Contents
What are thyroid nodules
Thyroid nodules are solid or fluid-filled cysts that form lumps within your thyroid, a small gland located at the base of your neck, just above your breastbone (see Figures 1 to 3). Thyroid nodules have been defined by the American Thyroid Association as “discrete lesions within the thyroid gland, radiologically distinct from surrounding thyroid parenchyma”1. Thyroid nodules are common, their prevalence being largely dependent on the identification method. The estimated prevalence by palpation alone ranges from 4% to 7% 2, whereas ultrasound scan detects nodules in 20% to 76% of the adult population 3, particularly with the current use of high-resolution ultrasound scan techniques 4. The reported frequencies detected by ultrasound scan correlate with the prevalence reported at surgery and autopsy with ranges between 50% and 65% 5.
The estimated annual incidence of thyroid nodules in the United States is approximately 0.1% per year, conferring a 10% lifetime probability for developing a thyroid nodule 3. Thyroid nodules are 4 times more common in women than men and their frequency increases with age and low iodine intake 6. The gender disparity is perhaps explained by the hormonal influences of both estrogen and progesterone, as increasing nodule size and new nodule development have been demonstrated to be related to pregnancy and multiparity (number of pregnancies) 7. Exposure to ionizing radiation, either during childhood or as an occupational exposure, will cause a rate of development of thyroid nodules of 2% per year, reaching a peak incidence in 15 to 25 years 8.
However, the great majority of thyroid nodules aren’t serious and don’t cause symptoms. You often won’t know you have a thyroid nodule until your doctor discovers it during a routine medical exam. Some thyroid nodules, however, may become large enough to be visible or may cause pain or hoarseness or get in the way of swallowing or breathing.
Doctors are concerned about thyroid nodules, because they can sometimes be cancerous. Thyroid cancer is found in about 8 percent of thyroid nodules in men (or 8 out of 100) and in 4% of nodules in women. Thus, about 90% of all thyroid nodules are benign (non-cancerous).
A patient with a multinodular thyroid has the same risk of having a malignancy as a patient with a single thyroid nodule and is independent of the number of nodules 9. However, the likelihood of malignancy per nodule decreases as the number of thyroid nodules increases 10. If 2 or more thyroid nodules larger than 1 cm are present, the selection of nodules for fine needle aspiration (FNA) biopsy should be made on the basis of the previously described suspicious thyroid ultrasound characteristics. Otherwise, the largest nodule should be targeted for biopsy 11.
Totally cystic lesions are generally considered benign and, unless a solid component is present, further diagnostic investigation is not required 9.
Table 1. Features suggestive of increased potential for thyroid carcinoma (cancer) in a patient with thyroid nodule
| Patient History or Characteristics | Findings on Physical Examination | Findings Seen on Imaging |
|---|---|---|
| Family history of MEN (multiple endocrine neoplasia), MTC (medullary thyroid cancer), and PTC (papillary thyroid cancer) | Firm nodule | Suspicious ultrasound features |
| History of head and neck irradiation | Nodule fixed to adjacent structures | Lymphadenopathy |
| History of Hodgkin and non-Hodgkin lymphoma | Growth of nodule, especially during therapy to suppress serum thyroid stimulating hormone (TSH) | |
| Age <20 | Abnormal cervical lymphadenopathy | |
| Age >70 | Paralysis of the vocal cords | |
| Male sex | ||
| Symptoms of compression: hoarseness, dysphagia, dysphonia, dyspnea, cough |
The cause of most benign thyroid nodules is not known, but they are often found in members of the same family. Worldwide, lack of iodine in the diet is a very common cause of thyroid nodules.
Treatment options depend on the type of thyroid nodule you have.
Although most thyroid nodules are noncancerous (benign) and don’t cause problems, ask your doctor to evaluate any unusual swelling in your neck, especially if you have trouble breathing or swallowing. It’s important to evaluate the possibility of thyroid cancer.
Also seek medical care if you develop signs and symptoms of hyperthyroidism, such as:
- Sudden weight loss even though your appetite is normal or has increased
- A pounding heart
- Trouble sleeping
- Muscle weakness
- Nervousness or irritability
What is the thyroid gland
The thyroid gland is the largest adult gland to have a purely endocrine function, weighing about 25-30 g. The butterfly-shaped thyroid gland is located adjacent to the trachea just inferior to the larynx (voice box) and is named for the nearby shield like thyroid cartilage of the larynx.
The thyroid gland is composed of right and left lateral lobes, one on either side of the trachea, that are connected by an isthmus in front of the trachea. About 50% of thyroid glands have a small third lobe, called the pyramidal lobe. It extends superiorly from the isthmus.
Microscopic spherical sacs called thyroid follicles make up most of the thyroid gland. The wall of each follicle consists primarily of cells called follicular cells, most of which extend to the lumen (internal space) of the follicle. A basement membrane surrounds each follicle. When the follicular cells are inactive, their shape is low cuboidal to squamous, but under the influence of thyroid stimulating hormone (TSH) they become active in secretion and range from cuboidal to low columnar in shape. The follicular cells produce two hormones: thyroxine, which is also called tetraiodothyronine (T4) because it contains four atoms of iodine and triiodothyronine (T3), which contains three atoms of iodine. T3 and T4 together are also known as thyroid hormones.
A few cells called parafollicular cells or C cells lie between follicles. They produce the hormone calcitonin, which helps regulate calcium homeostasis.
Like other endocrine glands, the thyroid releases these hormones directly into the bloodstream. Each follicle is surrounded by a basket like network of capillaries, the globular clusters of blood vessels. These are supplied by the superior and inferior thyroid arteries. The thyroid receives one of the body’s highest rates of blood flow per gram of tissue and consequently has a dark reddish brown color.
Thyroid hormone is secreted or inhibited in response to fluctuations in metabolic rate. The brain monitors the body’s metabolic rate and stimulates thyroid hormone (TH) secretion through the action of thyrotropin-releasing hormone (TRH) and thyroid stimulating hormone (TSH) as depicted in figure 3.
The primary effect of thyroid hormone (TH) is to increase one’s metabolic rate. As a result, it raises oxygen consumption and has a calorigenic effect—it increases heat production. To ensure an adequate blood and oxygen supply to meet this increased metabolic demand, thyroid hormone also raises the respiratory rate, heart rate, and strength of the heartbeat. It stimulates the appetite and accelerates the breakdown of carbohydrates, fats, and protein for fuel. Thyroid hormone also promotes alertness and quicker reflexes; growth hormone secretion; growth of the bones, skin, hair, nails, and teeth; and development of the fetal nervous system.
The thyroid gland also contains nests of parafollicular cells, also called clear (C) cells, at the periphery of the follicles. They respond to rising levels of blood calcium by secreting the hormone calcitonin. Calcitonin antagonizes parathyroid hormone and stimulates osteoblast activity, thus promoting calcium deposition and bone formation. It is important mainly in children, having relatively little effect in adults.
