mass of fatty tissue surrounding the renal capsule. It also protects the kidney from trauma and holds it firmly in place within the abdominal cavity. The superficial layer, the renal fascia, is another thin layer of dense irregular connective tissue that anchors the kidney to the surrounding structures and to the abdominal wall. On the anterior surface of the kidneys, the renal fascia is deep to the peritoneum.
Figure 1. Kidney location
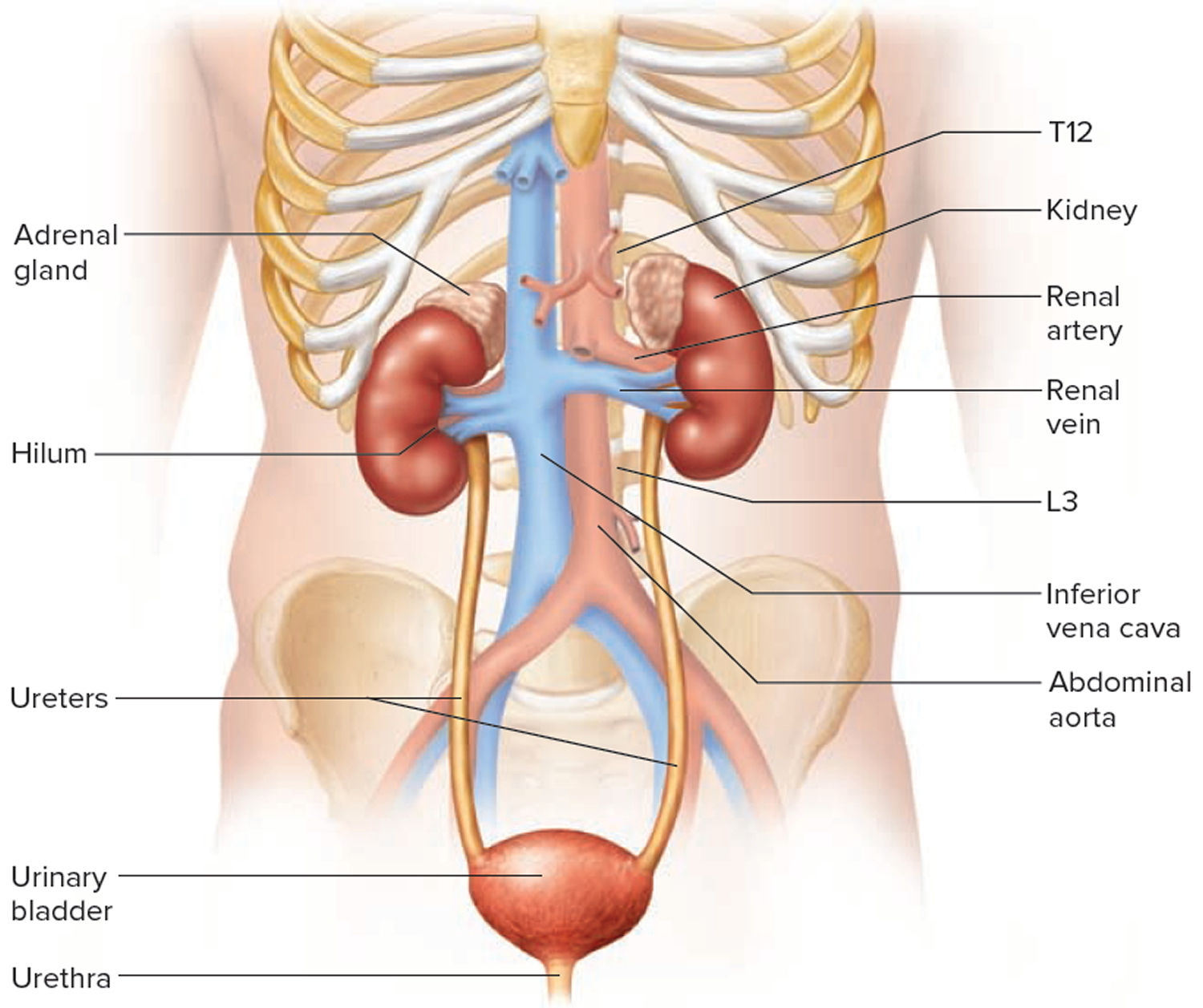
Figure 2. Kidney location (transverse section)
Kidney Anatomy
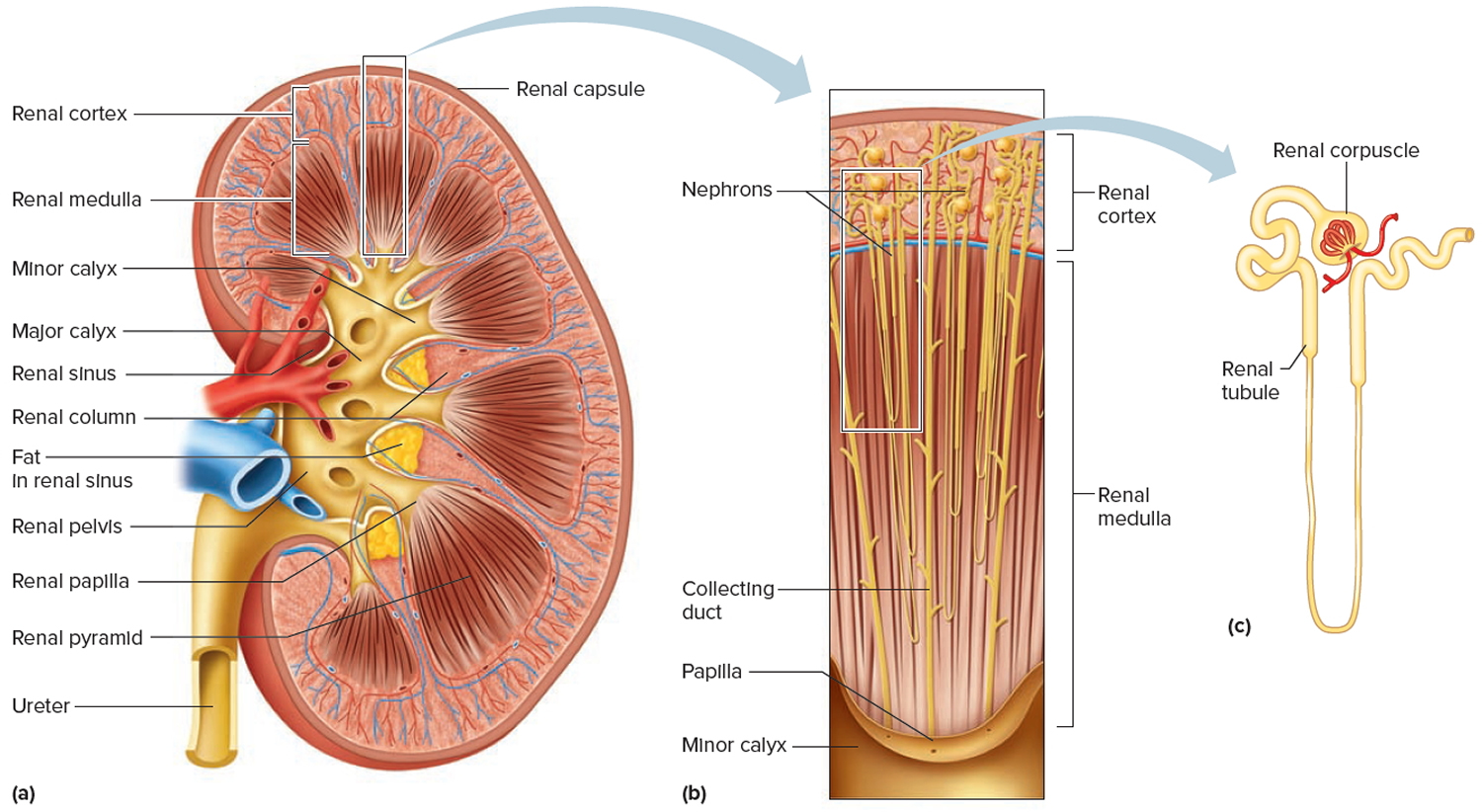
A frontal section through the kidney reveals two distinct regions: a superficial, light red region called the renal cortex and a deep, darker reddish-brown inner region called the renal medulla (medulla = inner portion) (Figure 3). The renal medulla consists of several cone-shaped renal pyramids. The base (wider end) of each pyramid faces the renal cortex, and its apex (narrower end), called a renal papilla, points toward the renal hilum. The renal cortex is the smooth-textured area extending from the renal capsule to the bases of the renal pyramids and into the spaces between them. It is divided into an outer cortical zone and an inner juxtamedullary zone. Those portions of the renal cortex that extend between renal pyramids are called renal columns.
