
Contents
What is stuttering
Stuttering is a speech disorder characterized by disruptions in the production of speech sounds with repetition of sounds, syllables, or words; prolongation of sounds; and interruptions in speech known as blocks. These problems cause a break in the flow of speech (called disfluency). An individual who stutters exactly knows what he or she would like to say but has trouble producing a normal flow of speech. Stuttering affects the fluency of speech. Stuttering is sometimes referred to as stammering and by a broader term, disfluent speech. These speech disruptions may be accompanied by struggle behaviors, such as rapid eye blinks or tremors of the lips. Stuttering can make it difficult to communicate with other people, which often affects a person’s quality of life and interpersonal relationships. Stuttering can also negatively influence job performance and opportunities, and treatment can come at a high financial cost.
While the root cause of stuttering is not fully known, brain functioning (neurology), genetics, and environmental factors all play a role. Because speaking and communication are highly complex and depend on interaction with others, many factors can make stuttering worse in some situations. Stuttering most often begins in children between the ages of 2 and 6 as they are developing their language skills and in some cases, lasts throughout life. Most people produce brief disfluent speech from time to time. For instance, some words are repeated and others are preceded by “um” or “uh.” Disfluencies are not necessarily a problem; however, they can impede communication when a person produces too many of them. Approximately 5 to 10 percent of all children will stutter for some period in their life, lasting from a few weeks to several years. Boys are 2 to 3 times as likely to stutter as girls and as they get older this gender difference increases; the number of boys who continue to stutter is three to four times larger than the number of girls. Most children outgrow stuttering. Approximately 75 percent of children recover from stuttering. For the remaining 25 percent who continue to stutter, stuttering can persist as a lifelong communication disorder.
- Many preschoolers who show early signs of stuttering will outgrow it. However, scientists cannot predict who will recover spontaneously. Speech therapy at an early age can increase the likelihood that the child will recover.
Because stuttering is a multi-dimensional disorder, it is often defined in three parts:
- Affective: The way you feels about stuttering, such as: feeling ashamed, embarrassed, anxious, etc.
- Behavioral: The observable characteristics, such as repetitions (c-c-car), prolongations (mmmine), blocks (—-book), physical struggle, avoidance behaviors, etc.
- Cognitive: The way you think about stuttering and yourself, such as: thinking people don’t like you, thinking you are stupid, thinking you are less of a person, etc.
While people who stutter may experience embarrassment, anxiety, stress, and fear regarding speaking, stuttering is NOT an emotional or psychological disorder.
Symptoms of stuttering can vary significantly throughout a person’s day. In most cases, stuttering has an impact on at least some daily activities. The specific activities that a person finds challenging to perform vary across individuals. For some people, communication difficulties only happen during specific activities, for example, talking on the telephone or talking before large groups, while singing, reading, or speaking in unison may temporarily reduce stuttering. For most others, however, communication difficulties occur across a number of activities at home, school, or work. Some people may limit their participation in certain activities. Such “participation restrictions” often occur because the person is concerned about how others might react to stuttering. Other people may try to hide their stuttering from others by rearranging the words in their sentence (circumlocution), pretending to forget what they wanted to say, or declining to speak. Other people may find that they are excluded from participating in certain activities because of stuttering. Clearly, the impact of stuttering on daily life can be affected by how the person and others react to the disorder.
Stuttering can lead to:
- Problems communicating with others
- Being anxious about speaking
- Not speaking or avoiding situations that require speaking
- Loss of social, school, or work participation and success
- Being bullied or teased
- Low self-esteem
There are no cures for stuttering. Speech therapy can help a person communicate effectively and make long-term changes over time.
Children and adults who stutter may benefit from treatments such as speech therapy, using electronic devices to improve speech fluency or cognitive behavioral therapy.
There is no 1 best treatment for stuttering. Most early cases are short-term and resolve on their own.
Speech therapy may be helpful if:
- Stuttering has lasted more than 3 to 6 months, or the “blocked” speech lasts several seconds
- The child appears to be struggling when stuttering, or is embarrassed
- There is a family history of stuttering
Speech therapy can help make the speech more fluent or smooth.
Parents are encouraged to:
- Avoid expressing too much concern about the stuttering, which can actually make matters worse by making the child more self-conscious.
- Avoid stressful social situations whenever possible.
- Listen patiently to the child, make eye contact, don’t interrupt, and show love and acceptance. Avoid finishing sentences for them.
- Set aside time for talking.
- Talk openly about stuttering when the child brings it up to you. Let them know you understand their frustration.
- Talk with the speech therapist about when to gently correct the stuttering.
Taking medicine has not been shown to be helpful for stuttering.
It is not clear whether electronic devices help with stuttering.
Self-help groups are often helpful for both the child and family.
I read about a new cure for stuttering. Is there such a thing?
There are no instant miracle cures for stuttering. Therapy, electronic devices, and even drugs are not an overnight process. However, a specialist in stuttering can help not only children but also teenagers, young adults and even older adults make significant progress toward fluency.
It’s common for children between the ages of 2 and 5 years to go through periods when they may stutter. For most children, this is part of learning to speak, and it gets better on its own. However, stuttering that persists may require treatment to improve speech fluency.
See your doctor for a referral or contact a speech-language pathologist directly for an appointment if stuttering:
- Lasts more than six months
- Occurs with other speech or language problems
- Becomes more frequent or continues as the child grows older
- Occurs with muscle tightening or visibly struggling to speak
- Affects the ability to effectively communicate at school, at work or in social interactions
- Causes anxiety or emotional problems, such as fear or avoidance of situations where speaking is required
- Begins as an adult
What are signs and symptoms of stuttering?
Stuttered speech often includes repetitions of words or parts of words, as well as prolongations of speech sounds. These disfluencies occur more often in persons who stutter than they do in the general population. Some people who stutter appear very tense or “out of breath” when talking. Speech may become completely stopped or blocked. Blocked is when the mouth is positioned to say a sound, sometimes for several seconds, with little or no sound forthcoming. After some effort, the person may complete the word. Interjections such as “um” or “like” can occur, as well, particularly when they contain repeated (“u- um- um”) or prolonged (“uuuum”) speech sounds or when they are used intentionally to delay the initiation of a word the speaker expects to “get stuck on.”
