Contents
- What is eye pain
- Table 1. Causes of Eye Pain: Key Features and Management Options
- How is eye pain diagnosed
- Clinical History
- Functional Assessment
- Anatomic Assessment
- What is Hyphema ?
- What Is Bacterial Keratitis ?
- What is Eye Cellulitis ?
- What is Conjunctivitis (Pink Eye) ?
- What is Fungal Keratitis ?
- What is Herpes Keratitis ?
- What is Corneal Abrasion ?
- What Is Corneal Laceration ?
- What is a Corneal Ulcer ?
- What is Fuchs’ Dystrophy ?
- What Is Glaucoma ?
- What Is Uveitis ?
- What Is Optic Neuritis ?
- What Is Microvascular Cranial Nerve Palsy ?
- What Is Bell’s Palsy ?
- What is a Black Eye ?
- What Is a Blocked Tear Duct ?
What is eye pain
Pain in the eye is defined as physical discomfort due to an eye condition or injury 1. Whereas pain and tenderness around the eye can be caused by disease involving the eyelids and tissues around the eye 2.
- Eye pain with vision loss requires immediate ophthalmology referral.
It’s important to remember that many people do not know they have eye disease because there are often no warning signs or symptoms, or they assume that poor sight is a natural part of growing older. Early detection and treatment of eye problems is the best way to keep your healthy vision throughout your life. In many cases, blindness and vision loss are preventable.
The symptoms and possible related eye conditions/diseases in this section are for general reference only, and do not contain all visual symptoms or all possible related conditions or diseases. If you have any unusual vision symptoms, see your ophthalmologist.
Pain in Eye may be associated with 1. Whereas pain and tenderness around the eye can be caused by disease involving the eyelids and tissues around the eye 2:
- Bacterial Keratitis
- Cellulitis
- Conjunctivitis (Pink Eye)
- Corneal Abrasion
- Corneal Laceration
- Corneal Ulcer
- Fuchs’ Dystrophy
- Fungal Keratitis
- Glaucoma
- Herpes Keratitis
- Hyphema
- Microvascular Cranial Nerve Palsy
- Optic Neuritis
- Uveitis
Pain Around Eye may be associated with 2:
- Bell’s Palsy
- Black Eye
- Blocked Tear Duct
- Cellulitis
- Glaucoma
- Microvascular Cranial Nerve Palsy.
Emergency Eye Disease
A history of trauma and signs of hyphema or corneal penetration warrant urgent, same-day evaluation by an ophthalmologist 3. A hyphema is a collection or pooling of blood in the anterior chamber between the cornea and the iris. A positive result on the Seidel test indicates a foreign body that has penetrated the full thickness of the cornea. This occurs when the anterior chamber has been punctured and its aqueous humor dilutes the fluorescein dye, causing it to flow across the cornea 4.
In acute angle-closure glaucoma, optic nerve atrophy and permanent loss of vision can occur within hours if not adequately treated. Prompt consultation with an ophthalmologist is recommended for treatment to lower the intraocular pressure 5.
Orbital cellulitis requires hospital admission, broad-spectrum intravenous antibiotics, and ophthalmology consultation. Workup includes contrast-enhanced computed tomography of the orbits and paranasal sinuses, as well as complete blood count and blood cultures 6.
Because scleritis (inflammation of the sclera of the eye) can cause vision loss, the involvement of the more posterior structure, such as the retina, should be determined and managed accordingly.
Immediate referral is important if anterior uveitis is suspected because this disorder can also impair vision. A slit lamp examination looking for inflammatory cells in the anterior chamber is key to the diagnosis.
Optic neuritis warrants neurology and ophthalmology consultation. Acute management of optic neuritis includes administration of high-dose corticosteroids, which improves short-term recovery and expedites resolution of vision loss 7.
Infectious keratitis (caused by bacteria, Acanthamoeba, Herpes simplex virus and herpes zoster ophthalmicus) necessitates ophthalmologic referral. Recurrent Herpes simplex virus keratitis increases risk of visual loss from corneal damage 8, and herpes zoster ophthalmicus can cause chronic ocular inflammation, vision loss, and disabling pain 9.
Figure 1. Human eye
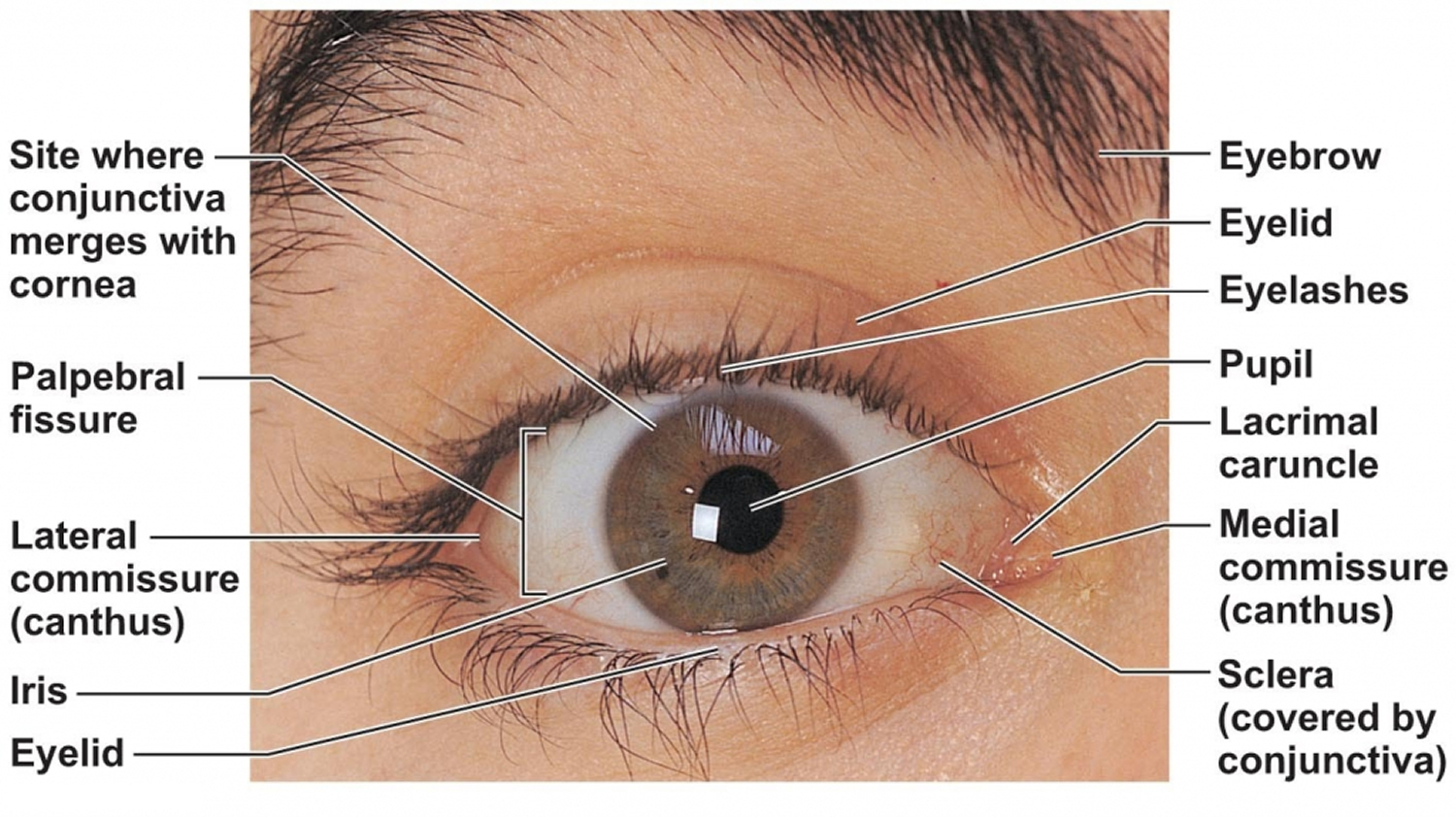
Figure 2. Eye anatomy
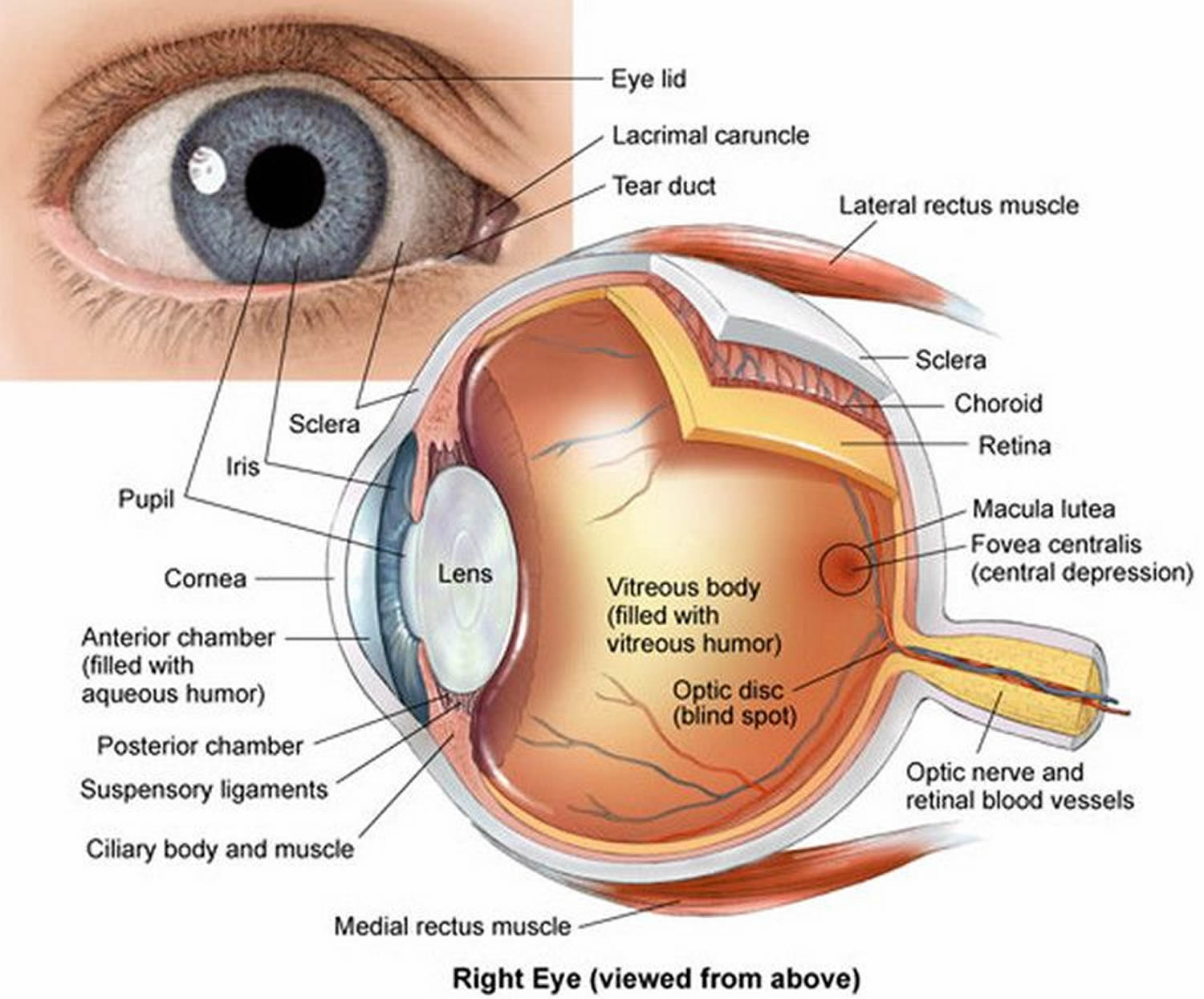
Note: The Uvea is a layer of tissue beneath the white of the eye (sclera). The Uvea has three parts: the iris, which is the colored part of the eye; the choroid layer, which is the layer of blood vessels and connective tissue between the sclera and the retina; and the ciliary body, which secretes the transparent liquid (aqueous humor) into the eye.
Eye problems constitute 2% to 3% of all primary care and emergency department visits 10, 11. Conjunctivitis, corneal abrasion, and hordeolum (stye) account for more than 50% of eye problems 10, 11. A hordeolum (ie, stye) is a localized infection or inflammation of the eyelid margin involving hair follicles of the eyelashes (ie, external hordeolum) or meibomian glands (ie, internal hordeolum). A hordeolum usually is painful, erythematous, and localized. Disorders that cause eye pain can be divided by anatomic area, with most affecting the cornea. Because most conditions that cause eye pain are associated with ocular signs and symptoms, familiarity with the differential diagnosis allows clinicians to appropriately tailor the history and physical examination (Table 1 3–20 and Table 2 11).
Table 1. Causes of Eye Pain: Key Features and Management Options
| Diagnosis | Key features | Management options |
|---|---|---|
Conjunctiva | ||
|
|
|
|
|
|
Sclera | ||
|
|
|
Cornea | ||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Anterior chambers | ||
|
|
|
Uvea | ||
|
|
|
Other | ||
|
| First-line treatment for acute cluster headache: sumatriptan (Imitrex) or zolmitriptan (Zomig) plus oxygen, 12 to 15 L per minute for 15 minutes, administered through a nonrebreather face mask |
|
|
|
|
|
|
How is eye pain diagnosed
Clinical History
Initial evaluation should include questions about vision loss or changes.
- Eye pain with vision loss requires immediate ophthalmology referral.
A foreign body sensation suggests a corneal process, such as a corneal abrasion, retained foreign body, or keratitis.3 In contrast, a scratchy, gritty, or sandy sensation is more likely to be associated with conjunctivitis 13.
When assessing for keratitis (inflammation of the cornea of the eye), clinicians should ask about contact lens use and discuss lens care regimens. A contact lens history includes wearing schedule; overnight wear; contact lens hygiene protocol; use of tap water to rinse contact lenses; and swimming, using a hot tub, or showering while wearing contact lenses. Bacterial and Acanthamoeba keratitis are associated with inappropriate contact lens use or care 18, 27, 28.
Photophobia (extreme sensitivity to light) can be a sign of corneal involvement 12, 13. Photophobia with eye pain is associated with most forms of keratitis, but can also occur with anterior uveitis and less commonly with migraine headache 14, 29.
Headache with associated eye pain can be a sign of ophthalmologic and neurologic conditions, such as acute angle-closure glaucoma, scleritis, cluster headaches, and less commonly migraines 14. Cluster headaches present as severe unilateral eye pain, ptosis, ipsilateral conjunctival injection, and headache 14, 15, 8.
Systemic disease should be considered in patients with certain ocular conditions. For example, one study demonstrated that about 50% of patients with scleritis (inflammation of the sclera of the eye) had associated rheumatologic disease 25, 26. Another study showed that about 40% of patients with optic neuritis (inflammation of an optic nerve, causing blurred vision) will develop multiple sclerosis over a 10-year period 30. Although uveitis (inflammation of the uvea) is idiopathic in 60% of cases, workup for systemic inflammatory disease and infectious etiologies should be considered when uveitis is recurrent or bilateral 30, 12, 13.