Together, the renal cortex and renal pyramids of the renal medulla constitute the parenchyma or functional portion of the kidney. Within the parenchyma are the functional units of the kidney—about 1 million microscopic structures called nephrons. Filtrate (filtered fluid) formed by the nephrons drains into large papillary ducts, which extend through the renal papillae of the pyramids. The papillary ducts drain into cuplike structures called minor and major calyces. Each kidney has 8 to 18 minor calyces and 2 or 3 major calyces. A minor calyx receives filtrate from the papillary ducts of one renal papilla and delivers it to a major calyx. Once the filtrate enters the calyces it becomes urine because no further reabsorption can occur. The reason for this is that the simple epithelium of the nephron and ducts becomes transitional epithelium in the calyces. From the major calyces, urine drains into a single large cavity called the renal pelvis and then out through the ureter to the urinary bladder.
The hilum expands into a cavity within the kidney called the renal sinus, which contains part of the renal pelvis, the calyces, and branches of the renal blood vessels and nerves. Adipose tissue helps stabilize the position of these structures in the renal sinus.
Figure 3. Kidney anatomy
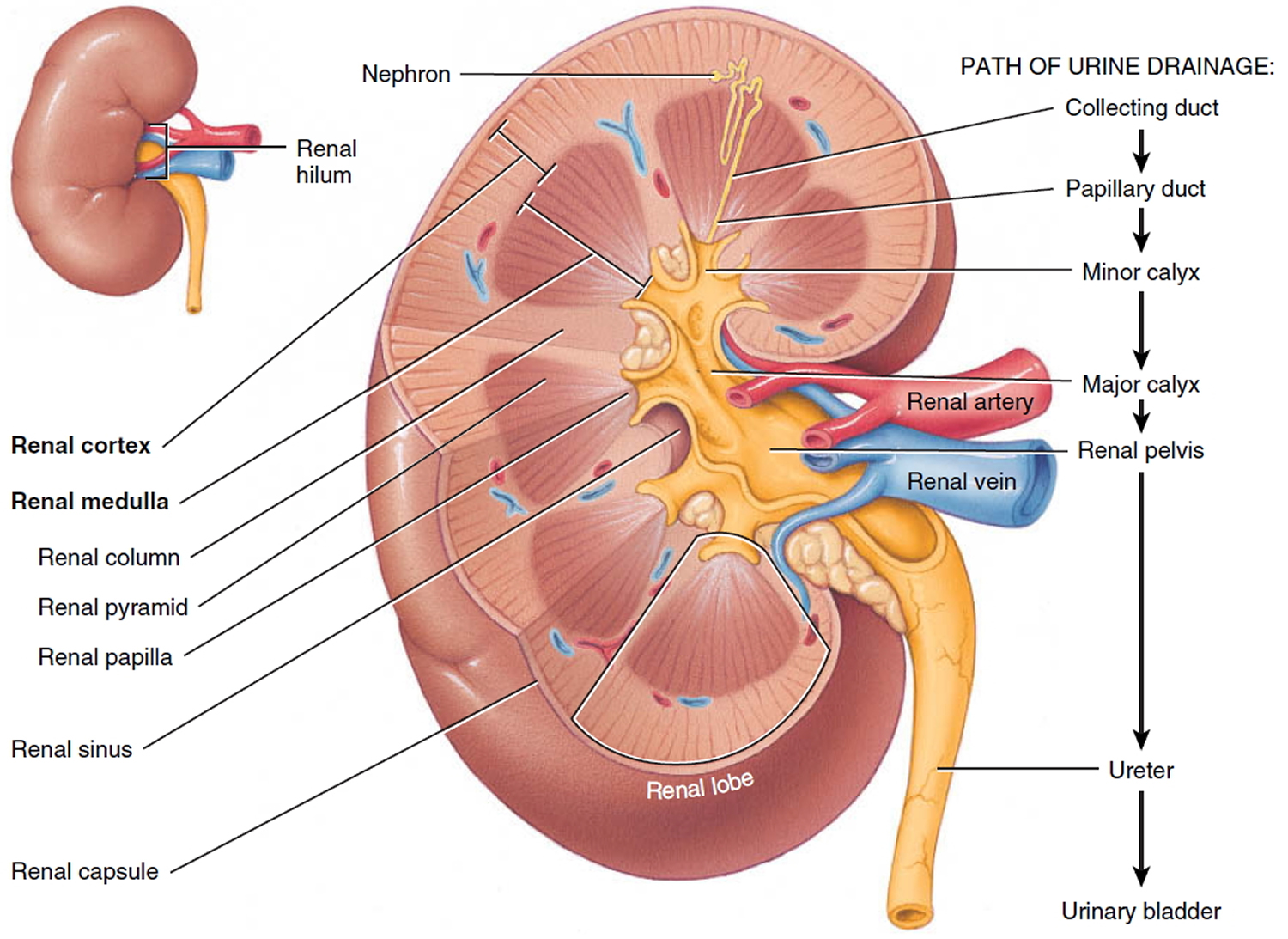
Figure 4. Kidney structure
Blood and Nerve Supply of the Kidneys
Because the kidneys remove wastes from the blood and regulate its volume and ionic composition, it is not surprising that they are abundantly supplied with blood vessels. Although the kidneys constitute less than 0.5% of total body mass, they receive 20–25% of the resting amount of blood pumped by the heart per minute via the right and left renal arteries (Figure 4 and 5). In adults, renal blood flow, the blood flow through both kidneys, is about 1200 mL per minute.
Within the kidney, the renal artery divides into several segmental arteries, which supply different segments (areas) of the kidney. Each segmental artery gives off several branches that enter the parenchyma and pass through the renal columns between the renal lobes as the interlobar arteries. A renal lobe consists of a renal pyramid, some of the renal column on either side of the renal pyramid, and the renal cortex at the base of the renal pyramid. At the bases of the renal pyramids, the interlobar arteries arch between the renal medulla and cortex; here they are known as the arcuate arteries.
Divisions of the arcuate arteries produce a series of cortical radiate (interlobular) arteries. These arteries radiate outward and enter the renal cortex. Here, they give off branches called afferent arterioles. Each nephron receives one afferent arteriole, which divides into a tangled, ball-shaped capillary network called the glomerulus. The glomerular capillaries then reunite to form an efferent arteriole that carries blood out of the glomerulus. Glomerular capillaries are unique among capillaries in the body because they are positioned between two arterioles, rather than between an arteriole and a venule. Because they are capillary networks and they also play an important role in urine formation, the glomeruli are considered part of both the cardiovascular and the urinary systems.
The efferent arterioles divide to form the peritubular capillaries, which surround tubular parts of the nephron in the renal cortex. Extending from some efferent arterioles are long, loop-shaped capillaries called vasa recta that supply tubular portions of the nephron in the renal medulla. The peritubular capillaries eventually reunite to form cortical radiate (interlobular) veins, which also receive blood from the vasa recta. Then the blood drains through the arcuate veins to the interlobar veins running between the renal pyramids. Blood leaves the kidney through a single renal vein that exits at the renal hilum and carries venous blood to the inferior vena cava.
Many renal nerves originate in the renal ganglion and pass through the renal plexus into the kidneys along with the renal arteries. Renal nerves are part of the sympathetic division of the autonomic nervous system. Most are vasomotor nerves that regulate the flow of blood through the kidney by causing vasodilation or vasoconstriction of renal arterioles.
Ultrafiltration of plasma is the main function of the glomeruli
Filtration is based on size and charge.
- Small solutes cross readily.
- Larger substances are generally restricted.
- Negatively charged molecules are restricted.
Volume of ultrafiltrate = 135–180 liters(L)/day
- 99% water reabsorbed 1–1.5 L urine excreted
- Glomerular filtration rate (GFR) provides an estimate of how much blood is filtered by the kidneys each minute. In normal kidneys are GFR > 60 ml/minute
- The formula used to estimate GFR uses serum creatinine, age, gender, and race.
- eGFR (mL/min/1.73 m2) = 175 x (serum creatinine)–1.154 x (Age)–0.203 x (0.742 if female) x (1.212 if African American)
- Kidney failure is an eGFR < 15 ml/minute.