Figure 1. Thyroid gland location
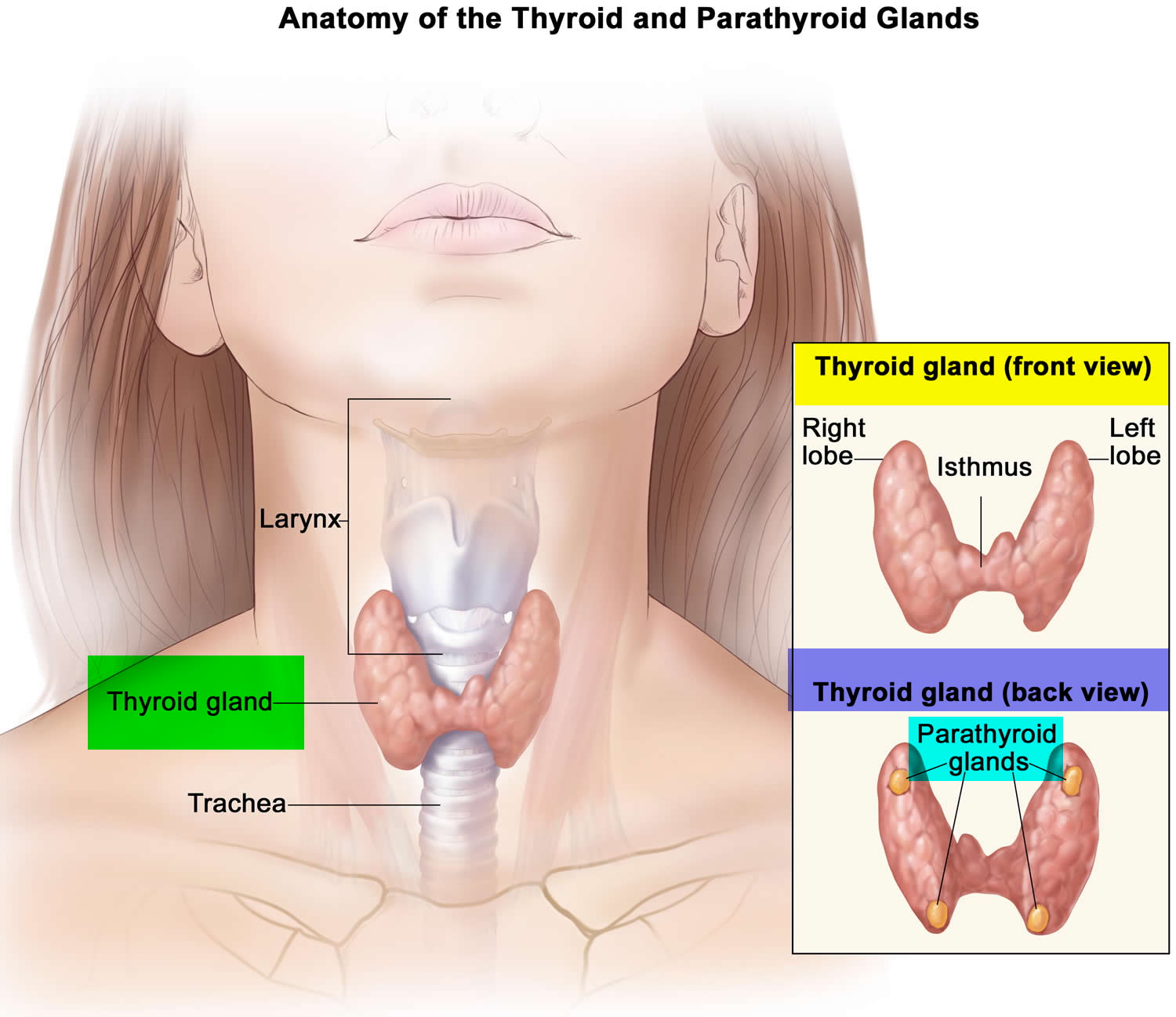
Figure 2. Thyroid gland location
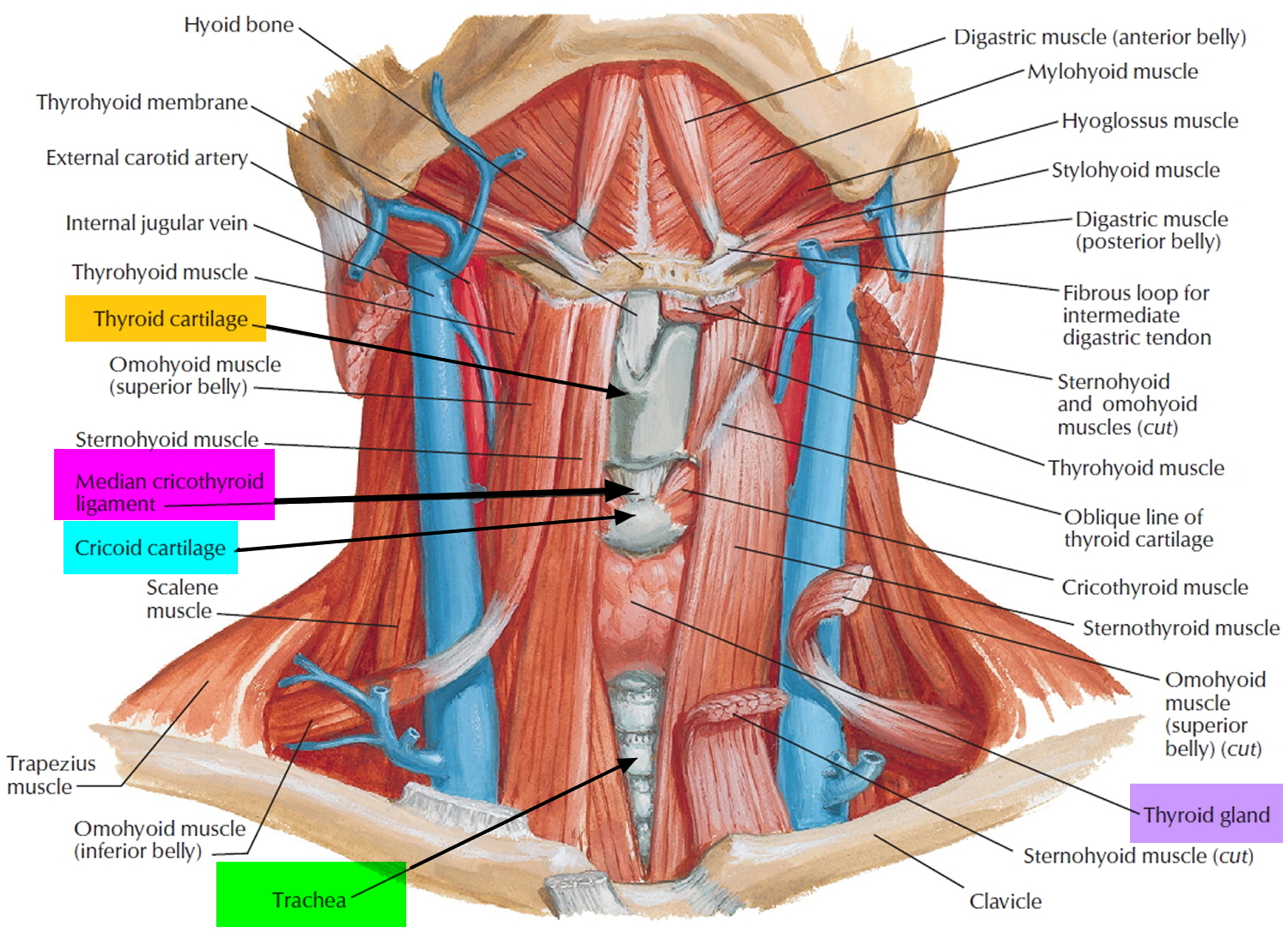
Figure 3. Thyroid gland
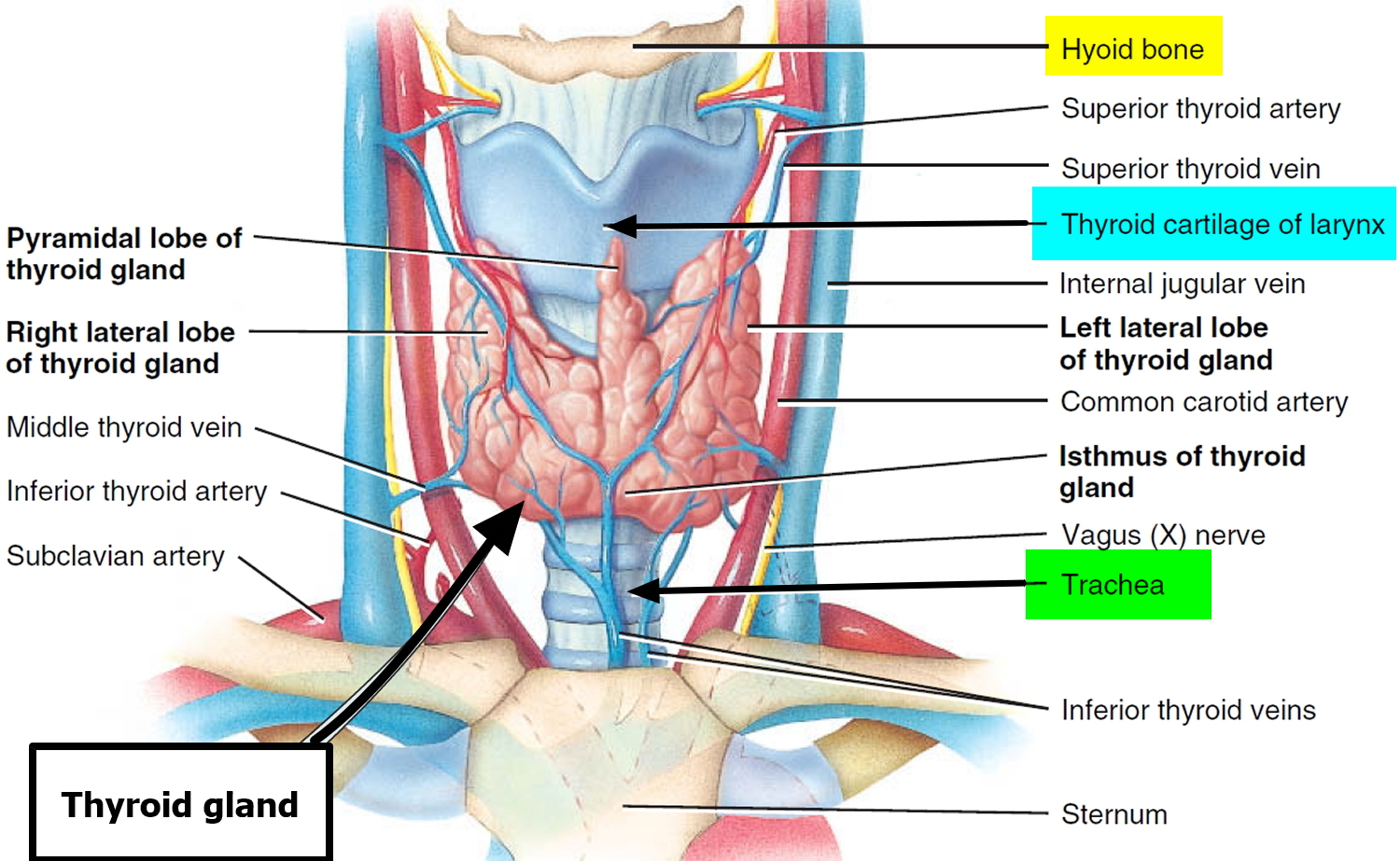
Figure 4. Thyroid gland anatomy
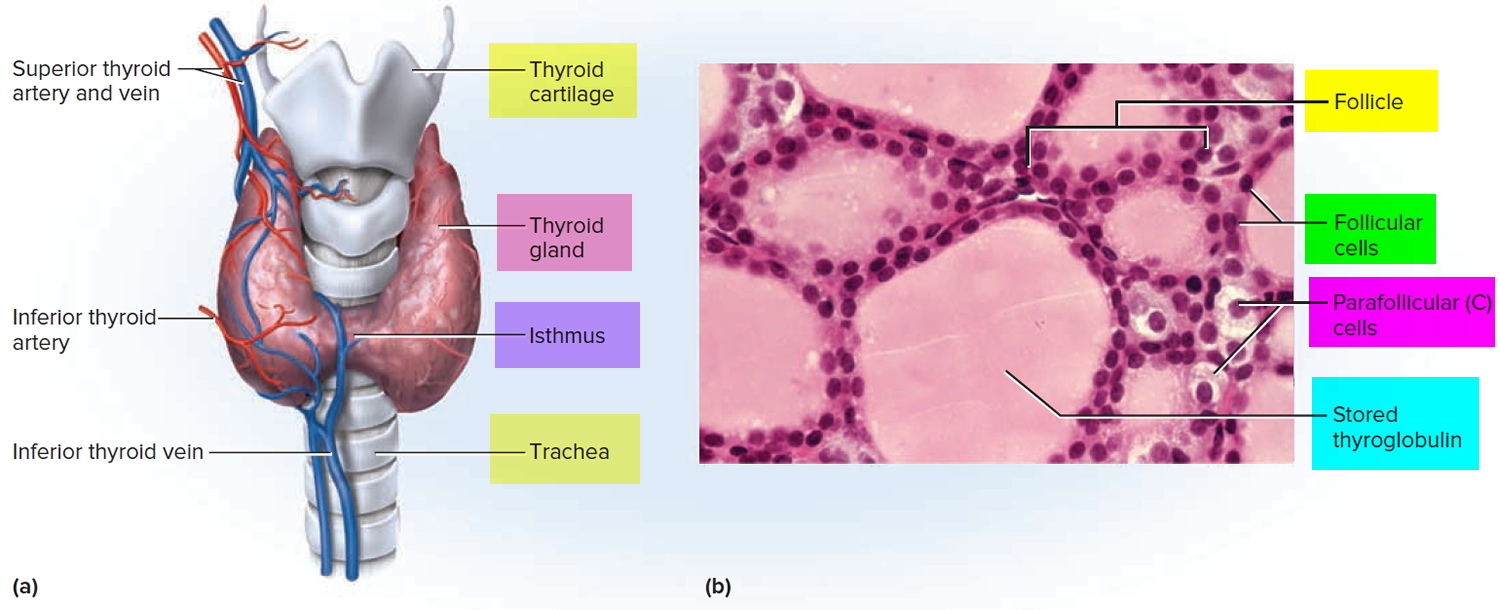
Note: (a) Gross anatomy, anterior view. (b) Histology, showing the saccular thyroid follicles (the source of thyroid hormone) and nests of C cells (the source of calcitonin).
Thyroid nodules ultrasound
Thyroid ultrasound is an important technique widely used in the detection and evaluation of thyroid nodules. It is a noninvasive, inexpensive procedure that provides information with regard to nodule dimensions, structure, and thyroid parenchymal changes. Nowadays, the use of brightness-mode thyroid ultrasound and high-frequency transducers may detect lesions as small as 2 to 3 mm, which raises the question of which thyroid nodules are clinically relevant for further evaluation.
