Contents
What is MRSA infection
MRSA is methicillin-resistant Staphylococcus aureus, a type of staph bacteria that is resistant to many antibiotics. You might have heard it called a “superbug”. Staph and MRSA can cause a variety of problems ranging from are skin infections and sepsis to pneumonia to bloodstream infections. MRSA infections mainly affect people who are staying in hospital. They can be serious, but can usually be treated with antibiotics that work against MRSA.
Staphylococcus aureus bacteria are amongst the populations of bacteria normally found existing on your skin surface. However, over time, various populations of these bacteria have become resistant to a number of antibiotics, which makes them very difficult to fight when attempting to treat infections where MRSA bacteria are the responsible pathogens. These antibiotics include methicillin and other more common antibiotics such as oxacillin, penicillin and amoxicillin.
MRSA lives harmlessly on the skin of around 1 in 30 people – usually in the nose, armpits, groin or buttocks. This is known as “colonisation” or “carrying” MRSA.
You can get MRSA on your skin by:
- touching someone who has it
- sharing things like towels, sheets and clothes with someone who has MRSA on their skin
- touching surfaces or objects that have MRSA on them
Getting MRSA on your skin won’t make you ill, and it may go away in a few hours, days, weeks or months without you noticing. But MRSA could cause an infection if it gets deeper into your body.
People staying in hospital are most at risk of this happening because:
- they often have a way for the bacteria to get into their body, such as a wound, burn, feeding tube, drip into a vein, or urinary catheter
- they may have other serious health problems that mean their body is less able to fight off the bacteria
- they’re in close contact with a large number of people, so the bacteria can spread more easily
Healthy people (including children and pregnant women) aren’t usually at risk of MRSA infections.
However, Methicillin-resistant Staphylococcus aureus (MRSA) has emerged as a cause of skin infections and, less commonly, invasive infections among otherwise healthy adults and children in the community. In the general community, MRSA most often causes skin infections. In some cases, MRSA causes pneumonia (lung infection) and other issues. If left untreated, MRSA infections can become severe and cause MRSA blood infection (sepsis) – a life-threatening reaction to severe infection in the body.
In a healthcare setting, such as a hospital or nursing home, MRSA can cause severe problems such as bloodstream infections, pneumonia and surgical site infections.
Studies show that about one in three people carry staph in their nose, usually without any illness. Two in 100 people carry MRSA. There are not data showing the total number of people who get MRSA skin infections in the community.
Figure 1. MRSA bacteria (Methicillin Resistant Staphylococcus Aureus) under scanning electron micrograph

MRSA infection is highly contagious
Anyone can get MRSA on their body from contact with an infected wound or by sharing personal items, such as towels or razors, that have touched infected skin. MRSA infection risk can be increased when a person is in activities or places that involve crowding, skin-to-skin contact, and shared equipment or supplies. People including athletes, daycare and school students, military personnel in barracks, and those who recently received inpatient medical care are at higher risk.
How To Prevent Spreading MRSA infection
- Cover your wounds. Keep wounds covered with clean, dry bandages until healed. Follow your doctor’s instructions about proper care of the wound. Pus from infected wounds can contain MRSA so keeping the infection covered will help prevent the spread to others. Bandages and tape can be thrown away with the regular trash.
- Do NOT try to treat the infection yourself by picking or popping the sore.
- Clean your hands often. You, your family, and others in close contact should wash their hands often with soap and water or use an alcohol-based hand rub, especially after changing the bandage or touching the infected wound.
- Do not share personal items. Personal items include towels, washcloths, razors and clothing, including uniforms.
- Wash used sheets, towels, and clothes with water and laundry detergent. Use a dryer to dry them completely.
- Wash clothes according to manufacturer’s instructions on the label. Clean your hands after touching dirty clothes.
What is MRSA skin infection
MRSA skin infections often appear as wounds or boils that are red, swollen, painful, or that have pus or other drainage. Many people first think they have spider bites. These infections commonly happen where skin has been cut or wounded, and on areas covered by hair (e.g., back of neck, groin, buttocks, armpit, beard area).
