Contents
What is metastatic melanoma
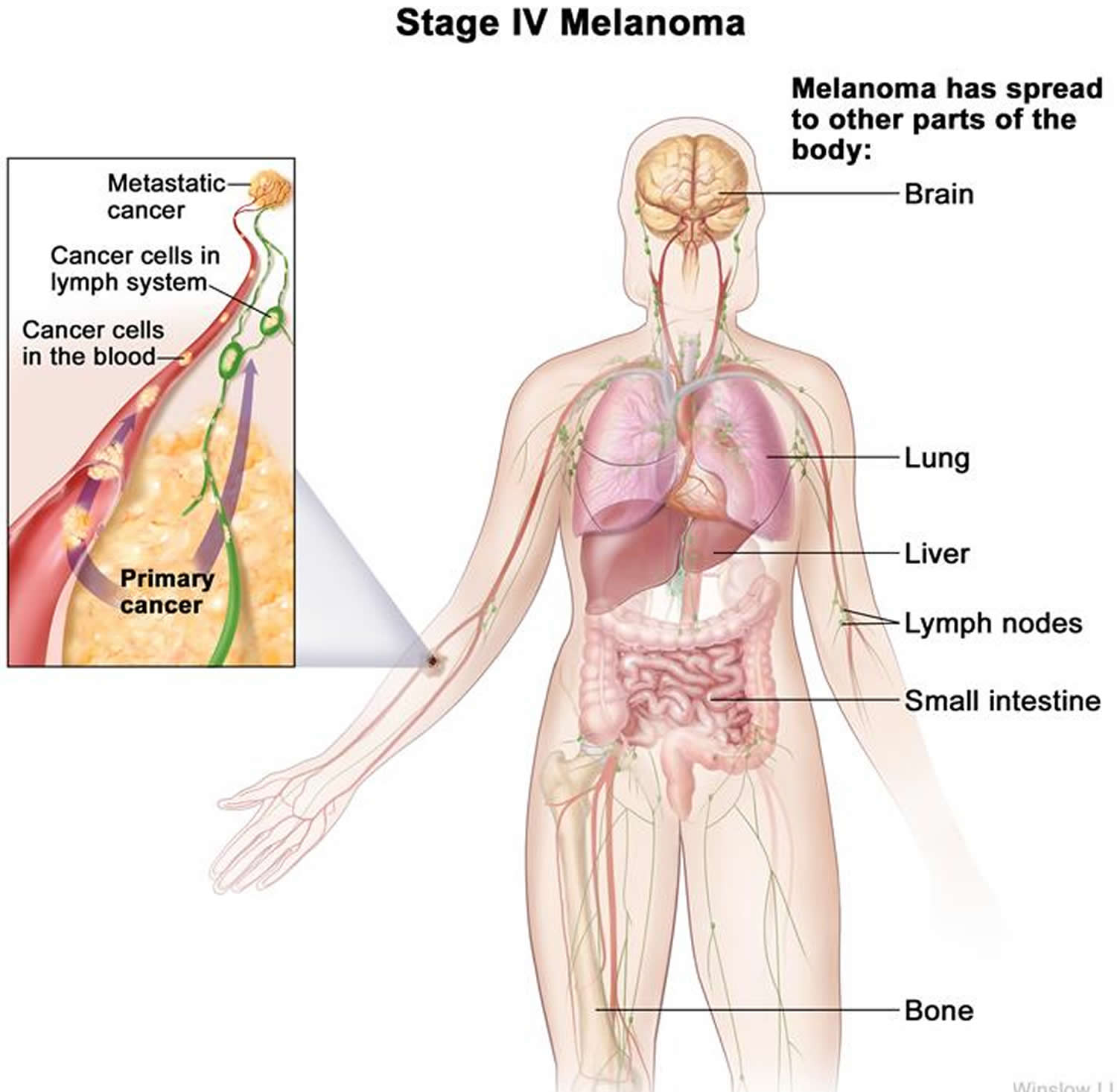
Melanoma is a cancer that begins in the melanocytes (a type of skin cells). Metastatic melanoma is considered to be a late form of stage IV (stage 4) of melanoma cancer and occurs when cancerous melanoma cells in the epidermis metastasize (spread) and progress to other organs of the body that are located far from the original site to internal organs, most often the lung, followed in descending order of frequency by the liver, brain, bone and gastrointestinal tract 1). The two main factors in determining how advanced the melanoma is into Stage IV (the “M” category, for “metastases”) are the site of the distant metastases (nonvisceral, lung or any other visceral metastatic sites) and whether or not the serum lactate dehydrogenase (LDH) level is elevated. LDH (lactate dehydrogenase), an enzyme found in your blood and almost every other cell of your body, turns sugar into energy, and the more you have in your blood or other body fluid, the more damage has been done to your body’s tissues.
