Contents
- Multiple system atrophy
- Who gets multiple system atrophy?
- Will my children or family get multiple system atrophy?
- How are the nerve cells in the brain damaged by multiple system atrophy?
- Why do nerve cells become damaged?
- How is multiple system atrophy different from Parkinson’s disease?
- What are the earliest signs of multiple system atrophy?
- Will I experience cognitive difficulties?
- Can I still travel abroad on holidays?
- Is there a diet for multiple system atrophy?
- Multiple system atrophy types
- Multiple system atrophy causes
- Multiple system atrophy signs and symptoms
- Multiple system atrophy complications
- Multiple system atrophy diagnosis
- Multiple system atrophy differential diagnosis
- Multiple system atrophy treatment
- Multiple system atrophy prognosis
Multiple system atrophy
Multiple System Atrophy (MSA) previously known as Shy-Drager syndrome, sporadic olivopontocerebellar atrophy or striatonigral degeneration is a rare, progressive neurological disorder that causes a gradual loss of nerve cells in your brain and spinal cord (central nervous system) that control movement and involuntary actions (autonomic functions) such as blood pressure and bladder control leading to problems similar to Parkinson’s disease symptoms with movement disorder like slow movement, stiffness, and lack of coordination, balance problem, and involuntary body function disorders such as blood pressure and bladder control 1, 2, 3, 4, 5, 6, 7, 8, 9, 10. The autonomic nervous system controls body functions that are mostly involuntary, such as regulation of blood pressure. The most frequent autonomic symptoms associated with multiple system atrophy are a sudden drop in blood pressure upon standing (orthostatic hypotension), urinary difficulties, and erectile dysfunction in men.
Multiple system atrophy (MSA) symptoms affect many parts of the body and symptoms usually begin in adulthood in people between the ages of 50 and 60 and it is seen slightly more frequently in males; however, females, younger and older cases have occurred.
The exact cause of multiple system atrophy is unknown, but multiple system atrophy is characterized by the accumulation of a protein called alpha-synuclein build up in cells in many parts of the brain and spinal cord 11. Over time, these clumps which are known as glial cytoplasmic inclusions (GCIs) damage cells in parts of the nervous system that control movement, balance and coordination, and autonomic functioning 12, 13, 14. The progressive loss of cells in these regions underlies the major features of multiple system atrophy. It is believed that a combination of genetic and environmental factors likely contributes to the development and progression of multiple system atrophy (MSA).
Researchers have described 2 major types of multiple system atrophy, which are distinguished by their major signs and symptoms at the time of diagnosis 15.
- Multiple system atrophy- parkinsonian type (MSA-P): Primarily affects the basal ganglia, causing movement-related symptoms like Parkinson’s disease leading to problems with coordination and balance. These abnormalities include unusually slow movement (bradykinesia), muscle rigidity, tremors, and an inability to hold the body upright and balanced (postural instability). However, people with multiple system atrophy – parkinsonian type (MSA-P) have more widespread damage to the part of the autonomic nervous system that regulates important functions such as heart rate, blood pressure, and sweating.
- Multiple system atrophy – cerebellar type (MSA-C): Affects the cerebellum that is characterized by cerebellar ataxia, which causes problems with coordination and balance. Multiple system atrophy – cerebellar type (MSA-C) can also include speech difficulties (dysarthria) and problems controlling eye movement. Multiple system atrophy – cerebellar type (MSA-C) used to be known as olivopontocerebellar atrophy (OPCA).
Multiple system atrophy symptoms vary depending on which part of the brain is affected, but common symptoms include:
- Movement problems: Slowed movement, muscle stiffness, and rigidity, similar to Parkinson’s disease.
- Balance and coordination issues: Clumsiness, unsteadiness, and a wide-based gait.
- Stiffness in the hands or limbs caused by contractures (chronic shortening of muscles or tendons around joints, which prevents the joints from moving freely)
- Autonomic nervous system dysfunction: Problems with blood pressure regulation, such as fainting or lightheadedness when standing, and bladder control problems.
- Voice problems: A croaky or quivering voice.
- Sleep disturbances: Including noisy breathing and sleep apnea.
- Swallowing and chewing difficulties: Leading to a risk of aspiration and pneumonia.
- Bowel problems: Constipation and difficulty with bowel control.
- Emotional changes: Unpredictable laughing or crying.
- REM sleep behavior disorder (RBD): Many people with Multiple system atrophy have a history of acting out their dreams
- A posture in which the body leans involuntarily to one side known as Pisa syndrome
- Anterocollis, in which the neck bends forward and the head drops down
- Anxiety or depression
Multiple system atrophy is a progressive disease, and the condition worsens over time. People with multiple system atrophy may eventually require assistive devices for walking and may become bedridden.
Multiple system atrophy is a rare disease. Each year, about 0.6 people out of every 100,000 are newly diagnosed 16. In people over 50, the rate is a little higher, about 3 cases per 100,000 16. The peak onset of multiple system atrophy is between 55 to 60 years of age with a range from 30 to over 90 years 16.
In the United States, it is estimated that multiple system atrophy affects about 15,000 to 50,000 people 17. Most people start to have symptoms in their 50s or early 60s. Males and females are affected about equally, though some studies show males may be diagnosed more often (possibly because early symptoms like impotence are easier to spot in males).
Multiple system atrophy affects people of all races and ethnicities and has been reported worldwide. There are no proven environmental risks. A risk factor for multiple system atrophy is having rapid eye movement sleep behavior disorder (RBD). Rapid eye movement sleep behavior disorder (RBD) is a sleep disorder where people act out their dreams due to a loss of normal muscle paralysis (atonia) during rapid eye movement (REM) sleep 18, 19, 20. Another risk factor is having a condition caused by the autonomic nervous system not working properly. Symptoms such as urinary incontinence could be an early sign of multiple system atrophy. The autonomic nervous system controls involuntary functions.
Diagnosing multiple system atrophy can be challenging. Symptoms such as stiffness and trouble walking can happen in other diseases, including Parkinson’s disease. This can make multiple system atrophy hard to diagnose. Many people affected with multiple system atrophy (MSA) may be first incorrectly diagnosed as having Parkinson’s disease because there are many similar features between these conditions. Your primary care doctor gives you a physical exam, reviews your medical history and tests your autonomic functions such as blood pressure. You also may need blood tests and imaging tests, such as an MRI. These tests can help diagnose multiple system atrophy or point to another causes of your symptoms.
If your primary care doctor thinks you have multiple system atrophy, test results help determine whether the diagnosis is clinically established multiple system atrophy or clinically probable multiple system atrophy. Because it’s hard to make a diagnosis, some people are never properly diagnosed.
You may be referred to a neurologist or another specialist for further evaluation. A specialist can help diagnose the condition.
Many neurological conditions look similar in the early stages so it’s important that a more common or treatable condition is ruled out before a diagnosis of multiple system atrophy is made.
Improved brain scanning techniques may show abnormalities in some people with multiple system atrophy but it is not unusual for a standard MRI brain scan to be normal.
There are a number of symptoms your neurologist might note and highlight when looking for a possible multiple system atrophy diagnosis. These are:
- Erectile dysfunction (impotence) in men and sexual dysfunction in women
- Bladder issues including urgency, frequency, nocturia (passing urine at night) and retention (inability to empty the bladder)
- Postural hypotension (orthostatic hypotension) which is a sudden drop in blood pressure when changing position – particularly from lying or sitting to standing
- Poor response to Levodopa (a commonly used Parkinson’s Disease drug)
- Cold extremities
- Difficulty speaking and swallowing
- Inspiratory sighs or stridor (a high-pitched breath sound)
- Faster progression than Parkinson’s disease and Cerebellar ataxia.
| Criteria for definite multiple system atrophy (MSA) include neuropathological findings during postmortem examination of: |
| a) Widespread and abundant cerebral alpha-synuclein–positive glial cytoplasmic inclusions b) Neurodegenerative changes in striatonigral or olivopontocerebellar region |
| Criteria for probable multiple system atrophy (MSA) include a sporadic progressive adult (> 30 years old)–onset disease characterized by: |
| a) Autonomic failure involving urinary incontinence (inability to control the release of urine from the bladder with erectile dysfunction in males) or an orthostatic decrease of blood pressure within 3 min of standing by at least 30 mmHg systolic or 15 mmHg diastolic, and |
| b) Poorly levodopa-responsive parkinsonism (bradykinesia with rigidity, tremor or postural instability), or |
| c) A cerebellar syndrome (gait ataxia with cerebellar dysarthria, limb ataxia or cerebellar oculomotor dysfunction) |
| Criteria for possible multiple system atrophy (MSA) include a sporadic progressive adult (> 30 years old)–onset disease characterized by: |
| a) Parkinsonism (bradykinesia with rigidity tremor or postural instability), or |
| b) Cerebellar syndrome (gait ataxia with cerebellar dysarthria limb ataxia or cerebellar oculomotor dysfunction), and |
| c) At least one feature suggesting autonomic dysfunction (otherwise unexplained urinary urgency frequency or incomplete bladder emptying erectile dysfunction in males or significant orthostatic BP decline that does not meet the level required in probable multiple system atrophy (MSA)), and |
d) At least one of the following features:
|
There is no cure for multiple system atrophy, but treatments are focused on managing your symptoms and improving your daily functions. This can involve medications, therapies like physical and speech therapy and lifestyle adjustments
To treat specific symptoms, your healthcare team may recommend:
- Medicines to raise blood pressure. These medicines can treat low blood pressure that happens when standing after sitting or lying down, known as postural hypotension. There are several medicines your doctor may recommend. The corticosteroid fludrocortisone can increase blood pressure by helping your body retain more salt and water. Midodrine (Orvaten) can raise your blood pressure quickly. This medicine needs to be taken carefully because it can increase blood pressure while lying down. Don’t lie flat for four hours after taking this medicine. The medicine pyridostigmine (Mestinon, Regonol) can raise your blood pressure while standing without causing a large increase when you’re lying down. Another medicine called droxidopa (Northera) also treats postural hypotension. The most common side effects of droxidopa include headaches, dizziness and nausea.
- Medicines to reduce Parkinson’s disease-like symptoms. Medicines that treat Parkinson’s disease, such as combined levodopa and carbidopa (Sinemet, Duopa, others), can help some people with multiple system atrophy. The medicine can treat stiffness, trouble with balance and slow movements. Many people with multiple system atrophy do not respond to Parkinson’s medicines. The medicines also may become less effective after a few years.
- Medicines to treat erection problems. If you have trouble getting or keeping an erection, you can be treated with medicines such as sildenafil (Revatio, Viagra). This medicine helps manage erectile dysfunction but it can lower blood pressure.
- Steps to manage swallowing and breathing symptoms. If you have trouble swallowing, try eating softer foods. If swallowing or breathing symptoms become worse, you might need surgery to insert a feeding or breathing tube. A gastrostomy tube delivers food directly into your stomach.
- If you have sleep apnea, you might be treated with continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP). Stridor also can be treated with CPAP.
- Bladder care. If you have trouble with bladder control, medicines can help in the earlier stages. But as multiple system atrophy gets worse, you may need to have a soft tube inserted to drain your bladder. The soft tube is known as a catheter.
- Physical therapy. A physical therapist can help you maintain as much of your movement and strength as possible as the disease gets worse.
- Walkers and wheelchairs can help as mobility declines in the person with multiple system atrophy. Occupational therapists can help with home safety and learning new ways to address activities of daily living, such as dressing and eating.
- A speech-language pathologist can help you improve or maintain your speech.
- Doctors may prescribe Botulinum toxin (Botox) injections to ease abnormal muscle postures (dystonia).
Figure 1. Brain and spinal cord (central nervous system)
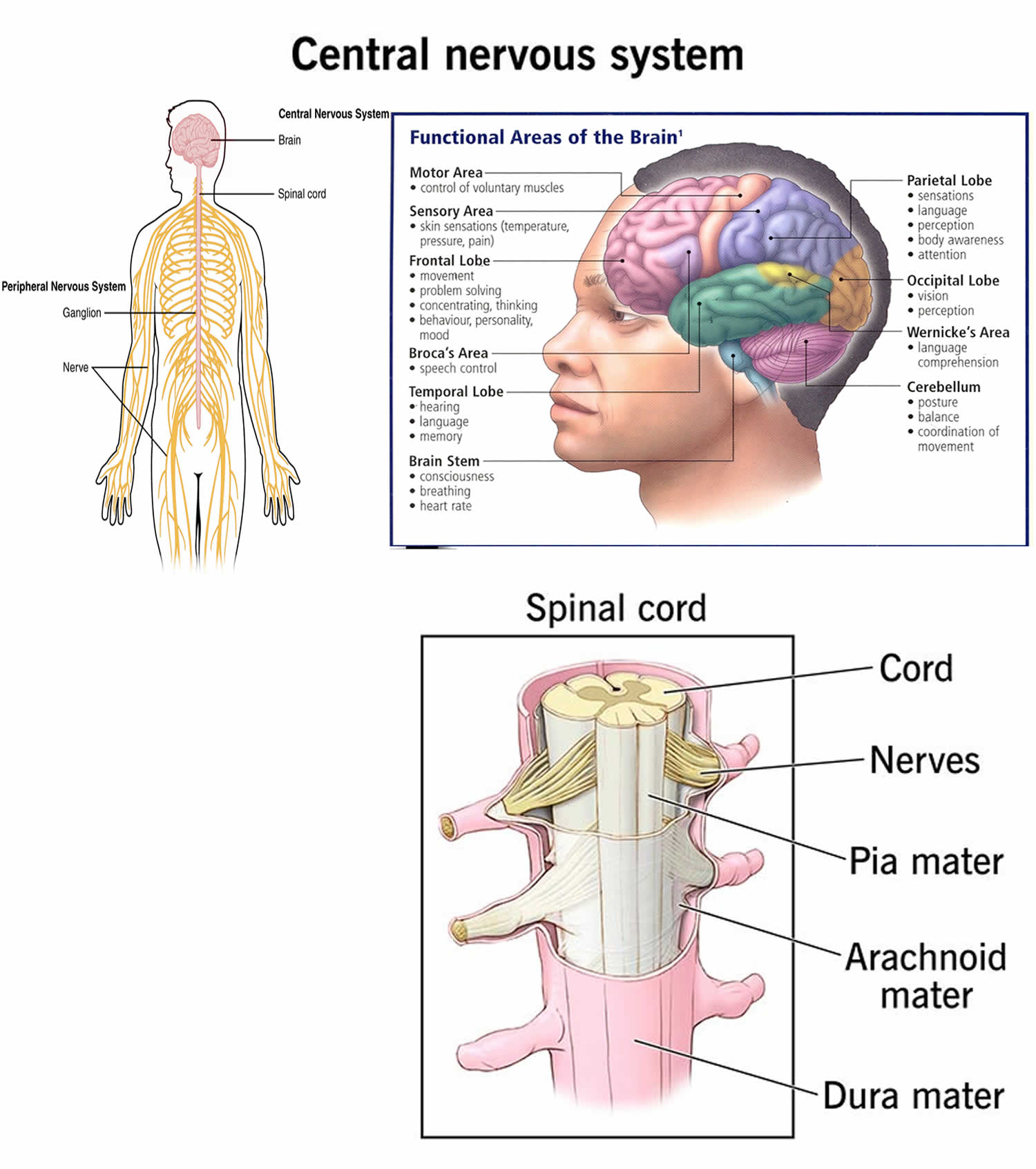
Footnotes: The central nervous system (CNS) consists of the brain and the spinal cord. The spinal cord is the highway for communication between the body and the brain. When the spinal cord is injured, the flow of information between the brain and other parts of the body is disrupted. The brain controls motor and sensory information, conscious and unconscious behaviors, feelings, intelligence, and memory 21. The left hemisphere controls speech and abstract thinking (the ability to think about things that are not present) 21. The right hemisphere controls spatial thinking (thinking that finds meaning in the shape, size, orientation, location, and phenomena) 21. The motor and sensory neurons descending from the brain cross to the opposite side in the brainstem. This crossing means that the right side of the brain controls the motor and sensory functions of the left side of the body, and the left side controls the motor and sensory functions of the right side of the body. For exampla, a stroke affecting the left brain hemisphere, for example, exhibit motor and sensory deficits on the right side of the body. Sensory neurons bring sensory input from the body to the thalamus, which relays this information to the cerebrum. The hypothalamus controls hunger, thirst, and sleep.
