Outer ear anatomy
The ear, has outer, middle, and inner parts. The ear also functions in the sense of equilibrium.
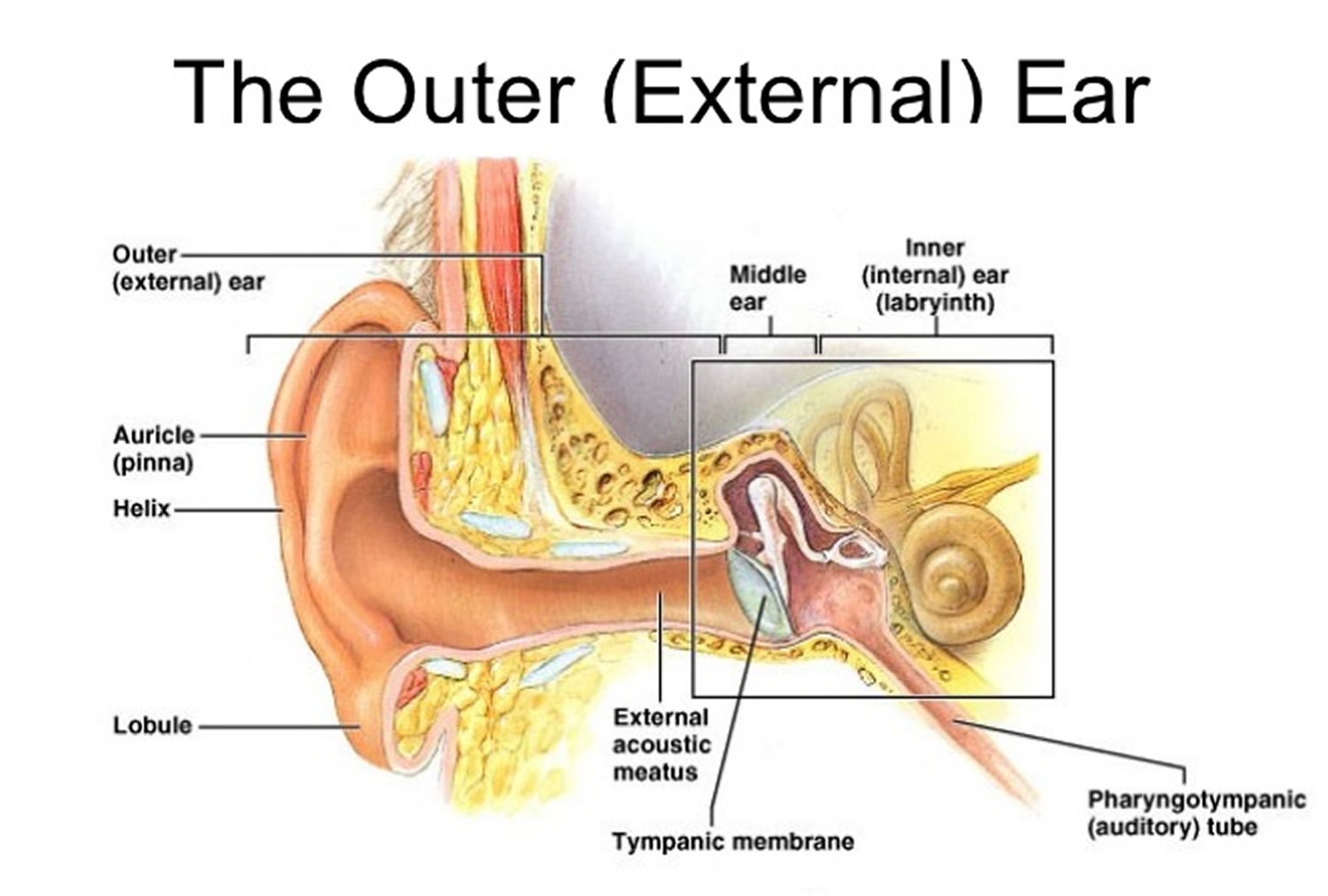
Outer (External) Ear
The outer ear consists of three parts. The first is an outer, funnel-like structure called the auricle or pinna. The second is an S-shaped tube called the external acoustic meatus or external auditory canal, that leads inward through the temporal bone for about 2.5 centimeters (Figure 1). The meatus terminates with the third part, the eardrum or tympanic membrane.
