
Contents
- What are Carbs (Carbohydrate) ?
- What happens when you eat foods containing carbohydrates ?
- How much carbohydrate do you need each day ?
- How can you find out how much carbohydrate is in the foods you eat ?
- What is Low Carb Diet
- Table 1. Summary of Popular Low-Carbohydrate Diets 5
- Low-Carb Diet: Can it help you lose weight ?
- Table 4. Low-Carbohydrate Diet and Weight Loss
- Low-Carbohydrate Diets versus Low-Fat Diets on Metabolic Risk Factors
- Low Carb Diet details
- Typical foods for a low-carb diet
- 1) Low Carb Atkins Diet vs Zone Diet vs LEARN Diet vs Ornish Diet for Weight loss
What are Carbs (Carbohydrate) ?
There are three main types of carbohydrate (carbs) in food.
- Starches (also known as complex carbohydrates)
- Sugars
- Fiber
You’ll also hear terms like naturally occurring sugar, added sugar, low-calorie sweeteners, sugar alcohols, reduced-calorie sweeteners, processed grains, enriched grains, complex carbohydrate, sweets, refined grains and whole grains.
No wonder knowing what kind and how much carbohydrate to eat can be confusing !
On the nutrition label, the term “total carbohydrate” includes all three types of carbohydrates. This is the number you should pay attention to if you are carbohydrate counting for your low carb dieting.
What happens when you eat foods containing carbohydrates ?
When you eat foods containing carbohydrates, your digestive system breaks down the sugars and starches into glucose. Glucose is one of the simplest forms of sugar. Glucose then enters your bloodstream from your digestive tract and raises your blood glucose levels. The hormone insulin, which comes from the pancreas or from insulin shots, helps cells throughout your body absorb glucose and use it for energy. Once glucose moves out of the blood into cells, your blood glucose levels go back down.
How much carbohydrate do you need each day ?
How much carbohydrate you eat is very individual. Finding the right amount of carbohydrate depends on many things including how active you are (sedentary lifestyle or elite athlete), your body weight (healthy weight or overweight or obese) and what, if any, medicines you take. Some people are active and can eat more carbohydrate. You may need to have less carbohydrate to keep your blood glucose in control 1.
The daily amount of carbohydrate ~ 130 grams of carbohydrate / day, (protein, and fat) for Americans can be found in the U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th Edition. December 2015 2. Experts suggest that carbohydrate intake for most people should be between 45 and 65 percent of total calories. People on low-calorie diets and people who are physically inactive may want to aim for the lower end of that range 2.
You and your health care team can figure out the right amount for you. Once you know how much carb to eat at a meal, choose your food and the portion size to match.
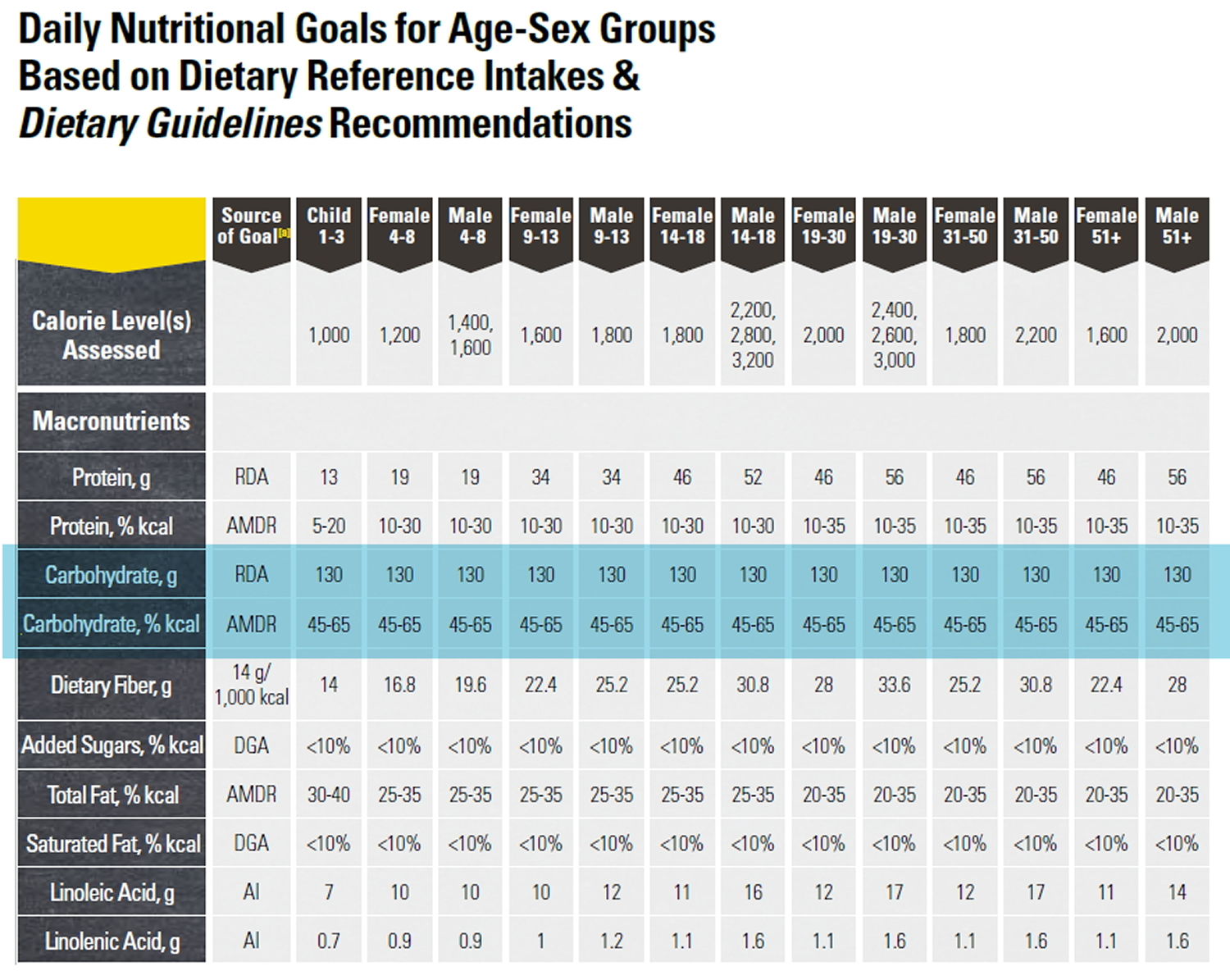
Table of Daily Dietary Reference Intake for Carbohydrate, Protein and Fat (source 2).
However, the daily amount of carbohydrate, protein, and fat for people with diabetes has not been defined—what is best for one person may not be best for another. Everyone needs to get enough carbohydrate to meet the body’s needs for energy, vitamins and minerals, and fiber. Finding the balance for yourself is important so you can feel your best, do the things you enjoy, and lower your risk of diabetes complications. A place to start is at about 45-60 grams of carbohydrate at a meal. You may need more or less carbohydrate at meals depending on how you manage your diabetes 1.
One gram of carbohydrate provides about 4 calories, so you’ll have to divide the number of calories you want to get from carbohydrates by 4 to get the number of grams. For example, if you want to eat 1,800 total calories per day and get 45 percent of your calories from carbohydrates, you would aim for about 200 grams of carbohydrate daily.
You would calculate that amount as follows:
.45 x 1,800 calories = 810 calories
810 ÷ 4 = 202.5 grams of carbohydrate
You’ll need to spread out your carbohydrate intake throughout the day. A dietitian or diabetes educator can help you learn what foods to eat, how much to eat, and when to eat based on your weight, activity level, medicines, and blood glucose targets.