Symptoms of stuttering may include:
- Feeling frustrated when trying to communicate
- Pausing or hesitating when starting or during sentences, phrases, or words, often with the lips together
- Putting in (interjecting) extra sounds or words (“We went to the…uh…store”)
- Repeating sounds, words, parts of words, or phrases (“I want…I want my doll,” “I…I see you,” or “Ca-ca-ca-can”)
- Tension in the voice
- Very long sounds within words (“I am Booooobbbby Jones” or “Llllllllike”)
- Difficulty starting a word, phrase or sentence
- Prolonging a word or sounds within a word
- Repetition of a sound, syllable or word
- Brief silence for certain syllables or words, or pauses within a word (broken word)
- Addition of extra words such as “um” if difficulty moving to the next word is anticipated
- Excess tension, tightness, or movement of the face or upper body to produce a word
- Anxiety about talking
- Limited ability to effectively communicate
Other symptoms that might be seen with stuttering include:
- Eye blinking
- Jerking of the head or other body parts
- Jaw jerking
- Tremors of the lips or jaw
- Facial tics
- Clenching fists
Stuttering may be worse when the person is excited, tired or under stress, or when feeling self-conscious, hurried or pressured. Situations such as speaking in front of a group or talking on the phone can be particularly difficult for people who stutter.
However, most people who stutter can speak without stuttering when they talk to themselves and when they sing or speak in unison with someone else.
Some examples of stuttering include:
- “W- W- W- Where are you going?” (Part-word repetition: The person is having difficulty moving from the “w” in “where” to the remaining sounds in the word. On the fourth attempt, he successfully completes the word.)
- “SSSS ave me a seat.” (Sound prolongation: The person is having difficulty moving from the “s” in “save” to the remaining sounds in the word. He continues to say the “s” sound until he is able to complete the word.)
- “I’ll meet you – um um you know like – around six o’clock.” (A series of interjections: The person expects to have difficulty smoothly joining the word “you” with the word “around.” In response to the anticipated difficulty, he produces several interjections until he is able to say the word “around” smoothly.)
Children with mild stuttering are often unaware of their stuttering. In severe cases, children may be more aware. Facial movements, anxiety, and increased stuttering may occur when they are asked to speak.
When does stuttering typically start?
Usually, the symptoms of developmental stuttering first appear between the ages of 2½ and 4 years. Although less common, stuttering may start during elementary school. Stuttering is more common among males than females. Among elementary school-age children, it is estimated that boys are three to four times more likely to stutter than girls. Preschoolers may show little or no awareness of their speech difficulties, particularly during the early stages of the problem. Throughout the school years and beyond, however, most people who stutter become increasingly aware of their speech difficulties and how others react when they do not speak fluently.
The development of stuttering varies considerably across individuals. Some children show significant difficulty with speech fluency within days or weeks of onset. Others show a gradual increase in fluency difficulties over months or years. Furthermore, the severity of children’s stuttering can vary greatly from day to day and week to week. With some children, the disfluencies may appear to go away for several weeks, only to start again for no apparent reason. For teens and adults who stutter, the symptoms of stuttering tend to be more stable than they are during early childhood. Still, teen and adult speakers may report that their speech fluency is significantly better or worse than usual during specific activities.
About 75% of preschoolers who begin to stutter will eventually stop. Many children who “recover” from stuttering do so within months of the time their stuttering started. Nonetheless, there are some people who have stuttered for many years and then improve. Why some people recover is unclear, and it is not possible to say with certainty whether the stuttering symptoms for any particular child will continue into adulthood. Children’s recovery from stuttering may happen when they receive speech therapy. The role of speech therapy in the recovery process needs to be studied further, however, because some preschoolers appear to recover without ever having seen an speech-language pathologist. It is hoped that, with continued research, speech-language pathologists will someday be able to precisely answer questions about why and how recovery takes place, both with and without speech therapy.
Basic Facts about Stuttering
- Stress, anxiety, and nerves can increase a child’s stuttering, but they are not the cause of stuttering.
- More than 76 million people worldwide stutter, which is about 1% of the population. In the United States, that’s over 3 million Americans who stutter.
- Stuttering exists in all languages and all parts of the world.
- Stuttering is more common among boys than girls; about 4 times more adult males stutter than females.
- Stuttering usually begins in childhood, between the ages of 2 and 5 years.
- Stuttering behaviors will develop and vary throughout the lifespan, although stuttering can begin suddenly in childhood.
- Sometimes, in early childhood years, children will have periods in which the stuttering will appear to “go away”, only to return in a more severe pattern. As many as 80% of preschool children who begin to stutter appear to develop out of their stuttering. For those who continue to stutter into the school-age years and adolescence, however, there is a much greater likelihood that stuttering will be something that the individual will deal with throughout his or her life.
- Many people who stutter report that they experience significant variability in their stuttering–sometimes they stutter a lot, and sometimes they may stutter just a little.
- For most, when they are stuttering it feels like their speech is out of their control. The loss of control is intermittent and unpredictable. This can be disconcerting and commonly causes embarrassment, anxiety about speaking, and fear of stuttering again.
- These feelings may result in the child who stutters trying to speak quickly or trying to force his way through dysfluent moments. These behaviors usually increase the likelihood that more stuttering will result.
- From one perspective it can be said that stuttering and feeling out of control lead to anxieties about speaking and a series of behaviors that increase the frequency and severity of stuttering — a cycle which perpetuates the stuttering.
- Children and adults who stutter are no more likely to have psychological or emotional problems than children and adults who do not. There is no reason to believe that emotional trauma causes stuttering.
- Stuttering is generally not caused by psychological or physical trauma.
- Stuttering is not related to intelligence
Common Myths About Stuttering
These are just a few of the common myths out there. Instead of perpetuating such myths, it is important to have the facts about stuttering!
Myths about stuttering persist today. Here are just a few of them:
- People stutter because they are nervous. Because fluent speakers occasionally become more disfluent when they are nervous or under stress, some people assume that people who stutter do so for the same reason. While people who stutter may be nervous because they stutter, nervousness is not the cause.
- People who stutter are shy and self-conscious. Children and adults who stutter often are hesitant to speak up, but they are not otherwise shy by nature. Once they come to terms with stuttering, people who stutter can be assertive and outspoken. Many have succeeded in leadership positions that require talking
- Stuttering is a psychological disorder. Emotional factors often accompany stuttering but it is not primarily a psychological condition. Stuttering treatment often includes counseling to help people who stutter deal with attitudes and fears that may be the result of stuttering.
