
Contents
Tension headaches
Tension headaches also known as tension type headaches, stress headache, ordinary headache, muscle contraction headache, essential headache, idiopathic headache, psychogenic headache or psychomyogenic headache, feels like a band squeezing your head, scalp, or neck, that is often associated with muscle tightness in these areas 1, 2, 3, 4. Tension headaches classically present as a non-pulsatile, bandlike pressure or tightening that wraps around your head of mild to moderate intensity, and affecting both side of your head in location, and does not worsen with the routine physical activity 5, 6, 7, 8. Nausea and vomiting is usually absent, but abnormal sensitivity to light (photophobia) or abnormal sensitivity to sound (phonophobia) may be present 9. Frequent episodic tension‐type headache means having between one and 14 headaches per month. People with tension headaches try to relieve pain by massaging their scalp, temples, or the bottom of the neck.
A tension headache is the most common type of headache, accounting for 90% of all headaches diagnosed by healthcare professionals and affects more than 40 percent of the adult population worldwide 10. Tension headaches are slightly more common in women than men and tends to run in families 11. Tension headaches may occur at any age, but are most common in adults and older teens.
The 2018 International Classification of Headache Disorders (ICHD) divides tension headaches into three subtypes based on the frequency of episodes 1:
- Infrequent episodic tension type headache
- (A) At least 10 episodes of headache occurring on less than 1 day/month on average (less than 12 days/year) and fulfilling criteria B-D
- (B) Lasting from 30 minutes to 7 days
- (C) At least two of the following four characteristics:
- bilateral location
- pressing or tightening (non-pulsating) quality
- mild or moderate intensity
- not aggravated by routine physical activity such as walking or climbing stairs
- (D) Both of the following:
- no nausea or vomiting
- no more than one of photophobia or phonophobia
- (E) Not better accounted for by another International Classification of Headache Disorders, 3rd edition diagnosis.
- Frequent episodic tension type headache
- Same as Infrequent episodic tension type headache except:
- (A) At least 10 episodes of headache occurring on 1-14 days/month on average for more than 3 months (greater than or equal to 12 and less than 180
days/year) and fulfilling criteria B-D.
- (A) At least 10 episodes of headache occurring on 1-14 days/month on average for more than 3 months (greater than or equal to 12 and less than 180
- Same as Infrequent episodic tension type headache except:
- Chronic tension type headache
- Same as Infrequent episodic tension type headache except:
- (A) Headache occurring on greater than or equal to 15 days/month on average for >3 months (greater than or equal to 180 days/year), fulfilling criteria B-D
- (B) Lasting hours to days, or unremitting
- (C) Both of the following:
- no more than one of photophobia, phonophobia or mild nausea
- neither moderate or severe nausea nor vomiting
- Same as Infrequent episodic tension type headache except:
Although there are differences between the tension-type headache subtypes, they all share the common feature of bilateral non-throbbing pain, of a crushing nature, with mild-to-moderate intensity and without worsening with physical activity or association with nausea or vomiting 1. Mild nausea is only seen in the chronic tension-type headache subtype 1. According to the 2018 International Classification of Headache Disorders (ICHD), chronic tension-type headache appears as a result of the natural history of an episodic tension-type headache sustained over time, with a frequency of onset of 15 or more days per month for, at least, 3 months 1.
Comparing episodic tension-type headache and chronic tension-type headache, it has been observed that headaches in patients with chronic tension-type headache are more frequent, intense, and require more medical attention 12, 13. Although there are few studies on the clinical characteristics of chronic tension-type headaches 12, 14, 15, they have been found to be similar to those of episodic tension-type headaches, except for greater pain intensity 14. In a population sample, it has been found that pain in chronic tension-type headache is bilateral in 88% of cases, of a pressure or hardening quality in 83%, and of mild or moderate intensity in 96% of cases 14. In addition, in 71% of cases, it is not aggravated by routine physical activity, and in 58%, there are no accompanying symptoms such as nausea, photophobia, or phonophobia 14.
The exact mechanisms of tension-type headache are not known 1. Tension headaches are believed to occur when neck and scalp muscles become tense or contract. The muscle contractions can be a response to anxiety, stress, depression, head injury, poor health, sleep disturbances or poor posture 7, 8.
Tension headaches are often misdiagnosed as mild forms of migraine without aura (visual disturbances such as seeing bright spots or flashes of light) 1. This is more so because patients with frequent headaches often suffer from both disorders 1. Individuals who meet the criteria for tension-type headache but who have normal neurologic examination results require no additional laboratory testing or neuroimaging 16. With a tension headache, there are usually no problems with your nervous system. But tender points (trigger points) in the muscles are often found in the neck and shoulder areas.
Headaches “Red Flags” that can signal a more serious disorder that requires prompt medical care. Immediately call or see a doctor if you or someone you’re with experience any of these symptoms 17, 18, 19:
- Sudden, severe headache that may be accompanied by a stiff neck
- Severe headache accompanied by fever, nausea, or vomiting that is not related to another illness
- “First” or “worst” headache, often accompanied by confusion, weakness, double vision, or loss of consciousness
- Headache that worsens over days or weeks or has changed in pattern or behavior
- Recurring headache in children
- Headache following a head injury
- Headache and a loss of sensation or weakness in any part of the body, which could be a sign of a stroke
- Headache associated with convulsions and/or shortness of breath
- Two or more headaches a week
- Persistent headache in someone who has been previously headache-free, particularly in someone over age 50
- New headaches in someone with a history of cancer or HIV/AIDS
If your headache is mild to moderate, without other “Red Flags” symptoms, and responds to home treatment within a few hours, you may not need further examination or testing.
Tension type headache treatment involves treating your headache symptoms right away and headaches prevention by avoiding or changing your triggers. A key step in doing this involves learning to manage your tension headaches at home by:
- Keeping a headache diary to help you identify your headache triggers so that you and your health care provider can make changes in your lifestyle to reduce the number of headaches you get. Note when your headaches start and your activities. Also record how long the headaches last and anything that provides relief. The diary may help you spot patterns in your daily habits that may lead to headaches.
- Learning what to do to relieve a headache when it starts.
- Learning how to take your headache medicines the correct way.
Many people can treat their tension headaches with conservative therapy, such as relaxation or stress-management training, including:
- Massage. Massage can help reduce stress and relieve tension 20. Massage therapy is especially effective for relieving tight, tender muscles in the back of the head, neck and shoulders. For some people, it may also provide relief from headache pain.
- Biofeedback training. Biofeedback measures body functions and gives you information about them so that you can become more aware of those functions and learn to control them. For example, a biofeedback device may show you measurements of muscle tension. By watching how these measurements change, you can become more aware of when your muscles are tense and learn to relax them. Biofeedback training teaches you to control certain body responses that help reduce pain. A device monitors and gives you feedback on your muscle tension, heart rate and blood pressure. You then learn how to reduce muscle tension and slow your heart rate and breathing. Many studies have tested biofeedback for tension headaches, and several evaluations of this research have concluded that biofeedback may be helpful. However, an evaluation that included only the highest quality studies concluded that there is conflicting evidence about whether biofeedback is helpful for tension headaches 21.
- Cognitive behavioral therapy. This type of talk therapy may help you learn to manage stress. Doing this may help you have fewer or less painful headaches.
- Acupuncture. Acupuncture may provide temporary relief from chronic headache pain 22. Acupuncture involves using very thin, disposable needles that generally cause little pain or discomfort. Acupuncture is typically safe when performed by an experienced acupuncturist who follows safety guidelines and uses sterile needles. Much of acupuncture’s benefit may be due to nonspecific factors including expectation, beliefs, and placebo responses rather than specific effects of needling.
- Tai Chi. Tai Chi combines meditation with slow, graceful movements, deep breathing, and relaxation. One small randomized study has evaluated tai chi for tension headaches. Some evidence of improvements in headache status and health-related quality of life was found among patients on the tai chi program compared to others on a wait list. These data are too limited to draw meaningful conclusions about whether this practice is helpful for tension headaches 23.
- Ice or hot packs. Rest, ice packs or a long, hot shower may be all you need to relieve a tension-type headache.
- Relaxation techniques. Anything that helps you relax may help your headaches. This can include deep breathing, yoga, meditation and progressive muscle relaxation. You can learn these methods in classes or at home using books or apps.
When needed, medicines that may relieve a tension headache include:
- Over-the-counter (OTC) pain medicines, such as aspirin, ibuprofen, or acetaminophen (paracetamol)
- Narcotic pain relievers are generally not recommended
- Muscle relaxers
- Tricyclic antidepressants to prevent recurrences
Using medicines along with stress management may be more effective than any one treatment in reducing your tension-type headaches.
Be aware that:
- Taking medicines more than 3 days a week may lead to rebound headaches. These are headaches that keep coming back due to overuse of pain medicine.
- Taking too much acetaminophen (paracetamol) can damage your liver.
- Too much ibuprofen or aspirin can irritate your stomach or damage the kidneys.
If these medicines do not help, see your doctor about prescription medicines.
