Contents
- What is a tethered spinal cord
- What causes tethered spinal cord ?
- Tethered spinal cord symptoms
- How is tethered spinal cord diagnosed ?
- Treatment for tethered spinal cord
- What is myelomeningocele ?
- What is lipomyelomeningocele ?
- What is Syringomyelia
- What is Chiari malformations ?
- How common are Chiari malformations ?
- What causes these malformations ?
- How are Chiari malformations classified ?
- What are the symptoms of a Chiari malformation ?
- What other conditions are associated with Chiari malformations ?
- How are Chiari malformations diagnosed ?
- How are Chiari malformations treated ?
- Surgery
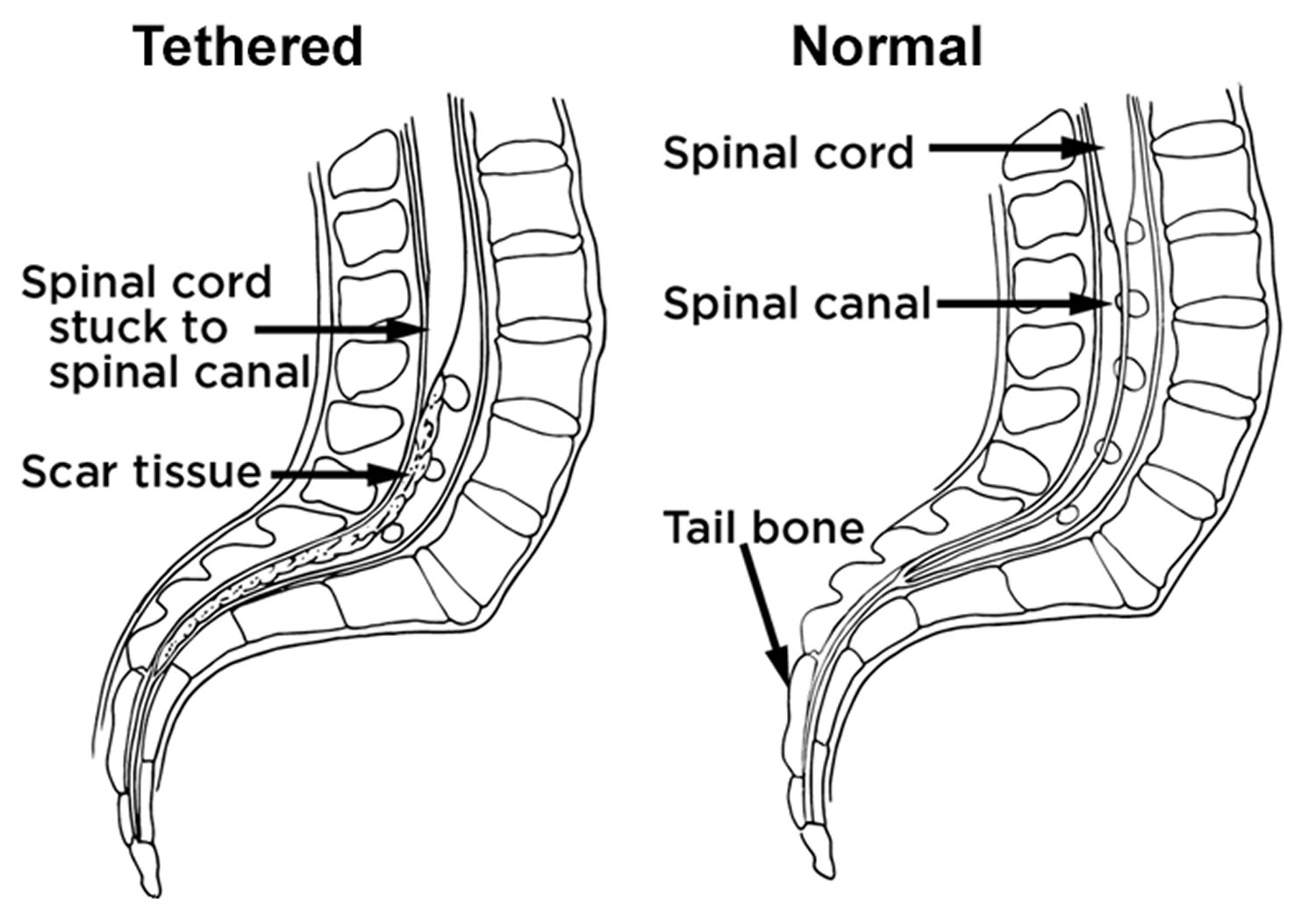
What is a tethered spinal cord
A tethered spinal cord is a spinal cord that is pulled down and stuck, or fixed, to the spinal canal 1. The spinal cord normally floats free inside the spinal canal.
