
Contents
- What is krill oil
- Seafood vs. Supplements
- What are omega-3 fatty acids?
- Krill oil benefits
- Is krill oil better than fish oil?
- Krill oil dosage
- Krill oil side effects
What is krill oil
Krill (Euphausia superba) are small red-colored crustaceans, similar to shrimp, that flourish in the extremely cold waters of the Antarctic Ocean. Krill primarily serve as a food source for other animals in the ocean, for example – whales, seals, penguins, squid and fish. Similar to fish, krill consume a diet rich in omega-3 fatty acids (e.g, algae) and are thereby a natural source of Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) Omega-3 essential fatty acids 1. Although there are other sources you can get the Omega-3 essential fatty acids from, for example Alpha-linolenic acid (ALA) from plant oils such as flaxseed, soybean, and canola oils; only krill oil and fish oil is rich in Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) Omega-3 essential fatty acids. Omega-3 Eicosapentaenoic acid (EPA) and Omega-3 Docosahexaenoic acid (DHA) are found in seafood, including fatty fish (e.g., salmon, tuna, and trout) and shellfish (e.g., crab, mussels, and oysters).
- Note the differences between the Omega-3 fatty acids found in flaxseed, soybean, vegetable oils [alpha-linolenic acid (ALA)] from those in fish and seafoods [Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA)].
- Your bodies can convert plant omega-3 fatty acids, Alpha-linolenic acid (ALA), to fish omega-3 fatty acids, Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA), but only a small fraction about 5% of Alpha-linolenic acid (ALA) to eicosapentaenoic acid (EPA), the level of eicosapentaenoic acid (EPA) in blood does not rise when you eat α-linolenic acid (ALA) 2.
Krills survival in such a frigid environment is attributable to krill having a high content of long-chain polyunsaturated fatty acids (PUFAs), including eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), attached to their cell membranes via phospholipids (primarily phosphatidylcholine). This structure provides optimum membrane fluidity in cold temperatures and an ideal source of omega-3 fatty acids 3. Fish oil contains abundant amounts of Omega-3 PUFAs, most of which is stored as triglycerides. Animal and human studies indicate long-chain polyunsaturated fatty acids bound to phospholipids, like those found in krill oil, have better absorption and delivery to the brain than their methyl ester or triglyceride-formed fish oil counterparts 4, 5, 6.
Seafood vs. Supplements
- For some health conditions, the evidence for benefits from seafood (fish and shellfish) is stronger than the evidence for omega-3 supplements.
How could this happen?
Here are some possibilities:
- Seafood may provide enough omega-3s; more may not be better.
- Other nutrients in seafood besides omega-3s may play a role in its benefits.
- Some of the benefits of seafood may result from people eating it in place of less healthful foods.
- There’s evidence that people who eat seafood have generally healthier lifestyles.
The Federal Government’s Dietary Guidelines for Americans 7 recommends that adults eat 8 or more ounces of a variety of seafood (fish or shellfish) per week for the total package of nutrients seafood provides, and that some seafood choices with higher amounts of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) be included. Smaller amounts of seafood are recommended for young children.
The American Heart Association recommends eating fish (particularly fatty fish) at least two times (two servings) a week. Each serving is 3.5 ounce cooked, or about ¾ cup of flaked fish. Fatty fish like salmon, mackerel, herring, lake trout, sardines and albacore tuna are high in omega-3 fatty acids 8.
Increasing omega-3 fatty acid consumption through foods is preferable. However, those with coronary artery disease, may not get enough omega-3 by diet alone. These people may want to talk to their doctor about supplements. And for those with high triglycerides, even larger doses could help.
Patients taking more than 3 grams of omega-3 fatty acids from capsules should do so only under a physician’s care. High intakes could cause excessive bleeding in some people.
Eating fish, is there a catch?
Some types of fish may contain high levels of mercury, PCBs (polychlorinated biphenyls), dioxins and other environmental contaminants. Levels of these substances are generally highest in older, larger, predatory fish and marine mammals.
The benefits and risks of eating fish vary depending on a person’s stage of life.
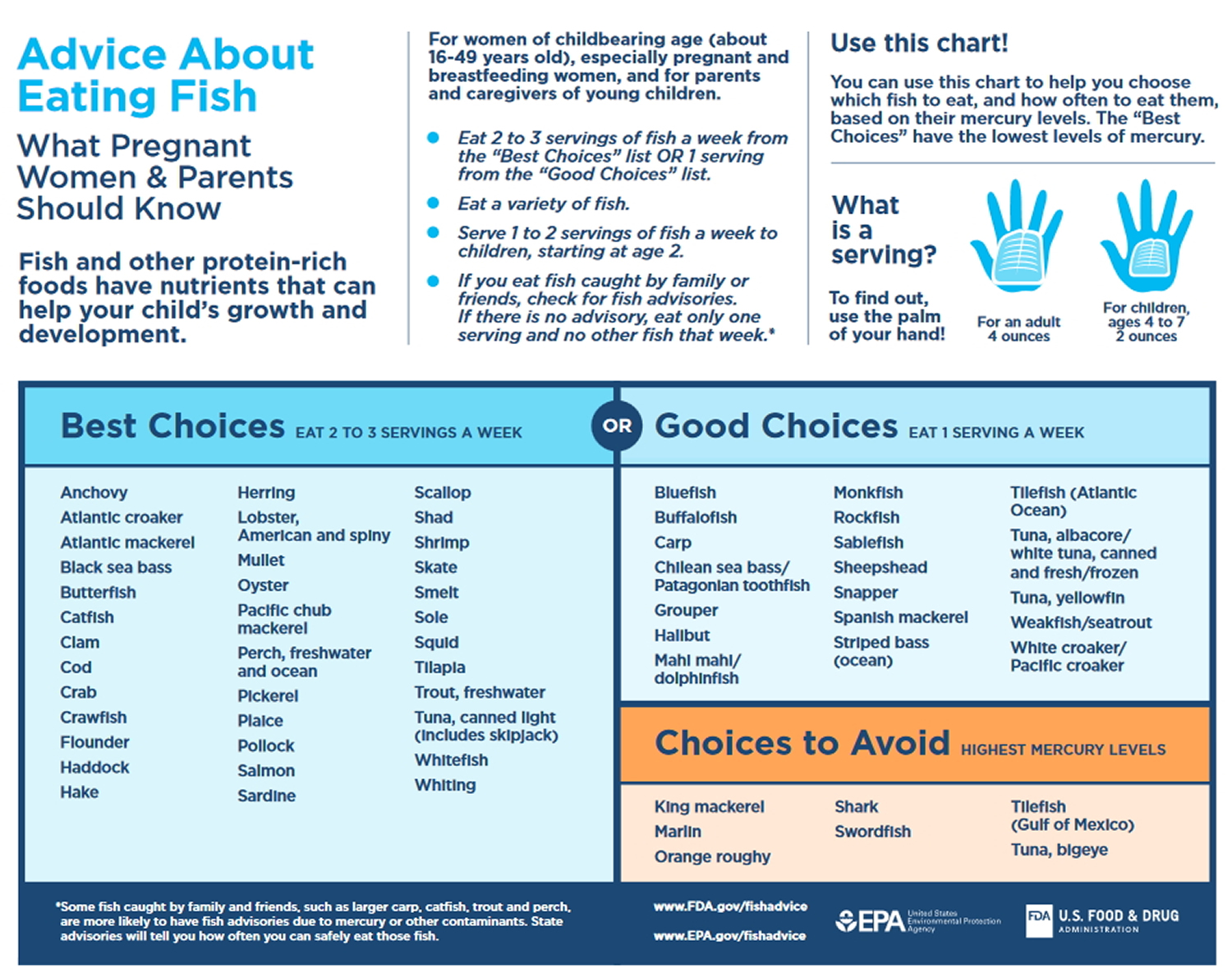
- Children and pregnant women are advised by the U.S. Food and Drug Administration (FDA) to avoid eating those fish with the potential for the highest level of mercury contamination (e.g., shark, swordfish, king mackerel or tilefish); to eat up to 12 ounces (two average meals) per week of a variety of fish and shellfish that are lower in mercury (e.g., canned light tuna, salmon, pollock, catfish); and check local advisories about the safety of fish caught by family and friends in local lakes, rivers and coastal areas.
- For middle-aged and older men and postmenopausal women, the benefits of fish consumption far outweigh the potential risks when the amount of fish are eaten is within the recommendations established by the FDA and Environmental Protection Agency.
- Eating a variety of fish will help minimize any potentially adverse effects due to environmental pollutants.
Five of the most commonly eaten fish or shellfish that are low in mercury are shrimp, canned light tuna, salmon, pollock, and catfish. Avoid eating shark, swordfish, king Mackerel, or tilefish because they contain high levels of mercury.
Avoid large predatory fish (e.g. marlin, pike, swordfish and shark), which are more likely to be contaminated with methylmercury.
What are omega-3 fatty acids?
Omega-3 fatty acids are essential fatty acids, a type of polyunsaturated fatty acid (PUFA) that are vital for brain and nerve function. They are called an “essential fatty acid” because you cannot manufacture them yourself and must get them from food.
Polyunsaturated fatty acids (PUFAs) can be further subdivided on the basis of the location of the first double bond relative to the methyl terminus of the chain. For example, Omega-3 and Omega-6 fatty acids are two of the most biologically significant polyunsaturated fatty acid classes, and have their first double bond on either the third or sixth carbon from the chain terminus, respectively. The final carbon in the fatty acid chain is also known as the omega carbon, hence the common reference to these fatty acids as Omega-3 or Omega-6 PUFAs. The distinction between omega-6 and omega-3 fatty acids is based on the location of the first double bond, counting from the methyl end of the fatty acid molecule (see Figure 2). Omega-6 fatty acids are represented by Linoleic acid (LA) (18:2ω-6) and Arachidonic acid (AA) (20:4ω-6) and omega-3 fatty acids by Alpha-linolenic acid (ALA) (18:3ω-3), Eicosapentaenoic acid (EPA) (20:5ω-3) and Docosahexaenoic acid (DHA) (22:6ω-3).
There are three main types of omega-3 fatty acids:
- Eicosapentaenoic acid (EPA)
- Docosahexaenoic acid (DHA)
- Alpha-linolenic acid (ALA).
The general structures for Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) are shown in Figure 2. Commonly available dietary sources of Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA)are listed in Table 2. Whereas plant foods and vegetable oils lack EPA and DHA, some do contain varying amounts of the Omega-3 PUFA alpha-linolenic acid (ALA), which has 18 carbon atoms and 3 double bonds (Figure 2). Many vegetable oils are greatly enriched in Omega-6 fatty acids (mainly as linoleic acid [LA] in corn, safflower, sunflower and soybean oils), but canola oil (nonhydrogenated), ground flaxseed and walnuts are rich sources of ALA.
The typical North American diet provides about 1–3 g of Omega-3 PUFA alpha-linolenic acid (ALA) per day but only 0.10–0.15 g of EPA (Eicosapentaenoic acid) plus DHA (Docosahexaenoic acid) per day 10, 11. The very high intake of Omega-6 PUFA, mostly as linoleic acid (LA) (Figure 2) in our diet (12–15 g/day) from common vegetable oils (corn, safflower, soybean) and other sources, yields an overall n-6:n-3 dietary ratio (total omega-6 fatty acids in the diet: total omega-3 fatty acids in the diet) of about 8:1. Health Canada has recommended that this ratio be as low as 4:19 to reduce the competitive influence of high Omega-6 PUFA linoleic acid (LA) intakes on omega-3 PUFA alpha-linolenic acid (ALA) metabolism to its longer chain products (such as EPA and DHA). Although high intakes of Omega-6 PUFA linoleic acid (LA) can provide some modest blood cholesterol lowering, experimental studies in animals have raised concerns regarding the enhancing effect of these high intakes on certain cancers 12. This association has not been established in human studies 13.
Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) are synthesised by algae and marine plants, particularly in cold water. As a result, most marine-based supplements, including fish oil and krill oil, contain Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA).
Omega-3 fatty acid alpha-linolenic acid (ALA) is made by plants and high amounts of alpha-linolenic acid (ALA) can be found in vegetable oils and nuts. Flax seeds, canola, soy, perilla, and walnuts are all high in ALA. In addition, alpha-linolenic acid (ALA) is also found in the fat of animals that eat grass. Our bodies are able to convert ALA into EPA and DHA; however, research suggests only a small fraction about 5% of Alpha-linolenic acid (ALA) to eicosapentaenoic acid (EPA), the level of eicosapentaenoic acid (EPA) in blood does not rise when we eat α-linolenic acid (ALA) 2.