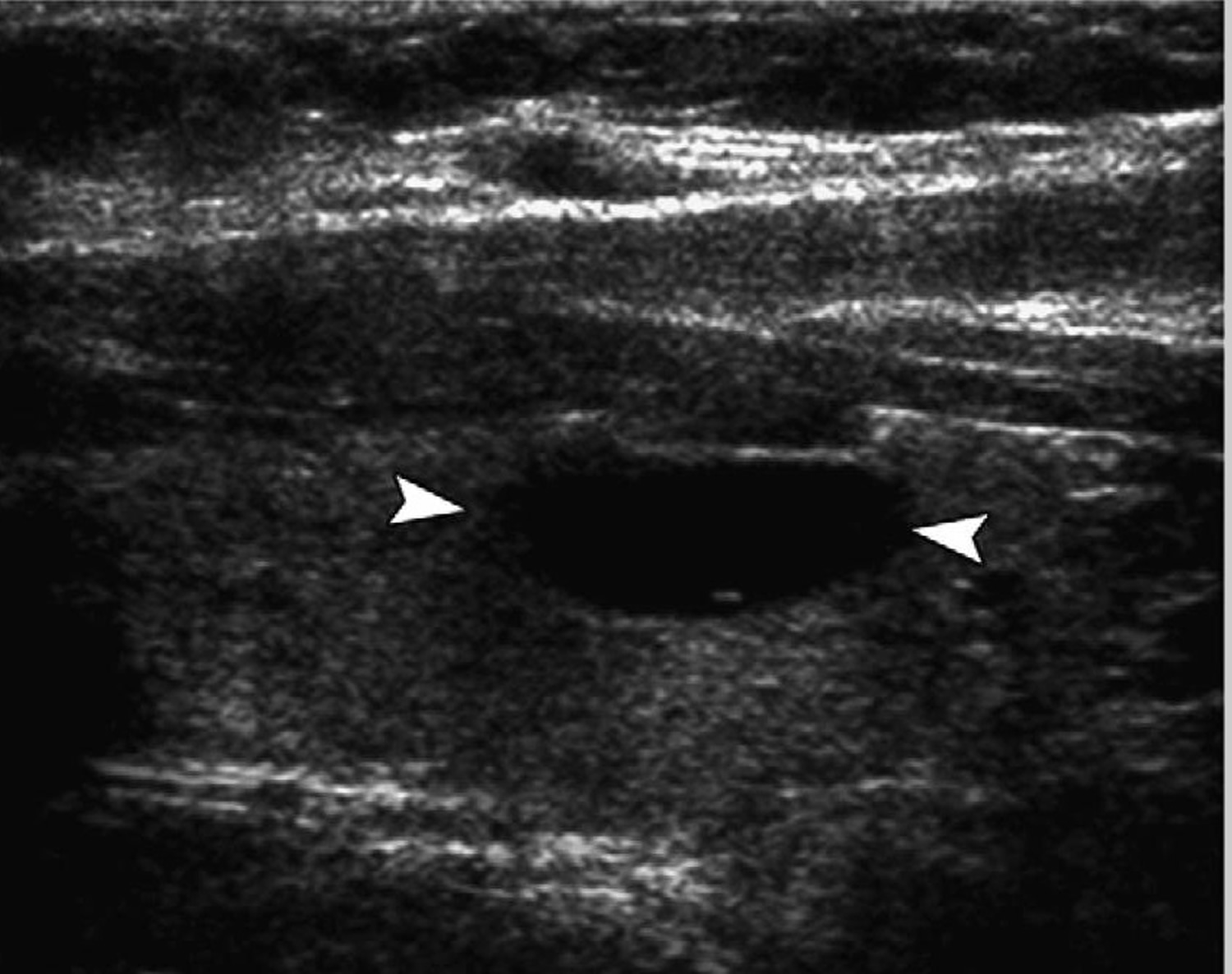
Previous studies have investigated the ability of thyroid ultrasound to differentiate between benign and malignant lesions to avoid the unnecessary use of invasive procedures 12. As a result, several thyroid ultrasound features have been found to be indicative of malignant potential. Microcalcifications (Figure 4), irregular or microlobulated margins, hypoechogenicity, taller-than-wide shape, and increased intranodular vascularity (Figure 5) were found to be independent risk factors for malignancy 13. Even though these suspicious features are characterized by high specificity, their positive predictive value is lowered by their relatively low sensitivity (Table 2). It is important to know that none of these thyroid ultrasound features alone is sufficient to differentiate benign from malignant tumors, but a combination of at least 2 of them better succeeds in pointing out a subset of lesions at high risk for malignancy 14. Papini and colleagues 13 demonstrated that nodules with a hypoechoic appearance and one of the other suspicious thyroid ultrasound characteristics successfully identifies thyroid lesions that need to undergo further cytologic examination. For example, a predominantly solid nodule with micro-calcifications has a 31.6% likelihood of malignancy, whereas a predominantly cystic lesion (Figure 6) with no microcalcifications lowers the probability for being cancer to 1.0% 15. Thyroid ultrasound findings such as isoechogenicity and spongiform appearance (defined as aggregations of multiple microcysts in more than 50% of the nodule) are features highly suggestive of benignity 16.
The number of thyroid nodules and their size are not predictive of malignancy, as a nodule smaller than 1 cm is as likely as a larger nodule to harbor neoplastic cells in the presence of suspicious thyroid ultrasound features 15, 17. Choosing an arbitrary size as cutoff for the likelihood of cancer or stratifying the risk in a multinodular goiter based on the “dominant” nodule has fallen into disfavor 13.
Thyroid ultrasound identification of neck lymph nodes demonstrating microcalcifications, increased vascularity, cystic changes, and rounded shape, along with coexisting ipsi-lateral thyroid nodules, are also very important clues for malignant etiology 16. Evidence of extracapsular growth, which may range from invasion of the thyroid capsule to perithyroidal muscle infiltration and recurrent laryngeal nerve extension, is another strong indicator of malignancy 14.
Screening for thyroid nodules by ultrasound, or by any other types of imaging studies, is not recommended in the general population because of the minimal aggressiveness and indolent course of most of the thyroid cancers. Current American Thyroid Association guidelines1 recommend diagnostic thyroid ultrasonography to be performed only in patients with known or suspected thyroid nodules, or in the presence of risk factors 18.
Other diagnostic imaging techniques, such as MRI and CT scans, are not indicated for routine thyroid nodule evaluation, but they may be helpful for the assessment of nodule size, substernal extension of a nodular goiter, and airway compression 19.
Table 2. Ultrasound characteristics of thyroid nodules predictive of malignancy
| Ultrasound Feature | Sensitivity, % | Specificity, % | Positive Predictive Value, % | Negative Predictive Value, % |
|---|---|---|---|---|
| Microcalcifications | 26.1–59.1 | 85.8–95.0 | 24.3–70.7 | 41.8–94.2 |
| Hypoechogenicity | 26.5–87.1 | 43.4–94.3 | 11.4–68.4 | 73.5–93.8 |
| Irregular margins or no halo | 17.4–77.5 | 38.9–85.0 | 9.3–60.0 | 38.9–97.8 |
| Solid | 69.0–75.0 | 52.5–55.9 | 15.6–27.0 | 88.0–92.1 |
| Intranodule vascularity | 54.3–74.2 | 78.6–80.8 | 24.0–41.9 | 85.7–97.4 |
| More tall than wide | 32.7 | 92.5 | 66.7 | 74.8 |
Table 3. Thyroid ultrasound and clinical features of thyroid nodules and recommendations for fine-needle aspiration (FNA)
| Nodule Sonographic or Clinical Features | Recommendeda Nodule Threshold Size for FNA | |
|---|---|---|
| High-risk history | ||
| Nodule with suspicious sonographic features | >5 mm | Recommendation A |
| Nodule without suspicious sonographic features | >5 mm | Recommendation I |
| Abnormal cervical lymph nodes | All | Recommendation A |
| Microcalcifications present in nodule | ≥1 cm | Recommendation B |
| Solid nodule | ||
| And hypoechoic | >1 cm | Recommendation B |
| And iso- or hyperechoic | ≥1–1.5cm | Recommendation C |
| Mixed cystic-solid nodule | ||
| With any suspicious ultrasound features | ≥1.5–2.0cm | Recommendation B |
| Without suspicious ultrasound features | ≥2.0 cm | Recommendation C |
| Spongiform nodule | ≥2.0 cmb | Recommendation C |
| Purely cystic nodule | FNA not indicatedc | Recommendation E |
Abbreviation: FNA, fine-needle aspiration.
