
Contents
- What are nonsteroidal anti-inflammatory drugs
- Nonsteroidal anti-inflammatory drugs contraindications
- How do nonsteroidal anti inflammatory drugs work?
- Nonsteroidal anti inflammatory drugs uses
- How to take nonsteroidal anti-inflammatory drugs
- Example of nonsteroidal anti-inflammatory drugs
- Nonsteroidal anti inflammatory drugs side effects
- Nonsteroidal anti inflammatory drugs special precautions
- Best nonsteroidal anti inflammatory drugs
What are nonsteroidal anti-inflammatory drugs
Nonsteroidal anti-inflammatory drugs commonly abbreviated as NSAIDs are medications that are used widely to relieve mild-to-moderate pain, inflammation (swelling & redness) and fever, because these drugs possess antipyretic, analgesic, and anti-inflammatory properties 1, 2, 3. Examples of nonsteroidal anti-inflammatory drugs (NSAIDs) include aspirin, naproxen (e.g., Aleve), ibuprofen (Advil, Motrin, etc.), diclofenac, and COX-2 inhibitors such as celecoxib and meloxicam. COX-2 inhibitors (Cyclooxygenase-2 inhibitors) are a newer class of NSAIDs designed to avoid upset stomach. You can buy nonsteroidal anti-inflammatory drugs (NSAIDs) with a doctor’s prescription or over-the-counter (OTC) for various acute and chronic inflammatory conditions such as arthritis (rheumatoid arthritis, osteoarthritis, ankylosing spondylitis, gout and others), muscle pain, systemic connective tissue diseases, period pain (dysmenorrhea), fever (pyrexia), migraines, ankle sprains, achilles tendinitis, costochondritis, frozen shoulder, golfer’s elbow, jumper’s knee, herniated disc, iliotibial band syndrome and as opioid-sparing agents in certain acute trauma cases 4, 5, 6. Topical nonsteroidal anti-inflammatory drugs (NSAIDs) such as diclofenac sodium 1.5% topical solution, diclofenac hydroxyethyl pyrrolidine 1.3% patch, and diclofenac sodium gel 1% are also available for use in acute tenosynovitis, ankle sprains, and soft tissue injuries 7, 8, 9, 10. Aside from these major uses, the therapeutic benefit of NSAIDs is also indicated for other conditions; neonatal cases of patent ductus arteriosus (PDA), to increase niacin tolerability, and in rare disorders of upregulated prostaglandin synthesis such as systemic mastocytosis resistant to antihistamines 11, 12, 13, 14. There are numerous reports concerning the cancer-protective effects of NSAIDs in the published literature 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25. However, the role of NSAIDs in cancer prevention remains unclear due to contradicting and inconsistent findings. While some studies revealed a reduction in cancer risk, others demonstrated no association between cancer and NSAID use. For example, in a prospective study on about 20,000 women (aged 58–76 years), it was shown that nonaspirin NSAIDs were associated with neither ovarian nor uterine cancer risk 26.
More than 30 million Americans are taking nonsteroidal anti-inflammatory drugs (NSAIDs) every year 27. Common side effects of all nonsteroidal anti-inflammatory drugs (NSAIDs) include stomach problems (such as bleeding, ulcer, and stomach upset), kidney problems, high blood pressure or heart problems, fluid retention, rashes, or allergic reactions and other adverse reactions. NSAIDs, including those bought over-the-counter, have also been linked to a small increase in the risk of stroke and heart attack. This increase in risk affects people who already have heart disease and those who don’t. However, the risk is greater in those who have heart disease. NSAIDs (including aspirin) can also trigger asthma in some people. If you have asthma and need an NSAID for pain relief, talk to your doctor first.
Do not give aspirin to children under age 12. Teens with a virus should also avoid drugs containing aspirin. There is a risk of Reye’s syndrome, a rare but deadly illness that can affect the brain and liver. Previous studies have shown that 5% to 7% of hospital admissions result from drug toxicity, with non-aspirin NSAIDs contributing to 11% to 12% of those admissions 28, 29.
You should discuss with your doctor whether it is okay to take NSAIDs if any of the following apply to you:
- Known problems with kidneys or liver
- History of stomach problems (such as reflux or ulcers)
- Inflammatory bowel disease (Crohn’s disease or ulcerative colitis)
- If you take blood thinners or corticosteroids
- If you have cardiovascular problems (such as high blood pressure, heart failure, past stroke or a heart attack)
Don’t take NSAIDs if you:
- are allergic or hypersensitive to them
- are pregnant or planning a pregnancy
- have a kidney or liver condition
- have a gastrointestinal (gut) ulcer or bleeding
Certain medicines also increase your chance of experiencing nonsteroidal anti-inflammatory drugs side effects, including:
- medicines for cardiovascular disease including medicines for high blood pressure such as beta blockers, ACE inhibitors and angiotensin receptor blockers (ARBs)
- blood thinners such as warfarin or new oral anticoagulants (also known as NOACs, including rivaroxaban, dabigatran and apixaban)
- the osteoporosis treatment alendronate
- the rheumatoid arthritis treatment methotrexate
The American College of Rheumatology recommends monitoring a complete blood count (CBC), kidney function and liver function in rheumatoid arthritis (RA) patients who use NSAIDs long term and who have no comorbidities nor history of complications. Monitoring is less common in patients not considered high risk for NSAID toxicity. However, NSAIDs are either contraindicated, or their use requires monitoring in patients with liver or kidney problems 30.
Nonsteroidal anti-inflammatory drugs contraindications
According to the package insert, nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated in patients:
- With NSAID hypersensitivity or salicylate hypersensitivity, as well as in patients who have experienced an allergic reaction (urticaria, asthma, etc.) after taking NSAIDs
- Who have undergone coronary artery bypass graft surgery
- During the third trimester of pregnancy
Most NSAIDs are derived from organic acids and are rapidly absorbed from the gastrointestinal tract. These drugs undergo extensive liver metabolism and are excreted through glomerular filtration and tubular secretion in your kidneys. For these reasons, NSAIDs are typically contraindicated in patients with severe liver and kidney dysfunction.
U.S. Food and Drug Administration (FDA) is warning that use of NSAIDs around 20 weeks or later in pregnancy may cause rare but serious kidney problems in an unborn baby. This can lead to low levels of amniotic fluid surrounding the baby and possible complications.
For prescription NSAIDs, FDA is requiring changes to the prescribing information to describe the risk of kidney problems in unborn babies that result in low amniotic fluid.
For over-the-counter (OTC) NSAIDs intended for use in adults, FDA will also update the Drug Facts labels, available at: http://bit.ly/2Uadlbz. These labels already warn to avoid using NSAIDs during the last 3 months of pregnancy because the medicines may cause problems in the unborn child or complications during delivery. The Drug Facts labels already advise pregnant and breastfeeding women to ask a health care professional before using these medicines.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
- are a class of medicines available by prescription and OTC. They are some of the most commonly used medicines for pain and fever.
- are used to treat medical conditions such as arthritis, menstrual cramps, headaches, colds, and the flu.
- work by blocking the production of certain chemicals in the body that cause inflammation.
- are available alone and combined with other medicines. Examples of NSAIDs include aspirin, ibuprofen, naproxen, diclofenac, and celecoxib.
Common side effects of NSAIDs include: stomach pain, constipation, diarrhea, gas, heartburn, nausea, vomiting, and dizziness.
RECOMMENDATION:
Consumers/Patients
- If you are pregnant, do not use NSAIDs at 20 weeks or later in pregnancy unless specifically advised to do so by your health care professional because these medicines may cause problems in your unborn baby.
- Many OTC medicines contain NSAIDs, including those used for pain, colds, flu, and insomnia, so it is important to read the Drug Facts labels, to find out if the medicines contain NSAIDs.
- Talk to your health care professional or pharmacist if you have questions or concerns about NSAIDs or which medicines contain them.
- Other medicines, such as acetaminophen, are available to treat pain and fever during pregnancy. Talk to your pharmacist or health care professional for help deciding which might be best.
Health Care Professionals
- FDA recommends that health care professionals should limit prescribing NSAIDs between 20 to 30 weeks of pregnancy and avoid prescribing them after 30 weeks of pregnancy. If NSAID treatment is determined necessary, limit use to the lowest effective dose and shortest duration possible. Consider ultrasound monitoring of amniotic fluid if NSAID treatment extends beyond 48 hours and discontinue the NSAID if oligohydramnios is found. FDA is warning that use of NSAIDs around 20 weeks gestation or later in pregnancy may cause fetal renal dysfunction leading to oligohydramnios and, in some cases, neonatal renal impairment.
- These adverse outcomes are seen, on average, after days to weeks of treatment, although oligohydramnios has been infrequently reported as soon as 48 hours after NSAID initiation.
- Oligohydramnios is often, but not always, reversible with treatment discontinuation.
- Complications of prolonged oligohydramnios may include limb contractures and delayed lung maturation. In some postmarketing cases of impaired neonatal renal function, invasive procedures such as exchange transfusion or dialysis were required.
- If NSAID treatment is deemed necessary between 20 to 30 weeks of pregnancy, limit use to the lowest effective dose and shortest duration possible. As currently described in the NSAID labels, avoid prescribing NSAIDs at 30 weeks and later in pregnancy because of the additional risk of premature closure of the fetal ductus arteriosus.
- The above recommendations do not apply to low-dose 81 mg aspirin prescribed for certain conditions in pregnancy.
- Consider ultrasound monitoring of amniotic fluid if NSAID treatment extends beyond 48 hours. Discontinue the NSAID if oligohydramnios occurs and follow up according to clinical practice.
How do nonsteroidal anti inflammatory drugs work?
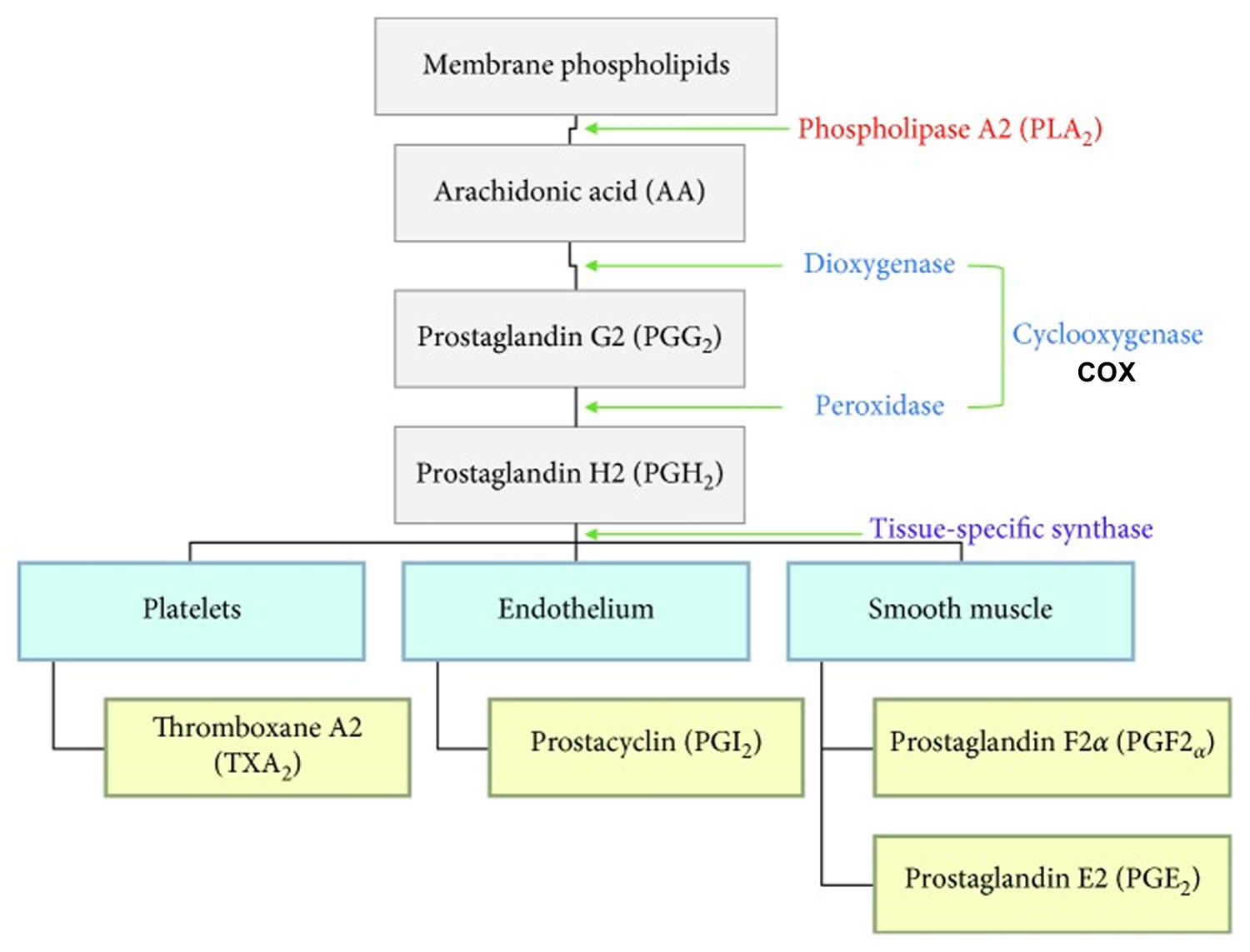
Nonsteroidal anti-inflammatory drugs (NSAIDs) work by inhibition of cyclooxygenase enzymes (COX-1 and COX-2) 31, 32. Cyclooxygenase (COX) is required to convert arachidonic acid into thromboxanes, prostaglandins, and prostacyclins 33. The therapeutic effects of nonsteroidal anti-inflammatory drugs (NSAIDs) are attributed to reducing the amount of thromboxanes, prostaglandins and prostacyclins in your body. Specifically, thromboxanes play a role in platelet adhesion, prostaglandins cause vasodilation, increase the temperature set-point in the hypothalamus, and play a role as pain reliever (anti-nociception).
There are two cyclooxygenase isoenzymes, Cyclooxygenase-1 (COX-1) and Cyclooxygenase-2 (COX-2).