It is crucial to diagnose melanoma in its early stages before it metastasizes, as once it has spread, it is difficult to locate its origin and so treatment and patient’s survival rate tends to be hindered 2).
An estimated 178,560 cases of melanoma will be diagnosed in the U.S. in 2018 3). Of those, 87,290 cases will be in situ (noninvasive), confined to the epidermis (the top layer of skin), and 91,270 cases will be invasive, penetrating the epidermis into the skin’s second layer (the dermis) 4).
The most common cause of melanoma is attributed to ultraviolet radiation (UV) exposure, family history, and personal history of melanoma 5). In 2016, the World Health Organization (WHO) reported that the incidence of skin cancer is on the rise due to the excessive UV rays that individuals are being exposed to. Additionally, lighter skinned people who have lack of skin pigmentation have a much higher risk of getting nonmelanoma or melanoma skin cancers than compared to dark-skinned patients, due to their increased risk of UV-induced sunburn skin damage 6).
Melanomas can develop anywhere on the skin, but they are more likely to start on the trunk (chest and back) in men and on the legs in women. The neck and face are other common sites.
Having darkly pigmented skin lowers your risk of melanoma at these more common sites, but anyone can get melanoma on the palms of the hands, soles of the feet, and under the nails. Melanomas in these areas make up a much larger portion of melanomas in African Americans than in whites.
Melanomas can also form in other parts of your body such as the eyes, mouth, genitals, and anal area, but these are much less common than melanoma of the skin.
Melanoma is much less common than basal cell and squamous cell skin cancers. But melanoma is more dangerous because it’s much more likely to spread to other parts of the body if not caught early.
Most melanoma cells still make melanin, so melanoma tumors are usually brown or black. But some melanomas do not make melanin and can appear pink, tan, or even white.
Metastatic melanoma staging
The staging system most often used for melanoma is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
The extent of the tumor (T): How deep has the cancer grown into the skin? Is the cancer ulcerated?
- Tumor thickness: The thickness of the melanoma is called the Breslow measurement. In general, melanomas less than 1 millimeter (mm) thick (about 1/25 of an inch) have a very small chance of spreading. As the melanoma becomes thicker, it has a greater chance of spreading.
- Ulceration: Ulceration is a breakdown of the skin over the melanoma. Melanomas that are ulcerated tend to have a worse outlook.
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant lymph nodes or distant organs such as the lungs or brain?
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The staging system in the table below uses the pathologic stage (also called the surgical stage). It is determined by examining tissue removed during an operation. Sometimes, if surgery is not possible right away or at all, the cancer will be given a clinical stage instead. This is based on the results of a physical exam, biopsy, and imaging tests. The clinical stage will be used to help plan treatment. Sometimes, though, the cancer has spread further than the clinical stage estimates, and may not predict the patient’s outlook as accurately as a pathologic stage.
There are both clinical and pathologic staging systems for melanoma. Since most cancers are staged with the pathologic stage, we have included that staging system below. If your cancer has been clinically staged, it is best to talk to your doctor about your specific stage.
The table below is a simplified version of the TNM system. It is based on the most recent American Joint Committee on Cancer (AJCC) system, effective January 2018. It’s important to know that melanoma cancer staging can be complex. If you have any questions about the stage of your cancer or what it means, please ask your doctor to explain it to you in a way you understand.
