Contents
- What is a prolapsed uterus
- What does a prolapsed uterus look like ?
- Causes of prolapsed uterus
- Signs and Symptoms of prolapsed uterus
- Prolapsed uterus diagnosis
- Treatment of prolapsed uterus
- Outlook (Prognosis) of prolapsed uterus
- Possible Complications of prolapsed uterus
- Prevention of prolapsed uterus
- Diagnosis of prolapsed uterus
- Treatment of prolapsed uterus
- Prolapsed uterus treatment at home
What is a prolapsed uterus
Prolapsed uterus occurs when pelvic floor muscles and ligaments stretch and weaken and no longer provide enough support for the uterus 1. As a result, the uterus slips down into or protrudes out of the vagina.
Prolapsed uterus affects up to half of all women who have had children by some degree and it is rare in women who have not had children.
Prolapsed uterus is also associated with being overweight and with having a persistent cough. It is the most common reason for hysterectomy in women aged over 50.
Uterine prolapse can occur in women of any age. But it often affects postmenopausal women who’ve had one or more vaginal deliveries.
Uterine prolapse can be categorized as incomplete or complete 2:
- Incomplete uterine prolapse: when an incomplete uterine prolapse occurs, the uterus is partially displaced into the vagina but does not protrude
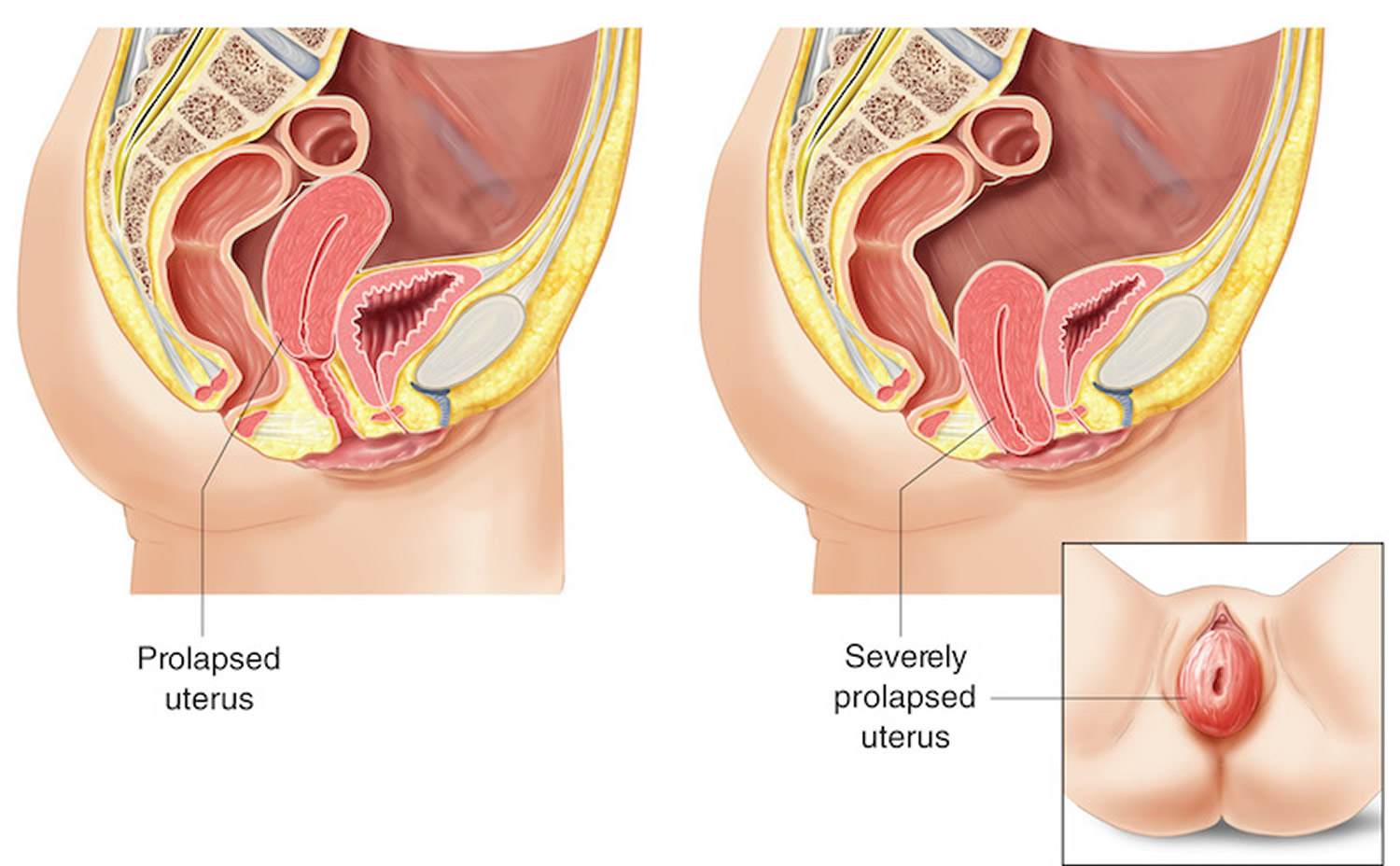
- Complete uterine prolapse: when a complete uterine prolapse occurs, there is a portion of the uterus protruding out of the vaginal opening.