Note the differences between the Omega-3 fatty acids found in flaxseed, soybean, vegetable oils and walnuts [alpha-linolenic acid (ALA)] from those in fish and seafoods [Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA)].
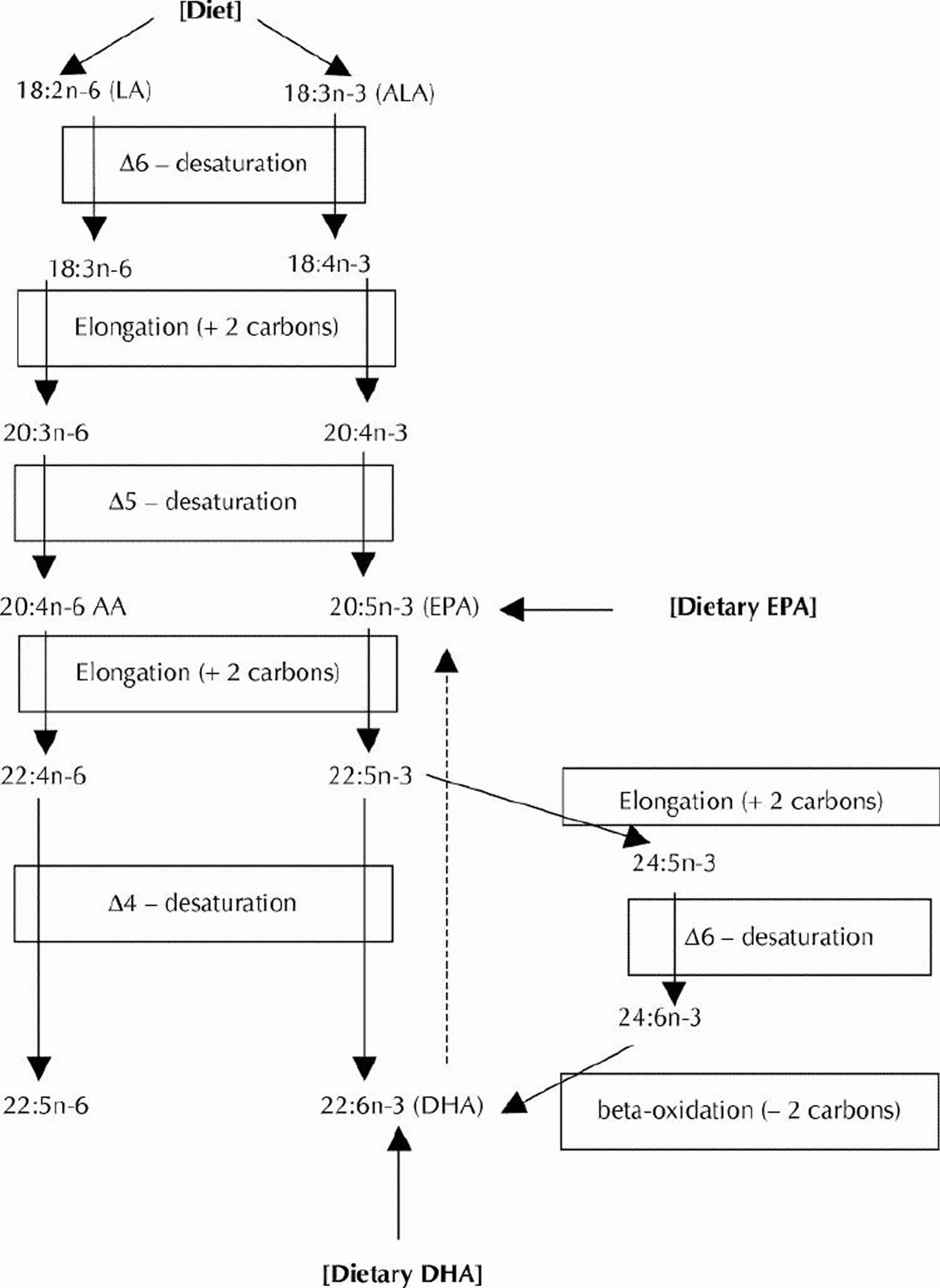
Long-chain Omega-3 and Omega-6 PUFAs are synthesized from the essential fatty acids: alpha-linolenic acid (ALA) and linoleic acid (LA), respectively. Basic structures of these two parent PUFAs are shown in Figure 2. An essential fatty acid cannot be made by the body and must be obtained through dietary sources. Animals and humans have the capacity to metabolize essential fatty acids to long-chain derivatives. Because the Omega-3 and Omega-6 pathways compete with one another for enzyme activity, the ratio of Omega-6 to Omega-3 PUFAs is very important to human health. An overabundance of fatty acids from one family will limit the metabolic production of the longer chain products of the other. The typical Western diet provides Omega-6 and Omega-3 PUFAs in a ratio ranging from 8:1 to 25:1 14, values in severe contrast with the recommendations from national health agencies of approximately 4:1 15. Lowering the Omega-6/Omega-3 ratio would reduce competition for the enzymes and facilitate the metabolism of more downstream products of alpha-linolenic acid (ALA).
Mammalian cells cannot convert Omega-6 to Omega-3 fatty acids because they lack the converting enzyme, omega-3 desaturase. Omega-6 and Omega-3 fatty acids are not interconvertible, are metabolically and functionally distinct, and often have important opposing physiological effects, therefore their balance in the diet is important 16.
This study 16 showed a balanced oOmega-6/Omega-3 ratio 1–2/1 is one of the most important dietary factors in the prevention of obesity, along with physical activity. A lower Omega-6/Omega-3 ratio should be considered in the management of obesity 16.
Because most diets are already very rich in Omega-6 PUFAs, greater focus needs to be placed on incorporating Omega-3 PUFAs into our diet. Dietary sources of Omega-3 PUFAs are readily available but in limited quantities. Many foods contain alpha-linolenic acid (ALA), including certain vegetable oils, dairy products, flaxseed, walnuts and vegetables 17. Fatty fish, such as mackerel, herring and salmon, provide an excellent source of the long-chain derivatives of ALA, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) 15.
Figure 1. Polyunsaturated Fatty Acids Structure (PUFA)
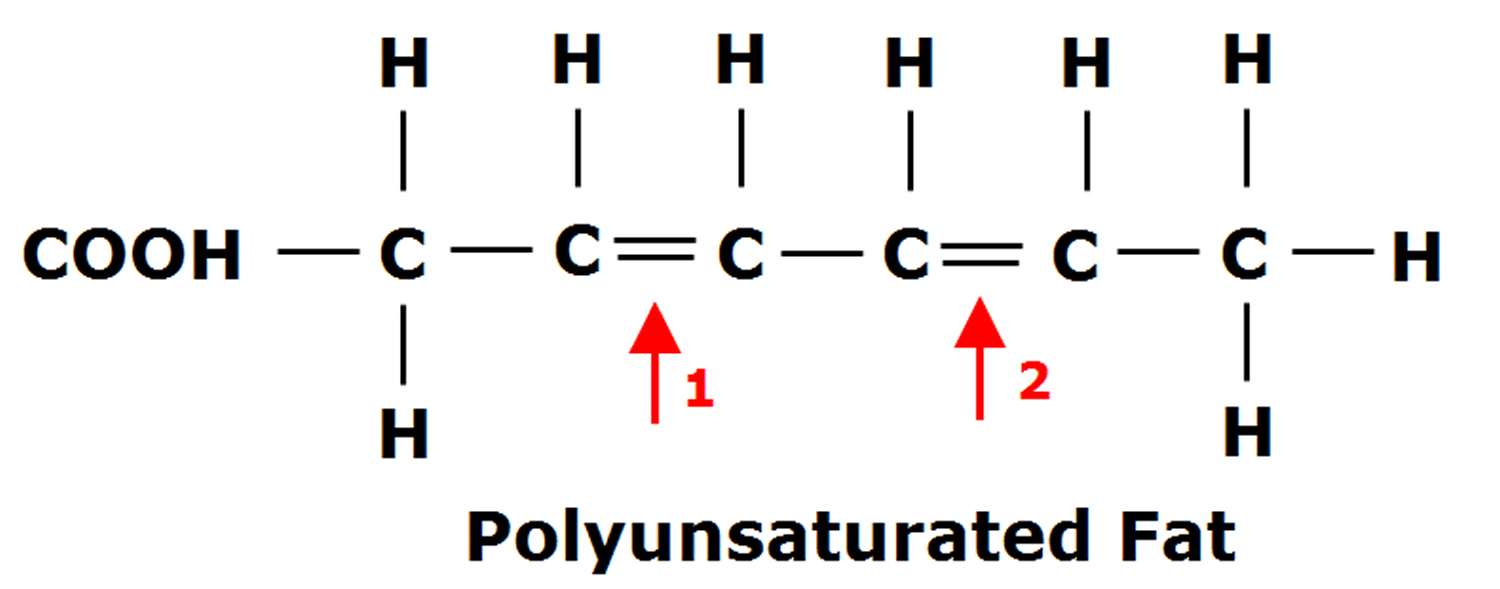
Figure 2. Omega-3 fatty acids and Omega-6 fatty acids structure
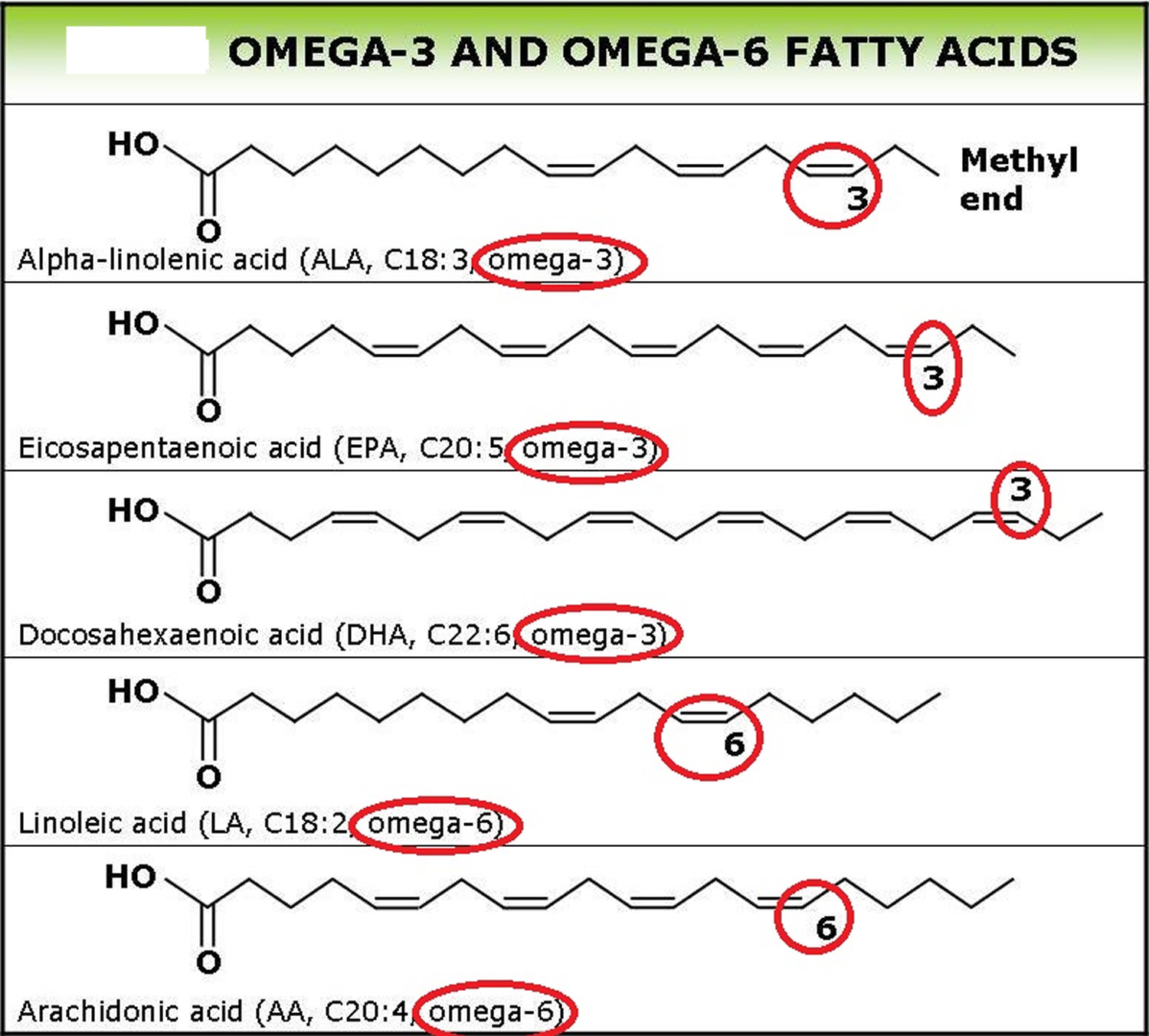
Figure 3. Conversion of dietary ALA to EPA and DHA via Desaturation, elongation and retroconversion of polyunsaturated fatty acids.
