What are tonsils ?
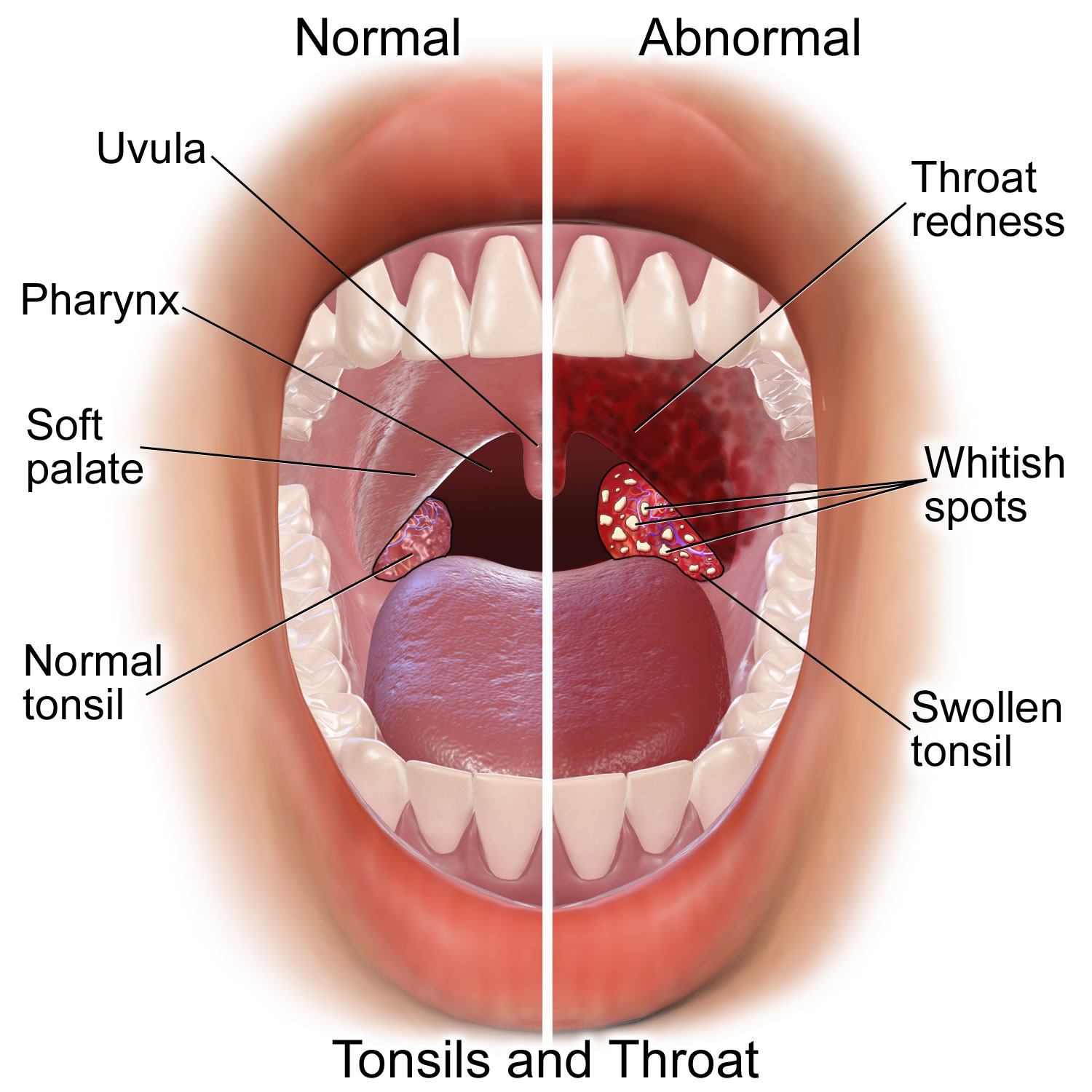
In the back of the mouth, on either side of the tongue and closely associated with the palate, are masses of lymphatic tissue called palatine tonsils (see Figures 1 and 2). Like other lymphatic tissues, the two palatine tonsils help protect the body against infection.
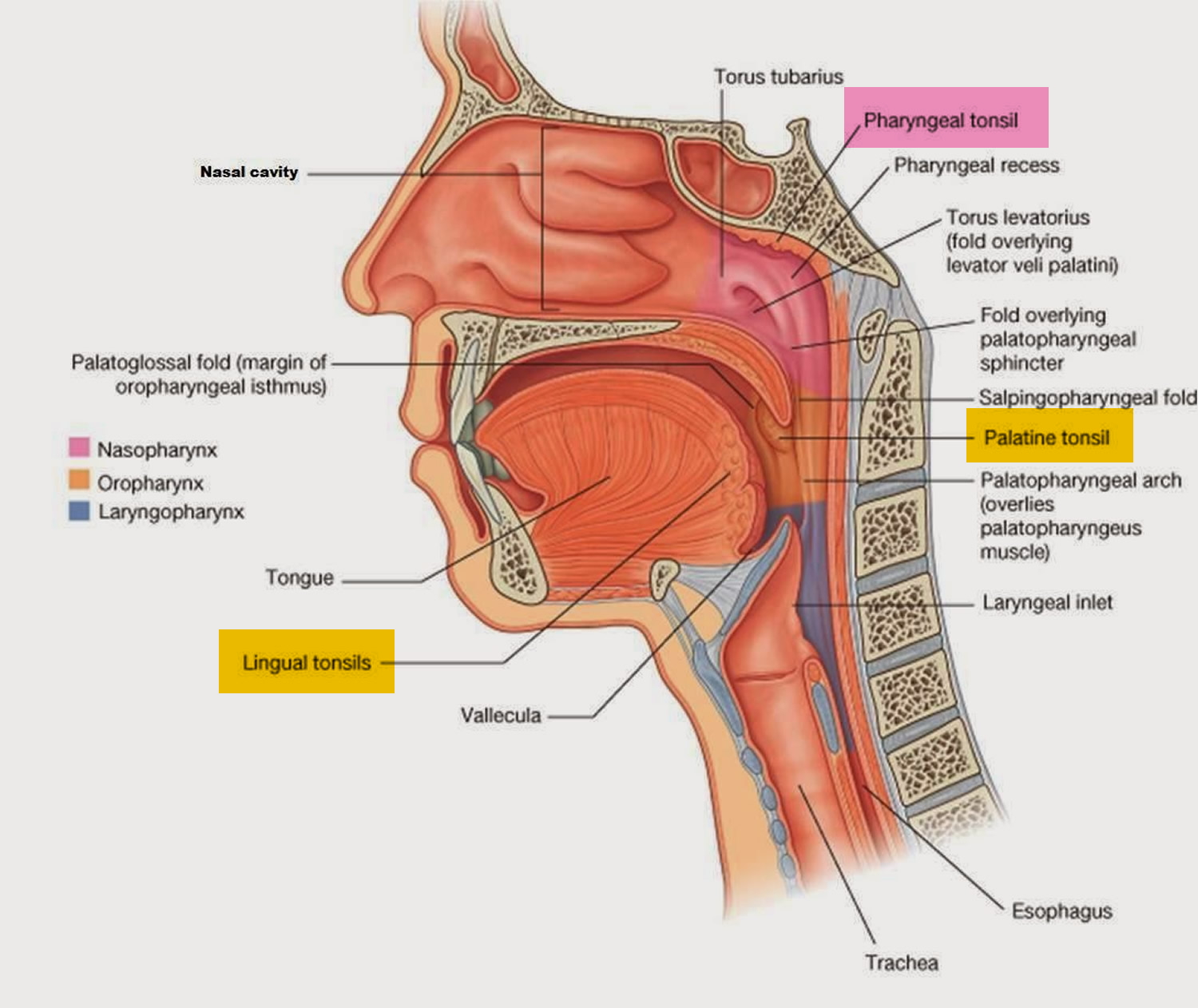
Other masses of lymphatic tissue, called pharyngeal tonsils or adenoids, are on the posterior wall of the pharynx, above the border of the soft palate (Figure 2). The posterior region of the tongue is covered with rounded masses of lymphatic tissue called lingual tonsils (Figure 2).
The 2 palatine tonsils are found to the right and to the left in the palatal arch’s fold of mucous membrane, and are the only tonsils that can be seen unaided when you open your mouth (see Figure 1). The adenoids are situated above the roof of the throat and visible only during rhinoscopy (examination of the inside of the nose). The lingual tonsil is located far back at the base of the tongue on its rear surface.
All tonsils together form a ring around where the mouth and nasal cavity meet the throat. For this reason they are called the tonsillar ring 1. This position allows them to trap germs like viruses or bacteria that could enter the body through the mouth or the nose. There are also more defense cells located behind the tonsillar ring on the sides of the throat. These cells can take on the function of the adenoids after they have been removed.
