
Contents
Period pain
Period pain also called dysmenorrhea, dysmenorrhoea, menstrual pain or menstrual cramps, is a throbbing, cramping pain in your lower abdomen that you get with your menstrual period. Menstrual cramps can feel like a dull ache or a shooting pain. Menstrual cramps most often occur in your low stomach. You may also feel them in your low back, hips, or thighs. Period pain may start before your period or when your period begins. Menstrual cramps last about 1 to 3 days. The pain may be bad enough to keep you from normal activities.
More than half of women who have periods get some pain around their period for 1 to 2 days each month 1). Usually, period pain is mild. But for some women, the pain is so severe that it keeps them from doing their normal activities for several days a month. Some women may get just a feeling of heaviness in the abdomen or tugging in the pelvic area. Other women experience severe cramps different from premenstrual syndrome (PMS) pain. You may also have other symptoms, such as lower back pain, nausea, diarrhea, and headaches. Period pain is not the same as premenstrual syndrome (PMS). PMS (premenstrual syndrome) causes many different symptoms, including weight gain, bloating, irritability, and fatigue. PMS (premenstrual syndrome) often starts one to two weeks before your period starts.
For some women, menstrual cramps (dysmenorrhea) is merely annoying. For others, menstrual cramps can be severe enough to interfere with everyday activities for a few days every month.
Conditions such as endometriosis, adenomyosis or uterine fibroids can cause menstrual cramps. Treating the cause is key to reducing your period pain. Menstrual cramps that aren’t caused by another condition tend to lessen with age and often improve after giving birth.
For most women, to help ease your period pain, you can try:
- Using a heating pad or hot water bottle on your lower abdomen
- Getting some exercise
- Taking a hot bath
- Doing relaxation techniques, including yoga and meditation
- It may also help to get enough rest and avoid using alcohol and tobacco.
You might also try taking over-the-counter pain relievers such as nonsteroidal anti-inflammatory drugs (NSAIDs) 2). NSAIDs (nonsteroidal anti-inflammatory drugs) include ibuprofen and naproxen. Besides relieving pain, nonsteroidal anti-inflammatory drugs (NSAIDs) reduce the amount of prostaglandins (PGs) that your uterus makes and lessen their effects. This helps to lessen the cramps. The choice of NSAID should be based on effectiveness and tolerability for the individual patient, because no NSAID has been proven more effective than others 3). You can take NSAIDs (nonsteroidal anti-inflammatory drugs) when you first have symptoms, when your period starts or one to two days before the anticipated onset of menses. You can keep taking them for two to three days 4), 5). You should not take nonsteroidal anti-inflammatory drugs (NSAIDs) if you have ulcers or other stomach problems, bleeding problems, or liver disease. You should also not take them if you are allergic to aspirin. Always check with your doctor if you are not sure whether or not you should take NSAIDs.