- COX-1 (Cyclooxygenase-1) is expressed in normal cells and produces prostaglandins (PGs) and thromboxane A2 (TXA2) that plays a role in maintaining gastrointestinal mucosa lining, kidney function, platelet aggregation and other physiological functions.
- COX-2 (Cyclooxygenase-2) is not constitutively expressed in the body, instead it is induced in inflammatory cells during an inflammatory response and stress 34, 35, 36, 37. COX-2 produces prostaglandins (PGs) that is related to inflammation, pain and fever.
- COX-2 (Cyclooxygenase-2) inhibition most likely represents the desired effect of NSAIDs’ anti-inflammatory, antipyretic and analgesic response; while COX-1 inhibition plays a major role in the undesired side effects such as gastrointestinal and kidney toxicities.
- The role of NSAIDs in thrombosis and cardioprotection highlights the particular actions of aspirin in mature platelets where COX-1 is irreversibly inhibited, preventing the generation of Thromboxane A2 (TXA2) and its potent effects on platelet activation and vasoconstriction. Aspirin’s irreversibility allows its effects to last the life of the platelet, averaging approximately one week. For this reason, continued doses of aspirin produce a cumulative antiplatelet effect.
Despite the distinct roles of each isozyme, COX-1 and COX-2 can work together, and both contribute to the development of an inflammatory response 38, 39. Most of the NSAIDs are nonselective and inhibit both COX-1 and COX-2. However, cyclooxygenase-2 (COX-2)-selective nonsteroidal antiinflammatory drugs (NSAIDs) (e.g., celecoxib), a newer class of NSAIDs, only target COX-2 and therefore have a different side effect profile compared to non-selective NSAIDs. Importantly, because COX-1 (Cyclooxygenase-1) is the prime mediator for ensuring gastric mucosal integrity and COX-2 (Cyclooxygenase-2) is mainly involved in inflammation, COX-2 selective NSAIDs (e.g., celecoxib) should provide anti-inflammatory relief without compromising the gastric mucosa thus avoiding upset stomach 40.
Inflammation is your body immune system’s response to infection and injury. Inflammation is an intrinsically beneficial event that leads to removal of offending factors and restoration of tissue structure and physiological function. The acute phase of inflammation is characterized by the rapid influx of blood granulocytes, typically neutrophils, followed swiftly by monocytes that mature into inflammatory macrophages that subsequently proliferate and thereby affect the functions of resident tissue macrophages. This process causes the cardinal signs of acute inflammation: redness, heat, swelling and pain 13. The usual outcome of the acute inflammatory program is successful resolution and repair of tissue damage, rather than persistence and dysfunction of the inflammatory response, which can lead to scarring and loss of organ function 41.
There are four principal bioactive prostaglandins generated in the body: prostaglandin (PG) E2 (PGE2), prostacyclin (PGI2), prostaglandin D2 (PGD2) and prostaglandin F2α (PGF2α) 13. During an inflammatory response, both the level and the profile of prostaglandin production changes dramatically. Prostaglandin production is generally very low in uninflamed tissues, but increases immediately in acute inflammation prior to the recruitment of leukocytes and the infiltration of immune cells.
Prostaglandin E2 (PGE2) is a potent inflammatory mediator that is generated by cyclooxygenase-2 (COX-2) conversion of arachidonic acid and are known effectors of pain and inflammation. During inflammation, prostaglandin E2 (PGE2) increases blood flow and vascular permeability by way of PGE2-mediated arterial dilation, which lead to the classical signs of redness and swelling. Prostaglandin E2 (PGE2) also acts on the neurons of the peripheral sensory neurons as well as of certain sites within the central nervous system and gives rise to pain experienced during the inflammatory process 42. The antipyretic effects (reducing fever) of NSAIDs are due in part to the drug class’ ability to suppress PGE2-triggered hypothalamic elevation of body temperature in response to infection or inflammation. On the other hand, prostacyclin (PGI2) is a potent vasodilator and an inhibitor of platelet aggregation 43. Prostacyclin (PGI2) is mainly produced by vascular, endothelial, and smooth muscle cells and is involved in the regulation of cardiovascular homeostasis, whereas prostaglandin D2 (PGD2) is the major eicosanoid synthesized in the central nervous system and peripheral tissues, which appears to play a role in both inflammation and homeostasis 44. Research has shown that prostaglandin D2 (PGD2) is produced as the predominant prostanoid by activated mast cells and plays a role in the initiation of type 1 acute allergic responses mediated by immunoglobulin E (IgE) 45. Another prostaglandin, prostaglandin F2α (PGF2α), is derived from COX-1 in the female reproductive system predominantly. Other than its involvement in ovulation, uterine contraction, and parturition initiation, prostaglandin F2α (PGF2α) has been found at sites of inflammation such as in the synovial fluid collected from the joints of patients with rheumatoid arthritis, psoriatic arthritis, osteoarthritis, and reactive arthritis 46.
Platelets are also active players in the inflammatory processes as a result of COX’s activity on prostaglandin synthesis. Although platelets were once primarily recognized as a key player in hemostasis, its role in inflammation and cancer has been increasingly described in the published literature. Thromboxane A2 (TXA2) is a prostaglandin H2 (PGH2)-derived substance produced by activated platelets, which exerts a potent vasoconstrictor effect and a stimulatory effect on platelet aggregation. However, other than its hemostatic role, thromboxane A2 (TXA2) has been shown to be involved in inflammation and linked to allergic reactions, modulation of acquired immunity, angiogenesis, and cancer cell metastasis 47.
Figure 1. Role of cyclooxygenase (COX) in prostaglandin synthesis
What’s the difference between traditional NSAIDs and COX-2 inhibitors?
You have 2 types of COX enzymes in your body: COX-1 and COX-2. Researchers believe that one of the jobs of COX-1 enzymes is to help protect your stomach lining. The COX-2 enzyme doesn’t play a role in protecting your stomach.
Traditional NSAIDs stop both COX-1 and COX- 2 enzymes from doing their jobs. When COX-1 enzymes are blocked, pain and inflammation are reduced. But the protective lining of your stomach is also reduced. This can cause problems such as upset stomach, ulcers, bloating, and bleeding in your stomach and intestines. Certain NSAIDs may be more likely to cause some of these problems.
COX-2 inhibitors only stop COX-2 enzymes from working. The COX-2 enzyme doesn’t help to protect your stomach. So COX-2 inhibitors may be less likely to irritate your stomach or intestines.
Nonsteroidal anti inflammatory drugs uses
In 1986, the World Health Organization (WHO) developed the analgesic ladder for the treatment of cancer pain to provide adequate pain relief for cancer patients (Figure 2) 49, 50. The World Health Organization (WHO) analgesic ladder, has undergone several modifications over the years and is currently applied for managing cancer pain but also acute and chronic non-cancer painful conditions due to a broader spectrum of diseases such as degenerative disorders, musculoskeletal diseases, neuropathic pain disorders, and other types of chronic pain 51, 52. In the World Health Organization (WHO) analgesic ladder, nonsteroidal anti-inflammatory drugs (NSAIDs) are considered group 1 medications, recommended for mild pain and are the first step in treating pain 53. NSAIDs are commonly prescribed in the setting of acute pain, such as acute musculoskeletal injury. In addition, NSAIDs are also commonly used in the setting of arthritic pain and exceed the analgesic effects of acetaminophen, because of their anti-inflammatory effects 54, 55.
Professional societies, including American Geriatric Society, American College of Rheumatology, and the European League Against Rheumatism, recommend using NSAIDs with caution and limit their use to the lowest effective dose and shortest duration. They recommend that common gastrointestinal, renal and cardiovascular side effects should be routinely monitored 54, 56, 57. Considering this recommendation, the prevalence of inappropriate use of NSAIDs is concerning. In 2015, Ussai et al. 58, did a retrospective study of 3,050 subjects with chronic pain. They found that 97% of chronic pain subjects took NSAIDs for more than 21 consecutive days 58.
The American Geriatric Society updated the Beers Criteria in 2015. They recommended that the chronic use of all NSAIDs, including high dose aspirin, should be avoided because of the risk of gastrointestinal bleeding. High-risk groups include: age above 75 years, corticosteroid use, current use of anticoagulants or antiplatelet agents 59.
Figure 2. WHO analgesic ladder

Footnotes: Adjuvant medications include steroids, anxiolytics, antidepressants, hypnotics, anticonvulsants, antiepileptic-like gabapentinoids (gabapentin and pregabalin), membrane stabilizers, sodium channel blockers, and N-methyl-d-aspartate receptor antagonists for the treatment of neuropathic pain. Cannabinoids can be added to this group of adjuvant medications, not only because they hold a place as adjuvants in the care of palliative cancer patients and patients affected by AIDS, but also because they can be used to offer a better quality of life to patients with chronic pain. They can also be used to treat chronic neuropathic pain 60, 61, 62, 63, 64
Abbreviations: NSAID = nonsteroidal anti-inflammatory drug; PCA = patient-controlled analgesia.
[Source 65 ]How to take nonsteroidal anti-inflammatory drugs
Most commonly, nonsteroidal anti-inflammatory drugs (NSAIDs) are available as oral tablets. Each nonsteroidal anti-inflammatory drug (NSAID) has its own dosing. The dosage size of over-the-counter (OTC) medicine is often less than prescription versions of the same medicine. NSAIDs usually start to work within a few hours. Pain control tends to occur much quicker than its effect on swelling and redness.
According to the package insert, the dosage for the most common over-the-counter (OTC) NSAIDs are as follows:
- Ibuprofen: for 200 mg tablets, 1 to 2 tablets every 4 to 6 hours while symptoms persist. The daily limit for ibuprofen is 1200 mg.
- Aspirin regular strength: for 325 mg tablets, 1 to 2 tablets every 4 hours, or 3 tablets every 6 hours. The daily limit for aspirin is 4000 mg.
- Naproxen sodium: for 220 mg tablets, 1 to 2 tablets every 8 to 12 hours. The daily limit for naproxen sodium is 660 mg.
DO NOT combine nonsteroidal anti-inflammatory drugs (NSAIDs) or take more than the recommended dose. DO NOT give aspirin to children under age 12. Teens with a virus should also avoid drugs containing aspirin. Children should NOT take aspirin because it has been linked to a rare but serious condition called Reye’s syndrome, a rare but deadly illness that can affect the brain and liver.
Topical NSAIDs are also available (diclofenac sodium 1.5% topical solution, diclofenac hydroxyethyl pyrrolidine 1.3% patch, and diclofenac sodium gel 1%). They are most useful for treating pain due to soft-tissue injuries and osteoarthritis 10.
Specific nonsteroidal anti-inflammatory drugs (NSAIDs) can also be administered parenterally; for example, intravenous ibuprofen is available, given as a 30-minute infusion; this can be used as a non-opioid analgesic to manage pain and can also reduce fever. Trials have shown that using intravenous ibuprofen and morphine in postoperative adult patients can lower the total use of morphine. For treating fever, an initial 400mg dose then 400 or 100 to 200 mg every 4 to 6 hours as needed. For the treatment of pain, 400 to 800 mg, every 6 hours as needed, is the recommended dose regimen 66. Ketorolac is also available for parenteral administration.
Example of nonsteroidal anti-inflammatory drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) are typically divided into groups based on their chemical structure and selectivity , which can be categorized into the five classes (see Table 1): acetylated salicylates (aspirin), non-acetylated salicylates (diflunisal, salsalate), propionic acids (naproxen, ibuprofen, acetic acids (diclofenac, indomethacin), enolic acids (meloxicam, piroxicam) anthranilic acids (meclofenamate, mefenamic acid), naphthylalanine (nabumetone), and selective COX-2 inhibitors (celecoxib, etoricoxib). Not all of these listed medications in Table 1 are currently available either in the United States or elsewhere. Only ibuprofen and naproxen are available over-the-counter in the United States; the rest are by prescription only. Carprofen and phenylbutazone are available in the United States as veterinary medications. NSAIDs in use in other countries of the world include acemetacin, azaproprazone, fenbufen, feprazone, floctafenine, flufenamic acid, nimesulide, pirprofen, and tiaprofenic acid.
NSAIDs withdrawn from use or testing because of liver damage or other serious adverse events include benoxaprofen, sudoxicam, isoxicam, fluproquazone, bromfenac, oxyphenbutazone and phenylbutazone (aplastic anemia), indoprofen (gastrointestinal bleeding), suprofen and zomepirac (anaphylaxis).
Listed below are the FDA-approved NSAIDs (organized alphabetically):
- Non-selective nonsteroidal anti-inflammatory drugs (non-selective NSAIDs):
- Diclofenac
- Diflunisal
- Etodolac
- Fenoprofen
- Flurbiprofen
- Ibuprofen
- Indomethacin
- Ketoprofen
- Ketorolac
- Mefenamic acid
- Meloxicam
- Nabumetone
- Naproxen
- Oxaprozin
- Piroxicam
- Sulindac
- Tolmetin
- COX-2 inhibitors NSAIDs:
- Celecoxib
- Rofecoxib (withdrawn from the market 2004)
- Valdecoxib (withdrawn from the market 2005)
Note: Rofecoxib and valdecoxib were withdrawn from the market in 2004 and 2005, respectively, due to adverse cardiovascular events such as edema, myocardial infarction, thrombotic events, stroke and hypertension.
Table 1. Nonsteroidal anti-inflammatory drugs (NSAIDs) list
| Propionic acids | Acetic acids | Fenamic acids | Pyrazalones | Oxicams |
|---|---|---|---|---|
| Carprofen Benoxaprofen Fenbufen Fenoprofen* Flurbiprofen* Ibuprofen* Indoprofen Ketoprofen* Loxoprofen Oxaprozin* Naproxen* Pirprofen Tiaprofenic acid | Aceclofenac* Acemetacin Bromfenac Diclofenac* Etodolac* Indomethacin* Ketorolac* Nabumetone* Sulindac* Tolmetin* Zomepirac | Floctafenine Flufenamic Meclofenamate* Mefenamic acid* | Azapropazone Feprazone Oxyphenbutazone Phenylbutazone | Isoxicam Lornoxicam Meloxicam* Piroxicam* Sudoxicam |
Footnote: * Currently available for human use in the United States.