The tonsils form during the last months of gestation and grow irregularly, reaching their largest size at approximately six or seven years of age 2. The tonsils begin to gradually involute at puberty, and by older age little tonsillar tissue remains 3. When healthy, the tonsils do not project beyond the tonsillar pillars towards the centre of the oropharynx 4.
Each palatine tonsil is separated by a more or less rough capsule from the surrounding muscle (superior pharyngeal constrictor) 5. The palatine tonsils have a strong blood flow from four different vessels, the lingual artery, the ascending pharyngeal artery and the ascending and descending palatine arteries. These vessels radiate mainly to the upper and lower tonsil pole, as well as the exact centre of the tonsils laterally 6. The tonsils have deep crypts to keep the organ surface as large as possible and to create a docking surface for potential antigens 7. The crypts and their adjacent germinal centres are separated from each other by delicate connective tissue 8.
The palatine tonsils are common sites of infection, and become inflamed in tonsillitis. Infected tonsils may swell so greatly that they block the passageways of the pharynx and interfere with breathing and swallowing. When tonsillitis recurs and does not respond to antibiotic treatment, the tonsils may be surgically removed. Such tonsillectomies are done less often today than they were a generation ago because the tonsils’ role in immunity is now recognized.
If the tonsils are often inflamed, especially the palatine tonsils can become permanently enlarged. In children the adenoids can become very large, making breathing difficult and causing chronic runny nose. In both cases it may be necessary to surgically remove the tonsils or adenoids.
