
Contents
What is a stress fracture
Stress fractures are tiny cracks or incomplete break in a bone 1. Stress fractures are common injuries that begin with repetitive and excessive stress on the bone, often from overuse — such as repeatedly jumping up and down or running long distances. Stress fractures tend to occur when you start a new exercise regimen or get back to an old one after taking time off. This leads to the acceleration of normal bone remodeling, the production of microfractures (caused by insufficient time for the bone to repair), the creation of a bone stress injury (i.e., stress reaction), and eventually, a stress fracture 2. In contrast, pathological (insufficiency) fractures occur under normal stress in bone weakened by a tumor, infection, or osteoporosis 3.
Many factors such as the frequency and duration of activity, faulty foot structure, poor footwear and type of surface can contribute to the development of a stress fracture.
Stress fractures are most common in the weight-bearing bones of the lower leg and foot. Track and field athletes and military recruits who carry heavy packs over long distances are particularly susceptible, but anyone can have a stress fracture. If you start a new exercise program, for example, you might develop stress fractures if you do too much too soon.
Recreational runners who average more than 25 miles per week are at increased risk of stress fractures 4, as well as athletes who participate in track and field, basketball, soccer, or dance 5. Women are at higher risk of stress fracture than men 6, especially women in the military 3, although there are conflicting data among female athletes 7.
The most common locations for stress fractures are 7, 6:
- Tibia (23.6 percent),
- Tarsal navicular (17.6 percent),
- Metatarsal (16.2 percent),
- Fibula (15.5 percent),
- Femur (6.6 percent),
- Pelvis (1.6 percent), and
- Spine (0.6 percent).
- Although less common, upper extremity stress fractures can occur in persons who participate in sports involving throwing or other overhead motions 5.
Persons who participate in repetitive, high-intensity training, such as athletes and military recruits, are at increased risk of developing stress fractures.3–6
Pain, bruising and redness can all present when this occurs, and rest, ice, compression and elevation (RICE) protocol should be started followed by a visit to your local foot and ankle surgeon.
Stress fracture symptoms
At first, you might barely notice the pain associated with a stress fracture, but it tends to worsen with time. The tenderness usually originates from a specific spot and decreases during rest. You might have swelling around the painful area.
When to see a doctor
Contact your doctor if your pain becomes severe or persists even at rest.
Causes of stress fracture
Stress fractures often result from increasing the amount or intensity of an activity too quickly.
Bone adapts gradually to increased loads through remodeling, a normal process that speeds up when the load on the bone increases. During remodeling, bone tissue is destroyed (resorption), then rebuilt.
Bones subjected to unaccustomed force without enough time for recovery resorb cells faster than your body can replace them, which makes you more susceptible to stress fractures.
Risk factors for stress fracture
Factors that can increase your risk of stress fractures include:
- Certain sports. Stress fractures are more common in people who participate in sports such as track and field, basketball, tennis, dance or gymnastics.
- Sudden increase in physical activity. Stress fractures often occur in people who suddenly shift from a sedentary lifestyle to an active training regimen or who rapidly increase the intensity, duration or frequency of training sessions.
- Excessive physical activity with limited rest periods.
- Sex. Women, especially those who have abnormal or absent menstrual periods, are at higher risk of developing stress fractures.
- Female athlete triad (eating disorders, amenorrhea, osteoporosis)
- Foot problems. People who have flat feet or high, rigid arches are more likely to develop stress fractures. Worn footwear contributes to the problem.
- Weakened bones. Conditions such as osteoporosis can weaken your bones and make it easier for stress fractures to occur.
- Previous stress fractures. Having had one or more stress fractures puts you at higher risk of having more.
- Lack of nutrients. Eating disorders and lack of vitamin D (low levels of 25-hydroxy vitamin D) and calcium can make bones more likely to develop stress fractures.
- Consuming more than 10 alcoholic drinks per week.
- Recreational running (more than 25 miles per week).
- Smoking.
Poor nutrition and lifestyle habits may increase the risk of stress fracture. One study found lower 25-hydroxyvitamin D levels in Finnish male military recruits with stress fractures 8. Women with the female athlete triad (i.e., eating disorders, functional hypothalamic amenorrhea, and osteoporosis) are at higher risk of stress fracture 9. A study of female military recruits demonstrated an increased risk of stress fracture with a history of smoking, exercising less than three times per week, and consuming more than 10 alcoholic drinks per week before the start of basic training 10. Additionally, 16.2 percent of white recruits who smoked and did not exercise developed a stress fracture 10.
