Contents
What is transient ischemic attack
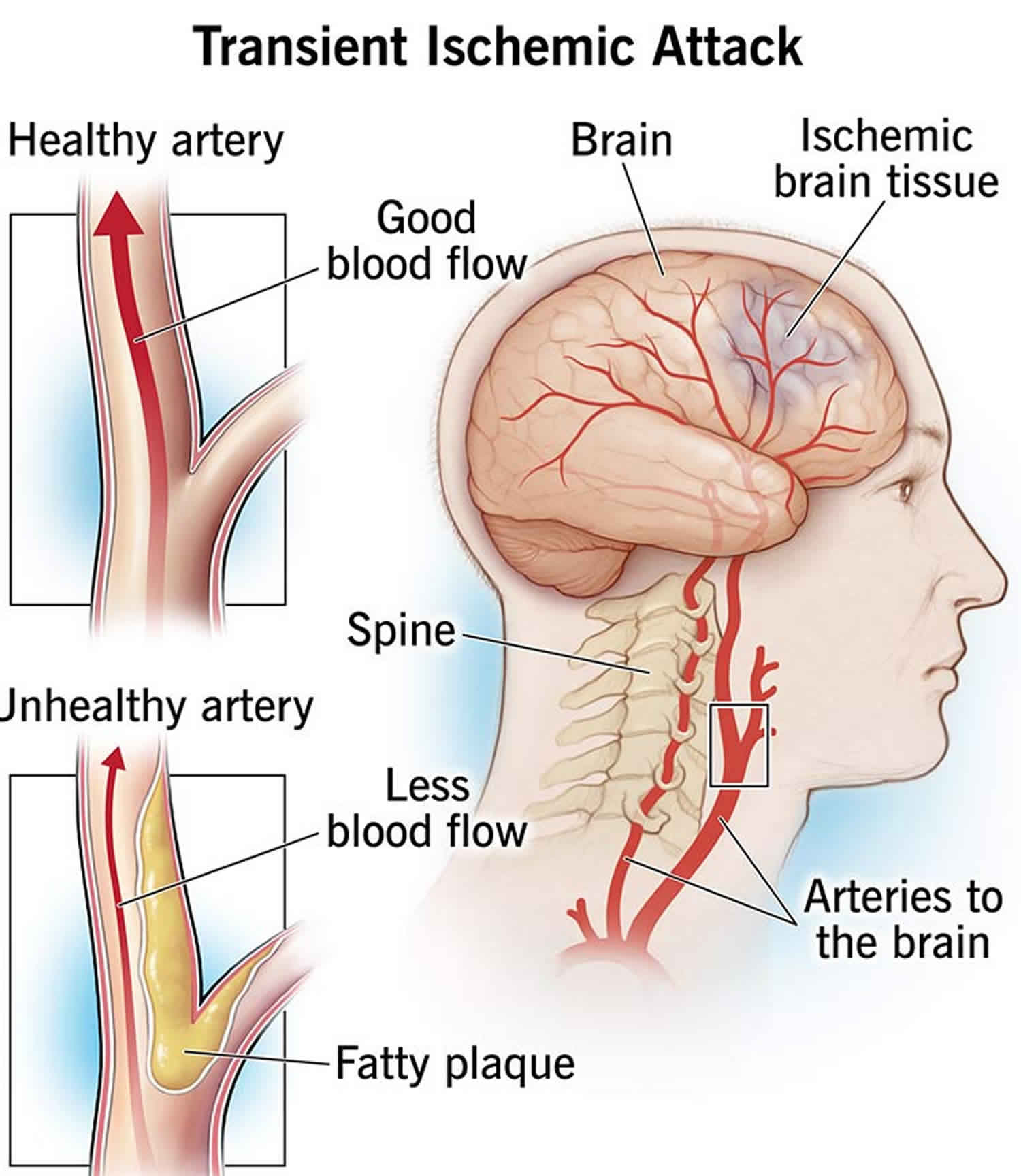
Transient ischemic attack also called transient ischaemic attack, “TIA” or often incorrectly called “mini stroke” is a temporary blockage of blood flow to part of your brain and it’s a “warning symptom of a stroke“, because TIA and stroke symptoms are the same, although most TIA symptoms last less than five minutes (but can be up to 24 hours) 1, 2, 3, 4, 5, 6, 7, 8. In the early stages of a TIA, it’s not possible to tell whether you’re having a TIA or a full stroke. While a TIA doesn’t cause permanent damage, it’s a major warning sign of a possible full-blown stroke in the future and should not be ignored. Having a TIA often means you could have a stroke in the very near future. Up to 20% of people who have a TIA have a stroke within 90 days, and half of those strokes happen within the first two days after a TIA. TIA is a medical emergency you shouldn’t ignore. A transient ischemic attack is a medical emergency just like a stroke is. That’s because there’s no way to predict how long a TIA will last, and every minute counts. When you first notice TIA symptoms, call for an ambulance or your local emergency number and ask for ambulance immediately, even if your symptoms go away.
- A transient ischemic attack occurs before about 15 percent of all strokes.
- About 240,000 Americans experience a transient ischemic attack every year.
- Mini-strokes are often followed by more severe strokes.
- About 1 in 3 people who has a TIA go on to have a more severe stroke, with about half occurring within a year after the TIA.
- People who have severe strokes often report having earlier warning strokes.
A TIA is caused by a brief blockage of blood flow to your brain due to a blood clot that dissolves on its own or gets dislodged. This can cause sudden symptoms similar to a stroke, such as speech and visual disturbance, and numbness or weakness in the face, arms and legs. But a TIA does not last as long as a stroke. The effects last a few minutes to a few hours and fully resolve within 24 hours.
The main symptoms of a transient ischemic attack or TIA can be remembered with the word FAST:
- Face – loss of muscle control on 1 side of your face or facial droop, the person may not be able to smile, or their mouth or eye may have dropped.
- Arms – the person may not be able to lift both arms and keep them raised because of weakness or numbness in 1 arm (hemiplegia = one-sided weakness or paralysis).
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all, despite appearing to be awake; they may also have problems understanding what you’re saying to them.
- Time – it’s time to call for an ambulance or your local emergency number and ask for ambulance immediately if you see any of these signs or symptoms. Even if your symptoms disappear while you’re waiting for an ambulance to arrive, you still need to be assessed by a doctor in the hospital. Because a stroke occurs when a blood vessel that carries oxygen and nutrients to the brain is either blocked by a clot or bursts (or ruptures). When that happens, part of your brain cannot get the blood and oxygen it needs, so your brain cells die, causing lasting brain damage.
Other stroke symptoms include:
- NUMBNESS or weakness of face, arm, or leg, especially on one side of the body
- CONFUSION, trouble speaking or understanding speech (aphasia) or slurred or garbled speaking (dysarthria)
- TROUBLE SEEING in one or both eyes or blurred or double vision (diplopia).
- Sudden loss, either partial or total, of one or more senses (vision, hearing, smell, taste and touch)
- TROUBLE WALKING, dizziness or vertigo, loss of balance or coordination (ataxia)
- SEVERE HEADACHE (usually sudden and severe) with no known cause
- Nausea and vomiting.
- Neck stiffness.
- Emotional instability and personality changes.
- Confusion or agitation.
- Memory loss (amnesia).
- Headaches.
- Passing out or fainting.
TIAs are usually caused by one of three things:
- Low blood flow in a major artery carrying blood to the brain.