Figure 1. Normal palatine tonsils
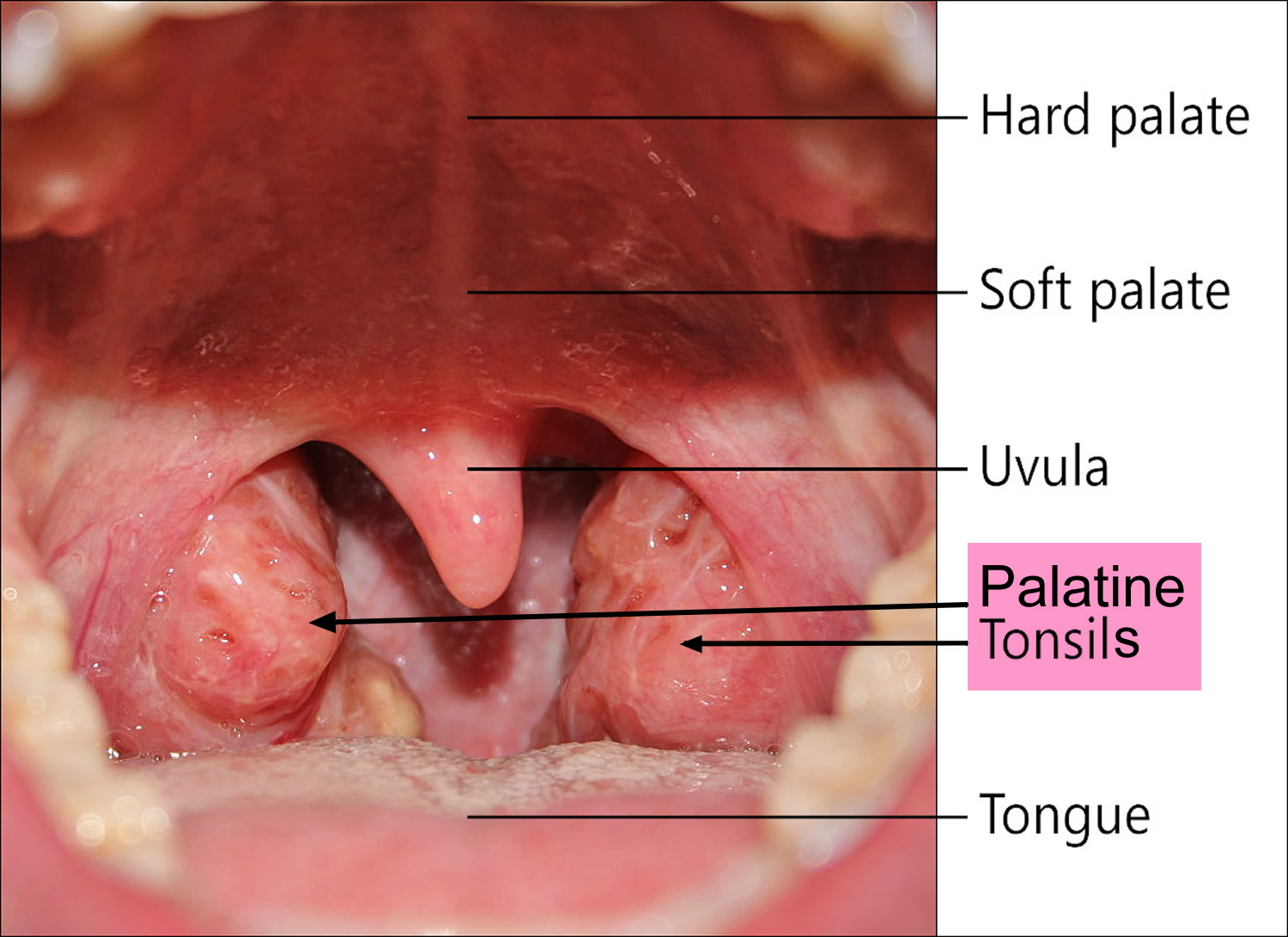
Figure 2. Palatine tonsil, Pharyngeal tonsil and Lingual tonsil
What do tonsils do
The tonsils are part of your body’s defense system. The tonsils serve immune acquisition and immune defence by antigen presentation, which is why they contain T-lymphocytes, macrophages and germinal centres of B-lymphocytes 6. Because of their location at the throat and palate, they have a kind of guardian function. They come into contact with germs especially soon after they enter through the mouth or the nose. Tonsils are the first and easiest-to-reach station of the mucosa associated lymphoid tissue system (MALT) in humans 9. This allows them to activate the immune system early. The greatest immunological activity of the tonsils is found between the ages of 3 and 10 years 10. As a result, the tonsils are most prominent during this period of childhood and subsequently demonstrate age-dependent involution 11. Since the main phase of the immune acquisition continues until the age of 6, the palatine tonsils are physiologically enlarged at this time 12. Then there is shrinkage, which is reflected mostly in a regression until the age of 12 13.
The oral cavity and especially the furrowed tonsil is a reservoir for multiple pathogens (viruses and bacteria), parasites 14 and fungi 15. However, all these microbes belong to the transient flora and we live in symbiosis with them for aeons 16. Jensen A. et al. 17 were able to detect more than 100 bacteria in the tonsils of children and adults with and without recurrent tonsillitis. 52 different bacterial strains form the basis were detectable in each patient, whether child or adult, whether sick or healthy. These represent 90% of the total pathogen load 17.
What are tonsillar crypts
In a studies on the human palatine tonsils, scientists observed the crypts of the palatine tonsil contain many pores, ranging in diameter from 10 to 100 microns, on the luminal surface of the crypts 18. All of the crypt surface except at the sites of pores was covered by epithelial cells. Non-epithelial round cells, mostly lymphocytes, were exposed directly to the crypt lumen through these pores. In the lumen of palatine tonsillar crypts, numerous round cells were present which evidently pass through these pores from the parenchyma. This finding indicates that the tonsillar tissue is directly open to the crypt. Similar findings were obtained in the recess of the pharyngeal tonsil (adenoid).
