
Contents
- Normal Tension Glaucoma
Normal Tension Glaucoma
Normal tension glaucoma (NTG), also known as normal or low-pressure glaucoma, is a type of primary open-angle glaucoma (POAG) where the optic nerve damage and vision loss characteristic of glaucoma occur despite eye pressure (intraocular pressure [IOP]) remaining within the normal range and an open, normal appearing anterior chamber angle 1, 2, 3, 4, 5, 6. The definitions of normal tension glaucoma (NTG), however, may vary slightly amongst different countries. The European Glaucoma Society Guidelines, published in 2021 7, state that “normal tension glaucoma is a specific type of POAG characterized by glaucomatous optic nerve head damage and corresponding visual field defects in patients with IOP consistently less than 21 mmHg”. The Preferred Practice Pattern Guidelines published in 2021 by the American Academy of Ophthalmology 8 define the normal tension glaucoma as “a common form of POAG, i.e., a chronic, progressive optic neuropathy that results in a characteristic optic nerve head cupping, retinal nerve fiber layer thinning and functional visual field loss, in which there is no measured elevation of the IOP”. In 2015, the Canadian Ophthalmological Society Guidelines 9 reported normal tension glaucoma as “a subgroup of POAG with characteristic visual field defects and glaucomatous optic nerve head changes in patients having normal IOP levels less than 21 mmHg”. The Asia-Pacific Glaucoma Guidelines, published in 2016 10, reported that “the normal tension glaucoma is a condition in which the typical glaucomatous progressive optic nerve damage and visual field loss occur although the intraocular pressure remains normal”. The Japanese Glaucoma Society published guidelines in 2023 11, which defined normal tension glaucoma as “a subtype of POAG in which the IOP always remains within the statistically determined normal range during the developmental process of glaucomatous optic neuropathy (GON)”.
Normal eye pressure is 10 to 21 mmHg and approximately 95% of general population will have an intraocular pressure (IOP) between 11 and 21 mmHg 12. A cut-off of 21 mmHg intraocular pressure (IOP) is often applied to define normal tension glaucoma 1. One of the main risk factors for the development of glaucoma is the increased intraocular pressure (the pressure within your eyeball is higher than normal). The higher the intraocular pressure (IOP), the more likely glaucoma is to develop. However this is not the only risk factor for glaucoma. It is also widely recognized that in about 1/3rd of cases of glaucoma the characteristic optic nerve changes and visual field loss can develop in an eye with normal pressure – this is termed normal tension glaucoma. Unlike the typical glaucoma, where high intraocular pressure (increased IOP) is the primary cause, normal tension glaucoma is often linked to other factors, such as blood flow issues to the optic nerve. Normal-tension glaucoma can also lead to vision loss and blindness. Drance and colleagues 13 described two forms of normal tension glaucoma: 1) a non-progressive form typically associated with a transient episode of vascular compromise, and 2) a progressive form thought to result from a chronic vascular insufficiency at the optic nerve. While some try to delineate normal tension glaucoma and primary open angle glaucoma (POAG) as two completely unique disease processes, it has also been suggested that the diseases exist on a continuum with intraocular pressure (IOP) playing a larger role in primary open angle glaucoma (POAG), and vascular or mechanical factors at the etiologic root in normal tension glaucoma 14.
The histopathological changes in normal tension glaucoma are the same as those found in primary open angle glaucoma (POAG), namely loss of retinal ganglion cell axons (retinal nerve fiber layer – RNFL) and glial tissue at the optic nerve head, leading to optic disc excavation and cupping 15. Typically, retinal nerve fiber layer loss is more common in the supero- and inferotemporal neuroretinal bundles, leading to notches, but loss may also be global and concentric 1. Classically, the presence of small flame shaped optic disc hemorrhages also known as Drance hemorrhages, has been associated with normal tension glaucoma though this finding can be observed in any form of primary open angle glaucoma (POAG) (see Figure 2). Optic disc hemorrhages or Drance hemorrhages are splinter or flame-shaped hemorrhages oriented perpendicular to the optic disc margin 16, 17, 18, 19. Classically, Drance hemorrhages are located in the prelaminar optic disc, cross the peripapillary zone, and extend into the adjacent superficial retinal nerve fiber layer, although they may not occupy the entire length from disc to retina 16, 17, 18. Alternately, deeper disc hemorrhages may appear round and blotchy 16. Less commonly, a optic disc hemorrhage may be noted in the peripapillary retinal nerve fiber layer reaching within one disc diameter of the optic disc margin 19. Additional research is needed to determine exactly why optic disc hemorrhages or Drance hemorrhages occur and to clarify why only some glaucoma patients develop optic disc hemorrhages 20. Drance hemorrhages and temporal retinal nerve fiber layer defects with localized, deep paracentral scotomas, more often in the superior hemifield are more common in normal tension glaucoma than in primary open angle glaucoma (POAG) 21, 22. Anderson et al 23 reported the presence of optic disc hemorrhages at the time of diagnosis of normal tension glaucoma as an unfavorable prognostic marker for likely visual field progression.
A recent cross-sectional study aimed to further describe a potential link between the incidence of normal tension glaucoma in patients with dementia 24. The study demonstrated an association between normal tension glaucoma status and poor cognition (measured with the Telephone Version of the Montreal Cognitive Assessment, T-MoCA) thereby concluding that there exists a disease association and shared features between normal tension glaucoma and dementia when compared to those with high tension glaucoma (HTG) 24. Conversely, a recent study demonstrated that persons with normal tension glaucoma had increased risk for developing vascular dementia, with particular increased risk when diagnosed with glaucoma at ages >70 25.
While the exact prevalence of normal tension glaucoma can vary by geographic region, normal tension glaucoma is estimated to comprise a significant proportion of all glaucoma cases, with some studies suggesting it may account for up to 30-40% of all glaucoma patients amongst Caucasians or Africans 26, 2. Whereas, for unclear reasons, the proportion of normal tension glaucoma amongst primary open angle glaucoma (POAG) in Asian populations was reported as high as 92.3% in Japan (the Tajimi Study), 84.6% in Singapore (the Singapore Malay Eye Study), 83.58% in northern China (the Handan Eye Study), 82% in south India (the Chennai Glaucoma Study), 79.6% in southern China (the Liwan Eye Study), 77% in South Korea (the Namii Study), yet only 31.7% in the United states of America (the Beaver Dam Eye Study) demonstrating that there is a predilection for those of Asian descent 27, 28. Current research tackles the disparity demonstrated by the aforementioned data, suggesting that other factors/predispositions within specific ethnic groups may be playing a significant role in the pathogenesis of normal tension glaucoma.
The therapeutic approaches to normal tension glaucoma are still strongly debated. Intraocular pressure (IOP)-lowering treatment management should be tailored specifically to each patient. Treatment may need to be changed as the disease progresses or a patient’s response to medicine changes. Considering that large prospective, multicenter, randomized and controlled clinical trials such as the Collaborative Normal-Tension Glaucoma Study (CNTGS) and the Early Manifest Glaucoma Trial (EMGT) have demonstrated that an intraocular pressure (IOP) reduction of at least 25–30% from baseline values is effective in delaying the progression of the visual field damage in a high percentage of normal tension glaucoma patients 29, 30. It is thus important to note that despite the fact that individuals with normal tension glaucoma have by definition normal intraocular pressure (IOP) levels, lowering the intraocular pressure (IOP) remains the gold standard in the normal tension glaucoma treatment 31, 32, 33.
Many different ocular hypotensive drugs are available on the market: prostaglandin and prostamide analogs, beta-blockers, alpha agonists and carbonic anhydrase inhibitors are examples of topical glaucoma drugs that are frequently used to reduce intraocular pressure (IOP), taken both as topical single therapy or in combination. Prostaglandins and prostamide analogs are the most safe and effective intraocular pressure (IOP)-lowering medications and represent the first choice in normal tension glaucoma therapy 32, 34, 35, 36.
The use of local and systemic beta-blockers and oral calcium channel blockers, especially in the evening, is of particular concern in normal tension glaucoma patients, because they may induce severe nocturnal systemic hypotension, with subsequent ocular perfusion pressure drop 37, 34, 38, 39, which is considered one of the most important risk factors for normal tension glaucoma onset and progression 40, 41.
Besides providing an intraocular pressure (IOP)-lowering effect, some ocular hypotensive drugs have also shown the ability to increase the optic nerve head blood flow (latanoprost, bimatoprost, betaxolol, carteolol, levobunolol, carvedilol and nebivolol) or neuroprotective properties (brimonidine, betaxolol, carteolol, carvedilol, latanoprost, bimatoprost and tafluprost) 42, 43, 44, 45, 46, 47, 36. These adjunctive (add-on) properties could be particularly useful in treating normal tension glaucoma patients. Moreover, the confirmation of the ability of the novel beta-blockers, carvedilol and nebivolol, to reduce intraocular pressure (IOP) and increase the ocular blood flow in clinical trials in glaucomatous patients may lead to the development of new glaucoma therapies.
For optimal management of normal tension glaucoma, regular monitoring of intraocular pressure (IOP), visual field and optic nerve head by eye care specialists is important. Moreover, performing diurnal intraocular pressure (IOP) curves and addressing intraocular pressure (IOP) peaks are considered to be the most important therapeutic strategies in normal tension glaucoma patients with normal office intraocular pressure (IOP) values 40, 32.
Considering that normal tension glaucoma patients have, by definition, a baseline intraocular pressure (IOP) within the statistically normal range, it is often difficult to reduce the intraocular pressure (IOP) values with medications alone, so non-medical options are often used, including laser and surgical treatments 32. The Collaborative Normal-Tension Glaucoma Study (CNTGS) 29 showed that 57% of the patients achieved a 30% intraocular pressure (IOP) reduction with topical medications, laser trabeculoplasty or both; the remaining 43% required filtering surgery, which remains the most proven option in the treatment of normal tension glaucoma patients when medications or laser treatments are unable to stop the visual field and/or optic nerve head damage progression 32, 48.