- A blood clot in another part of the body (such as the heart) that breaks off, travels to the brain and blocks a blood vessel (thromboembolism).
- The narrowing of a smaller blood vessel in the brain, usually caused by plaque (a fatty substance) build-up.
Although the symptoms of a transient ischemic attack (TIA) resolve in a few minutes or hours, you’ll need treatment to help prevent another TIA or a full stroke happening in the future. If the doctor in the emergency room suspects you’ve had a TIA, you’ll be given aspirin to take straight away to prevent a stroke, unless there’s a medical reason why you cannot take aspirin.
You’ll usually be seen by a doctor who specializes in conditions that affect the brain and spine (neurologist), or a doctor who specializes in strokes. This may be in a specialist stroke or TIA clinic, or an acute stroke unit. You’ll be asked about the symptoms you experienced during the TIA and how long they lasted. This will help to rule out other conditions that may have caused your symptoms. Even if you no longer have symptoms, you may still need a neurological examination. This involves simple tasks designed to check your strength, sensation and co-ordination skills.
Several tests may be done to confirm a TIA and look for problems that may have caused it. Some of these tests include:
- Blood pressure tests. Your blood pressure will be checked, because high blood pressure (hypertension) can lead to TIAs.
- Blood tests. You might need blood tests to check whether you have high cholesterol, homocysteine or diabetes.
- Electrocardiogram (ECG). An electrocardiogram (ECG) measures your heart’s electrical activity using a number of electrodes (small, sticky patches) attached to your skin. An ECG can detect abnormal heart rhythms, which may be a sign of conditions such as where your heart beats irregularly (atrial fibrillation), which can increase your risk of TIAs.
- Carotid ultrasound. A carotid ultrasound scan can show if there is narrowing or any blockages in the neck arteries (carotid arteries) leading to your brain. A small probe (transducer) sends high-frequency sound waves into your body. When these sound waves bounce back, they can be used to create an image of the inside of your body.
- Brain scans. Brain scans are not always necessary if you’ve had a TIA. They’re usually only done if it’s not clear which part of your brain was affected.
- CT (computerized tomography). CT scans of your head use X-ray beams to create a 3D image. This allows your doctor to look at your brain or the arteries in your neck and brain.
- CTA (computerized tomography angiography). This combines a CT scan with an injection of a special dye into a blood vessel that will help create pictures of blood vessels and tissues in your body. Unlike a carotid ultrasound, a computerized tomography angiography (CTA) scan can look at blood vessels in the neck and head.
- MRI (magnetic resonance imaging). Magnetic resonance imaging (MRI) uses strong magnetic fields and radio waves to create a 3D view of your brain. An MRI (magnetic resonance imaging) is most often used.
- MRA (magnetic resonance angiography). Similar to an MRI, magnetic resonance angiography (MRA) specifically looks at the arteries in your neck and brain. MRA may include an injection of a contrast material into a blood vessel.
- TTE (transthoracic echocardiogram). A transthoracic echocardiogram (TTE) involves moving an instrument called a transducer across the chest to look at the heart. The transducer emits sound waves that bounce off different parts of the heart, creating an ultrasound image.
- TEE (transesophageal echocardiogram). In transesophageal echocardiogram (TEE), a flexible probe with a transducer is inserted into your esophagus to take pictures of your heart. Since your esophagus and heart are next to each other in your chest, this shows details of your heart that may not be seen on a transthoracic echocardiogram (TTE). Transesophageal echocardiogram (TEE) allows a better view of some things, such as blood clots, that might not be seen clearly in a traditional echocardiography exam.
- Arteriography (a test that creates a picture of your arteries using dye and X-rays). This procedure is used in some people to get a view of arteries in the brain not usually seen in an X-ray. A radiologist inserts a thin, flexible tube called a catheter through a small incision, usually in the groin. The catheter is guided through the major arteries and into the carotid or vertebral artery in the neck. Then a dye is injected through the catheter. The dye allows the arteries to be seen on X-ray images.
Although the symptoms of a transient ischemic attack (TIA) resolve in a few minutes or hours without any specific treatment, you’ll need treatment to help prevent another TIA or a full stroke from happening in the future. A TIA is a warning sign that you’re at increased risk of having a full stroke in the near future. The highest risk is in the days and weeks following the TIA.
A stroke is a serious health condition that can cause permanent disability and can be fatal in some cases, but appropriate treatment after a TIA can help to reduce your risk of having a stroke.
Your treatment will depend on your individual circumstances, such as your age and medical history. Your doctor can discuss treatment options with you and tell you about possible benefits and risks.
Transient ischemic attack treatments include 5, 9, 10, 11, 12, 13, 14:
- Lifestyle changes. Lifestyle changes include:
- Eating a healthy, balanced diet – a low-fat, reduced-salt, high-fiber diet is usually recommended, including plenty of fresh fruit and vegetables
- Maintaining a healthy weight or losing weight.
- Exercising regularly – for most people this means at least 150 minutes of moderate-intensity activity, such as cycling or fast walking, or 75 minutes of vigorous-intensity activity such as running, swimming, or riding a bike up a hill, every week. Plus, strength exercises on 2 days every week
- Stopping smoking – if you smoke, stopping may significantly reduce your risk of having a stroke in the future
- Cutting down on alcohol – men and women are advised to limit alcohol intake to 14 units per week
- Getting 7 to 9 hours of sleep daily.
- Medicines. Most people who have had a TIA will need to take 1 or more medicines every day, long term, to help reduce their chances of having a stroke or another TIA.
- Anti-platelet drugs prevent blood cells called platelets from clumping together to form a clot. Platelets are blood cells that help blood to clot. Antiplatelet medicines make platelets less likely to stick together. Sticky platelets begin to form clots when blood vessels are injured. Clotting proteins in blood plasma also are involved in the process. Aspirin is the most commonly used anti-platelet medicine. You’ll probably be given low-dose aspirin straight after a TIA. Aspirin (acetylsalicylic acid) is also the least expensive treatment with the fewest potential side effects. An alternative to aspirin is the anti-platelet drug clopidogrel (Plavix). Aspirin and clopidogrel may be prescribed together for about a month after the TIA. Research shows that taking aspirin and clopidogrel together in certain situations reduces the risk of a future stroke more than taking aspirin alone. Sometimes both medicines are taken together for a longer period. This may be recommended when the cause of the TIA is a narrowing of a blood vessel in the head. When there’s a serious block of a major artery, the medicine cilostazol may be prescribed with aspirin or clopidogrel. Alternatively, your doctor may prescribe ticagrelor (Brilinta) and aspirin for 30 days to decrease your risk of recurrent stroke. Your doctor also may consider prescribing a combination of low-dose aspirin and the anti-platelet drug dipyridamole (Persantine) to reduce blood clotting. The way dipyridamole works is slightly different from aspirin. Dipyridamole is a vasodilator and inhibitor of platelet aggregation that is used to decrease the risk of thromboembolic complications and recurrence of stroke in patients known to have atherosclerotic cerebrovascular disease. The main side effects of antiplatelet medicines include indigestion and an increased risk of bleeding. For example, you may bleed for longer if you cut yourself and you may bruise easily.
