Contents
- Types of skin cancer
- Basal and Squamous Cell Skin Cancer
- Basal cell carcinoma
- Squamous cell carcinoma
- Risk Factors for Basal and Squamous Cell Skin Cancer
- Ultraviolet (UV) light exposure
- Having light-colored skin
- Being older
- Being male
- Radiation exposure
- Previous skin cancer
- Long-term or severe skin inflammation or injury
- Psoriasis treatment
- Xeroderma pigmentosum (XP)
- Basal cell nevus syndrome (also known as nevoid basal cell carcinoma syndrome or Gorlin syndrome)
- Weakened immune system
- Human papilloma virus (HPV) infection
- Smoking
- What Causes Basal and Squamous Cell Skin Cancers ?
- Basal and Squamous Cell Skin Cancers Prevention
- Signs and Symptoms of Basal and Squamous Cell Skin Cancers
- Tests for Basal and Squamous Cell Skin Cancers
- Basal and Squamous Cell Skin Cancer Stages
- Treating Basal and Squamous Cell Skin Cancer
- Melanoma Skin Cancer
- Risk Factors for Melanoma Skin Cancer
- What Causes Melanoma Skin Cancer ?
- Prevention of Melanoma Skin Cancer
- Sunscreen
- Can Melanoma Skin Cancer Be Found Early ?
- Signs and Symptoms of Melanoma Skin Cancer
- ABCDE Criteria of Melanoma
- Tests for Melanoma Skin Cancer
- Melanoma Skin Cancer Stages
- Survival Rates for Melanoma Skin Cancer, by Stage
- How is Melanoma Skin Cancer Treated
- Can you lower your risk of the melanoma progressing or coming back ?
- Less common types of skin cancer
- Pre-cancerous and pre-invasive skin conditions
- Benign skin tumors
- Basal and Squamous Cell Skin Cancer
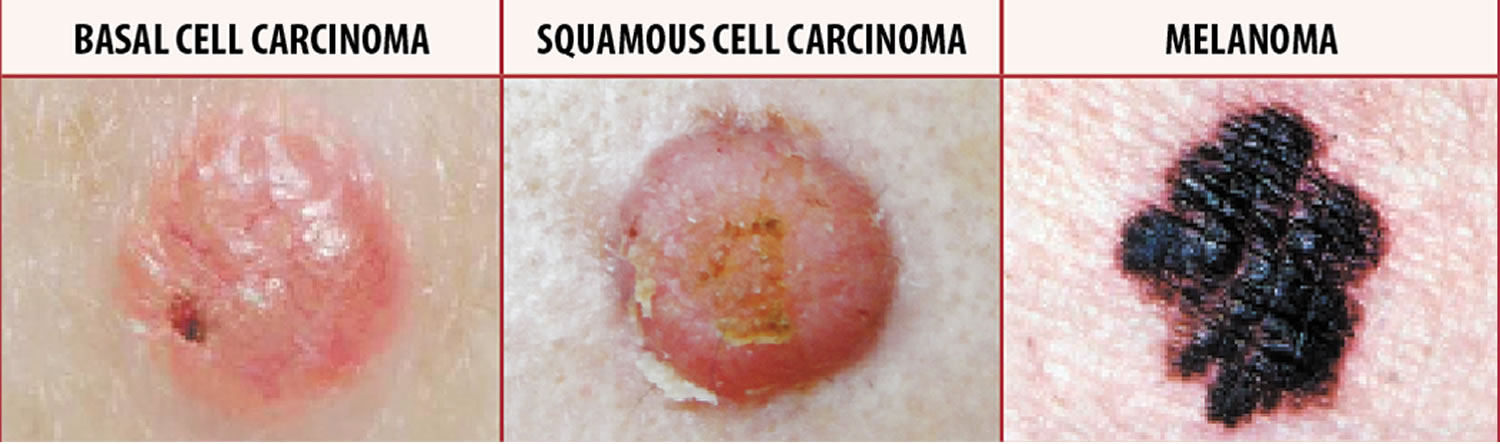
Types of skin cancer
Skin cancer is is by far the most common type of cancer in the United States 1. The two most common types are basal cell cancer and squamous cell cancer. They usually form on the head, face, neck, hands, and arms. Another type of skin cancer, melanoma, is more dangerous but less common. However, if you suspect you may have skin cancer, it is important to know which type you have because it affects your treatment options and your outlook (prognosis). If you aren’t sure which type of skin cancer you have, see your doctor so you can get the right information.
- If you find a new, unusual, or changing mole, you should have it checked by a doctor experienced in recognizing skin cancers.
- Any spots on the skin that are new or changing in size, shape, or color should be seen by a doctor promptly. Be sure to show your doctor any areas that concern you, and ask your doctor to look at areas that may be hard for you to see.
Anyone can get skin cancer, but it is more common in people who:
- Spend a lot of time in the sun or have been sunburned
- Have light-colored skin, hair and eyes
- Have a family member with skin cancer
- Are over age 50
You should have your doctor check any suspicious skin markings and any changes in the way your skin looks. Treatment is more likely to work well when cancer is found early. If not treated, some types of skin cancer cells can spread to other tissues and organs. Treatments include surgery, radiation therapy, chemotherapy, photodynamic therapy and biologic therapy. Photodynamic therapy uses a drug and a type of laser light to kill cancer cells. Biologic therapy boosts your body’s own ability to fight cancer.
While it may seem more convenient to shave off or cut out a mole yourself, there are 3 very good reasons a dermatologist should remove it:
- Skin cancer: If the mole contains skin cancer, some of the cancer cells can stay in the skin and even spread.
- Scarring: You can disfigure your skin causing a scar.
- Infection: A dermatologist uses sterile equipment to prevent infection.
Types of skin cells
There are 3 main types of cells in the top layer of the skin (called the epidermis):
- Squamous cells: These are flat cells in the outer part of the epidermis that are constantly shed as new ones form.
- Basal cells: These cells are in the lower part of the epidermis, called the basal cell layer. These cells constantly divide to form new cells to replace the squamous cells that wear off the skin’s surface. As these cells move up in the epidermis, they get flatter, eventually becoming squamous cells.
- Melanocytes: These cells make the brown pigment called melanin, which gives the skin its tan or brown color. Melanin acts as the body’s natural sunscreen, protecting the deeper layers of the skin from some of the harmful effects of the sun. For most people, when skin is exposed to the sun, melanocytes make more of the pigment, causing the skin to tan or darken. These are the cells that can become melanoma. They make a brown pigment called melanin, which gives the skin its tan or brown color. Melanin protects the deeper layers of the skin from some of the harmful effects of the sun. For most people, when skin is exposed to the sun, melanocytes make more of the pigment, causing the skin to tan or darken.
The epidermis is separated from the deeper layers of skin by the basement membrane. Skin cancer begins when cells in the skin start to grow uncontrollably. When a skin cancer becomes more advanced, it generally grows through this barrier and into the deeper layers.
See a doctor immediately if you notice a change in a mole!
It’s important to get a new or existing mole checked out if it:
- changes shape or looks uneven
- changes color, gets darker or has more than 2 colors
- starts itching, crusting, flaking or bleeding
- gets larger or more raised from the skin
These changes can happen over weeks or months. They’re sometimes a sign of malignant melanoma, a type of potentially deadly form of skin cancer that is diagnosed in about 70,000 Americans each year.
Melanoma is a form of cancer that begins in melanocytes (cells that make the pigment melanin). It may begin in a mole (skin melanoma), but infrequently can also begin in other pigmented tissues, such as in the eye or the intestines. Melanoma is potentially dangerous because it can spread to nearby tissues and other parts of the body, such as the lung, liver, bone, or brain. The earlier that melanoma is detected and removed, the more likely that treatment will be successful.
Unusual moles that may indicate melanoma
This ABCDE guide can help you determine if a mole or a spot may indicate melanoma or other skin cancers:
- A is for asymmetrical shape. One half is unlike the other half.
- B is for border. Look for moles with irregular, notched or scalloped borders.
- C is for color. Look for growths that have changed color, have many colors or have uneven color.
- D is for diameter. Look for new growth in a mole larger than 1/4 inch (about 6 millimeters).
- E is for evolving. Watch for moles that change in size, shape, color or height, especially if part or all of a mole turns black. Moles may also evolve to develop new signs and symptoms, such as itchiness or bleeding.
Cancerous (malignant) moles vary greatly in appearance. Some may show all of the features listed above. Others may have only one or two.
Figure 1. Skin structure

Basal and Squamous Cell Skin Cancer
These cancers are most often found in areas exposed to the sun, such as the head, neck, and arms, but they also can occur elsewhere. They are by far the most common skin cancers, but are also usually very treatable 2.
Cancers of the skin (most of which are basal and squamous cell skin cancers) are by far the most common of all types of cancer. According to one estimate, about 5.4 million basal and squamous cell skin cancers are diagnosed each year (occurring in about 3.3 million Americans, as some people have more than one). About 8 out of 10 of these are basal cell cancers. Squamous cell cancers occur less often.
Death from these cancers is uncommon. It’s thought that about 2,000 people in the US die each year from these cancers, and that this rate has been dropping in recent years. Most people who die from these cancers are elderly and may not have seen a doctor until the cancer had already grown quite large. Other people more likely to die of these cancers are those whose immune system is suppressed, such as those who have had organ transplants.
The exact number of people who develop or die from basal and squamous cell skin cancers each year is not known for sure. Statistics of most other cancers are known because they are reported to and tracked by cancer registries, but basal and squamous cell skin cancers are not.
Basal cell carcinoma
This the most common type of skin cancer. About 8 out of 10 skin cancers are basal cell carcinomas (also called basal cell cancers). When seen under a microscope, the cells in these cancers look like cells in the lowest layer of the epidermis, called the basal cell layer.
These cancers usually develop on sun-exposed areas, especially the head and neck. These cancers tend to grow slowly. It’s very rare for a basal cell cancer to spread to other parts of the body. But if a basal cell cancer is left untreated, it can grow into nearby areas and invade the bone or other tissues beneath the skin.
If not removed completely, basal cell carcinoma can recur (come back) in the same place on the skin. People who have had basal cell skin cancers are also more likely to get new ones in other places.
Figure 2. Basal Cell Carcinoma

Note: Basal cell carcinomas can appear as raised areas (like this one), and can be pale, pink, or red. They may have one or more abnormal blood vessels.
Figure 3. Basal cell carcinoma

Note: Basal cell carcinomas can appear as flat, pale or pink areas, like this one. Larger basal cell carcinomas may have oozing or crusted areas.
Squamous cell carcinoma
About 2 out of 10 skin cancers are squamous cell carcinomas (also called squamous cell cancers). The cells in these cancers look like abnormal versions of the squamous cells seen in the outer layers of the skin.
These cancers commonly appear on sun-exposed areas of the body such as the face, ears, neck, lips, and backs of the hands. They can also develop in scars or chronic skin sores elsewhere. They sometimes start in actinic keratoses (described below). Less often, they form in the skin of the genital area.
Squamous cell cancers are more likely to grow into deeper layers of skin and spread to other parts of the body than basal cell cancers, although this is still uncommon.
Keratoacanthomas are dome-shaped tumors that are found on sun-exposed skin. They may start out growing quickly, but their growth usually slows down. Many keratoacanthomas shrink or even go away on their own over time without any treatment. But some continue to grow, and a few may even spread to other parts of the body. Their growth is often hard to predict, so many skin cancer experts consider them a type of squamous cell skin cancer and treat them as such.
Figure 4. Squamous cell carcinoma

Note: Squamous cell skin cancers tend to grow slowly and can almost always be cured if found early. But if not treated, these cancers can grow into nearby areas or even spread to other parts of the body, where they can be much harder to treat.
Figure 5. Squamous cell carcinoma

Note: Squamous cell carcinomas can also develop in scars or skin sores on any part of the body. Squamous cell cancers are more likely to grow into deeper layers of skin and spread to other parts of the body than basal cell cancers, although this is still uncommon.
Risk Factors for Basal and Squamous Cell Skin Cancer
A risk factor is anything that affects your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking and excess sun exposure, can be changed. Others, like your age or family history, can’t be changed.