Figure 3. Tonsillar crypts
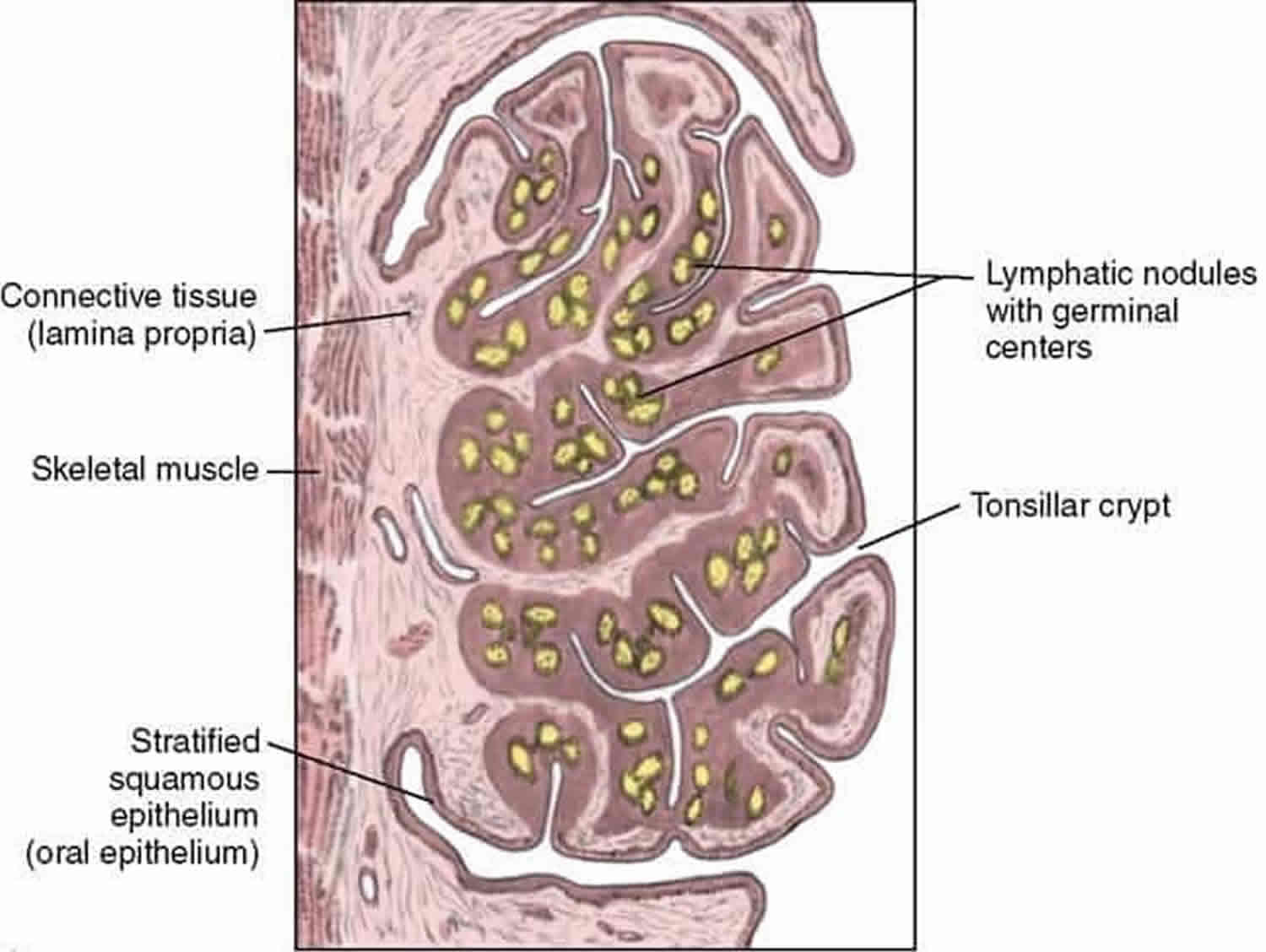
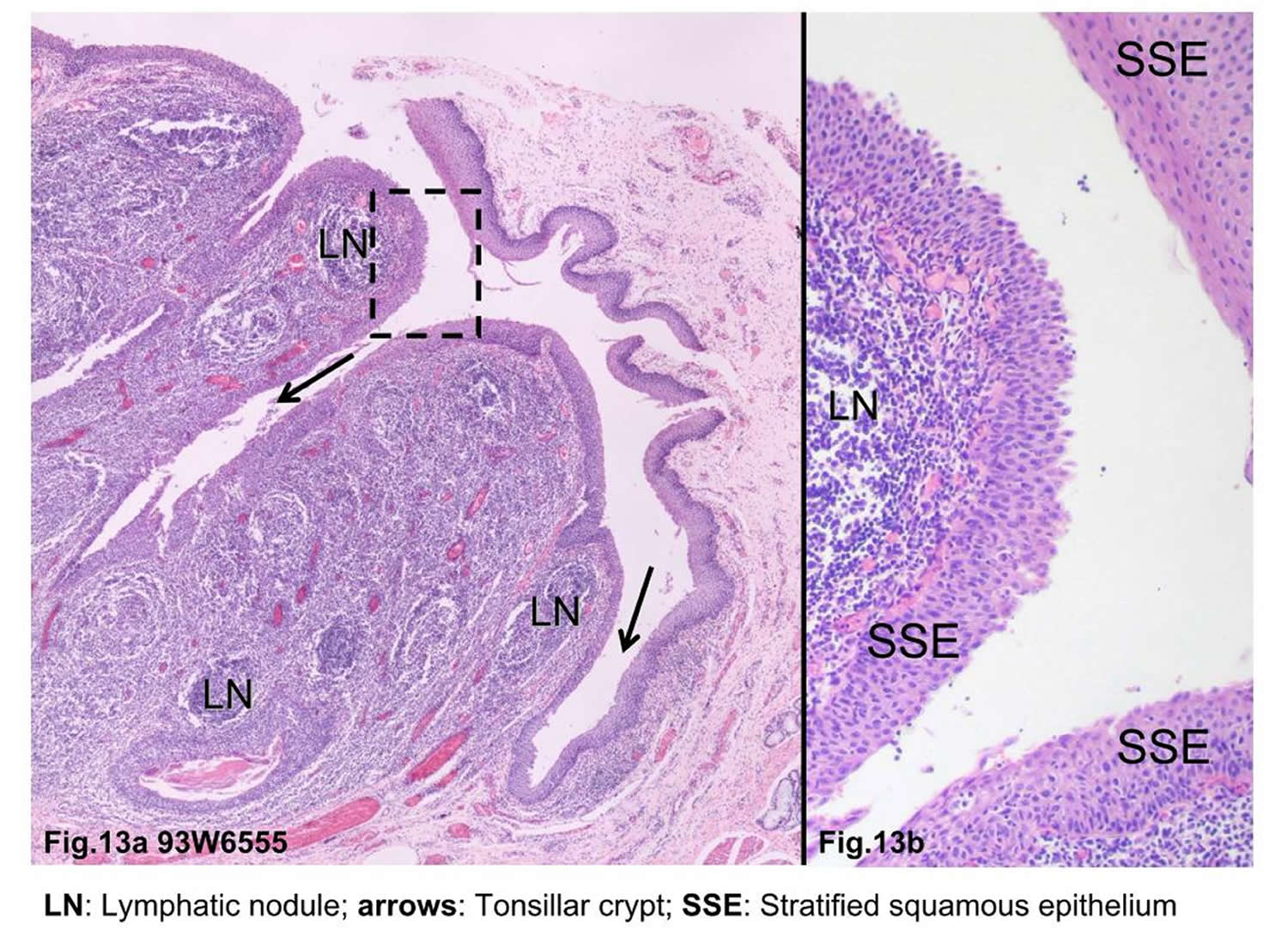
The epithelium of the human palatine tonsil is a site of interest because it overlies a mass of lymphoid tissue that forms a first line of defence in protecting the oropharyngeal isthmus, and as such is constantly exposed both to airborne and alimentary antigens. The surface area of the tonsillar epithelium available for this defensive role is maximised by the 10-30 blind-ending crypts and their rami extending through the full thickness of the tonsil almost to reach its hemicapsule.