Uterine prolapse is graded by its severity, determined by how far the uterus has descended 3:
- Grade 1: the prolapsed uterus is more than 1 cm above the opening of the vagina.
- Grade 2: the prolapsed uterus is 1 cm or less from the opening of the vagina.
- Grade 3: the prolapsed uterus sticks out of the vagina opening more than 1 cm, but not fully.
- Grade 4: the full length of the prolapsed uterus bulges out of the vagina.
In some cases, uterine prolapse can cause complications, including ulceration of exposed tissue and prolapse of other pelvic organs such as the prolapsed bladder (cystocele) or prolapsed rectum (rectocele).
Mild uterine prolapse usually doesn’t require treatment. But if uterine prolapse makes you uncomfortable or disrupts your normal life, you might benefit from treatment.
What does a prolapsed uterus look like ?
Figure 1. Normal uterus
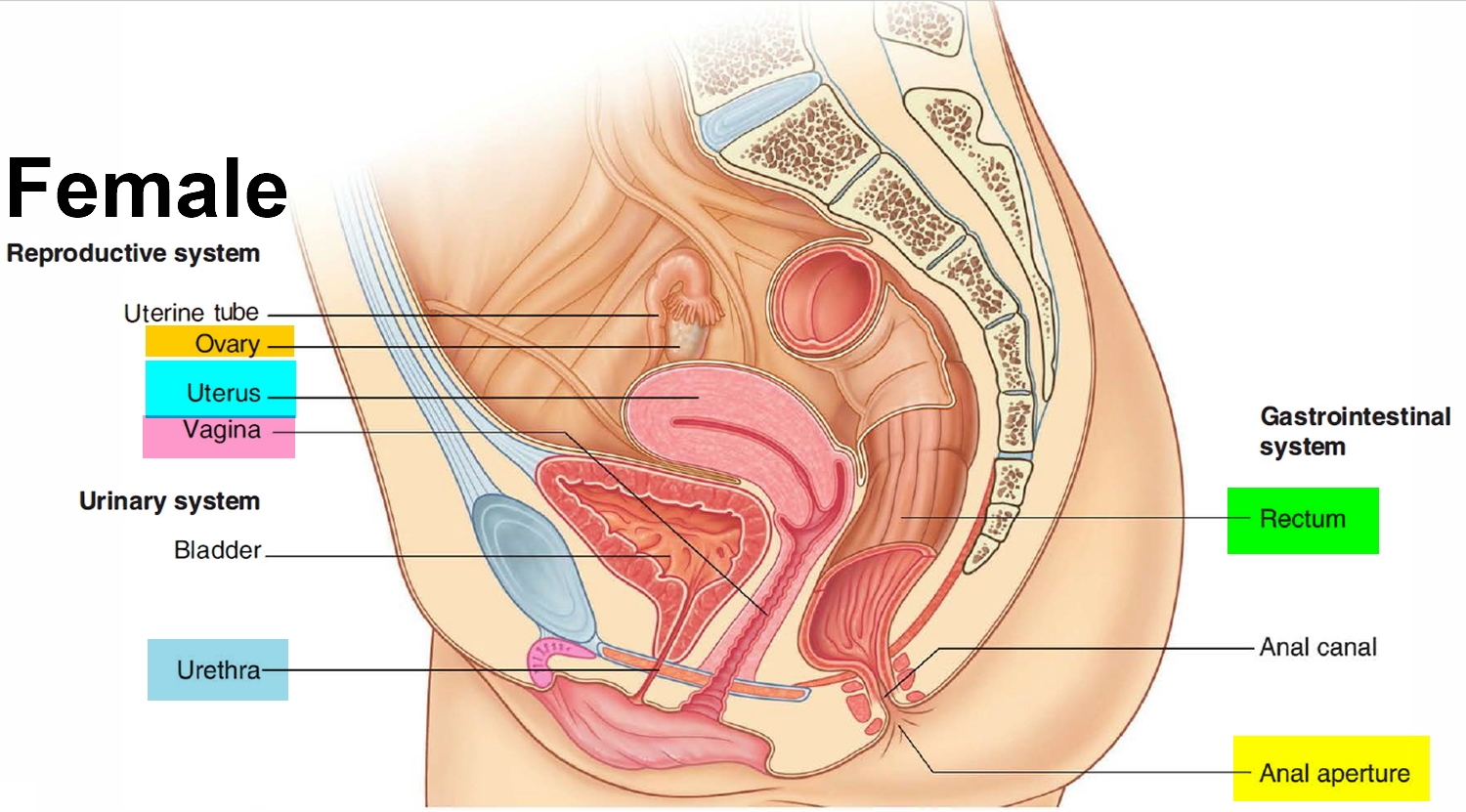