Having a risk factor, or even many risk factors, does not mean that you will get skin cancer. Many people with risk factors for skin cancer, never get it. Others with this disease may have few or no known risk factors.
Still, it’s important to know about the risk factors for skin cancer because there may be things you can do that could lower your risk of getting it. If you are at higher risk because of certain factors, there are also things you can do that might help find it early, when it’s likely to be easier to treat.
Several risk factors make a person more likely to get basal cell or squamous cell skin cancer. (These factors don’t necessarily apply to some other forms of skin cancer, such as Kaposi sarcoma and skin lymphoma.)
Ultraviolet (UV) light exposure
Exposure to ultraviolet (UV) rays is thought to be the major risk factor for most skin cancers. Sunlight is the main source of UV rays. Tanning beds are another source of UV rays.
Ultraviolet light (lightwaves 200-400nm) from the sun can cause sunburn if your skin is exposed for too long. It is always best to try to avoid excessive sun exposure between the peak hours of 10 a.m. to 4 p.m. – this is when UV rays are the strongest.
While UV rays make up only a very small portion of the sun’s rays, they are the main cause of the damaging effects of the sun on the skin. UV rays damage the DNA of skin cells. Skin cancers begin when this damage affects the DNA of genes that control skin cell growth.
Having light-colored skin
Whites have a much higher risk of skin cancer than African Americans or Hispanics. This is because the skin pigment melanin has a protective effect in people with darker skin. Whites with fair (light-colored) skin that freckles or burns easily are at especially high risk.
Albinism is an inherited lack of protective skin pigment. People with this condition may have pink-white skin and white hair. They have a high risk of getting sunburns and skin cancer, so they need to be careful to protect their skin.
Being older
The risk of getting basal and squamous cell skin cancers rises as people get older. This is probably because of the buildup of sun exposure over time. These cancers are becoming more common in younger people as well, probably because they are spending more time in the sun with their skin exposed.
Being male
Men are more likely than women to have basal and squamous cell cancers of the skin. This is thought to be due mainly to getting more sun exposure.
Exposure to certain chemicals
Being exposed to large amounts of arsenic increases the risk of developing skin cancer. Arsenic is an element found naturally in well water in some areas. It’s also used in making some pesticides and in some other industries.
Workers exposed to coal tar, paraffin, and certain types of oil may also have an increased risk of skin cancer.
Radiation exposure
People who have had radiation treatment have a higher risk of developing skin cancer in the area that received the treatment. This is particularly a concern in children who have had radiation treatment for cancer.
Previous skin cancer
People who have had a basal or squamous cell cancer have a much higher chance of developing another one.
Long-term or severe skin inflammation or injury
Scars from severe burns, areas of skin over serious bone infections, and skin damaged by some severe inflammatory skin diseases are more likely to develop skin cancers, although this risk is generally small.
Psoriasis treatment
Psoralens and ultraviolet light (PUVA) treatments given to some patients with psoriasis (a long-lasting inflammatory skin disease) can increase the risk of developing squamous cell skin cancer and probably other skin cancers.
Xeroderma pigmentosum (XP)
This very rare inherited condition reduces the ability of skin cells to repair DNA damage caused by sun exposure. People with this disorder often develop many skin cancers, starting in childhood.
Basal cell nevus syndrome (also known as nevoid basal cell carcinoma syndrome or Gorlin syndrome)
In this rare congenital (present at birth) condition, people develop many basal cell cancers over their lifetime. People with this syndrome may also have abnormalities of the jaw (and other bones), eyes, and nervous tissue.
Most of the time this condition is inherited from a parent. In families with this syndrome, those affected often start to develop basal cell cancers as children or teens. Exposure to UV rays can increase the number of tumors these people get.
Weakened immune system
The immune system helps the body fight cancers of the skin and other organs. People with weakened immune systems (from certain diseases or medical treatments) are more likely to develop many types of skin cancer, including squamous cell cancer, melanoma, and less common types such as Kaposi sarcoma and Merkel cell carcinoma.
For example, people who get organ transplants are usually given medicines that weaken their immune system to help prevent their body from rejecting the new organ. This increases their risk of developing skin cancer. Skin cancers in people with weakened immune systems tend to grow faster and are more likely to be fatal.
Treatment with large doses of corticosteroid drugs can also weaken the immune system. This may also increase a person’s risk of skin cancer.
People infected with HIV, the virus that causes AIDS, often have weakened immune systems and also are at increased risk for basal and squamous cell cancers.
Human papilloma virus (HPV) infection
Human papilloma viruses (HPVs) are a group of more than 150 viruses, many of which can cause papillomas, or warts. The warts that people commonly get on their hands and feet are not related to any form of cancer. But some HPV types, especially those that affect the genital and anal areas and the skin around the fingernails, seem to be related to skin cancers in these areas.
Smoking
People who smoke are more likely to develop squamous cell skin cancer, especially on the lips. Smoking is not a known risk factor for basal cell cancer.
What Causes Basal and Squamous Cell Skin Cancers ?
While many risk factors for basal and squamous cell skin cancers have been found, it’s not always clear exactly how these factors might cause cancer.
Most basal cell and squamous cell skin cancers are caused by repeated and unprotected skin exposure to ultraviolet (UV) rays from sunlight, as well as from man-made sources such as tanning beds.
UV rays can damage the DNA inside skin cells. DNA is the chemical in each of our cells that makes up our genes, which control how our cells function. We usually look like our parents because they are the source of our DNA. But DNA affects more than just how we look.
Some genes help control when our cells grow, divide into new cells, and die:
- Genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that keep cell growth in check by slowing down cell division or causing cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes. Changes in several different genes are usually needed for a cell to become cancer.
Researchers don’t yet know all of the DNA changes that result in skin cancer, but they have found that in many skin cancers the cells have changes in tumor suppressor genes.
The gene most often altered in squamous cell cancers is called TP53. This tumor suppressor gene normally causes cells with damaged DNA to die. When TP53 is altered, these abnormal cells may live longer and perhaps go on to become cancerous.
A gene often mutated in basal cell cancers is the PTCH1 gene, which is part of the “hedgehog” signaling pathway inside cells. PTCH1 is a tumor suppressor gene that normally helps keep cell growth in check, so changes in this gene can allow cells to grow out of control. People who have basal cell nevus syndrome (Gorlin syndrome), which is often inherited from a parent and results in getting many basal cell cancers, have an altered PTCH1 gene in all the cells of their body.
These are not the only gene changes that play a role in the development of skin cancer. There are likely to be many others as well.
People with xeroderma pigmentosum have a high risk for skin cancer. Xeroderma pigmentosum is a rare, inherited condition resulting from a defect in an enzyme that repairs DNA damage. Because people with xeroderma pigmentosum are less able to repair DNA damage caused by sunlight, they often develop many cancers on sun-exposed areas of their skin.
The link between squamous cell skin cancer and infection with some types of the human papilloma virus (HPV) also involves DNA and genes. These viruses have genes that affect growth-regulating proteins of infected skin cells. This can cause skin cells to grow too much and to not die when they’re supposed to.
Scientists are studying other links between DNA changes and skin cancer. A better understanding of how damaged DNA leads to skin cancer might be used to design treatments to overcome or repair that damage.
Basal and Squamous Cell Skin Cancers Prevention
There is no sure way to prevent all basal and squamous cell skin cancers. Some risk factors such as your age, gender, race, and family history can’t be controlled. But there are things you can do that could lower your risk of getting these and other skin cancers.
Limit your exposure to ultraviolet (UV) rays
The most important way to lower your risk of basal and squamous cell skin cancers is to limit your exposure to UV rays. Practice sun safety when you are outdoors.
Look for shade
Simply staying in the shade is one of the best ways to limit your UV exposure.
“Slip! Slop! Slap! and Wrap”
This catchphrase can help you remember some of the key steps you can take to protect yourself from UV rays. If you are going to be in the sun:
- Slip on a shirt.
- Slop on sunscreen.
- Slap on a hat.
- Wrap on sunglasses to protect the eyes and sensitive skin around them.
Avoid tanning beds and sun lamps
Many people believe the UV rays of tanning beds are harmless. This is not true. Tanning lamps give off UV rays, which can cause long-term skin damage and can contribute to skin cancer. Most skin doctors and health organizations recommend not using tanning beds and sun lamps.
Protect children from the sun
Children need special attention, since they tend to spend more time outdoors and can burn more easily. Parents and other caregivers should protect children from excess sun exposure by using the steps above. Children need to be taught about the dangers of too much sun exposure as they become more independent.
Avoid harmful chemicals
Exposure to certain chemicals, such as arsenic, can increase a person’s risk of skin cancer. People can be exposed to arsenic from well water in some areas, pesticides and herbicides, some medicines and imported traditional herbal remedies, and in certain occupations (such as mining and smelting).
Check your skin regularly
Checking your skin regularly may help you spot any new growths or abnormal areas and show them to your doctor before they even have a chance to turn into skin cancer. To learn more, see Can Basal and Squamous Cell Skin Cancers be Found Early?
Don’t smoke
Smoking has been linked to an increased risk of squamous cell skin cancer, as well as to many other types of cancer.
Avoid weakening your immune system (when possible)
Having a weakened immune system increases your risk of getting skin cancer, and if you do get it, it might be harder to treat.
Infection with HIV, the virus that causes AIDS, can weaken the immune system. Avoiding known risk factors for HIV infection, such as intravenous (IV) drug use and having unprotected sex with many partners, can also lower your risk of getting skin cancer and many other types of cancer.
Some people need to take medicines to suppress their immune system. This includes people who have had organ transplants and some people with autoimmune diseases. People with cancer also sometimes need to take medicines such as chemotherapy that can lower their immune function. For these people, the benefit from taking these medicines will likely far outweigh the small increased risk of getting skin cancer.
Signs and Symptoms of Basal and Squamous Cell Skin Cancers
Skin cancers often do not cause bothersome symptoms until they have grown quite large. Then they may itch, bleed, or even hurt. But typically they can be seen or felt long before they reach this point.
Basal cell carcinomas
Basal cell cancers usually develop on areas exposed to the sun, especially the face, head, and neck, but they can occur anywhere on the body.
These cancers can appear as:
- Flat, firm, pale or yellow areas, similar to a scar
- Raised reddish patches that might be itchy
- Small, pink or red, translucent, shiny, pearly bumps, which might have blue, brown, or black areas
- Pink growths with raised edges and a lower area in their center, which might contain abnormal blood vessels spreading out like the spokes of a tire
- Open sores (which may have oozing or crusted areas) that don’t heal, or that heal and then come back
Basal cell cancers are often fragile and might bleed after shaving or after a minor injury. Sometimes people go to the doctor because they have a sore or a cut from shaving that just won’t heal, which turns out to be a basal cell cancer. A simple rule of thumb is that most shaving cuts heal within a week or so.
Squamous cell carcinomas
Squamous cell cancers tend to occur on sun-exposed areas of the body such as the face, ear, neck, lip, and back of the hands. Less often, they form in the skin of the genital area. They can also develop in scars or skin sores elsewhere.
These cancers can appear as:
- Rough or scaly red patches, which might crust or bleed
- Raised growths or lumps, sometimes with a lower area in the center
- Open sores (which may have oozing or crusted areas) that don’t heal, or that heal and then come back
- Wart-like growths
Both basal and squamous cell skin cancers can also develop as a flat area showing only slight changes from normal skin.
- These and other types of skin cancers can also look different from the descriptions above. This is why it’s important to have any new or changing skin growths, sores that don’t heal, or other areas that concern you checked by your doctor.
Tests for Basal and Squamous Cell Skin Cancers
Most skin cancers are brought to a doctor’s attention because of signs or symptoms a person is having.
If you have an abnormal area that might be skin cancer, your doctor will examine it and might do tests to find out if it is cancer or some other skin condition. If there is a chance the skin cancer has spread to other areas of the body, other tests might be done as well.
Medical history and physical exam
Usually the first step is for your doctor to ask about your symptoms, such as when the mark first appeared on the skin, if it has changed in size or appearance, and if it has been painful, itchy, or bleeding. You might also be asked about past exposures to causes of skin cancer (including sunburns and tanning practices) and if you or anyone in your family has had skin cancer.