- Anticoagulants also called blood thinners are medicines that prevent blood clots from forming. Anticoagulant medicines can help to prevent blood clots by changing the chemical composition of your blood in a way that stops clots from forming. Anticoagulants do not break up clots that you already have. But they can stop those clots from getting bigger. These medicines include heparin and warfarin (Jantoven). They lower the risk of blood clots by affecting clotting-system proteins instead of platelet function. Heparin is used for a short time and is rarely used in the management of TIAs. If you have atrial fibrillation, your doctor may prescribe a direct oral anticoagulant such as apixaban (Eliquis), rivaroxaban (Xarelto), edoxaban (Savaysa) or dabigatran (Pradaxa), which may be safer than warfarin due to lower bleeding risk. A side effect of all anticoagulants is the risk of bleeding, because these medicines reduce your blood’s ability to clot. You may need regular blood tests while taking warfarin, so doctors can check your dose is not too high or too low.
- Surgery. In some cases, a carotid artery surgery called a carotid endarterectomy may be recommended after having a TIA. Carotid artery surgery is done to restore proper blood flow to your brain. Surgery to remove the buildup in your carotid artery may be done if the artery is narrowed by more than 70%. If you have had a stroke or transient ischemic attack, your doctor will consider whether treating your blocked carotid artery with surgery is safe for you.
- Carotid endarterectomy. If the carotid artery in your neck is very narrowed, your doctor may suggest a surgery called carotid endarterectomy. This preventive surgery clears carotid arteries of fatty deposits before another TIA or stroke can occur.
- Angioplasty with stent placement. Some people need a procedure called carotid angioplasty and stent placement. Carotid angioplasty and stenting is likely to be used when carotid endarterectomy would not be safe. This procedure involves using a balloon-like device to open a clogged artery. Then a small wire tube called a stent is placed into the artery to keep it open. Carotid artery angioplasty with stent placement is a good alternative to carotid endarterectomy in some cases, when done by experienced surgeons.
Transient ischemic attack causes
The cause of a transient ischemic attack is similar to the cause of an ischemic stroke, which is the most common type of stroke. In an ischemic stroke, the blockage in the brain is usually caused by a piece of plaque or a blood clot that blocks the blood supply to part of your brain 15. In a TIA, the blockage of blood flow to your brain is brief and there is no permanent damage. The blockage that occurs during a TIA often results from a buildup of cholesterol-containing fatty deposits called plaques in an artery. This is known as atherosclerosis. The buildup also may occur in an artery’s branches that supply oxygen and nutrients to your brain. Plaques can decrease the blood flow through an artery or lead to the development of a blood clot. A blood clot that moves from another part of your body, such as your heart, to an artery that supplies your brain also may cause a TIA.
Risk factors for getting transient ischemic attack
Certain risk factors make it more likely that you will develop transient ischemic attack and have a stroke.
- Family history. Your risk may be greater if one of your family members has had a TIA or a stroke.
- Age. Your risk increases as you get older, especially after age 55. At younger ages, men are more likely than women to have a stroke. But women tend to live longer, so their lifetime risk of having a stroke is higher. Women who take birth control pills or use hormone replacement therapy are at higher risk. Women are also at higher risk during pregnancy and in the weeks after giving birth. High blood pressure during pregnancy — such as from preeclampsia — raises the risk of stroke later in life.
- Race and ethnicity. In the United States, stroke occurs more often in Black, Asian, Alaska Native, American Indian, and Hispanic adults than in white adults.
- Sex. Men have a slightly higher risk of a TIA and a stroke. But as women age, their risk of a stroke goes up.
- Prior transient ischemic attack. If you’ve had one or more TIAs, you’re much more likely to have a stroke.
- Sickle cell disease. Stroke is a frequent complication of sickle cell disease, also known as sickle cell anemia. Sickle-shaped blood cells carry less oxygen and also tend to get stuck in artery walls, affecting blood flow to the brain. But with proper treatment of sickle cell disease, you can lower your risk of a stroke.
- Cigarette smoking including vaping. Smoking increases your risk of blood clots, raises blood pressure and plays a part in the development of atherosclerosis. But quitting smoking lowers your risk of having a TIA or a stroke.
- Physical inactivity. Doing 30 minutes of moderate-intensity exercise most days helps lower your risk.
- Poor nutrition. Eating less fat and salt decreases the risk of a TIA and a stroke.
- Heavy drinking. If you drink alcohol, limit yourself to up to one drink a day for women and up to two drinks a day for men.
- Use of illicit drugs. Avoid cocaine and other illicit drugs.
- Anxiety, depression, and high stress levels, as well as working long hours and not having much contact with family, friends, or others outside the home, may raise your risk for stroke.
- High blood pressure. The risk of a stroke begins to increase at blood pressure readings of 140/90 millimeters of mercury (mm Hg) and higher. Your doctor can help you decide on a target blood pressure based on your age and other factors, such as whether you have diabetes.
- High cholesterol. Eating less cholesterol and fat, especially saturated fat and trans fat, may reduce the plaques in your arteries. If you can’t control your cholesterol through dietary changes alone, your provider may prescribe a statin or another type of cholesterol-lowering medicine.
- Cardiovascular disease includes heart failure, a heart defect, a heart infection (infective endocarditis) or a heart rhythm condition (arrhythmia).
- Atrial fibrillation (Afib). This irregular heart rhythm (arrhythmia) can cause blood to swirl and pool in one of your heart’s chambers rather than smoothly flow through. That can allow clots to form, and these can then travel through your carotid arteries and into your brain.
- Carotid artery disease. In this condition, the blood vessels in your neck (carotid arteries) that lead to the brain become clogged. The carotid artery brings needed blood to your brain and face. You have one of these arteries on each side of your neck. Blood flow in carotid artery can become partly or totally blocked by fatty material called plaque. This can reduce the blood supply to your brain and cause a transient ischemic attack (TIA) or stroke.
- Peripheral artery disease (PAD). Peripheral artery disease causes the blood vessels that carry blood to your arms and legs to become clogged.
- Diabetes. Diabetes speeds up and worsens the narrowing of arteries due to a buildup of fatty deposits, known as atherosclerosis.
- High levels of homocysteine. Elevated levels of homocysteine (an amino acid) in your blood can cause your arteries to thicken and scar. This makes them more susceptible to clots.
- Having excess weight or obesity, especially carrying extra weight in the stomach, increases stroke risk.
- Viral infections or autoimmune conditions such as lupus or rheumatoid arthritis, can cause inflammation.
Transient ischemic attack pathophysiology
The pathophysiology of TIA depends on the subtype classified according to the pathophysiological mechanisms, which are similar to ischemic stroke subtypes 18. They include large artery atherothrombosis, cardiac embolism, small vessel (lacunar), cryptogenic, and uncommon subtypes such as vascular dissection, vasculitis, etc. The common risk factors for all TIA include diabetes, hypertension, age, smoking, obesity, alcoholism, unhealthy diet, psychosocial stress, and lack of regular physical activity. The common issue is the transient interruption of arterial blood flow to an area of the brain supplied by that particular artery 18.
- Large artery atherothrombosis. This may be intracranial or extracranial atherothrombosis. The mechanism may be a lack of blood flow distal to the site of arterial stenosis or an artery-to-artery embolism, the more common mechanism.
- Small vessel ischemic diseases. The underlying pathology is either lipohyalinosis or small vessel arteriolosclerosis. The commonest risk factor is hypertension, followed by diabetes and age.
- Cardiac embolism. A clot in the cardiac chamber, most commonly in the left atrium, is secondary to atrial fibrillation.