Table 2. History and Physical Examination Findings Suggestive of Different Causes of Eye Pain
| Finding | Possible causes |
|---|---|
History | |
Contact lens use | Corneal abrasion, keratitis, bacterial conjunctivitis |
Decreased vision | Optic neuritis, scleritis, keratitis, uveitis, acute angle-closure glaucoma, cellulitis |
Foreign body sensation | Corneal abrasion, dry eye syndrome, keratitis, retained foreign body |
Headache | Acute angle-closure glaucoma, scleritis, cluster headache, migraine |
Photophobia | Keratitis, uveitis, corneal abrasion, migraine, acute angle-closure glaucoma |
Stabbing or boring eye pain | Scleritis, cluster headache |
Systemic inflammatory or autoimmune disease | Scleritis, uveitis, optic neuritis |
Physical examination | |
Conjunctival injection | Conjunctivitis, uveitis, scleritis, keratitis, corneal abrasion, cluster headache, acute angle-closure glaucoma |
Eyelid swelling | Hordeolum, orbital cellulitis, preseptal cellulitis |
Increased intraocular pressure | Acute angle-closure glaucoma |
Pain with extraocular movement | Optic neuritis, orbital cellulitis, scleritis, acute angle-closure glaucoma |
Positive penlight test | Uveitis, keratitis |
Positive swinging flashlight test | Optic neuritis |
Uptake of fluorescein stain | Corneal abrasion, keratitis |
[Source 6]
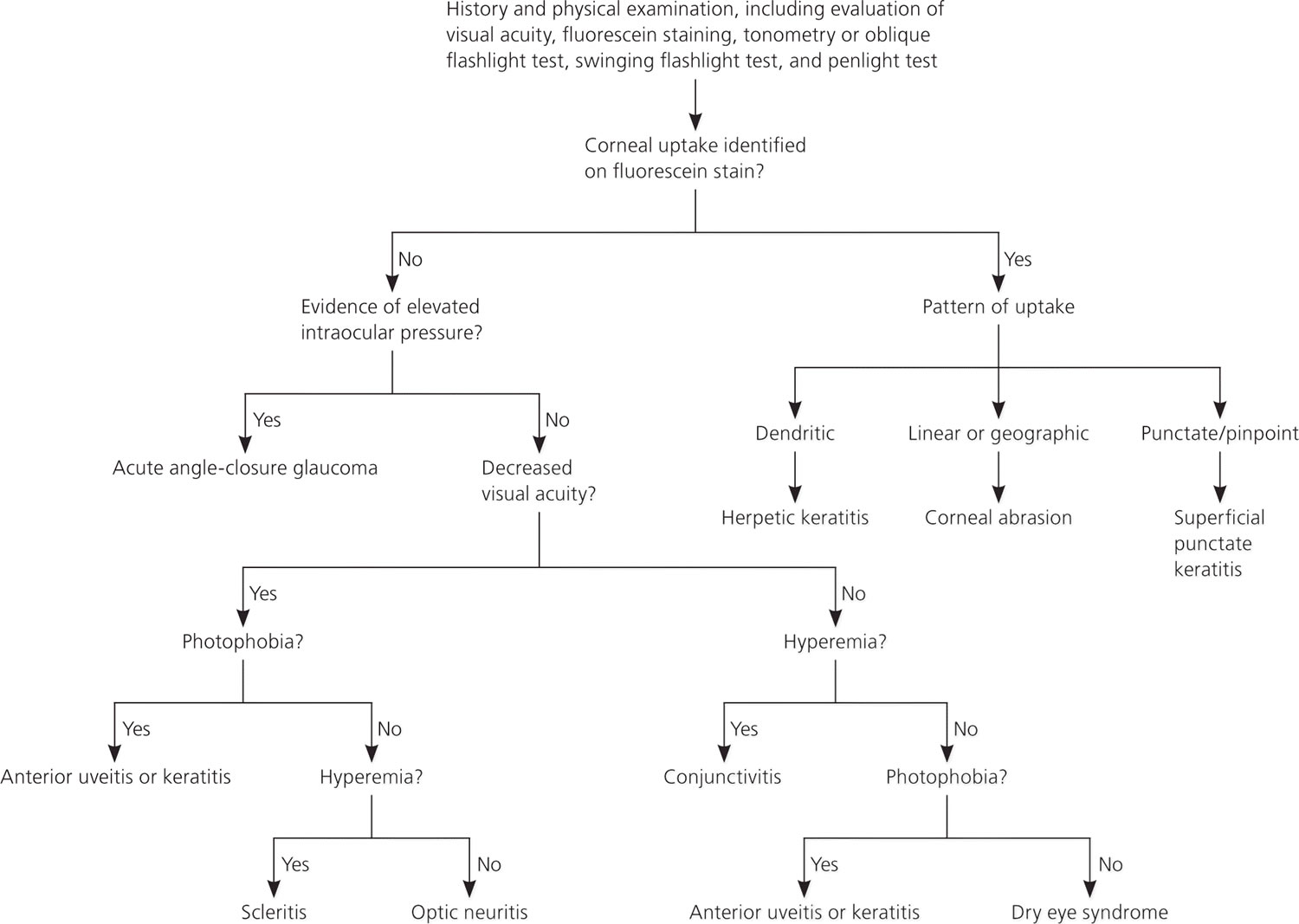
Figure 3. How to Diagnose Causes of Eye Pain
Functional Assessment
VISION
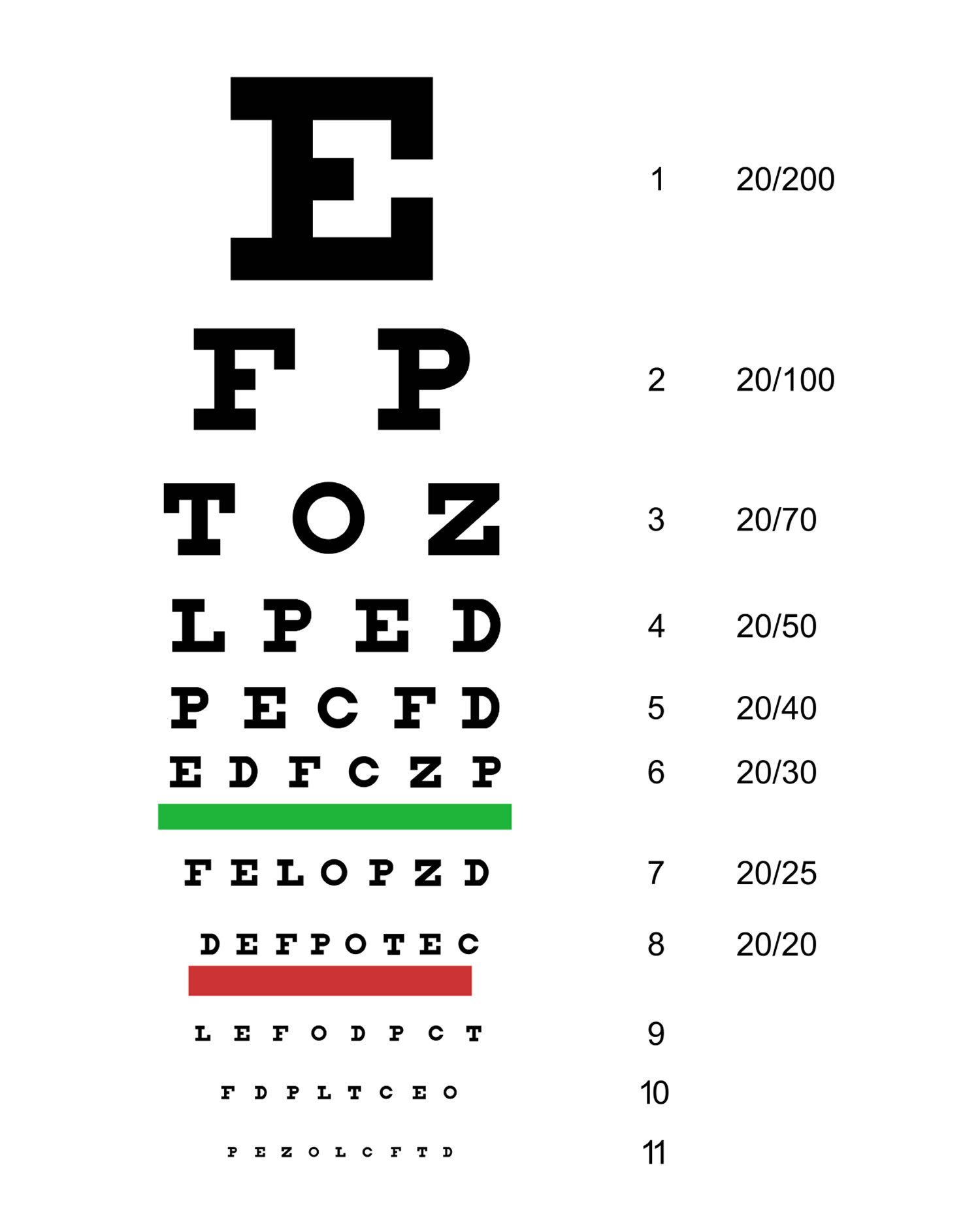
All patients presenting with eye pain should be assessed for vision loss. Having the patient read a Snellen chart (Figure 4) at a distance of 20 ft (6 m) is the standard test to evaluate visual acuity. Gross visual deficits are assessed using confrontational testing. The kinetic red test is performed by taking a 5-mm, red-topped pen and moving it inward from the boundary of each visual quadrant until the patient can see it. This test may be combined with the more common static finger wiggle test to improve sensitivity for detecting visual field loss. This combination is the most sensitive way to assess for visual field deficit in the primary care setting 31. Determining more subtle differences, such as whether vision loss is diffuse, central, or peripheral, may require ophthalmology referral for more precise testing.
Conditions that cause eye pain and can cause decreased visual acuity include:
- acute angle-closure glaucoma,
- herpes simplex virus (HSV) keratitis,
- optic neuritis, and
- orbital cellulitis.
Acute angle-closure glaucoma can cause severe central visual field defects 32; similar visual findings may occur in patients with optic neuritis, with diffuse and central loss predominant in the affected eye 33. Visual acuity of the affected eye is reduced to 20/100 in 10% of recurrent herpes simplex virus (HSV) keratitis cases 8. Most painful eye conditions causing decreased visual acuity require ophthalmology referral.
Figure 4. Snellen chart
EXTRAOCULAR MOVEMENT
To test extraocular movements, the patient should be instructed to fixate on a target with both eyes and follow it in at least four different directions. Increased intraocular pressure from acute angle-closure glaucoma may cause disordered eye motility or pain with eye movement 35. Pain associated with eye movement may also occur with scleritis, optic neuritis, and orbital cellulitis (inflammation of eye tissues behind the orbital septum).
Anatomic Assessment
EXTERNAL STRUCTURES
Clinicians should look for inflammation and erythema of the eyelids, making note of any lesions or abnormalities. A hordeolum is a tender, inflamed nodule and can be observed with careful inspection of the external or internal eyelid. The upper lid should be everted if a corneal abrasion is suspected to look for a foreign body. Orbital cellulitis presents as unilateral erythema, swelling, and ptosis of the eyelid, with associated pain with eye movement and decreased visual acuity 16.
The eyelid and surrounding region should also be inspected for rashes or vesicles. Conjunctival or eyelid vesicles occur in about one-half of patients with herpes simplex virus (HSV) keratitis 36, whereas herpes zoster ophthalmicus leads to associated pain and vesicular lesions appearing in a larger dermatome pattern on the forehead, nose, and upper eyelid (V1 distribution of the trigeminal nerve) 9, 35.
CONJUNCTIVA
The conjunctiva is a thin mucous membrane that covers the posterior eyelids (palpebral conjunctiva) and anterior sclera (bulbar conjunctiva). Injection of the conjunctiva is a result of inflammation or infection. Diffuse injection is caused by disease within the conjunctiva itself, whereas a ciliary flush sign (injection radiating outward from the limbus) is more common with a disease process in the uvea or anterior chamber, such as anterior uveitis or acute angle-closure glaucoma 37.
SCLERA
The sclera is a fibrous, protective coating of the eye. The episclera covers the sclera anteriorly and is continuous with the cornea. The sclera’s bluish discoloration helps to distinguish it and differentiate scleritis from episcleritis. Inflammation of the sclera is usually very painful, whereas inflammation of the episclera is not. Scleritis can also impair vision, and vision is unaffected with episcleritis 26. Episcleritis causes engorgement of the more superficial vessels, which are often sectoral and easily blanched with topical application of phenylephrine 12.
CORNEA
The cornea (transparent structure covering the anterior of the eye) should be evaluated with fluorescein staining. In the primary care setting, a Wood lamp or ophthalmoscope with a cobalt filter is often used for fluorescein visualization. If pain precludes evaluation, proparacaine 0.5% or other topical anesthetic should be applied first.
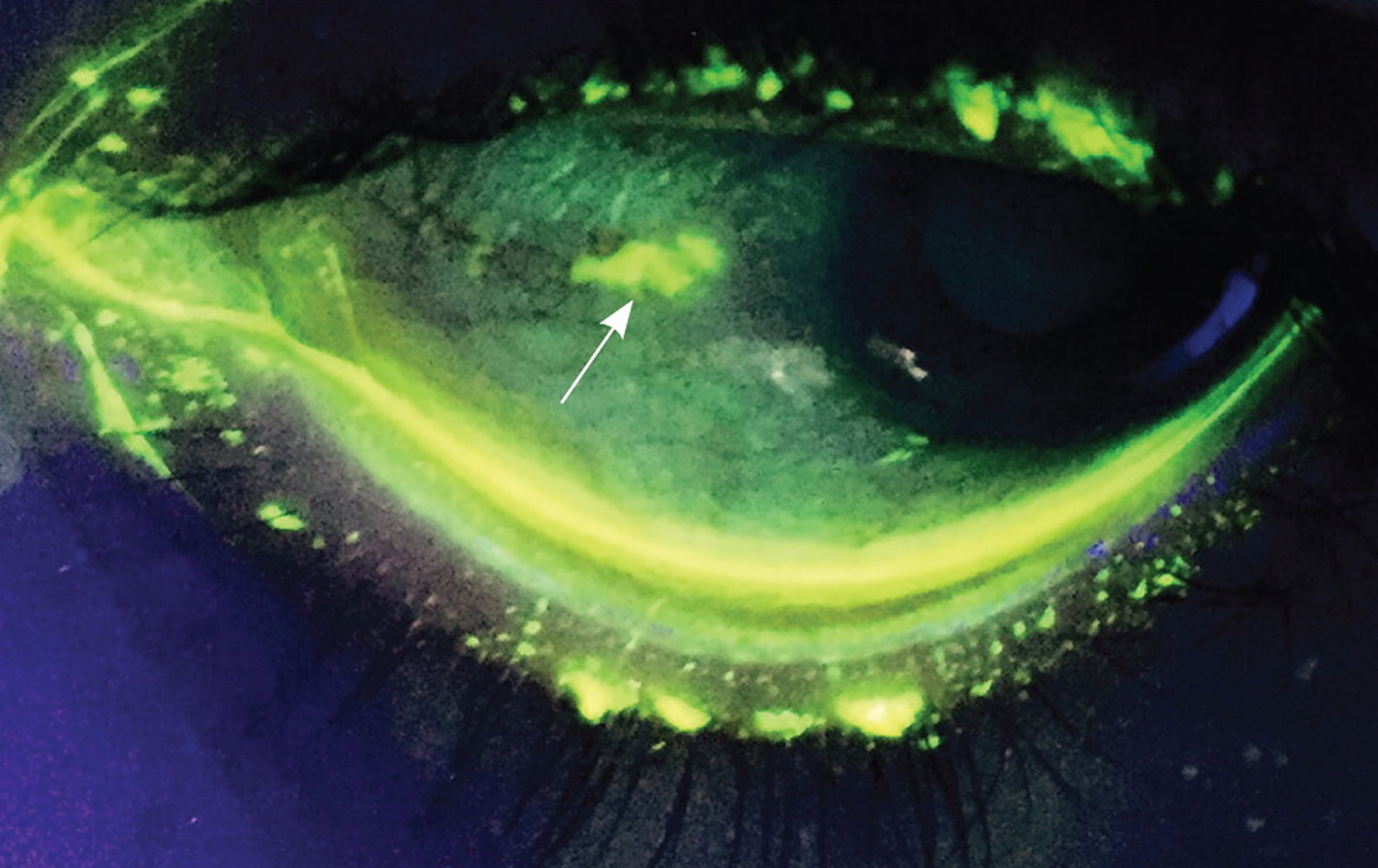
A healthy cornea is smooth, shiny, and clear. In normal light, corneal lesions appear yellow. Illumination with cobalt light or a Wood lamp causes the lesion to fluoresce green (Figure 5). An abrasion caused by trauma or a foreign body is typically linear or has a geographic shape. Abrasions from the use of contact lenses often consist of several punctate lesions that coalesce into a round central defect. Herpetic keratitis has a branching, dendritic appearance 17.