Figure 1. Retinal layers showing retinal ganglion cell
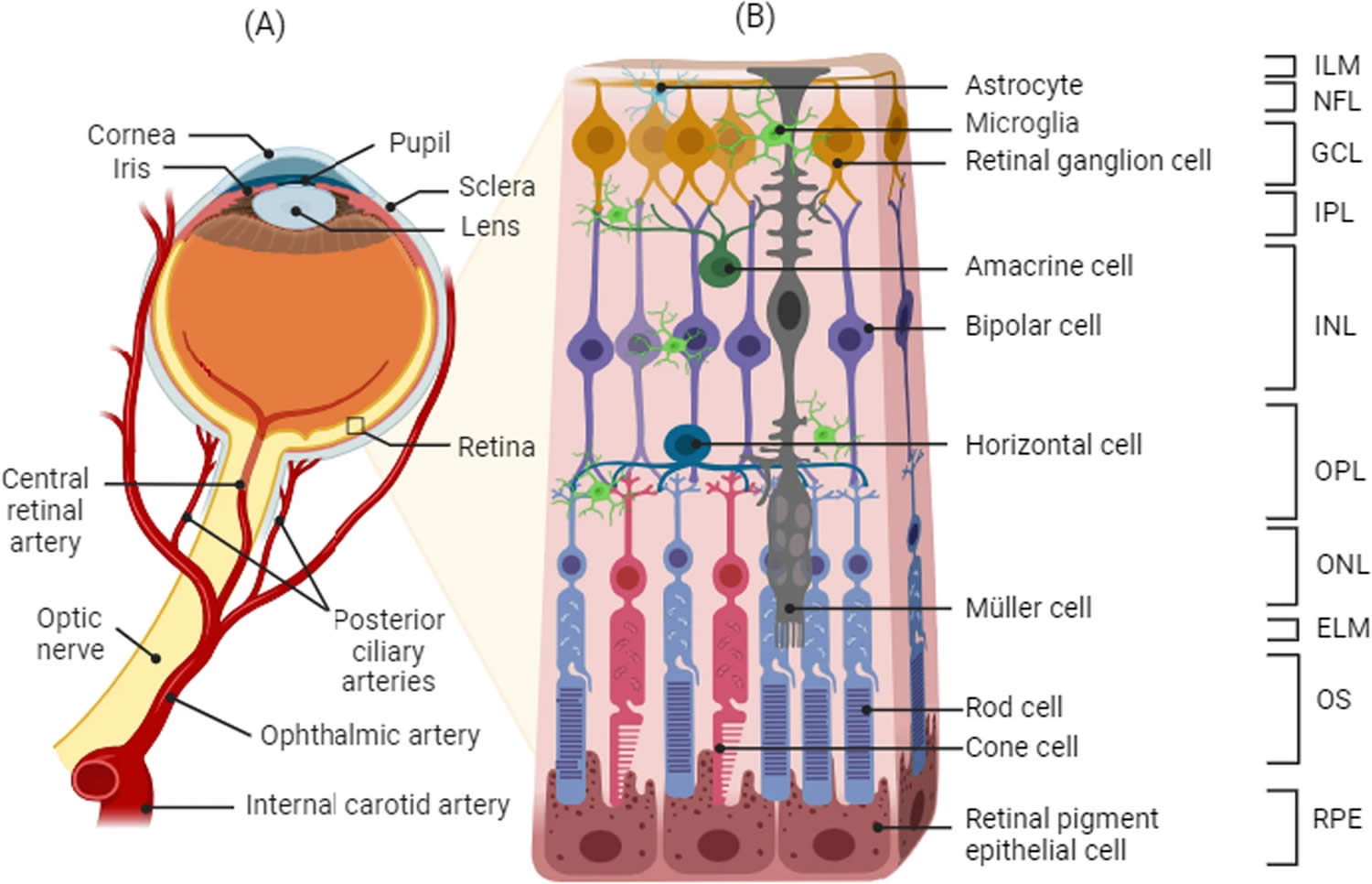
Footnotes: Schematic representation of the retina and the retinal cell layers. (A) Blood supply and (B) structure of the retina. The retina is a layered structure lining the back of the eye consisting of a pigmented layer called retinal pigment epithelium (RPE), and a multilayered neuroretina. The retinal pigment epithelium (RPE) is in close contact with the outer segments of the photosensitive rod and cone cells of the neuroretina. The connecting cilium connects the photoreceptor outer segments with the cell bodies, which constitute a layer known as the outer nuclear layer (ONL). The axons of the photoreceptors synapse with the neuronal (bipolar, amacrine, and horizontal) cells of the inner nuclear layer (INL) via the outer plexiform layer (OPL). The axons of the inner nuclear layer (INL) cells in turn synapse with the ganglion cell layer (GCL) via the inner plexiform layer (IPL). The axons of the ganglion cells converge to form the optic nerve. A retinal ganglion cell (RGC) is a type of neuron located near the inner surface (ganglion cell layer [GCL]) of the retina of the eye. A retinal ganglion cell (RGC) receives visual information from photoreceptors via two intermediate neuron types: bipolar cells and retina amacrine cells. Retina amacrine cells, particularly narrow field cells, are important for creating functional subunits within the ganglion cell layer and making it so that ganglion cells can observe a small dot moving a small distance. Retinal ganglion cells collectively transmit image-forming and non-image forming visual information from the retina in the form of action potential to several regions in the thalamus, hypothalamus, and mesencephalon, or midbrain.
Abbreviations: ILM: internal limiting membrane, NFL: nerve fiber layer, GCL: ganglion cell layer, IPL: inner plexiform layer, INL: inner nuclear layer, OPL: outer plexiform layer, ONL: outer nuclear layer, ELM: external limiting membrane, OS: photoreceptor outer segment, RPE: retinal pigment epithelium
[Source 49 ]Figure 2. Drance hemorrhage (optic disc hemorrhage)
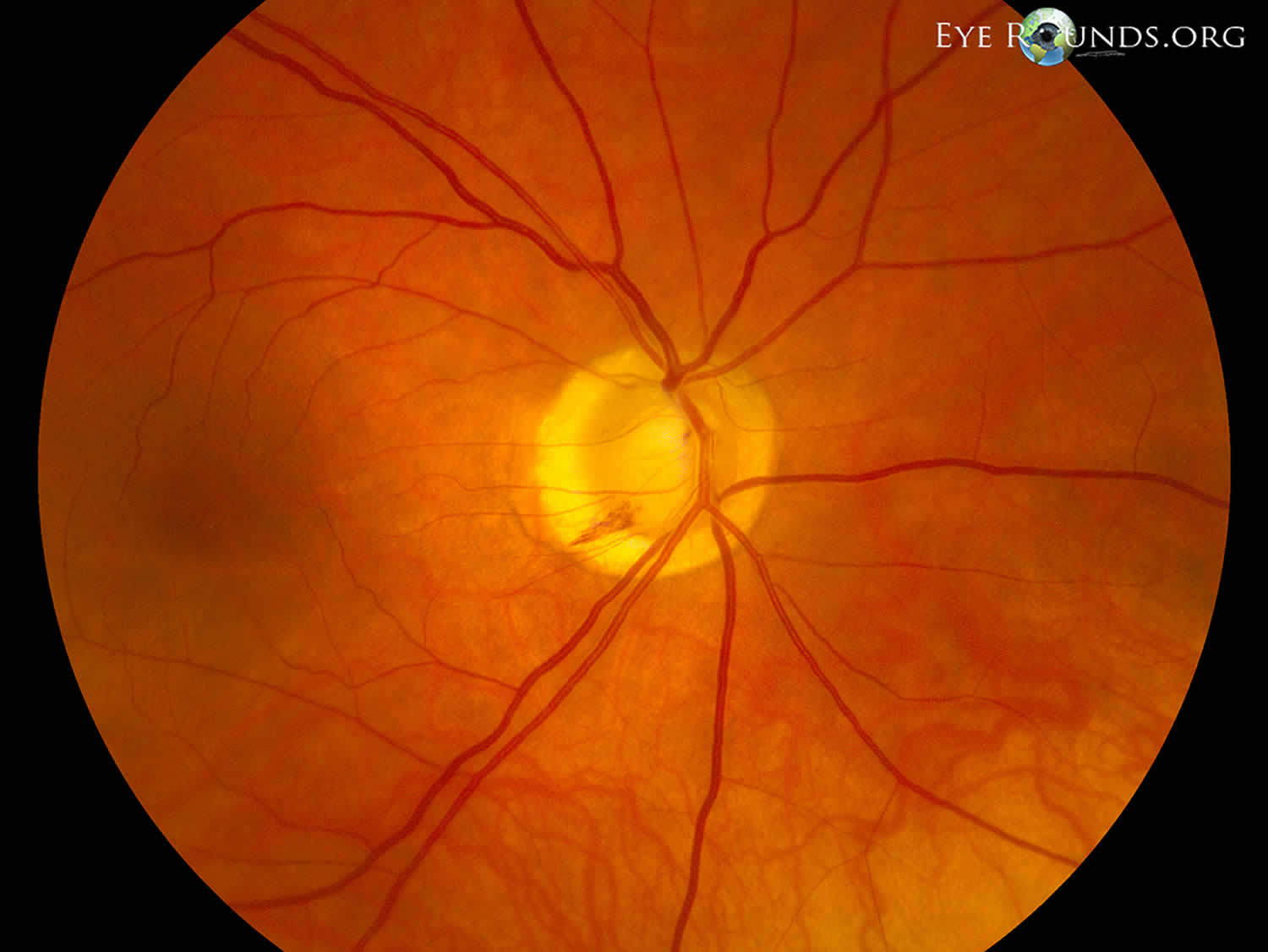
Footnotes: Optic disc hemorrhage or Drance hemorrhage indicating inadequate intraocular pressure control in a patient with normal tension glaucoma. Disc hemorrhages are more common in normal tension glaucoma than in primary open angle glaucoma (POAG). This patient also has peripapillary atrophy, visible as a pale ring around the optic nerve.
[Source 50 ]Figure 3. Normal tension glaucoma optic disc photographs
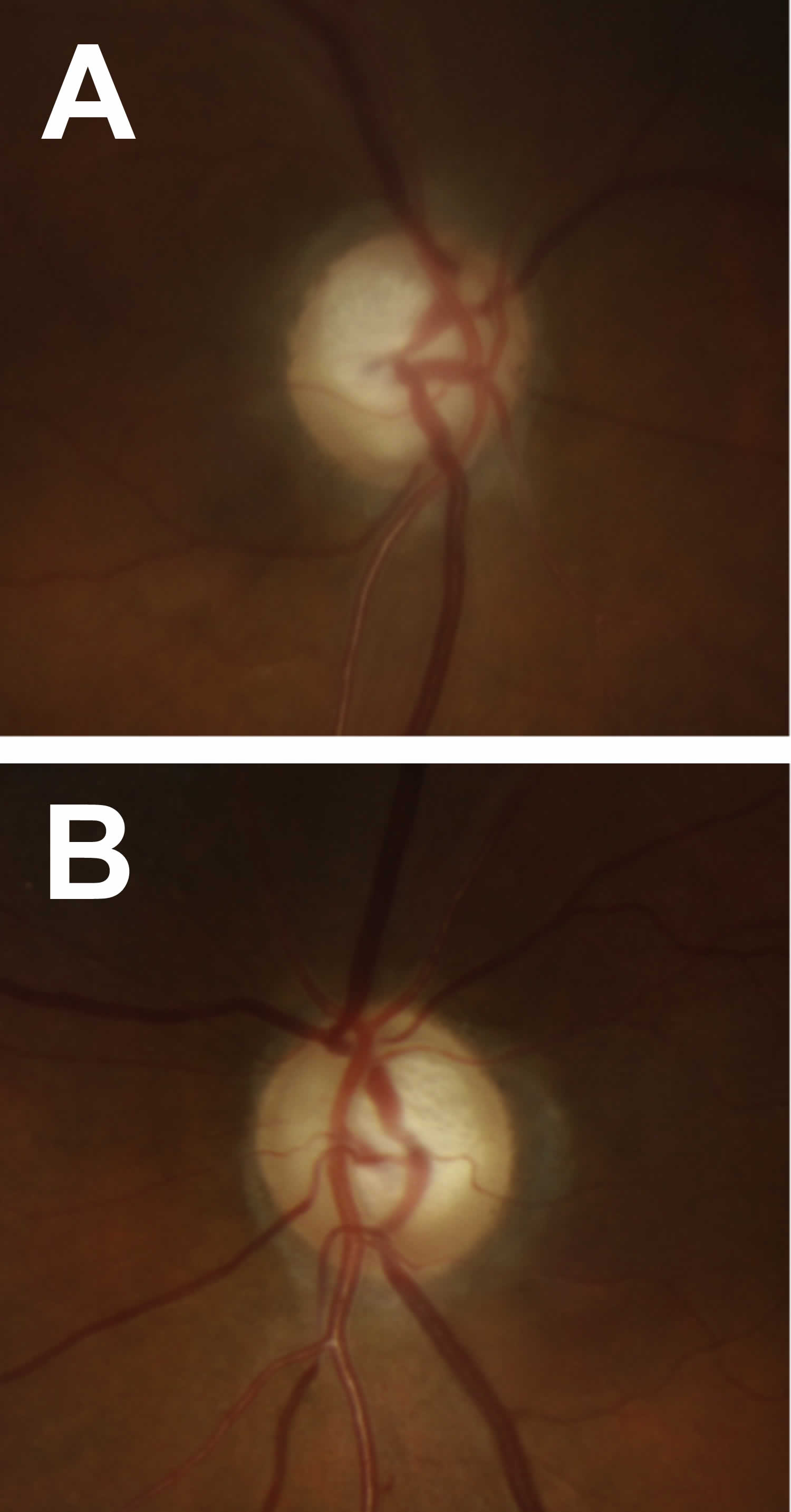
Footnotes: Normal tension glaucoma optic disc photographs. (A) Right and (B) Left eye in a patient with normal tension glaucoma. Note the focal superotemporal thinning and associated dropout of the retinal nerve fiber layer. The corresponding visual field defects are seen in Figure 4 below.