The transmission of vibrations through matter produces sound. These vibrations travel in waves, much like ripples on the surface of a pond. The higher the wave, the louder the sound. The more waves per second, the higher the frequency, or pitch, of the sound. Vibrating strings on a guitar or reeds on an oboe produce the sounds of these musical instruments, and vibrating vocal folds (vocal cords) in the larynx produce the voice. The auricle of the ear helps collect sound waves traveling through the air and directs them into the external acoustic meatus. At the end of the meatus, the sound waves reach the eardrum.
The eardrum is a semitransparent membrane covered by a thin layer of skin on its outer surface and by mucous membrane on the inside. It has an oval margin and is coneshaped, with the apex of the cone directed inward. The attachment of one of the auditory ossicles (the malleus) maintains the eardrum’s cone shape. Sound waves that enter the external acoustic meatus change the pressure on the eardrum, which vibrates back and forth in response and thus reproduces the vibrations of the sound-wave source.
Middle Ear
The middle ear, or tympanic cavity, is an air-filled space in the temporal bone. It contains three small bones called auditory ossicles: the malleus, the incus, and the stapes (Figure 1). Tiny ligaments attach them to the wall of the tympanic cavity, and they are covered by mucous membrane. These bones bridge the eardrum and the inner ear, transferring vibrations between these parts. Specifically, the malleus attaches to the eardrum, and when the eardrum vibrates, the malleus vibrates in unison. The malleus causes the incus to vibrate, and the incus passes the movement on to the stapes. An oval ligament holds the stapes to an opening in the wall of the tympanic cavity called the oval window, which leads into the inner ear. Vibration of the stapes at the oval window moves a fluid in the inner ear, which stimulates the hearing receptors.
The auditory ossicles help increase (amplify) the force of vibrations as they pass from the eardrum to the oval window, in addition to transferring vibrations. The vibrational force concentrates as it moves from the outer to the inner ear because the ossicles transmit vibrations from the relatively large surface of the eardrum to a much smaller area at the oval window. As a result, the pressure (per square millimeter) that the stapes applies on the oval window is many times greater than the pressure that sound waves exert on the eardrum.
Auditory Tube
An auditory tube or eustachian tube, connects each middle ear to the back of the nasal cavity (nasopharynx). This tube conducts air between the tympanic cavity and the outside of the body by way of the nose and mouth. The auditory tube helps maintain equal air pressure on both sides of the eardrum, which is necessary for normal hearing.
The function of the auditory tube is noticeable during rapid changes in altitude. As a person moves from a higher altitude to a lower one, air pressure on the outside of the eardrum increases. This may push the eardrum inward, impairing hearing. When the air pressure difference is great enough, air movement through the auditory tube equalizes the pressure on both sides of the eardrum, and the membrane moves back into its regular position. This restores normal hearing and is associated with a popping sound.
Inner (Internal) Ear
Next to the middle ear in the bone of the skull is a small compartment which contains the hearing and balance apparatus known as the inner ear. The inner ear is a complex system of communicating chambers and tubes called a labyrinth. Each ear has two parts to the labyrinth—the bony (osseus) labyrinth and the membranous labyrinth. The bony labyrinth is a cavity within the temporal bone. The membranous labyrinth is a tube of similar shape that lies within the bony labyrinth. Between the bony and membranous labyrinths is a fluid called perilymph, which is secreted by cells in the wall of the bony labyrinth. The membranous labyrinth contains another fluid, called endolymph.
The parts of the labyrinths include three membranous semicircular ducts within three bony semicircular canals, and a cochlea. The semicircular canals and associated structures provide a sense of equilibrium or balance. The cochlea functions in hearing.
The cochlea is shaped like a snail and is divided into two chambers by a membrane. The chambers are full of fluid which vibrates when sound comes in and causes the small hairs which line the membrane to vibrate and send electrical impulses to the brain.
The semi-circular canals are also known as the labyrinthine. These little canals are lined up at right angles (90°) to each other. This allows the brain to know in which direction the head is moving. These semi-circular canals are filled with fluid and have some small calcium crystals embedded in the lining.