[Source 3 ]Aceclofenac
Aceclofenac is used for the treatment of pain and inflammation in osteoarthritis (arthritis caused by a breakdown of the lining of the joints), rheumatoid arthritis (arthritis caused by swelling of the lining of the joints), and ankylosing spondylitis (arthritis that mainly affects the spine) 67, 68, 69. Aceclofenac works by blocking the effect of cyclooxygenase (COX) enzymes that make chemical prostaglandins at sites of injury or injury causing pain, swelling, and inflammation.
Like other NSAIDs, aceclofenac is generally well tolerated, but side effects can include headache, dizziness, somnolence, dyspepsia, nausea, abdominal discomfort, heartburn, diarrhea, peripheral edema, pruritus and hypersensitivity reactions.
Celecoxib
Celecoxib is a nonsteroidal antiinflammatory drug (NSAID) with selectively for inhibition of cycloxgenase-2 (COX-2), which is widely used in the therapy of arthritis. The specificity for COX-2 inhibition is believed to make celecoxib less likely to cause gastrointestinal mucosal injury compared to standard NSAIDs that inhibit both COX-1 and COX-2 enzymes. Celecoxib is indicated for therapy of chronic arthritis due to osteoarthritis (arthritis caused by a breakdown of the lining of the joints), rheumatoid arthritis (arthritis caused by swelling of the lining of the joints), juvenile rheumatoid arthritis and ankylosing spondylitis (arthritis that mainly affects the spine) 70, 71. Celecoxib is also approved for use in acute pain from musculoskeletal conditions and trauma and for primary dysmenorrheal (period pain and cramps) and to relieve other types of short-term pain including pain caused by injuries, surgery and other medical or dental procedures, or medical conditions that last for a limited time. Because of the role of the COX-2 enzyme system in the growth of adenomatous polyps, celecoxib has also been used to prevent adenomatous polyps formation. Celecoxib was first approved for use in the United States in 2000 and became the only COX-2 specific NSAID available when rofecoxib was withdrawn in 2006 because of increased rate of cardiovascular events associated with its long term use. Celecoxib is available by prescription as capsules of 50, 100, 200 and 400 mg under the commercial name Celebrex and is usually given in several week courses or long term. The recommended dose varies by indication, the usual adult dose in arthritis being 100 to 200 mg twice daily. Like most NSAIDs, celecoxib is generally well tolerated, but side effects can include dizziness, headache, somnolence, rash, nausea, diarrhea, abdominal discomfort, heartburn, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as celecoxib may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as celecoxib if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take celecoxib right before or right after the surgery.
NSAIDs such as celecoxib may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking celecoxib. Tell your doctor if you drink large amounts of alcohol or if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines or other bleeding disorders. If you experience any of the following symptoms, stop taking celecoxib and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to celecoxib. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with celecoxib and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Diclofenac
Diclofenac is a commonly used nonsteroidal antiinflammatory drug (NSAID) used for the therapy of chronic forms of arthritis and mild-to-moderate acute pain. Like other NSAIDs, diclofenac acts as by inhibiting cellular cyclooxygenases (Cox-1 and Cox-2), which results in a decrease in production of pro-inflammatory prostaglandin, prostacyclin and thromboxane products, important mediators of inflammation and pain. Diclofenac has analgesic as well as antipyretic and antiinflammatory activities. Diclofenac was first approved in the United States in 1988 and currently over 5 million prescriptions are filled yearly. Current indications include mild-to-moderate forms of joint pain, caused by osteoarthritis, rheumatoid arthritis and ankylosing spondylitis as well as relief of symptoms of dysmenorrhea and mild-to-moderate pain. Diclofenac is available in multiple generic and brand formulations, either alone or in combination with other analgesics or gastointestinal mucosal protective agents (such as misoprostol). Diclofenac is not available over-the-counter in the United States, but it is in many other countries where indications include joint and muscle pain from trauma, bursitis, tendonitis, headache and dysmenorrhea. As a result, diclofenac is one of the most frequently used NSAIDs worldwide. Common commercial names for agents containing diclofenac include: Arthrotec, Cataflam, Duravolten, Novo-Difenac, Nu-Diclo, Voltaren and Zorvoflex. Diclofenac is available in multiple dose formulations, including 25, 50 and 75 mg tablets or capsules.
Diclofenac capsules (Zipsor, Zorvolex) and tablets (Cataflam) are used to relieve mild to moderate pain. Diclofenac extended-release tablets (Voltaren XR), tablets (Cataflam), and delayed-release tablets (available generically) are used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints), and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Diclofenac extended-release tablets and delayed-release tablets are also used to treat ankylosing spondylitis (arthritis that mainly affects the spine). Diclofenac tablets (Cataflam) are also used to treat painful menstrual periods. Diclofenac solution (Cambia) is used to treat migraine headaches in adults, but cannot be used to prevent migraines or to treat other types of headaches.
The recommended dose of diclofenac for chronic arthritis in adults is 50 mg orally three times daily; lower and intermittent doses are used for pain. Like most NSAIDs, diclofenac is generally well tolerated, but side effects can include headache, dizziness, somnolence, rash, nausea, diarrhea, dyspepsia, abdominal pain, heartburn, gastrointestinal bleeding, peripheral edema and hypersensitivity reactions.
Diclofenac is also available in several topical forms. Ophthalmic solutions (0.1%) are available for relief of pain or decrease in inflammation after cataract or corneal surgery. Dermatological gels are used for treatment of actinic keratoses. Diclofenac dermatologic patches are available for treatment of acute pain from minor strains, sprains and contusions. Diclofenac gels and creams have also been used for topical therapy of osteoarthritis for specific joints that are amenable to topical treatment. Topical formulations are available generically and under brand names such as Flector patch, Pennsaid, Solaraze, Surpass and Voltaren gel.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as diclofenac may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as diclofenac if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take diclofenac right before or right after the surgery.
NSAIDs such as diclofenac may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking diclofenac. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking diclofenac and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to diclofenac. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with diclofenac and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Diflunisal
Diflunisal is a nonsteroidal anti-inflammatory drug (NSAID) that is used to treat mild to moderate pain, tenderness, swelling and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Diflunisal is also used to relieve mild to moderate pain from other causes. Diflunisal is available by prescription only.
Diflunisal was approved for use in the United States in 1982 and current indications are for chronic arthritis due to osteoarthritis or rheumatoid arthritis and for mild-to-moderate pain. Diflunisal has been shown to stabilize transthyretin variants which are involved in the pathogenesis of amyloidosis, which has led to the off-label use of diflunisal in familial amyloidosis. Diflunisal is available as tablets of 500 mg in generic forms and formerly under the brand name of Dolobid. The recommended regimen in adults is an initial dose of 1000 mg, followed by 500 to 1500 mg daily in two to three divided doses based upon response and tolerance. Diflunisal, like most NSAIDs, is generally well tolerated, but side effects can include intestinal upset, nausea, heartburn, headache, somnolence, dizziness, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as diflunisal may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as diflunisal if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take diflunisal right before or right after the surgery.
NSAIDs such as diflunisal may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while you are taking diflunisal. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking diflunisal and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to diflunisal. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with diflunisal and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Etodolac
Etodolac is a nonsteroidal antiinflammatory drug (NSAID) that is available by prescription only and is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Etodolac tablets and capsules are also used to relieve pain from other causes.
Etodolac was approved in the United States in 1991 and is available by prescription only. Currently more than 3 million prescriptions are filled yearly. Current indications include treatment of osteoarthritis and rheumatoid arthritis and for short term treatment of acute pain. Etodolac is available as capsules or tablets in doses of 200, 300, 400 and 500 mg generically and under the trade name Lodine. Extended release formulations of 400, 500 and 600 mg are also available for once or twice daily dosing. The recommended dose is 400 to 1200 mg in 2 to 4 divided doses daily, based upon response and tolerance. Like other NSAIDs, etodolac is generally well tolerated, but side effects can include headache, dizziness, somnolence, dyspepsia, nausea, abdominal discomfort, heartburn, diarrhea, peripheral edema, pruritus and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as etodolac may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as etodolac if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take etodolac right before or right after the surgery.
NSAIDs such as etodolac may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while you are taking etodolac. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines or other bleeding disorders. If you experience any of the following symptoms, stop taking etodolac and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to etodolac. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with etodolac and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Fenoprofen
Fenoprofen is a nonsteroidal antiinflammatory drug (NSAID) used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Fenoprofen is also used to relieve mild to moderate pain from other causes.
Fenoprofen was approved in the United States in 1976 and is still in clinical use. Current indications include chronic joint pain due to osteoarthritis and rheumatoid arthritis, as well as mild-to-moderate acute pain. The recommended dose in adults with pain is 200 mg every 4 to 6 hours. Higher doses are used for chronic arthritis, in the range of 400 to 600 mg 3 or 4 times per day, with a maximum dose of 3,200 mg daily. Fenoprofen is available by prescription only in the form of capsules or tablets of 200, 300, 400 and 600 mg in both generic and trade formulations (Nalfon). As with other NSAIDs, fenoprofen is generally well tolerated, but side effects can include headache, dizziness, somnolence, gastrointestinal upset, nausea, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as fenoprofen may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as fenoprofen if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke,and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take fenoprofen right before or right after the surgery.
NSAIDs such as fenoprofen may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking fenoprofen. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking fenoprofen and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to fenoprofen. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with fenoprofen and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Flurbiprofen
Flurbiprofen is a nonsteroidal antiinflammatory drug (NSAID) used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints).
Flurbiprofen was approved in the United States in 1988. Current indications include chronic joint pain due to osteoarthritis and rheumatoid arthritis, as well as mild-to-moderate acute pain. The recommended dose in adults with chronic arthritis is 50 to 100 mg two to four times daily, with a maximum dose of 300 mg daily. Flurbiprofen is available by prescription in the form of capsules or tablets of 50 and 100 mg in both generic and trade formulations (Ansaid). As with other NSAIDs, flurbiprofen is generally well tolerated, but side effects can include headache, dizziness, somnolence, gastrointestinal upset, nausea, abdominal discomfort, diarrhea, edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as flurbiprofen may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as flurbiprofen if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take flurbiprofen right before or right after the surgery.
NSAIDs such as flurbiprofen may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while you are taking flurbiprofen. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines or other bleeding disorders. If you experience any of the following symptoms, stop taking flurbiprofen and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to flurbiprofen. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with flurbiprofen and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Ibuprofen
Ibuprofen is a commonly used nonsteroidal antiinflammatory (NSAID) drug which is available both by prescription and over-the-counter (OTC). Prescription ibuprofen is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Prescription ibuprofen is also used to relieve mild to moderate pain, including menstrual pain (pain that happens before or during a menstrual period). Over-the-counter (OTC) ibuprofen is used to reduce fever and to relieve minor aches and pain from headaches, muscle aches, arthritis, menstrual periods, the common cold, toothaches, and backaches.
Ibuprofen was approved for use by prescription in the United States in 1974 and was made available over-the-counter in 1984. Currently, more than 20 million prescriptions for ibuprofen are filled yearly, a number that does not include its vast over-the-counter use. Ibuprofen is used for treatment of mild-to-moderate forms of joint pain and arthritis from trauma, osteoarthritis or rheumatoid arthritis. Ibuprofen is also active against other forms of pain including headache and dysmenorrhea. The recommended dose for chronic arthritis in adults is 400 to 800 mg orally three to four times daily, whereas intermittent dosing with lesser amounts is used for headache and pain. Ibuprofen is available both by prescription and over-the-counter in multiple generic formulations, either alone or in combination with other analgesics, antihistamines or anticholinergic agents usually in doses of 200, 400, 600, or 800 mg. Pediatric formulations are also available. Common brand names for ibuprofen include Advil, Motrin, Nuprin, Rufen and Trendar. Ibuprofen is also found in many combination formulations for dysmenorrhea, headache, allergies, upper respiratory tract symptoms and other pain syndromes under names such as Dristan, Haltran, and Aches-N-Pain. Side effects are not common, but may include headache, dizziness, somnolence, dyspepsia, nausea, abdominal discomfort, heartburn, diarrhea, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as ibuprofen may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. These problems may develop at any time during treatment, but the risk may be higher for people who take NSAIDs for a long time or at higher doses. Do not take an NSAID such as ibuprofen if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke; if you smoke; and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take ibuprofen right before or right after the surgery.
NSAIDs such as ibuprofen may cause ulcers, bleeding, or holes in the esophagus (tube between the mouth and stomach), stomach, or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, who smoke, or who drink large amounts of alcohol while taking ibuprofen. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’); aspirin; other NSAIDs such as naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos);selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking ibuprofen and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to ibuprofen. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with prescription ibuprofen and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Indomethacin
Indomethacin is a potent nonsteroidal antiinflammatory drug (NSAID) typically used to relieve moderate to severe pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints), rheumatoid arthritis (arthritis caused by swelling of the lining of the joints), and ankylosing spondylitis (arthritis that mainly affects the spine). Indomethacin is also used to treat pain in the shoulder caused by bursitis (inflammation of a fluid-filled sac in the shoulder joint) and tendinitis (inflammation of the tissue that connects muscle to bone). Indomethacin immediate-release capsules and suspension (liquid) are also used to treat acute gouty arthritis (attacks of severe joint pain and swelling caused by a build-up of certain substances in the joints).
Indomethacin was approved for use in the United States in 1965 and it continues to be widely used, with more than 2.5 million prescriptions filled yearly. Indomethacin is indicated for management of various forms of chronic arthritis, including osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, and gouty arthritis, as well as acute shoulder pain and dysmenorrhea. Intravenous formulations of indomethacin are approved for the special indication of closure of patent ductus arteriosis in premature infants. Indomethacin is available by prescription as capsules of 25, 50 and 75 mg, in sustained release forms, as suppositories and as suspensions for oral use, in multiple generic forms as well as under several commercial names, including Indocin, Indochron, Indolar, Indo-Lemmon and Zendole. The recommended dosage in adults with chronic arthritis is 25 to 50 mg taken orally two to three times daily, increasing the dose until the symptoms are controlled or a maximum dose of 200 mg is reached. Injectible formulations of indomethacin are available in single dose 1 mg vials for intravenous use in premature infants with patent ducutus arteriosis. Non-hepatic side effects of indomethacin include headache, dizziness, somnolence, dyspepsia, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as indomethacin may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as indomethacin if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take indomethacin right before or right after the surgery.