Figure 1. Period pain diagnostic and treatment algorithm
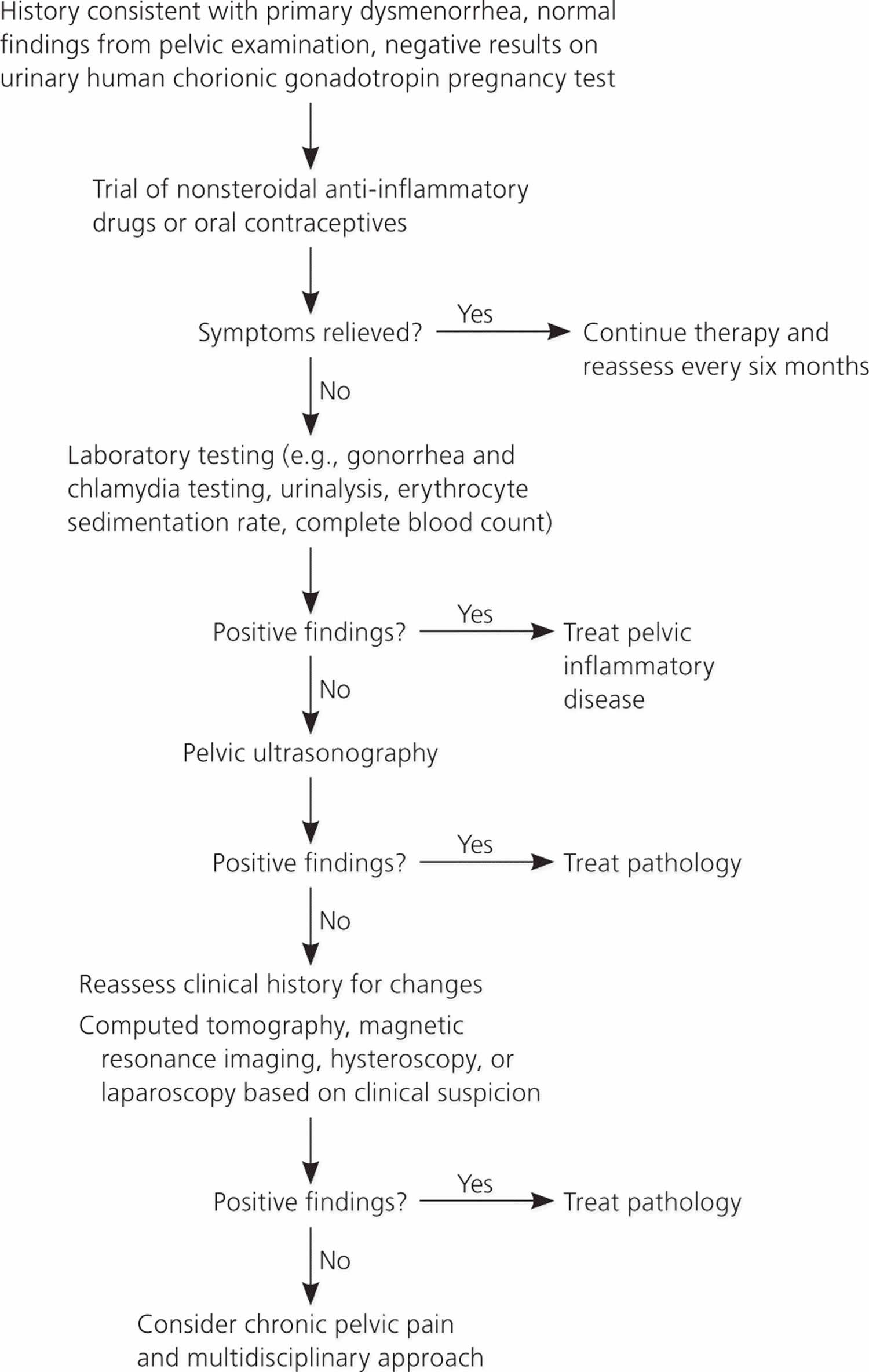
For many women, some pain during your period is normal. However, see your doctor if:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) and self-care measures don’t help, and the pain interferes with your life
- Menstrual cramps disrupt your life every month
- Your symptoms progressively worsen
- Your cramps suddenly get worse
- You are over 25 and you get severe cramps for the first time
- You have a fever with your period pain
- You have the pain even when you are not getting your period
What cause period pain?
There are two types of menstrual cramps (dysmenorrhea): primary and secondary 7), 8). Each type has different causes. Primary dysmenorrhea the menstrual pain has no organic disease and in secondary dysmenorrhea the menstrual pain is associated with conditions that affect your uterus or other reproductive organs, such as endometriosis, adenomyosis and uterine fibroids 9), 10).