Recommended Intakes of Omega-3 Fatty Acids
Intake recommendations for fatty acids and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board of the Institute of Medicine. DRI is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and sex, include:
- Recommended Dietary Allowance (RDA): average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals.
- Adequate Intake (AI): established when evidence is insufficient to develop an RDA; intake at this level is assumed to ensure nutritional adequacy.
- Estimated Average Requirement (EAR): average daily level of intake estimated to meet the requirements of 50% of healthy individuals. It is usually used to assess the adequacy of nutrient intakes in populations but not individuals.
- Tolerable Upper Intake Level (UL): maximum daily intake unlikely to cause adverse health effects.
- Acceptable Macronutrient Distribution Range (AMDR): range of intake for a particular energy source (macronutrient) that is associated with reduced risk of chronic disease while providing intakes of essential nutrients.
When the Food and Nutrition Board of the Institute of Medicine last reviewed omega-3s, insufficient data were available to establish an Estimated Average Requirement (EAR), so the Food and Nutrition Board of the Institute of Medicine established AIs for all ages based on omega-3 intakes in healthy populations 19.
Table 1 lists the current Adequate Intake (AIs) for omega-3s in grams per day. Human milk contains omega-3s as ALA, EPA and DHA, so the Institute of Medicine established an AI for infants from birth to 12 months that is equivalent to the mean intake of omega-3s in healthy, breastfed infants.
For infants, the AIs apply to total omega-3s. For ages 1 and older, the AIs apply only to ALA because ALA is the only omega-3 that is essential. The Institute of Medicine did not establish specific intake recommendations for EPA, DHA or other long chain omega-3s.
The Federal Government’s Dietary Guidelines for Americans 7 recommends that adults eat 8 or more ounces of a variety of seafood (fish or shellfish) per week for the total package of nutrients seafood provides, and that some seafood choices with higher amounts of EPA and DHA be included. Smaller amounts of seafood are recommended for young children.
Table 1: Adequate Intakes (AIs) for Omega-3s
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months* | 0.5 g | 0.5 g | ||
| 7–12 months* | 0.5 g | 0.5 g | ||
| 1–3 years** | 0.7 g | 0.7 g | ||
| 4–8 years** | 0.9 g | 0.9 g | ||
| 9–13 years** | 1.2 g | 1.0 g | ||
| 14–18 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
| 19-50 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
| 51+ years** | 1.6 g | 1.1 g |
*As total omega-3s
**As ALA
Table 2. Omega-3 Fatty Acid Foods EPA (Eicosapentaenoic acid) and DHA (Docosahexaenoic acid) – Fish and Seafood Sources
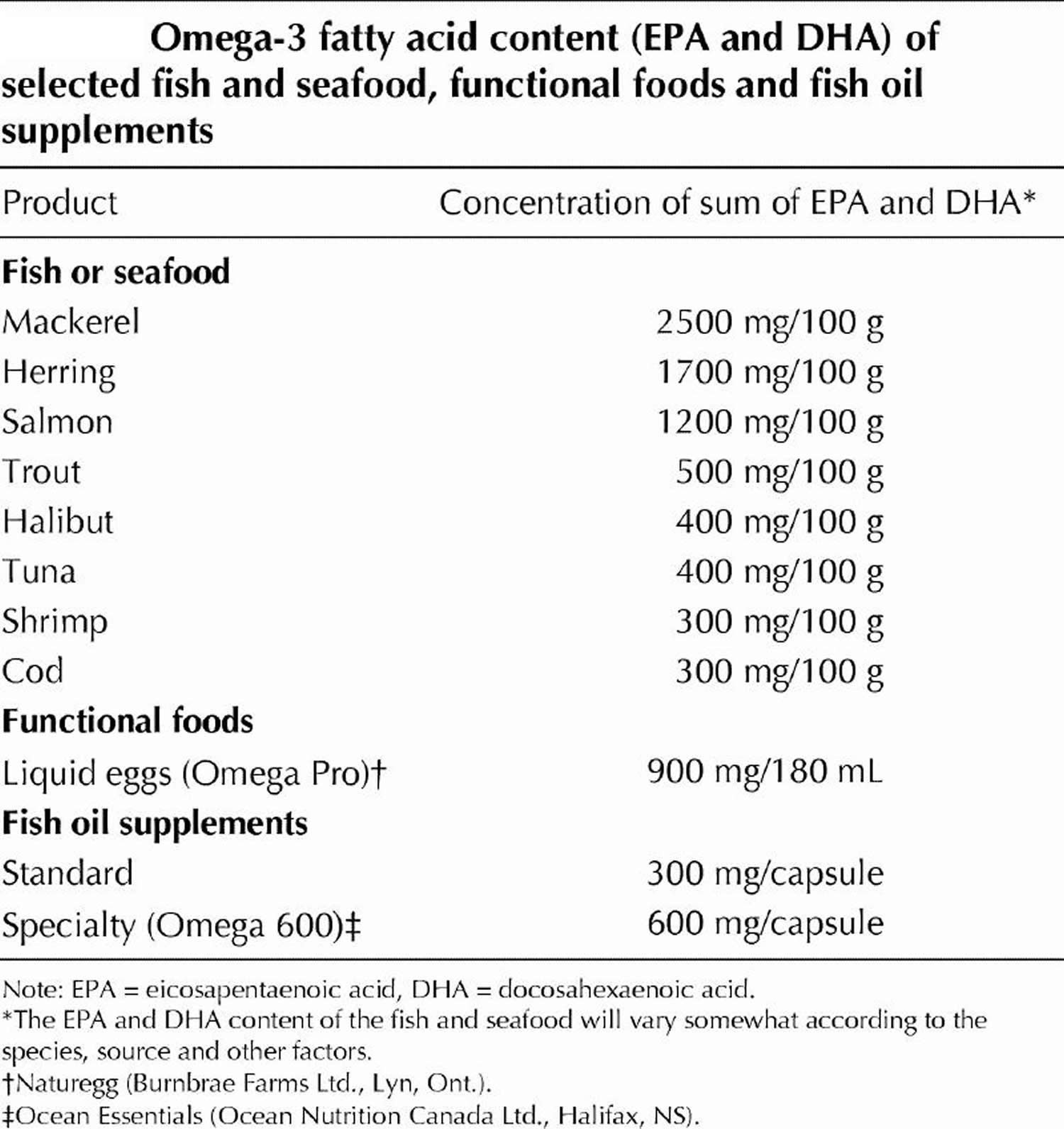
Table 3. EPA (Eicosapentaenoic acid) and DHA (Docosahexaenoic acid) Content of Fish Species
| Fish Species and Description | DHA per 100 g | EPA per 100 g | DHA+EPA per 100 g | DHA+EPA per 85 g (3 oz.) |
|---|---|---|---|---|
| Crustaceans, crab, Alaska king, cooked, moist heat | 0.118 | 0.295 | 0.413 | 0.351 |
| Crustaceans, crab, blue, cooked, moist heat | 0.231 | 0.243 | 0.474 | 0.403 |
| Crustaceans, crab, Dungeness, cooked, moist heat | 0.113 | 0.281 | 0.394 | 0.335 |
| Crustaceans, crab, queen, cooked, moist heat | 0.145 | 0.332 | 0.477 | 0.405 |
| Crustaceans, crayfish, mixed species, farmed, cooked, moist heat | 0.038 | 0.124 | 0.162 | 0.138 |
| Crustaceans, crayfish, mixed species, wild, cooked, moist heat | 0.047 | 0.119 | 0.166 | 0.141 |
| Crustaceans, lobster, northern, cooked, moist heat | 0.031 | 0.053 | 0.084 | 0.071 |
| Crustaceans, shrimp, mixed species, cooked, moist heat | 0.144 | 0.171 | 0.315 | 0.268 |
| Crustaceans, spiny lobster, mixed species, cooked, moist heat | 0.139 | 0.341 | 0.480 | 0.408 |
| Fish, anchovy, European, raw | 0.911 | 0.538 | 1.449 | 1.232 |
| Fish, anchovy, European, canned in oil, drained solids | 1.292 | 0.763 | 2.055 | 1.747 |
| Fish, bass, freshwater, mixed species, cooked, dry heat | 0.458 | 0.305 | 0.763 | 0.649 |
| Fish, bass, striped, cooked, dry heat | 0.750 | 0.217 | 0.967 | 0.822 |
| Fish, bluefish, cooked, dry heat | 0.665 | 0.323 | 0.988 | 0.840 |
| Fish, turbot, cooked, dry heat | 0.123 | 0.09 | 0.213 | 0.181 |
| Fish, carp, cooked, dry heat | 0.146 | 0.305 | 0.451 | 0.383 |
| Fish, catfish, channel, farmed, cooked, dry heat | 0.128 | 0.049 | 0.177 | 0.150 |
| Fish, catfish, channel, wild, cooked, dry heat | 0.137 | 0.100 | 0.237 | 0.201 |
| Fish, caviar, black and red, granular | 3.800 | 2.741 | 6.541 | 5.560 |
| Fish, cod, Atlantic, cooked, dry heat | 0.154 | 0.004 | 0.158 | 0.134 |
| Fish, cod, Pacific, cooked, dry heat | 0.173 | 0.103 | 0.276 | 0.235 |
| Fish, croaker, Atlantic, raw | 0.097 | 0.123 | 0.22 | 0.187 |
| Fish, dolphin fish, cooked, dry heat | 0.113 | 0.026 | 0.139 | 0.118 |
| Fish, drum, freshwater, cooked, dry heat | 0.368 | 0.295 | 0.663 | 0.564 |
| Fish, eel, mixed species, cooked, dry heat | 0.081 | 0.108 | 0.189 | 0.161 |
| Fish, fish portions and sticks, frozen, preheated | 0.128 | 0.086 | 0.214 | 0.182 |
| Fish, flatfish (flounder and sole species), cooked, dry heat | 0.258 | 0.243 | 0.501 | 0.426 |
| Fish, grouper, mixed species, cooked, dry heat | 0.213 | 0.035 | 0.248 | 0.211 |
| Fish, haddock, cooked, dry heat | 0.162 | 0.076 | 0.238 | 0.202 |
| Fish, halibut, Atlantic and Pacific, cooked, dry heat | 0.374 | 0.091 | 0.465 | 0.395 |
| Fish, halibut, Greenland, cooked, dry heat | 0.504 | 0.674 | 1.178 | 1.001 |
| Fish, herring, Atlantic, cooked, dry heat | 1.105 | 0.909 | 2.014 | 1.712 |
| Fish, herring, Atlantic, kippered | 1.179 | 0.97 | 2.149 | 1.827 |
| Fish, herring, Pacific, cooked, dry heat | 0.883 | 1.242 | 2.125 | 1.806 |
| Fish, lingcod, cooked, dry heat | 0.130 | 0.133 | 0.263 | 0.224 |
| Fish, mackerel, Atlantic, cooked, dry heat | 0.699 | 0.504 | 1.203 | 1.023 |
| Fish, mackerel, king, cooked, dry heat | 0.227 | 0.174 | 0.401 | 0.341 |
| Fish, mackerel, Pacific and jack, mixed species, cooked, dry heat | 1.195 | 0.653 | 1.848 | 1.571 |
| Fish, mackerel, Spanish, cooked, dry heat | 0.952 | 0.294 | 1.246 | 1.059 |
| Fish, mullet, striped, cooked, dry heat | 0.148 | 0.18 | 0.328 | 0.279 |
| Fish, ocean perch, Atlantic, cooked, dry heat | 0.271 | 0.103 | 0.374 | 0.318 |
| Fish, perch, mixed species, cooked, dry heat | 0.223 | 0.101 | 0.324 | 0.275 |
| Fish, pike, northern, cooked, dry heat | 0.095 | 0.042 | 0.137 | 0.116 |
| Fish, pike, walleye, cooked, dry heat | 0.288 | 0.11 | 0.398 | 0.338 |
| Fish, pollock, Atlantic, cooked, dry heat | 0.451 | 0.091 | 0.542 | 0.461 |
| Fish, pompano, Florida, cooked, dry heat | ?? | ?? | ?? | 0.620 est |
| Fish, rockfish, Pacific, mixed species, cooked, dry heat | 0.262 | 0.181 | 0.443 | 0.377 |
| Fish, roe, mixed species, cooked, dry heat | 1.747 | 1.26 | 3.007 | 2.556 |
| Fish, roe, mixed species, raw | 1.363 | 0.983 | 2.346 | 1.994 |
| Fish, roughy, orange, raw | 0 | 0.001 | 0.001 | 0.001 |
| Fish, sablefish, cooked, dry heat | 0.920 | 0.867 | 1.787 | 1.519 |
| Fish, sablefish, smoked | 0.945 | 0.891 | 1.836 | 1.561 |
| Fish, salmon, Atlantic, farmed, cooked, dry heat | 1.457 | 0.69 | 2.147 | 1.825 |
| Fish, salmon, Atlantic, wild, cooked, dry heat | 1.429 | 0.411 | 1.84 | 1.564 |
| Fish, salmon, Chinook, cooked, dry heat | 0.727 | 1.01 | 1.737 | 1.476 |
| Fish, salmon, chum, cooked, dry heat | 0.505 | 0.299 | 0.804 | 0.683 |
| Fish, salmon, chum, drained solids with bone | 0.702 | 0.473 | 1.175 | 0.999 |
| Fish, salmon, coho, farmed, cooked, dry heat | 0.871 | 0.408 | 1.279 | 1.087 |
| Fish, salmon, coho, wild, cooked, dry heat | 0.658 | 0.401 | 1.059 | 0.900 |
| Fish, salmon, pink, cooked, dry heat | 0.751 | 0.537 | 1.288 | 1.095 |
| Fish, salmon, sockeye, cooked, dry heat | 0.700 | 0.53 | 1.23 | 1.046 |
| Fish, sardine, Atlantic, canned in oil, drained solids with bone | 0.509 | 0.473 | 0.982 | 0.835 |
| Fish, scup, raw (Porgy—assigned to low omega-3 group) | no data | no data | no data | no data |
| Fish, sea bass, mixed species, cooked, dry heat | 0.556 | 0.206 | 0.762 | 0.648 |
| Fish, sea trout, mixed species, cooked, dry heat | 0.265 | 0.211 | 0.476 | 0.405 |
| Fish, shad, American, raw | 1.321 | 1.086 | 2.407 | 2.046 |