Figure 2. Basal ganglia
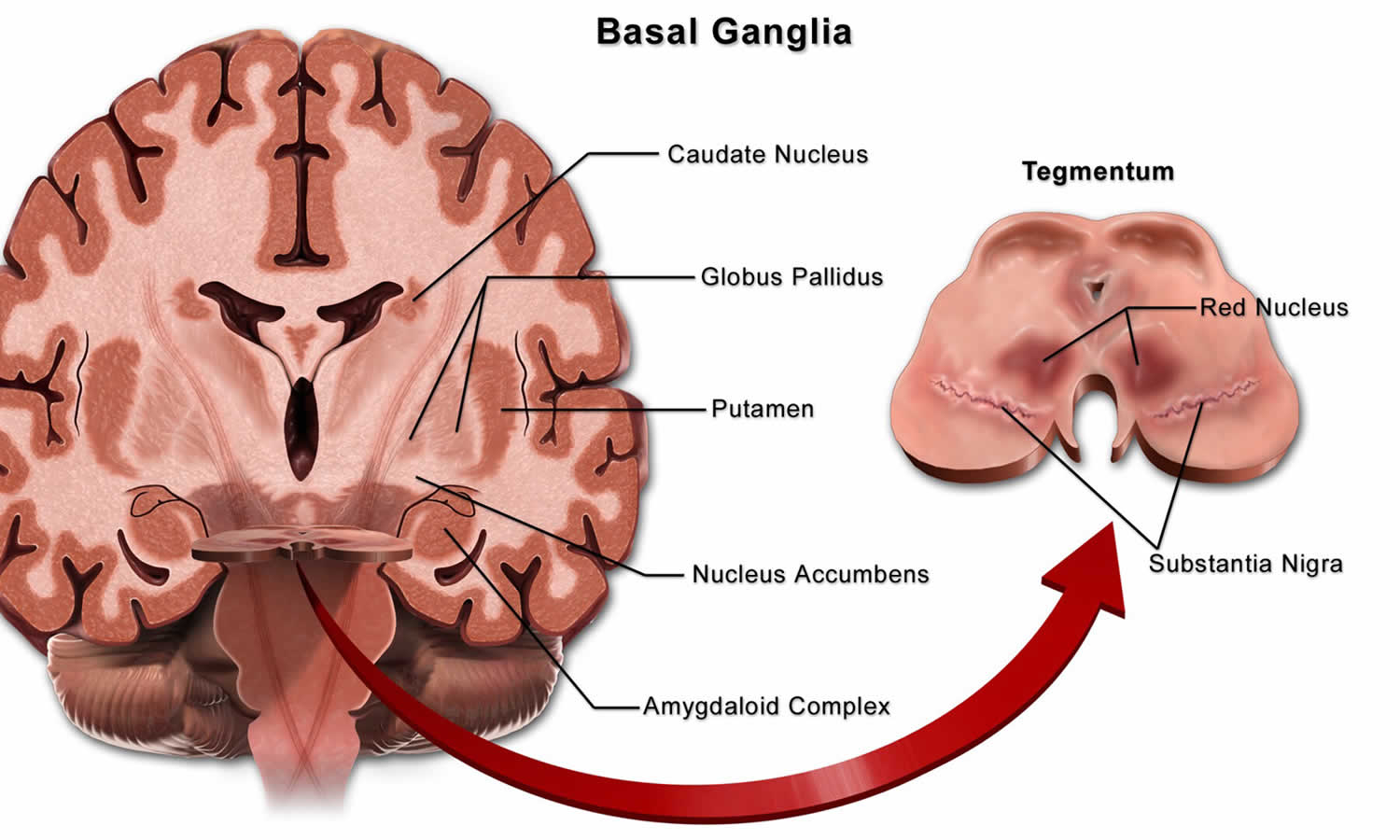
Footnotes: The basal ganglia or basal nuclei are a cluster of subcortical nuclei found deep to cerebral hemispheres 22. The largest component of the basal ganglia is the corpus striatum which contains the caudate and lenticular nuclei (the putamen, globus pallidus externus, and internus), the subthalamic nucleus (STN), and the substantia nigra (SN). Positioned at the base of the forebrain and the top of the midbrain, the basal ganglia have strong connections (synapses) with the cerebral cortex, thalamus, brainstem and other brain areas to promote or antagonize movement. The basal ganglia’s primary function is to control conscious and proprioceptive motor movements 23, 22. It receives signals from the cortex, weighs those signals, and determines what actions to “disinhibit” (to lose emotional or behavioral control, resulting in the inability to withhold inappropriate or socially unacceptable actions or comments) 24, 25. Damage to the basal ganglia, as in Parkinson’s disease, leads to motor impairments like a shuffling gait when walking. The basal ganglia also regulate motivation.
[Source 26 ]Figure 3. Cerebellum
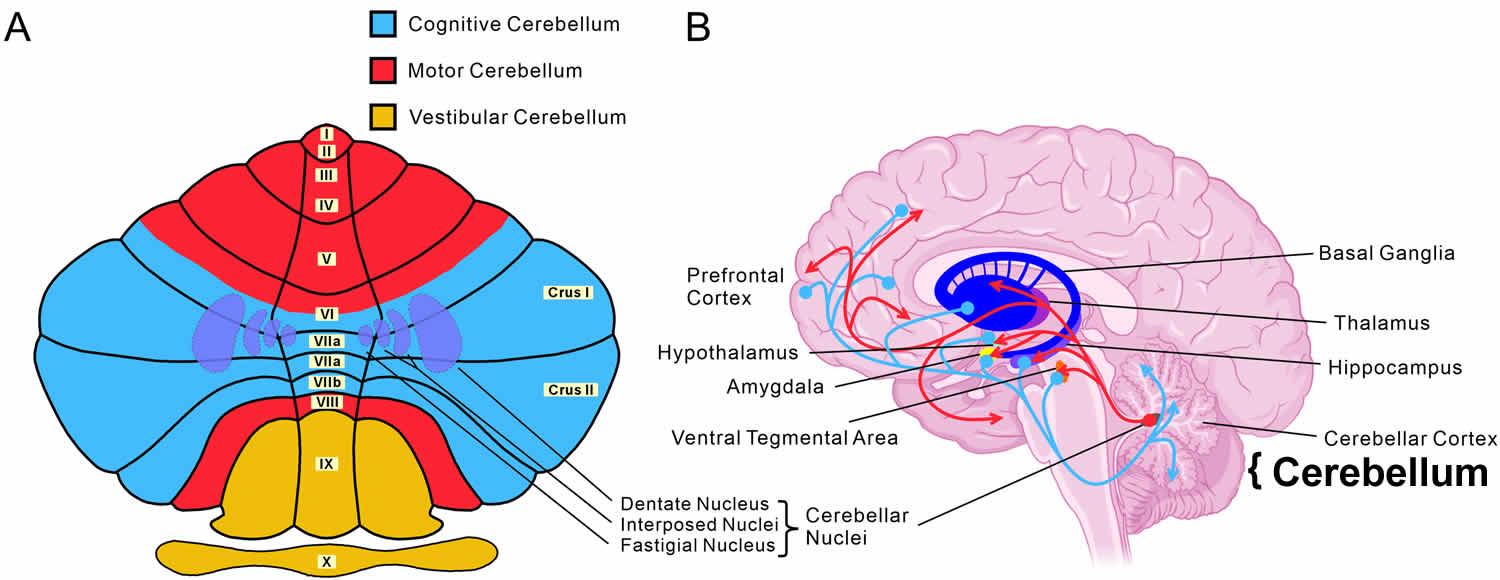
Footnotes: The cerebellum, which is the largest part of the hindbrain, is located in the posterior cranial fossa, behind the fourth ventricle, the pons, and the medulla oblongata 27. The cerebellum is a vital component in the human brain that plays a role in motor movement regulation and balance control. The cerebellum coordinates gait and maintains posture, controls muscle tone and voluntary muscle activity but is unable to initiate muscle contraction 27. Damage to the cerebellum in humans results in a loss in the ability to control fine movements, maintain posture, and motor learning 28, 29, 30. The cerebellum is composed of two hemispheres joined by the vermis and is sub-divided into three lobes – anterior, posterior, and flocculonodular, which are separated by two transverse fissures. The V-shaped primary fissure separates the anterior and posterior lobe, while the posterolateral fissure separates the posterior and flocculonodular lobes. A deep horizontal fissure found within the posterior lobe separates the superior and inferior surfaces of the cerebellum. The cerebellum is neuron-rich, containing 80% of the brain’s neurons organized in a dense cellular layer 31, 28.
[Source 32 ]Figure 4. Autonomic nervous system
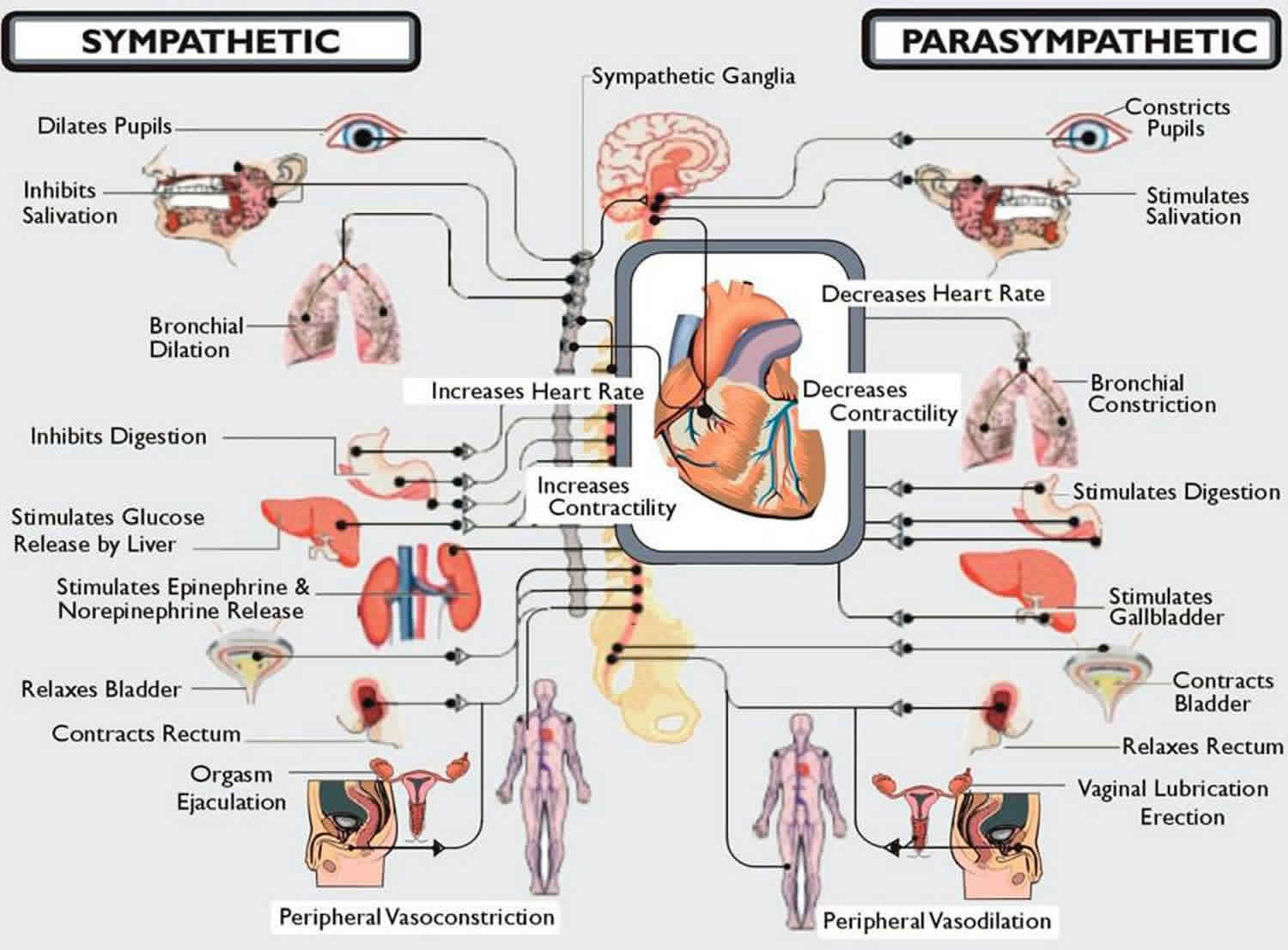
Footnotes: The autonomic nervous system (ANS) is made up of pathways of neurons that control various organ systems inside the body, using many diverse chemicals and signals to maintain homeostasis. The autonomic nervous system (ANS) divides into the sympathetic and parasympathetic systems 33. The sympathetic system is better known as “fight or flight” and the parasympathetic system as “rest and digest”33. The autonomic nervous system (ANS) functions without conscious control throughout the lifespan of an organism to control heart muscle, smooth muscle, and exocrine and endocrine glands, which in turn regulate blood pressure, urination, bowel movements, and temperature regulation 34.
