Contents
What is thyrotropin
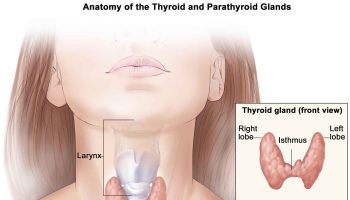
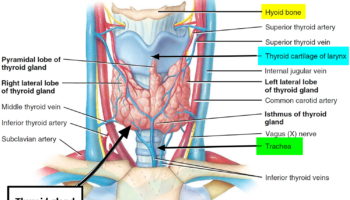
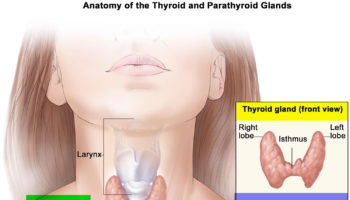
Thyrotropin also called thyroid-stimulating hormone (TSH) is a regulator of thyroid function. Thyrotropin (TSH) is a heterodimeric 28-kDa-glycoprotein hormone released from the anterior pituitary gland, a small organ located below the brain and behind the sinus cavities 1. Thyrotropin (TSH) stimulates your thyroid gland, a small butterfly-shaped gland located inside the neck in front of the windpipe, by binding to the TSH receptor to release the hormones thyroxine (T4) and triiodothyronine (T3) into the blood. Thyrotropin (TSH) synthesis is controlled by the hypothalamic neuropeptide thyrotropin-releasing hormone (TRH).
Thyroxine (T4) and triiodothyronine (T3) help control the rate at which the body uses energy. Most of the hormone produced by the thyroid gland is T4. This hormone is relatively inactive, but it is converted into the much more active T3 in the liver and other tissues.
Thyrotropin, along with its regulatory hormone thyrotropin releasing hormone (TRH), which comes from the hypothalamus, is part of the feedback system that the body uses to maintain stable amounts of thyroid hormones in the blood.
When thyroid hormone levels decrease in the blood, the pituitary gland produces more thyrotropin in response to TRH stimulation. thyrotropin in turn stimulates the thyroid to produce and release more T4 and T3.
When thyroid hormone levels increase in the blood, the pituitary gland produces less thyrotropin, and the thyroid produces less T4 and T3.
When all three organs (hypothalamus, pituitary and thyroid) are functioning normally, thyroid production is regulated to maintain relatively stable levels of thyroid hormones in the blood.
If the thyroid releases inappropriately large amounts of T4 and T3, the affected person may experience symptoms associated with overactive thyroid (hyperthyroidism), such as rapid heart rate, weight loss, nervousness, hand tremors, irritated eyes, and difficulty sleeping. Graves disease is the most common cause of hyperthyroidism. It is a chronic autoimmune disorder in which the affected person’s immune system produces autoantibodies that act like thyrotropin, bind and activate the thyrotropin receptor, leading to the production of excessive amounts of thyroid hormone. In response, the pituitary produces less thyrotropin, usually leading to a low level in the blood.
If there is decreased production of thyroid hormones by the thyroid (underactive thyroid or hypothyroidism), the person may experience symptoms such as weight gain, dry skin, constipation, cold intolerance, and fatigue. Hashimoto thyroiditis is the most common cause of hypothyroidism in the U.S. It is a chronic autoimmune condition in which the immune response causes inflammation and damage to the thyroid as well as the production of autoantibodies. However, the autoantibodies do not cause the hypothyroidism. The detection of thyroid-related autoantibodies (e.g., thyroperoxidase autoantibodies and/or thyroglobulin autoantibodies) indicate that thyroid autoimmunity is present. These autoantibodies can be detected in Graves disease or Hashimoto thyroiditis. With Hashimoto thyroiditis, the thyroid produces low levels of thyroid hormone. In response, the pituitary normally produces more thyrotropin, usually resulting in a high level in the blood.
However, the level of thyrotropin alone does not always predict or reflect thyroid hormone levels. Some people with pituitary disease produce an abnormal form of thyrotropin that does not function properly. They often have hypothyroidism despite having normal or even mildly elevated thyrotropin levels.
Rarely, pituitary dysfunction may result in increased or decreased amounts of thyrotropin. In addition to pituitary dysfunction, hyperthyroidism or hypothyroidism can occur if there is a problem with the hypothalamus (insufficient or excessive TRH).
Thyrotropin chemical structure
Thyrotropin (TSH) is a glycoprotein hormone consisting of 2 subunits. The alpha subunit is similar to those of follicle-stimulating hormone, human chorionic gonadotropin, and luteinizing hormone. The beta subunit is different from those of the other glycoprotein hormones and confers its biochemical specificity. The two peptide subunits of thyrotropin (TSH) are noncovalently linked and cotranslationally glycosylated with mannose-rich oligosaccharides 2. Posttranslationally, the two subunits are combined and the attached oligosaccharides are further processed. Synthesis of a mature thyrotropin (TSH) molecule requires the excision of signal peptides from both thyrotropin (TSH) α- and β-subunits, followed by trimming of mannose and further addition of fucose, galactose, and sialic acids 3. Thus, mature thyrotropin (TSH) molecules are asparagine-(N)-linked [Asp(N)-linked] complex carbohydrate structures capped with sulfate and/or sialic acid molecules (see Figure 2) 4. Thyrotropin (TSH) oligosaccharide structures vary according to the source of thyrotropin (TSH) : human pituitary–derived thyrotropin (TSH) comprises fucosylated biantennary glycans with terminal N-acetylgalactosamine sulfate and low sialic acid content 5, while recombinant human thyrotropin (rhTSH), synthesized in Chinese hamster ovary cells, specifically terminates in α2,3-linked sialic acid 6 and recombinant human thyrotropin (rhTSH) formed in yeast lacks sialic acid residues altogether 7.