Coming from the inner ear and running to the brain is the eighth cranial nerve, the auditory nerve. This nerve carries both balance and hearing information to the brain. Along with the eighth cranial nerve runs the seventh cranial nerve. The seventh cranial nerve is also known as the facial nerve because it supplies nerve impulses to the muscles of the face.
How does the hearing system work ?
The outer ear captures sound waves. The sound travels down the ear canal and hits the ear drum. The ear drum vibrates which causes the ossicles (middle ear bones) to vibrate. A piston action of the ossicles creates a wave in the fluid in the inner ear. The fluid wave stimulates the hair cells in the cochlea and an electrical impulse is sent through the eighth cranial nerve to the brain.
The balance system works by sending continuous electrical impulses to the brain. Moving the head causes the fluid in the semi-circular canals to shift. This in turn changes the electrical impulses to the brain. The brain uses this information to make any adjustments the body needs for balance.
Figure 1. Outer ear (pinna or auricle)
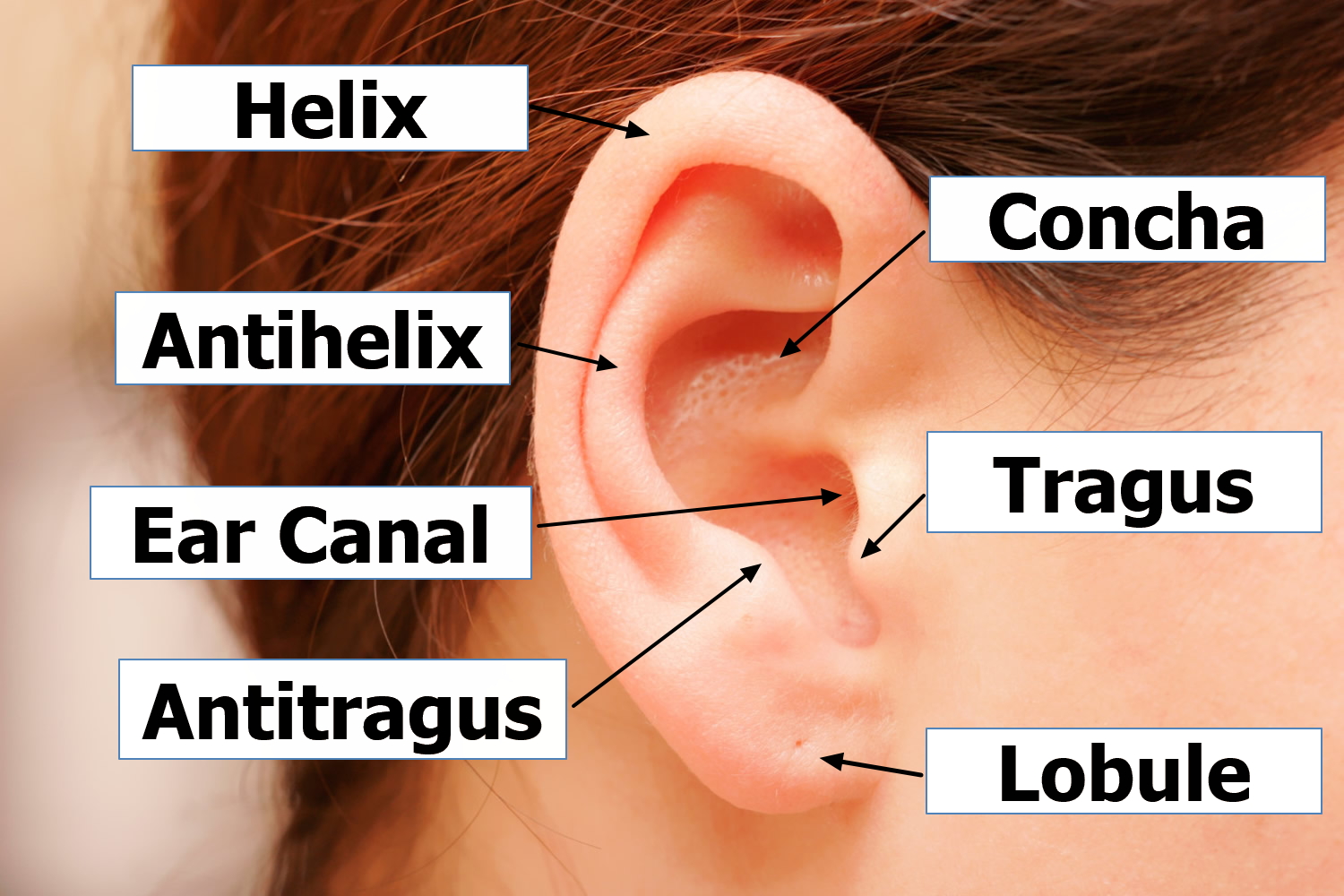
Figure 2. Outer ear anatomy

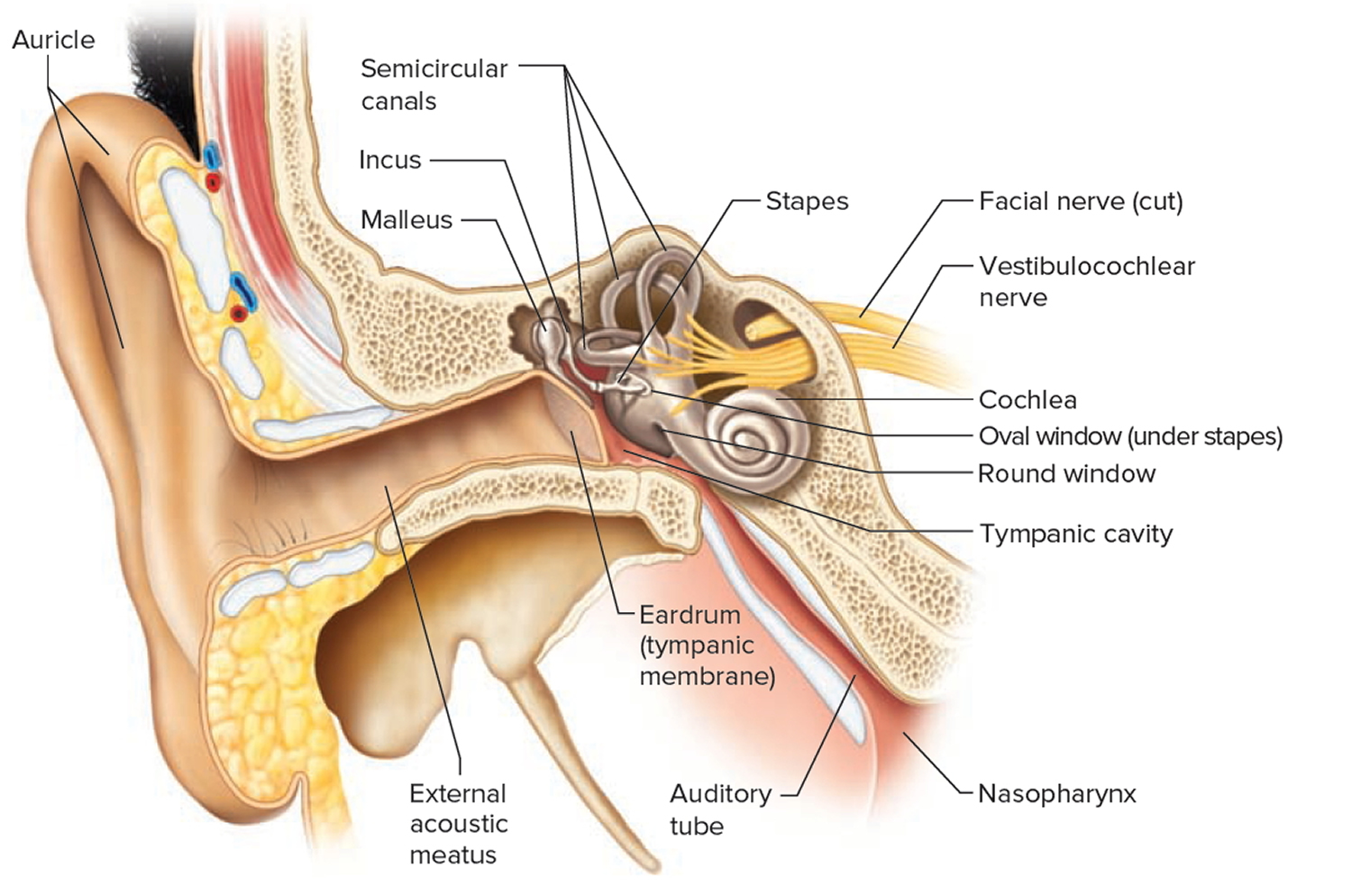
Figure 3. The Ear showing outer (auricle), middle and inner parts
Outer ear infection (Acute otitis externa)
Otitis externa, also called swimmer’s ear, involves diffuse inflammation of the external ear canal that may extend distally to the pinna and proximally to the tympanic membrane 1. The acute form has an annual incidence of approximately 1 percent 2 and a lifetime prevalence of 10 percent 3. On rare occasions, the infection invades the surrounding soft