Figure 5. Increased fluorescein uptake depicting a corneal abrasion (arrow), visible under Wood lamp illumination.
PUPIL
Normal pupillary size is 2 to 4 mm. Each pupil should constrict with consensual and direct light. Anisocoria (unequal pupil size) of less than 1 mm occurs in up to 20% of the general population 38. Anisocoria associated with eye pain can be a sign of anterior uveitis. A fixed dilated pupil at 4 to 6 mm can occur with acute angle-closure glaucoma 3.
Photophobia using the penlight test can identify patients with uveitis (inflammation of the uvea) or keratitis (inflammation of the cornea of the eye) 29. This test is performed by shining a penlight directly into each eye independently from a distance of 6 in (15 cm) for two seconds to determine if there is discomfort with light. A negative result makes uveitis and keratitis unlikely (negative predictive value = 90%) 29, 39.
The swinging flashlight test is used to diagnose an afferent pupillary defect (Marcus Gunn pupil). The defect is present in a pupil that dilates when the light is swung to it from the opposite pupil (constricting more with consensual light than with direct light). A relative afferent pupillary defect in a patient presenting with eye pain can indicate optic neuritis, although a negative result does not rule it out 40, 41.
ANTERIOR CHAMBER
The anterior chamber between the cornea and iris is filled with aqueous humor. This fluid is absorbed where the cornea and iris meet at the Schlemm canal. The oblique flashlight test can be used to approximate the depth of the anterior chamber angle. The examiner shines a penlight tangentially across the cornea from the temporal side. Illumination of the entire cornea implies a wide anterior chamber angle, and a shadow over the nasal portion of the cornea implies a narrow angle 35. Acute angle-closure glaucoma is more common in persons with a narrow angle. If acute angle-closure glaucoma is suspected, tonometry should be performed. Pressures greater than 40 to 50 mm Hg are consistent with the diagnosis.
ANTERIOR UVEA
The iris and ciliary body make up the anterior uvea. Inflammation of one or both of these structures is considered anterior uveitis. Although hypopyon (white blood cells in the anterior chamber) can often be seen without magnification, a slit lamp is necessary for adequate evaluation. The hallmark of acute anterior uveitis is the presence of white blood cells floating in the aqueous humor of the anterior chamber and a cloudy appearance consistent with a proteinaceous flare. Symptoms include achy eye pain, photophobia, and blurred vision in the involved eye 37.
Imaging
There are a few indications for imaging when evaluating eye pain. Gadolinium-enhanced magnetic resonance imaging (MRI) of the brain and orbits is essential in the workup of suspected optic neuritis. In suspected orbital cellulitis, computed tomography of the orbits and paranasal passages helps confirm the diagnosis and evaluate for associated complications, such as an abscess. However, the diagnostic yield of neuroimaging is minimal in patients with unilateral eye or facial pain, normal examination findings, and no history findings suggestive of a specific diagnosis or pain syndrome 42.
What is Hyphema ?
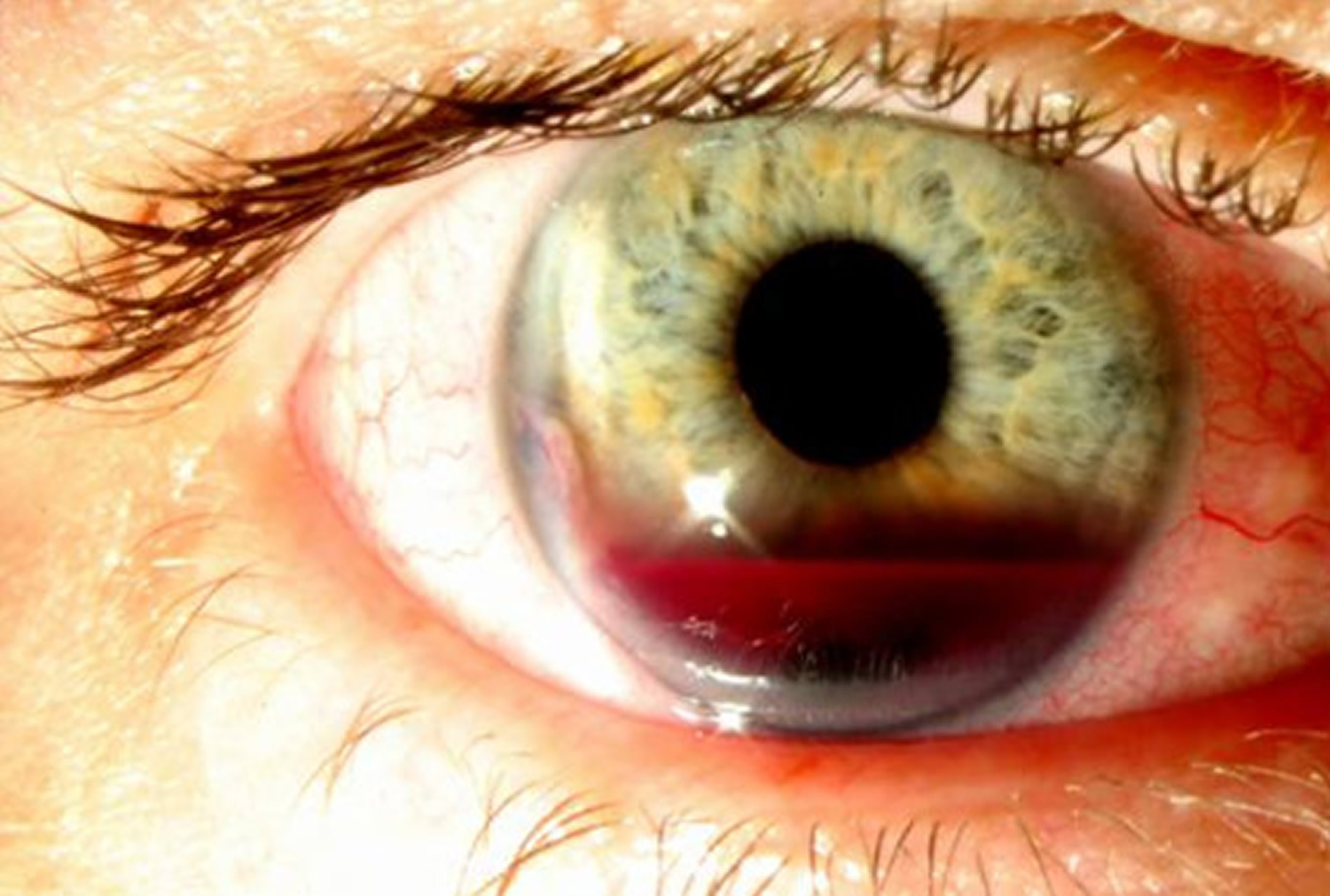
A hyphema is when blood collects inside the front of the eye. This happens between the cornea (the clear covering of the eye) and the iris (the colored part of the eye) 43. The blood may cover part or all of the iris and the pupil (the round, dark circle in the middle of your eye). If you have a hyphema, your vision might be partly or totally blocked in that eye.
A hyphema usually happens when an injury causes a tear to the iris or pupil of the eye. Sometimes people mistake a broken blood vessel in the front of the eye for a hyphema. A broken blood vessel in the eye is a common, harmless condition called subconjunctival hemorrhage. A subconjunctival hemorrhage does not hurt. A hyphema, though, is usually painful. A hyphema must be treated properly or it can cause permanent vision problems 43.
Figure 6. Hyphema
Hyphema Symptoms
Hyphema symptoms include 44:
- bleeding in the front of the eye
- being sensitive to light
- pain in the eye
- blurry, clouded or blocked vision
What Causes Hyphema ?
Hyphema is usually caused by injuries to the eye from accidents or playing sports. Hyphema can be caused by other, less common things, including 45:
- abnormal blood vessels on the surface of the iris
- eye infections caused by a herpes virus
- blood clotting problems
- problems with artificial lenses placed in the eye after cataract surgery
- very rarely, cancers of the eye
Because most hyphemas happen because of sports injuries, it is important to wear sports glasses or goggles. Sports injuries, especially with small balls like racquetballs, can cause serious eye problems. Besides hyphema, these injuries can cause cataracts, retinal detachments and glaucoma and lead to blindness. If you hurt your eye, see an ophthalmologist right away.
Hyphema Diagnosis
An ophthalmologists will examine your eye completely to diagnose a hyphema. He or she will check:
- how well you can see
- the pressure in your eye
- the inside of your eye
In some cases, the ophthalmologist may order a CT scan. This scan checks the condition of the bones that form your eye sockets and other parts of your face 46.
Hyphema Treatment
Based on what the ophthalmologist finds, he or she may ask you to 47:
- wear a special shield over your eye to protect it
- cut back on physical activity, or rest in bed
- raise the head of your bed to help your eye drain
- see your ophthalmologist often so he or she can check your healing and eye pressure
Your ophthalmologist may tell you not to use aspirin because it can lead to more bleeding. In some cases, your ophthalmologist might tell you to go to the hospital so that your eye can be cared for and checked often. If the hyphema makes your eye pressure rise too high, it can lead to glaucoma or damage your cornea. If this happens, you may need surgery to remove the excess blood or eye drops for treatment.
What Is Bacterial Keratitis ?
Bacterial keratitis is an infection of the cornea 48. The cornea is the clear, dome-shaped window of the front of your eye.
Bacterial keratitis usually develops quickly. Left untreated it can cause blindness.
There are many different bacteria that cause keratitis. The two bacteria most commonly responsible for this type of infection in the U.S. are:
- Staphylococcus aureus
- Pseudomonas aeruginosa
Symptoms of bacterial keratitis may include:
- pain in the eye (often sudden)
- reduced vision
- increased light sensitivity
- excessive tearing
- discharge from your eye
See your doctor or ophthalmologist right away if you have any of these symptoms. This is especially important if they come on suddenly. If not treated, a bacterial keratitis eye infection can lead to blindness. Treatment must start right away to prevent vision loss 48.
Causes of Bacterial Keratitis
The two main causes of bacterial keratitis are:
- contact lens use, especially extended-wear lenses
- eye injury
You risk an infection from contact lenses if you wear them too long or do not take care of them correctly. Proper care of your contacts will lower your risk of developing a keratitis infection.
Prevent Infection With Proper Contact Lens Care
Follow your eye care provider’s instructions to wear, clean and store your contacts. These are some things to keep in mind:
- Wash your hands with soap and water and dry them with a lint-free towel before handling your contacts.
- Minimize contact with water. Remove lenses before going swimming or in a hot tub.
- Do not rinse or store your contacts in water (tap or sterile water).
- Do not put your lenses in your mouth to wet them.
- Do not use saline solution and rewetting drops to disinfect lenses. Neither is an effective or approved disinfectant.
- Follow your eye care professional’s schedule for wearing and replacing your contacts.
- Use the “rub and rinse” method to clean your contacts. Rub your contact lenses with your fingers, then rinse them with solution before soaking. Use this method even if the solution you are using is a “no-rub” variety.
- Rinse the contact lens case with fresh solution — not water. Then leave the empty case open to air dry.
- Keep the contact lens case clean and replace it regularly, at least every three months. Lens cases can be a source of contamination and infection. Do not use cracked or damaged lens cases.
- Do not re-use old solution or “top off” the solution in your lens case.
- Do not transfer contact lens solution into smaller travel-size containers.
- Do not allow the tip of the solution bottle to touch any surface. Keep the bottle tightly closed when not in use.
- Never wear your lenses after storage for 30 or more days without disinfecting them again.
Bacterial Keratitis Treatment
To diagnose bacterial keratitis, your ophthalmologist will discuss your symptoms with you. They may gently scrape the eye to take a small sample and test it for infection.
Bacterial keratitis is usually treated with antibiotic drops. Drops are usually put in frequently. Treatment may also involve steroid drops. You may need to return to your ophthalmologist several times.
If you and your ophthalmologist find and treat bacterial keratitis early, you may preserve your vision. In severe cases decreased vision or blindness may be the result. This is also true if the infection affects the center of the cornea. Sometimes a cornea transplant is needed to restore vision.
What is Eye Cellulitis ?
Cellulitis is an infection that can affect the skin and/or the eyes 49.
There are two types of cellulitis that affect the eyes:
- preseptal
- orbital
Preseptal cellulitis only affects eyelid tissue. This type of cellulitis usually happens in children, especially young children.
Orbital cellulitis affects the eye socket (called the orbit). This form of cellulitis can cause the eye or eyelid to swell, keeping the eye from moving properly.
Orbital cellulitis is a serious condition 49. It often needs to be treated more aggressively than preseptal cellulitis.
Figure 7. Orbital cellulitis

Causes and Symptoms of Eye Cellulitis
Cellulitis is often caused by an infection from bacteria. It can also be caused by a fungal infection.
Other problems that can lead to cellulitis include 50:
- insect bites
- a skin wound (especially on the face)
- dental surgery or other surgery of the head and neck
- sinus infection
- asthma
An infection can start in the sinuses, then spread to the orbit or eyelid. Because sinus infections are more common in cold weather, cellulitis occurs more in the winter.
It is important to clean any wounds carefully. You also need to follow your doctor or dentist’s instructions for caring for yourself after surgery.
- Cellulitis is serious because the infection spreads quickly. That is why it must be treated right away.
If you think you or your child have cellulitis, see a doctor right away. If it is not treated immediately, cellulitis can cause vision loss or even spread throughout your body.
It appears that as more people are getting flu vaccinations, fewer people are getting cellulitis–especially pre-septal cellulitis.
What are symptoms of cellulitis ?
Cellulitis symptoms include:
- bulging eye
- swelling of the eyelid or tissue around the eye
- red eyelids
- problems moving your eye
- blurry vision or double vision
- fever
- feeling as if you do not have much energy
- problems seeing well
Cellulitis Diagnosis
To see if you have cellulitis, your doctor will ask if you have had any recent surgery or dental work. They will also ask if you have had recent face or skin wounds, and chest, lung or sinus infections 51.