- Nutrition Labels
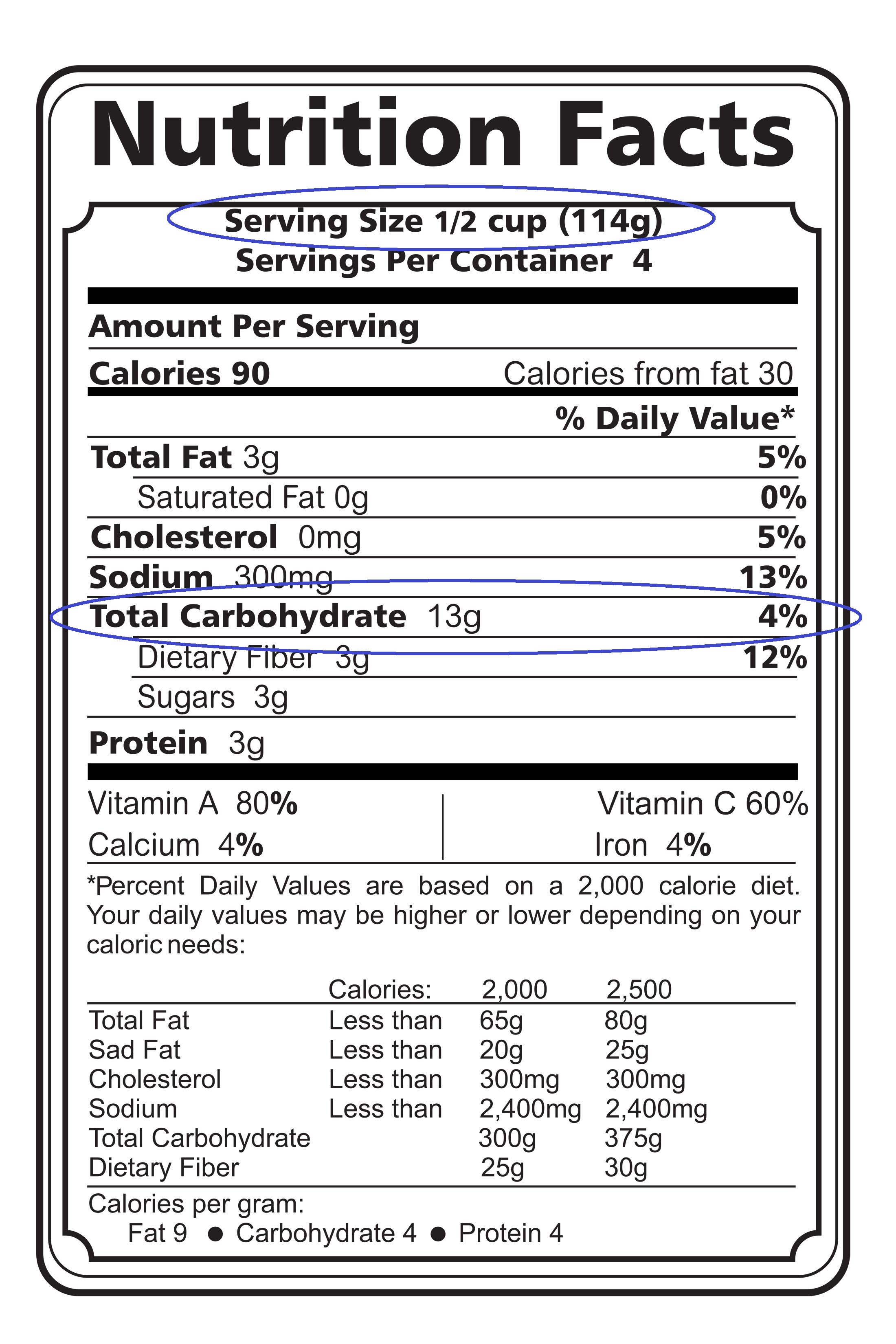
You can find out how many grams of carbohydrate are in the foods you eat by checking the nutrition labels on food packages.
Nutrition labels tell you
- the food’s serving size––such as one slice or 1/2 cup
- the total grams of carbohydrate per serving
- other nutrition information, including calories and the amount of protein and fat per serving
If you have two servings instead of one, such as one cup of pinto beans instead of 1/2 cup, you multiply the number of grams of carbohydrate in one serving—for example, 15—by two to get the total number of grams of carbohydrate—30.
15 x 2 = 30
Following is an example of a nutrition label:
How can you find out how much carbohydrate is in the foods you eat ?
To find out the amount of carbohydrate in homemade foods, you’ll need to estimate and add up the grams of carbohydrate from the ingredients. You can use books or websites that list the typical carbohydrate content of homemade items to estimate the amount of carbohydrate in a serving.
You can also weigh foods with a scale or measure amounts with measuring cups or spoons to estimate the amount of carbohydrate. For example, if a nutrition label shows that 1 1/2 cups of cereal contain 45 grams of carbohydrate, then 1/2 cup will have 15 grams of carbohydrate and 1 cup will have 30 grams of carbohydrate.
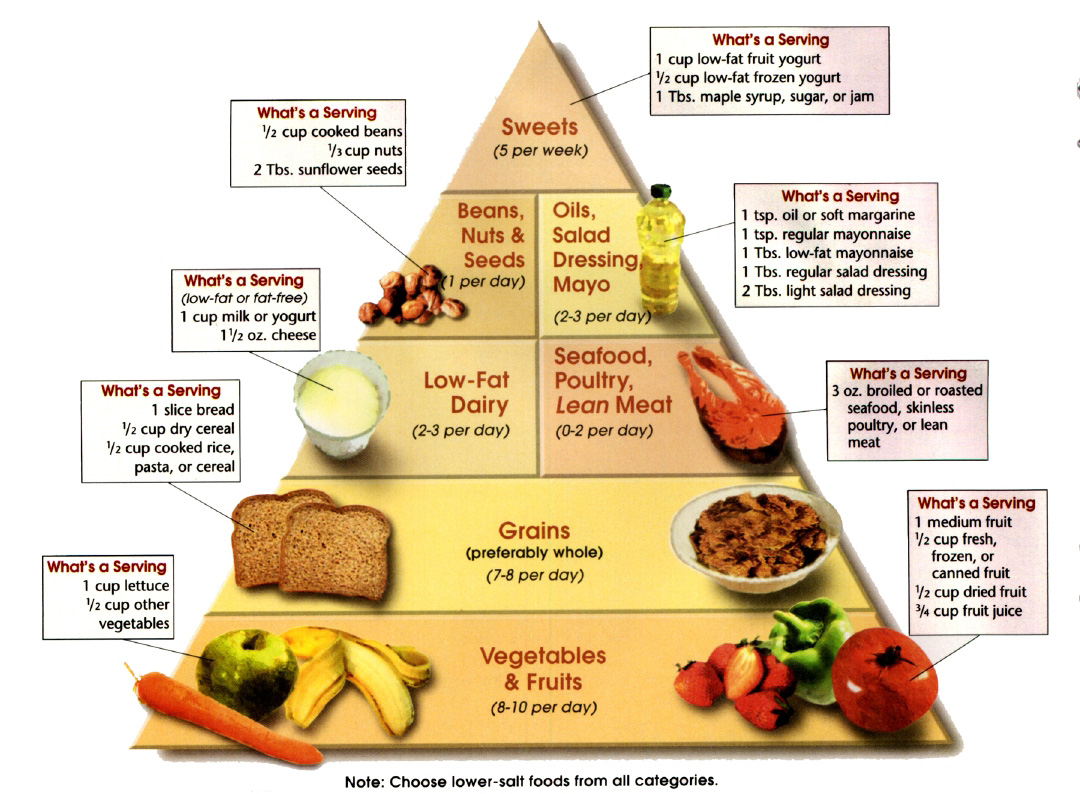
You will need to learn to estimate the amount of carbohydrate in foods you typically eat. For example, the following amounts of carbohydrate-rich foods each contain about 15 grams of carbohydrate:
- one slice of bread
- one 6-inch tortilla
- 1/3 cup of pasta
- 1/3 cup of rice
- 1/2 cup of canned or fresh fruit or fruit juice or one small piece of fresh fruit, such as a small apple or orange
- 1/2 cup of pinto beans
- 1/2 cup of starchy vegetables such as mashed potatoes, cooked corn, peas, or lima beans
- 3/4 cup of dry cereal or 1/2 cup cooked cereal
- 1 tablespoon of jelly
- 1 small piece of fresh fruit (4 oz)
- 1/2 cup of canned or frozen fruit
- 1 slice of bread (1 oz) or 1 (6 inch) tortilla
- 1/2 cup of oatmeal
- 1/3 cup of pasta or rice
- 4-6 crackers
- 1/2 English muffin or hamburger bun
- 1/2 cup of black beans or starchy vegetable
- 1/4 of a large baked potato (3 oz)
- 2/3 cup of plain fat-free yogurt or sweetened with sugar substitutes
- 2 small cookies
- 2 inch square brownie or cake without frosting
- 1/2 cup ice cream or sherbet
- 1 Tbsp syrup, jam, jelly, sugar or honey
- 2 Tbsp light syrup
- 6 chicken nuggets
- 1/2 cup of casserole
- 1 cup of soup
- 1/4 serving of a medium french fry
Some foods are so low in carbohydrates that you may not have to count them unless you eat large amounts. For example, most nonstarchy vegetables are low in carbohydrates. A 1/2-cup serving of cooked nonstarchy vegetables or a cup of raw vegetables has only about 5 grams of carbohydrate.
As you become familiar with which foods contain carbohydrates and how many grams of carbohydrate are in food you eat, carbohydrate counting will be easier.