Figure 1. Thyroid gland
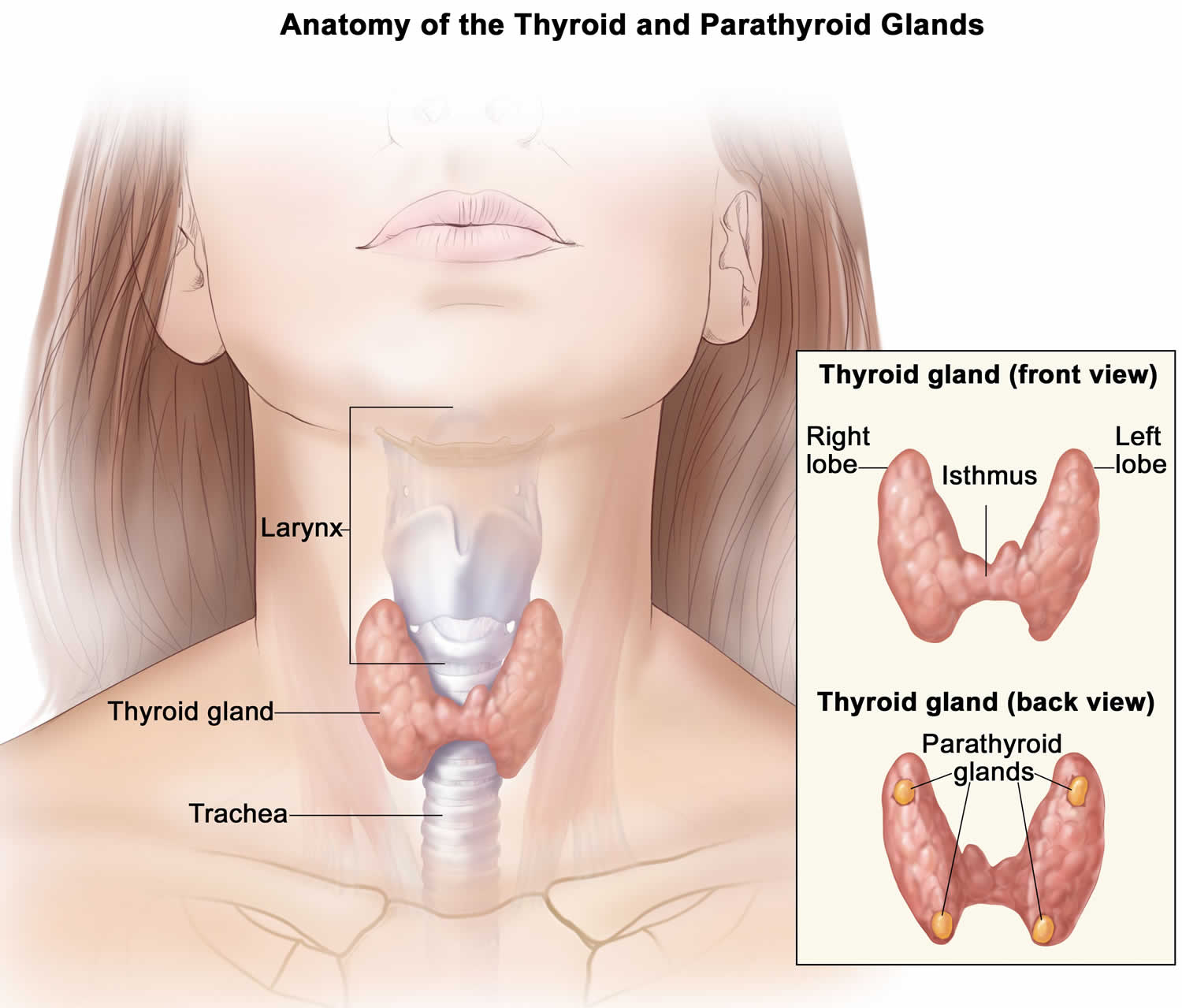
Figure 2. Thyrotropin
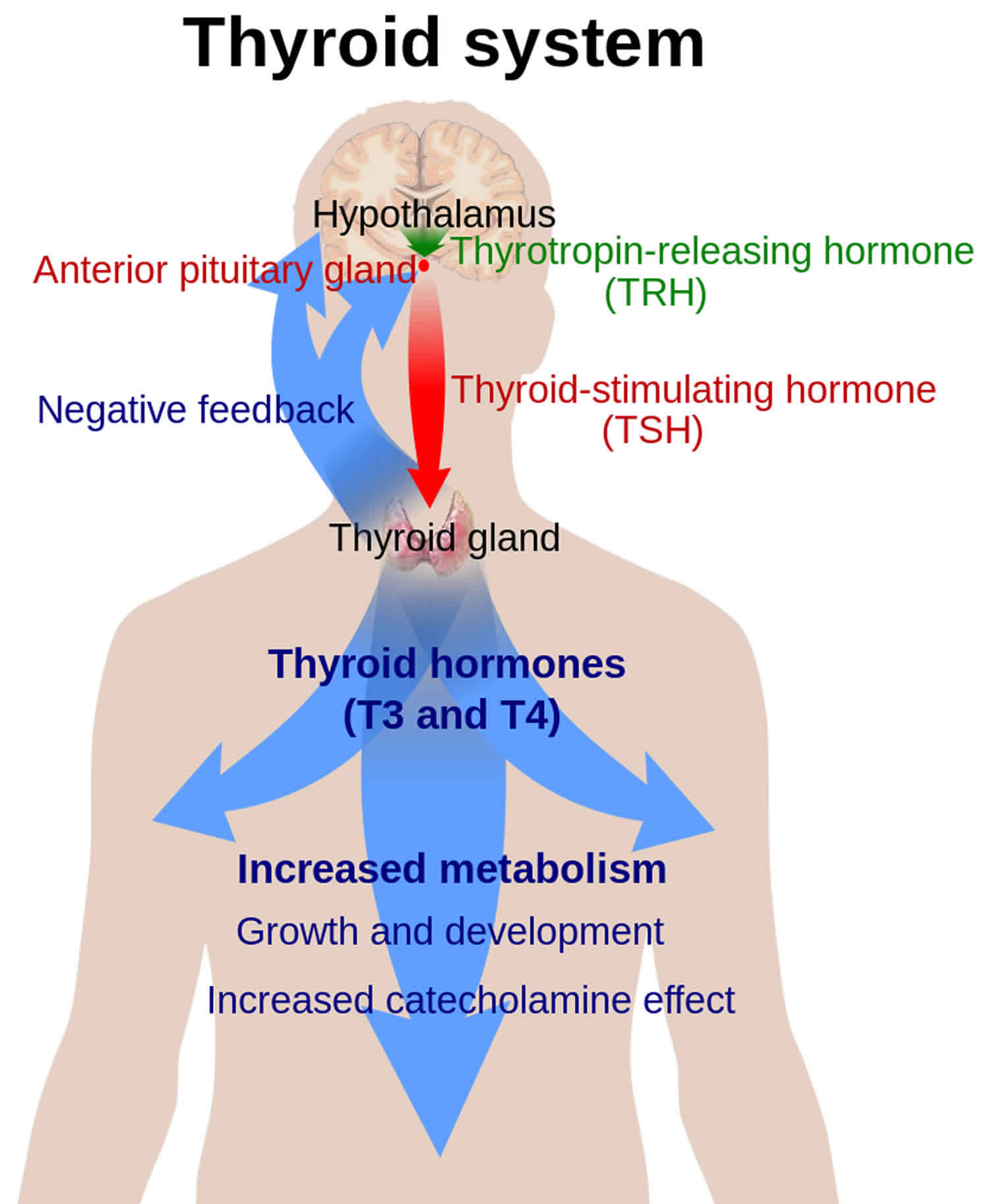
Figure 3. Thyrotropin structure
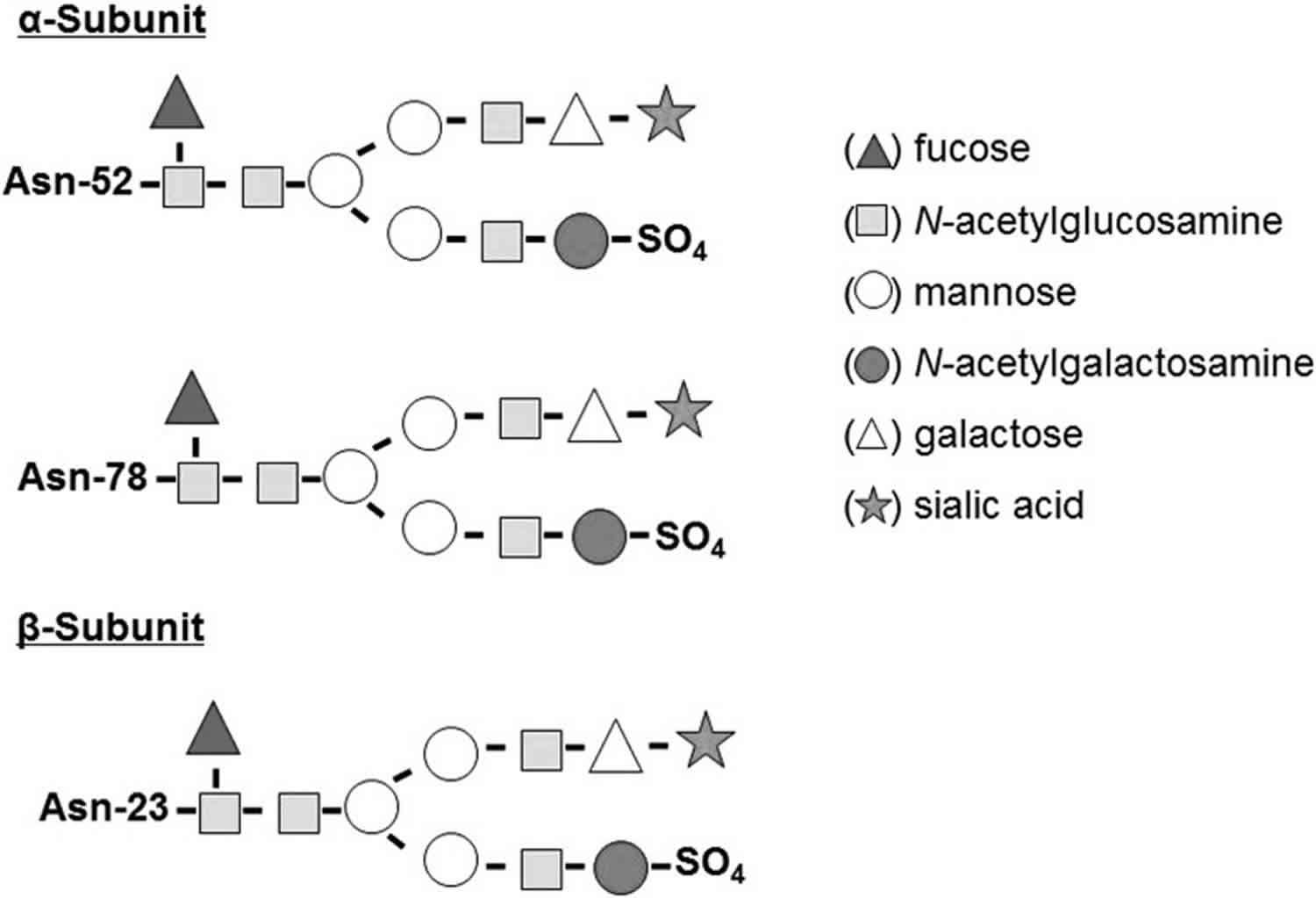
Footnote: Thyrotropin α- and β-subunits. A normal human Thyrotropin (TSH) molecule contains an α-subunit with two oligosaccharide chains (located at Asn-52 and Asn-78) and a β-subunit with one oligosaccharide chain (located at Asn-23). Each subunit contains a terminal sialic acid and a sulfate residue that confer TSH binding and biological activity.
Abbreivations: Asn = asparagine; TSH = thyrotropin.
[Source 1 ]Thyrotropin function
Thyrotropin-releasing hormone (TRH) from the hypothalamus and thyrotropin or thyroid-stimulating hormone (TSH) from the anterior pituitary stimulate secretion of thyroid hormones, as shown in Figure 4:
- Low blood levels of T3 and T4 or low metabolic rate stimulate the hypothalamus to secrete thyrotropin-releasing hormone (TRH).
- Thyrotropin-releasing hormone (TRH) enters the hypothalamic–hypophyseal portal system and flows to the anterior pituitary, where it stimulates thyrotrophs to secrete thyroid stimulating hormone (TSH) or thyrotropin.
