Contents
- Retinopathy of prematurity
- Who is at risk for retinopathy of prematurity?
- How will I know if my baby is getting retinopathy of prematurity?
- How many babies have retinopathy of prematurity?
- Why are eye exams recommended after discharge from the hospital?
- What determines how bad retinopathy of prematurity gets?
- How can vision loss be prevented?
- If my baby has retinopathy of prematurity, what happens?
- Can retinopathy of prematurity be treated?
- Retinopathy of Prematurity Stages
- Retinopathy of prematurity causes
- Retinopathy of prematurity pathophysiology
- Retinopathy of prematurity prevention
- Retinopathy of prematurity signs and symptoms
- Retinopathy of prematurity complications
- Retinopathy of prematurity diagnosis
- Retinopathy of prematurity differential diagnosis
- Retinopathy of prematurity treatment
- Retinopathy of prematurity prognosis
Retinopathy of prematurity
Retinopathy of prematurity (ROP) is a serious eye condition that affects the retina of extremely premature babies (born before 30 weeks or who weigh less than 3 pounds [less than 1500 grams] at birth) 1, 2, 3, 4, 5, 6, 7. Retinopathy of prematurity (ROP) occurs when blood vessels in the developing retina (the light-sensitive tissue at the back of the eye) grow abnormally, which can lead to scarring and potentially retinal detachment – a serious eye condition where the retina, the light-sensitive tissue at the back of the eye, pulls away from its normal position. Premature babies, especially those born very early before 30 weeks or with a birth weight of less than 3 pounds are at higher risk for retinopathy of prematurity (ROP). The retina’s blood vessels are still developing in the womb, and a premature birth can disrupt this process. While the exact cause of retinopathy of prematurity (ROP) isn’t fully understood, high levels of supplemental oxygen used in the neonatal intensive care unit (NICU) to premature infants especially for an extended duration can also contribute to the development of retinopathy of prematurity (ROP). Today, the use of oxygen is closely monitored, very carefully calculated and controlled. As a result oxygen use is no longer implicated as the sole or even a primary factor in retinopathy of prematurity development. It is well known that the sicker and smaller a baby is the more likely to develop retinopathy of prematurity. Therefore, retinopathy of prematurity prevention strategies include reducing the likelihood of premature birth through good prenatal care and careful monitoring of babies in the neonatal intensive care unit (NICU).
Retinopathy of prematurity has no signs or symptoms when it first develops in a newborn. The only way to diagnose it is through an eye exam by an pediatric ophthalmologist who is experienced in the diagnosis and treatment of retinopathy of prematurity. Infants of low birthweight (under 1500 grams or 3.3 pounds) and gestational age (30 weeks or less)—as well as infants deemed higher risk by the neonatologist due to multiple births, oxygen exposure after birth are screened with either bedside eye exams or digital pictures of the back of the eye (retina). Once retinopathy of prematurity progresses to a certain level of severity, treatment is recommended. Treatment is most often required between 34 to 38 weeks of gestation. Retinopathy of prematurity (ROP) is graded from Stage 1 to Stage 5, with Stage 1 being the mildest and Stage 5 being the most severe, potentially leading to blindness.
Milder forms of retinopathy of prematurity often regress or heal without treatment; however, more advanced retinopathy of prematurity can lead to severe visual impairment or blindness. Retinopathy of prematurity remains a serious eye problem despite recent advances in neonatology because it can lead to eye problems such as nearsightedness (myopia), lazy eye (amblyopia), crossed eyes (strabismus) or glaucoma for premature infants later in life.
Retinopathy of prematurity treatments may include monitoring, laser surgery, or eye injections. There are typically 2 options for treatment once it is found that a child has severe retinopathy of prematurity. The first treatment type is laser which is applied to the immature or undeveloped part of the retina. This treatment has been around for many years and is still the most common treatment for retinopathy of prematurity. The second type of treatment is an injection of anti-VEGF drugs (bevacizumab, ranibizumab, and aflibercept have been used) into your baby’s eye. This medication injection stops a signal that is causing the abnormal blood vessels in retinopathy of prematurity to form. These medications may be used as an alternative to, or in addition to, laser treatment. The injection is a newer treatment than the laser treatment. The effect of laser or injection treatment for retinopathy of prematurity is usually good with the disappearance of abnormal blood vessels from retinopathy of prematurity. But, even with good diagnosis and timely treatment, the retinopathy of prematurity sometimes continues to worsen and the retina pulls away from the back of the eye this is called a retinal detachment. Eyes with retinal detachment caused by retinopathy of prematurity can have very poor vision. A retinal detachment can be treated with a different type of surgery by a retina surgeon who has experience treating retinopathy of prematurity. Despite best treatment, some eyes with retinopathy of prematurity get worse and go on to permanent and severe vision loss.
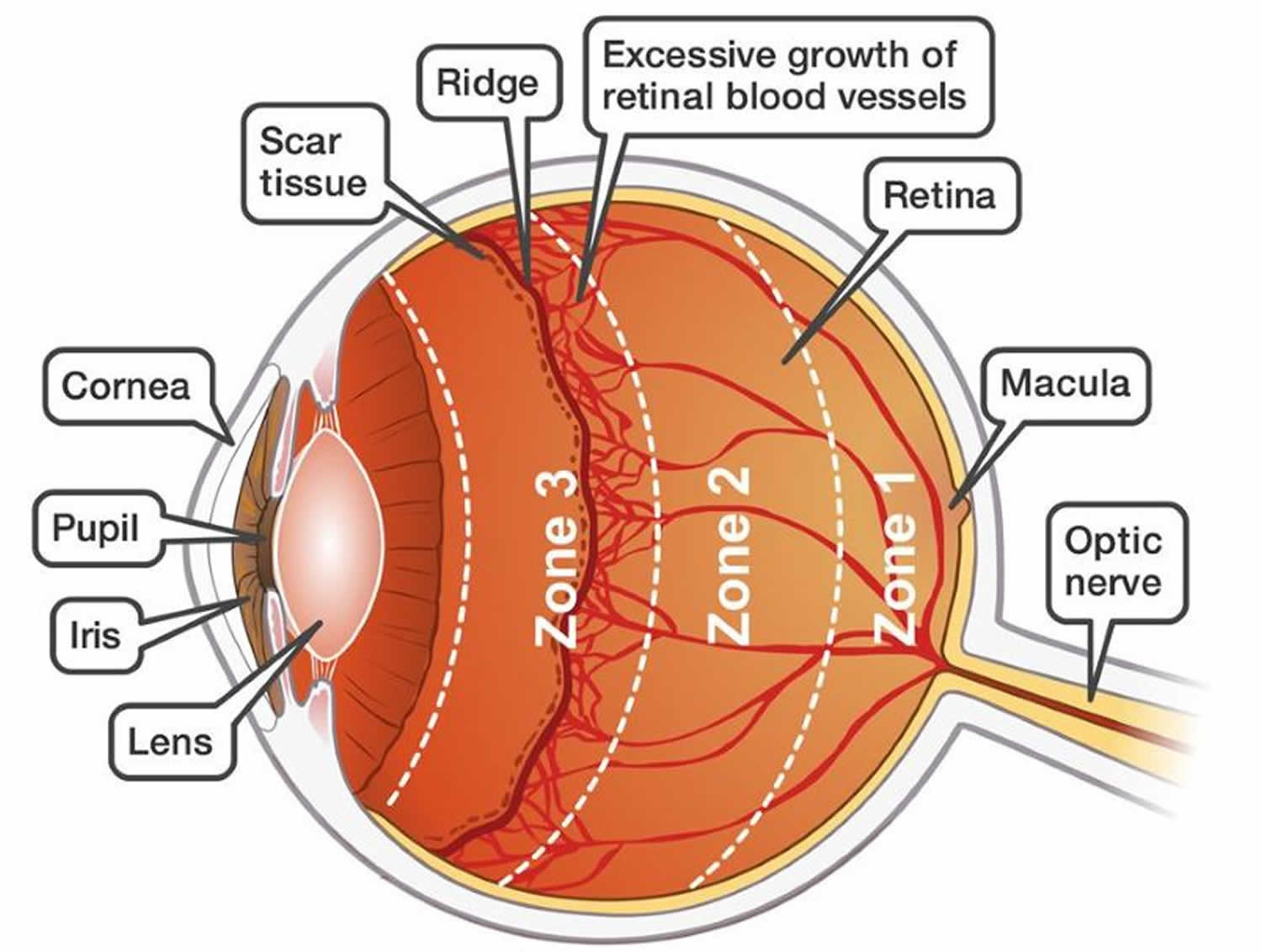
Figure 1. Eye anatomy

Figure 2. Retinopathy of prematurity with pre-plus disease
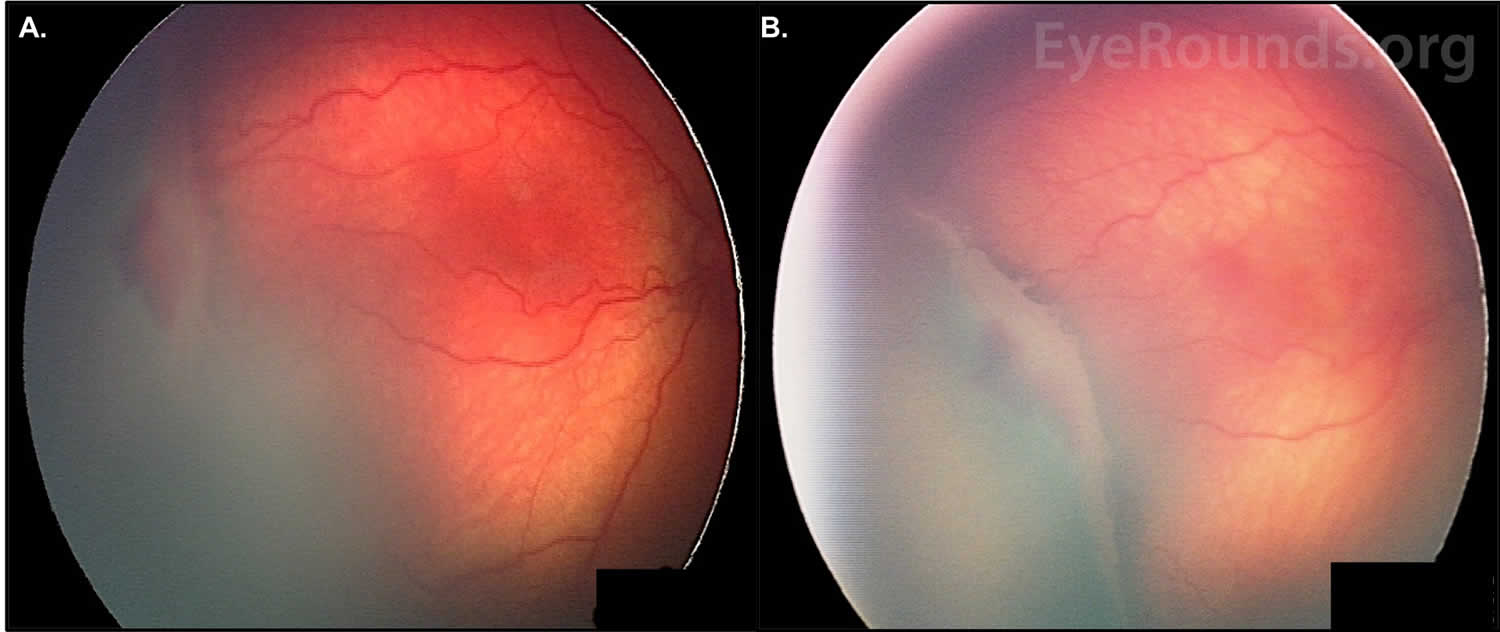
Footnotes: Fundus photos of a baby taken at 46 weeks post-conceptual age. (A – Right eye) Stage 3 retinopathy of prematurity is present temporally. A thick ridge separates the posterior vascularized retina from the avascular anterior. There is a section of hemorrhage immediately anterior to the ridge. (B) A wider view of the ridge, offering a better depiction of its raised dimensions. There is fibrovascular proliferation on the posterior edge.