tissue and bone; this is known as malignant (necrotizing) otitis externa, and is a medical emergency that occurs primarily in older patients with diabetes mellitus 4. Otitis externa lasting three months or longer, known as chronic otitis externa, is often the result of allergies, chronic dermatologic conditions, or inadequately treated acute otitis externa.
In North America, 98 percent of cases of acute otitis externa are caused by bacteria 5. The two most common isolates are Pseudomonas aeruginosa and Staphylococcus aureus. However, a wide variety of other aerobic and anaerobic bacteria have been isolated 6, 7. Approximately one-third of cases are polymicrobial 5. Fungal pathogens, primarily those of the Aspergillus and Candida species, occur more often in tropical or subtropical environments and in patients previously treated with antibiotics 8, 9, 10. Otomycosis is classically associated with itching, thick material in the ear canal, and failure to improve with use of topical antibacterials. Otomycosis can sometimes be identified during otoscopy, although nonpathogenic saprophytic fungi may also be found. Inflammatory skin disorders and allergic reactions may cause noninfectious otitis externa, which can be chronic.
Malignant otitis externa may be suspected in older patients with diabetes mellitus or immunocompromise who have refractory purulent otorrhea and severe otalgia that may worsen at night. Clinical findings include granulation tissue in the external auditory canal, especially at the bone-cartilage junction. Extension of the infection beyond the auditory canal can cause lymphadenopathy, trismus, and facial nerve and other cranial nerve palsies.