Your doctor will also examine your eyes.
To diagnose the type of infection you have, your doctor will probably do some tests. If they think you might have preseptal cellulitis, they may test tissue from your nose or eye. If they suspect orbital cellulitis, they may do a blood test.
In some cases, your doctor may also have you get a scan of the affected area. These images will help your doctor see where the infection is within the orbit.
Cellulitis Treatment
In most cases, your doctor will have you take an antibiotic medicine to treat your cellulitis.
With pre-septal cellulitis, you should start to notice the infection getting better in about a day or two while taking antibiotics 52.
Because it is more serious, orbital cellulitis may not improve with (oral) antibiotics 52. If that happens, you may need to stay in the hospital to be treated. They will give you special antibiotics continuously through a vein in your body 52.
In some cases, your doctor may need to drain fluid from the infected area. Sometimes this can be performed in your doctor’s office. Other times, it may mean having surgery in a hospital or outpatient clinic.
Your doctor will explain the cellulitis treatment chosen for you. If you have any questions, be sure to ask. Your ophthalmologist is committed to protecting your sight.
What is Conjunctivitis (Pink Eye) ?
Conjunctivitis is often called “pink eye” 53. It happens when the conjunctiva is irritated by an infection or allergies. Your eyes are red and swollen (inflamed), and sometimes they have a sticky discharge. You can have conjunctivitis in one or both eyes. Some types of pink eye are very contagious (easily spread from person to person).
There are four main types of conjunctivitis.
- Viral conjunctivitis is the most common type of pink eye. This conjunctivitis is very contagious and often spreads through schools and other crowded places. It usually causes burning, red eyes with a watery discharge.
- Bacterial conjunctivitis is also very contagious. An infection from bacteria causes this form of pink eye. With bacterial conjunctivitis, you have sore, red eyes with a lot of sticky pus.
- Allergic conjunctivitis is a type of pink eye that comes from an allergic reaction to something. It is not contagious. Allergic pink eye makes your eyes very itchy, red and watery.
- Irritants such as contact lenses and lens solutions, chlorine in a swimming pool, smog or cosmetics may also be an underlying cause of conjunctivitis.
Figure 8. Conjunctivitis (pink eye)

Causes of Pink Eye (Conjunctivitis)
Conjunctivitis is most commonly caused by the same virus that causes the runny nose and sore throat of the common cold.
Bacterial infections cause conjunctivitis that produces lots of sticky pus in the eye. Some bacterial infections, however, may cause little or no discharge. Sometimes the bacteria that cause pink eye are the same that cause strep throat. Both bacterial and viral conjunctivitis are easily spread from person to person.
Sometimes having an allergic reaction to pollen or animals can cause conjunctivitis. So can irritation from cigarette smoke, car fumes, pool chlorine or other toxic substances. The main symptom of allergic pink eye is itchy eyes. Other symptoms include red, burning and tearing eyes and puffy eyelids. Allergic or irritant conjunctivitis is not contagious.
Pink Eye Symptoms
Pink eye symptoms may include 54:
- the feeling that something is in your eye, or a gritty sensation in your eye
- red eyes
- burning eyes
- itchy eyes
- painful eyes (this is usually with the bacterial form)
- watery eyes
- puffy eyelids
- blurry or hazy vision
- being extra sensitive to light
- lots of mucus, pus, or thick yellow discharge from your eye. There can be so much that your eyelashes stick together (usually with bacterial conjunctivitis).
Pink Eye Treatment
Treating your pink eye usually depends on the type of conjunctivitis you have.
If your conjunctivitis is caused by a viral infection, there are no specific treatments 55. Your body fights the virus on its own. Placing a cool, wet washcloth on your eyes can help make them feel more comfortable.
If your pink eye is caused by a bacterial infection, your ophthalmologist may prescribe antibiotic eye drops 55. Antibiotics do not treat an infection caused by a virus or by allergy 55.
If your conjunctivitis is due to allergies, you might be told to use certain eye drops to help with the itchiness and puffiness.
Sometimes conjunctivitis can be caused by a chemical or other substance in your eye. In this case, rinse the eye free of the substance. You might be told to use certain eye drops or ointment for the eyes.
Stop pink eye from spreading
Some conjunctivitis can spread from person to person 55. Follow these tips so you will not infect other people or re-infect yourself.
- Use a clean towel or tissue each time you wipe your face and eyes.
- Wash your hands very often. Always wash them before and after you eat, when you go to the bathroom, or after you sneeze or cough.
- Try not to touch your eyes. If you do, wash your hands right away.
- Bacteria can live in makeup. This can cause pink eye and even a dangerous infection of the cornea. Do not use eye makeup while your eyes are infected.
- Replace your makeup if you have an eye infection. And never share eye makeup with others.
- Make sure to clean your contact lenses exactly as your ophthalmologist recommends.
- If you have conjunctivitis, wash any discharge from around the eyes several times a day.
- Do not use the same eye drop dispenser/bottle for infected and non-infected eyes—even for the same person.
- Avoid sharing articles like towels, blankets, and pillowcases.
- Clean your eyeglasses.
- Clean, store, and replace your contact lenses as instructed by your eye health professional.
- Do not share eye makeup, face makeup, makeup brushes, contact lenses or containers, or eyeglasses.
- Avoid touching or rubbing your eyes.
Conjunctivitis usually goes away on its own within 1–2 weeks. If your symptoms last longer than that, you should see your ophthalmologist. He or she can make sure you don’t have a more serious eye problem.
What is Fungal Keratitis ?
Fungal keratitis is an infection of the cornea 56. Fungal keratitis can develop quickly from an eye injury or contact lens use. It can cause blindness if it is not treated 56. In some cases, treatment cannot restore vision 56. In these cases, permanent vision impairment or blindness may occur.
There are many different fungi that can infect the cornea such as Fusarium, Aspergillus or Candida.
Keratitis. Keratitis is an infection or inflammation of the cornea.
Superficial keratitis involves the outer layers of the cornea. After this form of keratitis heals, there is usually no scar on the cornea.
Deep keratitis affects deeper layers of the cornea. There can be a scar on the cornea after it heals, which may or may not affect your vision. This will depend on the location of the scar.
Besides fungal keratitis, other types of keratitis include 56:
- Amoebic keratitis, which is an infection with amoeba. It is often caused by Acanthamoeba and usually affects contact lens wearers.
- Bacterial keratitis, which is an infection with bacteria
- Herpes keratitis, which is an infection with herpes simplex or herpes zoster viruses
- Photokeratitis, due to intense ultraviolet (UV) radiation exposure. Examples include snow blindness or welder’s arc eye.
Fungal Keratitis Causes
Fusaria are common fungi found in soil, water, and plants throughout the world 57. They are particularly common in warmer climates. Fungal keratitis can happen after an injury to the cornea involving plant material. One example is getting hit in the eye with a palm branch.
People who have a low immune response can also get fungal keratitis if they come in contact with the fungus. There is also a risk of developing fungal keratitis with contact lens use. Proper use and care of contact lenses can reduce your risk of getting a fungal infection if you wear contacts. Ask your ophthalmologist about proper contact lens care.
Fungal Keratitis Symptoms
Symptoms of fungal keratitis may include 58:
- reduced vision
- pain in the eye (often sudden)
- increased light sensitivity
- tearing
- excessive tearing or discharge from your eye
See your ophthalmologist right away if you experience any of these symptoms. This is especially important if these symptoms come on suddenly. You must start treatment right away to prevent possible blindness.
Fungal Keratitis Treatment
Your ophthalmologist may gently scrape the eye to take a small sample of material. They will test the sample for infection. This test will help diagnose whether your infection is fungal keratitis or bacterial keratitis 59.
Treatment of fungal keratitis usually includes antifungal eye drops and oral medications. If these medicines are not effective, you may need surgery, including corneal transplantation. In some cases, even corneal surgery will not restore vision. In these cases, permanent vision impairment or blindness may occur. That is why it is so important to see your ophthalmologist at the first sign of any ocular infection.
What is Herpes Keratitis ?
Herpes keratitis is a viral infection of the eye caused by the herpes simplex virus (HSV). There are two major types of the virus 60:
- Type I is the most common and primarily infects the face, causing the familiar “cold sore” or “fever blister.”
- Type II is the sexually transmitted form of herpes, infecting the genitals.
While both Type I and Type II herpes can spread to the eye and cause infection, Type I is by far the most frequent cause of eye infections. Infection can be transferred to the eye by touching an active lesion (a cold sore or blister) and then your eye.
Herpes Keratitis Causes
Type I herpes is very contagious and is commonly transmitted by skin contact with someone who has the virus 61. Almost everyone — about 90 percent of the population — is exposed to Type I herpes, usually during childhood Herpes Keratitis Causes. https://www.aao.org/eye-health/diseases/herpes-keratitis-cause.
After the original infection, the virus lies in a dormant state, living in nerve cells of the skin or eye. Reactivation can be triggered in a number of ways, including:
- stress
- sun exposure
- fever
- trauma to the body (such as injury or surgery)
- menstruation
- certain medications
Once herpes simplex is present in the eye, it typically infects the eyelids, conjunctiva and cornea 61. It may also infect the inside of the eye; however, this is much less common.
Herpes Keratitis Symptoms
The symptoms of herpes keratitis may include pain, redness, blurred vision, tearing, discharge and sensitivity to light 62.
If the infection is superficial, involving only the cornea’s outer layer (called the epithelium), it will usually heal without scarring. However, it if involves the deeper layers of cornea (which can happen after time), the infection may lead to scarring of the cornea, loss of vision and sometimes even blindness.
Left untreated, herpes keratitis can severely damage your eye.
Herpes Keratitis Treatment
Treatment of herpes keratitis depends on its severity 63. Mild infection is typically treated with topical and sometimes oral antiviral medication 63. Your ophthalmologist may gently scrape the affected area of the cornea to remove the diseased cells. In case of severe scarring and vision loss, a corneal transplant may be required.
It is very important to consult an ophthalmologist before beginning any treatment, because some medications or eyedrops may actually make the infection worse 63.
There is no complete cure for herpes; once the virus is in the body, you cannot get rid of it 63. However, if you develop herpes keratitis, there are some things you can do to help prevent recurring outbreaks:
- If you have an active cold sore or blister, avoid touching your eyes.
- Steroids can increase the herpes virus in the body. You should not use steroid eye drops unless you are taking an anti-viral medicine as well.
- Stop wearing contact lenses if you keep getting infections.
- See an ophthalmologist immediately if symptoms of ocular herpes return.
What is Corneal Abrasion ?
Corneal abrasion is a scratch or scrape on the cornea, the clear, round dome covering the eye’s iris and pupil 64. By helping to focus light as it enters the eye, the cornea plays an important role in vision. When a corneal abrasion scars the cornea, it can affect vision.
Corneal abrasions can often be prevented by using protective eyewear when performing activities that put your eyes at risk of injury.
What Causes Corneal Abrasion ?
Small children are a common source of corneal abrasions because they can accidentally poke the eyes of whoever is holding them 65. In some cases, the immediate cause of a corneal abrasion may not be apparent, as symptoms may occur hours after the injury to the cornea.
There are a variety of causes of corneal abrasions. These include:
- Something hitting or blowing into the eye, such as plant matter, sawdust, or ash;
- Foreign matter, such as dust, dirt or sand, getting stuck under your eyelid;
- Sports injuries;
- Improperly fitted or maintained contact lenses;
- Something poking you in the eye;
- Rubbing your eyes vigorously, especially if you feel something is caught in your eye;
- Certain eye conditions, including trachoma, a bacterial infection;
- Undergoing surgery under general anesthesia.
Corneal Abrasion Symptoms
If you suffer a corneal abrasion, you may experience the following symptoms 66:
- Pain, which may feel worse when you open or close your eye
- A feeling that there is something in your eye
- Tearing
- Redness
- Sensitivity to light
- Blurred vision or loss of vision
- Headache
- Sometimes you may not be aware you have suffered a corneal abrasion or how it happened, as symptoms may occur hours after the injury.
If something flies in your eye, you can try to flush it out with tap water. However, it is important that you do not rub your eye, as that may only worsen the abrasion.
Corneal Abrasion Diagnosis
If you have any of the symptoms of a corneal abrasion, you should seek care from your doctor or an ophthalmologist. He or she will perform a thorough eye examination. During the examination, your doctor may put numbing drops in your eye so that it can stay open for the examination.
To accurately diagnose a corneal abrasion, your doctor may perform a fluorescein eye stain. This is a test that uses orange dye (fluorescein) and a blue light to detect damage to the cornea.
Corneal Abrasion Treatment
A minor corneal abrasion will heal on its own in a few days 67. Your doctor may put antibiotic eye drops or ointment in your eyes or use steroid eyedrops to reduce inflammation and reduce the chance of scarring 67.
If you have a corneal abrasion, your ophthalmologist may patch your eye so that you are more comfortable. You may also be given medication to reduce the pain. Wearing sunglasses may also lessen the symptoms of corneal abrasion while you are healing.
If you wear contact lenses, you should not wear them until your dcotor says that it is safe to do so 67.
What Is Corneal Laceration ?
A corneal laceration is a cut on the cornea 68. It is usually caused by something sharp flying into the eye. It can also be caused by something striking the eye with significant force, like a metallic hand tool. A corneal laceration is deeper than a corneal abrasion, cutting partially or fully through the cornea. If the corneal laceration is deep enough it can cause a full thickness laceration. This is when the laceration cuts completely through the cornea and causes a ruptured globe, a tear in the outer surface of the eyeball itself.
- A corneal laceration is a very serious injury and requires immediate medical attention to avoid severe vision loss 68.
If your eye has been injured, you should do the following:
- gently place a shield over the eye to protect it. Cut away the bottom part of a paper cup and tape this piece to the area around the eye. Wear this to protect your eye until you get medical help.
- do not rinse with water
- do not remove the object stuck in eye
- do not rub or apply pressure to eye
- avoid giving aspirin, ibuprofen or other non-steroidal, anti-inflammatory drugs. These drugs thin the blood and may increase bleeding
- after you have finished protecting the eye, see a physician immediately.
Corneal Laceration Symptoms
Corneal laceration symptoms may include 69:
- severe pain
- tearing
- sensitivity to light
- blurred or decreased vision
- bleeding (blood in the eye)
- the feeling that there is something in the eye
What Causes Corneal Laceration ?
Any activity in which objects can fly into the eye at high speed can cause a corneal laceration 70. The most common causes of a corneal laceration are such activities as:
- cutting wood
- grinding metal
- trimming grass
- carving stone
Contact with dust, dirt, sand, or even an edge of a piece of paper can possibly cut the cornea if enough force is involved.
Most corneal lacerations can be prevented by using protective eye wear during high-risk activities.
Corneal Laceration Diagnosis
If you have any corneal laceration symptoms, you should see an ophthalmologist immediately 71. He or she will perform a complete eye examination to determine the extent of the injury. Your ophthalmologist will seek to learn whether the cut is a partial thickness or full thickness laceration.
To examine your corneal laceration, your ophthalmologist may put numbing drops in your eye so that it can stay open for the exam. He or she may also perform a fluorescein eye stain. This is a test that uses orange dye (fluorescein) and a blue light to detect damage to the cornea.