NSAIDs such as indomethacin may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking indomethacin. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as diflunisal (Dolobid), ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking indomethacin and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to indomethacin. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with indomethacin and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Ketoprofen
Ketoprofen is a nonsteroidal antiinflammatory drug (NSAID) used to treat mild to moderate pain, such as menstrual cramps or arthritis. Prescription ketoprofen is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Prescription ketoprofen capsules are also used to relieve pain, including menstrual pain (pain that occurs before or during a menstrual period). Over-the-counter (OTC) ketoprofen is used to relieve minor aches and pain from headaches, menstrual periods, toothaches, the common cold, muscle aches, and backaches, and to reduce fever.
Ketoprofen was approved in the United States in 1986 and is still widely used. Current indications include chronic joint pain due to osteoarthritis and rheumatoid arthritis as well as mild-to-moderate acute pain and dysmenorrhea. The recommended dose in adults with chronic arthritis is 50 to 75 mg 3 or 4 times per day with a maximum dose of 300 mg daily. Ketoprofen is available by prescription in the form of capsules or tablets of 25, 50 and 75 mg in both generic and trade formulations (Orudis, Oruvail, among others). Extended release formulations of 100, 150 and 200 mg are also available for once daily dosing. Ketoprofen is also available in over-the-counter formulations of 12.5 mg tablets for treatment of mild-to-moderate pain and dysmenorrhea. As with other NSAIDs, ketoprofen is generally well tolerated, but side effects can include headache, dizziness, somnolence, gastrointestinal upset, nausea, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) other than aspirin, such as ketoprofen, may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as ketoprofen if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take ketoprofen right before or right after the surgery.
NSAIDs such as ketoprofen may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink more than three alcoholic drinks per day while taking ketoprofen. Tell your doctor if you drink large amounts of alcohol or if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn); or oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines or other bleeding disorders. If you experience any of the following symptoms, stop taking ketoprofen and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to ketoprofen. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with prescription ketoprofen and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Ketorolac
Ketorolac is a potent, short acting nonsteroidal antiinflammatory drug (NSAID) that is available in both parenteral and oral forms. Ketorolac is used to relieve moderately severe pain, usually after surgery.
Ketorolac was approved in the United States in 1991 and current indications are limited to the short term management of moderately severe, acute pain. Ketorolac is available in parenteral and oral forms in multiple generic forms and under the brand name Toradol. The recommended dose is 60 mg intramuscularly or 30 mg intravenously initially, followed by 30 mg every 6 hours for up to 5 days. An oral form is available in 10 mg tablets for switching from the parenteral form and is given every 6 to 8 hours, but continuation beyond 5 days is not recommended. Ketorolac is available by prescription only and it is used largely for management of postoperative pain. Common side effects include gastrointestinal upset, nausea, headache and itching.
Ketorolac is used for the short-term relief of moderately severe pain and should not be used for longer than 5 days, for mild pain, or for pain from chronic (long-term) conditions. You will receive your first doses of ketorolac by intravenous (into a vein) or intramuscular (into a muscle) injection in a hospital or medical office. After that, your doctor may choose to continue your treatment with oral ketorolac. You must stop taking oral ketorolac on the fifth day after you received your first ketorolac injection. Talk to your doctor if you still have pain after 5 days or if your pain is not controlled with this medication. Ketorolac may cause serious side effects, especially when taken improperly. Take ketorolac exactly as directed. Do not take more of it or take it more often than prescribed by your doctor.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as ketorolac may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as ketorolac if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke or ‘ministroke;’ if you smoke; and if you have or have ever had high cholesterol, high blood pressure, bleeding or clotting problems, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you are having surgery, including dental surgery, tell the doctor or dentist that you are taking ketorolac. If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take ketorolac right before or right after the surgery.
NSAIDs such as ketorolac may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking ketorolac. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Do not take aspirin or other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn) while you are taking ketorolac. Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines. If you experience any of the following symptoms, stop taking ketorolac and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Ketorolac may cause kidney failure. Tell your doctor if you have kidney or liver disease, if you have had severe vomiting or diarrhea or think you may be dehydrated, and if you are taking angiotensin-converting enzyme (ACE) inhibitors such as benazepril (Lotensin, in Lotrel), captopril, enalapril (Vasotec, in Vaseretic), fosinopril, lisinopril (in Zestoretic), moexipril (Univasc), perindopril (Aceon, in Prestalia), quinapril (Accupril, in Quinaretic), ramipril (Altace), and trandolapril (Mavik, in Tarka); or diuretics (‘water pills’). If you experience any of the following symptoms, stop taking ketorolac and call your doctor: swelling of the hands, arms, feet, ankles, or lower legs; unexplained weight gain; confusion; or seizures.
Some people have severe allergic reactions to ketorolac. Tell your doctor if you are allergic to ketorolac, aspirin or other NSAIDs such as ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn), or any other medications. Also tell your doctor if you have or have ever had asthma, especially if you also have frequent stuffed or runny nose or nasal polyps (swelling of the lining of the nose). If you experience any of the following symptoms, stop taking ketorolac and call your doctor right away: rash; hives; itching; swelling of the eyes, face, throat, tongue, arms, hands, ankles, or lower legs; difficulty breathing or swallowing; or hoarseness.
Do not breastfeed while you are taking ketorolac.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to ketorolac. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with ketorolac and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Meclofenamate
Meclofenamate is a nonsteroidal anti-inflammatory drug (NSAID) used to reduce fever, relieve mild to moderate pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints), rheumatoid arthritis (arthritis caused by swelling of the lining of the joints) and and juvenile arthritis in children who are at least 14 years old. Meclofenamate is also used to relieve the symptoms of ankylosing spondylitis (arthritis that mainly affects the spine), painful shoulder (eg, acute subacromial bursitis, supraspinatus tendinitis), or gouty arthritis. Meclofenamate is also used to relieve other types of mild to moderate pain, including menstrual pain (pain that happens before or during a menstrual period). Meclofenamate also may be used to decrease bleeding in women who have abnormally heavy menstrual blood loss.
Meclofenamate comes as a capsule to take by mouth. It is usually taken three or four times a day for arthritis, three times a day for heavy menstrual blood loss, or every 4 to 6 hours as needed for pain. Meclofenamate may be taken with food or milk to prevent nausea. If you take meclofenamate regularly, take it at the same times every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take meclofenamate exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
If you are taking meclofenamate to reduce heavy menstrual bleeding, your bleeding should decrease during your treatment. Call your doctor if your bleeding does not decrease or if you experience spotting or bleeding between menstrual periods.
If you are taking meclofenamate to relieve the symptoms of arthritis, your symptoms may begin to improve within a few days. It may take 2 to 3 weeks or longer for you to feel the full benefit of meclofenamate.
Meclofenamate may cause side effects:
- diarrhea
- constipation
- gas
- sores in the mouth
- headache
- ringing in the ears
Meclofenamate may cause other side effects. Call your doctor if you have any unusual problems while taking this meclofenamate.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as meclofenamate may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take meclofenamate right before or right after the surgery.
NSAIDs such as meclofenamate may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking meclofenamate. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); or oral steroids such as dexamethasone (Decadron, Dexone), methylprednisolone (Medrol), and prednisone (Deltasone). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking meclofenamate and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to meclofenamate. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with meclofenamate and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Mefenamic acid
Mefenamic acid is a nonsteroidal antiinflammatory drug (NSAID) used largely to relieve mild to moderate pain, including menstrual pain (pain that happens before or during a menstrual period).
Mefenamic acid was approved in the United States in 1967, but is not a commonly used agent. Mefenamic acid is indicated for the treatment of mild-to-moderate acute pain or dysmenorrhea (menstrual pain). Mefenamic acid is available by prescription only in capsules of 250 and 500 mg in generic forms and under the brand name Ponstel. The recommended dose is 250 to 500 mg 3 to 4 times daily for periods of less than 7 days. Like most NSAIDs, mefenamic acid is generally well tolerated, but side effects can include headache, dizziness, somnolence, nausea, diarrhea, abdominal discomfort, heartburn, peripheral edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as mefenamic acid may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as mefenamic acid if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take mefenamic acid right before or right after the surgery.
NSAIDs such as mefenamic acid may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or who drink large amounts of alcohol while taking mefenamic acid. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking mefenamic acid and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to mefenamic acid. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with mefenamic acid and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Meloxicam
Meloxicam is a long acting nonsteroidal antiinflammatory drug (NSAID) available by prescription only and used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Meloxicam is also used to relieve the pain, tenderness, swelling, and stiffness caused by juvenile rheumatoid arthritis (a type of arthritis that affects children) in children 2 years of age and older. Oral meloxicam has a delayed time to onset, requiring several days to achieve its full effect, which makes it unsuitable for treating acute pain, but more appropriate for chronic use as in the chronic arthritis.
Meloxicam has a ten-fold selectivity in inhibiting Cox-2 over Cox-1 in test tube studies. The specificity for Cox-2 is believed to make meloxicam less likely to cause gastrointestinal mucosal injury compared to standard NSAIDs that inhibit both Cox enzymes, which would suggest that it should have fewer gastrointestinal side effects and less effects on platelet function than the nonselective Cox inhibitors (Cox-1 and Cox-2). However, in humans, meloxicam in full doses has a similar side effect profile as most nonselective NSAIDs, and its clinical advantage has yet to be proven.
Meloxicam was approved in the United States in 2000 and currently more than 9 million prescriptions are filled yearly. Current indications are for chronic osteoarthritis, rheumatoid arthritis and juvenile rheumatoid arthritis. Meloxicam is available by prescription only in 7.5 and 15 mg tablets in generic forms and under the brand name Mobic. The recommended dose is 7.5 to 15 mg once daily. Like most NSAIDs, meloxicam is generally well tolerated, but side effects can include gastrointestinal upset and pain, nausea, headache, dizziness, somnolence, itching, peripheral edema and hypersensitivity reactions. As with other NSAIDS, meloxicam has potential serious adverse events, including gastrointestinal bleeding, increase risk of cardiovascular thrombotic events, renal dysfunction, heart failure and edema and hypersensitivity reactions.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as meloxicam may have a higher risk of having a heart attack, or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as meloxicam if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take meloxicam right before or right after the surgery.
NSAIDs such as meloxicam may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking meloxicam. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking meloxicam and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to meloxicam. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with meloxicam and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Nabumetone
Nabumetone is a long acting nonsteroidal antiinflammatory drug (NSAID) that is available by prescription only and is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints).
Nabumetone was approved in the United States in 1991 and its current indications are for treatment of chronic arthritis due to osteoarthritis or rheumatoid arthritis. Nabumetone is available by prescription only, and currently more than 4 million prescriptions are filled yearly. Generic formulations are available of 500 and 750 mg; specific commercially available names include Relafen. The usual dose in adults is 1000 mg once daily, increasing to as much as 2000 mg daily based upon response and tolerance. As with other NSAIDs, nabumetone is generally well tolerated, but side effects can included headache, dizziness, somnolence, dyspepsia, nausea, abdominal discomfort, heartburn, peripheral edema and hypersensitivity reactions. Rare but serious adverse events from NSAIDs include gastrointestinal ulceration and bleeding, increased risk for cardiovascular disease, renal dysfunction and hypersensitivity reactions including anaphylaxis, exfoliative dermatitis and Stevens Johnson syndrome.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as nabumetone may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as nabumetone if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take nabumetone right before or right after the surgery.
NSAIDs such as nabumetone may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or who drink large amounts of alcohol while taking nabumetone. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos) selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking nabumetone and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to nabumetone. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with nabumetone and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Naproxen
Naproxen is a popular over-the-counter nonsteroidal antiinflammatory drug (NSAID) that is widely used for therapy of mild-to-moderate pain from headaches, muscle aches, arthritis, menstrual periods, the common cold, toothaches, and backaches. Prescription naproxen is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints), rheumatoid arthritis (arthritis caused by swelling of the lining of the joints), juvenile arthritis (a form of joint disease in children), and ankylosing spondylitis (arthritis that mainly affects the spine). Prescription naproxen tablets, extended-release tablets, and suspension are also used to relieve shoulder pain caused by bursitis (inflammation of a fluid-filled sac in the shoulder joint), tendinitis (inflammation of the tissue that connects muscle to bone), gouty arthritis (attacks of joint pain caused by a build-up of certain substances in the joints), and pain from other causes, including menstrual pain (pain that happens before or during a menstrual period). Naproxen has a longer half-life than other commonly used NSAIDs, making a twice daily regimen feasible.
Naproxen was approved for use by prescription in the United States in 1976 and for over-the-counter use in 1994. Currently more than 10 million prescriptions for naproxen are filled yearly and these numbers do not capture the wide scale over-the-counter sales. Naproxen is indicated for mild-to-moderate pain from various causes including trauma, tendonitis, headache, dysmenorrhea, and various forms of arthritis including osteoarthritis, rheumatoid arthritis, gout and ankylosing spondylitis. Generic and over-the-counter formulations are available as tablets, capsules and oral suspensions in multiple doses (125, 250, 225, 375, 500, 550 mg) under multiple commercial names including: Aleve, Anaprox, Naprosyn, Naxen, Naxodol, Neo-Prox, Nu-Naprox, Nycopren, Proxen, Synflex. Over-the-counter combinations with antihistamines are also available. The typical dose is 250 to 500 mg taken orally twice daily. As with other NSAIDs, naproxen is generally well tolerated, but side effects can include headache, dizziness, somnolence, dyspepsia, nausea, abdominal discomfort, heartburn, peripheral edema and hypersensitivity reactions. Rare but serious adverse events from NSAIDs include gastrointestinal ulceration and bleeding, increased risk for cardiovascular disease, renal dysfunction, exacerbation of asthma and hypersensitivity reactions including anaphylaxis, exfoliative dermatitis and Stevens Johnson syndrome.