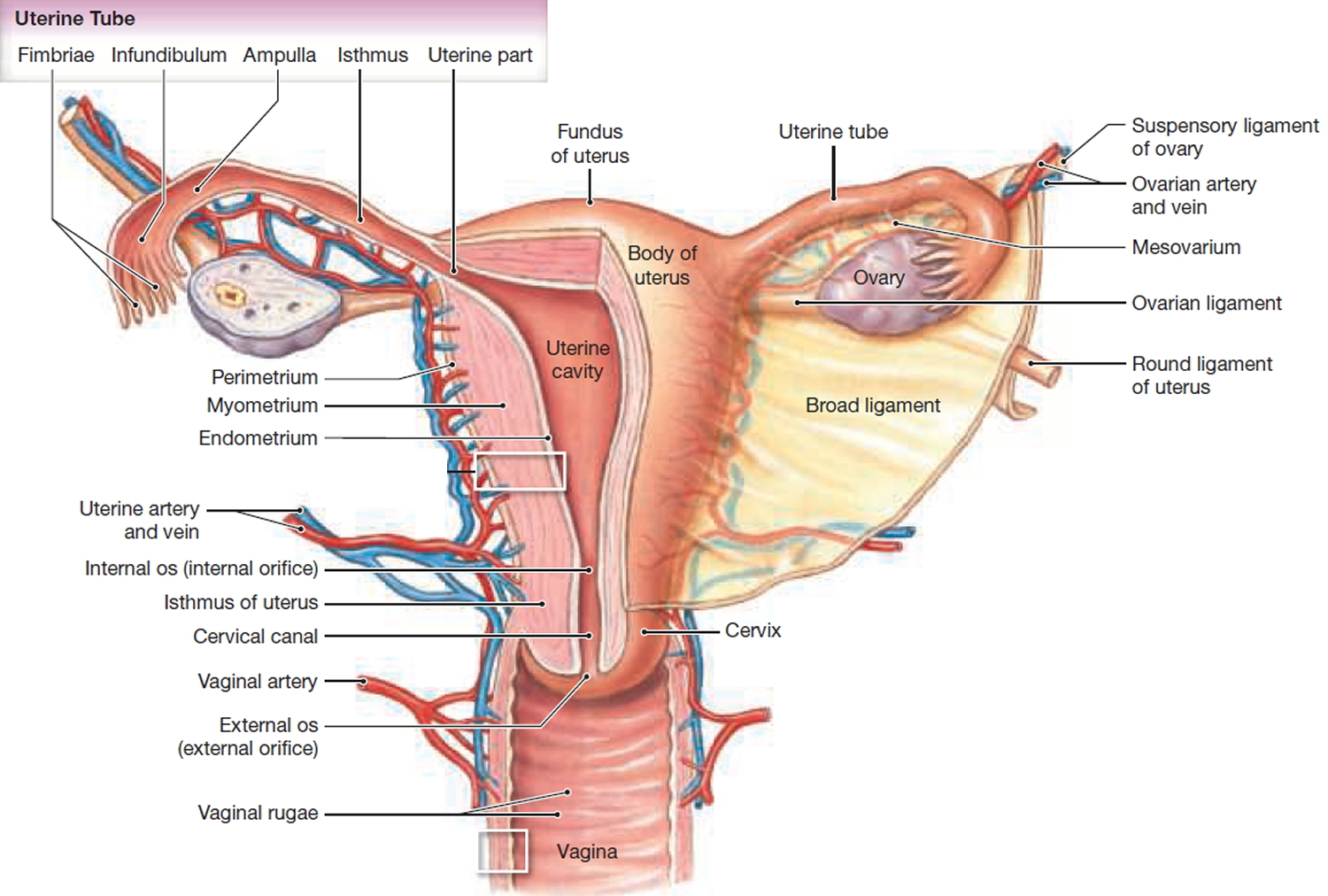
Figure 2. Prolapsed uterus
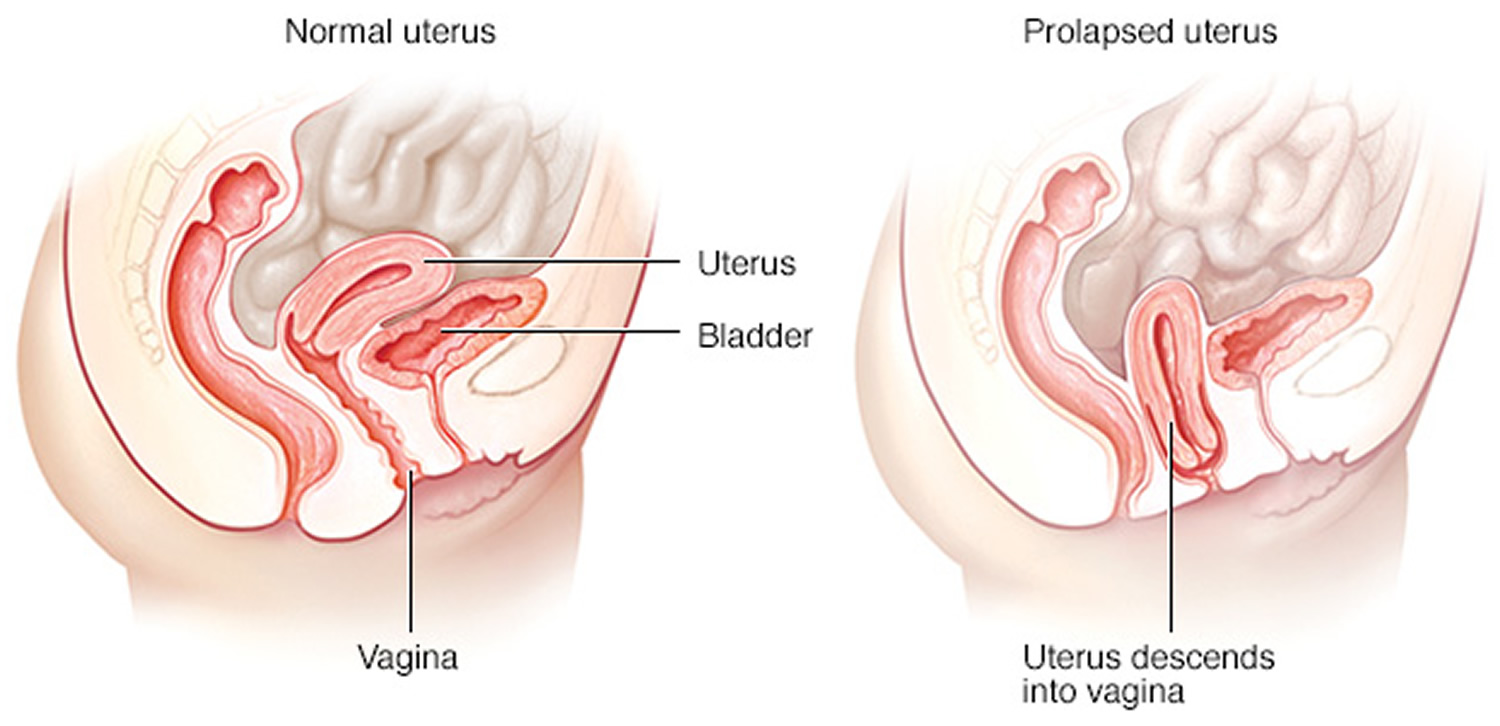
Figure 3. Severely prolapsed uterus (Grade 4)
Causes of prolapsed uterus
Muscles, ligaments, and other structures hold the uterus in the pelvis. If these tissues are weak or stretched, the uterus drops into the vaginal canal. This is called prolapse.
This condition is more common in women who have had 1 or more vaginal births.