The epithelium lining the tonsillar crypts is a highly modified form of the stratified squamous epithelium (SSE) called the “lymphoepithelium” that covers the oropharyngeal surface of the tonsil 19. The epithelium lining the crypts varied in structure from a stratified squamous epithelium (SSE) to a psuedostratified ciliated columnar epithelium (associated with the glands) or a single to double layer of round/cuboidal cells with round/oval nuclei 20. In places the epithelium appeared absent, its position being occupied by concentrations of lymphoid tissue. Lymphocytes were observed to traverse both the psuedostratified ciliated columnar epithelium and the epithelium composed of round/cuboidal cells. In places this took the form of individual or small groups of lymphocytes distorting the base of the epithelial lining cells and forming small pockets in which they were housed. These features were typical of specialised epithelial cells, the M cells, the presence of which, together with the infiltrating lymphocytes, is indicative of a lymphoepithelium or follicle-associated epithelium 21. These “M” cells cells take up antigens into vesicles and transport them to the extrafollicular region or the lymphoid follicles. In the extrafollicular region, interdigitating dendritic cells and macrophages process the antigens and present them to helper T lymphocytes. These lymphocytes stimulate proliferation of follicular B lymphocytes and their development into either antibody-expressing B memory cells capable of migration to the nasopharynx and other sites or plasma cells that produce antibodies and release them into the lumen of the crypt 22.
The presence, and sometimes the predominance, of nonepithelial cells was characteristic of the reticulated epithelium. T and B lymphocytes often infiltrated the whole epithelial thickness, and many plasma cells were located around intraepithelial vessels, while macrophages and interdigitating cells showed a patchy distribution. It is proposed that the major functions of the reticulated epithelium are: (1) to provide a favorable environment for the intimate contact between the effector cells of immune responses; (2) to facilitate direct transport of antigens; (3) to synthesize the secretory component continually; and (4) to contain a pool of immunoglobulins. Thus the reticulated epithelium lining the tonsillar crypts represents a specialized compartment, important in the immunological functions of the tonsil as a whole.
The lymphoid tissue was well vascularised and the capillaries and venules were lined by endothelial cells with round to oval, pale nuclei. Many lymphocytes were present in the lumen of the blood vessels, showing a high degree of trafficking. Lymph nodules were surrounded by a delicate layer of connective tissue.
It is now recognized that crypts epithelium are usually infiltrated by lymphocytes 23. This observations are later confirmed that the function of the palatine tonsil was ‘protection and defence’. Scientists likened the network of epithelial cells to a sponge, which holds the lymphoid cells in its interstices.
While all 5 immunoglobulin (Ig) isotypes are produced in the palatine tonsils, IgA is arguably the most important product of the tonsillar immune system. In its dimeric form, IgA may attach to the transmembrane secretory component to form secretory IgA, a critical component of the mucosal immune system of the upper airway. Although the secretory component is produced only in the extratonsillar epithelium, the tonsils do produce immunocytes bearing the J (joining) chain carbohydrate 24. This component is necessary for binding of IgA monomers to each other and to the secretory component and is an important product of B-cell activity in the follicles of the tonsil.
Effects of Tonsillitis and Tonsillectomy on Immunity
With chronic or recurrent tonsillitis, the controlled process of antigen transport and presentation is altered due to shedding of the M cells from the tonsil epithelium 22. The direct influx of antigens disproportionately expands the population of mature B-cell clones and, as a result, fewer early memory B cells go on to become J-chain–positive IgA immunocytes. In addition, the tonsillar lymphocytes can become so overwhelmed with persistent antigenic stimulation that they may be unable to respond to other antigens. Once this immunological impairment occurs, the tonsil is no longer able to function adequately in local protection, nor can it appropriately reinforce the secretory immune system of the upper respiratory tract. There would therefore appear to be a therapeutic advantage to removing recurrently or chronically diseased tonsils. On the other hand, some studies demonstrate minor alterations of Ig concentrations in the serum and adjacent tissues following tonsillectomy 25. Nevertheless, there are no studies to date that demonstrate a significant clinical impact of tonsillectomy on the immune system 26.
What are tonsils stones ?
Tonsils stones or tonsilloliths are not just stones but are living biofilm similar to dental biofilms, containing corncob structures, filaments, and cocci 27. Microelectrodes showed that the microorganisms respired oxygen and nitrate. The addition of sugar resulted in acid production within the tonsillolith, dropping the pH from 7.3 to 5.8.
What is tonsillitis ?