- Cryptogenic. This is usually a cortical pattern of ischemia without any identifiable large artery atherothrombosis or cardiac source of emboli. More recently it is often referred to as ESUS (embolic stroke of unknown source).
- Other uncommon causes such as arterial dissection or hypercoagulable states.
Transient ischemic attack prevention
You can lower your risk of a transient ischemic attack or stroke by changing your behaviors that can raise your risks or get treatment for other health conditions that raise your risk of transient ischemic attack are the best things you can do to prevent a transient ischemic attack. A healthy lifestyle includes healthy eating, regular exercise, quitting smoking, managing stress, maintaining a healthy weight and getting regular medical checkups.
- Don’t smoke. Stopping smoking reduces your risk of a TIA or a stroke.
- Limit cholesterol and fat. Cutting back on cholesterol and fat, especially saturated fat and trans fat, in your diet may reduce buildup of plaques in the arteries.
- Eat plenty of fruits and vegetables. These foods contain nutrients such as potassium, folate and antioxidants, which may protect against a TIA or a stroke.
- Limit salt or sodium. If you have high blood pressure, avoid salty foods and don’t add salt to food. These habits may help reduce your blood pressure. Limiting salt may not prevent high blood pressure, but excess sodium may increase blood pressure in some people.
- Exercise regularly. If you have high blood pressure, regular exercise is one of the few ways you can lower your blood pressure without medicines.
- Limit alcohol intake. Drink alcohol in moderation, if at all. The recommended limit is no more than one drink daily for women and two drinks a day for men.
- Maintain a healthy weight. Being overweight contributes to other risk factors, such as high blood pressure, cardiovascular disease and diabetes. Losing weight with diet and exercise may lower your blood pressure and improve your cholesterol levels.
- Don’t use illicit drugs. Illicit drugs such as cocaine are associated with an increased risk of a TIA or a stroke.
- Control diabetes. You can manage diabetes and high blood pressure with diet, exercise, weight control and, when necessary, medicine.
Transient ischemic attack symptoms
Transient ischemic attacks usually last less than five minutes but can be up to 24 hours. Most TIA symptoms disappear within an hour. Rarely, symptoms may last up to 24 hours. The symptoms of a TIA are similar to those found early in a stroke. Because you cannot tell if these symptoms are from a TIA or a stroke, you should go to the hospital right away.
TIA symptoms happen suddenly and may include:
- Weakness, numbness or paralysis in the face, arm or leg, typically on one side of the body.
- Slurred speech or trouble understanding others.
- Blindness in one or both eyes or double vision.
- Dizziness or loss of balance or coordination.
Use the letters in F.A.S.T. to spot a stroke:
- F = Face Drooping – Does one side of the face droop or is it numb? Ask the person to smile. Is the person’s smile uneven?
- A = Arm Weakness – Is one arm weak or numb? Ask the person to raise both arms. Does one arm drift downward?
- S = Speech Difficulty – Is speech slurred?
- T = Time to call for an ambulance – Stroke is an emergency. Every minute counts. Call your local emergency number and ask for an ambulance immediately. Note the time when any of your symptoms first appear.
Other stroke symptoms include:
- NUMBNESS or weakness of face, arm, or leg, especially on one side of the body
- CONFUSION, trouble speaking or understanding speech (aphasia) or slurred or garbled speaking (dysarthria)
- TROUBLE SEEING in one or both eyes or blurred or double vision (diplopia).
- Sudden loss, either partial or total, of one or more senses (vision, hearing, smell, taste and touch)
- TROUBLE WALKING, dizziness or vertigo, loss of balance or coordination (ataxia)
- SEVERE HEADACHE (usually sudden and severe) with no known cause
- Nausea and vomiting.
- Neck stiffness.
- Emotional instability and personality changes.
- Confusion or agitation.
- Memory loss (amnesia).
- Headaches.
- Passing out or fainting.
SEVERE HEADACHE with no known cause
You may have more than one TIAs. Their symptoms may be similar or different depending on which area of the brain is involved.
TIAs most often occur hours or days before a stroke. If you think you’re having or have had a transient ischemic attack, see a doctor in the emergency room right away. Being evaluated quickly means your doctor can pinpoint potential treatable conditions. Treating those conditions may help you prevent a stroke.
Transient ischemic attack diagnosis
It’s difficult to identify a TIA from a major stroke as it’s happening. Self-awareness is important! Getting to a hospital or your local emergency number and ask for an ambulance also is important. That’s because treating a TIA early prevents further damage. A doctor will perform a physical exam. They will ask you about your medical history. This includes questions about other medical conditions and your lifestyle. Your doctor will listen to your heart and lungs and test you for signs of numbness, weakness, or other neurologic problems.
A TIA may only last minutes but could last longer. You, a family member or friend should remember your symptoms and what time they began. All tests and exams will happen after you have the TIA.
To pinpoint the cause of your TIA and to assess your risk of a stroke, your doctor may rely on the following:
- Carotid ultrasound. If your doctor suspects that a narrowed carotid artery in your neck may be the cause of your TIA, you may need a carotid ultrasound. Carotid ultrasonography uses sound waves to examine the blood flow through your carotid arteries. These are the arteries in your neck that supply blood to your brain. The sound waves pass through the tissue and create images on a screen. The images can show narrowing or clotting in the carotid arteries.
- CT (computerized tomography). CT scans of your head use X-ray beams to create a 3D image. This allows your doctor to look at your brain or the arteries in your neck and brain.
- CTA (computerized tomography angiography). This combines a CT scan with an injection of a special dye into a blood vessel that will help create pictures of blood vessels and tissues in your body. Unlike a carotid ultrasound, a computerized tomography angiography (CTA) scan can look at blood vessels in the neck and head.
- MRI (magnetic resonance imaging). Magnetic resonance imaging (MRI) uses strong magnetic fields and radio waves to create a 3D view of your brain.
- MRA (magnetic resonance angiography). Similar to an MRI, magnetic resonance angiography (MRA) specifically looks at the arteries in your neck and brain. MRA may include an injection of a contrast material into a blood vessel.
- TTE (transthoracic echocardiogram). A transthoracic echocardiogram (TTE) involves moving an instrument called a transducer across the chest to look at the heart. The transducer emits sound waves that bounce off different parts of the heart, creating an ultrasound image.
- TEE (transesophageal echocardiogram). In transesophageal echocardiogram (TEE), a flexible probe with a transducer is inserted into your esophagus to take pictures of your heart. Since your esophagus and heart are next to each other in your chest, this shows details of your heart that may not be seen on a transthoracic echocardiogram (TTE). Transesophageal echocardiogram (TEE) allows a better view of some things, such as blood clots, that might not be seen clearly in a traditional echocardiography exam.
- Arteriography (a test that creates a picture of your arteries using dye and X-rays). This procedure is used in some people to get a view of arteries in the brain not usually seen in an X-ray. A radiologist inserts a thin, flexible tube called a catheter through a small incision, usually in the groin. The catheter is guided through the major arteries and into the carotid or vertebral artery in the neck. Then a dye is injected through the catheter. The dye allows the arteries to be seen on X-ray images.
Routine blood tests, including complete blood count (CBC), PT/INR, comprehensive metabolic panel, fasting blood sugar, lipid panel, urine drug screen, and ESR, should be considered 17, 19, 20.
