Contents
- Lactic acidosis
- Lactic acidosis symptoms
- Lactic acidosis causes
- Lactic acid blood test
- Lactic acid normal range
- Elevated lactic acid
- When is lactate test ordered?
- Why would a health practitioner choose to measure lactate in a blood sample from an artery rather than blood from a vein?
- Are there other ways to measure lactate than by sending a blood sample to the lab for testing?
- What is the lactate/pyruvate ratio and how is it used?
- Lactic acidosis treatment
Lactic acidosis
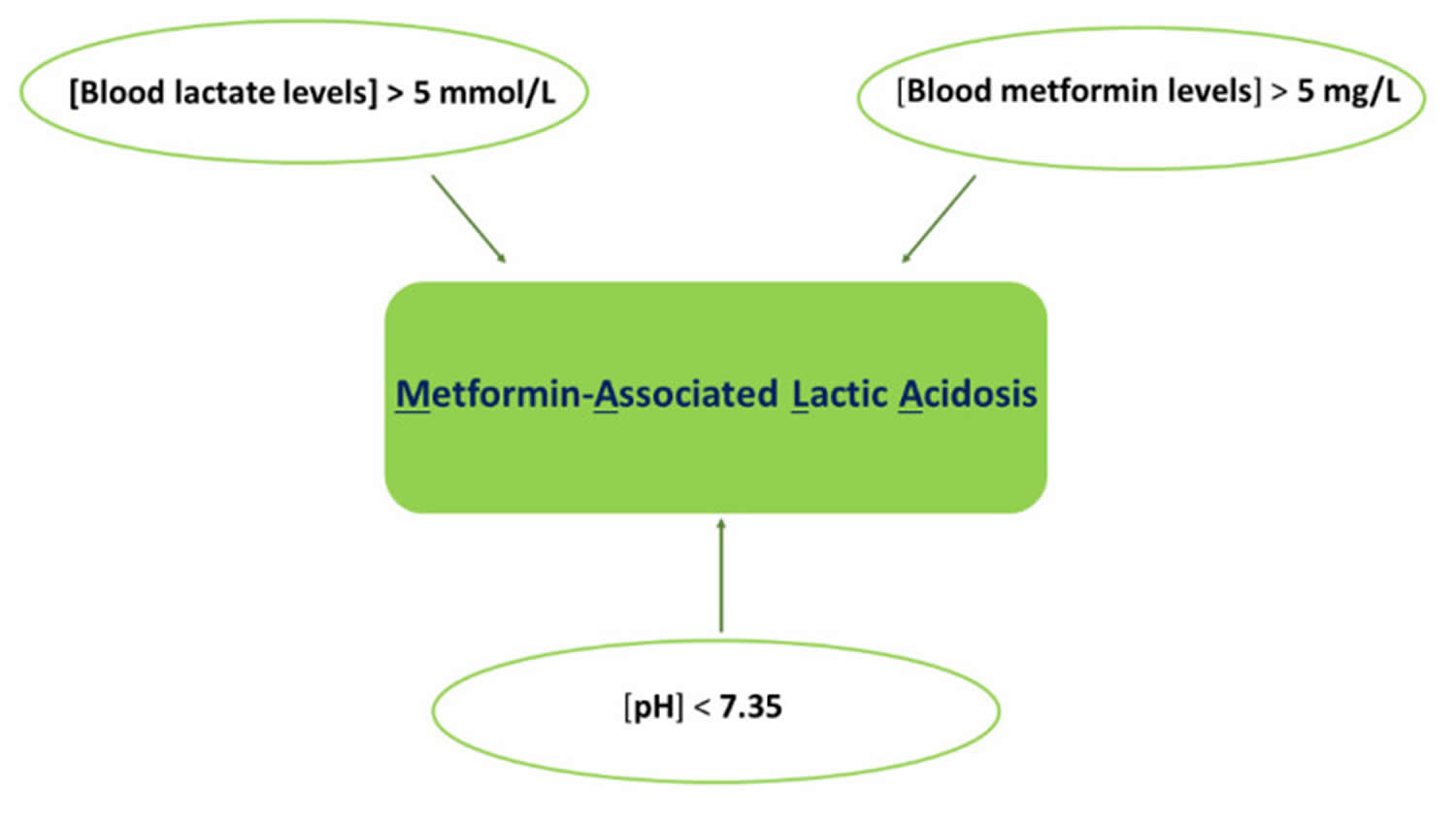
Lactic acidosis occurs when lactate production exceeds its metabolism in your body. Common criteria for the diagnosis of lactic acidosis include a plasma lactate concentration in excess of 5 mmol/L [normal range 0.5–2.2 mmol/L; (4.5–19.8 mg/dL)] and a blood pH lower than 7.35 (normal blood pH 7.35–7.45) 1, 2. These values are obtained through arterial blood gas analysis, and they can co-present with several clinical conditions such as alveolar gas exchange deficit, kidney injury, dehydration (vomiting and diarrhea), and sepsis 3.
Normal blood pH must be maintained within a narrow range of 7.35-7.45 to ensure the proper functioning of metabolic processes and for the delivery of the right amount of oxygen to tissues. Acidosis refers to an excess of acid in your blood that causes the pH to fall below 7.35. Many conditions and diseases can interfere with pH control in your body and cause a person’s blood pH to fall outside of healthy limits. Bicarbonate (HCO3–) functions as an alkalotic substance. Carbon dioxide (CO2) functions as an acidic substance. Therefore, a decrease in serum bicarbonate (HCO3–) or an increase in CO2 (carbon dioxide) will make blood more acidic. Carbon dioxide (CO2) levels are physiologically regulated by the pulmonary system through respiration, whereas the serum bicarbonate (HCO3–) levels are regulated through your kidneys with reabsorption rates. Acidosis may be caused by decreased carbon dioxide (CO2) elimination in respiratory disorders such as emphysema or by the loss of bicarbonate (HCO3–) in your body due to problems such as kidney disease and diabetes, or as the result of ingesting poisons (ethlylene glycol, methanol) or overdosing on certain medication (salicylates); it can also be caused by losing HCO3, as in diarrhea.
Lactate is produced by most tissues in the human body the end product of anaerobic carbohydrate metabolism and amino acid metabolism. Major sites of production are skeletal muscle, brain, and erythrocytes, with the highest level of production found in muscle 4. Lactate is also a natural component of very many foods, in particular fruits and fermented milk products. Under normal conditions, lactate is rapidly metabolized and cleared by the liver with a small amount of additional clearance by the kidneys 5. In aerobic conditions, pyruvate is produced via glycolysis and then enters the Krebs cycle, largely bypassing the production of lactate. Under anaerobic conditions, lactate is an end product of glycolysis and feeds into the Cori cycle as a substrate for gluconeogenesis (see Figure 1). Lactate exists in two isomers: L-lactate and D-lactate. Current lactate measurements only include L-lactate (the primary isomer produced in humans). D-lactate is produced by bacteria in the human colon when they are exposed to large amounts of unabsorbed carbohydrates. In the setting of alteration in the intestinal flora and a high carbohydrate load (such as in short bowel syndrome) there will be an excess production of D-lactate, which can cross into the bloodstream and potentially cause neurologic symptoms.
The concentration of lactate depends on the rate of production and the rate of liver clearance. The liver can adequately clear lactate until the concentration reaches approximately 2 mmol/L. When this level is exceeded, lactate begins to accumulate rapidly. For example, while resting lactate levels are usually <1 mmol/L, during strenuous exercise levels can rise >20 mmol/L within a few seconds.
Lactic acidosis signals the deterioration of the cellular oxidative process and is associated with hyperpnea, weakness, fatigue, stupor, and finally coma. These conditions may be irreversible, even after treatment is administered. Lactate acidosis may be associated with hypoxic conditions (eg, shock, hypovolemia, heart failure, pulmonary insufficiency), metabolic disorders (e.g, diabetic ketoacidosis, malignancies), and toxin exposures (e.g, ethanol, methanol, salicylates).
There are a number of conditions that can cause high levels of lactate.