During the physical exam, the doctor will note the size, shape, color, and texture of the area(s) in question, and whether it is bleeding, oozing, or crusting. The rest of your body may be checked for moles and other spots that could be related to skin cancer.
The doctor may also feel the nearby lymph nodes, which are bean-sized collections of immune system cells under the skin in certain areas. Some skin cancers can spread to lymph nodes. When this happens, the lymph nodes might be felt as lumps under the skin.
If you are being seen by your primary doctor and skin cancer is suspected, you may be referred to a dermatologist (a doctor who specializes in skin diseases), who will look at the area more closely.
Along with a standard physical exam, some dermatologists use a technique called dermatoscopy (also known as dermoscopy, epiluminescence microscopy [ELM] or surface microscopy) to see spots on the skin more clearly. The doctor uses a dermatoscope, which is a special magnifying lens and light source held near the skin. Sometimes a thin layer of alcohol or oil is used with this instrument. The doctor may take a digital photo of the spot.
When used by an experienced dermatologist, this test can improve the accuracy of finding skin cancers early. It can also often help reassure you if a spot on the skin is probably benign (non-cancerous) without the need for a biopsy.
Skin biopsy
If the doctor thinks that a suspicious area might be skin cancer, the area (or part of it) will be removed and sent to a lab to be looked at under a microscope. This is called a skin biopsy. If the biopsy removes the entire tumor, it’s often enough to cure basal and squamous cell skin cancers without further treatment.
There are different types of skin biopsies. The doctor will choose one based on the suspected type of skin cancer, where it is on your body, its size, and other factors. Any biopsy will probably leave at least a small scar. Different methods can result in different scars, so if this is a concern, ask your doctor about possible scarring before the biopsy is done.
Skin biopsies are done using a local anesthetic (numbing medicine), which is injected into the area with a very small needle. You will probably feel a small prick and a little stinging as the medicine is injected, but you should not feel any pain during the biopsy.
Shave (tangential) biopsy
For a shave biopsy, the doctor shaves off the top layers of the skin with a small surgical blade. Bleeding from the biopsy site is then stopped by applying an ointment or a chemical that stops bleeding, or by using a small electrical current to cauterize the wound.
Punch biopsy
For a punch biopsy, the doctor uses a tool that looks like a tiny round cookie cutter to remove a deeper sample of skin. The doctor rotates the punch biopsy tool on the skin until it cuts through all the layers of the skin. The sample is removed and the edges of the biopsy site are often stitched together.
Incisional and excisional biopsies
To examine a tumor that may have grown into deeper layers of the skin, the doctor may use an incisional or excisional biopsy.
- An incisional biopsy removes only a portion of the tumor.
- An excisional biopsy removes the entire tumor.
For these types of biopsies, a surgical knife is used to cut through the full thickness of skin. A wedge or sliver of skin is removed for examination, and the edges of the wound are usually stitched together.
Examining the biopsy samples
All skin biopsy samples are sent to a lab, where they are looked at with a microscope by a doctor called a pathologist. Often, the samples are sent to a dermatopathologist, a doctor who has special training in looking at skin samples.
Lymph node biopsy
It’s rare for basal or squamous cell cancer to spread beyond the skin, but if it does it usually goes first to nearby lymph nodes, which are bean-sized collections of immune cells. If your doctor feels lymph nodes under the skin near the tumor that are too large or too firm, a lymph node biopsy may be done to find out if cancer has spread to them.
Fine needle aspiration biopsy
For a fine needle aspiration (FNA) biopsy, the doctor uses a syringe with a thin, hollow needle to remove very small fragments of the lymph node. The needle is smaller than the needle used for a blood test. A local anesthetic is sometimes used to numb the area first. This test rarely causes much discomfort and does not leave a scar.
FNA biopsies are not as invasive as some other types of biopsies, but they may not always provide a large enough sample to find cancer cells.
Surgical (excisional) lymph node biopsy
If an FNA does not find cancer in a lymph node but the doctor still suspects the cancer has spread there, the lymph node may be removed by surgery and examined. If the lymph node is just under the skin, this can often be done in a doctor’s office or outpatient surgical center using local anesthesia. This will leave a small scar.
Basal and Squamous Cell Skin Cancer Stages
The stage of a cancer describes how widespread it is. For skin cancers, the stage is based on the cancer’s size and location, whether it has grown into nearby tissues or bones, whether it has spread to the lymph nodes or other parts of the body, and certain other factors.
Determining the stage of basal cell skin cancers is rarely needed, because these cancers are almost always cured before they spread to other parts of the body.
Squamous cell skin cancers are more likely to spread (although this risk is still small), so determining the stage can be more important, particularly in people who are at higher risk. This includes people with weakened immune systems, such as those who have had organ transplants and people infected with HIV, the virus that causes AIDS.
In rare cases, imaging tests such as x-rays, CT scans, or MRI scans may be used as well.
Understanding your skin cancer stage
A staging system is a standard way to sum up how far a cancer has spread. This helps members of the cancer care team determine a patient’s prognosis (outlook) as well as the best treatment options.
The system most often used to stage basal and squamous cell skin cancers is the American Joint Commission on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
- T stands for the main (primary) tumor (its size, location, and how far it has spread within the skin and to nearby tissues).
- N stands for spread to nearby lymph nodes (bean-sized collections of immune system cells, to which cancers often spread first).
- M is for metastasis (spread to other parts of the body).
T categories
TX: The main (primary) tumor cannot be assessed.
T0: No evidence of primary tumor.
Tis: Carcinoma in situ (the tumor is still just in the epidermis, the outermost skin layer).
T1: The tumor is 2 centimeters (cm) across (about 4/5 inch) or smaller and has no or only 1 high-risk feature (see below).
T2: The tumor is larger than 2 cm across, or is any size with 2 or more high-risk features.
T3: The tumor has grown into facial bones, such as the jaw bones or bones around the eye.
T4: The tumor has grown into other bones in the body or into the base of the skull.
High-risk features: These features are used to tell between some T1 and T2 tumors.
- The tumor is thicker than 2 millimeters (mm).
- The tumor has invaded down into the lower dermis or subcutis (Clark level IV or V).
- The tumor has grown into tiny nerves in the skin (perineural invasion).
- The tumor started on an ear or on a part of the lip.
- The tumor cells look very abnormal (poorly differentiated or undifferentiated) under a microscope.
N categories
NX: Nearby lymph nodes cannot be assessed.
N0: The cancer has not spread to nearby lymph nodes.
N1: The cancer has spread to 1 nearby lymph node, which is on the same side of the body as the main tumor and is 3 centimeters (cm) or less across.
N2a: The cancer has spread to 1 nearby lymph node, which is on the same side of the body as the main tumor and is larger than 3 cm but not larger than 6 cm across.
N2b: The cancer has spread to more than 1 nearby lymph node on the same side of the body as the main tumor, none of which are larger than 6 cm across.
N2c: The cancer has spread to nearby lymph node(s) on the other side of the body from the main tumor, none of which are larger than 6 cm across.
N3: The cancer has spread to any nearby lymph node that is larger than 6 cm across.
M categories
M0: The cancer has not spread to other parts of the body.
M1: The cancer has spread to other parts of the body.
Stages of skin cancer
To assign an overall stage, the T, N, and M categories are combined. The stages are described using the number 0 and Roman numerals from I to IV. In general, people with lower stage cancers tend to have a better outlook for a cure or long-term survival.
Table 1. Basal and Squamous Cell Skin Cancer Stages
| Stage 0 | Tis, N0, M0 |
| Stage I | T1, N0, M0 |
| Stage II | T2, N0, M0 |
| Stage III | T3, N0, M0 T1 to T3, N1, M0 |
| Stage IV | T1 to T3, N2, M0 Any T, N3, M0 T4, any N, M0 Any T, any N, M1 |
Treating Basal and Squamous Cell Skin Cancer
If you’ve been diagnosed with basal or squamous cell skin cancer, your doctor will discuss your treatment options with you. It’s important that you think carefully about your choices. You will want to weigh the benefits of each treatment option against the possible risks and side effects.
Which treatments are used for basal and squamous cell skin cancers ?
Based on the type and stage of the cancer and other factors, your treatment options may include:
- Surgery
- Other forms of local therapy
- Radiation therapy
- Systemic chemotherapy
- Targeted therapy
Different approaches might be used to treat basal cell carcinoma, squamous cell carcinoma, actinic keratosis, and Bowen disease. Fortunately, most of these cancers and pre-cancers can be cured with fairly minor surgery or other types of local treatments.
(Other skin cancers, such as melanoma, lymphoma of the skin, Merkel cell carcinoma, Kaposi sarcoma, and other sarcomas are treated differently and are covered elsewhere.)
Making treatment decisions
It’s important to discuss all of your treatment options, including their goals and possible side effects, with your doctors to help make the decision that best fits your needs. Some important things to consider include:
- The type and location of your skin cancer
- The likelihood that treatment will cure your cancer (or help in some other way)
- Your age and overall health
- Possible side effects of treatment, such as scars or changes in your appearance, and your feelings about them
You might feel that you need to make a decision quickly, but it’s important to give yourself time to absorb the information you have just learned. It’s also very important to ask questions if there is anything you’re not sure about.
Getting a second opinion
Before treatment, you might want to consider getting a second opinion, especially if you’re unsure about which option might be best for you. This can give you more information and help you feel more certain about the treatment plan you choose. If you aren’t sure where to go for a second opinion, ask your doctor for help.
Taking part in a clinical trial
Clinical trials are carefully controlled research studies that are done to get a closer look at promising new treatments or procedures. Clinical trials are one way to get state-of-the art cancer treatment. Sometimes they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat cancer. Still, they are not right for everyone.
If you would like to learn more about clinical trials that might be right for you, start by asking your doctor if your clinic or hospital conducts clinical trials.
Melanoma Skin Cancer
Melanoma is a cancer that begins in the melanocytes 3. Other names for this cancer include malignant melanoma and cutaneous melanoma. Most melanoma cells still make melanin, so melanoma tumors are usually brown or black. But some melanomas do not make melanin and can appear pink, tan, or even white.
- Melanoma is less common than some other types of skin cancer, but it is more likely to grow and spread.
- Melanoma accounts for only about 1% of skin cancers but causes a large majority of skin cancer deaths.
Melanomas can develop anywhere on the skin, but they are more likely to start on the trunk (chest and back) in men and on the legs in women. The neck and face are other common sites.
Having darkly pigmented skin lowers your risk of melanoma at these more common sites, but anyone can get melanoma on the palms of the hands, soles of the feet, and under the nails. Melanomas in these areas make up a much larger portion of melanomas in African Americans than in whites.
Melanomas can also form in other parts of your body such as the eyes, mouth, genitals, and anal area, but these are much less common than melanoma of the skin.
Melanoma is much less common than basal cell and squamous cell skin cancers. But melanoma is more dangerous because it’s much more likely to spread to other parts of the body if not caught early.
Figure 6. Melanoma

Note: Melanomas can occur anywhere on the skin, but they are more likely to start in certain areas. The trunk (chest and back) is the most common site in men. The legs are the most common site in women. The neck and face are other common sites.
Figure 7. Melanoma
Note: It’s very important to see a doctor if you have any new moles, moles that are growing or changing in any way, or moles that concern you for any other reason.
The American Cancer Society’s estimates for melanoma in the United States for 2017 are 4:
- About 87,110 new melanomas will be diagnosed (about 52,170 in men and 34,940 in women).
- About 9,730 people are expected to die of melanoma (about 6,380 men and 3,350 women).
The rates of melanoma have been rising for the last 30 years.
Risk Factors for Melanoma Skin Cancer
A risk factor is anything that affects your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking and excess sun exposure, can be changed. Others, like your age or family history, can’t be changed.
- Melanoma is more than 20 times more common in whites than in African Americans. Overall, the lifetime risk of getting melanoma is about 2.5% (1 in 40) for whites, 0.1% (1 in 1,000) for blacks, and 0.5% (1 in 200) for Hispanics.