Figure 4. Thyroid nodule ultrasound
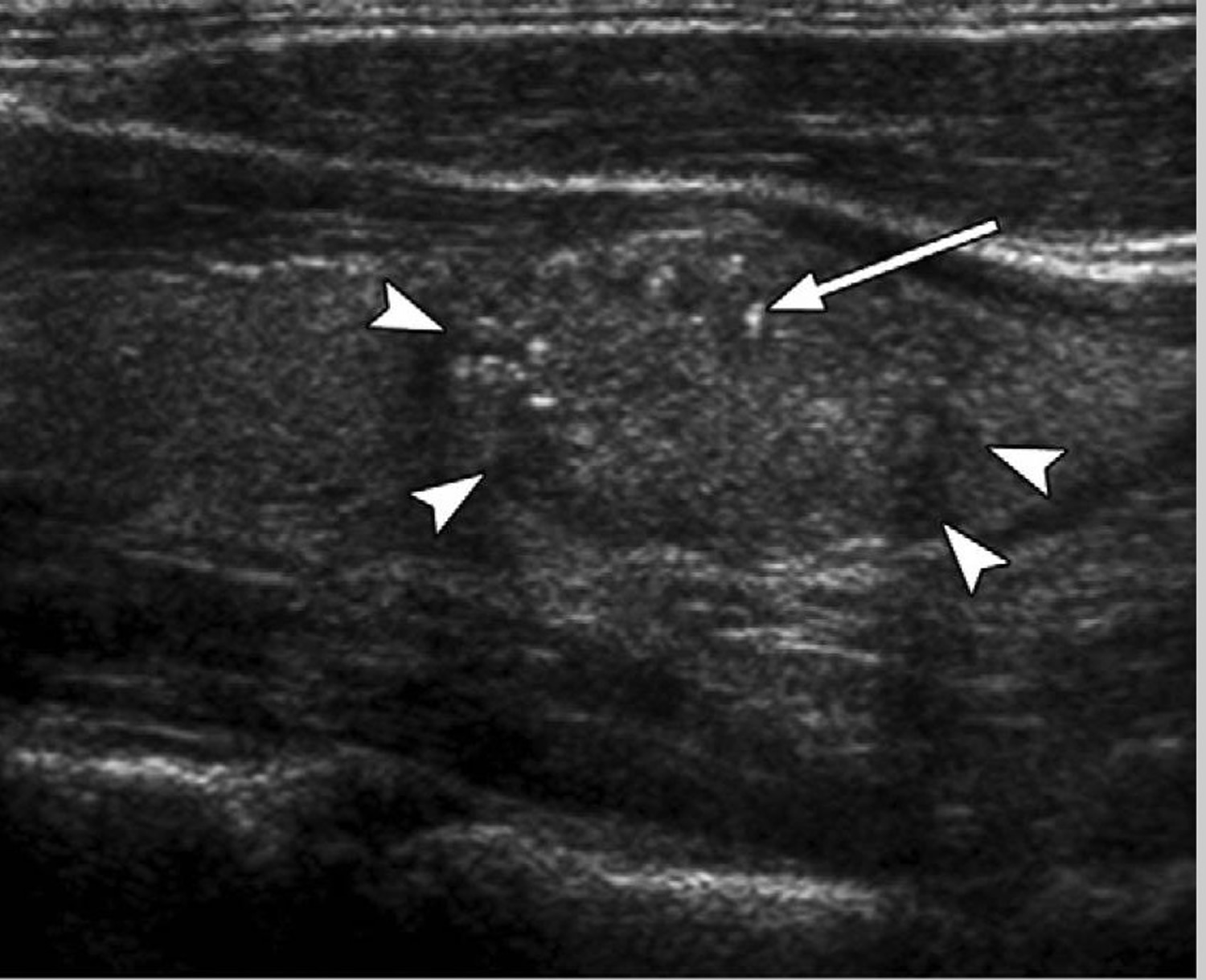
Note: Ultrasound image of a thyroid nodule (arrowheads) containing multiple fine punctuate echo-genicities (arrow) with no comet-tail artifact, indicating high suspicion for malignancy. Fine needle aspiration biopsy and surgery confirmed papillary thyroid cancer.
Figure 5. Thyroid nodule ultrasound (color doppler ultrasound of a thyroid nodule showing marked internal vascularity, indicating increased likelihood of malignancy. Histology demonstrated papillary thyroid cancer).
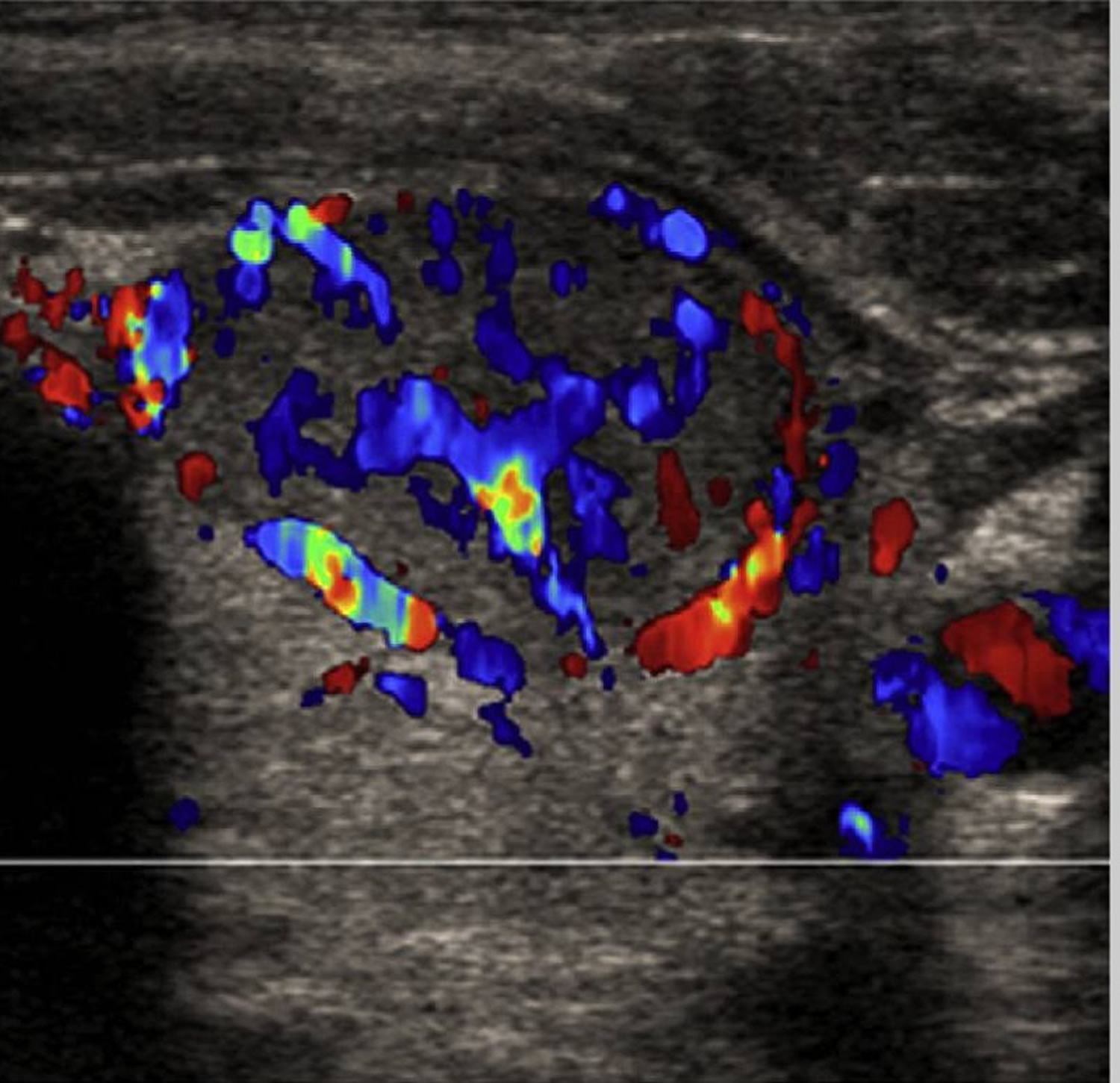
Figure 6. Thyroid nodule ultrasound of a cystic thyroid nodule
Thyroid nodules causes
What causes thyroid nodules
Thyroid nodules are growths of cells in the thyroid gland. These growths can be:
- Not cancer (benign)
- Thyroid cancer (malignant): Although the chances that a nodule is malignant are small, certain factors increase your risk of thyroid cancer, such as a family history of thyroid or other endocrine cancers. Other risk factors include being younger than 30 or older than 60, being a male, or having a history of radiation exposure, particularly to the head and neck. A nodule that is large and hard or causes pain or discomfort is more worrisome in terms of malignancy.