Other things that can cause or lead to uterine prolapse include:
- Normal aging
- Lack of estrogen after menopause
- Conditions that put pressure on the pelvic muscles, such as chronic cough and obesity
- Pelvic tumor (rare)
- Difficult labor and delivery or trauma during childbirth
- Giving birth to a large baby
- Being overweight or obese
- Lower estrogen level after menopause
- Chronic constipation or straining with bowel movements
- Chronic cough or bronchitis
- Repeated heavy lifting
- Prior pelvic surgery
- Family history of weakness in connective tissue
- Being Hispanic or white
Repeated straining to have a bowel movement due to long-term constipation can make the problem worse.
Signs and Symptoms of prolapsed uterus
Mild uterine prolapse generally doesn’t cause signs or symptoms.
Symptoms may include 4:
- Sensation of heaviness, pressure or pulling in your pelvis or vagina
- Tissue protruding from your vagina
- Urinary problems, such as urine leakage (incontinence) or urine retention or sudden urge to empty the bladder
- Trouble having a bowel movement
- Feeling as if you’re sitting on a small ball or as if something is falling out of your vagina
- Problems with sexual intercourse, such as a sensation of looseness in the tone of your vaginal tissue
- Low backache
- Uterus and cervix that bulge into the vaginal opening
- Repeated bladder infections
- Vaginal bleeding
- Increased vaginal discharge
Often, symptoms are less bothersome in the morning and worsen as the day goes on.
Symptoms may be worse when you stand or sit for a long time. Exercise or lifting may also make symptoms worse.
Prolapsed uterus diagnosis
Your health care provider will do a pelvic exam. You will be asked to bear down as if you are trying to push out a baby. This shows how far your uterus has dropped.
Uterine prolapse is mild when the cervix drops into the lower part of the vagina.
Uterine prolapse is moderate when the cervix drops out of the vaginal opening.
Other things the pelvic exam may show are:
The bladder and front wall of the vagina are bulging into the vagina (cystocele).
The rectum and back wall of the vagina (rectocele) are bulging into the vagina.
The urethra and bladder are lower in the pelvis than usual.
Treatment of prolapsed uterus
You do not need treatment unless you are bothered by the symptoms.
Many women will get treatment by the time the uterus drops to the opening of the vagina.
Lifestyle Changes
The following can help you control your symptoms:
- Lose weight if you are obese.
- Avoid heavy lifting or straining.
- Get treated for a chronic cough. If you cough is due to smoking, try to quit.
Vaginal Pessary
Your provider may recommend placing a rubber or plastic donut-shaped device, into the vagina. This is called a pessary. This device holds the uterus in place.
The pessary may be used for short-term or long-term. The device is fitted for your vagina. Some pessaries are similar to a diaphragm used for birth control.
Pessaries must be cleaned regularly. Sometimes they need to be cleaned by the provider. Many women can be taught how to insert, clean, and remove a pessary.
Side effects of pessaries include:
- Foul smelling discharge from the vagina
- Irritation of the lining of the vagina
- Ulcers in the vagina
- Problems with normal sexual intercourse
Surgery
Surgery should not be done until the prolapse symptoms are worse than the risks of having surgery. The type of surgery will depend on:
- The severity of the prolapse
- The woman’s plans for future pregnancies
- The woman’s age, health, and other medical problems
- The woman’s desire to retain vaginal function
There are some surgical procedures that can be done without removing the uterus, such as a sacrospinous fixation. This procedure involves using nearby ligaments to support the uterus. Other procedures are also available.
Often, a vaginal hysterectomy is used to correct uterine prolapse. Any sagging of the vaginal walls, urethra, bladder, or rectum can be surgically corrected at the same time.
Outlook (Prognosis) of prolapsed uterus
Most women with mild uterine prolapse do not have symptoms that require treatment.
Vaginal pessaries can be effective for many women with uterine prolapse.
Surgery often provides very good results. However, some women may need to have the treatment again in the future.
Possible Complications of prolapsed uterus
Severe uterine prolapse can displace part of the vaginal lining, causing it to protrude outside the body. Vaginal tissue that rubs against clothing can lead to vaginal sores (ulcers.) Rarely, the sores can become infected.
Uterine prolapse is often associated with prolapse of other pelvic organs. You might experience:
- Anterior prolapse (cystocele). Weakness of connective tissue separating the bladder and vagina may cause the bladder to bulge into the vagina. Anterior prolapse is also called prolapsed bladder.
- Urinary tract infections and other urinary symptoms may occur because of a cystocele.
- Posterior vaginal prolapse (rectocele). Weakness of connective tissue separating the rectum and vagina may cause the rectum to bulge into the vagina. You might have difficulty having bowel movements.