Excess lactate may indicate one or a combination of the following:
- Lack of oxygen (hypoxia)
- The presence of a condition that causes increased lactate production
- The presence of a condition that causes decreased clearance of lactate from the body
Times when your body’s oxygen level might drop include:
- During intense exercise
- When you have an infection or disease
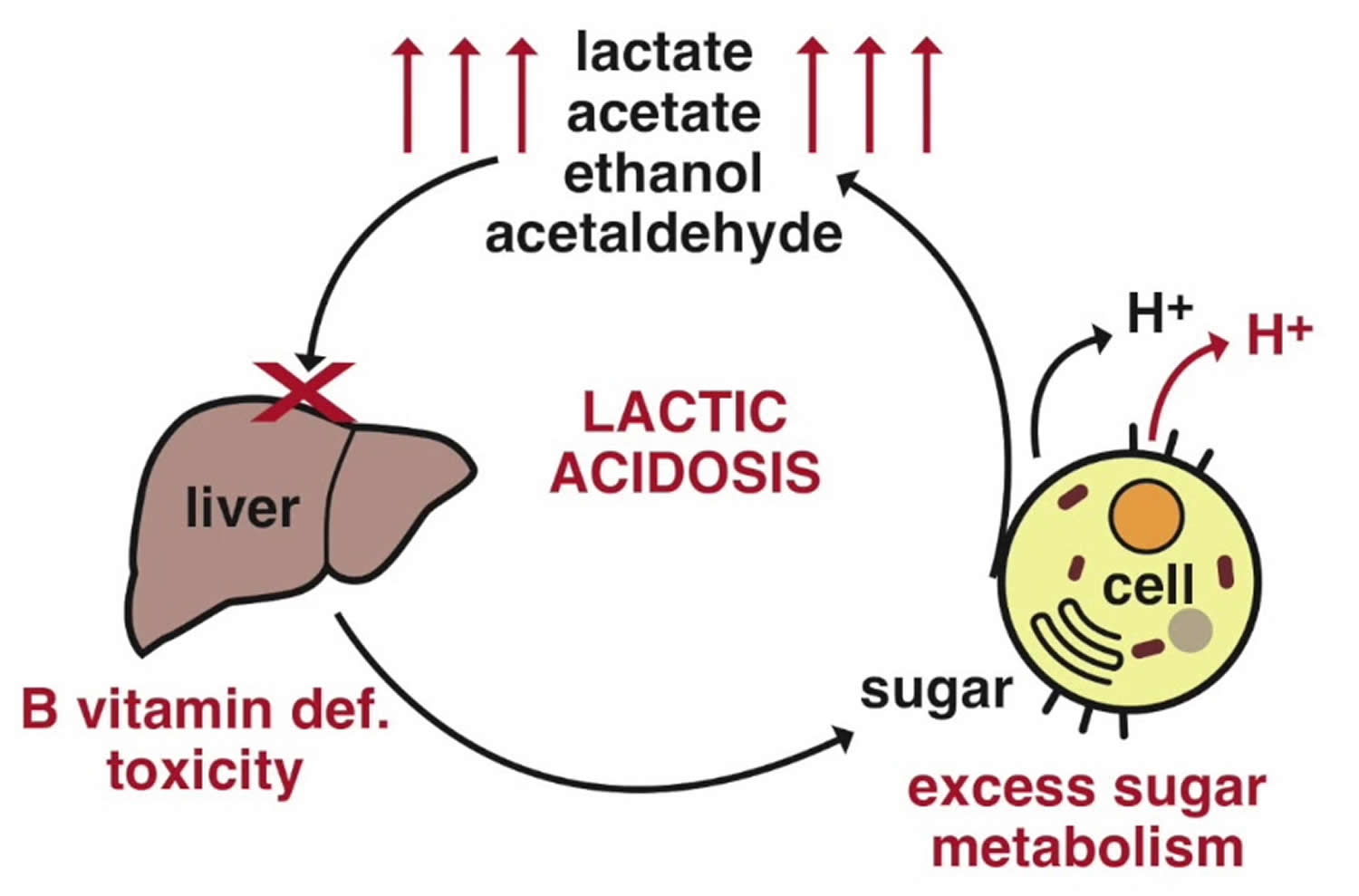
Increased lactate levels may also be seen with thiamine (vitamin B1) deficiency. Thiamine serves as a co-factor for multiple cellular enzymes including pyruvate dehydrogenase and α-ketoglutarate dehydrogenase, components essential to the tricarboxylic acid cycle and aerobic carbohydrate metabolism (see Figure 1). In the absence of thiamine, anaerobic metabolism predominates and lactate production increases 6. The development of elevated lactate in both serum and cerebrospinal fluid secondary to thiamine deficiency has been well described 7.
Lactate is one of the substances produced by cells as your body turns food into energy (cell metabolism). Lactate is formed by reduction of pyruvate, and is metabolized by oxidation to pyruvate in the reaction catalyzed by the cytosolic NAD-dependent lactate dehydrogenase (Figure 2). Depending on pH, lactate is sometimes present in the form of lactic acid. However, with the neutral pH maintained by the body, most of it will be present in the blood in the form of lactate.
Normally, the level of lactate in blood and cerebrospinal fluid (CSF) is low. Lactate is produced in excess by muscle cells, red blood cells, brain, and other tissues when there is insufficient oxygen at the cellular level or when the primary way of producing energy in the body’s cells is disrupted. Excess lactate can lead to lactic acidosis.
Lactic acid is mainly produced in muscle cells and red blood cells. Under conditions of heavy energy demand (and thus high oxygen need) skeletal muscles convert glucose into lactic acid to use for energy when oxygen levels are low (anaerobic), which is excreted from the muscle cells into the blood. In the liver this lactic acid is reduced to glucose.
The principal means of producing energy within cells occurs in the mitochondria, tiny power stations inside most cells of the body. The mitochondria use glucose and oxygen to produce ATP (adenosine triphosphate), the body’s primary source of energy. This is called aerobic energy production.
Whenever cellular oxygen levels decrease and/or the mitochondria are not functioning properly, the body must turn to less efficient energy production to metabolize glucose and produce ATP (adenosine triphosphate). This is called anaerobic energy production and the primary byproduct is lactic acid, which is processed (metabolized) by the liver.
Lactic acid can accumulate in the body and blood when it is produced faster than the liver can break it down.
When lactic acid production increases significantly, the affected person is said to have hyperlactatemia, which can then progress to lactic acidosis as more lactic acid accumulates. The body can often compensate for the effects of hyperlactatemia, but lactic acidosis can be severe enough to disrupt a person’s acid/base (pH) balance and cause symptoms such as muscular weakness, rapid breathing, nausea, vomiting, sweating, and even coma.
A test can be done to measure the amount of lactic acid in your blood. The lactate test measures the level of lactate in the blood at a given point in time or less commonly, in the cerebrospinal fluid (CSF). A normal lactate level indicates that a person does not have lactic acidosis, that there is sufficient oxygen at the cellular level, and/or that their signs and symptoms are not caused by lactic acidosis.
Key points
- Lactic acidosis occurs when lactate production exceeds its metabolism. Common criteria for the diagnosis of lactic acidosis include a plasma lactate concentration in excess of 4 mmol/L 2, usually with plasma pH <7.35.