What is Low Carb Diet
A low-carbohydrate diet was first characterized by William Banting in the 1860s 3) and this type of diet has currently received much attention due to Dr. Atkins’ New Diet Revolution 4). The Atkins’ Diet recommends two weeks of extreme carbohydrate restriction, followed by gradually increasing carbohydrates to 35 g/day. The Atkins’ Diet has 68% of total calories from fat, 27% from protein, and 5% from carbohydrates 5. Other popular low-carbohydrate diets are summarized in Table 1.
Table 1. Summary of Popular Low-Carbohydrate Diets 5
| The Atkins’ Diet |
| 68% fat, 27% protein, 5% carbohydrates |
| <35 g carbohydrate per day |
| Protein Power |
| 54% fat, 26% protein, 16% carbohydrates |
| The Zone Diet |
| 30% fat, 40% protein, 30% carbohydrates |
Low-carbohydrate diets recommend limiting complex and simple sugars, causing the body to oxidize fat to meet energy requirements. During the initial carbohydrate restriction, the body resorts to ketosis for energy needs. Ketones are excreted in the urine with fluid. Rapid initial weight loss may be from this diuretic effect 5, which can be encouraging.
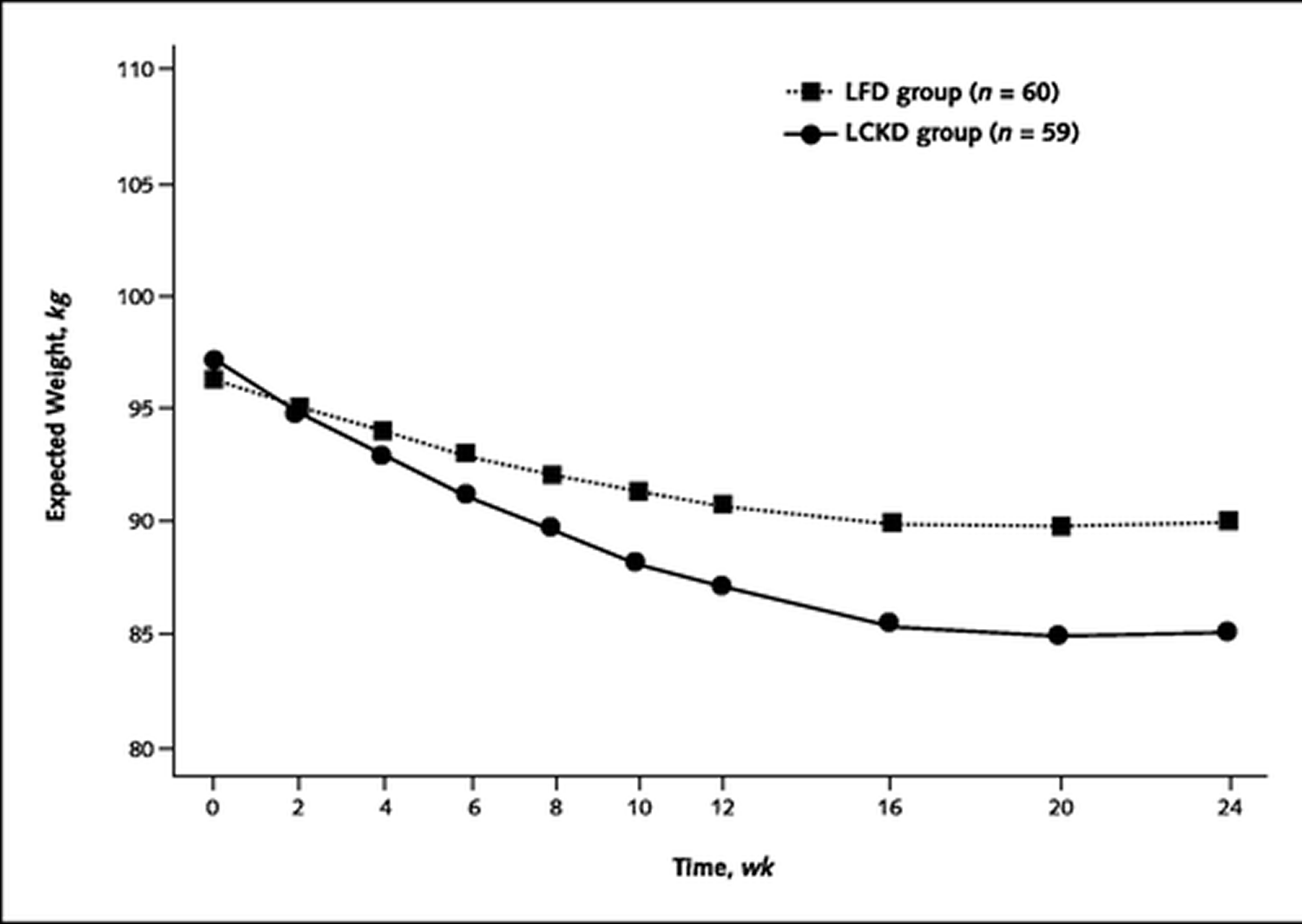
In a small randomized, controlled trial with 120 overweight comparing low-carbohydrate ketogenic diet (also known as low-carb high fat diet) versus a low-fat diet over 24 weeks to treat obesity and hyperlipidemia involving hyperlipidemic volunteers from the community 6. Participants in the low-carb ketogenic diet were restricted to intake of carbohydrates to less than 20 g/d and were permitted unlimited amounts of animal foods (meat, fowl, fish, and shellfish), unlimited eggs, 4 oz of hard cheese, 2 cups of salad vegetables (such as lettuce, spinach, or celery), and 1 cup of low-carbohydrate vegetables (such as broccoli, cauliflower, or squash) daily. On the other hand the low-fat diet group was restricted to less than 30% of daily energy intake from fat, less than 10% of daily energy intake from saturated fat, and less than 300 mg of cholesterol daily and calorie intake was 500 to 1000 kcal less than the participant’s calculated energy intake for weight maintenance. Restriction of dietary intake of carbohydrates (low-carbohydrate ketogenic diet) to less than 40 g/d typically results in ketonuria that is detectable by urine dipstick analysis, which can be used to monitor adherence to the low-carbohydrate diet. Patients in both groups lost substantially more fat mass (change, -9.4 kg with the low-carbohydrate ketogenic diet vs. -4.8 kg with the low-fat diet) than lean body mass (change, -3.3 kg vs. -2.4 kg, respectively) (see Figure 1 below). Low-carbohydrate ketogenic diet had greater decreases in serum triglyceride levels and greater increases in high-density (HDL) “good” lipoprotein cholesterol levels. Changes in low-density (LDL) “bad” lipoprotein cholesterol level did not differ statistically between the diets. Minor adverse effects were more frequent in the low-carbohydrate diet group, such as constipation, headache, halitosis, muscle cramps, diarrhea, general weakness and rash 6.
Figure 1. Body weight loss over 24 weeks, by diet group. LFD: Low Fat Diet and LCKD: Low Carb Ketogenic Diet (Source 6)
A drastic reduction in carbohydrates also leads to an overall decrease in caloric intake 7. Even when calories are not actively restricted, low-carbohydrate dieters consume fewer calories compared with baseline 8. Weight loss can be sustained by this reduction in caloric intake. Although palatable for the short term, low-carbohydrate diets raise several nutritional and cardiovascular concerns, as summarized in Table 2.
Table 2. Low-Carbohydrate Diet Pros and Cons
| Pros | Cons |
|---|---|
| Initial weight loss | High-protein diet |
| Diuretic effect | Calcium balance |
| Palatable diet | Renal and hepatic complications |
| Easier to maintain | Potentially atherogenic |
| Caloric restriction | High in saturated fat and cholesterol |
| Reason for weight loss? | |
| Low in fruits, vegetables, and whole grains |
Table 2 summarizes the positive and negative aspects of low-carbohydrate diets. Adapted from data in references 4), 9, 10, 11.

Low-Carb Diet: Can it help you lose weight ?
A low-carb diet limits carbohydrates — such as those found in grains, starchy vegetables and fruit — and emphasizes foods high in protein and fat. Many types of low-carb diets exist. Each diet has varying restrictions on the types and amounts of carbohydrates you can eat.
A low-carb diet is generally used for losing weight. Some low-carb diets may have health benefits beyond weight loss, such as reducing risk factors associated with diabetes and metabolic syndrome.
Research shows Americans have increased their carb consumption in recent years, but they’re not eating the right kind of carbohydrates. They’re not eating a lot more fruit. They’re eating a lot more liquid calories, such as sweet juice-like drinks and sodas.