[Source 14 ]Figure 4. Normal tension glaucoma visual fields
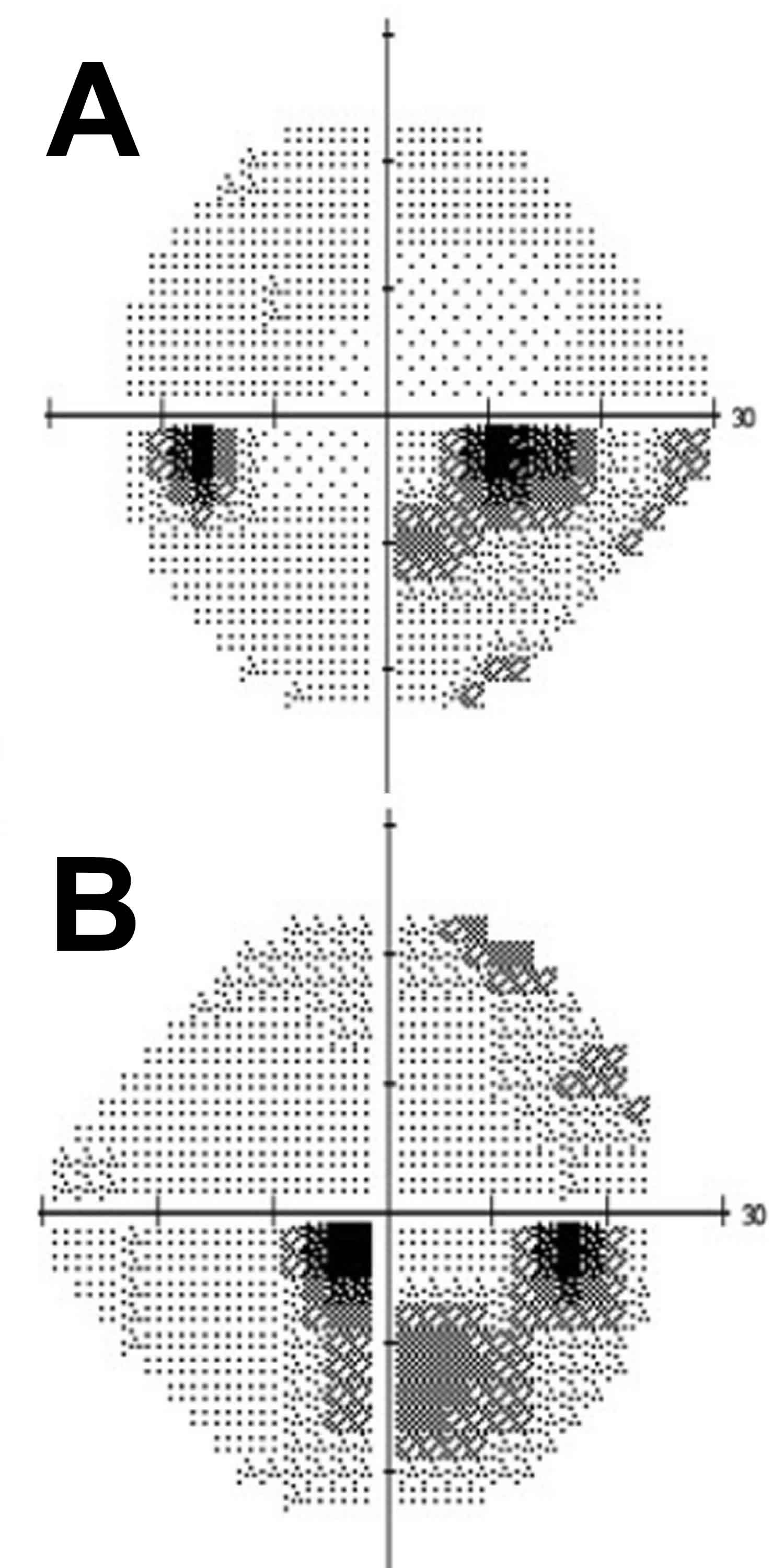
Footnotes: Standard automated perimetry of (A) Left and (B) Right eye in a patient with normal tension glaucoma. Note the dense inferior arcuate scotomas occurring near fixation with minimal involvement of periphery. The corresponding optic disc photographs are seen in Figure 3 above.
[Source 14 ]Normal tension glaucoma causes
The cause and mechanism for the development of normal tension glaucoma is unknown and remains an area of active research and debate. Several theories have been proposed to explain the onset and progression of normal tension glaucoma (NTG). Whereas intraocular pressure (IOP) is the main driver of progressive visual loss in most patients with primary open angle glaucoma (POAG), normal tension glaucoma (NTG) likely represents a diverse and multifactorial group of causes with a common final pathway of retinal ganglion cell loss 1. Despite intraocular pressure (IOP) in the normal range of 10 to 21 mmHg, there is evidence that an intraocular pressure (IOP)-dependent mechanism plays a role in the cause in many eyes with normal tension glaucoma 51, 52. Proposed intraocular pressure (IOP)-independent mechanisms include vascular insufficiency (lower blood pressure or reduced ocular blood flow) at the optic nerve head, impaired cerebrospinal fluid (CSF) circulation resulting in low retrobulbar cerebrospinal fluid pressure causing stagnation and decreased optic nerve protection, failure of the glymphatic system in the optic nerve, metabolic and neurodegenerative disorders, oxidative stress, and structural anomalies including structural weakness of the lamina cribrosa 53, 54, 55, 56, 57, 27. All of these mechanisms need further research to better define the pathophysiology of the disease process 14.
It has been theorized that the disease process in normal tension glaucoma results from an enhanced sensitivity to what would otherwise be physiologic intraocular pressure (IOP), resulting in glaucomatous damage of the optic nerve. This enhanced sensitivity may be due to impaired optic nerve blood flow, a higher translaminar pressure gradient (intraocular pressure [IOP] minus intracranial pressure [ICP]) due to lower intracranial pressure (ICP), or a structurally abnormal lamina cribrosa, which cannot withstand a normal range of intraocular pressure (IOP) 14. This theory of enhanced sensitivity is useful, at least conceptually, to rationalize the impact of intraocular pressure (IOP) in a disease process that may have an intraocular pressure (IOP) independent underlying etiology 14. The evidence for a role of IOP contributing to normal tension glaucoma comes from the Collaborative Normal Tension Glaucoma Study, which showed a slowing of disease progression in patients achieving a 30% or more reduction of already normal intraocular pressure (IOP) 51, 58. While some try to delineate normal tension glaucoma and primary open angle glaucoma (POAG) as two completely unique disease processes, it has also been suggested that the diseases exist on a continuum with IOP playing a larger role in primary open angle glaucoma (POAG), and vascular or mechanical factors at the etiologic root in normal tension glaucoma 14.
Specific histological studies of eyes with normal tension glaucoma are scarse but in general mimic those changes seen in primary open angle glaucoma (POAG) 14. Histopathologic changes of the optic nerve head include disarrangement and posterior bowing of the lamina cribrosa along with loss of nerve fibers 59. Non-invasive imaging by OCT and scanning laser modalities have characterized thinning of the peripapillary choroid 60, as well as thinning of the ganglion cell layers in normal tension glaucoma patients compared to other primary open angle glaucoma (POAG) and normal patients 61. In Asian patients this thinning has been correlated with vascular narrowing in asymmetric normal tension glaucoma when compared to normal fellow eyes and primary open angle glaucoma (POAG) patients with elevated pressures 62, 63, 64.
Genetics is also known to play a role in normal tension glaucoma, because of the strong association with family history with 21% of patients reporting a family history of glaucoma and variation in prevalence in different ethnicities that persists after migration 1. Four major genes have been implicated in normal tension glaucoma: optineurin (OPTN), TANK binding kinase 1 (TBK1), methyltransferase-like 23 (METTL23), and myocilin (MYOC) 56. Optineurin (OPTN) gene mutations, particularly the E50K variant, have been strongly associated with normal tension glaucoma, causing early-onset disease, large cup-to-disc ratios, and retinal ganglion cell death 14. TANK binding kinase 1 (TBK1) copy number variations have also been linked to normal tension glaucoma, with duplications and triplications contributing to retinal ganglion cell (RGC) loss 14. Methyltransferase-like 23 (METTL23) gene mutations were recently identified in familial normal tension glaucoma cases, with evidence suggesting that these mutations impact histone arginine methylation, potentially leading to retinal ganglion cell (RGC) degeneration 14. Myocilin (MYOC) gene commonly associated with primary open angle glaucoma (POAG) has been implicated in some normal tension glaucoma cases, though its role remains less clear 14. Further genetic research is certainly needed to better understand the role of these genes in normal tension glaucoma 56.
Genes associated with normal tension glaucoma 1, 56:
- Optineurin (OPTN)
- TANK binding kinase (TBK1)
- Methyltransferase-like 23 (METTL23)
- Myocilin (MYOC)
Normal tension glaucoma is typically not considered to be a heritable disease, as approximately 2% of normal tension glaucoma cases are caused primarily by a mutation of a single gene and found to be transmitted by an autosomal dominant inheritance pattern 14. Nevertheless, individuals who carry one of the many autosomal dominant gene mutations may present with symptoms of normal tension glaucoma as early as 23 years old 65. Genetic and pedigree studies continue to further identify numerous new genes associated with the development of normal tension glaucoma, but further studies that demonstrate a higher incidence of disease are necessary before a clinical indication for genetic screening and counseling can be recommended 14.
Though the quantity of axons that compose optic nerves in humans remains a predictable constant between individuals, variability in surface area of optic discs is observed. It is unclear if certain optic nerve head parameters place an eye at increased risk of normal tension glaucoma 14. Optic nerves with a larger surface area and with thinner inferior/inferotemporal rims have been reported to be at an increased risk for developing normal tension glaucoma 66, 67. Other studies evaluating the optic nerve head by scanning laser ophthalmoscopy found no morphologic differences between high-tension and normal tension glaucoma patients 68.
Frequently an area of peripapillary atrophy in a crescent or halo configuration is observed in patients with normal tension glaucoma. While this pattern of atrophy can be a finding in eyes without normal tension glaucoma, in glaucomatous eyes, peripapillary atrophy often occurs adjacent to areas of greatest disc thinning and corresponding visual field loss 69. While thinning of the optic nerve rim is observed in all primary open angle glaucoma (POAG), focal thinning or ‘notching’ is more commonly observed in normal tension glaucoma 70.
Intraocular Pressure (IOP)
Although always residing within the normal range for intraocular pressure (IOP), patients with normal tension glaucoma have been suggested to have higher-normal intraocular pressure (IOP) levels 71. By contrast, prospective evaluation of patients in the Low-Pressure Glaucoma Treatment Study found no relation between intraocular pressure (IOP) asymmetry and visual field asymmetry 72. Wide diurnal fluctuations in intraocular pressure (IOP) and nocturnal intraocular pressure (IOP) spikes have also been correlated with normal tension glaucoma 71.
Systemic vascular disease
Patients with systemic conditions that result in ischemic vascular disease such as diabetes and patients with a history of stroke have been shown to be at increased risk for bilateral normal tension glaucoma compared to unilateral normal tension glaucoma 14. Patients with normal tension glaucoma may have increased diastolic blood pressure and display larger dips in blood pressure overnight compared to normal 14. Similarly, it has been suggested that obstructive sleep apnea (OSA) may lead to transient episodes of nocturnal hypoxemia and compromised optic nerve head perfusion 14. A higher prevalence of obstructive sleep apnea (OSA) among normal tension glaucoma patients has been noted in several studies 73, 74, 75. Moreover, one study demonstrated a correlation between moderate/severe obstructive sleep apnea (OSA) and higher progression of retinal nerve fiber layer (RNFL) loss 76.
Certain vasospastic conditions such as Raynaud disease (a condition where blood vessels in the fingers and toes narrow in response to cold or stress, causing temporary blood flow restriction) are thought to be associated with normal tension glaucoma, with the most reported associated condition being migraine 77. Recently, a disease entity termed primary vascular dysregulation (also known as vasospastic syndrome, refers to a condition where the regulation of blood flow isn’t adapted to the needs of tissues, despite anatomically healthy vessels and the absence of an underlying disease) has been described pointing to retinal and optic nerve vasculature dysregulation as a potential risk factor for normal tension glaucoma 78. As above, a recent study demonstrated a significantly increased risk of developing vascular dementia in individuals diagnosed with normal tension glaucoma, further supporting a vascular deregulatory element in the pathogenesis of normal tension glaucoma 25.
A recent cross-sectional study investigated the prevalence of normal tension glaucoma in patients with Conn’s syndrome also called primary aldosteronism. Of the 212 patients with primary hyperaldosteronism included in the study, the prevalence of normal tension glaucoma in primary hyperaldosteronism patients was 11.8%, significantly higher than in hypertensive patients without primary aldosteronism (5.2%) 79. The study found a fourfold increase in the odds of developing normal tension glaucoma in primary hyperaldosteronism patients compared to those without primary hyperaldosteronism 79. These findings suggest that aldosterone dysregulation may contribute to the development of normal tension glaucoma, independent of blood pressure, and highlight the need for further research on the potential neuroprotective effects of mineralocorticoid receptor antagonists in normal tension glaucoma patients with primary hyperaldosteronism 79.
