Contents
- What is portal hypertension
- Portal hypertension causes
- Portal hypertension pathophysiology
- Portal hypertension signs and symptoms
- Portal hypertension complications
- Portal hypertension diagnosis
- Portal hypertension treatment
- Living with portal hypertension
- Portal hypertension diet
- Portal hypertension prognosis
What is portal hypertension
Your liver receives blood from two sources: about 70% from the hepatic portal vein and 30% from the hepatic arteries. The hepatic portal vein or portal vein is a blood vessel that carries blood from your gastrointestinal tract, as well as from your gallbladder, pancreas and spleen to your liver (Figure 1). This blood contains nutrients and toxins extracted from your digested contents. Intestinal blood is richly laden with nutrients for a few hours following a meal. The hepatic portal system gives your liver first claim to these nutrients before the blood is distributed to the rest of your body. The hepatic portal system also allows your blood to be cleansed of bacteria and toxins picked up from your intestines, an important function of your liver. Approximately 70% of total liver blood flow is through your portal vein, with the remainder coming from your hepatic artery. The hepatic portal system is called a portal system because it connects capillaries of your intestines and other digestive organs to modified capillaries called hepatic sinusoids of your liver. After entering the liver, the portal vein divides into right and left branches and then into tiny channels (hepatic sinusoids) that run through your liver. When blood leaves your liver and returns to your heart, it flows back into the general circulation through the hepatic vein (Figure 2).
The hepatic portal venous system principal veins are as follows:
- Inferior mesenteric vein receives blood from the rectum and distal part of the colon. It converges in a fanlike array in the mesentery and empties into the splenic vein.
- Superior mesenteric vein receives blood from the entire small intestine, ascending colon, transverse colon, and stomach. It, too, exhibits a fanlike arrangement in the mesentery and then joins the splenic vein to form the hepatic portal vein.
- Splenic vein drains the spleen and travels across the abdominal cavity toward the liver. Along the way, it picks up pancreatic veins from the pancreas, then the inferior mesenteric vein, then ends where it meets the superior mesenteric vein.
- Portal vein is usually formed by the confluence of the superior mesenteric, splenic veins, inferior mesenteric, left, right gastric veins and the pancreatic vein. It travels about 8 cm upward and to the right, receives the cystic vein from the gallbladder, then enters the inferior surface of the liver. In the liver, it ultimately leads to the innumerable microscopic liver sinusoids. Blood from the liver sinusoids empties into the hepatic veins and they empty into the inferior vena cava (IVC). Note that the portal vein is not a true vein, because it conducts blood to capillary beds in your liver and not directly to your heart.
- The left and right gastric veins form an arc along the lesser curvature of the stomach and empty into the hepatic portal vein.
Portal hypertension is high blood pressure (hypertension) or an increase in portal venous pressure or hepatic venous pressure gradient (HVPG) above the nominal value of 1 to 5 mmHg in your hepatic portal system (the portal vein and its branches – the superior mesenteric vein, splenic vein, inferior mesenteric vein, left and right gastric veins and the pancreatic vein), that drain from most of your intestine to your liver (Figure 4) 1. The gold standard for assessing portal hypertension is the hepatic venous pressure gradient (HVPG), which is the pressure gradient between the portal vein and inferior vena cava (IVC) 2, 3. Hepatic venous pressure gradient (HVPG) is measured by retrograde insertion of a balloon‐tipped central vein catheter into a main hepatic vein (Figure 6) 4, 5, 6, 7. Portal hypertension is defined as a sustained increase in the pressure gradient between portal and systemic circulation 8. In healthy individuals, the normal hepatic venous pressure gradient (HVPG) is 1 to 5 mmHg. A hepatic venous pressure gradient (HVPG) of 6 to 10 mmHg between the portal and hepatic veins or inferior vena cava (IVC) suggests the presence of mild subclinical portal hypertension in most cases 9, 10, 6. When the hepatic venous pressure gradient (HVPG) is greater than 10 mmHg, portal hypertension becomes clinically significant 11. A hepatic venous pressure gradient (HVPG) above 12 mmHg usually reflects decompensated cirrhosis, which is manifested by the development of porto-systemic shunting, variceal rupture and bleeding 12, 13. Moreover, it has been reported that the probability of survival in cirrhotic patients with HVPG above 16 mmHg was below 70% of those patients who have an HVPG below this level and that this poor survival rate was related to Child-Pugh class 14.
For cirrhotic patients awaiting liver transplantation, for every 1 mmHg increase in hepatic venous pressure gradient (HVPG), the risk of death is increased by 3% 15. Hepatic venous pressure gradient (HVPG) > 5 mmHg is associated with chronic hepatitis progression and hepatitis recurrence after liver transplantation 16, 17. Hepatic venous pressure gradient (HVPG) > 10 mmHg represents clinically significant portal hypertension, predicts the development of varices and ascites, and high risk of decompensation and recurrence of liver cancer after hepatectomy 18, 19, 20, 21, 7. Hepatic venous pressure gradient (HVPG) > 12 mmHg significantly increases the risk of variceal bleeding 22; when HPVG > 16 mmHg, the risk of death was significantly increased 23.
Portal hypertension leads to the development of new veins called collateral vessels that divert portal blood to the systemic circulation, bypassing your liver 24. These veins or collateral vessels directly connect the portal blood vessels to veins that take blood away from the liver into the general circulation. Because of this bypass, substances such as toxins that are normally removed from your blood by your liver can pass into the general circulation. Collateral vessels develop at specific places. The most important are located at the lower end of the esophagus and at the upper part of the stomach. Here, the vessels enlarge and become full of twists and turns—that is, they become varicose veins in the esophagus (esophageal varices) or stomach (gastric varices). These enlarged vessels are fragile and prone to bleeding, sometimes seriously and occasionally with fatal results. Other collateral vessels may develop on the abdominal wall and at the rectum.
Portal hypertension often causes your spleen to enlarge because the pressure interferes with blood flow from your spleen into the portal blood vessels. When the spleen enlarges, the number (count) of white blood cells can decrease (leukopenia) increasing your risk of infections and the number (count) of platelets can decrease (thrombocytopenia) increasing your risk of bleeding. If your spleen is not enlarged on physical examination or imaging studies, the diagnosis of portal hypertension should be questioned 9.
Increased pressure in the portal blood vessels may also cause protein-containing (ascitic) fluid to leak from the surface of your liver and intestine and to accumulate within the abdomen. This condition is called ascites (a condition where fluid builds up in your abdomen).
Portal hypertension can lead to a multitude of signs and symptoms that include bleeding from the abnormally dilated veins (variceal bleeding) found throughout your gastrointestinal tract, such as bleeding in your digestive tract e.g., your esophagus, stomach, and rectum, ascites (a condition where fluid builds up in your abdomen), brain dysfunction due to liver dysfunction (hepatic encephalopathy), hepatorenal syndrome, and spontaneous bacterial peritonitis 25. Bleeding from the abnormally dilated veins (variceal bleeding), resulting from the development of dilated and fragile veins in the esophagus or stomach, is one of the most severe complications and can be life-threatening if not promptly managed.
There are numerous causes of portal hypertension, with the most common cause of portal hypertension being cirrhosis, a chronic liver disease characterized by extensive scar tissues (fibrosis) and nodular regeneration that distort the structure of the liver and impairs its function. Cirrhosis is the most common cause of portal hypertension, accounting for approximately 90% of portal hypertension cases worldwide 26.
Cirrhosis is most often caused by:
- Chronic hepatitis C and hepatitis B (hepatitis that has lasted at least 6 months)
- Drinking large amounts of alcohol over a long period of time
- Nonalcoholic fatty liver disease (NAFLD). This occurs when too much fat builds up in your liver. People who are overweight or have obesity are more at risk for this disease. People with diabetes, high cholesterol, or high blood pressure also are at risk.
- Certain genetic diseases, such as Wilson disease or autoimmune hepatitis.
- Continued exposure to toxic chemicals.
- Infections caused by parasites.
- Continued use of certain medicines.
- Certain congenital heart defects or chronic heart failure.
Other causes of portal hypertension include hepatic vein thrombosis, schistosomiasis, portal vein thrombosis, and congenital abnormalities 27.
To diagnose cirrhosis, your doctor will begin with a physical exam. They also will review your symptoms, health history, and lifestyle. Tests are needed to check your liver and confirm diagnosis. These include blood and imaging tests. Blood tests can detect hepatitis, abnormal enzyme levels, or abnormal blood cells. Imaging tests take pictures of your liver. In some cases, your doctor may do a biopsy on your liver. This involves taking a sample of liver tissue to look at it in the lab.
If you have cirrhosis, your doctor will likely check for portal hypertension. They will check your abdomen for extra fluid (ascites). Your doctor will check for swelling or pressure in the blood vessels around your portal vein. They may perform other tests to diagnose portal hypertension. Your doctor also may do an endoscopy (using a lighted camera scope to look at your digestive system).
The goal for cirrhosis treatment is to relieve symptoms and prevent further damage. Treatment also can avoid or manage complications caused by cirrhosis. With this condition, blood can’t flow normally through the portal vein. The blood has to return to your heart through other blood vessels. Most often it goes through blood vessels in your stomach, esophagus, or intestines. These vessels then swell due to the increased amount of blood flowing through them. This puts pressure on the vessels and can cause them to burst. Bleeding from a broken blood vessel is serious and can be fatal.
Your doctor may prescribe medicine to help prevent your blood vessels from bursting. These medicines have some side effects and may interact with other medicines. They’re not suitable for everyone. Your doctor may prescribe medicine to lower your blood pressure if you have portal hypertension. If you have hepatitis, your doctor will prescribe an antiviral medicine. You may need other medicines, depending on the cause of cirrhosis.
If medicine isn’t enough, you may need surgery. Surgery can decrease pressure by interrupting the blood flow in your blood vessels. The doctor or surgeon will insert a long tube through your mouth to your stomach. Then, they will place rubber bands or hardened chemicals in the swollen blood vessels to block them off. Another type of procedure, called transjugular intrahepatic portosystemic shunt or TIPS, may be done in some cases.
People who have portal hypertension may need surgery to connect certain blood vessels. If a blood vessel bursts, you’ll need surgery to stop the bleeding and repair it.
If surgery doesn’t work or you have liver failure, you may need a liver transplant.