| Fish, shark, mixed species, raw | 0.527 | 0.316 | 0.843 | 0.717 |
| Fish, sheepshead, cooked, dry heat | 0.107 | 0.083 | 0.19 | 0.162 |
| Fish, smelt, rainbow, cooked, dry heat | 0.536 | 0.353 | 0.889 | 0.756 |
| Fish, snapper, mixed species, cooked, dry heat | 0.273 | 0.048 | 0.321 | 0.273 |
| Fish, spot, cooked, dry heat | 0.526 | 0.282 | 0.808 | 0.687 |
| Fish, sturgeon, mixed species, cooked, dry heat | 0.119 | 0.249 | 0.368 | 0.313 |
| Fish, sucker, white, cooked, dry heat | 0.371 | 0.244 | 0.615 | 0.523 |
| Fish, sunfish, pumpkin seed, cooked, dry heat | 0.092 | 0.047 | 0.139 | 0.118 |
| Fish, swordfish, cooked, dry heat | 0.681 | 0.138 | 0.819 | 0.696 |
| Fish, tilefish, cooked, dry heat | 0.733 | 0.172 | 0.905 | 0.769 |
| Fish, trout, mixed species, cooked, dry heat | 0.677 | 0.259 | 0.936 | 0.796 |
| Fish, trout, rainbow, farmed, cooked, dry heat | 0.820 | 0.334 | 1.154 | 0.981 |
| Fish, trout, rainbow, wild, cooked, dry heat | 0.520 | 0.468 | 0.988 | 0.840 |
| Fish, tuna, fresh, bluefin, cooked, dry heat | 1.141 | 0.363 | 1.504 | 1.278 |
| Fish, tuna, light, canned in oil, drained solids | 0.101 | 0.027 | 0.128 | 0.109 |
| Fish, tuna, light, canned in water, drained solids | 0.223 | 0.047 | 0.27 | 0.230 |
| Fish, tuna, skipjack, fresh, cooked, dry heat | 0.237 | 0.091 | 0.328 | 0.279 |
| Fish, tuna, white, canned in water, drained solids | 0.629 | 0.233 | 0.862 | 0.733 |
| Fish, tuna, yellowfin, fresh, cooked, dry heat | 0.232 | 0.047 | 0.279 | 0.237 |
| Fish, whitefish, mixed species, cooked, dry heat | 1.206 | 0.406 | 1.612 | 1.370 |
| Fish, whiting, mixed species, cooked, dry heat | 0.235 | 0.283 | 0.518 | 0.440 |
| Fish, wolffish, Atlantic, cooked, dry heat | 0.405 | 0.393 | 0.798 | 0.678 |
| Frog legs, raw | 0.034 | 0.020 | ||
| Mollusks, abalone, mixed species, raw | 0 | 0.049 | 0.049 | 0.042 |
| Mollusks, clam, mixed species, cooked, moist heat | 0.146 | 0.138 | 0.284 | 0.241 |
| Mollusks, conch, baked or broiled | 0.072 | 0.048 | 0.12 | 0.102 |
| Mollusks, cuttlefish, mixed species, cooked, moist heat | 0.132 | 0.078 | 0.21 | 0.179 |
| Mollusks, mussel, blue, cooked, moist heat | 0.506 | 0.276 | 0.782 | 0.665 |
| Mollusks, octopus, common, cooked, moist heat | 0.162 | 0.152 | 0.314 | 0.267 |
| Mollusks, oyster, eastern, farmed, cooked, dry heat | 0.211 | 0.229 | 0.44 | 0.374 |
| Mollusks, oyster, eastern, wild, cooked, dry heat | 0.291 | 0.26 | 0.551 | 0.468 |
| Mollusks, oyster, Pacific, cooked, moist heat | 0.500 | 0.876 | 1.376 | 1.170 |
| Mollusks, scallop, mixed species, cooked, breaded and fried | 0.103 | 0.086 | 0.18 | 0.161 |
| Mollusks, whelk, unspecified, cooked, moist heat | 0.012 | 0.008 | 0.02 | 0.017 |
Table 4. Other sources of Omega-3 Alpha-Linolenic Acid (ALA) – Non-Seafood Sources
| Source of ALA | ALA content, g |
|---|---|
| Pumpkin seeds (1 tbsp) | 0.051 |
| Olive oil (1 tbsp) | 0.103 |
| Walnuts, black (1 tbsp) | 0.156 |
| Soybean oil (1 tbsp) | 1.231 |
| Rapeseed oil (1 tbsp) | 1.302 |
| Walnut oil (1 tbsp) | 1.414 |
| Flaxseeds (1 tbsp) | 2.350 |
| Walnuts, English (1 tbsp) | 2.574 |
| Flaxseed oil (1 tbsp) | 7.249 |
| Almonds (100 g) | 0.4 |
| Peanuts (100 g) | 0.003 |
| Beans, navy, sprouted (100 g) | 0.3 |
| Broccoli, raw (100 g) | 0.1 |
| Lettuce, red leaf (100 g) | 0.1 |
| Mustard (100 g) | 0.1 |
| Purslane (100 g) | 0.4 |
| Spinach (100 g) | 0.1 |
| Seaweed, spirulina, dried (100 g) | 0.8 |
| Beans, common, dry (100 g) | 0.6 |
| Chickpeas, dry (100 g) | 0.1 |
| Soybeans, dry (100 g) | 1.6 |
| Oats, germ (100 g) | 1.4 |
| Rice, bran (100 g) | 0.2 |
| Wheat, germ (100 g) | 0.7 |
| Avocados, California, raw (100 g) | 0.1 |
| Raspberries, raw (100 g) | 0.1 |
| Strawberries, raw (100 g) | 0.1 |
| Novel sources of ALA | ALA content, g |
| Breads and pasta (100 g) | 0.1–1.6 |
| Cereals (and granola bars) (55 g) | 1.0–4.9 |
| Eggs (50 g or 1 egg) | 0.1–0.6 |
| Processed meats (100 g) | 0.5 |
| Salad dressing (14 g – 31 g) | 2.0–4.0 |
| Margarine spreads (10 g – 100 g) | 0.3–1.0 |
| Nutrition bars (50 g) | 0.1–2.2 |
Note: 1 tablespoon (tbsp) oil = 13.6 g; 1 tbsp seeds or nuts = 12.35 g.
Supplements that contain Omega-3s
- Several types of dietary supplements contain omega-3s.
- Fish oil supplements contain EPA and DHA.
- Fish liver oil supplements, such as cod liver oil, contain EPA and DHA, and they also contain vitamins A and D, in amounts that vary from product to product. Vitamins A and D can be harmful in excessive amounts.
- Krill oil contains EPA and DHA.
- Algal oils are a vegetarian source of DHA; some also contain EPA.
- Flaxseed oil contains ALA.
What do scientists know about the effectiveness of omega-3 supplements?
- Research indicates that omega-3 supplements don’t reduce the risk of heart disease. However, people who eat seafood one to four times a week are less likely to die of heart disease.
- High doses of omega-3s can reduce levels of triglycerides.
- Omega-3 supplements may help relieve symptoms of rheumatoid arthritis.
- Omega-3 supplements have not been convincingly shown to slow the progression of the eye disease age-related macular degeneration.
- For most other conditions for which omega-3 supplements have been studied, the evidence is inconclusive or doesn’t indicate that omega-3s are beneficial.
Conditions Affecting the Circulatory System
Heart Disease
- A 2011 evaluation of 17 studies indicated that people who eat seafood (fish and shellfish) one to four times a week are less likely to die of heart disease than those who rarely or never eat seafood.
- A 2018 analysis of 10 major omega-3 supplementation studies (77,917 total participants, all at high risk of heart disease), each of which involved at least 500 participants and a treatment duration of at least a year, found no evidence that omega-3s could reduce the risk of fatal or nonfatal coronary heart disease.
- In 2016, the U.S. Government’s Agency for Healthcare Research and Quality 22 did a comprehensive evaluation of 98 studies of omega-3s and heart disease, including both diet and supplementation studies. They did not find evidence that omega-3s can reduce the risk of heart attacks or death from heart disease.
- Several other analyses of the evidence have been done in the last few years (2012 or later), and like the 2018 analysis and the AHRQ report 22, most found little or no evidence for a protective effect of omega-3 supplements against heart disease. However, some earlier analyses suggested that omega-3s could be helpful. The difference between the newer conclusions and the older ones may reflect two changes over time:
- Public health messages that urge people to eat more seafood may have led to greater consumption of omega-3s from food. Additional omega-3s, beyond the amounts consumed by people who eat seafood, may not have extra benefits.
- More people are taking medicines that reduce the risk of heart attacks, such as statin drugs to treat high cholesterol. Omega-3s may not offer extra benefits beyond those of modern drug treatment.
Stroke
- Eating seafood (fish and shellfish) has been linked to a moderate reduction in the risk of stroke.
- According to the Agency for Healthcare Research and Quality 22 report, there is some evidence that omega-3s from marine sources (such as fish oil) may reduce the risk of one type of stroke (ischemic stroke—the type caused by narrowing or blockage of a blood vessel in the brain), but omega-3s have not been shown to reduce total strokes or death from stroke.
Triglycerides
- Triglycerides are a type of fat found in people’s blood. Excessive levels of triglycerides may raise the risk of heart disease. Dietary changes, weight control, and exercise are used to lower triglyceride levels. Some people also need to take medicine to lower their triglyceride levels.
- High doses of omega-3 fatty acids can reduce triglyceride levels.
- Several products containing omega-3s have been approved as prescription drugs to be used in combination with diet to reduce triglyceride levels in patients whose triglyceride levels are very high.
- The composition of these products is not the same as that of typical omega-3 supplements, and the testing and regulation of prescription drugs differ from those for dietary supplements. Therefore, the effects of these prescription products may not be the same as those of omega-3 dietary supplements.