Another recent study explored potential clinical links between normal tension glaucoma and Alzheimer’s disease, focusing on shared neurodegenerative mechanisms 80. Both normal tension glaucoma and Alzheimer’s disease are progressive conditions, sharing risk factors such as age, female sex, and vascular dysfunction. Neuroimaging studies reveal that normal tension glaucoma may have cerebral manifestations similar to Alzheimer’s disease, further suggesting common mechanisms 80. Moreover, biomarkers like amyloid beta (Aβ) and tau proteins, traditionally linked with Alzheimer’s disease, have been implicated in normal tension glaucoma, indicating overlapping pathological processes. While connections between the two diseases remain debated, understanding normal tension glaucoma as part of a broader neurodegenerative spectrum may enhance both diagnostics and treatments for normal tension glaucoma, potentially offering insights into Alzheimer’s disease pathogenesis. Further research is needed to elucidate the exact relationship between normal tension glaucoma and Alzheimer’s disease 80.
Risk factors for normal tension glaucoma
Risk factors for normal tension glaucoma include 1, 81, 3, 82, 83, 84, 52:
- Over 40 years of age
- Family history of glaucoma
- Female gender
- Asian
- High Myopia
- Above-average intraocular pressure (IOP)
- Thin central corneal thickness
- Systemic hypertension
- Nocturnal hypotension
- Migraine
- Raynaud phenomenon
- Primary vascular dysfunction also called Flammer syndrome where the body’s blood vessels react abnormally to stimuli like cold or emotional stress 85. It’s associated with a cluster of symptoms and signs that can be present in both healthy individuals and those with various diseases, particularly normal-tension glaucoma.
- Frontotemporal dementia and Alzheimer disease
- Obstructive sleep apnea (OSA).
Normal tension glaucoma prevention
Due to the irreversible loss of vision due to normal tension glaucoma, early detection and treatment is important. Screening for and treatment of risk factors associated with normal tension glaucoma, such as nocturnal hypotension, currently does not have a defined role in primary prevention of normal tension glaucoma, particularly in the United States 14. A recent study that took place in China aimed to evaluate the effectiveness of a glaucoma screening program in identifying early-stage glaucoma cases 86. They compared 76 patients identified through glaucoma screening program with 272 consecutive outpatient cases from the same hospital. The findings indicate that patients detected through the screening program had significantly lower intraocular pressure (IOP) and were more likely to have normal tension glaucoma 86. These screening-detected patients also had less visual impairment and better visual field test results compared to clinic patients 86. The study suggests that health examination center-based glaucoma screening is effective in detecting early-stage glaucoma, especially those with normal tension glaucoma, and can complement opportunistic glaucoma detection 86. This is important in a country like China, where glaucoma is a significant public health concern. Further studies must take place to further characterize the role of primary prevention/screening for normal tension glaucoma before it potentially develops into standard practice, particularly in the US where the incidence of normal tension glaucoma is significantly less than in China 14. Nevertheless, the Chinese study demonstrates a potential role for glaucoma screening in patients who are particularly high risk of developing glaucoma.
Normal tension glaucoma signs and symptoms
Most patients with normal tension glaucoma in the early stages have no symptoms of the condition 87. There is no pain and vision seems normal with suspicion of glaucoma raised only by an optometrist during a routine eye testing or an incidental finding with an ophthalmologist 87, 88.
Even with moderately advanced disease, patients may be unaware of field defects because of unilateral disease, negative scotoma, and gradual onset 1. Because the intraocular pressure (IOP) is normal, suspicion is usually roused by optic disc appearance or a visual field defect on automated perimetry 1. If the presentation is advanced, patients may have symptoms of reduced vision, difficulty with low-contrast situations, and awareness of visual field defects. They may experience glare and difficulty adjusting to extreme lighting conditions 1. A family history of glaucoma and blindness should be obtained. Past medical history should include assessing risk factors for glaucoma, such as the history of steroid use, ocular trauma or surgery, and contraindications to treatments, including allergies. Medication usage should be reviewed.
A relative afferent pupillary defect is typical, though it may not be present in the early or symmetrical disease 1. Color vision is usually preserved, except in advanced disease. By definition, the intraocular pressure (IOP) is in the normal range 89. Slit-lamp examination and gonioscopy are essential to determine an open iridocorneal angle status and exclude secondary glaucoma causes. In particular, evidence of angle closure, uveitis, pigment dispersion, and pseudoexfoliation syndrome should be sought, as these are common causes of glaucoma presenting with an intraocular pressure (IOP) in the normal range.
A dilated fundus examination revealed changes in the glaucomatous optic disc. There is a progressive loss of ganglion cell neurons, leading to enlargement of the cup-to-disc ratio. This may be a focal (notch, retinal nerve fiber layer (RNFL) defect) or concentric defect (excavation, senile sclerotic disc) 1. Disc pallor occurs in advanced disease. Measurement of the optic disc size can help identify hypoplasia, physiological disc cupping, and disc asymmetry 1. Optic disc hemorrhages are more common in normal tension glaucoma than in primary open angle glaucoma (POAG) 82. So-called Drance hemorrhages are typically small flame hemorrhages at the disc margin in superior or inferior quadrants. Peripapillary atrophy may be seen but is non-specific. Glaucomatous disc abnormalities typically precede visual field defects in early (preperimetric) disease 90.
Normal tension glaucoma diagnosis
The only sure way to diagnose glaucoma is with a complete eye exam. An eye specialist can diagnose glaucoma using an eye exam, including several tests that are part of routine eye exams. A comprehensive eye exam can detect glaucoma long before you have eye damage and the symptoms that follow. Many of these tests involve pupil dilation (mydriasis), so your eye doctor can get a better look inside your eye. Your eye care specialist examines your eyes using a special magnifying lens. This provides a clear view of important tissues at the back of your eye to check for glaucoma or other eye problems. For a few hours after the exam your vision may be blurry and sensitive to light, so you will need someone to take you home.
Some of the most helpful glaucoma tests include:
- Visual acuity testing. A visual acuity test assesses how clearly someone can see at a distance, typically using a Snellen chart or other standardized chart. The test is performed by an optometrist or ophthalmologist and involves reading progressively smaller letters or identifying shapes, with the results expressed as a fraction like 20/20 or 6/6, indicating the distance at which the person can see the letters or shapes
- Visual field testing also called perimetry. This check of your peripheral (side) vision allows your eye care provider to find out how well you can see objects off to the side of your vision without moving your eyes. This test measures the entire area the forward-looking eye sees to document straight-ahead (central) and side (peripheral) vision. It measures the dimmest light seen at each spot tested. Each time patients perceive a flash of light, they respond by pressing a button.
- Depth perception testing. A depth perception test assesses your ability to see the world in three dimensions (3D) and judge distances accurately. It checks if your eyes work together and if your brain processes the visual information correctly. These tests use 3D images or patterns like the Randot Stereo test to gauge how well your eyes coordinate to perceive depth. Some tests involve holding a finger in front of your eyes and focusing on a distant object, checking for double vision of the finger.
- Tonometry. This measures the pressure inside your eye. Increased eye pressure is the most important risk factor for glaucoma. There are several methods of measuring eye pressure. The most common method is known as applanation, in which a tiny instrument contacts the eye’s surface after it is numbed with an eye drop.
- Air-puff test. You’ll rest your chin on a machine and your eye specialist will blow a puff of air into your eye. This quick and painless test is used as part of a routine glaucoma screening. If the results show that your eye pressure is high, your eye specialist will do other eye-pressure tests to get a more accurate measurement.
- Applanation tonometry. Your eye specialist will numb your eyes with drops before measuring your eye pressure using one of these methods:
- You’ll rest your chin on a special magnifying device called a slit lamp. Your eye care specialist will examine your eye through the slit lamp while gently pressing a special tool on your eye to test the pressure.
- Your eye care specialist will gently press a handheld device against your eye. The device measures your eye pressure.
- Pachymetry. Pachymetry is a simple, painless test that measures the thickness of the cornea, the clear front part of the eye. The eye doctor uses an ultrasonic wave instrument to help determine the thickness of the cornea and better evaluate eye pressure.
- Ophthalmoscopy. Your eye care specialist will do a dilated eye exam to look for damage to your optic nerve. This exam is part of a routine glaucoma check-up. You’ll be given eye drops that widen (dilate) your pupils (the openings that let light into your eyes). You’ll look straight ahead while your eye care specialist looks into your eye using a device with a light and magnifying lens.
- Slit lamp exam. A slit lamp exam is a common eye test that uses a microscope with a focused beam of light to examine the front of your eye and the back of your eye with the aid of special lenses.
- Gonioscopy. Gonioscopy is a specialized eye examination that allows an ophthalmologist to visualize the anterior chamber angle, the space between the iris and the cornea where fluid drains out of the eye. Gonioscopy is a crucial part of diagnosing and monitoring glaucoma and other eye conditions
If your eye specialist has a reason to suspect damage to your retina and/or optic nerve, they may also use additional types of eye imaging. These include:
- Optical coherence tomography (OCT). Optical Coherence Tomography (OCT) measures the reflection of laser light similar to the way that ultrasound measures the reflection of sound. Using this device, a 3D reconstruction of the optic nerve can be created. Optical coherence tomography (OCT) is valuable for monitoring morphological changes in the optic nerve and retinal nerve fiber layer, especially in patients with ocular hypertension and early-to-moderate glaucoma 91. The most recent advances of OCT include OCT-A, or OCT-Angiography, whereby the blood flow to vessels surrounding the optic nerve and in the macula can be measured. This is still an active area of research, but scientists do know that some patients’ optic nerves are very vulnerable to changes in optic nerve blood flow, and this new measurement may be useful in evaluating these patients.
- Heidelberg Retina Tomograph (HRT): Heidelberg Retina Tomograph (HRT) is also a laser that can produce a 3D representation of the optic nerve.
- Nerve Fiber Analyzer (GDx): Nerve Fiber Analyzer (GDx) uses laser light to measure the thickness of the nerve fiber layer.
- Fluorescein angiography. Fluorescein angiography is a diagnostic test used to examine the blood vessels in the retina and choroid of the eye. Fluorescein angiography involves injecting a fluorescent dye into the bloodstream and taking photographs of your retina and its blood vessels as the dye circulates, revealing potential blockages, leaks, or other abnormalities in the blood vessels. Fluorescein angiography is often recommended to find and diagnose eye disease including 92:
- macular edema (swelling in the retina that distorts vision)
- diabetic retinopathy (damaged or abnormal blood vessels in the eye caused by diabetes)
- macular degeneration
- blockage of veins inside the eye, called branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO)
- macular pucker (a wrinkle in the retina caused by a buildup of fluid behind it)
- ocular melanoma (a type of cancer affecting the eye)
- rack changes in eye disease over time
- target treatment areas
- Less commonly, ultrasound, computed tomography (CT) or magnetic resonance imaging (MRI).
Normal tension glaucoma clinical diagnosis
Normal tension glaucoma is a diagnosis made based on similar criteria to primary open angle glaucoma (POAG) but with important clinical features that include:
- Progressive excavation or ‘cupping’ of the optic nerve head from retinal nerve fiber layer loss resulting in corresponding visual field deficits.
- Gonioscopic confirmation of open anterior chamber angle and absence of findings consistent with pigment dispersion or pseudoexfoliation syndrome.
- Pre-treatment intraocular pressure (IOP) must always be less than 22 mm Hg. (diurnal measurement of intraocular pressure (IOP) to ensure there is not a circadian elevation in pressure that is missed by single period clinical measurement)
The diagnosis of normal tension glaucoma is only reached once other forms of optic neuropathy have been ruled out (e.g. ischemic, traumatic, toxic inflammatory, infectious, congenital, and compressive).
Careful history taking should be undertaken to elucidate any prior events that can mimic normal tension glaucoma such as:
- Traumatic injuries
- Inflammation
- Severe blood-loss or hypotensive events
- Medications that may precipitate a transient pathologic elevation in intraocular pressure (IOP)
After reasonable exclusion of all other causes, the demonstration of visual field loss on static, or less often kinetic, perimetry in conjunction with characteristic optic nerve central cupping with no elevation in intraocular pressure (IOP) above 21 mm Hg cement the diagnosis of normal tension glaucoma.
Other classically associated examination findings with normal tension glaucoma that can be helpful clues in raising suspicion for pursuing a diagnosis include optic nerve or “Drance” hemorrhages (also called optic disc hemorrhage) and peripapillary atrophy. While these findings are not specific, patients with normal tension glaucoma have a higher propensity for optic nerve hemorrhages compared to patients with primary open angle glaucoma (POAG). Focal defects in the retinal nerve fiber layer may be more commonly observed as well.
Visual field testing
Automated static perimetry is the most common modality used to detect and monitor for progression of the field loss associated with normal tension glaucoma 14. Visual field defects may include those common to primary open angle glaucoma (POAG) including nasal step and arcuate scotoma. However, defects noted in normal tension glaucoma tend to be more focal and occur closer to fixation early in the disease (Figure 4A and B). Dense paracentral scotomas may characteristically be noted at initial diagnosis.