[Source 8 ]Figure 3. Retinopathy of prematurity with dilated veins and tortuous arteries in the posterior pole of both eyes
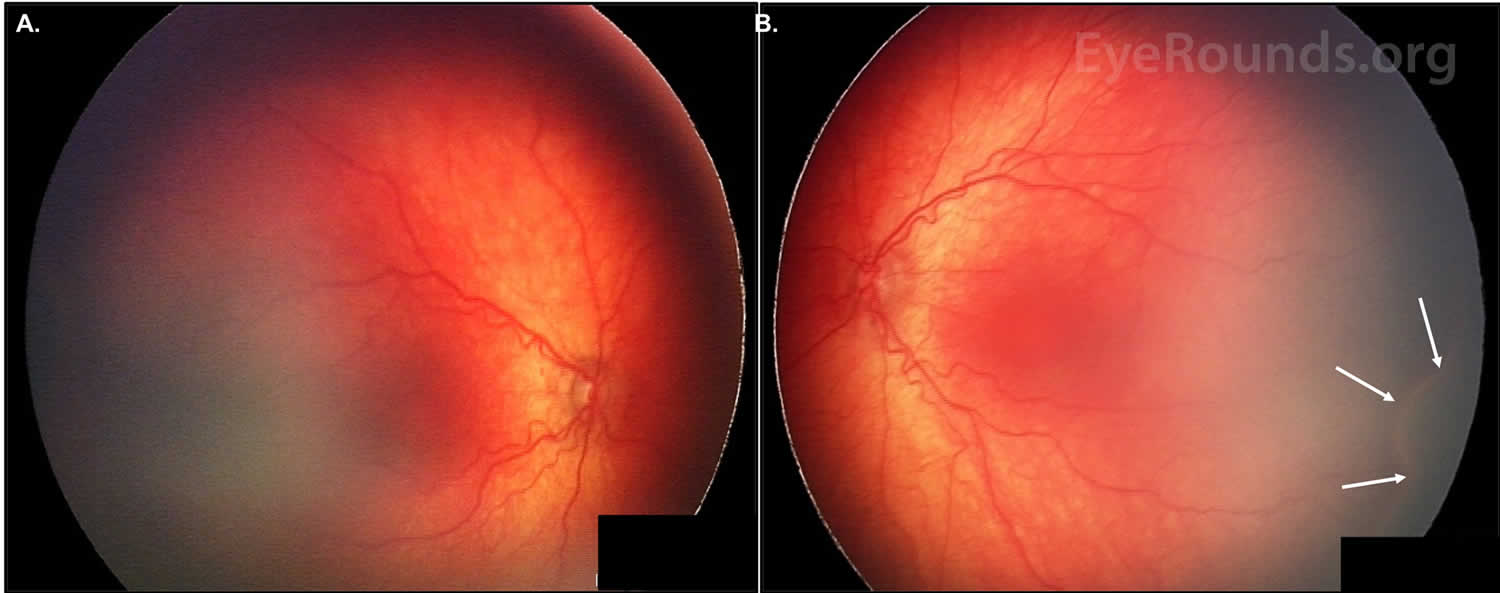
Footnotes: Fundus photos of a baby, taken at 46 weeks post-conceptual age. (A) Pre-plus disease is present right eye. (B) Plus disease is present left eye. A ridge can be seen inferotemporally (white arrows).
[Source 8 ]Who is at risk for retinopathy of prematurity?
Babies are at risk for retinopathy of prematurity if they’re born before 30 weeks of pregnancy or weigh less than about 3 pounds at birth. If your baby is at risk, an eye specialist will check them for retinopathy of prematurity.
Babies are also more likely to develop retinopathy of prematurity if they have:
- Breathing problems (and if they get too much oxygen therapy to treat breathing problems)
- Infections or other medical problems that premature babies may have — like problems with their heart, lungs, or brain.
How will I know if my baby is getting retinopathy of prematurity?
Doctors cannot predict which babies will develop retinopathy of prematurity. All babies weighing less than 1250 grams at birth will have regular eye examinations after their gestational age reaches 30 to 31 weeks. These examinations are undertaken by a medical eye specialist known as an ophthalmologist. To look at the back of your baby’s eyes the pupil (black circle in the middle of the colored part at the front of the eye) needs to be dilated. Eye drops are used to dilate the pupils. The examination only takes a couple of minutes. Your baby may be minimally upset by these examinations and will settle very quickly once the eyes have been checked.
How many babies have retinopathy of prematurity?
There are about 3.9 million infants born in the U.S. each year. About 14,000 get retinopathy of prematurity and 90% of those with retinopathy of prematurity have only mild disease 9. About 1,100- 1,500 develop retinopathy of prematurity severe enough to need medical treatment and 400-600 infants each year in the U.S. become legally blind from retinopathy of prematurity 9. According to the World Health Organization (WHO) estimates, there are 1.4 million blind children worldwide, retinopathy of prematurity is the cause of blindness in about 50,000 of these children 10, 11.
A Korean study reported a 20.7% incidence of retinopathy of prematurity (88 of 425 premature babies), with a gestational age of 28 weeks or less and a birth weight of 1000 g or less were the most significant risk factors 12. A study from Singapore reported a 29.2% incidence of retinopathy of prematurity (165 of 564 extremely low birth weight babies), with a median age of onset of 35 weeks (range, 31-40 week) postmenstrual age 13. The risk factors for development of threshold retinopathy of prematurity by regression analysis were maternal preeclampsia, birth weight, pulmonary hemorrhage, duration of ventilation, and duration of continuous positive airway pressure (CPAP) 13.
Why are eye exams recommended after discharge from the hospital?
It is VERY IMPORTANT to have your baby’s eyes examined after discharge from the hospital since retinopathy of prematurity may not be gone before discharge. The timing of these eye exams is
very important because delays in examination will delay treatment. Delay of treatment can increase the risk of vision loss from retinopathy of prematurity since you will not be able to tell whether your baby’s retinopathy of prematurity has gotten worse just by looking at him or her. Also, even with successful treatment of retinopathy of prematurity, prematurity may lead to other vision problems. Prematurity is a risk factor for the development of amblyopia (lazy eye), crossed eyes (strabismus), the need for glasses (even at a young age), and cortical visual impairment. Therefore, every premature infant needs the long-term care with an pediatric ophthalmologist (children eye doctor).
It is recommended that all babies who are small enough to have their eyes checked while in hospital should be offered an eye examination at one year of age. A small number of these children are found to have crossed eyes (strabismus) or need glasses for clearer vision, even if they did not have any retinopathy of prematurity while in hospital. It is strongly recommended that you make sure your baby has an eye examination at about one year of age. Depending on the finding at this check-up further eye checks may be needed.
What determines how bad retinopathy of prematurity gets?
Birth weight and gestational age are the most important risk factors for getting severe retinopathy of prematurity 9. Other things seen in infants with retinopathy of prematurity include anemia, poor weight gain, blood transfusion, respiratory distress/breathing difficulties, bleeding in the brain and the overall health of the infant 9. Close monitoring of oxygen levels can limit how bad the retinopathy of prematurity gets. The amount of light the baby is exposed to does not affect how bad the retinopathy of prematurity gets 9.
How can vision loss be prevented?
The early prediction or control of premature birth poses significant challenges, but effective neonatal care coupled with timely screening and urgent laser therapy can substantially decrease the occurrence of blindness or visual impairment in infants with retinopathy of prematurity.
Early screening for retinopathy of prematurity is imperative to identify infants at risk of developing severe, vision-threatening stages of the condition. Typically, screening is conducted by a skilled ophthalmologist within the neonatal unit using indirect ophthalmoscopy. Determining whom to screen and the timing of screening hinges on various factors, including the quality of neonatal care provided. In settings where care falls short, larger, more mature infants should also undergo screening, as they too can be susceptible to vision-threatening retinopathy of prematurity.
Given that retinopathy of prematurity manifests after birth, with onset occurring within the initial weeks of life, the initial screening examination should occur no later than 30 days post-birth. Subsequent follow-up screenings may be necessary, potentially even after the infant has been discharged from the neonatal unit.
Prompt treatment is essential for all infants exhibiting sight-threatening stages of retinopathy of prematurity and should be initiated within 48 to 72 hours.
Furthermore, diligent monitoring of all preterm infants is crucial, as they face heightened risks of other conditions that can result in vision loss. Such risks are amplified among infants with a history of retinopathy of prematurity, particularly those who have undergone treatment. Refractive errors, including early-onset severe myopia, are the most prevalent conditions. Additionally, conditions such as crossed eyes (strabismus) and cerebral visual impairment (amblyopia) occur at higher rates compared to full-term infants.
If my baby has retinopathy of prematurity, what happens?
In most babies retinopathy of prematurity is mild and over a period of weeks the retinopathy of prematurity gradually disappears. Your baby’s eye doctor (ophthalmologist) will check your baby’s eyes every one or two weeks and you will be told the result of each examination.
Can retinopathy of prematurity be treated?
Yes, but remember very few babies develop retinopathy of prematurity that is bad enough to need treatment. Mild retinopathy of prematurity does not need treatment as it almost always goes away by itself. If your baby needs treatment this is called threshold disease (severe stage 3 retinopathy of prematurity). If your baby develops threshold retinopathy of prematurity treatment options will be discussed with you. The treatment is generally done with laser and in 90% of babies needing treatment the retinopathy of prematurity disappears and sight is preserved.