The sympathetic nervous system contains cell bodies that lie within the lateral gray column of the spinal cord running from T1 to L2 33. These neurons are known as preganglionic neurons and travel to ganglia, where they synapse and activate nicotinic receptors on postganglionic neurons using acetylcholine. The postganglionic neurons then travel to the target site and release norepinephrine to activate adrenergic receptors.
The parasympathetic nervous system is comprised of a cranial portion, consisting of cranial nerves III, VII, IX, and X and pelvic splanchnic nerves that exit from S2 to S4 33. The organization of the parasympathetic nerves is similar to the sympathetic nervous system, as preganglionic fibers synapse on postganglionic fibers, which then innervate target sites. A notable difference is that the preganglionic nerve fibers synapse on ganglia that are close to or embedded within their respective target sites, resulting in short postganglionic neurons 35.
Figure 5. Multiple system atrophy brain pathological findings
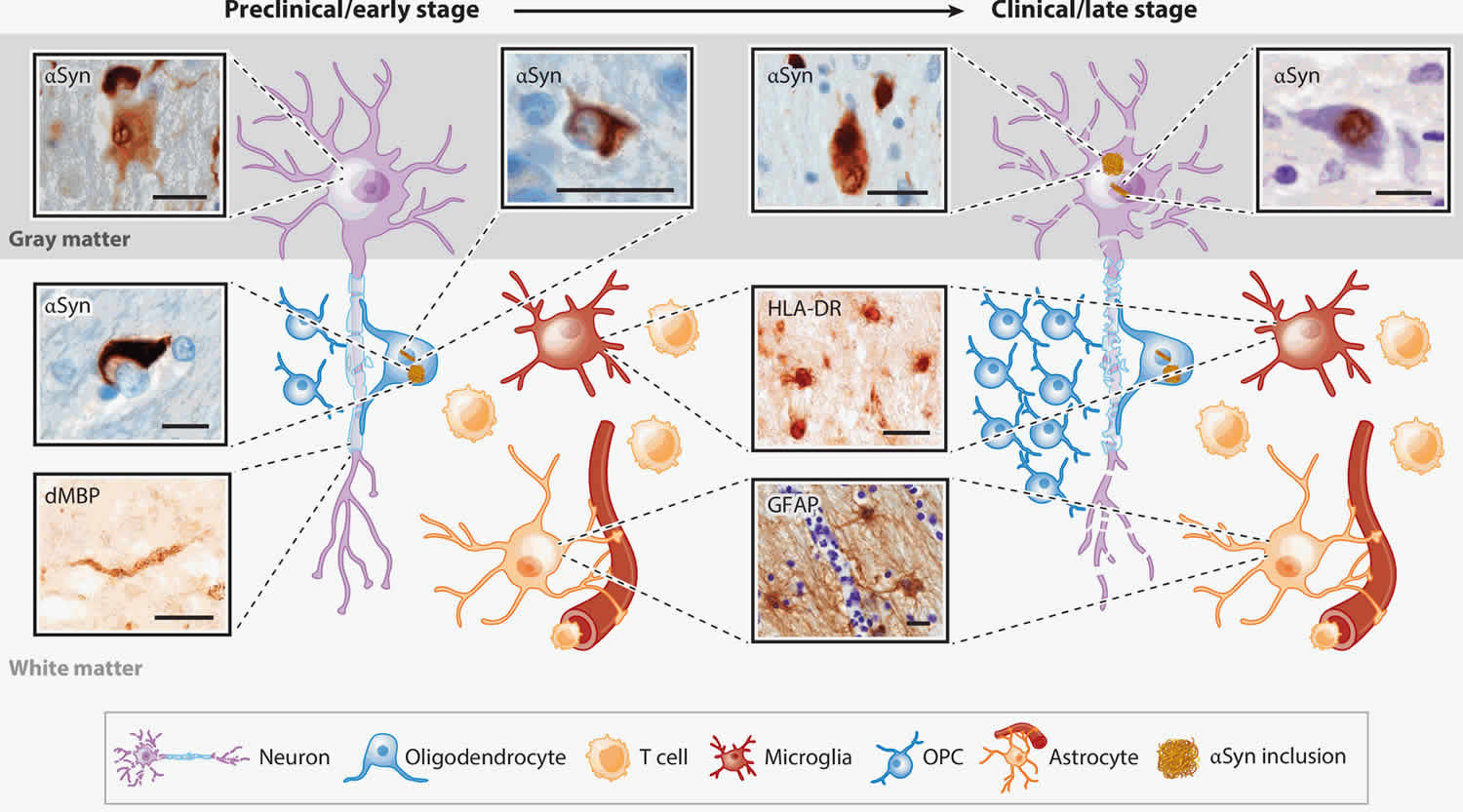
Footnotes: Early- and late-stage pathological findings in multiple system atrophy brain. Postmortem brain findings in early-stage MSA brains include diffuse neuronal alpha-synuclein accumulation in neurons, glial cytoplasmic and nuclear inclusions, myelin degeneration, astrocytosis, and microgliosis. Late-stage pathologies additionally involve the formation of neuronal nuclear and cytoplasmic inclusions. T cell infiltration and proliferation of oligodendrocyte precursors in white matter is observed, but it is currently unknown how early these findings are. Scale bars indicate 20 μm.
Abbreviations: αSYN = α-synuclein; dMBP = degraded myelin basic protein; GFAP = glial fibrillary acidic protein; HLA-DR = human leukocyte antigen–DR isotype; MSA = multiple system atrophy; OPC = oligodendrocyte precursor cell.
[Source 1 ]Figure 6. Hot cross bun sign
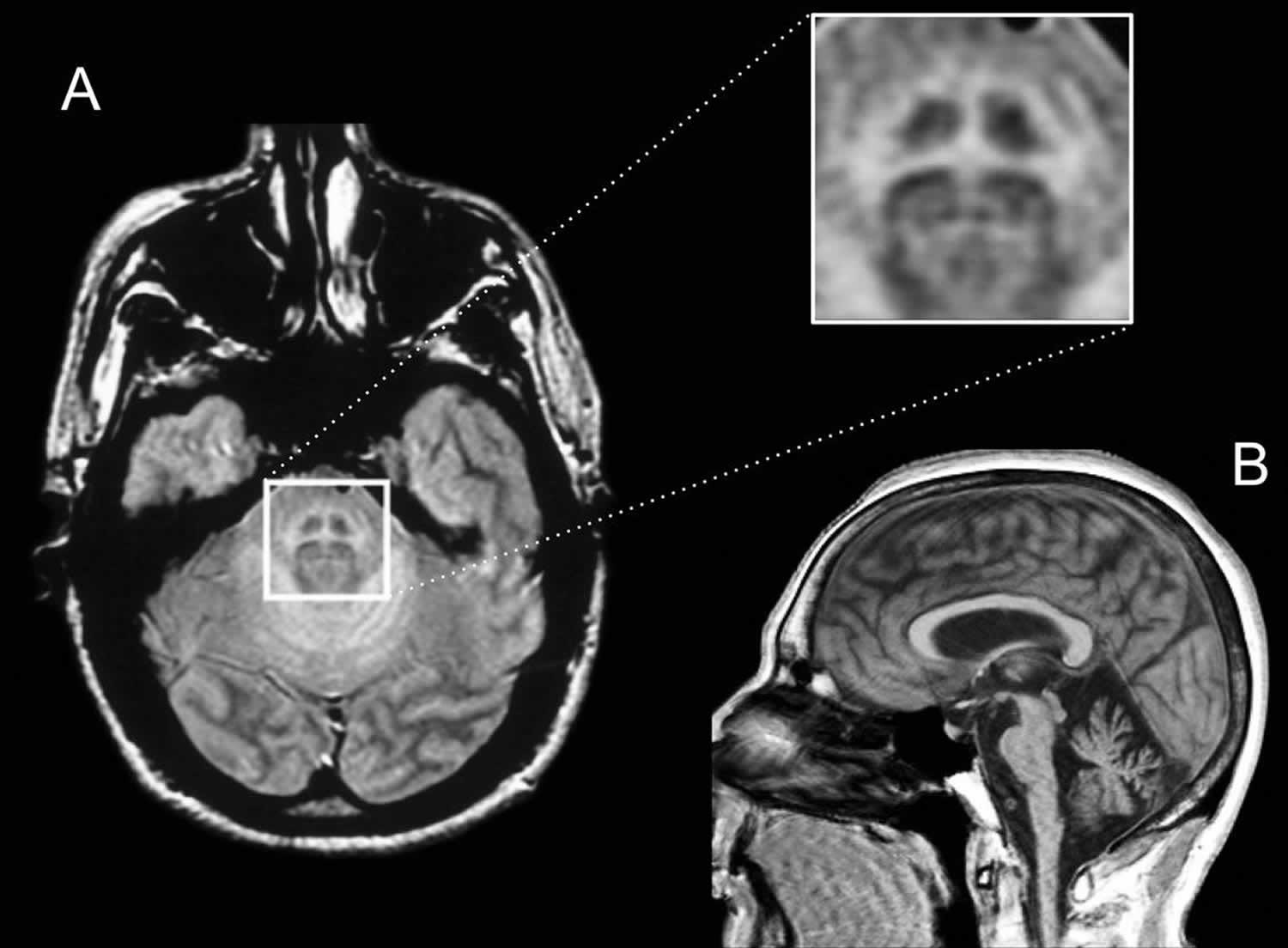
Footnotes: Conventional brain magnetic resonance imaging (MRI). The hot cross bun sign refers to the MRI appearance of the pons when T2/FLAIR hyperintensity forms a cross on axial images, representing selective degeneration of transverse pontocerebellar tracts (forming a horizontal line) and median pontine raphe nuclei (forming a vertical line) 36. The hot cross bun sign has been described in a variety of neurodegenerative and other conditions. (A) Axial image showing the “hot cross bun” sign and atrophy of cerebellar peduncles, which is shown in detail inset. (B) Sagittal figure showing atrophy in pons, medulla and cerebellum.
[Source 11 ]Figure 7. Multiple system atrophy brain MRI
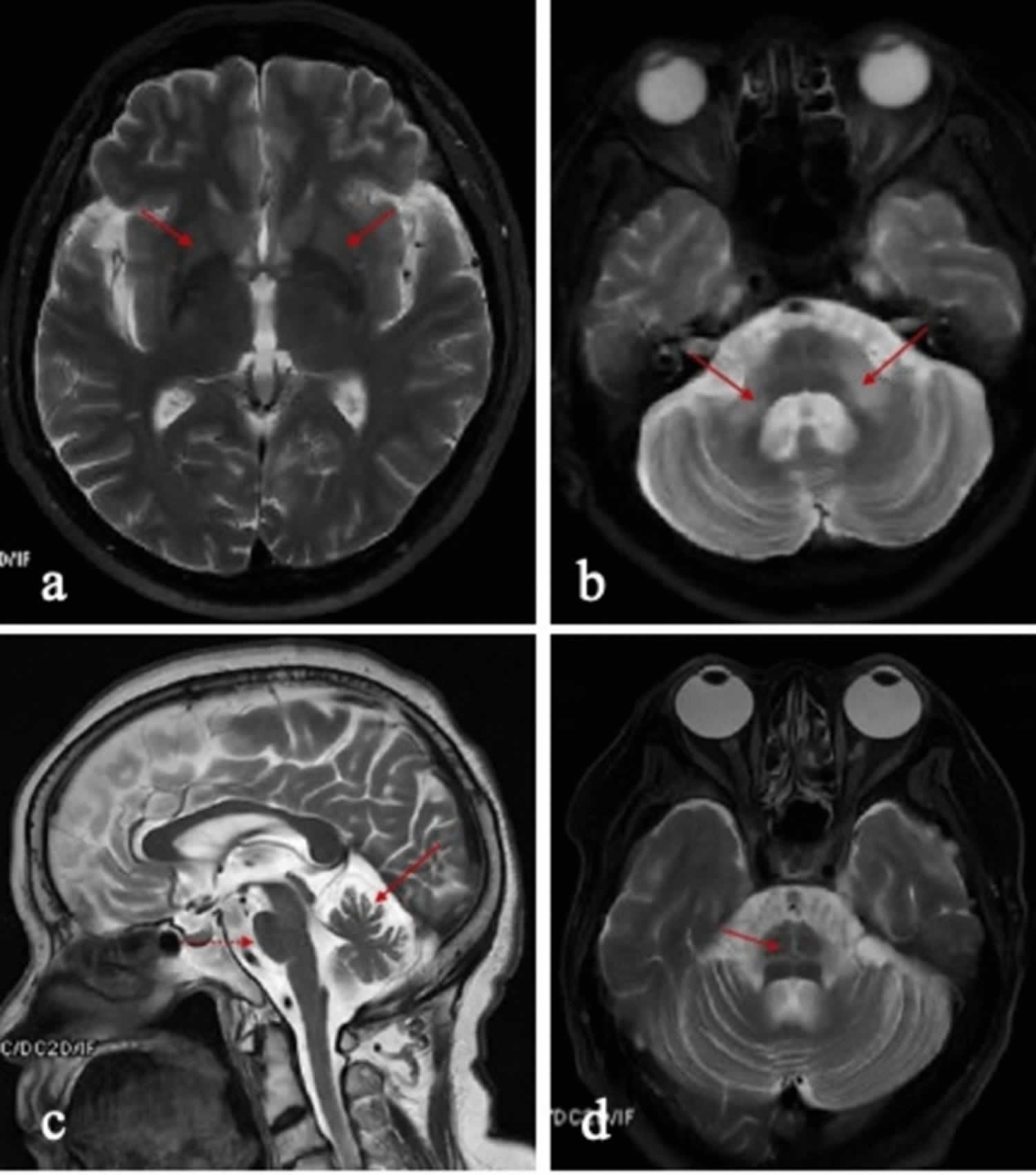
Footnotes: MRI brain imaging in multiple system atrophy patients. (a) Demonstrates putaminal atrophy (red arrows). (b) Atrophy and hyper-intensity signal of middle cerebellar peduncles (red arrows). (c) Pontine atrophy (red dashed arrow) and cerebellar atrophy (red solid arrow). (d) “Hot cross bun” sign (red arrow)
[Source 3 ]Figure 8. Multiple system atrophy

Footnotes: (A). Bluish discoloration in the foot of a patient with multiple system atrophy – cerebellar type (MSA-C). (B) “Striatal toe”, spontaneous extensor toe response in a patient with multiple system atrophy – cerebellar type (MSA-C). (C) Antecollis in a patient with multiple system atrophy – parkinsonian type (MSA-P).