Conditions Affecting the Brain, Nervous System, or Mental Health
Depression
- It’s uncertain whether omega-3 fatty acid supplements are helpful for depression. Although some studies have had promising results, a 2015 evaluation of 26 studies that included more than 1,400 people concluded that if there is an effect, it may be too small to be meaningful. Other analyses have suggested that if omega-3s do have an effect, EPA may be more beneficial than DHA and that omega-3s may best be used in addition to antidepressant medication rather than in place of it.
- Omega-3s have not been shown to relieve symptoms of depression that occur during pregnancy or after childbirth.
- Depression can be a serious illness. If you or someone in your family may have depression, consult a health care provider.
Attention-Deficit Hyperactivity Disorder (ADHD)
- Research on omega-3s for ADHD has had conflicting results. It’s uncertain whether omega-3s have any benefit for symptoms of this condition.
Alzheimer’s Disease/Cognitive Impairment
- Some research indicates that people who eat more seafood may have a reduced risk of cognitive decline. However, omega-3 supplements haven’t been shown to help prevent cognitive impairment or Alzheimer’s disease or to improve symptoms of these conditions. For example, a large NIH-sponsored study completed in 2015 indicated that taking EPA and DHA supplements did not slow cognitive decline in older adults. The people studied were participants in a larger eye disease study, and all of them had age-related macular degeneration (AMD).
- It’s possible that omega-3s might have different effects in people with different genetic backgrounds. A 2017 research review suggested that people who carry a gene called APOE4, which is associated with an increased risk of Alzheimer’s disease, might benefit from taking DHA before developing signs of Alzheimer’s.
Other Conditions Affecting the Brain, Nervous System, or Mental Health
- Omega-3s have also been studied for autism spectrum disorders, borderline personality disorder, multiple sclerosis, and schizophrenia, but the evidence regarding their effects on these conditions is inconclusive.
Eye Diseases
Age-Related Macular Degeneration
- Age-related macular degeneration (AMD) is an eye disease that can cause vision loss in older people. Two major National Institutes of Health (NIH)-sponsored studies, called Age-Related Eye Disease Study (AREDS) and Age-Related Eye Disease Study 2 (AREDS2), showed that dietary supplements containing specific combinations of vitamins, antioxidants, and zinc helped slow the progression of AMD in people who were at high risk of developing the advanced stage of this disease. AREDS2, which had more than 4,000 participants and was completed in 2013, also tested EPA and DHA. The results showed that adding these omega-3s to the supplement formulation didn’t provide any additional benefits. Other, smaller studies of omega-3 supplements also haven’t shown them to have a beneficial effect on the progression of AMD.
Dry Eye Disease
- The results of several small studies had suggested that taking omega-3 supplements might help relieve symptoms of dry eye disease. However, a 2018 NIH-sponsored study that tested omega-3 supplements for a full year in a larger group (535 study participants) with moderate-to-severe dry eye disease found that the supplements were no more helpful than a placebo (an inactive substance).
Retinitis Pigmentosa
- Only a few studies have been conducted on omega-3s for retinitis pigmentosa, and these studies have not shown any clear evidence of beneficial effects.
Other Conditions
Rheumatoid Arthritis
- The types of omega-3s found in seafood and fish oil may be modestly helpful in relieving symptoms of rheumatoid arthritis and decreasing patients’ need for nonsteroidal anti-inflammatory drugs.
- Conventional medical treatment for rheumatoid arthritis can slow joint damage. If you have rheumatoid arthritis, don’t change your use of prescribed medications without consulting your health care provider.
Infant Development
- The nutritional value of seafood is important during early development. The Dietary Guidelines for Americans 2015–2020 and guidance from the U.S. Food and Drug Administration and Environmental Protection Agency recommend that women who are pregnant or breastfeeding eat at least 8 ounces but no more than 12 ounces of a variety of seafood each week, from choices that are lower in methyl mercury. Methyl mercury can be harmful to the brain and nervous system if a person is exposed to too much of it.
- In 2016, Agency for Healthcare Research and Quality 22 reviewed 143 studies that evaluated the effects of giving omega-3 supplements to pregnant or breastfeeding women or giving formulas with added DHA to infants. They found that when women took omega-3 supplements during pregnancy, their babies’ birth weight was slightly higher, but the risk of an undesirably low birth weight did not change. Also, when women took omega-3 supplements during pregnancy, their pregnancies lasted a little longer, but there was no effect on the risk of premature birth. Omega-3s were not found to have effects on any other aspects of the mothers’ or infants’ health or the infants’ long-term development. Aspects of the infants’ health that were not shown to be affected by omega-3s include growth after birth, visual acuity, long-term neurological and cognitive development, and the risks of autism, ADHD, learning disorders, and allergies.
- In a study published after the Agency for Healthcare Research and Quality report 22, scientists in Denmark gave high-dose fish oil supplements or placebos to 736 pregnant women during the third trimester of pregnancy. Children born to mothers who had taken fish oil were less likely to develop asthma or persistent wheezing in early childhood, and this was most noticeable in children whose mothers had low blood levels of EPA and DHA before they started to take the supplements. However, other studies that evaluated the effects of omega-3 supplementation during pregnancy on childhood asthma risk have had inconsistent results.
Miscellaneous Conditions
- Omega-3s have been studied for other conditions, with either inconclusive or negative results. These conditions include allergies, atopic eczema (an allergic skin condition), cystic fibrosis, diabetes, inflammatory bowel diseases (Crohn’s disease or ulcerative colitis), intermittent claudication (a circulatory problem), nonalcoholic fatty liver disease, and osteoporosis.
What do scientists know about the safety of omega-3 supplements?
- Omega-3s usually produce only mild side effects, if any. Side effects of omega-3 supplements are usually mild. They include unpleasant taste, bad breath, bad-smelling sweat, headache, and gastrointestinal symptoms such as heartburn, nausea, and diarrhea.
- Several large studies have linked higher blood levels of long-chain omega-3s with higher risks of prostate cancer. However, other research has shown that men who frequently eat seafood have lower prostate cancer death rates and that dietary intakes of long-chain omega-3s aren’t associated with prostate cancer risk. The reason for these apparently conflicting findings is unclear.
- Omega-3 supplements may interact with drugs that affect blood clotting.
- It’s uncertain whether people with seafood allergies can safely take fish oil supplements. If you’re taking medicine that affects blood clotting or if you’re allergic to fish or shellfish, consult your health care provider before taking omega-3 supplements.
In general taking fish oil supplement is quite safe. Commonly reported side effects of omega-3 supplements are usually mild. These include unpleasant taste, bad breath, heartburn, nausea, gastrointestinal discomfort, diarrhea, headache, and odoriferous sweat 23, 24.
Common gastrointestinal symptoms like nausea occurred at rates of ≈4% at dosages <3 g/d and increased to ≈20% at a dosage of 4 g/d.
The Institute of Medicine did not establish a UL for any omega-3s, although it noted that high doses of DHA and/or EPA (900 mg/day of EPA plus 600 mg/day DHA or more for several weeks) might reduce immune function due to suppression of inflammatory responses. Doses of 2–15 g/day EPA and/or DHA might also increase bleeding time by reducing platelet aggregation 19. However, according to the European Food Safety Authority, long-term consumption of EPA and DHA supplements at combined doses of up to about 5 g/day appears to be safe 25. It noted that these doses have not been shown to cause bleeding problems or affect immune function, glucose homeostasis, or lipid peroxidation. The FDA recommends not exceeding 3 g/day EPA and DHA combined, with up to 2 g/day from dietary supplements. Some doses used in clinical trials exceed these levels.
Omega-3 supplements may extend bleeding time (the time it takes for a cut to stop bleeding). People who take drugs that affect bleeding time, such as anticoagulants (“blood thinners”) or nonsteroidal anti-inflammatory drugs (NSAIDs), should discuss the use of omega-3 fatty acid supplements with a health care provider.
Krill oil benefits
Most of krill oil’s health benefits are attributed to its high Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) content. Numerous studies have identified the antithrombotic, antiarrhythmic, antiatherosclerotic, and anti-inflammatory mechanisms associated with an increased consumption of these omega-3 fatty acids 26, 27, 28.
More studies are needed to determine whether phosphatidylcholine and astaxanthin provide an additive effect.
Phosphatidylcholine by itself has shown promise as a dietary supplement to improve homocysteine status, liver disorders, and respiratory distress 29.
Astaxanthin may have independent positive effects due to its antioxidant capabilities. When oxygen radical absorptive capacity values of various antioxidants were compared, astaxanthin was found to be 34-times more effective than CoQ10 and 48-times more effective than fish oil 30.
Preliminary human studies indicate krill oil may be superior to fish oil in the reduction of premenstrual syndrome (PMS) complications 31 and biomarkers of dyslipidemia 32.
Krill oil consumption has also shown a positive effect on markers of inflammation 33.
Is krill oil better than fish oil?
Although there are similarities, numerous differences exist between krill oil and fish oil. Krill oil is only available as a supplement, primarily in softgel formulation 34. The size of krill oil softgels is markedly smaller and may be more suitable for individuals with swallowing difficulties. On the other hand, fish oil is available in both prescription and supplement formulations including softgels and liquid 34. More important, however, are the differences in omega-3 content and delivery 1. The EPA+DHA content of krill oil is markedly less per softgel (and serving) compared to fish oil. For example, the dose of EPA+DHA of pure krill oil products may range from ~45 to 200 mg/softgel compared to ~300 to 2,250 mg/softgel or teaspoon among the various fish oil formulations 35, 36, 37.
Fish oil is a type of polyunsaturated fatty acids that is derived from fish and contain a rich source of Omega-3 essential fatty acids that are important for a number of functions in your body. Fish oil is commonly found in fatty fish such as salmon, tuna, and trout—and shellfish—such as crab, mussels, and oysters. Omega-3 fatty acids are called essential fatty acids because your body cannot make them and you need it them in your diet.
Both fish oil and krill oil are a source of omega-3 fatty acids, predominantly Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA). Harvesting of both fish and krill for their respective oils has an impact on our environment, and most human studies have failed to show significant health benefits. Krill oil is inherently more stable than fish oil, and lacks a fishy smell and taste. Krill oil appears to be better absorbed than fish oil, but more studies are needed to determine whether this translates into any further health benefits. The best way to improve your omega-3 intake is to eat fish at least twice a week, as recommended by the American Heart Association (who notably prefer increasing dietary intake of fish over supplements) 38.
The fatty acid form is also a key factor differentiating these agents. The Eicosapentaenoic acid (EPA) + Docosahexaenoic acid (DHA) found in krill oil is primarily incorporated in phospholipids, whereas omega-3 fatty acids in fish oil are generally present as triglycerides or ethyl esters 39. Some data have suggested that phospholipids are more efficient at delivering EPA+DHA 40. This difference in chemical form may therefore impact the absorption and bioavailability of the Eicosapentaenoic acid (EPA) + Docosahexaenoic acid (DHA) and the dose required to achieve the various cardiovascular effects.
Although a limited number of studies comparing the effects of krill oil and fish oil on the omega-3 index have suggested greater increases with krill oil 41, 42 newer data do not support these findings 43.
Unlike fish oil, krill oil also contain a potent antioxidant carotenoid, astaxanthin, that helps prevent long-chain polyunsaturated fatty acids oxidation 32. This colorful carotenoid antioxidant, astaxanthin is responsible for the red color observed in salmon meat, cooked shellfish, and certain krill oil supplements. Although this powerful antioxidant has previously demonstrated HDL “good” cholesterol increasing properties, clinical benefits and therapeutic use of astaxanthin remain unclear 44.
Cost may also be an important consideration for patients choosing omega-3 products. Typically, supplemental fish oil is considerably less expensive compared to krill oil. A cost analysis of common products indicated that fish oil supplements range from 1 to 15 cents while krill oil is approximately 30 cents per 100 mg of EPA+DHA 35.
Krill Oil vs Fish Oil on Cholesterol
Very few randomized studies have examined the effects of krill oil on cardiovascular health or hyperlipidemia. Researchers in Quebec compared Neptune Krill Oil (NKO®) with high EPA and DHA fish oil (3:2 ratio) or placebo in a 12-week, prospective, randomized, double-blind clinical trial 32. 120 participants ages 25-75, with moderate-to-high cholesterol (193.9-347.9 mg/dL) and triglycerides (203.8-354.4 mg/dL) for a minimum of six months, were divided into four groups.
- Group 1 received 2 or 3 gram Neptune Krill Oil daily, depending on body mass index (BMI).