If your baby may need treatment more information will be given to you and you can discuss the situation with the pediatricians and ophthalmologist caring for your baby.
Retinopathy of Prematurity Stages
There are 5 different stages of retinopathy of prematurity. Eye doctors use these stages to keep track of how serious retinopathy of prematurity is. The stages range from stage 1 (mild) to stage 5 (severe):
- Stages 1 and 2: Babies in these stages usually get better without treatment and go on to have healthy vision. Your baby’s eye doctor will watch your baby’s eye carefully to see if his/her retinopathy of prematurity gets worse.
- Stage 3: Some babies who develop stage 3 retinopathy of prematurity get better with no treatment and go on to have healthy vision. But others need treatment to stop abnormal blood vessels from damaging the retina and causing retinal detachment (an eye problem that can cause vision loss).
- Stage 4: Babies in stage 4 retinopathy of prematurity have partially detached retinas and need treatment.
- Stage 5: In stage 5 retinopathy of prematurity, the retina detaches completely. Even with treatment, babies in stage 5 may have vision loss or blindness.
Both stages 4 and 5 retinopathy of prematurity with detached retinas are very serious. Babies in these stages often need surgery, but even with treatment, they may have vision loss. That’s why eye doctors usually start treatment in stage 3.
It’s also possible for babies in any stage to get worse quickly and need treatment. That’s why it’s so important to make sure your baby gets their follow-up exams on schedule. Finding and treating retinopathy of prematurity early is the best way to lower the chances it will cause serious problems.
How do eye doctors describe retinopathy of prematurity?
Retinopathy of prematurity is described by its location in the eye (the Zone), by the severity of the disease/how bad it is (the Stage) and by how the retinal vessels look (Plus Disease).
The first stage of retinopathy of prematurity is seen as a line on the retina that separates normal retina from premature retina. Stage 2 retinopathy of prematurity is when a ridge which has height and thickness forms on the retina. Stage 3 is when there is growth of fragile new abnormal blood vessels on the retina. As retinopathy of prematurity gets worse the blood vessels may get thick and wavy this is called “Plus Disease”. “Plus disease” is the dilation and tortuosity of the retinal vessels in the posterior pole (most posterior part) of the retina.
Retinopathy of prematurity causes
Normally, the blood vessels of the retina start to develop in the fourth month of pregnancy (around 16 weeks of gestational age) and finish developing around the due date, or 9 months of pregnancy, which is why retinopathy of prematurity is rare in term babies 6. This process is considered complete when the retinal blood vessels reach the boundary between the retina and ciliary body, known as the ora serrata. In normal fetal development the retinal blood vessel reaches the nasal ora serrata by 36 weeks gestational age and the temporal ora serrata by 40 weeks gestational age 14. If a baby is born very early, these blood vessels may stop developing normally 5, 6. The retina then develops new blood vessels that are abnormal. This is called retinal neovascularization (NV) – the formation of new blood vessels. These abnormal blood vessels in the retina can grow in the wrong direction. These abnormal blood vessels are attached to the retina — so if they grow too far in the wrong direction, they can pull the retina up off the back of the eye. This is a type of retinal detachment. This can lead to vision loss or blindness if not treated promptly. Treatment typically involves surgery to reattach the retina.
Most research suggests that a low birth weight, a young gestational age, and the severity of illness (eg, infant respiratory distress syndrome [RDS], bronchopulmonary dysplasia [BPD], sepsis) are associated risk factors 15. Other associations have been described; however, the severity of systemic illness appears to be a major predictor of severe disease. The smallest, sickest, and most immature infants are at the highest risk for serious disease 15, 16, 17.. Race is also a factor: Black infants appear to have less severe retinopathy of prematurity 16, 17. The exact mechanism for the decreased incidence of progression to surgery in Black infants has not been described. Bizzaro et al 18 showed a strong genetic predisposition to retinopathy of prematurity when comparing monozygotic twins with dizygotic twins.
Risk factors for developing retinopathy of prematurity
Retinopathy of prematurity is a disease of the smallest and the sickest infants. Premature birth (<30 weeks gestational age) and low birthweight (<1500 grams) are the primary risk factors 19. In a review of 1413 infants with birth weight less than 1500 g and/or gestational age of 26 to 31 weeks, infants with a birth weight below the tenth percentile for gestational age were more likely to develop any stage of retinopathy of prematurity than their appropriate-for-gestational age peers and they were more likely to develop severe retinopathy of prematurity 19.
Other risk factors for the development of retinopathy of prematurity include 20:
- Multiple births 21
- Infant respiratory distress syndrome, duration of mechanical ventilation, and steroid use for bronchopulmonary dysplasia are considered risk factors for the development of retinopathy of prematurity 22, 21
- bronchopulmonary dysplasia is considered a risk factor for the progression of retinopathy of prematurity 20
- Central nervous system (brain and spinal cord) injuries: intraventricular hemorrhage and periventricular leukomalacia are considered risk factors for the progression of retinopathy of prematurity 23, 24
- Low plasma immunoglobulin factor 1 (IGF-1) levels: Immunoglobulin factor 1 (IGF-1) is thought to mediate vascular endothelial growth factor (VEGF); hence, low plasma immunoglobulin factor 1 (IGF-1) levels may be a potential risk factor for the development of retinopathy of prematurity 23
- Hyperglycemia (high blood sugar in baby) 25
- Sepsis, White race and blood transfusion 21
- Proteinuria due to shared embryogenesis between retinal vascularity and kidney function 23.
Retinopathy of prematurity pathophysiology
Retinopathy of prematurity occurs in premature infants who are born before the retinal vessels complete their normal growth, and occurs in 2 phases:
- Delays in physiologic retinal vascular development that leads to damages in newly developed capillaries. Occurs in the setting of oxygen stresses and other stresses (described below)
- Aberrant neovascularization that grows into the vitreous instead of the retina
Normal retinovascular development in humans is believed to occur initially through vasculogenesis, or de novo formation of vessels from precursor endothelial cells, before and at about 14–16 weeks of gestation, vascularizing the posterior pole through 22 weeks of gestation. Following vasculogenesis, angiogenesis occurs via budding from existing vessels to extend the retinal vessels into the periphery and the other plexi. The vascularization of the deeper plexi is associated with Müller cells in human. In mice, astrocytes may also play a role in sensing physiologic hypoxia and upregulating vascular endothelial growth factor (VEGF). Ensuing migrating endothelial cells are attracted by a gradient of vascular endothelial growth factor (VEGF) toward the ora serrata 26.
In a representative animal model of retinopathy of prematurity that recapitulated stresses to premature infants, regulation of signaling through the VEGF receptor 2 (VEGFR2) specifically restored the orientation of dividing endothelial cells to allow them to grow in an ordered fashion toward the ora serrata 27, 28. This discovery showed that inhibition of an overactivated angiogenic pathway through VEGF receptor 2 (VEGFR2) in endothelial cells caused abnormal vascularization into the vitreous and interfered with normal retinal vascular development. Regulation of the VEGF receptor 2 (VEGFR2) pathway not only inhibited intravitreal and extraretinal neovascularization but also facilitated angiogenesis into the peripheral retina 29, 30. This process is different from the pathophysiology of many adult retinovascular diseases 31.
Clinical studies have attempted to regulate VEGF receptor 2 (VEGFR2) signaling in endothelial cells using intravitreal neutralizing antibodies to vascular endothelial growth factor (VEGF), because these can be delivered safely in the premature infant eye with intravitreal injections. However, the intravitreal delivery of an antibody or fusion protein that binds the ligand (VEGF) does not allow for specific regulation of VEGFR2 in endothelial cells, since VEGF receptors on glia and neural cells are also affected. An additional study in a representative model showed that intravitreal neutralizing antibody to VEGFA led to retinal capillary dropout after oxygen stresses, followed by reactivation of neovascularization into the vitreous 32. This is similar to what happens in some infant eyes 33. In addition, reduced expression of vascular endothelial growth factor A (VEGFA) in the experimental model caused thinning of the retinal layers, whereas reduction in only some of the forms of VEGF did not lead to retinal thinning 34. This research led to the idea to pursue studies identifying an appropriate dose of intravitreal anti-VEGF medications that would be effective and safe 34. Recently, a clinical study compared infants with type 1 retinopathy of prematurity, who received bilateral intravitreal bevacizumab (0.25 mg), to an untreated control group of infants with less severe retinopathy of prematurity matched by sex, degree of prematurity, and postmenstrual age. Vascularization into the peripheral avascular retina was measured on retinal images taken with the same contact camera. The treated group all responded with retinopathy of prematurity regression and had greater extension of retinal vascularization peripherally than the less severe, untreated group 35 This study provides evidence supporting the basic research and suggests that inhibition of vitreous vascular endothelial growth factor (VEGF) may allow linear intraretinal blood vessel development to extend to the ora serrata and reduce neovascularization into the vitreous. Long-term and additional studies are needed, including for safety.
In retinopathy of prematurity, premature birth delays the normal process of retinal vascularization. Other factors, such as oxygen-induced vascular injury, also play a role. Risk factors for retinopathy of prematurity can include high oxygen at birth, fluctuations in oxygenation, poor postnatal growth, poor nutrition, and possible oxidative stress. The role of oxygen in the causation of retinopathy of prematurity is complex. Some studies have shown that keeping the oxygen saturation at a lower level from birth can reduce the rate of advanced retinopathy of prematurity, but other studies have found increased mortality rates following lower oxygen saturation 36.
Retinopathy of prematurity prevention
Screenings of infants at risk of retinopathy of prematurity with appropriate timing of exams and follow up is essential to identify infants in need of treatment 21. It is important to recognize that screening recommendations may vary by location. For example, in some countries in Asia, retinopathy of prematurity can occur in babies of older gestational age or larger birth weight 37.
The text and table below summarize the current recommendations for retinopathy of prematurity screening in United States 38.
- Low birthweight (≤1500 g)
- Gestational age ≤30 weeks
- Birthweight between 1500 and 2000 g or gestational age >30 weeks, but believed by their pediatrician or neonatologist to be at risk for retinopathy of prematurity (e.g., history of hypotension requiring inotropic support; received supplemental oxygen for more than a few days or without oxygen saturation monitoring)
Recommendations published by a multisociety consortium in 2018 state that infants should be screened “by an ophthalmologist who is experienced in the examination of preterm infants for retinopathy of prematurity using a binocular indirect ophthalmoscope” 38.