[Source 11 ]Who gets multiple system atrophy?
Multiple system atrophy usually starts between the ages of 40 to 60 years, but it can affect people between the ages of 30 to 70. Multiple system atrophy affects men and women.
Most cases of multiple system atrophy are sporadic, which means they occur in people with no history of the disorder in their family, so it cannot be passed from parent to child. Rarely, multiple system atrophy has been reported to run in families; however, it usually does not have a clear pattern of inheritance. There is still much to learn and understand about multiple system atrophy and research is ongoing to better understand the condition.
Will my children or family get multiple system atrophy?
There is no evidence that multiple system atrophy is a hereditary condition and it is not contagious or infectious. You may read or hear about genetic factors; this does not mean that there is a known
faulty gene. As a greater understanding of genetic make-up is achieved, there is increasing interest as to whether an individual’s specific unique combination of genes can cause them to be more susceptible to developing conditions like multiple system atrophy.
How are the nerve cells in the brain damaged by multiple system atrophy?
Nerve cells in the affected areas of your brain atrophy or shrink, this shrinkage can sometimes be seen on MRI scans. The shrinkage is caused by abnormal alpha-synuclein protein building up in the nerve cells which then causes them to die. Loss of these nerve cells shows up as shrinkage in the affected area of the brain.
According to research, all humans have alpha-synuclein in their brain cells. However, in people with multiple system atrophy the abnormal alpha-synuclein protein building up in the cells of the control centers of the brain involved in movement, balance and autonomic function, damaging these areas and causing symptoms of multiple system atrophy.
Why do nerve cells become damaged?
It is still unclear why alpha-synuclein gathers together and the cells become damaged in people with multiple system atrophy. Further research is being conducted into why and how this happens. The progression of nerve cells damage is also unclear and is different for each individual. Studies of the brains of people who have been affected by multiple system atrophy compared to unaffected brains are aiding research.
How is multiple system atrophy different from Parkinson’s disease?
Many people with multiple system atrophy may have received an initial diagnosis of Parkinson’s disease or cerebellar ataxia because they both cause similar symptoms initially. Additional problems
that develop in multiple system atrophy which are unusual in early Parkinson’s disease may have made your neurologist suspect that you do not have typical Parkinson’s but a “parkinsonism”- one of which is multiple system atrophy. The changes in the brain in multiple system atrophy are different from that of Parkinson’s disease.
What are the earliest signs of multiple system atrophy?
For men, the first symptom of multiple system atrophy is often erectile dysfunction (inability to achieve or sustain an erection). Other causes may be explored by your doctor before connecting it to a
neurological cause. Both men and women may have early bladder problems including urgency, frequency, nocturia (night time passing of urine) and retention (not emptying the bladder fully). Often these bladder issues are linked to other causes such as ageing. Other early problems can be feeling stiff and slow as well as changes in handwriting. Some people become clumsy or unsteady when walking. If blood pressure control has been affected, people may feel dizzy when standing up or experience episodes of fainting.
Will I experience cognitive difficulties?
People with multiple system atrophy might experience cognitive difficulties, including cognitive slowing and cognitive dysfunction as the illness progresses. People may find they struggle with planning, organizing, memory, attention, problem-solving and flexible thinking. Emotional control can also be affected. This will likely come on gradually. Confusion or hallucinations are not usual in multiple system atrophy, unless there is an acute infection which can sometimes cause a sudden onset of these symptoms. The symptoms should subside after treatment.
Giving people with multiple system atrophy more time to think and answer, and also concentrating on one task at a time are strategies that can help. Fatigue and tiredness can also affect cognitive abilities.
Can I still travel abroad on holidays?
Travel abroad is possible for people with multiple system atrophy with the correct arrangements and good planning in place. Travel companies will need to be made aware of your special requirements and you will need to ensure your accommodation is suitable.
Is there a diet for multiple system atrophy?
There is no special dietary requirement for multiple system atrophy, although eating a balanced diet with high fiber, protein, fresh fruit and vegetables is important. If you have swallowing difficulties, ask your Speech and Language Therapist for advice on the best type of food and drink for you. If you have postural hypotension also called orthostatic hypotension there are some dietary suggestions to prevent a drop in blood pressure.
Bolus water drinking has been used to activate the osmopressor reflex to counteract orthostatic hypotension. In this approach, water is rapidly ingested (e.g, 500 mL in 2-3 minutes), which decreases osmolarity and triggers sympathetic nervous system activation. This reflex is believed to be mediated by hepatoreceptors and renal sympathetic nerves. Importantly, this effect is not reproduced by hypo-osmolar or iso-osmolar fluids, so plain water should be consumed 37, 38.
A high-salt diet of up to 10 grams of salt daily, combined with a liberal water intake of 2 to 3 L/day, has been recommended to promote intravascular expansion. However, this should be carefully balanced with your heart function parameters and the potential for end-organ damage 39.
Note that if you have a kidney condition or are on prescribed fluid restrictions it is essential you adhere to fluid restrictions prescribed by your doctor.
Other non-drug treatments for postural hypotension include:
- Gradually changing position in phases (from lying to sitting to standing) rather than abruptly.
- Move your feet up and down
- Bend and straighten your knees
- Clench and unclench your hands
- Get out of bed slowly
- Sit on the side of the bed first
- Count to 10 slowly, then stand
- Stand up slowly when rising from a chair
- Make sure you have something to hold onto if required
- Wait for a moment before walking
- Avoid standing still for long periods
- Wiggle toes in shoes
- March on the spot
- Sit down immediately if you feel dizzy while walking
- Avoid very hot baths or showers
- Sleep with extra pillows to raise your head or sleeping with the head of the bed elevated.
- Maintaining adequate hydration.
- Avoiding alcohol, warm environments, large meals, and hot showers or baths.
- Crossing your legs while standing.
- Tensing the muscles in your legs and hips after standing.
- Using binders or stockings to compress the abdomen and lower limbs.
- Engaging in recumbent exercises or swimming.
Multiple system atrophy types
Before the name change in 1998, multiple system atrophy (MSA) was known as Shy Drager syndrome, a neurological disorder that resulted in orthostatic hypotension of unknown etiology 40, 9, 41. In a 1998 consensus statement, the term “Shy Drager syndrome” was formally taken out of use and placed under the categorization of “multiple system atrophy” (MSA) 9. As indicated in its name, the anatomical hallmark of multiple system atrophy is “atrophy” (wasting away of a body part, cell, tissue, or organ). Specifically, the cerebellum, pons, and putamen are the primary areas of brain involvement.
Researchers have described 2 major types of multiple system atrophy, which are distinguished by their major signs and symptoms at the time of diagnosis 15.
- Multiple system atrophy- parkinsonian type (MSA-P): Primarily affects the basal ganglia, causing movement-related symptoms like Parkinson’s disease leading to problems with coordination and balance. These abnormalities include unusually slow movement (bradykinesia), muscle rigidity, tremors, and an inability to hold the body upright and balanced (postural instability). However, people with multiple system atrophy – parkinsonian type (MSA-P) have more widespread damage to the part of the autonomic nervous system that regulates important functions such as heart rate, blood pressure, and sweating.
- Multiple system atrophy – cerebellar type (MSA-C): Affects the cerebellum that is characterized by cerebellar ataxia, which causes problems with coordination and balance. Multiple system atrophy – cerebellar type (MSA-C) can also include speech difficulties (dysarthria) and problems controlling eye movement. Multiple system atrophy – cerebellar type (MSA-C) used to be known as olivopontocerebellar atrophy (OPCA).
Multiple system atrophy- parkinsonian type (MSA-P) and MSA-C differ in the amount of involvement in each of these areas of the brain. In the spinal column, both MSA-P and MSA-C include the intermediolateral area of the spinal cord in addition to Onuf’s nucleus and the vagal nucleus.[4]
Multiple system atrophy- parkinsonian type (MSA-P)
Multiple system atrophy- parkinsonian type (MSA-P) primarily affects the basal ganglia, causing movement-related symptoms like Parkinson’s disease leading to problems with coordination and balance. These abnormalities include unusually slow movement (bradykinesia), muscle rigidity, tremors, and an inability to hold the body upright and balanced (postural instability). However, people with multiple system atrophy – parkinsonian type (MSA-P) have more widespread damage to the part of the autonomic nervous system that regulates important functions such as heart rate, blood pressure, and sweating. Multiple system atrophy – parkinsonian type (MSA-P) is most often diagnosed in men older than 60. Multiple system atrophy damages your nervous system. The disease tends to progress rapidly. About one half of people with multiple system atrophy – parkinsonian type (MSA-P) have lost most of their motor skills within 5 years of onset of the disease.
The cause of multiple system atrophy – parkinsonian type (MSA-P) is unknown. The affected areas of the brain overlap with areas affected by Parkinson disease, with similar symptoms. For this reason, this subtype of multiple system atrophy is called parkinsonian.
Multiple system atrophy – parkinsonian type (MSA-P) symptoms are similar to those of Parkinson’s disease may include 42:
- Stiff muscles.
- Trouble bending the arms and legs.
- Slow movement, known as bradykinesia.
- Tremors at rest or when moving the arms or legs.
- Passing out (syncope) due to drops in blood pressure
- Movement difficulties, such as slowness, loss of balance, shuffling when walking
- Trouble with posture and balance
- Frequent falls
- Muscle aches and pains (myalgia), and stiffness
- Face changes, such as a masklike appearance to the face and staring
- Difficulty chewing or swallowing (occasionally), not able to close the mouth
- Disrupted sleep patterns (often during rapid eye movement [REM] sleep late at night)
- Dizziness or fainting when standing up or after standing still
- Erection problems
- Loss of control over bowels or bladder
- Problems with activities that requires small movements (loss of fine motor skills), such as writing that is small and hard to read
- Loss of sweating in any part of the body
- Decline in mental function
- Nausea and problems with digestion
- Posture problems, such as unstable, stooped, or slumped over
- Vision changes, decreased or blurred vision
- Slurred, slow or soft speech known as dysarthria
Other symptoms that may occur with multiple system atrophy – parkinsonian type (MSA-P) include 42:
- Confusion
- Dementia
- Depression
- Sleep-related breathing difficulties, including sleep apnea or a blockage in the air passage that leads to a harsh vibrating sound (stridor)
- Restless legs
To diagnose multiple system atrophy your doctor will examine you, and check your eyes, nerves, and muscles. Your blood pressure will be taken while you are lying down and standing up.
There are no specific tests to confirm multiple system atrophy. A specialist in the nervous system (neurologist) can make the diagnosis based on your:
- History of symptoms
- Physical exam results
- And by ruling out other causes of symptoms
Testing to help confirm the diagnosis may include:
- Autonomic nervous system testing
- MRI of head
- Plasma norepinephrine levels
- Urine exam for norepinephrine breakdown products (urine catecholamines)
There is no cure for multiple system atrophy – parkinsonian type (MSA-P). There is no known way to prevent the disease from getting worse. The goal of treatment is to control your symptoms.
- Dopaminergic medicines, such as levodopa and carbidopa, may be used to reduce early or mild tremors. But, for many people with multiple system atrophy – parkinsonian type (MSA-P), these medicines do not work well.
- Medicines may be used to treat low blood pressure (hypotension).
- A pacemaker that is programmed to stimulate your heart to beat at a rapid rate (faster than 100 beats per minute) may increase blood pressure for some people.
- Constipation can be treated with a high-fiber diet and laxatives. Medicines are available to treat erection problems.
Multiple system atrophy – cerebellar type (MSA-C)
Multiple system atrophy – cerebellar type (MSA-C) used to be known as olivopontocerebellar atrophy (OPCA) affects the cerebellum that is characterized by cerebellar ataxia, which causes problems with coordination and balance. Multiple system atrophy – cerebellar type (MSA-C) can also include speech difficulties (dysarthria) and problems controlling eye movement.
Multiple system atrophy – cerebellar type (MSA-C) can be passed down through families (inherited form) 43. Researchers have identified certain genes that are involved in the inherited form of this condition.
Multiple system atrophy – cerebellar type (MSA-C) can also affect people without a known family history (sporadic form) 43. The cause of multiple system atrophy – cerebellar type (MSA-C) in people with the sporadic form is not known. The disease slowly gets worse or is progressive.
Multiple system atrophy – cerebellar type (MSA-C) is slightly more common in men than in women. The average age of onset is 54 years.
Symptoms of multiple system atrophy – cerebellar type (MSA-C) tend to start at a younger age in people with the inherited form. The main symptom is clumsiness (ataxia) that slowly gets worse. There may also be:
- Trouble with movement and coordination. This includes loss of balance and not being able to walk steadily (gait ataxia) where walking becomes wide-based and wobbly. Clumsiness such as trouble with hand movements, buttoning clothes and other activities.
- Slurred, slow or soft speech, known as dysarthria.
- Changes in vision. This may include blurred or double vision and not being able to focus the eyes.
- Trouble chewing or swallowing, known as dysphagia.
- Difficulty coordinating muscles where it is harder to do tasks that need precise movements
Other symptoms of multiple system atrophy – cerebellar type (MSA-C) may include 43:
- Abnormal eye movements (nystagmus)
- Abnormal movements
- Abnormal sweating
- Bowel or bladder problems
- Difficulty swallowing
- Cold hands and feet
- Lightheadedness when standing
- Headache while standing that is relieved by lying down
- Muscle stiffness or rigidity, spasms, tremor
- Nerve damage (neuropathy)
- Problems in speaking and sleeping due to spasms of the vocal cords
- Sexual function problems
Complications of multiple system atrophy – cerebellar type (MSA-C) include 43:
- Choking
- Infection from inhaling food into the lungs (aspiration pneumonia)
- Injury from falls
- Nutrition problems due to difficulty swallowing
To diagnose multiple system atrophy, your doctor will do a thorough medical and nervous system examination, as well as a symptom review and ask about your family history.
There are genetic tests to look for the causes of some forms of the multiple system atrophy. But, no specific test is available in many cases. An MRI of the brain may show changes in the size of affected brain structures, especially as the disease gets worse. But it is possible to have the disorder and have a normal MRI.
Other tests such as positron emission tomography (PET) may be done to rule out other conditions. These may include swallowing studies to see if a person can safely swallow food and liquid.