Figure 1. Tethered spinal cord
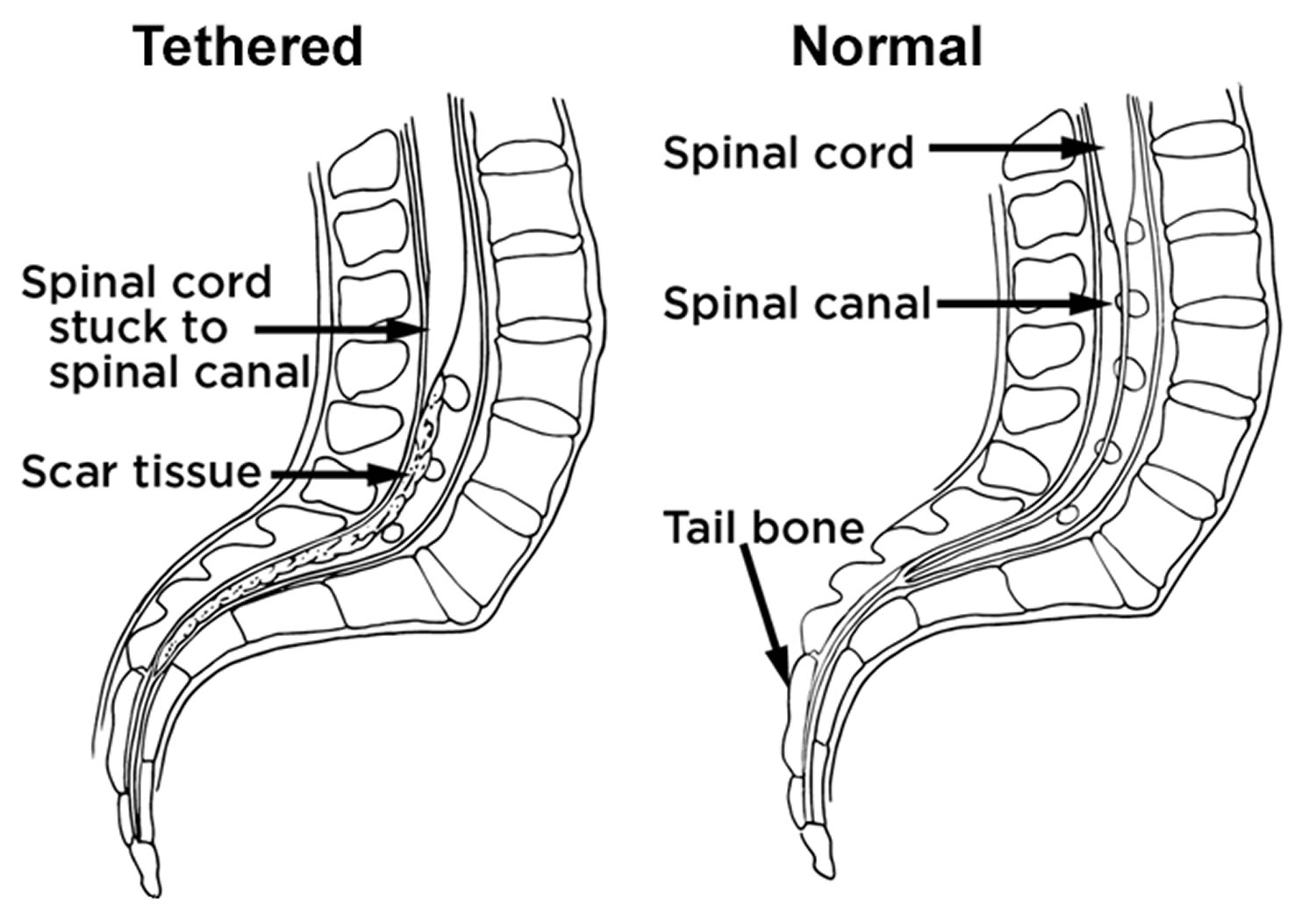
Tethered spinal cord syndrome is a neurological disorder caused by tissue attachments that limit the movement of the spinal cord within the spinal column 2. Attachments may occur congenitally (at birth) at the base of the spinal cord (conus medullaris) or they may develop near the site of an injury to the spinal cord. These attachments cause an abnormal stretching of the spinal cord.
The course of the tethered spinal cord disorder is progressive. In children, symptoms may include lesions, hairy patches, dimples, or fatty tumors on the lower back; foot and spinal deformities; weakness in the legs; low back pain; scoliosis; and incontinence. This type of tethered spinal cord syndrome appears to be the result of improper growth of the neural tube during fetal development, and is closely linked to spina bifida.
Tethered spinal cord syndrome may go undiagnosed until adulthood, when pain, sensory and motor problems, and loss of bowel and bladder control emerge. This delayed presentation of symptoms is related to the degree of strain placed on the spinal cord over time and may be exacerbated during sports or pregnancy, or may be due to narrowing of the spinal column (stenosis) with age.
Tethering of the spinal cord may also develop after spinal cord injury and scar tissue can block the flow of cerebrospinal fluids (CSF) around the spinal cord. Fluid pressure may cause cysts to form in the spinal cord, a condition called syringomyelia. This can lead to additional loss of movement, feeling or the onset of pain or autonomic symptoms.
What causes tethered spinal cord ?
Children have tethered spinal cords for many reasons. Tethered spinal cord most often happens in children who have birth defects called myelomeningoceles or lipomyelomeningoceles 1. Over time, the spinal cords of children with these conditions may become stuck, or tethered, to the myelomeningocele or lipomyelomeningocele. This pulls on the spinal cord as the child grows, causing symptoms.
A child also may have a tethered spinal cord for one of these reasons 1:
- The very end of their spinal cord is held down more tightly than normal (filum terminale).
- There is a small tract that is not normal, going from the skin into the spinal canal (dermal sinus tract).
- The spinal cord is split into 2 cords near the end (diastematomyelia or diplomyelia).
Tethered spinal cord symptoms
Children may have several symptoms of tethered spinal cord, including:
- Back pain or shooting pain in the legs
- Weakness, numbness or problems with muscle function in the legs
- Tremors or spasms in the leg muscles
- Changes in the way the feet look, like higher arches or curled toes
- Loss of bladder or bowel control that gets worse
- Scoliosis or abnormal curve of the spine that changes or gets worse
- Repeated bladder infections
- In a child with an unknown tethered cord, signs on the back such as a fatty mass, dimple, birthmark, tuft of hair or anorectal malformations
Children may also have myelomeningocele symptoms or lipomyelomeningocele symptoms if they have one of these birth defects.
If a tethered spinal cord is not repaired, it can cause lasting nerve damage and loss of function over time.
How is tethered spinal cord diagnosed ?
To diagnose tethered spinal cord, the doctor examines your child, looking for signs and symptoms. Your child most likely will have an MRI (magnetic resonance imaging). This test will help the doctor see inside your child’s body and assess their condition.
The place where the spinal cord ends can differ from child to child. Differences in the place where the cord ends are normal and happen even in children with no spinal cord problems. Also, some children with a tethered spinal cord have only a small tether at the end of the cord.
Often for children with mild signs or symptoms experts in Neurology, Neurosurgery, Urology and Neurodevelopmental are needed to evaluate a child and tell whether surgery is needed.
Treatment for tethered spinal cord
Treatment for a tethered spinal cord usually is surgery to free the spinal cord.
Neurosurgeons use advanced neuromonitoring during surgery. This lets them keep watch on the nerves and muscles of the lower part of your child’s body. It helps neurosurgeons avoid the risk of further damage to your child’s nerves.