Complications of Stress fractures
Certain stress fractures may lead to complications, including progression to complete fractures, development of avascular necrosis, or delays in healing or nonunion. Examples of these high-risk stress fractures include the superolateral femoral neck, patella, anterior tibia, medial malleolus, talus, tarsal navicular, and the fifth metatarsal 11. High-risk stress fractures may warrant consultation with an orthopedist or sports medicine subspecialist.
In special circumstances, such as in competitive athletes during their sport’s season, patients may choose to modify their activity to a decreased level of intensity (tolerable without exacerbation), and delay complete rest until the season is finished 11. In these situations, athletes should be aware of the potential for prolonged recovery or the need for additional interventions, including surgery.
Prevention of stress fractures
Simple steps can help you prevent stress fractures.
- Make changes slowly. Start any new exercise program slowly and progress gradually.
- Use proper footwear. Make sure your shoes fit well and are appropriate for your activity. If you have flat feet, ask your doctor about arch supports for your shoes.
- Address abnormal biomechanics if needed, and consider shock-absorbing shoe inserts 12
- Cross-train. Add low-impact activities to your exercise regimen to avoid repetitively stressing a particular part of your body.
- Get proper nutrition. To keep your bones strong, make sure your diet includes adequate calcium, vitamin D and other nutrients.
- Consider daily supplementation of calcium (2,000 mg) and vitamin D (800 IU) 13
- Modify activity level or training patterns, and ensure adequate rest 12
Diagnosis of stress fractures
Stress fracture should be suspected in persons with a drastic recent increase in physical activity or repeated excessive activity with limited rest. Pain is a common presenting symptom that can vary by location, such as knee pain with a proximal tibial injury, hip pain with a femoral neck injury, or groin pain with a pelvic fracture. Specifically, pain with ambulation is common (81 percent) 14. On examination, patients usually demonstrate focal tenderness (65.9 to 100 percent) and edema (18 to 44 percent) at the site of injury 15.
Although the hop test (i.e., single leg hopping that produces severe localized pain) is often used and cited in texts as a diagnostic test for lower extremity fractures, no recent literature was found to validate its accuracy. In some studies, a positive hop test was an inclusion criterion 6 or a common finding (70 to 100 percent) 16 in patients with presumed stress fractures, but was also noted in nearly one-half (45.6 percent) of patients with suspected medial tibial stress syndrome (shin splints) 17. Another diagnostic measure used often, but with little supporting evidence, is the tuning fork test (i.e., applying a tuning fork to the fracture site to produce focal pain). One small study found that the tuning fork test had a sensitivity of 75 percent, a specificity of 67 percent, a positive predictive value of 77 percent, and a negative predictive value of 63 percent for tibial stress fractures 18.
Diagnosing stress fractures can be challenging and warrants consideration of the differential diagnosis, based on location (Table 1). The differential diagnosis may include tendinopathy, compartment syndrome, and nerve or artery entrapment syndrome. Medial tibial stress syndrome is a common condition that can be distinguished from tibial stress fractures by nonfocal tenderness (diffuse along the mid-distal, posteromedial tibia) and a lack of edema 17. The differential diagnosis may also include a variety of malignancies, such as osteosarcoma and Ewing sarcoma 2.
Table 1. Risk Factors, Signs and Symptoms, and Differential Diagnosis of Common Stress Fractures
Fracture type | Risk factors | Signs and symptoms | Differential diagnosis |
| Tibial | Running, walking, jumping, dancing, female athlete triad | Shin pain, focal tenderness over anterior aspect of tibia, edema | Medial tibial stress syndrome (shin splints) |
| Comments: Shin splints may cause pain along the posteromedial border of the distal tibia; no abnormalities will appear on radiography | |||
| ———————————————– | |||
Fracture type | Risk factors | Signs and symptoms | Differential diagnosis |
| Metatarsal | Running, walking, dancing, marching | Foot or ankle pain, focal tenderness, swelling | Plantar fasciitis, metatarsalgia, Morton neuroma |
| Comments: Plantar fasciitis may cause pain or tenderness along the fascia; Metatarsalgia may cause tenderness on metatarsal heads ; Morton neuroma may cause pain (with compression) between the third and fourth metatarsals | |||
| ———————————————– | |||
Fracture type | Risk factors | Signs and symptoms | Differential diagnosis |
| Femoral or sacral | Running, walking, female athlete triad, cycling | Groin pain, pain with activity, pain with passive hip range of movement | Pathologic fracture, rectus femoris strain |
| Comments: Urgent imaging is needed to identify underlying pathology | |||
| ———————————————– | |||
Fracture type | Risk factors | Signs and symptoms | Differential diagnosis |
| Spondylolysis | Soccer, gymnastics, volleyball, dancing, football, weightlifting | Tenderness, extension-related pain during “stork” test (single-leg hyperextension/rotation) | Lumbar sprain, pathologic fracture |
| Comments: Most commonly associated with L4 and L5 vertebrae; confirm diagnosis with scintigraphy with single-photon emission computed tomography. | |||
Doctors can sometimes diagnose a stress fracture from a medical history and a physical exam, but imaging tests are often needed.