- People who stutter are less intelligent or capable. People who stutter are disproving this every day. The stuttering community has its share of scientists, writers, and college professors. People who stutter have achieved success in every profession imaginable.
- Stuttering is caused by emotional trauma. Some have suggested that a traumatic episode may trigger stuttering in a child who already is predisposed to it, but the general scientific consensus is that this is not usually the root cause of the disorder.
- Stuttering is caused by bad parenting. When a child stutters, it is not the parents’ fault. Stress in a child’s environment child can exacerbate stuttering, but is not the cause.
- Stuttering is just a habit that people can break if they want to. Although the manner in which people stutter may develop in certain patterns, the cause of stuttering itself is not due to a habit. Because stuttering is a neurological condition, many, if not most, people who stutter as older children or adults will continue to do so—in some fashion—even when they work very hard at changing their speech.
- Children who stutter are imitating a stuttering parent or relative. Stuttering is not contagious. Since stuttering often runs in families, however, children who have a parent or close relative who stutters may be at risk for stuttering themselves. This is due to shared genes, not imitation.
- Forcing a left-handed child to become right-handed causes stuttering. This was widely believed early in the 20th century but has been disproven in most studies since 1940. Although attempts to change handedness do not cause stuttering, the stress that resulted when a child was forced to switch hands may have exacerbated stuttering for some individuals.
- Identifying or labeling a child as a stutterer results in chronic stuttering. This was the premise of a famous study in 1939. The study was discredited decades ago, but this outdated theory still crops up occasionally. Today, we know that talking about stuttering does not cause a child to stutter.
Types of stuttering
The precise mechanisms that cause stuttering are not understood. Stuttering is commonly grouped into two types termed developmental and neurogenic.
Developmental stuttering
Developmental stuttering occurs in young children while they are still learning speech and language skills. It is the most common form of stuttering. Some scientists and clinicians believe that developmental stuttering occurs when children’s speech and language abilities are unable to meet the child’s verbal demands. Most scientists and clinicians believe that developmental stuttering stems from complex interactions of multiple factors. Recent brain imaging studies have shown consistent differences in those who stutter compared to nonstuttering peers. Developmental stuttering may also run in families and research has shown that genetic factors contribute to this type of stuttering. Starting in 2010, researchers at the National Institute on Deafness and Other Communication Disorders have identified four different genes in which mutations are associated with stuttering. More information on the genetics of stuttering can be found in the research section of this fact sheet.
Neurogenic stuttering
Neurogenic stuttering may occur after a stroke, head trauma, or other type of brain injury. With neurogenic stuttering, the brain has difficulty coordinating the different brain regions involved in speaking, resulting in problems in production of clear, fluent speech.
At one time, all stuttering was believed to be psychogenic, caused by emotional trauma, but today scientists know that psychogenic stuttering is rare.
Stuttering in children
Approximately 5 percent of all children go through a period of stuttering that lasts six months or more. Three-quarters of those will recover by late childhood, leaving about 1% with a long-term problem. The best prevention tool is early intervention. If you think your child is stuttering, it is best to seek ways that you can help as soon as possible. If the stuttering persists beyond three to six months or is particularly severe, you may want to seek help from a speech-language pathologist who specializes in stuttering right away.
If your child has difficulty speaking and tends to hesitate on or repeat certain syllables, words, or phrases, he may have a stuttering problem. But he may simply be going through periods of normal disfluency that most children experience as they learn to speak.
The normally disfluent child
- The normally disfluent child occasionally repeats syllables or words once or twice, li-li-like this. Disfluencies may also include hesitancies and the use of fillers such as “uh”, “er”, “um”.
- Disfluencies occur most often between ages one and one-half and five years, and they tend to come and go. They are usually signs that a child is learning to use language in new ways. If disfluencies disappear for several weeks, then return, the child may just be going through another stage of learning.
The child with milder stuttering
- A child with milder stuttering repeats sounds more than twice, li-li-li-li-like this. Tension and struggle may be evident in the facial muscles, especially around the mouth.
- The pitch of the voice may rise with repetitions, and occasionally the child will experience a “block” — no airflow or voice for several seconds.
- Disfluencies may come and go but are now present more often than absent.
- Try to model slow and relaxed speech when talking with your child, and encourage other family members to do the same. Don’t speak so slowly that it sounds abnormal, but keep it unhurried, with many pauses. Television’s Mr. Rogers is a good example of this style of speech.
- Slow and relaxed speech can be the most effective when combined with some time each day for the child to have one parent’s undivided attention. A few minutes can be set aside at a regular time when you are doing nothing else but listening to your child talk about whatever is on his mind.
- When your child talks to you or asks you a question, try to pause a second or so before you answer. This will help make talking to your child less hurried, more relaxed.
- Try not to be upset or annoyed when stuttering increases. Your child is doing his best as he copes with learning many new skills all at the same time. Your patient, accepting attitude will help him immensely.
- Effortless repetitions or prolongations of sounds are the healthiest form of stuttering. Anything that helps your child stutter like this instead of stuttering tensely or avoiding words is helping.
- If your child is frustrated or upset at times when his stuttering is worse, reassure him. Some children respond well to hearing, “I know it’s hard to talk at times…but lots of people get stuck on words…it’s okay.” Other children are most reassured by a touch or a hug when they seem frustrated.
The child with more severe stuttering
- If your child stutters on more than 10% of his speech, stutters with considerable effort and tension, or avoids stuttering by changing words and using extra sounds to get started, he will profit from having therapy with a specialist in stuttering. Complete blocks of speech are more common than repetitions or prolongations. Disfluencies tend to be present in most speaking situations now.
- Seek help from speech pathologists with a Certificate of Clinical Competence from the American Speech-Language-Hearing Association.
- The suggestions for parents of a child with mild stuttering are also appropriate when the child has a severe problem. Try to remember that slowing and relaxing your own speaking style is far more helpful than telling the child to slow down.
- Encourage your child to talk to you about his stuttering. Show patience and acceptance as you discuss it. Overcoming stuttering is often more a matter of losing fear of stuttering than a matter of trying harder.
7 Tips For Talking With Your Child
- Speak with your child in an unhurried way, pausing frequently. Wait a few seconds after your child finishes speaking before you begin to speak. Your own slow, relaxed speech will be far more effective than any criticism or advice such as “slow down” or “try it again slowly.”
- Reduce the number of questions you ask your child. Children speak more freely if they are expressing their own ideas rather than answering an adult’s questions. Instead of asking questions, simply comment on what your child has said, thereby letting him know you heard him.
