Contents
What is spermatocele
A spermatocele, also known as a spermatic cyst, is a typically painless, noncancerous (benign), fluid-filled and dead sperm cells sac that forms within the epididymis near the top of a testicle. They typically don’t reduce fertility or require treatment.
A spermatocele can be left untreated unless it is growing too large or causing the individual discomfort. If a spermatocele grows large enough to cause discomfort, your doctor might suggest surgery.
Spermatoceles occur more commonly in the epididymis, but they are also sometimes seen within the testis, and particularly within the subcapsular rete testis. Spermatoceles are distinguished from sperm granuloma by the absence of an inflammatory response.
Spermatoceles can occur in association with reduced fluid absorption in the efferent ducts leading to sperm impaction and obstruction within the rete testis and adjacent seminiferous tubules. This can be a chemically induced finding, but in general spermatoceles the exact cause of spermatoceles is unknown and are incidental, age-related findings. An association between age-related germ cell degeneration and spermatocele formation has been described.
Because a spermatocele usually doesn’t cause symptoms, you might discover it only during a testicular self-exam, or your doctor might find it during a routine physical exam.
It’s a good idea to have your doctor evaluate any scrotal mass to rule out a serious condition, such as testicular cancer. Also, be sure to call your doctor if you experience pain or swelling in your scrotum. A number of conditions can cause testicular pain, and some require immediate treatment.