- Group 2 received 1 or 1.5 g Neptune Krill Oil daily(depending on BMI) during the 12 weeks of the study and an additional 500 mg Neptune Krill Oil as a maintenance dose for a 90 day follow-up period. In bothgroups a BMI >30 justified the higher of the two doses.
- Group 3 received 3 g Fish Oil (180 mg EPA, 120 mg DHA per g) daily, while
- Group 4 received aplacebo.
Parameters examined at baseline, 30, and 90 days (180 days for the follow-up in group 2) included HDL (good cholesterol), LDL (bad cholesterol) and total cholesterol, blood glucose, and triglycerides. At the end of 90 days those taking krill oil at a daily dose of 1 g, 1.5 g, 2 g, or 3 g achieved significant reductions of LDL of 32 %, 36 %, 37% and 39 percent, respectively. Reductions in total cholesterol were 13.4%, 13.7%, 18.1% and 18 percent, respectively, while triglyceride reductions were 11.03%, 11.89%, 27.62%, and 26.51 percent respectively. Blood glucose was reduced 6.3 percent in the 1-g and 1.5-g krill group, and 5.6 percent in those taking 2 or 3 g krill daily.
In comparison, the fish oil group had an average 5.9% reduction in cholesterol and the placebo group had a 9.1-percent increase. Subjects taking the fish oil also had a non-significant 4.6-percent decrease in LDL cholesterol.
Those receiving the placebo had a significant 13% increase in LDL cholesterol. There was a non-significant decrease in glucose and triglycerides for both the 3 g fish oil and placebo groups.
The largest changes in serum lipids occurred for HDL cholesterol. After 90 days, the 1, 1.5, 2, and 3 g krill oil groups had significant HDL “good” increases of 44%, 43%, 55% and 59 percent, while the fish oil group had only a 4.2% increase; the placebo group had a non-significant decrease of HDL.
During the 12-week follow-up, when subjects in the 1- and 1.5-g krill group were maintained on 500 mg krill oil daily, all markers maintained statistical significance except glucose 32.
While the findings for krill oil were impressive, the magnitude of the changes in lipid measures was considerably higher than what one might expect. Additionally, comparison is limited by the fact that the EPA and DHA content of the krill oil supplements was not provided. Thus these findings require further validation.
Another open-label randomized parallel study 42 examined the comparative effects of krill oil and fish oil in 122 participants documented to have no other routine sources of omega-3s. Participants were randomized to 1 of 3 groups: krill oil 3 g daily, fish oil 1.8 g daily, or no supplementation for 7 weeks. A total of 115 participants finished the study. The krill oil used in this study was extracted from Antarctic krill. The daily dose was 6 capsules, each containing 500 mg of oil providing 90.5 mg EPA + DHA and 103.5 mg of omega-3 polyunsaturated fatty acids (PUFAs). The omega-3 fish oil source was a Norway product given in a daily dose of 3 capsules containing 600 mg each of fish oil with 288 mg EPA + DHA and 330 mg of omega-3 PUFAs. In total, the daily amount of krill oil was approximately 63% of the dosage contained in the fish oil 42.
Blood samples were taken after an overnight fast of at least 12 hours at baseline and at the final visit. Plasma levels of EPA, DHA, and docosapentaenoic acid (DPA) increased significantly during the intervention in both the krill oil and fish oil groups compared to control. During the intervention phase, small changes were seen in levels of HDL “good” cholesterol, LDL “bad” cholesterol, and triglycerides. However, the only significant change was the increase in LDL-Cholesterol within the fish oil group. No differences were seen in the HDL-C / triglyceride ratio within the fish oil or control groups. Conversely, the ratio was significantly increased in the krill oil group. Changes in apolipoprotein B (Apo B-100) were minor and nonsignificant for all study groups. Only the within change in Apo B-100 levels for the krill oil group was significant. In addition, no significant increases were seen among the 3 groups in markers for inflammation, hemostasis, or oxidative stress. Withdrawal rates were similar among the 3 groups. The comparable increases in EPA and DHA among the krill oil users despite a lower dose of omega-3 PUFAs compared to the fish oil group are consistent with earlier studies suggesting that krill oil is a more bioavailable source of omega-3 PUFAs 42.
Another study specifically addressed the impact of krill oil on serum triglycerides and the omega-3 index 45. In a double-blind, randomized, placebo-controlled trial, 300 patients with triglyceride levels of 150 to 499 mg/dL were given varying doses of krill oil (0.5, 1, 2, or 4 g per day) or olive oil (placebo) for 12 weeks. These amounts of krill oil corresponded to 100, 200, 400, or 800 mg of EPA+DHA per day. Participants reported low consumption of fatty fish defined as less than twice per month. Fasting triglyceride levels were measured at baseline, 6, and 12 weeks. Compared to placebo, patients on krill oil demonstrated a 10.2% reduction in triglyceride levels 45. No differences in LDL-C levels were observed. Perhaps the most important finding from this study was the significant increase in the omega-3 index in all krill oil groups seen at both 6 and 12 weeks. The corresponding changes were 8%, 18%, 29%, and 73% for the 0.5, 1, 2, and 4 g krill oil dose compared to -3% (minus 3 percent) with placebo. A major limitation of this study is the high intra-individual variability that occurred in the fasting triglyceride measurements. Overall, the average daily dose of krill oil was 1.875 g providing 385 mg of EPA+DHA. This resulted in approximately a 6% reduction in triglyceride levels compared to baseline 45. This daily dose is lower than that used in earlier studies evaluating triglycerides. Additional studies with multiple measurements of triglyceride levels for each individual will be needed to confirm these findings.
The minimal number of clinical studies and substantial heterogeneity of designs preclude any definitive conclusions. Taken as a whole, however, these randomized trials provide preliminary evidence that krill oil is at least equivalent to and perhaps better than fish oil at increasing blood levels of EPA and DHA 46. However, it is not known whether these changes would translate into improved cardiovascular outcomes. Additional studies are needed to further explore the effects of krill oil on the lipid panel and, in particular, the potential impact on triglyceride reduction.
The American Heart Association position statement, published in 2002 47, does not recognize krill oil as an omega-3 supplement. This is understandable considering that the emergence of krill oil began after the American Heart Association recommendations. However, no other major position statements regarding cholesterol or cardiovascular risk prevention that have been published more recently address the appropriate use of krill oil, including the 2013 American College of Cardiology and the American Heart Association cholesterol guidelines 48. As such, krill oil should not be considered first-line therapy for omega-3 intake and cardioprotection. Additionally, krill oil does not appear to be effective for clinically relevant triglyceride lowering, because randomized controlled trials indicate only modest reductions 49. Therefore, krill oil cannot be recommended for hypertriglyceridemia at this time.
Because of these factors, krill oil currently has a limited role in cardiovascular risk prevention, with the potential to expand as more research is completed. Most studies evaluating the impact of krill oil on the omega-3 index indicate efficient absorption of EPA+DHA. The omega-3 index is reflective of the EPA+DHA consumption recommended by the American Heart Association and the potential for cardioprotection 50. Thus, it is reasonable to consider krill oil as an alternative for achieving cardiovascular benefits in patients who are unable to increase fish consumption or utilize fish oil. Specific patient groups that may be candidates for krill oil include those with an aversion to dietary fish and individuals unable to swallow the large fish oil softgels or who have a dislike for the liquid. If the efficient uptake of EPA+DHA from krill oil that has been observed in smaller studies is replicated in larger randomized controlled trials, patients may be able to obtain cardioprotection at a lower EPA+DHA intake than what is currently recommended by the American Heart Association. Additionally, krill is sensitive to degradation and the process for obtaining the key components is more complex than that of fish oil. In view of these issues, we emphasize the importance of getting your krill oil products only from reliable manufacturers.
Krill Oil and Osteoarthritis
A double-blind, placebo-controlled, randomized, prospective study examined the effect of 300 mg Neptune Krill Oil daily on C-reactive protein (CRP) and
functional testing scores for arthritis 33.
Ninety participants had a diagnosis of cardiovascular disease and/or rheumatoid arthritis and/or osteoarthritis, and an elevated CRP (>1.0 mg/dL) for three consecutive weeks. Western Ontario and McMaster Universities (WOMAC) osteoarthritis score and CRP were measured at baseline and at days 7, 14, and 30.
After seven days of krill supplementation, CRP decreased by 19.3 percent in the experimental group, while it increased by 15.7 percent in the control group. By day 14 and day 30, CRP decreased by 29.7 and 30.9 percent, respectively, in the krill oil group, while the placebo group experienced an increase of 32.1 percent by day 14 and a lowering to a total increase of 25.1 percent by day 30. When comparing krill supplementation to placebo, differences at day 7, day 14 and day 30 were all statistically significant. When compared to placebo, WOMAC osteoarthritis score results showed krill significantly reduced pain scores and stiffness scores and functional33.
Krill Oil vs Fish Oil on Premenstrual Syndrome
In a 90-day study, Sampalis et al. 31 compared the effects of Neptune Krill Oil to fish oil on multiple parameters of function in Premenstrual Syndrome (PMS) via an assessment questionnaire and the total consumption of analgesics for pain and discomfort associated with PMS.
Seventy subjects of child-bearing age were assigned to ingest 2 grams krill oil daily (800 mg phospholipids, 600 mg EPA and DHA) (n=36) or 2 grams fish oil daily (600 mg EPA and DHA at an 3:2 ratio) (n=34) for the first 30 days of the trial. In the final 60 days both groups were instructed to take the assigned supplements eight days prior to and two days during menstruation.
Questionnaires were completed and analgesic medication intakes were measured at baseline, 45, and 90 days.
After the first 45 days the krill oil group showed significant for all parameters improvements in breast tenderness, joint pain, weight gain, abdominal pain, swelling, and bloating, as well as feelings of being overwhelmed, stressed, irritable, and depressed. The fish oil group demonstrated significant improvements in weight gain and abdominal pain at day 45, and improvements in weight gain, abdominal pain, and swelling at day 90. When consumption of analgesic medication during menstruation by the krill oil group was compared to the fish oil group, it was found that the average consumption of 1.2 g ibuprofen or 2.5 g
acetaminophen taken at baseline changed in both groups. The krill oil group had reduced consumption to 0.9 g ibuprofen and 1.5 g acetaminophen at day 45, and 0.6 g ibuprofen and 1.0 g acetaminophen at day 9) – a total decrease in analgesics of 50 percent after 90 days. The fish oil group decreased intake to 0.9 g ibuprofen and 1.65 g acetaminophen by day 45, and 0.8 g ibuprofen and 1.48 g acetaminophen by day 90 – a total reduction of 33% and 41 percent, respectively.
Interestingly, the authors noted, “Patients taking NKO did not experience any gastrointestinal difficulties such as regurgitation, while 64 percent of the women in the fish oil group complained of unpleasant reflux” 31.
Krill Oil vs Fish Oil on Human Brain Function in Healthy Elderly Volunteers
Aging reduces regional cerebral blood flow, which causes deterioration of cerebral function 51. Aging has also been shown to reduce the level of dorsolateral prefrontal cortex activity during execution of working memory tasks 52.
In a study involving 45 healthy male subjects in their 60s and 70s who had retired from employment in the Japanese business sector 53. Eligibility for participation was as follows: right-handedness, not requiring prescription medication, no history of mental disorders or cerebrovascular disease, absence of serious liver, kidney, heart, respiratory, endocrine, or metabolic diseases, and absence of food allergies to fish or crustaceans. The participants were clinically confirmed by a psychiatrist to have no cognitive impairment.
Three types of experimental supplement were used: krill oil as a typical oil rich in PUFAs incorporated in phosphatidylcholine, sardine oil as a typical fish oil, and medium-chain triglycerides as placebo. Subjects were asked to take four capsules twice a day after breakfast and dinner for 12 weeks (eight capsules daily), from the day following the initial measurements to the day of the final measurements.
The results of this study suggest that long-term ingestion of krill oil and sardine oil promotes working memory function by activating the dorsolateral prefrontal cortex in elderly people, and thus prevents deterioration in cognitive activity 53. However, sardine oil, which contains the largest amounts of EPA and DHA fatty acids, was not shown to possess any activation effects regarding the calculation task, and only krill oil, containing lesser amounts of these fatty acids, was shown to have an effect, possibly due to its higher percentage of phospholipids, in particular phosphatidylcholine 53. This finding indicates that n-3 PUFAs incorporated in phosphatidylcholine act on brain function more efficiently than those incorporated in triglycerides 54.
Krill oil dosage
Therapeutic doses range from 1-3 grams krill oil per day, with maintenance dosing of 500 mg daily 3.