Optic disc imaging
Visual field testing is useful in early detection but may miss early, pre-perimetric disease, as substantial retinal nerve fiber layer may be lost before functional field defects are noted 14. Therefore, optic disc imaging is an important and objective structural assessment of the optic nerve health 14. For several decades, the gold standard for detecting disease and monitoring changes in the optic nerve head has been stereo disc photography (Figure 3 A and B). In recent years, scanning laser ophthalmoscopy and optical coherence tomography (OCT) is gaining popularity as another means of detecting pathologic thinning of neural tissue and monitoring progression 14. Furthermore, with the introduction of Artificial Intelligence (AI), OCT interpretation continues to become more prevalent when classifying an eye as either a glaucoma suspect or early normal tension glaucoma 14. This was demonstrated in a recent study where a deep-learning algorithm was developed to discriminate between the normal tension glaucoma by using the parameter of Bruch’s membrane opening — minimum rim width, peripapillary retinal nerve fiber layer (RNFL) thickness and color classification of retinal nerve fiber layer (RNFL) — achieving an area under the curve of 0.966 93. Ultimately, these advances continue to improve the diagnostic specificity associated with either normal tension glaucoma or primary open angle glaucoma (POAG) 93.
A recent meta-analysis investigated differences in peripapillary choroidal thickness (PPCT) between primary open angle glaucoma (POAG), normal tension glaucoma, and healthy eyes 94. A systematic review of 18 studies, including 935 healthy control eyes, 446 normal tension glaucoma eyes, and 934 POAG eyes, was performed 94. OCT revealed significant reductions in peripapillary choroidal thickness (PPCT) in both POAG and normal tension glaucoma eyes compared with healthy eyes. POAG eyes demonstrated a mean reduction in peripapillary choroidal thickness (PPCT) of −16.32 µm compared to healthy controls, while normal tension glaucoma eyes showed a larger reduction of −34.96 µm compared to controls 94. Additionally, normal tension glaucoma eyes exhibited significantly thinner peripapillary choroidal thickness (PPCT) compared with POAG eyes, with a mean difference of −26.64 µm 94. These findings suggest that glaucomatous eyes, especially normal tension glaucoma eyes, have significantly reduced peripapillary choroidal thickness (PPCT), highlighting the potential role of peripapillary choroidal thickness (PPCT) as a diagnostic and monitoring tool in glaucoma management 94.
Pachymetry
Assessment of central corneal thickness (CCT) through pachymetry is essential in the work up of normal tension glaucoma 14. The measured intraocular pressure (IOP) by applanation may be artifactually low in eyes with low central corneal thickness (CCT) 14. Many patients with a diagnosis of normal tension glaucoma will demonstrate a low central corneal thickness (CCT) 95, 96. In some cases, correction of this under measurement may reveal an actual intraocular pressure (IOP) more consistent with primary open angle glaucoma (POAG) 95, 96.
Neurological Evaluation
At times, the diagnosis of normal tension glaucoma may simulate other neurological conditions. Most concerning to the clinician is an intracranial tumor masquerading as normal tension glaucoma. While these diagnoses are rare, clinicians should maintain a low threshold for neuroimaging with CT or MRI and a full neurological evaluation whenever the following exist 14:
- Marked asymmetry or unilateral optic nerve involvement
- Unexplained visual acuity loss
- Color vision deficits in the absence of visual field deficits
- Visual field defects not corresponding or out of proportion to optic nerve damage
- Vertically aligned visual field defects
- Atypical neurologic symptoms for glaucoma
- Optic nerve pallor in excess of cupping
- Age less than 50 years
Normal tension glaucoma differential diagnosis
Glaucomatous causes
- Primary open angle glaucoma with diurnal fluctuation between normal and elevated intraocular pressure (IOP)
- Intermittent acute angle closure glaucoma
- Tonometric underestimation of actual intraocular pressure (IOP) (e.g. thin central corneas)
- Resolved corticosteroid-induced, uveitic, or traumatic glaucoma
- Uveitic glaucoma/glaucomatocyclitic crisis (Posner-Schlossman)
- ‘Burned out’ pigmentary glaucoma
- Myopia with peripapillary atrophy
- Optic nerve coloboma or pits
- Congenital disc anomalies/cupping
Compressive, metabolic, toxic, inflammatory or infectious optic neuropathy causes
- Pituitary adenoma
- Meningioma
- Empty sella syndrome
- Leber’s optic atrophy
- Methanol optic neuropathy
- Optic neuritis
- Syphilis
Vascular injuries causes
- Giant cell arteritis
- Non-arteritic anterior ischemic optic neuropathy
- Posterior ischemic optic neuropathy
- Central retinal artery occlusion
- Carotid/ophthalmic artery occlusion 97
Normal tension glaucoma treatment
Management of normal tension glaucoma mirrors the medical and surgical management of the other forms of glaucoma and hinges on reduction of intraocular pressure (IOP) from baseline 14. Identification of patients with clinical evidence of progression is important in the decision to initiate treatment for normal tension glaucoma. The natural history of normal tension glaucoma does not always include progression without treatment. As initially described by Drance 13, a significant portion of patients with normal tension glaucoma may not demonstrate clinical progression regardless of treatment.These patients typically had a history of systemic vascular compromise resulting in a one-time insult to the optic nerve. Nonetheless, for the majority of patients with normal tension glaucoma, reduction of intraocular pressure (IOP) remains the focus of treatment.
The Collaborative Normal-Tension Glaucoma Study (CNTGS) 51, 58 demonstrated the benefit of intraocular pressure (IOP) reduction for the treatment of patients with normal tension glaucoma. The Collaborative Normal-Tension Glaucoma Study (CNTGS) concluded that a 30 percent reduction in baseline intraocular pressure (IOP) resulted in a reduced risk of disease progression 51, 58. Criteria for initiation of treatment of the normal tension glaucoma patients in this study were defined as: documented visual field or optic nerve progression, visual field loss threatening fixation, or presence of disc hemorrhage 51, 58. The treatment group had a 12% risk of progression at 5 years compared to 35% progressing in the non-treatment group 58. The Collaborative Normal-Tension Glaucoma Study (CNTGS) was therefore instrumental in demonstrating the role of IOP in the pathogenesis of normal tension glaucoma and the benefit of treatment to lower it. The Collaborative Normal-Tension Glaucoma Study (CNTGS) also presents a reasonable goal for treatment in 30% intraocular pressure (IOP) reduction from patient’s baseline. Treatment intraocular pressure (IOP) goals may then be modified over the course of treatment to a level that sufficiently prevents or slows progression of disease.
Outside of intraocular pressure (IOP) lowering therapy, other aspects should be considered in the management of normal tension glaucoma patients. This may include cardiovascular problems such as systemic hypotension, nocturnal hypotension, anemia, and cardiac arrhythmias that can compromise optic nerve head perfusion 14. Consultation with primary care physicians can be helpful in addressing these concerns, but limited evidence is available to confirm a treatment benefit for normal tension glaucoma 14.
Medications
Topical intraocular pressure (IOP) lowering medications including prostaglandin analogues, alpha-2 agonists, beta-blockers, carbonic anhydrase inhibitors, and more recently Rho-kinase inhibitors are the mainstays of normal tension glaucoma medical therapy 14. Medications should be chosen on an individual basis to provide treatment that achieves a sufficient intraocular pressure (IOP) reduction with minimal side effects and ease of administration. Medication choice should also be cost-effective for the patient based on their resources.
Particularly with normal tension glaucoma, the effect of medications on systemic blood pressure, heart rate, and optic nerve perfusion should be considered. Furthermore, medications that have neuroprotective or intraocular pressure (IOP) independent effects would be extremely beneficial and remain an ongoing search. The Low-Pressure Glaucoma Study (LoGTS) demonstrated the importance of intraocular pressure (IOP) independent factors when choosing medical therapy for normal tension glaucoma 98. In the Low-Pressure Glaucoma Study (LoGTS), patients with low-tension glaucoma were randomized to treatment with either brimonidine tartrate 0.2% or timolol maleate 0.5% 98. While intraocular pressure (IOP) reduction was similar between the two treatment groups, patients treated with brimonidine were less likely to have visual field progression compared to patients treated with timolol 98. It is unclear whether this difference is due to an additional neuroprotective effect of brimonidine or a detrimental vascular effect from timolol 98. Moreover, Rho-kinase inhibitors are thought to be neuroprotective and increase vascular flow at the optic nerve head via the nitric oxide pathway 99, 100. The newer class of Rho-kinase inhibitor showed efficacy in both intraocular pressure (IOP) reduction in normal tension glaucoma and as add-on treatment in normal tension glaucoma patients with inadequate baseline intraocular pressure (IOP). The Rho-kinase (ROCK) inhibitor class of medication blocks the contraction of trabecular meshwork cells and increases the outflow of aqueous humor, thereby reducing intraocular pressure (IOP) 101, 102.
In patients with evidence of vasospasm, calcium channel blockers have been proposed to stabilize vascular tone, particularly in patients with concurrent hypertension, though the benefit has not been evaluated in large clinical trials 14.
Medical follow up
Once medical treatment is initiated, patients should be followed up 6-8 weeks later to ensure good adherence, minimal side effects, and adequate intraocular pressure (IOP) lowering efficacy 14. Different medication classes, laser treatment or surgical therapy may be trialed until an appropriate treatment is found 14. Once treatment goals have been met, periodic measurement of IOP during medical therapy is recommended every 3-4 months to ensure maintenance of goal intraocular pressure (IOP) and absence of progression 14. New technology has allowed for patients to partake in home tonometry. Patients can frequently report their findings to their supervising ophthalmologists allowing for a more complete representation of intraocular pressure (IOP) mean, peak and range (numerous measurements can be taken throughout the day) and closer follow-up 14. In addition to intraocular pressure (IOP), patients should be monitored for signs of progression by periodic assessment of the optic nerve head (disc photos, HRT, OCT, etc.) and visual field testing every 6-12 months, with more frequent intervals in advanced or actively progressing disease 14. If progression is detected despite goal intraocular pressure (IOP), treatment goals should be lowered with advance of therapy to achieve them 14.
Surgery
Laser and surgical treatment options for normal tension glaucoma mirror those for primary open angle glaucoma (POAG) 14. These include laser trabeculoplasty, minimally invasive glaucoma surgery (MIGS), trabeculectomy, and glaucoma drainage devices.
Selective Laser trabeculoplasty (SLT) may be a useful moderately invasive treatment with or without medical therapy 14. There is some literature that supports an IOP lowering, and decreased IOP variability, effect of Selective Laser trabeculoplasty (SLT) in normal tension glaucoma patients 103. For patients with IOP targets that are not achievable with medical/laser therapy, filtration surgery with or without a drainage device has traditionally been the mainstay of surgically lowering IOP 14. However, recent trends and practice patterns according to the American Academy of Ophthalmology Intelligent Research Insight Registry (IRIS) reveal a significant increase in the use of minimally invasive glaucoma surgery (MIGS) procedures from 2013-2018, and normal tension glaucoma is no exception 104.
Minimally invasive glaucoma procedures such as goniotomy with Kahook Dual Blade (KDB), the iStent trabecular bypass device, and the XEN gel stent have demonstrated an important although limited role in the surgical management of normal tension glaucoma 14. In theory, angle-based MIGS procedures can only lower IOP to a level equal to or above episcleral venous pressure of approximately 8-11 mm Hg 14. Goal IOP for normal tension glaucoma patients may be below this level making it difficult to achieve treatment goals by surgical means alone 14. However, maintaining a goal IOP with fewer medications is a reasonable indication for minimally invasive glaucoma surgery (MIGS) in normal tension glaucoma. This rationale also applies to laser trabeculoplasty, which augments aqueous outflow to the downstream episcleral venous system as well. According to American Academy of Ophthalmology Intelligent Research Insight Registry (IRIS) data regarding initial surgery for normal tension glaucoma, iStent has been the most common performed surgery and minimally invasive glaucoma surgery (MIGS) procedures in general are performed at a higher rate than filtration surgeries for normal tension glaucoma 104.
In the Collaborative Normal-Tension Glaucoma Study (CNTGS), the IOP reduction of 30% was only achieved in 57% of patients by topical medication and/or laser trabeculoplasty, while the remaining 43% required filtering surgery 14. While IOP lowering with filtration surgery has been shown to be effective in decreasing visual field progression a continued, slowed progression has been reported in postoperative patients followed for up to 6 years 14.