National Stroke Association has established guidelines for TIA evaluation as follows in 2006 21:
- CBC = complete blood count
- TCD = transcranial Doppler
- TEE = transesophageal echocardiogram
- TTE = transthoracic echocardiogram
Transient ischemic attack treatment
If you are diagnosed with a TIA in an emergency room, you should follow up as soon as possible with a neurologist, a doctor who specializes in treating disorders of the brain, spinal cord, and nervous system or a doctor who specializes in strokes. Once your doctor has found the cause or source of your transient ischemic attack, you may need medicines to prevent blood clots or you might need surgery. Most of the time, your body treats a TIA on its own. The blood clot quickly dissolves.
Although the symptoms of a transient ischemic attack (TIA) resolve in a few minutes or hours without any specific treatment, you’ll need treatment to help prevent another TIA or a full stroke from happening in the future. A TIA is a warning sign that you’re at increased risk of having a full stroke in the near future. The highest risk is in the days and weeks following the TIA.
A stroke is a serious health condition that can cause permanent disability and can be fatal in some cases, but appropriate treatment after a TIA can help to reduce your risk of having a stroke.
Your treatment will depend on your individual circumstances, such as your age and medical history. Your doctor can discuss treatment options with you and tell you about possible benefits and risks.
Transient ischemic attack treatments include:
- Lifestyle changes
- Medicines
- Surgery
Lifestyle changes
The best way to help prevent a TIA is to eat a healthy diet, exercise regularly, and not smoke or drink too much alcohol. These lifestyle changes can reduce your risk of problems such as your arteries becoming clogged by fatty substances atherosclerosis, high blood pressure and high cholesterol, all of which can lead to TIAs.
If you’ve already had a TIA, making these changes can help reduce your risk of having a full stroke or another TIA in the future.
Lifestyle changes include:
- Eating a healthy, balanced diet – a low-fat, reduced-salt, high-fiber diet is usually recommended, including plenty of fresh fruit and vegetables
- Maintaining a healthy weight or losing weight.
- Exercising regularly – for most people this means at least 150 minutes of moderate-intensity activity, such as cycling or fast walking, or 75 minutes of vigorous-intensity activity such as running, swimming, or riding a bike up a hill, every week. Plus, strength exercises on 2 days every week
- Stopping smoking – if you smoke, stopping may significantly reduce your risk of having a stroke in the future
- Cutting down on alcohol – men and women are advised to limit alcohol intake to 14 units per week
- Getting 7 to 9 hours of sleep daily.
Transient ischemic attack medications
Several medicines may lower your risk of stroke after a TIA. Your doctor recommends a medicine based on what caused your TIA, where it was located, its type and how bad the blockage was. Your doctor may prescribe:
- Anti-platelet drugs prevent blood cells called platelets from clumping together to form a clot. Platelets are blood cells that help blood to clot. Antiplatelet medicines make platelets less likely to stick together. Sticky platelets begin to form clots when blood vessels are injured. Clotting proteins in blood plasma also are involved in the process. Aspirin is the most commonly used anti-platelet medicine. Aspirin (acetylsalicylic acid) is also the least expensive treatment with the fewest potential side effects. An alternative to aspirin is the anti-platelet drug clopidogrel (Plavix). Aspirin and clopidogrel may be prescribed together for about a month after the TIA. Research shows that taking aspirin and clopidogrel together in certain situations reduces the risk of a future stroke more than taking aspirin alone. Sometimes both medicines are taken together for a longer period. This may be recommended when the cause of the TIA is a narrowing of a blood vessel in the head. When there’s a serious block of a major artery, the medicine cilostazol may be prescribed with aspirin or clopidogrel. Alternatively, your doctor may prescribe ticagrelor (Brilinta) and aspirin for 30 days to decrease your risk of recurrent stroke. Your doctor also may consider prescribing a combination of low-dose aspirin and the anti-platelet drug dipyridamole (Persantine) to reduce blood clotting. The way dipyridamole works is slightly different from aspirin. Dipyridamole is a vasodilator and inhibitor of platelet aggregation that is used to decrease the risk of thromboembolic complications and recurrence of stroke in patients known to have atherosclerotic cerebrovascular disease. The main side effects of antiplatelet medicines include indigestion and an increased risk of bleeding. For example, you may bleed for longer if you cut yourself and you may bruise easily.
- Anticoagulants also called blood thinners are medicines that prevent blood clots from forming. Anticoagulant medicines can help to prevent blood clots by changing the chemical composition of your blood in a way that stops clots from forming. Anticoagulants do not break up clots that you already have. But they can stop those clots from getting bigger. These medicines include heparin and warfarin (Jantoven). They lower the risk of blood clots by affecting clotting-system proteins instead of platelet function. Heparin is used for a short time and is rarely used in the management of TIAs. If you have atrial fibrillation, your doctor may prescribe a direct oral anticoagulant such as apixaban (Eliquis), rivaroxaban (Xarelto), edoxaban (Savaysa) or dabigatran (Pradaxa), which may be safer than warfarin due to lower bleeding risk. A side effect of all anticoagulants is the risk of bleeding, because these medicines reduce your blood’s ability to clot. You may need regular blood tests while taking warfarin, so doctors can check your dose is not too high or too low.
Most people who have had a TIA will need to take 1 or more medicines every day, long term, to help reduce their chances of having a stroke or another TIA.
Transient ischemic attack surgery
In some cases, a carotid artery surgery called a carotid endarterectomy may be recommended after having a TIA. Carotid artery surgery is done to restore proper blood flow to your brain. Surgery to remove the buildup in your carotid artery may be done if the artery is narrowed by more than 70%. If you have had a stroke or transient ischemic attack, your doctor will consider whether treating your blocked carotid artery with surgery is safe for you.
There are 2 procedures to treat a carotid artery that has plaque buildup in it.
Carotid endarterectomy
If the carotid artery in your neck is very narrowed, your doctor may suggest a surgery called carotid endarterectomy. This preventive surgery clears carotid arteries of fatty deposits before another TIA or stroke can occur.
During carotid endarterectomy:
- You receive general anesthesia. You are asleep and pain free. Some hospitals use local anesthesia instead. Only the part of your body being worked on is numbed with medicine so that you do not feel pain. You are also given a medicine to help you relax.
- You lie on your back on an operating table with your head turned to one side. The side your blocked carotid artery is on faces up.
- The surgeon makes a cut (incision) on your neck over your carotid artery. A flexible tube (catheter) is put in the artery. Blood flows through the catheter around the blocked area during surgery.
- Your carotid artery is opened. The surgeon removes the plaque inside the artery.
- After the plaque is removed, the artery is closed with stitches or a patch from one of your veins or synthetic material. Blood now flows through the artery to your brain.
- Your heart activity is monitored closely during the surgery.
The surgery takes about 2 hours. After the procedure, your surgeon may do a test to confirm that the artery has been opened.
Carotid endarterectomy risks include:
- Risks of anesthesia:
- Allergic reactions to medicines
- Breathing problems
- Risks of carotid surgery:
- Blood clots or bleeding in the brain
- Bleeding requiring re-operation to remove clot
- Brain damage
- Heart attack
- More blockage of the carotid artery over time
- Seizures
- Stroke
- Swelling near your airway (the tube you breathe through)
- Infection
You may have a drain in your neck that goes into your incision. It will drain fluid that builds up in the area. It will be removed within a day.
After surgery, your surgeon may want you to stay in the hospital overnight so that nurses can watch you for any signs of bleeding, stroke, or poor blood flow to your brain. You may be able to go home the same day if your operation is done early in the day and you are doing well.
