Contents
What is a Myoma?
A myoma also known as uterine fibroid or uterine leiomyoma is a noncancerous (benign) smooth muscle tumor that grows in the uterus (womb), within the muscle wall of the uterus or on the outer surface of the uterus 1, 2, 3. Myomas are very common affecting up to 80% of women of reproductive age and can cause heavy periods or painful periods, pelvic pain, and infertility. Once a fibroid is formed, it tends to grow larger until menopause. After menopause, fibroids tend to shrink because women have less estrogen at that stage of their lives 4.
Womb myoma or uterine fibroids are common growths of the uterus. They often appear in women of reproductive age during the years women are usually able to get pregnant and give birth. Between 20% and 80% of women develop uterine fibroids by the time they reach 50 years of age 4. Most women get uterine fibroids in their 40s and 50s, and many women have them without knowing it 4. The major risk factors for fibroid development are increasing age until menopause and African descent 5, 6. Compared with white women, black women have a higher lifetime prevalence of fibroids and more severe symptoms, which can affect their quality of life 7. The results of this study suggest that most black and white women in the United States develop uterine fibroid tumors before menopause and that uterine fibroid tumors develop in black women at earlier ages than in white women 3.
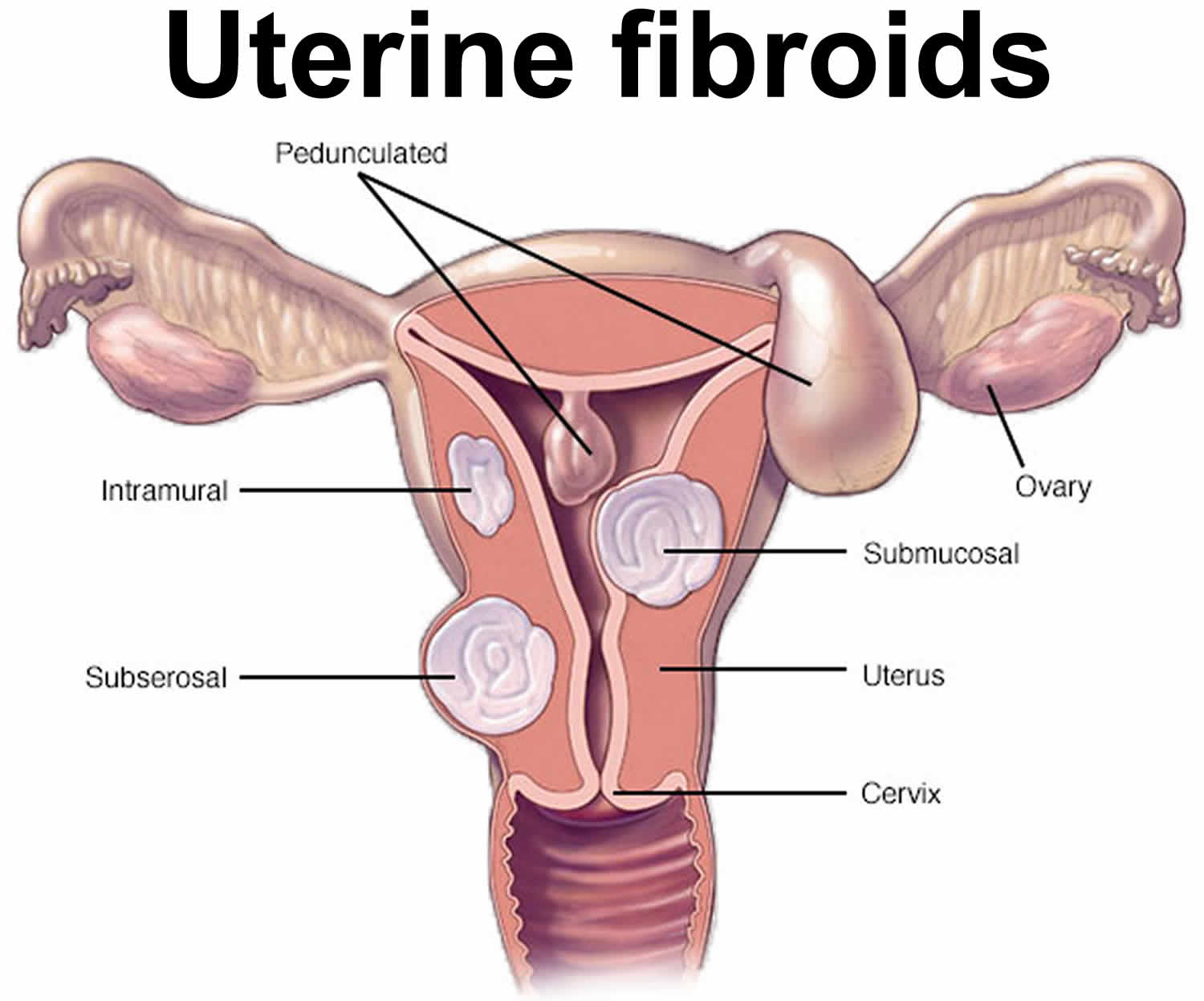
There are 5 types of uterine fibroids:
- The most common are intramural fibroids, which grow in the wall of the uterus.
- Subserosal fibroids grow in the wall on the outside of the uterus. As they grow larger, they can cause pressure on nearby organs or pain due to their size.
- Submucosal fibroids grow just beneath the uterine lining and can push into the uterus cavity, leading to heavy bleeding and other more serious complications.
- Pedunculated fibroids grow on small stalks or stems inside or outside the uterus.
- Intracavitary fibroids grow into the uterine cavity.
You may develop more than one type of fibroid.
Uterine fibroids are not cancer (benign) and they almost never turn into cancer. Uterine fibroids aren’t linked with a higher risk of other types of cancer in the uterus either. However, in addition to causing heavy periods or painful periods, pelvic pain, and infertility, they can increase your risk of pregnancy complications, such as placental abruption and preterm labor.
Fibroids in womb can vary in number and size. You can have a single fibroid or more than one. Some of these growths are too small to see with the eyes. Others can grow to the size of a grapefruit or larger. A fibroid that gets very big can distort the inside and the outside of your uterus. In extreme cases, some fibroids grow large enough to fill your pelvis or stomach area. Womb myomas can make a woman look pregnant.
Many women have uterine fibroids sometime during their lives. But you might not know you have them, because they often cause no symptoms. Your doctor may just happen to find fibroids during a pelvic exam or pregnancy ultrasound.
Not all uterine fibroids cause symptoms, but when they do, symptoms can include heavy bleeding during the menstrual period, periods may last much longer than usual, back pain, a constant feeling that you need to urinate or frequent urination and pain during sex. Fibroids may also cause pain or a feeling of pressure or heaviness in the lower pelvic area (the area between the hip bones), the back or the legs. There may also be a feeling of pressure in the bowel. Some women have constipation or bloating. Uterine fibroids can also cause infertility as well as complications during pregnancy and labor.
There are many treatment options for women who have uterine fibroids. Fibroids that don’t cause any symptoms may not need treatment. For uterine fibroids that do cause symptoms, treatment options include medicine, noninvasive or minimally invasive procedures, or traditional surgery. Your doctor will help you figure out the best treatment option for your fibroid.
Your doctor will consider many things before helping you choose a treatment. Some of these things include:
- Whether or not you are having symptoms from the fibroids
- If you might want to become pregnant in the future
- The size of the fibroids
- The location of the fibroids
- Your age and how close to menopause you might be
Uterine fibroid treatment options:
- Medicines don’t get rid of fibroids, but they can help control symptoms and make fibroids smaller. Painful uterine fibroids can be treated with medications such as hormonal contraception (oral contraceptive pills), progestin-releasing intrauterine device (IUD), rings or injections and medications to shrink fibroids (gonadotropin-releasing hormone [GnRH] agonists).