- Constipation and hemorrhoids may occur because of a rectocele.
Prevention of prolapsed uterus
To reduce your risk of uterine prolapse, try to:
- Perform Kegel exercises regularly (see below prolapsed uterus treatment at home ). These exercises can strengthen your pelvic floor muscles — especially important after you have a baby.
- Treat and prevent constipation. Drink plenty of fluids and eat high-fiber foods, such as fruits, vegetables, beans and whole-grain cereals.
- Avoid heavy lifting and lift correctly. When lifting, use your legs instead of your waist or back.
- Control coughing. Get treatment for a chronic cough or bronchitis, and don’t smoke.
- Avoid weight gain. Talk with your doctor to determine your ideal weight and get advice on weight-loss strategies, if you need them.
Diagnosis of prolapsed uterus
A diagnosis of uterine prolapse generally occurs during a pelvic exam.
During the pelvic exam your doctor is likely to ask you:
- To bear down as if having a bowel movement. Bearing down can help your doctor assess how far the uterus has slipped into the vagina.
- To tighten your pelvic muscles as if you’re stopping a stream of urine. This test checks the strength of your pelvic muscles.
You might fill out a questionnaire that helps your doctor assess how uterine prolapse affects your quality of life. This information helps guide treatment decisions.
If you have severe incontinence, your doctor might recommend tests to measure how well your bladder functions (urodynamic testing).
Treatment of prolapsed uterus
Treatment depends on the severity of uterine prolapse. Your doctor might recommend:
- Self-care measures. If your uterine prolapse causes few or no symptoms, simple self-care measures may provide relief or help prevent worsening prolapse. Self-care measures include performing Kegel exercises to strengthen your pelvic muscles, losing weight and treating constipation.
- Pessary. A vaginal pessary is a plastic or rubber ring inserted into your vagina to support the bulging tissues. A pessary must be removed regularly for cleaning.
Vaginal pessaries
A vaginal ring pessary is a device that is similar to a diaphragm or cap. It is inserted into your vagina to hold the vaginal walls in place. Ring pessaries are usually made of latex (rubber) or silicone and come in different shapes and sizes. Ring pessaries may be an option if your prolapse is more severe but you would prefer not to have surgery. A gynaecologist (a specialist in treating conditions of the female reproductive system) or a specialist nurse usually fits a pessary. The pessary will be removed every three to six months and replaced with a new one.
Types of Pessary
Ring pessary