The American Academy of Pediatrics (AAP) and the American Academy of Ophthalmology (AAO) have joint recommendations for infants who should be screened for retinopathy of prematurity 39. Screening should include those infants with a birth weight of less than 1500 g or a gestational age (GA) of 31 weeks or less, as well as selected infants with a birth weight of 1500-2000 g or a gestational age of more than 31 weeks with an unstable clinical course, including those who require cardiorespiratory support and those who are believed to be at high risk by their attending pediatrician or neonatologist.
The retinal screening examinations should be performed by an experienced ophthalmologist after pupillary dilation using binocular indirect ophthalmoscopy to detect retinopathy of prematurity.
The time of initiation of retinopathy of prematurity screening should be based on the infant’s age. The onset of serious retinopathy of prematurity correlates better with postmenstrual age (gestational age at birth + chronologic age) than with postnatal age; this means that the youngest infants at birth take the longest time to develop serious retinopathy of prematurity.
- Postmenstrual age (PMA) = Gestational Age (GA or the number of weeks the baby was in the womb) + Chronological Age (the number of weeks and days since the baby was born)
Postmenstrual Age (PMA) is calculated by adding the baby’s gestational age at birth (GA) to the number of weeks and days that have passed since birth (Chronological Age). Postmenstrual Age (PMA) is crucial for determining when and how to screen and treat retinopathy of prematurity (ROP), as the condition’s progression is often linked to Postmenstrual Age (PMA).
Screening guidelines have been the focus of relatively recent studies. The issue of cost-effectiveness versus missing cases is controversial. In addition, Subhani et al 40 suggested that infants should be examined by age 4-6 weeks, contrary to the standard postmenstrual age criteria. The American Academy of Pediatrics guidelines for retinopathy of prematurity screening suggested a schedule for detecting prethreshold retinopathy of prematurity (99% confidence), usually well before any required treatment. See Table 1 below.
The American Academy of Pediatrics (AAP) and the American Academy of Ophthalmology (AAO) guideline should be considered tentative rather than evidence-based for infants with a gestational age of 22-23 weeks because of the small number of survivors in these categories.
Follow-up examinations are based on initial examination findings. Most infants are screened every 2 weeks. More frequent (once a week or less) follow-up is recommended in stage 1 or 2 retinopathy of prematurity in zone 1 and in stage 3 retinopathy of prematurity in zone 2. The presence of “plus disease” requires careful evaluation because, in these cases, peripheral ablation is more appropriate rather than observation alone.
Screening examinations are continued until the blood vessels reach the anterior edge of the retina (complete retinal vascularization around 40 weeks gestation) or until postmenstrual age of 45 weeks with no prethreshold disease (defined as stage 3 retinopathy of prematurity in zone 2, any retinopathy of prematurity in zone 1) or no worse retinopathy of prematurity is present.
Table 1. Timing of First Eye Examination Based on Gestational Age at Birth
| Gestational Age at Birth (weeks) | Chronologic Age (weeks) | Postmenstrual Age (weeks) |
|---|---|---|
| 22 | 9, but consider earlier screening per clinical judgment | 31 |
| 23 | 8, but consider earlier screening per clinical judgment | 31 |
| 24 | 7 | 31 |
| 25 | 6 | 31 |
| 26 | 5 | 31 |
| 27 | 4 | 31 |
| 28 | 4 | 32 |
| 29 | 4 | 33 |
| 30 | 4 | 34 |
| 31 (if necessary) | 4 | 35 |
| 32 (if necessary) | 4 | 36 |
Follow-Up Intervals
Current recommendations for retinopathy of prematurity screening in United States 38.
- Low birthweight (≤1500 g)
- Gestational age ≤30 weeks
- Birthweight between 1500 and 2000 g or gestational age >30 weeks, but believed by their pediatrician or neonatologist to be at risk for retinopathy of prematurity (e.g., history of hypotension requiring inotropic support; received supplemental oxygen for more than a few days or without oxygen saturation monitoring)
Preterm infants meeting screening criteria should have retinal exams performed by ophthalmologists with adequate training in retinopathy of prematurity management. There is increasing use of obtaining retinal images by trained personnel that are then reviewed by ophthalmologists 41. The initial exam should be based on the infant’s age (see Table 1 above). Follow-up recommendations were updated in 2019 by the American Academy of Pediatrics and depend on the location and stage of retinopathy of prematurity 38.
The timings of follow-up examinations are based on retinal exam findings as classified by International Classification of Retinopathy of Prematurity 3 38, 42:
- Recommended follow-up visit within 1 week
- Zone 1: immature vascularization, stage 1 or 2 retinopathy of prematurity
- Posterior zone 2: immature vascularization
- Suspected presence of aggressive retinopathy of prematurity (A-ROP)
- Recommended follow-up visit in 1–2 weeks
- Zone 1: unequivocally regressing retinopathy of prematurity
- Posterior zone 2: immature vascularization
- Zone 2: stage 2 retinopathy of prematurity
- Recommended follow-up visit in 2 weeks
- Zone 2: immature vascularization, stage 1 retinopathy of prematurity, or unequivocally regressing retinopathy of prematurity
- Recommended follow-up visit in 2–3 weeks
- Zone 2: regressing retinopathy of prematurity
- Zone 3: stage 1 or 2 retinopathy of prematurity
Termination of acute retinal screening examinations is based on age and retinal findings. Examinations can be stopped in these cases 38, 42:
- Retina is fully vascularized
- Zone 3 retinal vascularization without previous retinopathy of prematurity in zones 1 or 2 (may need a confirmatory exam if post-menstrual age (PMA) <35 weeks)
- Post-menstrual age (PMA) = 45 weeks and no type 1 retinopathy of prematurity (i.e. ,”pre-threshold disease”, defined as stage 3 retinopathy of prematurity in zone 2 or any retinopathy of prematurity in zone 1, or worse retinopathy of prematurity)
- If previously treated with anti-VEGF injections, follow until at least post-menstrual age =65 weeks (infant will need close follow-up during the time of highest risk for disease reactivation [post-menstrual age = 45–55 weeks]) 38
- Retinopathy of prematurity has fully regressed (ensure there is no abnormal vascular tissue present that can reactivate and progress)
After acute retinal screening examinations are terminated, preterm infants should be seen within 4–6 months after discharge from the neonatal intensive care unit for vision development. Preterm infants are at increased risk for developing strabismus, amblyopia, high refractive error, cataract, and glaucoma.
NOTE: Postmenstrual age (PMA) = Gestational Age (GA or the number of weeks the baby was in the womb) + Chronological Age (the number of weeks and days since the baby was born)
Postmenstrual Age (PMA) is calculated by adding the baby’s gestational age at birth (GA) to the number of weeks and days that have passed since birth (Chronological Age). Postmenstrual Age (PMA) is crucial for determining when and how to screen and treat retinopathy of prematurity (ROP), as the condition’s progression is often linked to Postmenstrual Age (PMA).
Retinopathy of prematurity signs and symptoms
There are no signs of retinopathy of prematurity that you can see. In advanced cases of retinopathy of prematurity (ROP), the retina may partially or completely pull away from its normal position at the back of the eye. This is called retinal detachment and it can cause vision loss and blindness.
If your baby had retinopathy of prematurity that caused eye damage, you may later notice that:
- Your baby’s eyes wander, shake, or make other unusual movements
- Your baby’s eyes don’t follow objects
- Your baby’s eye pupils (the dark, circular opening in the center of your eye that allows light to enter and is surrounded by the colored iris, which controls the pupil’s size) look white
- Your baby has trouble recognizing faces
Babies who had retinopathy of prematurity are also more likely to have other eye problems as they get older, including:
- Retinal detachment
- Nearsightedness (myopia)
- Amblyopia (lazy eye)
- Crossed eyes (strabismus).
If your child had retinopathy of prematurity when he/she was younger, it’s important to make sure your child get regular checkups and eye exams. Finding and treating eye problems early will help protect your child’s vision as they get older.
Retinopathy of prematurity complications
Late complications of retinopathy of prematurity include nearsightedness (myopia), amblyopia (“lazy eye” – reduced vision in one eye caused by abnormal visual development early in life), strabismus (crossed eyes), nystagmus (a condition where your eyes make rapid, repetitive, uncontrolled movements), cataracts, retinal breaks, and retinal detachment.
VanderVeen et al 43 observed strabismus is often variable and may improve by age 9 months.
Follow-up by an ophthalmologist is required on a long-term basis.
The peripheral retina of adults with regressed or treated retinopathy of prematurity is not normal. The abnormal development of the peripheral retina can lead to thinning (lattice degeneration) of the peripheral retina, retinal holes, tears, and detachments later in life 44. Young adults with treated or regressed retinopathy of prematurity should be counselled about these risks and should have regular dilated funduscopic examinations by a retina specialist. Special attention should be paid to teenagers who engage in contact sports; they and their parents should be taught the signs and symptoms of retinal tears and detachments. More frequent examinations (eg, at the start and conclusion of their sport’s season) may be prudent.
The most feared complication in retinopathy of prematurity is retinal detachment or macular folds, which can lead to severe vision deficits and blindness. There are a number of other complications related to this disease that can affect visual development. Myopia is a common finding in premature infants with or without retinopathy of prematurity. Infants with regressed retinopathy of prematurity also have an increased incidence of strabismus, amblyopia, and anisometropia. Research is ongoing to determine if myopia is reduced after anti-VEGF vs. laser. However, progressive stage 4 or 5 retinopathy of prematurity can be treated and preserve vision and the eye. Some vision is not only helpful for development but for future treatments with advances in research.[58]
Even in the absence of macular folds or structural abnormalities, exudative detachment may occur after laser for type 1 retinopathy of prematurity, leading to macular scarring and decreased visual outcomes.[59]
Extreme prematurity is a risk for retinopathy of prematurity and for reduced neurocognitive function. Some large studies have found an association with reduced neurocognitive function following certain types of anti-VEGF agents for retinopathy of prematurity.[60] [61] However, these large-scale studies have selection bias. Smaller studies have not reported adverse effects on neurocognitive function following anti-VEGF treatment for retinopathy of prematurity, but these studies had small sample sizes. In one meta-analysis, anti-VEGF treatment was not associated severe cognitive impairment,[62] but another meta-analysis did report increased risk of moderate cognitive impairment.[63] Long-term follow-up is needed from clinical trials (BEAT-retinopathy of prematurity, retinopathy of prematurity3 and 4, RAINBOW, FIREFLEYE and BUTTERFLEYE). Although data from BEAT-retinopathy of prematurity was limited to a small sample size,[64] neurodevelopmental data from FIREFLEYE and RAINBOW are reassuring.[65] [66]
Retinopathy of prematurity diagnosis
If your baby is at risk for retinopathy of prematurity, she/he need a dilated eye exam by an eye doctor (pediatric ophthalmologist) a few weeks after they’re born — usually between 4 to 9 weeks after birth. Ask your baby’s eye doctor when your baby needs an eye exam before you leave the hospital.