Spermatocele complications
A spermatocele is unlikely to cause complications.
However, if your spermatocele is painful or has grown so large that it’s causing you discomfort, you might need to have surgery to remove the spermatocele. Surgical removal might damage the epididymis or the vas deferens, a tube that transports sperm from the epididymis to the penis. Damage to either can reduce fertility. Another possible complication that can occur after surgery is that the spermatocele might come back, though this is uncommon.
Figure 1. Spermatocele cyst
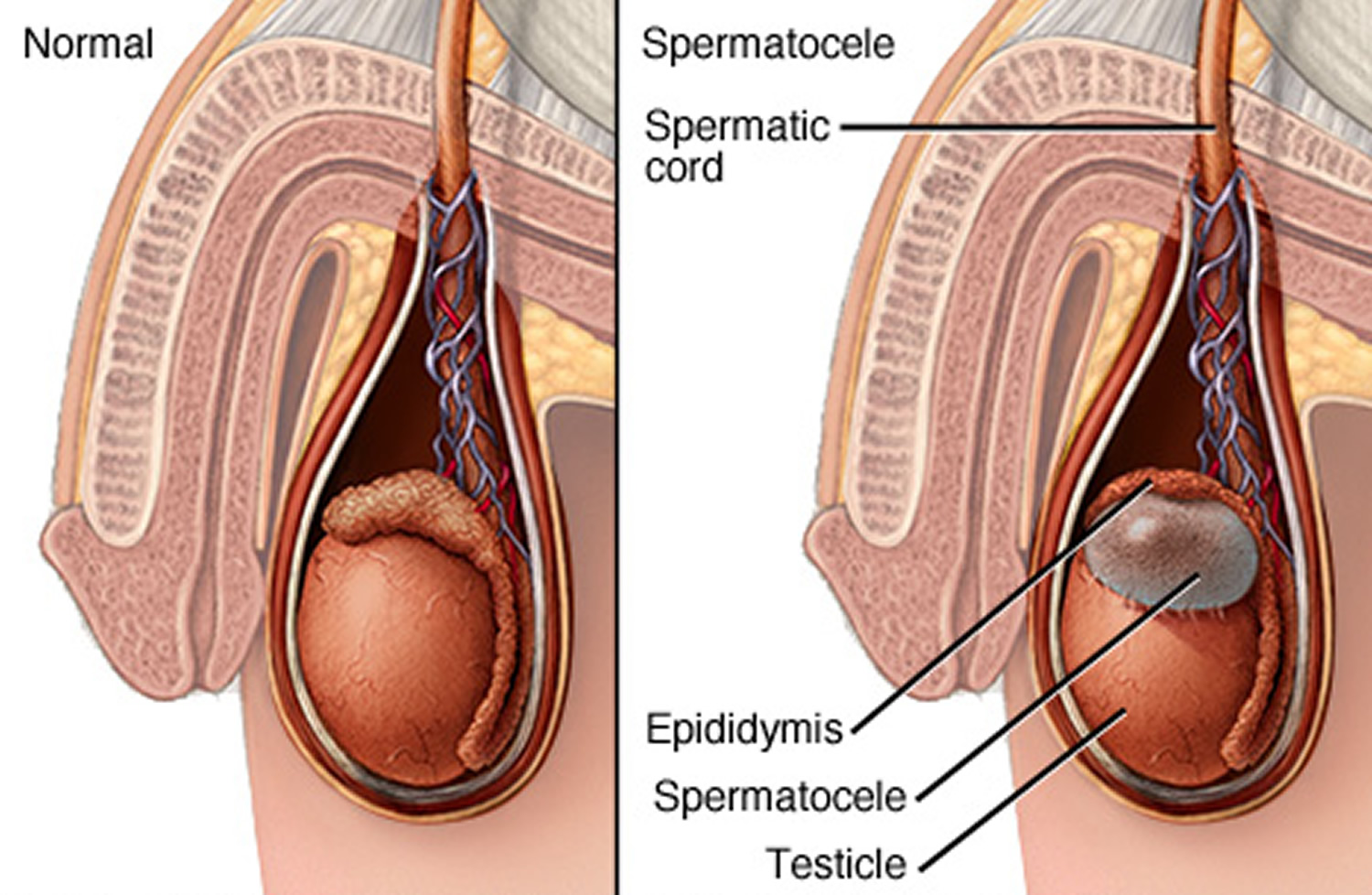
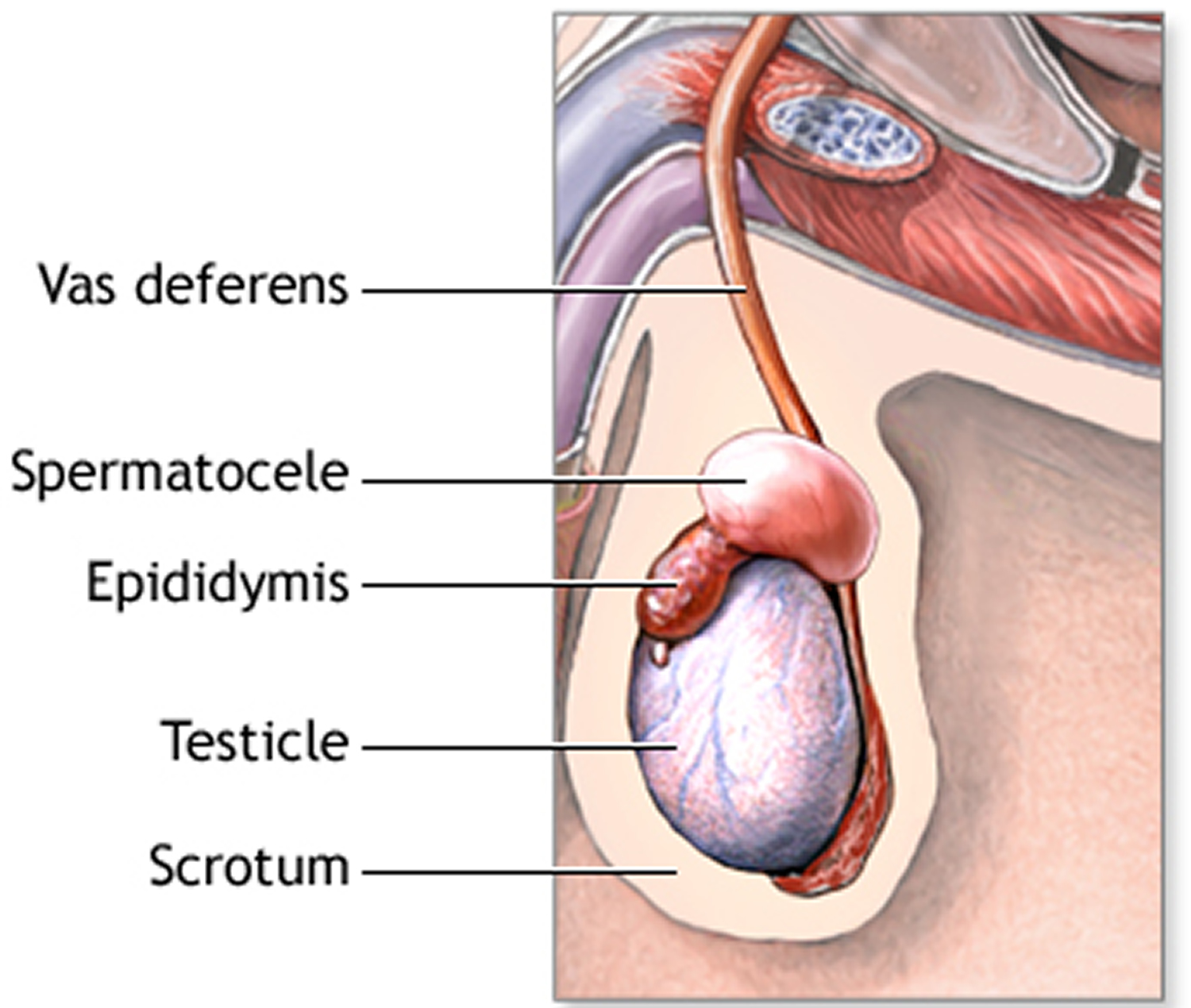
Figure 3. Testis (normal)
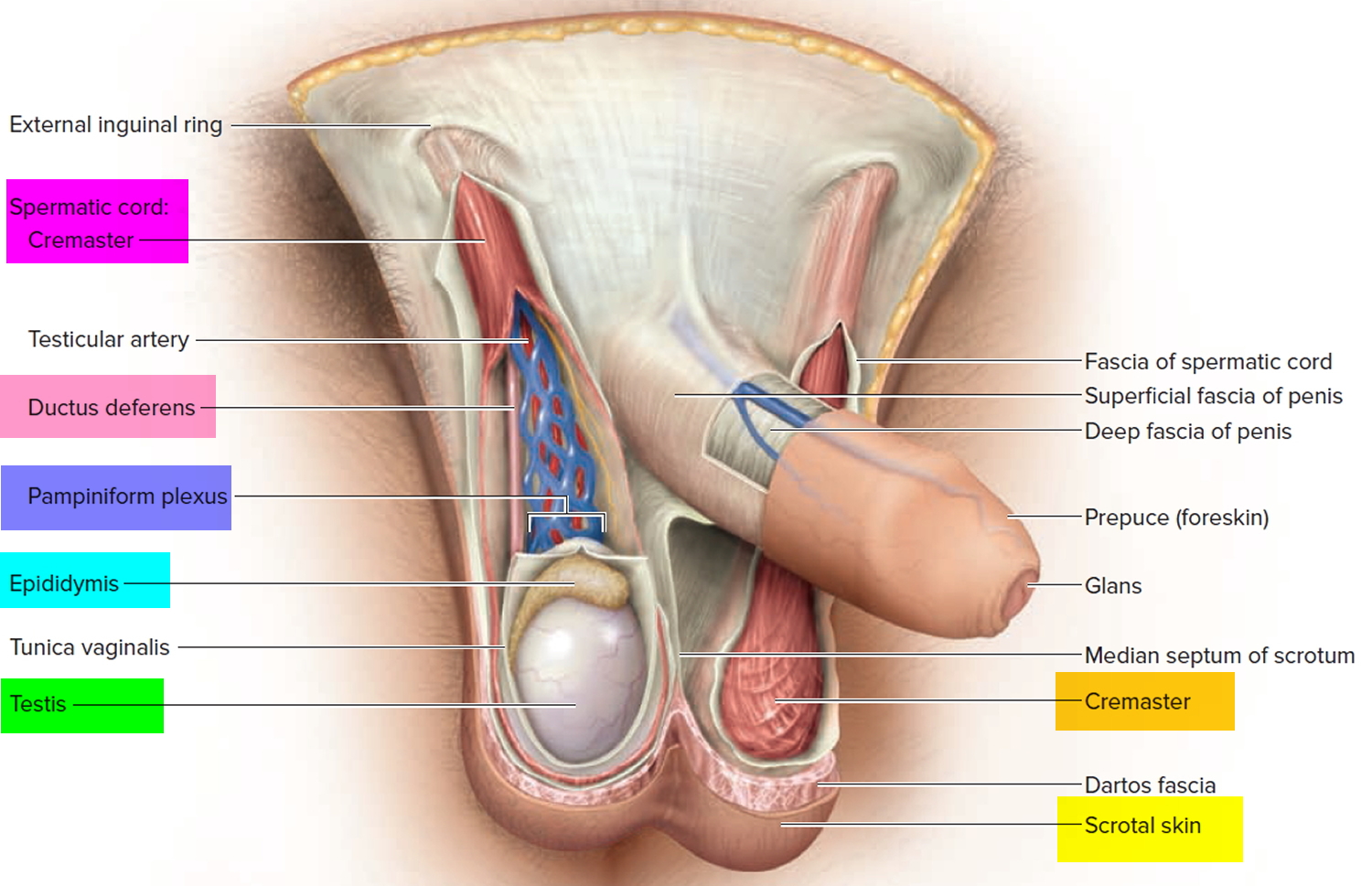 Figure 2. Testicle anatomy (normal)
Figure 2. Testicle anatomy (normal)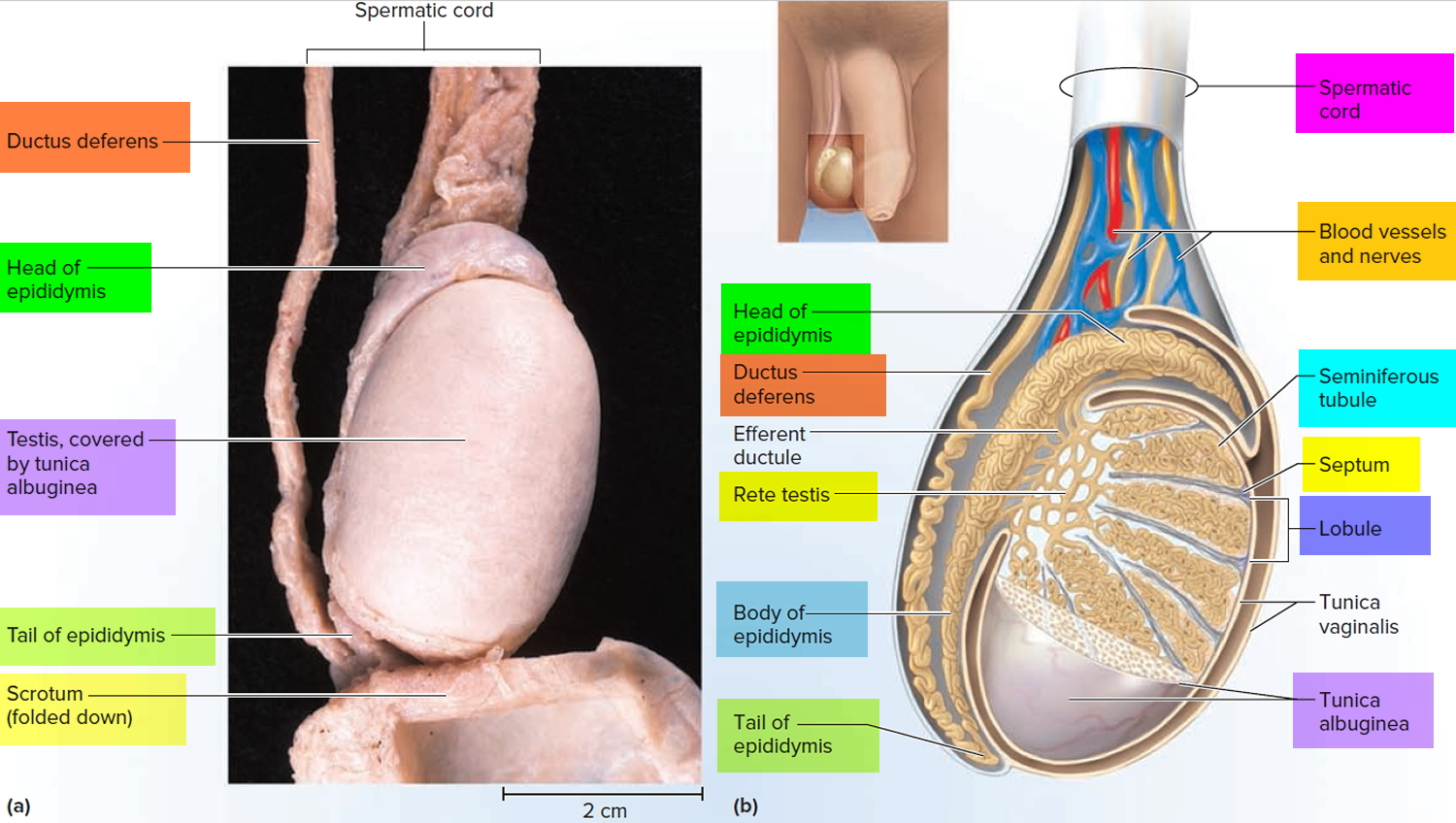
Spermatocele causes
The cause of spermatoceles is unknown. Spermatoceles might result from a blockage in one of the multiple tubes within the epididymis that transport and store sperm from the testicle. Trauma and inflammation also might play a role in causing the blockage.
Risk factors for spermatocele
There aren’t many known risk factors for developing a spermatocele, except for increasing age. Spermatoceles are most often found in men between the ages of 20 and 50.
Spermatocele prevention
Although there’s no way to prevent a spermatocele, it’s important for you to conduct scrotal self-exams at least monthly to detect changes, such as masses, in your scrotum. Any new mass in your scrotum should be evaluated promptly.
Your doctor can instruct you in how to conduct a testicular self-examination, which can improve your chances of finding a mass.
