Contents
- LDL cholesterol
- What is cholesterol?
- How is my cholesterol tested?
- Cholesterol levels
- What is HDL cholesterol?
- Symptoms for high cholesterol
- Why is high cholesterol bad?
- High cholesterol causes
- Foods not to eat with high cholesterol
- How to lower LDL cholesterol
- Foods to lower cholesterol
LDL cholesterol
LDL cholesterol or LDL-C is an abbreviation for low-density lipoprotein cholesterol that’s often called “bad” cholesterol because high levels of LDL-cholesterol can contribute to the formation of plaque buildup in walls of your arteries. This fatty deposits or “plaque” buildup in the walls of your arteries is called atherosclerosis and it can increase your risk of heart disease and stroke. LDL is a spherical particle with a 22 nm diameter and a molecular weight of 2500 kDa 1. LDL cholesterol particles are derived from very low density lipoprotein (VLDL) and intermediate-density lipoprotein (IDL) particles and are even more enriched in cholesterol 2. LDL consists of a spectrum of particles varying in size and density with a hydrophobic nucleus of about 1600 cholesterol ester molecules and 170 triglyceride molecules surrounded by a superficial monolayer of 700 phospholipids molecules (mainly phosphatidylcholine) and 600 molecules of free cholesterol. The predominant apolipoprotein B-100 (apoB-100) is found embedded in a monolayer; it consists of 4536 residues of amino acids, with a molecular weight of 500 kDa and each LDL particle contains one apolipoprotein B-100 (apoB-100) molecule (Figure 1).
LDL cholesterol functions as a carrier for most of the cholesterol in your blood, it delivers cholesterol to your cells. An abundance of small dense LDL particles is seen in association with hypertriglyceridemia, low HDL levels, obesity, type 2 diabetes (i.e. patients with the metabolic syndrome) and infectious and inflammatory states. These small dense LDL particles are considered to be more pro-atherogenic than large LDL particles for a number of reasons 3. Small dense LDL particles have a decreased affinity for the LDL receptor (LDLR) resulting in a prolonged retention time in your blood. Additionally, LDL particles more easily enter the arterial wall and bind more avidly to intra-arterial proteoglycans, which traps them in the arterial wall. Finally, small dense LDL particles are more susceptible to oxidation, which could result in an enhanced uptake by macrophages. So when your body has too much LDL cholesterol, the LDL cholesterol can build up on the walls of your arteries and this buildup can lead to blood vessels blockages that prevent blood from flowing properly to your heart causing health problems, such as heart disease and stroke.
Since LDL-cholesterol is the “bad” kind of cholesterol, a low LDL level is considered good for your heart health. You want your LDL below 70 milligrams per deciliter (mg/dl). A diet high in saturated fat and trans fat is unhealthy because it tends to increase your LDL cholesterol levels. Your LDL levels may be high if you eat a diet with a lot of saturated fat, cholesterol, or both. Sometimes, an under-active thyroid called hypothyroidism may also increase your LDL levels.
An unhealthy lifestyle is the most common cause of high “bad” LDL cholesterol or low “good” HDL cholesterol. However, the genes that you inherit from your parents, other medical conditions, and some medicines may also raise “bad” LDL cholesterol levels or lower “good” HDL cholesterol levels.
Factors that can affect “bad” LDL cholesterol:
- Your genes and lifestyle habits play a major role in your cholesterol levels.
- Unhealthy lifestyle habits:
- Eating a lot of foods high in saturated fats raises “bad” LDL cholesterol levels. Saturated fats are found in fatty cuts of red meat and dairy products. No more than 10% of your daily calories should come from saturated fats.
- Lack of physical activity is linked to a higher risk of having unhealthy blood cholesterol levels.
- Smoking lowers “good” HDL cholesterol, particularly in women, and raises “bad” LDL cholesterol.
- Stress may raise levels of certain hormones, such as corticosteroids. These can cause your body to make more cholesterol.
- Drinking too much alcohol (more than two drinks a day for men or one drink a day for women) can raise your total cholesterol level.
- Getting little or low-quality sleep has been linked to lower cardiovascular health. Getting 7 to 9 hours of sleep a day lowers your risk for high “bad” cholesterol (LDL) and total cholesterol.
- Familial hypercholesterolemia. Familial hypercholesterolemia is a genetic disorder caused by gene mutations involving the LDLR gene (codes for the LDL receptor), APOB gene (which codes for apolipoprotein B-100) or PCSK9 gene (which codes for Proprotein Convertase Subtilisin/Kexin Type 9 [PCSK9]) that causes high levels of “bad” LDL cholesterol in your blood and increases the risk of early heart disease 4, 5, 6. People with familial hypercholesterolemia have a high risk of developing a form of heart disease called coronary artery disease at a young age 7.