Laminectomy
To free the spinal cord, neurosurgeons do a surgery called a laminectomy. They remove one or more parts of bones in the spine (vertebrae). This lets them reach the spinal cord, the spinal nerve roots and the thecal sac around the spinal cord.
The neurosurgeons then free the spinal cord by gently cutting, or teasing, it away from the scar tissue or fat. Neurosurgeons use a microscope to help them see the area during the surgery.
After the spinal cord is free, neurosurgeons sometimes apply a patch to the covering of the spinal cord (dura mater). This limits the chances cerebrospinal fluid (CSF) will leak.
Future surgeries
Once a child has had surgery to repair the spinal cord or has had the spinal cord freed up (detethered), there is a chance the cord will attach again as the child grows. Some children need more surgeries; this is more common in children who have myelomeningoceles or lipomyelomeningoceles.
What is myelomeningocele ?
Myelomeningocele is a birth defect in which the backbone and spinal canal do not close before birth 3.
Normally, during the first month of a pregnancy, the two sides of the baby’s spine (or backbone) join together to cover the spinal cord, spinal nerves and meninges (the tissues covering the spinal cord). The developing brain and spine at this point are called the neural tube. Spina bifida refers to any birth defect involving incomplete closure of the neural tube in the area of the spine.
Myelomeningocele is a severe form of spina bifida in which the spinal cord and nerves develop outside of the body and are contained in a fluid-filled sac that is visible outside of the back area 4.
Myelomeningocele is a neural tube defect in which the bones of the spine do not completely form. This results in an incomplete spinal canal. The spinal cord and meninges (the tissues covering the spinal cord) protrude from (stick out of) the child’s back.
Myelomeningocele may affect as many as 1-5 out of every 1,000-4,000 infants 4, 3.
In babies with myelomeningocele 5:
- The bones of the spine (vertebrae) do not form the normal way.
- A small sac extends through an opening in the spine. A membrane covers the sac.
- The sac holds cerebrospinal fluid (CSF) and tissues that protect the spinal cord (meninges).
- The sac may also contain parts of the spinal cord and nerves.
Other congenital disorders or birth defects may also be present in a child with myelomeningocele. Hydrocephalus may affect as many as 90% of children with myelomeningocele 3. Other disorders of the spinal cord or musculoskeletal system may be seen, including syringomyelia (a fluid-filled cyst within the spinal cord) and hip dislocation 3.
Sometimes the sac opens up. It can open because of normal movements of your baby, either before or during birth.
A myelomeningocele can happen anywhere along the spinal cord. It is most common in the lower back (lumbar and sacral areas). There is nerve damage below the level of the myelomeningocele. As a result of the nerve damage, babies may have symptoms.
Babies with myelomeningoceles lower in the spine have less severe symptoms. Babies with higher myelomeningoceles have more severe symptoms.
These babies typically have weakness and loss of sensation below the sac 4. This can result in muscle weakness and/or paralysis, bowel and bladder problems, excessive fluid on the brain (hydrocephalus), change in positioning of the brain (Chiari Malformation), seizures, and orthopedic conditions (scoliosis, hip problems, and foot deformities) 4.
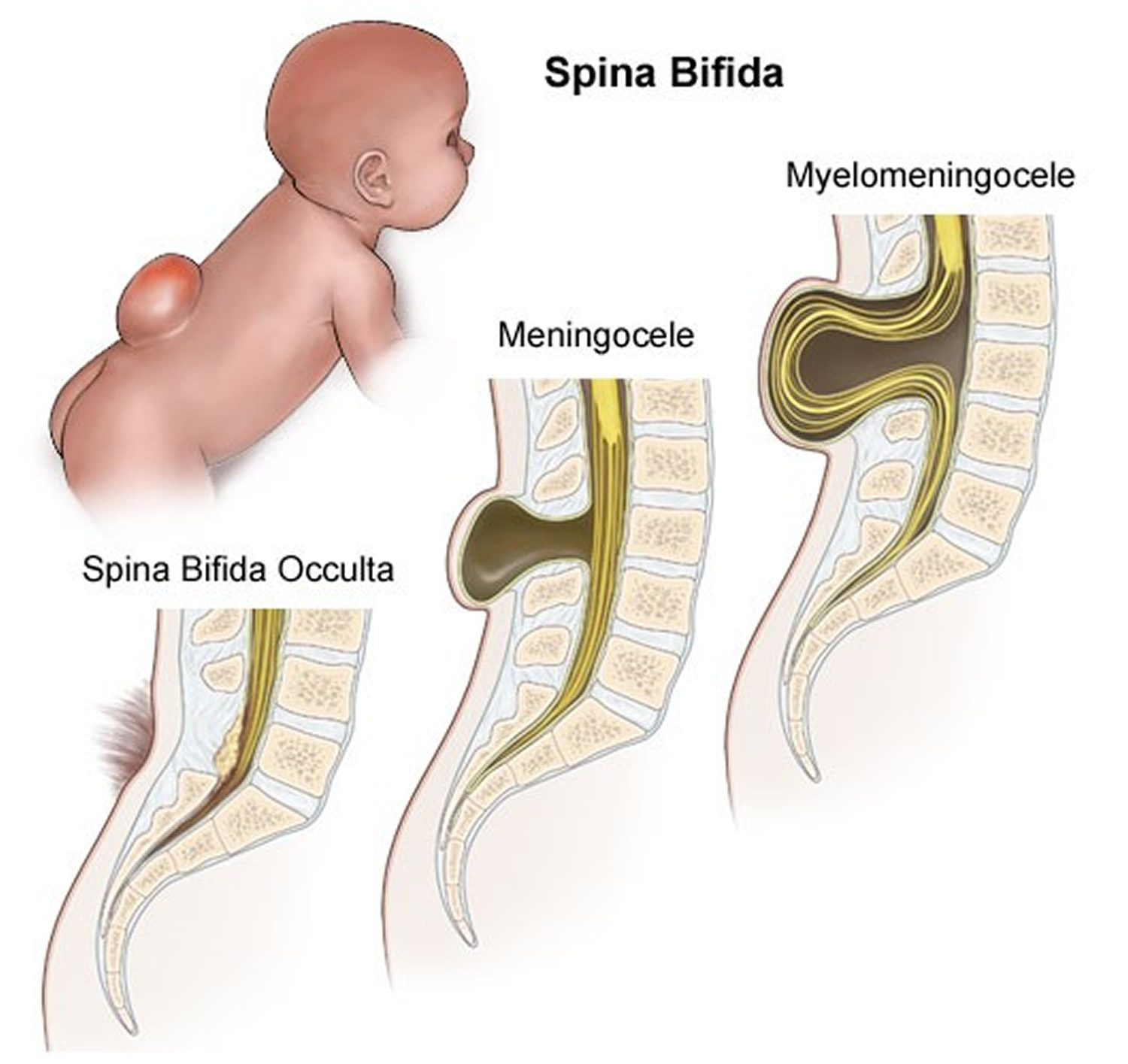
The rest of spina bifida cases are most commonly:
- Spina bifida occulta, a condition in which the bones of the spine do not close but the spinal cord and meninges remain in place and skin usually covers the defect.