Risk Factors for outer ear infection
Several factors may predispose patients to the development of acute outer ear infection (Table 1) 5, 11. One of the most common predisposing factors is swimming, especially in fresh water. Other factors include skin conditions such as eczema and seborrhea, trauma from cerumen removal, use of external devices such as hearing aids and cerumen buildup 5. These factors appear to work primarily through loss of the protective cerumen barrier, disruption of the epithelium (including maceration from water retention), inoculation with bacteria, and increase in the pH of the ear canal 11, 12, 13.
Table 1. Predisposing Factors for Outer Ear Infection
Anatomic abnormalities |
Canal stenosis |
Exostoses |
Hairy ear canals |
Canal obstruction |
Cerumen obstruction |
Foreign body |
Sebaceous cyst |
Cerumen/epithelial integrity |
Cerumen removal |
Earplugs |
Hearing aids |
Instrumentation/itching |
Dermatologic conditions |
Eczema |
Psoriasis |
Seborrhea |
Other inflammatory dermatoses |
Water in ear canal |
Humidity |
Sweating |
Swimming or other prolonged water exposure |
Miscellaneous |
Purulent otorrhea from otitis media |
Soap |
Stress |
Type A blood |
Prevention of Outer Ear Infection
A number of preventive measures have been recommended, including use of earplugs while swimming, use of hair dryers on the lowest settings and head tilting to remove water from the ear canal, and avoidance of self-cleaning or scratching the ear canal. Acetic acid 2% (Vosol) otic solutions are also used, either two drops twice daily or two to five drops after water exposure. However, no randomized trials have examined the effectiveness of any of these measures.