Figure 1. Headache Classification
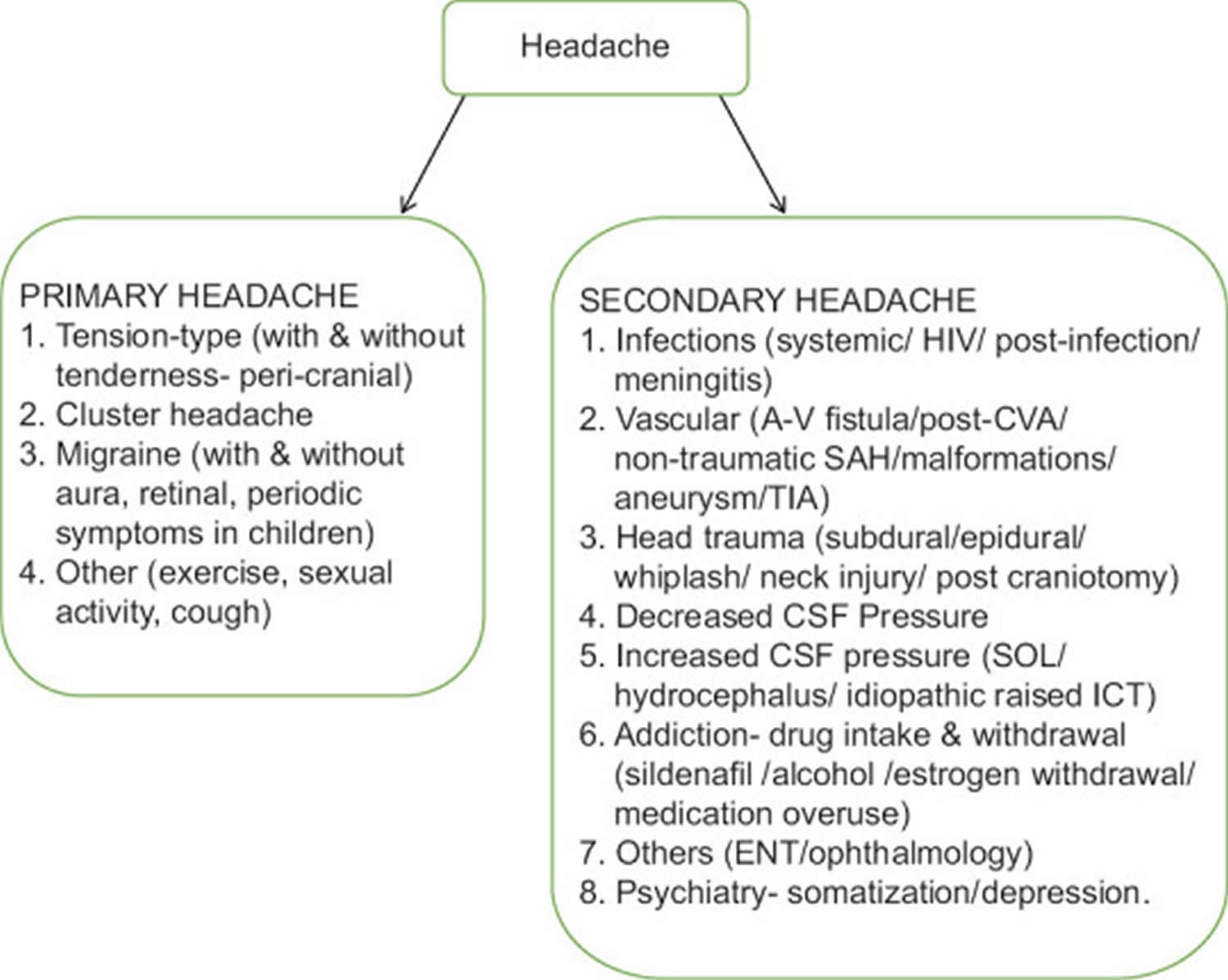
Footnotes: Primary headaches occur independently and are not caused by another medical condition. Secondary headaches are symptoms of another health disorder that causes pain-sensitive nerve endings to be pressed on or pulled or pushed out of place. Secondary headaches result from underlying conditions that affect the brain. Some of the more serious causes of secondary headache include: brain tumor, head injury, increased intracranial pressure, disorders of blood vessels in the brain including stroke, exposure to a substance or its withdrawal (e.g., alcohol, following carbon monoxide poisoning, or from exposure to toxic chemicals and metals, cleaning products or solvents, and pesticides), brain and spinal cord inflammation from infections, structural abnormalities of the head, neck, and spine
[Source 24, 25 ]Figure 2. Headaches diagnostic algorithm
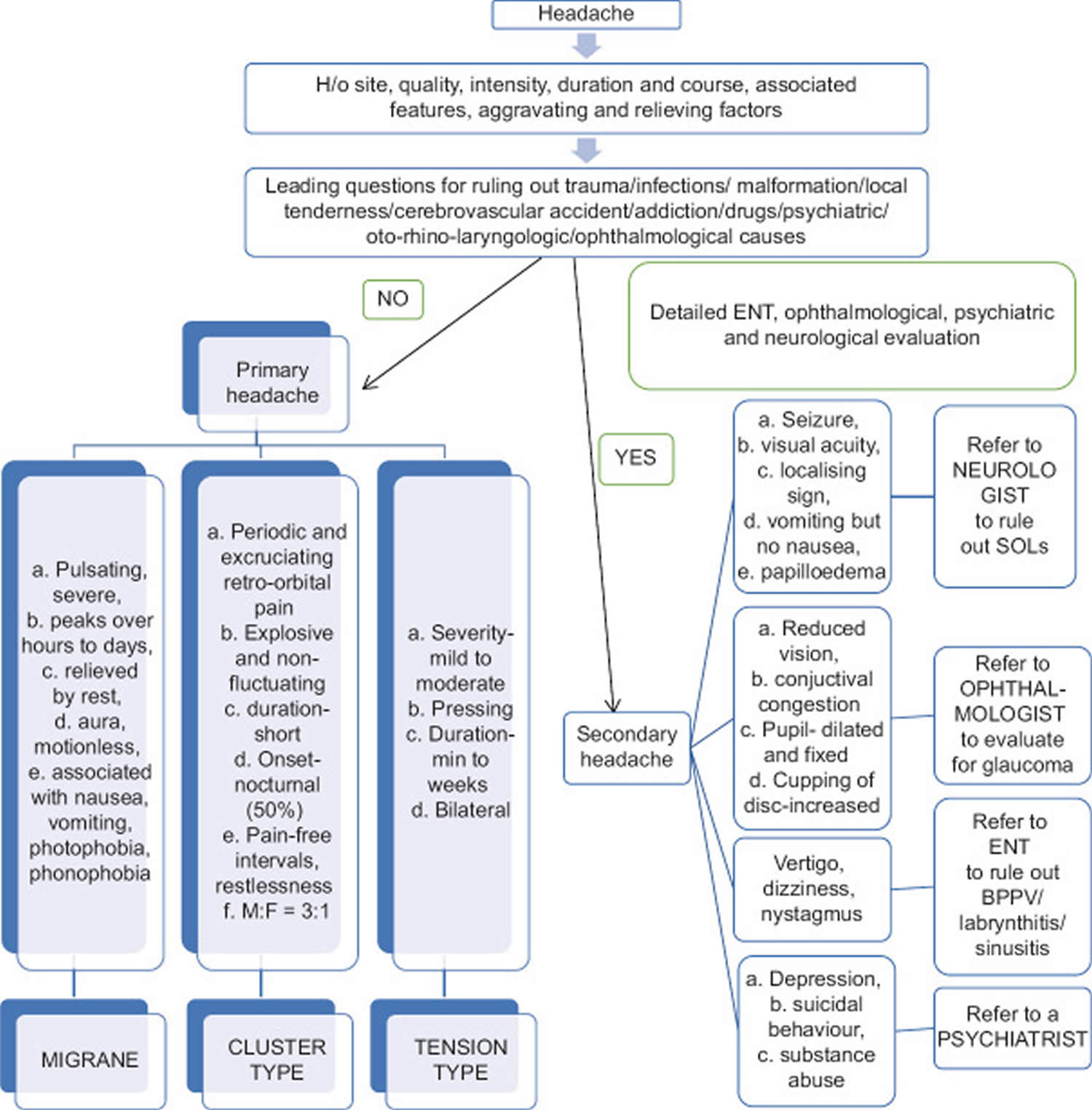
Footnotes: Distinguishing dangerous headaches from benign or low-risk headaches is a significant challenge because the symptoms can overlap 26. Recommendations for differentiating dangerous from benign headaches are provided above. The high-risk headaches are associated with certain red flag symptoms, therefore, patients showing features of secondary headaches should be examined and investigated thoroughly to rule out any high-risk pathology. Various radiological examinations are available to make this task easier, such as CT scan and MRI. MRI is much more sensitive in identifying smaller lesions 27.
[Source 28 ]Call your local emergency services number and get emergency care if:
- You are experiencing “the worst headache of your life”.
- You have speech, vision, or movement problems or loss of balance, especially if you have not had these symptoms with a headache before.
- You have headache with a fever, stiff neck, mental confusion, seizures, double vision, weakness, numbness or trouble speaking.
- The headache starts very suddenly.
- The headache occurs with repeated vomiting.
- You have a high fever.
- Your headache starts after a head injury, especially if your headache gets worse.
Also, see your doctor if:
- Your headache patterns or pain change. Even if you have a history of headaches, see your doctor if the headache pattern changes. Also see your doctor if your headaches suddenly feel different. Occasionally, headaches may be caused by a serious medical condition. These can include a brain tumor or rupture of a weakened blood vessel, known as an aneurysm.
- Treatments that once worked are no longer helpful.
- You need to take medicine for tension-type headaches more than twice a week.
- You have side effects from medicines, including irregular heartbeat, pale or blue skin, extreme sleepiness, persistent cough, depression, fatigue, nausea, vomiting, diarrhea, constipation, stomach pain, cramps, dry mouth, or extreme thirst.
- You are pregnant or could become pregnant. Some medicines should not be taken when pregnant.
Also make an appointment if tension-type headaches disrupt your life.
Tension-type headaches versus migraines
Tension-type headaches can be hard to tell apart from migraines. And if you have frequent episodic tension-type headaches, you also can have migraines. But unlike some forms of migraine, tension-type headaches usually aren’t associated with visual disturbances such as seeing bright spots or flashes of light. People with tension-type headaches also don’t usually experience nausea or vomiting with head pain. While physical activity tends to make migraine pain worse, it doesn’t affect tension-type headache pain. Sometimes a tension-type headache occurs with sensitivity to light or sound, but this symptom isn’t common.