Corneal Laceration Treatment
Surgery is usually done to close the corneal laceration 72. Surgery helps:
- prevent further damage to the eye
- remove any foreign object remaining in the eye after the injury
Severe lacerations may need several surgeries for repair and can result in permanent vision loss 72.
Following surgery, your eye may be patched to protect it. Also, your ophthalmologist may give you medications. These can include medication for pain and to help you to heal.
If you have a corneal laceration, you may be at risk for complications, including retinal detachment, infection and glaucoma 72. It is important that you follow up with your ophthalmologist for care after your immediate treatment.
What is a Corneal Ulcer ?
A corneal ulcer is an open sore on the cornea 73. The cornea covers the iris and the round pupil, much like a watch crystal covers the face of a watch. A corneal ulcer usually results from an eye infection, but severe dry eye or other eye disorders can cause it.
Corneal Ulcer Symptoms
Symptoms of corneal ulcers include 74:
- redness of the eye
- severe pain and soreness of the eye
- the feeling of having something in your eye
- tearing
- pus or other discharge
- blurred vision
- sensitivity to light
- swelling of the eyelids
- a white spot on your cornea that you may or may not be able to see when looking in the mirror
See your ophthalmologist immediately if you think you have a corneal ulcer or have any eye symptoms that concern you. Corneal ulcers can badly and permanently damage your vision and even cause blindness if they are not treated 74.
Who is At Risk for Corneal Ulcers ?
People at risk for corneal ulcers include 75:
- contact lens wearers
- people who have or have had cold sores, chicken pox or shingles
- people who use steroid eye drops
- people with dry eye
- people with eyelid disorders that prevent proper functioning of the eyelid
- people who injure or burn their cornea
If you wear contact lenses, safe handling, storage and cleaning of your lenses are key steps to reduce your risk of a corneal ulcer. It is important to learn how to take care of your contact lenses.
What Causes Corneal Ulcers ?
You can prevent many causes of corneal ulcers. Use the correct protective eyewear when doing any work or play that can lead to eye injury. And if you wear contact lenses, it is important to care for your contact lenses correctly.
Corneal ulcers are usually caused by the following types of infections 76:
Bacterial infections. These are common in contact lens wearers, especially in people using extended-wear lenses.
Viral infections. The virus that causes cold sores (the herpes simplex virus) may cause recurring attacks. These attacks are triggered by stress, an impaired immune system, or exposure to sunlight. Also, the virus that causes chicken pox and shingles (the varicella virus) can cause corneal ulcers.
Fungal infections. Improper use of contact lenses or steroid eye drops can lead to fungal infections, which in turn can cause corneal ulcers. Also, a corneal injury that results in plant material getting into the eye can lead to fungal keratitis.
Parasitic (Acanthamoeba) infections. Acanthamoeba are microscopic, single-celled amoeba that can cause human infection. They are the most common amoebae in fresh water and soil 76. When Acanthamoeba enters the eye it can cause a bad infection, particularly for contact lens users 76.
Other causes of corneal ulcers include 76:
- Abrasions or burns to the cornea caused by injury to the eye. Scratches, scrapes and cuts can become infected by bacteria and lead to corneal ulcers. These injuries can happen from fingernail scratches, paper cuts, makeup brushes and tree branches. Burns caused by corrosive chemicals found in the workplace and at home can cause corneal ulcers.
- Dry eye syndrome. If your eyes do not produce enough tears, it is called dry eye. Dry eye is also when your eyes do not make the right type of tears.
- Bell’s palsy and other eyelid disorders that prevent proper eyelid function. If the eyelid does not function properly, the cornea can dry out, and an ulcer can develop. Bell’s palsy is a nerve problem that affects the muscles of your face. It causes weakness or partial paralysis of the muscles on one side of your face 77. With Bell’s palsy, your eyelid may not close properly and your smile may seem uneven. Bell’s palsy usually affects adults only. It is more likely to happen to people who have diabetes, are pregnant, or have a family history of Bell’s palsy.
Corneal Ulcer Diagnosis
Your ophthalmologist will use a special dye called fluorescein to light up any damage to your cornea 78. They will then examine your cornea using a special microscope called a slit lamp. The slit-lamp exam will allow your ophthalmologist to see the damage to your cornea and determine if you have a corneal ulcer.
If your ophthalmologist thinks that an infection has caused your corneal ulcer, they may take a tiny tissue sample. Examination of this sample helps identify and properly treat the infection.
Corneal Ulcer Treatment
Antibiotic, antifungal or antiviral eye drops are the treatments of choice 79. Sometimes your ophthalmologist will prescribe antifungal tablets. In other cases, they will treat you with an injection of medication near the eye.
Your ophthalmologist may prescribe steroid or anti-inflammatory eye drops after your infection has improved or is gone. This should reduce swelling and help prevent scarring. Steroid eye drop use is controversial for corneal ulcer. You should only use them under close supervision by your ophthalmologist. It is possible that steroid eye drops may worsen an infection.
Your ophthalmologist may prescribe pain medication to take by mouth to reduce pain.
If your symptoms suddenly change or get worse during treatment, then let your ophthalmologist know right away.
Symptoms to look for include:
- pain and redness of the eye
- tearing and discharge from the eye
- blurry vision
Surgical treatment. A corneal transplant can replace your damaged cornea with a healthy donor cornea to restore vision 79. When the infection is gone and the ulcer is healed after treatment with medication, sometimes a significant scar remains. In this case, a transplant may be done to improve vision. And if corneal ulcers cannot be treated with medication, you may also need corneal transplant surgery to keep your vision.
What is Fuchs’ Dystrophy ?
Fuchs’ dystrophy is a disease of the cornea. It is when cells in the corneal layer called the endothelium die off 80. These cells normally pump fluid from the cornea to keep it clear 80. When they die, fluid builds up and the cornea gets swollen and puffy. Vision becomes cloudy or hazy.
Fuchs’ dystrophy has two stages.
In the early stage (stage 1), you may notice few, if any, problems. Vision is usually hazy in the morning but gets better throughout the day 80. This is because your eyes normally stay moist when they are closed during sleep. But when you are awake, the fluid dries normally.
With the later stage 2, vision remains blurry all day 80. Too much fluid builds up during sleep and not enough dries up during the day. Also, tiny blisters may form in the cornea. The blisters get bigger and eventually break open, causing eye pain.
People in their 30s and 40s may have Fuchs’ dystrophy but not know it 80. Vision problems might not appear until age 50 or later. Women are more likely than men to have Fuchs’ dystrophy.
Fuchs’ Dystrophy Symptoms
In the early stage (stage 1), you may notice few, if any, symptoms. Your vision may be hazy or blurry when you first wake up, but improve throughout the day.
In the later stage (stage 2), your blurry or hazy vision will not get better as the day goes on. Here are other symptoms 81:
- Sandy or gritty feeling in your eyes
- Eye pain from the tiny blisters in the cell layer of the cornea
- Being extra sensitive to bright light
- Eye problems get worse in humid areas
- Very blurry or hazy vision from scarring at the center of the cornea.
Fuchs’ Dystrophy Diagnosis
Your ophthalmologist will look closely at your cornea and measure its thickness 82. This is called pachymetry. They will also check for tiny blisters. Using a special photograph of your cornea, your ophthalmologist may count the cells in your endothelium.
Fuchs’ Dystrophy Treatment
There is no cure for Fuchs’ dystrophy 83. However, you can control vision problems from corneal swelling. Your treatment depends on how Fuchs’ dystrophy affects your eye’s cells.
Here are treatments for early Fuchs’ dystrophy:
- Use an eyedrop medicine or ointment to reduce swelling of the cornea’s cells.
- Use a hair dryer, held at arm’s length, to blow warm air on your face. This helps dry the surface of your cornea.
For very poor vision or scarred corneas, you may need a cornea transplant. This surgery could be one of two types:
- Endothelial keratoplasty (EK): Healthy endothelial cells are transplanted into your cornea.
- Full corneal transplant: The center of your cornea is replaced with a healthy donor cornea.
Your ophthalmologist will discuss what treatments are best for your condition.
What Is Glaucoma ?
Glaucoma is a group of diseases that can damage the eye’s optic nerve and result in vision loss and blindness 84. It usually happens when fluid builds up in the front part of your eye. That extra fluid increases the pressure in your eye, damaging the optic nerve. Open-angle glaucoma, is the most common form of the disease.
Glaucoma is a leading cause of blindness for people over 60 years old 85. But blindness from glaucoma can often be prevented with early treatment.
Types of glaucoma
There are two major types of glaucoma.
1)Primary open-angle glaucoma
This is the most common type of glaucoma 85. It happens gradually, where the eye does not drain fluid as well as it should (like a clogged drain). As a result, eye pressure builds and starts to damage the optic nerve. This type of glaucoma is painless and causes no vision changes at first.
Some people can have optic nerves that are sensitive to normal eye pressure. This means their risk of getting glaucoma is higher than normal. Regular eye exams are important to find early signs of damage to their optic nerve.
2) Angle-closure glaucoma (also called “closed-angle glaucoma” or “narrow-angle glaucoma”)
This type happens when someone’s iris is very close to the drainage angle in their eye. The iris can end up blocking the drainage angle 85. You can think of it like a piece of paper sliding over a sink drain.
- When the drainage angle gets completely blocked, eye pressure rises very quickly. This is called an acute attack. It is a true eye emergency, and you should call your ophthalmologist right away or you might go blind 85.
Here are the signs of an acute angle-closure glaucoma attack 85:
- Your vision is suddenly blurry
- You have severe eye pain
- You have a headache
- You feel sick to your stomach (nausea)
- You throw up (vomit)
- You see rainbow-colored rings or halos around lights
Many people with angle-closure glaucoma develop it slowly 85. This is called chronic angle-closure glaucoma. There are no symptoms at first, so they don’t know they have it until the damage is severe or they have an attack.
Angle-closure glaucoma can cause blindness if not treated right away 85.
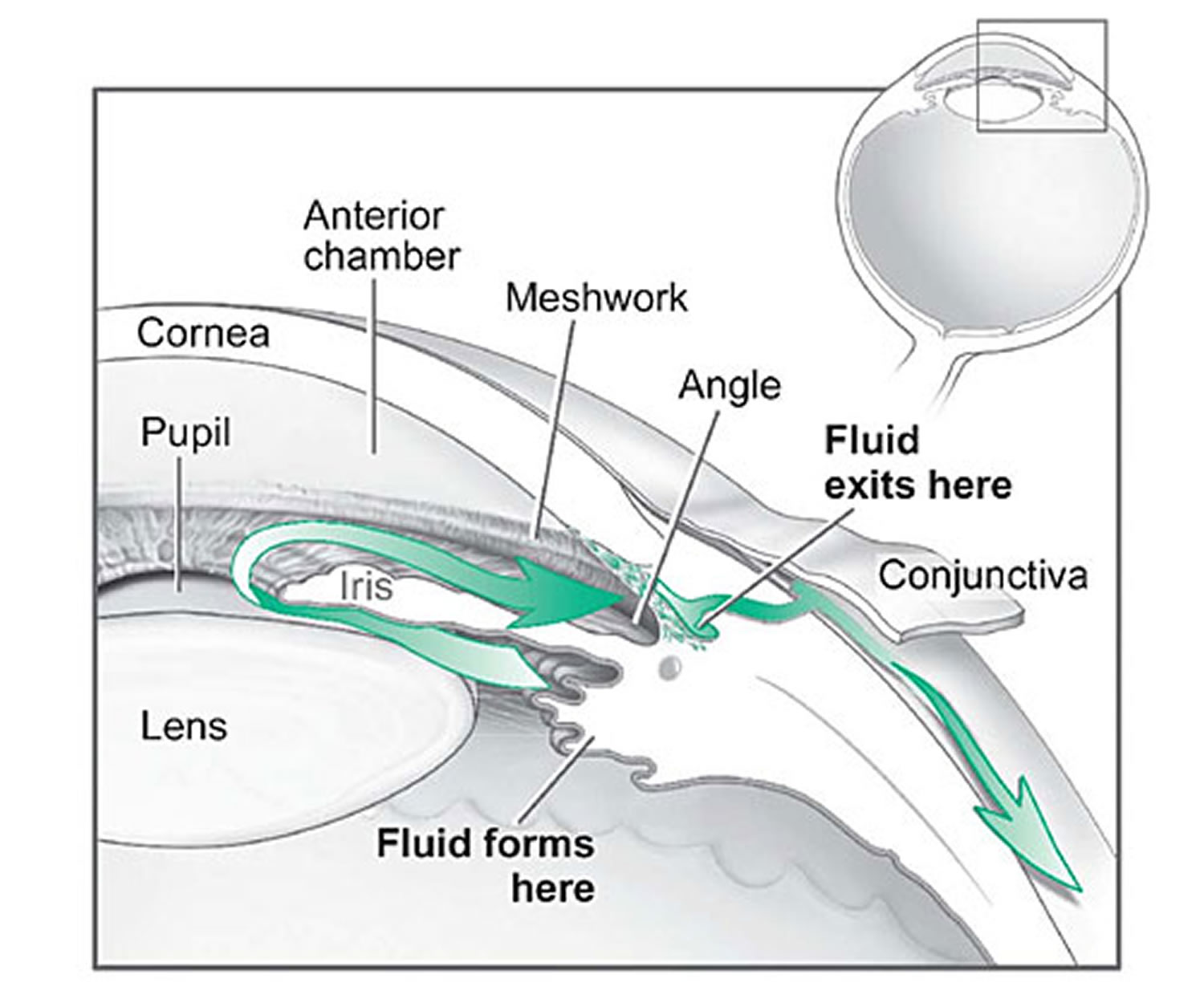
Figure 9. Flow and absorption of fluid in the front of the eye
What Are the Symptoms of Glaucoma ?
How does glaucoma affect your vision ?
The optic nerve is made up of many nerve fibers that carry images to the brain. It’s like an electric cable containing numerous wires. When glaucoma damages the optic nerve fibers, blind spots develop. If the entire nerve is destroyed, blindness results.
As the optic nerve becomes more damaged, blank spots begin to appear in your field of vision. You typically won’t notice these blank spots in your day-to-day activities until the optic nerve is significantly damaged and these spots become large.
Open-angle glaucoma
With open-angle glaucoma, there are no warning signs or obvious symptoms in the early stages. As the disease progresses, blind spots develop in your peripheral (side) vision 86.
Most people with open-angle glaucoma do not notice any change in their vision until the damage is quite severe 86. This is why glaucoma is called the “silent thief of sight.” Having regular eye exams can help your ophthalmologist find this disease before you lose vision. Your ophthalmologist can tell you how often you should be examined.
Angle-closure glaucoma
People at risk for angle-closure glaucoma usually show no symptoms before an attack. Some early symptoms of an attack may include blurred vision, halos, mild headaches or eye pain 86. People with these symptoms should be checked by their ophthalmologist as soon as possible. An attack of angle-closure glaucoma includes the following:
- severe pain in the eye or forehead
- redness of the eye
- decreased vision or blurred vision
- seeing rainbows or halos
- headache
- nausea
- vomiting
Normal tension glaucoma
People with “normal tension glaucoma” have eye pressure that is within normal ranges, but show signs of glaucoma, such as blind spots in their field of vision and optic nerve damage 86.
Glaucoma suspects
Some people have no signs of damage but have higher than normal eye pressure (called ocular hypertension) 86. These patients are considered “glaucoma suspects” and have a higher risk of eventually developing glaucoma. They should be carefully monitored by an ophthalmologist.