An acute inflammation of the tonsils caused by viruses or bacteria. Signs and symptoms include fever, enlargement of the tonsils, difficulty swallowing, and enlarged tender lymph nodes on the side of the neck 28.
Because appropriate treatment for tonsillitis depends on the cause, it’s important to get a prompt and accurate diagnosis. Surgery to remove tonsils, once a common procedure to treat tonsillitis, is usually performed only when bacterial tonsillitis occurs frequently, doesn’t respond to other treatments or causes serious complications.
Tonsillitis is most common in children over age two. Almost every child in the United States gets it at least once. Tonsillitis caused by bacteria is more common in kids ages 5-15 29. Tonsillitis caused by a virus is more common in younger children 30.
Adults can get tonsillitis, but it is not very common.
Is tonsillitis contagious ?
Although tonsillitis is not contagious, the viruses and bacteria that cause it are contagious. Frequent handwashing can help prevent spreading or catching the infections.
Symptoms of tonsillitis
Tonsillitis most commonly affects children between preschool ages and the mid-teenage years. Common signs and symptoms of tonsillitis include 31:
- Red, swollen tonsils
- White or yellow coating or patches on the tonsils
- Sore throat
- Difficult or painful swallowing
- Fever
- Enlarged, tender glands (lymph nodes) in the neck
- A scratchy, muffled or throaty voice
- Bad breath
- Stomachache, particularly in younger children
- Stiff neck
- Headache
In young children who are unable to describe how they feel, signs of tonsillitis may include:
- Drooling due to difficult or painful swallowing
- Refusal to eat
- Unusual fussiness
Peritonsillar abscess
Individuals often have severe throat pain, fever, drooling, foul breath, trismus (difficulty opening the mouth), and muffled voice quality, such as the hot potato voice (as if talking with a hot potato in his or her mouth) 29.
Unilateral bulging above and to the side of one of the tonsils when peritonsillar abscess exists. A stiff jaw, difficulty opening the mouth, and pain referred to the ear may be present in varying severity.
When to see a doctor
It’s important to get an accurate diagnosis if your child has symptoms that may indicate tonsillitis.
See your doctor if your child is experiencing:
- A sore throat that doesn’t go away within 24 to 48 hours
- Painful or difficult swallowing
- Extreme weakness, fatigue or fussiness
Get immediate care if your child has any of these symptoms:
- Difficulty breathing
- Extreme difficulty swallowing
- Drooling
Causes of Tonsillitis
Tonsillitis is most often caused by common viruses, but bacterial infections can also be the cause.
The herpes simplex virus, Streptococcus pyogenes (Group A Beta-Hemolytic Streptococci), Epstein-Barr virus, cytomegalovirus, adenovirus, and the measles virus cause most cases of acute pharyngitis and acute tonsillitis 29. Bacteria cause 15-30 percent of pharyngotonsillitis cases; Group A Beta-Hemolytic Streptococci is the cause for most bacterial tonsillitis (i.e., strep throat) 29. Other strains of strep and other bacteria also may cause tonsillitis.
Group A beta-hemolytic Streptococcus pyogene can cause tonsillitis (strep throat) associated with the presence of palatal petechiae (tiny hemorrhagic spots, of pinpoint to pinhead size, on the soft palate). Neck nodes may be enlarged. A fine red rash over the body suggests scarlet fever. Group A beta-hemolytic Streptococcus pyogene pharyngitis usually occurs in children 5-15 years old 29.
The possibility of infectious mononucleosis due to Epstein-Barr virus in an adolescent or younger child with acute tonsillitis, particularly when cervical, axillary, and/or groin nodes are tender. Severe lethargy, malaise, and low-grade fever accompany acute tonsillitis.
A grey membrane covering tonsils that are inflamed from an Epstein-Barr virus infection. This membrane can be removed without bleeding 29. Palatal petechiae (pinpoint spots on the soft palate) may also be seen with an Epstein-Barr virus infection.
Red swollen tonsils that may have small ulcers on their surfaces in individuals with herpes simplex virus tonsillitis 29.
Why do tonsils get infected ?
The tonsils are the immune system’s first line of defense against bacteria and viruses that enter your mouth. This function may make the tonsils particularly vulnerable to infection and inflammation. However, the tonsil’s immune system function declines after puberty — a factor that may account for the rare cases of tonsillitis in adults 32.
Risk factors for tonsillitis
Risk factors for tonsillitis include:
- Young age. Tonsillitis most often occurs in children, but rarely in those younger than age 2. Tonsillitis caused by bacteria is most common in children ages 5 to 15, while viral tonsillitis is more common in younger children.
- Frequent exposure to germs. School-age children are in close contact with their peers and frequently exposed to viruses or bacteria that can cause tonsillitis.
Complications of tonsillitis
Inflammation or swelling of the tonsils from frequent or ongoing (chronic) tonsillitis can cause complications such as:
- Difficulty breathing
- Disrupted breathing during sleep (obstructive sleep apnea)
- Difficulty swallowing
- Infection that spreads deep into surrounding tissue (tonsillar cellulitis)
- Infection that results in a collection of pus behind a tonsil (peritonsillar abscess)
Strep infection
If tonsillitis caused by group A streptococcus or another strain of streptococcal bacteria isn’t treated, or if antibiotic treatment is incomplete, your child has an increased risk of rare disorders such as 33:
- Rheumatic fever, an inflammatory disorder that affects the heart, joints and other tissues
- Poststreptococcal glomerulonephritis, an inflammatory disorder of the kidneys that results in inadequate removal of waste and excess fluids from blood
Tests and diagnosis for tonsillitis
Your child’s doctor will start with a physical exam that will include:
- Using a lighted instrument to look at your child’s throat and likely his or her ears and nose, which may also be sites of infection
- Checking for a rash known as scarlatina, which is associated with some cases of strep throat (Group A beta-hemolytic Streptococcus pyogene)
- Gently feeling (palpating) your child’s neck to check for swollen glands (lymph nodes)
- Listening to his or her breathing with a stethoscope
- Checking for enlargement of the spleen (for consideration of mononucleosis, which also inflames the tonsils)
Throat swab
With this simple test, the doctor rubs a sterile swab over the back of your child’s throat to get a sample of secretions. The sample will be checked for streptococcal bacteria.