- Overgrowth of normal thyroid tissue. Why this occurs isn’t clear, but such a growth — which is sometimes referred to as a thyroid adenoma — is noncancerous and isn’t considered serious unless it causes bothersome symptoms from its size. Some thyroid adenomas (autonomous or hyperfunctioning thyroid nodules) produce thyroid hormones outside of your pituitary gland’s normal regulatory influence, leading to an overproduction of thyroid hormones (hyperthyroidism).
- Fluid-filled (cysts): Fluid-filled cavities (cysts) in the thyroid most commonly result from degenerating thyroid adenomas. Often, solid components are mixed with fluid in thyroid cysts. Cysts are usually benign, but they occasionally contain malignant solid components.
- One nodule or a group of small nodules: Multinodular goiter. “Goiter” is a term used to describe any enlargement of the thyroid gland, which can be caused by iodine deficiency or a thyroid disorder. A multinodular goiter contains multiple distinct nodules within the goiter (enlarged thyroid gland), but its cause is less clear.
- Producing thyroid hormones (hot nodule)
- Not making thyroid hormones (cold nodule)
- Chronic inflammation of the thyroid (thyroiditis). Hashimoto’s disease, a thyroid disorder, can cause thyroid inflammation resulting in nodular enlargement. This often is associated with reduced thyroid gland activity (hypothyroidism).
Thyroid nodules are more common in women than in men. A person’s chance of getting a thyroid nodule increases with age.
Only a few thyroid nodules are due to thyroid cancer. A thyroid nodule is more likely to be cancer if you:
- Have a hard nodule
- Have a nodule that is stuck to nearby structures
- Have a family history of thyroid cancer
- Have noticed a change in your voice
- Are younger than 20 or older than 70
- Have a history of radiation exposure to the head or neck
- Are male
Causes of thyroid nodules are not always found, but can include:
- Hashimoto’s disease
- Iodine deficiency. Lack of iodine in your diet can sometimes cause your thyroid gland to develop thyroid nodules. But iodine deficiency is uncommon in the United States, where iodine is routinely added to table salt and other foods.
Thyroid nodules complications
Complications associated with thyroid nodules include:
- Problems swallowing or breathing. Large nodules or a multinodular goiter — an enlargement of the thyroid gland containing several distinct nodules — can interfere with swallowing or breathing.
- Hyperthyroidism. Problems can occur when a nodule or goiter produces thyroid hormone, leading to hyperthyroidism. Hyperthyroidism can result in weight loss, muscle weakness, heat intolerance, and anxiousness or irritability. Potential complications of hyperthyroidism include an irregular heartbeat (atrial fibrillation); weak bones (osteoporosis); and thyrotoxic crisis, a sudden and potentially life-threatening intensification of signs and symptoms that requires immediate medical care.
- Problems associated with thyroid cancer. If a thyroid nodule is cancerous, surgery is usually required. Generally, most or all of your thyroid gland is removed, after which you’ll need to take thyroid hormone replacement therapy for the rest of your life.
Thyroid nodules symptoms
Most thyroid nodules do not cause symptoms.
Large nodules can press against other structures in the neck. This can cause symptoms such as:
- A visible goiter (enlarged thyroid gland)
- Hoarseness or changing voice
- Pain in the neck
- Problems breathing, especially when lying down flat
- Problems swallowing food
Nodules that produce thyroid hormones will likely cause symptoms of overactive thyroid gland (hyperthyroidism), including:
- Warm, sweaty skin
- Fast pulse
- Increased appetite
- Nervousness
- Restlessness
- Skin blushing or flushing
- Weight loss
- Irregular menstrual periods
Older people with a nodule that produces too much thyroid hormone may have only vague symptoms, including:
- Fatigue
- Palpitations
- Chest pain
- Memory loss
Thyroid nodules are sometimes found in people who have Hashimoto’s disease.
This may cause symptoms of an underactive thyroid gland (hypothyroidism), such as:
- Dry skin
- Face swelling
- Fatigue
- Hair loss
- Feeling cold when other people do not
- Weight gain
- Irregular menstrual periods
Very often, nodules produce no symptoms. Health care providers find thyroid nodules only during a routine physical exam or imaging tests that are done for another reason. A few people have thyroid nodules that are big enough that they notice the nodule on their own, and ask a provider to examine their neck.
Thyroid nodules diagnosis
In assessing a lump or nodule in your neck, one of your doctor’s main goals is to rule out the possibility of cancer. But your doctor will also want to know if your thyroid is functioning properly.
Physical exam. You’ll likely be asked to swallow while your doctor examines your thyroid because a nodule in your thyroid gland will usually move up and down during swallowing.
Your doctor will also look for signs and symptoms of hyperthyroidism, such as tremor, overly active reflexes, and a rapid or irregular heartbeat; and signs and symptoms of hypothyroidism, such as a slow heartbeat, dry skin and facial swelling.
If a doctor finds a nodule or you have symptoms of a nodule, the following tests may be done:
- Thyroid function tests. Tests that measure blood levels of thyroxine (T4) and triiodothyronine (T3), hormones produced by your thyroid gland, and thyroid-stimulating hormone (TSH), which is released by your pituitary gland, can indicate whether your thyroid is producing too much thyroxine (hyperthyroidism) or too little (hypothyroidism).
- Thyroid nodules ultrasound. This imaging technique uses high-frequency sound waves rather than radiation to produce images. It provides the best information about the shape and structure of nodules. It may be used to distinguish cysts from solid nodules or to determine if multiple nodules are present. It may also be used as a guide in performing a fine-needle aspiration biopsy.