Terms such as “low carb” or “net carbs” often appear on product labels, but the Food and Drug Administration (FDA) doesn’t regulate these terms, so there’s no standard meaning. Typically net carbs is used to mean the amount of carbohydrates in a product excluding fiber or excluding both fiber and sugar alcohols. To add to the confusion, there is no legal definition of what “low-carb” means. Any food or beverage product that says “low-carb” on the label is technically breaking the law, but the FDA has generally only issued a warning letter to offenders.
Therefore, any definition of low-, reduced-, or net carb is entirely up to the manufacturer. And manufacturers are using this terminology, and it really doesn’t mean anything. But one thing is clear: low-carb doesn’t mean low calorie !
You probably have also heard talk about the glycemic index. The glycemic index classifies carbohydrate-containing foods according to their potential to raise your blood sugar level.
Weight-loss diets based on the glycemic index typically recommend limiting foods that are higher on the glycemic index. Foods with a relatively high glycemic index ranking include potatoes and corn, and less healthy options such as snack foods and desserts that contain refined flours. Many healthy foods, such as whole grains, legumes, vegetables, fruits and low-fat dairy products, are naturally lower on the glycemic index.
Although low fat and energy-restricted diets are generally recommended for obese and overweight individuals 12, 13 1S- 40S. http://onlinelibrary.wiley.com/doi/10.1038/oby.2001.113/abstract;jsessionid=BE222215A3449DCE32557CA68A507841.f03t03)), low-carbohydrate, high-protein diets are one of the most popular alternative weight loss approaches 14. However, because low carbohydrate diets derive large proportions of calories from protein and fat, there has been considerable concern for their potentially detrimental impact on cardiovascular risk 15. Increased consumption of fat, particularly saturated fat, has been linked to increased plasma concentrations of lipids 16, 17, 18, 19, insulin resistance, glucose intolerance 20, 21, and obesity 22, 23. Therefore, it is possible that many Americans could actually suffer adverse health effects by using very low carbohydrate diets in an attempt to lose weight.
To evaluate the effects of a very low carbohydrate diet on weight loss and cardiovascular risk factors, the researchers 24 randomized 53 healthy obese women to 6 months of a very low carbohydrate diet or a calorie-restricted, low fat diet conforming to the guidelines currently recommended by the American Heart Association and other expert panels 25.
In that randomized clinical trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women 24. One group of dieters was instructed to follow a low carb diet of their own choosing with a maximum intake of 20 g carbohydrate/day. It was anticipated that this diet would induce ketosis. After 2 wk of dieting, subjects were permitted to increase their intake of carbohydrate to 40–60 g/d only if self-testing of urinary ketones continued to indicate ketosis. The other group of dieters was instructed on a calorie-restricted, moderately low fat diet with a recommended macronutrient distribution of 55% carbohydrate, 15% protein, and 30% fat. Calorie prescriptions were based on body size and calculated using the Harris-Benedict equation 26.
Two registered dietitians delivered a 3-month intervention aimed at promoting dietary compliance. Group meetings with subjects on the same diet were held biweekly on the University of Cincinnati campus and addressed cooking tips, stress management, behavior modification, and relapse prevention. On alternating weeks, subjects met for individual counseling sessions during which their assigned dietitian reviewed their 3-day food records from the previous week, analyzed by Nutritionist V (First Data Bank, San Bruno, CA), and provided dietary recommendations and positive reinforcement. Subjects were advised to continue their baseline level of activity. To control for possible bias, each dietitian was assigned subjects from each diet group for counseling and alternated as the meeting facilitator for both groups of dieters. Before each weekly session, subjects submitted 3-day food records and were weighed on a single electronic scale. Blood pressure was measured, and assessment of urinary ketones was performed using Ketostix. At the end of the 3-month intervention, subjects were instructed to continue with their weight loss efforts, but without scheduled contact with the dietitians until the 6-month assessment.
Results: Body weight and body fat in the low fat and very low carbohydrate groups were similar at baseline. Although caloric intakes in the two groups were similar, the proportions of carbohydrate, protein, and fat consumed differed dramatically.
- After the initiation of the diets, both groups had a decrease in body weight that was more rapid in the earlier weeks of observation and became less pronounced as the study progressed (see Low Carb Diet vs Low Fat Diet – Weight Loss Graph below). Most diets that have a significant restriction of calories cause a sodium diuresis or was due to decreased body water, presumably accompanying depletion of stored glycogen, that occurs over the first wk or 2 of their use 27, 28. In fact, it was noted the most rapid weight loss in both groups occur over this period. The low fat diet group lost 1.6 kg in the first 2 wk, representing 38% of their mean weight loss during the first 3 months of the study. The very low carbohydrate group lost 3.0 kg during the first 2 wk, or 39% of their mean 3-month weight loss. In analyzing the body composition at 3 and 6 months of dieting, well after the expected period of diuresis – the analysis of body composition showed that the weight lost in the very low carbohydrate diet group consisted of a similar percentage of fat mass as in the low fat diet group. Thus, the authors think it is very unlikely that differences in weight between the two groups at 3 and 6 months are a result of disproportionate changes in body water in the very low carbohydrate dieters.
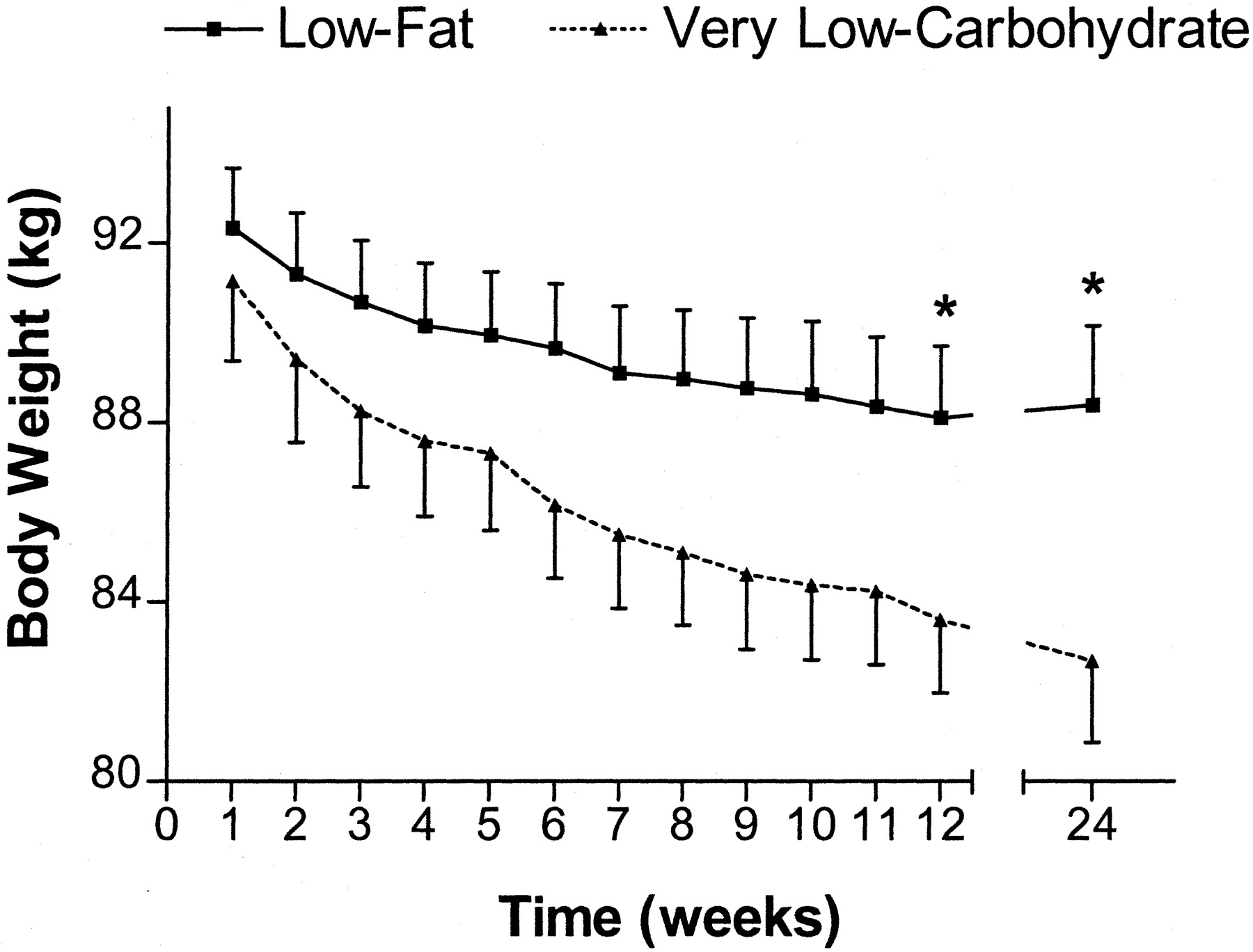
(Source 24).