- The risk of melanoma increases as people age. The average age of people when it is diagnosed is 63. But melanoma is not uncommon even among those younger than 30. In fact, it’s one of the most common cancers in young adults (especially young women).
Having a risk factor, or even many risk factors, does not mean that you will get melanoma. Many people with risk factors never get melanoma, while others with this disease may have few or no known risk factors.
Still, it’s important to know about the risk factors for melanoma because there may be things you can do to lower your risk of getting it. If you are at higher risk because of certain factors, there are also things you can do that might help find it early, when it’s likely to be easier to treat.
Several risk factors can make a person more likely to develop melanoma.
Ultraviolet (UV) light exposure
Exposure to ultraviolet (UV) rays is a major risk factor for most melanomas. Sunlight is the main source of UV rays. Tanning beds and sun lamps are also sources of UV rays.
Ultraviolet light (lightwaves 200-400nm) from the sun can cause sunburn if your skin is exposed for too long. It is always best to try to avoid excessive sun exposure between the peak hours of 10 a.m. to 4 p.m. – this is when UV rays are the strongest.
While UV rays make up only a very small portion of the sun’s rays, they are the main cause of the damaging effects of the sun on the skin. UV rays damage the DNA of skin cells. Skin cancers begin when this damage affects the DNA of genes that control skin cell growth.
The nature of the UV exposure may play a role in melanoma development. For example, melanoma on the trunk (chest and back) and legs has been linked to frequent sunburns (especially in childhood). This might also have something to do with the fact that these areas are not constantly exposed to UV light. Some experts think that melanomas that start in these areas are different from those on the face, neck, and arms, where the sun exposure is more constant. And different from either of these are melanomas on the palms of the hands, soles of the feet, under the nails, or on internal surfaces such as the mouth and vagina, where there has been little or no sun exposure.
Moles
A mole (also known as a nevus) is a benign (non-cancerous) pigmented tumor. Babies are not usually born with moles; they often begin to appear in children and young adults. Most moles will never cause any problems, but someone who has many moles is more likely to develop melanoma.
Atypical moles (dysplastic nevi): These moles look a little like normal moles but also have some features of melanoma. They are often larger than other moles and have an abnormal shape or color. They can appear on skin that is exposed to the sun as well as skin that is usually covered, such as on the buttocks or scalp.
Dysplastic nevi often run in families. A small percentage of dysplastic nevi may develop into melanomas. But most dysplastic nevi never become cancer, and many melanomas seem to arise without a pre-existing dysplastic nevus.
Dysplastic nevus syndrome (also known as familial atypical multiple mole melanoma syndrome, or FAMMM): People with this inherited condition have many dysplastic nevi and at least one close relative who has had melanoma.
People with this condition have a very high lifetime risk of melanoma, so they need to have very thorough, regular skin exams by a dermatologist (a doctor who specializes in skin problems). Sometimes full body photos are taken to help the doctor recognize if moles are changing and growing. Many doctors recommend that these patients be taught to do monthly skin self-exams as well.
Congenital melanocytic nevi: Moles present at birth are called congenital melanocytic nevi. The lifetime risk of melanoma developing in congenital melanocytic nevi is estimated to be between 0 and 10%, depending on the size of the nevus. People with very large congenital nevi have a higher risk, while the risk is lower for those with small nevi. For example, the risk for melanoma in congenital nevi smaller than the palm of your hand is very low, while those that cover large portions of back and buttocks (“bathing trunk nevi”) have significantly higher risks.
Congenital nevi are sometimes removed by surgery so that they don’t have a chance to become cancer. Whether doctors advise removing a congenital nevus depends on several factors including its size, location, and color. Many doctors recommend that congenital nevi that are not removed should be examined regularly by a dermatologist and that the patient should be taught how to do monthly skin self-exams.
Again, the chance of any single mole turning into cancer is very low. However, anyone with lots of irregular or large moles has an increased risk for melanoma.
Fair skin, freckling, and light hair
The risk of melanoma is much higher for whites than for African Americans. Whites with red or blond hair, blue or green eyes, or fair skin that freckles or burns easily are at increased risk.
Family history of melanoma
Your risk of melanoma is higher if one or more of your first-degree relatives (parents, brothers, sisters, or children) has had melanoma. Around 10% of all people with melanoma have a family history of the disease.
The increased risk might be because of a shared family lifestyle of frequent sun exposure, a family tendency to have fair skin, certain gene changes (mutations) that run in a family, or a combination of factors.
Most experts don’t recommend that people with a family history of melanoma have genetic testing to look for mutations, as it’s not yet clear how helpful this is. Rather, experts advise that they do the following:
- Have regular skin exams by a dermatologist
- Thoroughly examine their own skin once a month
- Be particularly careful about sun protection and avoiding artificial UV rays (such as those from tanning booths)
Personal history of melanoma or other skin cancers
A person who has already had melanoma has a higher risk of getting melanoma again. People who have had basal or squamous cell skin cancers are also at increased risk of getting melanoma.
Having a weakened immune system
A person’s immune system helps fight cancers of the skin and other organs. People with weakened immune systems (from certain diseases or medical treatments) are more likely to develop many types of skin cancer, including melanoma.
For example, people who get organ transplants are usually given medicines that weaken their immune system to help prevent them from rejecting the new organ. This increases their risk of melanoma.
People infected with HIV, the virus that causes AIDS, often have weakened immune systems and are also at increased risk for melanoma.
Being older
Melanoma is more likely to occur in older people, but it is also found in younger people. In fact, melanoma is one of the most common cancers in people younger than 30 (especially younger women). Melanoma that runs in families may occur at a younger age.
Being male
In the United States, men have a higher rate of melanoma than women, although this varies by age. Before age 50, the risk is higher for women; after age 50 the risk is higher in men.
Xeroderma pigmentosum
Xeroderma pigmentosum is a rare, inherited condition that affects skin cells’ ability to repair damage to their DNA. People with xeroderma pigmentosum have a high risk of developing melanoma and other skin cancers when they are young, especially on sun-exposed areas of their skin.
What Causes Melanoma Skin Cancer ?
Many risk factors for melanoma have been found, but it’s not always clear exactly how they might cause cancer.
For example, while most moles never turn into a melanoma, some do. Researchers have found some gene changes inside mole cells that may cause them to become melanoma cells. But it’s still not known exactly why some moles become cancerous while most don’t.
DNA is the chemical in each of our cells that makes up our genes, which control how our cells function. You usually look like your parents because they are the source of our DNA. But DNA affects more than just how you look.
Some genes control when your cells grow, divide into new cells, and die:
- Genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that keep cell growth in check or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes. Changes in several different genes are usually needed for a cell to become a cancer cell.
Ultraviolet (UV) rays are clearly a major cause of melanoma. UV rays can damage the DNA in skin cells. Sometimes this damage affects certain genes that control how skin cells grow and divide. If these genes no longer work properly, the affected cells may become cancer cells.
Most UV rays come from sunlight, but some can come from man-made sources such as tanning beds. Usually it’s not clear exactly when the DNA damage from UV exposure occurs. Some of the damage may take place in the few years before the cancer appears. But much of it may be from exposures that happened many years earlier. Children and young adults often get a lot of intense sun exposure that might not result in cancer until many years or even decades later.
Most of the gene changes commonly seen in melanoma cells are not inherited. They are more likely the result of damage caused by sunlight. In some people, such as those with xeroderma pigmentosum, the skin cells are not as able to repair damaged DNA. These people are more likely to develop melanoma.
Some melanomas occur in parts of the body that are rarely exposed to sunlight. These melanomas often have different gene changes than those in melanomas that develop in sun-exposed areas.
When melanomas run in families, gene changes (mutations) that greatly increase the risk of melanoma are often passed from one generation to the next. Familial (inherited) melanomas most often have changes in tumor suppressor genes such as CDKN2A (also known as p16) and CDK4 that prevent them from doing their normal job of controlling cell growth. This could eventually lead to cancer.
- If you’re considering genetic testing, it’s very important to meet first with a genetic counselor or other health professional with knowledge of genetic testing. They can describe the tests to you and explain what the results may or may not tell you about your risk. Genetic testing is not perfect, and sometimes the tests might not provide clear answers.
At this time, because it’s not clear how useful the test results might be, most melanoma experts don’t recommend genetic testing for people with a personal or family history of melanoma. Still, some people may choose to get tested. In any event, people with a family history of melanoma should ask their doctor about getting regular skin exams, learning to do skin self-exams, and being particularly careful about sun safety.
Many other gene changes have been found in melanoma cells as well. Some of these have proven to be good targets for drugs to help treat this disease. For example, about half of all melanomas have a change in the BRAF oncogene that helps drive their growth. This change is not inherited. It seems to occur during the development of the melanoma. Several drugs that specifically target cells with this gene change are now used to treat these melanomas.
Prevention of Melanoma Skin Cancer
There is no sure way to prevent melanoma. Some risk factors such as your age, gender, race, and family history can’t be controlled. But there are things you can do that could lower your risk of getting melanoma and other skin cancers.
Limit your exposure to ultraviolet (UV) rays
The most important way to lower your risk of melanoma is to protect yourself from exposure to UV rays. Practice sun safety when you are outdoors.
Seek shade
Simply staying in the shade is one of the best ways to limit your UV exposure.
Wear sunglasses that block UV rays
UV-blocking sunglasses are important for protecting the delicate skin around the eyes, as well as the eyes themselves. Research has shown that long hours in the sun without protecting your eyes increase your chances of developing certain eye diseases.
The ideal sunglasses should block 99% to 100% of UVA and UVB rays. Before you buy, check the label to make sure they do.
Labels that say:
- “UV absorption up to 400 nm” or
- “Meets ANSI UV Requirements” mean the glasses block at least 99% of UV rays.
- Those labeled “cosmetic” block about 70% of UV rays.
- If there is no label, don’t assume the sunglasses provide any UV protection.
Darker glasses are not necessarily better because UV protection comes from an invisible chemical in or applied to the lenses, not from the color or darkness of the lenses. Look for an ANSI label.
Large-framed and wraparound sunglasses are more likely to protect your eyes from light coming in from different angles. Children need smaller versions of real, protective adult sunglasses – not toy sunglasses.
Ideally, all types of eyewear, including prescription glasses and contact lenses, should protect against UV rays. Some contact lenses are now made to block most UV rays. But because they don’t cover the whole eye and surrounding areas, they are not sufficient eye protection when used alone.
Protect your skin with clothing
When you are out in the sun, wear clothing to cover your skin. Clothes provide different levels of UV protection. Long-sleeved shirts, long pants, or long skirts cover the most skin and are the most protective. Dark colors generally provide more protection than light colors. A tightly woven fabric protects better than loosely woven clothing. Dry fabric is generally more protective than wet fabric.
Be aware that covering up doesn’t block out all UV rays. If you can see light through a fabric, UV rays can get through, too.
Many companies now make clothing that’s lightweight, comfortable, and protects against UV exposure even when wet. It tends to be more tightly woven, and some have special coatings to help absorb UV rays. These sun-protective clothes may have a label listing the UV protection factor (UPF) value (the level of protection the garment provides from the sun’s UV rays, on a scale from 15 to 50+). The higher the UPF, the higher the protection from UV rays.
Sunscreen
If you are going to be in the sun, this catchphrase can help you remember some of the key steps you can take to protect yourself from UV rays:
- Slip on a shirt.
- Slop on sunscreen.
- Slap on a hat.
- Wrap on sunglasses to protect the eyes and sensitive skin around them.
Sunscreen is a product that you put on your skin to protect it from the sun’s UV rays. But it’s important to know that sunscreen is just a filter – it does not block all UV rays. Sunscreen should not be used as a way to prolong your time in the sun. Even with proper sunscreen use, some UV rays still get through. Because of this, sunscreen should not be thought of as your first line of defense. Consider sunscreen as one part of your skin cancer protection plan, especially if staying in the shade and wearing protective clothing aren’t available as your first options.
Sunscreens are available in many forms – lotions, creams, ointments, gels, sprays, wipes, and lip balms, to name a few.
Some cosmetics, such as moisturizers, lipsticks, and foundations, are considered sunscreen products if they have sunscreen. Some makeup contains sunscreen, but you have to check the label – makeup, including lipstick, without sunscreen does not provide sun protection.