A lower starting IOP with normal tension glaucoma patients and a 30% reduction target may result in a narrower margin between therapeutic IOP reduction and hypotony in these patients 14. Increase risk of filtering surgery complications has been reported in this subset of primary open angle glaucoma (POAG) patients 14.
Selection of anti-metabolite drugs and means of application in filtering surgery is an important consideration and should be guided by specific treatment goals and surgeon specific experience with these agents 14. Mitomycin C (MMC) has been associated with achievement of lower IOPs post operatively compared to 5-fluorouracil (5-FU) in some studies, though literature also suggests equivalence of efficacy of these two agents in primary trabeculectomy for primary open angle glaucoma (POAG) 14. Mitomycin C use in normal tension glaucoma glaucoma has an associated increased risk of over-filtration complications that may play a role in the risk of visual field progression. Therefore, meticulous use of mitomycin C (e.g. 0.2-0.4 mg/ml for 1-3 minutes), careful flap suturing, and judicious use of viscoelastic with frequent postoperative follow up have been proposed as methods to mitigate the risks of hypotony early in the post operative phase while achieving target IOP 14. Early suture lysis may be required to achieve low target IOPs but should be weighed against the risk of resultant over-filtration. Given the context of a higher risk of hypotony following filtering surgery in patients with normal tension glaucoma, the XEN gel stent has recently been deployed to achieve a lower IOP goal while maintaining a lower rate of hypotony 14. One recent study demonstrated a mean IOP decrease of 5.6 +/- 2.7 mmHg in normal tension glaucoma patients, which represented an IOP reduction of 29% 105. Also, the use of the EX-PRESS glaucoma mini shunt has been employed as a means of preventing complications, while still achieving similar IOP goals compared to standard trabeculectomy 14. In one experience, the smaller, consistent outflow opening of the EX-PRESS shunt allows for earlier suture lysis to achieve low IOP targets with less risk of hypotony 14. The utility of this device remains an area of debate considering the additional cost of the device and mixed outcomes in the literature 14.
Cyclodestructive procedures provide the only surgical means of suppressing aqueous production to lower IOP. Due to their potentially vision threatening side effects, these procedures are typically reserved for eyes refractory to treatment or with poor visual potential 14. Ablation of the ciliary processes may be accomplished by transscleral cyclophotocoagulation (CPC) or by endoscopic cyclophotocoagulation (ECP) 14. Endoscopic cyclophotocoagulation (ECP) offers the unique advantage of direct visualization of the target tissue allowing a more targeted approach to achieve less inflammation and side effects 14.
A recent systematic review and meta-analysis evaluated the efficacy of angle-based minimally invasive glaucoma surgery (MIGS) in patients with normal tension glaucoma 106. The study analyzed outcomes from 15 studies, totaling 367 normal tension glaucoma eyes, with procedures including the iStent, iStent inject, Hydrus Microstent, Kahook Dual Blade, and Trabectome 106. The review found significant reductions in IOP and glaucoma medication usage postoperatively 106. Specifically, combined phacoemulsification and angle-based MIGS showed a mean IOP reduction of 2.44 mmHg at 6 months, 2.28 mmHg at 12 months, and sustained reductions up to 36 months 106. Glaucoma medication usage was also significantly reduced by 1.21 medications at 6 months and 1.18 at 12 months postoperatively. These findings suggest that angle-based MIGS, particularly in combination with cataract surgery, can be effective in reducing IOP and medication burden in normal tension glaucoma patients while maintaining a favorable safety profile 106.
Normal tension glaucoma prognosis
Like any form of glaucoma, normal tension glaucoma may progress to irreversible blindness, but is dependent on factors that include the disease severity at diagnosis, effectiveness of treatment, individual risk factors, overall ocular health and your general health 107, 108, 109, 110, 111, 1, 14. Similar to other types of glaucoma, normal tension glaucoma can progress to irreversible unilateral or bilateral blindness in the worst cases, even despite therapy 108. The prognosis for visual preservation is good in patients who undergo adequate treatment through intraocular pressure (IOP) reduction 14. The main risk factors associated with the normal tension glaucoma disease progression in both treated and untreated patients have been demonstrated to be female gender, greater variation in diurnal IOP and diastolic blood pressure, presence of disk hemorrhage, greater vertical cup/disc ratio and migraine at baseline 2. Age, mean IOP and baseline IOP were not shown to be risk factors for progression 2. Epidemiology studies have shown that Asians tend to show a slower rate of disease progression 107, 109, 110, 111. On average, the visual field damage progression has been reported to be slower in normal tension glaucoma than in primary open angle glaucoma (POAG), but with higher inter-patient variability 110.
The cumulative risk to develop legal unilateral blindness in treated normal tension glaucoma patients under standard ophthalmic care has been calculated to be 5.8% and 9.9% at 10 years and 20 years, respectively 2. The risk for bilateral blindness at 10 and 20 years was 0.3% and 1.4%, respectively 108. Patients presenting advanced damage at the diagnosis or rapidly progressing visual field loss, the so-called “rapid progressors”, are most likely to become blind due to the disease 2. It is fundamental that these patients need to be identified and managed with more aggressive treatment to avoid irreversible visual loss 108.
In the Collaborative Normal-Tension Glaucoma Study (CNTGS), 65% of patients in the control group with normal tension glaucoma did not progress even without treatment 58, 51. However, an intraocular pressure (IOP) reduction of 30% with treatment further lowered the likelihood of progression to only 12% 58, 51. The Early Manifest Glaucoma Trial (EMGT), a randomized double-masked clinical trial conducted on 255 open-angle glaucoma patients with early visual field defects, including 53% of normal tension glaucoma cases, showed that a 25% reduction in IOP can reduce the risk of disease progression to 45% in the study group, compared to 62% in the control group, after a 6-year follow-up 30. These studies have suggested that, to be significantly effective in decreasing the risk of normal tension glaucoma progression, the reduction in IOP should be at least 30% or more 112, 29. Moreover, studies with long follow-ups have shown that the amount of IOP reduction seems to be directly related to the reduction in the visual field progression rate in normal tension glaucoma patients 32. Additionally, the benefits of the IOP reduction in normal tension glaucoma patients seem to be significantly higher in females with migraine and a family history of glaucoma, without disk hemorrhages, family history of stroke and personal history of cardiovascular disease 109.
Patients with normal tension glaucoma that previously suffered an acute vascular compromise have also been shown to not progress over time as well 13. Given this relatively high rate of non-progression, some clinicians have suggested a conservative “wait and see” approach to initiating treatment 14. This recommendation should be cautioned, as it is often difficult to determine which patients will progress, and other studies have shown variable rates of progression in this disease 14. Risk factors for progression of visual field defects in normal tension glaucoma include migraine, disc hemorrhage, and female gender. Asians have been shown to have a slower rate of progression 84.
- Gosling D, Meyer JJ. Normal Tension Glaucoma. [Updated 2022 Dec 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK576377[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Salvetat ML, Pellegrini F, Spadea L, Salati C, Zeppieri M. Pharmaceutical Approaches to Normal Tension Glaucoma. Pharmaceuticals (Basel). 2023 Aug 17;16(8):1172. doi: 10.3390/ph16081172[↩][↩][↩][↩][↩][↩]
- Shields MB. Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol. 2008 Mar;19(2):85-8. doi: 10.1097/ICU.0b013e3282f3919b[↩][↩]
- Lee BL, Bathija R, Weinreb RN. The definition of normal-tension glaucoma. J Glaucoma. 1998 Dec;7(6):366-71.[↩]
- Van Buskirk EM. The tale of normal-tension glaucoma. J Glaucoma. 1998 Dec;7(6):363-5.[↩]
- Sowka J. New thoughts on normal tension glaucoma. Optometry. 2005 Oct;76(10):600-8. doi: 10.1016/j.optm.2005.08.020[↩]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. British Journal of Ophthalmology 2021;105:1-169. doi: 10.1136/bjophthalmol-2021-egsguidelines[↩]
- Gedde SJ, Vinod K, Wright MM, Muir KW, Lind JT, Chen PP, Li T, Mansberger SL; American Academy of Ophthalmology Preferred Practice Pattern Glaucoma Panel. Primary Open-Angle Glaucoma Preferred Practice Pattern®. Ophthalmology. 2021 Jan;128(1):P71-P150. doi: 10.1016/j.ophtha.2020.10.022[↩]
- Wu AM, Wu CM, Young BK, Wu DJ, Chen A, Margo CE, Greenberg PB. Evaluation of primary open-angle glaucoma clinical practice guidelines. Can J Ophthalmol. 2015 Jun;50(3):192-6. doi: 10.1016/j.jcjo.2015.03.005[↩]
- Asia-Pacific Glaucoma Society (APGS) Amsterdam, The Netherlands: Kugler Publications, 3th Edition. 2016. http://medi-guide.meditool.cn/ymtpdf/80C3C8C0-BED9-6460-F2FA-8C56BBF88EDF.pdf[↩]
- Kiuchi Y, Inoue T, Shoji N, Nakamura M, Tanito M; Glaucoma Guideline Preparation Committee, Japan Glaucoma Society. The Japan Glaucoma Society guidelines for glaucoma 5th edition. Jpn J Ophthalmol. 2023 Mar;67(2):189-254. doi: 10.1007/s10384-022-00970-9[↩]
- Colton T, Ederer F. The distribution of intraocular pressures in the general population. Surv Ophthalmol. 1980 Nov-Dec;25(3):123-9. doi: 10.1016/0039-6257(80)90086-7[↩]
- Drance SM, Morgan RW, Sweeney VP. Shock-induced optic neuropathy: a cause of nonprogressive glaucoma. N Engl J Med. 1973 Feb 22;288(8):392-5. doi: 10.1056/NEJM197302222880804[↩][↩][↩]
- Normal Tension Glaucoma. https://eyewiki.org/Normal_Tension_Glaucoma[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Tomita G. The optic nerve head in normal-tension glaucoma. Curr Opin Ophthalmol. 2000 Apr;11(2):116-20. doi: 10.1097/00055735-200004000-00009[↩]