Figure 1. Hepatic portal venous system
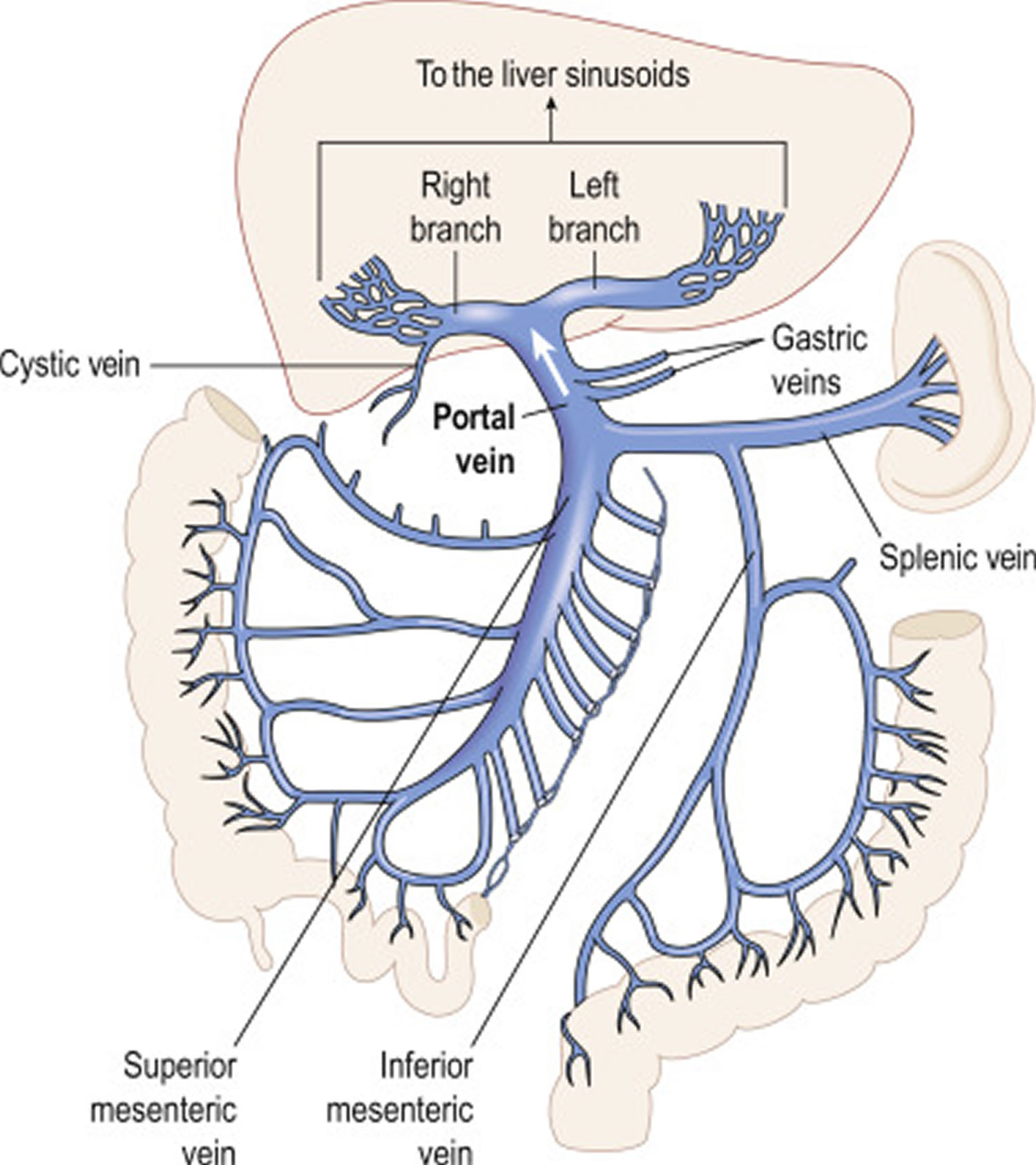
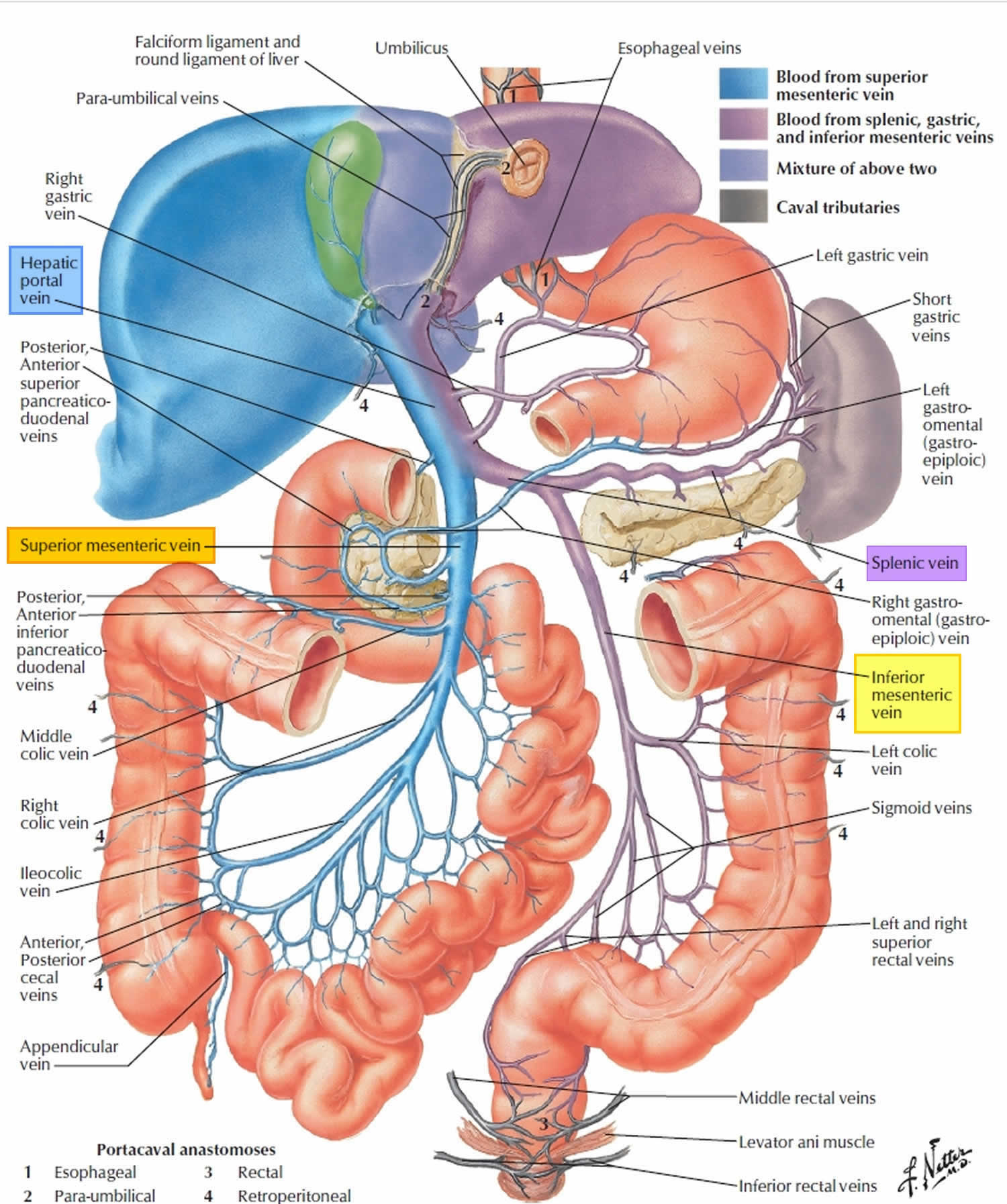
Figure 2. Portal Vein
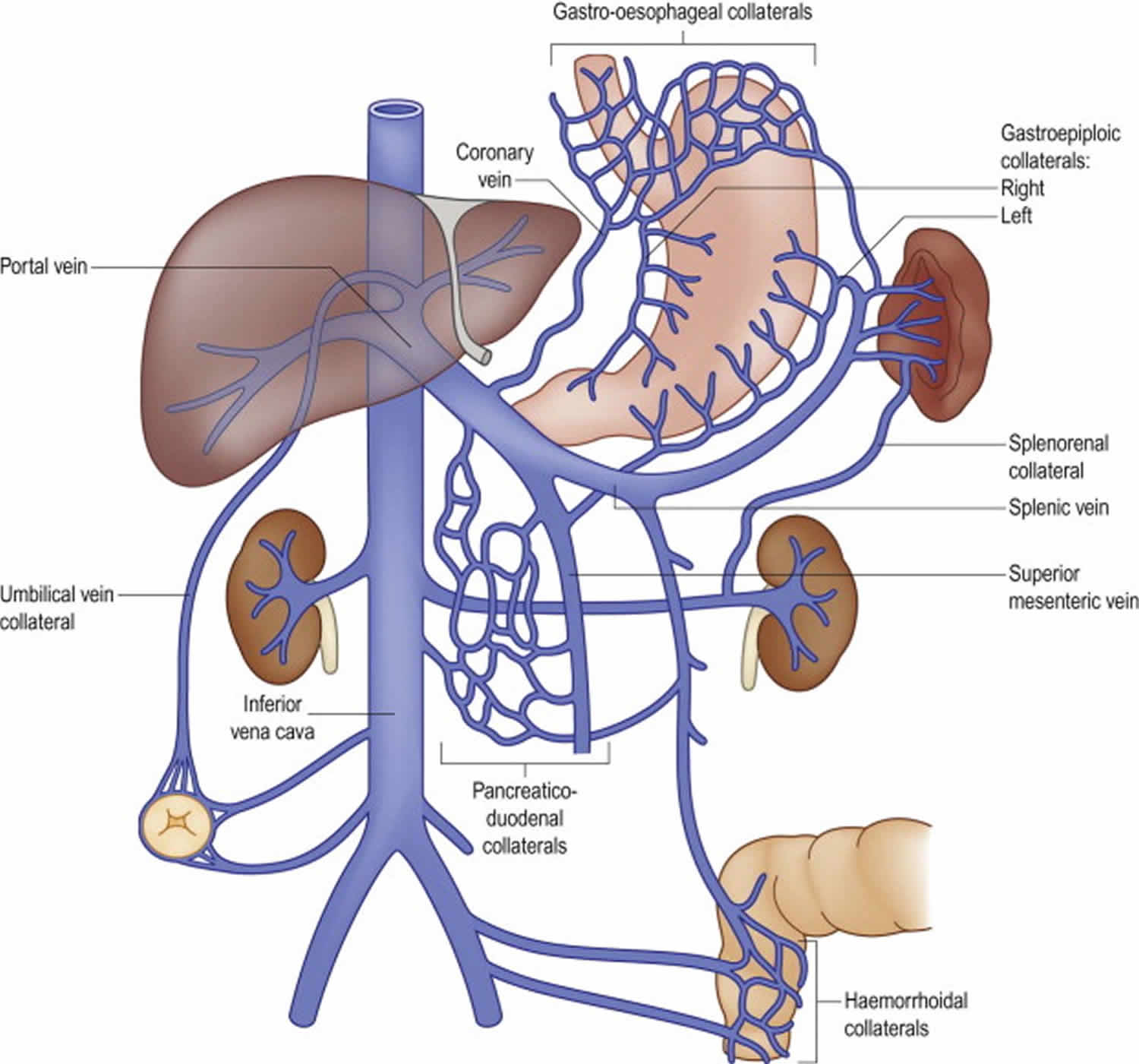
Figure 3. Microscopic anatomy of the liver
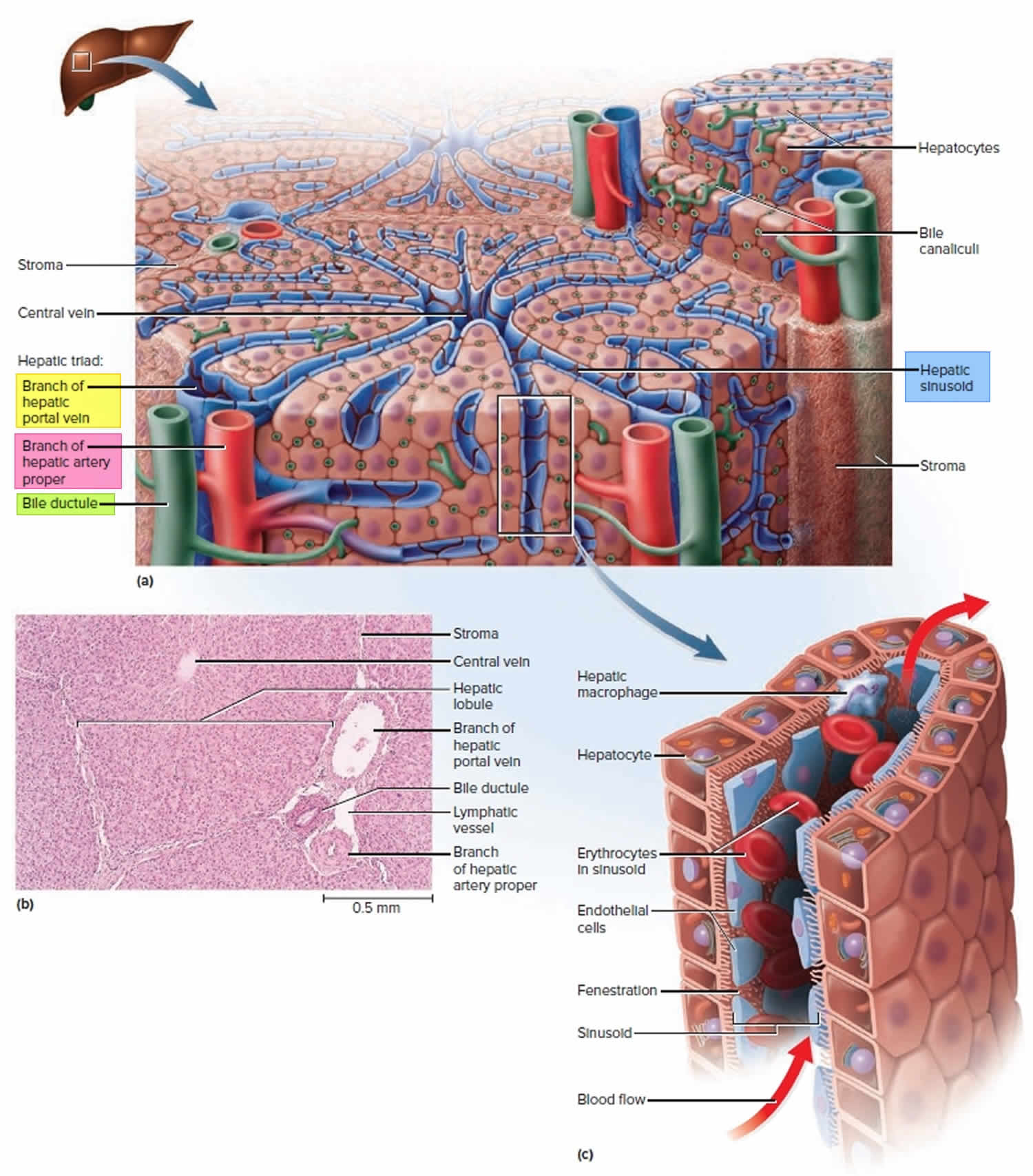
Figure 4. Portal hypertension
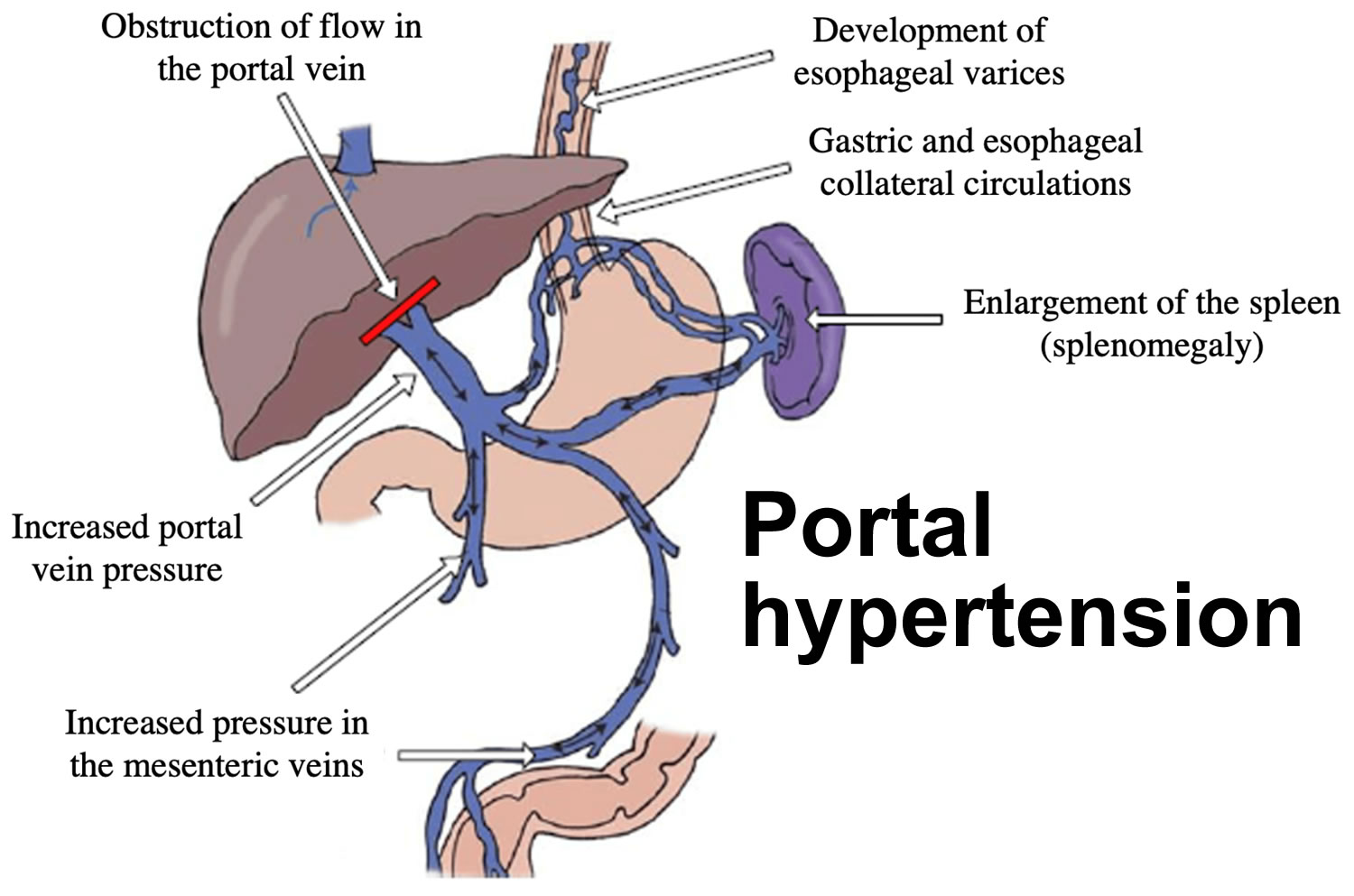
Figure 5. Portal hypertension signs and symptoms
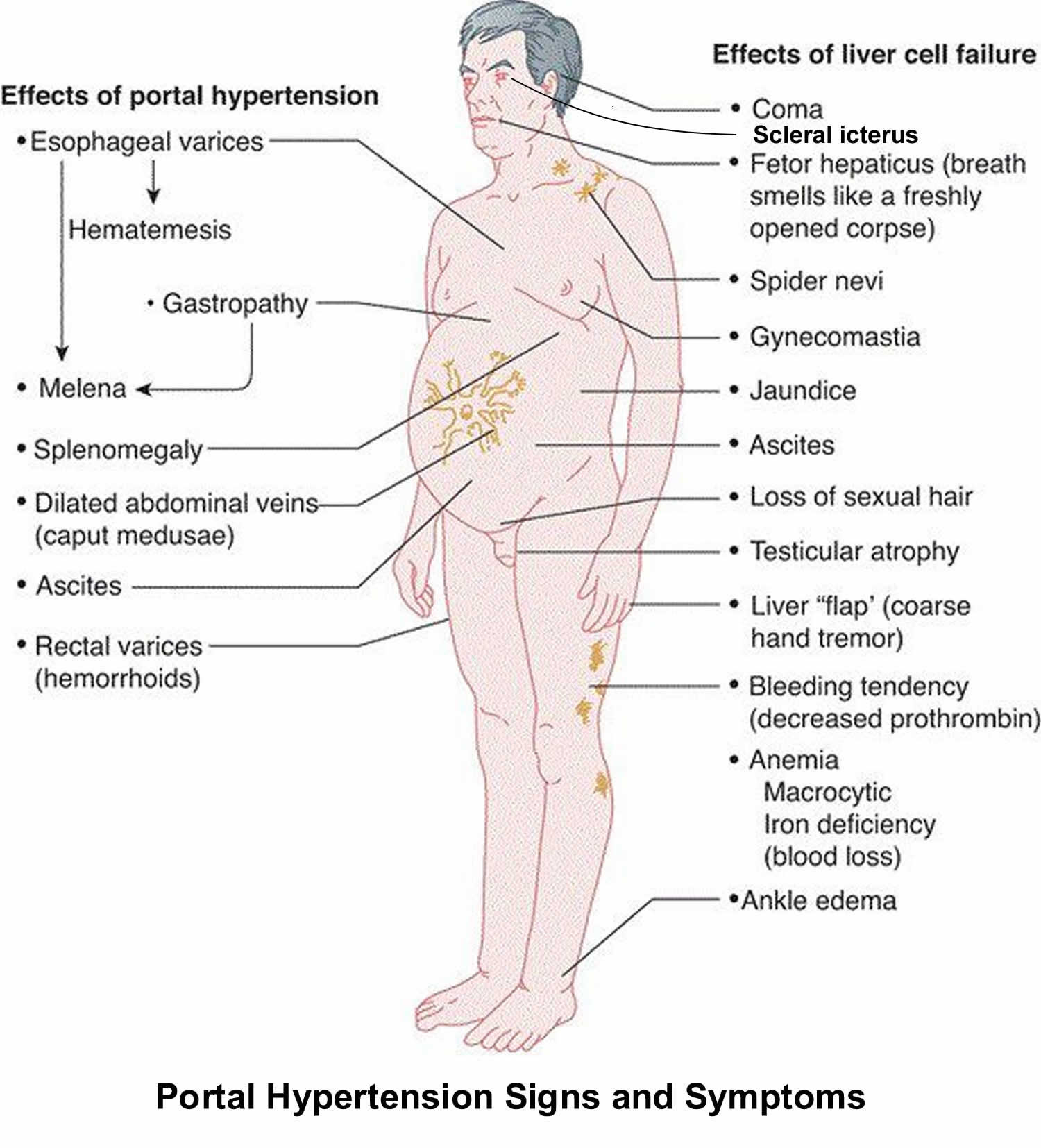
Figure 6. Hepatic venous pressure gradient (HVPG) measurement
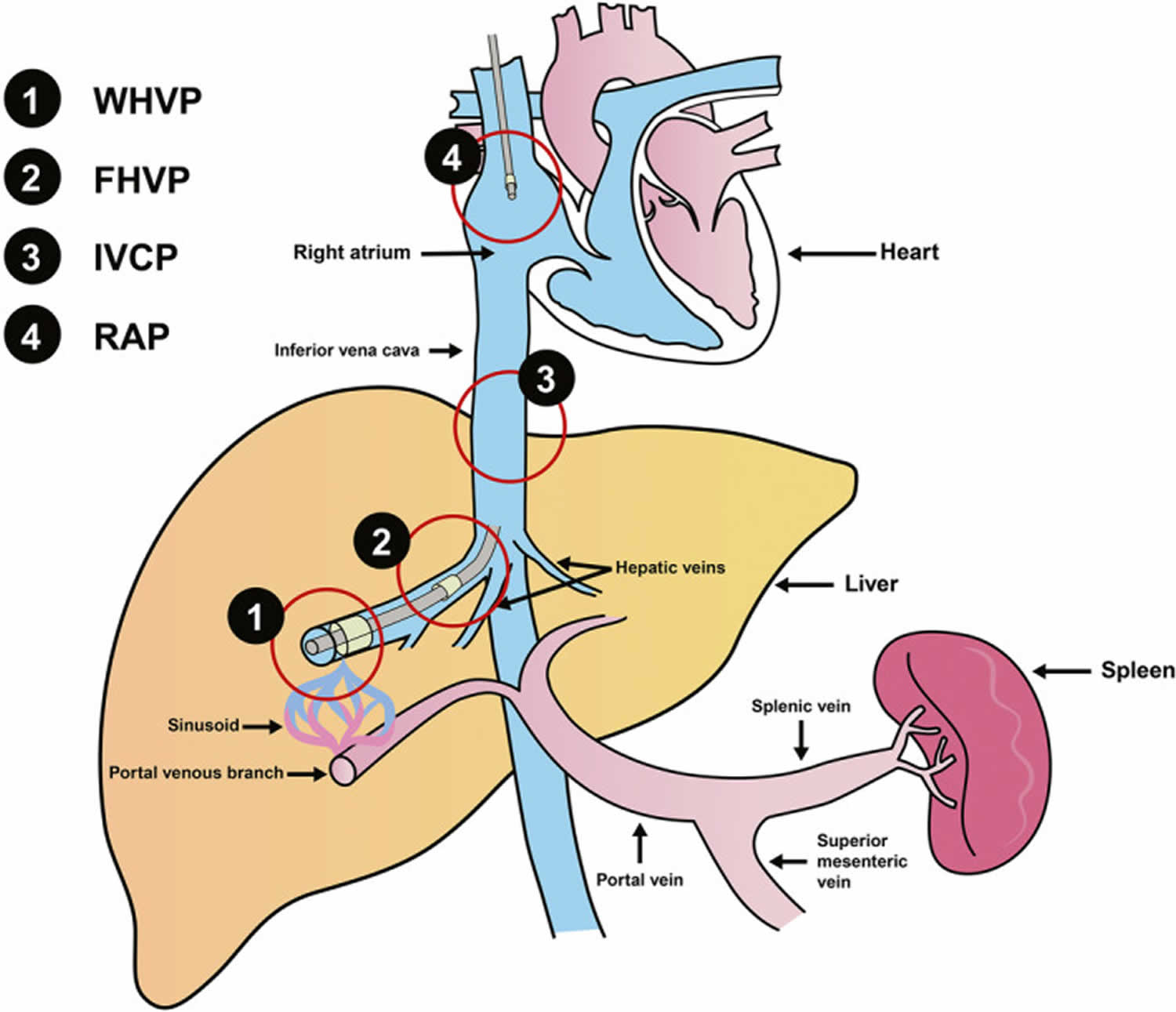
Footnotes: Hepatic venous pressure gradient (HVPG) is measured by retrograde insertion of a balloon‐tipped central vein catheter into a main hepatic vein. Hepatic venous pressure gradient (HVPG) represents the difference between the occluded hepatic sinusoidal capillary network (wedged hepatic venous) pressure and the free hepatic venous (systemic) pressure.
Abbreviations: HVPG = hepatic venous pressure gradient; FHVP = free hepatic venous pressure; IVCP= inferior vena cava pressure; RAP = right atrium pressure; WHVP = wedged hepatic venous pressure.
[Source 28 ]Portal hypertension causes
Portal hypertension has different causes and results mainly from increased resistance to blood flow in the portal vein. Portal hypertension develops when resistance to portal blood flow increases. A common cause of this resistance is disease within the liver as in cirrhosis. Uncommon causes include blockage of the splenic or portal vein and impaired hepatic venous outflow, such as prehepatic in portal vein thrombosis or posthepatic in the case of constrictive pericarditis or Budd-Chiari syndrome. Increased flow volume is a rare cause, although it often contributes to portal hypertension in cirrhosis and in hematologic disorders that cause massive splenomegaly.
The most common cause of portal hypertension is cirrhosis 26.
Cirrhosis is most often caused by 29:
- Long-term, or chronic infection with the hepatitis C and hepatitis B viruses.
- Alcohol-associated liver disease, which is damage to the liver and its function from drinking too much alcohol.
- Nonalcoholic fatty liver disease (NAFLD). This occurs when too much fat builds up in your liver. People who are overweight or have obesity are more at risk for nonalcoholic fatty liver disease (NAFLD). People with diabetes, metabolic syndrome, high cholesterol, or high blood pressure are also at risk.
Some less common causes of cirrhosis include 29:
- Autoimmune hepatitis, a disease in which your immune system attacks your liver
- Diseases that damage, destroy, or block bile ducts, such as primary biliary cholangitis and primary sclerosing cholangitis
- Inherited liver diseases: Diseases passed from parents to children through genes that affect how the liver works such as Wilson disease, hemochromatosis, and alpha-1 antitrypsin deficiency
- Long-term use of certain medicines and high doses of vitamin A daily
- Chronic heart failure or congenital heart defects with liver congestion, a condition in which blood flow out of the liver is slowed.
- Continued exposure to toxic chemicals.
- Infections caused by parasites.
Other causes of portal hypertension include 27, 30:
- Splenic or portal vein thrombosis
- Arteriovenous fistula