How to examine your testicles
A good time to examine your testicles is during or after a warm bath or shower. The heat from the water relaxes your scrotum, making it easier for you to detect anything unusual.
By regularly performing this exam, you’ll become more familiar with your testicles and aware of any changes that might be of concern. If you find a lump, call your doctor as soon as possible.
Regular self-examination is an important health habit. But it can’t substitute for a doctor’s examination. Your doctor normally checks your testicles whenever you have a physical exam.
Most health care providers agree that checking a man’s testicles should be part of a routine physical exam. And some doctors recommend that all men examine their testicles monthly after puberty.
How to do a testicular self-exam
The best time to do the self-exam is during or after a bath or shower, when the skin of the scrotum is relaxed.
- Hold your penis out of the way and check one testicle at a time.
- Hold the testicle between your thumbs and fingers of both hands and roll it gently between your fingers.
- Look and feel for any hard lumps or smooth rounded bumps or any change in the size, shape, or consistency of the testicles.
It’s normal for one testicle to be slightly larger than the other, and for one to hang lower than the other. You should also know that each normal testicle has a small, coiled tube (epididymis) that can feel like a small bump on the upper or middle outer side of the testicle. Normal testicles also have blood vessels, supporting tissues, and tubes that carry sperm. Some men may confuse these with abnormal lumps at first. If you have any concerns, ask your health care provider.
If you check your testicles regularly, in time you will learn what’s normal for you and will be able to tell when something is different.
What if you find something different?
If you find something unusual or something you’re not sure about, either during a self-exam or at any other time, see a health care provider right away.
The provider will ask if you’re having any symptoms (such as pain) and how long you’ve had them. During a physical exam, the provider will feel your testicles for swelling or tenderness and for the size and location of any lumps. The provider might also examine your abdomen (belly), groin area, and other parts of your body, looking for any possible signs of cancer spread.
If anything abnormal is found, an ultrasound may be done to look at the scrotum and testicles. This is an easy and painless way of finding out whether there’s a tumor or another problem. Other tests might be done as well.
Spermatocele signs and symptoms
A spermatocele usually causes no signs or symptoms and might remain stable in size. If it becomes large enough, however, you might feel:
- Pain or discomfort in the affected testicle
- A feeling of heaviness in the testicle with the spermatocele
- A mass, or fullness, behind and above the testicle
Spermatocele diagnosis
To diagnose a spermatocele, you’ll need a physical exam. Although a spermatocele generally isn’t painful, you might feel discomfort when your doctor examines (palpates) the mass.
You might also undergo the following diagnostic tests:
- Transillumination. Your doctor might shine a light through your scrotum. With a spermatocele, the light will indicate that the mass is fluid-filled rather than solid.
- Spermatocele ultrasound. If transillumination doesn’t clearly indicate a cyst, an ultrasound can help determine what else it might be. This test, which uses high-frequency sound waves to create images of structures, might be used to rule out a testicular tumor or other cause of scrotal swelling.
Spermatocele treatment
Although your spermatocele probably won’t go away on its own, most spermatoceles don’t need treatment. They generally don’t cause pain or complications. If yours is painful, your doctor might recommend over-the-counter pain medications, such as acetaminophen (Tylenol, others) or ibuprofen (Advil, Motrin IB, others).
Spermatocele surgery
A procedure called a spermatocelectomy generally is performed on an outpatient basis, using a local or general anesthetic. The surgeon makes an incision in the scrotum and separates the spermatocele from the epididymis.
After surgery, you might need to wear a gauze-filled athletic supporter to apply pressure to and protect the site of the incision. Your doctor might also tell you to:
- Apply ice packs for two or three days to keep swelling down
- Take oral pain medications for a day or two
- Return for a follow-up exam about two weeks after surgery
Possible complications from surgical removal that might affect fertility include damage to the epididymis or to the tube that transports sperm (vas deferens). It’s also possible that a spermatocele might come back, even after surgery.
Aspiration, with or without sclerotherapy
Another treatment that’s not used as often is aspiration, sometimes with sclerotherapy. During aspiration, a special needle is inserted into the spermatocele, and fluid is removed (aspirated). If the spermatocele recurs, your doctor might recommend aspirating the fluid again, and then injecting an irritating chemical into the sac. The irritating agent causes the spermatocele sac to scar, which takes up the space the fluid occupied and lowers the risk of the spermatocele coming back.
Damage to the epididymis is a possible complication of sclerotherapy. It’s also possible that your spermatocele might come back. Sclerotherapy usually is used only for men who are beyond their reproductive years.





{kind=link}