- Meningoceles, a condition where the tissue covering the spinal cord protrudes from the spinal defect, but the spinal cord remains in place.
Figure 2. Myelomeningocele
What causes myelomeningocele ?
The cause of myelomeningocele is unknown. However, low levels of folic acid in a woman’s body before and during early pregnancy appear to play a part in this type of birth defect. Doctors now know what can help prevent myelomeningoceles. Early in pregnancy, it is very important for women to get enough folic acid in their diets. The vitamin folic acid (or folate) is important for brain and spinal cord development. The neural tube develops into the baby’s brain and spinal cord. Neural tube defects like myelomeningocele have become less common as doctors have learned about the link with folic acid and as more women have taken folic acid supplements during pregnancy.
If a child is born with myelomeningocele, future children in that family have a higher risk than the general population. However, in many cases, there is no family connection.
Some theorize that exposure to viruses may play a role, since there is a higher rate of this condition in children born in the early winter months. Research also indicates possible environmental factors such as radiation and/or genetics are suspected 4.
How to prevent myelomeningocele
Folic acid supplements may help reduce the risk of neural tube defects such as myelomeningocele. It is recommended that any woman considering becoming pregnant take 0.4 mg of folic acid a day. Pregnant women need 1 mg per day.
It is important to remember that folic acid deficiencies must be corrected before becoming pregnant, because the defects develop very early.
Prospective mothers may be screened to determine the amount of folic acid in their blood.
Symptoms of Myelomeningocele
A newborn with a myelomeningocele will have an open area or a fluid-filled sac on the mid to lower back. The baby is missing function, like movement or sensation, below the level of the problem. The higher the myelomeningocele is on the baby’s spinal cord, the more function is missing.
Myelomeningocele can cause symptoms that include 6:
- Problems moving parts of the body below the opening in the back
- Lack of sensation in their legs and feet
- Poor or no bowel and bladder control
- Twisted or abnormal legs and feet; for example, clubfoot
- Too much cerebrospinal fluid in the head (hydrocephalus)
- Problems with how the back of the brain formed (Chiari 2 malformation)
- Learning differences or delayed milestones (impaired cognitive development)
How is myelomeningocele diagnosed ?
Prenatal screening can help diagnose this condition. During the second trimester, pregnant women can have a blood test called the quadruple screen. This test screens for myelomeningocele, Down syndrome, and other congenital diseases in the baby. Most women carrying a baby with spina bifida will have a higher-than-normal level of a protein called maternal alpha fetoprotein (AFP).
If the quadruple screen test is positive, further testing is needed to confirm the diagnosis.
Such tests may include:
- Pregnancy ultrasound
- Amniocentesis
Myelomeningocele can be seen after the child is born. A neurologic exam may show that the child has loss of nerve-related functions below the defect. For example, watching how the infant responds to pinpricks at various locations may reveal where the baby can feel the sensations.
Doctors also find myelomeningoceles after a baby is born. The baby may have imaging tests that let doctors see the spine. They include:
- X-ray
- Ultrasound
- Computed tomography (CT) scan
- Magnetic resonance imaging (MRI)
Treating Myelomeningocele
Genetic counseling may be recommended. In some cases where a severe defect is detected early in the pregnancy, abortion may be considered 3. However, intrauterine surgery to close the defect (before the baby is born) is offered in some highly specialized centers and appears to reduce the risk of some later complications 3.
Infants and children with myelomeningocele may require surgery to reposition the spinal cord and close the opening in the back. Findings from the National Institutes of Health show that this surgery is most effective when it is done prenatally (while the baby is still in the womb) instead of after birth. The prenatal surgery reduces the occurrence of hydrocephalus and restores the cerebellum and brain stem to a more normal alignment.
After your baby is born, surgery to repair the defect is most often recommended within the first few days of life. Before surgery, the infant must be handled carefully to reduce damage to the exposed spinal cord. This may include special care and positioning, protective devices, and changes in the methods of handling, feeding, and bathing.
Children who also have hydrocephalus may need a ventriculoperitoneal shunt placed. This will help drain the extra fluid from the ventricles (in the brain) to the peritoneal cavity (in the abdomen).
Antibiotics may be used to treat or prevent infections such as meningitis or urinary tract infections.
Most children will require lifelong treatment for problems that result from damage to the spinal cord and spinal nerves.
This includes:
- Bladder and bowel problems. Gentle downward pressure over the bladder may help drain the bladder. Drainage tubes, called catheters, may be needed as well. Bowel training programs and a high fiber diet may improve bowel function.
- Muscle and joint problems. Orthopedic or physical therapy may be needed to treat musculoskeletal symptoms. Braces may be needed. Many people with myelomeningocele primarily use a wheelchair.
Follow-up exams generally continue throughout the child’s life. These are done to check the child’s developmental progress and to treat any intellectual, neurological, or physical problems.
Visiting nurses, social services, support groups, and local agencies can provide emotional support and assist with the care of a child with a myelomeningocele who has significant problems or limitations.
Outlook (Prognosis) for myelomeningocele
A myelomeningocele can most often be surgically corrected, but the affected nerves may still not function normally. The higher the location of the defect on the baby’s back, the more nerves will be affected.