Diagnosis of Outer Ear Infection
Acute outer ear infection is diagnosed clinically based on signs and symptoms of canal inflammation. Presentation can range from mild discomfort, itching, and minimal edema to severe pain, complete canal obstruction, and involvement of the pinna and surrounding skin. Pain is the symptom that best correlates with the severity of disease 14. Mild fever may be present, but a temperature greater than 101°F (38.3°C) suggests extension beyond the auditory canal.
- Onset of symptoms within 48 hours in the past three weeks and
Symptoms of ear canal inflammation 15:
- Ear pain, itching, or fullness
- With or without hearing loss or jaw pain
and
Signs of ear canal inflammation 15:
- Tenderness of tragus/pinna or ear canal edema/erythema
- With or without otorrhea, tympanic membrane erythema, cellulitis of the pinna, or local lymphadenitis
Table 2. Conditions That May Be Confused with Acute Outer Ear Infection
| Condition | Distinguishing characteristics | Comment |
|---|---|---|
Acute middle ear infection (acute otitis media) | Presence of middle ear effusion, no tragal/pinnal tenderness | Use pneumatic otoscopy or tympanometry, treat with systemic antibiotics |
Chronic outer ear infection (chronic otitis externa) | Itching is often predominant symptom, erythematous canal, lasts more than three months | Treat underlying causes/conditions |
Chronic suppurative middle ear infection (suppurative otitis media) | Chronic otorrhea, nonintact tympanic membrane | Control otitis externa symptoms, then treat otitis media |
Contact dermatitis | Allergic reaction to materials (e.g., metals, soaps, plastics) in contact with the skin/epithelium; itching is predominant symptom | Check for piercings, hearing aids, or earplug use; discontinue exposure when possible |
Eczema | Itching is predominant symptom; often chronic; history of atopy, outbreaks in other locations | Consider treatment with topical corticosteroids |
Furunculosis | Focal infection, may be pustule or nodule, often in distal canal | Consider treatment with heat, incision and drainage, or systemic antibiotics; can progress to diffuse otitis externa |
Malignant outer ear infection (malignant otitis externa) | High fever, granulation tissue or necrotic tissue in ear canal, may have cranial nerve involvement; patient with diabetes mellitus or immunocompromise, elevated erythrocyte sedimentation rate, findings on computed tomography | Medical emergency with high morbidity rate and possible mortality; warrants emergent consultation with otolaryngologist, hospitalization, intravenous antibiotics, debridement |
Myringitis | Tympanic membrane inflammation, may have vesicles; pain is often severe, no canal edema | Usually results from acute otitis media or viral infection |
Otomycosis (fungal ear infection of the outer ear canal) | Itching is predominant symptom, thick material in canal, less edema; may see fungal elements on otoscopy | Can coexist with bacterial infections; treat with acetic acid (Vosol), half acetic acid/half alcohol, or topical antifungals; meticulous cleaning of ear canal |
Ramsay Hunt syndrome | Herpetic ulcers in canal; may have facial numbness/paralysis, severe pain, loss of taste | Treatment includes antivirals, systemic corticosteroids |
Referred pain | Normal ear examination | Look for other causes based on patterns of referred pain |
Seborrhea | Itching and rash on hairline, face, scalp | Treatment includes lubricating or moisturizing the external auditory canal |
Sensitization to otics | Severe itching, maculopapular or erythematous rash in conchal bowl and canal; may have streak on pinna where preparation contacted skin; vesicles may be present | Type IV delayed hypersensitivity reaction to neomycin or other components of otic solutions; discontinue offending agent; treat with topical corticosteroids |
Chronic Outer Ear Infection
In chronic outer ear infection (chronic otitis externa), the symptoms and signs occur for more than three months. Classic symptoms include itching and mild discomfort; there may also be lichenification on otoscopy.