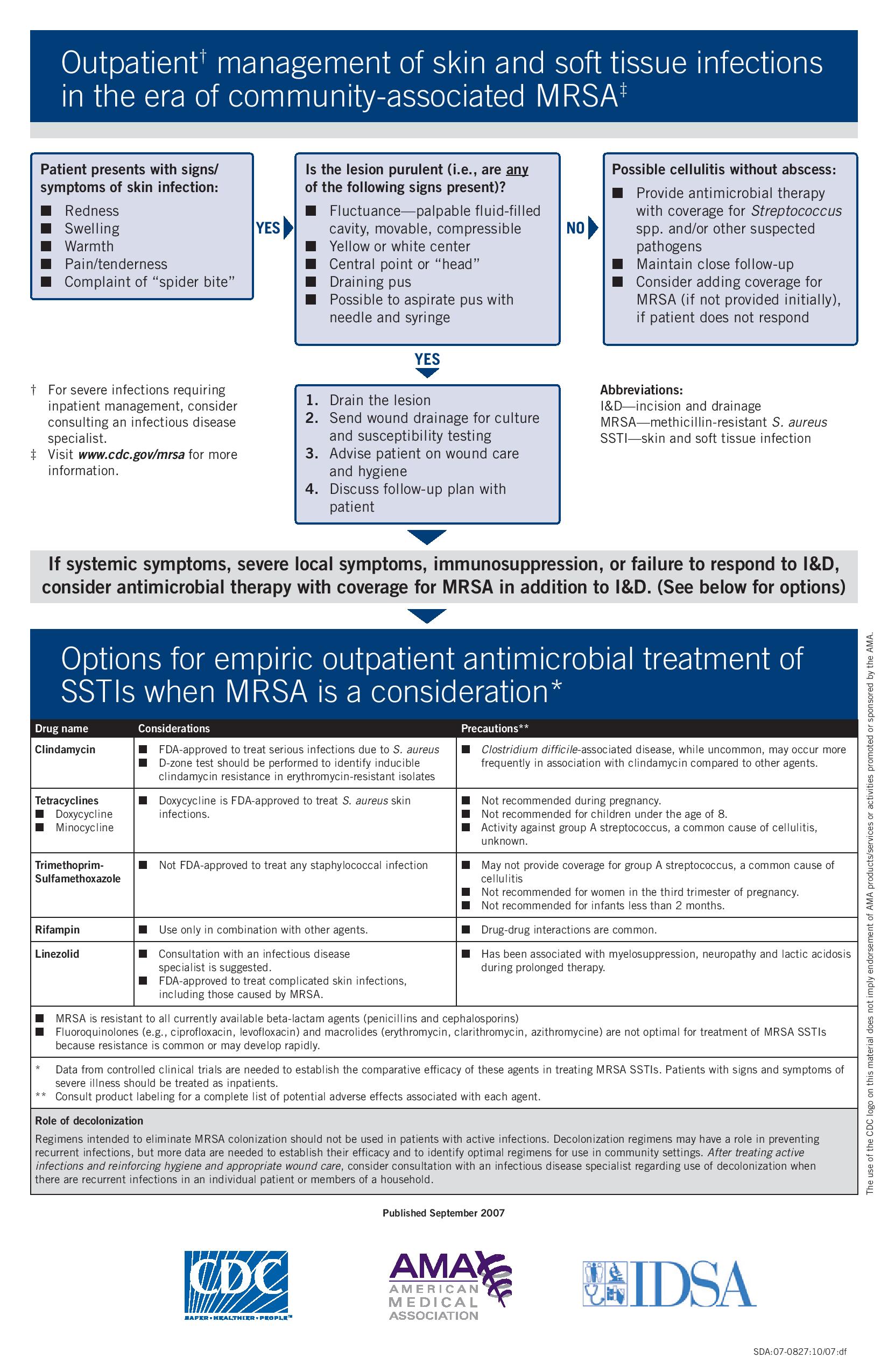
Recent data suggest that MRSA as a cause of skin infections in the general community remains at high probability. The spectrum of disease caused by MRSA appears to be similar to that of Staphylococcus aureus in the community. Skin and soft tissue infections specifically furuncles (abscessed hair follicles or “boils”), carbuncles (coalesced masses of furuncles) and abscesses, are the most frequently reported clinical manifestations. The role of MRSA in cellulitis without abscess or purulent drainage is less clear since cultures are rarely obtained.