- Both fat mass and fat-free mass decreased significantly in the two groups over the course of the trial. However, similar to body weight, fat mass and lean body mass decreased significantly more in the very low carbohydrate group compared with the low fat group at both 3 and 6 months. The reduced fat mass comprised 50–60% of the weight lost in both groups. There were no changes in bone mineral content over the course of the study. Body composition data for the two groups of women are shown in Table 3. The women in the very low carbohydrate group lost an average of 7.6 ± 0.7 kg after 3 months and 8.5 ± 1.0 kg after 6 months of diet. Women following the low fat diet lost 4.2 ± 0.8 and 3.9 ± 1.0 kg at 3 and 6 months, respectively.
- Cardiovascular risk factors: There were no electrocardiographic (EKG) abnormalities in any of the subjects during the study. The blood pressures in the two groups were within the normal range at the outset of the study and remained so throughout the study. Significant differences in blood pressure were not found between the groups during the study.
- Plasma Lipids: Mean plasma concentrations of total cholesterol, triglycerides, LDL cholesterol, and HDL cholesterol were normal in each of the two groups before starting the diets. A significant reduction was found for plasma triglycerides (148.73 (mg/dl) at baseline to 113.86 (mg/dl) a 23.44 percent reduction in 6 months; Low Fat Diet Group 109.25 (mg/dl) at baseline to 111.00 (mg/dl) unchanged in 6 months) , but the researchers put the significant difference in triglycerides was probably due to a difference between the groups at baseline. Differences in total cholesterol and HDL cholesterol between the groups were not detected at the 3- or 6-month assessments. Significantly were the diet effects for all of the plasma lipids indicated that the subjects improved their lipid profiles during the course of the study, with significant decreases in total cholesterol, LDL cholesterol, and triglycerides at 3 months and significant increases in HDL cholesterol at 6 months.
- Fasting hormones and substrates: Fasting glucose and insulin did not differ between the two groups at the 3- or 6-month assessments. However, significant time effects for glucose and insulin indicate that the glucose and insulin levels decreased significantly in the women on both diets over the 6-month study. There were no differences in leptin levels between the two groups. Yet a significant time effect shows that plasma leptin levels decreased significantly in both groups of subjects at 3 months. A significant difference between the groups was detected for plasma β-hydroxybutyrate, with this ketone increasing significantly more in the very low carbohydrate group at 3 months. Weekly testing of urinary ketones was positive in the majority of subjects on the very low carbohydrate diet and negative in those on the low fat diet.
- At 3 months, caloric intake in the very low carbohydrate diet group was distributed as 15% carbohydrate, 28% protein, and 57% fat.
- In contrast, the low fat diet group had daily calories distributed as 54% carbohydrate, 18% protein, and 28% fat.
- At 3 months, the very low carbohydrate diet group consumed significantly less carbohydrate, vitamin C, and fiber and significantly more protein, total fat, saturated fat, monounsaturated fat, polyunsaturated fat, and cholesterol than the low fat diet group.
- At 6 months, the two groups still differed significantly for most of these measures.
- 42 of the 53 subjects (79%) completed the 6-month study, with 4 dropouts from the very low carbohydrate diet group and 7 dropouts from the low fat diet group. The majority of subjects discontinuing the study cited difficulty maintaining the scheduled visits as the primary reason, and follow-up measurements were obtained for only 1 of the these women. For subjects missing a follow-up visit, their last recorded weight is included in the calculation of the group mean. One subject from each diet group dropped out due to dislike for their assigned diet.
Table 3. Means of body composition measures of women before and after 3 and 6 months of dieting | ||
Very low carbohydrate diet group (n=22) | Low Fat diet group (n = 20) | |
Body fat (kg) | ||
Baseline | 37.327 kg | 37.827 kg |
3 months | 33.035 kg | 35.305 kg |
6 months | 32.554 kg | 35.853kg |
Lean body mass (kg) | ||
Baseline | 50.385 kg | 51.026 kg |
3 months | 47.565 kg | 50.181 kg |
6 months | 48.418 kg | 50.295kg |
Bone mineral content (kg) | ||
Baseline | 2.782 kg | 2.819 kg |
3 months | 2.799 kg | 2.827 kg |
6 months | 2.775 kg | 2.792 kg |
(Source 24) | ||
Summary: The results of this study demonstrate that a very low carbohydrate diet, taken without a specified restriction of caloric intake, is effective for weight loss over a 6-month period in healthy, obese women. However, the mechanism of the enhanced weight loss in the very low carbohydrate diet group relative to the low fat diet group is not clear. One possibility could be that the very low carbohydrate group could be consuming approximately 300 fewer calories/day over the first 3 months relative to the low fat diet group and that it is possible also that the women in the very low carbohydrate diet group exercised more than those in the low fat diet group. Additionally, it is possible that consuming a very low carbohydrate diet increases resting basal metabolic rate (Resting BMR) or postprandial energy expenditure. Although it has been proposed that ketosis developing from severe carbohydrate intake contributes to a decrease in appetite 29. Although the women following the very low carbohydrate diet developed significant ketonemia, the elevation of circulating β-hydroxybutyrate was mild, well below what is seen in other clinical states of ketosis, such as starvation and diabetic ketoacidosis 30, 31 and was noted only at 3 months. In addition, there was no correlation between the level of plasma β-hydroxybutyrate and weight loss.
In addition, despite eating a high percentage of calories as fat and having relatively high intakes of saturated fat and cholesterol, the women in the very low carbohydrate group maintained normal levels of blood pressure, plasma lipids, glucose, and insulin. These data suggest that the deleterious effects of diets containing a high percentage of fat on body weight and cardiac risk factors are mitigated by restriction of caloric intake and associated weight loss.
Several points of caution need to be emphasized. Firstly, whether the very low carbohydrate diet will produce sustained weight loss and continued improvement in cardiovascular risk factors over longer periods of time remains to be determined. Secondly, increased dietary saturated fat has been linked to certain types of cancer 32 and may have effects on cardiovascular health beyond the risk factors assessed in this study 18.
The possibility that differences in the macronutrient composition of the diet alter energy expenditure is an interesting question that bears further investigation 4), 9, 10, 11.
A recent meta-analysis 33 of randomized controlled trials comparing the effects of low-carbohydrate diets without restriction of energy intake vs low-fat diets in individuals with a body mass index (calculated as weight in kilograms divided by the square of height in meters) of at least 25 on weight loss, blood pressure, and their lipid values in randomized controlled trials with diet interventions for at least 6 months. The review comparing the effects of a low-carbohydrate diet (defined as a diet allowing a maximum intake of 60 g of carbohydrates per day) without energy intake restriction vs a low-fat diet (defined as a diet allowing a maximum of 30% of the daily energy intake from fat) with energy intake restriction in individuals with a body mass index (BMI) of at least 25. The review conclusions were that low-carbohydrate, non–energy-restricted diets appear to be at least as effective as low-fat, energy-restricted diets in inducing weight loss for up to 1 year. However, potential favorable changes in triglyceride and high-density lipoprotein (HDL) cholesterol values should be weighed against potential unfavorable changes in low-density lipoprotein (LDL) cholesterol values when low-carbohydrate diets to induce weight loss are considered.
In another small randomised controlled trial involving 132 severely obese subjects (including 77 blacks and 23 women) with a mean body-mass index (BMI) of 43 kg/m2 and a high prevalence of diabetes (39 percent) or the metabolic syndrome (43 percent) to a carbohydrate-restricted (low-carbohydrate) diet or a calorie- and fat-restricted (low-fat) diet 34. Out of the seventy-nine subjects who completed the six-month study showed that subjects on the low-carbohydrate diet lost more weight than those on the low-fat diet (-5.8 kg vs. -1.9 kg) and had greater decreases in triglyceride levels (-20 percent vs. -4 percent), irrespective of the use or nonuse of hypoglycemic or lipid-lowering medications. Insulin sensitivity, measured only in subjects without diabetes, also improved more among subjects on the low-carbohydrate diet. The amount of weight lost and assignment to the low-carbohydrate diet were independent predictors of improvement in triglyceride levels and insulin sensitivity 34.
Four randomized, controlled clinical trials (Table 4) have compared low-carbohydrate diets with low-fat diets 35, 36, 37, 38, 39. Although the trials differed in design, all found an average of 4 to 6 kg greater weight loss in the low-carbohydrate group at six months. However, the two studies followed to one year showed no significant weight difference 40, 41.
Low-carbohydrate diets may increase HDL cholesterol, decrease triglyceride levels, and improve glycemic control, but there appears to be no significant difference in weight loss compared with a low-fat diet at one year. Because the longest trial extends to one year with relatively few subjects, more studies are required to assess the efficacy of a low-carbohydrate diet on long-term weight loss and cardiovascular outcomes 42.