With early treatment, length of life is not severely affected. Kidney problems due to poor drainage of urine are the most common cause of death.
Most children with myelomeningocele will have normal intelligence. However, because of the risk of hydrocephalus and meningitis, more of these children will have learning problems and seizure disorders.
New problems within the spinal cord can develop later in life, especially after the child begins growing rapidly during puberty. This can lead to more loss of function as well as orthopedic problems such as scoliosis, foot or ankle deformities, dislocated hips, and joint tightness or contractures.
Many people with myelomeningocele primarily use a wheelchair.
Possible Complications of myelomeningocele
Complications of spina bifida may include:
- Traumatic birth and difficult delivery of the baby
- Frequent urinary tract infections
- Fluid buildup on the brain (hydrocephalus)
- Loss of bowel or bladder control
- Low blood oxygen level in the baby
- Brain infection (meningitis)
- Permanent weakness or paralysis of legs
This list may not be all-inclusive.
Ongoing Care for myelomeningocele
Some children with myelomeningoceles have other conditions, like hydrocephalus, tethered spinal cord, Chiari malformation and syringomyelia, that need treatment.
Often, children with myelomeningoceles have other complex problems related to their nervous systems, such as problems with movement, lack of sensation, and lack of bowel and bladder control. These problems may require long-term care.
Each child is different, and we will tailor your child’s treatment to their needs. Your child’s neurosurgeon will work closely with other experts at Seattle Children’s to assess all your child’s needs and provide long-term coordinated care.
What is lipomyelomeningocele ?
A lipomyelomeningocele is a birth defect that affects a child’s backbone (spine).
A lipomyelomeningocele is a fatty mass under the skin on the child’s back. It is usually in the middle of the back. The mass attaches to the spinal cord and may slowly pull on the cord 7.
A lipomyelomeningocele is covered by skin. You can usually see it on the outside of the child’s body. It looks like a large lump.
Lipomyelomeningoceles are present when a baby is born (congenital).
- Lipomyelomeningoceles happen in only 1 to 2 of every 10,000 babies born in the United States.
- Lipomyelomeningocele is slightly more common in girls.
Babies develop lipomyelomeningoceles early in their mother’s pregnancy – during the fourth to sixth week. There is no known cause. The genes babies get from their parents do not play a role. It is not caused by mothers getting too little folic acid during pregnancy 7.
Symptoms of Lipomyelomeningocele
All babies with a lipomyelomeningocele have a spinal cord that is stuck (tethered) into the fatty mass on their back. This may pull the spinal cord downward. Tethered spinal cord can cause symptoms, including:
- Back and leg pain
- Weak and numb legs
- Changes in bladder and bowel control
Diagnosing Lipomyelomeningocele
Usually, doctors can see a lipomyelomeningocele when a baby is born. They may see a lump or some other type of mark on your baby’s back, such as a fat pad, birthmark, dimple or tuft of hair.
Your child’s doctor will ask for a magnetic resonance imaging (MRI) of the spine to get a better view of your baby’s spinal cord and any problems that relate to it.
Sometimes, there is no lump or other mark on the baby’s back, and the child has no symptoms early on or never has symptoms at all. These cases may be diagnosed later in life, if symptoms develop, or if a scan done for some other reason shows the lipomyelomeningocele.
Lipomyelomeningocele Treatment
Most babies with a lipomyelomeningocele need surgery.
Some lipomyelomeningoceles are not diagnosed until later in life because they caused no signs or symptoms earlier. These cases may not require surgery, unless the condition starts to cause pain or other problems.
Even after surgery to repair a lipomyelomeningocele, the spinal cord can become tethered. This can lead to neurological damage over time, especially during growth, because growth can stretch the tethered spinal cord. Slowly, the child may lose sensory and motor function. The feet may get weaker. Bladder and bowel function may get worse or be lost. These changes may last forever.
About 2 in 10 children in the United States who have had surgery for lipomyelomeningocele develop a tethered spinal cord and need more surgeries.
Treatment Options for Lipomyelomeningocele
Most often, babies treated with surgery before age 1.
Your child’s neurosurgeon begins with a surgery called a laminectomy. The neurosurgeon removes parts of some bones in the spine (vertebrae). This lets the neurosurgeon get to the spinal cord or spinal nerve roots that need repair.
Next neurosurgeons remove some of the fatty mass (sometimes using a laser), and they free the spinal cord. Then they close the hole where the fatty mass enters your baby’s spinal canal. The neurosurgeon will monitor your child’s nerve function electrically during the surgery.
What is Syringomyelia
Syringomyelia is a rare disorder that causes a cyst to form in your spinal cord 8. This cyst, also called a syrinx, gets bigger and longer over time, destroying part of the spinal cord 8.
A watery liquid known as cerebrospinal fluid (CSF) normally surrounds and protects the brain and spinal cord. Cerebrospinal fluid also fills connected cavities within the center of the brain called the ventricles which continue to a small central canal that runs the length of the spinal cord. When a person has syringomyelia this fluid collects within the tissue of the spinal cord, expands the central canal and forms a syrinx. Generally, a syrinx develops when the normal flow of cerebrospinal fluid fluid around the spinal cord or lower brain stem is disturbed. When syrinxes affect the brain stem, the condition is called syringobulbia.
Damage to the spinal cord from the syrinx can cause symptoms such as:
- Pain and weakness in the back, shoulders, arms or legs
- Headaches
- Inability to feel hot or cold
Symptoms vary according to the size and location of the syrinx. They often begin in early adulthood.
What are the forms of syringomyelia ?
There are two major forms of syringomyelia:
- Congenital syringomyelia (also known as communicating syringomyelia). In most cases, syringomyelia is caused by a Chiari malformation which may allow a syrinx to develop, most often in the spine’s cervical (neck) region. Symptoms usually begin between the ages of 25 and 40. People with congenital syringomyelia may also have hydrocephalus, a buildup of excess CSF in the brain with enlargement of the cerebral ventricles. Straining or coughing can force CSF into the ventricles, causing the person to develop headache or even lose consciousness (so called cough syncope). In addition, they may have a disorder called arachnoiditis—an inflammation of the arachnoid, one of the three membranes that surrounds the spinal cord.