Read the labels
When choosing a sunscreen, be sure to read the label. Sunscreens with broad spectrum protection (against both UVA and UVB rays) and with sun protection factor (SPF) values of 30 or higher are recommended.
Sun protection factor (SPF)
The SPF number is the level of protection the sunscreen provides against UVB rays, which are the main cause of sunburn. A higher SPF number means more UVB protection (although it says nothing about UVA protection). For example, when applying an SPF 30 sunscreen correctly, you get the equivalent of 1 minute of UVB rays for each 30 minutes you spend in the sun. So, 1 hour in the sun wearing SPF 30 sunscreen is the same as spending 2 minutes totally unprotected. People often do not apply enough sunscreen, so they get less actual protection.
Sunscreens labeled with SPFs as high as 100+ are available. Higher numbers do mean more protection, but many people don’t understand the SPF scale.
- SPF 15 sunscreens filter out about 93% of UVB rays,
- SPF 30 sunscreens filter out about 97%,
- SPF 50 sunscreens about 98%,
- SPF 100 about 99%.
- The higher you go, the smaller the difference becomes.
- No sunscreen protects you completely.
Sunscreens with an SPF lower than 15 must now include a warning on the label stating that the product has been shown only to help prevent sunburn, not skin cancer or early skin aging.
Broad spectrum sunscreen
Sunscreen products can only be labeled “broad spectrum” if they have been tested and shown to protect against both UVA and UVB rays. Some of the chemicals in sunscreens that help protect against UVA rays include avobenzone (Parsol 1789), ecamsule, zinc oxide, and titanium dioxide.
- Only broad spectrum sunscreen products with an SPF of 15 or higher can state that they help protect against skin cancer and early skin aging if used as directed with other sun protection measures.
Water resistant sunscreen: Sunscreens are no longer allowed to be labeled as “waterproof” or “sweatproof” because these terms can be misleading. Sunscreens can claim to be “water resistant,” but they have to state whether they protect the skin for 40 or 80 minutes of swimming or sweating, based on testing.
Expiration dates: Check the expiration date on the sunscreen to be sure it’s still effective. Most sunscreen products are good for at least 2 to 3 years, but you may need to shake the bottle to remix the sunscreen ingredients. Sunscreens that have been exposed to heat for long periods, such as if they were kept in a glove box or car trunk through the summer, may be less effective.
Be sure to apply the sunscreen properly
Always follow the label directions. Most recommend applying sunscreen generously. When putting it on, pay close attention to your face, ears, neck, arms, and any other areas not covered by clothing. If you’re going to wear insect repellent or makeup, put the sunscreen on first.
Ideally, about 1 ounce of sunscreen (about a shot glass or palmful) should be used to cover the arms, legs, neck, and face of the average adult. Sunscreen needs to be reapplied at least every 2 hours to maintain protection. Sunscreens can wash off when you sweat or swim and then wipe off with a towel, so they might need to be reapplied more often. And don’t forget your lips; lip balm with sunscreen is also available.
Some people might think that if they use a sunscreen with a very high SPF, they don’t need to be as careful about how they use it, but this is not true. If you choose to use a sunscreen with a very high SPF, keep in mind that this doesn’t mean you can stay out in the sun longer, use less sunscreen, or apply it less often. Always be sure to read the label.
Some sunscreen products can irritate your skin. Many products claim to be hypoallergenic or dermatologist tested, but the only way to know for sure if a product will irritate your skin is to try it. One common recommendation is to apply a small amount to the soft skin on the inside of your elbow every day for 3 days. If your skin does not turn red or become itchy, the product is probably OK for you.
Avoid using tanning beds and sunlamps
Many people believe the UV rays of tanning beds are harmless. This is not true. Tanning lamps give out UVA and usually UVB rays as well. Both UVA and UVB rays can cause long-term skin damage, and can contribute to skin cancer. Tanning bed use has been linked with an increased risk of melanoma, especially if it’s started before a person is 30. Most skin doctors and health organizations recommend not using tanning beds and sun lamps.
If you want a tan, one option is to use a sunless tanning lotion, which can provide a darker look without the danger.
Small UV lamps are also used in nail salons (or at home) to dry some types of nail polish. These lamps give off UVA rays. The amount given off is much lower than from tanning beds, and the risk of skin cancer from these lamps is thought to be low. Still, to be safe, some expert groups recommend applying sunscreen to the hands before using one of these lamps.
Protect children from the sun
Children need special attention. They tend to spend more time outdoors, can burn more easily, and may not be aware of the dangers. Parents and other caregivers should protect children from excess sun exposure by using the steps above. It’s important, particularly in sunnier parts of the world, to cover your children as fully as is reasonable. You should develop the habit of using sunscreen on exposed skin for yourself and your children whenever you go outdoors and may be exposed to large amounts of sunlight. Children need to be taught about the dangers of too much sun exposure as they become more independent. If you or your child burns easily, be extra careful to cover up, limit exposure, and apply sunscreen.
Babies younger than 6 months should be kept out of direct sunlight and protected from the sun using hats and protective clothing. Sunscreen may be used on small areas of exposed skin only if adequate clothing and shade are not available.
Watch for abnormal moles
Checking your skin regularly may help you spot any new or abnormal moles or other growths and show them to your doctor before they even have a chance to turn into skin cancer.
Certain types of moles are more likely to develop into melanoma (see Melanoma Skin Cancer Risk Factors). If you have moles, depending on how they look, your doctor may want to watch them closely with regular exams or may remove some of them if they have features that suggest they might change into a melanoma.
Routine removal of many moles is not usually recommended as a way to prevent melanoma. Some melanomas develop from moles, but most do not. If you have many moles, getting careful, routine exams by a dermatologist, along with doing monthly skin self-exams are, might be recommended.
If you find a new, unusual, or changing mole, you should have it checked by a doctor experienced in recognizing skin cancers.
Avoid weakening your immune system (when possible)
Having a weakened immune system increases your risk of getting melanoma and other types of skin cancer.
Infection with HIV, the virus that causes AIDS, can weaken the immune system. Avoiding known risk factors for HIV infection, such as intravenous (IV) drug use and having unprotected sex with many partners, might lower your risk of skin cancer and many other types of cancer.
Some people need to take medicines to suppress their immune system. This includes people who have had organ transplants and some people with autoimmune diseases. People with cancer also sometimes need to take medicines such as chemotherapy that can lower their immune function. For these people, the benefit from taking these medicines will likely far outweigh the small increased risk of getting skin cancer.
Can Melanoma Skin Cancer Be Found Early ?
Melanoma can often be found early, when it is most likely to be cured. Some people have a higher risk of getting melanoma than others, but it’s important to know that anyone can get melanoma.
Skin self-exam
It’s important to check your own skin, preferably once a month. You should know the pattern of moles, blemishes, freckles, and other marks on your skin so that you’ll notice any new moles or changes in existing moles.
Skin self-exams are best done in a well-lit room in front of a full-length mirror. Use a hand-held mirror to help look at areas that are hard to see, such as the backs of your thighs. Examine all areas, including your palms and soles, scalp, ears, nails, and your back (in men, about 1 of every 3 melanomas occurs on the back). Friends and family members can also help you with these exams, especially for those hard-to-see areas, such as your scalp and back.
Exam by a health care professional with experience in skin cancers
Some doctors and other health care professionals do skin exams as part of routine health check-ups.
If your primary doctor finds any unusual moles or other suspicious areas, he or she may refer you to a dermatologist, a doctor who specializes in skin problems. Dermatologists can also do regular skin exams. Many dermatologists use a technique called dermatoscopy (also known as dermoscopy, epiluminescence microscopy [ELM], or surface microscopy) to look at spots on the skin more clearly. A photo of the spot may be taken as well.
Regular skin exams are especially important for people who are at higher risk of melanoma, such as people with dysplastic nevus syndrome, people with a strong family history of melanoma, and people who have had melanoma before. If you have many moles, your doctor might advise taking full-body photos so your moles can be tracked over time and new ones can be seen more readily. This is sometimes called total body photography or mole mapping. Talk to your doctor about how often you should have your skin examined.
Signs and Symptoms of Melanoma Skin Cancer
Unusual moles, sores, lumps, blemishes, markings, or changes in the way an area of the skin looks or feels may be a sign of melanoma or another type of skin cancer, or a warning that it might occur.
Normal moles
A normal mole is usually an evenly colored brown, tan, or black spot on the skin. It can be either flat or raised. It can be round or oval. Moles are generally less than 6 millimeters (about ¼ inch) across (about the width of a pencil eraser). Some moles can be present at birth, but most appear during childhood or young adulthood. New moles that appear later in life should be checked by a doctor.
Once a mole has developed, it will usually stay the same size, shape, and color for many years. Some moles may eventually fade away.
Most people have moles, and almost all moles are harmless. But it’s important to recognize changes in a mole – such as in its size, shape, or color – that can suggest a melanoma may be developing.
Possible signs and symptoms of melanoma
The most important warning sign of melanoma is a new spot on the skin or a spot that is changing in size, shape, or color. Another important sign is a spot that looks different from all of the other spots on your skin (known as the ugly duckling sign). If you have one of these warning signs, have your skin checked by a doctor.
The ABCDE rule is another guide to the usual signs of melanoma. Be on the lookout and tell your doctor about spots that have any of the following features:
- A is for Asymmetry: One half of a mole or birthmark does not match the other.
- B is for Border: The edges are irregular, ragged, notched, or blurred.
- C is for Color: The color is not the same all over and may include different shades of brown or black, or sometimes with patches of pink, red, white, or blue.
- D is for Diameter: The spot is larger than 6 millimeters across (about ¼ inch – the size of a pencil eraser), although melanomas can sometimes be smaller than this.
- E is for Evolving: The mole is changing in size, shape, or color.
Some melanomas don’t fit these rules.
- It’s important to tell your doctor about any changes or new spots on the skin, or growths that look different from the rest of your moles.
Other warning signs are:
- A sore that doesn’t heal
- Spread of pigment from the border of a spot into surrounding skin
- Redness or a new swelling beyond the border of the mole
- Change in sensation, such as itchiness, tenderness, or pain
- Change in the surface of a mole – scaliness, oozing, bleeding, or the appearance of a lump or bump
Be sure to show your doctor any areas that concern you and ask your doctor to look at areas that may be hard for you to see. It’s sometimes hard to tell the difference between melanoma and an ordinary mole, even for doctors, so it’s important to show your doctor any mole that you are unsure of.