- Fine-needle aspiration (FNA) biopsy. Nodules are often biopsied to make sure no cancer is present. Fine-needle aspiration (FNA) biopsy helps to distinguish between benign and malignant thyroid nodules. During the procedure, your doctor inserts a very thin needle in the nodule and removes a sample of cells. The procedure, which is carried out in your doctor’s office, takes about 20 minutes and has few risks. Often, your doctor will use ultrasound to help guide the placement of the needle. The samples are then sent to a laboratory and analyzed under a microscope.
- Thyroid scan (nuclear medicine). In some cases, your doctor may recommend a thyroid scan to help evaluate thyroid nodules. During this test, an isotope of radioactive iodine is injected into a vein in your arm. You then lie on a table while a special camera produces an image of your thyroid on a computer screen. The length of a thyroid scan varies, depending on how long it takes the isotope to reach your thyroid gland. You may have some neck discomfort because your neck is stretched back during the scan, and you’ll be exposed to a small amount of radiation.
- Nodules that produce excess thyroid hormone — called hot nodules — show up on the scan because they take up more of the isotope than normal thyroid tissue does. Hot nodules are almost always noncancerous.
- Cold nodules are nonfunctioning and appear as defects or holes in the scan. A few cold nodules are cancerous. The disadvantage of a thyroid scan is that it can’t distinguish between benign and malignant cold nodules.
Thyroid nodules treatment
Treatment depends on the type of thyroid nodule you have.
Treating benign thyroid nodules
If a thyroid nodule isn’t cancerous, there are several treatment options:
- Watchful waiting. If a biopsy shows that you have a benign thyroid nodule, your doctor may suggest simply watching your condition. This usually means having a physical exam and thyroid function tests at regular intervals. You’re also likely to have another biopsy if the nodule grows larger. If a benign thyroid nodule remains unchanged, you may never need treatment.
- Careful follow-up with a physical exam and ultrasound
- A thyroid biopsy repeated 6 to 12 months after diagnosis, especially if the nodule has grown
- Another possible treatment is an ethanol (alcohol) injection into the nodule to shrink it.
- Thyroid hormone suppression therapy. This involves treating a benign thyroid nodule with levothyroxine (Levoxyl, Synthroid, others), a synthetic form of thyroxine that you take in pill form. The idea is that supplying additional thyroid hormone will signal the pituitary to produce less TSH, the hormone that stimulates the growth of thyroid tissue. Although this sounds good in theory, levothyroxine therapy is a matter of some debate. There’s no clear evidence that the treatment consistently shrinks nodules or even that shrinking small, benign nodules is necessary.
- Surgery. Occasionally, a thyroid nodule that’s clearly benign may require surgery, especially if it’s so large that it makes it hard to breathe or swallow. Surgery is also considered for people with large multinodular goiters, particularly when the goiters constrict airways, the esophagus or blood vessels. Nodules diagnosed as indeterminate or suspicious by a biopsy also need surgical removal, so they can be examined for signs of cancer.
Percutaneous ethanol injection has been studied in several large randomized controlled studies, with reported success in 82–85% of the cases after an average of 2 sessions, with a volume reduction of more than 85% from baseline size 22. Percutaneous ethanol injection may also be considered for hyperfunctioning nodules, particularly if a large fluid component is present. It has a success rate ranging from 64% to 95% 23, with a mean volume reduction of 66% 23, but recurrences are more common and the number of sessions required to achieve good response is higher (about 4 sessions per patient). Percutaneous ethanol injection is a safe procedure, with the most common reported adverse effects being local pain, dysphonia, flushing, dizziness, and, rarely, recurrent laryngeal nerve damage 22.
Treating thyroid nodules that cause hyperthyroidism
If a thyroid nodule is producing thyroid hormones, overloading your thyroid gland’s normal hormone production levels, your doctor may recommend treating you for hyperthyroidism.
This may include:
- Radioactive iodine. Doctors often use radioactive iodine to treat hyperfunctioning adenomas or multinodular goiters. Taken as a capsule or in liquid form, radioactive iodine is absorbed by your thyroid gland. This causes the thyroid nodules to shrink and signs and symptoms of hyperthyroidism to subside, usually within two to three months. Pregnant women are NOT given this treatment.
- Anti-thyroid medications. In some cases, your doctor may recommend an anti-thyroid medication such as methimazole (Tapazole) to reduce symptoms of hyperthyroidism. Treatment is generally long term and can have serious side effects on your liver, so it’s important to discuss the treatment’s risks and benefits with your doctor.
- Surgery. If treatment with radioactive iodine or anti-thyroid medications isn’t an option, you may be a candidate for surgery to remove the overactive thyroid nodule. Surgery also carries certain risks that should be thoroughly discussed with your doctor.
Both surgery to remove thyroid gland tissue and radioactive iodine treatment can cause lifelong hypothyroidism (underactive thyroid). This condition needs to be treated with thyroid hormone replacement.
Treating cancerous nodules
Treatment for a nodule that’s cancerous usually involves surgery.
- Surgery. The usual treatment for malignant nodules is surgical removal, often along with the majority of thyroid tissue — a procedure called near-total thyroidectomy. Risks of thyroid surgery include damage to the nerve that controls your vocal cords (laryngeal nerve) and damage to your parathyroid glands — four tiny glands located on the back of your thyroid gland that help control the level of calcium in your blood. After a thyroidectomy, you’ll need lifelong treatment with levothyroxine to supply your body with normal amounts of thyroid hormone.
- Alcohol ablation. Another option for management of certain small cancerous nodules is alcohol ablation. This technique involves injecting a small amount of alcohol in the cancerous thyroid nodule. This treatment is helpful for treating cancer that occurs in areas that aren’t easily accessible during surgery. Multiple treatment sessions are often required.
Thyroid nodules surgery
Your doctor may recommend surgery to remove all or part of your thyroid gland if the nodule is:
- A small thyroid growth (nodule or cyst)
- A thyroid gland that is making too much thyroid hormone that it’s so overactive it is dangerous (thyrotoxicosis)
- Cancer of the thyroid
- If the fine needle biopsy is inconclusive, and your doctor can’t tell whether the thyroid nodule is a cancer
- Noncancerous (benign) tumors of the thyroid that are causing symptoms such as swallowing or breathing problems
- Thyroid swelling (nontoxic goiter) that makes it hard for you to breathe or swallow
You may also have surgery if you have an overactive thyroid gland and do not want to have radioactive iodine treatment, or you cannot be treated with antithyroid medicines.
Thyroid gland removal is surgery to remove all or part of the thyroid gland. The thyroid gland is part of the hormone (endocrine) system. It helps your body regulate your metabolism.
Depending on the reason you are having your thyroid gland removed, the type of thyroidectomy you have will be either a:
- Total thyroidectomy, which removes the entire gland
- Subtotal or partial thyroidectomy, which removes part of the thyroid gland
Before the Procedure
During the weeks before your surgery:
- You may need to have tests that show exactly where the abnormal thyroid growth is located. This will help the surgeon find the growth during surgery. You may have a CT scan, ultrasound, or other imaging tests.
- Your doctor may also do a fine needle aspiration to find out if the growth is noncancerous or cancerous. Before surgery, your vocal cord function may be checked.
- You may also need thyroid medicine or iodine treatments 1 to 2 weeks before your surgery.
Several days to a week before surgery:
- You may be asked to stop taking medicines that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil), naproxen (Aleve), clopidogrel (Plavix), warfarin (Coumadin).