- Thyrotropin or thyroid stimulating hormone (TSH) stimulates virtually all aspects of thyroid follicular cell activity, including iodide trapping, hormone synthesis and secretion, and growth of the follicular cells.
- The thyroid follicular cells release T3 and T4 into the blood until the metabolic rate returns to normal.
- An elevated level of T3 inhibits release of thyrotropin-releasing hormone (TRH) and thyrotropin (TSH) (negative feedback inhibition).
Conditions that increase ATP demand—a cold environment, hypoglycemia, high altitude, and pregnancy—increase the secretion of the thyroid hormones.
Thyrotropin (TSH) is synthesized and secreted by the anterior pituitary in response to a negative feedback mechanism involving concentrations of free triiodothyronine (free T3) and free thyroxine (free T4). Additionally, the hypothalamic tripeptide, thyrotropin-releasing hormone (TRH), directly stimulates thyrotropin (TSH) production. Thyrotropin (TSH) interacts with specific cell receptors on the thyroid cell surface and gives rise to 2 main actions. First, it stimulates cell reproduction and hypertrophy. Second, it stimulates the thyroid gland to synthesize and secrete triiodothyronine (T3) and thyroxine (T4).
Thyrotropin (TSH) modulates the release of triiodothyronine (T3) or thyroxine (T4) from thyroid follicular cells. Thyroxine (T4) is deiodinated to triiodothyronine (T3), which is a more potent thyroid hormone. While about 20% of triiodothyronine (T3) originates from the thyroid gland, 80% of triiodothyronine (T3) is produced by peripheral conversion via a deiodinase. More than 99% of thyroid hormone is protein bound to thyroid binding globulin, prealbumin, and albumin. Triiodothyronine (T3) then binds to its receptor in the nucleus; this activates the transcription of DNA, which promotes translation of mRNA, which activates the synthesis of new proteins.
These new proteins influence many organ systems, promoting growth and bone maturation as well as maturation of the central nervous system (CNS) 8. The basal metabolic rate is increased, with an increase in synthesis of Na+-K+ ATPases, increase in oxygen consumption, and increased heat production. Metabolism is activated as well, with an increase in glucose absorption, glycogenolysis, gluconeogenesis, lipolysis, and protein synthesis and degradation (net catabolic). These proteins also influence the cardiovascular system by increasing cardiac output by increasing the number of beta-1 receptors on the myocardium such that the myocardium is more sensitive to stimulation by the sympathetic nervous system, thereby increasing contractility 9.