- Elevated lactate can be caused by a number of conditions including shock, sepsis, cardiac arrest, trauma, seizure, ischemia, diabetic ketoacidosis, thiamine deficiency, malignancy, liver dysfunction, genetic disorders, toxins, and medications
- Elevated lactate has been associated with increased mortality in a number of diseases such as sepsis, trauma and cardiac arrest
- Decreased lactate clearance has been found to be associated with increased mortality in sepsis, post-cardiac arrest, trauma, burns and other conditions
- When approaching the patient with elevated lactate, the possibility of a multifactorial causes must be considered
- In spite of its imperfect sensitivity and specificity, the lactate blood test remains a clinically useful test that can alert a clinician to underlying hypoperfusion in need of immediate treatment or an etiology not readily apparent on initial evaluation
Figure 1. Lactic acid production and aerobic and anaerobic metabolism
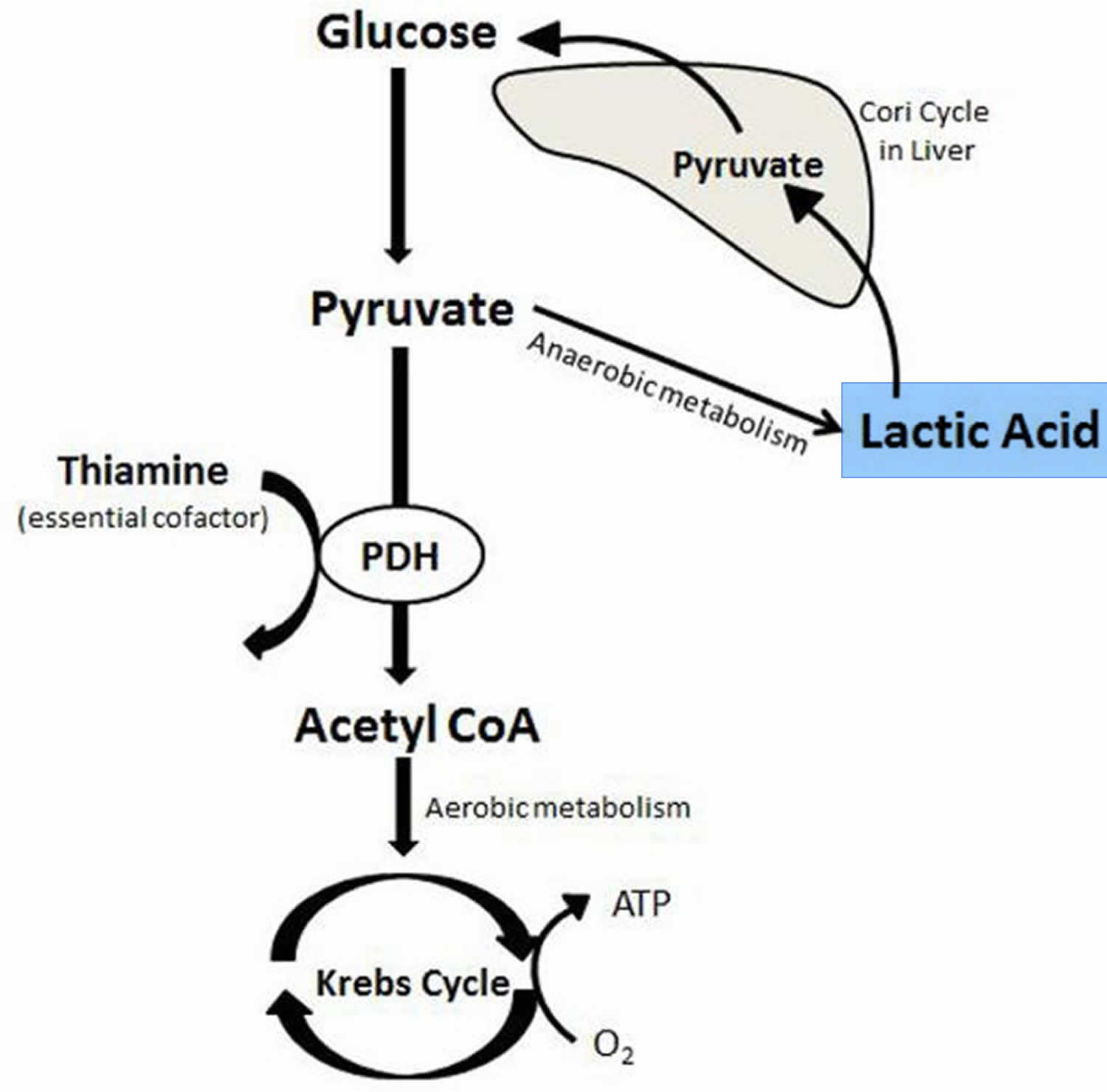
Abbreviatons: ATP = Adenosine triphosphate; CoA = Coenzyme A; PDH = Pyruvate dehydrogenase
[Source 8 ]Lactate is one of the substances produced by cells as your body turns food into energy (cell metabolism). Lactate is formed by reduction of pyruvate, and is metabolized by oxidation to pyruvate in the reaction catalyzed by the cytosolic NAD-dependent lactate dehydrogenase (Figure 2). Depending on pH, lactate is sometimes present in the form of lactic acid. However, with the neutral pH maintained by the body, most of it will be present in the blood in the form of lactate.
Normally, the level of lactate in blood and cerebrospinal fluid (CSF) is low. Lactate is produced in excess by muscle cells, red blood cells, brain, and other tissues when there is insufficient oxygen at the cellular level or when the primary way of producing energy in the body’s cells is disrupted. Excess lactate can lead to lactic acidosis.
Lactic acid is mainly produced in muscle cells and red blood cells. Under conditions of heavy energy demand (and thus high oxygen need) skeletal muscles convert glucose into lactic acid to use for energy when oxygen levels are low (anaerobic), which is excreted from the muscle cells into the blood. In the liver this lactic acid is reduced to glucose.
The principal means of producing energy within cells occurs in the mitochondria, tiny power stations inside most cells of the body. The mitochondria use glucose and oxygen to produce ATP (adenosine triphosphate), the body’s primary source of energy. This is called aerobic energy production.
Whenever cellular oxygen levels decrease and/or the mitochondria are not functioning properly, the body must turn to less efficient energy production to metabolize glucose and produce ATP (adenosine triphosphate). This is called anaerobic energy production and the primary byproduct is lactic acid, which is processed (metabolized) by the liver.
Lactic acid can accumulate in the body and blood when it is produced faster than the liver can break it down.
Figure 2. Lactate metabolism
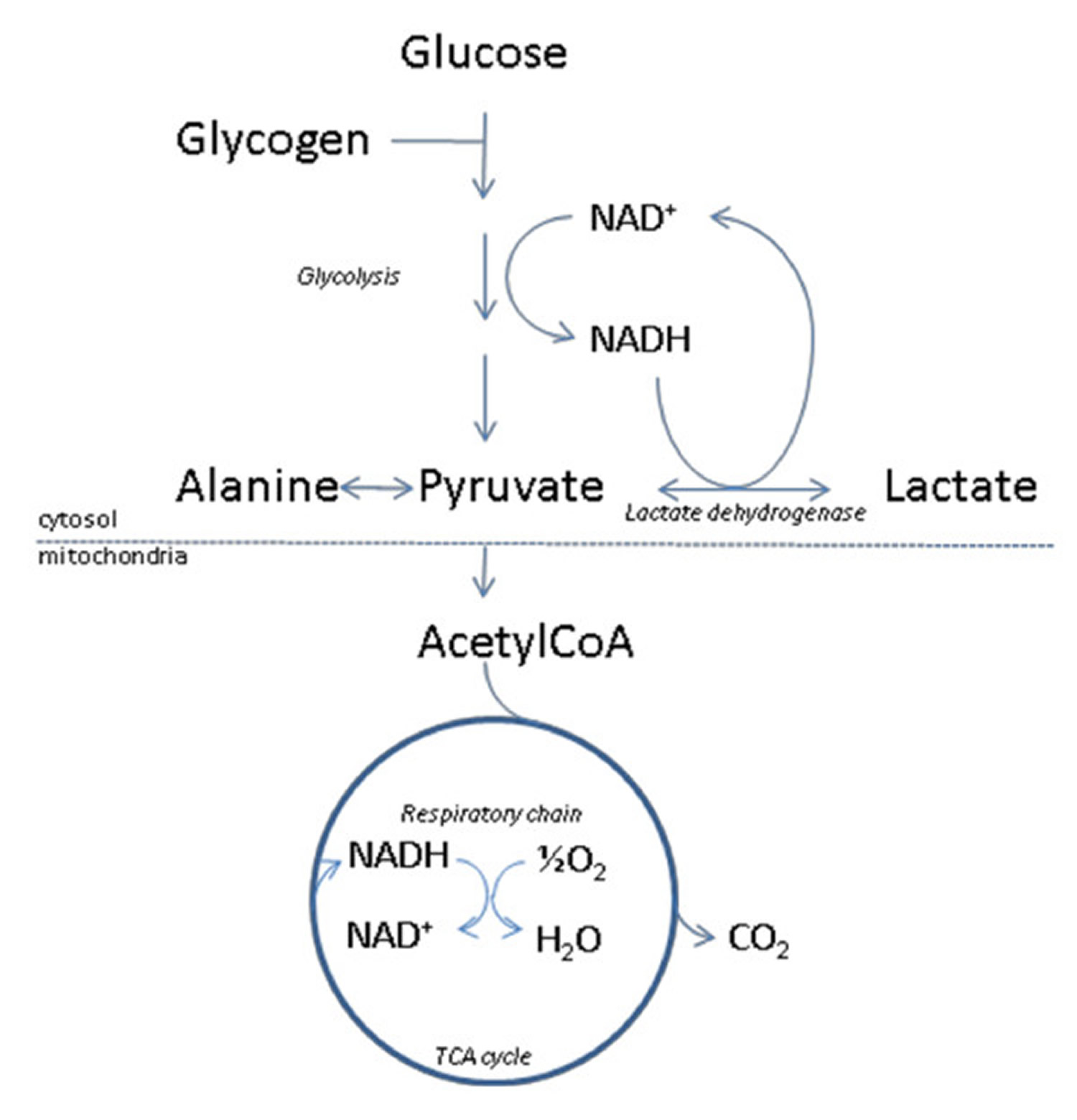
Footnote: Outline of lactate metabolism. With insufficient oxygen supply, pyruvate will be diverted to lactate, thereby assuring regeneration of NAD+ from NADH. This will enable glycolysis, and the accompanying ATP production to proceed.