- Acquired syringomyelia (also known as primary spinal syringomyelia or noncommunicating syringomyelia). Causes of acquired syringomyelia include spinal cord injury, meningitis (an inflammation of brain and spinal cord membranes usually caused by an infection), arachnoiditis, tethered cord syndrome (a condition that is present at birth that causes the spinal cord to abnormally attach to the tissues in the lower spine, limiting its movement), a spinal cord tumor, and bleeding into the cord (hemorrhage)
What causes syringomyelia ?
Syringomyelia may have several possible causes but most cases are associated with Chiari malformation—an abnormal condition in which brain tissue extends through the hole at the bottom of the skull (foramen magnum) and into the spinal canal, and obstructs the flow of cerebrospinal fluid (CSF). Syringomyelia may also be caused by spinal cord injuries, spinal cord tumors, and damage caused by inflammation in around the spinal cord. In some cases, the cause is unknown (idiopathic).
Syringomyelia in Children
Children who have other problems involving the brain and spinal cord often have syringomyelia too. Many times, these other neurological problems are present when the baby is born (congenital). Congenital problems that can cause syringomyelia include:
- Chiari 1 and 2 malformations
- Hydrocephalus
- Myelomeningocele
- Lipomyelomeningocele
Other childhood conditions, such as spinal cord tethering or a spinal cord tumor, can also cause syringomyelia.
Not all children with these conditions develop syringomyelia. But any of the conditions can change the normal flow of a child’s cerebrospinal fluid (CSF). The cerebrospinal fluid often collects inside the spinal cord to form a cyst.
Children can also develop syringomyelia later on in life. Conditions that may trigger the formation of a cyst include:
- Injury to the neck or spine
- Meningitis
- Tumors
Syringomyelia can also occur without a clear cause.
Symptoms of Syringomyelia
Symptoms of damage to the spinal cord vary among individuals according to where the syrinx forms, how large it is, and how long it extends. Symptoms develop slowly over time and may occur on one or both sides of the body. Sometimes coughing and straining can trigger symptoms, but they do not cause syringomyelia.
Symptoms may include:
- Headaches
- Weakness
- Pain
- Numbness (decreased feeling of touch)
- Tingling, especially in the arms and hands
- Abnormal reflexes of arms and legs
- Spasticity of arms or legs (stiff, rigid or uncontrollable muscle reflexes)
- Abnormal curve in the spine (scoliosis)
- Progressive weakness in the arms and legs
- Loss of muscle mass in the arms and legs
- Loss of bowel and bladder control
- Problems with sexual function
- Stiffness in the back, shoulders, neck, arms, or legs
- Loss of sensitivity to pain or hot and cold, especially in the hands
- Imbalance
- Curvature of the spine (scoliosis) that may be the only symptom in children.
Syringomyelia Diagnosis
Doctors will watch for signs of syringomyelia if your child has one of the brain and spinal cord conditions that are associated with it. Your child’s doctor may also do a neurological exam. This helps the doctor find out if your child has lost any ability to move or feel due to pressure on the spine.
In addition, your child may have an MRI (magnetic resonance imaging) of the spine to help doctors look for the cyst.
Syringomyelia Treatment Options 9
The type of treatment for syringomyelia depends on the severity and progression of an individual’s symptoms. Your child’s treatment depends on what has caused syringomyelia to develop. Whenever possible, doctors will correct the basic cause of the cyst.
It is common for children with a Chiari malformation to have syringomyelia. In these cases, doctorse know your child needs surgery to repair the Chiari malformation. This surgery will provide more space in your child’s head for the brain. It will allow for more normal flow of the cerebrospinal fluid that fills the cyst.
Monitoring
In the absence of symptoms, syringomyelia is usually not treated. In addition, a physician may recommend not treating the condition in individuals of advanced age or in cases where there is no progression of symptoms. However, people should be carefully monitored by a neurologist or neurosurgeon as symptoms can worsen over time. Individuals may also want to avoid activities that involve straining (e.g., lifting heavy objects, jumping) since these actions can trigger symptoms. People with an associated Chiari malformation are especially apt to experience headache with straining.
Surgery
Surgery is usually recommended for individuals with symptomatic or progressive syringomyelia. There are two general forms of treatment: restoration of normal CSF flow around the spinal cord, and direct drainage of the syrinx. The type of treatment depends on what is causing the symptoms.
- Treating the Chiari malformation. The main goal of Chiari surgery is to provide more space at the base of the skull and upper neck. This reduces pressure on the brain and spinal cord and restores the normal flow of CSF. Surgery can allow the syrinx to drain, sometimes becoming smaller or even disappearing entirely. Symptoms may improve even if the syrinx remains the same size or is reduced only slightly. Individuals should get treated sooner rather than later since delaying treatment can cause irreversible spinal cord damage. Syringomyelia can reoccur after surgery, making additional operations necessary.
- Preventing a syrinx from forming or expanding after an injury. In the case of trauma-related syringomyelia, the primary strategy is to prevent a syrinx from developing or growing in the first place. This somewhat controversial procedure (called expansive duraplasty) is done in a surgical operation on the spine that involves removing scar tissue around the spinal cord and sometimes adding a patch to expand the “dura,” the membrane that surrounds the spinal cord. By clearing and expanding the space around the spinal cord, the normal flow of CSF may be restored.
- Removing the obstruction. Surgical removal of obstructions such as scar tissue, bone from the spinal canal, or tumors can help restore the normal flow of CSF. If a tumor is causing syringomyelia, removing the tumor almost always eliminates the syrinx. Occasionally, radiation may also be used to shrink the tumor.
- Draining the syrinx. Especially if there is no associated Chiari malformation or tumor, it may be necessary to drain the syrinx. This is usually done in cases where the syrinx is growing or the cause of the CSF obstruction cannot be identified. To perform this procedure a surgeon inserts a drain called a stent or shunt. A stent consists of a small tube that is inserted into the syrinx fluid and allows fluid from within the cord to drain into the space just outside the spinal cord. Similarly, a shunt consists of a flexible tube and a valve that drains the syrinx fluid into another part of the body, usually the abdomen. By draining the syrinx, both of these procedures can halt the progression of symptoms and relieve headache. However, these procedures carry the risk of spinal cord injury, infection, or bleeding, and may not help all individuals.