Causes of Glaucoma
Your eye constantly makes aqueous humor. As new aqueous flows into your eye, the same amount should drain out. The fluid drains out through an area called the drainage angle. This process keeps pressure in the eye (called intraocular pressure or IOP) stable. But if the drainage angle is not working properly, fluid builds up. Pressure inside the eye rises, damaging the optic nerve 87.
The optic nerve is made of more than a million tiny nerve fibers. It is like an electric cable made up of many small wires. As these nerve fibers die, you will develop blind spots in your vision. You may not notice these blind spots until most of your optic nerve fibers have died. If all of the fibers die, you will become blind.
Who is at Risk for Glaucoma ?
Some people have a higher than normal risk of getting glaucoma. This includes people who 88:
- are over age 40
- have family members with glaucoma
- are of African or Hispanic heritage
- have high eye pressure
- are farsighted or nearsighted
- have had an eye injury
- have corneas that are thin in the center
- have thinning of the optic nerve
- have diabetes, migraines, poor blood circulation or other health problems affecting the whole body
Talk with an ophthalmologist about your risk for getting glaucoma. People with more than one of these risk factors have an even higher risk of glaucoma.
Glaucoma Diagnosis
The only sure way to diagnose glaucoma is with a complete eye exam. A glaucoma screening that only checks eye pressure is not enough to find glaucoma 89.
During a glaucoma exam, your ophthalmologist will:
- measure your eye pressure
- inspect your eye’s drainage angle
- examine your optic nerve for damage
- test your peripheral (side) vision
- take a picture or computer measurement of your optic nerve
- measure the thickness of your cornea
Glaucoma Treatment
Treating glaucoma successfully is a team effort between you and your doctor. Your ophthalmologist will prescribe your glaucoma treatment. It is up to you to follow your doctor’s instructions and use your eye drops.
Once you are taking medications for glaucoma, your ophthalmologist will want to see you regularly. You can expect to visit your ophthalmologist about every 3–6 months. However, this can vary depending on your treatment needs.
If you have any questions about your eyes or your treatment, talk to your ophthalmologist.
Glaucoma damage is permanent—it cannot be reversed 90. But medicine and surgery help to stop further damage. To treat glaucoma, your ophthalmologist may use one or more of the following treatments.
Medication
Glaucoma is usually controlled with eyedrop medicine. Used every day, these eye drops lower eye pressure. Some do this by reducing the amount of aqueous fluid the eye makes. Others reduce pressure by helping fluid flow better through the drainage angle.
Glaucoma medications can help you keep your vision, but they may also produce side effects. Some eye drops may cause 90:
- a stinging or itching sensation
- red eyes or red skin around the eyes
- changes in your pulse and heartbeat
- changes in your energy level
- changes in breathing (especially if you have asthma or breathing problems)
- dry mouth
- blurred vision
- eyelash growth
- changes in your eye color, the skin around your eyes or eyelid appearance.
All medications can have side effects. Some drugs can cause problems when taken with other medications. It is important to give your doctor a list of every medicine you take regularly. Be sure to talk with your ophthalmologist if you think you may have side effects from glaucoma medicine.
Never change or stop taking your glaucoma medications without talking to your ophthalmologist 90. If you are about to run out of your medication, ask your ophthalmologist if you should have your prescription refilled.
Laser surgery
There are two main types of laser surgery to treat glaucoma. They help aqueous drain from the eye. These procedures are usually done in the ophthalmologist’s office or an outpatient surgery center.
- Trabeculoplasty. This surgery is for people who have open-angle glaucoma. The eye surgeon uses a laser to make the drainage angle work better. That way fluid flows out properly and eye pressure is reduced.
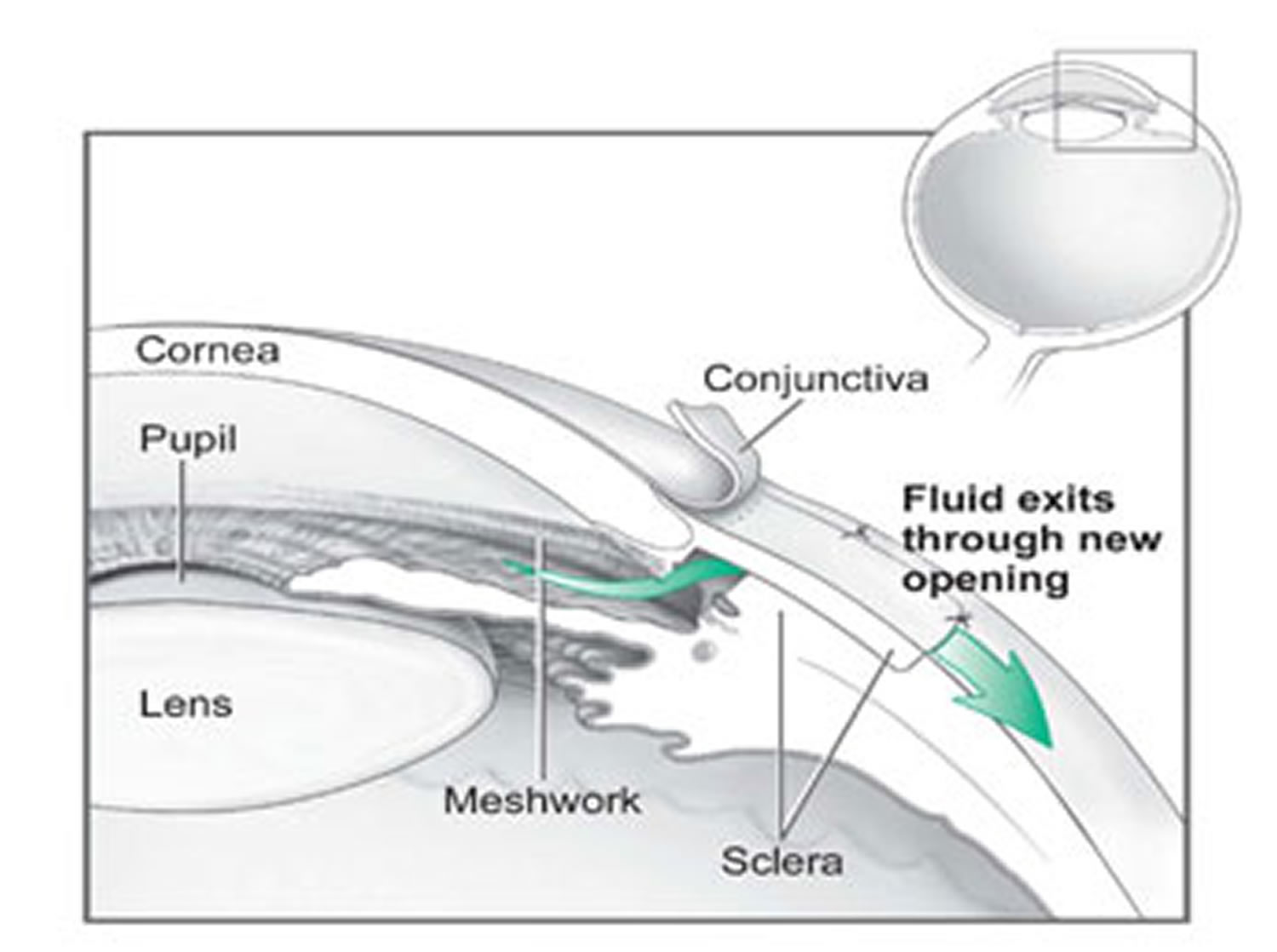
In trabeculectomy, a flap is first created in the sclera (the white part of the eye). Then a small opening is made into the eye to release fluid from the eye.
Figure 10. Trabeculoplasty surgery for glaucoma
- Iridotomy. This is for people who have angle-closure glaucoma. The ophthalmologist uses a laser to create a tiny hole in the iris. This hole helps fluid flow to the drainage angle.
Operating room surgery
Some glaucoma surgery is done in an operating room. It creates a new drainage channel for the aqueous humor to leave the eye.
- Trabeculectomy. This is where your eye surgeon creates a tiny flap in the sclera (white of your eye). He or she will also create a bubble (like a pocket) in the conjunctiva called a filtration bleb. It is usually hidden under the upper eyelid and cannot be seen. Aqueous humor will be able to drain out of the eye through the flap and into the bleb. In the bleb, the fluid is absorbed by tissue around your eye, lowering eye pressure.
- Glaucoma drainage devices. Your ophthalmologist may implant a tiny drainage tube in your eye. It sends the fluid to a collection area (called a reservoir). Your eye surgeon creates this reservoir beneath the conjunctiva (the thin membrane that covers the inside of your eyelids and white part of your eye). The fluid is then absorbed into nearby blood vessels.
What Is Uveitis ?
Uveitis occurs when the middle layer of the eyeball gets inflamed (red and swollen). This layer, called the uvea, has many blood vessels that nourish the eye. Uveitis can damage vital eye tissue, leading to permanent vision loss 91.
Three types of uveitis
There are 3 types of uveitis. They are based on which part of the uvea is affected.
- Swelling of the uvea near the front of the eye is called anterior uveitis. It starts suddenly and symptoms can last up to 8 weeks. Some forms of anterior uveitis are ongoing, while others go away but keep coming back.
- Swelling of the uvea in the middle of the eye is called intermediate uveitis. Symptoms can last for a few weeks to many years. This form can go through cycles of getting better, then getting worse.
- Swelling of the uvea toward the back of the eye is called posterior uveitis. Symptoms can develop gradually and last for many years.
In severe cases, all layers may be involved 91.
Uveitis Causes
Doctors do not always know what causes uveitis. You are more likely to get uveitis if you have or have had 92:
- infections such as shingles virus, herpes simplex virus, syphilis, Lyme disease, and parasites such as toxoplasmosis.
- a systemic inflammatory disease such as inflammatory bowel disease (IBS), rheumatoid arthritis or lupus
- an eye injury
Smoking (cigarettes, cigars or pipes) also increases your risk of getting uveitis.
Uveitis Symptoms
Uveitis can develop suddenly. Symptoms can include 93:
- having a red eye with or without pain
- being very sensitive to bright light
- having blurry vision
- seeing “floaters” (specks or moving clouds in your vision) all of a sudden
See your ophthalmologist right away if you notice any of these symptoms.
Uveitis Diagnosis
Your ophthalmologist will examine the inside of your eye. Since uveitis is often connected with other diseases or conditions, some tests may be needed. They may include a physical exam, blood or skin tests, examination of eye fluids, and imaging tests, such as X-rays 94. Your ophthalmologist may ask about other diseases or health problems you have had.
How is uveitis treated ?
Uveitis needs to be treated right away to prevent lasting problems 94. Ophthalmologists often treat uveitis with eyedrop medicine that reduces inflammation (corticosteroids). They may also use an eye drop to widen (dilate) the pupil, which helps reduce pain and swelling. Sometimes medicine may need to be given by injection (shots) or taken by mouth. Often times, your ophthalmologist will work with a special kind of doctor called a rheumatologist to help treat you.
What Is Optic Neuritis ?
Optic neuritis is swelling of the eye’s optic nerve 95. The optic nerve carries light signals from the back of your eye to your brain so you can see. If the optic nerve is swollen, damaged or infected, you cannot see clearly.
Doctors do not know for sure what causes optic neuritis 95. This condition may be caused by the body’s immune system attacking optic nerve tissue by mistake 95. It seems more likely to happen in people who have had viral problems like mumps, measles, flu or multiple sclerosis, among others.
Optic Neuritis Symptoms
You can have optic neuritis in one or both eyes. Symptoms may appear all of a sudden or develop gradually over a few days. They can include 96:
- Blurry vision
- Dim vision, as if someone turned down the lights
- Colors appearing dull and faded
- Pain in the back of your eye socket
- Pain when you move your eyes
Optic neuritis symptoms can be worse when you are hot or very tired. For instance, you might notice more symptoms when you exercise or take a bath.
If optic neuritis is not treated, its symptoms can get worse. If you have optic neuritis symptoms, see your ophthalmologist.
Optic Neuritis Diagnosis
Your ophthalmologist will check your eyes thoroughly and do the following things 97:
- Check to see if your optic nerve is swollen by looking inside your eye with an instrument called an ophthalmoscope.
- Test your side (peripheral) vision.
- Test to check how well you see colors.
- Check to see how your pupils respond to light.
Your ophthalmologist may also want certain tests to show detailed images of your visual system. They could include a CT scan, MRI scan or visual brain wave recording (which shows how your brain processes visual information).
Optic Neuritis Treatment
Some people get better without any treatment for optic neuritis. However, many people need treatment to improve vision or, at least, keep their symptoms from getting worse 98.
The most common treatment is a medicine called corticosteroids. For most people, taking corticosteroids helps improve their vision a lot. Sometimes, it can even help vision return to what it was before optic neuritis. However, for people with multiple sclerosis or other conditions, treatment usually does not bring their vision back to what it was before optic neuritis.
It is very important to see an ophthalmologist if you have optic neuritis symptoms. Treatment can keep symptoms from getting worse and could save your vision.
What Is Microvascular Cranial Nerve Palsy ?
Microvascular Cranial Nerve Palsy is when blood flow to certain nerves in your head (called cranial nerves) is blocked 99. As a result, you may not be able to move your eye a certain way. Also, you will have double vision. Double vision is when you see two of a single image—either side by side, or one above the other.
Your brain sends signals to your eye muscles through 3 nerves. If blood flow to one of these nerves is reduced, certain muscles cannot move the eye.
Doctors do not know for sure why the tiny blood vessels that go to your cranial nerves get blocked. Microvascular Cranial Nerve Palsy is very common in older adults. It is more likely to happen to those who have diabetes and high blood pressure. In fact, it is sometimes called “diabetic palsy.”
Microvascular Cranial Nerve Palsy almost always gets better on its own in about 6–12 weeks, and your vision returns to normal.
Microvascular Cranial Nerve Palsy Symptoms
The most common Microvascular Cranial Nerve Palsy symptoms are problems moving your eyes, blurry vision and double vision 100. You may find that it takes longer than usual to move your eyes. Or you may not be able to move your eyes at all in one or more directions.
In some cases, you may have vertical double vision 100. This is where you see two of the same image, one above the other. Tilting your head toward one of your shoulders may reduce or get rid of this double vision. You may also have both up and down (vertical) and side by side double vision.
You may have a droopy eyelid 100. You could also have pain in, or around, your eye. This may happen just before you notice double vision. Rarely, your pupil (the black dot in the center of your eye) gets larger.
Microvascular Cranial Nerve Palsy Diagnosis
Your ophthalmologist will do a complete medical eye exam. He or she will want to learn more about the type of double vision you are having. That can help show which nerves are affected.
Sometimes, you will have tests to provide detailed images of your eye, such as a CT scan, MRI, or angiogram.
Your ophthalmologist may also refer you to a neurologist.
Microvascular Cranial Nerve Palsy and stroke
Risk factors for Microvascular Cranial Nerve Palsy include high blood pressure, diabetes and smoking. These same risk factors increase your chances for having a stroke. Work closely with your doctor to reduce or treat these risk factors.