- X-rays. Stress fractures often aren’t apparent on regular X-rays taken shortly after your pain begins. It can take several weeks — and sometimes longer than a month — for evidence of stress fractures to show on X-rays.
- Bone scan. A few hours before a bone scan, you’ll receive a small dose of radioactive material through an intravenous line. The radioactive substance accumulates most in areas where bones are being repaired — showing up on the scan image as a bright white spot. However, many types of bone problems look alike on bone scans, so the test isn’t specific for stress fractures.
- Magnetic resonance imaging (MRI). An MRI uses radio waves and a strong magnetic field to produce detailed images of your internal structures. An MRI usually can visualize stress fractures within the first week of injury, and can visualize lower-grade stress injuries (stress reactions) before an x-ray shows changes. This type of test is also better able to distinguish between stress fractures and soft tissue injuries.
Despite limitations of cost and availability, MRI has replaced bone scan as the confirmation test used in most studies 20. MRI is extremely sensitive and demonstrates stress abnormalities as early as bone scintigraphy and with as much sensitivity. The recent literature favors MRI as the procedure of choice for making an early diagnosis of both varieties of stress fractures. In this regard, MRI outperforms radiography, bone scintigraphy, and computed tomography (CT). Fluid-sensitive sequences are the favored initial sequence for MRI screening. With a small field of view, short tau inversion recovery and/or T1-weighted imaging will usually demonstrate a fracture line surrounded by edema. In the absence of an actual stress fracture, stress reaction or muscle/tendon injuries can be identified using fluid-sensitive sequences. Thus, MRI may be as sensitive as bone scintigraphy but also considerably more specific. Intravenous contrast is not needed for diagnosis and has yet to provide any additional information. MRI examination of an osseous stress injury contains prognostic as well as diagnostic information. For this reason, an expert panel of the American College of Radiology says that MRI may be considered next when plain radiography is negative 21. Because MRI provides greater detail of surrounding tissue (see Figure 3), it may be advantageous for evaluating the differential diagnosis. One prospective study compared MRI, CT, and bone scintigraphy for evaluation of early tibial bone stress injuries based on the premise that early detection could prevent stress fractures 20. MRI was superior for detection of early stress injury, although both MRI and bone scintigraphy identified the actual stress fractures. However, MRI may also identify reactive bone remodeling (interpreted as early stress injuries) and, therefore, should be clinically correlated for stress fracture 22. In a study of asymptomatic collegiate runners, 43 percent were found to have stress injury on MRI 22. None of the stress injuries progressed to stress fractures, and all were resolved at the one-year followup 22. Another study of shin splints demonstrated similar bone stress changes on MRI, including 80 percent of asymptomatic control patients 17.