Figure 4. Control of thyroid hormone secretion
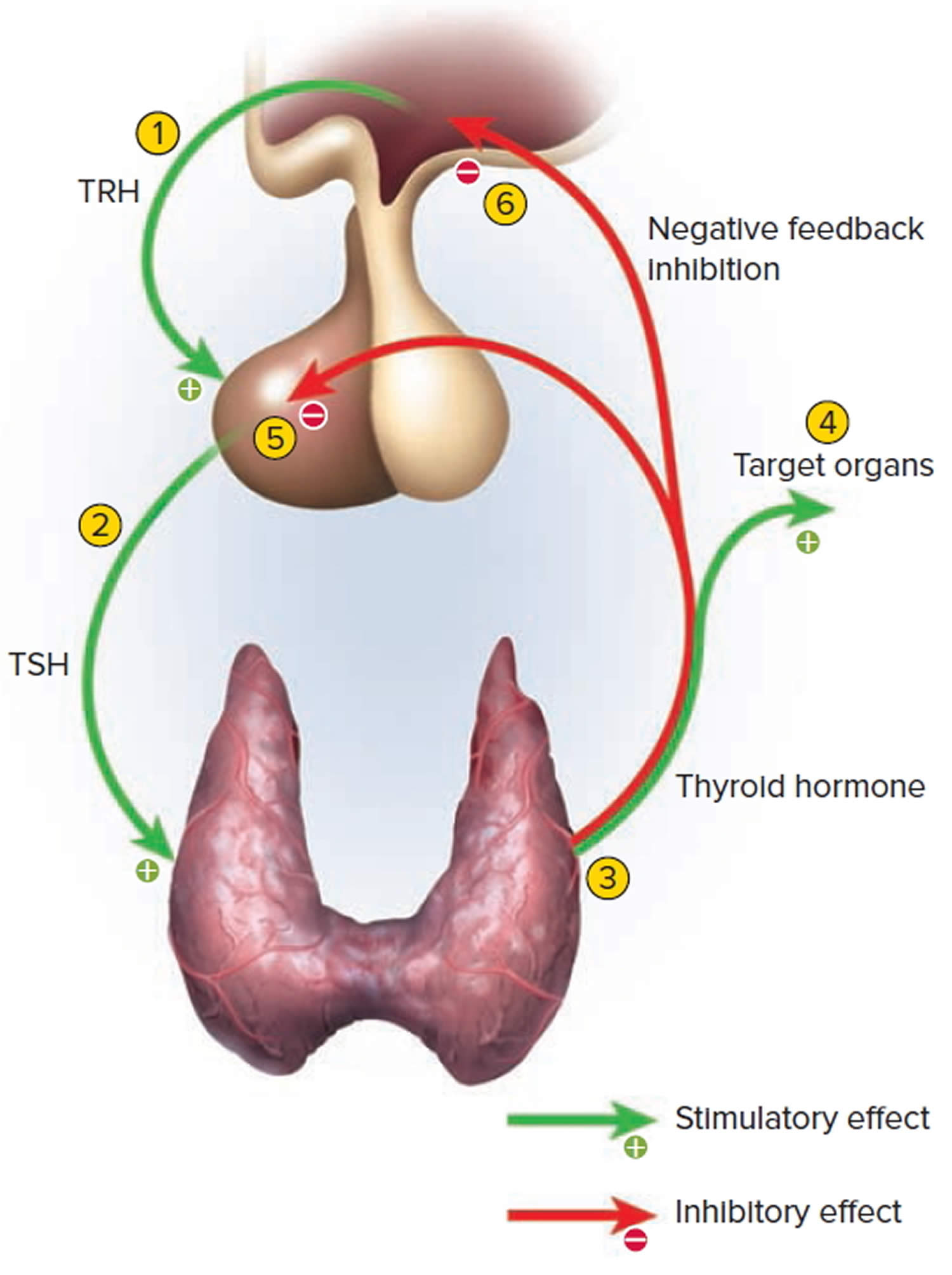
Footnote: Negative Feedback Inhibition of the Anterior Pituitary Gland by the Thyroid Gland
Thyrotropin test
The thyrotropin test is often the test of choice for initially evaluating thyroid function and/or symptoms of a thyroid disorder, including overactive or underactive thyroid (hyperthyroidism or hypothyroidism).
Serum thyrotropin (TSH) concentrations exhibit a diurnal variation with the peak occurring during the night and the nadir occurring between 10 a.m. and 4 p.m. This biological variation does not influence the interpretation of the test result since most clinical thyrotropin (TSH) measurements are performed on ambulatory patients between 8 a.m. and 6 p.m.
When hypothalamic-pituitary function is normal, a log/linear inverse relationship between serum thyrotropin (TSH) and free thyroxine exists.
A thyrotropin test is frequently ordered along with or prior to a free thyroxine (free T4) test. Other thyroid tests that may be ordered include total or free triiodothyronine (free T3) tests and thyroid antibodies (if autoimmune-related thyroid disease is suspected). Thyrotropin, free T4 and sometimes free T3 may be ordered together as a thyroid panel. Total triiodothyronine (T3) and free T3 should not both be ordered.
Thyrotropin testing may be used with free T4 and sometimes total or free T3 tests to:
- Help diagnose a thyroid disorder in a person with signs and symptoms
- Monitor thyroid replacement therapy in people with hypothyroidism
- Monitor anti-thyroid treatment in people with hyperthyroidism
- Help evaluate the function of the pituitary gland (occasionally)
To assess whether thyroid disease is primary or secondary, the thyrotropin (TSH) must be evaluated in comparison to triiodothyronine (T3) or thyroxine (T4) levels. If thyrotropin (TSH) and triiodothyronine (T3) or thyroxine (T4) both increase or both decrease together, this indicates either secondary (central) hypothyroidism or secondary hyperthyroidism. However, if the thyrotropin (TSH) and triiodothyronine (T3) or thyroxine (T4) change in the opposite directions, this indicates primary thyroid disease 10.