- Tension headaches the most common type of headache—are caused by tight muscles in the shoulders, neck, scalp, and jaw. They may be related to stress, depression, or anxiety and may occur more often in people who work too much, sleep too little, miss meals, or drink alcoholic beverages.
- Migraine headaches, which affect about 12 percent of Americans, involve moderate to severe throbbing pain, often on one side of the head. During a migraine, people are sensitive to light and sound and may feel nauseated. Some people have visual disturbances before a migraine—like seeing zigzag lines or flashing lights, or temporarily losing their vision. Anxiety, stress, lack of food or sleep, exposure to light, or hormonal changes (in women) can trigger migraines. Genes that control the activity of some brain cells may play a role in causing migraines.
Tension headache causes
The cause of tension-type headaches is not known 1, 29. In the past, scientists thought tension-type headaches were caused by muscle contractions in the face, neck and scalp. They thought the muscle contractions were a result of anxiety, stress, depression, head injury, poor health, sleep disturbances or poor posture 7, 8. But research suggests that muscle contraction isn’t the cause.
The most common theory is that people who have tension-type headaches have increased sensitivity to pain. Muscle tenderness, a common symptom of tension-type headaches, may result from this sensitized pain system. Pain receptors (nociceptors) in the pericranial myofascial tissues are a likely source of tension headaches 30, 31, 2. Several studies have found that individuals who experience chronic tension-type headaches (headache occurring on greater than or equal to 15 days/month on average for >3 months) have increased sensitivity to pressure, electrical stimuli, and thermal stimuli in the pericranial myofascial tissue, and can find even normally harmless stimuli painful 31, 32, 33.
Most people experience a tension-type headache at some point in their lives. However, some research has found that women are more likely to have frequent episodic tension-type headaches and chronic tension-type headaches. Age also might play a factor. One study found that episodic tension-type headaches were more likely to affect people in their 40s.
Any activity that causes your head to be held in one position for a long time without moving can cause a headache 34. Activities may include typing or other computer work, fine work with the hands, and using a microscope. Sleeping in a cold room or sleeping with the neck in an abnormal position may also trigger a tension headache 34. However, stress is the most commonly reported trigger for tension-type headaches.
Other triggers of tension headaches include 34:
- Physical or emotional stress
- Alcohol use
- Caffeine (too much or withdrawal)
- Colds, the flu, or a sinus infection
- Dental problems such as jaw clenching or teeth grinding
- Eye strain
- Excessive smoking
- Fatigue or overexertion
Tension headaches can occur when you also have a migraine. Tension headaches are not associated with brain diseases.
Tension headaches risk factors
Most people experience a tension-type headache at some point in their lives. However, some research has found that women are more likely to have frequent episodic tension-type headaches and chronic tension-type headaches. Age also might play a factor. One study found that episodic tension-type headaches were more likely to affect people in their 40s.
Among the comorbidities that have been associated with tension type headache are:
- Genetic comorbidities 35, 36, 37, 38, 39, 40, 41, 42. Regarding genetic comorbidity, specific genes that can cause tension type headache have not yet been identified, but a possible contribution of the genotype of the 5-HTT gene-linked polymorphic region (5-HTTLPR) and the Val158Met COMT polymorphism (encoding of catechol-O-methyltransferase) in the risk of suffering from chronic tension type headache or its phenotype 35, 41, 42. Moreover, it has been suggested that the APOE-ε 4 gene could be protective against tension type headache 43.
- Bad habits 44,
- Fibromyalgia 45. Fibromyalgia has been suggested as an important comorbidity of tension type headache, with a prevalence two times higher in patients with chronic tension type headache compared to those with episodic tension type headache, which could be explained by a shared mechanism of central sensitization 45.
- Neck pain 46,
- Low back pain 47, 48,
- Migraine 14. A population study found that 83% of individuals with migraine in the last year also experienced tension-type headache 14.
Some investigations found the association of tension type headache with neck pain and low back pain, since almost 90% of people with tension type headache have comorbid neck pain 46 and approximately 80% of people with tension type headache have low back pain 48.
Increased sensitivity to pressure of the pericranial musculature has been observed in both episodic tension type headache and chronic tension type headache patients, not only during a chronic tension type headache but also on a regular basis 49, 36, 50. However, compared to episodic tension type headache patients, chronic tension type headache patients have greater sensitivity to pressure of this muscle 50, 51, 52. The literature suggests that pressure sensitivity increases proportionally to the severity and frequency of tension type headache episodes 37, 50.
Some studies indicated that the increased sensitivity to pressure of the pericranial musculature in patients with chronic tension type headache is a consequence of the progression from episodic tension type headache to chronic tension type headache and not the cause 51, 53, 50, 2.
Tension headaches pathophysiology
There have been multiple theories proposed for the presumed pathophysiology of tension type headaches, but the exact pathophysiology is unknown 3, 29. Myofascial trigger points have been implicated in the possible pathogenesis of tension type headache. Trigger points are specific areas, usually located at the level of skeletal muscles, that when pressed may be painful and elicit pain in specific areas of the body. The pericranial musculatures are the presumed trigger points for the tension type headaches. Excessive pericranial muscle contractions may lead to ischemia and the release of noxious substances, such as substance P, that may lead to further pain. Over time, these trigger points may be latent, meaning radiate pain only with palpation, or active, which causes constant pain 54. Osteopathic studies have stipulated that the tightening of the suboccipital and the upper neck musculature can lead to a “pull” of the dural matter, forming the myodural bridges, which can be very painful 55.
There is also a hypothesis that autonomic dysfunction may also play a role in the pathophysiology of tension type headache, especially due to sleep disturbance 3, 56, 57, 58, 59, 60. Sleep loss can lead to an increase in fatigue that can lead to a greater sympathetic overdrive, which would subsequently worsen or cause a headache.
Sleep apnea, insomnia, insufficient sleep, poor sleep quality, restless legs syndrome and excessive daytime sleepiness have been associated with the initiation and exacerbation of tension type headache attacks 61. Likewise, it has been suggested that sleep disorders can lead to an alteration in the functioning of the supraspinal structures related to the perception and modulation of pain in chronic tension type headache 62, 63. In this framework, it has been suggested that adequate treatment of sleep disorders and regulation of sleep/wake cycles can improve the management of tension type headache 61. However, the role of sleep disorders in the progression from episodic tension-type headache to chronic tension-type headache is still a matter of debate 2.
Tension type headaches may also occur due to dysfunction within the brain’s cortical matter. Imaging studies in patients with tension type headache have suggested a fundamental role for the anterior cingulate cortex and the insula, both areas recognized for contributing to the cognitive and affective processing of sensory information 64, 65. The trigeminal nucleus caudalis contains the nociceptive pathways of the face, which transmits pain signals to the ventral posteromedial thalamus. When stimulated with a molecule known as orexin, the nociceptive pathways within the trigeminal nucleus caudalis become inhibited. With inconsistent sleep, researchers postulate that the release of orexin becomes reduced, and therefore, less blocking of the trigeminal nucleus caudalis results in headaches 66.
There is also a role for nitric oxide (NO) mediated mechanisms for a chronic tension-type headache. Part of this is due to the treatments, which have shown that the inhibition of nitric oxide (NO) is effective in the treatment of a chronic-tension-type headache. This area is under further investigation at this time 67.
In tension type headache, it is believed that the pain experienced during the attacks is related to the malfunction of some supraspinal structures 68, 2. In patients with tension type headache, it has been found that the pain inhibitory mechanism called diffuse nociceptive inhibitory control (DNIC) does not work properly 48, 51, 50, 69, 70, 71. The diffuse nociceptive inhibitory control (DNIC) is a mechanism of the central nervous system that helps to reduce the perception of pain. In tension type headache patients, a decreased ability of the supraspinal structures to perform this task effectively has been observed, which may contribute to the onset and persistence of tension headache attacks 72, 73. However, the explanation of the factors underlying the dysfunction of the diffuse nociceptive inhibitory control (DNIC) is still being studied 74. Evidence favoring a central origin of a tension headache attack includes both psychosomatic factors and sleep disturbances that would favor activation of structures within the central nervous system at the onset of and during a tension headache attack 2.
In tension headache, nociception of the craniocervical musculature is transmitted peripherally through thin myelinated A-delta fibers and unmyelinated C fibers 75. In normal situations, thick myelinated fibers, such as the A-alpha and A-beta mechanosensitive fibers, only carry innocuous stimuli 75. However, the literature suggests that in cases of sustained sensory input from the musculature, abnormal nociception occurs not only from A-delta and C fibers, but also from low-threshold A-beta mechanosensitive fibers 75, 76. According to this concept, the increased sensitivity to pressure of the pericranial musculature in patients with tension-type headache could be due to sensitization of the peripheral nervous system as a result of sustained sensory input from the involved musculature.
Despite the fact that tension type headache constitutes one of the most common headaches, the debate as to whether tension type headache attacks are initiated by peripheral or central factors remains unresolved 75, 2.
Tension headaches prevention
Learn and practice stress management. Some people find relaxation exercises or meditation helpful. Biofeedback may help you improve the effect of doing relaxation exercises, and may be helpful for long-term (chronic) tension headache.
Tension headaches prevention tips:
- Keep warm if the headache is associated with cold.
- Use a different pillow or change sleeping positions.
- Practice good posture when reading, working, or doing other activities. Good posture can help keep your muscles from tensing. When standing, hold your shoulders back and your head level. Pull in your abdomen and buttocks. When sitting, make sure your thighs are parallel to the ground and your head isn’t slumped forward.