- Other factors that can contribute to unhealthy cholesterol levels include:
- Obesity. Having a body mass index (BMI) of 30 or greater puts you at risk of high cholesterol.
- Unhealthy diet. Eating too much saturated fat or trans fats can result in unhealthy cholesterol levels. Saturated fats are found in fatty cuts of meat and full-fat dairy products. Trans fats are often found in packaged snacks or desserts.
- Medical conditions, such as chronic kidney disease, diabetes, HIV/AIDS, hypothyroidism (under-active thyroid), polycystic ovary syndrome (PCOS), sleep apnea and lupus
- Certain medicines that you take for other health problems can raise your level of “bad” LDL cholesterol or lower your level of “good” HDL cholesterol, including:
- Arrhythmia medicines, such as amiodarone
- Beta-blockers for relieving angina chest pain or treating high blood pressure
- Chemotherapy medicines used to treat cancer
- Diuretics (water pills), such as thiazide, to treat high blood pressure
- Immunosuppressive medicines, such as cyclosporine, to treat inflammatory diseases or to prevent rejection after organ transplant
- Retinoids to treat acne
- Steroids, such as prednisone, to treat inflammatory diseases such as lupus, rheumatoid arthritis, and psoriasis
- Your race or ethnicity may affect your risk of high blood cholesterol:
- Overall, non-Hispanic White people are more likely than other groups to have high levels of total cholesterol.
- Asian Americans, including those of Indian, Filipino, Japanese, and Vietnamese descent, are more likely to have high levels of “bad” LDL cholesterol than other groups.
- Hispanic Americans are more likely to have lower levels of “good” HDL cholesterol than other groups.
- African Americans are more likely than other groups to have high levels of “good” HDL cholesterol.
- Your age. Unhealthy levels of cholesterol can affect people of all ages, even young children. However, high cholesterol is most commonly diagnosed in people between ages 40 and 59. As you get older, your body’s metabolism changes. Your liver does not remove “bad” LDL cholesterol as well as it did when you were young. These normal changes may increase your risk for developing high blood cholesterol as you age.
- Your sex. Between ages 20 and 39, men have a greater risk for high total cholesterol than women. A woman’s risk goes up after menopause. Menopause lowers levels of female hormones that may protect against high blood cholesterol. After menopause, women’s levels of total and “bad” LDL cholesterol usually go up, while their levels of “good” HDL cholesterol go down.
Unfortunately, high cholesterol has no symptoms (asymptomatic) and only a blood test called lipoprotein panel, lipid panel or lipid profile can detect if you have high cholesterol. Most people do not know they have high blood cholesterol until they have a blood test during a routine healthcare visit. Your doctor may ask you to fast for 8 to 12 hours (consuming no food or liquids other than water) before having a blood test for cholesterol (lipid panel). According to the National Heart, Lung, and Blood Institute, a person’s first cholesterol screening should occur between the ages of 9 and 11, and then be repeated every five years after that 8.
Here is a general guide for when a blood cholesterol test should be done 8:
- Ages 19 or younger: Screening begins at ages 9 to 11 and should be repeated every 5 years. Screening may be performed as early as age 2 if there is a family history of high blood cholesterol, heart attack, or stroke.
- Ages 20 to 65: Younger adults should be screened every 5 years. Men ages 45 to 65 and women ages 55 to 65 should be screened every 1 to 2 years.
- Older than 65: Older adults should be screened every year.
In the United States, cholesterol levels are measured in milligrams (mg) of cholesterol per deciliter (dL) of blood. In Canada and many European countries, cholesterol levels are measured in millimoles per liter (mmol/L). To interpret your test results, use these general guidelines.
Table 1. Total Cholesterol Levels
| Total cholesterol (U.S. and some other countries) | Total cholesterol* (Canada and most of Europe) | Results |
|---|---|---|
| Below 200 mg/dL | Below 5.2 mmol/L | Desirable |
| 200 to 239 mg/dL | 5.2 to 6.2 mmol/L | Borderline high |
| 240 mg/dL and above | Above 6.2 mmol/L | High |
Footnotes: Total cholesterol = HDL “good” cholesterol + LDL “bad” cholesterol + 20% triglycerides. “Total cholesterol” is the total amount of cholesterol that’s circulating in your blood. Your “Total cholesterol” should be below 200 milligrams per deciliter of blood (less than 200 mg/dL) or 5.18 mmol/L.