The metabolic fate of pyruvate is mainly mitochondrial oxidation to carbon dioxide and water with accompanying energy production in the respiratory chain. The latter sequence of reactions are oxygen requiring, and with insufficient oxygen supply, or if pyruvate production for other reasons exceeds the capacity of oxidative metabolism, pyruvate will be diverted to lactate. This assures regeneration of NAD+ from NADH, which will enable glycolysis, and the accompanying ATP production to proceed. Due to the central role of the NAD-redox state for lactate production and metabolism, any metabolic condition giving rise to a steady-state increase in the cytosolic NADH/NAD+ ratio, will cause an increased net lactate production. This applies not only to conditions of hypoxia/anoxia in all tissues, but is also observed e.g. during extensive muscular work, and during alcohol metabolism by the liver. Lactate is released from tissues accompanied by a proton, and because lactic acid is fully dissociated at pH above approximately 6, excessive lactate production may thus give rise to lactic acidosis. The uptake of lactate from plasma takes place predominantly in liver and heart, where lactate will be used as an energy producing substrate or, in case of the liver, as a precursor for glucose formation.
[Source 9]Figure 3. Lactic acid and lactate chemical structure
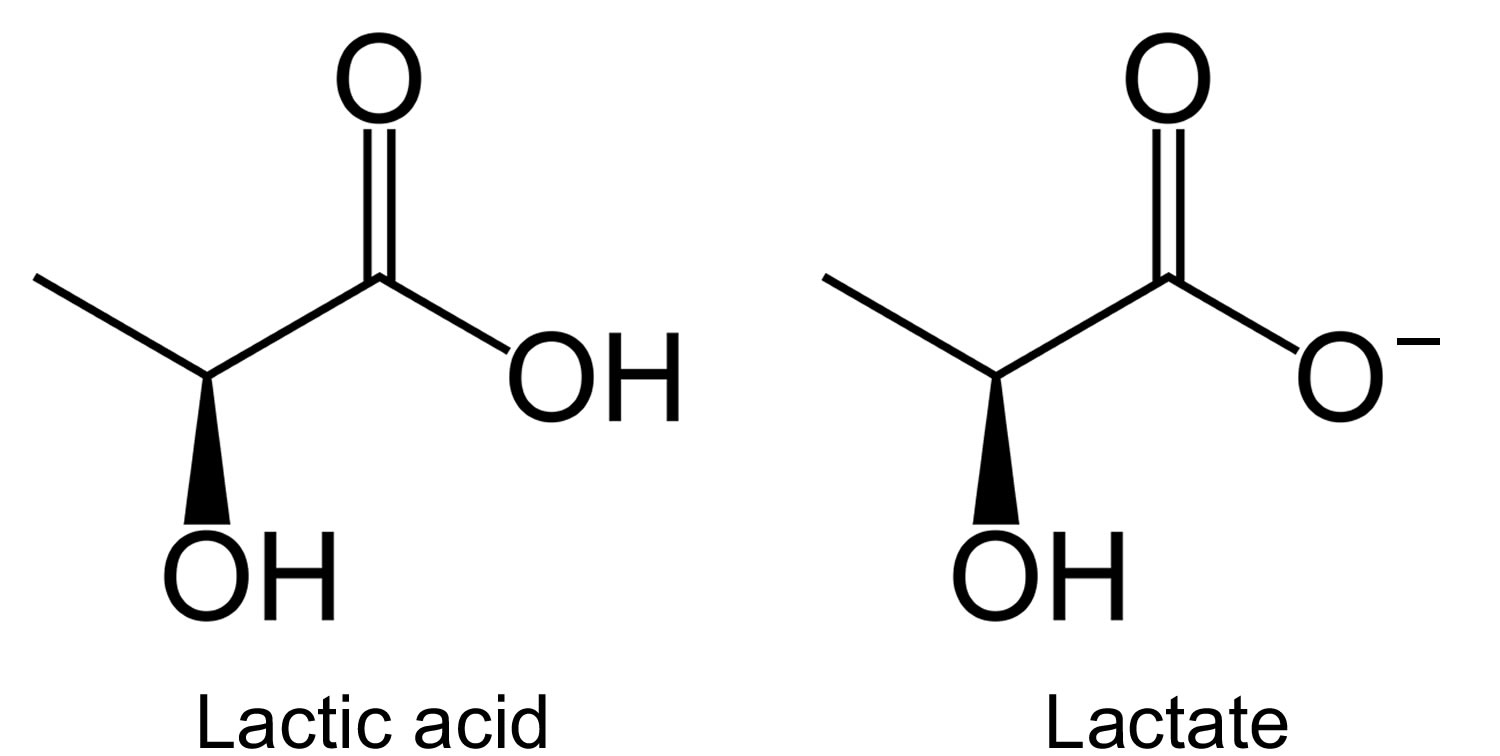
Figure 4. Acid-base buffering system
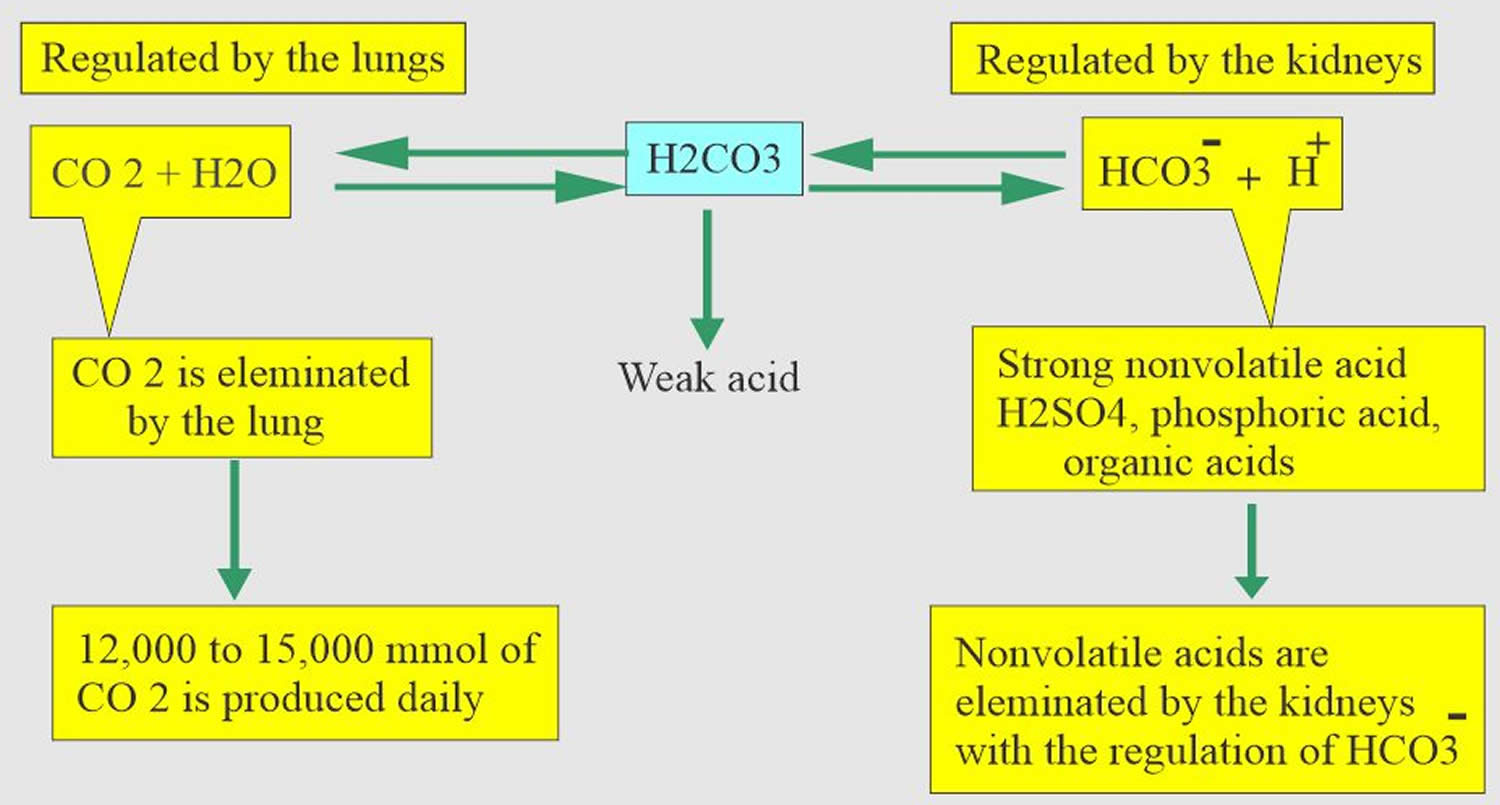
Table 1. Causes of elevated lactate
| Shock | Pharmacological agents* |
| Distributive | Linezolid |
| Cardiogenic | Nucleoside reverse transcriptase inhibitors |
| Hypovolemic | Metformin |
| Obstructive | Epinephrine |
| Post-cardiac arrest | Propofol |
| Regional tissue ischemia | Acetaminophen |
| Mesenteric ischemia | Beta2 agonists |
| Limb ischemia | Theophylline |
| Burns | |
| Trauma | Anaerobic muscle activity |
| Compartment syndrome | Seizures |
| Necrotizing soft tissue infections | Heavy exercise |
| Diabetic ketoacidosis | Excessive work of breathing |
| Drugs/toxins | Thiamine deficiency |
| Alcohols | Malignancy |
| Cocaine | Liver failure |
| Carbon monoxide | Mitochondrial disease |
| Cyanide |
Table 2. Common drugs and toxins associated with elevated lactate
| Drug/toxin | Risk factors | Proposed mechanism | Suggested treatment in addition to cessation of the offending agent |
|---|---|---|---|
| Metforminb | Congestive heart failure, kidney failure, liver failure or overdose | Inhibition of gluconeogenesis and mitochondrial impairment, inhibition of lactate elimination | Consider hemodialysis |
| Acetaminophen | Overdose | Impairment of the mitochondrial electron transport chain. Later hepatotoxicity and systemic effects. | Enteral activated charcoal and N-acetylcysteine. |
| NRTI | Female gender | Direct mitochondrial toxicity | No specific treatment |
| Linezolid | Possibly prolonged use in elderly patients | Direct mitochondrial toxicity | No specific treatment |
| Beta2-agonists | Not applicable | Beta2-adrenergic stimulation causing increased glycogenolysis, glycolysis and lipolysis. Free fatty acids released by lipolysis may inhibit PDH. | Depending on the clinical situation the beta2-agonist may/should be continued |
| Propofol | Prolonged high-dose use (Propofol Infusion Syndromed) | Impairment of the mitochondrial electron transport chain and fatty acid oxidation | Supportive treatment and potentially hemodialysis should be considered |
| Epinephrine | Not applicable | Likely due to beta2-adrenergic stimulation (see beta2-agonists) | Depending on the clinical situation epinephrine may be continued. |
| Theophylline | Overdose, though reported in standard doses | Increased levels of catecholamines (see beta2-agonists) | Enteral activated charcoal. Hemodialysis in severe cases. |
| Alcohols (ethanol, methanol, propylene glycol)b,c | Clinical relevance controversial and may be confounded by comorbidities (thiamine deficiency, seizures, sepsis, and other toxins) | Increased NADH levels due to ethanol metabolism may inhibit PDH and the utilization of lactate. Contributions from underlying comorbidities or possibly ketoacidosis may play a role | Identification and treatment of underlying disorders including administration of thiamine. |
| Cocaine | Not applicable | Beta2-adrenergic stimulation (see beta2-agonists). Vasoconstriction causing ischemia. | Supportive care and benzodiazepine |
| Carbon monoxide | Not applicable | Decreased oxygen-carrying capacity of the blood. | High-flow/hyperbaric oxygen. Consider co-exposure to cyanide |