There is no specific treatment or cure for multiple system atrophy – cerebellar type (MSA-C). The aim is to treat the symptoms and prevent complications. This may include:
- Tremor medicines, such as those for Parkinson’s disease
- Speech, occupational and physical therapy
- Ways to prevent choking
- Walking aids to help with balance and prevent falls
- Devices to treat sleep apnea (such as CPAP)
- Treatment for low blood pressure
Multiple system atrophy – cerebellar type (MSA-C) slowly gets worse, and there is no cure. The outlook is generally poor. But, it may be years before someone is very disabled.
Multiple system atrophy causes
The cause of multiple system atrophy (MSA) is unknown. Some researchers are studying the possible role of genetics or environmental causes such as a toxin in multiple system atrophy. Initial studies suggested that exposure to solvents, certain types of plastic or metal, and other potential toxins might be associated with the condition. However, these associations have not been confirmed. In rare cases, changes in several genes have been found. For example, changes in the genes called COQ2, LRRK2, GBA1, CHCHD2 and SNCA have been linked to multiple system atrophy in at least one patient. The SNCA gene provides instructions for making a protein called alpha-synuclein, which is abundant in normal brain cells but whose function is unknown. Studies suggest that several common variations in the SNCA gene are associated with an increased risk of multiple system atrophy in people of European descent. It is unclear whether these variations also affect disease risk in other populations. The COQ2 gene provides instructions for making a protein called coenzyme Q2. The coenzyme Q2 carries out one step in the production of a molecule called coenzyme Q10, which has a critical role in energy production within cells 44. Brain tissue gathered from autopsies of patients with multiple system atrophy show a significant decrease in coenzyme Q10, but this was only seen in the cerebellum, suggesting that coenzyme Q10 deficiency may predominate the cerebellar form of multiple system atrophy 45. Variations in the COQ2 gene have been associated with multiple system atrophy in people of Japanese descent, but this association has not been found in other populations 46. It is unclear how changes in the SNCA or COQ2 gene increase the risk of developing multiple system atrophy. Moreover, large genetic studies have not found any major genetic risk factors for multiple system atrophy. One study looking at people from Europe and North America didn’t find strong links to genes like COQ2 or SNCA (which had been suspected earlier). They did find a possible connection with a gene called MAPT, but more research is needed.
Multiple system atrophy causes parts of your brain to shrink. This is known as atrophy. The areas of the brain that shrink due to multiple system atrophy include the cerebellum, basal ganglia and brainstem. The atrophy of these parts of the brain affect internal body functions and movement.
Under a microscope, the brain tissue of people with multiple system atrophy shows a buildup of a protein called alpha-synuclein. Some research suggests that the buildup of alpha-synuclein protein leads to multiple system atrophy. Multiple system atrophy is a type of synucleinopathy, meaning it involves clumps of a protein called alpha-synuclein building up inside brain cells. Accumulation of alpha-synuclein in the brain has also been seen in other neurological disorders such as Parkinson’s disease. But unlike Parkinson’s disease, where the clumps are inside neurons, in multiple system atrophy, the intranuclear accumulation of alpha-synuclein also referred as glial cytoplasmic inclusions (GCIs) mostly form inside support cells called oligodendrocytes. These clumps are known as glial cytoplasmic inclusions (GCIs) which are always present in the brain of someone with multiple system atrophy and are unique to this disease 47. Concomitant with neuronal intranuclear and glial inclusion formation, loss of distinct neuronal populations is observed across multiple brain regions including striatonigral and olivopontocerebellar structures 48. Additional consistent findings include early and severe myelin loss with predilection for small axons and astrocyte and microglial state changes that parallel the degree of myelin and neuronal degeneration 49, 50. They damage different parts of the brain including areas that control movement, balance and vital body functions like blood pressure and bladder control.
Researchers have found other proteins (tau, ubiquitin and LRRK2) inside these clumps too. The structure of alpha-synuclein clumps in multiple system atrophy is different from those seen in Parkinson’s, which may explain why the diseases behave differently.
The areas most affected in multiple system atrophy are:
- Basal ganglia (movement control)
- Brainstem (vital functions like breathing and blood pressure)
- Cerebellum (balance and coordination)
- Spinal cord pathways
The specific brain areas that are most damaged explain why some people with multiple system atrophy more problems with movement (multiple system atrophy – parkinsonian type [MSA-P]) and others have more problems with balance and coordination (multiple system atrophy – cerebellar type [MSA-C]).
More research is necessary to determine the exact role that alpha-synuclein plays in the development of multiple system atrophy and to fully understand the complex, underlying mechanisms that ultimately lead to the disorder.
Finally, the role of inflammation has largely been elucidated in brain tissue, demonstrating increased microglial activation 51.
A risk factor for multiple system atrophy is having rapid eye movement sleep behavior disorder (RBD). Rapid eye movement sleep behavior disorder (RBD) is a sleep disorder where people act out their dreams due to a loss of normal muscle paralysis (atonia) during rapid eye movement (REM) sleep 18, 19, 20.
Another risk factor is having a condition caused by the autonomic nervous system not working properly. Symptoms such as urinary incontinence could be an early sign of multiple system atrophy. The autonomic nervous system controls involuntary functions.
Risk factors for developing multiple system atrophy
A risk factor for multiple system atrophy is having rapid eye movement sleep behavior disorder (RBD). Rapid eye movement sleep behavior disorder (RBD) is a sleep disorder where people act out their dreams due to a loss of normal muscle paralysis (atonia) during rapid eye movement (REM) sleep 18, 19, 20. This can lead to dangerous movements, such as punching or falling out of bed. Normally during REM (rapid eye movement) sleep, the body experiences temporary paralysis of most of the body’s muscles known as atonia while the brain is active and dreaming. Blood pressure rises, breathing becomes irregular, and the eyes dart in all directions rapidly hence, the term “rapid eye movement” (REM). The temporary paralysis of REM sleep allows you to dream quietly and safely throughout the night, lying still while your brain is active. This paralysis involves most skeletal muscles and excludes muscles that help us breathe, digest, and some muscles of the eyes. REM sleep accounts for about 25 percent of a total night’s sleep, with most of it taking place during the second half of the night.
Another risk factor is having a condition caused by the autonomic nervous system not working properly. Symptoms such as urinary incontinence could be an early sign of multiple system atrophy. The autonomic nervous system controls involuntary functions.
For individuals with rapid eye movement sleep behavior disorder (RBD), paralysis does not occur during the REM stage. Instead, their body and voice perform their dreams while they remain asleep. REM sleep behavior disorder (RBD) can manifest as small muscle twitches and quiet sleep talking to loud shouting, punching, kicking, grabbing their bed partner, and jumping out of bed. Interestingly, the dreams associated with REM sleep behavior disorder (RBD) are often intense and frightening. Individuals may dream about being chased or attacked, and they can unknowingly enact the dream in real life.
Due to the potentially violent nature of their movements, individuals with REM sleep behavior disorder (RBD) can put themselves and anyone they share their bed with at risk of physical injury. Depending on the nature of the dream and their bedroom environment, these injuries can be life-threatening. Up to 90 percent of spouses of those with REM sleep disorder report having sleep issues and over 60 percent have experienced a physical injury 52. Even when the potential for physical injury has been reduced, the disruption of sleep to the individual or their sleep partner can still be severe enough to cause relationship problems. However, nearly two-thirds of couples continue sleeping together despite the risk of disturbed sleep.
Scientists do not know what causes REM sleep behavior disorder (RBD). Animal studies suggest that it has to do with certain neural pathways in the brain. In an individual without REM sleep behavior disorder (RBD), certain neural pathways inhibit muscle activity during REM sleep, and disruption in these neural pathways lead to REM sleep without atonia.
Less than one percent of people are estimated to have REM sleep behavior disorder (RBD) 53. Rapid eye movement sleep behavior disorder (RBD) usually begins after age 50, and the disease is associated with other neurodegenerative disorders, including Parkinson’s disease, Lewy body dementia, and multiple system atrophy 20. One study found that 38 percent of men aged 50 or older with REM sleep behavior disorder (RBD) eventually developed Parkinson’s disease, Lewy body dementia, or multiple symptom atrophy, usually within 13 years 54.. That number increased to nearly 81 percent in a followup study conducted 16 years later 55. These findings have been confirmed in subsequent research; 30 percent of individuals with REM sleep disorder developed a Parkinsonian disorder or dementia within 3 years and 66 percent did so within 7.5 years 56.
REM sleep disorder can also be brought on by antidepressants, including tricyclic antidepressants and serotonin-specific reuptake inhibitors 57.
Risk factors for REM sleep behavior disorder (RBD) include 20:
- Being male
- Being over 50 years old
- Having another neurological disorder, like Parkinson’s disease, Lewy body dementia, or multiple system atrophy
- Having narcolepsy
- Using some medications or antidepressants 58
- Use or withdrawal from drugs or alcohol 59
The average age of onset is about 61 years old, with 87 percent being male. More research is needed to understand environmental contributors to REM sleep behavior disorder. Sleep deprivation, smoking, head injury, and exposure to pesticides may be environmental risk factors.
According to the American Academy of Sleep Medicine’s International Classification of Sleep Disorders, a person must meet four criteria to receive a diagnosis of REM sleep behavior disorder (RBD):
- You have repeatedly experienced episodes of acting out your dreams with vocalizations or arm and leg movements that correspond to what’s taking place in your dream.
- Episodes occur during REM sleep, as confirmed by an in-laboratory polysomnogram (in-lab sleep study) or your clinical history.
- Episodes include sleep without atonia, as confirmed by polysomnography.
- The episodes are not attributed to something else, like another sleep or mental health disorder, a side effect of medication, or substance abuse.
If you think you may have REM sleep behavior disorder (RBD), it’s best to consult your doctor. Your doctor may then refer you to a sleep physician. Here’s what you can expect to happen when you meet with them.
- First, your doctor will conduct a physical and neurological exam. The point of this is to rule out any other potential causes, like alcohol, medications, or narcolepsy, a sleep disorder that often coexists with REM sleep behavior disorder (RBD) 60
- Due to the common co-occurrence of Parkinsonian syndromes and REM sleep behavior disorder (RBD), your doctor will also look for symptoms of Parkinson’s disease, such as hand tremors or muscle stiffness.
- If you sleep with a partner, your doctor may ask them if they’ve seen you act out your dreams while you sleep. They’ll ask them to describe the dream enactment behaviors they observed.
Your doctor may refer you to a sleep lab for a polysomnogram, an overnight sleep study. During the study, sensors monitor your breathing, eye movements, arm and leg movements, brain and heart activity, and blood oxygen levels. It’s common to videotape the exam to record any dream enactment behavior.
After the exam, a sleep physician will review your medical history, symptoms, and the results of your polysomnogram to determine whether a diagnosis of REM sleep behavior disorder (RBD) is appropriate.
The treatment for REM sleep behavior disorder (RBD) is tailored to an individual and can involve a combination of lifestyle changes, medication, and injury prevention techniques.
Avoiding Triggers
Because the use of certain alcohol or prescription drugs can contribute to REM sleep behavior disorder, making lifestyle changes to reduce or eliminate their use may be part of a person’s treatment. These changes can be part of a larger set of steps to improve sleep hygiene, such as setting a consistent sleep schedule, that normalize sleep and promote sleep quality.
Medications
Melatonin is the preferred, first-line medication for REM sleep behavior disorder. It usually has fewer side effects than other medication options but has similar efficacy 61. Melatonin is also a safer option for elderly individuals, individuals with dementia, fall risk, or those with sleep apnea. The dosage of melatonin one should take for REM sleep behavior is different than when taking it to fall asleep, and you should consult a sleep physician.
The prescription drug clonazepam has proven effective in reducing symptoms for 50-80% of individuals with REM sleep disorder 62. However, it can cause some side effects, including sleepiness, forgetfulness, and impaired balance in the morning. It can also contribute to or worsen sleep apnea 63.
Always consult a doctor before taking any prescription or over-the-counter medication. They can best advise you on a treatment plan based on your medical history and symptoms.
Injury Prevention Techniques
Establishing a safe sleep environment is one of the most important things someone with REM behavior sleep disorder can do. Sleep-related injuries — including bruising, cuts, fractures, blunt trauma, and head trauma have been reported among 30 to 81 percent of individuals with REM sleep behavior disorder. In addition, the bed partner is also at risk for injury when they are sleeping next to someone who unknowingly acts out violent dreams
Recommendations for injury prevention may include:
- Removing sharp objects and weapons from the bedroom
- Placing padding on the floor around the bed
- Installing padded bed rails on the side of the bed
- Putting the mattress on the floor
- Moving furniture and clutter away from the bed
- Padding the corners of furniture in the bedroom
- Protecting bedroom windows
If the individual shares their bed with a sleep partner, it may also be recommended that they sleep in separate beds or separate rooms until symptoms are well treated.
Multiple system atrophy signs and symptoms
Multiple system atrophy (MSA) affects people in different ways, depending on which muscles are affected. The main symptom of multiple system atrophy (MSA) is losing control of muscles in your body. This happens gradually in some people and quickly in others.
For both types of multiple system atrophy, the autonomic nervous system doesn’t work properly. The autonomic nervous system controls involuntary functions in the body, such as blood pressure. When this system doesn’t work properly, it can cause the following symptoms.
Some of the most common symptoms multiple system atrophy (MSA) include:
- Bladder problems including urgency, frequency (needing to pee more often), nocturia (passing urine at night), urine retention (inability to empty the bladder) and leaking urine (incontinence)
- Feeling dizzy and faint when standing up (orthostatic hypotension or postural hypotension) due to a sudden drop in blood pressure when changing position – particularly from lying or sitting to standing.
- Postural hypotension (orthostatic hypotension) is a form of low blood pressure. People who have this type of low blood pressure feel dizzy or lightheaded when they stand up after sitting or lying down. They may even faint. Not everyone with multiple system atrophy has postural hypotension (orthostatic hypotension).
- People with multiple system atrophy also can develop dangerously high blood pressure levels while lying down. This is called supine hypertension.
- Erectile dysfunction (trouble getting or keeping an erection) in men and sexual dysfunction in women (trouble with lubrication during sex and having an orgasm and loss of interest in sex)
- Bowel problems such as constipation.
- Loss of bladder or bowel control, known as incontinence.
- Slow, clumsy or unsteady movement
- Slurred speech
- Stiff, tense muscles that may be painful.
- A posture in which the body leans involuntarily to one side known as Pisa syndrome
- Anterocollis, in which the neck bends forward and the head drops down
- Changes in sweat production. People with multiple system atrophy may:
- Produce less sweat. Dry skin due to reduced sweating (anhidrosis)
- Have heat intolerance because they sweat less.