If the rapid in-clinic test comes back positive, then your child almost certainly has a bacterial infection. If the test comes back negative, then your child likely has a viral infection. Your doctor will wait, however, for the more reliable out-of-clinic lab test to determine the cause of the infection.
Complete blood cell count (CBC)
Your doctor may order a CBC with a small sample of your child’s blood. The result of this test, which can often be completed in a clinic, produces a count of the different types of blood cells. The profile of what’s elevated, what’s normal or what’s below normal can indicate whether an infection is more likely caused by a bacterial or viral agent. A CBC is not often needed to diagnose strep throat. However, if the strep throat lab test is negative, the CBC may be needed to help determine the cause of tonsillitis.
Treatments and drugs for tonsillitis
Home remedy and home care
Whether tonsillitis is caused by a viral or bacterial infection, at-home care strategies can make your child more comfortable and promote better recovery.
If a virus is the expected cause of tonsillitis, these strategies are the only treatment. Your doctor won’t prescribe antibiotics. Your child will likely be better within seven to 10 days.
At-home care strategies to use during the recovery time include the following:
- Encourage rest. Encourage your child to get plenty of sleep.
- Provide adequate fluids. Give your child plenty of water to keep his or her throat moist and prevent dehydration.
- Provide comforting foods and beverage. Warm liquids — broth, caffeine-free tea or warm water with honey — and cold treats like ice pops can soothe a sore throat.
- Prepare a saltwater gargle. If your child can gargle, a saltwater gargle of 1 teaspoon (5 milliliters) of table salt to 8 ounces (237 milliliters) of warm water can help soothe a sore throat. Have your child gargle the solution and then spit it out.
- Humidify the air. Use a cool-air humidifier to eliminate dry air that may further irritate a sore throat, or sit with your child for several minutes in a steamy bathroom.
- Offer lozenges. Children older than age 4 can suck on lozenges to relieve a sore throat.
- Avoid irritants. Keep your home free from cigarette smoke and cleaning products that can irritate the throat.
Treat pain and fever. Talk to your doctor about using ibuprofen (Advil, Children’s Motrin, others) or acetaminophen (Tylenol, others) to minimize throat pain and control a fever. Low fevers without pain do not require treatment.
- Except for certain diseases, children and teenagers should not take aspirin because when used to treat symptoms of cold or flu-like illnesses, it has been linked to Reye’s syndrome, a rare but potentially life-threatening condition.
Antibiotics
If tonsillitis is caused by a bacterial infection, your doctor will prescribe a course of antibiotics. Penicillin taken by mouth for 10 days is the most common antibiotic treatment prescribed for tonsillitis caused by group A streptococcus. If your child is allergic to penicillin, your doctor will prescribe an alternative antibiotic.
Your child must take the full course of antibiotics as prescribed even if the symptoms go away completely. Failure to take all of the medication as directed may result in the infection worsening or spreading to other parts of the body. Not completing the full course of antibiotics can, in particular, increase your child’s risk of rheumatic fever and serious kidney inflammation.
Surgery
Surgery to remove tonsils (tonsillectomy) may be used to treat frequently recurring tonsillitis, chronic tonsillitis or bacterial tonsillitis that doesn’t respond to antibiotic treatment. Frequent tonsillitis is generally defined as:
- More than seven episodes in one year
- More than four to five episodes a year in each of the preceding two years
- More than three episodes a year in each of the preceding three years
A tonsillectomy may also be performed if tonsillitis results in difficult-to-manage complications, such as:
- Obstructive sleep apnea
- Breathing difficulty
- Swallowing difficulty, especially meats and other chunky foods
- An abscess that doesn’t improve with antibiotic treatment
Tonsillectomy is usually done as an outpatient procedure, unless your child is very young, has a complex medical condition or if complications arise during surgery. That means your child should be able to go home the day of the surgery. A complete recovery usually takes seven to 14 days.