What is Chiari malformations ?
Chiari malformations are structural defects in the base of the skull and cerebellum, the part of the brain that controls balance 10. Normally the cerebellum and parts of the brain stem sit above an opening in the skull that allows the spinal cord to pass through it (called the foramen magnum). When part of the cerebellum extends below the foramen magnum and into the upper spinal canal, it is called a Chiari malformation 10.
Chiari malformations may develop when part of the skull is smaller than normal or misshapen, which forces the cerebellum to be pushed down into the foramen magnum and spinal canal 10. This causes pressure on the cerebellum and brain stem that may affect functions controlled by these areas and block the flow of cerebrospinal fluid (CSF)—the clear liquid that surrounds and cushions the brain and spinal cord. The cerebrospinal fluid also circulates nutrients and chemicals filtered from the blood and removes waste products from the brain.
How common are Chiari malformations ?
In the past, it was estimated that the condition occurs in about one in every 1,000 births. However, the increased use of diagnostic imaging has shown that Chiari malformation may be much more common. Complicating this estimation is the fact that some children who are born with this condition may never develop symptoms or show symptoms only in adolescence or adulthood. Chiari malformations occur more often in women than in men and Type II malformations are more prevalent in certain groups, including people of Celtic descent.
What causes these malformations ?
Chiari malformation has several different causes. Most often it is caused by structural defects in the brain and spinal cord that occur during fetal development. This can be the result of genetic mutations or a maternal diet that lacked certain vitamins or nutrients. This is called primary or congenital Chiari malformation. It can also be caused later in life if spinal fluid is drained excessively from the lumbar or thoracic areas of the spine either due to traumatic injury, disease, or infection. This is called acquired or secondary Chiari malformation. Primary Chiari malformation is much more common than secondary Chiari malformation.
How are Chiari malformations classified ?
Chiari malformations are classified by the severity of the disorder and the parts of the brain that protrude into the spinal canal 10.
Chiari malformation Type I
Type 1 happens when the lower part of the cerebellum (called the cerebellar tonsils) extends into the foramen magnum. Normally, only the spinal cord passes through this opening. Type 1—which may not cause symptoms—is the most common form of Chiari malformation. It is usually first noticed in adolescence or adulthood, often by accident during an examination for another condition. Adolescents and adults who have Chiari malformation but no symptoms initially may develop signs of the disorder later in life.
Chiari malformation Type II
Individuals with Type II have symptoms that are generally more severe than in Type 1 and usually appear during childhood. This disorder can cause life-threatening complications during infancy or early childhood, and treating it requires surgery.
In Type II, also called classic Chiari malformation, both the cerebellum and brain stem tissue protrude into the foramen magnum. Also the nerve tissue that connects the two halves of the cerebellum may be missing or only partially formed. Type II is usually accompanied by a myelomeningocele—a form of spina bifida that occurs when the spinal canal and backbone do not close before birth. Spina bifida is a disorder characterized by the incomplete development of the brain, spinal cord, and/or their protective covering. A myelomeningocele usually results in partial or complete paralysis of the area below the spinal opening. The term Arnold-Chiari malformation (named after two pioneering researchers) is specific to Type II malformations.
Chiari malformation Type III
Type III is very rare and the most serious form of Chiari malformation. In Type III, some of the cerebellum and the brain stem stick out, or herniate, through an abnormal opening in the back of the skull. This can also include the membranes surrounding the brain or spinal cord.
The symptoms of Type III appear in infancy and can cause debilitating and life-threatening complications. Babies with Type III can have many of the same symptoms as those with Type II but can also have additional severe neurological defects such as mental and physical delays, and seizures.
Chiari malformation Type IV
Type IV involves an incomplete or underdeveloped cerebellum (a condition known as cerebellar hypoplasia). In this rare form of Chiari malformation, the cerebellum is located in its normal position but parts of it are missing, and portions of the skull and spinal cord may be visible.
What are the symptoms of a Chiari malformation ?
Headache is the hallmark sign of Chiari malformation, especially after sudden coughing, sneezing, or straining. Other symptoms may vary among individuals and may include 10:
- neck pain
- hearing or balance problems
- muscle weakness or numbness
- dizziness
- difficulty swallowing or speaking
- vomiting
- ringing or buzzing in the ears (tinnitus)
- curvature of the spine (scoliosis)
- insomnia
- depression
- problems with hand coordination and fine motor skills.
Some individuals with Chiari malformation may not show any symptoms. Symptoms may change for some individuals, depending on the compression of the tissue and nerves and on the buildup of CSF pressure.
Infants with a Chiari malformation may have difficulty swallowing, irritability when being fed, excessive drooling, a weak cry, gagging or vomiting, arm weakness, a stiff neck, breathing problems, developmental delays, and an inability to gain weight.
What other conditions are associated with Chiari malformations ?
Hydrocephalus is an excessive buildup of CSF in the brain. A Chiari malformation can block the normal flow of this fluid and cause pressure within the head that can result in mental defects and/or an enlarged or misshapen skull. Severe hydrocephalus, if left untreated, can be fatal. The disorder can occur with any type of Chiari malformation, but is most commonly associated with Type II.
Spina bifida is the incomplete closing of the backbone and membranes around the spinal cord. In babies with spina bifida, the bones around the spinal cord do not form properly, causing defects in the lower spine. While most children with this birth defect have such a mild form that they have no neurological problems, individuals with Type II Chiari malformation usually have myelomeningocele, and a baby’s spinal cord remains open in one area of the back and lower spine. The membranes and spinal cord protrude through the opening in the spine, creating a sac on the baby’s back. This can cause a number of neurological impairments such as muscle weakness, paralysis, and scoliosis.
Syringomyelia is a disorder in which a CSF-filled tubular cyst, or syrinx, forms within the spinal cord’s central canal. The growing syrinx destroys the center of the spinal cord, resulting in pain, weakness, and stiffness in the back, shoulders, arms, or legs. Other symptoms may include a loss of the ability to feel extremes of hot or cold, especially in the hands. Some individuals also have severe arm and neck pain.