Characteristic symptoms of primary dysmenorrhea include lower abdominal or pelvic pain with or without radiation to the back or legs, with initial onset six to 12 months after menarche (Table 2) 11), 12), 13), 14), 15), 16), 17), 18). Pain typically lasts 8 to 72 hours and usually occurs at the onset of menstrual flow. Other associated symptoms may include low back pain, headache, diarrhea, fatigue, nausea, or vomiting 19). A family history may be helpful in differentiating primary from secondary dysmenorrhea; patients with a family history of endometriosis in first-degree relatives are more likely to have secondary dysmenorrhea 20).
About 10% of young adults and adolescents with dysmenorrhea have secondary dysmenorrhea; the most common cause is endometriosis 21). Changes in timing and intensity of the pain or dyspareunia may suggest endometriosis, and menstrual flow abnormalities may be associated with adenomyosis or leiomyomata. A history of sexually transmitted infection or vaginal discharge associated with dyspareunia raises suspicion for pelvic inflammatory disease (PID). Asking about a history of sexual trauma is also recommended 22).
Table 1. Differential diagnosis of primary and secondary dysmenorrhea
| Primary dysmenorrhea | Secondary dysmenorrhea |
|---|---|
| Onset shortly after menarche (the first menstrual period in a female adolescent) | Onset can occur at any time after menarche (typically after 25 years of age) |
| Lower pelvic or abdominal pain is usually associated with onset of menstrual flow and lasts 8 to 72 hours | Women may complain of change in time of pain onset during menstrual cycle or in intensity of pain |
| Back and thigh pain, headache, diarrhea, nausea, and vomiting may be present | Other gynaecological symptoms (such as dyspareunia [painful intercourse], menorrhagia [heavy or prolonged menstrual bleeding]) may be present |
| No abnormal findings on examination | Pelvic abnormality on physical examination |
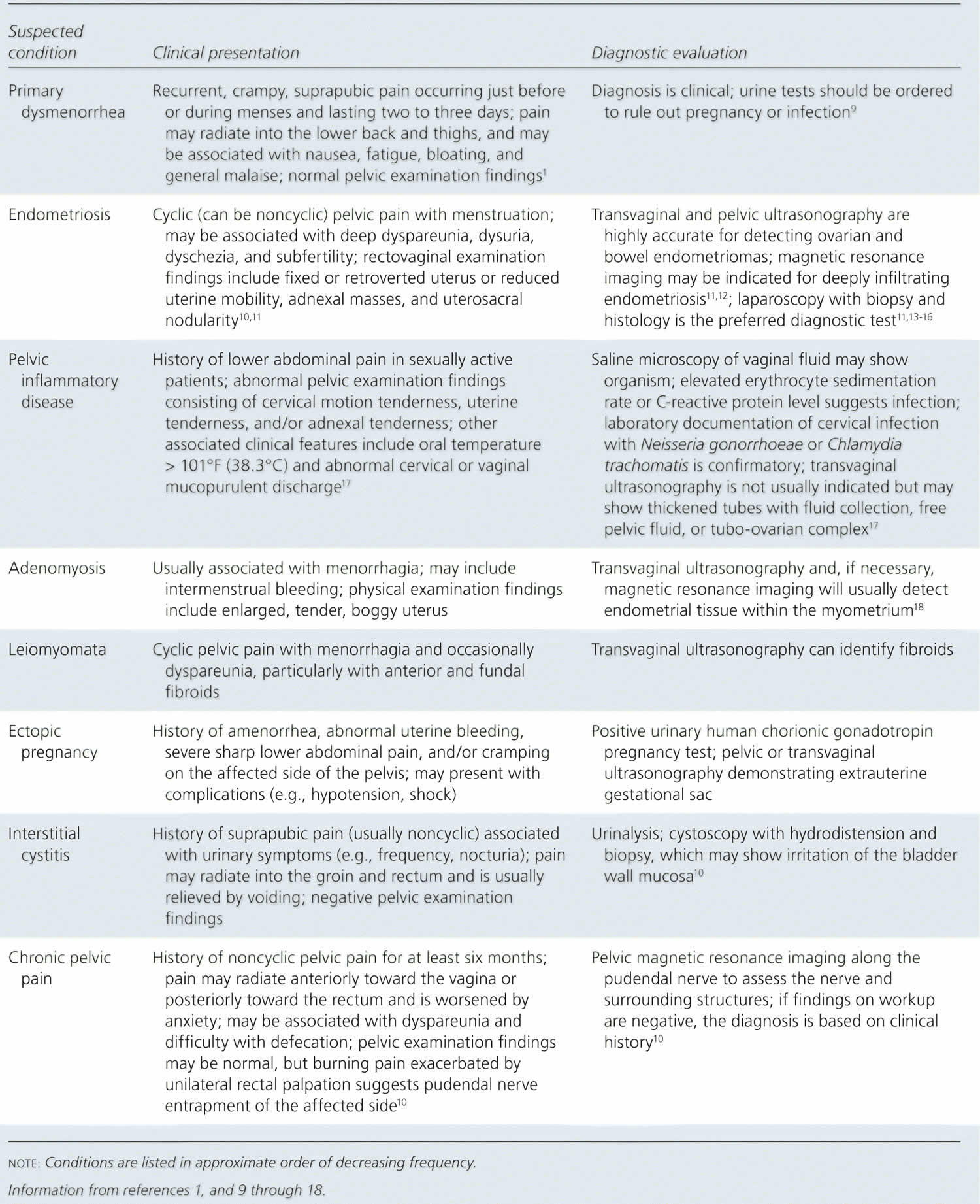
Table 2. Differential diagnosis of Dysmenorrhea
Primary dysmenorrhea