- In primary thyroid disease (the disease that originates in the thyroid gland itself): If the thyroid gland is secreting high levels of triiodothyronine (T3) or thyroxine (T4), this will negatively feedback on the anterior pituitary and thus, decrease the secretion of thyrotropin (TSH). If the thyroid gland is secreting low levels of triiodothyronine (T3) or thyroxine (T4), the absence of negative feedback on the anterior pituitary will increase thyrotropin (TSH) secretion from the anterior pituitary.
- For secondary disease or central hyperthyroid or hypothyroid disease (the disease that originates in the anterior pituitary itself): If a tumor in the anterior pituitary is secreting excessively high thyrotropin (TSH), this will stimulate the thyroid follicular cells to secrete high levels of triiodothyronine (T3) or thyroxine (T4). If the anterior pituitary is secreting low levels of thyrotropin (TSH) such as in panhypopituitarism, this lack of stimulation of thyroid follicular cells will cause them to secrete low levels of thyroxine (T4).
At present, screening the general population for thyroid disorders is not recommended. However, expert opinions vary on this. In 2015, the U.S. Preventive Services Task Force found insufficient evidence to recommend for or against routine screening for thyroid disease in asymptomatic adults.
On the other hand, guidelines released in 2012 by the American Thyroid Association and the American Association of Clinical Endocrinologists summarize recommendations endorsed by several societies. They say that screening for hypothyroidism should be considered in people over the age of 60. Because the signs and symptoms of both hypothyroidism and hyperthyroidism are so similar to those seen in many common disorders, healthcare practitioners often need to rule out thyroid disease even though the patient has another problem.
Normal thyrotropin levels
- Age 0-5 days: 0.7-15.2 mIU/L
- Age 6 days-2 months: 0.7-11.0 mIU/L
- Age 3-11 months: 0.7-8.4 mIU/L
- Age 1-5 years: 0.7-6.0 mIU/L
- Age 6-10 years: 0.6-4.8 mIU/L
- Age 11-19 years: 0.5-4.3 mIU/L
- Age > or =20 years: 0.3-4.2 mIU/L
When is thyrotropin test ordered?
Your doctor may order a thyrotropin (TSH) test when you have signs and symptoms of hyperthyroidism (overactive thyroid) or hypothyroidism (underactive thyroid) and/or when you have an enlarged thyroid gland (goiter) or thyroid nodule.
Signs and symptoms of hyperthyroidism (overactive thyroid) may include:
- Increased heart rate
- Anxiety
- Weight loss
- Difficulty sleeping
- Tremors in the hands
- Weakness
- Diarrhea (sometimes)
- Light sensitivity, visual disturbances
- There may be puffiness around the eyes with dryness, irritation, and, in some cases, bulging of the eyes.
- Menstrual irregularity in women
Signs and symptoms of hypothyroidism (underactive thyroid) may include:
- Weight gain
- Dry skin
- Constipation
- Cold intolerance
- Puffy skin
- Hair loss
- Fatigue
- Menstrual irregularity in women and/or fertility problems in women
Thyrotropin (TSH) may be ordered at regular intervals when an individual is being treated for a known thyroid disorder. When a person’s dose of thyroid medication is adjusted, the American Thyroid Association recommends waiting 6-8 weeks before testing the level of thyrotropin (TSH) again.
What does the thyrotropin test result mean?
Thyrotropin (TSH) results may be evaluated with other thyroid testing results (i.e., free T4 and sometimes total or free T3).
A high thyrotropin (TSH) result may mean that:
- The person tested has an underactive thyroid gland that is not responding adequately to the stimulation of thyrotropin (TSH) due to some type of acute or chronic thyroid dysfunction; Hashimoto thyroiditis is the most common cause of hypothyroidism.
- A person with hypothyroidism or who has had their thyroid gland removed is receiving too little thyroid hormone replacement medication and the dose may need to be adjusted
- A person with hyperthyroidism is receiving too much anti-thyroid medication and the dose needs adjusting
- There is a problem with the pituitary gland, such as a tumor producing unregulated levels of thyrotropin (TSH)
- A rare inherited disorder is present in which the body and/or pituitary do not respond normally to thyroid hormones, resulting in high thyrotropin (TSH) despite clinically normal thyroid function
A low thyrotropin (TSH) result may indicate:
- An overactive thyroid gland (hyperthyroidism); Graves disease is the most common cause of hyperthyroidism.
- Excessive amounts of thyroid hormone medication taken by those who are being treated for an underactive (or removed) thyroid gland
- Insufficient anti-thyroid medication in a person being treated for hyperthyroidism; however, it may take a while for thyrotropin (TSH) production to resume after successful anti-thyroid treatment. This is why the American Thyroid Association recommends monitoring this treatment with tests for thyroid hormones (free T4 and total and free T3) as well as thyrotropin (TSH) levels.