Always talk to your doctor before taking supplements of any kind, including omega-3’s, and particularly if you have a medical condition such as asthma, inflammatory bowel disease, liver disease or a heart rhythm disorder. Take a supplement from a reputable manufacturer with good quality control measures to ensure the supplement is as free from contaminants, including heavy metal toxins (such as mercury), as possible. Pregnant women and young children should be especially cautious about taking fish oil supplements.
A study specifically addressed the impact of krill oil on serum triglycerides and the omega-3 index 45. In a double-blind, randomized, placebo-controlled trial, 300 patients with triglyceride levels of 150 to 499 mg/dL were given varying doses of krill oil (0.5, 1, 2, or 4 g per day) or olive oil (placebo) for 12 weeks. These amounts of krill oil corresponded to 100, 200, 400, or 800 mg of EPA+DHA per day. Participants reported low consumption of fatty fish defined as less than twice per month. Fasting triglyceride levels were measured at baseline, 6, and 12 weeks. In an effort to increase statistical power, the final analyses pooled all krill oil patients regardless of dose. Compared to placebo, patients on krill oil demonstrated a 10.2% reduction in triglyceride levels. No differences in LDL-C “bad” cholesterol levels were observed. Perhaps the most important finding from this study was the significant increase in the omega-3 index in all krill oil groups seen at both 6 and 12 weeks. The corresponding changes were 8%, 18%, 29%, and 73% for the 0.5, 1, 2, and 4 g krill oil dose compared to -3% with placebo. A major limitation of this study is the high intra-individual variability that occurred in the fasting triglyceride measurements. Because this had not been taken into account in the power calculations, the investigators were forced to pool all of the krill oil users into one group despite varying doses. Overall, the average daily dose of krill oil was 1.875 g providing 385 mg of EPA+DHA 45. This resulted in approximately a 6% reduction in triglyceride levels compared to baseline. This daily dose is lower than that used in earlier studies evaluating triglycerides. Additional studies with multiple measurements of triglyceride levels for each individual will be needed to confirm these findings.
Usual Adult Dose for Hypertriglyceridemia
- 1 gram prescription only products:
- 4 grams orally daily; may be given as a single dose or 2 divided doses.
Comments:
- Assess triglyceride levels carefully before starting therapy and identify other possible causes (e.g. diabetes, hypothyroidism, medications) and manage appropriately.
- Patients should be on a lipid lowering diet prior to using this medication, and continue the diet during use of this medication.
- Capsules should be swallowed whole; do not break, crush, chew or dissolve capsules.
- In clinical trials, the medication was administered with meals.
Renal Dose Adjustments
- Data not available
Liver Dose Adjustments
- Data not available
Hemodialysis
- Data not available
Pregnancy
Pregnancy Category C: There are no adequate and well-controlled studies in pregnant women. It is unknown whether Omega-3-Acid Ethyl Esters capsules can cause fetal harm when administered to a pregnant woman or can affect reproductive capacity. Omega-3-Acid Ethyl Esters capsules should be used during pregnancy only if the potential benefit to the patient justifies the potential risk to the fetus.
Animal Data: Omega-3-Acid Ethyl Esters have been shown to have an embryocidal effect in pregnant rats when given in doses resulting in exposures 7 times the recommended human dose of 4 grams/day based on a body surface area comparison.
In female rats given oral gavage doses of 100, 600, and 2,000 mg/kg/day beginning 2 weeks prior to mating and continuing through gestation and lactation, no adverse effects were observed in the high dose group (5 times human systemic exposure following an oral dose of 4 grams/day based on body surface area comparison).
In pregnant rats given oral gavage doses of 1,000, 3,000, and 6,000 mg/kg/day from gestation day 6 through 15, no adverse effects were observed (14 times human systemic exposure following an oral dose of 4 grams/day based on a body surface area comparison).
In pregnant rats given oral gavage doses of 100, 600, and 2,000 mg/kg/day from gestation day 14 through lactation day 21, no adverse effects were seen at 2,000 mg/kg/day (5 times the human systemic exposure following an oral dose of 4 grams/day based on a body surface area comparison). However, decreased live births (20% reduction) and decreased survival to postnatal day 4 (40% reduction) were observed in a dose-ranging study using higher doses of 3,000 mg/kg/day (7 times the human systemic exposure following an oral dose of 4 grams/day based on a body surface area comparison).
In pregnant rabbits given oral gavage doses of 375, 750, and 1,500 mg/kg/day from gestation day 7 through 19, no findings were observed in the fetuses in groups given 375 mg/kg/day (2 times human systemic exposure following an oral dose of 4 grams/day based on a body surface area comparison). However, at higher doses, evidence of maternal toxicity was observed (4 times human systemic exposure following an oral dose of 4 grams/day based on a body surface area comparison).
Breastfeeding
Studies with Omega-3-Acid Ethyl Esters have demonstrated excretion in human milk. The effect of this excretion on the infant of a nursing mother is unknown; caution should be exercised when Omega-3-Acid Ethyl Esters capsules are administered to a nursing mother. An animal study in lactating rats given oral gavage 14C-ethyl EPA demonstrated that drug levels were 6 to 14 times higher in milk than in plasma.
Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
Geriatric Use
A limited number of subjects older than 65 years were enrolled in the clinical trials of Omega-3-Acid Ethyl Esters capsules. Safety and efficacy findings in subjects older than 60 years did not appear to differ from those of subjects younger than 60 years.
Krill oil side effects
There are currently no known toxicity levels for krill oil. Side effects associated with the consumption of krill oil may include an increase in gastrointestinal
complaints such as flatulence, gas, bloating, and/or diarrhea 6.
Commonly reported side effects of omega-3 supplements are usually mild. These include unpleasant taste, bad breath, heartburn, nausea, gastrointestinal discomfort, diarrhea, headache, and odoriferous sweat 55, 56.
Along with its needed effects, omega-3 polyunsaturated fatty acids may cause some unwanted effects. Although not all of these side effects may occur, if they do occur they may need medical attention.
Fish Allergy
Omega-3 capsules contains ethyl esters of omega-3 fatty acids (EPA and DHA) obtained from the oil of several fish sources. It is not known whether patients with allergies to fish and/or shellfish, are at increased risk of an allergic reaction to Omega-3-Acid Ethyl Esters capsules. Omega-3-Acid Ethyl Esters capsules should be used with caution in patients with known hypersensitivity to fish and/or shellfish.
Theoretically, people who are allergic to fish or shellfish should avoid fish oil or krill oil supplements. However, there has only been one documented case of an anaphylactic reaction to fish oil and none to krill oil, indicating that an allergy to supplements is extremely rare. Always speak to your doctor before taking supplements if you have a fish or shellfish allergy 57.
In general, omega-3 supplements (includes both fish and krill oil) may affect blood sugar levels, lower blood pressure, and increase the risk of bleeding, particularly at higher dosages or in those with bleeding disorders or already taking medications that increase the risk of bleeding (such as warfarin or aspirin). Higher dosages of fish oil may also lead to vitamin A or D toxicity. Cough, diarrhoea, nausea, and flatulence are common side effects associated with their use.
Recurrent Atrial Fibrillation (AF) or Flutter
In a double-blind, placebo-controlled trial of 663 subjects with symptomatic paroxysmal AF (n = 542) or persistent AF (n = 121), recurrent AF or flutter was observed in subjects randomized to Omega-3-Acid Ethyl Esters who received 8 grams/day for 7 days and 4 grams/day thereafter for 23 weeks at a higher rate relative to placebo. Subjects in this trial had median baseline triglycerides of 127 mg/dL, had no substantial structural heart disease, were taking no anti-arrhythmic therapy (rate control permitted), and were in normal sinus rhythm at baseline.
At 24 weeks, in the paroxysmal AF stratum, there were 129 (47%) first recurrent symptomatic AF or flutter events on placebo and 141 (53%) on Omega-3-Acid Ethyl Esters [primary endpoint, HR 1.19; 95% CI: 0.93, 1.35]. In the persistent AF stratum, there were 19 (35%) events on placebo and 34 (52%) events on Omega-3-Acid Ethyl Esters. Although the clinical significance of these results is uncertain, there is a possible association between Omega-3-Acid Ethyl Esters and more frequent recurrences of symptomatic atrial fibrillation or flutter in patients with paroxysmal or persistent atrial fibrillation, particularly within the first 2 to 3 months of initiating therapy.
Omega-3-Acid Ethyl Esters capsules are not indicated for the treatment of AF or flutter.
Check with your doctor immediately if any of the following side effects occur while taking omega-3 polyunsaturated fatty acids:
Incidence Not Known
- bleeding gums
- cough
- coughing up blood
- difficulty with breathing or swallowing
- dizziness
- fast or irregular heartbeat
- headache
- hives, itching, or skin rash
- increased menstrual flow or vaginal bleeding
- nosebleeds
- paralysis
- prolonged bleeding from cuts
- puffiness or swelling of the eyelids or around the eyes, face, lips, or tongue
- red or black, tarry stools
- red or dark brown urine
- sweating
- tightness in the chest
- unusual tiredness or weakness
Some side effects of omega-3 polyunsaturated fatty acids may occur that usually do not need medical attention. These side effects may go away during treatment as your body adjusts to the medicine. Also, your health care professional may be able to tell you about ways to prevent or reduce some of these side effects. Check with your health care professional if any of the following side effects continue or are bothersome or if you have any questions about them:
Less Common
- acid or sour stomach
- bad, unusual, or unpleasant (after) taste
- belching
- bloated or full feeling
- change in taste
- excess air or gas in the stomach
- heartburn
- indigestion
- stomach discomfort, upset, or pain
Incidence Not Known
- diarrhea
- difficulty having a bowel movement (stool)
- loss of appetite
- nausea or vomiting
- passing of gas
- stomach fullness
Gastrointestinal
Common (1% to 10%): Eructation, dyspepsia, nausea, gastrointestinal disorders (including abdominal distension, abdominal pain, constipation, diarrhea, flatulence, gastroesophageal reflux disease, vomiting)
Uncommon (0.1% to 1%): Gastrointestinal hemorrhage, gastroenteritis
Rare (less than 0.1%): Gastrointestinal pain
Very rare (less than 0.01%): Lower gastrointestinal hemorrhage
General
The most common adverse events were eructation, dyspepsia, and taste perversion
Other
Common (1% to 10%): Infection, pain
Uncommon (0.1% to 1%): Death
Dermatologic
Common (1% to 10%): Rash
Uncommon (0.1% to 1%): Atopic dermatitis
Rare (less than 0.1%): Urticaria, acne, rash pruritic
Frequency not reported: Pruritus
Cardiovascular
Uncommon (0.1% to 1%): Hypotension
Musculoskeletal
Common (1% to 10%): Back pain
Metabolic
Uncommon (0.1% to 1%): Hyperglycemia, gout, high triglycerides
Very rare (less than 0.01%): Blood lactate dehydrogenase increased
Nervous system
Common (1% to 10%): Taste perversion
Uncommon (0.1% to 1%): Dizziness, dysgeusia, headache, hyperactivity
Respiratory
Uncommon (0.1% to 1%): Epistaxis
Very rare (less than 0.01%): Nasal dryness
Frequency not reported: Influenza
Hypersensitivity
Rare (less than 0.1%): Hypersensitivity
Postmarketing reports: Anaphylactic reaction
Hematologic
Very rare (less than 0.01%): White blood count increased,
Frequency not reported: Slight prolongation of bleeding time
Postmarketing reports: Hemorrhagic diathesis
Psychiatric
Uncommon (0.1% to 1%): Tics, tantrum, insomnia
Hepatic
Rare (less than 0.1%): Liver disorders (including increased ALT, increased AST, and transaminases increased).