- eGFR is not reliable for patients with rapidly changing creatinine levels, extremes in muscle mass and body size, or altered diet patterns.
- For a free Glomerular Filtration Rate (GFR) Calculators please go here: https://www.niddk.nih.gov/health-information/communication-programs/nkdep/laboratory-evaluation/glomerular-filtration-rate-calculators
Table 1. Reference Table for Population Mean eGFR from NHANES III
Age (years) | Mean eGFR (mL/min/1.73 m2) |
20–29 | 116 |
30–39 | 107 |
40–49 | 99 |
50–59 | 93 |
60–69 | 85 |
70 | 75 |
Figure 5. Microcirculation of the kidney
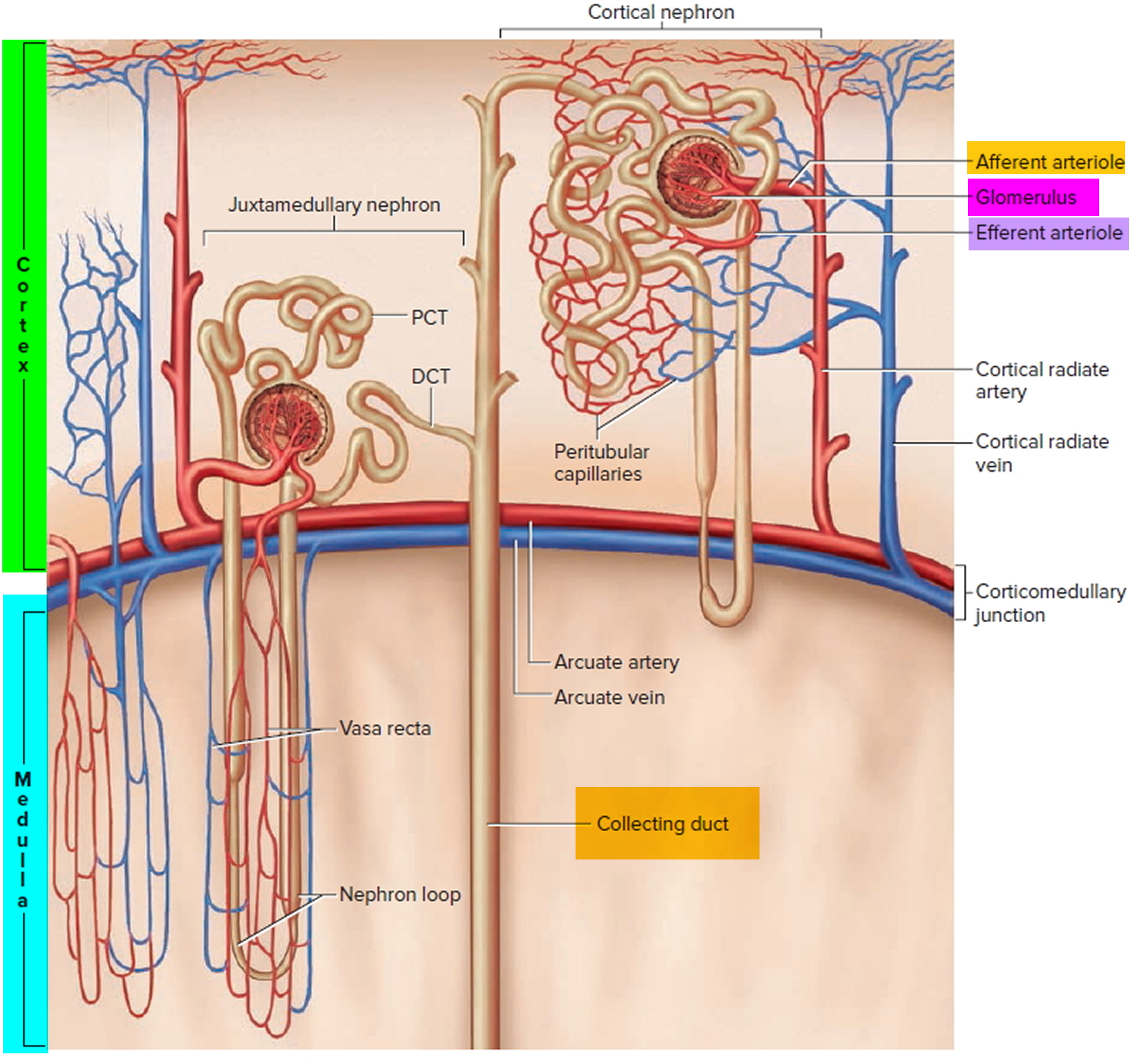
Note: DCT = distal convoluted tubule; PCT = proximal convoluted tubule
Kidney function
The primary function of the kidneys is to help maintain homeostasis by regulating the composition (including pH) and the volume of the extracellular fluid. The kidneys accomplish this by removing metabolic wastes from the blood and combining the wastes with excess water and electrolytes to form urine, which they then excrete.
Kidneys maintain homeostasis
- Regulatory function
+ Control composition and volume of blood
+ Maintain stable concentrations of inorganic anions such as sodium (Na), potassium (K), and calcium (Ca)
+ Maintain acid-base balance - Excretory function
+ Produce urine
+ Remove metabolic wastes
+ Including nitrogenous waste
Kidneys blood filtration and urine production
- Filtration: Glomeruli generate ultrafiltrate of the plasma.
- Reabsorption: Tubules selectively reabsorb substances from the ultrafiltrate.
- Secretion: Tubules secrete substances into the urine.
Examples:
- Potassium is reabsorbed from and secreted into the urine by the tubules.
- Sodium is generally reabsorbed by the tubules.
- Organic acids are secreted into the urine.
- Albumin is generally reabsorbed within the tubules.
Damaged kidneys allow albumin to cross the filtration barrier into the urine
- Increased glomerular permeability allows albumin (and other proteins) to cross the glomerulus into the urine.
- Higher levels of protein within the tubule may exacerbate kidney damage by exceeding tubules’ ability to reabsorb the proteins.
- An elevated urine albumin-to-creatinine ratio (UACR) is used to identify damaged kidneys. Urine albumin (UACR) results are used for screening, diagnosing, and treating chronic kidney disease. Forty percent of people are identified with chronic kidney disease on the basis of urine albumin alone.
The kidneys have several other important functions:
- Produce Erythropoietin which stimulates marrow production of red blood cells.
- Playing a role in the activation of vitamin D [activate 25(OH)D to 1,25 (OH)2D (active vitamin D)].
- Helping to maintain blood volume and blood pressure by secreting the enzyme Renin.
- Metabolize drugs and endogenous substances (e.g., insulin).
In patients with kidney failure:
- Kidneys cannot maintain homeostasis.
- Kidney failure is associated with fluid, electrolyte, and hormonal imbalances and metabolic abnormalities.
- End stage kidney failure means the patient is on dialysis or has a kidney transplant.
Kidney problems
For about one-third of older people, kidney (also called renal) function remains steady throughout life. But for the rest of us, kidney function gradually starts to decline around age 35, sometimes worsening quickly in later years with increasing structural and hormonal changes. Your kidneys are normally more than capable of meeting the body’s demands, so there is a built-in reserve of kidney function, even as you age. Older kidneys, however, may not be as resilient as younger ones if they have been stressed. The result may be a higher risk of fluid imbalances, build-up of waste products, and other serious consequences in later years. Doses of medications must also be reduced if kidney function has declined, since your body can accumulate “overdose” levels if your kidneys cannot get rid of drugs efficiently.
Because the kidneys are important in regulating a variety of bodily functions, you may eventually develop problems requiring medical attention if your kidneys are not working well. These problems from kidney disease may include:
- Fluid and electrolyte imbalance – for example, having too much or too little sodium, potassium, or water in your body
- Build-up of waste products in your body—for example, urea or acids
- Loss of protein through your kidneys
- High blood pressure from too much fluid in your body
- Anemia, or low blood counts
- Brittle bones
If these problems become severe enough or don’t recover, you may end up needing dialysis – a procedure that uses a machine to wash out your blood to make up for the loss of kidney function.
Other kidney problems include:
- Kidney Cancer
- Kidney Cysts
- Kidney Stones
- Kidney Infections
Your doctor can do blood and urine tests to check if you have kidney disease. If your kidneys fail, you will need dialysis or a kidney transplant.