The severity of MRSA skin and soft tissue infections varies from mild superficial infections to deeper soft-tissue abscesses requiring hospital admission for surgical incision and drainage and delivery of parenteral antibiotics 1. Anecdotal reports suggest that recurrent MRSA skin infections and clustering of infections within a household are relatively common occurrences.
Less commonly, MRSA has been associated with severe and invasive staphylococcal infections in the community, including necrotizing pneumonia and empyema (pus in chest cavity), sepsis syndrome, musculoskeletal infections including pyomyositis and osteomyelitis, necrotizing fasciitis, purpura fulminans and disseminated infections with septic emboli. Invasive manifestations occur as complications of preceding skin and soft tissue infections or viral respiratory tract infections (particularly influenza), as well as in otherwise healthy persons without recognized preceding infections or risk factors.
Incidence of community acquired MRSA varies geographically in the United States. To date, reported community acquired MRSA infections have disproportionately affected children and young adults and individuals from racial minority groups or low socioeconomic status. Transmission of MRSA has occurred among inmates in correctional facilities, competitive sports participants, military recruits, day care attendees, men who have sex with men and Native Americans. Factors common to these settings that facilitate the spread of infection include crowding, frequent skin-to-skin contact between individuals, participation in activities that result in compromised skin surfaces, sharing of personal items that may become contaminated with wound drainage, and challenges in maintaining personal cleanliness and hygiene. Limited access to health care and frequent antibiotic exposure may also facilitate spread of MRSA infection in some settings.
Unlike hospital acquired MRSA isolates, which are usually resistant in vitro to multiple classes of antimicrobial agents, many community acquired MRSA isolates to date have been resistant only to beta-lactams (the antimicrobial class that includes penicillins and cephalosporins) and macrolides / azalides (e.g., erythromycin, clarithromycin, azithromycin) 2. However, resistance to other classes of antimicrobial agents, such as fluoroquinolones and tetracyclines, occurs and may be increasing in prevalence 2. Most community acquired MRSA isolates to date have been susceptible to trimethoprim-sulfamethoxazole (TMP/SMX), gentamicin, tetracycline, and clindamycin, although some Staphylococcus aureus isolates that appear erythromycin-resistant and clindamycin-susceptible by routine susceptibility testing exhibit in vitro resistance to clindamycin during therapy (“inducible resistance”) 3.
Community acquired MRSA isolates commonly possess genes for the Panton-Valentine leukocidin (PVL) toxin, rarely identified in hospital acquired MRSA isolates 4. Presence of Panton-Valentine leukocidin genes in Staphylococcus aureus isolates has been associated with primary skin infections 5, severe necrotizing pneumonia 5 and increased complications of hematogenous osteomyelitis 6; however, the role of Panton-Valentine leukocidin in the pathogenesis of Staphylococcus aureus infections has not been fully elucidated.
Data from controlled clinical trials are needed to establish optimal therapy for MRSA skin and soft tissue infections. Various antimicrobial agents, including clindamycin, TMP/SMX, tetracyclines, and linezolid have been used for empiric outpatient treatment of skin and soft tissue infections possibly caused by MRSA. Incision and drainage alone may be adequate therapy for some previously healthy patients with cutaneous abscesses and no systemic signs of infection. In recent investigations, receiving an antimicrobial agent to which the infecting isolate was later found to be resistant was not associated with adverse outcomes among immune-competent patients with community acquired-MRSA skin and soft tissue infections. Furthermore, in a recent randomized, placebo-controlled trial in adult patients with deep skin abscesses and surrounding cellulitis, the majority of which were caused by MRSA, treatment success rates were over 90% for patients treated with incision and drainage alone and those treated with incision and drainage plus cephalexin.
It is not known if antimicrobial therapy of less serious skin infections prevents invasive complications.
Figure 2. MRSA skin infection – cutaneous abscess on the foot

Figure 3. MRSA skin infection – cutaneous abscess on the back

Figure 4. MRSA skin infection – cutaneous abscess on the hand

Figure 5. MRSA skin infection – cutaneous abscess

What should I do if I think I have a MRSA skin infection?
- You can’t tell by looking at the skin if it is a staph infection (including MRSA).