People who take nonsteroidal anti-inflammatory drugs (NSAIDs) (other than aspirin) such as naproxen may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. These problems may develop at any time during treatment, but the risk may be higher for people who take NSAIDs for a long time or at higher doses. Do not take an NSAID such as naproxen if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take naproxen right before or right after the surgery.
NSAIDs such as naproxen may cause ulcers, bleeding, or holes in the esophagus (tube between the mouth and stomach), stomach, or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time or at higher doses, are older in age, have poor health, who smoke, or who drink large amounts of alcohol while taking naproxen. Tell your doctor if you take any of the following medications: anticoagulants (”blood thinners”) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and ketoprofen; oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); salicylate pain relievers such as diflunisal, magnesium salicylate (Doan’s, others), and salsalate; selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, other bleeding disorders, or liver disease. If you experience any of the following symptoms, stop taking naproxen and call your doctor: stomach pain, heartburn, vomit that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to naproxen. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with prescription naproxen and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Nimesulide
Nimesulide is a nonsteroidal antiinflammatory drug (NSAID) with relative specificity for COX-2 that is not available in the United States, but has been widely used in many countries of the world since its introduction in the 1990s. Current indications vary by country, but are generally limited to mild-to-moderate acute pain. Nimesulide has a rapid onset of action and has other activities besides its effects of cyclo-oxygenases that may be important in its antiinflammatory and analgesic actions.
Nimesulide recommended dose in adults is 100 mg twice daily for no more than 15 days. Chronic therapy is not generally recommended, and nimesulide is considered contraindicated in children. Nimesulide is available by prescription in the form of capsules or granules for oral suspension of 100 mg and as suppositories of 200 mg in both generic and trade formulations (Sulide, Nimside and others). Nimesulide is generally well tolerated, but side effects can include headache, dizziness, somnolence, gastrointestinal upset, nausea, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions.
Oxaprozin
Oxaprozin is a long acting nonsteroidal antiinflammatory drug (NSAID) available by prescription only which is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Oxaprozin is also used to relieve pain, tenderness, swelling, and stiffness caused by juvenile rheumatoid arthritis in children 6 years of age and older. Because of oxaprozin long half-life, oxaprozin can be given once daily.
Oxaprozin was approved in the United States in 1992 and is still widely used. Oxaprozin is indicated for the treatment of chronic arthritis due to osteoarthritis, rheumatoid arthritis and juvenile rheumatoid arthritis. Oxaprozin is available in capsules of 600 mg in several generic forms and under the brand name Daypro. The recommended dose in adults is 600 to 1200 mg once daily. As with other NSAIDs, oxaprozin is generally well tolerated, but side effects can include headache, dizziness, somnolence, dyspepsia, nausea, abdominal discomfort, heartburn, peripheral edema and hypersensitivity reactions. Rare but serious adverse events from NSAIDs include gastrointestinal ulceration and bleeding, increased risk for cardiovascular disease, renal dysfunction, exacerbation of asthma and hypersensitivity reactions including anaphylaxis, exfoliative dermatitis and Stevens Johnson syndrome.
People who take nonsteroidal anti-inflammatory medications (NSAIDs) (other than aspirin) such as oxaprozin may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as oxaprozin if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take oxaprozin right before or right after the surgery.
NSAIDs such as oxaprozin may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health. or drink large amounts of alcohol while you are taking oxaprozin. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines or other bleeding disorders. If you experience any of the following symptoms, stop taking oxaprozin and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to oxaprozin. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with oxaprozin and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Piroxicam
Piroxicam is a commonly used nonsteroidal antiinflammatory drug (NSAID) that is available by prescription only and is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints).
Piroxicam was approved for use in the United States in 1982 and is still widely used, with several million prescriptions filled yearly. Current indications include rheumatoid arthritis and osteoarthritis. Piroxicam is available as capsules of 10 and 20 mg in several generic forms as well as under brand names such as Feldene, Novo-Pirocam and Nu-Pirox. The recommended dose is 10 to 20 mg orally once daily. Piroxicam is available by prescription only. Other oxicam NSAIDs include meloxicam, tenoxicam, and droxicam, the latter two being available in other countries, but not the United States. As with other NSAIDs, piroxicam is generally well tolerated, but side effects can include headache, dizziness, somnolence, dyspepsia, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions. Rare but serious adverse events from NSAIDs include gastrointestinal ulceration and bleeding, increased risk for cardiovascular disease, renal dysfunction and hypersensitivity reactions including anaphylaxis, exfoliative dermatitis and Stevens Johnson syndrome.
People who take nonsteroidal anti-inflammatory medications (NSAIDs) (other than aspirin) such as piroxicam may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as piroxicam if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take piroxicam right before or right after the surgery.
NSAIDs such as piroxicam may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while you are taking piroxicam. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines or other bleeding disorders. If you experience any of the following symptoms, stop taking piroxicam and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to piroxicam. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with piroxicam and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Sulindac
Sulindac is a commonly used nonsteroidal antiinflammatory drug (NSAID) that is available by prescription only and used predominantly to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints), rheumatoid arthritis (arthritis caused by swelling of the lining of the joints), and ankylosing spondylitis (arthritis that mainly affects the spine). Sulindac also is used to treat pain in the shoulder caused by bursitis (inflammation of a fluid-filled sac in the shoulder joint) and tendinitis (inflammation of the tissue that connects muscle to bone). It is also used to relieve gouty arthritis (attacks of severe joint pain and swelling caused by a build-up of certain substances in the joints). When given chronically, sulindac has also been shown to decrease adenoma formation in persons with familial adenomatous polyposis.
Sulindac was approved for use in chronic arthritis in the United States in 1978 and its indications have been expanded since. Current indications include acute and chronic use for osteoarthritis, rheumatoid arthritis, anklyosing spondylitis, acute gouty arthritis and for acute bursitis. Generic formulations are available (150 and 200 mg) and specific commercial names include Clinoril (100, 150, 200 mg). The recommended dose in adults is 150 to 200 mg twice daily. As with other NSAIDs, sulindac is generally well tolerated, but side effects can include headache, dizziness, somnolence, gastrointestinal upset, nausea, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions. Rare but serious adverse events from NSAIDs include gastrointestinal ulceration and bleeding, increased risk for cardiovascular disease, renal dysfunction and hypersensitivity reactions including anaphylaxis, exfoliative dermatitis and Stevens Johnson syndrome.
People who take nonsteroidal anti-inflammatory medications (NSAIDs) (other than aspirin) such as sulindac may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as sulindac if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke, and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take sulindac right before or right after the surgery.
NSAIDs such as sulindac may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while you are taking sulindac. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as diflunisal, ibuprofen (Advil, Motrin) or naproxen (Aleve, Naprosyn), or oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers or bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking sulindac and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to sulindac. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with sulindac and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Tolmetin
Tolmetin is a nonsteroidal antiinflammatory drug (NSAID) that is available by prescription only and is used to relieve pain, tenderness, swelling, and stiffness caused by osteoarthritis (arthritis caused by a breakdown of the lining of the joints) and rheumatoid arthritis (arthritis caused by swelling of the lining of the joints). Tolmetin is also used to relieve pain, tenderness, swelling, and stiffness caused by juvenile rheumatoid arthritis in children 2 years of age and older.
Tolmetin is one of the oldest NSAIDs in clinical use having been approved in the United States in 1976. Tolmetin is currently not commonly used, having been replaced by NSAIDs with longer half-lives and better tolerance. The current indications for tolmetin include osteoarthritis, rheumatoid arthritis, ankylosing spondylitis and juvenile rheumatoid arthritis. Tolmetin is available only by prescription and in several generic forms of 200, 400 and 600 mg tablets or capsules and formerly under the brand name Tolectin. The usual dose in adults is 1200 to 1800 mg per day in divided doses. As with other NSAIDs, tolmetin is generally well tolerated, but side effects can include headache, dizziness, somnolence, dyspepsia, abdominal discomfort, diarrhea, peripheral edema and hypersensitivity reactions. Rare but serious adverse events from NSAIDs include gastrointestinal ulceration and bleeding, increased risk for cardiovascular disease, renal dysfunction and hypersensitivity reactions including anaphylaxis, exfoliative dermatitis and Stevens Johnson syndrome.
People who take nonsteroidal anti-inflammatory medications (NSAIDs) (other than aspirin) such as tolmetin may have a higher risk of having a heart attack or a stroke than people who do not take these medications. These events may happen without warning and may cause death. This risk may be higher for people who take NSAIDs for a long time. Do not take an NSAID such as tolmetin if you have recently had a heart attack, unless directed to do so by your doctor. Tell your doctor if you or anyone in your family has or has ever had heart disease, a heart attack, or a stroke, if you smoke,and if you have or have ever had high cholesterol, high blood pressure, or diabetes. Get emergency medical help right away if you experience any of the following symptoms: chest pain, shortness of breath, weakness in one part or side of the body, or slurred speech.
If you will be undergoing a coronary artery bypass graft (CABG; a type of heart surgery), you should not take tolmetin right before or right after the surgery.
NSAIDs such as tolmetin may cause ulcers, bleeding, or holes in the stomach or intestine. These problems may develop at any time during treatment, may happen without warning symptoms, and may cause death. The risk may be higher for people who take NSAIDs for a long time, are older in age, have poor health, or drink large amounts of alcohol while taking tolmetin. Tell your doctor if you take any of the following medications: anticoagulants (‘blood thinners’) such as warfarin (Coumadin, Jantoven); aspirin; other NSAIDs such as ibuprofen (Advil, Motrin) and naproxen (Aleve, Naprosyn); oral steroids such as dexamethasone, methylprednisolone (Medrol), and prednisone (Rayos); selective serotonin reuptake inhibitors (SSRIs) such as citalopram (Celexa), fluoxetine (Prozac, Sarafem, Selfemra, in Symbyax), fluvoxamine (Luvox), paroxetine (Brisdelle, Paxil, Pexeva), and sertraline (Zoloft); or serotonin norepinephrine reuptake inhibitors (SNRIs) such as desvenlafaxine (Khedezla, Pristiq), duloxetine (Cymbalta), and venlafaxine (Effexor XR). Also tell your doctor if you have or have ever had ulcers, bleeding in your stomach or intestines, or other bleeding disorders. If you experience any of the following symptoms, stop taking tolmetin and call your doctor: stomach pain, heartburn, vomiting a substance that is bloody or looks like coffee grounds, blood in the stool, or black and tarry stools.
Keep all appointments with your doctor and the laboratory. Your doctor will monitor your symptoms carefully and will probably order certain tests to check your body’s response to tolmetin. Be sure to tell your doctor how you are feeling so that your doctor can prescribe the right amount of medication to treat your condition with the lowest risk of serious side effects.
Your doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with tolmetin and each time you refill your prescription. Read the information carefully and ask your doctor or pharmacist if you have any questions.
Nonsteroidal anti inflammatory drugs side effects
All nonsteroidal anti-inflammatory drugs (NSAIDs) have well-known side effects that include stomach problems (such as bleeding, ulcer, and stomach upset), kidney problems, liver problems, high blood pressure or heart problems, fluid retention, rashes, or allergic reactions and other adverse reactions. DO NOT give aspirin to children under age 12. Teens with a virus should also avoid drugs containing aspirin. Children should NOT take aspirin because it has been linked to a rare but serious condition called Reye’s syndrome, a rare but deadly illness that can affect the brain and liver.
- Stomach adverse effects such as gastric ulceration, bleeding, or perforation are likely due to the inhibition of COX-1, preventing the creation of prostaglandins that protect the gastric mucosa. The damage is more likely in a patient that has a prior history of peptic ulcers and present more commonly in the elderly 72, 54. Other undesirable gastrointestinal side effects may include nausea, dyspepsia, loss of appetite, abdominal pain, and diarrhea from erosion of the alimentary canal. Since gastrointestinal (GI) adverse effects is COX-1 specific, the use of COX-2 selective NSAIDs (e.g., celecoxib) is a lower-risk alternative 73. Multiple studies have revealed that COX-2 inhibitors, such as lumiracoxib, celecoxib, and rofecoxib, caused less damage to gastrointestinal mucosa compared to non-selective NSAIDs 74, 75, 76. Rhame et al. 77 found that celecoxib has superior gastrointestinal safety profile, compared with non-selective NSAIDs. However, there are increase risks of cardiovascular adverse effects with the use of COX-2 inhibitors 78, 79, 80, 81. Therefore, tailoring a patient’s gastrointestinal risk factors versus cardiovascular risk factors is necessary to determine the choice of gastrointestinal protection options for patients on chronic NSAIDs 82. NSAIDs-induced gastroduodenal ulcers can be prevented by the use of gastrointestinal protective agents, such as, Misoprostol, H2-receptor antagonists (H2RA) or proton pump inhibitors (PPIs) 82.
- Cardiovascular adverse effects can also be increased with NSAID use; these include heart attack (myocardial infarction), thromboembolic events (umbrella term for a blood clot [a thrombus] that dislodges to travel in the blood [an embolus] e.g., deep vein thrombosis [DVT] and pulmonary embolism [PE]), and atrial fibrillation 77, 78, 79, 80, 81. In general, NSAIDs can increase blood pressure by 5 mmHg in average. The mechanism of NSAIDs promoting hypertension is hypothesized to be related to the inhibition of prostaglandin synthesis, which leads to an interference of renal vasculature which manipulates the regulation of blood pressure. In addition, NSAIDs themselves can cause elevation of serum aldosterone, leading to sodium retention and hypertension 83. Diclofenac seems to be the NSAID with the highest reported increase in adverse cardiovascular events 84. Historically, much attention had been drawn to the increased incidence of heart attack (myocardial infarction) and stroke, particularly with the selective COX-2 inhibitor rofecoxib, which was removed from the market in 2004 37. Since then, similar inquiries regarding the cardiovascular safety of the remaining selective COX-2 inhibitor, celecoxib, and non-selective NSAIDs have been investigated. A 2016 study, known as the PRECISION (Prospective Randomized Evaluation of Celecoxib Integrated Safety versus Ibuprofen or Naproxen) trial, provided strong evidence that celecoxib is not associated with a higher rate of cardiovascular events compared to non-selective drugs 37. However, widely recognized adverse effects include blood pressure elevation and potentiation or exacerbation of congestive heart failure, through inhibition of natural prostanoid-induced salt excretion and changes in renal arteriolar tone. Such risks tend to be dose and duration dependent. Ultimately, it is important to establish that the risk of unfavorable cardiovascular events associated with NSAID use is further increased with tobacco use, alcohol consumption, and generally unhealthy habits 37.