Table 1. American Joint Committee on Cancer (AJCC) TNM system for Melanoma
| AJCC Stage | Melanoma Stage description | |
| 0 | The cancer is confined to the epidermis, the outermost skin layer. It has not spread to nearby lymph nodes or distant sites. This stage is also known as melanoma in situ. | |
| I
| The cancer is no more than 2mm (2/25 of an inch) thick and might or might not be ulcerated. It has not spread to nearby lymph nodes or to distant sites. | |
| II | The cancer is at least 1.01 mm and may be thicker than 4.0 mm. It might or might not be ulcerated. It has not spread to nearby lymph nodes (N0) or to distant sites (M0).
| |
| IIIA | The cancer is no more than 2.0 mm thick. It might or might not be ulcerated. It has spread to 3 or less lymph node(s), but it is so small that it is only seen under the microscope. It has not spread to distant sites. | |
| IIIB
| There is no sign of the primary cancer AND:
It has not spread to distant sites. | |
| OR | ||
The cancer is no more than 4.0 mm thick. It might or might not be ulcerated AND:
It has not spread to distant sites. | ||
| IIIC | There is no sign of the primary cancer AND:
It has not spread to distant sites. | |
| OR | ||
The cancer is no more than 4.0 mm thick. It might or might not be ulcerated AND:
It has not spread to distant sites. | ||
| OR | ||
The cancer is between 2.1 and 4.0mm OR thicker than 4.0 mm. It might or might not be ulcerated AND:
It has not spread to distant sites. | ||
| OR | ||
The cancer is thicker than 4.0 mm and is ulcerated AND:
It has not spread to distant sites. | ||
| IIID | The cancer is thicker than 4.0 mm and is ulcerated AND:
It has not spread to distant sites. | |
| IV | The cancer can be any thickness and might or might not be ulcerated. It might or might not have spread to nearby lymph nodes. It has spread to distant lymph nodes or organs such as the lungs, liver or brain. | |
Metastatic melanoma life expectancy
The 5-year survival rate for a metastatic melanoma is about 15% to 20% 7). The 10-year survival is about 10% to 15% 8). The outlook is better if the spread is only to distant parts of the skin or distant lymph nodes rather than to other organs, and if the blood level of lactate dehydrogenase (LDH) is normal.
- The survival differences among M categories will be useful for clinical trial stratification; however, the overall prognosis of all patients with stage IV melanoma remains poor, even among patients with M1a. For this reason, the Melanoma Staging Committee recommended no stage groupings for stage IV.
Table 2. American Joint Committee on Cancer (AJCC) TNM system (M category) for Stage 4 Melanoma
| M (metastasis) | Site | Serum LDH |
|---|---|---|
| M0 | No distant metastases | NA |
| M1a | Distant skin, subcutaneous, or nodal metastases | Normal |
| M1b | Lung metastases | Normal |
| M1c | All other visceral metastases | Normal |
| Any distant metastasis | Elevated |
Abbreviations: NA = not applicable; LDH = lactate dehydrogenase.
[Source 9)]Staging for Distant Metastatic Melanoma (stage 4)
In patients with distant metastases, the site(s) of metastases and elevated serum levels of lactate dehydrogenase (LDH) are used to delineate the M1 stage into three M categories: M1a, M1b, and M1c. One-year survival rates among 7,972 stage 4 patients were 62% for M1a, 53% for M1b, and 33% for M1c melanomas (see Figure 1A) 10).
Patients with distant metastasis in the skin, subcutaneous tissue, or distant lymph nodes and a normal LDH level are categorized as M1a; they have a relatively better prognosis compared with those patients with metastases located in any other distant anatomic site (see Figure 1A) 11). Patients with metastasis to the lung (or with a combination of lung and skin or subcutaneous metastases) and a normal LDH level are categorized as M1b and have an intermediate prognosis. Those patients with metastases to any other visceral sites or at any location with an elevated LDH level are designated as M1c and have the worst prognosis (see Figure 1A and 1B).
Elevated serum LDH
The updated AJCC Melanoma Staging Database demonstrated that an elevated serum LDH is an independent and highly significant predictor of survival outcome among patients with stage IV disease. Thus 1- and 2-year overall survival rates for those stage IV patients in the 2008 AJCC Melanoma Staging Database with a normal serum LDH were 65% and 40%, respectively, compared with 32% and 18%, respectively, when the serum LDH was elevated at the time of staging (Figure 1B). Therefore, serum LDH should be measured at the time stage IV disease is documented, and if the LDH level is elevated, those patients are assigned to M1c regardless of the site of their distant metastases.
Factors other than stage can also affect survival. For example:
- Older people generally have shorter survival times than younger people, regardless of stage.