| Cyanide | Not applicable | Noncompetitive inhibition of cytochrome c oxidase causing mitochondrial dysfunction and inability to utilize oxygen | Hydroxocobalamin or other cyanide antidote kit (Sodium nitrite, amyl nitrite, sodium thiosulfate). Consider co-exposure to carbon monoxide. |
Footnotes:
- a: NRTI = Nucleoside reverse transcriptase inhibitor, PDH = Pyruvate dehydrogenase, NADH = Reduced nicotinamide adenine dinucleotide
- b: See text for more details
- c: Ethylene glycol may cause falsely elevated lactate levels
- d: The Propofol Infusion Syndrome is characterized by cardiac failure, rhabdomyolysis, metabolic acidosis and renal failure.
How to get rid of lactic acid?
Generally you cannot get rid of lactic acid. However, if your elevated lactate level is due to an underlying condition that can be addressed, such as uncontrolled diabetes or a substance that can be avoided, such as ethanol, then you may be able to lower it. If you have been diagnosed with a condition, such as a metabolic disorder, following your prescribed treatment regimen should control your lactate level. If the increase is due to a temporary condition, such as shock or infection, then it will usually return to normal after the condition has been resolved.
Lactic acidosis symptoms
Acidosis may not cause any symptoms or it may be associated with nonspecific symptoms such as fatigue, nausea, and vomiting. Acute acidosis may also cause an increased rate and depth of breathing, confusion, and headaches, and it can lead to seizures, coma, and in some cases death.
Lactic acidosis causes
A high lactate level in the blood means that the disease or condition a person has is causing lactate to accumulate. In general, a greater increase in lactate means a greater severity of the condition. When associated with lack of oxygen, an increase in lactate can indicate that organs are not functioning properly.
However, the presence of excess lactate is not diagnostic. A health practitioner must consider a person’s medical history, physical examination, and the results of other diagnostic tests in order to determine the cause and to diagnose the underlying condition or disease.
A number of conditions can cause elevated lactate levels. They are separated into two groups according to the mechanism by which they cause lactic acidosis.
Type A lactic acidosis
Type A lactic acidosis is the most common type, may be due to conditions that cause a person to be unable to breathe in enough oxygen (inadequate oxygen uptake in the lungs) and/or cause reduced blood flow, resulting in decreased transport of oxygen to the tissues (decreased tissue perfusion). Examples of type A conditions include:
- Shock from trauma or extreme blood loss (hypovolemia)
- Sepsis
- Heart attack
- Congestive heart failure
- Severe lung disease or respiratory failure
- Fluid accumulation in the lungs (Pulmonary edema)
- Very low level of red blood cells and/or low hemoglobin (severe anemia)
Type B lactic acidosis
Type B lactic acidosis is not related to delivery of oxygen but reflects excess demand for oxygen or metabolic problems. Examples of type B causes include:
- Excessive lactate production
- Alcohols
- Ethanol
- Methanol
- Ethylene glycol
- Propylene glycol
- Impaired lactate use
- Liver disease
- Kidney disease
- Fructose metabolic defects
- Diabetes mellitus/Inadequately treated (uncontrolled) diabetes
- Leukemia
- AIDS
- Rare glycogen storage diseases (such as glucose-6-phosphatase deficiency)
- Use of certain drugs such as salicylates and metformin
- Exposure to toxins such as cyanide and methanol
- A variety of rare inherited metabolic and mitochondrial diseases that are forms of muscular dystrophy and affect normal ATP production (see the Related
- Content below for links to more information on these)
- Strenuous exercise, as with marathon runners
- Impaired oxygen use
- Disruption of mitochondrial oxidative phosphorylation
- Cyanide intoxication
- Carbon monoxide intoxication
- Linezolid
- Biguanides
- Nucleoside analog reverse transcription inhibitors
- Acetaminophen intoxication
- Acquired defects of the citric acid cycle or tricarboxylic acid cycle
- Thiamine deficiency
- Nutritional
- Cancer
- Alcoholism
- Gastrectomy
- Congenital defects of:
- Pyruvate transport
- Citric acid cycle or tricarboxylic acid cycle enzymes
- Pyruvate dehydrogenase complex
When someone is being treated for lactic acidosis or hypoxia, decreasing concentrations of lactate over time reflect a response to treatment.