- Drance SM. Disc hemorrhages in the glaucomas. Surv Ophthalmol. 1989 Mar-Apr;33(5):331-7. doi: 10.1016/0039-6257(89)90010-6[↩][↩][↩]
- Uhler TA, Piltz-Seymour J. Optic disc hemorrhages in glaucoma and ocular hypertension: implications and recommendations. Curr Opin Ophthalmol. 2008 Mar;19(2):89-94. doi: 10.1097/ICU.0b013e3282f3e6bc[↩][↩]
- Budenz DL, Anderson DR, Feuer WJ, Beiser JA, Schiffman J, Parrish RK 2nd, Piltz-Seymour JR, Gordon MO, Kass MA; Ocular Hypertension Treatment Study Group. Detection and prognostic significance of optic disc hemorrhages during the Ocular Hypertension Treatment Study. Ophthalmology. 2006 Dec;113(12):2137-43. doi: 10.1016/j.ophtha.2006.06.022[↩][↩]
- Schacknow PN, Samples JR eds. The glaucoma book: a practical, evidence-based approach to patient care. New York: Springer; 2010.[↩][↩]
- Optic Disc Hemorrhage. https://eyewiki.org/Optic_Disc_Hemorrhage[↩]
- Kosior-Jarecka E, Wróbel-Dudzińska D, Łukasik U, Żarnowski T. Ocular and Systemic Risk Factors of Different Morphologies of Scotoma in Patients with Normal-Tension Glaucoma. J Ophthalmol. 2017;2017:1480746. doi: 10.1155/2017/1480746[↩]
- Kottler MS, Drance SM. Studies of hemorrhage on the optic disc. Can J Ophthalmol. 1976 Apr;11(2):102-5.[↩]
- Anderson DR; Normal Tension Glaucoma Study. Collaborative normal tension glaucoma study. Curr Opin Ophthalmol. 2003 Apr;14(2):86-90. doi: 10.1097/00055735-200304000-00006[↩]
- Mullany S, Xiao L, Qassim A, Marshall H, Gharahkhani P, MacGregor S, Hassall MM, Siggs OM, Souzeau E, Craig JE. Normal-tension glaucoma is associated with cognitive impairment. Br J Ophthalmol. 2022 Jul;106(7):952-956. doi: 10.1136/bjophthalmol-2020-317461[↩][↩]
- Crump C, Sundquist J, Sieh W, Sundquist K. Risk of Alzheimer’s Disease and Related Dementias in Persons with Glaucoma: A National Cohort Study. Ophthalmology. 2024 Mar;131(3):302-309. doi: 10.1016/j.ophtha.2023.10.014[↩][↩]
- Klein B.E., Klein R., Sponsel W.E., Franke T., Cantor L.B., Martone J., Menage M.J. Prevalence of glaucoma. The Beaver Dam Eye Study. Ophthalmology. 1992;99:1499–1504. doi: 10.1016/S0161-6420(92)31774-9[↩]
- Leung DYL, Tham CC. Normal-tension glaucoma: Current concepts and approaches-A review. Clin Exp Ophthalmol. 2022 Mar;50(2):247-259. doi: 10.1111/ceo.14043[↩][↩]
- Zhao J., Solano M.M., Oldenburg C.E., Liu T., Wang Y., Wang N., Lin S.C. Prevalence of Normal-Tension Glaucoma in the Chinese Population: A Systematic Review and Meta-Analysis. Am. J. Ophthalmol. 2019;199:101–110. doi: 10.1016/j.ajo.2018.10.017[↩]
- Collaborative Normal-Tension Glaucoma Study Group The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Am. J. Ophthalmol. 1998;126:498–505. doi: 10.1016/S0002-9394(98)00272-4[↩][↩][↩]
- Heijl A., Leske M.C., Bengtsson B., Hyman L., Bengtsson B., Hussein M., Early Manifest Glaucoma Trial Group Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002;120:1268–1279. doi: 10.1001/archopht.120.10.1268[↩][↩]
- Killer H.E., Pircher A. Normal tension glaucoma: Review of current understanding and mechanisms of the pathogenesis. Eye Lond. 2018;32:924–930. doi: 10.1038/s41433-018-0042-2[↩]
- Razeghinejad M.R., Lee D. Managing normal tension glaucoma by lowering the intraocular pressure. Surv. Ophthalmol. 2019;64:111–116. doi: 10.1016/j.survophthal.2018.07.003[↩][↩][↩][↩][↩][↩]
- Lusthaus J., Goldberg I. Current management of glaucoma. Med. J. Aust. 2019;210:180–187. doi: 10.5694/mja2.50020[↩]
- Hoyng P.F., Kitazawa Y. Medical treatment of normal tension glaucoma. Surv. Ophthalmol. 2002;47, Suppl. S1:S116–S124. doi: 10.1016/S0039-6257(02)00322-3[↩][↩]
- Kim J.M., Sung K.R., Kim H.K., Park S.W., Lee E.J., Jeoung J.W., Park H.L., Ahn J., Yoo C., Kim C.Y. Long-Term Effectiveness and Safety of Tafluprost, Travoprost, and Latanoprost in Korean Patients with Primary Open-Angle Glaucoma or Normal-Tension Glaucoma: A Multicenter Retrospective Cohort Study (LOTUS Study) J. Clin. Med. 2021;10:2717. doi: 10.3390/jcm10122717[↩]
- Islam S, Spry C. Prostaglandin Analogues for Ophthalmic Use: A Review of Comparative Clinical Effectiveness, Cost-Effectiveness, and Guidelines [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2020 Feb 18. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562924[↩][↩]
- Quaranta L., Katsanos A., Russo A., Riva I. 24-hour intraocular pressure and ocular perfusion pressure in glaucoma. Surv. Ophthalmol. 2013;58:26–41. doi: 10.1016/j.survophthal.2012.05.003[↩]
- McKibbin M., Menage M.J. The effect of once-daily latanoprost on intraocular pressure and pulsatile ocular blood flow in normal tension glaucoma. Pt 1Eye Lond. 1999;13:31–34. doi: 10.1038/eye.1999.6[↩]
- Araie M., Mayama C. Use of calcium channel blockers for glaucoma. Prog. Retin. Eye Res. 2011;30:54–71. doi: 10.1016/j.preteyeres.2010.09.002[↩]
- Dinakaran S., Mehta P., Mehta R., Tilva B., Arora D., Tejwani S. Significance of non-intraocular pressure (IOP)-related factors particularly in normal tension glaucoma: Looking beyond IOP. Indian J. Ophthalmol. 2022;70:569–573. doi: 10.4103/ijo.IJO_861_21[↩][↩]
- Shin J.W., Jo Y.H., Song M.K., Won H.J., Kook M.S. Nocturnal blood pressure dip and parapapillary choroidal microvasculature dropout in normal-tension glaucoma. Sci. Rep. 2021;11:206. doi: 10.1038/s41598-020-80705-3[↩]
- Shen J., Wang Y., Yao K. Protection of retinal ganglion cells in glaucoma: Current status and future. Exp. Eye Res. 2021;205:108506. doi: 10.1016/j.exer.2021.108506[↩]
- Krupin T., Liebmann J.M., Greenfield D.S., Ritch R., Gardiner S., Low-Pressure Glaucoma Study Group A randomized trial of brimonidine versus timolol in preserving visual function: Results from the Low-Pressure Glaucoma Treatment Study. Am. J. Ophthalmol. 2011;151:671–681. doi: 10.1016/j.ajo.2010.09.026. Erratum in Am. J. Ophthalmol. 2011, 151, 1108[↩]
- Nocentini A., Supuran C.T. Adrenergic agonists and antagonists as antiglaucoma agents: A literature and patent review (2013–2019) Expert Opin. Ther. Pat. 2019;29:805–815. doi: 10.1080/13543776.2019.1665023[↩]
- Liu B., Liu Y.J. Carvedilol Promotes Retinal Ganglion Cell Survival Following Optic Nerve Injury via ASK1-p38 MAPK Pathway. CNS Neurol. Disord Drug Targets. 2019;18:695–704. doi: 10.2174/1871527318666191002095456[↩]
- Szumny D., Szeląg A. The influence of new beta-adrenolytics nebivolol and carvedilol on intraocular pressure and iris blood flow in rabbits. Graefes Arch. Clin. Exp. Ophthalmol. 2014;252:917–923. doi: 10.1007/s00417-014-2623-5[↩]
- Oh D.J., Chen J.L., Vajaranant T.S., Dikopf M.S. Brimonidine tartrate for the treatment of glaucoma. Expert Opin. Pharmacother. 2019;20:115–122. doi: 10.1080/14656566.2018.1544241[↩]
- Schulzer M., The Normal Tension Glaucoma Study Group Intraocular pressure reduction in normal-tension glaucoma patients. Ophthalmology. 1992;99:1468–1470. doi: 10.1016/S0161-6420(92)31782-8[↩]
- Shahror, R.A., Morris, C.A., Mohammed, A.A. et al. Role of myeloid cells in ischemic retinopathies: recent advances and unanswered questions. J Neuroinflammation 21, 65 (2024). https://doi.org/10.1186/s12974-024-03058-y[↩]
- Optic disc hemorrhage in normal tension glaucoma. https://eyerounds.org/atlas/pages/Optic-Disc-Hemorrhage-in-NTG.htm#gsc.tab=0[↩]
- The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Collaborative Normal-Tension Glaucoma Study Group. Am J Ophthalmol. 1998 Oct;126(4):498-505. doi: 10.1016/s0002-9394(98)00272-4[↩][↩][↩][↩][↩][↩][↩]
- Heijl A, Leske MC, Bengtsson B, et al. Reduction of Intraocular Pressure and Glaucoma Progression: Results From the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268[↩][↩]
- Mozaffarieh M, Flammer J. New insights in the pathogenesis and treatment of normal tension glaucoma. Curr Opin Pharmacol. 2013 Feb;13(1):43-9. doi: 10.1016/j.coph.2012.10.001[↩]
- Crawford Downs J, Roberts MD, Sigal IA. Glaucomatous cupping of the lamina cribrosa: a review of the evidence for active progressive remodeling as a mechanism. Exp Eye Res. 2011 Aug;93(2):133-40. doi: 10.1016/j.exer.2010.08.004[↩]
- Wostyn P, Killer HE. Normal-Tension Glaucoma: A Glymphopathy? Eye Brain. 2023 Apr 6;15:37-44. doi: 10.2147/EB.S401306[↩]
- Pan Y, Iwata T. Molecular genetics of inherited normal tension glaucoma. Indian J Ophthalmol. 2024 May 1;72(Suppl 3):S335-S344. doi: 10.4103/IJO.IJO_3204_23[↩][↩][↩][↩]
- Adeghate J, Rahmatnejad K, Waisbourd M, Katz LJ. Intraocular pressure-independent management of normal tension glaucoma. Surv Ophthalmol. 2019 Jan-Feb;64(1):101-110. doi: 10.1016/j.survophthal.2018.08.005[↩]
- Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Collaborative Normal-Tension Glaucoma Study Group. Am J Ophthalmol. 1998 Oct;126(4):487-97. doi: 10.1016/s0002-9394(98)00223-2. Erratum in: Am J Ophthalmol 1999 Jan;127(1):120.[↩][↩][↩][↩][↩][↩][↩]
- Holländer R. Der Einfluss der Membranpermeabilität auf die TMPD-Oxydase-Aktivität bei Bakterien [The Influence of the Permeability of the Cell Membrane on TMPD Oxydase Activity (author’s transl)]. Zentralbl Bakteriol Orig A. 1977;237(2-3):351-7. German.[↩]
- Hirooka K, Tenkumo K, Fujiwara A, Baba T, Sato S, Shiraga F. Evaluation of peripapillary choroidal thickness in patients with normal-tension glaucoma. BMC Ophthalmol. 2012 Jul 28;12:29. doi: 10.1186/1471-2415-12-29[↩]
- Firat PG, Ozsoy E, Demirel S, Cumurcu T, Gunduz A. Evaluation of peripapillary retinal nerve fiber layer, macula and ganglion cell thickness in amblyopia using spectral optical coherence tomography. Int J Ophthalmol. 2013;6(1):90-4. doi: 10.3980/j.issn.2222-3959.2013.01.19[↩]
- Zheng Y, Cheung N, Aung T, Mitchell P, He M, Wong TY. Relationship of retinal vascular caliber with retinal nerve fiber layer thickness: the singapore malay eye study. Invest Ophthalmol Vis Sci. 2009 Sep;50(9):4091-6. doi: 10.1167/iovs.09-3444[↩]
- Kim JM, Sae Kim M, Ju Jang H, Ho Park K, Caprioli J. The association between retinal vessel diameter and retinal nerve fiber layer thickness in asymmetric normal tension glaucoma patients. Invest Ophthalmol Vis Sci. 2012 Aug 17;53(9):5609-14. doi: 10.1167/iovs.12-9783[↩]
- Lee JY, Yoo C, Park JH, Kim YY. Retinal vessel diameter in young patients with open-angle glaucoma: comparison between high-tension and normal-tension glaucoma. Acta Ophthalmol. 2012 Nov;90(7):e570-1. doi: 10.1111/j.1755-3768.2011.02371.x[↩]
- Fox AR, Fingert JH. Familial normal tension glaucoma genetics. Prog Retin Eye Res. 2023 Sep;96:101191. doi: 10.1016/j.preteyeres.2023.101191[↩]
- Burk RO, Rohrschneider K, Noack H, Völcker HE. Are large optic nerve heads susceptible to glaucomatous damage at normal intraocular pressure? A three-dimensional study by laser scanning tomography. Graefes Arch Clin Exp Ophthalmol. 1992;230(6):552-60. doi: 10.1007/BF00181778[↩]