Tethered spinal cord syndrome occurs when a child’s spinal cord abnormally attaches to the tissues around the bottom of the spine. This means the spinal cord cannot move freely within the spinal canal. As a child grows, the disorder worsens, and can result in permanent damage to the nerves that control the muscles in the lower body and legs. Children who have a myelomeningocele have an increased risk of developing a tethered cord later in life.
Spinal curvature is common among individuals with syringomyelia or Chiari malformation Type I. The spine either may bend to the left or right (scoliosis) or may bend forward (kyphosis).
How are Chiari malformations diagnosed ?
Currently, no test is available to determine if a baby will be born with a Chiari malformation. Since Chiari malformations are associated with certain birth defects like spina bifida, children born with those defects are often tested for malformations. However, some malformations can be seen on ultrasound images before birth.
Many people with Chiari malformations have no symptoms and their malformations are discovered only during the course of diagnosis or treatment for another disorder. The doctor will perform a physical exam and check the person’s memory, cognition, balance (functions controlled by the cerebellum), touch, reflexes, sensation, and motor skills (functions controlled by the spinal cord). The physician may also order one of the following diagnostic tests:
- Magnetic resonance imaging (MRI) is the imaging procedure most often used to diagnose a Chiari malformation. It uses radio waves and a powerful magnetic field to painlessly produce either a detailed three-dimensional picture or a two-dimensional “slice” of body structures, including tissues, organs, bones, and nerves.
- X-rays use electromagnetic energy to produce images of bones and certain tissues on film. An X-ray of the head and neck cannot reveal a Chiari malformation but can identify bone abnormalities that are often associated with the disorder.
- Computed tomography (CT) uses X-rays and a computer to produce two-dimensional pictures of bone and blood vessels. CT can identify hydrocephalus and bone abnormalities associated with Chiari malformation.
How are Chiari malformations treated ?
Some Chiari malformations do not show symptoms and do not interfere with a person’s activities of daily living. In these cases, doctors may only recommend regular monitoring with MRI. When individuals experience pain or headaches, doctors may prescribe medications to help ease symptoms.
Surgery
In many cases, surgery is the only treatment available to ease symptoms or halt the progression of damage to the central nervous system. Surgery can improve or stabilize symptoms in most individuals. More than one surgery may be needed to treat the condition.
The most common surgery to treat Chiari malformation is posterior fossa decompression. It creates more space for the cerebellum and relieves pressure on the spinal cord. The surgery involves making an incision at the back of the head and removing a small portion of the bone at the bottom of the skull (craniectomy). In some cases the arched, bony roof of the spinal canal, called the lamina, may also be removed (spinal laminectomy). The surgery should help restore the normal flow of CSF, and in some cases it may be enough to relieve symptoms.
Next, the surgeon may make an incision in the dura, the protective covering of the brain and spinal cord. Some surgeons perform a Doppler ultrasound test during surgery to determine if opening the dura is even necessary. If the brain and spinal cord area is still crowded, the surgeon may use a procedure called electrocautery to remove the cerebellar tonsils, allowing for more free space. These tonsils do not have a recognized function and can be removed without causing any known neurological problems.
The final step is to sew a dura patch to expand the space around the tonsils, similar to letting out the waistband on a pair of pants. This patch can be made of artificial material or tissue harvested from another part of an individual’s body.
Infants and children with myelomeningocele may require surgery to reposition the spinal cord and close the opening in the back. Findings from the National Institutes of Health show that this surgery is most effective when it is done prenatally (while the baby is still in the womb) instead of after birth. The prenatal surgery reduces the occurrence of hydrocephalus and restores the cerebellum and brain stem to a more normal alignment.
Hydrocephalus may be treated with a shunt (tube) system that drains excess fluid and relieves pressure inside the head. A sturdy tube, surgically inserted into the head, is connected to a flexible tube placed under the skin. These tubes drain the excess fluid into either the chest cavity or the abdomen so it can be absorbed by the body.
An alternative surgical treatment in some individuals with hydrocephalus is third ventriculostomy, a procedure that improves the flow of CSF out of the brain. A small hole is made at the bottom of the third ventricle (brain cavity) and the CSF is diverted there to relieve pressure. Similarly, in cases where surgery was not effective, doctors may open the spinal cord and insert a shunt to drain a syringomyelia or hydromyelia (increased fluid in the central canal of the spinal cord).
- What is a tethered spinal cord ? Seattle Children’s Hospital. http://www.seattlechildrens.org/medical-conditions/brain-nervous-system-mental-conditions/tethered-spinal-cord/[↩][↩][↩]
- Tethered Spinal Cord Syndrome Information Page. National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/Disorders/All-Disorders/Tethered-Spinal-Cord-Syndrome-Information-Page[↩]
- Myelomeningocele. Medline Plus. https://medlineplus.gov/ency/article/001558.htm[↩][↩][↩][↩][↩][↩]
- Myelomeningocele. Washington University Orthopedics. http://www.ortho.wustl.edu/content/Patient-Care/6885/Services/Pediatric-and-Adolescent-Orthopedic-Surgery/Overview/Spine-Education-Overview/Myelomeningocele.aspx[↩][↩][↩][↩][↩]
- What is a myelomeningocele ? Seattle Children’s Hospital. http://www.seattlechildrens.org/medical-conditions/chromosomal-genetic-conditions/myelomeningocele/[↩]
- Myelomeningocele. Seattle Children’s Hospital. http://www.seattlechildrens.org/medical-conditions/chromosomal-genetic-conditions/myelomeningocele/[↩]
- Lipomyelomeningocele. Seattle Children’s Hospital. http://www.seattlechildrens.org/medical-conditions/chromosomal-genetic-conditions/lipomyelomeningocele/[↩][↩]
- Syringomyelia. Medline Plus. https://medlineplus.gov/syringomyelia.html[↩][↩]
- Syringomyelia Treatment. Seattle Children’s Hospital. http://www.seattlechildrens.org/medical-conditions/chromosomal-genetic-conditions/syringomyelia-treatment/[↩]
- Chiari Malformation Fact Sheet. National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Chiari-Malformation-Fact-Sheet[↩][↩][↩][↩][↩]





{kind=link}