- See your doctor if you think you have an infection. Finding infections early and getting care make it less likely that the infection will become severe.
- Do NOT try to treat the infection yourself by picking or popping the sore.
- Cover possible infections with clean, dry bandages until you can be seen by a doctor, nurse, or other health care provider.
MRSA infection complications
MRSA infections can resist the effects of many common antibiotics, so they are more difficult to treat. This can allow the infections to spread and sometimes become life-threatening.
MRSA infections may affect your:
- Bloodstream
- Lungs
- Heart
- Bones
- Joints
MRSA infection causes
Different varieties of Staphylococcus aureus bacteria, commonly called “staph,” exist. Staph bacteria are normally found on the skin or in the nose of about one-third of the population. The bacteria are generally harmless unless they enter the body through a cut or other wound, and even then they usually cause only minor skin problems in healthy people.
According to the Centers for Disease Control and Prevention, less than 2 percent of the population chronically carries the type of staph bacteria known as MRSA.
Antibiotic resistance
MRSA is the result of decades of often unnecessary antibiotic use. For years, antibiotics have been prescribed for colds, flu and other viral infections that don’t respond to these drugs. Even when antibiotics are used appropriately, they contribute to the rise of drug-resistant bacteria because they don’t destroy every germ they target. Bacteria live on an evolutionary fast track, so germs that survive treatment with one antibiotic soon learn to resist others.
Risk factors MRSA infection
Because hospital and community strains of MRSA generally occur in different settings, the risk factors for the two strains differ.
Risk factors for community acquired-MRSA infection
Participating in contact sports. MRSA can spread easily through cuts and abrasions and skin-to-skin contact.
Living in crowded or unsanitary conditions. Outbreaks of MRSA have occurred in military training camps, child care centers and jails.
Men having sex with men. Homosexual men have a higher risk of developing MRSA infections.
Risk factors for hospital acquired-MRSA infection
Being hospitalized. MRSA remains a concern in hospitals, where it can attack those most vulnerable — older adults and people with weakened immune systems.
Having an invasive medical device. Medical tubing — such as intravenous lines or urinary catheters — can provide a pathway for MRSA to travel into your body.
Residing in a long-term care facility. MRSA is prevalent in nursing homes. Carriers of MRSA have the ability to spread it, even if they’re not sick themselves.
Preventing MRSA
Preventing community acquired-MRSA
- Wash your hands. Careful hand washing remains your best defense against germs. Scrub hands briskly for at least 15 seconds, then dry them with a disposable towel and use another towel to turn off the faucet. Carry a small bottle of hand sanitizer containing at least 62 percent alcohol for times when you don’t have access to soap and water.
- Keep wounds covered. Keep cuts and abrasions clean and covered with sterile, dry bandages until they heal. The pus from infected sores may contain MRSA, and keeping wounds covered will help prevent the bacteria from spreading.
- Keep personal items personal. Avoid sharing personal items such as towels, sheets, razors, clothing and athletic equipment. MRSA spreads on contaminated objects as well as through direct contact.
- Shower after athletic games or practices. Shower immediately after each game or practice. Use soap and water. Don’t share towels.
- Sanitize linens. If you have a cut or sore, wash towels and bed linens in a washing machine set to the hottest water setting (with added bleach, if possible) and dry them in a hot dryer. Wash gym and athletic clothes after each wearing.
Preventing hospital acquired-MRSA
In the hospital, people who are infected or colonized with MRSA often are placed in contact precautions as a measure to prevent the spread of MRSA. Visitors and health care workers caring for people in isolation may be required to wear protective garments and must follow strict hand hygiene procedures. Contaminated surfaces and laundry items should be properly disinfected.
If you’re staying in hospital, there are some simple things you can do to reduce your risk of getting or spreading MRSA.
You should:
- wash your hands often (hand wipes and alcohol hand gel are also effective) – especially before and after eating and after going to the toilet
- follow the advice you’re given about wound care and looking after devices that could lead to infection (such as urinary catheters or drips)
- report any unclean facilities to staff – don’t be afraid to talk to staff if you’re concerned about hygiene
If you’re visiting someone in hospital, clean your hands before and after entering the ward and before touching the person. Gel or wipes are often placed by patients’ beds and at the entrance to wards.