[Source 9 ]Table 2. LDL “bad” Cholesterol Levels
| LDL cholesterol (U.S. and some other countries) | LDL cholesterol* (Canada and most of Europe) | Results |
|---|---|---|
| Below 70 mg/dL | Below 1.8 mmol/L | Best for people who have coronary artery disease — including a history of heart attacks, angina, stents or coronary bypass. |
| Below 100 mg/dL | Below 2.6 mmol/L | Optimal for people at risk of coronary artery disease or who have diabetes. Near optimal for people with uncomplicated coronary artery disease. |
| 100-129 mg/dL | 2.6-3.3 mmol/L | Near optimal if there is no coronary artery disease. High if there is coronary artery disease. |
| 130-159 mg/dL | 3.4-4.1 mmol/L | Borderline high if there is no coronary artery disease. High if there is coronary artery disease. |
| 160-189 mg/dL | 4.1-4.9 mmol/L | High if there is no coronary artery disease. Very high if there is coronary artery disease. |
| 190 mg/dL and above | Above 4.9 mmol/L | Very high, likely representing a genetic condition. |
Table 3. HDL “good” Cholesterol Levels
| HDL cholesterol (U.S. and some other countries) | HDL cholesterol* (Canada and most of Europe) | Results |
|---|---|---|
| Below 40 mg/dL (men) | Below 1.0 mmol/L (men) | Poor |
| Below 50 mg/dL (women) | Below 1.3 mmol/L (women) | |
| 40-59 mg/dL (men) | 1.0-1.5 mmol/L (men) | Better |
| 50-59 mg/dL (women) | 1.3-1.5 mmol/L (women) | |
| 60 mg/dL and above | Above 1.5 mmol/L | Best |
Table 4. Triglycerides Levels
| Triglycerides (U.S. and some other countries) | Triglycerides* (Canada and most of Europe) | Results |
|---|---|---|
| Below 150 mg/dL | Below 1.7 mmol/L | Desirable |
| 150-199 mg/dL | 1.7-2.2 mmol/L | Borderline high |
| 200-499 mg/dL | 2.3-5.6 mmol/L | High |
| 500 mg/dL and above | Above 5.6 mmol/L | Very high |
Footnotes: Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels.