- Have poor body temperature control, often causing cold hands or feet.
- Conditions that affect sleep. Sleep symptoms may include:
- Agitated sleep due to “acting out” dreams. This is known as rapid eye movement sleep behavior disorder (RBD).
- Breathing that stops and starts during sleep, known as sleep apnea.
- A high-pitched whistling sound while breathing, called stridor.
Parkinsonism symptoms
- Feeling slow and stiff when moving
- Difficulty in starting to move
- Writing becoming small and spidery
- Difficulty turning in bed
Cerebellar dysfunction symptoms
- Feeling clumsy, dropping things
- Finding it difficult to fasten buttons
- Feeling unsteady in crowds
- Unable to balance without support
- Difficulty writing
- Slurred speech
Autonomic nervous system dysfunction symptoms
- Difficulties with sexual function
- Bladder problems
- Feeling dizzy or fainting (blood pressure problems)
- Pain around neck and shoulders known as ‘coat-hanger pain’
- Altered bowel function
- Cold hands and feet due to poor blood flow (Raynaud’s phenomenon)
- Color changes in the hands and feet.
- Problems with sweating control
Multiple system atrophy (MSA) can also cause a wide range of other symptoms, such as:
- feeling too hot or too cold
- trouble sleeping
- noisy breathing, unintentional sighing and snoring
- finding it difficult to chew or swallow
- constipation (finding it hard to poo)
- trouble controlling emotions, such as laughing or crying when not expected called emotional lability
- weakness in arms and legs
- restless sleep
- daytime sleepiness
- nightmares
- noisy breathing during the day, excessive snoring at night
- unintentional sighing
- weak, quiet voice
- difficulty with chewing, swallowing and coughing at mealtimes
- blurred vision.
The symptoms of multiple system atrophy most often begin in people over 50 years old. Multiple system atrophy (MSA) does not usually affect people under 30 years old.
Multiple system atrophy complications
Complications of multiple system atrophy (MSA) vary from person to person. Multiple system atrophy is a progressive disease where the symptoms get worse over time. The symptoms can make daily activities harder as time goes on.
Multiple system atrophy (MSA) possible complications include:
- Worsening breathing symptoms during sleep.
- Injuries from falls caused by poor balance or fainting.
- The breakdown of the skin in people who have trouble moving or can’t move.
- Not being able to care for yourself in day-to-day activities.
- Vocal cord paralysis, which affects speech and breathing.
- Increased trouble swallowing.
Multiple system atrophy diagnosis
If your family doctor thinks you have symptoms of multiple system atrophy (MSA) or a similar condition, she/he will usually refer you to a brain and nerve specialist called a neurologist. A neurologist may diagnose multiple system atrophy based on your symptoms, how long you’ve had them and how quickly they’re getting worse. In the early stages of multiple system atrophy (MSA), the symptoms can also be very similar to other conditions such as Parkinson’s disease.
The diagnosis of multiple system atrophy is a clinical one and depends on your neurologist recognizing a combination of symptoms and signs using a specific set of criteria. However, it can be difficult to diagnose multiple system atrophy, as there’s no specific test for it. Your neurologist may need to order some tests first to investigate your symptoms and what could be causing them.
Diagnosis of multiple system atrophy is based on medical history and detailed examination for the characteristic clinical features, brain scan findings and absence of certain features.
- Magnetic resonance imaging (MRI) may identify changes that suggest multiple system atrophy or rule out other causes of the symptoms.
- Positron emission tomography (PET) scans can be used to monitor metabolic function in specific parts of the brain.
- Dopamine transporter (DaT) scans can assess the distribution and activity of dopamine in the brain.
Core motor symptoms include:
- Parkinsonism, including bradykinesia along with stiffness (rigidity) or a tremor, that usually respond poorly to Parkinson’s medications like levodopa
- Cerebellar problems, including trouble with walking (gait ataxia), clumsy movements of the arms or legs (limb ataxia), slurred or difficult speech (cerebellar dysarthria) and problems moving the eyes normally (like constant eye jerking or over-shooting when moving between targets)
Core autonomic symptoms:
- Bladder problems including unexplained trouble urinating, frequent urgency, leakage, or a large amount of urine left in the bladder after trying to empty it (over 100 mL), without other causes like prostate issues
- Blood pressure problems: a significant drop in blood pressure, at least 20 points, when standing up or during a tilt table test, usually within 3 minutes
- In people with symptoms of faintness it is important to take the blood pressure first lying (supine) and then after 2 and 3 minutes standing, and to record the drop in the upper (systolic) and lower (diastolic) figure. An otherwise unexplained systolic drop of more than 20 mm is abnormal and one of over 30 mm more so.
- During a tilt table test, a patient lies down flat on a table and straps are placed around the body to hold the patient in place. Then, the table is raised with the person’s head in the upward position, which simulates the action of a person standing from a sitting or lying down position. This test allows the doctor to measure the heart rate and blood pressure in such situations.
Supportive clinical features not required for diagnosis but make the diagnosis more likely include:
- Rapid worsening of movement symptoms within the first 3 years
- Serious balance problems and falls within 3 years
- Abnormal twisting of the neck (dystonia) made worse by levodopa
- Severe speech or swallowing problems within 3 years
- Unexplained reflex changes (Babinski sign)
- Jerky or irregular tremor
- Postural problems like head dropping forward (anterocollis), leaning to the side (laterocollis), or forward bending of the spine (camptocormia)
- Stridor (a harsh breathing sound), frequent deep sighs, cold and discolored hands and feet
- Erectile dysfunction starting before age 60
- Episodes of sudden laughing or crying without clear cause
Brain scans (neuroimaging) may show:
- Shrinking (atrophy) of areas like the putamen, pons, middle cerebellar peduncles, or cerebellum
- Loss of normal signal in the putamen on special MRI scans
- A special finding called the “hot cross bun” sign in the pons (brainstem)
- Changes in water movement (diffusivity) in certain brain areas
The diagnosis of multiple system atrophy may be excluded if any of these are present:
- A strong and lasting response to Parkinson’s drugs
- Loss of smell without explanation
- Abnormal heart nerve imaging (MIBG scan)
- Early signs of dementia
- Early visual hallucinations (within the first 3 years)
- Eye movement problems typical of other diseases like PSP (difficulty moving eyes downward)
- Brain scans suggesting another disease (like multiple sclerosis, strokes, or other Parkinsonism types)
- A known medical condition that can cause similar symptoms
The diagnosis of multiple system atrophy can be made in a person who meets the following criteria:
- Symptoms starting in an adult older than 30 years
- Symptoms getting worse over time (progressive)
- At least one autonomic symptom (like bladder or blood pressure problems)
- Parkinsonism and/or cerebellar symptoms with at least two features
- At least two supportive clinical features
- At least one MRI finding that supports the diagnosis
- No features that suggest another disease
Multiple system atrophy is a probable diagnosis (likely but not 100% certain) in these situations:
- Starts after age 30 and worsens over time
- At least two of the following:
- Autonomic symptoms
- Parkinsonism
- Cerebellar symptoms
- At least one supportive clinical feature
- No features pointing to a different diagnosis
Tilt table test
Tilt table test evaluates your blood pressure control. In this procedure, you’re placed on a motorized table. Straps hold you in place. Then the table is tilted upward so that your body is positioned at a 70-degree angle. During the tilt table test, your doctor watches for changes in your blood pressure and heart rate. The test can show if your blood pressure doesn’t respond in a typical way when changing position.
Tests of autonomic functions
Other tests can look at blood pressure control and other involuntary functions, including:
- Blood pressure measurement, lying down and standing, without the use of a tilt table.
- A sweat test to evaluate areas of the body that sweat.
- Tests that look at bladder and bowel function.
- Electrocardiogram to track the electrical signals of your heart.
You might need a sleep study if you stop breathing during sleep or if you snore or have other sleep symptoms. The test can help diagnose a sleep condition that can be treated, such as sleep apnea.
Multiple system atrophy diagnostic criteria
| Essential features | A sporadic, progressive adult (>30 years) onset disease | ||
| Clinically established multiple system atrophy | Clinically probable multiple system atrophy | ||
| Core clinical features | Autonomic dysfunction defined as (at least one is required)
and at least one of
| At least two of:
2. Parkinsonism 3. Cerebellar syndrome (at least one of gait ataxia, limb ataxia, cerebellar dysarthria, or oculomotor features) | |
| Supportive clinical (motor or non‐motor) features | At least two | At least one a | |
| MRI marker | At least one | Not required | |
| Exclusion criteria | Absence | Absence | |
| Supportive clinical features | |||
| Supportive motor features | Rapid progression within 3 years of motor onset | Supportive non‐motor features | Stridor |
| Moderate to severe postural instability within 3 years of motor onset | Inspiratory sighs | ||
| Craniocervical dystonia induced or exacerbated by L‐dopa in the absence of limb dyskinesia | Cold discolored hands and feet | ||
| Severe speech impairment within 3 years of motor onset | Erectile dysfunction (below age of 60 years for clinically probable MSA) | ||
| Severe dysphagia within 3 years of motor onset | Pathologic laughter or crying | ||
| Unexplained Babinski sign | |||
| Jerky myoclonic postural or kinetic tremor | |||
| Postural deformities | |||
| MRI markers of clinically established MSA | |||
| Each affected brain region as evidenced by either atrophy or increased diffusivity counts as one MRI marker. | |||
| For MSA‐parkinsonian type (MSA‐P) Atrophy of:
Increased diffusivity of:
| For MSA‐cerebellar type (MSA‐C) Atrophy of:
Increased diffusivity of:
| ||
| Exclusion criteria | |||
| Substantial and persistent beneficial response to dopaminergic medications | |||
| Unexplained anosmia on olfactory testing | |||
| Fluctuating cognition with pronounced variation in attention and alertness and early decline in visuoperceptual abilities | |||
| Recurrent visual hallucinations not induced by drugs within 3 years of disease onset | |||
| Dementia according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM‐V) within 3 years of disease onset | |||
| Downgaze supranuclear palsy or slowing of vertical saccades | |||
| Brain MRI findings suggestive of an alternative diagnosis (eg, PSP, multiple sclerosis, vascular parkinsonism, symptomatic cerebellar disease, etc.) | |||
| Documentation of an alternative condition (MSA look‐alike, including genetic or symptomatic ataxia and parkinsonism) known to produce autonomic failure, ataxia, or parkinsonism and plausibly connected to the patient’s symptoms | |||
Footnotes: a Excluding erectile dysfunction as an isolated feature.
Abbreviations: MSA = multiple system atrophy; MSA‐P = MSA‐parkinsonian type; MSA‐C = MSA‐cerebellar type; OH = orthostatic hypotension; MRI = magnetic resonance imaging; DSM‐V = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; PSP = progressive supranuclear palsy.
[Source 36 ]Multiple system atrophy differential diagnosis
Symptoms of the following disorders can be similar to those of multiple system atrophy. Comparisons may be useful for a differential diagnosis.
Parkinson’s disease is a slowly progressive neurologic movement disorder characterized by involuntary, resting tremor, muscular stiffness or lack of flexibility (rigidity), slowness of movement (bradykinesia) and difficulty controlling voluntary movements. It also commonly causes autonomic symptoms and, in advanced, older, patients, dementia. Parkinson’s disease usually begins in late adulthood. It is slowly progressive but may not become incapacitating for many years.
Symptoms like those of Parkinson’s disease (Parkinsonian symptoms) may also develop secondary to hydrocephalus (a condition in which excessive cerebrospinal fluid accumulates the spaces in the brain (ventricles), increasing pressure in the brain. Parkinsonian symptoms may also occur because of head trauma, inflammation of the brain (encephalitis), strokes (infarcts), or tumors deep within the cerebral hemispheres (cerebrum) and base of the brain (i.e., basal ganglia), or exposure to certain drugs and toxins.
Progressive supranuclear palsy (PSP) is a rare degenerative neurological disorder characterized by postural instability and falls, often backwards, loss of control of voluntary eye movement (supranuclear gaze palsy or SNGP), impaired voluntary muscle activity (akinesia), abnormal stiffness (rigidity), speech difficulties (dysarthria) and problems related to swallowing and eating (dysphagia). The presence of vertical eye movement abnormalities and the absence of orthostatic hypotension suggest progressive supranuclear palsy (PSP). Unlike multiple system atrophy, in which alpha-synuclein accumulates in the brain, a different protein called tau accumulates in progressive supranuclear palsy (PSP). The mean onset age is 60-65 years.
Corticobasal degeneration (CBD) is an even rarer progressive neurological disorder characterized by cell loss and shrinkage (atrophy) in certain areas of the brain (cerebral cortex and substantia nigra). Apraxia is a relatively unusual sign, and its presence suggests corticobasal degeneration rather than multiple system atrophy. As in progressive supranuclear palsy (PSP), a different protein called tau accumulates in the brain in corticobasal degeneration.
Hereditary olivopontocerebellar atrophy (OPCA) describes a group of rare disorders characterized by progressive balance problems (disequilibrium), progressive impairment of the ability to coordinate voluntary movements (cerebellar ataxia) and difficulty speaking or slurred speech (dysarthria). Additional symptoms may include generalized weakness, difficulty swallowing (dysphagia) and/or the progressive loss of intellectual abilities and mental deterioration (dementia). There are several forms of hereditary olivopontocerebellar atrophy (OPCA).
Pure autonomic failure (PAF) is very rare and characterized by orthostatic hypotension that has been present for 5 years or more without other evidence of a neurological condition. Orthostatic hypotension is a condition in which an excessive decrease in blood pressure occurs upon standing potentially resulting in dizziness or momentary loss of consciousness (syncope). Additional symptoms associated with autonomic failure include fatigue, blurred vision, impaired bladder and bowel control and impotence. In some people, the skin may become extremely dry because of decreased ability to sweat.
Multiple system atrophy treatment
Treatment for people with multiple system atrophy involves a combination of medication, specialized equipment and the involvement of therapists to manage specific symptoms. Ideally, you will be supported by your primary care physician who will act as a care coordinator and refer you to other members of your healthcare team. It is quite possible your primary care physician has not previously seen a patient with multiple system atrophy before.
Affected people need to be seen by several specialists including neurologists, physical therapists, speech therapists and mental health professionals. These specialists should work together as a team, in a coordinated way, for the best management.
Depression often occurs in people with multiple system atrophy and can be treated with counseling, support for the family and sometimes medications.