- Fill any prescriptions for pain medicine and calcium you will need after surgery.
- Tell your health care provider about all the medicines you take, even those bought without a prescription. This includes herbs and supplements. Ask your provider which medicines you should still take on the day of surgery.
- If you smoke, try to stop. Ask your provider for help.
On the day of surgery:
- Follow instructions about when to stop eating and drinking.
- Take any medicines that your provider told you to take with a small sip of water.
- Be sure to arrive at the hospital on time.
You will have general anesthesia (asleep and pain-free) for this surgery. In rare cases, the surgery is done with local anesthesia and medicine to relax you. You will be awake, but pain-free.
During the surgery:
- The surgeon makes a 3- to 4-inch (7.5 to 10 centimeters) cut in the middle of your neck, right on top of the thyroid gland. Or, the surgeon makes a smaller cut less than 2 inches (5 centimeters) long.
- All or part of the gland is removed through the cut.
- The surgeon is careful not to damage the blood vessels and nerves in your neck.
- A small tube (catheter) may be placed into the area to help drain blood and other fluids that build up. The drain will be removed in 1 or 2 days.
- The cuts are closed with sutures (stitches).
Surgery to remove your whole thyroid may take up to 4 hours. It may take less time if only part of the thyroid is removed.
After the Procedure
You will probably go home the day after surgery. In rare cases, you may need to spend up to 3 days in the hospital. You must be able to swallow liquids before you can go home.
Your provider may check the calcium level in your blood after surgery. This is done more often when the whole thyroid gland is removed.
You may have some pain after surgery. Ask your provider for instructions on how to take pain medicines after you go home.
You will likely be able to get up and walk on the day after surgery. It should take about 3 to 4 weeks for you to fully recover.
Follow any instructions for taking care of yourself after you go home.
Thyroid nodules surgery risks
Risks of anesthesia and surgery in general include:
- Reactions to medicines, breathing problems
- Bleeding, blood clots, infection
Risks of thyroidectomy include:
- Injury to the nerves in your vocal cords and larynx.
- Bleeding and possible airway obstruction.
- A sharp rise in thyroid hormone levels (only around the time of surgery).
- Injury to the parathyroid glands (small glands near the thyroid) or to their blood supply. This can cause a temporary low level of calcium in your blood (hypocalcemia).
- Too much thyroid hormone (thyroid storm). If you have an overactive thyroid gland, you will be treated with medicine.
Thyroid nodules surgery outlook (prognosis)
Outcome of this surgery is usually excellent. Most people need to take thyroid hormone pills (thyroid hormone replacement) for the rest of their lives when the whole gland is removed.
- Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer., Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. Thyroid. 2009 Nov; 19(11):1167-214. https://deepblue.lib.umich.edu/bitstream/handle/2027.42/78131/thy.2009.0110.pdf[↩]
- Singer PA, Cooper DS, Daniels GH, et al. Treatment guidelines for patients with thyroid nodules and well-differentiated thyroid cancer. American Thyroid Association. Arch Intern Med. 1996;156(19):2165–72. https://www.ncbi.nlm.nih.gov/pubmed/8885814[↩]
- Tan GH, Gharib H. Thyroid incidentalomas: management approaches to non-palpable nodules discovered incidentally on thyroid imaging. Ann Intern Med. 1997;126(3):226–31. https://www.ncbi.nlm.nih.gov/pubmed/9027275[↩][↩]
- Guth S, Theune U, Aberle J, et al. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest. 2009;39(8):699–706. https://www.ncbi.nlm.nih.gov/pubmed/19601965[↩]
- Mortensen JD, Woolner LB, Bennett WA. Gross and microscopic findings in clinically normal thyroid glands. J Clin Endocrinol Metab. 1955;15(10):1270–80. https://www.ncbi.nlm.nih.gov/pubmed/13263417[↩]
- Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med. 1993;328(8):553–9. http://www.nejm.org/doi/full/10.1056/NEJM199302253280807[↩]
- Kung AW, Chau MT, Lao TT, et al. The effect of pregnancy on thyroid nodule formation. J Clin Endocrinol Metab. 2002;87(3):1010–4. https://www.ncbi.nlm.nih.gov/pubmed/11889153[↩]
- DeGroot LJ. Clinical review 2: diagnostic approach and management of patients exposed to irradiation to the thyroid. J Clin Endocrinol Metab. 1989;69(5):925–8. https://www.ncbi.nlm.nih.gov/pubmed/2793993[↩]
- Popoveniuc G, Jonklaas J. Thyroid Nodules. The Medical clinics of North America. 2012;96(2):329-349. doi:10.1016/j.mcna.2012.02.002. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3575959/[↩][↩][↩]
- Frates MC, Benson CB, Doubilet PM, et al. Prevalence and distribution of carcinoma in patients with solitary and multiple thyroid nodules on sonography. J Clin Endocrinol Metab. 2006;91(9):3411–7. https://www.ncbi.nlm.nih.gov/pubmed/16835280[↩]
- Cooper DS. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–214. https://www.ncbi.nlm.nih.gov/pubmed/19860577[↩]
- Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;237(3):794–800. http://pubs.rsna.org/doi/full/10.1148/radiol.2373050220[↩]
- Papini E, Guglielmi R, Bianchini A, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002;87(5):1941–6. https://www.ncbi.nlm.nih.gov/pubmed/11994321[↩][↩][↩]
- Papini E. The dilemma of non-palpable thyroid nodules. J Endocrinol Invest. 2003;26(1):3–4. https://www.ncbi.nlm.nih.gov/pubmed/12602527[↩][↩]
- Frates MC, Benson CB, Doubilet PM, et al. Radiological Society of North America Scientific Assembly and Annual Meeting Program. Radiological Society of North America; Oak Brook (IL): 2004. Likelihood of thyroid cancer based on sonographic assessment of nodule size and composition [abstract]. p. 395.[↩][↩]
- Frasoldati A, Valcavi R. Challenges in neck ultrasonography: lymphadenopathy and parathyroid glands. Endocr Pract. 2004;10(3):261–8. https://www.ncbi.nlm.nih.gov/pubmed/15310545[↩][↩]
- Kim EK, Park CS, Chung WY, et al. New sonographic criteria for recommending fine-needle aspiration biopsy of nonpalpable solid nodules of the thyroid. AJR Am J Roentgenol. 2002;178(3):687–91. https://www.ncbi.nlm.nih.gov/pubmed/11856699[↩]
- Gharib H, Papini E, Valcavi R, et al. American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2006;12(1):63–102 https://www.ncbi.nlm.nih.gov/pubmed/16596732[↩]
- Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations. J Endocrinol Invest. 2010;33(Suppl 5):51–6. https://www.ncbi.nlm.nih.gov/pubmed/20543551[↩]
- Frates MC. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology 2005;237(3):794–800[↩]
- Cooper D. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009;19(11):1167–214[↩]
- Bennedbaek FN, Hegedus L. Treatment of recurrent thyroid cysts with ethanol: a randomized double-blind controlled trial. J Clin Endocrinol Metab. 2003;88(12):5773–7. https://www.ncbi.nlm.nih.gov/pubmed/14671167[↩][↩]
- Tarantino L, Francica G, Sordelli I, et al. Percutaneous ethanol injection of hyperfunctioning thyroid nodules: long-term follow-up in 125 patients. AJR Am J Roentgenol. 2008;190(3):800–8. https://www.ncbi.nlm.nih.gov/pubmed/18287455[↩][↩]





{kind=link}