- Use your facial expressions and other body language to convey to your child that you are listening to the content of her message and not to how she’s talking.
- Set aside a few minutes at a regular time each day when you can give your undivided attention to your child. During this time, let the child choose what he would like to do. Let him direct you in activities and decide himself whether to talk or not. When you talk during this special time, use slow, calm, and relaxed speech, with plenty of pauses. This quiet, calm time can be a confidence-builder for younger children, letting them know that a parent enjoys their company. As the child gets older, it can be a time when the child feels comfortable talking about his feelings and experiences with a parent.
- Help all members of the family learn to take turns talking and listening. Children, especially those who stutter, find it much easier to talk when there are few interruptions and they have the listeners’ attention.
- Observe the way you interact with your child. Try to increase those times that give your child the message that you are listening to her and she has plenty of time to talk. Try to decrease criticisms, rapid speech patterns, interruptions, and questions.
- Above all, convey that you accept your child as he is. The most powerful force will be your support of him, whether he stutters or not.
What should I do when my child stutters?
The most important thing to do when someone is stuttering is be a good communicator yourself.
- Keep eye contact and give your child enough time to finish speaking.
- Try not to fill in words or sentences.
- Let your child know by your manner and actions that you are listening to what she says-not how she says it.
- Model wait time-taking two seconds before you answer a child’s question-and insert more pauses into your own speech to help reduce speech pressure.
Try not to make remarks like “slow down,” “take a deep breath,” “relax,” or “think about what you’re going to say, then say it.” We often say these things to children because slowing down, relaxing, or thinking about what we are going to say helps us when we feel like we’re having a problem tripping over our words. Stuttering, though, is a different kind of speaking problem and this kind of advice is simply not helpful to someone who stutters.
How to Help Your Child Right Away
- Try to model slow and relaxed speech when talking with your child, and encourage other family members to do the same. Don’t speak so slowly that it sounds abnormal, but keep it unhurried, with many pauses. Television’s Mr. Rogers is a good example of this style of speech.
- Slow and relaxed speech can be the most effective when combined with some time each day for the child to have one parent’s undivided attention. Set aside a few minutes at a regular time when you are doing nothing else but listening to your child talk about whatever is on his mind.
- When your child talks to you or asks you a question, try to pause a second or so before you answer. This will help make talking less hurried, more relaxed.
- Try not to be upset or annoyed when stuttering increases. Your child is doing his best as he copes with learning many new skills all at the same time. Your patient, accepting attitude will help him.
- If your child is frustrated or upset at times when her stuttering is worse, reassure her. Some children respond well to hearing, “I know it’s hard to talk at times, but lots of people get stuck on words…it’s okay.” Other children are most reassured by a touch or a hug when they seem frustrated.
What should I do when my child is having a difficult speaking day?
It’s always best to check with your child about what he would like you to do on days when talking is more difficult.
Children and teens who stutter vary greatly in how they want their families, teachers, and peers to respond when they are having an especially difficult time talking. One child may prefer that his teacher treat him in the same way as she would any other day, by spontaneously calling on him or asking him to read aloud.
On the other hand, another child may want his teacher to temporarily reduce her expectations for his verbal participation, by calling on him only if his hand is raised or allowing him to take a pass during activities such as round-robin reading.
What should I do when my child interrupts someone else?
Handle interruptions the same way that you would if your child didn’t stutter. Children who stutter sometimes interrupt others because it’s easier to get speech going while others are talking. Scientists are not sure exactly why it’s easier to talk over others, but it may be because less attention is called to the child at the beginning of her turn when stuttering is most likely to occur.
Even though it may be easier to get her speech going by interrupting someone else, it’s important for your child to learn the rules for good communication.
What about oral reports and other classroom demands?
There are many things you can do to help make oral reports a positive experience for your child. Together, you and your child can develop a plan, considering factors such as:
- Order ‘ whether he wants to be one of the first to present, in the middle, or one of the last to present;
- Practice opportunities ‘ ways he can practice that will help him feel more comfortable, such as at home with you, with a friend, or at a speech therapy session;
- Audience size ‘ whether to give the oral report in private, in a small group, or in front of the entire class;
- Other issues ‘ whether he should be timed, or whether grading criteria should be modified because of his stuttering;
- Being called on ‘ whether he feels comfortable being called on at any time in class, only when his hand is raised, or when signaled first by the teacher; and
- How to talk with his teacher about his preferences for talking in class.
How should I handle teasing?
One of the most painful experiences we can have as a parent is knowing that our child is being teased. Teasing is an experience common to many children, not just those who stutter.
- For the free ebook “Sometimes I Just Stutter” has great advice on how to handle teasing, please get it here: https://www.stutteringhelp.org/sites/default/files/Migrate/sometimes_stutter.pdf
What types of things can I say to encourage my child to talk?
The best way to encourage a child who stutters to talk is to let him know through your words and actions that what he says is important, not the way he says it. Other ways you can encourage the child:
- Praise him for sharing his ideas;
- Tell him that stuttering does not bother you;
- Give him opportunities to talk, such as starting a conversation or asking him for
his opinion; and, - Let him know it’s ok with you to stutter.
What causes stuttering
The exact cause of stuttering is unknown. There are four factors most likely to contribute to the development of stuttering:
- Genetics (approximately 60% of those who stutter have a family member who does also);
- Child development (children with other speech and language problems or developmental delays are more likely to stutter);
- Neurophysiology (recent neurological research has shown that people who stutter process speech and language slightly differently than those who do not stutter); and
- Family dynamics (high expectations and fast-paced lifestyles can contribute to stuttering).
Recent studies suggest that genetics plays a role in the disorder. It is thought that many, if not most, individuals who stutter inherit traits that put them at risk to develop stuttering. The exact nature of these traits is presently unclear. Whatever the traits are, they obviously impair the individual’s ability to string together the various muscle movements that are necessary to produce sentences fluently.
Stuttering may occur when a combination of factors comes together and may have different causes in different people. It is probable that what causes stuttering differs from what makes it continue or get worse.
Not everyone who is predisposed to stutter will develop the disorder. For many, certain life events are thought to “trigger” fluency difficulty. One of the triggers for developmental stuttering may be the development of grammar skills. Between the ages of 2 and 5 years, children learn many of the grammatical rules of language. These rules allow children to change immature messages (“Mommy candy”) into longer sentences that require coordination to produce fluently (“Mommy put the candy in my backpack”). A child who is predisposed to stutter may have no difficulty speaking fluently when sentences are only one or two words long. However, when the child starts trying to produce longer, more complex sentences, he or she may find himself or herself not quite up to the challenge-and disfluent speech results.