- How do the tonsils work ? PubMed Health, National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072590/[↩]
- Peritonsillar Abscess. Am Fam Physician. 2008 Jan 15;77(2):199-202. http://www.aafp.org/afp/2008/0115/p199.html[↩]
- Berkovitz BK, ed. Pharynx. In: Standring S, ed. Grays Anatomy. The Anatomical Basis of Clinical Practice. 39th ed. New York, NY: Churchill Livingstone, 2005:623–625.[↩]
- Khayr W, Taepke J. Management of peritonsillar abscess: needle aspiration versus incision and drainage versus tonsillectomy. Am J Ther. 2005;12(4):344–350.[↩]
- Formation of the tonsillar corpuscle. Perry ME, Slípka J. Funct Dev Morphol. 1993; 3(3):165-8. https://www.ncbi.nlm.nih.gov/pubmed/8167395/[↩]
- Westermann J. Organe des Abwehrsystems. Berlin, Heidelberg: Springer; 2010. pp. 361–362.[↩][↩]
- Cell mediated immune responses to bacterial antigens on human mucosal surfaces. Drucker M, Drucker I, Neter E, Bernstein J, Ogra PL. Adv Exp Med Biol. 1978; 107():479-88. https://www.ncbi.nlm.nih.gov/pubmed/311141/[↩]
- Structure of the crypt epithelium in human palatine tonsils. Perry ME, Jones MM, Mustafa Y. Acta Otolaryngol Suppl. 1988; 454():53-9. https://www.ncbi.nlm.nih.gov/pubmed/3223268/[↩]
- Morphology and immunology of the human palatine tonsil. Nave H, Gebert A, Pabst R. Anat Embryol (Berl). 2001 Nov; 204(5):367-73. https://www.ncbi.nlm.nih.gov/pubmed/11789984/[↩]
- Richardson, MA. Sore throat, tonsillitis, and adenoiditis. Med Clin North Am. 1999;83:75–83.[↩]
- Jung, KY, Lim, HH, Choi, G. Age-related changes of IgA immunocytes and serum and salivary IgA after tonsillectomy. Acta Otolaryngol Suppl. 1996;523:115–119.[↩]
- Early stage impacts of tonsillectomy on immune functions of children. Kaygusuz I, Gödekmerdan A, Karlidag T, Keleş E, Yalçin S, Aral I, Yildiz M. Int J Pediatr Otorhinolaryngol. 2003 Dec; 67(12):1311-5. https://www.ncbi.nlm.nih.gov/pubmed/14643474/[↩]
- Evaluation of long-term impacts of tonsillectomy on immune functions of children: a follow-up study. Kaygusuz I, Alpay HC, Gödekmerdan A, Karlidag T, Keles E, Yalcin S, Demir N. Int J Pediatr Otorhinolaryngol. 2009 Mar; 73(3):445-9. https://www.ncbi.nlm.nih.gov/pubmed/19150575/[↩]
- [The microbe colonization of the palatine tonsils of healthy school age children]. Mücke W, Huber HC, Ritter U. Zentralbl Hyg Umweltmed. 1994 Aug; 196(1):70-4. https://www.ncbi.nlm.nih.gov/pubmed/7802898/[↩]
- Tonsil surface and core cultures in recurrent tonsillitis: prevalence of anaerobes and beta-lactamase producing organisms. Mitchelmore IJ, Reilly PG, Hay AJ, Tabaqchali S. Eur J Clin Microbiol Infect Dis. 1994 Jul; 13(7):542-8. https://www.ncbi.nlm.nih.gov/pubmed/7805681/[↩]
- Molecular mapping to species level of the tonsillar crypt microbiota associated with health and recurrent tonsillitis. Jensen A, Fagö-Olsen H, Sørensen CH, Kilian M. PLoS One. 2013; 8(2):e56418. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3578847/[↩]
- Jensen A, Fagö-Olsen H, Sørensen CH, Kilian M. Molecular Mapping to Species Level of the Tonsillar Crypt Microbiota Associated with Health and Recurrent Tonsillitis. Xu P, ed. PLoS ONE. 2013;8(2):e56418. doi:10.1371/journal.pone.0056418. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3578847/[↩][↩]
- Pores of the palatine tonsillar crypt and pharyngeal tonsillar recess–a scanning electron microscopic study. Auris Nasus Larynx. 1979;6(1):23-30. https://www.ncbi.nlm.nih.gov/pubmed/549561[↩]
- The cells in tonsillar crypts. Clin Otolaryngol Allied Sci. 1982 Feb;7(1):35-44. https://www.ncbi.nlm.nih.gov/pubmed/7060282[↩]
- Functional morphology of tonsillar crypts in recurrent tonsillitis. Acta Otolaryngol Suppl. 1984;416:7-19. https://www.ncbi.nlm.nih.gov/pubmed/6598276[↩]
- Brandtzaeg, P. In: Immune functions and immunopathology of palatine and nasopharyngeal tonsils. Bernstein, JM, Ogra, PL, eds. Immunology of the Ear. New York, NY: Raven Press; 1987:63–106. [↩]
- Brandtzaeg, P. In: Immune functions and immunopathology of palatine and nasopharyngeal tonsils. Bernstein, JM, Ogra, PL, eds. Immunology of the Ear. New York, NY: Raven Press; 1987:63–106.[↩][↩]
- Perry ME. The specialised structure of crypt epithelium in the human palatine tonsil and its functional significance. Journal of Anatomy. 1994;185(Pt 1):111-127. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1166820/pdf/janat00135-0110.pdf[↩]
- Brandtzaeg, P. Immunology of tonsils and adenoids: everything the ENT surgeon needs to know. Int J Pediatr Otorhinolaryngol. 2003;67:S69–S76.[↩]
- Friday, GA, Paradise, JL, Rabin, BS. Serum immunoglobulin changes in relation to tonsil and adenoid surgery. Ann Allergy. 1992;69:225–230.[↩]
- Paulussen, CCJ, Claes, G, Jorissen, M. Adenoids and tonsils, indications for surgery and immunological consequences of surgery. Acta Otorhinolaryngol Belg. 2000;54:403-408.[↩]
- Tonsillolith, Not Just a Stone but a Living Biofilm. Otolaryngology-Head and Neck Surgery Vol 141, Issue 3, pp. 316 – 321. 10.1016/j.otohns.2009.05.019[↩]
- Tonsillitis. Mayo Clinic. http://www.mayoclinic.org/diseases-conditions/tonsillitis/basics/definition/con-20023538[↩]
- Tonsillitis. American Academy of Otolaryngology — Head and Neck Surgery. http://www.entnet.org/?q=node/1447[↩][↩][↩][↩][↩][↩][↩]
- Tonsillitis. Medline Plus. https://medlineplus.gov/tonsillitis.html[↩]
- Tonsillitis Symptoms. Mayo Clinic. http://www.mayoclinic.org/diseases-conditions/tonsillitis/basics/symptoms/con-20023538[↩]
- Tonsillitis Causes. Mayo Clinic. http://www.mayoclinic.org/diseases-conditions/tonsillitis/basics/causes/con-20023538[↩]
- Tonsillitis Complications. Mayo Clinic. http://www.mayoclinic.org/diseases-conditions/tonsillitis/basics/complications/con-20023538[↩]





{kind=link}