Although there is no consensus on what appropriate attrition rates for clinical trials of diets should be, attrition rates of 24% to 39% (Table 4) point to the difficulty of following a low-carbohydrate diet over time. Only in one six-month trial 43 was the attrition rate in the low-carbohydrate group significantly lower than that in the low-fat group.
Table 4. Low-Carbohydrate Diet and Weight Loss
| Foster et al. 44 | Stern et al. 41 | Brehm et al. 45 | Yancy et al. 46 | |
|---|---|---|---|---|
| Length of trial | 12 months | 12 months | 6 months | 6 months |
| Low-CHO baseline weight (kg) | 99 ± 20 | 130 ± 23 | 91 ± 8 | 97 ± 19 |
| Low-CHO diet weight change (kg) | −4% ± 7% | −5 ± 9 | −9 ± 1.0 | −12 ± 2 |
| Low-fat baseline weight (kg) | 98 ± 16 | 132 ± 27 | 92 ± 6 | 98 ± 15 |
| Low-fat diet weight change (kg) | −3% ± 6% | −3 ± 8 | −4 ± 1.0 | −7 ± 2 |
CHO = carbohydrate.
Low-Carbohydrate Diets versus Low-Fat Diets on Metabolic Risk Factors
Over the past several decades, low-fat diets have been recommended to the public for weight loss primarily because of their beneficial effects on metabolic risk factors 47.
In a meta-analysis of 23 randomized controlled trials across multiple countries with a total of 2,788 participants 48 comparing the effects of low-carbohydrate diets (≤45% of energy from carbohydrates) versus low-fat diets (≤30% of energy from fat) on metabolic risk factors (cholesterol, body weight, waist circumference, systolic blood pressure, fasting blood glucose) over a period of 6 months or more. 48. The outcome of this study was that both diets were equally effective at reducing body weight and waist circumference. Both diets reduced participants’ blood pressures, total to HDL cholesterol ratios, and total cholesterol, LDL cholesterol, triglycerides, blood glucose, and serum insulin levels and raised HDL cholesterol; however, participants on low-carbohydrate diets had greater increases in HDL cholesterol and greater decreases in triglycerides but experienced less reduction in total and LDL cholesterol compared with persons on low-fat diets.
The weighted mean changes in outcomes were, compared with participants on low-fat diets, those on low-carbohydrate diets experienced slightly but statistically significantly less reduction in total cholesterol and LDL cholesterol but a greater increase in HDL cholesterol and a greater decrease in triglycerides. Pooled mean net changes in systolic blood pressure, ratio of total to HDL cholesterol and fasting blood glucose were not significantly different between the 2 diets. The pooled mean net changes in diastolic blood pressures and serum insulin were also not significant (see data in table below).
Low-Carbohydrate Diets versus Low-Fat Diets on Metabolic Risk Factors | ||
Low-Carbohydrate Diets | Low-Fat diets | |
Body weight | −6.1 kg | −5.0 kg |
Waist circumference | −6.2 cm | −6.0 cm |
Total cholesterol | −4.6 mg/dL | −10.1 mg/dL |
LDL “Bad” cholesterol | −2.1 mg/dL | −6.0 mg/dL |
HDL “Good” cholesterol | 4.5 mg/dL | 1.6 mg/dL |
Ratio of Total cholesterol to HDL cholesterol | −0.7 | −0.5 |
Triglycerides | −30.4 mg/dL | −17.1 mg/dL |
Systolic blood pressure | −3.5 mm Hg | −3.0 mm Hg |
Fasting blood glucose | −10.4 mg/dL | −10.1 mg/dL |
(Source 47).
The results for lowering in blood pressure and lipids are consistent with those of a meta-analysis of randomized trials of Low-Carbohydrate vs Low-Fat dietary interventions conducted by Nordmann et al. in 2006 49. In that study (477 participants with BMI greater than 25) found that low-carbohydrate diets produced significantly greater weight loss (weighted mean difference, -3.3 kg) after 6 months than did low-fat diets, although the differences were not statistically significant at 1 year. There were no differences in blood pressure. Triglyceride and high-density lipoprotein cholesterol values changed more favorably in individuals assigned to low-carbohydrate diets (after 6 months, for triglycerides, weighted mean difference, -22.1 mg/dL; and for high-density (HDL) lipoprotein cholesterol, weighted mean difference, 4.6 mg/dL, but total cholesterol and low-density (LDL) lipoprotein cholesterol values changed more favorably in individuals assigned to low-fat diets (weighted mean difference in low-density lipoprotein cholesterol after 6 months, 5.4 mg/dL 49.
Low Carb Diet details
As the name says, a low-carb diet restricts the type and amount of carbohydrates you eat. Carbohydrates are a type of calorie-providing macronutrient found in many foods and beverages.
Many carbohydrates occur naturally in plant-based foods, such as grains. In natural form, carbohydrates can be thought of as complex and fibrous such as the carbohydrates found in whole grains and legumes, or they can be less complex such as those found in milk and fruit. Common sources of naturally occurring carbohydrates include:
- Grains
- Fruits
- Vegetables
- Milk
- Nuts
- Seeds
- Legumes (beans, lentils, peas)
Food manufacturers also add refined carbohydrates to processed foods in the form of flour or sugar. These are generally known as simple carbohydrates. Examples of foods that contain simple carbohydrates are white breads and pasta, cookies, cake, candy, and sugar-sweetened sodas and drinks.
Your body uses carbohydrates as its main fuel source. Sugars and starches are broken down into simple sugars during digestion. They’re then absorbed into your bloodstream, where they’re known as blood sugar (glucose). Fiber-containing carbohydrates resist digestion and although they have less effect on blood sugar, complex carbohydrates provide bulk and serve other body functions beyond fuel.
Rising levels of blood sugar trigger the body to release insulin. Insulin helps glucose enter your body’s cells. Some glucose is used by your body for energy, fueling all of your activities, whether it’s going for a jog or simply breathing. Extra glucose is usually stored in your liver, muscles and other cells for later use or is converted to fat. People who are resistant to insulin have a higher risk of prediabetes and type 2 diabetes.
The idea behind the low-carb diet is that decreasing carbs lower insulin levels, which causes the body to burn stored fat for energy and ultimately leads to weight loss.
Why you might follow a low-carb diet
You might choose to follow a low-carb diet because:
- You want a diet that restricts certain carbs to help you lose weight,
- You want to change your overall eating habits,
- You enjoy the types and amounts of foods featured in low-carb diets.
Understanding carbohydrates
Carbohydrates are a type of macronutrient found in many foods and beverages. Most carbohydrates are naturally occurring in plant-based foods, such as grains. Food manufacturers also add carbohydrates to processed foods in the form of starch or added sugar.
Think of carbs as raw material that powers your body. They come in two types: simple and complex. What’s the difference ? Simple carbs are like quick-burning fuels. They break down fast into sugar in your system. You want to eat less of this type.
Complex carbs are usually a better choice. It takes your body longer to break them down.
Common sources of naturally occurring carbohydrates include:
- Fruits
- Vegetables
- Milk
- Nuts
- Grains
- Seeds
- Legumes
Types of carbohydrates
There are three main types of carbohydrates:
- Sugar. Sugar is the simplest form of carbohydrates. Sugar occurs naturally in some foods, including fruits, vegetables, milk and milk products. Sugars include fruit sugar (fructose), table sugar (sucrose) and milk sugar (lactose).
- Starch. Starch is a complex carbohydrate, meaning it is made of many sugar units bonded together. Starch occurs naturally in vegetables, grains, and cooked dry beans and peas.
- Fiber. Fiber also is a complex carbohydrate. Fiber occurs naturally in fruits, vegetables, whole grains, and cooked dry beans and peas.
Typical foods for a low-carb diet
In general, a low-carb diet focuses on proteins, including meat, poultry, fish and eggs, and some nonstarchy vegetables. A low-carb diet generally excludes or limits most grains, legumes, fruits, breads, sweets, pastas and starchy vegetables, and sometimes nuts and seeds. Some low-carb diet plans allow small amounts of certain fruits, vegetables and whole grains.
A daily limit of 60 to 130 grams of carbohydrates is typical with a low-carb diet. These amounts of carbohydrates provide 240 to 520 calories.
Some low-carb diets greatly restrict carbs during the initial phase of the diet and then gradually increase the number of allowed carbs. Very low-carb diets restrict carbohydrates to 60 grams or less a day.
In contrast, the Dietary Guidelines for Americans recommend that carbohydrates make up 45 to 65 percent of your total daily calorie intake. So if you consume 2,000 calories a day, you would need to eat between 900 and 1,300 calories a day from carbohydrates or between 225 and 325 grams of carbohydrates a day.