- Massive splenomegaly caused by a primary hematologic disorder
- Idiopathic portal hypertension
- Other periportal disorders (eg, primary biliary cholangitis, sarcoidosis, congenital hepatic fibrosis)
- Schistosomiasis
- Hepatic sinusoidal obstruction syndrome (hepatic veno-occlusive disease)
- Hepatic vein thrombosis (Budd-Chiari syndrome)
- Obstruction of the inferior vena cava
- Resistance to right heart filling
- Constrictive pericarditis
- Restrictive cardiomyopathy.
Portal hypertension pathophysiology
In cirrhosis, liver scarring (fibrosis) and regeneration increase resistance in the liver sinusoids and terminal portal venules. However, other potentially reversible factors contribute; they include contractility of sinusoidal lining cells, production of vasoactive substances (eg, endothelins, nitric oxide), various systemic mediators of arteriolar resistance, and possibly swelling of liver cells 30.
Over time, portal hypertension creates portosystemic venous collaterals. They may slightly decrease portal vein pressure but can cause complications. Engorged serpentine submucosal vessels (varices) in the distal esophagus and sometimes in the gastric fundus can rupture, causing sudden, catastrophic gastrointestinal bleeding. Bleeding rarely occurs unless the portal pressure gradient is greater than 12 mm Hg 30. Gastric mucosal vascular congestion (portal hypertensive gastropathy) can cause acute or chronic bleeding independent of varices. Visible abdominal wall collaterals are common; veins radiating from the umbilicus (caput medusae) are much rarer and indicate extensive flow in the umbilical and periumbilical veins. Collaterals around the rectum can cause rectal varices that can bleed.
Portosystemic collaterals shunt blood away from the liver. Thus, less blood reaches the liver when portal flow increases (diminished hepatic reserve). In addition, toxic substances from the intestine are shunted directly to the systemic circulation, contributing to portosystemic encephalopathy. Venous congestion within visceral organs due to portal hypertension contributes to ascites via altered Starling forces. Splenomegaly and hypersplenism commonly occur as a result of increased splenic vein pressure. Thrombocytopenia, leukopenia, and, less commonly, hemolytic anemia may result.
Portal hypertension is often associated with a hyperdynamic circulation. Mechanisms are complex and seem to involve altered sympathetic tone, production of nitric oxide and other endogenous vasodilators, and enhanced activity of humoral factors (eg, glucagon).
Portal hypertension signs and symptoms
If you have an advanced liver disease, such as cirrhosis, you have an increased risk of developing portal hypertension. Portal hypertension itself does not cause symptoms (asymptomatic), but some of its consequences do. If a large amount of fluid accumulates in your abdomen called ascites, your abdomen swells (distends), sometimes noticeably and sometimes enough to make your abdomen greatly enlarged and taut. The large amount of fluid accumulates in your abdomen (ascites) can be uncomfortable or painful. An enlarged spleen may cause a vague sense of discomfort in the upper left part of your abdomen.