Treatment of outer ear infection
TOPICAL MEDICATIONS
Topical antimicrobials, with or without topical corticosteroids, are the mainstay of treatment for uncomplicated acute outer ear infection. Topical antimicrobials are highly effective compared with placebo, demonstrating an absolute increase in clinical cure rate of 46 percent or a number needed to treat of slightly more than two 5. Topical agents come in a variety of preparations and combinations; a recent systematic review included 26 different topical interventions 16. In some studies, ophthalmic preparations have been used off-label to treat outer ear infection 17, 16. Ophthalmic preparations may be better tolerated than otic preparations, possibly due to differences in pH between the preparations, and may help facilitate compliance with treatment recommendations. Commonly studied antimicrobial agents include aminoglycosides, polymyxin B, quinolones, and acetic acid. No consistent evidence has shown that any one agent or preparation is more effective than another 5, 18, 17, 16. There is limited evidence that use of acetic acid alone may require two additional days for resolution of symptoms compared with other agents, and that it is less effective if treatment is required for more than seven days 16.
Current guidelines recommend factoring in the risk of adverse effects, adherence issues, cost, patient preference, and physician experience. Some components found in otic preparations may cause contact dermatitis 19. Hypersensitivity to aminoglycosides, particularly neomycin, may develop in up to 15 percent of the population, and has been identified in approximately 30 percent of patients who also have chronic or eczematous outer ear infection 19, 20. Adherence to topical therapy increases with ease of administration, such as less frequent dosing 21. The addition of a topical corticosteroid yields more rapid improvement in symptoms such as pain, canal edema, and erythema. Cost varies considerably for the different preparations.
Outer Ear Infection Pain Relief
Pain is a common symptom of acute outer ear infection and can be debilitating 13. Oral analgesics are the preferred treatment. First-line analgesics include nonsteroidal anti-inflammatory drugs and acetaminophen. When ongoing frequent dosing is required to control pain, medications should be administered on a scheduled rather than as-needed basis. Opioid combination pills may be used when symptom severity warrants. Benzocaine otic preparations may compromise the effectiveness of otic antibiotic drops by limiting contact between the drop and the ear canal. The lack of published data supporting the effectiveness of topical benzocaine preparations in outer ear infection limits the role of such treatments 1.
CLEANING THE EAR CANAL
Acute outer ear infection can be associated with copious material in the ear canal. Consensus guidelines published by the American Academy of Otolaryngology recommend that such material be removed to achieve optimal effectiveness of the topical antibiotics 5, 18. However, no randomized controlled trials have examined the effectiveness of aural toilet, and this is not typically done in most primary care settings 16. Topical medications rely on direct contact with the infected skin of the ear canal; hence, aural toilet takes on greater importance when the volume or thickness of the debris in the ear canal is great. Guidelines recommend aural toilet by gentle lavage suctioning or dry mopping under otoscopic or microscopic visualization to remove obstructing material and to verify tympanic membrane integrity 5. Lavage should be used only if the tympanic membrane is known to be intact, and should not be performed on patients with diabetes because of the potential risk of causing malignant outer ear infection 5. Pain medications may be required during the procedure.
Treatment of chronic outer ear infection
The treatment of chronic outer ear infection depends on the underlying causes. Because most cases are caused by allergies or inflammatory dermatologic conditions, treatment includes the removal of offending agents and the use of topical or systemic corticosteroids. Chronic or intermittent otorrhea over weeks to months, particularly with an open tympanic membrane, suggests the presence of chronic suppurative otitis media (suppurative middle ear infection). Initial treatment efforts are similar to those for acute otitis media. With control of the symptoms of outer ear infection, attention can shift to the management of chronic suppurative otitis media.
Follow-up and Referral
Most patients will experience considerable improvement in symptoms after one day of treatment. If there is no improvement within 48 to 72 hours, physicians should reevaluate for treatment adherence, misdiagnosis, sensitivity to ear drops, or continued canal patency. The physician should consider culturing material from the canal to identify fungal and antibiotic-resistant pathogens if the patient does not improve after initial treatment efforts or has one or more predisposing risk factors, or if there is suspicion that the infection has extended beyond the external auditory canal. There is a lack of data regarding optimal length of treatment; as a general rule, antimicrobial otics should be administered for seven to 10 days, although in some cases complete resolution of symptoms may take up to four weeks 5, 16.
Consultation with an otolaryngologist or infectious disease subspecialist may be warranted if malignant outer ear infection is suspected; in cases of severe disease, lack of improvement or worsening of symptoms despite treatment, and unsuccessful lavage; or if the primary care physician determines that aural toilet or ear wick insertion is warranted, but is unfamiliar with or concerned about performing the procedure.