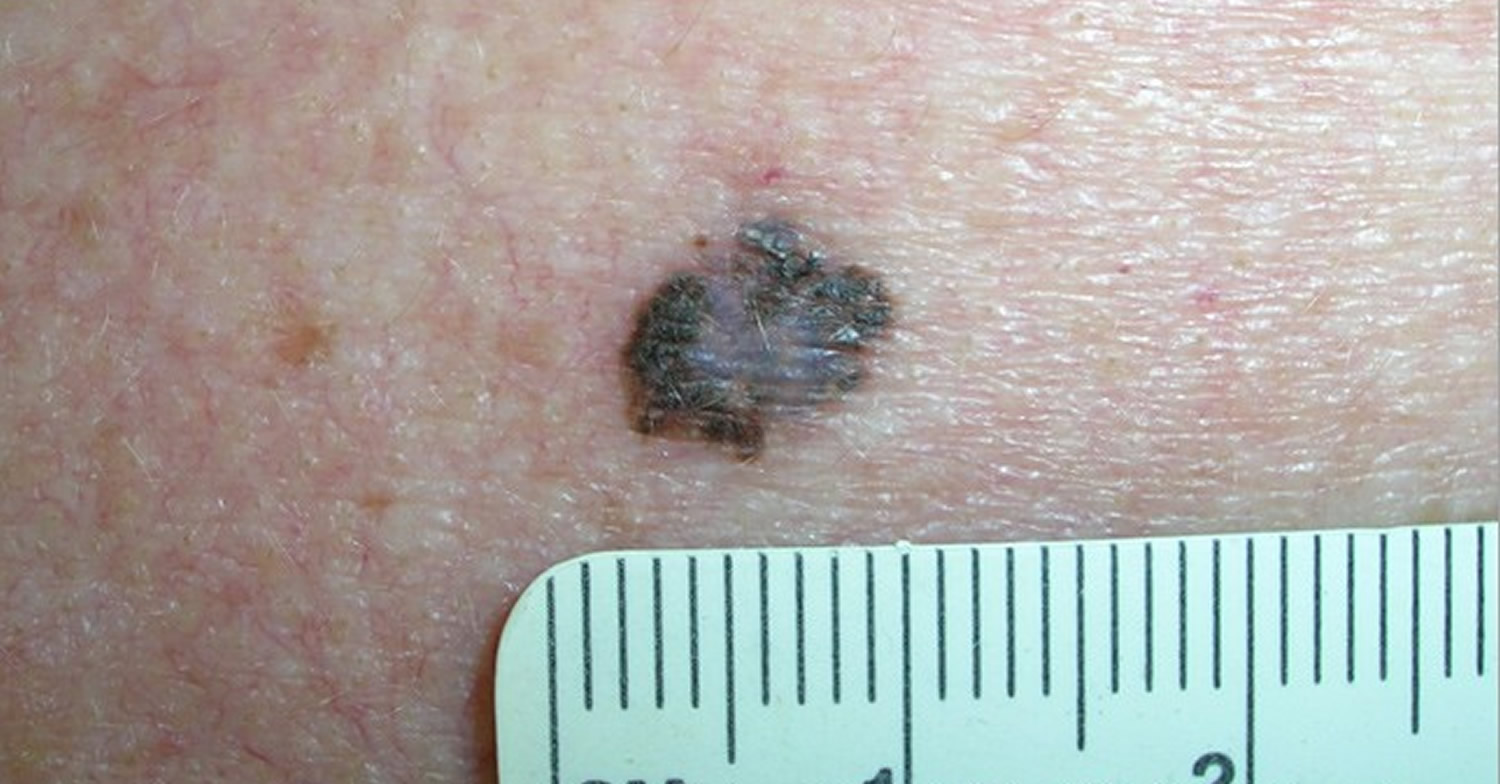
ABCDE Criteria of Melanoma
The “ABCDE” criteria describes the features of early melanoma 5:
- A is for Asymmetric shape. One half is unlike the other half.
- B is for Irregular Border. Look for moles with irregular, notched or scalloped borders.
- C is for Multiple Colors or dark black. Look for growths that have changed color, have many colors or have uneven color.
- D is for Diameter > 6 mm. Look for new growth in a mole larger than 1/4 inch (about 6 millimeters).
- E is for Evolving, changing (e.g., present for years unchanged and then suddenly grows). Watch for moles that change in size, shape, color or height, especially if part or all of a mole turns black. Moles may also evolve to develop new signs and symptoms, such as itchiness or bleeding.
Cancerous (malignant) moles vary greatly in appearance. Some may show all of the features listed above. Others may have only one or two.
Figure 8. Asymmetric shape (melanoma in-situ)

Figure 9. Irregular Border (melanoma)

Figure 10. Multiple Colors or dark black (melanoma)

Figure 11. Diameter > 6 mm (melanoma)

Figure 12. Evolving, changing (melanoma)

Tests for Melanoma Skin Cancer
Most melanomas are brought to a doctor’s attention because of signs or symptoms a person is having.
If you have an abnormal area that might be skin cancer, your doctor will examine it and might do tests to find out if it is melanoma, another type of skin cancer, or some other skin condition. If melanoma is found, other tests may be done to find out if it has spread to other areas of the body.
Medical history and physical exam
Usually the first step your doctor takes is to ask about your symptoms, such as when the mark on the skin first appeared, if it has changed in size or appearance, and if it has been painful, itchy, or bleeding. You may also be asked about your possible risk factors for skin cancer, such as history of tanning and sunburns, and if you or anyone in your family has had skin cancer.
During the physical exam, your doctor will note the size, shape, color, and texture of the area(s) in question, and whether it is bleeding, oozing, or crusting. The rest of your body may be checked for moles and other spots that could be related to skin cancer.
The doctor may also feel the lymph nodes (small, bean-sized collections of immune cells) under the skin in the neck, underarm, or groin near the abnormal area. When melanoma spreads, it often goes to nearby lymph nodes first, making them larger. Enlarged lymph nodes might suggest that melanoma could have spread there.
If you are being seen by your primary doctor and melanoma is suspected, you may be referred to a dermatologist, a doctor who specializes in skin diseases, who will look at the area more closely.
Along with a standard physical exam, many dermatologists use a technique called dermatoscopy (also known as dermoscopy, epiluminescence microscopy [ELM], or surface microscopy) to see spots on the skin more clearly. The doctor uses a dermatoscope, which is a special magnifying lens and light source held near the skin. Sometimes a thin layer of alcohol or oil is used with this instrument. The doctor may take a digital photo of the spot.
When used by an experienced dermatologist, this test can improve the accuracy of finding skin cancers early. It can also often help reassure you that a spot on the skin is probably benign (non-cancerous) and doesn’t need a biopsy.
Types of skin biopsies
If the doctor thinks a spot might be a melanoma, the suspicious area will be removed and sent to a lab to be looked at under a microscope. This is called a skin biopsy.
There are many ways to do a skin biopsy. The doctor will choose one based on the size of the affected area, where it is on your body, and other factors. Any biopsy is likely to leave at least a small scar. Different methods can result in different types of scars, so ask your doctor about scarring before the biopsy. No matter which type of biopsy is done, it should remove as much of the suspected area as possible so that an accurate diagnosis can be made.
Skin biopsies are done using a local anesthetic (numbing medicine), which is injected into the area with a very small needle. You will likely feel a small prick and a little stinging as the medicine is injected, but you should not feel any pain during the biopsy.
Shave (tangential) biopsy
For this type of biopsy, the doctor shaves off the top layers of the skin with a small surgical blade. Bleeding from the biopsy site is stopped by applying an ointment, a chemical that stops bleeding, or a small electrical current to cauterize the wound.
A shave biopsy is useful in diagnosing many types of skin diseases and in sampling moles when the risk of melanoma is very low. This type of biopsy is not generally used if a melanoma is strongly suspected unless the biopsy blade will go deep enough to get below the suspicious area. Otherwise, if it is a melanoma, the biopsy sample may not be thick enough to measure how deeply the cancer has invaded the skin.
Punch biopsy
For a punch biopsy, the doctor uses a tool that looks like a tiny round cookie cutter to remove a deeper sample of skin. The doctor rotates the punch biopsy tool on the skin until it cuts through all the layers of the skin. The sample is removed and the edges of the biopsy site are often stitched together.
Incisional and excisional biopsies
To examine a tumor that might have grown into deeper layers of the skin, the doctor may use an incisional or excisional biopsy. For these types of biopsies, a surgical knife is used to cut through the full thickness of skin. A wedge or sliver of skin is removed for examination, and the edges of the cut are usually stitched together.
An incisional biopsy removes only a portion of the tumor. An excisional biopsy removes the entire tumor, and is usually the preferred method of biopsy for suspected melanomas if it can be done. But this is not always possible, so other types of biopsies may be needed.
“Optical” biopsies
Some newer types of biopsies, such as reflectance confocal microscopy, can be done without needing to remove samples of skin.
Biopsies of melanoma that may have spread
Biopsies of areas other than the skin may be needed in some cases. For example, if melanoma has already been diagnosed on the skin, nearby lymph nodes may be biopsied to see if the cancer has spread to them.
Rarely, biopsies may be needed to figure out what type of cancer someone has. For example, some melanomas can spread so quickly that they reach the lymph nodes, lungs, brain, or other areas while the original skin melanoma is still very small. Sometimes these tumors are found with imaging tests (such as CT scans) or other exams even before the melanoma on the skin is discovered. In other cases they may be found long after a skin melanoma has been removed, so it’s not clear if it’s the same cancer.
In still other cases, melanoma may be found somewhere in the body without ever finding a spot on the skin. This may be because some skin lesions go away on their own (without any treatment) after some of their cells have spread to other parts of the body. Melanoma can also start in internal organs, but this is very rare, and if melanoma has spread widely throughout the body, it may not be possible to tell exactly where it started.
When melanoma has spread to other organs, it can sometimes be confused with a cancer starting in that organ. For example, melanoma that has spread to the lung might be confused with a primary lung cancer (cancer that starts in the lung).
Special lab tests can be done on the biopsy samples that can tell whether it is a melanoma or some other kind of cancer. This is important because different types of cancer are treated differently.
Biopsies of suspicious areas inside the body often are more involved than those used to sample the skin.
Fine needle aspiration (FNA) biopsy
FNA biopsy is not used on suspicious moles. But it may be used, for example, to biopsy large lymph nodes near a melanoma to find out if the melanoma has spread to them.
For this type of biopsy, the doctor uses a syringe with a thin, hollow needle to remove very small pieces of a lymph node or tumor. The needle is smaller than the needle used for a blood test. A local anesthetic is sometimes used to numb the area first. This test rarely causes much discomfort and does not leave a scar.
If the lymph node is just under the skin, the doctor can often feel it well enough to guide the needle into it. For a suspicious lymph node deeper in the body or a tumor in an organ such as the lung or liver, an imaging test such as ultrasound or a CT scan is often used to help guide the needle into place.
FNA biopsies are not as invasive as some other types of biopsies, but they may not always collect enough of a sample to tell if a suspicious area is melanoma. In these cases, a more invasive type of biopsy may be needed.
Surgical (excisional) lymph node biopsy
This procedure can be used to remove an enlarged lymph node through a small incision (cut) in the skin. A local anesthetic (numbing medicine) is generally used if the lymph node is just under the skin, but the person may need to be sedated or even asleep (using general anesthesia) if the lymph node is deeper in the body.
This type of biopsy is often done if a lymph node’s size suggests the melanoma has spread there but an FNA biopsy of the node wasn’t done or didn’t find any melanoma cells.
Sentinel lymph node biopsy
If melanoma has been diagnosed and has any concerning features (such as being at least a certain thickness), a sentinel lymph node biopsy is often done to see if the cancer has spread to nearby lymph nodes, which in turn might affect treatment options. This test can be used to find the lymph nodes that are likely to be the first place the melanoma would go if it has spread. These lymph nodes are called sentinel nodes (they stand sentinel, or watch, over the tumor, so to speak).
To find the sentinel lymph node (or nodes), a nuclear medicine doctor injects a small amount of a radioactive substance into the area of the melanoma. After giving the substance time to travel to the lymph node areas near the tumor, a special camera is used to see if it collects in one or more sentinel lymph nodes. Once the radioactive area has been marked, the patient is taken for surgery, and a blue dye is injected in the same place as the radioactive substance. A small incision is then made in the marked area, and the lymph nodes are then checked to find which one(s) became radioactive and turned blue. These sentinel nodes are removed and looked at under a microscope.
If there are no melanoma cells in the sentinel nodes, no more lymph node surgery is needed because it is very unlikely the melanoma would have spread beyond this point. If melanoma cells are found in the sentinel node, the remaining lymph nodes in this area are removed and looked at as well. This is known as a lymph node dissection.
If a lymph node near a melanoma is abnormally large, a sentinel node biopsy probably won’t be needed. The enlarged node is simply biopsied.
Lab tests of biopsy samples
Samples from any biopsies will be sent to a lab, where a doctor called a pathologist will look at them under a microscope for melanoma cells. Often, skin samples are sent to a dermatopathologist, a doctor who has special training in looking at skin samples.
If the doctor can’t tell for sure if melanoma cells are in the sample just by looking at it, special lab tests will be done on the cells to try to confirm the diagnosis. These tests have names such as immunohistochemistry, fluorescence in situ hybridization (FISH), and comparative genomic hybridization.
If melanoma is found in the samples, the pathologist will look at certain important features such as the tumor thickness and mitotic rate (the portion of cells that are actively dividing). These features help determine the stage of the melanoma , which in turn affects treatment options and prognosis (outlook).
Testing for gene changes: For people who have advanced melanoma, biopsy samples may be tested to see if the cells have mutations (changes) in certain genes, such as the BRAF gene. About half of melanomas have BRAF mutations. Some newer drugs used to treat advanced melanomas are only likely to work if the cells have BRAF mutations, so this test is important in helping to determine treatment options.