- Melanoma is uncommon among African Americans, but when it does occur, survival times tend to be shorter than when it occurs in whites. Some studies have found that melanoma tends to be more serious if it occurs on the sole of the foot or palm of the hand, or if it is in a nail bed. (Cancers in these areas make up a larger portion of melanomas in African Americans than in whites.)
- People with melanoma who have weakened immune systems, such as people who have had organ transplants or who are infected with HIV, also are at greater risk of dying from their melanoma.
Figure 1. Metastatic melanoma life expectancy
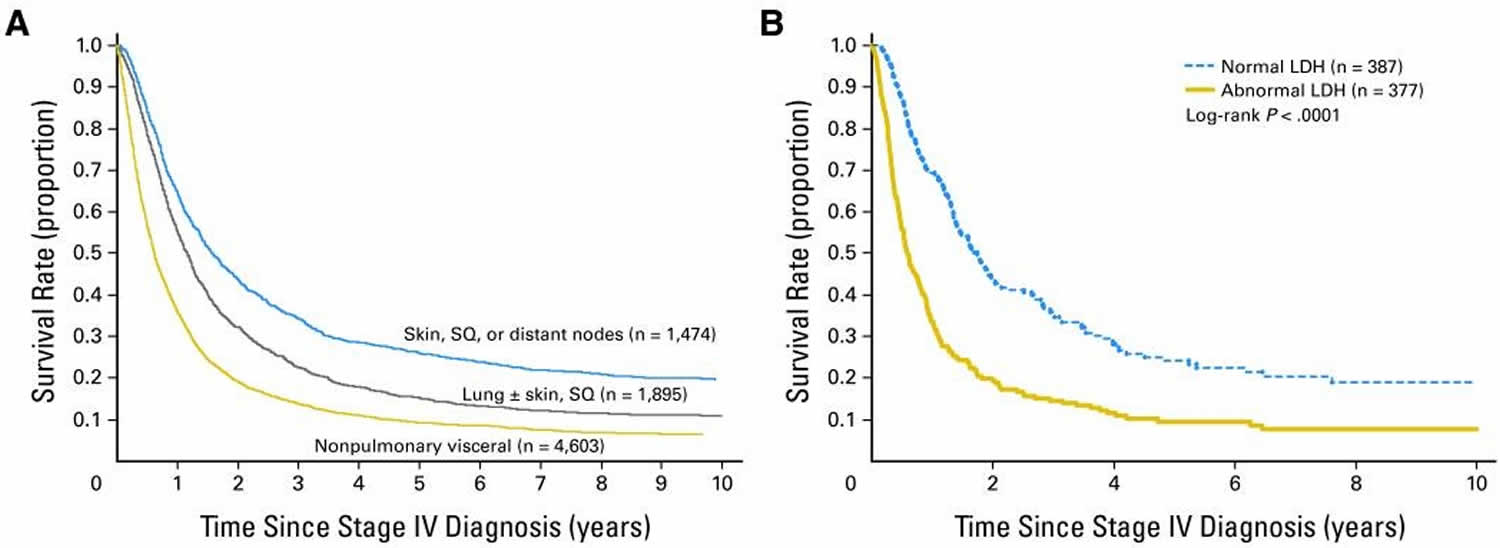 Footnote: Survival curves of 7,635 patients with metastatic melanomas at distant sites (stage 4) subgrouped by (A) the site of metastatic disease and (B) serum lactose dehydrogenase (LDH) levels. LDH values are not used to stratify patients. Curves in (A) are based only on site of metastasis. The number of patients is shown in parentheses.
Footnote: Survival curves of 7,635 patients with metastatic melanomas at distant sites (stage 4) subgrouped by (A) the site of metastatic disease and (B) serum lactose dehydrogenase (LDH) levels. LDH values are not used to stratify patients. Curves in (A) are based only on site of metastasis. The number of patients is shown in parentheses.SQ = subcutaneous.
[Source 12)]Metastatic melanoma prognosis
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The thickness of the tumor and where it is in the body.
- How quickly the cancer cells are dividing.
- Whether there was bleeding or ulceration of the tumor.
- How much cancer is in the lymph nodes.
- The number of places cancer has spread to in the body.
- The level of lactate dehydrogenase (LDH) in the blood.
- Whether the cancer has certain mutations (changes) in a gene called BRAF.
- The patient’s age and general health.