[Source 9 ]Figure 1. Low-density lipoprotein (LDL) cholesterol structure

Footnote: The LDL is a spherical particle consisting of the cholesterol ester, triglycerides, phospholipids, free cholesterol and apolipoprotein B-100.
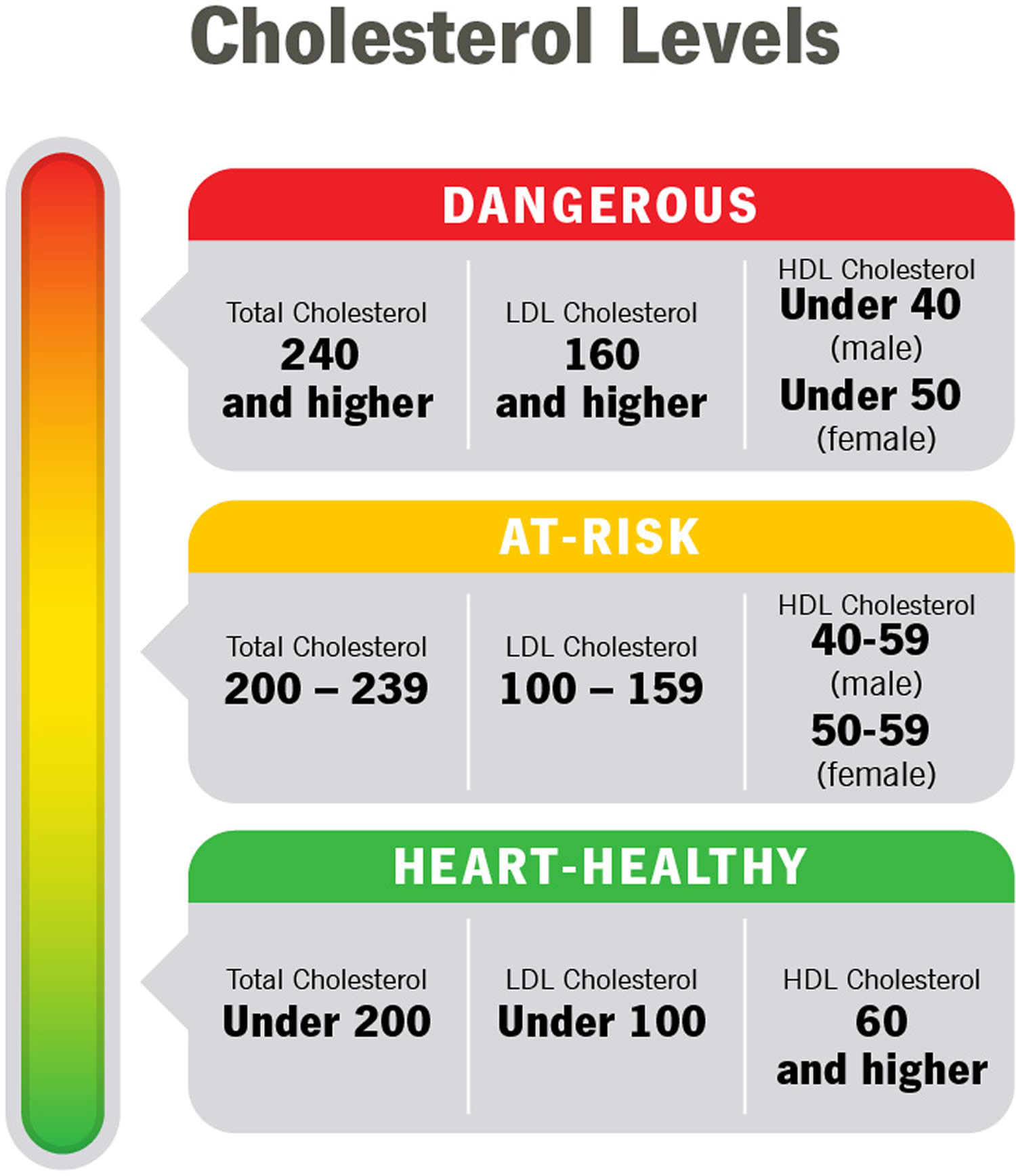
[Source 1 ]Figure 2. Cholesterol levels
If your cholesterol test results aren’t within desirable ranges, your doctor might recommend more-frequent measurements. Your doctor might also suggest more-frequent tests if you have a family history of high cholesterol, heart disease or other risk factors, such as diabetes or high blood pressure.
If your cholesterol levels are very high, you may notice the following signs:
- Fatty bumps (xanthomas) on your skin, especially on the elbows, joints, knees, hands, ankles, or buttocks
- Grayish-white rings (corneal arcus) that appear around the cornea in your eye
These signs develop mostly in people who have very high cholesterol that runs in families (familial hypercholesterolemia).
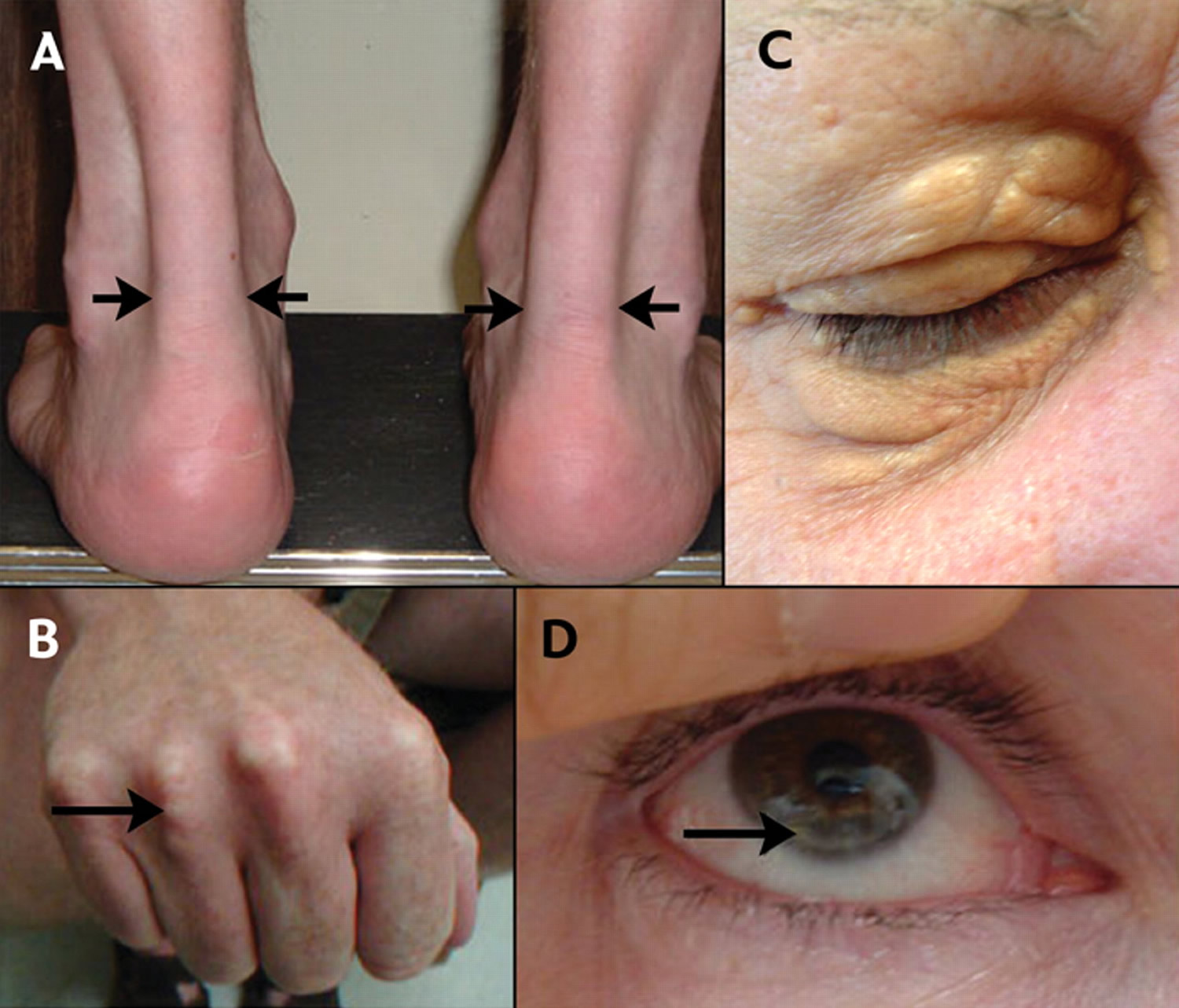
Figure 3. Familial hypercholesterolemia – Physical signs of heterozygous familial hypercholesterolemia, as a result of cholesterol deposition within macrophages in specific sites.
To treat unhealthy blood cholesterol levels, your doctor may recommend lifestyle changes such as exercising and eating a healthy diet. But, if you’ve made these important lifestyle changes and your cholesterol levels remain high, your doctor might recommend medication. If you have a medical condition or medicine is causing your blood cholesterol problem, your doctor may treat that condition or change your medicine or its dose.
If you have high LDL or total cholesterol, you can lower your risk of heart disease by:
- Stop smoking if you smoke
- Maintaining a healthy weight. Lose extra pounds and maintain a healthy weight. Research has shown that adults with overweight and obesity can lower “bad” LDL cholesterol and raise “good” HDL cholesterol by losing only 3% to 5% of their weight.