Figure 1. Distal fibular stress fracture

Figure 2. Bone scan (bone scintigram) of the same patient with distal fibular stress fracture
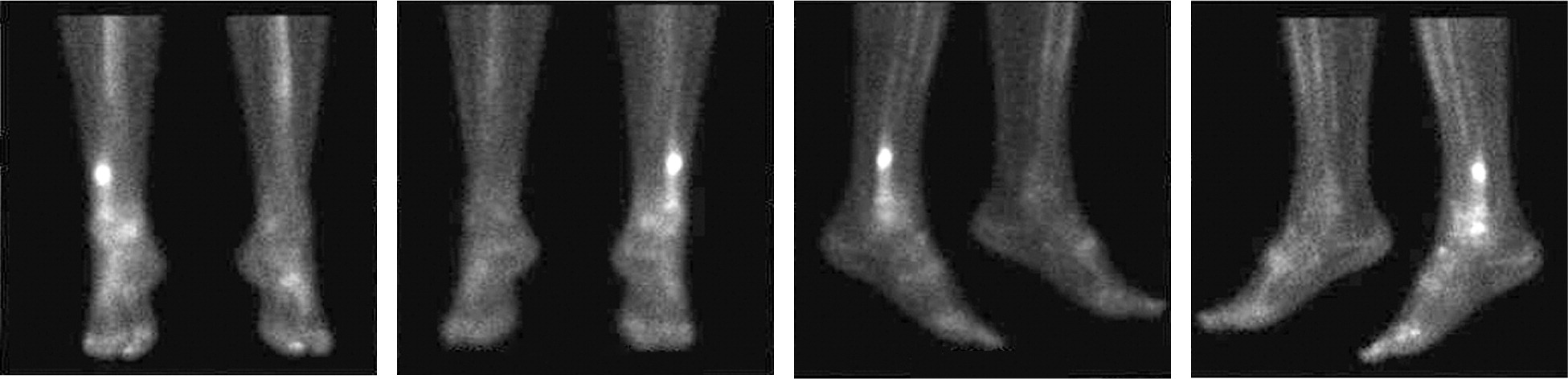
Figure 3. Stress fracture shin MRI imaging
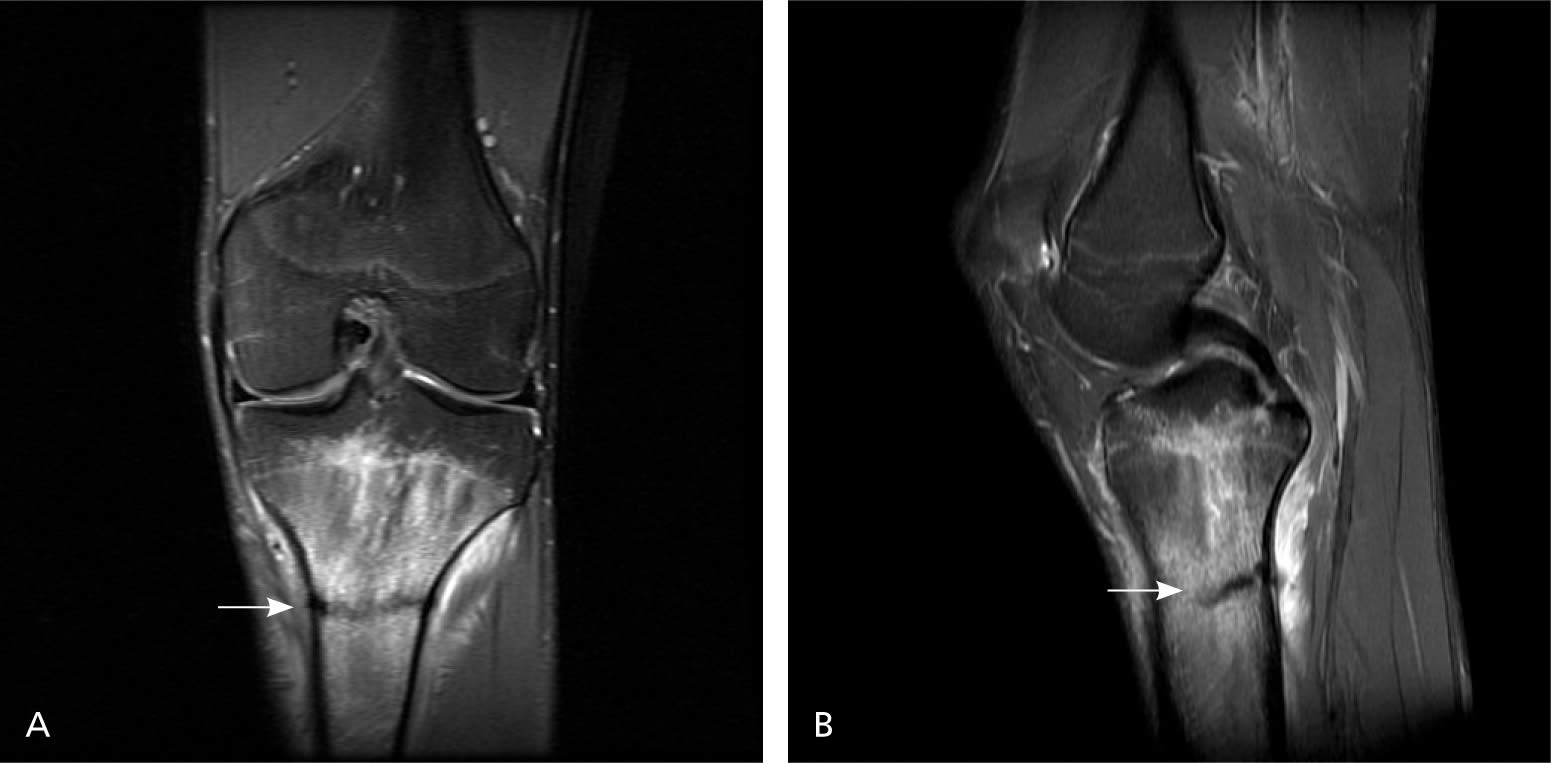
Note: Magnetic resonance imaging. (A) Proximal tibial stress fracture (arrow). (B) Sagittal view of same fracture (arrow).