Symptoms of kidney disease
Kidney disease is called a ‘silent disease’ as there are often few or no symptoms. In fact, you can lose up to 90 per cent of your kidneys’ functionality before seeing any symptoms 2. Some signs and symptoms include:
- a change in the frequency and quantity of urine passed, especially at night (usually an increase at first)
- blood in the urine (hematuria)
- foaming urine
- puffiness around the eyes and ankles (edema)
- pain in the back (under the lower ribs, where the kidneys are located)
- pain or burning when passing urine.
If your kidneys begin to fail, there is a build-up of waste products and extra fluid in the blood, as well as other problems, gradually leading to:
- tiredness and inability to concentrate
- generally feeling unwell
- loss of appetite
- nausea and vomiting
- shortness of breath.
Risk factors for kidney disease
You are more ‘at risk’ of developing chronic kidney disease if you:
- have high blood pressure
- have diabetes
- have established heart problems (heart failure or past heart attack) or have had a stroke
- are obese
- are over 60 years of age
- have a family history of kidney failure
- smoke
- have a history of acute kidney injury.
High blood pressure and kidney disease
High blood pressure (hypertension) is increased pressure inside the arteries that carry blood from your heart to all parts of your body. Untreated, high blood pressure can damage your kidneys.
Also, high blood pressure can develop as a result of kidney disease or renal artery stenosis (narrowing of the main artery to one or both kidneys). Your kidneys control the amount of fluid in your blood vessels and produce a hormone called renin that helps to control blood pressure.
Diabetes and kidney disease
About 20 to 30 per cent of people with diabetes develop a type of kidney disease called diabetic nephropathy. This is a serious disease and may worsen other diabetic complications such as nerve and eye damage, as well as increasing the risk of cardiovascular (heart) disease. Diabetic nephropathy is the main cause of kidney failure (also known as ‘end-stage kidney disease’ or ESKD).
Kidney disease and cardiovascular risks
Cardiovascular disease is the most common cause of death in people with chronic (ongoing) kidney disease. Compared to the general population, people with chronic kidney disease are two to three times more likely to have cardiovascular (heart and blood vessel) problems such as:
- angina (heart pain)
- heart attack
- stroke
- heart failure.
This increased risk is partly caused by factors common to both chronic kidney disease and cardiovascular disease, such as high blood pressure. However, researchers are discovering that chronic kidney disease is, in itself, an important risk factor for the development of cardiovascular disease, and a history of cardiovascular disease is a risk factor for the development of chronic kidney disease.
The kidneys regulate water and salts, remove certain wastes and make various hormones. Kidney disease increases the risk of cardiovascular disease in many ways, including:
- high blood pressure – the kidneys help to regulate blood pressure by producing a hormone called renin. They also help to regulate the amount of salt and fluid in the body
- heart strain – holding excess fluid in the body puts strain on the heart and increases the risk of complications such as left ventricular hypertrophy (enlarged left heart chamber), which can cause heart failure
- stiff arteries – kidneys make a hormone that helps to regulate the use of calcium throughout the body. A person with chronic kidney disease may develop calcified (stiffened) arteries and heart valves, perhaps caused by hormones not being produced efficiently
- increased blood fats (hyperlipidemia) – some people with chronic kidney disease have increased levels of low-density lipoprotein (LDL) “bad” cholesterol, which may be caused by disturbed hormone levels. High levels of LDL “bad” cholesterol is a known risk factor in the development of cardiovascular disease
- blood clots – the blood of people with some types of chronic kidney disease, and those with kidney failure, is prone to clotting. A clot (thrombus) lodged within a blood vessel may cut off the blood supply. This increases the risk of many complications, including heart attack and stroke. A clot in one of the kidney arteries may cause high blood pressure.
Diagnosis of kidney disease
Early diagnosis and optimal management can often prevent kidney damage from becoming worse and reduce the risk of kidney failure.
Chronic kidney disease often has very few symptoms, or only general symptoms, such as tiredness, headaches and feeling sick. The doctor may begin by reviewing your medical history and performing a physical examination.
The diagnostic tests for kidney disease chosen by your doctor depend on factors including your symptoms, age, medical history, lifestyle and general health. Tests for kidney disease include:
- urine tests
- blood tests
- imaging
- kidney biopsy.
Urine tests for kidney disease
Damaged or inflamed kidneys ‘leak’ substances such as blood or protein into the urine. The preferred test for detecting protein in the urine is a urine albumin-to-creatinine ratio (urine ACR) test, which shows the amount of albumin (a type of protein) in the urine.
A urine albumin-to-creatinine ratio (urine ACR) test should be done at least once a year if the person has diabetes or high blood pressure, and every two years if the person has any of the other identified risk factors for developing chronic kidney disease.
A urine albumin-to-creatinine ratio (urine ACR) test is performed by sending a sample of your urine to a laboratory for analysis.
Blood tests for kidney disease
The best measure of kidney function is the glomerular filtration rate (GFR), which can be estimated from a blood test that checks the blood for creatinine (a waste product made by muscle tissue). A normal result is higher than 90 mL/min/1.73 m2. If the result is persistently less than 60 mL/min/1.73 m2 for at least three months, this confirms that the person has chronic kidney disease.
Blood tests can reveal other abnormalities of kidney function, such as:
- high levels of acids (acidosis)
- anemia (insufficient red blood cells or hemoglobin, the protein in red blood cells that transports oxygen)
- high levels of potassium (hyperkalemia)
- low levels of salt (hyponatremia)
- changes to the levels of calcium and phosphate.
Imaging tests for kidney disease
Tests that create various pictures or images may include:
- x-rays – to check the size of the kidneys and look for kidney stones
- cystogram – a bladder x-ray
- voiding cystourethrogram – where the bladder is x-rayed before and after urination
- ultrasound – sound waves are ‘bounced’ off the kidneys to create a picture. Ultrasound may be used to check the size of the kidneys. Kidney stones and blood vessel blockages may be visible on ultrasound
- computed tomography (CT) – x-rays and digital computer technology are used to create an image of the urinary tract, including the kidneys
- magnetic resonance imaging (MRI) – a strong magnetic field and radio waves are used to create a three-dimensional image of the urinary tract, including the kidneys.
Biopsy for kidney disease
A biopsy means that a small piece of tissue is taken for testing in a laboratory. Biopsies used in the investigation of kidney disease may include:
- Kidney biopsy – the doctor inserts a special needle into the back, under local anaesthesia, to obtain a small sample of kidney tissue. A kidney biopsy can confirm a diagnosis of chronic kidney disease.
- Bladder biopsy – the doctor inserts a thin tube (cystoscope) into the bladder via the urethra. This allows the doctor to view the inside of the bladder and check for abnormalities. This procedure is called a cystoscopy. The doctor may take a biopsy of bladder tissue for examination in a laboratory.
Your doctor may arrange other tests, depending on the suspected cause of your kidney disorder.
Prevention of kidney disease
Medication and changes to lifestyle, along with an early referral to a kidney specialist (nephrologist), can prevent or delay kidney failure.
Healthy lifestyle choices to keep your kidneys functioning well include:
- Eat lots of fruit and vegetables including legumes (peas or beans), and grain-based food such as bread, pasta, noodles and rice.
- Eat lean meat such as chicken and fish each week.
- Eat only small amounts of salty or fatty food.
- Drink plenty of water instead of other drinks. Minimise consumption of sugary soft drinks.
- Maintain a healthy weight.
- Stay fit. Do at least 30 minutes of physical activity that increases your heart rate on five or more days of the week, including walking, lawn mowing, bike riding, swimming or gentle aerobics.
- If you don’t smoke, don’t start. If you do, quit. Ask your doctor for help with quitting.
- Limit your alcohol to no more than two small drinks per day if you are male, or one small drink per day if you are female.
- Have your blood pressure checked regularly.
- Do things that help you relax and reduce your stress levels.
A range of medication is available for high blood pressure. Different blood pressure medications work in different ways, so it is not unusual for more than one type to be prescribed. The dose may change according to your needs.
Treatment for kidney disease
If detected early enough, the progress of kidney disease can be slowed and sometimes even prevented. In the early stages, changes to diet and medication can help to increase the life of your kidneys.
If kidney function is reduced to less than 10 per cent of normal, the loss of function must be replaced by dialysis or a kidney transplant. Dialysis is a treatment for kidney failure that removes waste products and extra water from the blood by filtering it through a special membrane (fine filter).