Metastatic melanoma symptoms
The most important warning sign of melanoma is a new spot on the skin or a spot that is changing in size, shape, or color. Another important sign is a spot that looks different from all of the other spots on your skin (known as the ugly duckling sign). If you have one of these warning signs, have your skin checked by a doctor.
The ABCDE rule is another guide to the usual signs of melanoma. Be on the lookout and tell your doctor about spots that have any of the following features:
- A is for Asymmetry: One half of a mole or birthmark does not match the other.
- B is for Border: The edges are irregular, ragged, notched, or blurred.
- C is for Color: The color is not the same all over and may include different shades of brown or black, or sometimes with patches of pink, red, white, or blue.
- D is for Diameter: The spot is larger than 6 millimeters across (about ¼ inch – the size of a pencil eraser), although melanomas can sometimes be smaller than this.
- E is for Evolving: The mole is changing in size, shape, or color.
Some melanomas don’t fit these rules. It’s important to tell your doctor about any changes or new spots on the skin, or growths that look different from the rest of your moles.
Other warning signs are:
- A sore that doesn’t heal
- Spread of pigment from the border of a spot into surrounding skin
- Redness or a new swelling beyond the border of the mole
- Change in sensation, such as itchiness, tenderness, or pain
- Change in the surface of a mole – scaliness, oozing, bleeding, or the appearance of a lump or bump
Be sure to show your doctor any areas that concern you and ask your doctor to look at areas that may be hard for you to see. It’s sometimes hard to tell the difference between melanoma and an ordinary mole, even for doctors, so it’s important to show your doctor any mole that you are unsure of.
Metastatic melanoma in the brain
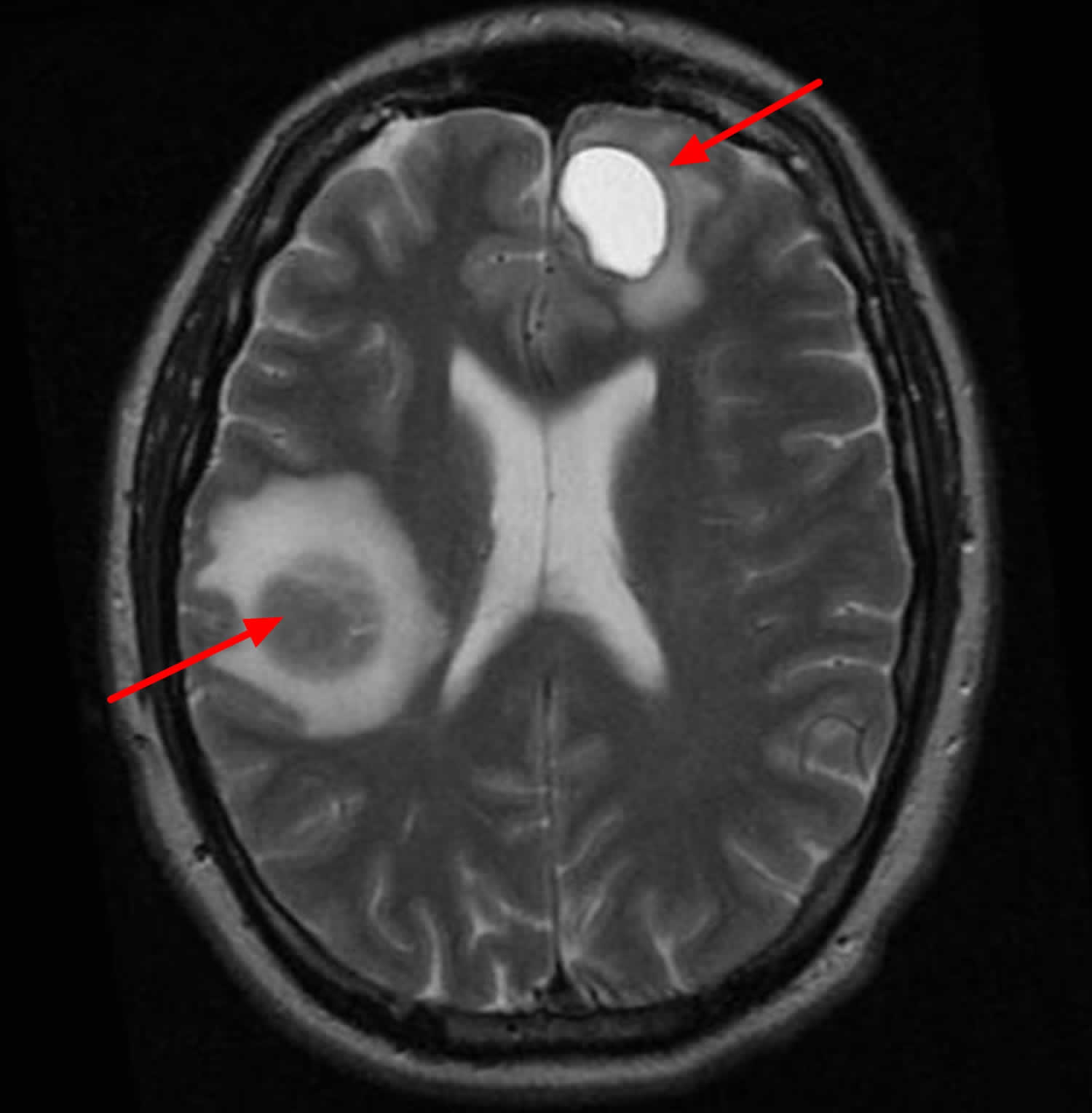
These patients can commonly present with headaches, seizures, mental status alterations, ataxia, nausea and vomiting, and visual disturbances. However, 10% of patients may be asymptomatic.
Figure 2. Metastatic melanoma in the brain (MRI scan)
Metastatic melanoma treatment
Stage 4 metastatic melanomas are often hard to cure, as they have already spread to distant lymph nodes or other areas of the body. Skin tumors or enlarged lymph nodes causing symptoms can often be removed by surgery or treated with radiation therapy.
Metastases in internal organs are sometimes removed, depending on how many there are, where they are, and how likely they are to cause symptoms. Metastases that cause symptoms but cannot be removed may be treated with radiation, immunotherapy, targeted therapy, or chemotherapy.