Treatment of stress fractures
Depending on the injury, healing time for stress fractures can vary from four to 12 weeks or longer from the time activity is restricted 6, 5. Initial treatment should include reducing activity to the level of pain-free functioning. Treatment should begin as soon as the injury is suspected, because delayed treatment has been correlated with prolonged return to activity 5. Table 4 summarizes general preventive measures and treatment options for stress fractures 12.
To reduce the bone’s weight-bearing load until healing occurs, you might need to wear a walking boot or brace or full nonweight-bearing crutches to reduce pain. A Cochrane review pooling data from three small studies suggested that patients with tibial stress fracture who used a pneumatic brace (e.g., a stirrup leg brace) showed a significant reduction in time to recommencing full activity; however, more evidence is needed for confirmation 12. Pneumatic compression walking boots may be used to reduce pain from lower extremity stress fractures. Physical therapy and cross training with non-aggravating activities may help maintain flexibility and strength, and cardiovascular fitness, respectively, during the rest period 6.
Bone stimulation via electrical or ultrasonic impulses has been an area of growing interest, but evidence is currently lacking. A single randomized controlled trial of 26 patients demonstrated no effect from low-intensity ultrasonic impulses in reducing healing time 23. Similarly, a single randomized controlled trial of 50 patients found no benefit from electrical field stimulation in tibial stress fracture clinical healing 24. However, there is some evidence for the use of stimulation in nonhealing traumatic fractures, and it may also be considered for recalcitrant stress fractures 25.
Although unusual, surgery is sometimes necessary to ensure complete healing of some types of stress fractures, especially those that occur in areas with a poor blood supply. Surgery also might be an option to facilitate healing for elite athletes who desire a more rapid return to sport or laborers whose work involves the stress fracture site.
Home remedies for stress fracture
It’s important to give the bone time to heal. This may take several months or even longer. In the meantime:
- Rest. Stay off the affected limb as directed by your doctor until you are cleared to bear normal weight.
- Ice. To reduce swelling and relieve pain, your doctor might recommend applying ice packs to the injured area as needed — up to three or four times a day for 15 minutes at a time.
- Analgesics, such as acetaminophen and nonsteroidal anti-inflammatory drugs, may be considered for pain control. However, antiinflammatories should be used with caution, because some animal studies have shown that they may inhibit healing in subjects with traumatic fractures 26.
- Resume activity slowly. When your doctor gives the OK, slowly progress from nonweight-bearing activities — such as swimming — to your usual activities.
- Cross training to maintain cardiovascular fitness.
- Resume high-impact activities, such as running, gradually, increasing time and distance slowly.