When someone has signs and symptoms of meningitis, significantly increased cerebrospinal fluid lactate levels suggest bacterial meningitis while normal or slightly elevated levels are more likely to be due to viral meningitis.
Lactic acidosis is also associated with both inherited and acquired metabolic diseases. Lactic acid metabolism in the presence of altered gluconeogenesis, anaerobic glycolysis, and acid-base balance is a major factor in many disorders. Lactic acid can be formed only from pyruvic acid; therefore, disorders that increase pyruvate concentration, enhance lactic acid formation, or reduce lactic acid degradation cause lactic acidosis. Inborn metabolic errors that are accompanied by derangement of metabolic pathways of glucose, pyruvate, amino acids, and organic acids as well as toxic and systemic conditions that promote tissue hypoxia or mitochondrial injury result in lactic acidosis.
Metformin lactic acidosis
Metformin is the most extensively used oral therapeutic agent for type 2 diabetes mellitus. The American Diabetes Association recommends metformin as the first line treatment for type 2 diabetes mellitus in conjunction with rigorous physical activity and dietary restriction. Metformin is an insulin sensitizer 11; metformin is ineffective in the absence of insulin. Metformin acts mainly by reducing hepatic gluconeogenesis 11, in large part by inhibiting mitochondrial oxidative phosphorylation 12 and mitochondrial glycerophosphate dehydrogenase 13. Metformin also has some effect to increase peripheral glucose disposal 11. Unlike phenformin, metformin is not metabolized and is eliminated entirely by the kidney. Its plasma clearance is by glomerular filtration and to a greater extent, tubular secretion through a variety of transporters 11. Despite a tremendous volume of distribution, its half-time of elimination is estimated to be only 2.7 hours 11.
Metformin, however, can cause lactic acidosis in conditions where lactic acid production is high and the disposal of lactic acid is reduced. In conditions such as circulatory failure, sepsis, and anoxia or hypoxia, metformin use may result in lactic acidosis and should be avoided. It should also be avoided in patients who have renal failure with creatinine clearance below 30 mL/min/1.73 m² or hepatic failure. Metformin interacts with some medications, including cimetidine because its metabolism is partially inhibited by metformin, thereby increasing cimetidine concentration.
Because of Metformin’s effect to reduce hepatic gluconeogenesis, for which lactate is a substrate, and because it acts partly by inhibiting mitochondrial oxidative phosphorylation and lowering the mitochondrial redox state 13, it is somewhat surprising that metformin administration has been found to cause only a slight increase in basal and postprandial plasma lactate concentrations 11. Among the many studies corroborating metformin’s low potential to cause lactic acidosis are a systematic review of 347 clinical trials, finding no patients with fatal or nonfatal lactic acidosis in 70,490 subject-years of metformin exposure 14, and a case-control study of over 50,000 patients with type 2 diabetes mellitus, yielding about three cases of lactic acidosis per 100,000 patient-years of metformin use—an incidence no different from that among patients using sulfonylurea drugs 15. Nonetheless, very shortly after the drug was marketed in the United States, a case series of metformin-associated lactic acidosis was reported 16. This was followed by hundreds of case reports and a dozen case series over the past two decades 17. However, given the predisposition of patients with diabetes mellitus to hyperlactatemia and lactic acidosis 18, questions arose regarding metformin’s role in the reported lactic acidosis. Does metformin cause lactic acidosis, or is it merely associated with it?
The fact that metformin is capable of causing lactic acidosis is obvious from patients with pure metformin overdose 11. This serves to emphasize that, from both mechanistic and logical standpoints, metformin accumulation is the risk for lactic acidosis 19, with studies suggesting that a metformin plasma level of at least 40 mg/L (10 times the therapeutic level) may be necessary to cause lactic acidosis 20. On this basis, there are three possible relevant conditions: (1) metformin-independent lactic acidosis (in which metformin cannot possibly be implicated), (2) metformin-induced lactic acidosis (in which no other possible cause of lactic acidosis is present), and (3) metformin-associated lactic acidosis (in which metformin is among the factors that might have caused lactic acidosis) 11. Despite a tremendous volume of distribution, its half-time of elimination is estimated to be only 2.7 hours 11. Strictly speaking, these defined conditions require measurement of plasma metformin concentration; the latter two conditions may only be considered in the presence of a high metformin concentration. Most large, tertiary referral centers, plasma metformin measurement cannot be performed in-house. Specimens are sent to a reference laboratory, and results may take days to return. Thus, metformin levels usually cannot help to guide acute management. Furthermore, metformin levels correlate poorly with pH, plasma lactate levels, or clinical outcomes 21.
Recently a major Cochrane meta-analysis concluded that there was no increased risk of the development of elevated lactate for metformin compared to non-metformin treatment, however this may reflect usage in selected study populations and not necessarily those with overdoses or use in renal insufficiency, for example 22. The estimated rate of confirmed elevated lactate (lactate >5 mmol/L) was reported to be around 5 cases per 100,000 patients based on numbers from the Food and Drug Administration (FDA) from 1996 23. Patients with diabetes who develop this complication are often ill and have numerous comorbid issues, such as renal insufficiency and congestive heart failure. The elevated lactate observed in metformin users may be related to an exacerbation of their chronic disease or another acute insult and is not necessarily related to metformin 24. Pure metformin-associated elevated lactate is often seen with accumulation due to kidney failure, liver failure or overdose. In cases with renal failure, the suggested treatment is hemodialysis, which will correct the metabolic acidosis and remove metformin 24.
Metformin removal by dialysis has figured prominently in the management of patients with metformin-associated lactic acidosis 25. Metformin is readily dialyzable, owing to its low molecular weight and lack of protein binding 26. Because of its very high volume of distribution and two-compartment elimination kinetics 25, metformin’s removal may be best accomplished with prolonged extracorporeal therapy, either intermittent 27 or continuous 28. In one series, it took an average of 15 hours of conventional hemodialysis to reduce metformin levels to <20% of predialysis levels 27. Continuous renal replacement therapy may be the preferred modality for patients with hemodynamic instability, such as in this patient. The ambiguities regarding the most efficacious modality of renal replacement therapy in metformin-associated lactic acidosis and lactic acidosis in general point to the need for future controlled clinical trials in this area.
Figure 5. Metformin-associated lactic acidosis
Lactic acid blood test
The lactate test is primarily ordered to help determine if someone has lactic acidosis, a level of lactate that is high enough to disrupt a person’s acid-base (ph) balance.
Depending on pH, lactate is sometimes present in the form of lactic acid. However, with the neutral pH maintained by the body, most lactic acid will be present in the blood as lactate.
- Lactic acidosis is most commonly caused by an inadequate amount of oxygen in cells and tissues (hypoxia). If someone has a condition that may lead to a decreased amount of oxygen delivered to cells and tissues, such as shock or congestive heart failure, this test can be used to help detect and evaluate the severity of hypoxia and lactic acidosis. It may be ordered along with blood gases to evaluate a person’s acid/base balance and oxygenation.
- As lactic acidosis may also be caused by conditions unrelated to oxygen levels, this test may be used to evaluate someone who has a disease that can lead to increased lactate levels and who has signs and symptoms of acidosis. It may be ordered along with groups of tests, such as the comprehensive metabolic panel, basic metabolic panel or complete blood count (CBC), to determine if an underlying condition, such as liver or kidney disease, is causing lactic acidosis.
- The lactate test may also be used as part of an initial evaluation of someone who is suspected of having sepsis. Typically, if the person’s lactate level is above normal limits, treatment will be initiated without delay. If a person with sepsis can be diagnosed and treated promptly, their chances of recovery are significantly improved.
- Lactate levels may be ordered at intervals to help monitor hypoxia and response to treatment in a person being treated for an acute condition, such as sepsis, shock or heart attack, or a chronic condition, such as severe congestive heart failure.
A cerebrospinal fluid (CSF) lactate test may be ordered, along with a blood lactate test, to help distinguish between viral and bacterial meningitis.
Lactic acid normal range
Under 2 years of age: 0.6-3.2 mmol/L of lactate
Over 2 years of age: 0.6-2.3 mmol/L of lactate
Elevated lactic acid
While no definitive concentration of lactate has been established for the diagnosis of lactic acidosis, lactate concentrations exceeding 5 mmol/L and pH below 7.25 are generally considered indicative of significant lactic acidosis.
When is lactate test ordered?