Primary dysmenorrhea is the most common kind of period pain. It is period pain that is not caused by another condition. The cause of primary dysmenorrhea is not well established. However, the responsible cause has been identified on the hyper-production of uterine biologically active compounds called prostaglandins (PGs), particularly of Prostaglandin F2alpha (PGF2α) and Prostaglandin E2 (PGE2), which are chemicals that your uterus makes, resulting in increased uterine tone and high-amplitude contractions 25), 26), 27), 28), 29), 30). Prostaglandins (PGs) make the muscles of your uterus tighten and relax, and this causes the cramps. Prostaglandins (PGs) are also involved in pain and inflammation.
Women with menstrual cramps (dysmenorrhea) have higher levels of prostaglandins (PGs), which are highest during the first two days of menses 31). Higher levels of prostaglandins (PGs) have been noted in the menstrual fluid and endometrial tissue of women with dysmenorrhea 32). Endometrial shedding begins due to the decreasing hormone levels in the menstrual cycle. The time of endometrial shedding during the beginning of menstruation is when the endometrial cells release prostaglandins (PGs). Prostaglandins (PGs) cause uterine contractions, and the intensity of the cramps is proportionate to the amount of prostaglandins (PGs) released 33), 34). Uterine contractions cause tissue hypoxia and ischemia, which in turn cause pain and sometimes associated nausea and diarrhea 35).
Prostaglandin production is controlled by progesterone: when progesterone levels drop, immediately prior to menstruation, prostaglandin levels increase 36), 37). If the exposure of endometrium to luteal phase is crucial for the increased production of progesterone, menstrual cramps (dysmenorrhea) occurs only with ovulatory cycles. This could explain why primary dysmenorrhea onset is shortly after menarche (the first menstrual period in a female adolescent) and why dysmenorrhea responds well to ovulation inhibition. However, multiple other factors may play a role in the perception and the severity of pain, which does not depend only on endocrine factors 38).
The pain can start a day or two before your period. It normally lasts for a few days, though in some women it can last longer.
You usually first start having period pain when you are younger, just after you begin getting periods. Often, as you get older, you have less pain. The pain may also get better after you have given birth.