- Exercise the neck and shoulders frequently when working on computers or doing other close work.
- Exercise regularly. Exercise is a proven way to prevent — and sometimes treat — tension-type headaches. Exercise also provides a break from the stress of daily life. Be careful to warm up slowly. Sudden, intense exercise can cause headaches.
- Eat smart. A diet rich in fruits, vegetables and whole grains can give you more energy and help keep stress under control.
- Get plenty of sleep and rest. Stress can make it hard to sleep, but not getting enough sleep can make it harder to cope with stress. Lack of sleep stresses your body and may trigger the release of stress hormones, such as adrenaline and cortisol.
- Simplify your schedule. Rather than looking for ways to squeeze more activities or chores into the day, trim your daily to-do list. Ask yourself what really needs to be done, what can wait and what you need not do. It’s OK to say no.
- Manage your time wisely. Update your to-do list every day — both at work and at home. Delegate what you can and break large projects into manageable steps. Tackle the rest, one task at a time.
- Seek support. Talking things out with family or friends or allowing them to help you through a difficult time can help you manage stress. Talking to a therapist might also help.
- Organize your day. Anticipate challenges. Try to keep your plan flexible, in case a headache strikes and you need to change course.
- Letting go. Try not to worry about things you can’t control.
- Adjust your attitude. Encourage yourself with positive self-talk. Putting a positive spin on negative thoughts can help you work through stressful situations. If you need help with this process, consider cognitive behavioral therapy.
- Take a break. If you feel overwhelmed, take some time to clear your mind. A few slow stretches or a brisk walk may renew your energy for the task at hand. Or take a mental vacation by imagining yourself in a calm, relaxing place.
- Laugh more. Humor is a great way to relieve stress. Laughter releases endorphins, natural substances that help you feel better and maintain a positive attitude. Try watching funny movies or reading a funny book.
- Break away from your routine and try something new. A vacation or weekend getaway may help you develop a new outlook.
- Change your habits. If you smoke, quit. Cut down on caffeine and, if you drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women and up to two drinks a day for men.
Massaging sore muscles may also help.
Most headaches are nothing to worry about. But if headaches get in the way of your daily activities, work or personal life, ask your doctor for help. You may be stressed, but perhaps there’s something else going on as well.
Make healthy lifestyle choices
A healthy lifestyle can promote good overall health. It also may help prevent all types of headaches, including tension-type headaches. Here are the basics:
- Eat nutritious foods. Don’t skip meals, especially breakfast. Drink plenty of water each day.
- Exercise regularly. Exercise releases chemicals in the body that block pain signals to the brain. Talk with your health care provider about exercise and choose activities you enjoy. They might include walking, swimming or cycling. But be sure to start slowly. Exercising too intensely can cause some types of headaches.
- Get enough sleep. Wake up and go to bed at the same time every day — even on weekends. Relax before you go to bed. If you don’t fall asleep within 15 minutes, get up and read or do something soothing until you’re drowsy. Avoid medicines that contains caffeine or other stimulants that can affect sleep. This can include some headache medicines. Also keep in mind that sleep apnea can cause tension-type headaches, especially if you have headaches in the mornings. Sleep apnea is a sleep disorder in which breathing stops and starts throughout the night. Seeing a doctor and getting treatment for sleep apnea can ease its symptoms.
- Avoid large amounts of caffeine. Caffeine may help curb headaches. But heavy daily caffeine use can lead to headaches. Generally, getting more than 400 milligrams of caffeine a day — more than about four cups of coffee — can cause headaches and irritability. Regular caffeine use also increases the risk of headaches. Even quitting caffeine can cause headaches. This may happen whether you quit suddenly or cut back gradually.
- Be mindful of common pain medicines. You can buy pain medicine at the store. But using this medicine more than nine days a month can make headaches harder to treat. If this is the case, see a health care provider.
- Quit smoking. The nicotine in cigarette smoke reduces blood flow to the brain. It also triggers a reaction in the nerves at the back of the throat. These changes can lead to a headache.
Look for improvements in your headaches as you make healthy lifestyle changes.
Keep stress under control
Stress and tension-type headaches often go hand in hand. To reduce stress, try these simple tips:
- Simplify your life. Don’t look for ways to squeeze more activities or chores into the day. Instead, try to do less.
- Take a break. If you feel overwhelmed, a few slow stretches or a quick walk may help lower your stress level.
- Breathe. Take several deep breaths and count to 10 to help reduce feelings of stress.
- Adjust your attitude. Think positive thoughts. Don’t think that something is impossible. Tell yourself that you are up to the challenge.
- Let go. Don’t worry about things you can’t control.
Ease muscle tension
Tense muscles can trigger tension-type headaches. Apply heat to relieve tense neck and shoulder muscles. Use a heating pad set on low, a hot water bottle, a hot shower or bath, a warm compress, or a hot towel. Or apply ice or a cool washcloth to the forehead.
Massage also can relieve muscle tension — and sometimes headache pain. Gently massage your temples, scalp, neck and shoulders with your fingertips, or gently stretch your neck.
Relaxation
Take time to unwind every day. Try this deep-breathing exercise:
- Lie down on your back. Or sit comfortably with your feet flat on the floor and your hands in your lap.
- Imagine yourself in a peaceful place such as a beach or quiet forest. Keep this scene in your mind.
- Breathe in and out slowly and deeply for at least 10 minutes.
- When you’re done, sit quietly for a minute or two.
Try to practice these breathing exercises or another form of relaxation every day.
Preventive medicines
Your doctor may prescribe medicines that help you have fewer headaches or headaches that are less painful. Preventive medicines may help if you have regular headaches that aren’t relieved by pain medicine and other therapies.
Preventive medicines may include:
- Tricyclic antidepressants (TCAs). Tricyclic antidepressants are the most commonly used medicines to prevent tension-type headaches. They include amitriptyline, nortriptyline (Pamelor) and protriptyline. These medicines can cause side effects such as constipation, drowsiness and dry mouth.
- Other antidepressants. The antidepressants venlafaxine (Effexor XR) and mirtazapine (Remeron) also can help prevent tension-type headaches.
- Anti-seizure medicines and muscle relaxants. The anti-seizure medicines gabapentin (Gralise, Horizant, Neurontin) and topiramate (Topamax, Qsymia, others) may help prevent headache pain. But more study is needed to understand how well they work to prevent tension-type headaches. The muscle relaxant tizanidine (Zanaflex) also can be used for prevention.
It can take several weeks or more for preventive medicines to build up in your system and take effect.
Your doctor will monitor your treatment to see how the preventive medicine is working. In the meantime, overusing pain relievers may interfere with the effects of the preventive medicines. Ask your doctor about how often to use pain relievers while you’re taking preventive medicine.
Tension headache symptoms
Tension headache symptoms may be described as:
- Dull, pressure-like (not throbbing), aching head pain
- Feeling of tightness or pressure across your forehead or on the sides and back of the head.
- All over (not just in one point or one side)
- Worse in the scalp, temples, or back of the neck, and possibly in the shoulders
- Tenderness in the scalp, neck and shoulder muscles.
Tension headache pain may occur once, constantly, or daily. Tension headache pain may last for 30 minutes to 7 days. It may be triggered by or get worse with stress, fatigue, noise, or glare.
You may have difficulty sleeping. Tension headaches usually do not cause nausea or vomiting.
People with tension headaches try to relieve pain by massaging their scalp, temples, or the bottom of the neck.
There are two forms of tension-type headache:
- Episodic tension-type headaches occur between 10 and 15 days per month, with each attack lasting from 30 minutes to several days. Although the pain is not disabling, the severity of pain typically increases with the frequency of attacks.
- Chronic tension-type headaches usually occur more than 15 days per month over a three-month period. The pain, which can be constant over a period of days or months, strikes both sides of the head and is more severe and disabling than episodic headache pain. Chronic tension headaches can cause sore scalps-even combing your hair can be painful. Most individuals will have had some form of episodic tension-type headache prior to onset of chronic tension-type headache.
According to the 2018 International Classification of Headache Disorders (ICHD), chronic tension-type headache appears as a result of the natural history of an episodic tension-type headache sustained over time, with a frequency of onset of 15 or more days per month for, at least, 3 months 1.
Comparing episodic tension-type headache and chronic tension-type headache, it has been observed that headaches in patients with chronic tension-type headache are more frequent, intense, and require more medical attention 12, 13. Although there are few studies on the clinical characteristics of chronic tension-type headaches 12, 14, 15, they have been found to be similar to those of episodic tension-type headaches, except for greater pain intensity 14. In a population sample, it has been found that pain in chronic tension-type headache is bilateral in 88% of cases, of a pressure or hardening quality in 83%, and of mild or moderate intensity in 96% of cases 14. In addition, in 71% of cases, it is not aggravated by routine physical activity, and in 58%, there are no accompanying symptoms such as nausea, photophobia, or phonophobia 14.
Episodic tension-type headaches
Episodic tension-type headaches can last from 30 minutes to a week. Frequent episodic tension-type headaches occur less than 15 days a month for at least three months. Episodic tension-type headaches can become chronic. Although the pain is not disabling, the severity of pain typically increases with the frequency of attacks.
Chronic tension-type headaches
Chronic tension-type headaches last for hours and may be constant. Chronic tension-type headaches occur 15 or more days a month for at least three months. The pain, which can be constant over a period of days or months, strikes both sides of the head and is more severe and disabling than episodic headache pain. Chronic tension headaches can cause sore scalps-even combing your hair can be painful. Most individuals will have had some form of episodic tension-type headache prior to onset of chronic tension-type headache.
Tension headaches complications
Because tension-type headaches are so common, they can have an effect on job productivity and quality of life, particularly if they’re chronic. Frequent headache pain may make it hard to attend activities. You might need to stay home from work. If you do go to your job, it may be hard to function as usual.