- Gonadotropin-releasing hormone (GnRH) agonists medications work by shrinking fibroids. They’re sometimes used to shrink a fibroid before surgery, making it easier to remove the fibroid. However, these medications are temporary, and if you stop taking them, the fibroids can grow back. Gonadotropin-releasing hormone (GnRH) agonists include leuprolide (Lupron Depot, Eligard, others), goserelin (Zoladex) and triptorelin (Trelstar, Triptodur Kit). Many people have hot flashes while using GnRH agonists. Often, these medicines are used for no more than six months. That’s because symptoms return when the medicine is stopped, and long-term use can cause loss of bone. Sometimes, GnRH agonists are taken with low-dose estrogen or progestin. You might hear this called add-back therapy. It can ease side effects, and it might allow you to take GnRH agonists up to 12 months. Your doctor may prescribe a GnRH agonist to shrink the size of your fibroids before a planned surgery. Or you might be prescribed this medicine to help transition you into menopause.
- Gonadotropin-releasing hormone (GnRH) antagonists. Gonadotropin-releasing hormone (GnRH) antagonists also known as gonadotropin-releasing hormone (GnRH) blockers include elagolix (Oriahnn) and relugolix (Myfembree). Gonadotropin releasing hormone (GnRH) antagonist blocks GnRH stimulation of luteinizing hormone (LH) and follicular stimulating hormone (FSH) production by the pituitary gland, thereby decreasing the synthesis of estrogen by the ovaries in women. Gonadotropin-releasing hormone (GnRH) antagonists can treat heavy menstrual bleeding in people with uterine fibroids who haven’t gone through menopause. But they don’t shrink fibroids. Gonadotropin-releasing hormone (GnRH) antagonists can be used for up to two years. Taking them along with add-back therapy can lessen side effects such as hot flashes and bone loss. Sometimes, low-dose estrogen or progestin are already included in these medicines.
- Progestin-releasing intrauterine device (IUD). A progestin-releasing IUD can relieve heavy bleeding caused by fibroids. It only relieves symptoms, though. It doesn’t shrink fibroids or make them go away. It also prevents pregnancy.
- Tranexamic acid (Lysteda, Cyklokapron). This nonhormonal medicine can ease heavy menstrual periods. You take it only on heavy bleeding days.
- Other medicines. Your doctor might recommend low-dose birth control pills can help control menstrual bleeding. But they don’t reduce fibroid size. Medicines called nonsteroidal anti-inflammatory drugs (NSAIDs) may help relieve pain tied to fibroids, but they don’t reduce bleeding caused by fibroids. Nonsteroidal anti-inflammatory drugs (NSAIDs) aren’t hormonal medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) include ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve). Your doctor also may suggest that you take vitamins and iron if you have heavy menstrual bleeding and anemia.
- Your doctor may recommend a noninvasive or minimally invasive procedure to remove or destroy the fibroid. A noninvasive procedure means that your doctor does not have to make an incision (cut your skin) to destroy or remove the fibroid. On the other hand, a minimally invasive procedure means that your doctor makes only a very small incision (cut) in your skin to destroy or remove the fibroid.
- Myomectomy, a surgical procedure to remove the fibroids. During this procedure, your doctor surgically removes the fibroids from your uterus. The surgical tools are inserted in the body either through very small cuts in the abdomen, or through the vagina and cervix.
- Uterine fibroid embolization also called uterine artery embolization: Fibroids will shrink or go away completely if their blood supply is stopped. During uterine fibroid embolization, your doctor injects tiny particles into the arteries that supply blood to the fibroids. These particles stop the blood flow to the fibroid. Over time, the fibroid will shrink. The procedure works even if you have several fibroids.
- Magnetic resonance imaging (MRI)-guided ultrasound surgery to shrink fibroids. MRI-guided focused ultrasound therapy is a new, noninvasive way of treating fibroids. During this procedure, you lie in a magnetic resonance imaging (MRI) scanner while it takes pictures of your uterus. The scanner shows your doctor exactly where the fibroid is. Your doctor then points ultrasound (sound waves) at the fibroid. The ultrasound waves heat up and destroy the fibroid. This is the least invasive procedure for treating fibroids but not every patient is a candidate for it. Your doctor can help you determine if it would work for you.
- Hysterectomy. A hysterectomy is a surgical procedure to remove the uterus, or womb. If you have a number of fibroids or fibroids that are very large, your doctor may recommend a hysterectomy. During a hysterectomy, your doctor removes the entire uterus from your body. A hysterectomy can be done through an abdominal incision (cut) or through a vaginal incision. Hysterectomy remains the only proven permanent solution for uterine fibroids. Hysterectomy ends your ability to bear children. If you also decide to have your ovaries removed, the surgery brings on menopause. You’ll then choose whether to take hormone replacement therapy, which is medicine that can ease menopause side effects such as hot flashes. Most people with uterine fibroids may be able to choose to keep their ovaries.
With hysterectomy or endometrial ablation, you won’t be able to get pregnant in the future. Also, uterine artery embolization and radiofrequency ablation may not be the best options if you want to keep as much of your fertility as possible.
Talk with your doctor about the risks and benefits of these procedures if you want to keep the ability to become pregnant. And if you’re actively trying to get pregnant, get a complete fertility evaluation before you decide on a treatment plan for fibroids.
If fibroid treatment is needed and you want to preserve your fertility, myomectomy is often the treatment of choice. But all treatments have risks and benefits. Talk about these with your doctor.
For all procedures except hysterectomy, seedlings — tiny tumors that your doctor doesn’t detect during surgery — could one day grow and cause symptoms that need treatment. Often, this is called the recurrence rate. New fibroids also can form, and these may need treatment. Also, some procedures may only treat some of the fibroids present at the time of treatment. These include laparoscopic or robotic myomectomy, radiofrequency ablation, and MRI-guided focused ultrasound surgery.
Figure 1. Uterus anatomy
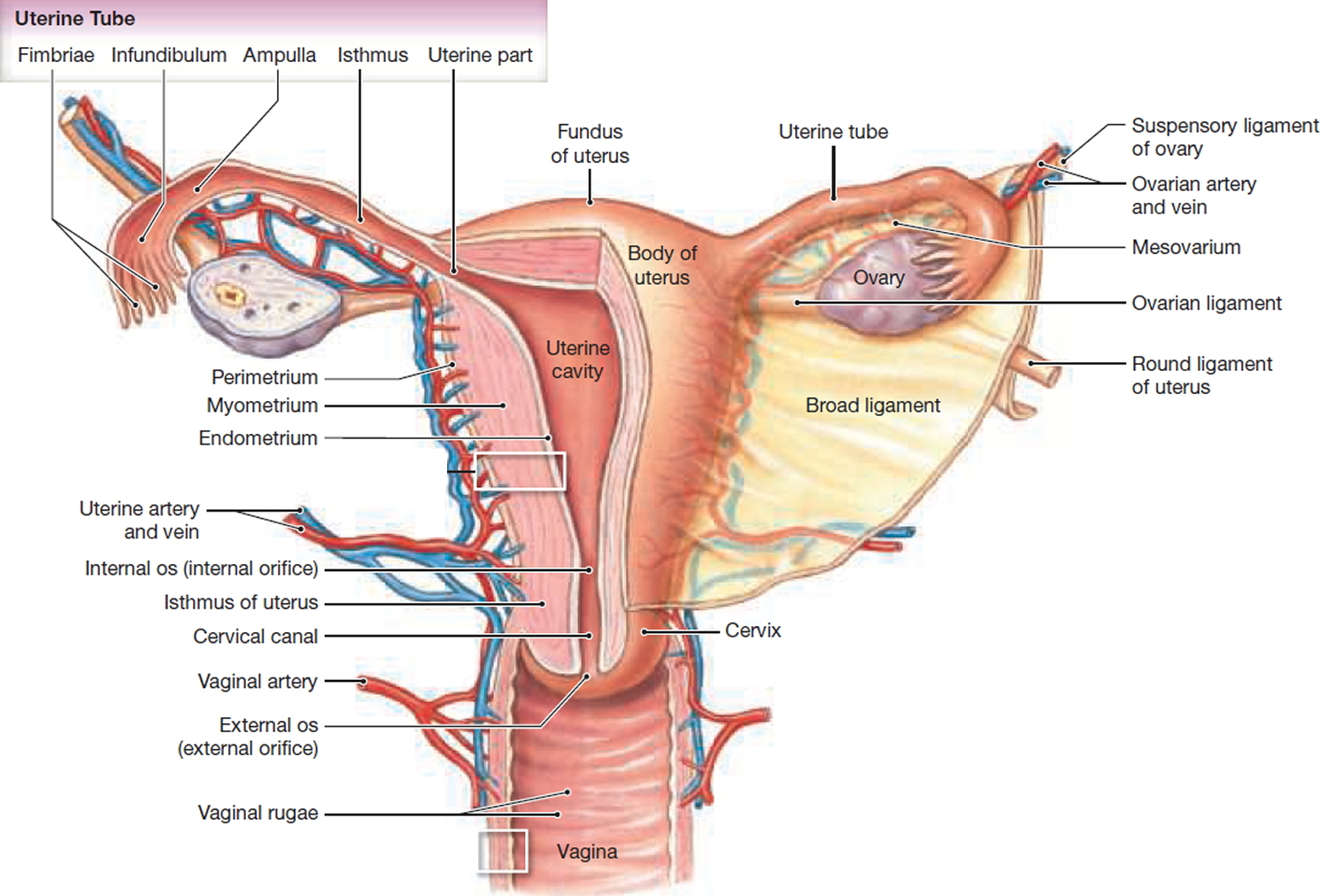
Footnotes: The uterus is a hollow organ, normally about the size and shape of a medium-sized pear. The uterus is where a fetus (baby) grows and develops when a woman is pregnant. It has 2 main parts:
- The upper part of the uterus is called the body or the corpus. (Corpus is the Latin word for body.)