After stuttering has started, other factors may cause more disfluencies. For example, a child who is easily frustrated may be more likely to tighten or tense speech muscles when disfluencies occur. Such tension may increase how long a disfluency lasts. Listeners’ responses to stuttering (e.g., teasing) can aggravate fluency difficulties as well. People who stutter vary widely in how they react to the disfluencies in their speech. Some appear to be minimally concerned. Others-especially those who have encountered unfavorable reactions from listeners-may develop emotional responses to stuttering that hinder speech production further. Examples of these emotions include shame, embarrassment, and anxiety.
Stuttering resulting from other causes
Speech fluency can be disrupted from causes other than developmental stuttering. A stroke, traumatic brain injury, or other brain disorders can cause speech that is slow or has pauses or repeated sounds (neurogenic stuttering).
Speech fluency can also be disrupted in the context of emotional distress. Speakers who do not stutter may experience dysfluency when they are nervous or feeling pressured. These situations may also cause speakers who stutter to be less fluent.
Speech difficulties that appear after an emotional trauma (psychogenic stuttering) are uncommon and not the same as developmental stuttering.
Risk factors for stuttering
Certain factors may place children at risk for stuttering. Knowing these factors will help you decide whether or not your child needs to see a speech-language pathologist 1, 2, 3, 4. Certain factors may place children at risk for stuttering. Knowing these factors will help you decide whether or not your child needs to see a speech-language pathologist.
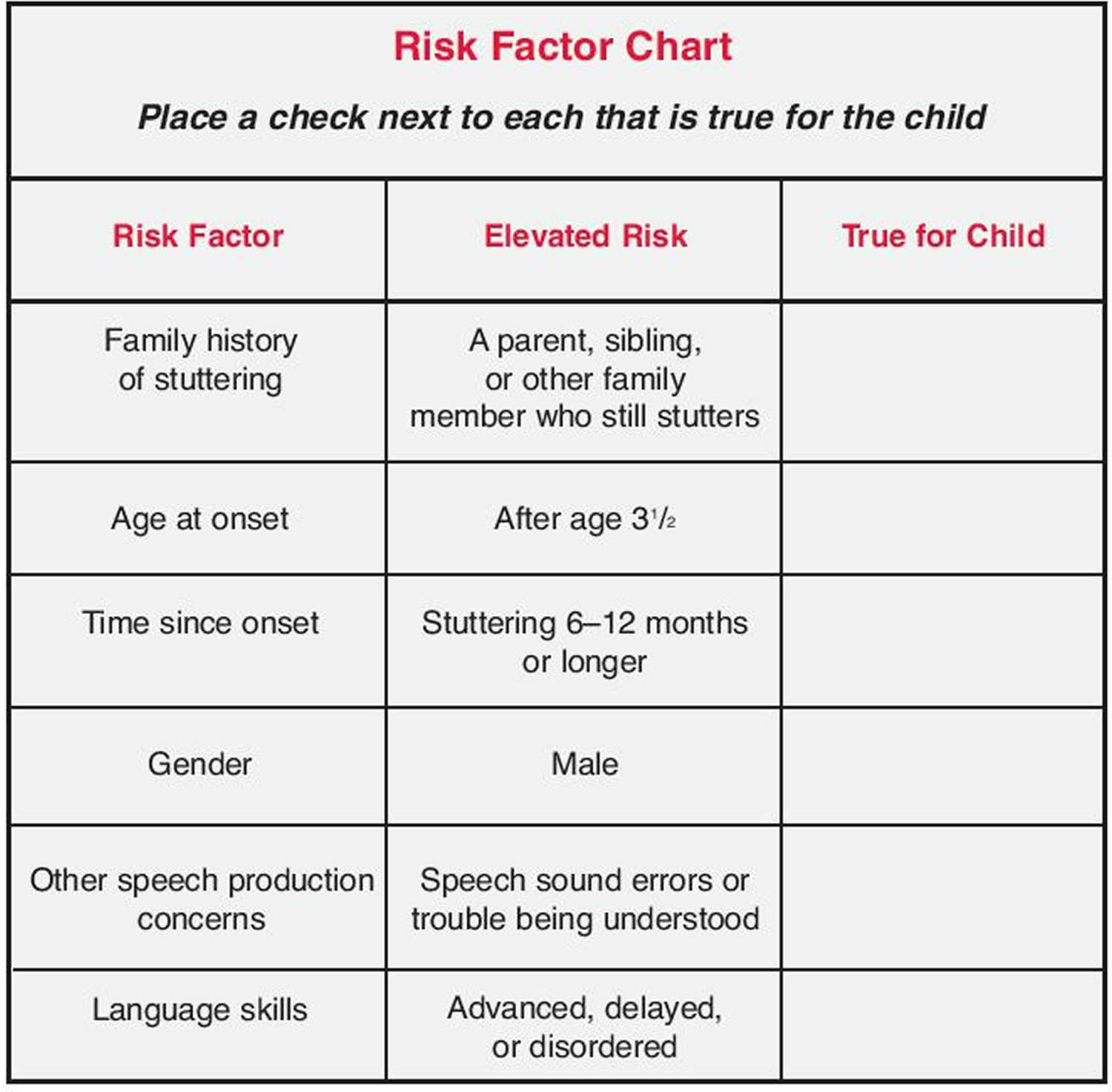
Figure 1 Stuttering risk factors chart below. If your child has one or more of these risk factors, you should be more concerned. You may want to schedule a speech screening with a speech therapist who specializes in stuttering. The therapist will decide whether your child is stuttering, and then determine whether to wait a bit longer or begin treatment right away.
Figure 1. Stuttering risk factors
 [Source 5]
[Source 5]
Family history
There is now strong evidence that almost half of all children who stutter have a family member who stutters. The risk that your child is actually stuttering instead of just having normal disfluencies increases if that family member is still stuttering. There is less risk if the family member outgrew stuttering as a child.
Age at onset
Children who begin stuttering before age 3 1/2 are more likely to outgrow stuttering; if your child begins stuttering before age 3, there is a much better chance she will outgrow it within 6 months.