- Kidney adverse effects because COX-1 and COX-2 facilitate the production of prostaglandins that play a role in kidney hemodynamics. In a patient with normal kidney function, inhibition of prostaglandin synthesis does not pose a large problem; however, in a patient with renal dysfunction (e.g., chronic kidney disease [CKD]), these prostaglandins play a greater role and can be the source of problems when reduced via NSAIDs. The American Geriatric Society recommends that all NSAIDs should be avoided in patients with stage 4 and 5 chronic kidney disease [CKD] (creatinine clearance less than 30 mL/min) 85, 86. Complications that can occur include fluid and electrolyte disorders such as hyperkalemia, reduce glomerular filtration rate, acute renal failure, nephrotic syndrome related to drug induced minimal change disease, chronic kidney disease, acute interstitial nephritis, sodium retention, edema, and renal papillary necrosis 84, 87.
- Liver adverse effects (raised aminotransferase levels) is not very common, and liver-related hospitalization is very rare. Among the various NSAIDs, Diclofenac has a higher rate of hepatotoxic effects 88.
- Hematologic adverse effects are possible, particularly with nonselective NSAIDs due to their antiplatelet activity. This antiplatelet effect typically only poses a problem if the patient has a history of gastrointestinal ulcers, diseases that impair platelet activity (hemophilia, thrombocytopenia, von Willebrand disease, etc.), and in some perioperative cases 89.
- Minor adverse effects include anaphylactoid reactions that involve the skin and pulmonary systems, like urticaria and aspirin-exacerbated respiratory disease 90, 91.
Table 2. Nonsteroidal anti-inflammatory drugs common adverse effects
| Gastrointestinal toxicity |
|
|---|---|
| Cardiovascular adverse effects |
|
| Kidney toxicity |
|
Drug Interactions
If you use 2 or more medicines at the same time, the way your body processes each one can change. As a result of their pharmacokinetics, NSAIDs may interact with other high plasma protein-bound drugs, displacing them and leading to an increase in the free serum concentration of these drugs. When this happens, the risk of side effects from each one increases. Each medicine may not work the way it should. This is called a drug-drug interaction. For example, NSAIDs thin the blood. If you take a blood thinning medicine such as warfarin and you take an NSAID, there could be a drug-drug interaction. Additionally, NSAIDs may increase the toxicity of drugs that are dependent on renal clearance (such as lithium) or hepatic metabolism because some NSAIDs reduce renal perfusion and inhibit cytochrome P450 (CYP) enzymes or glucuronidation.
Two NSAIDs or an NSAID and COX-2 should not be combined. A prescription NSAID or COX-2 should also not be taken with an OTC NSAID. You should be especially careful not to add an NSAID or COX-2 if you already take aspirin.
Other notable drug interactions occur during concurrent use of NSAIDs and antihypertensives, anticoagulants and antiplatelets, selective serotonin receptor inhibitors (SSRIs), and substances that injure gastrointestinal mucosa. The effects of many antihypertensives are diminished due to the ability of NSAIDs to reduce natriuresis. Besides decreased efficacy, specific use of NSAIDs with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers may exacerbate potassium retention, known to have significant cardiac consequences. Simultaneous use of NSAIDs and anticoagulants or antiplatelets can result in an increased risk of bleeding due to reduced platelet aggregation. Bleeding risk is also similarly increased with concomitant use of SSRIs (selective serotonin receptor inhibitors) and NSAIDs, as serotonin is one of many substances taken up by and released from platelets to stimulate aggregation and hemostasis. Lastly, the risk of peptic ulcer disease or a gastrointestinal bleed is markedly increased when NSAIDs are ingested in combination with alcohol or glucocorticoids which inhibit the activation of the arachidonic acid precursor phospholipase A2 73, 32, 92, 93, 94.
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking any of these medicines, it is especially important that your healthcare professional know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Table 3. Drug interaction of nonsteroidal anti-inflammatory drugs and commonly used medications
| Medication | Interactions |
|---|---|
| Antiplatelets (aspirin, clopidogrel) | Increases risk of gastrointestinal bleeding |
| Angiotensin-converting-enzyme inhibitor (ACEI) and Angiotensin Receptor Blockers (ARB) | Increases in blood pressure by attenuating antihypertensive effects |
| Beta blockers | Increases in blood pressure by attenuating antihypertensive effects |
| Calcium antagonists | Increases in blood pressure by attenuating antihypertensive effects |
| Corticosteroids | Increases risk of gastrointestinal bleeding |
| Digitalis glycosides | Increase serum digoxin level |
| Diuretics | Increases in blood pressure by attenuating antihypertensive effects |
| Methotrexate | NSAIDs reduce renal excretion of methotrexate, causing methotrexate toxicity. |
| Selective serotonin reuptake inhibitors (SSRIs) | Increases risk of gastrointestinal bleeding |
| Warfarin and other anticoagulants | Increases risk of gastrointestinal bleeding |
Using nonsteroidal anti inflammatory drugs (NSAIDs) with any of the following medicines is not recommended. Your doctor may decide not to treat you with a medication in this class or change some of the other medicines you take:
- Aceclofenac
- Acemetacin
- Amtolmetin Guacil
- Aspirin
- Bromfenac
- Bufexamac
- Celecoxib
- Choline Salicylate
- Clonixin
- Dexibuprofen
- Dexketoprofen
- Diclofenac
- Diflunisal
- Dipyrone
- Droxicam
- Etodolac
- Etofenamate
- Etoricoxib
- Felbinac
- Fenoprofen
- Fepradinol
- Feprazone
- Floctafenine
- Flufenamic Acid
- Flurbiprofen
- Ibuprofen
- Indomethacin
- Ketoprofen
- Lornoxicam
- Loxoprofen
- Lumiracoxib
- Meclofenamate
- Mefenamic Acid
- Meloxicam
- Morniflumate
- Nabumetone
- Naproxen
- Nepafenac
- Niflumic Acid
- Nimesulide
- Nimesulide Beta Cyclodextrin
- Oxaprozin
- Oxyphenbutazone
- Parecoxib
- Pentoxifylline
- Phenylbutazone
- Piketoprofen
- Piroxicam
- Proglumetacin
- Propyphenazone
- Proquazone
- Rofecoxib
- Salicylic Acid
- Salsalate
- Sodium Salicylate
- Sulfasalazine
- Sulindac
- Tenoxicam
- Tiaprofenic Acid
- Tolfenamic Acid
- Tolmetin
- Valdecoxib
Using nonsteroidal anti inflammatory drugs (NSAIDs) with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines:
- Abciximab
- Acenocoumarol
- Anagrelide
- Apixaban
- Ardeparin
- Argatroban
- Bemiparin
- Bivalirudin
- Budesonide
- Cangrelor
- Certoparin
- Cilostazol
- Ciprofloxacin
- Citalopram
- Clopidogrel
- Dabigatran Etexilate
- Dalteparin
- Danaparoid
- Deflazacort
- Desirudin
- Desvenlafaxine
- Dexamethasone
- Dipyridamole
- Duloxetine
- Edoxaban
- Emtricitabine
- Enoxaparin
- Epoprostenol
- Eptifibatide
- Escitalopram
- Feverfew
- Fluoxetine
- Fluvoxamine
- Fondaparinux
- Ginkgo
- Heparin
- Hydrocortisone
- Iloprost
- Lepirudin
- Levomilnacipran
- Meadowsweet
- Melphalan
- Methotrexate
- Methylprednisolone
- Milnacipran
- Nadroparin
- Nefazodone
- Parnaparin
- Paroxetine
- Phenindione
- Phenprocoumon
- Prasugrel
- Prednisolone
- Prednisone
- Protein C
- Reviparin
- Rivaroxaban
- Selexipag
- Sertraline
- Sibutramine
- Sulfinpyrazone
- Sulodexide
- Tenofovir Alafenamide
- Ticagrelor
- Ticlopidine
- Tinzaparin
- Tirofiban
- Treprostinil
- Venlafaxine
- Vilazodone
- Vorapaxar
- Vortioxetine
- Warfarin
Other Medical Problems
The presence of other medical problems may affect the use of nonsteroidal anti inflammatory drugs. Make sure you tell your doctor if you have any other medical problems, especially:
- Hemophilia or other bleeding problems. The possibility of bleeding may be increased.
- Viral eye infection (epithelial herpes simplex keratitis), or a history of having a viral eye infection. It is possible that a current infection could be made worse or an old infection could return.
- Use of soft contact lenses. Eye irritation, such as redness and burning of the eyes, may occur.
Nonsteroidal anti-inflammatory drugs overdose
There are NSAIDs in many over-the-counter medicines, not just in pain medicines, so you need to read medication labels carefully. There are many brand names for the same medicine and many different types of NSAID available, so you need to take care to avoid an accidental overdose. If you’re unsure, ask your doctor or pharmacist.
You may find NSAIDs in:
- medications for colds and flu
- arthritis creams
- teething gels
- complementary and alternative medicines such as:
- willow tree bark extract
- herbal arthritis pills
You need to be careful not to overdose on NSAIDs by accident. For example if you have a cold, don’t take one NSAID for headache and another NSAID at the same time in a medicine for a stuffy nose. If you take an NSAID for a chronic (long-term) condition such as arthritis, ask your doctor or pharmacist before taking cold and flu medicines.
Stop taking NSAIDs and see your doctor if you notice anything wrong, especially any signs of stomach bleeding, such as:
- abdominal pain
- blood in your stool (poop), or very dark stool
- dark coffee-colored vomit
Nonsteroidal anti-inflammatory drugs overdose can manifest as gastrointestinal bleeding, high blood pressure (hypertension), liver damage and renal damage 30. Typically, acute NSAID overdose is asymptomatic or has negligible gastrointestinal symptoms. However, other symptoms of NSAID overdose complications may include anion gap metabolic acidosis, coma, convulsions, and acute renal failure. Also, NSAIDs can cause gastrointestinal damage by inhibiting COX-1, which causes decrease gastric mucosa production. Kidney damage can also occur with NSAID use because these medications reduce prostaglandin levels, which are essential for the widening of the renal arterioles. Lastly, neurologic toxicity can present with drowsiness, confusion, nystagmus, blurred vision, diplopia, headache, and tinnitus 95.
Nonsteroidal anti inflammatory drugs special precautions
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to nonsteroidal anti inflammatory drugs (NSAIDs) or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Pregnancy
FDA is warning that use of NSAIDs around 20 weeks or later in pregnancy may cause rare but serious kidney problems in an unborn baby. This can lead to low levels of amniotic fluid surrounding the baby and possible complications.
For prescription NSAIDs, FDA is requiring changes to the prescribing information to describe the risk of kidney problems in unborn babies that result in low amniotic fluid.
For over-the-counter (OTC) NSAIDs intended for use in adults, FDA will also update the Drug Facts labels, available at: http://bit.ly/2Uadlbz. These labels already warn to avoid using NSAIDs during the last 3 months of pregnancy because the medicines may cause problems in the unborn child or complications during delivery. The Drug Facts labels already advise pregnant and breastfeeding women to ask a health care professional before using these medicines.
Nonsteroidal anti-inflammatory drugs (NSAIDs)
- are a class of medicines available by prescription and OTC. They are some of the most commonly used medicines for pain and fever.
- are used to treat medical conditions such as arthritis, menstrual cramps, headaches, colds, and the flu.
- work by blocking the production of certain chemicals in the body that cause inflammation.
- are available alone and combined with other medicines. Examples of NSAIDs include aspirin, ibuprofen, naproxen, diclofenac, and celecoxib.
Common side effects of NSAIDs include: stomach pain, constipation, diarrhea, gas, heartburn, nausea, vomiting, and dizziness.
RECOMMENDATION:
Consumers/Patients
- If you are pregnant, do not use NSAIDs at 20 weeks or later in pregnancy unless specifically advised to do so by your health care professional because these medicines may cause problems in your unborn baby.
- Many OTC medicines contain NSAIDs, including those used for pain, colds, flu, and insomnia, so it is important to read the Drug Facts labels, to find out if the medicines contain NSAIDs.
- Talk to your health care professional or pharmacist if you have questions or concerns about NSAIDs or which medicines contain them.
- Other medicines, such as acetaminophen, are available to treat pain and fever during pregnancy. Talk to your pharmacist or health care professional for help deciding which might be best.
Health Care Professionals
- FDA recommends that health care professionals should limit prescribing NSAIDs between 20 to 30 weeks of pregnancy and avoid prescribing them after 30 weeks of pregnancy. If NSAID treatment is determined necessary, limit use to the lowest effective dose and shortest duration possible. Consider ultrasound monitoring of amniotic fluid if NSAID treatment extends beyond 48 hours and discontinue the NSAID if oligohydramnios is found. FDA is warning that use of NSAIDs around 20 weeks gestation or later in pregnancy may cause fetal renal dysfunction leading to oligohydramnios and, in some cases, neonatal renal impairment.
- These adverse outcomes are seen, on average, after days to weeks of treatment, although oligohydramnios has been infrequently reported as soon as 48 hours after NSAID initiation.
- Oligohydramnios is often, but not always, reversible with treatment discontinuation.
- Complications of prolonged oligohydramnios may include limb contractures and delayed lung maturation. In some postmarketing cases of impaired neonatal renal function, invasive procedures such as exchange transfusion or dialysis were required.
- If NSAID treatment is deemed necessary between 20 to 30 weeks of pregnancy, limit use to the lowest effective dose and shortest duration possible. As currently described in the NSAID labels, avoid prescribing NSAIDs at 30 weeks and later in pregnancy because of the additional risk of premature closure of the fetal ductus arteriosus.