It’s also a good idea to put a dressing over any breaks in your skin, such as sores or cuts, to stop MRSA getting into your body.
MRSA infection symptoms
Having MRSA on your skin doesn’t cause any symptoms and doesn’t make you ill. You won’t usually know if you have it unless you have a screening test before going into hospital.
If MRSA gets deeper into your skin, it can cause:
- Redness
- Swelling
- Pain
- Warmth to the touch
- Full of pus or other drainage
- Accompanied by a fever
Most staph skin infections, including MRSA, appear as a bump or infected area on the skin.
Sometimes people with MRSA skin infections first think they have a spider bite. However, unless a spider is actually seen, the irritation is likely not a spider bite.
If you or someone in your family experiences these signs and symptoms, cover the area with a bandage, wash your hands, and contact your doctor. It is especially important to see your doctor if signs and symptoms of an MRSA skin infection are accompanied by a fever.
If MRSA staph infection gets further into your body, it can also cause:
- a high temperature of 100.4 °F (38 °C ) or above
- chills
- aches and pains
- dizziness
- confusion
MRSA skin infection treatment
In the community, incision and drainage remains the primary therapy for these purulent skin infections. Empiric antimicrobial coverage for MRSA may be warranted in addition to incision and drainage based on clinical assessment (e.g., presence of systemic symptoms, severe local symptoms, immune suppression, extremes of patient age, infections in a difficult to drain area, or lack of response to incision and drainage alone). In some cases, antibiotics may not be necessary. For example, doctors may drain a superficial abscess caused by MRSA rather than treat the infection with drugs.
Antibiotic treatment, if indicated, should be guided by the susceptibility profile of the MRSA bacteria. Obtaining specimens for culture and susceptibility testing is useful to guide therapy, particularly for those with more severe infections and those who fail to respond adequately to initial management.
- If you get an MRSA infection, you’ll usually be treated with antibiotics that work against MRSA.
- These may be taken as tablets or given as injections. Treatment can last a few days to a few weeks.
- During treatment, you may need to stay in your own room or in a ward with other people who have an MRSA infection to help stop it spreading.
- You can normally still have visitors, but it’s important they take precautions to prevent MRSA spreading.
MRSA skin infections can develop into more serious infections. It is important to discuss a follow-up plan with your doctor in case you develop systemic symptoms (MRSA blood infection) or worsening local symptoms, or if symptoms do not improve within 48 hours.
MRSA infection treatment
Treatments for MRSA
Removing MRSA from your skin
If screening finds MRSA on your skin, you may need treatment to remove it. This is known as decolonization.
This usually involves:
- applying antibacterial cream inside your nose three times a day for five days
- washing with an antibacterial shampoo every day for five days
- changing your towel, clothes and bedding every day during treatment – the resulting laundry should be washed separately from other people’s and at a high temperature
Treatment is normally done at home, but may be started after going into hospital if you need to be admitted quickly.
- Frazee BW, Lynn J, Charlebois ED, Lambert L, Lowery D, Perdreau-Remington F. High prevalence of methicillin-resistant Staphylococcus aureus in emergency department skin and soft tissue infections. Ann Emerg Med. Mar 2005;45(3):311-320.[↩]
- Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistant Staphylococcus aureus disease in three communities. N Engl J Med. Apr 7 2005;352(14):1436-1444.[↩][↩]
- Lewis JS, 2nd, Jorgensen JH. Inducible clindamycin resistance in Staphylococci: should clinicians and microbiologists be concerned? Clin Infect Dis. Jan 15 2005;40(2):280-285.[↩]
- Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. Jama. Dec 10 2003;290(22):2976-2984.[↩]
- Lina G, Piemont Y, Godail-Gamot F, et al. Involvement of Panton-Valentine leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis. Nov 1999;29(5):1128-1132.[↩][↩]
- Martinez-Aguilar G, Avalos-Mishaan A, Hulten K, Hammerman W, Mason EO, Jr., Kaplan SL. Community-acquired, methicillin-resistant and methicillin-susceptible Staphylococcus aureus musculoskeletal infections in children. Pediatr Infect Dis J. Aug 2004;23(8):701-706.[↩]





 has emerged as a cause of skin infections){kind=link}