Multiple system atrophy medications
The medicines you are prescribed will vary depending on your symptoms. Medications are very individual and what works for one person may not be effective for another. Your specialist will prescribe the best combination to meet your needs. Below are some of the medications and treatments commonly used in multiple system atrophy.
Drugs to help stiffness and slowness are the same drugs used in Parkinson’s disease. They are often not as effective in multiple system atrophy and can make your blood pressure problems worse. It
may take time to find what suits you and if a medication is not useful it may be reduced or discontinued on the advice of your specialist.
- Levodopa (Madopar or Sinemet)
- Amantadine (Symmetrel)
- Dopamine agonists such as ropinirole (Requip) and pramipexole (Mirapexin) may be used in conjunction with levodopa
Medications that are used to treat people with Parkinson’s disease, most notably levodopa given in tablets of Sinemet (combination of levodopa and carbidopa), may also be prescribed for individuals with multiple system atrophy. However, the effectiveness of such medications varies greatly among affected people. In many people, it is not effective, or it is only partially effective. About 1/3 of affected people improve with levodopa therapy. However, in most people, the effectiveness of this therapy decreases over time. In addition, these drugs must be used with caution because they may lower blood pressure.
Other drugs used to treat Parkinson’s disease may be used to treat individuals with multiple system atrophy. These include dopamine agonists such as ropinirole (Requip) and pramipexole (Mirapexin) and an antiviral drug known as amantadine (Symmetrel).
If symptoms respond well to levodopa but pills are no longer enough, some patients might benefit from a special intestinal gel form of levodopa delivered through a pump.
Balance difficulties
Feeling unsafe on stairs and elsewhere may be due to problems with balance and people often feel they need to hold on to things for support.
Physical and occupational therapy are important:
- Physical therapy helps maintain walking ability and prevent falls.
- Occupational therapy helps people stay independent longer with everyday tasks.
Physiotherapists and occupational therapists can provide advice and equipment to help you move safely. For example, they can suggest where handrails can help or where raised seating can aid people when rising to stand.
Physiotherapy can be helpful and also provide you with tips to get you moving. Your physiotherapist can give you specific exercises to do which may help to prevent falls. In addition, affected individuals may be unable to walk unassisted or may require a wheelchair.
Dizziness
Dizziness may be due to your blood pressure falling when you stand up or change position. This drop in blood pressure upon standing is called postural hypotension or orthostatic hypotension. There are several ways to relieve this. These include increasing your fluid and salt intake as well as leg exercises to help blood flow in your calves. It is important that you avoid sudden changes in position like quickly rising to your feet and plan your periods of activity accordingly. Using a head-up tilt of the bed at night, by ingestion of 500mls water before exertion, rising slowly and avoiding heavy carbohydrate meals, and using abdominal binders and compression hosiery can also be helpful.
If the drop in blood pressure is significant, and cannot be managed by non-drug methods, medications may be suggested by your specialist:
- Fludrocortisone (Florinef) – A corticosteroid derivative, taken in very small doses. This drug must be used with caution and monitored carefully by a doctor for possible side effects.
- Ephedrine – Works quickly to raise blood pressure; usually taken three times a day
- Midodrine hydrochloride (ProAmatine) has been approved by the U.S. Food and Drug Administration (FDA) for the treatment of low blood pressure sometimes associated with multiple system atrophy. It works quickly to raise blood pressure within 30-60 minutes; usually taken three times a day. Only prescribed by specialists.
The drug L-threo-dihydroxyphenylserine (L-DOPS or L-threo-DOPS) can also be used to treat low blood pressure.
Blood pressure issues after meals (postprandial hypotension) can also happen. Simple changes like eating smaller meals and walking after eating can help. Some medications can be used in severe cases.
Difficulties with bladder control
Urologist and continence specialists can assess your symptoms and recommend treatment to help manage bladder issues. People with multiple system atrophy may also find that they are not fully emptying their bladder when urinating. If you are leaving behind some urine it can make you more likely to experience urine infections. If this becomes a major problem, there is currently no effective medication for this and bladder surgery is very unlikely to lead to improvement.
Bladder problems are usually managed with:
- Lifestyle tips like cutting down on caffeine and alcohol
- Medications like mirabegron which helps relax the bladder and has fewer side effects than older drugs. Some older bladder medications (like oxybutynin) can cause confusion and are usually avoided.
- Catheters for someone who can’t empty their bladder properly.
- Intermittent catheterization (a procedure to periodically drain urine from the bladder using a urinary catheter, which is inserted through the urethra and immediately removed once the bladder is empty), either by you or a carer, is the best management.
- Catheterization is the process of putting a tube into the bladder to allow urine to drain. This may be done intermittently and then removed. Or it may be placed permanently, either through the urethra or through the abdominal wall. A continence advisor can help you learn the technique.
People with multiple system atrophy who have postural hypotension produce less urine during the day and more at night. There are medications such as DDAVP or Desmopressin that can help with nocturia. These do have side effects so will be discussed between you and your specialist, if it is thought they may be helpful.
Also, you may want to think about having a commode or urinal at your bedside to reduce the effort of getting to the bathroom. This is especially important if you have low blood pressure (postural hypotension) or are prone to falls.
Antibiotics
An infection in someone with multiple system atrophy can suddenly worsen all symptoms of multiple system atrophy and should be promptly treated with antibiotics. Urinary and respiratory infections are the most common. People with multiple system atrophy may not have a raised temperature with an infection. If there is a sudden worsening of multiple system atrophy symptoms,
your doctor should always consider if an infection is present and treat it accordingly.
Constipation
Constipation is common in people living with multiple system atrophy. Constipation is to be avoided where possible as straining could affect your blood pressure and make other symptoms worse. It is important to drink plenty of fluids and eat a well-balanced diet. Dietary fiber, especially cereal-derived fiber, may not help with bowel emptying. Daily medication to prevent constipation is often needed to maintain a regular bowel habit. Suppositories can be helpful to avoid straining. For some people with multiple system atrophy loose bowel movements or diarrhea can be troublesome.
Swallowing difficulty
Coughing whilst eating and drinking may be an indication of swallowing difficulties. Coughing is a normal reaction to help prevent food going into your lungs and causing infection. A Speech and Language Therapist helps with swallowing and communication problems. Early referral to speech therapy is important because swallowing problems can get worse over time. A Speech and Language Therapist can assess the safety of your swallow and, together with a Dietitian, can advise on the best type of food for you.
When there is a risk of aspiration due to swallowing difficulty, a feeding tube may be inserted directly into the stomach (gastrostomy tube). A tracheostomy may be required for life-threatening breathing complications, daytime stridor, or abnormal vocal cord mobility. A tracheostomy is a procedure during which a tube is placed through a surgical opening in the throat to prevent breathing difficulties.
For specific muscle issues (twisted neck muscles or eyelid spasms), botulinum toxin injections (Botox) may help but they need to be used carefully, especially if the person already has trouble swallowing.
Sleep disorders
You may experience irregular breathing at night. Missing a breath or not taking deep enough breaths (sleep apnea) can sometimes happen and may be associated with increased snoring. If you feel tired and lethargic during the day, it may mean that you have a sleep disturbance. Sleep studies are recommended to check breathing during sleep. Studies of your sleeping behavior can be carried out at a sleep center to see how this may be affecting you. Breathing problems, especially a high-pitched breathing noise called stridor that can be serious and sometimes life-threatening, are managed with CPAP machines (continuous positive airway pressure) at night to help with breathing. This equipment can help improve your quality of sleep and can travel with you wherever there is electrical power.
Sleep disorders like acting out dreams (REM sleep behavior disorder) are also common and can be treated with melatonin or clonazepam to make sleep safer.
Sexual Dysfunction
For men, erectile dysfunction (inability to achieve or maintaining an erection) is often the first symptom of multiple system atrophy in men. Men often take medication for this problem such as sildenafil (Viagra), tadalafil (Cialis) or vardenafil (Levitra). However, these medications can worsen blood pressure control, these drugs may worsen low blood pressure and faintness, so other measures may be an option. Woman may also experience impaired libido and sexual function. Seeking help on this issue is therefore important so you should not be embarrassed to talk with your doctor, who can support you and refer you to a specialist if necessary.
Emotional lability
Emotional reactions may be appropriate in the situation, but the behavior or expression may be stronger, louder, or last longer than would be usual for you. This is called emotional lability. For example, a person may be genuinely happy but once the laughter has started they may be unable to stop or regulate the behavior. This could include laughing or crying too loudly, too much, or for too long.
An individual living with multiple system atrophy may also show extreme but genuine emotional responses, including sadness and grief, despair, frustration and irritability, anger, anxiety and
depression, joy, happiness and pleasure.
Aids and equipment
There are many items, aids and pieces of equipment that may prove useful to help overcome some of the difficulties connected with multiple system atrophy. However, some of these can be expensive so you should discuss with the relevant therapist in your support team before buying anything.
Home remedies
Some lifestyle and home remedies can help minimize multiple system atrophy (MSA) symptoms.
- Take steps to raise your blood pressure. Add a little salt to your diet and drink more fluids, especially before exercise. Salt and fluids can increase blood volume and raise your blood pressure.
- Drink coffee and other fluids that contain caffeine to increase your blood pressure.
- Raise the head of your bed. Raising the head of your bed by about 4 to 6 inches (10 to 15 centimeters) helps control your blood pressure when you sleep. Get up slowly after lying down.
- Make dietary changes. Eat more fiber to ease constipation. Laxatives or stool softeners may help. You can get them without a prescription. Also eat small, low-carbohydrate meals.
- Don’t get too hot. Stay in air-conditioned rooms on very hot days. Make sure the bathroom doesn’t become too hot when you shower or bathe.
- Wear elastic support stockings up to your waist. This can help keep your blood pressure from dropping.
Multiple system atrophy prognosis
The prognosis (outcome) for multiple system atrophy is poor. Multiple system atrophy is a progressive disease, which means that multiple system atrophy symptoms will worsen over time. As things progress, people will need help to manage day to day living. The speed of these changes is difficult to predict as people with multiple system atrophy experience the condition differently and the rate of progression varies. Symptoms of multiple system atrophy may vary depending on which form of multiple system atrophy predominates, but in general, it can cause the progressive loss of motor skills and approximately 50% of individuals are wheelchair-bound within 5-6 years of the onset of motor symptoms. Eventually, affected individuals may become confined to bed and have life-threatening complications. Loss of mental and physical functions slowly get worse. Early death is likely. People typically live 7 to 10 years after multiple system atrophy symptoms first appear, although some pathology-proven cases survived more than 15 years 64, 65, 42, 66. However, the survival rate with multiple system atrophy varies widely. About 80% of patients are disabled within 5 years of the onset of motor symptoms. It is estimated that only 20% of multiple system atrophy patients survive beyond 12 years. Patients continue to experience neurological degeneration until they lose motor skills, become confined to bed, and eventually pass away. Many multiple system atrophy patients succumb to pneumonia and other respiratory infections, choking or cardiac arrest. Death is often due to trouble breathing, infections or blood clots in the lungs. Other characteristics have been associated with increased mortality after diagnosis, including frequent falls, female gender, and the presence of severe autonomic symptoms 67.