Angioplasty with stent placement
Some people need a procedure called carotid angioplasty and stent placement. Carotid angioplasty and stenting is likely to be used when carotid endarterectomy would not be safe. This procedure involves using a balloon-like device to open a clogged artery. Then a small wire tube called a stent is placed into the artery to keep it open.
Carotid artery angioplasty with stent placement is a good alternative to carotid endarterectomy in some cases, when done by experienced surgeons. Certain factors may favor carotid artery angioplasty with stenting, such as:
- The person is too ill to have carotid endarterectomy.
- The location of the narrowing in the carotid artery makes surgery harder.
- The person has had neck or carotid surgery in the past.
- The person has had radiation to the neck.
Risks of carotid artery angioplasty with stenting depend on factors such:
- Allergic reaction to dye
- Blood clots or bleeding at the site of surgery
- Brain damage
- Clogging of the inside of the stent (in-stent restenosis)
- Heart attack
- Kidney failure (higher risk in people who already have kidney problems)
- More blockage of the carotid artery over time
- Seizures (this is rare)
- Stroke
After carotid artery angioplasty with stent placement, you may need to stay in the hospital overnight so that you can be watched for any signs of bleeding, stroke, or poor blood flow to your brain. You may be able to go home the same day if your procedure is done early in the day and you are doing well. Your surgeon will talk to you about how to care for yourself at home.
Managing underlying conditions
If you’ve been diagnosed with a condition that’s known to increase your risk of TIAs and strokes, such as atrial fibrillation, high cholesterol, high blood pressure, atrial fibrillation or type 1 diabetes and type 2 diabetes, it’s important to control the condition.
Medications for high cholesterol
Your doctor might suggest medication to help keep your cholesterol in the healthy range. The choice of medication or combination of medications depends on various factors, including your personal risk factors, your age, your health and possible drug side effects. Common choices include:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. Statins can also help your body reabsorb cholesterol from built-up deposits on your artery walls, potentially reversing coronary artery disease. Choices include atorvastatin (Lipitor), fluvastatin (Lescol XL), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor). The common side effects of statins are muscle pains and muscle damage, reversible memory loss and confusion, and elevated blood sugar.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can be used with a statin drug.
- Bempedoic acid. This newer drug works in much the same way as statins but is less likely to cause muscle pain. Adding bempedoic acid (Nexletol) to a maximum statin dosage can help lower LDL significantly. A combination pill containing both bempedoic acid and ezetimibe (Nexlizet) also is available.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- Injectable medications. A newer class of drugs, known as PCSK9 inhibitors, can help the liver absorb more LDL cholesterol — which lowers the amount of cholesterol circulating in your blood. Alirocumab (Praluent) and evolocumab (Repatha) might be used for people who have a genetic condition that causes very high levels of LDL or in people with a history of coronary disease who have intolerance to statins or other cholesterol medications. PCSK9 inhibitors are injected under the skin every few weeks and are expensive.
If you also have high triglycerides, your doctor might prescribe:
- Fibrates. Fibrates mostly lower triglycerides and, to a lesser degree, raise HDL levels. Fibrates are less effective in lowering LDL levels. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Using fibrates with a statin can increase the risk of statin side effects.
- Nicotinic acid also called niacin or vitamin B3. Niacin is the generic name for nicotinic acid (pyridine-3-carboxylic acid), nicotinamide (niacinamide or pyridine-3-carboxamide), and related derivatives, such as nicotinamide riboside 22. Niacin is a water-soluble B3 vitamin that should be taken only under physician supervision. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. It improves all lipoproteins—total cholesterol, LDL, triglycerides, and HDL—when taken in doses well abovethe vitamin requirement. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins.
- Omega-3 fatty acid supplements. Omega-3 fatty acid supplements can help lower your triglycerides. They are available by prescription or over-the-counter. If you choose to take over-the-counter supplements, get your doctor’s OK. Omega-3 fatty acid supplements could affect other medications you’re taking.
If you are on such medication, you might need regular cholesterol tests to check that they are working well and that you are taking the right dose. If you decide to take cholesterol medication, your doctor might recommend liver function tests to monitor the medication’s effect on your liver.
Experts from the National Cholesterol Education Program (NCEP) say that more aggressive cholesterol treatment is needed for people at high risk of dying from a heart attack or cardiovascular disease. The basic message of the group’s recommendations is the lower the better when it comes to levels of low-density lipoprotein (LDL) or “bad cholesterol”. The updated recommendations say that almost all high-risk patients with LDL cholesterol levels of 100 mg/dL or higher should begin taking cholesterol-lowering medicine.
Blood pressure medicines
If you have high blood pressure, you’ll be offered a type of medicine called an antihypertensive to control it. This is because high blood pressure increases your risk of having a TIA or stroke.
There are lots of different types of medicine to treat high blood pressure, including:
- Water pills (diuretics). These drugs help remove sodium and water from the body. They are often the first medicines used to treat high blood pressure. There are different classes of diuretics, including thiazide, loop and potassium sparing. Which one your provider recommends depends on your blood pressure measurements and other health conditions, such as kidney disease or heart failure. Diuretics commonly used to treat blood pressure include chlorthalidone, hydrochlorothiazide (Microzide) and others. A common side effect of diuretics is increased urination. Urinating a lot can reduce potassium levels. A good balance of potassium is necessary to help the heart beat correctly. If you have low potassium (hypokalemia), your provider may recommend a potassium-sparing diuretic that contains triamterene.
- Angiotensin-converting enzyme (ACE) inhibitors. These drugs help relax blood vessels. They block the formation of a natural chemical that narrows blood vessels. Examples include lisinopril (Prinivil, Zestril), benazepril (Lotensin), captopril and others.
- Angiotensin II receptor blockers (ARBs). These drugs also relax blood vessels. They block the action, not the formation, of a natural chemical that narrows blood vessels. angiotensin II receptor blockers (ARBs) include candesartan (Atacand), losartan (Cozaar) and others.
- Calcium channel blockers. These drugs help relax the muscles of the blood vessels. Some slow your heart rate. They include amlodipine (Norvasc), diltiazem (Cardizem, Tiazac, others) and others. Calcium channel blockers may work better for older people and Black people than do angiotensin-converting enzyme (ACE) inhibitors alone. Don’t eat or drink grapefruit products when taking calcium channel blockers. Grapefruit increases blood levels of certain calcium channel blockers, which can be dangerous. Talk to your provider or pharmacist if you’re concerned about interactions.
If you’re having trouble reaching your blood pressure goal with combinations of the above medicines, your cardiologist may prescribe:
- Alpha blockers. These medicines reduce nerve signals to blood vessels. They help lower the effects of natural chemicals that narrow blood vessels. Alpha blockers include doxazosin (Cardura), prazosin (Minipress) and others.
- Alpha-beta blockers. Alpha-beta blockers block nerve signals to blood vessels and slow the heartbeat. They reduce the amount of blood that must be pumped through the vessels. Alpha-beta blockers include carvedilol (Coreg) and labetalol (Trandate).
- Beta blockers. These medicines reduce the workload on the heart and widen the blood vessels. This helps the heart beat slower and with less force. Beta blockers include atenolol (Tenormin), metoprolol (Lopressor, Toprol-XL, Kapspargo sprinkle) and others. Beta blockers aren’t usually recommended as the only medicine prescribed. They may work best when combined with other blood pressure drugs.