The treatment of metastatic melanomas has changed in recent years as newer forms of immunotherapy and targeted drugs have been shown to be more effective than chemotherapy.
Immunotherapy drugs called checkpoint inhibitors such as pembrolizumab (Keytruda), nivolumab (Opdivo), and ipilimumab (Yervoy) have been shown to help some people with advanced melanoma live longer. These drugs can sometimes have serious side effects, so patients who get them need to be watched closely. Other types of immunotherapy might also help, but these are only available through clinical trials (https://www.cancer.gov/about-cancer/treatment/clinical-trials).
In about half of all melanomas, the cancer cells have changes in the BRAF gene. If this gene change is found, treatment with newer targeted therapy drugs – typically a combination of a BRAF inhibitor and a MEK inhibitor – might be helpful. They might be tried before or after the newer immunotherapy drugs, but they aren’t used at the same time. Like the checkpoint inhibitors, these drugs can help some people live longer, although they haven’t been shown to cure these melanomas.
A small portion of melanomas have changes in the C-KIT gene. These melanomas might be helped by targeted drugs such as imatinib (Gleevec) and nilotinib (Tasigna), although, again, these drugs aren’t known to cure these melanomas.
Immunotherapy using interferon or interleukin-2 can help a small number of people with stage IV melanoma live longer. Higher doses of these drugs seem to be more effective, but they can also have more severe side effects, so they might need to be given in the hospital.
Chemotherapy can help some people with stage IV melanoma, but other treatments are usually tried first. Dacarbazine (DTIC) and temozolomide (Temodar) are the chemo drugs used most often, either by themselves or combined with other drugs. Even when chemotherapy shrinks these cancers, the cancer usually starts growing again within several months.
Some doctors may recommend biochemotherapy, which is a combination of chemotherapy and either interleukin-2, interferon, or both. This can often shrink tumors, which might make patients feel better, although it has not been shown to help patients live longer.
It’s important to carefully consider the possible benefits and side effects of any recommended treatment before starting it.
Because stage 4 melanoma is hard to cure with current treatments, patients may want to think about taking part in a clinical trial (https://www.cancer.gov/about-cancer/treatment/clinical-trials). Many studies are now looking at new targeted drugs, immunotherapies, chemotherapy drugs, and combinations of different types of treatments.
Even though stage 4 melanoma is often hard to cure, a small portion of people respond very well to treatment and survive for many years after diagnosis.
References [ + ]





{kind=link}