Microvascular Cranial Nerve Palsy Treatment
Microvascular Cranial Nerve Palsy goes away on its own 101. There is no way to shorten the amount of time it takes to recover from it. In the meantime, there are ways to help cope with your double vision. For instance, you can wear a patch on one of your eyes. This often helps reduce the symptoms of double vision. You can also try wearing prism glasses. Your ophthalmologist can explain how they help with double vision, and prescribe them for you.
If you have pain from Microvascular Cranial Nerve Palsy, you might take an anti-inflammatory medicine such as ibuprofen (Advil® or Motrin®).
It is also important to make sure that your blood pressure and blood sugar levels are well controlled.
If your eye muscles do not recover fully on their own, your ophthalmologist may suggest you have eye muscle surgery.
It is very important to tell your doctor if your double vision does not go away or if you get new double vision symptoms.
What Is Bell’s Palsy ?
Bell’s palsy is a nerve problem that affects the muscles of your face 77. It causes weakness or partial paralysis of the muscles on one side of your face. With Bell’s palsy, your eyelid may not close properly and your smile may seem uneven.
Bell’s palsy usually affects adults only. It is more likely to happen to people who have diabetes, are pregnant, or have a family history of Bell’s palsy.
What causes Bell’s palsy ?
Generally, it is not known what causes Bell’s palsy 77. However, doctors believe it may be due to one or more of these problems:
- problems in your body’s immune system (how it fights disease)
- reduced blood flow to a nerve that goes to your face (the 7th cranial nerve)
- infection from a virus, causing swelling of the facial nerves
Bell’s Palsy Symptoms
Bell’s palsy symptoms can appear all of a sudden 102. You may notice that you cannot smile on one side of your face. You may have trouble speaking clearly, and you may lose feeling in your face. You may have some facial pain just before or as it becomes weakened or partially paralyzed.
Your eyes may become dry and you may have blurry vision. One eye may not close completely, and it may feel irritated.
You might not be able to taste food as well as you could before. Also, you could have hearing problems, such as having things sound distorted or unusual.
Tell your primary care doctor or ophthalmologist if any of your symptoms get worse.
If you have symptoms on both sides of your face, you may have something other than Bell’s palsy. If your symptoms do not improve in a few weeks, your ophthalmologist may recommend an MRI. An MRI is a scan that provides images of tissue inside the body.
How long do Bell’s palsy symptoms last ?
For about 8 out of 10 people, symptoms of Bell’s palsy start to improve in about 3 weeks. Symptoms should be nearly gone in about 2–3 months 102.
Some symptoms may remain, such as a small amount of facial paralysis or reduced movement on one side of your face. For about 2 out of 10 people, Bell’s palsy symptoms never go away.
Your ophthalmologist can tell you how to relieve uncomfortable eye-related symptoms with Bell’s palsy.
Bell’s Palsy Treatment
There is no treatment for Bell’s palsy 103. In most cases, it goes away on its own in a few weeks. However, your ophthalmologist can help manage the symptoms affecting your eye. Eye drops or other lubricants provide relief if you cannot fully shut your eye.
In some cases, corticosteroids, antiviral drugs or other medicine may be prescribed to help you heal from Bell’s palsy.
What is a Black Eye ?
Black eye is a phrase used to describe bruising around the eye due to an injury to the face or the head 104. Blood and other fluids collect in the space around the eye, causing swelling and dark bruising in the tissue.
When there is trauma or injury to the face, the skin around the eye — which is very loose — is one of the first places to swell as fluid builds up. Although the name “black eye” would indicate otherwise, the eye itself is usually not injured. Many black eyes heal on their own in a few days.
A black eye can be a sign of a more serious injury, such as a hyphema (bleeding in the eye) 104.
However, a black eye can be a sign of a more serious injury. For instance, if there is bleeding within the eye that is called a hyphema and should be looked for any time you see a black eye. It can affect your cornea and your vision. In some cases of face or eye trauma, increased pressure inside the eyeball (called ocular hypertension) can occur, resulting in damage to the eye and eyesight if not treated. If both eyes are black after a head injury, it could signify a skull fracture or other serious injury.
Black Eye Symptoms
After an injury to the eye, it is important to distinguish between symptoms of black eye and those that might indicate a more serious head injury.
Black eye symptoms may include:
- pain around the eye
- swelling around the eye, which can be mild at first, then increasing later. Swelling may make it difficult to open the eye
- discoloration (like a bruise) around the eye. The skin around the eye may be red at first, then grows darker, progressing to purple, yellow, green or black
- blurred vision
Signs of a more serious head injury require medical attention, and may include the following 105:
- double vision
- vision loss
- blood on the eyeball surface
- inability to move the eye
- severe or ongoing headache
- fainting/loss of consciousness
- blood or fluid coming from the ears or nose
What Causes a Black Eye ?
A black eye is most commonly caused by something hitting the eye or nose 106. Either one or both eyes may be blackened depending on where you get hit. If you suffer a blow to the nose, both eyes may swell; the swelling is due to the buildup of fluid in the loose skin beneath the eyes. Other types of trauma to the head can cause black eyes, including skull fractures.
Facial surgery can also cause black and swollen eyes, including facelifts, nose surgery or surgery on the jaw. Other conditions, such as allergies and infections, can lead to swelling around the eye, but not the bruising discoloration of a black eye.
Black Eye Diagnosis
In general, your doctor can simply do a physical exam to diagnose a black eye. He or she will check your vision and test the motion of your eye by moving his or her finger in front of your face and asking you to follow the movement with your eyes. The doctor will shine a light into your eyes to assess if your pupil is dilating normally and to look at the inside of your eye for any problems.
The doctor will also examine the bones in your face and around your eye. If he or she suspects you may have fractured any bones or that there might be something inside the eye, you may have an X-ray or CT scan 107.
Black Eye Treatment
A typical black eye that does not involve more serious symptoms is generally treated with self-care at home 108. To reduce swelling and ease pain the first day, an ice pack can be applied to the eye for 15-20 minutes at a time, once every hour. If an ice pack is not available, a bag of frozen vegetables can be used, or ice cubes wrapped in cloth (to avoid freezing the skin). Despite what you see in movies or on television, you should never put a raw steak or other raw meat on a black eye. The bacteria on raw meat poses a high risk of infection, and this method of treating a black eye has no scientific basis.
Finally, be sure to keep the affected eye(s) well-protected from further injury. Avoid sports or other similar activities where the eye can be hit until the eye has healed.
If pain or swelling from a black eye do not improve after a few days, or if you are experiencing vision changes or problems, see your ophthalmologist.
What Is a Blocked Tear Duct ?
A blocked tear duct is when the eye’s drainage system for tears is either partially or completely obstructed 109. Tears cannot drain normally, causing a watery, irritated or chronically infected eye.
Most of your tears come from your lacrimal glands, which are located above each eye. The tears flow down the surface of your eye to lubricate and protect it, and then drain into tiny holes (puncta) in the corners of your upper and lower eyelids. The tears then travel through the small canals in the lids (canaliculi) to a sac where the lids are attached to the side of the nose (lacrimal sac), then down a duct (the nasolacrimal duct) before emptying into your nose, where they evaporate or are reabsorbed.
A baby can be born with a blocked tear duct (a congenital blocked tear duct). It is estimated nearly 20 percent of newborns have a blocked tear duct, but the condition usually resolves on its own within four to six months. In adults, the tear duct obstruction can result from an eye infection, swelling, injury or a tumor.
Blocked Tear Duct Causes
A blockage can occur at any point in the tear drainage system. When that happens, your tears don’t drain properly, giving you watery eyes and increasing your risk of eye infections and inflammation.
Babies in utero have a thin membrane that seals the nasolacrimal duct. In newborns, a blocked tear duct may be the result of that membrane not opening as it should at birth.
Another cause of blocked tear duct may be chronic nose infections. Chronic sinusitis may irritate the tissues and form scars, which block the tear duct system.
Other causes of blocked tear duct:
- Abnormal development of the skull and face (craniofacial abnormalities), like those in Down syndrome or other disorders, increases the likelihood of blockage of the tear ducts.
- Age-related changes in older adults can cause blocked tear ducts, including narrowing of the punctal openings.
- Nose trauma, such as a broken nose; scar tissue can block the tear duct.
- Nose polyps, a growth from the lining of the nose (affecting some people who have nasal allergies), can obstruct the tear duct system
- Conjunctivitis, infection and inflammation of the conjunctiva, the thin membrane covering the eye. In rare cases, the tear duct system may become infected and blocked, especially after some viral infections
- Tumor, which may press on the tear duct system and prevent drainage.
If your eye has been watery and leaking or is continually irritated or infected, you should see your ophthalmologist.
Blocked Tear Duct Symptoms
Symptoms of a blocked tear duct may include watery eyes or tears running out of the eyes. The symptoms of a blocked tear duct may get worse after a cold or sinus infection. Also, symptoms may be more noticeable after exposure to cold, wind or sunlight.
When tear ducts are blocked, trapped bacteria in the nasolacrimal sac can lead to infection (called dacryocystitis). Symptoms of infection include:
- Inflammation (swelling), tenderness and redness of the inside corner of the eye or around the eye and nose
- Recurrent eye infections
- Eye mucus discharge
- Crusty eyelashes
- Blurred vision
- Blood-tinged tears
- Fever
Blocked Tear Duct Diagnosis
Your ophthalmologist diagnoses a blocked tear duct using a number of tests, including a complete medical eye exam. He or she will discuss your medical history and thoroughly examine your eyes to check for other possible causes.
Your Eye M.D. will also use certain tests to examine the tear drainage system for blockage. A special fluid is flushed into the affected tear duct opening and, if the fluid cannot be tasted in the throat, a blocked tear duct is diagnosed.
Other tests may include an X-ray or CT scan of the tear duct area (called a dacryocystogram).
Blocked Tear Duct Treatment 110
Sometimes, more than one treatment or procedure is needed before a blocked tear duct is fully opened. If an infection is suspected, your doctor will likely prescribe antibiotics.
Many babies with congenital blocked tear duct improve on their own in the first several months of life, after the drainage system matures or the extra membrane involving the nasolacrimal duct opens up 110. In some cases, your ophthalmologist may recommend that you use a special massage technique to help open up the membrane covering the lower opening into your baby’s nose 110. He or she will demonstrate how to correctly do this massage.
The purpose of massage is to put pressure on the lacrimal sac to pop open the membrane at the bottom of the tear duct. This is most easily accomplished by placing your hands on each side of the baby’s face with your index finger(s) between the inner corner of the eye and the side of the nose, pressing in and down over the lacrimal sac for a few seconds. The massage should be done once in the morning and once in the evening, and each massage should be ten strokes each. It is best to do the massage during a diaper change.
In most cases of blocked tear ducts after a facial injury, the drainage system starts working again on its own a few months after the injury, and no additional treatment is necessary. Your Eye M.D. may recommend waiting a few months after the injury before considering surgery to open the blocked tear duct.
For infants and toddlers whose blocked tear ducts aren’t opening on their own, or for adults who have a partially blocked duct or a partial narrowing of the puncta, a technique using dilation, probing and irrigation may be used 110. An instrument is used to enlarge (dilate) the punctal openings and a narrow probe is guided through the puncta, into the tear drainage system, then through the nasal opening and removed. The tear drainage system is flushed with a saline solution to clear out any residual blockage.
A balloon catheter dilation procedure opens tear drainage passages that are narrowed or blocked by scarring or inflammation 110. General anesthesia is used. A narrow catheter (tube) with a deflated balloon on the tip is guided through the lower nasolacrimal duct. The doctor then uses a pump to inflate and deflate the balloon along the drainage system.
With a procedure called stenting or intubation, tiny tubes are used to open up blockages and narrowing within the tear drainage system. Again, general anesthesia is usually used. Your Eye M.D. threads a very thin tube through one or both puncta in the corner of your eye, all the way through the tear drainage system and out through your nose. A tiny loop of tubing remains at the corner of your eye, but while it is visible, it’s usually not bothersome. These tubes are generally left in for three to four months, and then removed.
Surgery is usually the preferred option for people who develop blocked tear ducts. It is also effective in babies and toddlers with congenital blocked tear ducts, though usually an option only after other treatments have been tried.
Dacryocystorhinostomy is the surgical procedure usually used to treat most cases of blocked tear ducts in adults and rarely in children. This technique creates a new route for tears to drain out through your nose normally again by developing a new connection between your lacrimal sac and your nose. This new route bypasses the duct that empties into your nose (nasolacrimal duct), which is typically the blockage site. Stents or intubation typically are placed in the new route while it heals, and then removed three or four months after surgery. The steps in this procedure will vary depending on your particular tear duct blockage.
Depending on the type of blockage, your surgeon may recommend creating an entirely new route from the inside corner of your eyes (puncta) to your nose, bypassing the tear drainage system altogether. This reconstruction of your entire tear drainage system is called conjunctivodacryocystorhinostomy.
To prevent postoperative infection and inflammation, you will need to use a nasal decongestant spray and eye drops. After about three to six months, your Eye M.D. will remove any stents that were put in place to keep the new channel open while healing.
If a tumor is causing your blocked tear duct, surgery may be performed to remove the tumor, or other treatments may be used to shrink it 110.