A newer lab test known as DecisionDx-Melanoma looks at certain gene expression patterns in melanoma cells to help show if early-stage melanomas are likely to spread. This can be used to help determine treatment options.
Imaging tests
Imaging tests use x-rays, magnetic fields, or radioactive substances to create pictures of the inside of the body. They are used mainly to look for the possible spread of melanoma to lymph nodes or other organs in the body. They are not needed for people with very early-stage melanoma, which is very unlikely to have spread.
Imaging tests can also be done to help determine how well treatment is working or to look for possible signs of cancer coming back (recurring) after treatment.
Chest x-ray
This test may be done to help determine if melanoma has spread to the lungs.
Computed tomography (CT) scan
The CT scan uses x-rays to make detailed, cross-sectional images of your body. Unlike a regular x-ray, CT scans can show the detail in soft tissues (such as internal organs). This test can show if any lymph nodes are enlarged or if organs such as the lungs or liver have suspicious spots, which might be from the spread of melanoma.
CT-guided needle biopsy: CT scans can also be used to help guide a biopsy needle into a suspicious area within the body.
Magnetic resonance imaging (MRI) scan
MRI scans use radio waves and strong magnets instead of x-rays to create detailed images of parts of your body. MRI scans are very helpful in looking at the brain and spinal cord.
Positron emission tomography (PET) scan
A PET scan can help show if the cancer has spread to lymph nodes or other parts of the body. It is most useful in people with more advanced stages of melanoma, but it’s not usually done in people with early-stage melanoma.
For this test, you are injected with a slightly radioactive form of sugar, which collects mainly in cancer cells. A special camera is then used to create a picture of areas of radioactivity in the body.
PET/CT scan: Many centers have special machines that do both a PET and CT scan at the same time (PET/CT scan). This lets the doctor compare areas of higher radioactivity on the PET scan with the more detailed appearance of that area on the CT scan.
Blood tests
Blood tests aren’t used to diagnose melanoma, but some tests may be done before or during treatment, especially for more advanced melanomas.
Doctors often test blood for levels of a substance called lactate dehydrogenase (LDH) before treatment. If the melanoma has spread to distant parts of the body, a high LDH level is a sign that the cancer may be harder to treat. This affects the stage of the cancer.
Other tests of blood cell counts and blood chemistry levels may be done in a person who has advanced melanoma to see how well the bone marrow (where new blood cells are made), liver, and kidneys are working during treatment.
Melanoma Skin Cancer Stages
The stage of a cancer describes how widespread it is. For melanoma, this includes its thickness in the skin, whether it has spread to nearby lymph nodes or any other organs, and certain other factors. The stage is based on the results of physical exams, biopsies, and any imaging tests (CT or MRI scan, etc.) or other tests that have been done. These are described in Tests for Melanoma Skin Cancer. The stage of the melanoma is very important in planning your treatment and estimating your prognosis (outlook).
Understanding the stage of your melanoma
The staging system most often used for melanoma is the American Joint Commission on Cancer TNM system, which is based on 3 key pieces of information:
- T stands for the main (primary) tumor (how far it has grown within the skin and other factors).
- N stands for spread to nearby lymph nodes (bean-sized collections of immune system cells, to which cancers often spread first).
- M category is based on whether the melanoma has metastasized (spread) to distant organs.
T categories
The T category is based on:
- Tumor thickness: The thickness of the melanoma is called the Breslow measurement. In general, melanomas less than 1 millimeter (mm) thick (about 1/25 of an inch) have a very small chance of spreading. As the melanoma becomes thicker, it has a greater chance of spreading.
- Mitotic rate: The mitotic rate is the portion of cancer cells in the process of dividing (mitosis). A higher mitotic rate (having more cells that are dividing) means that the cancer is more likely to grow and spread. The mitotic rate is used to help stage thin melanomas (T1; see below).
- Ulceration: Ulceration is a breakdown of the skin over the melanoma. Melanomas that are ulcerated tend to have a worse outlook.
The possible values for T are:
- TX: Primary (main) tumor cannot be assessed.
- T0: No evidence of primary tumor.
- Tis: Melanoma in situ. (The tumor is only in the epidermis, the outermost layer of skin.)
- T1a: The melanoma is less than or equal to 1.0 mm thick (1.0 mm = 1/25 of an inch), without ulceration and with a mitotic rate of less than 1/mm2.
- T1b: The melanoma is less than or equal to 1.0 mm thick. It is ulcerated and/or the mitotic rate is equal to or greater than 1/mm2.
- T2a: The melanoma is between 1.01 and 2.0 mm thick without ulceration.
- T2b: The melanoma is between 1.01 and 2.0 mm thick with ulceration.
- T3a: The melanoma is between 2.01 and 4.0 mm thick without ulceration.
- T3b: The melanoma is between 2.01 and 4.0 mm thick with ulceration.
- T4a: The melanoma is thicker than 4.0 mm without ulceration.
- T4b: The melanoma is thicker than 4.0 mm with ulceration.
N categories
The possible values for N depend on whether or not a sentinel lymph node biopsy was done.
If the sentinel node biopsy is not done, doctors use the clinical stage of the lymph nodes, which is listed below.
- NX: Nearby (regional) lymph nodes cannot be assessed.
- N0: No spread to nearby lymph nodes.
- N1: Spread to 1 nearby lymph node.
- N2: Spread to 2 or 3 nearby lymph nodes, OR spread of melanoma to nearby skin (known as satellite tumors) or toward a nearby lymph node area (known as in-transit tumors) without reaching the lymph nodes.
- N3: Spread to 4 or more lymph nodes, OR spread to lymph nodes that are clumped together, OR spread of melanoma to nearby skin (satellite tumors) or toward a lymph node area and into the lymph node(s).
If a lymph node biopsy is done, the pathologic stage can be determined, in which small letters may be added in some cases:
- Any Na (N1a or N2a) means that the melanoma is in the lymph node(s), but it is so small that it is only seen under the microscope (also known as microscopic spread).
- Any Nb (N1b or N2b) means that the melanoma is in the lymph node(s) and was large enough to be seen on imaging tests or felt by the doctor before it was removed (also known as macroscopic spread).
- N2c means the melanoma has spread to very small areas of nearby skin (satellite tumors) or has spread to skin lymphatic channels around the tumor (without reaching the lymph nodes).
M categories
The M values are:
- M0: No distant metastasis.
- M1a: Metastasis to skin, subcutaneous (below the skin) tissue, or lymph nodes in distant parts of the body, with a normal blood LDH level.
- M1b: Metastasis to the lungs, with a normal blood LDH level.
- M1c: Metastasis to any other organs, OR distant spread to any site along with an elevated blood LDH level.
Stages of melanoma
Once the T, N, and M groups have been determined, they are combined to give an overall stage, using 0 and the Roman numerals I to IV (1 to 4). Some stages are further divided using capital letters.
In general, people with lower stage cancers have a better outlook for a cure or long-term survival, but other factors can also come into play. The staging of melanoma can be complex, so be sure to ask your doctor if you have any questions about the stage of your melanoma.
Table 2. Melanoma stages
| Stage | Stage grouping | Stage description |
| 0 | Tis, N0, M0 | The melanoma is still only in the epidermis (in situ) but has not spread to deeper skin layers. |
| IA | T1a, N0, M0 | The melanoma is less than 1.0 mm thick. It is not ulcerated and has a mitotic rate of less than 1/mm2. It has not been found in lymph nodes or distant organs. |
| IB | T1b or T2a, N0, M0 | The melanoma is less than 1.0 mm thick and is ulcerated or has a mitotic rate of at least 1/mm2, OR it is between 1.01 and 2.0 mm and is not ulcerated. It has not been found in lymph nodes or distant organs. |
| IIA | T2b or T3a, N0, M0 | The melanoma is between 1.01 mm and 2.0 mm thick and is ulcerated, OR it is between 2.01 and 4.0 mm thick and is not ulcerated. It has not been found in lymph nodes or distant organs. |
| IIB | T3b or T4a, N0, M0 | The melanoma is between 2.01 mm and 4.0 mm thick and is ulcerated, OR it is thicker than 4.0 mm and is not ulcerated. It has not been found in lymph nodes or distant organs. |
| IIC | T4b, N0, M0 | The melanoma is thicker than 4.0 mm and is ulcerated. It has not been found in lymph nodes or distant organs. |
| IIIA | T1a to T4a, N1a or N2a, M0 | The melanoma can be any thickness, but it is not ulcerated. It has spread to 1 to 3 lymph nodes near the affected skin area, but the nodes are not enlarged and the melanoma is found only when they are viewed under the microscope. There is no distant spread. |
| IIIB | T1b to T4b, N1a or N2a, M0 | The melanoma can be any thickness and is ulcerated. It has spread to 1 to 3 lymph nodes near the affected skin area, but the nodes are not enlarged and the melanoma is found only when they are viewed under the microscope. There is no distant spread. |
| OR | ||
| T1a to T4a, N1b or N2b, M0 | The melanoma can be any thickness, but it is not ulcerated. It has spread to 1 to 3 lymph nodes near the affected skin area. The nodes are enlarged because of the melanoma. There is no distant spread. | |
| OR | ||
| T1a to T4a, N2c, M0 | The melanoma can be any thickness, but it is not ulcerated. It has spread to small areas of nearby skin (satellite tumors) or lymphatic channels (in-transit tumors) around the original tumor, but the nodes do not contain melanoma. There is no distant spread. | |
| IIIC | T1b to T4b, N1b or N2b, M0 | The melanoma can be any thickness and is ulcerated. It has spread to 1 to 3 lymph nodes near the affected skin area. The nodes are enlarged because of the melanoma. There is no distant spread. |
| OR | ||
| T1b to T4b, N2c, M0 | The melanoma can be any thickness and is ulcerated. It has spread to small areas of nearby skin (satellite tumors) or lymphatic channels (in-transit tumors) around the original tumor, but the nodes do not contain melanoma. There is no distant spread. | |
| OR | ||
| Any T, N3, M0 | The melanoma can be any thickness and may or may not be ulcerated. It has spread to 4 or more nearby lymph nodes, OR to nearby lymph nodes that are clumped together, OR it has spread to nearby skin (satellite tumors) or lymphatic channels (in transit tumors) around the original tumor and to nearby lymph nodes. The nodes are enlarged because of the melanoma. There is no distant spread. | |
| IV | Any T, any N, M1(a, b, or c) | The melanoma has spread beyond the original area of skin and nearby lymph nodes to other organs such as the lung, liver, or brain, or to distant areas of the skin, subcutaneous tissue, or distant lymph nodes. Neither thickness nor spread to nearby lymph nodes is considered in this stage, but typically the melanoma is thick and has also spread to the lymph nodes. |
Survival Rates for Melanoma Skin Cancer, by Stage
Survival rates tell you what portion of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 or 10 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful. Some people will want to know the survival rates for their cancer, and some people won’t. If you don’t want to know, you don’t have to.
What is a 5-year or 10-year survival rate ?
Statistics on the outlook for a certain type and stage of cancer are often given as 5-year or 10-year survival rates, but many people live longer – often much longer. The survival rate is the percentage of people who live at least a certain amount of time after being diagnosed with cancer.
But remember, survival rates are estimates – your outlook can vary based on a number of factors specific to you. Cancer survival rates don’t tell the whole story
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a number of limitations to remember:
- The numbers below are among the most current available. But to get 5-year or 10-year survival rates, doctors have to look at people who were treated at least 5 or 10 years ago. As treatments are improving over time, people who are now being diagnosed with melanoma may have a better outlook than these statistics show.
- These statistics are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that later come back or spread, for example.
- The outlook for people with melanoma varies by the stage (extent) of the cancer – in general, the survival rates are higher for people with earlier stage cancers. But many other factors can affect a person’s outlook, such as age and overall health, and how well the cancer responds to treatment. The outlook for each person is specific to their circumstances.
Your doctor can tell you how these numbers may apply to you, as he or she is familiar with your particular situation.