A lactate test may be ordered when someone has signs and symptoms of inadequate oxygen (hypoxia) such as:
- Shortness of breath
- Rapid breathing
- Paleness
- Sweating
- Nausea
- Muscle weakness
- Abdominal pain
- Coma
The test may be ordered when a person has signs and symptoms that a health practitioner suspects are related to sepsis, shock, heart attack, severe congestive heart failure, kidney failure, or uncontrolled diabetes.
The lactate test may be initially ordered with other tests to help evaluate a person’s condition. If lactate is significantly elevated, it may be ordered at intervals to monitor the condition.
CSF and blood lactate levels may be ordered when a person has signs and symptoms of meningitis, such as severe headaches, fever, delirium, and loss of consciousness.
Why would a health practitioner choose to measure lactate in a blood sample from an artery rather than blood from a vein?
Lactate measurements from arterial blood are thought to be more accurate and, because a tourniquet is not used, they are not generally affected by the collection process. A health practitioner may order an arterial lactate for these reasons or because a group of other tests called arterial blood gases (ABGs) are also being collected and the same sample can be used. When other arterial blood tests are not being ordered, a health practitioner may order a venous lactate because it provides an adequate evaluation of a person’s lactate level and because the collection process is not as uncomfortable.
Are there other ways to measure lactate than by sending a blood sample to the lab for testing?
Yes. Lactate may be measured using a small hand-held device much like a glucose meter at the point of care at a patient’s bedside, instead of in a laboratory. This type of monitoring is useful, for example, in emergency departments and intensive care units where rapid results are vital to the care of critically ill people. However, since the methods of measurement are different, the results from lactate point of care tests may not be comparable with those from tests performed in a laboratory.
What is the lactate/pyruvate ratio and how is it used?
A lactate/pyruvate ratio is a calculated result that may be used to differentiate between causes of lactic acidosis.
Pyruvate is a substance produced by and used by cells in the production of energy. The mitochondria within cells metabolize glucose in a series of steps to produce ATP, the body’s energy source. One of the steps involves pyruvate and the following step requires oxygen. When the oxygen level is low, pyruvate accumulates and is converted to lactate, resulting in an accumulation of lactate and lactic acidosis. An alternative cause is when there is impaired mitochondrial function and the pathway is interrupted, resulting in increased pyruvate and hence more lactate. The lactate/pyruvate ratio will be high in these cases.
However, there are certain congenital disorders (inborn errors of metabolism) in which pyruvate is not converted to lactate. One example is pyruvate dehydrogenase deficiency. In these cases, pyruvate will accumulate, the blood level will be high, and the lactate to pyruvate ratio will be low.
Lactic acidosis treatment
Apart from supportive care, there are several possible therapeutic approaches to patients with lactic acidosis in general: treatment of the underlying cause, raising the systemic pH, and removal of lactate from the blood. Only the first of these is not controversial. For patients with type A lactic acidosis, ameliorating the cause of lactic acidosis involves improving tissue perfusion. Patients with shock should be treated with fluids and vasoactive medications to optimize their hemodynamics. To complicate even this straightforward recommendation, however, it must be noted that catecholamines (epinephrine more than norepinephrine) cause an increase in plasma lactate concentration 29. Treatment of type B lactic acidosis may involve removal of the causative toxin as discussed below.
Alkali therapy often is used to treat the acidemia that typically accompanies lactic acidosis. This practice is based, at least partly, on the recognition that acidemia has important hemodynamic effects. It impairs myocardial contractility 30 and causes venoconstriction with central vascular congestion 31, arterial vasodilation and resistance to the vasoconstrictive effects of catecholamines, especially when the pH is <7.10–7.20 (33). Although alkalinization has theoretical appeal, no animal or human studies of lactic acidosis have shown an improvement in myocardial performance 32 or survival with sodium bicarbonate administration 33, even among patients with the most profound acidemia 34. Indeed, there is some evidence that sodium bicarbonate administration for lactic acidosis may be harmful 35. There are several possible reasons for this. First, bicarbonate may cause paradoxical intracellular acidification because of the increased generation of cell-permeant CO2 by mass action effect on the carbonic acid equilibrium 36. Second, the increase in extracellular pH reduces ionized calcium concentration because of chelation by albumin 37, impairing myocardial contractility 38. Third, alkalinization may reduce tissue oxygen delivery by the Bohr effect on hemoglobin oxygen affinity. Fourth, bicarbonate administration may increase lactate generation by upregulating the pH-dependent rate-limiting step in the glycolytic pathway. Fifth, administration of large volumes of sodium bicarbonate may cause intravascular fluid overload. All this notwithstanding, international critical care guidelines for sepsis recommend giving sodium bicarbonate if the blood pH is <7.15 39.
Precise calculation of bicarbonate deficit would require an accurate estimate of the volume of distribution of bicarbonate. The apparent bicarbonate distribution space varies widely, however, and in inverse proportion to the bicarbonate concentration 40. Even if the deficit could be accurately calculated, the effect of administered bicarbonate on the final bicarbonate concentration may be far from the predicted value because of ongoing acid generation and the contraction of the apparent bicarbonate distribution space as the bicarbonate concentration rises. Therefore, it may be most practical to administer a short-term or bolus infusion of sodium bicarbonate (e.g., 1–2 mmol/kg body wt intravenously), rechecking the arterial blood gases and pH at the end of the infusion and frequently thereafter to guide additional therapy. Care must be taken to ensure the patient’s ventilation is appropriate at the start of the infusion (i.e., pCO2 no greater than the plasma bicarbonate concentration +15), because the bicarbonate infusion will lead to increased CO2 generation and may, thus, worsen the acidemia. Finally, continuous bicarbonate infusions carry a risk of overshoot alkalemia, especially if the patient’s underlying cause of lactic acidosis is improving and there is metabolism of the lactate to bicarbonate.
Tris-hydroxymethyaminomethane is an amino alcohol that buffers without generating CO2. It has the theoretical advantage, therefore, of avoiding both the superimposed respiratory acidosis that may accompany bicarbonate administration and its consequent intracellular acidification 31. There is no evidence to support the use of Tris-hydroxymethyaminomethane in this situation.
Renal replacement therapy offers a number of theoretical and practical advantages over alkali infusion for the treatment of lactic acidosis. First, renal replacement therapy can deliver large quantities of base without the risk of volume overload. Second, renal replacement therapy may reduce plasma lactate concentration. This may not necessarily be a benefit, because lactate serves as a preferred energy substrate for some tissues under conditions of metabolic stress and may, thus, confer an adaptive advantage 33. Third, renal replacement therapy has the potential to maintain the plasma ionized calcium concentration while raising pH, thus potentially improving myocardial contractility 41. There are few studies of renal replacement therapy relevant to the treatment of lactic acidosis, and most are in the setting of sepsis with hemodynamic instability 26. Almost all involve continuous renal replacement therapy (continuous renal replacement therapy). Early uncontrolled studies showed the feasibility of continuous renal replacement therapy modalities in the treatment of patients with renal failure and lactic acidosis 42 and emphasized the metabolic advantage of bicarbonate- over lactate-buffered dialysate 42. A recent single-center observational cohort study of 116 patients with acute kidney injury and lactic acidosis showed that continuous renal replacement therapy using bicarbonate-buffered fluids can reduce blood lactate levels and raise pH 43. The effect of continuous renal replacement therapy on survival in patients with lactic acidosis has never been assessed, and therefore, the use of renal replacement therapy in patient cannot be considered evidence based.