Time since onset
Between 75% and 80% of all children who begin stuttering will begin to show improvement within 12 to 24 months without speech therapy. If your child has been stuttering longer than 6 months, or if the stuttering has worsened, he may be less likely to outgrow it on his own.
Gender
Girls are more likely than boys to outgrow stuttering. In fact, three to four boys continue to stutter for every girl who stutters. Why this difference? First, it appears that during early childhood, there are innate differences between boys’ and girls’ speech and language abilities. Second, during this same period, parents, family members, and others often react to boys somewhat differently than girls. Therefore, it may be that more boys stutter than girls because of basic differences in boys’ speech and language abilities and differences in their interactions with others. That being said, many boys who begin stuttering will outgrow the problem. What is important for you to remember is that if your child is stuttering right now, it doesn’t necessarily mean he or she will stutter the rest of his or her life.
Other speech and language factors
A child who speaks clearly with few, if any, speech errors would be more likely to outgrow stuttering than a child whose speech errors make him difficult to understand. If your child makes frequent speech errors such as substituting one sound for another or leaving sounds out of words, or has trouble following directions, you should be more concerned. The most recent findings dispel previous reports that children who begin stuttering have, as a group, lower language skills. On the contrary, there are indications that they are well within the norms or above. Advanced language skills appear to be even more of a risk factor for children whose stuttering persists 6.
These risk factors place children at higher risk for developing stuttering. If your child has any of these risk factors and is showing some or all of the warning signs mentioned previously, you should be more concerned. You may want to schedule a speech screening with a speech therapist who specializes in stuttering. The therapist will decide whether your child is stuttering, and then determine whether to wait a bit longer or begin treatment right away.
Can stuttering be treated?
Yes, there are a variety of successful approaches for treating both children and adults. In general, the earlier, the better is good advice.
Why Go To Speech Therapy?
Many teens and adults who stutter have been to speech therapy for their stuttering at least once in their lives. Some people have been through years of therapy. Just because you may have had treatment for your stuttering in the past does not mean you shouldn’t consider it again. It is common for stuttering to change over time or for emotions and attitudes about your speech to change as you have new experiences.
It is important for you to have a clear idea about your motivation for going to therapy because your reasons for seeking treatment will help you decide:
- The speech-language pathologist who is right for you;
- The amount, length, and cost of treatment;
- Possible goals for speech therapy; and,
- The amount of success to be expected.
Choosing a Speech-Language Pathologist
The key to success with any kind of treatment is finding someone who is knowledgeable about that particular treatment. This is especially true of stuttering.
- The Stuttering Foundation’s referral list has names of people who specialize in treating stuttering – https://www.stutteringhelp.org/referrals-information.
- The American Speech-Language-Hearing Association (ASHA) has a list of certified speech-language pathologists –http://find.asha.org/pro#f:@Provider=[Speech-Language%20Pathologist]
If none are located near you, contact a local university, hospital, or speech and hearing clinic. Universities that have training programs in speech pathology often have a speech clinic that will provide therapy for stuttering.
Once you’ve contacted a speech pathologist, interview them. There are many important questions you will want to ask, but a few in particular are very important.
- How comfortable are you with treating stuttering? This is important because some speech pathologists are not comfortable working with stuttering.
- How many teens and adults who stutter have you worked with? This will help you determine whether the speech pathologist has the kind of experience you need.
- What do you think the primary goals of stuttering therapy should be for a teen/adult? This will help you decide whether the speech pathologist’s ideas about goals match your own.
- What approaches do you use in speech therapy? How often is therapy scheduled? These questions are important because some types of therapy work best when you can go on an intensive schedule (i.e., every day for several hours each day across several weeks). Sometimes the therapy schedule the speech pathologist offers will not work for you because of your job or family commitments. It’s important to know this up front.
Therapy Amount, Length, and Cost
The amount of stuttering therapy needed and length of time involved are related to each other and are usually different for each person. The decision about how much therapy is needed and how often it should be scheduled is usually made following a stuttering evaluation.
A thorough evaluation usually ranges from two to four hours and may cost between $300 and $500, depending on your location and the speech pathologist’s charges. These charges can vary greatly, so be sure to ask about costs when making the initial call to the speech pathologist. Also, check to see if your health insurance covers the cost of the evaluation.
Once you’ve completed the evaluation process, the speech pathologist will explain your results to you and then the two of you will begin thinking about the length of time that you can expect to be in therapy and how often it should be scheduled. Therapy length and amount needed depend on your goals, the type of therapy itself, and the severity of the stuttering handicap.
Some therapy programs offer a standard amount of therapy in a set length of time, such as 40 hours across a three-week time period in an intensive program. For many people, however, it takes a longer period of time to overcome the negative feelings about stuttering that build up over the years. In this situation, intensive therapy may not be the right approach to treat the stuttering. Keep in mind also that some speech pathologists do not offer intensive therapy.
If any of these factors are true for your situation, you might want to go to therapy one or two times a week for an hour across several months or even a year. In general, many adults who are seeking long-term changes in stuttering will attend twice-weekly therapy anywhere from 6 to 18 months. Hourly therapy charges can range from fifty to eighty-five dollars. Again, these charges will depend on your location and the speech pathologist’s hourly charges. Local university speech and hearing clinics often charge less because of their training mission. At many university programs, it is possible to get an evaluation and therapy at lower rates than those listed here.
Contact your insurance company before you get an evaluation or go for therapy to find out whether they cover stuttering therapy. It’s important to ask about stuttering therapy in particular because many insurance companies will pay for speech therapy that is restorative (i.e., after a stroke or brain injury), but may not pay for stuttering therapy when it’s viewed as a chronic speech disability.
Stuttering diagnosis
Identifying stuttering in an individual’s speech would seem like an easy task. Disfluencies often “stand out” and disrupt a person’s communication. Listeners can usually detect when a person is stuttering. At the same time, however, stuttering can affect more than just a person’s observable speech. Some characteristics of stuttered speech are not as easy for listeners to detect. As a result, diagnosing stuttering requires the skills of a certified speech-language pathologist.
Stuttering is usually diagnosed by a speech-language pathologist, a health professional who is trained to test and treat individuals with voice, speech, and language disorders. The speech-language pathologist will consider a variety of factors, including the child’s case history (such as when the stuttering was first noticed and under what circumstances), an analysis of the child’s stuttering behaviors, and an evaluation of the child’s speech and language abilities and the impact of stuttering on his or her life.