Secondary dysmenorrhea
Secondary dysmenorrhea often starts later in life. It can be a new symptom for females in their 30s or 40s. Secondary dysmenorrhea is menstrual pain due to an underlying disease, disorder, or structural abnormality within or outside the uterus such as endometriosis, adenomyosis or uterine fibroids 39). This kind of pain often gets worse over time. It may begin before your period starts and continue after your period ends.
Secondary dysmenorrhea can be caused by 40), 41), 42):
- Endometriosis. This condition happens when the lining of the uterus tissue grows outside of the uterus where it does not belong, most commonly on fallopian tubes, ovaries or the tissue lining your pelvis. In response to monthly changes in levels of the hormone estrogen, this lining breaks down and bleeds outside of the uterus and can cause swelling and pain.
- Uterine fibroids. Fibroids are tumors that grow in or on the wall of the uterus. They are almost always not cancerous. Some women with fibroids experience pelvic pain and vaginal bleeding at times when they do not have their period.
- Adenomyosis. The tissue that lines your uterus begins to grow into the muscular walls of the uterus. Adenomyosis is more common in older women who have had children.
- Pelvic inflammatory disease (PID). This infection of the female reproductive organs is usually caused by sexually transmitted bacteria.
- Ovarian cysts. Fluid-filled sacs in your ovary. Ovarian cysts are very common. They often occur during ovulation. This is when the ovary releases an egg each month. These are called functional cysts. Most are noncancerous. Many times, these cysts go away on their own without treatment.
- Use of an intrauterine contraceptive (IUD) system.
- Large cesarean scar niche.
- Cervical stenosis. In some women, the opening of the cervix is small enough to impede menstrual flow, causing a painful increase of pressure within the uterus.
- Problems with the uterus, fallopian tubes, and other reproductive organs. Certain defects that a woman is born with can result in pain during menstruation.
- Some medical conditions can flare up during a period and cause pain. These conditions include Crohn’s disease and urinary disorders.
Common findings that may indicate secondary dysmenorrhea include the following:
- Older age (older than years old) versus younger age, in which primary dysmenorrhea is more common
- Vaginal discharge that is whitish gray, mucopurulent, or has a foul odor (pelvic inflammatory disease concern)
- Friable cervix (sexually transmitted infection concern)
- Dysuria, dyspareunia, vaginismus, dyschezia, infertility, palpable nodularity, adnexal masses, or tenderness on pelvic exam 43)
- Heavy menstrual bleeding with a mildly enlarged symmetrical uterus (adenomyosis)
- Abnormal bleeding with an enlarged asymmetrical uterus (leiomyomas possible)
- Obstructive anatomical abnormalities or history of other congenital anomalies (concern for Müllerian anomaly)
- Pelvic masses (neoplasms, ovarian cysts, endometrioma) 44), 45)
Up to 29% of women with dysmenorrhea may have endometriosis. When considering NSAID-resistant dysmenorrhea, up to 35% of patients may have endometriosis 46). Adenomyosis is another common underlying disease that is associated with secondary dysmenorrhea. Up to 3.8% of young women have reproductive tract anomalies, and both obstructive and non-obstructive anomalies may be associated with secondary dysmenorrhea 47).
Risk factors for period pain and menstrual cramps
You might be at risk of menstrual cramps (dysmenorrhea) if 48):
- You’re younger than age 30
- You started puberty early, at age 11 or younger
- Younger age at menarche
- You have longer and heavier menstrual flow (menorrhagia)
- You have irregular menstrual bleeding (metrorrhagia)
- You have a family history of menstrual cramps (dysmenorrhea)
- You smoke 49)
- Attempts to lose weight
- Higher or lower than normal body mass index (BMI)
- Depression/anxiety
- Longer menstrual cycles
- Nulliparity (a woman who hasn’t given birth to a child)
- History of sexual assault
- Previous cesarean section with incomplete uterine scar healing (uterine niche)
- Disruption of social networks 50), 51)
Period pain symptoms
Symptoms of menstrual cramps include:
- Throbbing or cramping pain in your lower abdomen that can be intense
- Pain that starts 1 to 3 days before your period, peaks 24 hours after the onset of your period and subsides in 2 to 3 days
- Dull, continuous ache
- Pain that radiates to your lower back and thighs
Some women also have:
- Nausea
- Loose stools
- Headache
- Dizziness
Period pain complications
Period pain or menstrual cramps don’t cause other medical complications, but they can interfere with your school, work and social activities.