Tension headache diagnosis
If you suffer from frequent headaches, your doctor may give you a physical and a neurological exam. Your doctor works to pinpoint the type and cause of your headaches using following approaches:
Your pain description. Your doctor can learn a lot about your headaches from the information you provide about the pain. Be sure to include these details:
- Pain description. Is the pain throbbing? Is it constant and dull? Is it sharp or stabbing?
- Pain intensity. A good indicator of pain intensity is how much you’re able to do during the headache. Are you able to work? Do headaches wake you or prevent you from sleeping?
- Pain location. Do you feel pain all over your head? Is the pain on one side of your head? Or is the pain only on your forehead or behind your eyes?
Once your doctor reviews your medical and headache history and conducts physical and neurological exams, lab screening and diagnostic tests may be ordered to either rule out or identify conditions that might be the cause of your headaches.
Blood and urine tests can help diagnose brain or spinal cord infections, blood vessel damage, and toxins that affect the nervous system. Testing the fluid that surrounds the brain and spinal cord can detect infections, bleeding in the brain called a brain hemorrhage, and measure any buildup of pressure within the skull.
Imaging tests
Your doctor may order tests to rule out serious causes of headache, such as a brain tumor. Two common imaging tests include:
- Magnetic resonance imaging (MRI). An MRI scan is done using a powerful magnet and computer-generated radio waves to create images of your brain.
- Computerized tomography (CT). A CT scan combines a series of X-ray images taken from different angles. It creates cross-sectional images to provide a detailed view of your brain.
Diagnostic imaging, such as with computed tomography (CT) and magnetic resonance imaging (MRI), can detect irregularities in blood vessels and bones, certain brain tumors and cysts, brain damage from head injury, brain hemorrhage, inflammation, infection, and other disorders. Neuroimaging also gives doctors a way to see what’s happening in the brain during headache attacks. An electroencephalogram (EEG) measures brain wave activity and can help diagnose brain tumors, seizures, head injury, and inflammation that may lead to headaches.
Tension type headache diagnostic criteria
The 2018 International Classification of Headache Disorders (ICHD) 3rd edition proposed tension type headache diagnostic criteria 1:
- At least ten episodes of headache fulfilling criteria B-D
- Lasting from 30 minutes to as long as seven days
- Minimally two of the following four characteristics:
- Bilaterally located
- Pressing or tightening (non-pulsating) quality
- Mild or moderate in intensity
- Not exacerbated by routine physical activity, e.g., walking or climbing stairs.
- Both of the following:
- No nausea or vomiting
- No more than one of photophobia or phonophobia
- They are not better explained by another ICHD-3 diagnosis.
The above is a general 2018 International Classification of Headache Disorders (ICHD) 3rd edition diagnostic criterion for the tension type headache. If one of the above ICHD-3 features for tension type headache is missing and not fulfilling the criteria for another headache disorder, a diagnosis of probable tension-type headache is possible. These patients with probable tension type headache should undergo evaluation over time, and the clinician usually makes a diagnosis of tension type headache in these patients. tension type headaches are further subdivided into three subtypes based on the frequency of headache episodes 1.
- Infrequent episodic tension type headache: At least ten episodes of headache occurring on <1 day/month on average (<12 days/year).
- Frequent episodic tension type headache: At least ten episodes of headache occurring on 1 to 14 days/month on average for over 3 months (≥12 and <180 days/year).
- Chronic tension type headache: Headache occurring on ≥15 days/month on average for >3 months (≥180 days/year).
Tension headaches differential diagnosis
Tension headaches are often difficult to differentiate from high-risk headaches (secondary headaches) because there are overlapping signs and symptoms 26. The high-risk headaches (secondary headache disorders) are associated with certain red flag symptoms. Some causes of secondary headaches include giant cell arteritis, sleep apnea headache, cardiac cephalgia, cervicogenic headaches, etc. Therefore, patients showing features of secondary headaches should be examined and investigated thoroughly to rule out any high-risk pathology. Various radiological examinations are available to make this task easier, such as CT scan and MRI. MRI is much more sensitive in identifying smaller lesions.
Tension headaches differential diagnosis include the following 3:
- Migraine. Migraine is the second most common cause of primary headache disorders and requires differentiation from tension type headache because of different treatment options. Migraine headaches are moderate to severe in intensity and last for 4 to 72 hours in duration. Migraine headaches may be unilateral in location and typically have a pulsating or throbbing quality. They are also aggravated by routine physical activity. Nausea, vomiting, photophobia, and phonophobia are commonly associated with migraine headaches. A preceding aura may also be present in some of these patients.
- Medication overuse headache. Medication overuse headache is another important headache type to exclude. It may be present in concomitance with tension type headache or other headache disorders. It may mimic chronic tension type headache, therefore, making the diagnoses and treatment more difficult. The patient often takes analgesic medicines > 10 to 15 days a month. Patients may complain of headaches upon awakening that transiently responds to analgesics and returns as the drug effect wears off. These patients may also appear anxious, irritable, and restless. Discontinuing the overused analgesics medication is the primary treatment, which the patient needs to understand.
- Hypnic headache. Hypnic headache is a less frequent occurrence, which tends to have an onset of >50 years. Hypnic headaches will only occur during sleep and will typically wake the patient up. Since older adults also have a higher risk in general of developing secondary headaches, it is important to distinguish primary from secondary headaches within this subset of patients; this should be done in all age groups with risk factors, as discussed below.
Table 1. Tension headaches differential diagnosis
| Condition | Symptoms | Signs | Investigation |
|---|---|---|---|
| Cervicogenic headache 9 | Non-throbbing headache, starting in the neck Duration- varied | Precipitated by movement, reduced range of neck movement, neck/shoulder/arm pain- ipsilateral, no side shift | X-ray |
| Giant cell arteritis 9, 77 | Age at onset >50 years Onset- abrupt unilateral/bilateral headache, scalp tenderness, visual symptoms- diplopia, blurred vision/loss, limb claudication, constitutional symptoms- fever, malaise, fatigue, weight loss | Tender, thickened, reduced pulsation in superficial temporal artery, scalp tenderness, visual field defect, vascular bruit | ESR >50 mm/h Arterial biopsy- vasculitis characterised by mononuclear cell infiltration, multinucleated giant cells Fundoscopy Optic disc- pale and swollen with haemorrhage |
| Idiopathic intracranial hypertension 77 | Daily, non-pulsating, diffuse headache increased by coughing, straining | Papilloedema, visual field defect, enlarged blind spot, sixth nerve palsy | LP-CSF pressure >200 mm of H2O (non-obese) >250 mm of H2O (obese) MRI, CT |
| Post-traumatic headache 77 | Headache except any typical features within 7 days after head trauma | CT with bone window images X-ray- fracture, ligamentous injury of spine, subluxation Cranial MRI- focal contusion- non-haemorrhagic | |
| Subarachnoid hemorrhage 78 | Intense, incapacitating abrupt-onset headache associated with vomiting | Neck rigidity, altered mentation | CT scan & MRI (magnetic resonance imaging) – hemorrhage CSF examination if scan is normal Angiography |
| Central venous thrombosis 78 | Headache with no specific features | Seizure, signs of raised intracranial tension, focal neurological signs | MRI along with magnetic resonance venography (MRV) venous thrombosis |
| Trigeminal neuralgia 79 | Unilateral, onset- abrupt, electric shock-like sensations, duration- seconds to 2 min, along distribution of the fifth cranial nerve (second, third divisions), pain induced by washing, brushing, smoking, talking | Neurological deficit- absent | MRI- vascular/non-vascular Compression of fifth cranial nerve |
| Acute glaucoma | Painful red eye, sudden blindness/blurred vision | Clouding of cornea, conjunctival injection, visual disturbances | Elevated intraocular pressure>28 mmHg |
| Acute sinusitis | Frontal headache, pain in ear, face and teeth | Sinus tenderness | Elevated ESR, polymorphonuclear leucocytosis Pus culture- organism isolated X-ray- shadow/fluid level |
Abbreviations: CSF = cerebrospinal fluid; CT = computed tomography; ESR = erythrocyte sedimentation rate; IOP = intraocular pressure; MRI=magnetic resonance imaging; LP-CSF = Lumbar puncture-cerebro-spinal fluid; MRV = Magnetic resonance venography
[Source 28 ]Tension headache treatment
Some people with tension-type headaches don’t see their doctor and try to treat the headache on their own. But repeated use of pain medications available without a prescription can cause another type of headache known as medication overuse headache. Your doctor can work with you to find the right treatment for your headaches.
Tension headache remedy
A tension headache occurs when neck and scalp muscles become tense or contract. The muscle contractions can be a response to stress, depression, a head injury, or anxiety. When you have a tension headache hot or cold showers or baths may relieve the headache for some people. Applying heat or ice — whichever you prefer — to sore muscles may ease a tension-type headache. For heat, use a heating pad set on low, a hot-water bottle, a warm compress or a hot towel. For cold, wrap ice, an ice pack or frozen vegetables in a cloth to protect your skin.
You may also want to rest in a quiet room with a cool cloth on your forehead. Gently massaging your head and neck muscles may also provide relief. If your headaches are due to stress or anxiety, you may want to learn ways to relax. One way to help reduce stress is by planning ahead and organizing your day. Another way is to allow more time to relax.
Over-the-counter pain medicine, such as aspirin, ibuprofen, or acetaminophen, may relieve pain. If you are planning to take part in an activity that you know will trigger a headache, taking pain medicine beforehand may help.
Avoid smoking and drinking alcohol.
Follow your doctor’s instructions about how to take your medicines. Rebound headaches are headaches that keep coming back. They can occur from overuse of pain medicine. If you take pain medicine more than 3 days a week on a regular basis, you can develop rebound headaches.