Choosing carbohydrates wisely
Carbohydrates are an essential part of a healthy diet, and they also provide many important nutrients. Still, not all carbs are created equal. Here’s how to make healthy carbohydrates work in a balanced diet:
- Limit added sugars. Added sugar probably isn’t harmful in small amounts. But there’s no health advantage to consuming any amount of added sugar. In fact, too much added sugar, and in some cases naturally occurring sugar, can lead to such health problems as tooth decay, poor nutrition and weight gain. The chemical name for table sugar is sucrose. Other names you might see include fructose, dextrose, and maltose. The higher up they appear in the ingredients list, the more added sugar the food has.
- Emphasize fiber-rich fruits and vegetables. Aim for whole fresh, frozen and canned fruits and vegetables without added sugar. They’re better options than are fruit juices and dried fruits, which are concentrated sources of natural sugar and therefore have more calories. Also, whole fruits and vegetables add fiber, water and bulk, which help you feel fuller on fewer calories. Plus, most are a good source of nutrients like vitamin C and potassium. Fruits with skins you can eat, such as pears, apples, and berries, are especially high in fiber.
- Choose whole grains. Whole grains are better sources of fiber and other important nutrients, such as selenium, potassium and magnesium, than are refined grains. Refined grains go through a process that strips out parts of the grain — along with some of the nutrients and fiber.
- Eat more beans and legumes. Legumes, which include beans, peas and lentils, are among the most versatile and nutritious foods available. Legumes are typically low in fat; contain no cholesterol; and are high in folate, potassium, iron and magnesium. They also have beneficial fats and soluble and insoluble fiber. Because they’re a good source of protein, legumes can be a healthy substitute for meat, which has more saturated fat and cholesterol.
Results
1) Low Carb Atkins Diet vs Zone Diet vs LEARN Diet vs Ornish Diet for Weight loss
In a 2007 study 50, where researchers randomly assigned 311 individuals to four groups: one group was assigned the high-fat, high-protein and low-carbohydrate (Atkins diet); the second was assigned Ornish’s very low-fat vegetarian diet, which requires consuming fewer than 10 percent of calories from fat; the third was assigned the Zone diet, which aims for a 40/30/30 percent distribution of carbohydrate, protein and fat (macronutrient balance); and the fourth was assigned the high-carbohydrate, low–saturated fat LEARN (for: lifestyle, exercise, attitudes, relationships, nutrition) diet. Participants were randomly assigned to follow the Atkins (n = 77), Zone (n = 79), LEARN (n = 79), or Ornish (n = 76) diets and received weekly instruction for 2 months, then an additional 10-month follow-up. Weight loss at 12 months was the primary outcome. Secondary outcomes included lipid profile (low-density lipoprotein, high-density lipoprotein, and non–high-density lipoprotein cholesterol, and triglyceride levels), percentage of body fat, waist-hip ratio, fasting insulin and glucose levels, and blood pressure. Outcomes were assessed at months 0, 2, 6, and 12. The participants all had trouble adhering to their regimens, but all lost about the same statistically significant amounts of weight, and when compared head to head, the Atkins dieters saw greater improvements in blood pressure and HDL cholesterol than the Ornish dieters did.
Results 50: Weight loss was greater for women in the Atkins diet group compared with the other diet groups at 12 months, and mean 12-month weight loss was significantly different between the Atkins and Zone diets. Mean 12-month weight loss was as follows:
- Atkins, −4.7 kg ( −6.3 to −3.1 kg),
- Zone, −1.6 kg (−2.8 to −0.4 kg),
- LEARN, −2.6 kg (−3.8 to −1.3 kg), and
- Ornish, −2.2 kg (−3.6 to −0.8 kg).
- Weight loss was not statistically different among the Zone, LEARN, and Ornish groups.
- At 12 months, secondary outcomes for the Atkins group were comparable with or more favorable than the other diet groups.
Conclusions 50: In this study, premenopausal overweight and obese women assigned to follow the Atkins diet, which had the lowest carbohydrate intake, lost more weight and experienced more favorable overall metabolic effects at 12 months than women assigned to follow the Zone, Ornish, or LEARN diets. While questions remain about long-term effects and mechanisms, a low-carbohydrate, high-protein, high-fat diet may be considered a feasible alternative recommendation for weight loss.
Most people can lose weight on diet plans that restrict calories and what you can eat — at least in the short term. And low-carb diets, especially very low-carb diets, may lead to greater short-term weight loss than low-fat diets.
But most studies have found that at 12 or 24 months, the benefits of a low-carb diet are not very large. A 2014 review found that higher protein, low-carbohydrate diets may offer a slight advantage in terms of weight loss and loss of fat mass compared to a normal protein diet. At a year, the difference was only about a pound (about 0.4 kilograms), though, and those who had the greatest benefits stuck to the diet long term.
Cutting calories and carbs may not be the only reason for the weight loss. Some studies show that you may shed some weight because you eat less on low-carb diets because the extra protein and fat keep you feeling full longer.
2) Other health benefits
Low-carb diets may help prevent or improve serious health conditions, such as metabolic syndrome, diabetes, high blood pressure and cardiovascular disease. In fact, almost any diet that helps you shed excess weight can reduce or even reverse risk factors for cardiovascular disease and diabetes. Most weight-loss diets — not just low-carb diets — may improve blood cholesterol or blood sugar levels, at least temporarily.
Low-carb diets may improve HDL cholesterol and triglyceride values slightly more than do moderate-carb diets. That may not only be due to how many carbs you eat but also the quality of your other food choices. Lean protein (fish, poultry, legumes), healthy fats (monounsaturated and polyunsaturated) and unprocessed carbs — such as whole grains, legumes, vegetables, fruits and low-fat dairy products — are generally healthier choices.
A report from the American Heart Association, the American College of Cardiology and he Obesity Society concluded that there isn’t enough evidence to say whether most low-carbohydrate diets provide heart-healthy benefits.
Risks
Some diets restrict carbohydrate intake so much that in the long term they can result in vitamin or mineral deficiencies, bone loss, and gastrointestinal disturbances and may increase risks for various chronic diseases.
Severely restricting carbohydrates to less than 20 grams a day can result in a process called ketosis. Ketosis occurs when you don’t have enough sugar (glucose) for energy, so your body breaks down stored fat, causing ketones to build up in your body. Side effects from ketosis can include nausea, headache, mental and physical fatigue, and bad breath.
It’s not clear what kind of possible long-term health risks a low-carb diet may pose because most research studies have lasted less than a year. Some health experts believe that if you eat large amounts of fat and protein from animal sources your risk of heart disease or certain cancers may actually increase.
Conclusion:
The low-carbohydrate diet is very effective for short-term weight loss and for cardiovascular risk factor reduction than the low-fat diet. However, the long-term effects on cardiovascular disease risk factors, such as weight loss, HDL and LDL cholesterol, triglycerides, glycemic control, and blood pressure, are unknown.
Restricting carbohydrate is a good an option for persons seeking to lose weight and reduce cardiovascular risk factors. Rather than cutting carbs across the board, a more healthful goal is to increase the “good” or complex carbohydrates found in whole grains, fruits, and vegetables and cut back on “bad” or simple carbohydrates, such as sugar and processed grains. So choose your carbohydrates wisely. Just make sure you cut out processed foods and refined added sugary foods and drink from your diet- refined grains, such as sugary drinks, desserts and candy, which are packed with calories but low in nutrition. Instead, go for fruits, vegetables and whole grains. and eat plenty of vegetables and fruits so you get plenty of good vitamins and minerals.