- The cervix is the lower end of the uterus that joins it to the vagina.
The body of the uterus has 2 main layers:
- The myometrium is the outer layer. This thick layer of muscle is needed to push the baby out during birth.
- The endometrium is the inner layer. During a woman’s menstrual cycle, hormones cause the endometrium to change. Estrogen causes the endometrium to thicken so that it could nourish an embryo if pregnancy occurs. If there is no pregnancy, estrogen is produced in lower amounts and more of the hormone called progesterone is made. This causes the endometrial lining to shed from the uterus and become the menstrual flow (period). This cycle repeats until menopause.
- There is also a layer of tissue called the serosa which coats the outside of the uterus.
Figure 2. Myoma
See your doctor if you have:
- Unusual vaginal bleeding, spotting, or other discharge
- Pelvic pain, a mass, and weight loss
- Pelvic pain that doesn’t go away.
- Heavy or painful periods that limit what you can do.
- Spotting or bleeding between periods.
- Trouble emptying your bladder.
- Ongoing tiredness and weakness, which can be symptoms of anemia, meaning a low level of red blood cells.
Get medical care right away if you have severe bleeding from the vagina or sharp pelvic pain that comes on fast.
About 90% of women with endometrial cancer have abnormal vaginal bleeding. This might be a change in their periods, bleeding between periods, or bleeding after menopause. Non-cancer problems can also cause abnormal bleeding. But it’s important to have a doctor check out any irregular bleeding right away. If you’ve gone through menopause, it’s especially important to report any vaginal bleeding, spotting, or abnormal discharge to your doctor.
Non-bloody vaginal discharge may also be a sign of endometrial cancer. Even if you can’t see blood in the discharge, it doesn’t mean there’s no cancer. Any abnormal discharge should be checked out by a doctor.
Uterine fibroids types
There are 5 types of uterine fibroids depending on where they’re located and how they attach. Specific types of uterine fibroids include:
- Intramural fibroids: These fibroids are embedded into the muscular wall of your uterus. They’re the most common type.
- Submucosal fibroids: These fibroids grow under the inner lining of your uterus.
- Subserosal fibroids: This type of fibroid grows under the lining of the outer surface of your uterus. They can become quite large and grow into your pelvis.
- Pedunculated fibroids: The least common type, these fibroids attach to your uterus with a stalk or stem. They’re often described as mushroom-like because they have a stalk and then a wider top.
- Intracavitary fibroids grow into the uterine cavity.
Where do uterine fibroids grow?
Uterine fibroids can grow as a single nodule (one growth) or in a cluster. Clusters of fibroids can range in size from 1 millimeter to more than 20 centimeters (8 inches) in diameter or even larger. For comparison, fibroids can be as small as a seed or get as large as a watermelon. These growths can develop within the wall of your uterus, inside the main cavity of your uterus or on the outer surface of your uterus.
Will uterine fibroids go away on their own?
Uterine fibroids can shrink in some women after menopause. This happens because of a decrease in estrogen and progesterone hormones after menopause 8, 9. When the fibroids shrink, your symptoms may go away. Small fibroids may not need treatment if they aren’t causing any symptoms.
Can uterine fibroids become cancer?
Uterine fibroids are not cancerous. It’s extremely rare for a fibroid to go through changes that transform it into a cancerous (malignant) tumor. Less than one in a thousand cases of uterine fibroids develop into cancer of the uterus 10. However, women who have rapid growth of uterine fibroids or fibroids that grow after menopause should be evaluated immediately.
In a very small number of patients with a condition called hereditary leiomyomatosis and renal cell cancer (HLRCC), the fibroids are linked to kidney cancer. However, this association is not seen in women who do not have hereditary leiomyomatosis and renal cell cancer (HLRCC) 11.
Differential diagnosis of a uterine cancer should be considered in women presenting with a uterine mass, particularly if they are postmenopausal 12. One to two in 1000 women with uterine masses are estimated to have a uterine cancer 13.
Suspicion for cancer is raised for rapidly growing uterine fibroids, particularly in postmenopausal women who are not on hormone replacement therapy and women responding poorly to gonadotrophin releasing hormone (GnRH) agonists. A history of tamoxifen use for more than five years is associated with a threefold increase in the risk of leiomyosarcoma, and uterine ultrasound surveillance is recommended in such cases, especially in patients who have had prior pelvic radiation therapy 14, 15.
Preoperative differentiation between benign uterine fibroids and uterine cancer is extremely difficult, yet increasingly important because of trends for using conservative and minimally invasive treatments. Occasionally, morcellators (a surgical instrument that cuts tissue into smaller pieces for removal during minimally invasive procedures) are used in laparoscopic fibroid resection. These instruments divide tissue into smaller sections that are otherwise too large to remove via portholes or the vaginal outlet. Shorter operating times and smaller incisions reduce postoperative morbidity.
In 2014, the US Food and Drug Administration (FDA) released a statement discouraging the use of laparoscopic power morcellation following a case of inadvertent morcellation of a leiomyosarcoma and subsequent malignant upstaging 16. Many have since considered the therapeutic challenges and risks of minimally invasive surgery. A large retrospective trial showed that the risk of unintended morcellation of a uterine leiomyosarcoma (a type of uterine cancer) following preoperative selection of women with fibroids is one in 4791 women 17. While seemingly low, the risks of minimally invasive surgery should be carefully conveyed to patients to help them make fully informed decisions.
Uterine fibroids during pregnancy
If you have uterine fibroids, you may still be able to get pregnant. Many women who have fibroids get pregnant naturally. Advances in treatments for fibroids and for infertility have greatly improved the chances for a woman to conceive. If you have fibroids and wish to become pregnant, it is wise to consult with a knowledgeable doctor about the location of the fibroids and possible related problems with pregnancy or growth of a baby in the uterus.
However, some women with fibroids do have trouble getting pregnant. Current research suggests that submucosal and intramural fibroids—fibroids that change the shape and size of the uterine cavity—seem to affect a woman’s ability to get pregnant, even with in vitro fertilization (IVF) 18, 19. These fibroids may reduce fertility by as much as 70% 20. However, if the fibroid is treated, fertility may be restored.