- Luft D., Deichsel G., Schmülling R.M., Stein W., Eggstein M. Definition of Clinically Relevant Lactic Acidosis in Patients with Internal Diseases. Am. J. Clin. Pathol. 1983;80:484–489. doi: 10.1093/ajcp/80.4.484[↩]
- DuBose TD: Disorders of acid-base balance. In: Brenner & Rector’s The Kidney, 9th Ed., edited by Maarten WT, Chertow GM, Marsden PA, Skorecki K, Yu ASL, Brenner BM, editors. , Philadelphia, Saunders, 2012, pp 595–639.[↩][↩]
- Duong J.K., Furlong T.J., Roberts D.M., Graham G.G., Greenfield J.R., Williams K.M., Day R.O. The Role of Metformin in Metformin-Associated Lactic Acidosis (MALA): Case Series and Formulation of a Model of Pathogenesis. Drug Saf. 2013;36:733–746. doi: 10.1007/s40264-013-0038-6[↩]
- Lactate kinetics in human tissues at rest and during exercise. van Hall G. Acta Physiol (Oxf). 2010 Aug; 199(4):499-508. https://www.ncbi.nlm.nih.gov/pubmed/20345411[↩]
- Contribution of liver and skeletal muscle to alanine and lactate metabolism in humans. Consoli A, Nurjhan N, Reilly JJ Jr, Bier DM, Gerich JE. Am J Physiol. 1990 Nov; 259(5 Pt 1):E677-84. https://www.ncbi.nlm.nih.gov/pubmed/2240206/[↩]
- Butterworth RF. Thiamine deficiency-related brain dysfunction in chronic liver failure. Metab Brain Dis. 2009 Mar;24(1):189–196.[↩]
- Kountchev J, Bijuklic K, Bellmann R, Joannidis M. A patient with severe lactic acidosis and rapidly evolving multiple organ failure: a case of shoshin beri-beri. Intensive Care Med. 2005 Jul;31(7):1004.[↩]
- Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate. Mayo Clinic proceedings. 2013;88(10):1127-1140. doi:10.1016/j.mayocp.2013.06.012. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3975915/[↩]
- Kruse O, Grunnet N, Barfod C. Blood lactate as a predictor for in-hospital mortality in patients admitted acutely to hospital: a systematic review. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. 2011;19:74. doi:10.1186/1757-7241-19-74. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3292838/[↩]
- Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate. Mayo Clinic proceedings. 2013;88(10):1127-1140. doi:10.1016/j.mayocp.2013.06.012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3975915/[↩][↩]
- Lalau JD, Arnouts P, Sharif A, De Broe ME: Metformin and other antidiabetic agents in renal failure patients. Kidney Int 87: 308–322, 2015[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Kirpichnikov D, McFarlane SI, Sowers JR: Metformin: An update. Ann Intern Med 137: 25–33, 2002[↩]
- Madiraju AK, Erion DM, Rahimi Y, Zhang XM, Braddock DT, Albright RA, Prigaro BJ, Wood JL, Bhanot S, MacDonald MJ, Jurczak MJ, Camporez JP, Lee HY, Cline GW, Samuel VT, Kibbey RG, Shulman GI: Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature 510: 542–546, 2014[↩][↩]
- Salpeter SR, Greyber E, Pasternak GA, Salpeter EE: Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Database Syst Rev 4: CD002967, 2010[↩]
- Bodmer M, Meier C, Krähenbühl S, Jick SS, Meier CR: Metformin, sulfonylureas, or other antidiabetes drugs and the risk of lactic acidosis or hypoglycemia: A nested case-control analysis. Diabetes Care 31: 2086–2091, 2008[↩]
- Misbin RI, Green L, Stadel BV, Gueriguian JL, Gubbi A, Fleming GA: Lactic acidosis in patients with diabetes treated with metformin. N Engl J Med 338: 265–266, 1998[↩]
- Kajbaf F, Lalau JD: Mortality rate in so-called “metformin-associated lactic acidosis”: A review of the data since the 1960s. Pharmacoepidemiol Drug Saf 23: 1123–1127, 2014[↩]
- Scale T, Harvey JN: Diabetes, metformin and lactic acidosis. Clin Endocrinol (Oxf) 74: 191–196, 2011[↩]
- Lalau JD: Lactic acidosis induced by metformin: Incidence, management and prevention. Drug Saf 33: 727–740, 2010[↩]
- Adam WR, O’Brien RC: A justification for less restrictive guidelines on the use of metformin in stable chronic renal failure. Diabet Med 31: 1032–1038, 2014[↩]
- Vecchio S, Giampreti A, Petrolini VM, Lonati D, Protti A, Papa P, Rognoni C, Valli A, Rocchi L, Rolandi L, Manzo L, Locatelli CA: Metformin accumulation: Lactic acidosis and high plasmatic metformin levels in a retrospective case series of 66 patients on chronic therapy. Clin Toxicol (Phila) 52: 129–135, 2014[↩]
- Salpeter SR, Greyber E, Pasternak GA, Salpeter EE. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Database Syst Rev. 2010;(4):CD002967[↩]
- Misbin RI, Green L, Stadel BV, Gueriguian JL, Gubbi A, Fleming GA. Lactic acidosis in patients with diabetes treated with metformin. N Engl J Med. 1998 Jan 22;338(4):265–266.[↩]
- Lalau JD. Lactic acidosis induced by metformin: incidence, management and prevention. Drug safety : an international journal of medical toxicology and drug experience. 2010 Sep 1;33(9):727–740.[↩][↩]
- Lalau JD, Andrejak M, Morinière P, Coevoet B, Debussche X, Westeel PF, Fournier A, Quichaud J: Hemodialysis in the treatment of lactic acidosis in diabetics treated by metformin: A study of metformin elimination. Int J Clin Pharmacol Ther Toxicol 27: 285–288, 1989[↩][↩]
- Cerdá J, Tolwani A, Gibney N, Tiranathanagul K: Renal replacement therapy in special settings: Extracorporeal support devices in liver failure. Semin Dial 24: 197–202, 2011[↩][↩]
- Seidowsky A, Nseir S, Houdret N, Fourrier F: Metformin-associated lactic acidosis: A prognostic and therapeutic study. Crit Care Med 37: 2191–2196, 2009[↩][↩]
- Dichtwald S, Weinbroum AA, Sorkine P, Ekstein MP, Dahan E: Metformin-associated lactic acidosis following acute kidney injury. Efficacious treatment with continuous renal replacement therapy. Diabet Med 29: 245–250, 2012[↩]
- Levy B: Bench-to-bedside review: Is there a place for epinephrine in septic shock? Crit Care 9: 561–565, 2005[↩]
- Teplinsky K, O’Toole M, Olman M, Walley KR, Wood LD: Effect of lactic acidosis on canine hemodynamics and left ventricular function. Am J Physiol 258: H1193–H1199, 1990[↩]
- Kraut JA, Kurtz I: Use of base in the treatment of severe acidemic states. Am J Kidney Dis 38: 703–727, 2001[↩][↩]
- Kraut JA, Madias NE: Treatment of acute metabolic acidosis: A pathophysiologic approach. Nat Rev Nephrol 8: 589–601, 2012[↩]
- Rachoin JS, Weisberg LS, McFadden CB: Treatment of lactic acidosis: Appropriate confusion. J Hosp Med 5: E1–E7, 2010[↩][↩]
- Cooper DJ, Walley KR, Wiggs BR, Russell JA: Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled clinical study. Ann Intern Med 112: 492–498, 1990[↩]
- Arieff AI, Leach W, Park R, Lazarowitz VC: Systemic effects of NaHCO3 in experimental lactic acidosis in dogs. Am J Physiol 242: F586–F591, 1982[↩]
- Levraut J, Garcia P, Giunti C, Ichai C, Bouregba M, Ciebiera JP, Payan P, Grimaud D: The increase in CO2 production induced by NaHCO3 depends on blood albumin and hemoglobin concentrations. Intensive Care Med 26: 558–564, 2000[↩]
- Pedersen KO: Binding of calcium to serum albumin. II. Effect of pH via competitive hydrogen and calcium ion binding to the imidazole groups of albumin. Scand J Clin Lab Invest 29: 75–83, 1972[↩]
- Lang RM, Fellner SK, Neumann A, Bushinsky DA, Borow KM: Left ventricular contractility varies directly with blood ionized calcium. Ann Intern Med 108: 524–529, 1988[↩]
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K. World Federation of Societies of Intensive and Critical Care Medicine: Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med 36: 296–327, 2008[↩]
- Fernandez PC, Cohen RM, Feldman GM: The concept of bicarbonate distribution space: The crucial role of body buffers. Kidney Int 36: 747–752, 1989[↩]
- Orchard CH, Kentish JC: Effects of changes of pH on the contractile function of cardiac muscle. Am J Physiol 258: C967–C981, 1990[↩]
- Hilton PJ, Taylor J, Forni LG, Treacher DF: Bicarbonate-based haemofiltration in the management of acute renal failure with lactic acidosis. QJM 91: 279–283, 1998[↩][↩]
- De Corte W, Vuylsteke S, De Waele JJ, Dhondt AW, Decruyenaere J, Vanholder R, Hoste EA: Severe lactic acidosis in critically ill patients with acute kidney injury treated with renal replacement therapy. J Crit Care 29: 650–655, 2014[↩]





{kind=link}