Types of kidney diseases
Most kidney diseases attack the nephrons 3. This damage may leave kidneys unable to remove wastes. Causes can include genetic problems, injuries, or medicines. You have a higher risk of kidney disease if you have diabetes, high blood pressure, or a close family member with kidney disease.
Acute kidney injury
Acute kidney injury is sudden damage to the kidneys. In many cases it will be short term and your kidney function can continue to recover over time 4; however, long-term outcomes can vary from:
- full recovery and normal kidney function
- partial recovery with lower levels of kidney function, but no dialysis needed
- permanent kidney damage that requires dialysis.
People who have a history of acute kidney injury have a higher risk of chronic kidney disease (see below Chronic kidney disease).
Causes of acute kidney injury
The main causes are:
- reduced blood supply to the kidneys (for example as a result of major surgery or a heart attack)
- damage to the actual kidney tissue caused by a drug, severe infection or radioactive dye
- obstruction to urine leaving the kidney (for example because of kidney stones or an enlarged prostate).
People who have chronic kidney disease are also at increased risk of acute kidney injury.
Diagnosis for acute kidney injury
The kidney damage usually occurs quite quickly over a matter of days (compared to the months or years for chronic kidney disease to develop).
This leads to reduced output of urine, a sudden rise in toxins in the body, as well as a rapid build up of fluid.
Acute kidney injury may be diagnosed if you have a sharp increase in the levels of creatinine in your blood, or if your urine output is significantly decreased.
Treating acute kidney injury
The goals of treatment are to:
- find and treat the cause of the acute kidney injury
- use medications to support the kidneys
- closely monitor the urine output and creatinine levels to check for toxins and assess kidney function.
Severe acute kidney injury may require dialysis treatment for one to two weeks while the kidneys recover.
Prognosis (outcome) of acute kidney injury
After acute kidney injury, long-term outcomes can vary from:
- full recovery and normal kidney function
- partial recovery with lower levels of kidney function, but no dialysis needed
- permanent kidney damage that requires dialysis.
After an acute kidney injury your kidney function can continue to recover over time. People who have a history of acute kidney injury have a higher risk of chronic kidney disease.
It is recommended that you have a Kidney Health Check performed by your doctor every year for the first three years following an acute kidney injury.
The Kidney Health Check has three tests:
- A blood test to find out the level of waste products in your blood and calculate what’s called your estimated glomerular filtration rate (eGFR).
- A urine test to check for albumin (a type of protein) or blood in your urine.
- A blood pressure test, as kidney disease causes high blood pressure and high blood pressure causes kidney disease.
If kidney disease is suspected, your doctor may also organize a renal ultrasound scan. This test is taken to show the size of your kidneys, locate kidney stones or tumours, and find any problems in the structure of your kidneys and urinary tract.
Following your Kidney Health Check and depending on your circumstances, other tests and procedures may be required.
- If you have one or more risk factors for chronic kidney disease it is recommended that you see your doctor for a Kidney Health Check every two years.
- If you have diabetes or high blood pressure it is recommended that you have a Kidney Health Check every year.
These tests may be carried out by your doctor or you may be referred to a kidney specialist (nephrologist).
Chronic kidney disease
Chronic kidney disease refers to kidney damage that lasts for more than three months 5. Chronic kidney disease damages the nephrons slowly over many years. Many people don’t have any symptoms until their kidney disease is very advanced. Blood and urine tests are the only way to know if you have kidney disease.
Chronic kidney disease is classified into five stages based on how well your kidneys are able to filter your blood. In stage one, your kidneys retain much of their ability to filter out wastes. In stage five, however, the filtration rate is inadequate and your kidneys are considered to have failed.
Chronic kidney disease is very common in older people, with a prevalence of around 10%. Slowing or preventing its progress is an important and attainable goal.
Chronic kidney disease afflicts more than 20 million adults in this country. Diabetes and high blood pressure are the most common causes of chronic kidney disease. Chronic kidney disease affects 35% of diabetes patients, and about 20% of adults with high blood pressure.
Chronic kidney disease damage can cause wastes to build up in your body. It can also cause other problems that can harm your health.
Treatment may include medicines to lower blood pressure, control blood glucose, and lower blood cholesterol. Chronic kidney disease can get worse over time. Chronic kidney disease may lead to kidney failure. The only treatment options for kidney failure are dialysis or a kidney transplantation.
You can take steps to keep your kidneys healthier longer:
- Choose foods with less salt (sodium)
- Keep your blood pressure below 130/80
- Keep your blood glucose in the target range, if you have diabetes.
Kidney Cancer
Kidney cancer is a disease that starts in the kidneys 6. It happens when healthy cells in one or both kidneys grow out of control and form a lump (called a tumor).
Types of kidney cancer
Renal cell carcinoma
Renal cell carcinoma, also known as renal cell cancer or renal cell adenocarcinoma, is by far the most common type of kidney cancer. About 9 out of 10 kidney cancers are renal cell carcinomas 7.
Although renal cell carcinoma usually grows as a single tumor within a kidney, sometimes there are 2 or more tumors in one kidney or even tumors in both kidneys at the same time.
There are several subtypes of renal cell carcinoma, based mainly on how the cancer cells look under a microscope. Knowing the subtype of renal cell carcinoma can be a factor in deciding treatment and can also help your doctor determine if your cancer might be due to an inherited genetic syndrome.
Clear cell renal cell carcinoma: this is the most common form of renal cell carcinoma. About 7 out of 10 people with renal cell carcinoma have this kind of cancer. When seen under a microscope, the cells that make up clear cell renal cell carcinoma look very pale or clear.
Papillary renal cell carcinoma: this is the second most common subtype – about 1 in 10 renal cell carcinomas are of this type. These cancers form little finger-like projections (called papillae) in some, if not most, of the tumor. Some doctors call these cancers chromophilic because the cells take in certain dyes and look pink under the microscope.
Chromophobe renal cell carcinoma: this subtype accounts for about 5% (5 cases in 100) of renal cell carcinomas. The cells of these cancers are also pale, like the clear cells, but are much larger and have certain other features that can be recognized when looked at with a microscope .
Rare types of renal cell carcinoma: these subtypes are very rare, each making up less than 1% of renal cell carcinomas:
- Collecting duct renal cell carcinoma
- Multilocular cystic renal cell carcinoma
- Medullary carcinoma
- Mucinous tubular and spindle cell carcinoma
- Neuroblastoma-associated renal cell carcinoma
Unclassified renal cell carcinoma: rarely, renal cell cancers are labeled as unclassified because the way they look doesn’t fit into any of the other categories or because there is more than one type of cell present.
Other types of kidney cancers
Other types of kidney cancers include transitional cell carcinomas, Wilms tumors, and renal sarcomas.
Transitional cell carcinoma: of every 100 cancers in the kidney, about 5 to 10 are transitional cell carcinomas, also known as urothelial carcinomas.
Transitional cell carcinomas don’t start in the kidney itself, but in the lining of the renal pelvis (where the ureters meet the kidneys). This lining is made up of cells called transitional cells that look like the cells that line the ureters and bladder. Cancers that develop from these cells look like other urothelial carcinomas, such as bladder cancer, under the microscope. Like bladder cancer, these cancers are often linked to cigarette smoking and being exposed to certain cancer-causing chemicals in the workplace.
People with transitional cell carcinoma often have the same signs and symptoms as people with renal cell cancer − blood in the urine and, sometimes, back pain.
Wilms tumor (nephroblastoma): Wilms tumors almost always occur in children. This type of cancer is very rare among adults.
Renal sarcoma: renal sarcomas are a rare type of kidney cancer that begin in the blood vessels or connective tissue of the kidney. They make up less than 1% of all kidney cancers.
Benign (non-cancerous) kidney tumors
Some kidney tumors are benign (non-cancerous). This means they do not metastasize (spread) to other parts of the body, although they can still grow and cause problems.
Benign kidney tumors can be treated by removing or destroying them, using many of the same treatments that are also used for kidney cancers, such as surgery, radiofrequency ablation, and arterial embolization. The choice of treatment depends on many factors, such as the size of the tumor and if it is causing any symptoms, the number of tumors, whether tumors are in both kidneys, and the person’s general health.
Renal adenoma: renal adenomas are the most common benign kidney tumors. They are small, slow-growing tumors that are often found on imaging tests (such as CT scans) when the doctor is looking for something else. Seen with a microscope, they look a lot like low-grade (slow growing) renal cell carcinomas.