- The above recommendations do not apply to low-dose 81 mg aspirin prescribed for certain conditions in pregnancy.
- Consider ultrasound monitoring of amniotic fluid if NSAID treatment extends beyond 48 hours. Discontinue the NSAID if oligohydramnios occurs and follow up according to clinical practice.
Breastfeeding
Diclofenac, indomethacin, and suprofen pass into the breast milk when they are are taken by mouth. It is not known whether flurbiprofen passes into the breast milk when it is taken by mouth. However, these medicines have not been shown to cause problems in nursing babies.
Children
Nonsteroidal anti inflammatory drugs have been studied only in adults, and there is no specific information about their use in children.
Elderly
Nonsteroidal anti inflammatory drugs have been tested and have not been shown to cause different side effects or problems in older people than they do in younger adults.
Drug-food interaction
Certain foods or drinks can also prevent your medicine from working the way it should. Or they can make side effects worse. This is called a drug-food interaction. For example, if you’re taking a traditional NSAID, drinking alcohol can increase your risk of liver disease or stomach bleeding.
Best nonsteroidal anti inflammatory drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) are drugs commonly used to treat mild-to-moderate pain, inflammation (swelling and redness) and fever. Examples include the nonprescription NSAID medications ibuprofen (Advil, Motrin IB, others) and naproxen (Aleve, Anaprox DS, others). NSAIDs available by prescription include diclofenac sodium (Voltaren and Solaraze) and celecoxib (Celebrex).
NSAIDs are helpful to:
- Reduce fever
- Relieve menstrual cramps
- Relieve pain caused by muscle aches and stiffness
- Reduce and ease pain from inflammation (swelling), such as with muscle sprains
If you take NSAIDs you increase your risk of developing severe bleeding in your stomach. Research also shown that taking NSAIDs can raise your risk of heart attacks and strokes. This increase in risk affects people who already have heart disease and those who don’t. These risks get worse if you take higher doses. It also gets worse if you take these medicines for a long period of time. If you need to take pain medicine for longer than a week, you should discuss this risk with your doctor. You may want to explore other pain treatment options. To keep your risk of heart attack or stroke low, if you use NSAIDs, take the smallest dose possible for the shortest amount of time necessary to relieve your symptoms. Your doctor will help you decide how to control your pain and inflammation.
NSAIDs are generally safe for most people to take once in a while. But be aware that serious side effects can occur as early as the first weeks of daily NSAID use. The risk can increase the longer it’s taken.
The type and amount of nonsteroidal anti-inflammatory drugs you need varies. It will depend on your overall health and what kind of problem you have. Some nonsteroidal anti-inflammatory drugs may interact with other medicines. Talk to your doctor about what medicines you take regularly before starting a new pain medicine.
Common side effects of NSAIDs may include:
- Dizziness
- Headache
- Nausea
- Diarrhea
- Excess gas
- Constipation
- Extreme weakness or fatigue
- Dry mouth
Serious, but rare, side effects of NSAIDs may include:
- Allergic reaction (difficulty breathing, hives, and swelling of the lips, tongue, or face)
- Muscle cramps, numbness, or tingling
- Rapid weight gain
- Black, bloody, or tarry stools
- Bloody urine or bloody vomit
- Decreased hearing or ringing in the ears (also called tinnitus)
- Jaundice (the yellowing of the skin and the whites of the eyes)
- Abdominal cramping
- Heartburn
- Indigestion
In addition to the side effects listed above, people taking a COX-2 inhibitor may be at risk for:
- Swelling or water retention
- Skin rash or itching
- Unusual bruising or bleeding
- Difficulty sleeping (insomnia)
Call your doctor as soon as possible if your side effects become severe.
- Ghlichloo I, Gerriets V. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547742[↩]
- Phillips WJ, Currier BL. Analgesic pharmacology: II. Specific analgesics. J Am Acad Orthop Surg. 2004 Jul-Aug;12(4):221-33. doi: 10.5435/00124635-200407000-00003[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Nonsteroidal Antiinflammatory Drugs (NSAIDs) [Updated 2020 Mar 18]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548614[↩][↩]
- Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol. 2006 Aug;108(2):428-41. doi: 10.1097/01.AOG.0000230214.26638.0c[↩]
- Shekelle PG, Newberry SJ, FitzGerald JD, Motala A, O’Hanlon CE, Tariq A, Okunogbe A, Han D, Shanman R. Management of Gout: A Systematic Review in Support of an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2017 Jan 3;166(1):37-51. doi: 10.7326/M16-0461[↩]
- Oyler DR, Parli SE, Bernard AC, Chang PK, Procter LD, Harned ME. Nonopioid management of acute pain associated with trauma: Focus on pharmacologic options. J Trauma Acute Care Surg. 2015 Sep;79(3):475-83. doi: 10.1097/TA.0000000000000755[↩]
- Zacher J, Altman R, Bellamy N, Brühlmann P, Da Silva J, Huskisson E, Taylor RS. Topical diclofenac and its role in pain and inflammation: an evidence-based review. Curr Med Res Opin. 2008 Apr;24(4):925-50. doi: 10.1185/030079908×273066[↩]
- van den Bekerom MPJ, Sjer A, Somford MP, Bulstra GH, Struijs PAA, Kerkhoffs GMMJ. Non-steroidal anti-inflammatory drugs (NSAIDs) for treating acute ankle sprains in adults: benefits outweigh adverse events. Knee Surg Sports Traumatol Arthrosc. 2015 Aug;23(8):2390-2399. doi: 10.1007/s00167-014-2851-6[↩]
- May JJ, Lovell G, Hopkins WG. Effectiveness of 1% diclofenac gel in the treatment of wrist extensor tenosynovitis in long distance kayakers. J Sci Med Sport. 2007 Feb;10(1):59-65. doi: 10.1016/j.jsams.2006.05.009[↩]
- Barkin RL. Topical Nonsteroidal Anti-Inflammatory Drugs: The Importance of Drug, Delivery, and Therapeutic Outcome. Am J Ther. 2015 Sep-Oct;22(5):388-407. doi: 10.1097/MJT.0b013e3182459abd[↩][↩]
- Verbeeck RK, Blackburn JL, Loewen GR. Clinical pharmacokinetics of non-steroidal anti-inflammatory drugs. Clin Pharmacokinet. 1983 Jul-Aug;8(4):297-331. doi: 10.2165/00003088-198308040-00003[↩]
- Gong L, Thorn CF, Bertagnolli MM, Grosser T, Altman RB, Klein TE. Celecoxib pathways: pharmacokinetics and pharmacodynamics. Pharmacogenet Genomics. 2012 Apr;22(4):310-8. doi: 10.1097/FPC.0b013e32834f94cb[↩]
- Ricciotti E, FitzGerald GA. Prostaglandins and inflammation. Arterioscler Thromb Vasc Biol. 2011 May;31(5):986-1000. doi: 10.1161/ATVBAHA.110.207449[↩][↩][↩]
- Cardet JC, Akin C, Lee MJ. Mastocytosis: update on pharmacotherapy and future directions. Expert Opin Pharmacother. 2013 Oct;14(15):2033-45. doi: 10.1517/14656566.2013.824424[↩]
- Harris RE, Chlebowski RT, Jackson RD, Frid DJ, Ascenseo JL, Anderson G, Loar A, Rodabough RJ, White E, McTiernan A; Women’s Health Initiative. Breast cancer and nonsteroidal anti-inflammatory drugs: prospective results from the Women’s Health Initiative. Cancer Res. 2003 Sep 15;63(18):6096-101.[↩]
- Kim S., Shore D. L., Wilson L. E, et al. Lifetime use of nonsteroidal anti-inflammatory drugs and breast cancer risk: results from a prospective study of women with a sister with breast cancer. BMC Cancer. 2015;15(1):p. 960. doi: 10.1186/s12885-015-1979-1[↩]
- Dierssen-Sotos T., Gómez-Acebo I., de Pedro M, et al. Use of non-steroidal anti-inflammatory drugs and risk of breast cancer: the Spanish Multi-Case-control (MCC) study. BMC Cancer. 2016;16(1):p. 660. doi: 10.1186/s12885-016-2692-4[↩]
- Vidal A. C., Howard L. E., Moreira D. M., Castro-Santamaria R., Andriole G. L., Freedland S. J. Aspirin, NSAIDs, and risk of prostate cancer: results from the REDUCE study. Clinical Cancer Research. 2014;21(4):756–762. doi: 10.1158/1078-0432.CCR-14-2235[↩]
- Doat S., Cénée S., Trétarre B., et al. Nonsteroidal anti-inflammatory drugs (NSAIDs) and prostate cancer risk: results from the EPICAP study. Cancer Medicine. 2017;6(10):2461–2470. doi: 10.1002/cam4.1186[↩]
- Ruder E. H., Laiyemo A. O., Graubard B. I., Hollenbeck A. R., Schatzkin A., Cross A. J. Non-steroidal anti-inflammatory drugs and colorectal cancer risk in a large, prospective cohort. American Journal of Gastroenterology. 2011;106(7):1340–1350. doi: 10.1038/ajg.2011.38[↩]
- Friis S., Riis A. H., Erichsen R., Baron J. A., Sørensen H. T. Low-dose aspirin or nonsteroidal anti-inflammatory drug use and colorectal cancer risk. Annals of Internal Medicine. 2015;163(5):347–355. doi: 10.7326/M15-0039[↩]
- Trabert B., Ness R. B., Lo-Ciganic W.-H., et al. Asppirin, nonaspirin nonsteroidal anti-inflammatory drug, and acetaminophen use and risk of invasive epithelial ovarian cancer: a pooled analysis in the ovarian cancer association consortium. JNCI Journal of the National Cancer Institute. 2014;106(2):p. djt431. doi: 10.1093/jnci/djt431[↩]
- Shi J., Leng W., Zhao L, et al. Nonsteroidal anti-inflammatory drugs using and risk of head and neck cancer: a dose–response meta-analysis of prospective cohort studies. Oncotarget. 2017;8(58):99066–99074. doi: 10.18632/oncotarget.21524[↩]
- Thun M. J., Henley S. J., Patrono C. Nonsteroidal anti-inflammatory drugs as anticancer agents: mechanistic, pharmacologic, and clinical issues. JNCI Journal of the National Cancer Institute. 2002;94(4):252–266. doi: 10.1093/jnci/94.4.252[↩]
- Rakoff-Nahoum S. Why cancer and inflammation? Yale J Biol Med. 2006 Dec;79(3-4):123-30. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1994795[↩]
- Prizment A. E., Folsom A. R., Anderson K. E. Nonsteroidal anti-inflammatory drugs and risk for ovarian and endometrial cancers in the Iowa women’s health study. Cancer Epidemiology Biomarkers & Prevention. 2010;19(2):435–442. doi: 10.1158/1055-9965.EPI-09-0976[↩]
- Singh G, Triadafilopoulos G. Epidemiology of NSAID induced gastrointestinal complications. J Rheumatol Suppl. 1999 Apr;56:18-24.[↩]
- Davis JS, Lee HY, Kim J, Advani SM, Peng HL, Banfield E, Hawk ET, Chang S, Frazier-Wood AC. Use of non-steroidal anti-inflammatory drugs in US adults: changes over time and by demographic. Open Heart. 2017 Apr 28;4(1):e000550. doi: 10.1136/openhrt-2016-000550[↩]
- Pirmohamed M, James S, Meakin S, Green C, Scott AK, Walley TJ, Farrar K, Park BK, Breckenridge AM. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ. 2004 Jul 3;329(7456):15-9. doi: 10.1136/bmj.329.7456.15[↩]
- Rothenberg RJ, Holcomb JP Jr. Guidelines for Monitoring of NSAIDS: Who Listened? J Clin Rheumatol. 2000 Oct;6(5):258-65. doi: 10.1097/00124743-200010000-00005[↩][↩]
- Smith W. L., DeWitt D. L., Garavito R. M. Cyclooxygenases: structural, cellular, and molecular biology. Annual Review of Biochemistry. 2000;69(1):145–182. doi: 10.1146/annurev.biochem.69.1.145[↩]
- Varga Z, Sabzwari SRA, Vargova V. Cardiovascular Risk of Nonsteroidal Anti-Inflammatory Drugs: An Under-Recognized Public Health Issue. Cureus. 2017 Apr 8;9(4):e1144. doi: 10.7759/cureus.1144[↩][↩]
- Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nat New Biol. 1971 Jun 23;231(25):232-5. doi: 10.1038/newbio231232a0[↩]
- Vane JR, Botting RM. Mechanism of action of nonsteroidal anti-inflammatory drugs. Am J Med. 1998 Mar 30;104(3A):2S-8S; discussion 21S-22S. doi: 10.1016/s0002-9343(97)00203-9[↩]
- Cashman JN. The mechanisms of action of NSAIDs in analgesia. Drugs. 1996;52 Suppl 5:13-23. doi: 10.2165/00003495-199600525-00004[↩]
- Rainsford KD. Anti-inflammatory drugs in the 21st century. Subcell Biochem. 2007;42:3-27. doi: 10.1007/1-4020-5688-5_1[↩]
- Saad J, Mathew D. Nonsteroidal Anti-Inflammatory Drugs Toxicity. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526006[↩][↩][↩][↩]