- Damage to the pituitary gland that prevents it from producing adequate amounts of thyrotropin (TSH)
- People with thyroid cancer may be treated with medications intended to suppress thyroid hormones, so they may have a low thyrotropin (TSH).
Whether high or low, an abnormal thyrotropin (TSH) indicates an excess or deficiency in the amount of thyroid hormone available to the body, but it does not indicate the reason why. An abnormal thyrotropin (TSH) test result is usually followed by additional testing to investigate the cause of the increase or decrease.
The following table summarizes some examples of typical test results and their potential meaning.
Note: Laboratory results must always be correlated with the clinical findings of the patient.
It is important to note that thyrotropin (TSH), free T4, and free T3 tests are a “snapshot” of what is occurring within a dynamic system. An individual person’s thyroid testing results may vary and may be affected by:
- Increases, decreases, and changes (inherited or acquired) in the proteins that bind thyroid hormone (This is important for tests that measure total T3 but it is not likely important for free T4 and free T3 tests, which measure the thyroid hormones that are not bound to protein.)
- Pregnancy
- Liver disease
- Systemic illness
- Rarely, resistance to thyroid hormones
Illnesses not directly related to the thyroid, “nonthyroidal illnesses,” can affect thyroid hormones levels. In particular, the level of T3 can be low in nonthyroidal illness. Typically, the thyroid hormone levels return to normal after a person recovers from the nonthyroidal illness. Historically, this condition was referred to as “euthyroid sick syndrome” but that term is controversial because there is some question as to whether those affected have a thyroid gland that is functioning normally (euthyroid). Nevertheless, there is little data to support the treatment of nonthyroidal illness with thyroid hormone.
Table 1. Thyroid function test results interpretation
| Thyrotropin (TSH) | Free T4 | Total or Free T3 | Most likely diagnosis |
|---|---|---|---|
| Normal | Normal | Normal | Normal thyroid function (e.g., “euthyroid”) |
| Normal or decreased | Normal or decreased | Decreased | Normal adjustment in thyroid function due to illness (nonthyroidal illness or sick euthyroid syndrome) |
| Increased | Normal | Normal | Subclinical hypothyroidism1; in a person with hypothyroidism on treatment, not enough thyroid hormone is being given |
| Increased | Decreased | Normal of decreased | Hypothyroidism resulting from a problem with the thyroid gland itself (primary hypothyroidism) |
| Normal or increased | Increased | Increased | Hyperthyroidism resulting from a problem with the pituitary gland signals (central hyperthyroidism) or from a problem with the thyroid hormone receptor (thyroid hormone resistance) |
| Decreased | Normal | Normal | Subclinical hyperthyroidism2; in a person with hypothyroidism, too much thyroid hormone is being given |
| Decreased | Normal | Increased | Hyperthyroidism resulting from the thyroid gland making too much active thyroid hormone T3 (uncommon, also known as T3 toxicosis) |
| Decreased | Increased | Increased | Hyperthyroidism resulting from the gland making too much thyroid hormones (primary hyperthyroidism) |
| Decreased | Decreased | Decreased | Hypothyroidism resulting from a problem with the hypothalamus or pituitary signals that govern the thyroid gland (central hypothyroidism) |
Footnotes:
- 1) In affected adults, the diagnosis of subclinical hypothyroidism is applied when the thyrotropin (TSH) level is elevated and the free T4 level is normal on repeat testing over a number of weeks or months. Adults with subclinical hypothyroidism may have few or no overt symptoms of hypothyroidism. However, subclinical hypothyroidism places affected adults at somewhat increased risk for an elevated LDL cholesterol level, increased risk for cardiovascular disease, and reduced mental acuity.
- 2) In affected adults, the diagnosis of subclinical hyperthyroidism is applied when the thyrotropin (TSH) level is decreased and the free T4 level and T3 levels are normal on repeat testing over a number of weeks or months. Adults with subclinical hyperthyroidism may have few or no overt symptoms of hyperthyroidism. However, subclinical hyperthyroidism places affected persons at somewhat increased risk for atrial fibrillation and osteoporosis.
Are there things that I can do to raise or lower my thyrotropin level?
In general, thyrotropin (TSH) does not respond to lifestyle changes. What is important is that the pituitary and thyroid glands are healthy and working together to produce appropriate amounts of thyroid hormone.
What medications can affect a thyrotropin test?
Many multivitamins, supplements (especially hair and nail), and over-the-counter and prescription medications may affect thyroid test results and their use should be discussed with your healthcare practitioner prior to testing. For example, biotin (vitamin B7) can interfere with some lab tests, so your healthcare practitioner may advise you to refrain from taking biotin or supplements that contain biotin for a few days before having blood drawn for a thyrotropin (TSH) test. If you have a procedure done in which fluorescein dyes are injected into your blood (e.g., angiography), you may need to wait a few days before having a thyrotropin (TSH) test done.
Do healthcare practitioners test thyrotropin during pregnancy?
Pregnancy causes normal changes in the function of many endocrine glands, including the thyroid gland. Healthcare practitioners do not generally test asymptomatic women, but those with symptoms and/or a known thyroid disorder will usually be tested at intervals to detect and monitor hyperthyroidism or hypothyroidism during pregnancy and after delivery of the baby.
Some experts have advocated screening pregnant women for elevated thyrotropin (TSH) during the first trimester (or preconception) even if they do not have a history of thyroid disease. However, most guidelines do not support this course of action.