During the exam, the eye doctor (pediatric ophthalmologist) will give your baby some eye drops to dilate (widen) their pupils. Your baby’s eye doctor will check every part of your baby’s eye for problems — especially the retina.
The structure of the retina, especially the macula, of infants with retinopathy of prematurity does not closely correlate with the function (vision). Specialized testing (Teller Acuity Cards) may be necessary early on to fully appreciate the visual function of each eye. Significant differences in the acuity between the eyes can rapidly lead to amblyopia of the poorer-seeing eye.
Your baby’s eye doctor will decide if your baby needs a follow-up exam based on what he/she see during the first exam. If your baby needs follow-up care, your baby’s doctor will check his/her eyes again every 1 to 3 weeks until they aren’t worried about the risk for retinal detachment.
It’s important to get your baby’s follow-up exams on schedule. That way, your baby’s eye doctor (pediatric ophthalmologist) can catch retinopathy of prematurity in an early stage and start your baby’s treatment.
The International Committee for Classification of Retinopathy of Prematurity developed a diagnostic classification of retinopathy of prematurity in 1984 45. It has since has been further refined, most recently in 2021 with the International Classification of Retinopathy of Prematurity, 3rd edition 46, 47, 48. These diagnostic classifications define retinopathy of prematurity by location (zone), severity (stage) and vascular characteristics in the posterior pole (normal, pre-plus, or plus disease) 48.
Location (Zone)
To define the location, 3 concentric zones were established based on the most posterior zone, as the retina may be vascularized to different extents in different regions of the retina (i.e., nasal vs temporal vs superior vs inferior). Since retinal vascular development proceeds from the optic nerve to the ora serrata, the zones are centered on the optic disc rather than the macula.
- Zone 1: The area defined by a circle centered on the optic nerve, the radius of which extends from the center of the optic disc to twice the distance from the center of the optic disc to the center of the macula.
- Zone 2: The area extending centrifugally from the edge of zone 1 to a circle with a radius equal to the distance from the center of the optic disc to the nasal ora serrata.
- Posterior Zone 2: A region of 2 disc diameters peripheral to the zone 1 border. This was an addition in International Classification of Retinopathy of Prematurity 3 to allow for nuance in characterizing more posterior disease, which is often more aggressive.
- Zone 3: The residual temporal crescent of retina anterior to zone 2. By convention, zones 2 and 3 are considered to be mutually exclusive.
International Classification of Retinopathy of Prematurity 3 also added the notion of a “notch” in describing the location of retinopathy of prematurity, which is an incursion by the retinopathy of prematurity lesion of 1 to 2 clock hours from one zone into another” 46. If present, it should be documented by the most posterior zone with the qualifier “secondary to notch”. For example, if most of the vascularization is in zone 2 with a notch that extends into zone 1, the location would be “zone 1 secondary to notch” 46.
Disease Severity (Stage)
Prior to the development of retinopathy of prematurity in the premature infant, vascularization of the retina is “incomplete”.
More than one stage may be present in the same eye. However, staging for the eye as a whole is determined by the most severe stage present.
- Stage 1 Demarcation Line: This line is thin and flat (in the retina plane) and separates the avascular retina anteriorly from the vascularized retina posteriorly.
- Stage 2 Ridge: The ridge arises from the demarcation line and has height and width, which extends above the plane of the retina. The ridge may change from white to pink and vessels may leave the plane of the retina posterior to the ridge to enter it. Small, isolated tufts of neovascular tissue lying on the surface of the retina, commonly called “popcorn,” may be seen posterior to this ridge structure but do not constitute the degree of fibrovascular growth that is a necessary condition for stage 3.
- Stage 3 Extraretinal Fibrovascular Proliferation: Intravitreal neovascularization, or that which extends from the ridge into the vitreous. This extraretinal proliferating tissue is continuous with the posterior aspect of the ridge, causing a ragged appearance as the proliferation becomes more extensive. Seemingly flat-appearing extraretinal neovascularization can occur in eyes with zone 1 or posterior zone 2 disease, in the absence of an obvious ridge or demarcation line.
- Stage 4 Partial Retinal Detachment: In the initial International Classification of Retinopathy of Prematurity classification, this was the final stage and was known as the cicatricial phase.[28] It was later divided into stage 4A (extrafoveal partial retinal detachments) and stage 4B (foveal partial retinal detachments). Stage 4 retinal detachments are generally concave and most are circumferentially oriented. Retinal detachments usually begin at the point of fibrovascular attachment to the vascularized retina, and the extent of detachment depends on the amount of neovascularization present 47. They can be exudative or tractional.
- Stage 5 Total Retinal Detachment: Retinal detachments are generally tractional and usually funnel-shaped. The configuration of the funnel itself is used for subdivision of this stage, depending on if the anterior and posterior portions are open or narrowed 47. International Classification of Retinopathy of Prematurity 3 recommends subcategorizing stage 5 into 3 configurations:
- Stage 5A, when the optic disc is visible by ophthalmoscopy;
- Stage 5B, when the optic disc is not visible secondary to retrolental fibrovascular tissue or closed-funnel detachment; and
- Stage 5C, which contain stage 5B findings accompanied by anterior segment abnormalities (e.g., anterior lens displacement, marked anterior chamber shallowing, iridocapsular adhesions, capsule-endothelial adhesions with central corneal opacification) 46 Ultrasonography (B-scan) can be useful for the classification of stage 5B and 5C retinopathy of prematurity, but it is not necessary.
Aggressive retinopathy of prematurity (A-ROP)
Aggressive retinopathy of prematurity (A-ROP) is a new category initially presented in International Classification of Retinopathy of Prematurity 3 46. Aggressive retinopathy of prematurity (A-ROP) includes aggressive posterior retinopathy of prematurity, which was first recognized in the international classification in 2005 to indicate a rapidly progressing, posterior form of retinopathy of prematurity that can bypass the typical progression of stages (“rush disease”) 42. Aggressive retinopathy of prematurity (A-ROP) includes peripheral features such as vascular loops and areas of avascular retina, sometimes without obvious demarcation lines or ridges. Fundus fluorescein angiography may delineate the vascular changes more clearly in this disease 49.
With International Classification of Retinopathy of Prematurity 3, the term aggressive retinopathy of prematurity (A-ROP) replaced aggressive-posterior retinopathy of prematurity “because of increasing recognition that aggressive disease may occur in larger preterm infants and beyond the posterior retina, particularly in regions of the world with limited resources” 46. The key diagnostic features of aggressive retinopathy of prematurity (A-ROP) are, according to International Classification of Retinopathy of Prematurity 3, “the tempo of disease and appearance of vascular abnormalities, but not location of disease” 46. Eyes with aggressive retinopathy of prematurity (A-ROP) often demonstrate a form of stage 3 disease that may appear as deceptively featureless networks of so-called flat neovascularization, though the extra retinal neovascularization of classic stage 3 retinopathy of prematurity also can be seen 46.
Extent
The extent of disease is recorded as hours of the clock or as 30° sectors. As the observer looks at each eye, the 3-o’clock position is to the right and nasal in the right eye and temporal in the left eye, and the 9-o’clock position is to the left and temporal in the right eye and nasal in the left eye 50. Extent is useful in stages 4 and 5 retinopathy of prematurity, but in general is no longer used in the diagnosis of treatment-warranted (type 1) retinopathy of prematurity.
Vascular Characteristics in the Posterior Pole/Zone 1 (normal, pre-plus or plus disease)
Plus Disease Spectrum
In International Classification of Retinopathy of Prematurity 3, the recommendation is to evaluate the vessels within zone 1 46. International Classification of Retinopathy of Prematurity 3 emphasizes that the terms below should be thought of as “a continuous spectrum of retinal vascular changes” 46. In this spectrum of abnormal dilatation and tortuosity, plus disease is the most severe form.
Pre-Plus Disease
Pre-plus disease has been described as vascular abnormalities of the posterior pole that are insufficient for the diagnosis of plus disease, but that demonstrate more arterial tortuosity and more venous dilatation than normal 42. In International Classification of Retinopathy of Prematurity 3, these vascular abnormalities can either demonstrate more arterial tortuosity or more venous dilatation than normal 46.
Plus Disease
In the original International Classification of Retinopathy of Prematurity classification, plus disease was characterized by additional signs of increased venous dilatation and arteriolar tortuosity of the posterior retinal vessels, which can increase in severity to include iris vascular engorgement, poor pupillary dilatation, and vitreous haze 50. Thus, all patients with suspected retinopathy of prematurity should be seen, including those with poor dilation of pupils after topical mydriatics, to rule out plus disease and more importantly aggressive retinopathy of prematurity (A-ROP) 46.
The new recognition of plus disease being on a spectrum reduces the rigidity of the use of standard photos, as advocated in previous clinical trials. The International Classification of Retinopathy of Prematurity 3 criteria requires at least 2 quadrants with vascular dilatation and tortuosity 51.
Later Phases of retinopathy of prematurity (regression and reactivation)
Regression
A term introduced in International Classification of Retinopathy of Prematurity 3, regression refers to disease involution and resolution. Regression may be complete or incomplete, and may include persistence of retinal abnormalities 46. Signs of vascular regression include decreased plus disease, increased vascularization into the peripheral avascular retina, involution of the tunica vasculosa lentos, better pupillary dilation, greater media clarity, and resolution of intraretinal hemorrhages. Regression is characterized by thinning and whitening of neovascular tissue.
Reactivation
International Classification of Retinopathy of Prematurity 3 also introduced the term reactivation, which refers to recurrence of acute-phase features but not necessarily recurrence of type 1 retinopathy of prematurity 46. Reactivation may occur after incomplete or complete regression of the original retinopathy of prematurity and is seen more frequently after anti-VEGF treatment than after spontaneous regression. Reactivated disease may not progress through the normal sequence of stages of acute-phase disease. Vascular reactivation includes the recurrence of pre-plus or plus disease. Extraretinal new vessels can occur and may be relatively delicate compared with those of acute retinopathy of prematurity. Hemorrhages can occur around fronds of extraretinal vessels. Alternatively, extraretinal vessels may appear as a fibrovascular ridge, which can progress to fibrosis, contraction, and tractional detachment. These forms of progressive stage 4 retinopathy of prematurity can involve fibrosis at the original ridge that regressed and also have some features similar to those seen after laser treatment 52, 53. Documentation of reactivation should specify the presence and location(s) of new retinopathy of prematurity features, noted by zone and stage using the modifier “reactivated”. If multiple ridges are present, “reactivated” is applied to the more anterior ridge, which is typically more active.