The varicose veins in the esophagus and stomach bleed easily and sometimes massively. Then, people may vomit blood or dark material that resembles coffee grounds. Stools may be dark and tarry. Much less commonly, varicose veins in the rectum bleed. Then, stools may contain red blood. Bleeding from these veins may result in death.
Collateral blood vessels may be visible on the skin of the abdomen (Caput medusa) or around your rectum.
When substances that are normally removed by your liver pass into the general circulation and reach your brain, they may cause confusion or drowsiness (hepatic encephalopathy). Because most people with portal hypertension also have severe liver malfunction, they may have symptoms of liver failure, such as a tendency to bleed.
Portal hypertension symptoms and signs include:
- Gastrointestinal bleeding: You may notice blood in the stools, or you may vomit blood if any large vessels around your stomach that developed due to portal hypertension rupture.
- Ascites: When fluid accumulates in your abdomen, causing swelling. Symptoms of ascites include:
- Early feeling of fullness
- Increase in size of abdomen
- Feeling out of breath (if the fluid begins pushing on your lungs)
- Encephalopathy, confusion, difficulty thinking, memory loss, personality changes, fogginess in thinking
- Jaundice, the yellowing of the skin and the whites of the eyes
- Edema, (swelling) of the legs
- Caput medusa, a visible network of dilated veins surrounding your belly button.
As liver function gets worse, people with cirrhosis may have other symptoms, including 31:
- bruising and bleeding easily
- internal bleeding due to the bursting of enlarged veins—called varices—in the esophagus, stomach, or intestines
- swelling in the lower legs, ankles, or feet, called edema
- severe itchy skin
- darkening of the color of the urine.
Portal hypertension complications
When portal hypertension reaches a certain level, it can cause complications, such as 32:
- Ascites. Ascites is buildup of fluid in your abdomen or belly. Patients with chronic liver disease often develop ascites, though it may be caused by other factors. Mechanism of ascites in portal hypertension, showing leaking around the stomach, colon and intestine. Ascites can lead to a serious infection called peritonitis, in the space that surrounds the liver and intestines.
- Edema. Edema also known as fluid retention, is a condition where fluid builds up in your body’s tissues, causing swelling. It can affect the whole body or just one part, and is most common in your legs, ankles and feet.
- Varices (enlarged veins). Varices are varicose veins in the esophagus, stomach, or intestines as a result of portal hypertension. This is often because your liver tissue is scarred and blood cannot flow through normally. As the portal blood is rerouted due to the increased resistance, varices develop. In patients with cirrhosis, most often the bleeding is related to esophageal varices, which are enlarged veins in your esophagus. Your doctor can view them during an endoscopy (internal viewing of your gastrointestinal tract) or other imaging study. Acute bleeding from internal bleeding if the varices burst in patients with portal hypertension requires immediate attention in order to control the bleeding and prevent it from recurring.