Be aware that aspirin and ibuprofen (Advil, Motrin) can irritate your stomach. If you take acetaminophen (paracetamol), DO NOT take more than a total of 4,000 mg (4 grams) of regular strength or 3,000 mg (3 grams) of extra strength a day to avoid liver damage.
Dietary supplements
Butterbur is derived from the leaves of Petasites hybridus that grows in Europe and parts of Asia and North America 80. The name, butterbur, is attributed to the traditional use of its large leaves to wrap butter in warm weather. Butterbur appears to help reduce the frequency of migraines in adults and children 81, 82, 83, 84. In 2012, the American Academy of Neurology recommended its use for preventing migraines 85, 86. One major area of concern regarding butterbur safety is with pyrrolizidine alkaloids which are commonly found in the butterbur plant 87. Pyrrolizidine alkaloids can cause hepatotoxicity, lung toxicity, carcinogenesis, and thrombosis. Fortunately, the commercial preparation process of butterbur typically removes these substances. Therefore, it is recommended for consumers of butterbur only buy brands that are free of alkaloids and other plant carcinogens 80.
Severe liver damage may be associated with butterbur use, but the evidence is unclear 80. From the World Health Organization’s Vigibase, one study reported 40 cases of liver damage, including two liver transplants associated with the use of Petasites formulations 88. However, these cases may be the result of the use of butterbur contaminated with pyrrolizidine alkaloids. Another article reported detecting levels of toxic alkaloids in seven out of 21 commercially available compounds 88. Therefore, at least some brands are inadequately removing pyrrolizidine alkaloids from their butterbur formulations. In summary, it is unclear if liver damage is due to alkaloids in the formulation or the butterbur itself. To evaluate the hepatotoxic effects of butterbur more clearly, a future study can collect data on brands that claim to be alkaloid-free by thoroughly reviewing the literature and the Periodic Update Safety Report. The data can then be analyzed with the Roussel Uclaf Causality Assessment Method test to determine if butterbur carries an association with liver damage 89. Butterbur use is contraindicated in patients using anticholinergic medications. Also, there have not been studies establishing safety criteria in children under six or pregnant or lactating women. Therefore, butterbur use is not recommended in these groups 87. If you are considering using butterbur, discuss its risks and benefits with your health care provider.
There is some evidence that coenzyme Q10, feverfew, magnesium, and the B vitamin riboflavin might be helpful for reducing the frequency of migraines. However, for all of these supplements, the amount of evidence is small. A recent study of foods rich in omega-3 fatty acids found that they may reduce the frequency and severity of migraines, but studies of omega-3 fatty acid supplementation have not shown the same effects.
Tension-type headache medicines
Several medicines can help reduce the pain of a headache. They include medicines you can buy at the store without a prescription and medicines available with a prescription.
- Pain relievers. Pain relievers available without a prescription are usually the first line of treatment for reducing headache pain. These include aspirin, ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve).
- Combination medicines. Aspirin, acetaminophen (Tylenol, others) or both are often combined with caffeine or a sedative in a single medicine. Combination medicines may be more effective than single-ingredient pain relievers. Many combination medicines are available without a prescription.
- Triptans. For people who experience both migraines and episodic tension-type headaches, a triptan can effectively relieve the pain of both headaches.
Prescription opioids are rarely used because of their side effects and potential for addiction.
Episodic tension type headache treatment
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the mainstay treatment options to abort episodes of tension type headache. Recent metanalysis studies suggest that ibuprofen 400 mg and acetaminophen 1000 mg are the best pharmacological agents for acute treatment of tension type headache. There appears to be a synergistic effect of these two drugs together, as the number needed to treat for an additional beneficial outcome with ibuprofen alone was greater than that of both ibuprofen + acetaminophen in combination treatment. While aspirin alone is used frequently over the counter for treatment, a 500 mg dose showed to be equivalent to placebo 90. Other NSAIDs (e.g. naproxen sodium [375 to 550 mg], ketoprofen [25 to 50 mg], and diclofenac [50 to 100 mg] etc.) are also more effective than placebo in acute tension type headache. Patients should avoid the overuse of analgesic medicines as it may, ironically, lead to medication overuse headache. Evidence for the efficacy of muscle relaxants in tension type headache is weak, and there is a risk for habituation.
Chronic tension type headache treatment
The goal of chronic tension type headache therapy is to reduce the frequency of headaches through the use of preventive medications. Among pharmacologic agents, amitriptyline (a tricyclic antidepressant [TCA]), is the most efficacious and well-studied drug in the management of chronic tension type headache. Amitriptyline should be started on a low dose (10 to 25 mg daily) and slowly titrated (10 to 25 mg weekly) till achieving an appropriate therapeutic response, or the adverse effects appear. The therapeutic response usually occurs in 3 to 4 weeks. In responsive patients, amitriptyline usually continues for at least six months, and then withdrawal may be attempted. In case of recurrence of chronic tension type headache on withdrawal, amitriptyline may be continued long term. Adverse effects are common and include dry mouth, drowsiness, urinary retention, cardiac arrhythmias, and glaucoma 5.
Selective serotonin reuptake inhibitors (SSRIs) and serotonin/norepinephrine reuptake inhibitors (SNRIs) were not as effective as tricyclic antidepressants (TCAs) 5.
Evidence for the efficacy of muscle relaxants in tension type headache is weak, and there is a risk for habituation 5.
Unlike chronic migraine, botulinum toxin type A has varying efficacy in different studies for chronic tension type headache prevention and is usually not recommended as a first-line treatment. However, in refractory chronic tension type headache cases, a trial of botulinum toxin A may be given 5.
Non-pharmacological treatment
The best non-pharmacological therapy for chronic tension type headache are physical therapy, biofeedback, and cognitive-behavioral therapy 91. Relaxation, exercise programs, and improvement of posture are critical components of physical therapy. Several other treatments, including massage, manipulation, acupuncture, and osteopathic manipulative medicine, have also shown improvement in both acute and chronic presentations, using measures such as increasing range of motion of the head.
Tension headache prognosis
The prognosis of tension type headache is usually good. Most people respond with treatment. In a Danish study of 549 people, approximately half of the patients with episodic tension type headache experienced remission, and about 15% progressed to newly developed chronic tension type headache which can interfere with life and work 92. Frequent episodes of tension type headache or chronic tension type headache can lead to absent days and reduced work productivity. It may also result in increased stress and mood disorders.
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018 Jan;38(1):1-211. doi: 10.1177/0333102417738202[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Ashina S, Mitsikostas DD, Lee MJ, Yamani N, Wang SJ, Messina R, Ashina H, Buse DC, Pozo-Rosich P, Jensen RH, Diener HC, Lipton RB. Tension-type headache. Nat Rev Dis Primers. 2021 Mar 25;7(1):24. doi: 10.1038/s41572-021-00257-2[↩][↩][↩][↩][↩][↩][↩]
- Shah N, Hameed S. Muscle Contraction Tension Headache. [Updated 2023 Jul 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562274[↩][↩][↩][↩]
- de Tommaso M, Fernández-de-Las-Penas C. Tension Type Headache. Curr Rheumatol Rev. 2016;12(2):127-39. doi: 10.2174/1573397112666151231113625[↩]
- Chowdhury D. Tension type headache. Ann Indian Acad Neurol. 2012 Aug;15(Suppl 1):S83-8. doi: 10.4103/0972-2327.100023[↩][↩][↩][↩][↩]
- Derry S, Wiffen PJ, Moore RA, Bendtsen L. Ibuprofen for acute treatment of episodic tension-type headache in adults. Cochrane Database Syst Rev. 2015 Jul 31;2015(7):CD011474. doi: 10.1002/14651858.CD011474.pub2[↩]