Certain conditions associated with menstrual cramps can have complications, though. For example, endometriosis can cause fertility problems. Pelvic inflammatory disease can scar your fallopian tubes, increasing the risk of a fertilized egg implanting outside of your uterus (ectopic pregnancy).
Period pain diagnosis
To diagnose severe period pain, your doctor will ask you about your medical history and perform a physical exam, including a pelvic exam. During the pelvic exam, your doctor checks for anything unusual with the reproductive organs and looks for signs of infection.
Your doctor may also recommend certain tests, including:
- Ultrasound. This test uses sound waves to create an image of your uterus, cervix, fallopian tubes and ovaries.
- Other imaging tests. A Computed tomography (CT) scan or Magnetic resonance imaging (MRI) scan provides more detail than an ultrasound and can help your doctor diagnose underlying conditions. Computed tomography (CT) scan combines X-ray images taken from many angles to produce cross-sectional images of bones, organs and other soft tissues inside your body. Magnetic resonance imaging (MRI) uses radio waves and a powerful magnetic field to produce detailed images of internal structures. Both tests are noninvasive and painless.
- Laparoscopy. Although not usually necessary to diagnosis menstrual cramps, laparoscopy can help detect an underlying condition, such as endometriosis, adhesions, fibroids, ovarian cysts and ectopic pregnancy. During this outpatient surgery, your doctor views your abdominal cavity and reproductive organs by making tiny incisions in your abdomen and inserting a fiber-optic tube with a small camera lens.
Period pain differential diagnosis
The differential diagnosis of dysmenorrhea is broad. It can be categorized as gynecological conditions and non-gynecological conditions 52):
- Gynecological conditions
- Endometriosis
- Obstruction of the reproductive tract: Imperforate hymen, transverse vaginal septum, vaginal agenesis, OHVIRA syndrome (uterus didelphys with obstructed hemivagina and ipsilateral renal agenesis), and cervical stenosis
- Functional and nonfunctional adnexal cysts
- Adnexal torsion (this usually does not present with cyclic pain with menses)
- Adenomyosis
- Pelvic inflammatory disease/sexually transmitted infections
- Endometrial polyps
- Asherman syndrome
- Ectopic pregnancy
- Chronic pelvic pain
- Membranous dysmenorrhea: a very uncommon cause of colicky pain from uterine contractions with resultant shedding of the endometrium in one piece, which retains the shape of the uterus 53)
- Non-Gynecological conditions (gastrointestinal, urological, and musculoskeletal)
- Irritable bowel syndrome (IBS)
- Urinary tract infections (UTI)
- Interstitial cystitis
- Musculoskeletal causes: abdominal wall muscles, abdominal wall fascia, pelvic and hip muscles, sacroiliac joints, and lumbosacral muscles
Period pain treatment
If your period pain is primary dysmenorrhea (menstrual pain that is not caused by any organic disease) and you need medical treatment, your doctor might suggest using hormonal birth control, such as the oral contraceptives, patch, ring, or or an intrauterine device (IUD). Another treatment option might be prescription pain relievers such as nonsteroidal anti-inflammatory drugs (NSAIDs). Most patients with primary dysmenorrhea show subjective improvement with NSAID treatment 54). Various studies report successful pain relief in 64 to 100 percent of subjects 55). Although nonsteroidal anti-inflammatory drugs (NSAIDs) are highly effective and widely available without a prescription, many adolescents are not utilizing effective treatment regimens 56). In one study 57), 25 percent of adolescents used less than the recommended dosage of medications, and 43 percent failed to reach the maximum daily frequency.