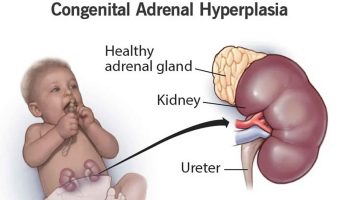
My newborn had a thyrotropin test done. Why?
A thyrotropin (TSH) test may be used to screen for congenital hypothyroidism. Screening for this condition is routinely performed in the United States on newborns soon after birth as part of each state’s newborn screening program. Congenital hypothyroidism occurs when a baby is born with an underactive thyroid gland or a thyroid gland that is not located where it should be or is missing completely.
Thyrotropin releasing hormone
The hypothalamic-pituitary axis regulates thyrotropin (TSH) release. The hypothalamus secretes the thyrotropin-releasing hormone (TRH), which is a tripeptide that stimulates the release of thyrotropin (TSH) and prolactin from the anterior pituitary gland 11. Thyrotropin (TSH) is released by the anterior pituitary and stimulates the thyroid follicular cells to release thyroxine (T4) (80%) and triiodothyronine (T3) (20%). When thyroxine (T4) is released into circulation, it can be converted to triiodothyronine (T3) through the process of deiodination. Thyroxine (T4) and triiodothyronine (T3) can then exert negative feedback on thyrotropin (TSH) levels, with high levels of triiodothyronine (T3) or thyroxine (T4) decreasing thyrotropin (TSH) and low levels of triiodothyronine (T3) or thyroxine (T4) increasing thyrotropin (TSH) levels from the anterior pituitary. Triiodothyronine (T3) is the predominant inhibitor of thyrotropin (TSH) secretion. Because thyrotropin (TSH) secretion is so sensitive to minor changes in serum-free T4 through this negative feedback loop, abnormal thyrotropin (TSH) levels are detected earlier than those of free T4 in hypothyroidism and hyperthyroidism. There is a log-linear relationship between triiodothyronine (T3) or thyroxine (T4) and thyrotropin (TSH) with minor changes in triiodothyronine (T3) or thyroxine (T4) results in major changes in thyrotropin (TSH).
Thyrotropin-releasing hormone (TRH) stimulation test differentiates all types of hypothyroidism (underactive thyroid) by observing the change in patient thyrotropin (TSH) levels in response to thyrotropin-releasing hormone (TRH). Typically, the thyrotropin (TSH) response to thyrotropin-releasing hormone (TRH) stimulation is exaggerated in cases of primary hypothyroidism, absent in secondary hypothyroidism, and delayed in tertiary hypothyroidism. Most individuals with primary hyperthyroidism have thyrotropin (TSH) suppression and do not respond to thyrotropin-releasing hormone (TRH) stimulation with an increase in thyrotropin (TSH) over their basal value.
- Estrada JM, Soldin D, Buckey TM, Burman KD, Soldin OP. Thyrotropin isoforms: implications for thyrotropin analysis and clinical practice. Thyroid. 2014;24(3):411–423. doi:10.1089/thy.2013.0119 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3949435[↩][↩]
- Novel insights into the molecular mechanisms of human thyrotropin action: structural, physiological, and therapeutic implications for the glycoprotein hormone family. Grossmann M, Weintraub BD, Szkudlinski MW. Endocr Rev. 1997 Aug; 18(4):476-501.[↩]
- Glycosylation and posttranslational processing of thyroid-stimulating hormone: clinical implications. Weintraub BD, Stannard BS, Magner JA, Ronin C, Taylor T, Joshi L, Constant RB, Menezes-Ferreira MM, Petrick P, Gesundheit N. Recent Prog Horm Res. 1985; 41():577-606.[↩]
- Thyroid-stimulating hormone: biosynthesis, cell biology, and bioactivity. Magner JA. Endocr Rev. 1990 May; 11(2):354-85.[↩]
- Glycoprotein hormones: structure and function. Pierce JG, Parsons TF. Annu Rev Biochem. 1981; 50():465-95.[↩]
- Recombinant human thyroid stimulating hormone: development of a biotechnology product for detection of metastatic lesions of thyroid carcinoma. Cole ES, Lee K, Lauziere K, Kelton C, Chappel S, Weintraub B, Ferrara D, Peterson P, Bernasconi R, Edmunds T. Biotechnology (N Y). 1993 Sep; 11(9):1014-24.[↩]
- Advances in the production of human therapeutic proteins in yeasts and filamentous fungi. Gerngross TU. Nat Biotechnol. 2004 Nov; 22(11):1409-14.[↩]
- Pirahanchi Y, Jialal I. Physiology, Thyroid Stimulating Hormone (TSH) [Updated 2019 Apr 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499850[↩]
- Delitala AP, Capobianco G, Cherchi PL, Dessole S, Delitala G. Thyroid function and thyroid disorders during pregnancy: a review and care pathway. Arch. Gynecol. Obstet. 2019 Feb;299(2):327-338[↩]
- Calsolaro V, Niccolai F, Pasqualetti G, Calabrese AM, Polini A, Okoye C, Magno S, Caraccio N, Monzani F. Overt and Subclinical Hypothyroidism in the Elderly: When to Treat? Front Endocrinol (Lausanne). 2019;10:177[↩]
- Shahid Z, Singh G. Physiology, Hypothalamus. [Updated 2018 Dec 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535380[↩]

{kind=link}