- Lenaerts ME. Burden of tension-type headache. Curr Pain Headache Rep. 2006 Dec;10(6):459-62. doi: 10.1007/s11916-006-0078-z[↩][↩][↩]
- Chin J, Qiu W, Lomiguen CM, Volokitin M. Osteopathic Manipulative Treatment in Tension Headaches. Cureus. 2020 Dec 12;12(12):e12040. doi: 10.7759/cureus.12040[↩][↩][↩]
- Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004;24 Suppl 1:9-160. doi: 10.1111/j.1468-2982.2003.00824.x[↩][↩][↩]
- Stovner Lj, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher A, Steiner T, Zwart JA. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007 Mar;27(3):193-210. doi: 10.1111/j.1468-2982.2007.01288.x[↩]
- Schwartz BS, Stewart WF, Simon D, Lipton RB. Epidemiology of tension-type headache. JAMA. 1998 Feb 4;279(5):381-3. doi: 10.1001/jama.279.5.381[↩]
- Gobel H, Petersen-Braun M, Soyka D. The epidemiology of headache in Germany: a nationwide survey of a representative sample on the basis of the headache classification of the International Headache Society. Cephalalgia. 1994;14(2):97–106. doi: 10.1046/j.1468-2982.1994.1402097.x[↩][↩][↩][↩]
- Rasmussen BK, Jensen R, Olesen J. Impact of headache on sickness absence and utilisation of medical services: a Danish population study. J Epidemiology Community Health. 1992;46(4):443–446. doi: 10.1136/jech.46.4.443[↩][↩]
- Rasmussen BK, Jensen R, Schroll M, Olesen J. Epidemiology of headache in a general population–a prevalence study. J Clin Epidemiol. 1991;44(11):1147–1157. doi: 10.1016/0895-4356(91)90147-2[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Aaseth K, Grande RB, Lundqvist C, Russell MB. Pericranial tenderness in chronic tension-type headache: the Akershus population-based study of chronic headache. J Headache Pain. 2014;15(1):1–7. doi: 10.1186/1129-2377-15-58[↩][↩]
- Edlow JA, Panagos PD, Godwin SA, Thomas TL, Decker WW; American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with acute headache. Ann Emerg Med. 2008 Oct;52(4):407-36. doi: 10.1016/j.annemergmed.2008.07.001[↩]
- Wijeratne T, Wijeratne C, Korajkic N, Bird S, Sales C, Riederer F. Secondary headaches – red and green flags and their significance for diagnostics. eNeurologicalSci. 2023 Jun 30;32:100473. doi: 10.1016/j.ensci.2023.100473[↩]
- Headache. https://www.ninds.nih.gov/health-information/disorders/headache[↩]
- Clinch CR. Evaluation of acute headaches in adults. Am Fam Physician. 2001 Feb 15;63(4):685-92. https://www.aafp.org/pubs/afp/issues/2001/0215/p685.html[↩]
- Massage Therapy: What You Need To Know. https://www.nccih.nih.gov/health/massage-therapy-what-you-need-to-know[↩]
- Headaches: What You Need To Know. https://www.nccih.nih.gov/health/headaches-what-you-need-to-know[↩]
- Acupuncture: What You Need To Know. https://www.nccih.nih.gov/health/acupuncture-what-you-need-to-know[↩]
- Tai Chi: What You Need To Know. https://www.nccih.nih.gov/health/tai-chi-what-you-need-to-know[↩]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. doi:10.1177/0333102417738202[↩]
- Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders: 3rd Edition. Abbreviated pocket version for reference by professional users only https://ihs-headache.org/wp-content/uploads/2020/05/ICHD-3-Pocket-version.pdf[↩]
- Hainer BL, Matheson EM. Approach to acute headache in adults. Am Fam Physician. 2013 May 15;87(10):682-7. https://www.aafp.org/pubs/afp/issues/2013/0515/p682.html[↩][↩]
- Edmeads J. Emergency management of headache. Headache. 1988 Nov;28(10):675-9. doi: 10.1111/j.1526-4610.1988.hed2810675.x[↩]
- Ravan JR, Pattnaik JI, Samantray S. Algorithm-based approach to headache. J Family Med Prim Care. 2023 Sep;12(9):1775-1783. doi: 10.4103/jfmpc.jfmpc_1553_22[↩][↩]
- Repiso-Guardeño Á, Moreno-Morales N, Labajos-Manzanares MT, Rodríguez-Martínez MC, Armenta-Peinado JA. Does Tension Headache Have a Central or Peripheral Origin? Current State of Affairs. Curr Pain Headache Rep. 2023 Nov;27(11):801-810. doi: 10.1007/s11916-023-01179-2[↩][↩]
- Ashina M. Neurobiology of chronic tension-type headache. Cephalalgia. 2004 Mar;24(3):161-72. doi: 10.1111/j.1468-2982.2003.00644.x[↩]
- Bendtsen L, Fernández-de-la-Peñas C. The role of muscles in tension-type headache. Curr Pain Headache Rep. 2011 Dec;15(6):451-8. doi: 10.1007/s11916-011-0216-0[↩][↩]
- Fernández-de-Las-Peñas C, Cuadrado ML, Arendt-Nielsen L, Ge HY, Pareja JA. Increased pericranial tenderness, decreased pressure pain threshold, and headache clinical parameters in chronic tension-type headache patients. Clin J Pain. 2007 May;23(4):346-52. doi: 10.1097/AJP.0b013e31803b3770[↩]
- Buchgreitz L, Lyngberg AC, Bendtsen L, Jensen R. Frequency of headache is related to sensitization: a population study. Pain. 2006 Jul;123(1-2):19-27. doi: 10.1016/j.pain.2006.01.040[↩]
- Tension headache. https://medlineplus.gov/ency/article/000797.htm[↩][↩][↩]
- Fernández-de-Las-Peñas C, Ambite-Quesada S, Palacios-Ceña M, Guillem-Mesado A, Guerrero-Peral Á, Pareja JA, et al. Catechol-O-methyltransferase [COMT] rs4680 Val158Met polymorphism is associated with widespread pressure pain sensitivity and depression in women with chronic, but not episodic, tension-type headache. Clin J Pain. 2019;35(4):345–352. doi: 10.1097/AJP.0000000000000684[↩][↩]
- Jensen R, Rasmussen BK, Pedersen B, Olesen J. Muscle tenderness and pressure pain thresholds in headache. A population study. Pain. 1993 Feb;52(2):193-199. doi: 10.1016/0304-3959(93)90131-8[↩][↩]
- Ulrich V, Gervil M, Olesen J. The relative influence of environment and genes in episodic tension-type headache. Neurology. 2004;62(11):2065–2069. doi: 10.1212/01.WNL.0000129498.50793.8A[↩][↩]
- Russell MB, Levi N, Kaprio J. Genetics of tension-type headache: a population based twin study. Am J Med Genet B Neuropsychiatric Gen. 2007;144(8):982–986. doi: 10.1002/ajmg.b.30497[↩]
- Russell MB, Šaltytš-Benth J, Levi N. Are infrequent episodic, frequent episodic and chronic tension-type headache inherited? A population-based study of 11 199 twin pairs. J Headache Pain. 2006;7:119–126. doi: 10.1007/s10194-006-0299-x[↩]
- Ostergaard S, Russell MB, Bendtsen L, Olesen J. Comparison of first degree relatives and spouses of people with chronic tension headache. BMJ. 1997;314(7087):1092–1093. doi: 10.1136/bmj.314.7087.1092[↩]
- Park JW, Kim JS, Lee HK, Kim YI, Lee KS. Serotonin transporter polymorphism and harm avoidance personality in chronic tension-type headache. Headache. 2004 Nov-Dec;44(10):1005-9. doi: 10.1111/j.1526-4610.2004.04194.x[↩][↩]
- Fernández-de-las-Peñas C, Ambite-Quesada S, Rivas-Martínez I, Ortega-Santiago R, de-la-Llave-Rincón AI, Fernández-Mayoralas DM, Pareja JA. Genetic contribution of catechol-O-methyltransferase polymorphism (Val158Met) in children with chronic tension-type headache. Pediatr Res. 2011 Oct;70(4):395-9. doi: 10.1203/PDR.0b013e318229448a[↩][↩]
- Gupta R, Kumar V, Luthra K, Banerjee B, Bhatia MS. Polymorphism in apolipoprotein E among migraineurs and tension-type headache subjects. J Headache Pain. 2009;10(2):115–120. doi: 10.1007/s10194-008-0094-y[↩]
- Schramm SH, Obermann M, Katsarava Z, Diener HC, Moebus S, Yoon MS. Epidemiological profiles of patients with chronic migraine and chronic tension-type headache. J Headache Pain. 2013 May 7;14(1):40. doi: 10.1186/1129-2377-14-40[↩]
- De Tommaso M, Federici A, Serpino C, Vecchio E, Franco G, Sardaro M, et al. Clinical features of headache patients with fibromyalgia comorbidity. J Headache Pain. 2011;12(6):629–638. doi: 10.1007/s10194-011-0377-6[↩][↩]
- Ashina S, Bendtsen L, Lyngberg AC, Lipton RB, Hajiyeva N, Jensen R. Prevalence of neck pain in migraine and tension-type headache: a population study. Cephalalgia. 2015;35(3):211–219. doi: 10.1177/0333102414535110[↩][↩]
- Yoon M-S, Manack A, Schramm S, Fritsche G, Obermann M, Diener H-C, et al. Chronic migraine and chronic tension-type headache are associated with concomitant low back pain: results of the German Headache Consortium study. Pain. 2013;154(3):484–492. doi: 10.1016/j.pain.2012.12.010[↩]
- Ashina S, Lipton R, Bendtsen L, Hajiyeva N, Buse D, Lyngberg A, et al. Increased pain sensitivity in migraine and tension-type headache coexistent with low back pain: a cross-sectional population study. Eur J Pain. 2018;22(5):904–914. doi: 10.1002/ejp.1176[↩][↩][↩]
- Sakai F, Ebihara S, Akiyama M, Horikawa M. Pericranial muscle hardness in tension-type headache: a non-invasive measurement method and its clinical application. Brain. 1995;118(2):523–531. doi: 10.1093/brain/118.2.523[↩]
- Langemark M, Jensen K, Jensen TS, Olesen J. Pressure pain thresholds and thermal nociceptive thresholds in chronic tension-type headache. Pain. 1989;38(2):203–210. doi: 10.1016/0304-3959(89)90239-X[↩][↩][↩][↩][↩]