During an evaluation, an speech-language pathologist will note the number and types of speech disfluencies a person produces in various situations. The speech-language pathologist will also assess the ways in which the person reacts to and copes with disfluencies. The speech-language pathologist may also gather information about factors such as teasing that may make the problem worse. A variety of other assessments (e.g., speech rate, language skills) may be completed as well, depending upon the person’s age and history. Information about the person is then analyzed to determine whether a fluency disorder exists. If so, the extent to which it affects the ability to perform and participate in daily activities is determined.
For young children, it is important to predict whether the stuttering is likely to continue. An evaluation consists of a series of tests, observations, and interviews designed to estimate the child’s risk for continuing to stutter. Although there is some disagreement among speech-language pathologists about which risk factors are most important to consider, factors that are noted by many specialists include the following:
- a family history of stuttering
- stuttering that has continued for 6 months or longer
- presence of other speech or language disorders
- strong fears or concerns about stuttering on the part of the child or the family
No single factor can be used to predict whether a child will continue to stutter. The combination of these factors can help speech-language pathologists determine whether treatment is indicated.
For older children and adults, the question of whether stuttering is likely to continue is somewhat less important, because the stuttering has continued at least long enough for it to become a problem in the person’s daily life. For these individuals, an evaluation consists of tests, observations, and interviews that are designed to assess the overall severity of the disorder. In addition, the impact the disorder has on the person’s ability to communicate and participate appropriately in daily activities is evaluated. Information from the evaluation is then used to develop a specific treatment program, one that is designed to:
- help the individual speak more fluently,
- communicate more effectively, and
- participate more fully in life activities.
Stuttering treatment
Although there is currently no cure for stuttering, there are a variety of treatments available. The nature of the treatment will differ, based upon a person’s age, communication goals, and other factors. If you or your child stutters, it is important to work with a speech-language pathologist to determine the best treatment options.
Most treatment programs for people who stutter are “behavioral.” They are designed to teach the person specific skills or behaviors that lead to improved oral communication. For instance, many speech-language pathologists teach people who stutter to control and/or monitor the rate at which they speak. In addition, people may learn to start saying words in a slightly slower and less physically tense manner. They may also learn to control or monitor their breathing. When learning to control speech rate, people often begin by practicing smooth, fluent speech at rates that are much slower than typical speech, using short phrases and sentences. Over time, people learn to produce smooth speech at faster rates, in longer sentences, and in more challenging situations until speech sounds both fluent and natural. “Follow-up” or “maintenance” sessions are often necessary after completion of formal intervention to prevent relapse.
Goals for Speech Therapy
Stuttering therapy for teens and adults usually means changing long-standing speech behaviors, emotions, and attitudes about talking and communication in general. As a result, length and type of therapy can vary greatly depending on your goals. A list of sample therapy goals for teens and adults includes:
- Reducing the frequency of stuttering;
- Decreasing the tension and struggle of stuttering moments;
- Working to decrease word or situation avoidances;
- Learning more about stuttering;
- Using effective communication skills such as eye contact or phrasing; and,
- Determining whether goals relate to long-term change or to meet a specific short-term need, such as a job interview.
Working together with a speech pathologist who is knowledgeable about stuttering will help you identify your personal goals.
What do speech-language pathologists do when working with individuals who stutter
Speech-language pathologists work to help people who stutter lessen the impact or severity of disfluency when it occurs. The goal is not so much to eliminate disruptions in fluency-which many people find difficult to do-but to minimize their impact upon communication when they do occur. People may be taught to identify how they react to or cope with breaks in speech fluency. They learn other reactions that will lead to fluent speech and effective communication. For instance, a person who often produces long, physically tense disfluencies would learn to modify these disfluencies so that they become fleeting, relatively effortless breaks in speech. As people become better at managing fluency in therapy, they practice the newly learned skills in real-life situations.
People usually find that these behavioral strategies are relatively easy to implement during therapy activities. In contrast, people may find that day-to-day fluency management-at least in the early stages of treatment-is hard work! Use of the various fluency management techniques requires mental effort. It is one thing to manage or monitor speech rate in a quiet, controlled setting like a therapy room, but quite another in a noisy, fast-paced office or classroom. For this reason, speech-language pathologists often work with family members, teachers, and others on what to expect from therapy. Generally, it is not reasonable to expect that a person who stutters will be able to monitor or control his speech fluency at all times of the day in all situations.
Traditionally, there has been some reluctance to treat stuttering during the preschool years. This reluctance has stemmed from at least two sources: the observation that many children “outgrow” stuttering, and the belief that therapy heightens a child’s awareness of fluency difficulty which in turn increases the child’s risk for persistent stuttering. Current thinking is somewhat different from these traditional views, however. It is now generally agreed that early intervention for stuttering is desirable. That said, an speech-language pathologist still may recommend a “wait and see” approach for children who have been stuttering for only a few months and who otherwise appear to be unconcerned and at low risk for persistent stuttering. If treatment is recommended for preschoolers, the approaches taken usually are somewhat different from those used with older children and adults. For example, parents may be trained to provide youngsters with feedback about their speech fluency, praising the fluent speech (“That was very smooth!”), and occasionally highlighting instances of disfluent speech (“That sounded a little bumpy”). Parents and/or speech-language pathologists may model smooth speech. speech-language pathologists teach parents when, where, and how to implement these treatments. Recent research suggests that intervention programs like these are quite effective at reducing, if not eliminating, the symptoms of stuttering with preschoolers.
In addition to the approaches described above, a variety of assistive devices have been developed to help those who stutter speak more smoothly. Most of these assistive devices alter the way in which an individual hears his or her voice while speaking. The devices often are small, so that they fit in or behind a speaker’s ear. Laboratory research suggests that some individuals who stutter speak more fluently when they hear their voice played back to them at a slight delay or at a higher or lower pitch, or when “white noise” is played into their ear as they speak. How effective these devices are in real-life settings continues to be studied. Early findings suggest that some people find some auditory feedback devices very helpful, while others do not.
Research is ongoing to identify:
- why some people benefit from the devices more than others
- whether the devices can be made to be more effective
- how much improvement one might expect in fluency when a device is used either alone or with speech therapy
- whether the benefits last over time
In addition to treatment provided by speech-language pathologists, some people who stutter have found help dealing with their stuttering through stuttering self-help and support groups. In general, stuttering support groups are not therapy groups. Instead, they are groups of individuals who are facing similar problems. These individuals work together to help themselves cope with the everyday difficulties of stuttering.