In rare cases, tumors first thought to be renal adenomas turn out to be small renal cell carcinomas. Because they are hard to tell apart, suspected adenomas are often treated like renal cell cancers.
Oncocytoma: oncocytomas are benign kidney tumors that can sometimes grow quite large. As with renal adenomas, it can sometimes be hard to tell them apart from kidney cancers. Oncocytomas do not normally spread to other organs, so surgery often cures them.
Angiomyolipoma: angiomyolipomas are rare. They often develop in people with tuberous sclerosis, a genetic condition that also affects the heart, eyes, brain, lungs, and skin. These tumors are made up of different types of connective tissues (blood vessels, smooth muscles, and fat). If they aren’t causing any symptoms, they can often just be watched closely. If they start causing problems (like pain or bleeding), they may need to be treated.
The American Cancer Society’s most recent estimates for kidney cancer in the United States are for 2017 8:
- About 63,990 new cases of kidney cancer (40,610 in men and 23,380 in women) will occur.
- About 14,400 people (9,470 men and 4,930 women) will die from this disease.
These numbers include all types of kidney and renal pelvis cancers.
Most people with kidney cancer are older. The average age of people when they are diagnosed is 64. Kidney cancer is very uncommon in people younger than age 45.
Kidney cancer is among the 10 most common cancers in both men and women. Overall, the lifetime risk for developing kidney cancer is about 1 in 63 (1.6%). This risk is higher in men than in women.
For reasons that are not totally clear, the rate of new kidney cancers has been rising since the 1990s, although this seems to have leveled off in the past few years. Part of this rise was probably due to the use of newer imaging tests such as CT scans, which picked up some cancers that might never have been found otherwise. The death rates for these cancers have gone down slightly since the middle of the 1990s.
Studies show there is a link between kidney cancer and kidney disease. Some studies show that people with kidney disease may have a higher risk for kidney cancer. On the other hand, about one-third of the 300,000 kidney cancer survivors in the United States have or will develop kidney disease 9. Some reasons are:
- Long-term dialysis. Some studies show that people on long-term dialysis have an increased risk for kidney cancer. Experts believe this risk is due to kidney disease rather than dialysis.
- Surgery on the kidney (called “nephrectomy”). Your risk for kidney disease is higher if all (rather than part) of the kidney must be removed due to cancer. If the tumor is small, it is better to remove only the tumor, but not the whole kidney. This lessens your chance of developing kidney disease. However, removing all of the kidney is often better for your survival if the tumor is large or centrally located.
- Immunosuppressant medicines. Some anti-rejection medicines that must be taken by kidney transplant recipients to prevent rejection can increase your risk for kidney cancer. However, taking your immunosuppressant medicine is important if you have a transplant. Without it, your body will reject your new kidney.
Remember, not everyone with kidney cancer will get kidney disease. Likewise, not everyone who has kidney disease or a transplant will get kidney cancer. Ask your healthcare provider what you can do to lessen your risk.
What treatments are used to treat kidney cancer ?
There are several ways to treat kidney cancer, depending on its type and stage.
Local treatments: Some treatments are called local therapies, meaning they treat the tumor without affecting the rest of the body. Types of local therapy used for kidney cancer include:
- Surgery
- Ablation and other local therapies
- Active surveillance
- Radiation therapy
These treatments are more likely to be useful for earlier stage (less advanced) cancers, although they might also be used in some other situations.
Systemic treatments: Kidney cancer can also be treated using drugs, which can be given by mouth or directly into the bloodstream. These are called systemic therapies because they can reach cancer cells almost anywhere in the body. Depending on the type of kidney cancer, several different types of drugs might be used, including:
- Targeted therapy
- Immunotherapy (biologic therapy)
- Chemotherapy
Depending on the stage of the cancer and other factors, different types of treatment may be combined at the same time or used after one another.
Some of these treatments can also be used as palliative treatment when all the cancer cannot be removed. Palliative treatment is meant to relieve symptoms, such as pain, but it is not expected to cure the cancer.
Kidney Stones
A kidney stone is a solid piece of material that forms in the kidney from substances in the urine 10. It may be as small as a grain of sand or as large as a pearl. Most kidney stones pass out of the body without help from a doctor. But sometimes a stone will not go away. It may get stuck in the urinary tract, block the flow of urine and cause great pain.
Depending on your situation, you may need nothing more than to take pain medication and drink lots of water to pass a kidney stone. In other instances — for example, if stones become lodged in the urinary tract, are associated with a urinary infection or cause complications — surgery may be needed.
The following may be signs of kidney stones that need a doctor’s help:
- Extreme pain in your back or side below the ribs that will not go away
- Pink, red or brown urine
- Fever and chills if an infection is present
- Nausea and vomiting
- Urine that smells bad or looks cloudy
- A burning feeling when you urinate
- Pain that radiates to the lower abdomen and groin
- Pain that comes in waves and fluctuates in intensity
- Pain on urination
- Persistent need to urinate
- Urinating more often than usual
- Urinating small amounts
Your doctor will diagnose a kidney stone with urine, blood, and imaging tests.
If you have a stone that won’t pass on its own, you may need treatment. It can be done with shock waves; with a scope inserted through the tube that carries urine out of the body, called the urethra; or with surgery.
Your doctor may recommend preventive treatment to reduce your risk of recurrent kidney stones if you’re at increased risk of developing them again.
Kidney Infections
Kidney infection (pyelonephritis) is a type of urinary tract infection (UTI) that generally begins in your urethra or bladder and travels to one or both of your kidneys 11. Most kidney infections are caused by bacteria or viruses that first infect your lower urinary tract, usually your bladder 12. Then, the infection moves upstream to one or both of your kidneys, which are part of the upper urinary tract.
In some cases, you can get a kidney infection after surgery if bacteria enter your body during the procedure and travel through your blood to the kidneys.
Your body has ways to defend against infections in the urinary tract. For example, urine normally flows one way from your kidneys to your bladder. Viruses or bacteria that enter are flushed out by urinating. This one-way flow of urine usually prevents an infection in your urinary tract.
Sometimes your body’s defenses fail and bacteria or viruses cause a urinary tract infection (UTI) in the bladder. If you have symptoms of a bladder infection, see a health care professional. You may need treatment to prevent the infection from spreading to your kidneys. Kidney infections are often very painful and can cause serious health problems.
A kidney infection requires prompt medical attention. If not treated properly, a kidney infection can permanently damage your kidneys or the bacteria can spread to your bloodstream and cause a life-threatening infection.
Kidney infection treatment, which usually includes antibiotics, might require hospitalization.
Who is more likely to develop a kidney infection ?
You are more likely to develop a kidney infection if you:
- Are a woman 13
- have a urinary tract infection (UTI) in the bladder.
- had a urinary tract infection (UTI) during the past 12 months.
- are pregnant. Scientists think that hormonal changes and shifts in the position of the urinary tract during pregnancy make it easier for bacteria to travel to the kidneys and cause infection.
- have a problem in your urinary tract that blocks or changes the normal flow of urine. The flow of urine may be blocked if you have a defect in the structure of your urinary tract, such as a narrowed urethra, an enlarged prostate, or a kidney stone.
- have vesicoureteral reflux, which is when urine can back up, or reflux, into one or both kidneys. Health care professionals most commonly diagnose vesicoureteral reflux in children 14.
- have diabetes or problems with your body’s immune, or natural defense, system.
- have a spinal cord injury or nerve damage around the bladder.
- have trouble emptying your bladder completely, called urinary retention.
What are the complications of kidney infections ?
In rare cases, kidney infections may cause:
- high blood pressure
- kidney failure
- permanent kidney scars, called renal scarring, which can lead to chronic kidney disease
Your chance of a complication is slightly greater if you have:
- kidney disease from other causes
- a problem with the structure of your urinary tract
- repeated episodes of kidney infection
Complications from a kidney infection are rare if a health care professional prescribes antibiotics to treat your infection.
Kidney Cysts
Kidney cysts are round pouches of fluid that form on or in the kidneys. Kidney cysts can be associated with serious disorders that may impair kidney function 15. But more commonly, kidney cysts are a type called simple kidney cysts — noncancerous cysts that rarely cause complications.
It’s not clear what causes simple kidney cysts. Typically, only one cyst occurs on the surface of a kidney, but multiple cysts can affect one or both kidneys. However, simple kidney cysts aren’t the same as the cysts that develop when a person has polycystic kidney disease, which is a genetic disorder. Simple kidney cysts do not enlarge the kidneys, replace their normal structure, or cause reduced kidney function like cysts do in people with polycystic kidney disease.