Fibroids can also raise the risk of certain pregnancy complications such as miscarriage, placental abruption, preterm delivery (when a baby is born too early before the 37th week of pregnancy), abnormal position of the fetus, fetal growth restriction (when an unborn baby doesn’t grow as well as expected) and the need for cesarean (C-section or surgical) delivery. Fibroids can also increase the risk of heavy bleeding after delivery 21.
Can I get pregnant if I have uterine fibroids?
Yes, you can get pregnant if you have uterine fibroids. If you already know you have fibroids when you get pregnant, your doctor will work with you to develop a monitoring plan for the fibroids. During pregnancy, your body releases elevated levels of hormones. These hormones support the pregnancy. However, they can also cause your fibroids to get bigger. Large fibroids can cause the following problems during pregnancy:
- Increased risk for a C-section delivery because the fetus can’t flip into a head-down position.
- Labor doesn’t progress.
- Placental abruption.
- Preterm delivery.
What causes myoma?
Doctors don’t know what causes uterine fibroids. Scientists have a number of theories, but none of these ideas explains fibroids completely. Some researchers believe they may be genetic (run in families). Other researchers think they could be related to hormone levels.
Some factors researchers believed to be related to fibroid growth are 22, 23:
- Estrogen and Progesterone. Estrogen and progesterone cause the tissue that lines the inside of your uterus to thicken during each menstrual cycle to prepare for pregnancy. These hormones also seem to help fibroids grow 8, 9. Fibroids contain more cells that estrogen and progesterone bind to than do typical uterine muscle cells. Aromatase in fibroid tissue allows for endogenous production of estradiol, and fibroid stem cells express estrogen and progesterone receptors that facilitate tumor growth in the presence of these hormones 8. Fibroids tend to shrink after menopause due to a drop in hormone levels.
- Growth hormones
- Other growth factors. Substances that help the body maintain tissues, such as insulin-like growth factor, may affect fibroid growth.
- Genetic changes. Many fibroids contain changes in genes that differ from those in typical uterine muscle cells.
- Misplaced cells present in the body before birth. Doctors believe that uterine fibroids may develop from a stem cell in the smooth muscular tissue of the uterus. A single cell divides over and over. In time it turns into a firm, rubbery mass distinct from nearby tissue.
- Extracellular matrix (ECM). The extracellular matrix (ECM) makes cells stick together, like mortar between bricks. Extracellular matrix (ECM) is increased in fibroids and makes them fibrous. Extracellular matrix (ECM) also stores growth factors and causes biologic changes in the cells themselves.
Other factors that may affect fibroid growth are:
- Quantity of micronutrients—nutrients such as iron that the body needs only small amounts of — in the blood 24. For instance, a deficiency of vitamin D may be associated with uterine fibroids 25.
- Major stresses 26, 27
It is likely that fibroids are caused by many factors interacting with one another.
The growth patterns of uterine fibroids vary. They may grow slowly or fast. Or they might stay the same size. Some fibroids go through growth spurts, and some shrink on their own.
Fibroids that form during pregnancy can shrink or go away after pregnancy, as the uterus goes back to its usual size.
Uterine Myoma Risk factors
There are few known risk factors that can increase a woman’s risk of developing uterine fibroids, these include 6, 5, 28, 29, 30, 31:
- Fibroids are common as women age (≥ 40 years of age), especially as they approach menopause.
- African descent. Black women are more likely to develop fibroids than women of other racial groups. Black women have fibroids at younger ages than do white women. Black women are also likely to have more or larger fibroids, along with worse symptoms, than do women of other racial groups.
- Women who are overweight or obese are at higher risk for fibroids. For heavy women, the risk is two to three times greater than average 32, 33. Each kilogram of excessive body weight is correlated with an increased risk of uterine fibroids development 34, 35.
- Eating habits. Eating a lot of red meat (e.g., beef) and ham is linked with a higher risk of fibroids. Eating plenty of green vegetables seems to protect women from developing fibroids.
- Family history. If your mother or sister had fibroids, you’re at higher risk of getting them.
- Other factors. Starting your period before the age of 10 (early menarche); never given birth to a live baby (nulliparity); late age for menopause; being low on vitamin D; drinking alcohol, including beer, seem to raise your risk of getting fibroids 36, 37, 38, 39, 40, 41.
Myoma prevention
Because doctors don’t know for sure what causes uterine fibroids, they cannot be completely prevented or avoided. However, healthy lifestyle changes, such as losing weight to stay at a healthy weight, eating less red meat, and eating more green vegetables, fruits and dairy can help reduce your risk.
Some research suggests that birth control pills or long-acting progestin-only contraceptives may lower the risk of fibroids. But using birth control pills before the age of 16 may be linked with a higher risk.
Myoma signs and symptoms
Many women who have womb myomas or uterine fibroids don’t have any symptoms. In those women who do, symptoms can be influenced by the location, size and number of fibroids. In other women, fibroids can cause heavy bleeding during the menstrual period. Periods may last much longer than usual. Fibroids may also cause pain or a feeling of pressure or heaviness in the lower pelvic area (the area between the hip bones), the back or the legs. Some women have pain during sexual intercourse. Others have a constant feeling that they need to urinate. There may also be a feeling of pressure in the bowel. Some women have constipation or bloating. Uterine fibroids can also cause infertility as well as complications during pregnancy and labor.
The most common symptoms of uterine fibroids include 42, 43, 44, 45:
- Heavy menstrual bleeding or painful periods (cramps). The most common symptom is abnormal uterine bleeding, usually excessive menstrual bleeding 44.
- Longer or more frequent periods.
- Bleeding between periods.
- Feeling “full” in the lower abdomen (belly) this is sometimes called “pelvic pressure”.
- Pelvic pain.
- Frequent urination or trouble urinating (caused by a fibroid pressing on the bladder).
- Growing stomach area.
- Constipation, rectal pain, or difficult bowel movements.
- Pain in the stomach area or lower back, or pain during sex.
- Lower back pain (often dull, heavy and aching, but may be sharp).
- Reproductive problems, such as infertility, multiple miscarriages or early onset of labor during pregnancy 46.
- Anemia (from blood loss).
- Obstetrical problems, such as increased likelihood of cesarean section.
Rarely, a fibroid can cause sudden, serious pain when it outgrows its blood supply and starts to die.
Often, fibroids are grouped by their location. Intramural fibroids grow within the muscular wall of the uterus. Submucosal fibroids bulge into the uterine cavity. Subserosal fibroids form on the outside of the uterus.
Fibroids may be found during a routine pelvic exam or during tests for other problems.
Myoma complications
Uterine fibroids that are attached to the uterus by a stem may twist and can cause pain, nausea, or fever. Uterine fibroids that grow rapidly, or those that start breaking down, also may cause pain. Rarely, uterine fibroids can be associated with cancer. A very large fibroid may cause swelling of the abdomen. This swelling can make it hard to do a thorough pelvic exam.
Uterine fibroids also may cause infertility, although other causes are more common. Other factors should be explored before fibroids are considered the cause of a couple’s infertility. When fibroids are thought to be a cause, many women are able to become pregnant after they are treated.
Uterine fibroids that cause heavy menstrual bleeding may cause a drop in red blood cells called anemia. Anemia can cause fatigue from heavy blood loss. If you bleed heavily during your period, your doctor may tell you to take an iron supplement to prevent or help manage anemia. Sometimes, a person with anemia needs to receive blood from a donor, called a transfusion, due to blood loss.
Myoma diagnosis
In many cases, your doctor may discover that you have fibroids during a routine pelvic exam. Your doctor may be able to feel the fibroids during the exam and even estimate the size. Quite often, heavy bleeding and other related symptoms may alert your doctor to consider fibroids as a part of the diagnosis.
Your doctor may order imaging tests to confirm the diagnosis. Or he/she may suggest looking inside you with a scope. This can be done through laparoscopy or hysteroscopy. In laparoscopy, your doctor will make a small incision (cut) near your navel and insert the scope. In hysteroscopy, your doctor will insert the scope into your vagina and cervix (no incision needed).