- Aldosterone antagonists. These drugs may be used to treat resistant hypertension. They block the effect of a natural chemical that can lead to salt and fluid buildup in the body. Examples are spironolactone (Aldactone) and eplerenone (Inspra).
- Renin inhibitors. Aliskiren (Tekturna) slows the production of renin, an enzyme produced by the kidneys that starts a chain of chemical steps that increases blood pressure. Due to a risk of serious complications, including stroke, you shouldn’t take aliskiren with angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs).
- Vasodilators. These medicines stop the muscles in the artery walls from tightening. This prevents the arteries from narrowing. Examples include hydralazine and minoxidil.
Central-acting agents. These medicines prevent the brain from telling the nervous system to increase the heart rate and narrow the blood vessels. Examples include clonidine (Catapres, Kapvay), guanfacine (Intuniv) and methyldopa.
Your doctor will advise you about which antihypertensive is the most suitable for you. Some people may be offered a combination of 2 or more different medicines.
Diabetes treatment
Depending on what type of diabetes you have, blood sugar monitoring, insulin and oral drugs may be part of your treatment. Eating a healthy diet, staying at a healthy weight and getting regular physical activity also are important parts of managing diabetes.
- Healthy eating. Your diabetes diet is simply a healthy-eating plan that will help you control your blood sugar. You’ll need to focus your diet on more fruits, vegetables, lean proteins and whole grains. These are foods that are high in nutrition and fiber and low in fat and calories. You’ll also cut down on saturated fats, refined carbohydrates and sweets. In fact, it’s the best eating plan for the entire family. Sugary foods are okay once in a while. They must be counted as part of your meal plan. Understanding what and how much to eat can be a challenge. A registered dietitian can help you create a meal plan that fits your health goals, food preferences and lifestyle. This will likely include carbohydrate counting, especially if you have type 1 diabetes or use insulin as part of your treatment.
- Physical activity. Everyone needs regular aerobic activity. This includes people who have diabetes. Physical activity lowers your blood sugar level by moving sugar into your cells, where it’s used for energy. Physical activity also makes your body more sensitive to insulin. That means your body needs less insulin to transport sugar to your cells. Get your doctor’s OK to exercise. Choose activities you enjoy, such as walking, swimming or biking. What’s most important is making physical activity part of your daily routine. Aim for at least 30 minutes or more of moderate physical activity most days of the week, or at least 150 minutes of moderate physical activity a week. Bouts of activity can be a few minutes during the day. If you haven’t been active for a while, start slowly and build up slowly. Also avoid sitting for too long. Try to get up and move if you’ve been sitting for more than 30 minutes.
Type 2 diabetes medications
If you can’t maintain your target blood sugar level with diet and exercise, your doctor may prescribe diabetes medications that help lower glucose levels, or your doctor may suggest insulin therapy.
Medicines for type 2 diabetes include the following:
- Metformin (Fortamet, Glumetza, others) is generally the first medicine prescribed for type 2 diabetes. It works mainly by lowering glucose production in the liver and improving the body’s sensitivity to insulin so it uses insulin more effectively. Some people experience vitamin B12 deficiency and may need to take supplements. Other possible side effects, which may improve over time, include:
- Nausea.
- Abdominal pain.
- Bloating.
- Diarrhea.
- Sulfonylureas help the body secrete more insulin. Examples include glyburide (DiaBeta, Glynase), glipizide (Glucotrol XL) and glimepiride (Amaryl). Possible side effects include:
- Low blood sugar.
- Weight gain.
- Glinides stimulate the pancreas to secrete more insulin. They’re faster acting than sulfonylureas. But their effect in the body is shorter. Examples include repaglinide and nateglinide. Possible side effects include:
- Low blood sugar.
- Weight gain.
- Thiazolidinediones make the body’s tissues more sensitive to insulin. An example of this medicine is pioglitazone (Actos). Possible side effects include:
- Risk of congestive heart failure.
- Risk of bladder cancer (pioglitazone).
- Risk of bone fractures.
- Weight gain.
- DPP-4 inhibitors help reduce blood sugar levels but tend to have a very modest effect. Examples include sitagliptin (Januvia), saxagliptin (Onglyza) and linagliptin (Tradjenta). Possible side effects include:
- Risk of pancreatitis.
- Joint pain.
- GLP-1 receptor agonists are injectable medications that slow digestion and help lower blood sugar levels. Their use is often associated with weight loss, and some may reduce the risk of heart attack and stroke. Examples include exenatide (Byetta, Bydureon Bcise), liraglutide (Saxenda, Victoza) and semaglutide (Rybelsus, Ozempic, Wegovy). Possible side effects include:
- Risk of pancreatitis.
- Nausea.
- Vomiting.
- Diarrhea.
- SGLT2 inhibitors affect the blood-filtering functions in the kidneys by blocking the return of glucose to the bloodstream. As a result, glucose is removed in the urine. These medicines may reduce the risk of heart attack and stroke in people with a high risk of those conditions. Examples include canagliflozin (Invokana), dapagliflozin (Farxiga) and empagliflozin (Jardiance). Possible side effects include:
- Vaginal yeast infections.
- Urinary tract infections.
- Low blood pressure.
- High cholesterol.
- Risk of gangrene.
- Risk of bone fractures (canagliflozin).
- Risk of amputation (canagliflozin).
Other medicines your doctor might prescribe in addition to diabetes medications include blood pressure and cholesterol-lowering medicines, as well as low-dose aspirin, to help prevent heart and blood vessel disease.
Insulin therapy
Some people who have type 2 diabetes need insulin therapy. In the past, insulin therapy was used as a last resort, but today it may be prescribed sooner if blood sugar targets aren’t met with lifestyle changes and other medicines.
Different types of insulin vary on how quickly they begin to work and how long they have an effect. Long-acting insulin, for example, is designed to work overnight or throughout the day to keep blood sugar levels stable. Short-acting insulin generally is used at mealtime.
Your doctor will determine what type of insulin is right for you and when you should take it. Your insulin type, dosage and schedule may change depending on how stable your blood sugar levels are. Most types of insulin are taken by injection.
Side effects of insulin include the risk of low blood sugar — a condition called hypoglycemia — diabetic ketoacidosis and high triglycerides.
Transient ischemic attack prognosis
Having a TIA is like having a temporary stroke. By definition, TIAs last less than 24 hours. But it’s rare for a TIA to last even that long. Most TIAs last for only minutes.
Several risk stratification scores have been developed to help physicians manage patients with a TIA. One widely used score is the ABCD2 score 23, 24, 25, 26, 27:
- A = Age more than 60 years (Score 1)
- B = Systolic BP> 140 or Diastolic BP> 90 (Score 1)
- C = Clinical features:
- Speech impairment without weakness (Score 1)
- Weakness with/without speech impairment (Score 2)
- D = Duration
- More than 60 mins (Score 2)
- Between 10-59 mins (Score 1)
- D = Diabetes (Score 1)
Patients with an ABCD2 score of 6 to 7 have an 8% risk of stroke within 48 hours.
Patients with an ABCD2 score of less than 4 have a 1% risk of stroke within 48 hours.
Most stroke centers will admit patients with TIA to the hospital for expedited management and observation if the ABCD2 score is 4, 5, or higher. For patients with a lower ABCD2 score, expedited evaluation and management are still warranted. This expedited approach has been proven to improve the outcome 23.