Simple kidney cysts are often detected during an imaging test performed for another condition. Simple kidney cysts that don’t cause signs or symptoms usually don’t require treatment.
Simple kidney cysts are more common as people age. An estimated 25 percent of people 40 years of age and 50 percent of people 50 years of age have simple kidney cysts 16.
What causes simple kidney cysts ?
The cause of simple kidney cysts is not fully understood. Obstruction of tubules—tiny structures within the kidneys that collect urine—or deficiency of blood supply to the kidneys may play a role. Diverticula—sacs that form on the tubules—may detach and become simple kidney cysts. The role of genetic factors in the development of simple kidney cysts has not been studied.
What are the symptoms of simple kidney cysts ?
Simple kidney cysts usually do not cause symptoms or harm the kidneys. In some cases, however, pain can occur between the ribs and hips when cysts enlarge and press on other organs. Sometimes cysts become infected, causing fever, pain, and tenderness. Simple kidney cysts are not thought to affect kidney function, but one study found an association between the presence of cysts and reduced kidney function in hospitalized people younger than 60 years of age 16. Some studies have found a relationship between simple kidney cysts and high blood pressure. For example, high blood pressure has improved in some people after a large cyst was drained. However, this relationship is not well understood 17.
How are simple kidney cysts diagnosed ?
Most simple kidney cysts are found during imaging tests done for other reasons. When a cyst is found, the following imaging tests can be used to determine whether it is a simple kidney cyst or another, more serious condition. These imaging tests are performed at an outpatient center or hospital by a specially trained technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging. Ultrasound may also be performed in a health care provider’s office. Anesthesia is not needed though light sedation may be used for people with a fear of confined spaces who undergo magnetic resonance imaging (MRI).
Ultrasound. Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. An abdominal ultrasound can create images of the entire urinary tract. The images can be used to distinguish harmless cysts from other problems.
Computerized tomography (CT) scan. CT scans use a combination of x-rays and computer technology to create three-dimensional (3-D) images. A CT scan may include the injection of a special dye, called contrast medium. CT scans require the person to lie on a table that slides into a tunnel-shaped device where the x-rays are taken. CT scans can show cysts and tumors in the kidneys.
Magnetic resonance imaging (MRI). MRI machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues without using x-rays. An MRI may include the injection of contrast medium. With most MRI machines, the person lies on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some newer machines are designed to allow the person to lie in a more open space. Like CT scans, MRIs can show cysts and tumors.
How are simple kidney cysts treated ?
Treatment is not needed for simple kidney cysts that do not cause any symptoms. Simple kidney cysts may be monitored with periodic ultrasounds.
Simple kidney cysts that are causing symptoms or blocking the flow of blood or urine through the kidney may need to be treated using a procedure called sclerotherapy. In sclerotherapy, the doctor punctures the cyst using a long needle inserted through the skin. Ultrasound is used to guide the needle to the cyst. The cyst is drained and then filled with a solution containing alcohol to make the kidney tissue harder. The procedure is usually performed on an outpatient basis with a local anesthetic.
If the cyst is large, surgery may be needed. Most surgeries can be performed using a laparoscope—a special tool with a small, lighted video camera. The procedure is usually done under general anesthesia in a hospital. The surgeon drains the cyst and then removes or burns away its outer tissue. This type of surgery allows for a smaller incision and quicker recovery.
Eating, Diet, and Nutrition
Eating, diet, and nutrition have not been shown to play a role in causing or preventing simple kidney cysts.
Kidney transplant
A kidney transplant is an operation that places a healthy kidney in your body. The transplanted kidney takes over the work of the two kidneys that failed, so you no longer need dialysis.
During a transplant, the surgeon places the new kidney in your lower abdomen and connects the artery and vein of the new kidney to your artery and vein. Often, the new kidney will start making urine as soon as your blood starts flowing through it. But sometimes it takes a few weeks to start working.
Many transplanted kidneys come from donors who have died. Some come from a living family member. The wait for a new kidney can be long.
On the plus side, there are fewer limits on what you can eat and drink, but you should follow a heart-healthy diet. Your health and energy should improve. In fact, a successful kidney transplant may allow you to live the kind of life you were living before you got kidney disease. Studies show that people with kidney transplants live longer than those who remain on dialysis.
On the minus side, there are the risks of surgery. And you must take anti-rejection medicines for the rest of your life, to keep your body from rejecting the new kidney, which can have side effects. You will have a higher risk for infections and certain types of cancer.
Although most transplants are successful and last for many years, how long they last can vary from one person to the next. Many people will need more than one kidney transplant during a lifetime.
What is a “preemptive” or “early” transplant ?
Getting a transplant before you need to start dialysis is called a preemptive transplant 18. It allows you to avoid dialysis altogether. Getting a transplant not long after kidneys fail (but with some time on dialysis) is referred to as an early transplant 18. Both have benefits. Some research shows that a pre-emptive or early transplant, with little or no time spent on dialysis, can lead to better long-term health. It may also allow you to keep working, save time and money, and have a better quality of life.
Who can get a kidney transplant ?
Kidney patients of all ages—from children to seniors—can get a transplant.
You must be healthy enough to have the operation. You must also be free from cancer and infection 18. Every person being considered for transplant will get a full medical and psychosocial evaluation to make sure they are a good candidate for transplant. The evaluation helps find any problems, so they can be corrected before transplant. For most people, getting a transplant can be a good treatment choice.
What if you’re older or have other health problems ?
In many cases, people who are older or have other health conditions like diabetes can still have successful kidney transplants. Careful evaluation is needed to understand and deal with any special risks. You may be asked to do some things that can lessen certain risks and improve the chances of a successful transplant. For example, you may be asked to lose weight or quit smoking.
If you have diabetes, you may also be able to have a pancreas transplant. Ask your healthcare professional about getting a pancreas transplant along with a kidney transplant.
How will you pay for a transplant ?
Medicare covers about 80% of the costs associated with an evaluation, transplant operation, follow-up care, and anti-rejection medicines. Private insurers and state programs may cover some costs as well. However, your post-transplant expenses may only be covered for a limited number of years. It’s important to discuss coverage with your social worker, who can answer your questions or direct you to others who can help.
Getting a Transplant
How do you start the process of getting a kidney transplant ?
Ask your healthcare provider to refer you to a transplant center for an evaluation, or contact a transplant center in your area. Any kidney patient can ask for an evaluation.
How does the evaluation process work ?
Medical professionals will give you a complete physical exam, review your health records, and order a series of tests and X-rays to learn about your overall health. Everything that can affect how well you can handle treatment will be checked. The evaluation process for a transplant is very thorough. Your healthcare team will need to know a lot about you to help them—and you—decide if a transplant is right for you. One thing you can do to speed the process is to get all the testing done as quickly as possible and stay in close contact with the transplant team. If you’re told you might not be right for a transplant, don’t be afraid to ask why—or if you might be eligible at some future time or at another center. Remember, being active in your own care is one of the best ways to stay healthy.
If someone you know would like to donate a kidney to you, that person will also need to go through a screening to find out if he or she is a match and healthy enough to donate.
If it’s your child who has kidney disease, you’ll want to give serious thought to getting a transplant evaluation for him or her. Because transplantation allows children and young adults to develop in as normal a way as possible in their formative years, it can be the best treatment for them.
If the evaluation process shows that a transplant is right for you or your child, the next step is getting a suitable kidney.
What does the kidney transplant operation involve ?
You may be surprised to learn that your own kidneys generally aren’t taken out when you get a transplant. The surgeon leaves them where they are unless there is a medical reason to remove them. The donated kidney is placed into your lower abdomen (belly), where it’s easiest to connect it to your important blood vessels and bladder. Putting the new kidney in your abdomen also makes it easier to take care of any problems that might come up.
The operation takes about four hours. You’ll be sore at first, but you should be out of bed in a day or so, and home within a week. If the kidney came from a living donor, it should start to work very quickly. A kidney from a deceased donor can take longer to start working—two to four weeks or more. If that happens, you may need dialysis until the kidney begins to work.
After surgery, you’ll be taught about the medicines you’ll have to take and their side effects. You’ll also learn about diet. If you’ve been on dialysis, you’ll find that there are fewer restrictions on what you can eat and drink, which is one of the benefits of a transplant.