Many such groups exist around the world. In the United States stuttering support groups have a long-standing and strong tradition of helping people overcome the burden of stuttering. Support groups often have local chapters that consist of anywhere from a few to a few dozen members who meet regularly (e.g., weekly or monthly) to discuss issues related to their stuttering. Some groups also have e-mail lists and chat rooms, newsletters and books, and annual conferences that bring together hundreds of people who stutter and their families.
Many support group members report that their experiences in the support group improve their ability to use techniques learned in therapy. Others report that the support group meets needs that their formal speech therapy did not meet. Thus, many people benefit from participating in treatment provided by an speech-language pathologist and a stuttering support group. Indeed, most support groups have developed strong partnerships with the speech-language pathology community to promote and expand treatment options for people who stutter.
Self-help groups
Many people find that they achieve their greatest success through a combination of self-study and therapy. Self-help groups provide a way for people who stutter to find resources and support as they face the challenges of stuttering. It can be helpful for children, parents and adults who stutter to connect with other people who stutter or who have children who stutter. Several organizations offer support groups. Along with providing encouragement, support group members may offer advice and coping tips that you might not have considered.
This list is not exhaustive:
- National Stuttering Association http://www.nsastutter.org/
- Stuttering Home Page http://www.mnsu.edu/comdis/kuster/stutter.html
- Stuttering Foundation of America https://www.stutteringhelp.org/
- The Canadian Stuttering Association http://www.stutter.ca/
- K12 Academics Stuttering Page http://www.k12academics.com/disorders-disabilities/stuttering
- University College London’s Archive of Stuttered Speech (UCLASS) Speech samples from children who stutter http://www.ucl.ac.uk/speech-research-group
- American Institute for Stuttering: http://stutteringtreatment.org/
- FRIENDS: The National Association of Young People Who Stutter: https://www.friendswhostutter.org/
Therapy for children
For very young children, early treatment may prevent developmental stuttering from becoming a lifelong problem. Certain strategies can help children learn to improve their speech fluency while developing positive attitudes toward communication. Health professionals generally recommend that a child be evaluated if he or she has stuttered for 3 to 6 months, exhibits struggle behaviors associated with stuttering, or has a family history of stuttering or related communication disorders. Some researchers recommend that a child be evaluated every 3 months to determine if the stuttering is increasing or decreasing. Treatment often involves teaching parents about ways to support their child’s production of fluent speech. Parents may be encouraged to:
- Provide a relaxed home environment that allows many opportunities for the child to speak. This includes setting aside time to talk to one another, especially when the child is excited and has a lot to say.
- Listen attentively when the child speaks and focus on the content of the message, rather than responding to how it is said or interruptng the child.
- Speak in a slightly slowed and relaxed manner. This can help reduce time pressures the child may be experiencing.
- Listen attentively when the child speaks and wait for him or her to say the intended word. Don’t try to complete the child’s sentences. Also, help the child learn that a person can communicate successfully even when stuttering occurs.
- Talk openly and honestly to the child about stuttering if he or she brings up the subject. Let the child know that it is okay for some disruptions to occur.
Stuttering therapy
Many of the current therapies for teens and adults who stutter focus on helping them learn ways to minimize stuttering when they speak, such as by speaking more slowly, regulating their breathing, or gradually progressing from single-syllable responses to longer words and more complex sentences. Most of these therapies also help address the anxiety a person who stutters may feel in certain speaking situations.
Drug therapy
The U.S. Food and Drug Administration has not approved any drug for the treatment of stuttering. However, some drugs that are approved to treat other health problems—such as epilepsy, anxiety, or depression—have been used to treat stuttering. These drugs often have side effects that make them difficult to use over a long period of time.
Electronic devices
Some people who stutter use electronic devices to help control fluency. For example, one type of device fits into the ear canal, much like a hearing aid, and digitally replays a slightly altered version of the wearer’s voice into the ear so that it sounds as if he or she is speaking in unison with another person. In some people, electronic devices may help improve fluency in a relatively short period of time. Additional research is needed to determine how long such effects may last and whether people are able to easily use and benefit from these devices in real-world situations. For these reasons, researchers are continuing to study the long-term effectiveness of these devices.
Coping and support
If you’re the parent of a child who stutters, these tips may help:
- Listen attentively to your child. Maintain natural eye contact when he or she speaks.
- Wait for your child to say the word he or she is trying to say. Don’t jump in to complete the sentence or thought.
- Set aside time when you can talk to your child without distractions. Mealtimes can provide a good opportunity for conversation.
- Speak slowly, in an unhurried way. If you speak in this way, your child will often do the same, which may help decrease stuttering.
- Take turns talking. Encourage everyone in your family to be a good listener and to take turns talking.
- Strive for calm. Do your best to create a relaxed, calm atmosphere at home in which your child feels comfortable speaking freely.
- Don’t focus on your child’s stuttering. Try not to draw attention to the stuttering during daily interactions. Don’t expose your child to situations that create a sense of urgency, pressure, or a need to rush or that require your child to speak in front of others.
- Offer praise rather than criticism. It’s better to praise your child for speaking clearly than to draw attention to stuttering. If you do correct your child’s speech, do so in a gentle, positive way.
- Accept your child just as he or she is. Don’t react negatively or criticize or punish your child for stuttering. This can add to feelings of insecurity and self-consciousness. Support and encouragement can make a big difference.
- Yairi, E. & Ambrose, N. (2005). Early Childhood Stuttering: For Clinicians by Clinicians, ProEd, Austin, TX.[↩]
- Yairi, E. & Ambrose, N. (1999). Early childhood stuttering I: Persistence and recovery rates. Journal of Speech, Language, and Hearing Research, 42, 1097-1112.[↩]
- Yairi, E. & Ambrose, N. (1992). A longitudinal study of stuttering in children: A preliminary report. Journal of Speech, Language, and Hearing Research, 35, 755-760.[↩]
- Ambrose, N. & Yairi, E. (1999). Normative disfluency data for early childhood stuttering. Journal of Speech, Language, and Hearing Research, 42, 895-909.[↩]
- Stuttering Risk Factors. Stuttering Foundation of America. https://www.stutteringhelp.org/risk-factors[↩]
- Yairi, E. & Ambrose, N. (2005). Early Childhood Stuttering: For Clinicians by Clinicians, Chapter 7, Pro-Ed, Austin, TX.[↩]





{kind=link}