Survival rates for melanoma
The following survival rates are based on nearly 60,000 patients who were part of the 2008 AJCC Melanoma Staging Database. These survival rates include some people diagnosed with melanoma who may have died later from other causes, such as heart disease. Therefore, the percentage of people surviving the melanoma itself may be higher.
- Stage IA: The 5-year survival rate is around 97%. The 10-year survival is around 95%.
- Stage IB: The 5-year survival rate is around 92%. The 10-year survival is around 86%.
- Stage IIA: The 5-year survival rate is around 81%. The 10-year survival is around 67%.
- Stage IIB: The 5-year survival rate is around 70%. The 10-year survival is around 57%.
- Stage IIC: The 5-year survival rate is around 53%. The 10-year survival is around 40%.
- Stage IIIA: The 5-year survival rate is around 78%. The 10-year survival is around 68%.*
- Stage IIIB: The 5-year survival rate is around 59%. The 10-year survival is around 43%.
- Stage IIIC: The 5-year survival rate is around 40%. The 10-year survival is around 24%.
- Stage IV: The 5-year survival rate is about 15% to 20%. The 10-year survival is about 10% to 15%. The outlook is better if the spread is only to distant parts of the skin or distant lymph nodes rather than to other organs, and if the blood level of lactate dehydrogenase (LDH) is normal.
*The survival rate is higher for stage IIIA cancers than for some stage II cancers. This is likely because the main (primary) tumor is often less advanced for IIIA cancers, although this is not clear.
Remember, these survival rates are only estimates – they can’t predict what will happen to any individual. We understand that these statistics can be confusing and might lead you to have more questions. Talk to your doctor to better understand your specific situation.
Other factors affecting survival
Factors other than stage can also affect survival. For example:
- Older people generally have shorter survival times than younger people, regardless of stage.
- Melanoma is uncommon among African Americans, but when it does occur, survival times tend to be shorter than when it occurs in whites. Some studies have found that melanoma tends to be more serious if it occurs on the sole of the foot or palm of the hand, or if it is in a nail bed. (Cancers in these areas make up a larger portion of melanomas in African Americans than in whites.)
- People with melanoma who have weakened immune systems, such as people who have had organ transplants or who are infected with HIV, also are at greater risk of dying from their melanoma.
How is Melanoma Skin Cancer Treated
Once melanoma has been diagnosed and staged, your cancer care team will discuss your treatment options with you. It’s important that you think carefully about your choices. You will want to weigh the benefits of each treatment option against its possible risks and side effects.
Which treatments are used for melanoma ?
Based on the stage of the cancer and other factors, your treatment options might include:
- Surgery
- Immunotherapy
- Targeted therapy
- Chemotherapy
- Radiation therapy
Early-stage melanomas can often be treated with surgery alone, but more advanced cancers often require other treatments. Sometimes more than one type of treatment is used.
Which doctors treat melanoma ?
Depending on your options, you may have different types of doctors on your treatment team. These doctors may include:
- A dermatologist: a doctor who treats diseases of the skin
- A surgical oncologist (or oncologic surgeon): a doctor who uses surgery to treat cancer
- A medical oncologist: a doctor who treats cancer with medicines such as chemotherapy, immunotherapy, or targeted therapy
- A radiation oncologist: a doctor who treats cancer with radiation therapy
Many other specialists might be part of your treatment team as well, including physician assistants, nurse practitioners, nurses, nutrition specialists, social workers, and other health professionals.
Making treatment decisions
It’s important to discuss all of your treatment options as well as their possible side effects with your treatment team to help make the decision that best fits your needs. Some important things to consider include:
- Your age and overall health
- The stage (extent) of your cancer
- The likelihood that treatment will cure your cancer (or help in some other way)
- Your feelings about the possible side effects from treatment
You may feel that you need to make a decision quickly, but it’s important to give yourself time to absorb the information you have just learned. It’s also very important to ask questions if there is anything you’re not sure about.
Getting a second opinion
If time allows, you may also want to get a second opinion from another doctor or medical team. This can give you more information and help you feel more certain about the treatment plan you choose. If you aren’t sure where to go for a second opinion, ask your doctor for help.
Taking part in a clinical trial
Clinical trials are carefully controlled research studies that are done to get a closer look at promising new treatments or procedures. Clinical trials are one way to get state-of-the art cancer treatment. Sometimes they may be the only way to get access to newer treatments. They are also the best way for doctors to learn better methods to treat cancer. Still, they are not right for everyone.
If you would like to learn more about clinical trials that might be right for you, start by asking your doctor if your clinic or hospital conducts clinical trials.
Considering complementary and alternative methods
You may hear about alternative or complementary methods that your doctor hasn’t mentioned to treat your cancer or relieve symptoms. These methods can include vitamins, herbs, and special diets, or other methods such as acupuncture or massage, to name a few.
Complementary methods refer to treatments that are used along with your regular medical care. Alternative treatments are used instead of a doctor’s medical treatment. Although some of these methods might be helpful in relieving symptoms or helping you feel better, many have not been proven to work. Some might even be dangerous.
Be sure to talk to your cancer care team about any method you are thinking about using. They can help you learn what is known (or not known) about the method, which can help you make an informed decision. See Complementary and Alternative Medicine to learn more.
Choosing to stop treatment or choosing no treatment at all
For some people, when treatments have been tried and are no longer controlling the cancer, it could be time to weigh the benefits and risks of continuing to try new treatments. Whether or not you continue treatment, there are still things you can do to help maintain or improve your quality of life.
Some people, especially if the cancer is advanced, might not want to be treated at all. There are many reasons you might decide not to get cancer treatment, but it’s important to talk this through with your doctors before you make this decision. Remember that even if you choose not to treat the cancer, you can still get supportive care to help with pain or other symptoms.
Help getting through cancer treatment
Your cancer care team will be your first source of information and support, but there are other resources for help when you need it. Hospital- or clinic-based support services can be an important part of your care. These might include nursing or social work services, financial aid, nutritional advice, rehab, or spiritual help.
Can you lower your risk of the melanoma progressing or coming back ?
If you have (or have had) melanoma, you probably want to know if there are things you can do that might lower your risk of the cancer coming back, or of getting a new skin cancer.
At this time, not enough is known about melanoma to say for sure if there are things you can do that will be helpful. Doctors do know that people who have had melanoma are at higher risk for developing another melanoma or other type of skin cancer. Because of this, it’s very important to limit your exposure to UV rays (from the sun or tanning beds) and to continue to examine your skin every month for signs of melanoma coming back or possible new skin cancers. Skin cancers that are found early are typically much easier to treat than those found at a later stage.
To help maintain good health, melanoma survivors should also:
- Get to and stay at a healthy weight
- Be physically active
- Eat a healthy diet, with an emphasis on plant foods
- Limit alcohol to no more than 1 drink per day for women or 2 per day for men
These steps may also lower the risk of other health problems.
Adopting healthy behaviors such as not smoking, eating well, being active, and staying at a healthy weight might help as well, but no one knows for sure. However, doctors do know that these types of changes can have positive effects on your health that can extend beyond your risk of melanoma or other cancers.
About dietary supplements
So far, no dietary supplements (including vitamins, minerals, and herbal products) have been shown to clearly help lower the risk of melanoma progressing or coming back. This doesn’t mean that no supplements will help, but it’s important to know that none have been proven to do so.
Dietary supplements are not regulated like medicines in the United States – they do not have to be proven effective (or even safe) before being sold, although there are limits on what they’re allowed to claim they can do. If you are thinking about taking any type of nutritional supplement, talk to your health care team. They can help you decide which ones you can use safely while avoiding those that might be harmful.
If the cancer comes back
If melanoma does come back at some point, your treatment options will depend on where the cancer is, what treatments you’ve had before, and your overall health.
Could you get a second cancer after melanoma treatment ?
People who’ve had melanoma can still get other cancers. In fact, melanoma survivors are at higher risk for getting some other types of cancer.
Less common types of skin cancer
Other types of skin cancer are much less common and are treated differently. These include:
- Merkel cell carcinoma
- Kaposi sarcoma
- Cutaneous (skin) lymphoma
- Skin adnexal tumors (tumors that start in hair follicles or skin glands)
- Various types of sarcomas
Together, these types account for less than 1% of all skin cancers.
Pre-cancerous and pre-invasive skin conditions
These conditions may develop into skin cancer or may be very early stages of skin cancer.
Actinic keratosis (solar keratosis)
Actinic keratosis, also known as solar keratosis, is a pre-cancerous skin condition caused by too much exposure to the sun. Solar keratosis are usually small (less than 1/4 inch across), rough or scaly spots that may be pink-red or flesh-colored. Usually they start on the face, ears, backs of the hands, and arms of middle-aged or older people with fair skin, although they can occur on other sun-exposed areas. People who have them usually develop more than one.
Solar keratosis tend to grow slowly and usually do not cause any symptoms (although some might be itchy or sore). They sometimes go away on their own, but they may come back.
Some solar keratosis may turn into squamous cell skin cancers. Most solar keratosis do not become cancer, but it can be hard sometimes to tell them apart from true skin cancers, so doctors often recommend treating them. If they are not treated, you and your doctor should check them regularly for changes that might be signs of skin cancer.
Squamous cell carcinoma in situ (Bowen disease)
Squamous cell carcinoma in situ, also called Bowen disease, is the earliest form of squamous cell skin cancer. “In situ” means that the cells of these cancers are still only in the epidermis (the upper layer of the skin) and have not invaded into deeper layers.
Bowen disease appears as reddish patches. Compared with solar keratosis, Bowen disease patches tend to be larger (sometimes over ½ inch across), redder, scalier, and sometimes crusted. Like solar keratosis, Bowen disease usually doesn’t cause symptoms, although it might be itchy or sore.
Like most other skin cancers (and solar keratosis), these patches most often appear in sun-exposed areas. Bowen disease can also occur in the skin of the anal and genital areas (where it is known as erythroplasia of Queyrat or Bowenoid papulosis). This is often related to sexually transmitted infection with human papilloma viruses (HPVs), the viruses that can also cause genital warts.
Bowen disease can sometimes progress to an invasive squamous cell skin cancer, so doctors usually recommend treating it. People who have these are also at higher risk for other skin cancers, so close follow-up with a doctor is important.
Benign skin tumors
Many types of benign (non-cancerous) tumors can develop from different types of skin cells.
Benign tumors that start in melanocytes
A mole (nevus) is a benign skin tumor that develops from melanocytes. Almost everyone has some moles. Nearly all moles (nevi) are harmless, but having some types can raise your risk of melanoma.
A Spitz nevus is a kind of mole that sometimes looks like melanoma. It’s more common in children and teens, but it can also be seen in adults. These tumors are generally benign and don’t spread. But sometimes doctors have trouble telling Spitz nevi from true melanomas, even when looking at them under a microscope. Therefore, they are often removed, just to be safe.
Benign tumors that develop from other types of skin cells
- Seborrheic keratoses: tan, brown, or black raised spots with a “waxy” texture
- Hemangiomas: benign blood vessel growths, often called strawberry spots
- Lipomas: soft growths made up of fat cells
- Warts: rough-surfaced growths caused by some types of human papilloma virus (HPV)
Most of these tumors rarely, if ever, turn into cancers. There are many other kinds of benign skin tumors, but most are not very common.
- Skin Cancer. Medline Plus. https://medlineplus.gov/skincancer.html[↩]
- Basal and Squamous Cell Skin Cancer. American Cancer Society. https://www.cancer.org/cancer/basal-and-squamous-cell-skin-cancer.html[↩]
- What Is Melanoma Skin Cancer ? American Cancer Society. https://www.cancer.org/cancer/melanoma-skin-cancer/about/what-is-melanoma.html[↩]
- Key Statistics for Melanoma Skin Cancer. American Cancer Society. https://www.cancer.org/cancer/melanoma-skin-cancer/about/key-statistics.html[↩]
- Rigel DS, Russak J, Friedman R. The evolution of melanoma diagnosis: 25 years beyond the ABCDs. CA: A Cancer Journal for Clinicians 2010; 60(5):301–316. https://onlinelibrary.wiley.com/doi/pdf/10.3322/caac.20074[↩]





{kind=link}