- Acute Otitis Externa: An Update. Am Fam Physician. 2012 Dec 1;86(11):1055-1061. http://www.aafp.org/afp/2012/1201/p1055.html[↩][↩][↩][↩]
- Rowlands S, Devalia H, Smith C, Hubbard R, Dean A. Otitis externa in UK general practice: a survey using the UK General Practice Research Database. Br J Gen Pract. 2001;51(468):533–538.[↩]
- Raza SA, Denholm SW, Wong JC. An audit of the management of acute otitis externa in an ENT casualty clinic. J Laryngol Otol. 1995;109(2):130–133.[↩]
- Rubin Grandis J, Branstetter BF IV, Yu VL. The changing face of malignant (necrotising) external otitis: clinical, radiological, and anatomic correlations. Lancet Infect Dis. 2004;4(1):34–39.[↩]
- Rosenfeld RM, Brown L, Cannon CR, et al.; American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 suppl):S4–S23.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Ninkovic G, Dullo V, Saunders NC. Microbiology of otitis externa in the secondary care in United Kingdom and antimicrobial sensitivity. Auris Nasus Larynx. 2008;35(4):480–484.[↩]
- Roland PS, Stroman DW. Microbiology of acute otitis externa. Laryngoscope. 2002;112(7 pt 1):1166–1177.[↩]
- Martin TJ, Kerschner JE, Flanary VA. Fungal causes of otitis externa and tympanostomy tube otorrhea. Int J Pediatr Otorhinolaryngol. 2005;69(11):1503–1508.[↩]
- Pontes ZB, Silva AD, Lima Ede O, et al. Otomycosis: a retrospective study. Braz J Otorhinolaryngol. 2009;75(3):367–370.[↩]
- Ahmad N, Etheridge C, Farrington M, Baguley DM. Prospective study of the microbiological flora of hearing aid moulds and the efficacy of current cleaning techniques. J Laryngol Otol. 2007;121(2):110–113.[↩]
- Russell JD, Donnelly M, McShane DP, Alun-Jones T, Walsh M. What causes acute otitis externa? J Laryngol Otol. 1993;107(10):898–901.[↩][↩]
- Kim JK, Cho JH. Change of external auditory canal pH in acute otitis externa. Ann Otol Rhinol Laryngol. 2009;118(11):769–772.[↩]
- van Asperen IA, de Rover CM, Schijven JF, et al. Risk of otitis externa after swimming in recreational fresh water lakes containing Pseudomonas aeruginosa. BMJ. 1995;311(7017):1407–1410.[↩][↩]
- Halpern MT, Palmer CS, Seidlin M. Treatment patterns for otitis externa. J Am Board Fam Pract. 1999;12(1):1–7.[↩]
- Rosenfeld RM, Brown L, Cannon CR, et al.; American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 suppl):S5.[↩][↩]
- Kaushik V, Malik T, Saeed SR. Interventions for acute otitis externa. Cochrane Database Syst Rev. 2010(1):CD004740.[↩][↩][↩][↩][↩][↩]
- Rosenfeld RM, Singer M, Wasserman JM, Stinnett SS. Systematic review of topical antimicrobial therapy for acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 suppl):S24–S48.[↩][↩]
- Hajioff D, Mackeith S. Otitis externa. Clin Evid (Online). 2010.[↩][↩]
- Smith IM, Keay DG, Buxton PK. Contact hypersensitivity in patients with chronic otitis externa. Clin Otolaryngol Allied Sci. 1990;15(2):155–158.[↩][↩]
- Yariktas M, Yildirim M, Doner F, Baysal V, Dogru H. Allergic contact dermatitis prevalence in patients with eczematous external otitis. Asian Pac J Allergy Immunol. 2004;22(1):7–10.[↩]
- Shikiar R, Halpern MT, McGann M, Palmer CS, Seidlin M. The relation of patient satisfaction with treatment of otitis externa to clinical outcomes: development of an instrument. Clin Ther. 1999;21(6):1091–1104.[↩]





{kind=link}