This is a soft plastic ring or device which is inserted into the vagina and pushes the prolapse back up. This usually gets rid of the dragging sensation and can improve urinary and bowel symptoms. It needs to be changed every 6-9 months and can be very popular. Other pessaries may be used if the Ring pessary is not suitable. Some couples feel that the pessary gets in the way during sexual intercourse, but many couples are not bothered by it.
Shelf Pessary or Gellhorn
If you are not sexually active this is a stronger pessary which can be inserted into the vagina and needs changing every 4-6 months.
Side effects of vaginal pessary
Ring pessaries can occasionally cause vaginal discharge. They may also cause some irritation and possibly bleeding and sores inside your vagina. Other common side effects include:
- An infection of your urinary tract (urinary tract infection)
- An imbalance of the usual bacteria that are found in your vagina (bacterial vaginosis)
- Passing a small amount of urine when you cough, sneeze or exercise (stress incontinence)
- Difficulty with bowel movements
- Interfering with sex
Figure 4. Vaginal pessary for prolapsed uterus
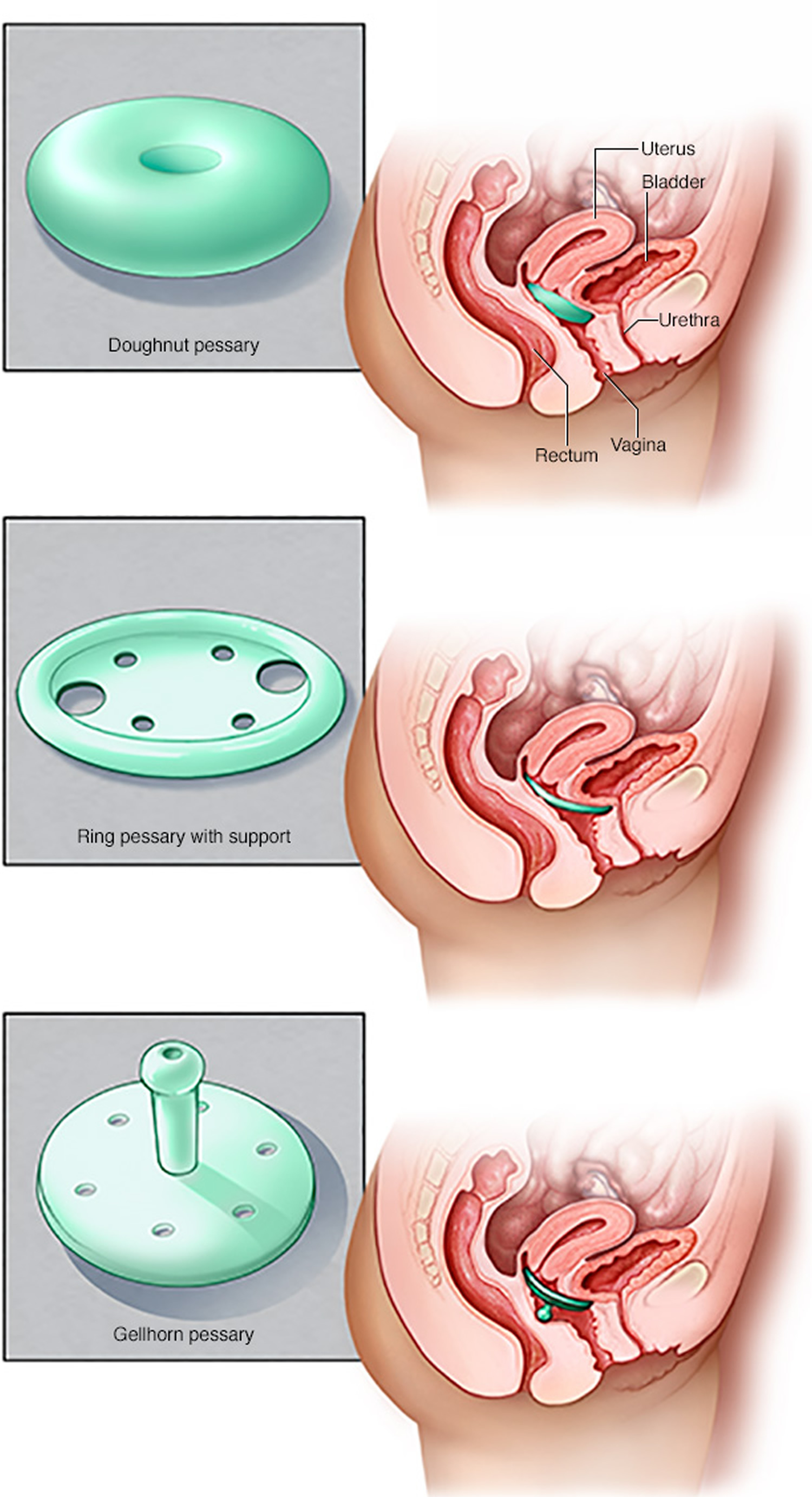
Note: Pessaries come in many shapes and sizes. The device fits into your vagina and provides support to vaginal tissues displaced by pelvic organ prolapse. Your health care provider can fit you for a pessary and help you decide which type would best suit your needs.
Surgery
If uterine prolapse is severe, your doctor might recommend surgery. Minimally invasive (laparoscopic) or vaginal surgery might be an option.
Surgery can involve:
- Repair of weakened pelvic floor tissues. This surgery is generally approached through the vagina but sometimes through the abdomen. The surgeon might graft your own tissue, donor tissue or a synthetic material onto weakened pelvic floor structures to support your pelvic organs.
- Removal of your uterus (hysterectomy). Hysterectomy might be recommended if uterine prolapse is severe.
Vaginal Repair
Prolapse of the vaginal wall (not the uterus) is the commonest type of prolapse. This type of prolapse may involve the front wall of the vagina (below the bladder), the back wall (below the rectum) or the top of the vagina (if the uterus has been removed) – called a vault prolapse. The surgery involves reinforcing the weakened area to prevent it from bulging and a mesh maybe considered for repeat surgery if the woman’s own tissues have not held together after a first operation. The surgery type is called:
- Anterior Repair
- Posterior Repair
- Vault Repair (Sacrospinous fixation or Abdominal Sacrocolpopexy)
Hysterectomy
A hysterectomy is a major operation that involves removing the womb (uterus). When performed for prolapse it is usually because the womb is protruding out of the vagina or is sitting very low in the vagina. It may be considered as a treatment for some types of pelvic organ prolapse, although there maybe an increased risk of vaginal vault prolapse (where the top of the vagina starts to prolapse). You cannot get pregnant after having a hysterectomy.