- Upon diagnosis of cirrhosis, varices are detected in about 30% and 60% of compensated and decompensated patients, respectively 33, 34, 35. Patients without varices develop them at a rate of 8% per year. Long term follow-up studies revealed up to 90% of the cirrhotic patients will eventually develop varices. There is a 10%-30% risk for variceal rupture within the first year of diagnosis 36. Despite the advances in the management of variceal bleeding in the past few decades, average 6 week in-hospital mortality of first variceal bleeding still approaches 20% 37, 38, 39.
- Hepatic encephalopathy causing confusion or difficulty thinking caused by a buildup of toxins in your brain. Hepatic encephalopathy is impairment in neuropsychiatric function associated with portal hypertension. Symptoms are usually mild, with subtle changes in behavior, changes in sleep pattern, mild confusion or slurred speech. However, it can progress to more serious symptoms, including severe lethargy and coma. Although scientists lack clear understanding of encephalopathy, there is an association with increase in ammonia concentration in the body. However this does not correlate to regular blood test levels of ammonia. Hepatic encephalopathy is diagnosed by doctor. It is usually treated with medications such as lactulose, which can decrease the ammonia absorption in the gastrointestinal tract. It is also treated with antibiotics, such as rifaximin and neomycin.
- Infections. Cirrhosis increases your chance of getting bacterial infections, such as urinary tract infections and pneumonia.
- Liver cancer. Cirrhosis increases the chance of getting liver cancer 40, 41, 42. Most people who develop liver cancer already have cirrhosis. Routine monitoring of cirrhotic patients for the development of liver cancer is recommended, with at least 6 monthly screenings using abdominal ultrasonography 41.
- Liver failure. Cirrhosis may eventually lead to liver failure, also called end-stage liver disease. With liver failure, your liver is badly damaged and stops working. People with liver failure may require a liver transplant.
Other complications of cirrhosis may include 43:
- bone diseases, such as osteoporosis
- gallstones
- problems with the bile ducts—the tubes that carry bile out of the liver
- malabsorption and malnutrition
- bruising and bleeding easily
- falls
- sensitivity to medicines
- insulin resistance and type 2 diabetes.
Portal hypertension diagnosis
There are a number of ways to diagnose portal hypertension. For patients with end-stage liver disease who present with large amount of fluid accumulates in their abdomen (ascites) and varices, the doctor may not need to perform any diagnostic tests and can confirm a diagnosis based on their symptoms. However, to help confirm a diagnosis, a combination of laboratory and imaging tests is usually done.
Your doctor may order one or more tests to check your liver, including:
- Laboratory tests. Your doctor may order blood tests to check for signs of liver malfunction, such as high bilirubin levels or certain enzymes. To evaluate kidney function, your blood is checked for creatinine. Your blood count would be measured. You’ll be screened for the hepatitis viruses. Your international normalized ratio (INR) is also checked for your blood’s ability to clot. Based on history and blood test results, your doctor may be able to diagnose the underlying cause of your liver disease. Blood tests also can help identify how serious your liver disease is.
- Your doctor may suspect cirrhosis if you have:
- higher levels of the liver enzymes alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP).
- higher levels of bilirubin.
- lower levels of blood proteins called albumin or higher levels of blood proteins called immunoglobulins.
- Complete blood count can show signs of infection and anemia that may be caused by internal bleeding.
- Tests for autoimmune liver conditions, which include the anti-nuclear antibody (ANA), anti-smooth muscle antibody (SMA), and anti-mitochondrial antibody (AMA) tests.
- Your doctor may suspect cirrhosis if you have:
- Imaging tests. An imaging study helps in the diagnosis of cirrhosis and portal hypertension. They are noninvasive and can give your doctor a detailed image of your portal venous system. Transient or magnetic resonance elastography (MRE) may be recommended. Elastography is a special test that measures the stiffness of your liver. An increase in liver stiffness may be a sign of fibrosis, or scarring. Your doctor can use stiffness measures to see if you may have cirrhosis and whether liver scarring is getting better or worse. Other imaging tests, such as MRI, CT and ultrasound, also may be done. A duplex Doppler ultrasound is typically the first imaging test ordered. A Doppler ultrasound uses sound waves to see how the blood flows through your portal vein. The ultrasound gives your doctor a picture of the blood vessel and its surrounding organs, as well as the speed and direction of the blood flow through the portal vein.
- Biopsy. A tissue sample, called a biopsy, is not necessarily needed for diagnosis. A liver biopsy can diagnose cirrhosis when the results of other tests are uncertain. The biopsy may also help your doctor identify the cause of cirrhosis, how severe liver damage is and determine whether you need treatment. During a liver biopsy, a doctor will use a needle to take small pieces of tissue from the liver. A pathologist will examine the tissue under a microscope.
- Pressure measurement studies (hepatic venous pressure gradient [HVPG]). Identification of the level of resistance to portal blood flow allows the determination of the cause of portal hypertension. An interventional radiologist may perform a pressure measurement study to evaluate the level of pressure in the hepatic (liver) vein. This can be done as an outpatient, where a radiologist will access one of your veins, usually via internal jugular vein.
- Portal hypertension is defined as increased pressure within the portal venous system (a sustained increase in the pressure gradient between portal and systemic circulation). The most common parameter used to measure portal pressure is the hepatic venous pressure gradient (HVPG), which is the pressure gradient between the portal vein and inferior vena cava (IVC) 2. Portal hypertension is determined by the increased portal pressure gradient, that is the difference in pressures between the portal venous pressure and the pressure within the inferior vena cava or the hepatic vein 9. In healthy individuals, the normal hepatic venous pressure gradient (HVPG) is 1 to 5 mmHg. A hepatic venous pressure gradient (HVPG) of 6 to 10 mmHg between the portal and hepatic veins or inferior vena cava (IVC) suggests the presence of mild subclinical portal hypertension in most cases 9. When the hepatic venous pressure gradient (HVPG) is greater than 10 mmHg, portal hypertension becomes clinically significant 11. A hepatic venous pressure gradient (HVPG) above 12 mmHg usually reflects decompensated cirrhosis, which is manifested by the development of porto-systemic shunting, variceal rupture and bleeding 12, 13. Moreover, it has been reported that the probability of survival in cirrhotic patients with HVPG above 16 mmHg was below 70% of those patients who have an HVPG below this level and that this poor survival rate was related to Child-Pugh class 14.
- Endoscopic diagnosis. Your doctor will perform an upper endoscopy to look for enlarged veins in your esophagus or stomach, which are large vessels associated with portal hypertension that may bleed. These veins are known as varices. If you develop varices, you likely will need medicine to lower the risk of bleeding. If you have signs that the varices are bleeding or are likely to bleed, you may need a procedure known as band ligation. Band ligation can stop the bleeding or reduce the risk of further bleeding. In severe cases, you may need a small tube — a transjugular intrahepatic portosystemic shunt (TIPS) — placed in your vein to reduce blood pressure in your liver. During a TIPS procedure, a stent (tube) is inserted to connect the portal veins to lower pressure blood vessels. This relieves pressure on the diseased liver, which can help stop bleeding and fluid buildup.
If you have cirrhosis, your doctor is likely to recommend regular tests to see if liver disease has progressed or check for signs of complications, especially esophageal varices and liver cancer. Noninvasive tests are becoming more widely available for monitoring liver disease.
Portal hypertension treatment
Doctors treat portal hypertension with medicines to lower high blood pressure in the portal vein. Doctors may also treat the following complications of portal hypertension.
Portal hypertension treatment may include the following:
- Low-sodium diet and water pills (diuretics). You will need to follow a low-sodium diet, as sodium causes fluid retention in your body. In severe cases, you may need to restrict your water intake as well. A prescription diuretic may help reduce sodium retention in your kidneys. More-severe fluid buildup may require procedures to drain the fluid called paracentesis or surgery to relieve pressure. During a paracentesis, your doctor inserts a needle into your abdomen to remove the fluid.
- Certain blood pressure medicines may control increased pressure in the veins that supply the liver and prevent severe bleeding.
- You may receive antibiotics or other treatments for infections. Your doctor also is likely to recommend vaccinations for influenza, pneumonia and hepatitis.
- Your doctor will likely recommend regular blood tests and ultrasound exams to look for signs of liver cancer.
- You may be prescribed medicines to help reduce the buildup of toxins in your blood caused by poor liver function.
Medication for portal hypertension
If there are enlarged veins in your esophagus or stomach due to portal hypertension, your doctor can treat it with medications to lower the pressure in these veins and prevent them from bleeding. Medications used to treat enlarged veins in the esophagus and stomach include:
- Beta blockers can be used to decrease portal pressure, although there are side effects. However, if you have cirrhosis but no varices, beta blockers cannot be used to prevent varices from developing. Studies have shown that the side effects of the medication outweigh the possible benefits.
- American Association for the Study of Liver Disease guidelines, British Society of Gastroenterology guidelines and the Baveno 6 consensus recommend the use of non-selective beta-blockers in both primary and secondary prophylaxis of variceal bleeding 44, 45, 46 and their effectiveness has been demonstrated by a number of clinical trials. In patients with existing small varices, non-selective beta-blockers slowed the progression of small varices into large varices (11% and 37%, non-selective beta-blockers vs placebo control, respectively) and decreased the incidence of first variceal hemorrhage (12% and 22%, non-selective beta-blockers vs placebo control, respectively) 47. In patients with medium or large varices and at a high risk of bleeding, non-selective beta-blockers reduced the risk of bleeding to 14% from 30% in control subjects 48. The effectiveness of non-selective beta-blockers in secondary prophylaxis has been shown by studies which demonstrated that at one year of treatment with propranolol, the drug reduced recurrent bleeding of cirrhotic patients with gastrointestinal bleeding 49, 50. However, non-selective beta-blockers are not similarly effective in preventing the development of new varices in early cirrhotic patients with mild subclinical portal hypertension 51. Moreover, non-selective beta-blockers are contraindicated in patients at the time of acute variceal bleeding due to their systemic hypotensive and cardiac side effects 52.
- The traditional and most widely used non-selective beta-blockers in clinical practice are propranolol and nadolol. Many clinical trials suggest that both drugs have a similar effectiveness in primary prophylaxis of variceal bleeding. However, some studies showed that the side effects produced by nadolol (9%-13%) were lower compared to those of propranolol (12%-31%), although direct comparison between the two groups has not been performed 53. Moreover, compared to propranolol, nadolol has a longer half-life in the circulation attributed to its low lipid solubility and hepatic metabolism, thus patients can be dosed less frequently 54.
- Similar to propranolol, the non-selective beta-blocker timolol is effective in reducing hepatic venous pressure gradient (HVPG), particularly in early cirrhosis (12% and 13% reduction in timolol and propranolol, respectively) 55, 56. Other non-selective beta-blockers used as antihypertensive drugs including sotalol, pindolol and penbutalol may also be effective in the treatment of portal hypertension; however, the efficacy of these drugs has not yet been tested in patients with esophageal varices.
- Selective beta-1 adrenergic receptor blockers such as atenolol and metoprolol also reduce hepatic venous pressure gradient (HVPG) in cirrhotic patients. The reduction of hepatic venous pressure gradient (HVPG) achieved with these selective blockers is related to their beta-1 adrenergic receptor blockade-mediated effect on cardiac index, which contrasts with the cumulative cardiac (1) and splanchnic (2) effects of non-selective beta-blockers such as propranolol. It was reported that the efficacy of atenolol in reducing HVPG and variceal bleeding was less and not sustained in cirrhotic patients compared to propranolol 57, 58. Similarly, treatment with metoprolol also was associated with higher rate of recurrent bleeding 59. Based on these findings and also due to their profound cardiac side effects, selective beta-1 adrenergic receptor blockers are not therefore recommended in the prophylaxis of variceal hemorrhage 60.