- Foot Health Facts for Athletes. https://www.foothealthfacts.org/article/foot-health-facts-for-athletes[↩]
- Fayad LM, Kamel IR, Kawamoto S, Bluemke DA, Frassica FJ, Fishman EK. Distinguishing stress fractures from pathologic fractures: a multimodality approach. Skeletal Radiol. 2005;34(5):245–259.[↩][↩]
- Niva MH, Mattila VM, Kiuru MJ, Pihlajamäki HK. Bone stress injuries are common in female military trainees: a preliminary study. Clin Orthop Relat Res. 2009;467(11):2962–2969.[↩][↩]
- Clement DB, Ammann W, Taunton JE, et al. Exercise-induced stress injuries to the femur. Int J Sports Med. 1993;14(6):347–352.[↩]
- Ohta-Fukushima M, Mutoh Y, Takasugi S, Iwata H, Ishii S. Characteristics of stress fractures in young athletes under 20 years. J Sports Med Phys Fitness. 2002;42(2):198–206.[↩][↩][↩][↩]
- Matheson GO, Clement DB, McKenzie DC, Taunton JE, Lloyd-Smith DR, MacIntyre JG. Stress fractures in athletes. A study of 320 cases. Am J Sports Med. 1987;15(1):46–58.[↩][↩][↩][↩][↩]
- Brukner P, Bradshaw C, Khan KM, White S, Crossley K. Stress fractures: a review of 180 cases. Clin J Sport Med. 1996;6(2):85–89.[↩][↩]
- Ruohola JP, Laaksi I, Ylikomi T, et al. Association between serum 25(OH)D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res. 2006;21(9):1483–1488.[↩]
- Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867–1882.[↩]
- Lappe J, Davies K, Recker R, Heaney R. Quantitative ultrasound: use in screening for susceptibility to stress fractures in female army recruits. J Bone Miner Res. 2005;20(4):571–578.[↩][↩]
- Kaeding CC, Yu JR, Wright R, Amendola A, Spindler KP. Management and return to play of stress fractures. Clin J Sport Med. 2005;15(6):442–447.[↩][↩]
- Rome K, Handoll HH, Ashford R. Interventions for preventing and treating stress fractures and stress reactions of bone of the lower limbs in young adults. Cochrane Database Syst Rev. 2005;(2):CD000450.[↩][↩][↩][↩]
- Lappe J, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin D supplementation decreases incidence of stress fractures in female navy recruits. J Bone Miner Res. 2008;23(5):741–749.[↩]
- Fredericson M, Bergman AG, Hoffman KL, Dillingham MS. Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med. 1995;23(4):472–481.[↩]
- Ishibashi Y, Okamura Y, Otsuka H, Nishizawa K, Sasaki T, Toh S. Comparison of scintigraphy and magnetic resonance imaging for stress injuries of bone. Clin J Sport Med. 2002;12(2):79–84.[↩]
- Ishibashi Y, Okamura Y, Otsuka H, Nishizawa K, Sasaki T, Toh S. Comparison of scintigraphy and magnetic resonance imaging for stress injuries of bone. Clin J Sport Med. 2002;12(2):79–84[↩]
- Batt ME, Ugalde V, Anderson MW, Shelton DK. A prospective controlled study of diagnostic imaging for acute shin splints. Med Sci Sports Exerc. 1998;30(11):1564–1571.[↩][↩][↩]
- Lesho EP. Can tuning forks replace bone scans for identification of tibial stress fractures? Mil Med. 1997;162(12):802–803.[↩]
- Stress Fractures: Diagnosis, Treatment, and Prevention. Am Fam Physician. 2011 Jan 1;83(1):39-46. http://www.aafp.org/afp/2011/0101/p39.html[↩]
- Gaeta M, Minutoli F, Scribano E, et al. CT and MR imaging findings in athletes with early tibial stress injuries: comparison with bone scintigraphy findings and emphasis on cortical abnormalities. Radiology. 2005;235(2):553–561.[↩][↩]
- Daffner RH, Weissman BN, Bennett DL, et al., Expert Panel on Musculoskeletal Imaging. ACR Appropriateness Criteria stress/insufficiency fracture, including sacrum, excluding other vertebrae. Reston, Va.: American College of Radiology; 2008. https://www.guideline.gov/summaries/summary/50498[↩]
- Bergman AG, Fredericson M, Ho C, Matheson GO. Asymptomatic tibial stress reactions: MRI detection and clinical follow-up in distance runners. AJR Am J Roentgenol. 2004;183(3):635–638.[↩][↩][↩]
- Rue JP, Armstrong DW III, Frassica FJ, Deafenbaugh M, Wilckens JH. The effect of pulsed ultrasound in the treatment of tibial stress fractures. Orthopedics. 2004;27(11):1192–1195.[↩]
- Beck BR, Matheson GO, Bergman G, et al. Do capacitively coupled electric fields accelerate tibial stress fracture healing? A randomized controlled trial. Am J Sports Med. 2008;36(3):545–553.[↩]
- Mollon B, da Silva V, Busse JW, Einhorn TA, Bhandari M. Electrical stimulation for long-bone fracture-healing: a meta-analysis of randomized controlled trials. J Bone Joint Surg Am. 2008;90(11):2322–2330[↩]
- Wheeler P, Batt ME. Do non-steroidal anti-inflammatory drugs adversely affect stress fracture healing? A short review. Br J Sports Med. 2005;39(2):65–69.[↩]





{kind=link}