- A brief review of krill oil history, research, and the commercial market. Kwantes JM, Grundmann O. J Diet Suppl. 2015 Mar; 12(1):23-35. https://www.ncbi.nlm.nih.gov/pubmed/24689485/[↩][↩]
- Jenkins DJA, Josse AR. Fish oil and omega-3 fatty acids. CMAJ : Canadian Medical Association Journal. 2008;178(2):150. doi:10.1503/cmaj.071754. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2174990/[↩][↩]
- Altern Med Rev. 2010 Apr;15(1):84-6. Krill oil. Monograph. http://www.altmedrev.com/publications/15/1/84.pdf[↩][↩]
- Wijendran V, Huang MC, Diau GY, et al. Efficacy of dietary arachidonic acid provided as triglyceride or phospholipid as substrates for brain arachidonic acid accretion in baboon neonates. Pediatr Res 2002;51:265-272.[↩]
- Goustard-Langelier B, Guesnet P, Durand G, et al. n-3 and n-6 fatty acid enrichment by dietary fish oil and phospholipid sources in brain cortical areas and nonneural tissues of formula-fed piglets. Lipids 1999;34:5-16.[↩]
- Maki KC, Reeves MS, Farmer M, et al. Krill oil supplementation increases plasma concentrations of eicosapentaenoic and docosahexaenoic acids in overweight and obese men and women. Nutr Res 2009;29:609-615.[↩][↩]
- Dietary Guidelines for Americans. https://health.gov/dietaryguidelines[↩][↩]
- Fish and Omega-3 Fatty Acids. http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/HealthyDietGoals/Fish-and-Omega-3-Fatty-Acids_UCM_303248_Article.jsp[↩]
- U.S. Food and Drug Administration. Eating Fish: What Pregnant Women and Parents Should Know. https://www.fda.gov/downloads/Food/FoodborneIllnessContaminants/Metals/UCM536321.pdf[↩]
- Omega-3 fatty acid content of the US food supply. Raper NR, Cronin FJ, Exler J. J Am Coll Nutr. 1992 Jun; 11(3):304-8. https://www.ncbi.nlm.nih.gov/pubmed/1619182/[↩]
- Kris-Etherton PM, Taylor DS, Yu-Poth S, Huth P, Moriarty K, Fishell V, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr 2000;71(Suppl 1):179-88.[↩]
- Breast cancer risk in rats fed a diet high in n-6 polyunsaturated fatty acids during pregnancy. Hilakivi-Clarke L, Onojafe I, Raygada M, Cho E, Clarke R, Lippman ME. J Natl Cancer Inst. 1996 Dec 18; 88(24):1821-7. https://www.ncbi.nlm.nih.gov/pubmed/8961971/[↩]
- Linoleic acid intake and cancer risk: a review and meta-analysis. Zock PL, Katan MB. Am J Clin Nutr. 1998 Jul; 68(1):142-53. https://www.ncbi.nlm.nih.gov/pubmed/9665108/[↩]
- Salem N., Jr Introduction to polyunsaturated fatty acids. Backgrounder. 1999;3:1–8.[↩]
- Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Holub BJ. CMAJ. 2002 Mar 5; 166(5):608-15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩][↩]
- Simopoulos AP. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients. 2016;8(3):128. doi:10.3390/nu8030128. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4808858/[↩][↩][↩]
- Alpha-linolenic acid and cardiovascular diseases. Lanzmann-Petithory D. J Nutr Health Aging. 2001; 5(3):179-83. https://www.ncbi.nlm.nih.gov/pubmed/11458289/[↩]
- Holub BJ. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Hoffer LJ, Jones PJ, eds. CMAJ: Canadian Medical Association Journal. 2002;166(5):608-615. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩][↩]
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.[↩][↩][↩]
- EPA and DHA Content of Fish Species. https://health.gov/dietaryguidelines/dga2005/report/html/table_g2_adda2.htm[↩]
- Rodriguez-Leyva D, Bassett CM, McCullough R, Pierce GN. The cardiovascular effects of flaxseed and its omega-3 fatty acid, alpha-linolenic acid. The Canadian Journal of Cardiology. 2010;26(9):489-496. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2989356/[↩]
- Omega-3 Fatty Acids and Cardiovascular Disease: An Updated Systematic Review. https://effectivehealthcare.ahrq.gov/topics/fatty-acids-cardiovascular-disease/[↩][↩][↩][↩][↩]
- Mazereeuw G, Lanctot KL, Chau SA, Swardfager W, Herrmann N. Effects of omega-3 fatty acids on cognitive performance: a meta-analysis. Neurobiol Aging 2012;33:1482 e17-29. https://www.ncbi.nlm.nih.gov/pubmed/22305186?dopt=Abstract[↩]
- Lev-Tzion R, Griffiths AM, Leder O, Turner D. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2014;2:CD006320. https://www.ncbi.nlm.nih.gov/pubmed/24585498?dopt=Abstract[↩]
- EFSA Panel on Dietetic Products NaA. Scientific opinion on the tolerable upper intake level of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) and docosapentaenoic acid (DPA). EFSA Journal 2012;10:2815.[↩]
- Chang JP, Chen YT, Su KP. Omega-3 polyunsaturated fatty acids (n-3 PUFAs) in cardiovascular diseases (CVDs) and depression: the missing link? Cardiovasc Psychiatry Neurol 2009;2009:725310. Epub 2009 Sep 27.[↩]
- Breslow J. n-3 fatty acids and cardiovascular disease. Am J Clin Nutr 2006;83:1477S-1482S.[↩]
- Calzolari I, Fumagalli S, Marchionni N, Di Bari M. Polyunsaturated fatty acids and cardiovascular disease. Curr Pharm Des 2009;15:4094-4102.[↩]
- Phosphatidylcholine. Altern Med Rev 2002;7:150-154.[↩]
- Naguib YM. Antioxidant activities of astaxanthin and related carotenoids. J Agric Food Chem 2000;48:1150-1154.[↩]
- Sampalis F, Bunea R, Pelland MF, et al. Evaluation of the effects of Neptune Krill Oil on the management of premenstrual syndrome and dysmenorrhea. Altern Med Rev 2003;8:171-179.[↩][↩][↩]
- Bunea R, El Farrah K, Deutsch L. Evaluation of the effects of Neptune Krill Oil on the clinical course of hyperlipidemia. Altern Med Rev 2004:9:420-428.[↩][↩][↩][↩]
- Deutsch L. Evaluation of the effect of Neptune Krill Oil on chronic inflammation and arthritic symptoms. J Am Coll Nutr 2007:26:39-48.[↩][↩][↩]
- ConsumerLab Product Review: Fish oil and omega-3 fatty acid supplements (EPA and DHA from fish A, and krill). 2010. www.consumerlab.com/news/fish_oil_supplements_reviewed/9_28_2010/[↩][↩]
- ConsumerLab Product Review: Fish oil and omega-3 fatty acid supplements (EPA and DHA from fish A, and krill). 2010. https://www.consumerlab.com/news/fish_oil_supplements_reviewed/9_28_2010/[↩][↩]
- Nature Made Krill Oil 300 mg. Nature Made Web site. 2014. http://www.naturemade.com/fish-oil-and-omegas/krill-oil-300-mg[↩]
- MegaRed Ultra Strength Omega-3 Krill Oil. Schiff MegaRed Web site. 2014. http://www.megared.com/?uci=US-MG-O-PS-GA-10002&cid=cov395p6063g-c[↩]
- Fish and Omega-3 Fatty Acids. American Heart Association 06/2015 http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/Nutrition/Fish-and-Omega-3-Fatty-Acids_UCM_303248_Article.jsp#.Vw2hsDB96M8[↩]
- Krill for human consumption: nutritional value and potential health benefits. Tou JC, Jaczynski J, Chen YC. Nutr Rev. 2007 Feb; 65(2):63-77. https://www.ncbi.nlm.nih.gov/pubmed/17345959/[↩]
- Incorporation of EPA and DHA into plasma phospholipids in response to different omega-3 fatty acid formulations–a comparative bioavailability study of fish oil vs. krill oil. Schuchardt JP, Schneider I, Meyer H, Neubronner J, von Schacky C, Hahn A. Lipids Health Dis. 2011 Aug 22; 10():145. https://www.ncbi.nlm.nih.gov/pubmed/21854650/[↩]
- Maki KC, Reeves MS, Farmer M, et al. Krill oil supplementation increases plasma concentrations of eicosapentaenoic and docosahexaenoic acids in overweight and obese men and women. Nutr Res. 2009;9:609–615. https://www.ncbi.nlm.nih.gov/pubmed/19854375[↩]
- Ulven SM, Kirkhus B, Lamglait A, et al. Metabolic effects of krill oil are essentially similar to those of fish oil but at lower dose of EPA and DHA, in healthy volunteers. Lipids. 2011;46:37–46. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3024511/[↩][↩][↩][↩]
- Laidlaw M, Cockerline CA, Rowe WJ. A randomized clinical trial to determine the efficacy of manufacturers’ recommended doses of omega-3 fatty acids from different sources in facilitating cardiovascular disease risk reduction. Lipids Health Dis. 2014;13:99. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4085663/[↩]
- Administration of natural astaxanthin increases serum HDL-cholesterol and adiponectin in subjects with mild hyperlipidemia. Yoshida H, Yanai H, Ito K, Tomono Y, Koikeda T, Tsukahara H, Tada N. Atherosclerosis. 2010 Apr; 209(2):520-3. https://www.ncbi.nlm.nih.gov/pubmed/19892350/[↩]
- Berge K, Musa-Veloso K, Harwood M, Hoem N, Burri L. Krill oil supplementation lowers serum triglycerides without increasing low-density lipoprotein cholesterol in adults with borderline high or high triglyceride levels. Nutr Res. 2014;2:126–133. https://www.ncbi.nlm.nih.gov/pubmed/24461313[↩][↩][↩][↩][↩]
- Backes JM, Howard PA. Krill Oil for Cardiovascular Risk Prevention: Is It for Real? Hospital Pharmacy. 2014;49(10):907-912. doi:10.1310/hpj4910-907. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4252213/[↩]
- Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Kris-Etherton PM, Harris WS, Appel LJ, American Heart Association. Nutrition Committee. Circulation. 2002 Nov 19; 106(21):2747-57. http://circ.ahajournals.org/content/106/21/2747.long[↩]
- Circulation. 2014 Jun 24;129(25 Suppl 2):S1-45. doi: 10.1161/01.cir.0000437738.63853.7a. Epub 2013 Nov 12. 2013 American College of Cardiology and the American Heart Association guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. http://circ.ahajournals.org/content/129/25_suppl_2/S1.long[↩]
- Krill oil supplementation lowers serum triglycerides without increasing low-density lipoprotein cholesterol in adults with borderline high or high triglyceride levels. Berge K, Musa-Veloso K, Harwood M, Hoem N, Burri L. Nutr Res. 2014 Feb; 34(2):126-33. https://www.ncbi.nlm.nih.gov/pubmed/24461313/[↩]
- The omega-3 index as a risk factor for coronary heart disease. Harris WS. Am J Clin Nutr. 2008 Jun; 87(6):1997S-2002S. https://www.ncbi.nlm.nih.gov/pubmed/18541601/[↩]
- Decreases in regional cerebral blood flow with normal aging. Martin AJ, Friston KJ, Colebatch JG, Frackowiak RS. J Cereb Blood Flow Metab. 1991 Jul; 11(4):684-9. https://www.ncbi.nlm.nih.gov/pubmed/2050757/[↩]
- Context-dependent, neural system-specific neurophysiological concomitants of ageing: mapping PET correlates during cognitive activation. Esposito G, Kirkby BS, Van Horn JD, Ellmore TM, Berman KF. Brain. 1999 May; 122 ( Pt 5)():963-79. https://www.ncbi.nlm.nih.gov/pubmed/10355679/[↩]
- Konagai C, Yanagimoto K, Hayamizu K, Han L, Tsuji T, Koga Y. Effects of krill oil containing n-3 polyunsaturated fatty acids in phospholipid form on human brain function: a randomized controlled trial in healthy elderly volunteers. Clinical Interventions in Aging. 2013;8:1247-1257. doi:10.2147/CIA.S50349. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3789637/[↩][↩][↩]
- Correlation between changes in blood fatty acid composition and visual sustained attention performance in children with inattention: effect of dietary n-3 fatty acids containing phospholipids. Vaisman N, Kaysar N, Zaruk-Adasha Y, Pelled D, Brichon G, Zwingelstein G, Bodennec J. Am J Clin Nutr. 2008 May; 87(5):1170-80. https://www.ncbi.nlm.nih.gov/pubmed/18469236/[↩]
- Christen WG, Schaumberg DA, Glynn RJ, Buring JE. Dietary omega-3 fatty acid and fish intake and incident age-related macular degeneration in women. Arch Ophthalmol 2011;129:921-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3134638/[↩]
- Lev-Tzion R, Griffiths AM, Ledder O, Turner D. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn’s disease. Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD006320. DOI: 10.1002/14651858.CD006320.pub4. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD006320.pub4/full[↩]
- Fish-oil capsule ingestion A case of recurrent anaphylaxis: Canadian Family Physician July 2012 vol. 58 no. 7 e379-e381 http://www.cfp.ca/content/58/7/e379.full[↩]





{kind=link}