Tests that can be done to confirm fibroids and determine their size and location include:
- Ultrasound. This noninvasive imaging test creates a picture of your internal organs with sound waves. It can confirm that you have fibroids, and map and measure them. A doctor or technician moves the ultrasound device, called a transducer, over your stomach area. This is called a transabdominal ultrasound. Or the device is placed inside your vagina to get images of your uterus. This is called a transvaginal ultrasound.
- Magnetic resonance imaging (MRI): This test creates detailed images of your internal organs by using magnets and radio waves. Magnetic resonance imaging (MRI) can show in more detail the size and location of fibroids. It also can identify different types of tumors and help determine treatment options. Most often, an MRI is used in people with a larger uterus or in those who are nearing menopause, also called perimenopause.
- Computed tomography (CT) scan: A CT scan uses X-ray images to make a detailed image of your internal organs from several angles.
- Hysteroscopy: During a hysteroscopy, your doctor will use a device called a hysteroscope (a thin, flexible tube with a camera on the end) to look at fibroids inside your uterus. The hysteroscope is passed through your vagina and cervix and then moved into your uterus. Then saline is injected into your uterus. This expands the uterine cavity and lets your doctor check the walls of your uterus and the openings of your fallopian tubes.
- Hysterosonography (saline infusion sonogram). Hysterosonography uses sterile salt water called saline to expand the space inside the uterus, called the uterine cavity. In this imaging test, your doctor places a small catheter in your vagina and then injects saline into your uterus. This extra fluid helps to create a clearer image of your uterus than you would see during a standard ultrasound. This makes it easier to get images of submucosal fibroids and the lining of the uterus if you’re trying to get pregnant or if you have heavy menstrual bleeding.
- Hysterosalpingography (HSG). Hysterosalpingography uses a dye to highlight the uterine cavity and fallopian tubes on X-ray images. Your doctor may recommend it if infertility is a concern. This test can help find out if your fallopian tubes are open or are blocked, and it can show some submucosal fibroids.
- Laparoscopy: During this test, your provider will make a small cut (incision) in your lower abdomen. A thin and flexible tube with a camera on the end will be inserted to look closely at your internal organs.
- Blood tests. If you have irregular menstrual bleeding, you may need blood tests to look for possible causes of it. These might include a complete blood count to check for anemia due to ongoing blood loss. Other blood tests can search for bleeding disorders or thyroid problems.
Histopathology
Uterine fibroids are benign tumors of monoclonal origin which arise from the smooth muscle of the uterus 47, 48. Uterine fibroids are primarily composed of extracellular matrix (ECM) and cells with a low mitotic index 49, 48. They are encapsulated with a pseudocapsule composed of areolar tissue 48.
Myoma treatment
There’s no single best treatment for uterine fibroids. Many treatment choices exist depending on your symptoms, the size, number, and location of the uterine fibroids and whether you are pregnant now or want to get pregnant in the future 50.
Watchful waiting
Many people with uterine fibroids have no symptoms or they have mildly annoying symptoms that they can live with. If that’s the case for you, watchful waiting could be the best option. However, only you and your doctor can decide the best course of treatment or if treatment is necessary.
If you have large fibroids or your symptoms are causing you pain and discomfort, getting treatment may be the best option.
Fibroids aren’t cancer. They rarely interfere with pregnancy. They often grow slowly or not at all and tend to shrink after menopause, when levels of reproductive hormones drop.
Medicines
Medicines for uterine fibroids target hormones that control the menstrual cycle. They treat symptoms such as heavy menstrual bleeding and pelvic pressure. They don’t get rid of fibroids, but they may shrink them.
Medicines for uterine fibroids include:
- Gonadotropin-releasing hormone (GnRH) agonists. These treat fibroids by blocking the body from making the hormones estrogen and progesterone. This puts you into a temporary menopause-like state. As a result, menstrual periods stop, fibroids shrink and anemia often gets better. Gonadotropin-releasing hormone (GnRH) agonists include leuprolide (Lupron Depot, Eligard, others), goserelin (Zoladex) and triptorelin (Trelstar, Triptodur Kit). Many people have hot flashes while using GnRH agonists. Often, these medicines are used for no more than six months. That’s because symptoms return when the medicine is stopped, and long-term use can cause loss of bone. Sometimes, GnRH agonists are taken with low-dose estrogen or progestin. You might hear this called add-back therapy. It can ease side effects, and it might allow you to take GnRH agonists up to 12 months. Your doctor may prescribe a GnRH agonist to shrink the size of your fibroids before a planned surgery. Or you might be prescribed this medicine to help transition you into menopause.
- Gonadotropin-releasing hormone (GnRH) antagonists. Gonadotropin-releasing hormone (GnRH) antagonists also known as gonadotropin-releasing hormone (GnRH) blockers include elagolix (Oriahnn) and relugolix (Myfembree). Gonadotropin releasing hormone (GnRH) antagonist blocks GnRH stimulation of luteinizing hormone (LH) and follicular stimulating hormone (FSH) production by the pituitary gland, thereby decreasing the synthesis of estrogen by the ovaries in women. Gonadotropin-releasing hormone (GnRH) antagonists can treat heavy menstrual bleeding in people with uterine fibroids who haven’t gone through menopause. But they don’t shrink fibroids. Gonadotropin-releasing hormone (GnRH) antagonists can be used for up to two years. Taking them along with add-back therapy can lessen side effects such as hot flashes and bone loss. Sometimes, low-dose estrogen or progestin are already included in these medicines.
- Progestin-releasing intrauterine device (IUD). A progestin-releasing IUD can relieve heavy bleeding caused by fibroids. It only relieves symptoms, though. It doesn’t shrink fibroids or make them go away. It also prevents pregnancy. It is not recommended for women who have very large fibroids, which can block the uterine cavity.
- Tranexamic acid (Lysteda, Cyklokapron). Tranexamic acid is a derivative of the amino acid, lysine. Tranexamic acid is a reversible inhibitor of lysine receptor sites on plasminogen that, when bound, prevent fibrin degradation and functionally stabilize clot formation 51. This nonhormonal medicine can ease heavy menstrual periods. You take it only on heavy bleeding days. There are few side effects associated with tranexamic acid. The most common is gastrointestinal upset, while the most feared is venous thromboembolism 51, 47. Clinical studies have found no significant evidence for the theoretical increased risk of venous thromboembolism from use of tranexamic acid 51. However, due to potential increased thrombotic risk with hormonal therapy, tranexamic acid is usually prescribed as a single agent therapy 47.
- Other medicines. Your doctor might recommend low-dose birth control pills can help control menstrual bleeding. But they don’t reduce fibroid size. Medicines called nonsteroidal anti-inflammatory drugs (NSAIDs) may help relieve pain tied to fibroids, but they don’t reduce bleeding caused by fibroids. Nonsteroidal anti-inflammatory drugs (NSAIDs) aren’t hormonal medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) include ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve). Your doctor may also suggest that you take vitamins and iron if you have heavy menstrual bleeding and anemia. Vitamin D deficiency is associated with increased risk of fibroids.
Other, less-studied options for the treatment of uterine fibroids include aromatase inhibitors and estrogen receptor antagonists 19. Aromatase inhibitors (e.g., letrozole [Femara], anastrozole [Arimidex], fadrozole) block the synthesis of estrogen 19. Limited data have shown that they help reduce fibroid size as well as decrease menstrual bleeding, with adverse effects including hot flashes, vaginal dryness, and musculoskeletal pain 52, 53. Overall, there is insufficient evidence to support the use of aromatase inhibitors for the treatment of uterine fibroids 54. Selective estrogen receptor modulators (SERM) act as partial estrogen receptor agonists in bone, cardiovascular tissue, and the endometrium. In a small prospective trial of 18 patients, tamoxifen did not reduce fibroid size or uterine volume, but did reduce menstrual blood loss by 40% to 50% and decrease pelvic pain compared with the control group 55. Based on its adverse effects (e.g., hot flashes, dizziness, endometrial thickening), the authors concluded that its risks outweigh its marginal benefits for fibroid treatment. Another selective estrogen receptor modulator (SERM), raloxifene (Evista), has also shown inconsistent results, with two of three studies included in a Cochrane review showing significant benefit 56.