- Morita I. Distinct functions of COX-1 and COX-2. Prostaglandins Other Lipid Mediat. 2002 Aug;68-69:165-75. doi: 10.1016/s0090-6980(02)00029-1[↩]
- Adelizzi RA. COX-1 and COX-2 in health and disease. J Am Osteopath Assoc. 1999 Nov;99(11 Suppl):S7-12.[↩]
- Chaiamnuay S, Allison JJ, Curtis JR. Risks versus benefits of cyclooxygenase-2-selective nonsteroidal antiinflammatory drugs. Am J Health Syst Pharm. 2006 Oct 1;63(19):1837-51. doi: 10.2146/ajhp050519[↩]
- Nathan C. Points of control in inflammation. Nature. 2002 Dec 19-26;420(6917):846-52. doi: 10.1038/nature01320[↩]
- Funk C. D. Prostaglandins and leukotrienes: advances in eicosanoid biology. Science. 2001;294(5548):1871–1875. doi: 10.1126/science.294.5548.1871[↩]
- Dorris S. L., Peebles R. S. PGI2 as a regulator of inflammatory diseases. Mediators of Inflammation. 2012;2012:9. doi: 10.1155/2012/926968.926968[↩]
- Ricciotti E., FitzGerald G. A. Prostaglandins and inflammation. Arteriosclerosis, Thrombosis, and Vascular Biology. 2011;31(5):986–1000. doi: 10.1161/atvbaha.110.207449[↩]
- Lewis RA, Soter NA, Diamond PT, Austen KF, Oates JA, Roberts LJ 2nd. Prostaglandin D2 generation after activation of rat and human mast cells with anti-IgE. J Immunol. 1982 Oct;129(4):1627-31.[↩]
- Basu S., Whiteman M., Mattey D. L., Halliwell B. Raised levels of F2-isoprostanes and prostaglandin F2alpha in different rheumatic diseases. Annals of the Rheumatic Diseases. 2001;60:627–631. doi: 10.1136/ard.60.6.627[↩]
- Nakahata N. Thromboxane A2: physiology/pathophysiology, cellular signal transduction and pharmacology. Pharmacology & Therapeutics. 2008;118(1):18–35. doi: 10.1016/j.pharmthera.2008.01.001[↩]
- Wong RSY. Role of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) in Cancer Prevention and Cancer Promotion. Adv Pharmacol Sci. 2019 Jan 31;2019:3418975. doi: 10.1155/2019/3418975[↩]
- World Health Organization. Traitement de la douleur cancéreuse. Geneva, Switz: World Health Organization; 1987.[↩]
- Ventafridda V, Saita L, Ripamonti C, De Conno F. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React. 1985;7(1):93-6.[↩]
- Orhan ME, Bilgin F, Ergin A, Dere K, Güzeldemir ME. Kanser hastalarinda WHO analjezik basamak tedavisine göre ağri tedavisi. Bir merkezin sekiz yillik deneyimi [Pain treatment practice according to the WHO analgesic ladder in cancer patients: eight years experience of a single center]. Agri. 2008 Oct;20(4):37-43. Turkish.[↩]
- Jadad AR, Browman GP. The WHO Analgesic Ladder for Cancer Pain Management: Stepping Up the Quality of Its Evaluation. JAMA. 1995;274(23):1870–1873. doi:10.1001/jama.1995.03530230056031[↩]
- Balding L. The World Health Organisation analgesic ladder: its place in modern Irish medical practice. Ir Med J. 2013 Apr;106(4):122-4.[↩]
- Abdulla A, Adams N, Bone M, Elliott AM, Gaffin J, Jones D, Knaggs R, Martin D, Sampson L, Schofield P; British Geriatric Society. Guidance on the management of pain in older people. Age Ageing. 2013 Mar;42 Suppl 1:i1-57. doi: 10.1093/ageing/afs200[↩][↩][↩]
- Malec M, Shega JW. Pain management in the elderly. Med Clin North Am. 2015 Mar;99(2):337-50. doi: 10.1016/j.mcna.2014.11.007[↩]
- Gnjidic D, Blyth FM, Le Couteur DG, Cumming RG, McLachlan AJ, Handelsman DJ, Seibel M, Waite L, Naganathan V. Nonsteroidal anti-inflammatory drugs (NSAIDs) in older people: prescribing patterns according to pain prevalence and adherence to clinical guidelines. Pain. 2014 Sep;155(9):1814-1820. doi: 10.1016/j.pain.2014.06.009[↩]
- Meara AS, Simon LS. Advice from professional societies: appropriate use of NSAIDs. Pain Med. 2013 Dec;14 Suppl 1:S3-10. doi: 10.1111/pme.12282[↩]
- Ussai S, Miceli L, Pisa FE, Bednarova R, Giordano A, Della Rocca G, Petelin R. Impact of potential inappropriate NSAIDs use in chronic pain. Drug Des Devel Ther. 2015 Apr 9;9:2073-7. doi: 10.2147/DDDT.S80686[↩][↩]
- Ungprasert P, Cheungpasitporn W, Crowson CS, Matteson EL. Individual non-steroidal anti-inflammatory drugs and risk of acute kidney injury: A systematic review and meta-analysis of observational studies. Eur J Intern Med. 2015 May;26(4):285-91. doi: 10.1016/j.ejim.2015.03.008[↩]
- Bruera E, Palmer JL, Bosnjak S, Rico MA, Moyano J, Sweeney C, Strasser F, Willey J, Bertolino M, Mathias C, Spruyt O, Fisch MJ. Methadone versus morphine as a first-line strong opioid for cancer pain: a randomized, double-blind study. J Clin Oncol. 2004 Jan 1;22(1):185-92. doi: 10.1200/JCO.2004.03.172[↩]
- Berlach DM, Shir Y, Ware MA. Experience with the synthetic cannabinoid nabilone in chronic noncancer pain. Pain Med. 2006 Jan-Feb;7(1):25-9. doi: 10.1111/j.1526-4637.2006.00085.x[↩]
- Frank B, Serpell MG, Huges J, Matthews JN, Kapur D. Comparison of analgesic effects and patients tolerability of nabilone and hydrocodeine for chronic neuropathic pain: randomized, crossover, double blind study. BMJ 2008;336:199-201. DOI: 10.1136/bmj39429.619653.80[↩]
- Dworkin RH, O’Connor AB, Backonja M, Farrar JT, Finnerup NB, Jensen TS, et al. Pharmacologic management of neuropathic pain: evidence-based recommendations. Pain 2007;132(3):237-51. Epub 2007 Oct 24. DOI: 10.1016/j.pain.2007.08.033[↩]
- Moulin DE, Clark AJ, Gilron I, Ware MA, Watson CP, Sessle BJ, Coderre T, Morley-Forster PK, Stinson J, Boulanger A, Peng P, Finley GA, Taenzer P, Squire P, Dion D, Cholkan A, Gilani A, Gordon A, Henry J, Jovey R, Lynch M, Mailis-Gagnon A, Panju A, Rollman GB, Velly A; Canadian Pain Society. Pharmacological management of chronic neuropathic pain – consensus statement and guidelines from the Canadian Pain Society. Pain Res Manag. 2007 Spring;12(1):13-21. doi: 10.1155/2007/730785[↩]
- Vargas-Schaffer G. Is the WHO analgesic ladder still valid? Twenty-four years of experience. Can Fam Physician. 2010 Jun;56(6):514-7, e202-5. https://www.cfp.ca/content/56/6/514[↩]
- Scott LJ. Intravenous ibuprofen: in adults for pain and fever. Drugs. 2012 May 28;72(8):1099-109. doi: 10.2165/11209470-000000000-00000[↩]
- Jarupongprapa S, Ussavasodhi P, Katchamart W. Comparison of gastrointestinal adverse effects between cyclooxygenase-2 inhibitors and non-selective, non-steroidal anti-inflammatory drugs plus proton pump inhibitors: A systematic review and meta-analysis. J. Gastroenterol. 2013;48:830–838. doi: 10.1007/s00535-012-0717-6[↩]
- Llorente Melero MJ, Tenías Burillo JM, Zaragoza Marcet A. Comparative incidence of upper gastrointestinal bleeding associated with individual non-steroidal anti-inflammatory drugs. Rev Esp Enferm Dig. 2002 Jan;94(1):7-18. English, Spanish.[↩]
- Yanagawa A, Endo T, Kusakari K, Kudo T, Shimada J, Mizushima Y. Endoscopic evaluation of aceclofenac-induced gastroduodenal mucosal damage: A double-blind comparison with sodium diclofenac and placebo. Mod. Rheumatol. 1998;8:249–259.[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Celecoxib. [Updated 2017 Jan 23]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548579[↩]
- Celecoxib. https://medlineplus.gov/druginfo/meds/a699022.html[↩]
- Sabzwari SR, Qidwai W, Bhanji S. Polypharmacy in elderly: a cautious trail to tread. J Pak Med Assoc. 2013 May;63(5):624-7.[↩]
- Sostres C, Gargallo CJ, Arroyo MT, Lanas A. Adverse effects of non-steroidal anti-inflammatory drugs (NSAIDs, aspirin and coxibs) on upper gastrointestinal tract. Best Pract Res Clin Gastroenterol. 2010 Apr;24(2):121-32. doi: 10.1016/j.bpg.2009.11.005[↩][↩]
- Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, Whelton A, Makuch R, Eisen G, Agrawal NM, Stenson WF, Burr AM, Zhao WW, Kent JD, Lefkowith JB, Verburg KM, Geis GS. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA. 2000 Sep 13;284(10):1247-55. doi: 10.1001/jama.284.10.1247[↩]
- Farkouh ME, Kirshner H, Harrington RA, Ruland S, Verheugt FW, Schnitzer TJ, Burmester GR, Mysler E, Hochberg MC, Doherty M, Ehrsam E, Gitton X, Krammer G, Mellein B, Gimona A, Matchaba P, Hawkey CJ, Chesebro JH; TARGET Study Group. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), cardiovascular outcomes: randomised controlled trial. Lancet. 2004 Aug 21-27;364(9435):675-84. doi: 10.1016/S0140-6736(04)16894-3[↩]
- Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-Vargas R, Davis B, Day R, Ferraz MB, Hawkey CJ, Hochberg MC, Kvien TK, Schnitzer TJ; VIGOR Study Group. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. N Engl J Med. 2000 Nov 23;343(21):1520-8, 2 p following 1528. doi: 10.1056/NEJM200011233432103[↩]
- Rahme E, Bardou M, Dasgupta K, Toubouti Y, Ghosn J, Barkun AN. Hospitalization for gastrointestinal bleeding associated with non-steroidal anti-inflammatory drugs among elderly patients using low-dose aspirin: a retrospective cohort study. Rheumatology (Oxford). 2007 Feb;46(2):265-72. doi: 10.1093/rheumatology/kel223[↩][↩]
- Stillman MJ, Stillman MT. Appropriate use of NSAIDs: considering cardiovascular risk in the elderly. Geriatrics. 2007 Mar;62(3):16-21.[↩][↩]
- Atukorala I, Hunter DJ. Valdecoxib : the rise and fall of a COX-2 inhibitor. Expert Opin Pharmacother. 2013 Jun;14(8):1077-86. doi: 10.1517/14656566.2013.783568[↩][↩]
- Whelton A, White WB, Bello AE, Puma JA, Fort JG; SUCCESS-VII Investigators. Effects of celecoxib and rofecoxib on blood pressure and edema in patients > or =65 years of age with systemic hypertension and osteoarthritis. Am J Cardiol. 2002 Nov 1;90(9):959-63. doi: 10.1016/s0002-9149(02)02661-9[↩][↩]
- Roumie CL, Mitchel EF Jr, Kaltenbach L, Arbogast PG, Gideon P, Griffin MR. Nonaspirin NSAIDs, cyclooxygenase 2 inhibitors, and the risk for stroke. Stroke. 2008 Jul;39(7):2037-45. doi: 10.1161/STROKEAHA.107.508549[↩][↩]
- Rostom A, Dube C, Wells G, Tugwell P, Welch V, Jolicoeur E, McGowan J. Prevention of NSAID-induced gastroduodenal ulcers. Cochrane Database Syst Rev. 2002;(4):CD002296. doi: 10.1002/14651858.CD002296[↩][↩]
- Kumar B, Swee ML (2015). Nonsteroidal Anti-inflammatory Drug Use in a Patient With Hypertension: A Teachable Moment. JAMA Intern Med, 175: 892-893[↩]
- Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16(5):821-47. doi: 10.18433/j3vw2f[↩][↩]
- Stillman MJ, Stillman MT. Choosing nonselective NSAIDs and selective COX-2 inhibitors in the elderly. A clinical use pathway. Geriatrics. 2007 Feb;62(2):26-34.[↩]
- By the American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2015 Nov;63(11):2227-46. doi: 10.1111/jgs.13702[↩]
- Whelton A. Nephrotoxicity of nonsteroidal anti-inflammatory drugs: physiologic foundations and clinical implications. Am J Med. 1999 May 31;106(5B):13S-24S. doi: 10.1016/s0002-9343(99)00113-8[↩]
- Sriuttha P, Sirichanchuen B, Permsuwan U. Hepatotoxicity of Nonsteroidal Anti-Inflammatory Drugs: A Systematic Review of Randomized Controlled Trials. Int J Hepatol. 2018 Jan 15;2018:5253623. doi: 10.1155/2018/5253623[↩]
- Schafer AI. Effects of nonsteroidal anti-inflammatory therapy on platelets. Am J Med. 1999 May 31;106(5B):25S-36S. doi: 10.1016/s0002-9343(99)00114-x[↩]
- Berkes EA. Anaphylactic and anaphylactoid reactions to aspirin and other NSAIDs. Clin Rev Allergy Immunol. 2003 Apr;24(2):137-48. doi: 10.1385/CRIAI:24:2:137[↩]
- Szczeklik A. Adverse reactions to aspirin and nonsteroidal anti-inflammatory drugs. Ann Allergy. 1987 Nov;59(5 Pt 2):113-8.[↩]
- Wongrakpanich S, Wongrakpanich A, Melhado K, Rangaswami J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The Elderly. Aging Dis. 2018 Feb 1;9(1):143-150. doi: 10.14336/AD.2017.0306[↩][↩][↩]
- Weinblatt ME. Drug interactions with non steroidal anti-inflammatory drugs (NSAIDs). Scand J Rheumatol Suppl. 1989;83:7-10. doi: 10.3109/03009748909101471[↩]
- Moore N, Pollack C, Butkerait P. Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Ther Clin Risk Manag. 2015 Jul 15;11:1061-75. doi: 10.2147/TCRM.S79135[↩]
- Hunter LJ, Wood DM, Dargan PI. The patterns of toxicity and management of acute nonsteroidal anti-inflammatory drug (NSAID) overdose. Open Access Emerg Med. 2011 Jul 6;3:39-48. doi: 10.2147/OAEM.S22795[↩]





{kind=link}