- Bendtsen L, Jensen R, Olesen J. Decreased pain detection and tolerance thresholds in chronic tension-type headache. Arch Neurol. 1996;53(4):373–376. doi: 10.1001/archneur.1996.00550040113021[↩][↩][↩]
- Schoenen J, Bottin D, Hardy F, Gerard P. Cephalic and extracephalic pressure pain thresholds in chronic tension-type headache. Pain. 1991;47(2):145–149. doi: 10.1016/0304-3959(91)90198-7[↩]
- Fernández-de-Las-Peñas C, Cuadrado ML, Arendt-Nielsen L, Ge H-Y, Pareja JA. Increased pericranial tenderness, decreased pressure pain threshold, and headache clinical parameters in chronic tension-type headache patients. Clin J Pain. 2007;23(4):346–352. doi: 10.1097/AJP.0b013e31803b3770[↩]
- Do TP, Heldarskard GF, Kolding LT, Hvedstrup J, Schytz HW. Myofascial trigger points in migraine and tension-type headache. J Headache Pain. 2018 Sep 10;19(1):84. doi: 10.1186/s10194-018-0913-8[↩]
- Lee E, Moloney S, Talsma J, Pierce-Talsma S. Osteopathic Manipulative Treatment Considerations in Tension-Type Headache. J Am Osteopath Assoc. 2019 Oct 1;119(10):e40-e41. doi: 10.7556/jaoa.2019.096[↩]
- Ashina S, Bendtsen L, Buse D, Lyngberg A, Lipton R, Jensen R. Neuroticism, depression and pain perception in migraine and tension-type headache. Acta Neurol Scand. 2017;136(5):470–476. doi: 10.1111/ane.12751[↩]
- Ødegård SS, Engstrøm M, Sand T, Stovner LJ, Zwart J-A, Hagen K. Associations between sleep disturbance and primary headaches: the third Nord-Trøndelag Health Study. JHeadache Pain. 2010;11:197–206. doi: 10.1007/s10194-010-0201-8[↩]
- Kim J, Cho S-J, Kim W-J, Yang KI, Yun C-H, Chu MK. Insomnia in tension-type headache: a population-based study. J Headache Pain. 2017;18(1):1–9. doi: 10.1186/s10194-017-0805-3[↩]
- Ødegård SS, Sand T, Engstrøm M, Zwart JA, Hagen K. The impact of headache and chronic musculoskeletal complaints on the risk of insomnia: longitudinal data from the Nord-Trøndelag health study. J Headache Pain. 2013 Mar 12;14(1):24. doi: 10.1186/1129-2377-14-24[↩]
- Song TJ, Cho SJ, Kim WJ, Yang KI, Yun CH, Chu MK. Anxiety and Depression in Tension-Type Headache: A Population-Based Study. PLoS One. 2016 Oct 26;11(10):e0165316. doi: 10.1371/journal.pone.0165316[↩]
- Cho S-J, Song T-J, Chu MK. Sleep and tension-type headache. Curr Neurol Neurosci Rep. 2019;19:1–9. doi: 10.1007/s11910-019-0953-8[↩][↩]
- Engstrøm M, Hagen K, Bjørk M, Stovner L, Stjern M, Sand T. Sleep quality, arousal and pain thresholds in tension-type headache: a blinded controlled polysomnographic study. Cephalalgia. 2014;34(6):455–463. doi: 10.1177/0333102413515339[↩]
- Fernández-de-Las-Peñas C, Fernández-Muñoz JJ, Palacios-Ceña M, Parás-Bravo P, Cigarán-Méndez M, Navarro-Pardo E. Sleep disturbances in tension-type headache and migraine. TherAdvNeurolDisord. 2018;11:1–6. doi: 10.1177/1756285617745444[↩]
- Schmidt-Wilcke T, Leinisch E, Straube A, Kampfe N, Draganski B, Diener HC, et al. Gray matter decrease in patients with chronic tension type headache. Neurology. 2005;65(9):1483–1486. doi: 10.1212/01.wnl.0000183067.94400.80[↩]
- Chen WT, Chou KH, Lee PL, Hsiao FJ, Niddam DM, Lai KL, Fuh JL, Lin CP, Wang SJ. Comparison of gray matter volume between migraine and “strict-criteria” tension-type headache. J Headache Pain. 2018 Jan 15;19(1):4. doi: 10.1186/s10194-018-0834-6[↩]
- Sullivan DP, Martin PR, Boschen MJ. Psychological Sleep Interventions for Migraine and Tension-Type Headache: A Systematic Review and Meta-Analysis. Sci Rep. 2019 Apr 23;9(1):6411. doi: 10.1038/s41598-019-42785-8[↩]
- Ashina S, Bendtsen L, Ashina M. Pathophysiology of tension-type headache. Curr Pain Headache Rep. 2005 Dec;9(6):415-22. doi: 10.1007/s11916-005-0021-8[↩]
- Bendtsen L, Jensen R. Tension-type headache. Neurol Clin. 2009;27(2):525–535. doi: 10.1016/j.ncl.2008.11.010[↩]
- Sait A, Lars B, Messoud A. Pathophysiology of tension-type headache. Curr Pain Headache Rep. 2005;9(6):415–422. doi: 10.1007/s11916-005-0021-8[↩]
- Palacios-Ceña M, Wang K, Castaldo M, Guillem-Mesado A, Ordás-Bandera C, Arendt-Nielsen L, et al. Trigger points are associated with widespread pressure pain sensitivity in people with tension-type headache. Cephalalgia. 2018;38(2):237–245. doi: 10.1177/0333102416679965[↩]
- Ashina S, Bendtsen L, Ashina M, Magerl W, Jensen R. Generalized hyperalgesia in patients with chronic tension-type headache. Cephalalgia. 2006;26(8):940–948. doi: 10.1111/j.1468-2982.2006.01150.x[↩]
- Sandrini G, Rossi P, Milanov I, Serrao M, Cecchini A, Nappi G. Abnormal modulatory influence of diffuse noxious inhibitory controls in migraine and chronic tension-type headache patients. Cephalalgia. 2006;26(7):782–789. doi: 10.1111/j.1468-2982.2006.01130.x[↩]
- Ashina M. Neurobiology of chronic tension-type headache. Cephalalgia. 2004;24(3):161–172. doi: 10.1111/j.1468-2982.2003.00644.x[↩]
- Rossi P, Vollono C, Valeriani M, Sandrini G. The contribution of clinical neurophysiology to the comprehension of the tension-type headache mechanisms. Clin Neurophysiol. 2011 Jun;122(6):1075-85. doi: 10.1016/j.clinph.2010.12.061[↩]
- Steel SJ, Robertson CE, Whealy MA. Current Understanding of the Pathophysiology and Approach to Tension-Type Headache. Curr Neurol Neurosci Rep. 2021 Oct 2;21(10):56. doi: 10.1007/s11910-021-01138-7[↩][↩][↩][↩]
- Woolf CJ, Doubell TP. The pathophysiology of chronic pain—increased sensitivity to low threshold Aβ-fibre inputs. Curr Opin Neurobiol. 1994;4(4):525–534. doi: 10.1016/0959-4388(94)90053-1[↩]
- Harrison TR, Longo DL, Dan L. Harrison’s Manual of Medicine. New York, USA: mcgraw-hil; 2013. p. 550.[↩][↩][↩]
- Ravishankar K, Chakravarty A, Chowdhury D, Shukla R, Singh S. Guidelines on the diagnosis and the current management of headache and related disorders. Ann Indian Acad Neurol. 2011 Jul;14(Suppl 1):S40-59. doi: 10.4103/0972-2327.83100[↩][↩]
- Chakravarty A, Mukherjee A, Roy D. Trigeminal autonomic cephalgias and variants: clinical profile in Indian patients. Cephalalgia. 2004 Oct;24(10):859-66. doi: 10.1111/j.1468-2982.2004.00759.x[↩]
- Din L, Lui F. Butterbur. [Updated 2023 Jun 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537160[↩][↩][↩]
- Butterbur. https://www.nccih.nih.gov/health/butterbur[↩]
- Malone M, Tsai G. The evidence for herbal and botanical remedies, Part 1. J Fam Pract. 2018 Jan;67(1):10-16. https://www.mdedge.com/familymedicine/article/155077/pain/evidence-herbal-and-botanical-remedies-part-1[↩]
- Orr SL. The Evidence for the Role of Nutraceuticals in the Management of Pediatric Migraine: a Review. Curr Pain Headache Rep. 2018 Apr 4;22(5):37. doi: 10.1007/s11916-018-0692-6[↩]
- Wells RE, Beuthin J, Granetzke L. Complementary and Integrative Medicine for Episodic Migraine: an Update of Evidence from the Last 3 Years. Curr Pain Headache Rep. 2019 Feb 21;23(2):10. doi: 10.1007/s11916-019-0750-8[↩]
- Holland S, Silberstein SD, Freitag F, Dodick DW, Argoff C, Ashman E; Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Evidence-based guideline update: NSAIDs and other complementary treatments for episodic migraine prevention in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2012 Apr 24;78(17):1346-53. doi: 10.1212/WNL.0b013e3182535d0c[↩]
- Diener H, Freitag F, Danesch U. Safety profile of a special butterbur extract from Petasites hybridus in migraine prevention with emphasis on the liver. Cephalalgia Reports. 2018;1. doi:10.1177/2515816318759304[↩]
- D’Andrea G, Cevoli S, Cologno D. Herbal therapy in migraine. Neurol Sci. 2014 May;35 Suppl 1:135-40. doi: 10.1007/s10072-014-1757-x[↩][↩]
- Rajapakse T, Pringsheim T. Nutraceuticals in Migraine: A Summary of Existing Guidelines for Use. Headache. 2016 Apr;56(4):808-16. doi: 10.1111/head.12789[↩][↩]
- Chen CW. [Carefully reviewing the history of diagnostic scales and paying more attention to the diagnostic value of Roussel – Uclaf causality assessment method scale for drug – induced liver injury]. Zhonghua Gan Zang Bing Za Zhi. 2016 Nov 20;24(11):801-803. Chinese. doi: 10.3760/cma.j.issn.1007-3418.2016.11.001[↩]
- Moore RA, Wiffen PJ, Derry S, Maguire T, Roy YM, Tyrrell L. Non-prescription (OTC) oral analgesics for acute pain – an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015 Nov 4;2015(11):CD010794. doi: 10.1002/14651858.CD010794.pub2[↩]
- Steger B, Rylander E. HelpDesk Answers: What treatments best prevent chronic tension headaches? J Fam Pract. 2015 Aug;64(8):493, 501. https://www.mdedge.com/familymedicine/article/101505/pain/what-treatments-best-prevent-chronic-tension-headaches[↩]
- Lyngberg AC, Rasmussen BK, Jørgensen T, Jensen R. Incidence of primary headache: a Danish epidemiologic follow-up study. Am J Epidemiol. 2005 Jun 1;161(11):1066-73. doi: 10.1093/aje/kwi139[↩]





{kind=link}