- American Diabetes Association. Carbohydrate Counting. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/understanding-carbohydrates/carbohydrate-counting.html[↩][↩]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th Edition. December 2015. https://health.gov/dietaryguidelines/2015/[↩][↩][↩]
- W. Banting. Letter on Corpulence, Addressed to the Public(2nd edition), Harisson and Sons, London (1863[↩]
- R.C. Atkins. Dr. Atkins’ New Diet Revolution. Avon Books, New York, NY (1998[↩][↩][↩]
- S.T. St. Jeor, B.V. Howard, T.E. Prewitt, et al.Dietary protein and weight reduction: a statement for healthcare professionals from the Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association Circulation, 104 (2001), pp. 1869-1874[↩][↩][↩]
- Yancy WS Jr, Olsen MK, Guyton JR, Bakst RP, Westman EC. Ann Intern Med. 2004 May 18;140(10):769-77. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: a randomized, controlled trial. https://www.ncbi.nlm.nih.gov/pubmed/15148063[↩][↩][↩]
- R.O. Bonow, R.H. EckelDiet, obesity, and cardiovascular risk. N Engl J Med, 348 (2003), pp. 2057-2058.[↩]
- D.M. Bravata, L. Sander, J. Huang, et al.Efficacy and safety of low-carbohydrate diets: a systematic reviewJAMA, 289 (2003), pp. 1837-1850.[↩]
- S.T. St. Jeor, B.V. Howard, T.E. Prewitt, et al.Dietary protein and weight reduction: a statement for healthcare professionals from the Nutrition Committee of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart AssociationCirculation, 104 (2001), pp. 1869-1874[↩][↩]
- R.O. Bonow, R.H. EckelDiet, obesity, and cardiovascular riskN Engl J Med, 348 (2003), pp. 2057-2058[↩][↩]
- D.M. Bravata, L. Sander, J. Huang, et al.Efficacy and safety of low-carbohydrate diets: a systematic reviewJAMA, 289 (2003), pp. 1837-1850[↩][↩]
- The Practical Guide, Identification, Evaluation and Treatment of Overweight and Obesity in Adults. Bethesda, Md US Dept of Health and Human Services2000;NIH publication 00-4084[↩]
- Freedman MRKing JKennedy E Popular diets: a scientific review. Obes Res 2001;9 ((suppl 1[↩]
- Atkins RC Dr. Atkins’ New Diet Revolution. New York, NY HarperCollins Publishers 1998[↩]
- Cleve Clin J Med. 2001 Sep;68(9):761, 765-6, 768-9, 773-4. Physician’s guide to popular low-carbohydrate weight-loss diets. https://www.ncbi.nlm.nih.gov/pubmed/11563479[↩]
- American Heart Association. Recipes for Cholesterol Management. http://www.heart.org/HEARTORG/Conditions/Cholesterol/CholesterolToolsResources/Recipes-for-Cholesterol-Management_UCM_305655_Article.jsp[↩]
- American Heart Association. Advisory: Replacing saturated fat with healthier fat could lower cardiovascular risks. http://news.heart.org/advisory-replacing-saturated-fat-with-healthier-fat-could-lower-cardiovascular-risks/[↩]
- American Heart Association. Saturated Fats. https://healthyforgood.heart.org/Eat-smart/Articles/Saturated-Fats[↩][↩]
- Law M. 2000 Dietary fat and adult diseases and the implications for childhood nutrition: an epidemiologic approach. Am J Clin Nutr 72:1291 S–1296S. [↩]
- Bennett PH RM, Knowler WC. 1997 Epidemiology of diabetes mellitus. In: Sherwin RS, ed. Diabetes mellitus. Stamford: Appleton and Lange; 373–400.[↩]
- Diabetologia. 1997 Apr;40(4):430-8. High saturated fat and low starch and fibre are associated with hyperinsulinaemia in a non-diabetic population: the San Luis Valley Diabetes Study. https://www.ncbi.nlm.nih.gov/pubmed/9112020[↩]
- Am J Clin Nutr. 1998 Dec;68(6):1157-73. Dietary fat intake does affect obesity! https://www.ncbi.nlm.nih.gov/pubmed/9846842[↩]
- Diabetes Care. 1998 Dec;21(12):2069-76. Genes versus environment. The relationship between dietary fat and total and central abdominal fat. https://www.ncbi.nlm.nih.gov/pubmed/9839096[↩]
- The Journal of Clinical Endocrinology and Metabolism. J Clin Endocrinol Metab (2003) 88 (4): 1617-1623. A Randomized Trial Comparing a Very Low Carbohydrate Diet and a Calorie-Restricted Low Fat Diet on Body Weight and Cardiovascular Risk Factors in Healthy Women. https://academic.oup.com/jcem/article-lookup/doi/10.1210/jc.2002-021480[↩][↩][↩][↩]
- National Institutes of Health NH, Lung, and Blood Institute 1998. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Bethesda: NIH[↩]
- Lutz C, Przytulski K. 2001 Nutrition and diet therapy. Philadelphia: Davis[↩]
- J Clin Invest. 1976 Sep;58(3):722-30. Composition of weight lost during short-term weight reduction. Metabolic responses of obese subjects to starvation and low-calorie ketogenic and nonketogenic diets. https://www.ncbi.nlm.nih.gov/pubmed/956398[↩]
- Am J Clin Nutr. 1967 Oct;20(10):1104-12. Fat, carbohydrate, salt, and weight loss. https://www.ncbi.nlm.nih.gov/pubmed/6069652[↩]
- Atkins R. 1992 Dr. Atkins new diet revolution. New York: Avon Books[↩]
- Clin Chem. 1986 Jan;32(1 Pt 1):224-5. Monitoring therapy with insulin in ketoacidotic patients by quantifying 3-hydroxybutyrate with a commercial kit. https://www.ncbi.nlm.nih.gov/pubmed/3079681[↩]
- Am J Clin Nutr. 1998 Jul;68(1):12-34. Protein, fat, and carbohydrate requirements during starvation: anaplerosis and cataplerosis. https://www.ncbi.nlm.nih.gov/pubmed/9665093[↩]
- Nutr Rev. 1998 May;56(5 Pt 2):S3-19; discussion S19-28. Dietary fat consumption and health. https://www.ncbi.nlm.nih.gov/pubmed/9624878[↩]
- Nordmann AJ, Nordmann A, Briel M. et al. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Arch Intern Med. 2006;166:285-293. http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/409791[↩]
- Samaha FF, Iqbal N, Seshadri P, Chicano KL, Daily DA, McGrory J, Williams T, Williams M, Gracely EJ, Stern L. N Engl J Med. 2003 May 22;348(21):2074-81. A low-carbohydrate as compared with a low-fat diet in severe obesity. https://www.ncbi.nlm.nih.gov/pubmed/12761364/[↩][↩]
- G.D. Foster, H.R. Wyatt, J.O. Hill, et al.A randomized trial of a low-carbohydrate diet for obesityN Engl J Med, 348 (2003), pp. 2082-2090.[↩]
- L. Stern, N. Iqbal, P. Seshadri, et al.The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year follow-up of a randomized trialAnn Intern Med, 140 (2004), pp. 778-785[↩]
- F.F. Samaha, N. Iqbal, P. Seshadri, et al. A low-carbohydrate as compared with a low-fat diet in severe obesityN Engl J Med, 348 (2003), pp. 2074-2081[↩]
- B.J. Brehm, R.J. Seeley, S.R. Daniels, D.A. D’AlessioA randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy womenJ Clin Endocrinol Metab, 88 (2003), pp. 1617-1623[↩]
- W.S. Yancy, M.K. Olsen, J.R. Guyton, et al.A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemiaAnn Intern Med, 140 (2004), pp. 769-777[↩]
- G.D. Foster, H.R. Wyatt, J.O. Hill, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med, 348 (2003), pp. 2082-2090[↩]
- L. Stern, N. Iqbal, P. Seshadri, et al.The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: one-year follow-up of a randomized trial. Ann Intern Med, 140 (2004), pp. 778-785[↩][↩]
- Journal of the American College of Cardiology Volume 45, Issue 9, 3 May 2005, Pages 1379-1387. Diets and Cardiovascular Disease: An Evidence-Based Assessment. http://www.sciencedirect.com/science/article/pii/S0735109705003670[↩]
- W.S. Yancy, M.K. Olsen, J.R. Guyton, et al.A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia. Ann Intern Med, 140 (2004), pp. 769-777[↩]
- G.D. Foster, H.R. Wyatt, J.O. Hill, et al.A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med, 348 (2003), pp. 2082-2090.[↩]
- B.J. Brehm, R.J. Seeley, S.R. Daniels, D.A. D’AlessioA randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J Clin Endocrinol Metab, 88 (2003), pp. 1617-1623[↩]
- W.S. Yancy, M.K. Olsen, J.R. Guyton, et al. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia. Ann Intern Med, 140 (2004), pp. 769-777[↩]
- Circulation. 2006 Jul 4;114(1):82-96. Epub 2006 Jun 19. Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. https://www.ncbi.nlm.nih.gov/pubmed/16785338/[↩][↩]
- Am J Epidemiol. 2012 Oct 1; 176(Suppl 7): S44–S54. doi: 10.1093/aje/kws264. Effects of Low-Carbohydrate Diets Versus Low-Fat Diets on Metabolic Risk Factors: A Meta-Analysis of Randomized Controlled Clinical Trials. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3530364/[↩][↩]
- Arch Intern Med. 2006 Feb 13;166(3):285-93. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. https://www.ncbi.nlm.nih.gov/pubmed/16476868/[↩][↩]
- JAMA. 2007 Mar 7;297(9):969-77. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. https://www.ncbi.nlm.nih.gov/pubmed/17341711[↩][↩][↩]





{kind=link}