- Tuulonen A, Takamoto T, Wu DC, Schwartz B. Optic disk cupping and pallor measurements of patients with a disk hemorrhage. Am J Ophthalmol. 1987 Apr 15;103(4):505-11. doi: 10.1016/s0002-9394(14)74272-2[↩]
- Vogel W, Dietze O, Judmaier G, Then P, Schmid T, Margreiter R. Delayed clearance of HBsAG after transplantation for fulminant delta-hepatitis. Lancet. 1988 Jan 2-9;1(8575-6):52. doi: 10.1016/s0140-6736(88)91025-2[↩]
- Buus DR, Anderson DR. Peripapillary crescents and halos in normal-tension glaucoma and ocular hypertension. Ophthalmology. 1989 Jan;96(1):16-9. doi: 10.1016/s0161-6420(89)32930-7[↩]
- Yamazaki Y, Hayamizu F, Miyamoto S, Nakagami T, Tanaka C, Inui S. Optic disc findings in normal tension glaucoma. Jpn J Ophthalmol. 1997 Jul-Aug;41(4):260-7. doi: 10.1016/s0021-5155(97)00052-x[↩]
- Gramer E, Leydhecker W. Glaukom ohne Hochdruck. Eine klinische Studie [Glaucoma without ocular hypertension. A clinical study]. Klin Monbl Augenheilkd. 1985 Apr;186(4):262-7. German. doi: 10.1055/s-2008-1050918[↩][↩]
- Krupin T, Liebmann JM, Greenfield DS, Ritch R, Gardiner S; Low-Pressure Glaucoma Study Group. A randomized trial of brimonidine versus timolol in preserving visual function: results from the Low-Pressure Glaucoma Treatment Study. Am J Ophthalmol. 2011 Apr;151(4):671-81. doi: 10.1016/j.ajo.2010.09.026 Erratum in: Am J Ophthalmol. 2011 Jun;151(6):1108.[↩]
- Chuang LH, Koh YY, Chen HSL, Lo YL, Yu CC, Yeung L, Lai CC. Normal tension glaucoma in obstructive sleep apnea syndrome: A structural and functional study. Medicine (Baltimore). 2020 Mar;99(13):e19468. doi: 10.1097/MD.0000000000019468[↩]
- Lin PW, Friedman M, Lin HC, Chang HW, Wilson M, Lin MC. Normal tension glaucoma in patients with obstructive sleep apnea/hypopnea syndrome. J Glaucoma. 2011 Dec;20(9):553-8. doi: 10.1097/IJG.0b013e3181f3eb81[↩]
- Bilgin G. Normal-tension glaucoma and obstructive sleep apnea syndrome: a prospective study. BMC Ophthalmol. 2014 Mar 10;14:27. doi: 10.1186/1471-2415-14-27[↩]
- Leggewie B, Gouveris H, Bahr K. A Narrative Review of the Association between Obstructive Sleep Apnea and Glaucoma in Adults. Int J Mol Sci. 2022 Sep 3;23(17):10080. doi: 10.3390/ijms231710080[↩]
- Phelps CD, Corbett JJ. Migraine and low-tension glaucoma. A case-control study. Invest Ophthalmol Vis Sci. 1985 Aug;26(8):1105-8. https://iovs.arvojournals.org/article.aspx?articleid=2159734[↩]
- Flammer J, Konieczka K, Flammer AJ. The primary vascular dysregulation syndrome: implications for eye diseases. EPMA J. 2013 Jun 7;4(1):14. doi: 10.1186/1878-5085-4-14[↩]
- Hirooka K, Higashide T, Sakaguchi K, Udagawa S, Sugiyama K, Oki K, Kometani M, Yoneda T, Fukunaga K, Akita T, Baba T, Kiuchi Y. Prevalence of Normal-Tension Glaucoma in Patients With Primary Aldosteronism. Am J Ophthalmol. 2025 Jan;269:339-345. doi: 10.1016/j.ajo.2024.09.014[↩][↩][↩]
- Ho K, Bodi NE, Sharma TP. Normal-Tension Glaucoma and Potential Clinical Links to Alzheimer’s Disease. J Clin Med. 2024 Mar 27;13(7):1948. doi: 10.3390/jcm13071948[↩][↩][↩]
- Fan N, Tan J, Liu X. Is “normal tension glaucoma” glaucoma? Med Hypotheses. 2019 Dec;133:109405. doi: 10.1016/j.mehy.2019.109405[↩]
- Killer HE, Pircher A. Normal tension glaucoma: review of current understanding and mechanisms of the pathogenesis. Eye (Lond). 2018 May;32(5):924-930. doi: 10.1038/s41433-018-0042-2[↩][↩]
- Chen YY, Lai YJ, Yen YF, Shen YC, Wang CY, Liang CY, Lin KH, Fan LW. Association between normal tension glaucoma and the risk of Alzheimer’s disease: a nationwide population-based cohort study in Taiwan. BMJ Open. 2018 Nov 5;8(11):e022987. doi: 10.1136/bmjopen-2018-022987[↩]
- Drance S, Anderson DR, Schulzer M; Collaborative Normal-Tension Glaucoma Study Group. Risk factors for progression of visual field abnormalities in normal-tension glaucoma. Am J Ophthalmol. 2001 Jun;131(6):699-708. doi: 10.1016/s0002-9394(01)00964-3[↩][↩]
- Konieczka K, Ritch R, Traverso CE, Kim DM, Kook MS, Gallino A, Golubnitschaja O, Erb C, Reitsamer HA, Kida T, Kurysheva N, Yao K. Flammer syndrome. EPMA J. 2014 Jul 8;5(1):11. doi: 10.1186/1878-5085-5-11[↩]
- Xie Y, Jiang J, Liu C, Lin H, Wang L, Zhang C, Chen J, Liang Y, Congdon N, Zhang S. Performance of a Glaucoma Screening Program Compared With Opportunistic Detection in China. J Glaucoma. 2023 Feb 1;32(2):80-84. doi: 10.1097/IJG.0000000000002125[↩][↩][↩][↩]
- Normal Tension Glaucoma. https://glaucoma.org.au/what-is-glaucoma/types-of-glaucoma/normal-tension-glaucoma[↩][↩]
- Quigley HA. Glaucoma. Lancet. 2011 Apr 16;377(9774):1367-77. doi: 10.1016/S0140-6736(10)61423-7[↩]
- Lawlor M, Quartilho A, Bunce C, Nathwani N, Dowse E, Kamal D, Gazzard G. Patients With Normal Tension Glaucoma Have Relative Sparing of the Relative Afferent Pupillary Defect Compared to Those With Open Angle Glaucoma and Elevated Intraocular Pressure. Invest Ophthalmol Vis Sci. 2017 Oct 1;58(12):5237-5241. doi: 10.1167/iovs.17-21688[↩]
- Spaeth GL, Henderer J, Liu C, Kesen M, Altangerel U, Bayer A, Katz LJ, Myers J, Rhee D, Steinmann W. The disc damage likelihood scale: reproducibility of a new method of estimating the amount of optic nerve damage caused by glaucoma. Trans Am Ophthalmol Soc. 2002;100:181-5; discussion 185-6[↩]
- Mahmoudinezhad G, Moghimi S, Proudfoot JA, Brye N, Nishida T, Yarmohammadi A, Kamalipour A, Zangwill LM, Weinreb RN. Effect of Testing Frequency on the Time to Detect Glaucoma Progression With Optical Coherence Tomography (OCT) and OCT Angiography. Am J Ophthalmol. 2023 Jan;245:184-192. doi: 10.1016/j.ajo.2022.08.030[↩]
- What Is Fluorescein Angiography? https://www.aao.org/eye-health/treatments/what-is-fluorescein-angiography[↩]
- Seo SB, Cho HK. Deep learning classification of early normal-tension glaucoma and glaucoma suspects using Bruch’s membrane opening-minimum rim width and RNFL. Sci Rep. 2020 Nov 4;10(1):19042. doi: 10.1038/s41598-020-76154-7[↩][↩]
- Betzler BK, Siat DJY, Agrawal R, Dorairaj S, Ang BCH. Comparison of Peripapillary Choroidal Thickness Between Primary Open-angle Glaucoma, Normal Tension Glaucoma, and Normal Eyes: A Systematic Review and Meta-analysis. Ophthalmol Glaucoma. 2024 Jul-Aug;7(4):359-371. doi: 10.1016/j.ogla.2024.02.008[↩][↩][↩][↩][↩]
- Shih CY, Graff Zivin JS, Trokel SL, Tsai JC. Clinical significance of central corneal thickness in the management of glaucoma. Arch Ophthalmol. 2004 Sep;122(9):1270-5. doi: 10.1001/archopht.122.9.1270[↩][↩]
- Shetgar AC, Mulimani MB. The central corneal thickness in normal tension glaucoma, primary open angle glaucoma and ocular hypertension. J Clin Diagn Res. 2013 Jun;7(6):1063-7. doi: 10.7860/JCDR/2013/4292.3022[↩][↩]
- Tsai, J. and M.A. Karim, Current concepts in normal tension glaucoma. Review of Ophthalmology, 2006. 6(24).[↩]
- Krupin T, Liebmann JM, Greenfield DS, Ritch R, Gardiner S; Low-Pressure Glaucoma Study Group. A randomized trial of brimonidine versus timolol in preserving visual function: results from the Low-Pressure Glaucoma Treatment Study. Am J Ophthalmol. 2011 Apr;151(4):671-81. doi: 10.1016/j.ajo.2010.09.026. Erratum in: Am J Ophthalmol. 2011 Jun;151(6):1108.[↩][↩][↩][↩]
- Tanna AP, Johnson M. Rho Kinase Inhibitors as a Novel Treatment for Glaucoma and Ocular Hypertension. Ophthalmology. 2018 Nov;125(11):1741-1756. doi: 10.1016/j.ophtha.2018.04.040[↩]
- Thomas NM, Nagrale P. Rho Kinase Inhibitors as a Neuroprotective Pharmacological Intervention for the Treatment of Glaucoma. Cureus. 2022 Aug 26;14(8):e28445. doi: 10.7759/cureus.28445[↩]
- Chihara E, Dimitrova G, Chihara T. Increase in the OCT angiographic peripapillary vessel density by ROCK inhibitor ripasudil instillation: a comparison with brimonidine. Graefes Arch Clin Exp Ophthalmol. 2018 Jul;256(7):1257-1264. doi: 10.1007/s00417-018-3945-5[↩]
- Kaneko Y, Ohta M, Inoue T, Mizuno K, Isobe T, Tanabe S, Tanihara H. Effects of K-115 (Ripasudil), a novel ROCK inhibitor, on trabecular meshwork and Schlemm’s canal endothelial cells. Sci Rep. 2016 Jan 19;6:19640. doi: 10.1038/srep19640[↩]
- El Mallah MK, Walsh MM, Stinnett SS, Asrani SG. Selective laser trabeculoplasty reduces mean IOP and IOP variation in normal tension glaucoma patients. Clin Ophthalmol. 2010 Aug 9;4:889-93. doi: 10.2147/opth.s11787[↩]
- Yang SA, Mitchell WG, Hall N, Elze T, Miller JW, Lorch AC, Zebardast N. Usage Patterns of Minimally Invasive Glaucoma Surgery (MIGS) Differ by Glaucoma Type: IRIS Registry Analysis 2013-2018. Ophthalmic Epidemiol. 2022 Aug;29(4):443-451. doi: 10.1080/09286586.2021.1955391[↩][↩]
- Schargus M, Theilig T, Rehak M, Busch C, Bormann C, Unterlauft JD. Outcome of a single XEN microstent implant for glaucoma patients with different types of glaucoma. BMC Ophthalmol. 2020 Dec 17;20(1):490. doi: 10.1186/s12886-020-01764-8[↩]
- Oo HH, Hong ASY, Lim SY, Ang BCH. Angle-based minimally invasive glaucoma surgery in normal tension glaucoma: A systematic review and meta-analysis. Clin Exp Ophthalmol. 2024 Sep-Oct;52(7):740-760. doi: 10.1111/ceo.14408[↩][↩][↩][↩][↩]
- Baek S.U., Ha A., Kim D.W., Jeoung J.W., Park K.H., Kim Y.K. Risk factors for disease progression in low-teens normal-tension glaucoma. Br. J. Ophthalmol. 2020;104:81–86. doi: 10.1136/bjophthalmol-2018-313375[↩][↩]
- Sawada A., Rivera J.A., Takagi D., Nishida T., Yamamoto T. Progression to Legal Blindness in Patients with Normal Tension Glaucoma: Hospital-Based Study. Investig. Ophthalmol. Vis. Sci. 2015;56:3635–3641. doi: 10.1167/iovs.14-16093[↩][↩][↩][↩]
- Anderson D.R., Drance S.M., Schulzer M., Collaborative Normal-Tension Glaucoma Study Group Factors that predict the benefit of lowering intraocular pressure in normal tension glaucoma. Am. J. Ophthalmol. 2003;136:820–829. doi: 10.1016/S0002-9394(03)00478-1[↩][↩][↩]
- Bach-Holm D., Jensen P.K., Kessing S.V. Long-term rate of progression and target intraocular pressure in patients with normal-tension glaucoma in clinical care. Acta Ophthalmol. 2018;96:e1034–e1035. doi: 10.1111/aos.13767[↩][↩][↩]
- Sakata R., Yoshitomi T., Iwase A., Matsumoto C., Higashide T., Shirakashi M., Aihara M., Sugiyama K., Araie M., Lower Normal Pressure Glaucoma Study Members in Japan Glaucoma Society Factors Associated with Progression of Japanese Open-Angle Glaucoma with Lower Normal Intraocular Pressure. Ophthalmology. 2019;126:1107–1116. doi: 10.1016/j.ophtha.2018.12.029[↩][↩]
- Daugeliene L., Yamamoto T., Kitazawa Y. Effect of trabeculectomy on visual field in progressive normal-tension glaucoma. Jpn. J. Ophthalmol. 1998;42:286–292. doi: 10.1016/S0021-5155(98)00013-6[↩]





{kind=link}