Prolapsed uterus treatment at home
Tightening the pelvic floor muscles using Kegel exercises helps to strengthen the muscles and reduces the risk of uterine prolapse 4.
Estrogen therapy after menopause may help with vaginal muscle tone.
Kegel Pelvic floor muscle training exercises
Pelvic floor muscle training exercises are a series of exercises designed to strengthen the muscles of the pelvic floor.
Pelvic floor muscle training exercises are recommended for:
- Women with urinary stress incontinence
- Men with urinary stress incontinence after prostate surgery
- People who have fecal incontinence
Pelvic floor muscle training exercises can help strengthen the muscles under the uterus, bladder, and bowel (large intestine). They can help both men and women who have problems with urine leakage or bowel control.
To perform Kegel exercises:
- Begin by emptying your bladder.
- Tighten (contract) your pelvic floor muscles as though you were trying to prevent urinating or passing gas.
- Hold the contraction for five seconds, and then relax for five seconds. If this is too difficult, start by holding for two seconds and relaxing for three seconds.
- Work up to holding the contractions for 10 seconds at a time.
- Aim for at least three to five sets of 10 repetitions each day (morning, afternoon, and night).
Because these muscles control the bladder, rectum, and vagina, the following tips may help:
- Insert a finger into your vagina. Tighten the muscles as if you are holding in your urine, then let go. You should feel the muscles tighten and move up and down.
It is very important that you keep the following muscles relaxed while doing pelvic floor muscle training exercises:
- Abdominal
- Buttocks (the deeper, anal sphincter muscle should contract)
- Thigh
A pelvic floor muscle training exercise is like pretending that you have to urinate, and then holding it. You relax and tighten the muscles that control urine flow. It is important to find the right muscles to tighten.
The next time you have to urinate, start to go and then stop. Feel the muscles in your vagina, bladder, or anus get tight and move up. These are the pelvic floor muscles. If you feel them tighten, you have done the exercise right.
You can do these exercises at any time and place. Most people prefer to do the exercises while lying down or sitting in a chair. After 4 to 6 weeks, most people notice some improvement. It may take as long as 3 months to see a major change.
After a couple of weeks, you can also try doing a single pelvic floor contraction at times when you are likely to leak (for example, while getting out of a chair).
A word of caution: Some people feel that they can speed up the progress by increasing the number of repetitions and the frequency of exercises. However, over-exercising can instead cause muscle fatigue and increase urine leakage.
If you feel any discomfort in your abdomen or back while doing these exercises, you are probably doing them wrong. Breathe deeply and relax your body when you do these exercises. Make sure you are not tightening your stomach, thigh, buttock, or chest muscles.
When done the right way, pelvic floor muscle exercises have been shown to be very effective at improving urinary continence.
If you are still not sure whether you are tightening the right muscles, keep in mind that all of the muscles of the pelvic floor relax and contract at the same time.
A woman can also strengthen these muscles by using a vaginal cone, which is a weighted device that is inserted into the vagina. Then you try to tighten the pelvic floor muscles to hold the device in place.
Kegel exercises may be most successful when they’re taught by a physical therapist and reinforced with biofeedback. If you are unsure whether you are doing the pelvic floor muscle training correctly, you can use biofeedback and electrical stimulation to help find the correct muscle group to work.
- Biofeedback is a method of positive reinforcement. Electrodes are placed on the abdomen and along the anal area. Some therapists place a sensor in the vagina in women or anus in men to monitor the contraction of pelvic floor muscles.
- A monitor will display a graph showing which muscles are contracting and which are at rest. The therapist can help find the right muscles for performing pelvic floor muscle training exercises.
There are physical therapists specially trained in pelvic floor muscle training. Many people benefit from formal physical therapy.
- Uterine prolapse. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/uterine-prolapse/symptoms-causes/syc-20353458[↩]
- The Causes, Symptoms and Treatment of Uterine Prolapse. FLEUR Womens Health. http://www.fleurhealth.com/blog/the-causes-symptoms-and-treatment-of-uterine-prolapse/[↩]
- Pelvic Organ Prolapse. http://www.gynaecologyspecialistlondon.co.uk/conditions-treatments/pelvic-organ-prolapse/[↩]
- Uterine prolapse. Medline Plus. https://medlineplus.gov/ency/article/001508.htm[↩][↩]





{kind=link}