- Despite their proven clinical effectiveness, traditional non-selective beta-blockers such as propranolol and nadolol are contraindicated or poorly tolerated in up to 15%-20% of patients and up to 60% of patients do not achieve any therapeutically useful fall in hepatic venous pressure gradient (HVPG) with these non-selective beta-blockers 60, 36, 61. Non-selective beta-blockers produce a number of cardiac and non-cardiac adverse effects, such as headaches, fatigue, asthma and shortness of breath, which led to the discontinuation of treatment in about 15% of the patients in clinical trials 62, 63.
- In end stage cirrhotic patients with refractory ascites and/or spontaneous bacterial peritonitis, non-selective beta-blockers blunt the ability to maintain an adequate systemic arterial blood pressure, and defective renal perfusion may lead to the development of hepato-renal syndrome 64, 65 and in end stage cirrhosis non-selective beta-blockers have been associated with increased mortality 66.The use of non-selective beta-blockers is also contraindicated in around 15% of the cirrhotic patients who have asthma, chronic obstructive pulmonary diseases poor cardiac function or low blood pressure 13.
- Reduction of intrahepatic and/or porto-collateral resistance using vasodilatory agents such as nitrates could also be an ideal therapeutic approach in the treatment of portal hypertension in cirrhosis. These agents such as isosorbide-5-mononitrate (isosorbide mononitrate), are ineffective when given as monotherapy but when given as a combined treatment with an non-selective beta-blocker improve the efficacy of non-selective beta-blockers in the reduction of hepatic venous pressure gradient (HVPG) and may be very useful in secondary prophylaxis for variceal bleeding 67. The combined treatment, has been shown to be effective for those patients who are non-responders to standard non-selective beta-blocker treatment alone 68, 47.
- Octreotide. Octreotide also known as Sandostatin or Olatuton is a man made (synthetic) version of somatostatin. Somatostatin is a hormone that regulates a variety of bodily functions by blocking the release of other hormones, the activity of your gastrointestinal tract and the rapid reproduction of cells. Octreotide decreases blood flow in the gastrointestinal region and is used to treat acute bleeding from esophageal varices, gastrointestinal ulcers, and gastritis; prevent pancreatic complications after surgery; and restrict secretions of the upper intestine, pancreas, and biliary tract.
- A recent meta-analysis showed that the efficacy of somatostatin or octreotide on variceal re-bleeding was similar to that of vasopressin or terlipressin 69. In current guidelines, somatostatin and its analogues such as octreotide and vapreotide are recommended for acute variceal bleeding 70, although they may have side-effects such as tachyphylaxis, bradycardia and hypertension 71, 72.
Buildup of fluid in the abdomen
A buildup of fluid in your abdomen or belly is called ascites. To treat ascites, doctors may prescribe medicines that remove fluid from the body. Doctors may also recommend that people with cirrhosis limit the amount of sodium they eat or drink. If large amounts of fluid build up in the abdomen, doctors may use a needle or tube to drain the fluid (paracentesis) and check the fluid for signs of infection. Doctors may prescribe medicines to treat infection or prevent infection.
Swelling in the legs, ankles, or feet
To treat swelling in the legs, ankles, or feet (edema), your doctor may prescribe medicines that remove fluid from your body. Doctors may also recommend that people with cirrhosis limit how much sodium they eat or drink.
Enlarged veins in the esophagus or stomach
Enlarged veins in the esophagus or stomach are called varices. To treat varices, doctors may prescribe medicines to lower the blood pressure in the veins. Lowering the pressure in the veins reduces the chance that the veins will become enlarged and burst, causing internal bleeding. People who vomit blood or have black or bloody stools should go to a hospital right away. Doctors may perform procedures during an upper gastrointestinal (GI) endoscopy or use surgical procedures to stop the bleeding.
Control of bleeding
Bleeding from esophageal varices is a medical emergency. Drugs such as vasopressin or octreotide may be given intravenously to make the bleeding veins contract and thus slow the bleeding 73. Blood transfusions are given to replace lost blood. Doctors usually use a flexible viewing tube (endoscope), inserted through the mouth into the esophagus to confirm that the bleeding is from varices. Working through the endoscope, doctors can use rubber bands to tie off the veins.
To reduce the risk of bleeding from esophageal varices, doctors may try to reduce pressure in the portal vein. One way is to give beta-blocker drugs, such as timolol, propranolol, nadolol, or carvedilol 73.
Doctors regularly monitor people who have had bleeding from varices because bleeding may recur.
Endoscopic therapy
An endoscopy can treat gastrointestinal hemorrhage. There are a number of endoscopic treatments for this purpose:
- Banding: This is the preferred method to manage variceal hemorrhage. During an endoscopy, your doctor places small elastic rings over the vein. The rings block the blood supply to each varix. You will undergo the initial banding session and then return for subsequent sessions in order to completely obliterate the varices, which is usually achieved after four to five procedures.
- Balloon tamponade: This is done to control severe variceal bleeding through compressing the vein. We inflate a small balloon within your stomach or esophagus to apply pressure to the bleeding veins. This compresses and stops the bleeding. This is a complex procedure that should only be performed by experienced physicians.
- Transjugular intrahepatic portosystemic shunt (TIPS): During a TIPS procedure, a stent (tube) is inserted to connect the portal veins to lower pressure blood vessels. This relieves pressure on the diseased liver, which can help stop bleeding and fluid buildup. Your doctor will access the hepatic vein through the jugular vein and pass a needle through the liver into the portal vein. The vein is then dilated and a stent is put in place to keep the vein open.
Portosystemic shunting procedures
Portosystemic shunting is a surgical procedure that connects the portal vein or one of its branches to a vein in the general circulation. Portosystemic shunting procedure reroutes most of the blood that normally goes to the liver so that it bypasses the liver. This bypass called a shunt lowers pressure in the portal vein because pressure is much lower in the general circulation.
Portosystemic shunting is another method of controlling acute bleeding. If you have had recurrent bleeding despite medical or endoscopic treatment, you may require either of the two methods of portosystemic shunting:
- Nonsurgical transjugular intrahepatic portosystemic shunt (TIPS): TIPS procedure should only be performed by a doctor with a high level of expertise and experience. In transjugular intrahepatic portosystemic shunting (TIPS), your doctor using x-rays for guidance, inserts a catheter with a needle into a vein in your neck (the jugular vein) and thread it to veins in the liver (the portal vein). The catheter is used to create a passage (shunt) that connects the portal vein (or one of its branches) directly with one of the hepatic veins. Less commonly, portosystemic shunts are created surgically. TIPS procedure is usually successful in stopping the bleeding but pose certain risks, particularly hepatic encephalopathy. TIPS procedure may have to be repeated because the shunt may become blocked.
- Surgical shunts: This is done to reduce the pressure in the portal vein, to maintain regular blood flow around the liver and to reduce (or not worsen) hepatic encephalopathy.
Buildup of toxins in the brain (hepatic encephalopathy)
A buildup of toxins in the brain called hepatic encephalopathy can cause confusion, difficulty thinking, memory loss, personality changes, sleep disorders and coma. Doctors may prescribe medicines that help lower the levels of toxins in the brain and improve brain function.
Infections
Doctors will prescribe antibiotics to treat bacterial infections .
Liver cancer
If you have cirrhosis, your doctor may suggest blood tests and an ultrasound or another type of imaging test to check for liver cancer. Doctors may recommend checking for liver cancer every 6 months 74. Finding cancer at an early stage improves the chance of curing the cancer.
For people who develop liver cancer, doctors may treat the cancer with medical procedures that remove or destroy cancer cells, such as surgery, radiation therapy , and chemotherapy. Doctors may also treat liver cancer with a liver transplant.
Liver transplant surgery
In advanced cases of cirrhosis, when the liver stops working properly also called end-stage liver disease or liver failure, a liver transplant may be the only treatment option. A liver transplant is a procedure to replace your liver with a healthy liver from a deceased donor or with part of a liver from a living donor. Cirrhosis is one of the most common reasons for a liver transplant. Liver transplantation surgery is long and complex, requiring the removal and replacement of your body’s largest solid organ. However, this option offers the highest survival rate and chance of complete rehabilitation. Candidates for liver transplant have extensive testing to determine whether they are healthy enough to have a good outcome following surgery.
Historically, those with alcoholic cirrhosis have not been liver transplant candidates because of the risk that they will return to harmful drinking after transplant. Recent studies, however, suggest that carefully selected people with severe alcoholic cirrhosis have post-transplant survival rates similar to those of liver transplant recipients with other types of liver disease.
Your doctor will discuss with you whether you are a candidate for liver transplantation and the steps you must take to be placed on the waiting list for a new liver.
For liver transplant to be an option if you have alcoholic cirrhosis, you would need to:
- Find a program that works with people who have alcoholic cirrhosis.
- Meet the requirements of the program. These would include lifelong commitment to alcohol abstinence as well as other requirements of the specific transplant center.
Living with portal hypertension
There is no cure for cirrhosis. However, work with your doctor on a treatment plan to manage symptoms and help prevent more damage.
- You shouldn’t drink any alcohol or use illegal drugs, as it continues to damage your liver.
- Talk with your doctor before taking any medicines. This includes antibiotics, birth control pills, and all over-the-counter medicines such as nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen (paracetamol) and sleep aids.
- Take care of yourself. Consume healthy foods and drinks. You may need to watch how much sugar and protein you eat. Avoid raw or undercooked shellfish, fish, and meat. If you have swelling or are retaining fluid, avoid salt or sodium.
- Try to reach and stay at a healthy body weight.
Your doctor may recommend screening for liver cancer. If left untreated, cirrhosis can get worse and be life threatening. It can cause a coma, liver failure, or death.
Portal hypertension diet
What you eat and drink is important. Cirrhosis can lead to malnutrition, meaning that your body is not getting the right amount of the vitamins, minerals, and other nutrients it needs to stay healthy. Research suggests that 50% to 90% of people with cirrhosis have malnutrition 75. Your doctor may refer you to a registered dietitian to help create healthy meal plans that fit your nutrition needs.
People with cirrhosis are at risk for malnutrition for several reasons. The symptoms of cirrhosis, such as nausea and vomiting, may cause people with cirrhosis to eat and drink less. Cirrhosis also affects how the liver works. When your liver isn’t working well, your body may have problems digesting foods and drinks or absorbing nutrients.
Meal plans will vary depending on how severe your cirrhosis is and other factors. Your doctor or a registered dietitian can recommend a meal plan that will provide the amount of calories and nutrients, especially protein, that your body needs. Your doctor or a registered dietitian may recommend that people who do not get enough nutrients, or who have low levels of some vitamins and minerals, take certain dietary supplements . If you have cirrhosis, talk with your doctor before taking dietary supplements, including herbal supplements.
Cirrhosis changes the way the body stores nutrients and uses them for energy. People with cirrhosis should avoid fasting, or going without food, for too long. Your doctor or a registered dietitian may recommend 76:
- Having smaller, more frequent meals
- Eating every 3 or 4 hours while awake
- Having a snack before going to sleep at night or having an early breakfast after waking up
What should I avoid eating and drinking if I have cirrhosis?