Oral contraceptives provide another effective and well-studied choice for therapy, especially in women desiring birth control. The necessity of daily medication to prevent symptoms for one or two days a month makes them too cumbersome as a first-line choice compared with the highly effective NSAIDs. Oral contraceptives prevent menstrual pain through a different mechanism than NSAIDs. The action of oral contraceptives is twofold: reduction of menstrual fluid volume and suppression of ovulation 58). Oral contraceptives are effective in about 90 percent of patients with primary dysmenorrhea 59). Any oral contraceptive will work. Studies attempting to prove the superiority of triphasic preparations over monophasic medications or of one type of progesterone component over another have been largely inconclusive 60). All oral contraceptives are very effective compared with placebo. In general, it may take up to three cycles of oral contraceptives for menstrual pain to noticeably diminish, so it is important to stress this point to patients at the time of the initial prescription and consider adding an NSAID for breakthrough pain during the interim 61).
Many adolescents are not aware that oral contraceptives reduce menstrual pain 62). In a prospective study of 308 adolescent females, those with severe symptoms of dysmenorrhea that responded to oral contraceptives were eight times as likely to be consistent users of oral contraceptives 63). Counseling patients about this added benefit might improve their motivation to comply with a daily medication. Norplant and DepoProvera are also effective in relieving dysmenorrhea. As with NSAIDs, it is important to inquire about contraindications: cardiovascular disease, cerebrovascular disease, hepatic disease, history of venous thrombosis or current pregnancy.
Because NSAIDs and oral contraceptives are so effective and work through different mechanisms, a combination of the two is a very attractive option in refractory cases. No consistent data demonstrate effectiveness rates for this combination, but it is probably at least 90 percent, given the previously stated rates of effectiveness for the individual treatments 64). Consequently, about 10 percent of patients may remain nonresponders to combination treatment.
For the approximately 10 percent who do not respond to these medical treatment options, a host of alternatives exists, ranging from laparoscopic surgery to acupuncture, although with much less evidence to support their use. A lack of pain relief should increase suspicion of a secondary cause of dysmenorrhea, that is menstrual pain due to an underlying disease, disorder, or structural abnormality within or outside the uterus 65).
To ease your menstrual cramps, your doctor might recommend:
- Pain relievers. Over-the-counter pain relievers, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve), at regular doses starting the day before you expect your period to begin can help control the pain of cramps. Prescription nonsteroidal anti-inflammatory drugs (NSAIDs) also are available. Start taking the pain reliever at the beginning of your period, or as soon as you feel symptoms, and continue taking the medicine as directed for two to three days, or until your symptoms are gone.
- Hormonal birth control. Oral birth control pills contain hormones that prevent ovulation and reduce the severity of menstrual cramps. These hormones can also be delivered in several other forms: an injection, a skin patch, an implant placed under the skin of your arm, a flexible ring that you insert into your vagina, or an intrauterine device (IUD).
If you have secondary dysmenorrhea (menstrual pain that is caused by uterus or other reproductive organs disease), your treatment depends upon the underlying condition that is causing your pain or cramps. In some cases, you may need surgery.
- Surgery. If your menstrual cramps are caused by a disorder such as endometriosis or uterine fibroids, surgery to correct the problem might help your symptoms. Surgical removal of the uterus also might be an option if other approaches fail to ease your symptoms and if you’re not planning to have children.