Even though ABCD2 scales are important in the evaluation of TIA, be aware that patients with critical carotid artery stenosis may sometimes present with a very low ABCD2 score 18.
- Albers GW, Caplan LR, Easton JD, Fayad PB, Mohr JP, Saver JL, Sherman DG; TIA Working Group. Transient ischemic attack–proposal for a new definition. N Engl J Med. 2002 Nov 21;347(21):1713-6. doi: 10.1056/NEJMsb020987[↩]
- Acheson J, Hutchinson EC: Observations on the natural history of transient cerebral ischæmia. The Lancet. 1964; 284(7365): 871–4. 10.1016/S0140-6736(64)90734-2[↩]
- Fisher CM: Concerning recurrent transient cerebral ischemic attacks. Can Med Assoc J. 1962; 86(24): 1091–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1849196/pdf/canmedaj00948-0002.pdf[↩]
- A classification and outline of cerebrovascular diseases. II. Stroke. 1975; 6(5): 564–616. 10.1161/01.str.6.5.564[↩]
- Lavallée PC, Meseguer E, Abboud H, et al.. A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects. Lancet Neurol. 2007;6(11):953-960. doi: 10.1016/S1474-4422(07)70248-X[↩][↩]
- Prabhakaran S, Silver AJ, Warrior L, McClenathan B, Lee VH. Misdiagnosis of transient ischemic attacks in the emergency room. Cerebrovasc Dis. 2008;26(6):630-635. doi: 10.1159/000166839[↩]
- Hackam DG, Spence JD. Combining multiple approaches for the secondary prevention of vascular events after stroke: a quantitative modeling study. Stroke. 2007;38(6):1881-1885. doi: 10.1161/STROKEAHA.106.475525[↩]
- Shahjouei S, Sadighi A, Chaudhary D, et al.. A 5-decade analysis of incidence trends of ischemic stroke after transient ischemic attack: a systematic review and meta-analysis. JAMA Neurol. 2020;17822:1-11. doi: 10.1001/jamaneurol.2020.3627[↩]
- Sanders LM, Srikanth VK, Jolley DJ, et al.. Monash transient ischemic attack triaging treatment: safety of a transient ischemic attack mechanism-based outpatient model of care. Stroke. 2012;43(11):2936-2941. doi: 10.1161/STROKEAHA.112.664060[↩]
- Jarhult SJ, Howell ML, Barnaure-Nachbar I, et al.. Implementation of a rapid, protocol-based TIA management pathway. West J Emerg Med. 2018;19(2):216-223. doi: 10.5811/westjem.2017.9.35341[↩]
- Webster F, Saposnik G, Kapral MK, Fang J, O’Callaghan C, Hachinski V. Organized outpatient care: stroke prevention clinic referrals are associated with reduced mortality after transient ischemic attack and ischemic stroke. Stroke. 2011;42(11):3176-3182. doi: 10.1161/STROKEAHA.111.621524[↩]
- Rothwell PM, Giles MF, Flossmann E, et al.. A simple score (ABCD) to identify individuals at high early risk of stroke after transient ischaemic attack. Lancet. 2005;366(9479):29-36. doi: 10.1016/S0140-6736(05)66702-5[↩]
- Sadighi A, Abedi V, Stanciu A, et al.. Six-month outcome of transient ischemic attack and its mimics. Front Neurol. 2019;10:294. doi: 10.3389/fneur.2019.00294[↩]
- Ranta A, Dovey S, Weatherall M, O’Dea D, Gommans J, Tilyard M. Cluster randomized controlled trial of TIA electronic decision support in primary care. Neurology. 2015;84(15):1545-1551. doi: 10.1212/WNL.0000000000001472[↩]
- Stroke – Causes and Risk Factors. https://www.nhlbi.nih.gov/health/stroke/causes[↩]
- Navis A, Garcia-Santibanez R, Skliut M. Epidemiology and Outcomes of Ischemic Stroke and Transient Ischemic Attack in the Adult and Geriatric Population. J Stroke Cerebrovasc Dis. 2019 Jan;28(1):84-89. doi: 10.1016/j.jstrokecerebrovasdis.2018.09.013[↩]
- Cereda CW, Olivot JM. Emergency Department (ED) Triage for Transient Ischemic Attack (TIA). Curr Atheroscler Rep. 2018 Sep 25;20(11):56. doi: 10.1007/s11883-018-0755-5[↩][↩]
- Panuganti KK, Tadi P, Lui F. Transient Ischemic Attack. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459143[↩][↩][↩]
- Liu L, Ding J, Leng X, Pu Y, Huang LA, Xu A, Wong KSL, Wang X, Wang Y. Guidelines for evaluation and management of cerebral collateral circulation in ischaemic stroke 2017. Stroke Vasc Neurol. 2018 May 30;3(3):117-130. doi: 10.1136/svn-2017-000135[↩]
- Bibok MB, Votova K, Balshaw RF, Penn M, Lesperance ML, Harris DR, Sedgwick C, Nealis M, Farrell B, Mathieson JR, Penn AM. Retrospective evaluation of a clinical decision support tool for effective computed tomography angiography utilization in urgent brain imaging of suspected TIA/minor stroke in the emergency department. CJEM. 2019 May;21(3):343-351. doi: 10.1017/cem.2018.449[↩]
- Johnston SC, Nguyen-Huynh MN, Schwarz ME, Fuller K, Williams CE, Josephson SA, Hankey GJ, Hart RG, Levine SR, Biller J, Brown RD Jr, Sacco RL, Kappelle LJ, Koudstaal PJ, Bogousslavsky J, Caplan LR, van Gijn J, Algra A, Rothwell PM, Adams HP, Albers GW. National Stroke Association guidelines for the management of transient ischemic attacks. Ann Neurol. 2006 Sep;60(3):301-13. doi: 10.1002/ana.20942[↩]
- Kirkland JB. Niacin. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease, 11th ed. Baltimore, MD: Williams & Wilkins; 2014:331-40.[↩]
- Cutting S, Regan E, Lee VH, Prabhakaran S. High ABCD2 Scores and In-Hospital Interventions following Transient Ischemic Attack. Cerebrovasc Dis Extra. 2016;6(3):76-83. doi: 10.1159/000450692[↩][↩]
- Wang J, et al. The ABCD2 score is better for stroke risk prediction after anterior circulation TIA compared to posterior circulation TIA. Int. J. Neurosci. 2015;125:50–55. doi: 10.3109/00207454.2014.905777[↩]
- Yang J, et al. Validation of the ABCD2 score to identify the patients with high risk of late stroke after a transient ischemic attack or minor ischemic stroke. Stroke. 2010;41:1298–1300. doi: 10.1161/STROKEAHA.110.578757[↩]
- Tao WD, et al. Posterior versus anterior circulation infarction: How different are the neurological deficits? Stroke. 2012;43:2060–2065. doi: 10.1161/STROKEAHA.112.652420[↩]
- Mayer L, Ferrari J, Krebs S, Boehme C, Toell T, Matosevic B, Tinchon A, Brainin M, Gattringer T, Sommer P, Thun P, Willeit J, Lang W, Kiechl S, Knoflach M; Austrian Stroke Unit Collaborators. ABCD3-I score and the risk of early or 3-month stroke recurrence in tissue- and time-based definitions of TIA and minor stroke. J Neurol. 2018 Mar;265(3):530-534. doi: 10.1007/s00415-017-8720-8[↩]





{kind=link}