Avoid eating raw or undercooked shellfish, fish, and meat, and unpasteurized milk and milk products. Bacteria or viruses from these foods may cause severe infections in people with cirrhosis.
Your doctor may recommend limiting sodium in foods and drinks.
You should completely stop drinking alcohol because it can cause more liver damage.
Portal hypertension prognosis
Portal hypertension prognosis depends on the underlying cause of your portal hypertension predicted by the degree of liver reserve and the degree of bleeding 11. Death during acute variceal bleed may exceed 50%. For survivors, the bleeding risk within the next 1 to 2 years is 50 to 75%. Ongoing endoscopic or drug therapy lowers the bleeding risk but decreases long-term mortality only marginally.
Liver cirrhosis is the 11th most common cause of death globally and the third leading cause of death among individuals aged 45–64 years 77, 78. When combined with liver cancers, cirrhosis accounts for 3.5% of all deaths worldwide 77, 78. A major study found that approximately 2.2 million adults in the U.S. have cirrhosis, and that the annual death rate from cirrhosis rose from 14.9 per 100,000 to 21.9 per 100,000 in the decade to 2021 79, 80. Surprisingly, deaths due to cirrhosis already accounted for 2.4% of global deaths in 2019, and the number of people dying from cirrhosis is expected to continue to increase over the next decade 81. Liver transplantation is indicated in decompensated cirrhosis that does not respond to medical treatment. The 1-year and 5-year survival rates after liver transplantation are approximately 85% and 72%, respectively. Recurrence of the underlying liver disease can occur after a transplant 82. Long-term side effects of immunosuppressant drugs are another cause of illness in transplant patients.
- Bosch J., Navasa M., Garcia-Pagan J., DeLacy A., Rodes J. Portal hypertension. Med. Clin. North Am. 1989;73:931–953. doi: 10.1016/S0025-7125(16)30646-0[↩]
- Sanyal AJ, Bosch J, Blei A, Arroyo V. Portal hypertension and its complications. Gastroenterology. 2008;134:1715–1728. doi: 10.1053/j.gastro.2008.03.007[↩][↩]
- Groszmann RJ, Wongcharatrawee S. The hepatic venous pressure gradient: anything worth doing should be done right. Hepatology. (2004) 39:280–2. 10.1002/hep.20062[↩]
- PATON A, REYNOLDS TB, SHERLOCK S. Assessment of portal venous hypertension by catheterisation of hepatic vein. Lancet. 1953 May 9;1(6767):918-21. doi: 10.1016/s0140-6736(53)92060-1[↩]
- Suk KT. Hepatic venous pressure gradient: clinical use in chronic liver disease. Clin Mol Hepatol. 2014 Mar;20(1):6-14. doi: 10.3350/cmh.2014.20.1.6[↩]
- de Franchis R; Baveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015 Sep;63(3):743-52. doi: 10.1016/j.jhep.2015.05.022[↩][↩]
- Groszmann RJ, Garcia-Tsao G, Bosch J, Grace ND, Burroughs AK, Planas R, Escorsell A, Garcia-Pagan JC, Patch D, Matloff DS, Gao H, Makuch R; Portal Hypertension Collaborative Group. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N Engl J Med. 2005 Nov 24;353(21):2254-61. doi: 10.1056/NEJMoa044456[↩][↩]
- Gunarathne LS, Rajapaksha H, Shackel N, Angus PW, Herath CB. Cirrhotic portal hypertension: From pathophysiology to novel therapeutics. World J Gastroenterol. 2020 Oct 28;26(40):6111-6140. doi: 10.3748/wjg.v26.i40.6111[↩]
- Berzigotti A, Seijo S, Reverter E, Bosch J. Assessing portal hypertension in liver diseases. Expert Rev Gastroenterol Hepatol. 2013 Feb;7(2):141-55. doi: 10.1586/egh.12.83[↩][↩][↩][↩]
- Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017 Jan;65(1):310-335. doi: 10.1002/hep.28906. Epub 2016 Dec 1. Erratum in: Hepatology. 2017 Jul;66(1):304. doi: 10.1002/hep.29169[↩]
- Oliver TI, Sharma B, John S. Portal Hypertension. [Updated 2023 Apr 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507718[↩][↩][↩]
- Kumar A, Sharma P, Sarin SK. Hepatic venous pressure gradient measurement: time to learn! Indian J Gastroenterol. 2008 Mar-Apr;27(2):74-80.[↩][↩]
- Garcia-Tsao G. The Use of Nonselective Beta Blockers for Treatment of Portal Hypertension. Gastroenterol Hepatol (N Y). 2017 Oct;13(10):617-619. https://pmc.ncbi.nlm.nih.gov/articles/PMC5718179[↩][↩][↩]
- Merkel C, Bolognesi M, Sacerdoti D, Bombonato G, Bellini B, Bighin R, Gatta A. The hemodynamic response to medical treatment of portal hypertension as a predictor of clinical effectiveness in the primary prophylaxis of variceal bleeding in cirrhosis. Hepatology. 2000 Nov;32(5):930-4. doi: 10.1053/jhep.2000.19322[↩][↩]
- Ripoll C, Bañares R, Rincón D, Catalina M-V, Lo Iacono O, Salcedo M, et al. Influence of hepatic venous pressure gradient on the prediction of survival of patients with cirrhosis in the meld era. Hepatology (Baltimore, Md). (2005) 42:793–801. 10.1002/hep.20871[↩]
- Kumar M, Kumar A, Hissar S, Jain P, Rastogi A, Kumar D, et al. Hepatic venous pressure gradient as a predictor of fibrosis in chronic liver disease because of hepatitis b virus. Liver Int. (2008) 28:690–8. 10.1111/j.1478-3231.2008.01711.x[↩]
- Blasco A, Forns X, Carrión JA, García-Pagán JC, Gilabert R, Rimola A, Miquel R, Bruguera M, García-Valdecasas JC, Bosch J, Navasa M. Hepatic venous pressure gradient identifies patients at risk of severe hepatitis C recurrence after liver transplantation. Hepatology. 2006 Mar;43(3):492-9. doi: 10.1002/hep.21090[↩]
- Ripoll C, Groszmann RJ, Garcia-Tsao G, Bosch J, Grace N, Burroughs A, et al. Hepatic venous pressure gradient predicts development of hepatocellular carcinoma independently of severity of cirrhosis. J Hepatol. (2009) 50:923–8. 10.1016/j.jhep.2009.01.014[↩]
- Berzigotti A, Reig M, Abraldes JG, Bosch J, Bruix J. Portal hypertension and the outcome of surgery for hepatocellular carcinoma in compensated cirrhosis: a systematic review and meta-analysis. Hepatology (Baltimore, Md). (2015) 61:526–36. 10.1002/hep.27431[↩]
- Ripoll C, Groszmann R, Garcia-Tsao G, Grace N, Burroughs A, Planas R, Escorsell A, Garcia-Pagan JC, Makuch R, Patch D, Matloff DS, Bosch J; Portal Hypertension Collaborative Group. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology. 2007 Aug;133(2):481-8. doi: 10.1053/j.gastro.2007.05.024[↩]
- Garcia-Tsao G, Groszmann RJ, Fisher RL, Conn HO, Atterbury CE, Glickman M. Portal pressure, presence of gastroesophageal varices and variceal bleeding. Hepatology. 1985 May-Jun;5(3):419-24. doi: 10.1002/hep.1840050313[↩]
- Bosch J, García-Pagán JC. Prevention of variceal rebleeding. Lancet. 2003 Mar 15;361(9361):952-4. doi: 10.1016/S0140-6736(03)12778-X[↩]
- Silva-Junior G, Baiges A, Turon F, Torres F, Hernández-Gea V, Bosch J, et al. The prognostic value of hepatic venous pressure gradient in patients with cirrhosis is highly dependent on the accuracy of the technique. Hepatology (Baltimore, Md). (2015) 62:1584–92. 10.1002/hep.28031[↩]
- Baldisseri F, Wrona A, Menegatti D, Pietrabissa A, Battilotti S, Califano C, Cristofaro A, Di Giamberardino P, Facchinei F, Palagi L, Giuseppi A, Delli Priscoli F. Deep Neural Network Regression to Assist Non-Invasive Diagnosis of Portal Hypertension. Healthcare (Basel). 2023 Sep 21;11(18):2603. doi: 10.3390/healthcare11182603[↩][↩]
- Bosch J, Abraldes JG, Berzigotti A, Garcia-Pagan JC. Portal hypertension and gastrointestinal bleeding. Semin Liver Dis. 2008 Feb;28(1):3-25. doi: 10.1055/s-2008-1040318[↩]
- Garcia-Tsao G., Bosch J. Management of varices and variceal hemorrhage in cirrhosis. N. Engl. J. Med. 2010;362:823–832. doi: 10.1056/NEJMra0901512[↩][↩]
- Sanyal A.J., Bosch J., Blei A., Arroyo V. Portal hypertension and its complications. Gastroenterology. 2008;134:1715–1728. doi: 10.1053/j.gastro.2008.03.007[↩][↩]
- Reiberger T. The Value of Liver and Spleen Stiffness for Evaluation of Portal Hypertension in Compensated Cirrhosis. Hepatol Commun. 2022 May;6(5):950-964. doi: 10.1002/hep4.1855[↩]
- Symptoms & Causes of Cirrhosis. https://www.niddk.nih.gov/health-information/liver-disease/cirrhosis/symptoms-causes[↩][↩]
- Portal Hypertension. https://www.msdmanuals.com/professional/hepatic-and-biliary-disorders/approach-to-the-patient-with-liver-disease/portal-hypertension[↩][↩][↩]
- [↩]
- Hayward KL, Weersink RA. Improving Medication-Related Outcomes in Chronic Liver Disease. Hepatol Commun. 2020 Oct 10;4(11):1562-1577. doi: 10.1002/hep4.1612[↩]
- Zipprich A, Garcia-Tsao G, Rogowski S, Fleig WE, Seufferlein T, Dollinger MM. Prognostic indicators of survival in patients with compensated and decompensated cirrhosis. Liver Int. 2012;32:1407–1414. doi: 10.1111/j.1478-3231.2012.02830.x[↩]
- Haq I, Tripathi D. Recent advances in the management of variceal bleeding. Gastroenterol Rep (Oxf) 5:113–126. doi: 10.1093/gastro/gox007[↩]
- Graham DY, Smith JL. The course of patients after variceal hemorrhage. Gastroenterology. 1981 Apr;80(4):800-9.[↩]
- D’Amico G, Pagliaro L, Bosch J. The treatment of portal hypertension: a meta-analytic review. Hepatology. 1995;22:332–354. doi: 10.1002/hep.1840220145[↩][↩]
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey WD Practice Guidelines Committee of American Association for Study of Liver Diseases; Practice Parameters Committee of American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Am J Gastroenterol. 2007;102:2086–2102. doi: 10.1111/j.1572-0241.2007.01481.x[↩]
- Hernández-Gea V, Berzigotti A. Clinical Evaluation and Prognosis. Dig Dis. 2015;33:515–523. doi: 10.1159/000374100[↩]
- Chalasani N, Kahi C, Francois F, Pinto A, Marathe A, Bini EJ, Pandya P, Sitaraman S, Shen J. Improved patient survival after acute variceal bleeding: a multicenter, cohort study. Am J Gastroenterol. 2003;98:653–659. doi: 10.1111/j.1572-0241.2003.07294.x[↩]