Persistent Avascular Retina
International Classification of Retinopathy of Prematurity 3 described persistent avascular retina (PAR) as cases of incomplete vascularization of the peripheral avascular retina. It is described by both its location (e.g., posterior zone 2) and extent (e.g., nasal) 46. It can occur spontaneously or after vascularization into the peripheral avascular retina, a feature more recognized now with the increased use of anti-VEGF therapy. Persistent avascular retina (PAR) may be a risk factor for delayed reactivation after anti-VEGF therapy, and cases of reactivation leading to retinal detachment have been reported in toddlers 54, 55. Retinal neovascularization and vitreous hemorrhage have even been reported 10 years after intravitreal bevacizumab treatment (without laser ablation therapy) 56. Laser ablation of persistent avascular retina (PAR) removes the opportunity for vascularization of the peripheral avascular retina and potential visual field expansion, although delaying laser until older postmenstrual age may minimize this effect.
Retinopathy of prematurity differential diagnosis
Retinopathy of prematurity differential diagnosis may include:
- Congenital Cataract: Congenital cataracts are clouding of the eye lens present at birth or developing in the first year of life, causing vision problems. They can affect one or both eyes and can lead to issues like “lazy eye” and eye misalignment if not treated early. Early intervention, including surgery and special eye care, is crucial to prevent vision loss and ensure proper visual development.
- Familial exudative vitreoretinopathy: Familial exudative vitreoretinopathy (FEVR) is a genetic disorder primarily affecting retinal blood vessel development mimicking late-stage retinopathy of prematurity (ROP), leading to vision loss and potentially blindness. Familial exudative vitreoretinopathy (FEVR) is characterized by incomplete vascularization in the peripheral retina, which can cause further complications like neovascularization, exudation, traction through the macula, and retinal detachment. Familial exudative vitreoretinopathy (FEVR) can be inherited in various patterns, including autosomal dominant, autosomal recessive, and X-linked recessive.
- Pediatric Rubella: Rubella also known as German measles, is a contagious viral illness and children who contract rubella from their mother while she is pregnant can have severe birth defects and other consequences called Congenital Rubella Syndrome.
- Retinoblastoma. Retinoblastoma (RB) is a rare genetically-driven eye cancer that develops in the retina, the light-sensing tissue at the back of the eye, and is the most common type of eye cancer in children. In some cases, a child inherits a faulty RB1 gene from a parent, increasing their risk of developing retinoblastoma. In other cases, the gene mutation occurs randomly, and the child does not inherit it from either parent. Retinoblastoma can occur in one or both eyes. Early diagnosis and treatment are essential to prevent vision loss and the spread of cancer.
- Norrie disease. Norrie disease is a rare, genetic eye disorder primarily affecting males, causing blindness or significant vision impairment from birth or soon after 57. Norrie disease is characterized by abnormal retinal development, often leading to retinal detachment and other eye issues such as cataracts, leukocoria, iris atrophy as well as other developmental issues in the eye 58. In addition to the congenital eye symptoms, many individuals with Norrie disease also experience hearing loss, developmental delays, intellectual disability, peripheral vascular disease and learning or behavioral problems.
- Persistent fetal vasculature: A cause of tractional retinal detachment which may be difficult to differentiate from ROP but is typically unilateral and is not correlated with prematurity
- Incontinentia pigmenti: Incontinentia pigmenti also known as Bloch-Sulzberger syndrome is a rare X-linked dominant genetic disorder that affects the skin, hair, teeth, nails, eyes, and central nervous system, often presenting with characteristic skin lesions and other systemic abnormalities. When noted, retinal abnormalities often include avascularity, neovascularization, and exudative and tractional retinal detachments.
- Coats disease: Coats disease is a rare, sporadic X-linked eye condition characterized by abnormal blood vessel development in the retina, potentially leading to vision loss or blindness, often unilateral and found in males 59
- Cutis marmorata telangiectatica congenita: Cutis marmorata telangiectatica congenita (CMTC) is a rare congenital vascular disorder characterized by a persistent, reticulated, marbled appearance of the skin that doesn’t fade with warming 60, 61, 62. It typically presents at birth with a network of small, dilated blood vessels (telangiectasias) and may be associated with skin atrophy and ulceration. While often benign, cutis marmorata telangiectatica congenita (CMTC) can also be associated with other congenital anomalies, such as limb asymmetry, vascular abnormalities, and neurological or ocular defects that include peripheral retinal neovascularization and glaucoma.
- Infectious causes that may mimic retinopathy of prematurity include Toxoplasma, Toxocara, and Herpes virus, especially cytomegalovirus.
Retinopathy of prematurity treatment
Many babies with retinopathy of prematurity have mild cases and get better without treatment. But some babies need treatment to keep retinopathy of prematurity from getting worse. It’s important to get retinopathy of prematurity treated early to protect your child’s vision. Treatment options include:
- Laser treatment. Babies with advanced retinopathy of prematurity may need laser treatment on the sides of the retina. This treatment can help keep retinopathy of prematurity from getting worse and help protect your child’s vision.
- Injections. Doctors can also inject medicines called anti-VEGF drugs into your baby’s eye. These medicines work by blocking the growth of blood vessels.
- Eye surgery. There are 2 types of retina surgery for babies with partially or completely detached retinas (stages 4 or 5):
- Scleral buckle surgery. The eye surgeon places a flexible band around the sclera (the white part of the eye). The band supports the detached retina until the eye starts growing normally, then the doctor removes it.
- Vitrectomy. The eye surgeon makes small openings in the eye wall to remove most of the vitreous (the gel-like fluid that fills the eye) and replace it with saline solution. The eye surgeon then removes the scar tissue on the retina. They may also do laser treatment to treat the retina and seal it in position.
The goal of retinopathy of prematurity surgery is to keep retinopathy of prematurity from getting worse and prevent blindness. Even with surgery, some babies with retinopathy of prematurity will still have vision loss or blindness.
Laser Photocoagulation
Laser photocoagulation treatment is currently recommended for the following (defined as “type 1” retinopathy of prematurity):
- Zone 1: any-stage retinopathy of prematurity with plus disease or stage 3 retinopathy of prematurity without plus disease
- Zone 1: stage 3 retinopathy of prematurity without plus disease
- Zone 2: stage 2 or 3 retinopathy of prematurity with plus disease
Eyes meeting these criteria should be treated as soon as possible, ideally within 72 hours. However, increasingly eyes with zone 1, type 1 retinopathy of prematurity are being treated with anti-VEGF agents. The number of clock hours of disease is no longer a determining factor for treatment.
Anti-VEGF Agents
Anti-VEGF treatment has shown promise for the treatment of stage 3 retinopathy of prematurity with plus disease in zone 1 (not zone 2) 63. Recent clinical trials have been performed to test de-escalating doses of bevacizumab 64 or ranibizumab 65 for type 1 retinopathy of prematurity. Treatment efficacy was seen with lower bevacizumab doses and with ranibizumab 0.2 mg 64, 65. Treatment with aflibercept in the FIREFLEYE study has also been found to be beneficial 66, but was found to be noninferior to laser in clinical trials 67.
Patient Monitoring Following Treatment
Follow-up is recommended in 3–7 days following either laser photocoagulation or anti-VEGF injections to monitor for reductions in retinal dilation, tortuosity, and/or stage 3 retinopathy of prematurity 38. Reduction in features can be seen within a week. Following anti-VEGF injections, close monitoring is needed in case endophthalmitis and other complications, including damage to the retina or lens, occur. Eyes must be watched carefully for retinopathy of prematurity regression and reactivation. Very late recurrences of proliferative retinopathy of prematurity have been reported following anti-VEGF therapy.
Despite treatment, some eyes will progress. In the CRYO-retinopathy of prematurity study 51, approximately 30% of eyes progressed to posterior pole macular fold or retinal detachment. In these situations, vitreoretinal surgery may be needed. At the reported 15-year outcome from the CRYO-retinopathy of prematurity study, new retinal folds, detachments, or obscuring the posterior pole occurred in 4.5% of eyes given treatment and 7.7% of eyes in the control group; thus, it was recommended that eyes that experience threshold retinopathy of prematurity have long-term, regular follow-up 68.
Additional monitoring is necessary for the fibrovascular progression of retinopathy of prematurity sometimes seen after anti-VEGF injections or laser treatments 69. Progressive stage 4 retinopathy of prematurity after laser is predicted by clock-hour extent of changes at the ridge, vitreous condensation, and persistent or new plus disease. Similar findings may be present after anti-VEGF treatment, but these changes can occur at the original ridge and around the optic nerve 52, 46. Stage 4 and 5 retinopathy of prematurity may require vitreous surgery by a pediatric retina-trained surgeon. Surgery is performed with the intent of preserving the natural lens whenever possible and to address the vitreoretinal adhesions that create the complex tractional detachments 70, 71. All attempts are made to avoid creating breaks during vitrectomy. Small studies have compared scleral buckling and vitrectomy for stage 4 retinopathy of prematurity, and lens-sparing vitrectomy was found to have better outcomes 72. However, there are times when scleral buckling can be considered, especially in cases of rhegmatogenous retinal detachment 69.
Retinopathy of prematurity prognosis
The prognosis (outlook) of retinopathy of prematurity (ROP) is predicted by the disease stage. Babies who did not progress beyond stage 1 or stage 2 have a good prognosis, as do most successfully treated babies with zone 2/3 disease. Babies with posterior zone 1 disease or stage 4 have a guarded prognosis for their vision. Infants with stage 5 disease mostly have extremely poor vision. If retinopathy of prematurity progresses to untreatable retinal detachment, the outcome is poor and vision-threatening.
Long-term outcomes for serious disease, especially those babies who received treatment for retinopathy of prematurity, include severe visual impairment and blindness. Infants with advanced retinopathy of prematurity may develop vision-threatening conditions such as myopia (nearsightedness), amblyopia (“lazy eye” – reduced vision in one eye caused by abnormal visual development early in life), and strabismus (crossed eyes), and these infants require close follow-up after discharge from the neonatal intensive care unit (NICU) 73. The CRYO-retinopathy of prematurity study showed that at the 15-year follow-up, treatment reduces the risk of unfavorable outcome from 52% to 30% 68. The same study showed improved outcomes in the treated group for visual acuity at the 3-year, 10-year, and 15-year follow-ups 68. Better outcomes are being reported with anti-VEGF agents and additional studies are awaited.