What are anti-rejection medicines ?
Normally, your body fights off anything that isn’t part of itself, like germs and viruses. That system of protection is called your immune system. To stop your body from attacking or rejecting the donated kidney, you will have to take medicines to keep your immune system less active (called anti-rejection medicines or immunosuppressant medicines). You’ll need to take them as long as your new kidney is working. Without them, your immune system would see the donated kidney as “foreign,” and would attack and destroy it.
Anti-rejection medicines can have some side effects. It is important to talk to your healthcare provider about them, so that you know what to expect. Fortunately, for most people, side effects are usually manageable. Changing the dose or type of medicine can often ease some of the side effects.
Besides the immunosuppressive medicines, you will take other medicines as well. You will take medicines to protect you from infection, too. Most people find taking medicines a small trade for the freedom and quality of life that a successful transplant can provide.
After Your Kidney Transplant
What happens after you go home ?
Once you are home from the hospital, the most important work begins—the follow-up. For your transplant to be successful, you will have regular checkups, especially during the first year. At first, you may need blood tests several times a week. After that, you’ll need fewer checkups, but enough to make sure that your kidney is working well and that you have the right amount of anti-rejection medication in your body.
What if your body tries to reject the new kidney ?
One thing that you and your healthcare team will watch for is acute rejection, which means that your body is suddenly trying to reject the transplanted kidney. A rejection episode may not have any clear signs or symptoms. That is why it is so important to have regular blood tests to check how well your kidney is working. Things you might notice that can let you know you are having rejection are fevers, decreased urine output, swelling, weight gain, and pain over your kidney.
The chances of having a rejection episode are highest right after your surgery. The longer you have the kidney, the lower the chance that this will happen. Unfortunately, sometimes a rejection episode happens even if you’re doing everything you’re supposed to do. Sometimes the body just doesn’t accept the transplanted kidney. But even if a rejection episode happens, there are many ways to treat it so you do not lose your transplant. Letting your transplant team know right away that you think you have symptoms of rejection is very important.
How often do rejection episodes happen ?
Rejections happen much less often nowadays. That’s because there have been many improvements in immunosuppressive medicines. However, the risk of rejection is different for every person. For most people, rejection can be stopped with special anti-rejection medicines. It’s very important to have regular checkups to see how well your kidney is working, and make sure you are not having rejection.
When can you return to work ?
How soon you can return to work depends on your recovery, the kind of work you do, and your other medical conditions. Many people can return to work eight weeks or more after their transplant. Your transplant team will help you decide when you can go back to work.
Will your sex life be affected ?
People who have not had satisfactory sexual relations due to kidney disease may notice an improvement as they begin to feel better. In addition, fertility (the ability to conceive children) tends to increase. Men who have had a kidney transplant have fathered healthy children, and women with kidney transplants have had successful pregnancies. It’s best to talk to your healthcare practitioner when considering having a child.
Women should avoid becoming pregnant too soon after a transplant. Most centers want women to wait a year or more. All pregnancies must be planned. Certain medications that can harm a developing baby must be stopped six weeks before trying to get pregnant. Birth control counseling may be helpful. It’s important to protect yourself against sexually transmitted diseases (STDs). Be sure to use protection during sexual activity.
Will you need to follow a special diet ?
In general, transplant recipients should eat a heart-healthy diet (low fat, low salt) and drink plenty of fluids. If you have diabetes or other health problems, you may still have some dietary restrictions. A dietitian can help you plan meals that are right for you.
Finding a Kidney
Where do donated kidneys come from ?
A donated kidney may come from someone who died and donated a healthy kidney. A person who has died and donated a kidney is called a deceased donor.
Donated kidneys also can come from a living donor. This person may be a blood relative (like a brother or sister) or non-blood relative (like a husband or wife). They can also come from a friend or even a stranger.
When a kidney is donated by a living person, the operations are done on the same day and can be scheduled at a convenient time for both the patient and the donor. A healthy person who donates a kidney can live a normal life with the one kidney that is left. But the operation is major surgery for the donor, as well as the recipient. As in any operation, there are some risks that you will need to consider.
Is it better to get a kidney from a living donor ?
Kidneys from living or deceased donors both work well, but getting a kidney from a living donor can work faster and be better. A kidney from a living donor may last longer than one from a deceased donor.
To get a deceased donor kidney, you will be placed on a waiting list once you have been cleared for a transplant. It can take many years for a good donor kidney to be offered to you. From the time you go on the list until a kidney is found, you may have to be on some form of dialysis. While you’re waiting, you’ll need regular blood tests to make sure you are ready when a kidney is found. If you’re on dialysis, your center will make the arrangements for these tests. Your transplant center should know how to reach you at all times. Once a kidney become available, the surgery must be done as soon as possible.
Are there disadvantages to living donation ?
A disadvantage of living donation is that a healthy person must undergo surgery to remove a healthy kidney. The donor will need some recovery time before returning to work and other activities. However, recent advances in surgery (often called minimally invasive or laparoroscopic surgery) allow for very small incisions. This means shorter hospital stays and recovery time, less pain, and a quicker return to usual activities. Living donors often experience positive feelings about their courageous gift.
What are the financial costs to the living donor ?
The surgery and evaluation is covered by Medicare or the recipient’s insurance. The living donor will not pay for anything related to the surgery. However, neither Medicare nor insurance covers time off from work, travel expenses, lodging, or other incidentals. The National Living Donor Assistance Program (www.livingdonorassistance.org) or other programs may help cover travel and lodging costs.
Donors may be eligible for sick leave, state disability, and benefits under the federal Family Medical Leave Act. In addition, federal employees, some state employees, and certain other workers may be eligible for 30 days paid leave.
- http://nkdep.nih.gov/professionals/gfr_calculators/gfr_faq.htm[↩]
- Kidney disease . Department of Health & Human Services, State Government of Victoria. https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/kidney-disease[↩]
- Kidney Diseases. Medline Plus. https://medlineplus.gov/kidneydiseases.html[↩]
- Acute kidney injury. Kidney Health Australia. http://kidney.org.au/your-kidneys/detect/accute-kidney-injury[↩]
- Chronic kidney disease. Medline Plus. https://medlineplus.gov/chronickidneydisease.html[↩]
- What is Kidney Cancer? National Kidney Foundation. https://www.kidney.org/atoz/content/what-kidney-cancer[↩]
- What Is Kidney Cancer? American Cancer Society. https://www.cancer.org/cancer/kidney-cancer/about/what-is-kidney-cancer.html[↩]
- What Are the Key Statistics About Kidney Cancer? American Cancer Society. https://www.cancer.org/cancer/kidney-cancer/about/key-statistics.html[↩]
- Chang A, Finelli A, Berns JS, Rosner M. Chronic kidney disease in patients with renal cell carcinoma. Adv Chronic Kidney Dis. Jan 2014;21(1):91-95.[↩]
- Kidney Stones. Medline Plus. https://medlineplus.gov/kidneystones.html[↩]
- Kidney infection. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/kidney-infection/symptoms-causes/syc-20353387[↩]
- Definition & Facts of Kidney Infection (Pyelonephritis). National Institute of Diabetes and Digestive and Kidney Diseases. https://www.niddk.nih.gov/health-information/urologic-diseases/kidney-infection-pyelonephritis/definition-facts[↩]
- Czaja CA, Scholes D, Hooton TM, Stamm WE. Population-based epidemiologic analysis of acute pyelonephritis. Clinical Infectious Diseases. 2007;45(3):273–280.[↩]
- Guarino N, Casamassima MG, Tadini B, Marras E, Lace R, Bianchi M. Natural history of vesicoureteral reflux associated with kidney anomalies. Urology. 2005;65(6):1208–1211.[↩]
- Kidney cysts. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/kidney-cysts/basics/definition/con-20035205[↩]
- Torres VE, Grantham JJ. Cystic diseases of the kidney. In: Brenner BM, ed. Brenner & Rector’s The Kidney. Vol. 2. 8th ed. Philadelphia: Saunders Elsevier; 2008: 1451–1453.[↩][↩]
- Zerem E, Imamovic G, Omerovic S. Simple renal cysts and arterial hypertension: does their evacuation decrease the blood pressure. Journal of Hypertension. 2009;27(10):2074–2078.[↩]
- Kidney Transplant. National Kidney Foundation. https://www.kidney.org/atoz/content/kidney-transplant[↩][↩][↩]

{kind=link}