- Ndayisaba A, Halliday GM, Khurana V. Multiple System Atrophy: Pathology, Pathogenesis, and Path Forward. Annu Rev Pathol. 2025 Jan;20(1):245-273. https://www.annualreviews.org/content/journals/10.1146/annurev-pathmechdis-051122-104528[↩][↩]
- Stankovic I, Kuijpers M, Kaufmann H. An update on multiple system atrophy. Curr Opin Neurol. 2024 Aug 1;37(4):400-408. doi: 10.1097/WCO.0000000000001285[↩]
- Liu M, Wang Z, Shang H. Multiple system atrophy: an update and emerging directions of biomarkers and clinical trials. J Neurol. 2024 May;271(5):2324-2344. doi: 10.1007/s00415-024-12269-5[↩][↩]
- Krismer F, Fanciulli A, Meissner WG, Coon EA, Wenning GK. Multiple system atrophy: advances in pathophysiology, diagnosis, and treatment. Lancet Neurol. 2024 Dec;23(12):1252-1266. doi: 10.1016/S1474-4422(24)00396-X[↩]
- Stankovic I, Fanciulli A, Sidoroff V, Wenning GK. A Review on the Clinical Diagnosis of Multiple System Atrophy. Cerebellum. 2023 Oct;22(5):825-839. doi: 10.1007/s12311-022-01453-w[↩]
- Leńska-Mieciek M, Madetko-Alster N, Alster P, Królicki L, Fiszer U, Koziorowski D. Inflammation in multiple system atrophy. Front Immunol. 2023 Jun 22;14:1214677. doi: 10.3389/fimmu.2023.1214677[↩]
- Claassen DO. Multiple System Atrophy. Continuum (Minneap Minn). 2022 Oct 1;28(5):1350-1363. doi: 10.1212/CON.0000000000001154[↩]
- Fecek C, Nagalli S. Shy-Drager Syndrome. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560502[↩]
- Gilman S, Low PA, Quinn N, Albanese A, Ben-Shlomo Y, Fowler CJ, Kaufmann H, Klockgether T, Lang AE, Lantos PL, Litvan I, Mathias CJ, Oliver E, Robertson D, Schatz I, Wenning GK. Consensus statement on the diagnosis of multiple system atrophy. J Auton Nerv Syst. 1998 Dec 11;74(2-3):189-92.[↩][↩][↩]
- Multiple system atrophy. https://medlineplus.gov/genetics/condition/multiple-system-atrophy[↩]
- Palma JA, Norcliffe-Kaufmann L, Kaufmann H. Diagnosis of multiple system atrophy. Auton Neurosci. 2018 May;211:15-25. doi: 10.1016/j.autneu.2017.10.007[↩][↩][↩][↩]
- Papp MI, Kahn JE, Lantos PL. Glial cytoplasmic inclusions in the CNS of patients with multiple system atrophy (striatonigral degeneration, olivopontocerebellar atrophy and Shy-Drager syndrome) J Neurol Sci. 1989;94(1–3):79–100. doi: 10.1016/0022-510x(89)90219-0[↩]
- Jellinger KA. Multiple system atrophy: an oligodendroglioneural synucleinopathy1. J Alzheimers Dis. 2018;62(3):1141–1179. doi: 10.3233/JAD-170397[↩]
- Spillantini MG, et al. Filamentous alpha-synuclein inclusions link multiple system atrophy with Parkinson’s disease and dementia with Lewy bodies. Neurosci Lett. 1998;251(3):205–208. doi: 10.1016/s0304-3940(98)00504-7[↩]
- Gilman S, Wenning GK, Low PA, Brooks DJ, Mathias CJ, Trojanowski JQ, Wood NW, Colosimo C, Dürr A, Fowler CJ, Kaufmann H, Klockgether T, Lees A, Poewe W, Quinn N, Revesz T, Robertson D, Sandroni P, Seppi K, Vidailhet M. Second consensus statement on the diagnosis of multiple system atrophy. Neurology. 2008 Aug 26;71(9):670-6. doi: 10.1212/01.wnl.0000324625.00404.15[↩][↩]
- Multiple System Atrophy. https://rarediseases.org/rare-diseases/multiple-system-atrophy[↩][↩][↩]
- Multiple System Atrophy. https://www.ninds.nih.gov/health-information/disorders/multiple-system-atrophy[↩]
- Pham CK, Sankari A, Slowik JM. Rapid Eye Movement Sleep Behavior Disorder. [Updated 2024 Feb 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555928[↩][↩][↩]
- Boeve BF. REM sleep behavior disorder: Updated review of the core features, the REM sleep behavior disorder-neurodegenerative disease association, evolving concepts, controversies, and future directions. Ann N Y Acad Sci. 2010 Jan;1184:15-54. doi: 10.1111/j.1749-6632.2009.05115.x[↩][↩][↩]
- REM Sleep Behavior Disorder. https://www.sleepfoundation.org/parasomnias/rem-sleep-behavior-disorder[↩][↩][↩][↩][↩]
- Maldonado KA, Alsayouri K. Physiology, Brain. [Updated 2023 Mar 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551718[↩][↩][↩]
- Young CB, Reddy V, Sonne J. Neuroanatomy, Basal Ganglia. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537141[↩][↩]
- Yahya K. The basal ganglia corticostriatal loops and conditional learning. Rev Neurosci. 2020 Oct 28;32(2):181-190. doi: 10.1515/revneuro-2020-0047[↩]
- Stocco A, Lebiere C, Anderson JR. Conditional routing of information to the cortex: a model of the basal ganglia’s role in cognitive coordination. Psychol Rev. 2010 Apr;117(2):541-74. doi: 10.1037/a0019077[↩]
- Mathai A, Smith Y. The corticostriatal and corticosubthalamic pathways: two entries, one target. So what? Front Syst Neurosci. 2011 Aug 1;5:64. doi: 10.3389/fnsys.2011.00064[↩]
- Basal Ganglia. https://storymd.com/journal/j47z2dgcnj-primary-familial-brain-calcification/page/49dp5flnroe-basal-ganglia[↩]
- Jimsheleishvili S, Dididze M. Neuroanatomy, Cerebellum. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538167[↩][↩]
- Roostaei T, Nazeri A, Sahraian MA, Minagar A. The human cerebellum: a review of physiologic neuroanatomy. Neurol Clin. 2014 Nov;32(4):859-69. doi: 10.1016/j.ncl.2014.07.013[↩][↩]
- Witter L, De Zeeuw CI. Regional functionality of the cerebellum. Curr Opin Neurobiol. 2015 Aug;33:150-5. doi: 10.1016/j.conb.2015.03.017[↩]
- Manto M, Bower JM, Conforto AB, et al. Consensus paper: roles of the cerebellum in motor control–the diversity of ideas on cerebellar involvement in movement. Cerebellum. 2012 Jun;11(2):457-87. doi: 10.1007/s12311-011-0331-9[↩]
- Van Essen DC, Donahue CJ, Glasser MF. Development and Evolution of Cerebral and Cerebellar Cortex. Brain Behav Evol. 2018;91(3):158-169. doi: 10.1159/000489943[↩]
- Xie YY, Zhang XY, Zhu JN. The cognitive functions of the cerebellum and its role in neurodegenerative diseases. Ageing Neur Dis 2024;4:18. https://dx.doi.org/10.20517/and.2024.27[↩]
- LeBouef T, Yaker Z, Whited L. Physiology, Autonomic Nervous System. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538516[↩][↩][↩][↩]
- McCorry LK. Physiology of the autonomic nervous system. Am J Pharm Educ. 2007 Aug 15;71(4):78. doi: 10.5688/aj710478[↩]
- Gibbins I. Functional organization of autonomic neural pathways. Organogenesis. 2013 Jul-Sep;9(3):169-75. doi: 10.4161/org.25126[↩]
- Wenning GK, Stankovic I, Vignatelli L, et al. The Movement Disorder Society Criteria for the Diagnosis of Multiple System Atrophy. Mov Disord. 2022 Jun;37(6):1131-1148. doi: 10.1002/mds.29005[↩][↩]
- McHugh J, Keller NR, Appalsamy M, Thomas SA, Raj SR, Diedrich A, Biaggioni I, Jordan J, Robertson D. Portal osmopressor mechanism linked to transient receptor potential vanilloid 4 and blood pressure control. Hypertension. 2010 Jun;55(6):1438-43. doi: 10.1161/HYPERTENSIONAHA.110.151860[↩]
- Mai TH, Garland EM, Diedrich A, Robertson D. Hepatic and renal mechanisms underlying the osmopressor response. Auton Neurosci. 2017 Mar;203:58-66. doi: 10.1016/j.autneu.2017.01.007[↩]
- Stock JM, Chelimsky G, Edwards DG, Farquhar WB. Dietary sodium and health: How much is too much for those with orthostatic disorders? Auton Neurosci. 2022 Mar;238:102947. doi: 10.1016/j.autneu.2022.102947[↩]
- SHY GM, DRAGER GA. A Neurological Syndrome Associated with Orthostatic Hypotension: A Clinical-Pathologic Study. AMA Arch Neurol. 1960;2(5):511–527. doi:10.1001/archneur.1960.03840110025004[↩]
- Gilman S, Low PA, Quinn N, Albanese A, Ben-Shlomo Y, Fowler CJ, Kaufmann H, Klockgether T, Lang AE, Lantos PL, Litvan I, Mathias CJ, Oliver E, Robertson D, Schatz I, Wenning GK. Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci. 1999 Feb 1;163(1):94-8. doi: 10.1016/s0022-510x(98)00304-9[↩]
- Multiple system atrophy – parkinsonian type. https://medlineplus.gov/ency/article/000757.htm[↩][↩][↩]
- Multiple system atrophy – cerebellar subtype. https://medlineplus.gov/ency/article/000758.htm[↩][↩][↩][↩]
- Barca E, Kleiner G, Tang G, Ziosi M, Tadesse S, Masliah E, Louis ED, Faust P, Kang UJ, Torres J, Cortes EP, Vonsattel JP, Kuo SH, Quinzii CM. Decreased Coenzyme Q10 Levels in Multiple System Atrophy Cerebellum. J Neuropathol Exp Neurol. 2016 Jul;75(7):663-72. doi: 10.1093/jnen/nlw037[↩]
- Schottlaender LV, Bettencourt C, Kiely AP, Chalasani A, Neergheen V, Holton JL, Hargreaves I, Houlden H. Coenzyme Q10 Levels Are Decreased in the Cerebellum of Multiple-System Atrophy Patients. PLoS One. 2016 Feb 19;11(2):e0149557. doi: 10.1371/journal.pone.0149557[↩]
- Multiple-System Atrophy Research Collaboration. Mutations in COQ2 in familial and sporadic multiple-system atrophy. N Engl J Med. 2013 Jul 18;369(3):233-44. doi: 10.1056/NEJMoa1212115 Erratum in: N Engl J Med. 2014 Jul 3;371(1):94.[↩]
- Papp MI, Kahn JE, Lantos PL. Glial cytoplasmic inclusions in the CNS of patients with multiple system atrophy (striatonigral degeneration, olivopontocerebellar atrophy and Shy-Drager syndrome). J Neurol Sci. 1989 Dec;94(1-3):79-100. doi: 10.1016/0022-510x(89)90219-0[↩]
- Trojanowski JQ, Revesz T; Neuropathology Working Group on MSA. Proposed neuropathological criteria for the post mortem diagnosis of multiple system atrophy. Neuropathol Appl Neurobiol. 2007 Dec;33(6):615-20. doi: 10.1111/j.1365-2990.2007.00907.x[↩]
- Song YJ, Halliday GM, Holton JL, Lashley T, O’Sullivan SS, McCann H, Lees AJ, Ozawa T, Williams DR, Lockhart PJ, Revesz TR. Degeneration in different parkinsonian syndromes relates to astrocyte type and astrocyte protein expression. J Neuropathol Exp Neurol. 2009 Oct;68(10):1073-83. doi: 10.1097/NEN.0b013e3181b66f1b[↩]
- Nishimura Y, Masaki K, Matsuse D, Yamaguchi H, Tanaka T, Matsuo E, Hayashida S, Watanabe M, Matsushita T, Sadashima S, Sasagasako N, Yamasaki R, Isobe N, Iwaki T, Kira JI. Early and extensive alterations of glial connexins, distal oligodendrogliopathy type demyelination, and nodal/paranodal pathology are characteristic of multiple system atrophy. Brain Pathol. 2023 May;33(3):e13131. doi: 10.1111/bpa.13131[↩]
- Ishizawa K, Komori T, Sasaki S, Arai N, Mizutani T, Hirose T. Microglial activation parallels system degeneration in multiple system atrophy. J Neuropathol Exp Neurol. 2004 Jan;63(1):43-52. doi: 10.1093/jnen/63.1.43[↩]
- Lam, S. P., Wong, C. C., Li, S. X., Zhang, J. H., Chan, J. W., Zhou, J. Y., Liu, Y. P., Yu, M. W., & Wing, Y. K. (2016). Caring burden of REM sleep behavior disorder – spouses’ health and marital relationship. Sleep medicine, 24, 40–43. https://doi.org/10.1016/j.sleep.2016.08.004[↩]
- American Academy of Sleep Medicine. (2014). The International Classification of Sleep Disorders – Third Edition (ICSD-3). Darien, IL.[↩]
- Schenck, C. H., Bundlie, S. R., & Mahowald, M. W. (1996). Delayed emergence of a parkinsonian disorder in 38% of 29 older men initially diagnosed with idiopathic rapid eye movement sleep behaviour disorder. Neurology, 46(2), 388–393. https://doi.org/10.1212/WNL.46.2.388[↩]
- Schenck, C. H., Boeve, B. F., & Mahowald, M. W. (2013). Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep medicine, 14(8), 744–748. https://doi.org/10.1016/j.sleep.2012.10.009[↩]
- Postuma RB, Gagnon JF, Bertrand JA, Génier Marchand D, Montplaisir JY. Parkinson risk in idiopathic REM sleep behavior disorder: preparing for neuroprotective trials. Neurology. 2015 Mar 17;84(11):1104-13. doi: 10.1212/WNL.0000000000001364[↩]
- Ronald B. Postuma, Jean-Francois Gagnon, Maria Tuineaig, Josie-Anne Bertrand, Veronique Latreille, Catherine Desjardins, Jacques Y. Montplaisir, Antidepressants and REM Sleep Behavior Disorder: Isolated Side Effect or Neurodegenerative Signal?, Sleep, Volume 36, Issue 11, 1 November 2013, Pages 1579–1585, https://doi.org/10.5665/sleep.3102[↩]
- Teman, P. T., Tippmann-Peikert, M., Silber, M. H., Slocumb, N. L., & Auger, R. R. (2009). Idiopathic rapid-eye-movement sleep disorder: associations with antidepressants, psychiatric diagnoses, and other factors, in relation to age of onset. Sleep medicine, 10(1), 60–65. https://doi.org/10.1016/j.sleep.2007.11.019[↩]
- Iranzo, A., & Santamaria, J. (1999). Bisoprolol-induced rapid eye movement sleep behavior disorder. The American journal of medicine, 107(4), 390–392. https://www.amjmed.com/article/S0002-9343(99)00245-4/abstract[↩]
- Nightingale, S., Orgill, J. C., Ebrahim, I. O., de Lacy, S. F., Agrawal, S., & Williams, A. J. (2005). The association between narcolepsy and REM behavior disorder (RBD). Sleep medicine, 6(3), 253–258. https://doi.org/10.1016/j.sleep.2004.11.007[↩]
- Boeve, B. F., Silber, M. H., & Ferman, T. J. (2003). Melatonin for treatment of REM sleep behavior disorder in neurologic disorders: results in 14 patients. Sleep medicine, 4(4), 281–284. https://doi.org/10.1016/S1389-9457(03)00072-8[↩]
- Aurora RN, Zak RS, Maganti RK, Auerbach SH, Casey KR, Chowdhuri S, Karippot A, Ramar K, Kristo DA, Morgenthaler TI; Standards of Practice Committee; American Academy of Sleep Medicine. Best practice guide for the treatment of REM sleep behavior disorder (RBD). J Clin Sleep Med. 2010 Feb 15;6(1):85-95. Erratum in: J Clin Sleep Med. 2010 Apr 15;6(2):table of contents. https://pmc.ncbi.nlm.nih.gov/articles/PMC2823283[↩]
- Schuld, A., Kraus, T., Haack, M., Hinze-Selch, D., & Pollmächer, T. (1999). Obstructive sleep apnea syndrome induced by clonazepam in a narcoleptic patient with REM-sleep-behavior disorder. Journal of sleep research, 8(4), 321–322. https://doi.org/10.1046/j.1365-2869.1999.00162.x[↩]
- Fanciulli A, Wenning GK. Multiple-system atrophy. The New England journal of medicine. 2015;372:249–263. doi: 10.1056/NEJMra1311488[↩]
- Petrovic IN, Ling H, Asi Y, Ahmed Z, Kukkle PL, Hazrati LN, Lang AE, Revesz T, Holton JL, Lees AJ. Multiple system atrophy-parkinsonism with slow progression and prolonged survival: a diagnostic catch. Movement disorders : official journal of the Movement Disorder Society. 2012;27:1186–1190. doi: 10.1002/mds.25115[↩]
- Monzio Compagnoni G, Di Fonzo A. Understanding the pathogenesis of multiple system atrophy: state of the art and future perspectives. Acta Neuropathol Commun. 2019 Jul 12;7(1):113. doi: 10.1186/s40478-019-0730-6[↩]
- Coon EA, Sletten DM, Suarez MD, Mandrekar JN, Ahlskog JE, Bower JH, Matsumoto JY, Silber MH, Benarroch EE, Fealey RD, Sandroni P, Low PA, Singer W. Clinical features and autonomic testing predict survival in multiple system atrophy. Brain. 2015 Dec;138(Pt 12):3623-31. doi: 10.1093/brain/awv274[↩]





{kind=link}