- Albanese GM, Visioli G, Alisi L, Armentano M, Giovannetti F, Lucchino L, Marenco M, Pontecorvi P, Gharbiya M. Retinopathy of Prematurity and MicroRNAs. Biomedicines. 2025 Feb 7;13(2):400. doi: 10.3390/biomedicines13020400[↩]
- Selvam S., Kumar T., Fruttiger M. Retinal Vasculature Development in Health and Disease. Prog. Retin. Eye Res. 2018;63:1–19. doi: 10.1016/j.preteyeres.2017.11.001[↩]
- Chen J., Smith L.E.H. Retinopathy of Prematurity. Angiogenesis. 2007;10:133–140. doi: 10.1007/s10456-007-9066-0[↩]
- Nair A, El Ballushi R, Anklesaria BZ, Kamali M, Talat M, Watts T. A Review on the Incidence and Related Risk Factors of Retinopathy of Prematurity Across Various Countries. Cureus. 2022 Nov 29;14(11):e32007. doi: 10.7759/cureus.32007[↩]
- Retinopathy of prematurity. Bashinsky AL. N C Med J. 2017;78:124–128. doi: 10.18043/ncm.78.2.124[↩][↩]
- Broxterman EC, Hug DA. Retinopathy of Prematurity: A Review of Current Screening Guidelines and Treatment Options. Mo Med. 2016 May-Jun;113(3):187-90. https://pmc.ncbi.nlm.nih.gov/articles/PMC6140066[↩][↩][↩]
- Parappil H, Pai A, Mahmoud NA, AlKhateeb MA, Al Rifai H, El Shafei MM. Management of retinopathy of prematurity in a neonatal unit: Current approach. J Clin Neonatol 2019;8:203‑11. https://www.researchgate.net/publication/336261256_Management_of_retinopathy_of_prematurity_in_a_neonatal_unit_Current_approach[↩]
- Retinopathy of Prematurity. https://eyerounds.org/cases/286-retinopathy-of-prematurity.htm#gsc.tab=0 [↩][↩]
- Retinopathy of Prematurity. https://aapos.org/glossary/retinopathy-of-prematurity[↩][↩][↩][↩][↩]
- Zin A, Gole GA. Retinopathy of prematurity-incidence today. Clin Perinatol. 2013 Jun;40(2):185-200. doi: 10.1016/j.clp.2013.02.001[↩]
- Gilbert C. Retinopathy of prematurity: a global perspective of the epidemics, population of babies at risk and implications for control. Early Hum Dev. 2008 Feb;84(2):77-82. doi: 10.1016/j.earlhumdev.2007.11.009[↩]
- Kim TI, Sohn J, Pi SY, Yoon YH. Postnatal risk factors of retinopathy of prematurity. Paediatr Perinat Epidemiol. 2004 Mar;18(2):130-4. doi: 10.1111/j.1365-3016.2003.00545.x[↩]
- Shah VA, Yeo CL, Ling YL, Ho LY. Incidence, risk factors of retinopathy of prematurity among very low birth weight infants in Singapore. Ann Acad Med Singap. 2005 Mar;34(2):169-78. https://doi.org/10.47102/annals-acadmedsg.V34N2p169[↩][↩]
- Wright KW, Strube YN. Pediatric Ophthalmology and Strabismus. New York, NY: Oxford University Press; 2012. Retinopathy of Prematurity; pp. 957–992.[↩]
- Retinopathy of Prematurity Pathophysiology. https://emedicine.medscape.com/article/976220-overview#a5[↩][↩]
- Lundgren P, Stoltz Sjöström E, Domellöf M, Källen K, Holmström G, Hård AL, Smith LE, Löfqvist C, Hellström A. WINROP identifies severe retinopathy of prematurity at an early stage in a nation-based cohort of extremely preterm infants. PLoS One. 2013 Sep 12;8(9):e73256. doi: 10.1371/journal.pone.0073256[↩][↩]
- Anuk İnce D, Gülcan H, Hanta D, Ecevit A, Akkoyun I, Kurt A, Tarcan A. Poor postnatal weight gain predicts stage 3+ retinopathy of prematurity in very low birth weight infants. Turk J Pediatr. 2013 May-Jun;55(3):304-8.[↩][↩]
- Bizzarro MJ, Hussain N, Jonsson B, Feng R, Ment LR, Gruen JR, Zhang H, Bhandari V. Genetic susceptibility to retinopathy of prematurity. Pediatrics. 2006 Nov;118(5):1858-63. doi: 10.1542/peds.2006-1088[↩]
- Dhaliwal CA, Fleck BW, Wright E, Graham C, McIntosh N. Retinopathy of prematurity in small-for-gestational age infants compared with those of appropriate size for gestational age. Arch Dis Child Fetal Neonatal Ed. 2009 May;94(3):F193-5. doi: 10.1136/adc.2008.143552[↩][↩]
- Chang JW. Risk factor analysis for the development and progression of retinopathy of prematurity. PLoS One. 2019 Jul 18;14(7):e0219934. doi: 10.1371/journal.pone.0219934[↩][↩]
- Charles JB, Ganthier R Jr, Appiah AP. Incidence and characteristics of retinopathy of prematurity in a low-income inner-city population. Ophthalmology. 1991 Jan;98(1):14-7. doi: 10.1016/s0161-6420(91)32350-9[↩][↩][↩][↩]
- Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Arch Ophthalmol. 1988 Apr;106(4):471-9. doi: 10.1001/archopht.1988.01060130517027[↩]
- Bujoreanu Bezman L, Tiutiuca C, Totolici G, Carneciu N, Bujoreanu FC, Ciortea DA, Niculet E, Fulga A, Alexandru AM, Stan DJ, Nechita A. Latest Trends in Retinopathy of Prematurity: Research on Risk Factors, Diagnostic Methods and Therapies. Int J Gen Med. 2023 Mar 14;16:937-949. doi: 10.2147/IJGM.S401122[↩][↩][↩]
- Chang E, Josan AS, Purohit R, Patel CK, Xue K. A Network Meta-Analysis of Retreatment Rates following Bevacizumab, Ranibizumab, Aflibercept, and Laser for Retinopathy of Prematurity. Ophthalmology. 2022 Dec;129(12):1389-1401. doi: 10.1016/j.ophtha.2022.06.042[↩]
- Almeida AC, Silva GA, Santini G, Brízido M, Correia M, Coelho C, Borrego LM. Correlation between hyperglycemia and glycated albumin with retinopathy of prematurity. Sci Rep. 2021 Nov 16;11(1):22321. doi: 10.1038/s41598-021-01861-8[↩]
- Lutty GA, McLeod DS. Development of the hyaloid, choroidal and retinal vasculatures in the fetal human eye. Prog Retin Eye Res. 2018 Jan;62:58-76. doi: 10.1016/j.preteyeres.2017.10.001[↩]
- York JR, Landers S, Kirby RS, Arbogast PG, Penn JS. Arterial oxygen fluctuation and retinopathy of prematurity in very-low-birth-weight infants. J Perinatol. 2004 Feb;24(2):82-7. doi: 10.1038/sj.jp.7211040[↩]
- Zeng G, Taylor SM, McColm JR, Kappas NC, Kearney JB, Williams LH, Hartnett ME, Bautch VL. Orientation of endothelial cell division is regulated by VEGF signaling during blood vessel formation. Blood. 2007 Feb 15;109(4):1345-52. doi: 10.1182/blood-2006-07-037952[↩]
- Geisen P, Peterson LJ, Martiniuk D, Uppal A, Saito Y, Hartnett ME. Neutralizing antibody to VEGF reduces intravitreous neovascularization and may not interfere with ongoing intraretinal vascularization in a rat model of retinopathy of prematurity. Mol Vis. 2008 Feb 11;14:345-57. https://pmc.ncbi.nlm.nih.gov/articles/PMC2258217[↩]
- Simmons AB, Bretz CA, Wang H, Kunz E, Hajj K, Kennedy C, Yang Z, Suwanmanee T, Kafri T, Hartnett ME. Gene therapy knockdown of VEGFR2 in retinal endothelial cells to treat retinopathy. Angiogenesis. 2018 Nov;21(4):751-764. doi: 10.1007/s10456-018-9618-5. Epub 2018 May 5. Erratum in: Angiogenesis. 2018 Nov;21(4):765. doi: 10.1007/s10456-018-9626-5[↩]
- Hartnett ME. Retinopathy of Prematurity: Evolving Treatment With Anti-Vascular Endothelial Growth Factor. Am J Ophthalmol. 2020 Oct;218:208-213. doi: 10.1016/j.ajo.2020.05.025. Epub 2020 May 23. Erratum in: Am J Ophthalmol. 2021 Nov;231:213. doi: 10.1016/j.ajo.2020.12.018[↩]
- McCloskey M, Wang H, Jiang Y, Smith GW, Strange J, Hartnett ME. Anti-VEGF antibody leads to later atypical intravitreous neovascularization and activation of angiogenic pathways in a rat model of retinopathy of prematurity. Invest Ophthalmol Vis Sci. 2013 Mar 21;54(3):2020-6. doi: 10.1167/iovs.13-11625[↩]
- Chiang MF, Quinn GE, Fielder AR, et al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology. 2021 Oct;128(10):e51-e68. doi: 10.1016/j.ophtha.2021.05.031[↩]
- Becker S, Wang H, Simmons AB, Suwanmanee T, Stoddard GJ, Kafri T, Hartnett ME. Targeted Knockdown of Overexpressed VEGFA or VEGF164 in Müller cells maintains retinal function by triggering different signaling mechanisms. Sci Rep. 2018 Jan 31;8(1):2003. doi: 10.1038/s41598-018-20278-4[↩][↩]
- Sauer L, Chandler M, Hartnett ME. Extending Peripheral Retinal Vascularization in Retinopathy of Prematurity Through Regulation of VEGF Signaling. Am J Ophthalmol. 2024 Apr;260:190-199. doi: 10.1016/j.ajo.2023.12.008[↩]
- Chow LC, Wright KW, Sola A; CSMC Oxygen Administration Study Group. Can changes in clinical practice decrease the incidence of severe retinopathy of prematurity in very low birth weight infants? Pediatrics. 2003 Feb;111(2):339-45. doi: 10.1542/peds.111.2.339[↩]
- Vedantham V. Retinopathy of prematurity screening in the Indian population: it’s time to set our own guidelines! Indian J Ophthalmol. 2007 Sep-Oct;55(5):329-30. doi: 10.4103/0301-4738.33816[↩]
- Fierson WM; AMERICAN ACADEMY OF PEDIATRICS Section on Ophthalmology; AMERICAN ACADEMY OF OPHTHALMOLOGY; AMERICAN ASSOCIATION FOR PEDIATRIC OPHTHALMOLOGY AND STRABISMUS; AMERICAN ASSOCIATION OF CERTIFIED ORTHOPTISTS. Screening Examination of Premature Infants for Retinopathy of Prematurity. Pediatrics. 2018 Dec;142(6):e20183061. doi: 10.1542/peds.2018-3061. Erratum in: Pediatrics. 2019 Mar;143(3):e20183810. doi: 10.1542/peds.2018-3810[↩][↩][↩][↩][↩][↩][↩][↩]