Noninvasive procedure
A noninvasive treatment doesn’t involve surgical cuts called incisions. It also doesn’t involve tools being placed in the body. With uterine fibroids, a procedure called magnetic resonance imaging (MRI)-guided ultrasound surgery is a noninvasive treatment option to shrink fibroids and preserves the uterus. MRI-guided focused ultrasound therapy is a new, noninvasive way of treating fibroids. It’s done on an outpatient basis, meaning you don’t have to spend the night at the hospital afterward.
During this procedure, you lie in a magnetic resonance imaging (MRI) scanner while it takes pictures of your uterus. The scanner shows your doctor exactly where the fibroid is. Your doctor then points ultrasound (sound waves) at the fibroid. The ultrasound waves heat up and destroy the fibroid. This is the least invasive procedure for treating fibroids but not every patient is a candidate for it. But so far data collected show that MRI-guided ultrasound surgery for uterine fibroids is safe and works well. Still, it might not improve symptoms as much as a slightly more invasive procedure called uterine artery embolization could. Your doctor can help you determine if it would work for you.
Minimally invasive procedures
Minimally invasive procedures use no cuts or small cuts. They’re linked with faster recovery times and fewer complications compared with traditional open surgery. However, with any procedure that doesn’t remove the uterus, there’s a risk that new fibroids could grow and cause symptoms.
Minimally invasive treatments for uterine fibroids include:
Uterine artery embolization (uterine fibroid embolization)
In uterine artery embolization procedure, the doctor makes a small cut in the groin area, inserts a tube called a catheter into the large blood vessel there, and slides the tube until it reaches the arteries that supply blood to the uterus. Your doctor then injects tiny plastic or gel particles (embolic agents) through the tube into the arteries that supply your uterus with blood. The particles block blood flow to the fibroids, so they eventually shrink and may relieve symptoms 57.
Uterine artery embolization can help shrink fibroids and relieve the symptoms they cause. Complications may happen if the blood supply to your ovaries or other organs is reduced. But research shows that complications are similar to surgical fibroid treatments. And the risk of needing a blood transfusion is lower.
Some research has shown that uterine artery embolization successfully treats fibroids but that about one-third of women who have uterine artery embolization need treatment again within 5 years 58.
Because this procedure stops blood flow to parts of the uterus, it can affect how the uterus functions. It can also affect how the ovaries function if the inserted particles drift into other areas of the pelvis, such as the ovarian artery. Its effect on pregnancy is not clear, but an increased risk of miscarriage has been reported. For this reason, most doctors do not recommend uterine artery embolization for women who want to have children.
Radiofrequency ablation
With radiofrequency ablation, heat from radiofrequency energy destroys uterine fibroids and shrinks the blood vessels that feed them. This can be done through small cuts in the stomach area, a type of surgery called laparoscopy. It also can be done through the vagina, called a transvaginal procedure, or through the cervix, called a transcervical procedure.
With laparoscopic radiofrequency ablation, your doctor makes two small cuts in the abdomen. A slim viewing tool with a camera at the tip, called a laparoscope, is placed through the cuts. Using the camera and an ultrasound tool, your doctor finds fibroids to be treated.
After finding a fibroid, your doctor uses a device to send small needles into the fibroid. The needles heat up the fibroid tissue and destroy it. The destroyed fibroid changes right away. For instance, it goes from being hard like a golf ball to being soft like a marshmallow. During the next 3 to 12 months, the fibroid continues to shrink, and symptoms get better.
Laparoscopic radiofrequency ablation is also known as the Acessa procedure or Lap-RFA. Because there’s no cutting of uterine tissue, doctors consider laparoscopic radiofrequency ablation (Lap-RFA) a less invasive treatment than surgeries such as a hysterectomy and a myomectomy. Most people who have the procedure get back to regular activities within a few days.
The transcervical or through the cervix approach to radiofrequency ablation is called Sonata. It also uses ultrasound guidance to locate fibroids.
Laparoscopic or robotic myomectomy
In a myomectomy, your surgeon removes the fibroids and leaves the uterus in place.
If the fibroids are few in number, you and your doctor may opt for a laparoscopic procedure. This uses slender instruments placed through small cuts in the abdomen to remove the fibroids from the uterus.
Sometimes, a robotic system is used for the laparoscopic procedure. Your doctor views your stomach area on a monitor using a small camera attached to one of the instruments. Robotic myomectomy gives your surgeon a magnified, 3D view of your uterus. This can make the procedure more precise than is possible using some other techniques.
Larger fibroids can be removed through smaller cuts by breaking them into pieces with a device that cuts tissue. This is called morcellation. It can be done inside a surgical bag to lower the risk of spreading any cancer cells that doctors hadn’t expected to find. Or it can be done by extending one incision to remove the fibroids without morcellation.
Hysteroscopic myomectomy
Hysteroscopic myomectomy may be an option if the fibroids are inside your uterus is the submucosal fibroids type. The fibroids are removed using tools placed through the vagina and cervix into the uterus.
Endometrial ablation
Endometrial ablation procedure can reduce heavy menstrual flow. A device that’s inserted into the uterus gives off heat, microwave energy, hot water, cold temperature or an electric current. This destroys the tissue that lines the inside of the uterus.
You aren’t likely to get pregnant after endometrial ablation. But it’s a good idea to take birth control to prevent a fertilized egg from forming in a fallopian tube, called an ectopic pregnancy. Without treatment, the growing tissue might cause life-threatening bleeding.
Traditional surgical procedures
There are several factors to consider when talking about the different types of surgery for fibroid removal. Not only can the size, location and number of fibroids influence the type of surgery, but your wishes for future pregnancies can also be an important factor when developing a treatment plan. Some surgical options preserve your uterus and allow you to become pregnant in the future, while other options can either damage or remove your uterus.
Options for traditional open surgeries that use a larger incision include:
- Abdominal myomectomy. This type of surgery removes fibroids through a larger cut in the stomach area, also called the abdomen. Your doctor may recommend it if you have more than one fibroid, very large fibroids or very deep fibroids. Many people who are told that hysterectomy is their only option can have an abdominal myomectomy instead. Scarring after surgery can lower the chances of being able to get pregnant in the future, though.
- Hysterectomy. A hysterectomy is a surgical procedure to remove the uterus, or womb. If you have a number of fibroids or fibroids that are very large, your doctor may recommend a hysterectomy. During a hysterectomy, your doctor removes the entire uterus from your body. A hysterectomy can be done through an abdominal incision (cut) or through a vaginal incision. Hysterectomy remains the only proven permanent solution for uterine fibroids. Hysterectomy ends your ability to bear children. If you also decide to have your ovaries removed, the surgery brings on menopause. You’ll then choose whether to take hormone replacement therapy, which is medicine that can ease menopause side effects such as hot flashes. Most people with uterine fibroids may be able to choose to keep their ovaries.
Morcellation during fibroid removal
Morcellation is a process of breaking fibroids into smaller pieces. It can raise the risk of spreading cancer if a cancerous tumor that hadn’t been found earlier gets broken up with morcellation during a myomectomy procedure. The risk can be lowered if:
- The surgical team looks into a person’s risk factors before surgery.
- The fibroid is broken up in a surgical bag during morcellation.
- The incision is expanded to remove a large fibroid without morcellation.
All myomectomies carry the risk of cutting into cancer that hasn’t been found. But younger people who haven’t reached menopause by and large have a lower risk of undiagnosed cancer than do people over the age of 50.
Also, complications during open surgery are more common than the chance of spreading an unsuspected cancer in a fibroid during a minimally invasive procedure. If your doctor is planning to use morcellation, ask the doctor to explain your risks before treatment.
In the United States, the Food and Drug Administration (FDA) advises against the use of a morcellator device for most people who have fibroids removed through myomectomy or hysterectomy. The FDA recommends that people who are nearing menopause or who have reached menopause stay away from power morcellation. Older people who are in or entering menopause may have a higher cancer risk. And people who no longer want to get pregnant have other treatment options for fibroids.