Home remedies for period cramps
At-home treatment is available for women who have menstrual cramps. The goal is to relieve symptoms. For period pain relief over-the-counter pain relievers such as nonsteroidal anti-inflammatory drugs (NSAIDs), ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve), at regular doses starting the day before you expect your period to begin can help control the pain of cramps. Besides relieving pain, NSAIDs reduce the amount of prostaglandins (PGs) that your uterus makes and lessen their effects. This helps to lessen the cramps. You can take NSAIDs (nonsteroidal anti-inflammatory drugs) when you first have symptoms, or when your period starts. You can keep taking them for a few days. You should not take nonsteroidal anti-inflammatory drugs (NSAIDs) if you have ulcers or other stomach problems, bleeding problems, or liver disease. You should also not take them if you are allergic to aspirin. Always check with your doctor if you are not sure whether or not you should take NSAIDs.
Furthermore, things you might want to try include 66), 67), 68), 69), 70), 71), 72):
- Getting enough sleep and rest. Getting enough sleep before and during your period is important. Being well rested can help you cope with discomfort.
- Exercise regularly. Physical activity, including sex, helps ease menstrual cramps for some women.
- Use heat. Soaking in a hot bath or using a heating pad, hot water bottle or heat patch on your lower abdomen might ease menstrual cramps.
- Try dietary supplements. A number of studies have indicated that vitamin E, omega-3 fatty acids, vitamin B-1 (thiamin), vitamin B-6 and magnesium supplements might reduce menstrual cramps.
- Reduce stress. Psychological stress might increase your risk of menstrual cramps and their severity.
- Relax. Meditating or practicing yoga also can help you cope with pain.
- Acupuncture. Acupuncture involves inserting extremely thin needles through your skin at strategic points on your body. Some studies have found that acupuncture helps relieve menstrual cramps.
- Acupressure. Like acupuncture, acupressure also involves stimulating certain points on the body, but with gentle pressure on the skin instead of needles. Although research on acupressure and menstrual cramps is limited, it appears that acupressure may be more effective than a placebo in easing menstrual cramps.
- Transcutaneous Electrical Nerve Stimulation (TENS). A transcutaneous electrical nerve stimulation (TENS) device connects to the skin using adhesive patches with electrodes in them. The electrodes deliver a varying level of electric current to stimulate nerves. Transcutaneous electrical nerve stimulation (TENS) might work by raising the threshold for pain signals and stimulating the release of your body’s natural painkillers (endorphins). In studies, transcutaneous electrical nerve stimulation (TENS) was more effective than a placebo in relieving menstrual cramp pain.
- Herbal medicine. Some herbal products, such as pycnogenol, fennel or combination products, might provide some relief from menstrual cramps.
Talk to your doctor if these don’t help. They may suggest a stronger pain reliever. They may want you to try using birth control pills or a birth control shot. These can help make your periods less painful.
Also talk to your doctor if you have any of the following symptoms:
- painful periods that start later in life
- pain at times other than the first couple days of your period
- abnormal vaginal discharge or bleeding
- pain that doesn’t go away when you take medicine to relieve it.
Period pain prognosis
After initial medical treatment is begun and continued for 2 to 3 months before a reassessment of symptoms is performed. If symptoms improve but are still present, a second treatment method may be added. If minimal to no response is noted, a change of treatment with discontinuation of the initial treatment may be offered. Patients are continued on treatment for an additional 3 months and then reassessed 73). If an adequate response is not obtained, evaluation for an underlying cause of secondary dysmenorrhea may be initiated. A multidisciplinary pelvic pain evaluation with physical therapy input and treatment may also be considered 74).
With the use of recommended treatment options, the prognosis for primary dysmenorrhea is generally good. Mild and moderate dysmenorrhea usually responds well to NSAIDs. Severe dysmenorrhea may still respond to NSAIDs but may require higher doses or combination/adjuvant therapy. In the case of persistent dysmenorrhea, secondary causes of dysmenorrhea should be investigated 75). The prognosis of secondary dysmenorrhea depends on the underlying cause, type, location, and severity of the cause 76).
References [ + ]



{kind=link}