- Section on Ophthalmology American Academy of Pediatrics; American Academy of Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus. Screening examination of premature infants for retinopathy of prematurity. Pediatrics. 2006 Feb;117(2):572-6. doi: 10.1542/peds.2005-2749. Erratum in: Pediatrics. 2006 Sep;118(3):1324.[↩][↩]
- Subhani M, Combs A, Weber P, Gerontis C, DeCristofaro JD. Screening guidelines for retinopathy of prematurity: the need for revision in extremely low birth weight infants. Pediatrics. 2001 Apr;107(4):656-9. doi: 10.1542/peds.107.4.656[↩]
- Quinn GE, Ying GS, Repka MX, Siatkowski RM, Hoffman R, Mills MD, Morrison D, Daniel E, Baumritter A, Hildebrand PL, Schron EB, Ells AL, Wade K, Kemper AR. Timely implementation of a retinopathy of prematurity telemedicine system. J AAPOS. 2016 Oct;20(5):425-430.e1. doi: 10.1016/j.jaapos.2016.06.007[↩]
- Classification of Retinopathy of Prematurity*. The International Classification of Retinopathy of Prematurity Revisited. Arch Ophthalmol. 2005;123(7):991–999. doi:10.1001/archopht.123.7.991[↩][↩][↩][↩]
- VanderVeen DK, Coats DK, Dobson V, Fredrick D, Gordon RA, Hardy RJ, Neely DE, Palmer EA, Steidl SM, Tung B, Good WV; Early Treatment for Retinopathy of Prematurity Cooperative Group. Prevalence and course of strabismus in the first year of life for infants with prethreshold retinopathy of prematurity: findings from the Early Treatment for Retinopathy of Prematurity study. Arch Ophthalmol. 2006 Jun;124(6):766-73. doi: 10.1001/archopht.124.6.766[↩]
- Quiram PA, Capone Jr A. Adult ROP: late complications of retinopathy of prematurity. Retinal Physician. 2007 Jun 1.[↩]
- An international classification of retinopathy of prematurity. The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol. 1984 Aug;102(8):1130-4. doi: 10.1001/archopht.1984.01040030908011[↩]
- Chiang MF, Quinn GE, Fielder AR, Ostmo SR, et al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology. 2021 Oct;128(10):e51-e68. doi: 10.1016/j.ophtha.2021.05.031[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Aaberg T, Ben-Sira I, Charles S, et al. An International Classification of Retinopathy of Prematurity: II. The Classification of Retinal Detachment. Arch Ophthalmol. 1987;105(7):906–912. doi:10.1001/archopht.1987.01060070042025[↩][↩][↩]
- International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity revisited. Arch Ophthalmol. 2005 Jul;123(7):991-9. doi: 10.1001/archopht.123.7.991[↩][↩]
- Temkar S, Azad SV, Chawla R, Damodaran S, Garg G, Regani H, Nawazish S, Raj N, Venkatraman V. Ultra-widefield fundus fluorescein angiography in pediatric retinal vascular diseases. Indian J Ophthalmol. 2019 Jun;67(6):788-794. doi: 10.4103/ijo.IJO_1688_18[↩]
- An International Classification of Retinopathy of Prematurity. Arch Ophthalmol. 1984;102(8):1130–1134. doi:10.1001/archopht.1984.01040030908011[↩][↩]
- The Natural Ocular Outcome of Premature Birth and Retinopathy: Status at 1 Year. Arch Ophthalmol. 1994;112(7):903–912. doi:10.1001/archopht.1994.01090190051021[↩][↩]
- Hartnett ME, McColm JR. Retinal features predictive of progressive stage 4 retinopathy of prematurity. Retina. 2004 Apr;24(2):237-41. doi: 10.1097/00006982-200404000-00008[↩][↩]
- Yonekawa Y, Thomas BJ, Thanos A, Todorich B, Drenser KA, Trese MT, Capone A Jr. THE CUTTING EDGE OF RETINOPATHY OF PREMATURITY CARE: Expanding the Boundaries of Diagnosis and Treatment. Retina. 2017 Dec;37(12):2208-2225. doi: 10.1097/IAE.0000000000001719[↩]
- Ittiara S, Blair MP, Shapiro MJ, Lichtenstein SJ. Exudative retinopathy and detachment: a late reactivation of retinopathy of prematurity after intravitreal bevacizumab. J AAPOS. 2013 Jun;17(3):323-5. doi: 10.1016/j.jaapos.2013.01.004[↩]
- Snyder LL, Garcia-Gonzalez JM, Shapiro MJ, Blair MP. Very Late Reactivation of Retinopathy of Prematurity After Monotherapy With Intravitreal Bevacizumab. Ophthalmic Surg Lasers Imaging Retina. 2016 Mar;47(3):280-3. doi: 10.3928/23258160-20160229-12[↩]
- Taylor K, Ghergherehchi L, Rao P, Harper CA 3rd, Chang E. Very late-onset reactivation of retinopathy of prematurity post anti-VEGF bevacizumab treatment for type 1 ROP: a case report. J AAPOS. 2021 Jun;25(3):180-184. doi: 10.1016/j.jaapos.2021.02.004[↩]
- Parkes JD. Genetic factors in human sleep disorders with special reference to Norrie disease, Prader-Willi syndrome and Moebius syndrome. J Sleep Res. 1999 Jun;8 Suppl 1:14-22. doi: 10.1046/j.1365-2869.1999.00004.x[↩]
- Norrie Disease. https://eyewiki.org/Norrie_Disease[↩]
- Grosso A, Pellegrini M, Cereda MG, Panico C, Staurenghi G, Sigler EJ. Pearls and pitfalls in diagnosis and management of coats disease. Retina. 2015 Apr;35(4):614-23. doi: 10.1097/IAE.0000000000000485[↩]
- Bui TNPT, Corap A, Bygum A. Cutis marmorata telangiectatica congenita: a literature review. Orphanet J Rare Dis. 2019 Dec 4;14(1):283. doi: 10.1186/s13023-019-1229-8[↩]
- Sassalos TM, Fields TS, Levine R, Gao H. RETINAL NEOVASCULARIZATION FROM A PATIENT WITH CUTIS MARMORATA TELANGIECTATICA CONGENITA. Retin Cases Brief Rep. 2021 Jan 1;15(1):77-80. doi: 10.1097/ICB.0000000000000736[↩]
- Taleb EA, Nagpal MP, Mehrotra NS, Bhatt K. RETINAL FINDINGS IN A CASE OF PRESUMED CUTIS MARMORATA TELANGIECTATICA CONGENITA. Retin Cases Brief Rep. 2018 Fall;12(4):322-325. doi: 10.1097/ICB.0000000000000492[↩]
- Mintz-Hittner HA, Kennedy KA, Chuang AZ; BEAT-ROP Cooperative Group. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011 Feb 17;364(7):603-15. doi: 10.1056/NEJMoa1007374[↩]
- Wallace DK, Dean TW, Hartnett ME, Kong L, Smith LE, Hubbard GB, McGregor ML, Jordan CO, Mantagos IS, Bell EF, Kraker RT; Pediatric Eye Disease Investigator Group. A Dosing Study of Bevacizumab for Retinopathy of Prematurity: Late Recurrences and Additional Treatments. Ophthalmology. 2018 Dec;125(12):1961-1966. doi: 10.1016/j.ophtha.2018.05.001[↩][↩]
- Stahl A, Lepore D, Fielder A, Fleck B, Reynolds JD, Chiang MF, Li J, Liew M, Maier R, Zhu Q, Marlow N. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. 2019 Oct 26;394(10208):1551-1559. doi: 10.1016/S0140-6736(19)31344-3[↩][↩]
- Eftekhari Milani A, Bagheri M, Niyousha MR, Rezaei L, Hazeri S, Safarpoor S, Abdollahi M. Comparison of Clinical Outcomes of Intravitreal Bevacizumab and Aflibercept in Type 1 Prethreshold Retinopathy of Prematurity in Posterior Zone II. J Curr Ophthalmol. 2022 Apr 16;34(1):87-92. doi: 10.4103/joco.joco_193_21[↩]
- Stahl A, Sukgen EA, Wu WC, Lepore D, Nakanishi H, Mazela J, Moshfeghi DM, Vitti R, Athanikar A, Chu K, Iveli P, Zhao F, Schmelter T, Leal S, Köfüncü E, Azuma N; FIREFLEYE Study Group. Effect of Intravitreal Aflibercept vs Laser Photocoagulation on Treatment Success of Retinopathy of Prematurity: The FIREFLEYE Randomized Clinical Trial. JAMA. 2022 Jul 26;328(4):348-359. doi: 10.1001/jama.2022.10564[↩]
- Cryotherapy for Retinopathy of Prematurity Cooperative Group. 15-Year Outcomes Following Threshold Retinopathy of Prematurity: Final Results From the Multicenter Trial of Cryotherapy for Retinopathy of Prematurity. Arch Ophthalmol. 2005;123(3):311–318. doi:10.1001/archopht.123.3.311[↩][↩][↩]
- Hansen ED, Hartnett ME. A review of treatment for retinopathy of prematurity. Expert Rev Ophthalmol. 2019;14(2):73-87. doi: 10.1080/17469899.2019.1596026[↩][↩]
- Capone A Jr, Trese MT. Evolution of stage 4 retinopathy of prematurity. In: Hartnett ME, Drack A, Capone A Jr, et al, eds. Pediatric Retina. 3rd ed. Wolters Kluwer; 2021:832-837.[↩]
- Capone A Jr, Trese MT, Hartnett ME. Treatment of stages 4 and 5 retinopathy of prematurity. In: Hartnett ME, Drack A, Capone A Jr, et al, eds. Pediatric Retina. 3rd ed. Wolters Kluwer; 2021:838-846.[↩]
- Hartnett ME, Maguluri S, Thompson HW, McColm JR. Comparison of retinal outcomes after scleral buckle or lens-sparing vitrectomy for stage 4 retinopathy of prematurity. Retina. 2004 Oct;24(5):753-7. doi: 10.1097/00006982-200410000-00011[↩]
- Repka MX, Summers CG, Palmer EA, Dobson V, Tung B, Davis B. The incidence of ophthalmologic interventions in children with birth weights less than 1251 grams. Results through 5 1/2 years. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Ophthalmology. 1998 Sep;105(9):1621-7. doi: 10.1016/s0161-6420(98)99028-5[↩]





{kind=link}