Myoma prognosis
The prognosis of uterine fibroids varies extensively for individual patients 59. Many women have an excellent prognosis and remain asymptomatic for many years or indefinitely 59. Whereas, others will fail medical management and depending on their desire for future fertility, may experience recurrent fibroids requiring multiple surgeries 59. About 3% to 7% of untreated fibroids in premenopausal women regress over six months to three years, and most decrease in size at menopause 19. Because there is minimal concern for cancer in women with asymptomatic fibroids, watchful waiting is preferred for management 60. There are no studies that support – surveillance with imaging or repeat imaging in asymptomatic women with fibroids 50, 60.
- Al-Hendy A, Myers ER, Stewart E. Uterine Fibroids: Burden and Unmet Medical Need. Semin Reprod Med. 2017 Nov;35(6):473-480. doi: 10.1055/s-0037-1607264[↩]
- Wise LA, Laughlin-Tommaso SK. Epidemiology of Uterine Fibroids: From Menarche to Menopause. Clin Obstet Gynecol. 2016 Mar;59(1):2-24. doi: 10.1097/GRF.0000000000000164[↩]
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003 Jan;188(1):100-7. doi: 10.1067/mob.2003.99[↩][↩]
- Uterine Fibroids. https://familydoctor.org/condition/uterine-fibroids[↩][↩][↩]
- Ross RK, Pike MC, Vessey MP, Bull D, Yeates D, Casagrande JT. Risk factors for uterine fibroids: reduced risk associated with oral contraceptives. Br Med J (Clin Res Ed). 1986 Aug 9;293(6543):359-62. doi: 10.1136/bmj.293.6543.359. Erratum in: Br Med J (Clin Res Ed) 1986 Oct 18;293(6553):1027.[↩][↩]
- Ryan GL, Syrop CH, Van Voorhis BJ. Role, epidemiology, and natural history of benign uterine mass lesions. Clin Obstet Gynecol. 2005 Jun;48(2):312-24. doi: 10.1097/01.grf.0000159538.27221.8c[↩][↩]
- Stewart EA, Nicholson WK, Bradley L, Borah BJ. The burden of uterine fibroids for African-American women: results of a national survey. J Womens Health (Larchmt). 2013 Oct;22(10):807-16. doi: 10.1089/jwh.2013.4334[↩]
- Bulun SE. Uterine fibroids. N Engl J Med. 2013 Oct 3;369(14):1344-55. doi: 10.1056/NEJMra1209993[↩][↩][↩]
- Ishikawa H, Ishi K, Serna VA, Kakazu R, Bulun SE, Kurita T. Progesterone is essential for maintenance and growth of uterine leiomyoma. Endocrinology. 2010 Jun;151(6):2433-42. doi: 10.1210/en.2009-1225[↩][↩]
- Levy B, Mukherjee T, Hirschhorn K. Molecular cytogenetic analysis of uterine leiomyoma and leiomyosarcoma by comparative genomic hybridization. Cancer Genet Cytogenet. 2000 Aug;121(1):1-8. doi: 10.1016/s0165-4608(00)00225-9[↩]
- Berger, L. (2008, October 23). A Decade of Developments in Fibroid Research. New York Times. http://www.nytimes.com/ref/health/healthguide/esn-fibroids-expert.html [↩]
- D’Angelo E, Prat J. Uterine sarcomas: a review. Gynecol Oncol. 2010 Jan;116(1):131-9. doi: 10.1016/j.ygyno.2009.09.023[↩]
- Pérez-López FR, Ornat L, Ceausu I, Depypere H, Erel CT, Lambrinoudaki I, Schenck-Gustafsson K, Simoncini T, Tremollieres F, Rees M; EMAS. EMAS position statement: management of uterine fibroids. Maturitas. 2014 Sep;79(1):106-16. doi: 10.1016/j.maturitas.2014.06.002[↩]
- del Carmen MG. Uterine Leiomyosarcoma. In: Uncommon gynecologic cancers. Chichester, UK: John Wiley & Sons, 2014; p. 167–77. doi:10.1002/9781118655344.ch15.[↩]
- Samuel A, Fennessy FM, Tempany CM, Stewart EA. Avoiding treatment of leiomyosarcomas: the role of magnetic resonance in focused ultrasound surgery. Fertil Steril. 2008 Sep;90(3):850.e9-12. doi: 10.1016/j.fertnstert.2007.08.019[↩]
- Wallis L. FDA warns against power morcellation for hysterectomy and fibroids. Am J Nurs. 2014 Jul;114(7):16. doi: 10.1097/01.NAJ.0000451664.53878.83[↩]
- Lieng M, Berner E, Busund B. Risk of morcellation of uterine leiomyosarcomas in laparoscopic supracervical hysterectomy and laparoscopic myomectomy, a retrospective trial including 4791 women. J Minim Invasive Gynecol. 2015 Mar-Apr;22(3):410-4. doi: 10.1016/j.jmig.2014.10.022[↩]
- Evans P, Brunsell S. Uterine fibroid tumors: diagnosis and treatment. Am Fam Physician. 2007 May 15;75(10):1503-8. https://www.aafp.org/pubs/afp/issues/2007/0515/p1503.html[↩]
- De La Cruz MS, Buchanan EM. Uterine Fibroids: Diagnosis and Treatment. Am Fam Physician. 2017 Jan 15;95(2):100-107. https://www.aafp.org/pubs/afp/issues/2017/0115/p100.html[↩][↩][↩][↩]
- Berger, L. (2008, October 23). A Decade of Developments in Fibroid Research. New York Times.[↩]
- Uterine fibroids. Medline Plus. https://medlineplus.gov/ency/article/000914.htm[↩]
- Lethaby, A., & Vollenhoven, B. (2007). Fibroids (uterine myomatosis, leiomyomas). Clinical Evidence 5. http://www.clinicalevidence.com/x/systematic-review/0814/overview.html[↩]
- American Congress of Obstetricians and Gynecologists. (2009). Uterine fibroids. https://www.acog.org/~/media/For%20Patients/faq074.pdf?dmc=1&ts=20120430T1057019423[↩]
- Martin, C.L., Huber, L.R., Thompson, M.E., & Racine, E.F. (2011). Serum micronutrient concentrations and risk of uterine fibroids. Journal of Women’s Health, 20, 915-922. http://online.liebertpub.com/doi/abs/10.1089/jwh.2009.1782[↩]
- Eunice Kennedy Shriver National Institute of Child Health and Human Development. (2012). Vitamin D shrinks fibroid tumors in rats. https://www.nichd.nih.gov/news/releases/Pages/030112-vitaminD-fibroids.aspx[↩]
- Baird, D., & Wise, L. (2011). Childhood abuse and fibroids. Epidemiology, 22, 15-17. http://journals.lww.com/epidem/Citation/2011/01000/Childhood_Abuse_and_Fibroids.3.aspx [↩]
- Vines, A.I., Ta, M., & Esserman, D.A. (2010). The association between self-reported major life events and the presence of uterine fibroids. Women’s Health Issues, 20, 294-298. http://www.whijournal.com/article/S1049-3867(10)00041-1/fulltext[↩]
- Chiaffarino F, Parazzini F, La Vecchia C, Marsico S, Surace M, Ricci E. Use of oral contraceptives and uterine fibroids: results from a case-control study. Br J Obstet Gynaecol. 1999 Aug;106(8):857-60. doi: 10.1111/j.1471-0528.1999.tb08409.x[↩]
- Faerstein E, Szklo M, Rosenshein N. Risk factors for uterine leiomyoma: a practice-based case-control study. I. African-American heritage, reproductive history, body size, and smoking. Am J Epidemiol. 2001 Jan 1;153(1):1-10. doi: 10.1093/aje/153.1.1[↩]