- Mittal S, El-Serag HB. Epidemiology of hepatocellular carcinoma: consider the population. J Clin Gastroenterol. 2013 Jul;47 Suppl(0):S2-6. doi: 10.1097/MCG.0b013e3182872f29[↩]
- Schuppan D, Afdhal NH. Liver cirrhosis. Lancet. 2008 Mar 8;371(9615):838-51. doi: 10.1016/S0140-6736(08)60383-9[↩][↩]
- Liver (Hepatocellular) Cancer Prevention (PDQ®)–Health Professional Version. https://www.cancer.gov/types/liver/PVPp/liver-prevention-pdq[↩]
- Definition & Facts for Cirrhosis. https://www.niddk.nih.gov/health-information/liver-disease/cirrhosis/definition-facts[↩]
- de Franchis R Baveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63:743–752. doi: 10.1016/j.jhep.2015.05.022[↩]
- Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65:310–335. doi: 10.1002/hep.28906[↩]
- Tripathi D, Stanley AJ, Hayes PC, Patch D, Millson C, Mehrzad H, Austin A, Ferguson JW, Olliff SP, Hudson M, Christie JM Clinical Services and Standards Committee of the British Society of Gastroenterology. U.K. guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut. 2015;64:1680–1704. doi: 10.1136/gutjnl-2015-309262[↩]
- Merkel C, Sacerdoti D, Bolognesi M, Buonamico P, Sticca A, Amodio P, Angeli P, Micotti L, Gatta A. Effect of chronic treatment with nadolol plus isosorbide mononitrate on liver blood flow and liver metabolic activity in cirrhosis. Eur J Gastroenterol Hepatol. 1999;11:1221–1225. doi: 10.1097/00042737-199911000-00006[↩][↩]
- D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment of portal hypertension: an evidence-based approach. Semin Liver Dis. 1999;19:475–505. doi: 10.1055/s-2007-1007133[↩]
- Poynard T, Lebrec D, Hillon P, Sayegh R, Bernuau J, Naveau S, Chaput JC, Klepping C, Rueff B, Benhamou JP. Propranolol for prevention of recurrent gastrointestinal bleeding in patients with cirrhosis: a prospective study of factors associated with rebleeding. Hepatology. 1987;7:447–451. doi: 10.1002/hep.1840070306[↩]
- Lebrec D, Poynard T, Hillon P, Benhamou JP. Propranolol for prevention of recurrent gastrointestinal bleeding in patients with cirrhosis: a controlled study. N Engl J Med. 1981;305:1371–1374. doi: 10.1056/NEJM198112033052302[↩]
- Groszmann RJ, Garcia-Tsao G, Bosch J, Grace ND, Burroughs AK, Planas R, Escorsell A, Garcia-Pagan JC, Patch D, Matloff DS, Gao H, Makuch R Portal Hypertension Collaborative Group. Beta-blockers to prevent gastroesophageal varices in patients with cirrhosis. N Engl J Med. 2005;353:2254–2261. doi: 10.1056/NEJMoa044456[↩]
- Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W Practice Guidelines Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46:922–938. doi: 10.1002/hep.21907[↩]
- Bolognesi M, Balducci G, Garcia-Tsao G, Gatta A, Gines P, Merli M, Rodes J, Stiegmann GV. Complications in the medical treatment of portal hypertension. In: de Franchis R. Portal Hypertension III: Proceedings of the Third Baverno International Consensus Workshop on Definitions, Methodology and Therapeutic Strategies. Oxford: Blackwell Science, 2001.[↩]
- Tripathi D, Hayes PC. Beta-blockers in portal hypertension: new developments and controversies. Liver Int. 2014;34:655–667. doi: 10.1111/liv.12360[↩]
- Escorsell A, Ferayorni L, Bosch J, García-Pagán JC, García-Tsao G, Grace ND, Rodés J, Groszmann RJ. The portal pressure response to beta-blockade is greater in cirrhotic patients without varices than in those with varices. Gastroenterology. 1997;112:2012–2016. doi: 10.1053/gast.1997.v112.pm9178694[↩]
- Groszmann RJ, Bosch J, Grace ND, Conn HO, Garcia-Tsao G, Navasa M, Alberts J, Rodes J, Fischer R, Bermann M. Hemodynamic events in a prospective randomized trial of propranolol versus placebo in the prevention of a first variceal hemorrhage. Gastroenterology. 1990;99:1401–1407. doi: 10.1016/0016-5085(90)91168-6[↩]
- Mills PR, Rae AP, Farah DA, Russell RI, Lorimer AR, Carter DC. Comparison of three adrenoreceptor blocking agents in patients with cirrhosis and portal hypertension. Gut. 1984;25:73–78. doi: 10.1136/gut.25.1.73[↩]
- Hillon P, Lebrec D, Muńoz C, Jungers M, Goldfarb G, Benhamou JP. Comparison of the effects of a cardioselective and a nonselective beta-blocker on portal hypertension in patients with cirrhosis. Hepatology. 1982;2:528–531. doi: 10.1002/hep.1840020503[↩]
- Westaby D, Melia WM, Macdougall BR, Hegarty JE, Gimson AE, Williams R. B1 selective adrenoreceptor blockade for the long term management of variceal bleeding. A prospective randomised trial to compare oral metoprolol with injection sclerotherapy in cirrhosis. Gut. 1985;26:421–425. doi: 10.1136/gut.26.4.421[↩]
- Ge PS, Runyon BA. The changing role of beta-blocker therapy in patients with cirrhosis. J Hepatol. 2014;60:643–653. doi: 10.1016/j.jhep.2013.09.016[↩][↩]
- García-Pagán JC, Villanueva C, Vila MC, Albillos A, Genescà J, Ruiz-Del-Arbol L, Planas R, Rodriguez M, Calleja JL, González A, Solà R, Balanzó J, Bosch J; MOVE Group. Mononitrato Varices Esofágicas. Isosorbide mononitrate in the prevention of first variceal bleed in patients who cannot receive beta-blockers. Gastroenterology. 2001 Oct;121(4):908-14.[↩]
- Garcia-Tsao G, Lim JK Members of Veterans Affairs Hepatitis C Resource Center Program. Management and treatment of patients with cirrhosis and portal hypertension: recommendations from the Department of Veterans Affairs Hepatitis C Resource Center Program and the National Hepatitis C Program. Am J Gastroenterol. 2009;104:1802–1829. doi: 10.1038/ajg.2009.191[↩]
- López-Méndez E, Uribe M. Beta blockers in portal hypertension. Are they really a good option? Ann Hepatol. 2006 Apr-Jun;5(2):86-91. https://doi.org/10.1016/S1665-2681(19)32023-X[↩]
- Sersté T, Melot C, Francoz C, Durand F, Rautou PE, Valla D, Moreau R, Lebrec D. Deleterious effects of beta-blockers on survival in patients with cirrhosis and refractory ascites. Hepatology. 2010;52:1017–1022. doi: 10.1002/hep.23775[↩]
- Mandorfer M, Bota S, Schwabl P, Bucsics T, Pfisterer N, Kruzik M, Hagmann M, Blacky A, Ferlitsch A, Sieghart W, Trauner M, Peck-Radosavljevic M, Reiberger T. Nonselective β blockers increase risk for hepatorenal syndrome and death in patients with cirrhosis and spontaneous bacterial peritonitis. Gastroenterology 2014; 146: 1680-90. :e1. doi: 10.1053/j.gastro.2014.03.005[↩]
- Blasco-Algora S, Masegosa-Ataz J, Alonso S, Gutiérrez ML, Fernández-Rodriguez C. Non-selective β-blockers in advanced cirrhosis: a critical review of the effects on overall survival and renal function. BMJ Open Gastroenterol. 2016;3:e000104. doi: 10.1136/bmjgast-2016-000104[↩]
- Bureau C, Péron JM, Alric L, Morales J, Sanchez J, Barange K, Payen JL, Vinel JP. “A La Carte” treatment of portal hypertension: Adapting medical therapy to hemodynamic response for the prevention of bleeding. Hepatology. 2002;36:1361–1366. doi: 10.1053/jhep.2002.36945[↩]
- García-Pagán JC, Feu F, Bosch J, Rodés J. Propranolol compared with propranolol plus isosorbide-5-mononitrate for portal hypertension in cirrhosis. A randomized controlled study. Ann Intern Med. 1991;114:869–873. doi: 10.7326/0003-4819-114-10-869[↩]
- Wang C, Han J, Xiao L, Jin CE, Li DJ, Yang Z. Efficacy of vasopressin/terlipressin and somatostatin/octreotide for the prevention of early variceal rebleeding after the initial control of bleeding: a systematic review and meta-analysis. Hepatol Int. 2015;9:120–129. doi: 10.1007/s12072-014-9594-9[↩]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69:406–460. doi: 10.1016/j.jhep.2018.03.024[↩]
- Bari K, Garcia-Tsao G. Treatment of portal hypertension. World J Gastroenterol. 2012;18:1166–1175. doi: 10.3748/wjg.v18.i11.1166[↩]
- Escorsell A, Bandi JC, Andreu V, Moitinho E, García-Pagán JC, Bosch J, Rodés J. Desensitization to the effects of intravenous octreotide in cirrhotic patients with portal hypertension. Gastroenterology. 2001;120:161–169. doi: 10.1053/gast.2001.20892[↩]
- Portal Hypertension. https://www.msdmanuals.com/home/liver-and-gallbladder-disorders/manifestations-of-liver-disease/portal-hypertension[↩][↩]
- Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913[↩]
- Calmet F, Martin P, Pearlman M. Nutrition in Patients With Cirrhosis. Gastroenterol Hepatol (N Y). 2019 May;15(5):248-254. https://pmc.ncbi.nlm.nih.gov/articles/PMC6589840[↩]
- Lai JC, Tandon P, Bernal W, et al. Malnutrition, frailty, and sarcopenia in patients with cirrhosis: 2021 practice guidance by the American Association for the Study of Liver Diseases [published correction appears in Hepatology. 2021 Dec;74(6):3563]. Hepatology. 2021;74(3):1611–1644. doi:10.1002/hep.32049[↩]
- Asrani S. K., Devarbhavi H., Eaton J., Kamath P. S. (2019). Burden of liver diseases in the world. J. Hepatol. 70 (1), 151–171. 10.1016/j.jhep.2018.09.014[↩][↩]
- GBD 2017 Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020 Mar;5(3):245-266. doi: 10.1016/S2468-1253(19)30349-8[↩][↩]
- Tapper E. B., Parikh N. D. (2023). Diagnosis and management of cirrhosis and its complications: a review. Jama 329 (18), 1589–1602. 10.1001/jama.2023.5997[↩]
- Wazir H., Abid M., Essani B., Saeed H., Ahmad Khan M., Nasrullah F., et al. (2023). Diagnosis and treatment of liver disease: current trends and future directions. Cureus 15 (12), e49920. 10.7759/cureus.49920[↩]
- Huang D. Q., Terrault N. A., Tacke F., Gluud L. L., Arrese M., Bugianesi E., et al. (2023). Global epidemiology of cirrhosis – aetiology, trends and predictions. Nat. Rev. Gastroenterol. Hepatol. 20 (6), 388–398. 10.1038/s41575-023-00759-2[↩]
- Vinaixa C, Rubín A, Aguilera V, Berenguer M. Recurrence of hepatitis C after liver transplantation. Ann Gastroenterol. 2013;26(4):304-313. https://pmc.ncbi.nlm.nih.gov/articles/PMC3959489[↩]





{kind=link}