- American Academy of Ophthalmology. Pain in Eye. https://www.aao.org/eye-health/symptoms/pain-in-eye-3[↩][↩]
- American Academy of Ophthalmology. Pain Around Eye. https://www.aao.org/eye-health/symptoms/pain-around-eye[↩][↩][↩]
- Evaluation of the Painful Eye. Am Fam Physician. 2016 Jun 15;93(12):991-998. http://www.aafp.org/afp/2016/0615/p991.html[↩][↩][↩][↩]
- Cain W Jr, Sinskey RM. Detection of anterior chamber leakage with Seidel’s test. Arch Ophthalmol. 1981;99(11):2013.[↩]
- Pokhrel PK, Loftus SA. Ocular emergencies [published correction appears in Am Fam Physician. 2008;77(7):920]. Am Fam Physician. 2007;76(6):829–836.[↩]
- Gerstenblith AT, Rabinowitz MP. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 6th ed. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2012.[↩][↩][↩]
- Waldman CW, Waldman SD, Waldman RA. A practical approach to ocular pain for the non-ophthalmologist. Pain Manag. 2014;4(6):413–426.[↩]
- Kaye S, Choudhary A. Herpes simplex keratitis. Prog Retin Eye Res. 2006;25(4):355–380.[↩][↩][↩][↩]
- Catron T, Hern HG. Herpes zoster ophthalmicus. West J Emerg Med. 2008;9(3):174–176.[↩][↩][↩]
- Shields T, Sloane PD. A comparison of eye problems in primary care and ophthalmology practices. Fam Med. 1991;23(7):544–546.[↩][↩]
- Nash EA, Margo CE. Patterns of emergency department visits for disorders of the eye and ocular adnexa. Arch Ophthalmol. 1998;116(9):1222–1226.[↩][↩]
- Dargin JM, Lowenstein RA. The painful eye. Emerg Med Clin North Am. 2008;26(1):199–216, viii.[↩][↩][↩][↩]
- Azari AA, Barney NP. Conjunctivitis [published correction appears in JAMA. 2014;311(1):95]. JAMA. 2013;310(16):1721–1729.[↩][↩][↩][↩]
- National Institute for Health and Care Excellence. Headaches in over 12s. https://www.nice.org.uk/guidance/cg150[↩][↩][↩][↩]
- Weaver-Agostoni J. Cluster headache. Am Fam Physician. 2013;88(2):122–128.[↩][↩]
- Lee S, Yen MT. Management of preseptal and orbital cellulitis. Saudi J Ophthalmol. 2011;25(1):21–29.[↩][↩]
- Wipperman JL, Dorsch JN. Evaluation and management of corneal abrasions. Am Fam Physician. 2013;87(2):114–120.[↩][↩]
- Walochnik J, Scheikl U, Haller-Schober EM. Twenty years of acanthamoeba diagnostics in Austria. J Eukaryot Microbiol. 2015;62(1):3–11.[↩][↩]
- Sambursky RP, Fram N, Cohen EJ. The prevalence of adenoviral conjunctivitis at the Wills Eye Hospital Emergency Room. Optometry. 2007;78(5):236–239.[↩]
- Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10.[↩]
- Shields SR. Managing eye disease in primary care. Part 3. When to refer for ophthalmologic care. Postgrad Med. 2000;108(5):99–106.[↩]
- Saw SM, Gazzard G, Friedman DS. Interventions for angle-closure glaucoma. Ophthalmology. 2003;110(10):1869–1878.[↩]
- Jabs DA, Rosenbaum JT, Foster CS, et al. Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders. Am J Ophthalmol. 2000;130(4):492–513.[↩]
- Smith JM, Bratton EM, DeWitt P, Davies BW, Hink EM, Durairaj VD. Predicting the need for surgical intervention in pediatric orbital cellulitis. Am J Ophthalmol. 2014;158(2):387–394.e1.[↩]
- Pula JH, Macdonald CJ. Current options for the treatment of optic neuritis. Clin Ophthalmol. 2012;6:1211–1223.[↩][↩]
- Jabs DA, Mudun A, Dunn JP, Marsh MJ. Episcleritis and scleritis. Am J Ophthalmol. 2000;130(4):469–476.[↩][↩][↩]
- Dart JK. Predisposing factors in microbial keratitis: the significance of contact lens wear. Br J Ophthalmol. 1988;72(12):926–930.[↩]
- Schein OD. Contact lens abrasions and the nonophthalmologist. Am J Emerg Med. 1993;11(6):606–608.[↩]
- Yaphe J, Pandher KS. The predictive value of the penlight test for photophobia for serious eye pathology in general practice. Fam Pract. 2003;20(4):425–427.[↩][↩][↩]
- Beck RW, Trobe JD, Moke PS, et al.; Optic Neuritis Study Group. High- and low-risk profiles for the development of multiple sclerosis within 10 years after optic neuritis. Arch Ophthalmol. 2003;121(7):944–949.[↩][↩]
- Kerr NM, Chew SS, Eady EK, et al. Diagnostic accuracy of confrontation visual field tests. Neurology. 2010;74(15):1184–1190.[↩]
- Han F, Yuan YS. Characteristics of visual field defects in primary angle-closure glaucoma [in Chinese]. Zhonghua Yan Ke Za Zhi. 2009;45(1):14–20.[↩]
- Keltner JL, Johnson CA, Cello KE, et al. Visual field profile of optic neuritis. Arch Ophthalmol. 2010;128(3):330–337.[↩]
- Wikipedia. Snellen chart. https://en.wikipedia.org/wiki/Snellen_chart[↩]
- Robinett DA, Kahn JH. The physical examination of the eye. Emerg Med Clin North Am. 2008;26(1):1–16, v.[↩][↩][↩]
- Liesegang TJ. Epidemiology of ocular herpes simplex. Natural history in Rochester, Minn, 1950 through 1982. Arch Ophthalmol. 1989;107(8):1160–1165[↩]
- Leibowitz HM. The red eye. N Engl J Med. 2000;343(5):345–351.[↩][↩]
- Spector RH. The pupils. In: Walker HK, Hall WD, Hurst JW. Clinical Methods: The History, Physical, and Laboratory Examinations. Boston, Mass.: Butterworths; 1990.[↩]
- Chong NV, Murray PI. Pen torch test in patients with unilateral red eye. Br J Gen Pract. 1993;43(371):259.[↩]
- Blazek P, Davis SL, Greenberg BM, et al. Objective characterization of the relative afferent pupillary defect in MS. J Neurol Sci. 2012;323(1–2):193–200.[↩]
- Stanley JA, Baise GR. The swinging flashlight test to detect minimal optic neuropathy. Arch Ophthalmol. 1968;80(6):769–771.[↩]
- Harooni H, Golnik KC, Geddie B, Eggenberger ER, Lee AG. Diagnostic yield for neuroimaging in patients with unilateral eye or facial pain. Can J Ophthalmol. 2005;40(6):759–763.[↩]
- American Academy of Ophthalmology. What Is Hyphema ? https://www.aao.org/eye-health/diseases/what-is-hyphema[↩][↩]
- American Academy of Ophthalmology. Hyphema Symptoms. https://www.aao.org/eye-health/diseases/hyphema-symptoms[↩]
- American Academy of Ophthalmology. What Causes Hyphema ? https://www.aao.org/eye-health/diseases/hyphema-cause[↩]
- American Academy of Ophthalmology. Hyphema Diagnosis. https://www.aao.org/eye-health/diseases/hyphema-diagnosis[↩]
- American Academy of Ophthalmology. Hyphema Treatment. https://www.aao.org/eye-health/diseases/hyphema-treatment[↩]
- American Academy of Ophthalmology. What Is Bacterial Keratitis ? https://www.aao.org/eye-health/diseases/what-is-bacterial-keratitis[↩][↩]
- American Academy of Ophthalmology. What Is Cellulitis ? https://www.aao.org/eye-health/diseases/what-is-cellulitis[↩][↩]
- American Academy of Ophthalmology. Cellulitis Causes and Symptoms. https://www.aao.org/eye-health/diseases/cellulitis-cause[↩]
- American Academy of Ophthalmology. Cellulitis Diagnosis. https://www.aao.org/eye-health/diseases/cellulitis-diagnosis[↩]
- American Academy of Ophthalmology. Cellulitis Treatment. https://www.aao.org/eye-health/diseases/cellulitis-treatment[↩][↩][↩]
- American Academy of Ophthalmology. Conjunctivitis: What Is Pink Eye ? https://www.aao.org/eye-health/diseases/pink-eye-conjunctivitis[↩]
- American Academy of Ophthalmology. Conjunctivitis: Pink Eye Symptoms. https://www.aao.org/eye-health/diseases/pink-eye-conjunctivitis-symptoms[↩]
- American Academy of Ophthalmology. Conjunctivitis: Pink Eye Treatment. https://www.aao.org/eye-health/diseases/pink-eye-conjunctivitis-treatment[↩][↩][↩][↩]
- American Academy of Ophthalmology. What is Fungal Keratitis ? https://www.aao.org/eye-health/diseases/what-is-fungal-keratitis[↩][↩][↩][↩]
- American Academy of Ophthalmology. Fungal Keratitis Causes. https://www.aao.org/eye-health/diseases/fungal-keratitis-cause[↩]
- American Academy of Ophthalmology. Fungal Keratitis Symptoms. https://www.aao.org/eye-health/diseases/fungal-keratitis-symptoms[↩]
- American Academy of Ophthalmology. Fungal Keratitis Treatment. https://www.aao.org/eye-health/diseases/fungal-keratitis-treatment[↩]
- American Academy of Ophthalmology. What is Herpes Keratitis ? https://www.aao.org/eye-health/diseases/herpes-keratitis[↩]
- American Academy of Ophthalmology. Herpes Keratitis Causes. https://www.aao.org/eye-health/diseases/herpes-keratitis-cause[↩][↩]
- American Academy of Ophthalmology. Herpes Keratitis Symptoms. https://www.aao.org/eye-health/diseases/herpes-keratitis-symptoms[↩]
- American Academy of Ophthalmology. Herpes Keratitis Treatment. https://www.aao.org/eye-health/diseases/herpes-keratitis-treatment[↩][↩][↩][↩]
- American Academy of Ophthalmology. What Is Corneal Abrasion ? https://www.aao.org/eye-health/diseases/what-is-corneal-abrasion[↩]
- American Academy of Ophthalmology. What Causes Corneal Abrasion ? https://www.aao.org/eye-health/diseases/corneal-abrasion-cause[↩]
- American Academy of Ophthalmology. Corneal Abrasion Symptoms. https://www.aao.org/eye-health/diseases/corneal-abrasion-symptoms[↩]
- American Academy of Ophthalmology. Corneal Abrasion Treatment. https://www.aao.org/eye-health/diseases/corneal-abrasion-treatment[↩][↩][↩]
- American Academy of Ophthalmology. What Is Corneal Laceration ? https://www.aao.org/eye-health/diseases/what-is-corneal-laceration[↩][↩]
- American Academy of Ophthalmology. Corneal Laceration Symptoms. https://www.aao.org/eye-health/diseases/corneal-laceration-symptoms[↩]
- American Academy of Ophthalmology. What Causes Corneal Laceration ? https://www.aao.org/eye-health/diseases/corneal-laceration-cause[↩]
- American Academy of Ophthalmology. Corneal Laceration Diagnosis. https://www.aao.org/eye-health/diseases/corneal-laceration-diagnosis[↩]
- American Academy of Ophthalmology. Corneal Laceration Treatment. https://www.aao.org/eye-health/diseases/corneal-laceration-treatment[↩][↩][↩]
- American Academy of Ophthalmology. What Is a Corneal Ulcer ? https://www.aao.org/eye-health/diseases/corneal-ulcer[↩]
- American Academy of Ophthalmology. Corneal Ulcer Symptoms. https://www.aao.org/eye-health/diseases/corneal-ulcer-symptoms[↩][↩]
- American Academy of Ophthalmology. Who Is At Risk for Corneal Ulcers ? https://www.aao.org/eye-health/diseases/corneal-ulcer-risk[↩]
- American Academy of Ophthalmology. What Causes Corneal Ulcers ? https://www.aao.org/eye-health/diseases/corneal-ulcer-cause[↩][↩][↩][↩]
- American Academy of Ophthalmology. What Is Bell’s Palsy ? https://www.aao.org/eye-health/diseases/bells-palsy[↩][↩][↩]
- American Academy of Ophthalmology. Corneal Ulcer Diagnosis. https://www.aao.org/eye-health/diseases/corneal-ulcer-diagnosis[↩]
- American Academy of Ophthalmology. Corneal Ulcer Treatment. https://www.aao.org/eye-health/diseases/corneal-ulcer-treatment[↩][↩]
- American Academy of Ophthalmology. What Is Fuchs’ Dystrophy ? https://www.aao.org/eye-health/diseases/what-is-fuchs-dystrophy[↩][↩][↩][↩][↩]
- American Academy of Ophthalmology. Fuchs’ Dystrophy Symptoms. https://www.aao.org/eye-health/diseases/fuchs-dystrophy-symptoms[↩]
- American Academy of Ophthalmology. Fuchs’ Dystrophy Diagnosis. https://www.aao.org/eye-health/diseases/fuchs-dystrophy-diagnosis[↩]
- American Academy of Ophthalmology. Fuchs’ Dystrophy Treatment. https://www.aao.org/eye-health/diseases/fuchs-dystrophy-treatment[↩]
- The National Eye Institute, National Institutes of Health. Facts About Glaucoma. https://nei.nih.gov/health/glaucoma/glaucoma_facts[↩][↩][↩]
- American Academy of Ophthalmology. What Is Glaucoma ? https://www.aao.org/eye-health/diseases/what-is-glaucoma[↩][↩][↩][↩][↩][↩][↩]
- American Academy of Ophthalmology. What Are the Symptoms of Glaucoma ? https://www.aao.org/eye-health/diseases/glaucoma-symptoms[↩][↩][↩][↩][↩]
- American Academy of Ophthalmology. Causes of Glaucoma. https://www.aao.org/eye-health/diseases/glaucoma-causes[↩]
- American Academy of Ophthalmology. Who Is at Risk for Glaucoma ? https://www.aao.org/eye-health/diseases/glaucoma-risk[↩]
- American Academy of Ophthalmology. Glaucoma Diagnosis. https://www.aao.org/eye-health/diseases/glaucoma-diagnosis[↩]
- American Academy of Ophthalmology. Glaucoma Treatment. https://www.aao.org/eye-health/diseases/glaucoma-treatment[↩][↩][↩]
- American Academy of Ophthalmology. What Is Uveitis ? https://www.aao.org/eye-health/diseases/what-is-uveitis[↩][↩]
- American Academy of Ophthalmology. Uveitis Causes. https://www.aao.org/eye-health/diseases/uveitis-causes[↩]
- American Academy of Ophthalmology. Uveitis Symptoms. https://www.aao.org/eye-health/diseases/uveitis-symptoms[↩]
- American Academy of Ophthalmology. Uveitis Diagnosis. https://www.aao.org/eye-health/diseases/uveitis-diagnosis[↩][↩]
- American Academy of Ophthalmology. What Is Optic Neuritis ? https://www.aao.org/eye-health/diseases/what-is-optic-neuritis[↩][↩][↩]
- American Academy of Ophthalmology. Optic Neuritis Symptoms. https://www.aao.org/eye-health/diseases/optic-neuritis-symptoms[↩]
- American Academy of Ophthalmology. Optic Neuritis Diagnosis. https://www.aao.org/eye-health/diseases/optic-neuritis-diagnosis[↩]
- American Academy of Ophthalmology. Optic Neuritis Treatment. https://www.aao.org/eye-health/diseases/optic-neuritis-treatment[↩]
- American Academy of Ophthalmology. What Is Microvascular Cranial Nerve Palsy ? https://www.aao.org/eye-health/diseases/microvascular-cranial-nerve-palsy[↩]
- American Academy of Ophthalmology. Microvascular Cranial Nerve Palsy Symptoms. https://www.aao.org/eye-health/diseases/microvascular-cranial-nerve-palsy-symptoms[↩][↩][↩]
- American Academy of Ophthalmology. Microvascular Cranial Nerve Palsy Treatment. https://www.aao.org/eye-health/diseases/microvascular-cranial-nerve-palsy-treatment[↩]
- American Academy of Ophthalmology. Bell’s Palsy Symptoms. https://www.aao.org/eye-health/diseases/bells-palsy-symptoms[↩][↩]
- American Academy of Ophthalmology. Bell’s Palsy Treatment. https://www.aao.org/eye-health/diseases/bells-palsy-treatment[↩]
- American Academy of Ophthalmology. What Is a Black Eye ? https://www.aao.org/eye-health/diseases/black-eye[↩][↩]
- American Academy of Ophthalmology. Black Eye Symptoms. https://www.aao.org/eye-health/diseases/black-eye-symptoms[↩]
- American Academy of Ophthalmology. What Causes a Black Eye ? https://www.aao.org/eye-health/diseases/black-eye-cause[↩]
- American Academy of Ophthalmology. Black Eye Diagnosis. https://www.aao.org/eye-health/diseases/black-eye-diagnosis[↩]
- American Academy of Ophthalmology. Black Eye Treatment. https://www.aao.org/eye-health/diseases/black-eye-treatment[↩]
- American Academy of Ophthalmology. What Is a Blocked Tear Duct ? https://www.aao.org/eye-health/diseases/what-is-blocked-tear-duct[↩]
- American Academy of Ophthalmology. Blocked Tear Duct Treatment. https://www.aao.org/eye-health/diseases/treatment-blocked-tear-duct[↩][↩][↩][↩][↩][↩]





{kind=link}