- Marshall LM, Spiegelman D, Barbieri RL, Goldman MB, Manson JE, Colditz GA, Willett WC, Hunter DJ. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race. Obstet Gynecol. 1997 Dec;90(6):967-73. doi: 10.1016/s0029-7844(97)00534-6[↩]
- Wise LA, Palmer JR, Stewart EA, Rosenberg L. Age-specific incidence rates for self-reported uterine leiomyomata in the Black Women’s Health Study. Obstet Gynecol. 2005 Mar;105(3):563-8. doi: 10.1097/01.AOG.0000154161.03418.e3[↩]
- Ciebiera M, Włodarczyk M, Słabuszewska-Jóźwiak A, Nowicka G, Jakiel G. Influence of vitamin D and transforming growth factor β3 serum concentrations, obesity, and family history on the risk for uterine fibroids. Fertil Steril. 2016 Dec;106(7):1787-1792. doi: 10.1016/j.fertnstert.2016.09.007[↩]
- Sun K, Xie Y, Zhao N, Li Z. A case-control study of the relationship between visceral fat and development of uterine fibroids. Exp Ther Med. 2019 Jul;18(1):404-410. doi: 10.3892/etm.2019.7575[↩]
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. Association of physical activity with development of uterine leiomyoma. Am J Epidemiol. 2007 Jan 15;165(2):157-63. doi: 10.1093/aje/kwj363[↩]
- Shikora SA, Niloff JM, Bistrian BR, Forse RA, Blackburn GL. Relationship between obesity and uterine leiomyomata. Nutrition. 1991 Jul-Aug;7(4):251-5.[↩]
- Takala H, Yang Q, El Razek AMA, Ali M, Al-Hendy A. Alcohol Consumption and Risk of Uterine Fibroids. Curr Mol Med. 2020;20(4):247-258. doi: 10.2174/1566524019666191014170912[↩]
- Baird DD, Hill MC, Schectman JM, Hollis BW. Vitamin d and the risk of uterine fibroids. Epidemiology. 2013 May;24(3):447-53. doi: 10.1097/EDE.0b013e31828acca0[↩]
- Brakta S, Diamond JS, Al-Hendy A, Diamond MP, Halder SK. Role of vitamin D in uterine fibroid biology. Fertil Steril. 2015 Sep;104(3):698-706. doi: 10.1016/j.fertnstert.2015.05.031[↩]
- Stewart EA, Cookson CL, Gandolfo RA, Schulze-Rath R. Epidemiology of uterine fibroids: a systematic review. BJOG. 2017 Sep;124(10):1501-1512. doi: 10.1111/1471-0528.14640[↩]
- Parazzini F, Negri E, La Vecchia C, Chatenoud L, Ricci E, Guarnerio P. Reproductive factors and risk of uterine fibroids. Epidemiology. 1996 Jul;7(4):440-2. doi: 10.1097/00001648-199607000-00018[↩]
- Laughlin SK, Herring AH, Savitz DA, Olshan AF, Fielding JR, Hartmann KE, Baird DD. Pregnancy-related fibroid reduction. Fertil Steril. 2010 Nov;94(6):2421-3. doi: 10.1016/j.fertnstert.2010.03.035[↩]
- Uterine fibroids. https://www.mayoclinic.org/diseases-conditions/uterine-fibroids/symptoms-causes/syc-20354288[↩]
- Uterine Fibroids. Medline Plus. https://medlineplus.gov/uterinefibroids.html[↩]
- Drayer SM, Catherino WH. Prevalence, morbidity, and current medical management of uterine leiomyomas. Int J Gynaecol Obstet. 2015 Nov;131(2):117-22. doi: 10.1016/j.ijgo.2015.04.051[↩][↩]
- Bukulmez O, Doody KJ. Clinical features of myomas. Obstet Gynecol Clin North Am. 2006 Mar;33(1):69-84. doi: 10.1016/j.ogc.2005.12.002[↩]
- Carranza-Mamane B, Havelock J, Hemmings R; REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY COMMITTEE; SPECIAL CONTRIBUTOR. The management of uterine fibroids in women with otherwise unexplained infertility. J Obstet Gynaecol Can. 2015 Mar;37(3):277-285. doi: 10.1016/S1701-2163(15)30318-2[↩]
- Stewart EA, Laughlin-Tommaso SK, Catherino WH, Lalitkumar S, Gupta D, Vollenhoven B. Uterine fibroids. Nat Rev Dis Primers. 2016 Jun 23;2:16043. doi: 10.1038/nrdp.2016.43[↩][↩][↩]
- Holdsworth-Carson SJ, Zaitseva M, Vollenhoven BJ, Rogers PA. Clonality of smooth muscle and fibroblast cell populations isolated from human fibroid and myometrial tissues. Mol Hum Reprod. 2014 Mar;20(3):250-9. doi: 10.1093/molehr/gat083[↩][↩][↩]
- Ghosh S, Naftalin J, Imrie R, Hoo WL. Natural History of Uterine Fibroids: A Radiological Perspective. Curr Obstet Gynecol Rep. 2018;7(3):117-121. doi: 10.1007/s13669-018-0243-5[↩]
- AAGL Advancing Minimally Invasive Gynecology Worldwide; Munro MG, Storz K, Abbott JA, Falcone T, Jacobs VR, Muzii L, Tulandi T, Indman P, Istre O, Jacobs VR, Loffer FD, Nezhat CH, Tulandi T. AAGL Practice Report: Practice Guidelines for the Management of Hysteroscopic Distending Media: (Replaces Hysteroscopic Fluid Monitoring Guidelines. J Am Assoc Gynecol Laparosc. 2000;7:167-168.). J Minim Invasive Gynecol. 2013 Mar-Apr;20(2):137-48. doi: 10.1016/j.jmig.2012.12.002[↩][↩]
- Kashani BN, Centini G, Morelli SS, Weiss G, Petraglia F. Role of Medical Management for Uterine Leiomyomas. Best Pract Res Clin Obstet Gynaecol. 2016 Jul;34:85-103. doi: 10.1016/j.bpobgyn.2015.11.016[↩][↩][↩]
- Hilário SG, Bozzini N, Borsari R, Baracat EC. Action of aromatase inhibitor for treatment of uterine leiomyoma in perimenopausal patients. Fertil Steril. 2009 Jan;91(1):240-3. doi: 10.1016/j.fertnstert.2007.11.006[↩]
- Gurates B, Parmaksiz C, Kilic G, Celik H, Kumru S, Simsek M. Treatment of symptomatic uterine leiomyoma with letrozole. Reprod Biomed Online. 2008 Oct;17(4):569-74. doi: 10.1016/s1472-6483(10)60246-5[↩]
- Song H, Lu D, Navaratnam K, Shi G. Aromatase inhibitors for uterine fibroids. Cochrane Database Syst Rev. 2013 Oct 23;2013(10):CD009505. doi: 10.1002/14651858.CD009505.pub2[↩]
- Sadan O, Ginath S, Sofer D, Rotmensch S, Debby A, Glezerman M, Zakut H. The role of tamoxifen in the treatment of symptomatic uterine leiomyomata — a pilot study. Eur J Obstet Gynecol Reprod Biol. 2001 Jun;96(2):183-6. doi: 10.1016/s0301-2115(00)00468-1[↩]
- Deng L, Wu T, Chen XY, Xie L, Yang J. Selective estrogen receptor modulators (SERMs) for uterine leiomyomas. Cochrane Database Syst Rev. 2012 Oct 17;10:CD005287. doi: 10.1002/14651858.CD005287.pub4[↩]
- Uterine artery embolization. https://medlineplus.gov/ency/article/007384.htm[↩]
- Agency for Healthcare Research and Quality (AHRQ). (2005). The FIBROID Registry: Report of Structure, Methods, and Initial Results. AHRQ Publication No. 05[06]-RG008.[↩]
- Florence AM, Fatehi M. Leiomyoma. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538273[↩][↩][↩]
- Vilos GA, Allaire C, Laberge PY, Leyland N; SPECIAL CONTRIBUTORS. The management of uterine leiomyomas. J Obstet Gynaecol Can. 2015 Feb;37(2):157-178. doi: 10.1016/S1701-2163(15)30338-8[↩][↩]





{kind=link}