- Avoid foods high in saturated fat, dietary cholesterol, and extra calories. Eat a low-salt diet that emphasizes fruits, vegetables and whole grains
- Limiting your alcohol and salt intake
- Exercise for at least 30 minutes on most days. Studies have shown that physical activity can lower LDL cholesterol and triglycerides and raise your “good” HDL cholesterol. For example, resistance training among postmenopausal women may decrease total cholesterol, LDL cholesterol, and triglycerides. Before starting any exercise program, ask your provider what level of physical activity is right for you.
- Getting 7 to 9 hours of sleep a day lowers your risk for high “bad” cholesterol (LDL) and total cholesterol.
- Managing stress. Research has shown that chronic stress can sometimes increase LDL cholesterol levels and decrease HDL cholesterol levels.
The following foods can lower your bad LDL cholesterol.
- Vegetables such as leafy greens (spinach, collard greens, kale, cabbage), broccoli, and carrots
- Fruits such as apples, bananas, oranges, pears, grapes, and prunes
- Whole grains such as plain oatmeal, brown rice, and whole-grain bread or tortillas
- Fat-free or low-fat dairy foods such as milk, cheese, or yogurt
- Protein-rich foods:
- Fish high in omega-3 fatty acids (salmon, tuna, and trout)
- Lean meats such as 95% lean ground beef or pork tenderloin or skinless chicken or turkey
- Eggs
- Nuts, seeds, and soy products (tofu)
- Beans and legumes such as kidney beans, lentils, chickpeas, black-eyed peas, and lima beans
- Oils and foods high in monounsaturated and polyunsaturated fats:
- Canola, corn, olive, safflower, sesame, sunflower, and soybean oils (not coconut or palm oil)
- Nuts such as walnuts, almonds, and pine nuts
- Nut and seed butters
- Salmon and trout
- Seeds (sesame, sunflower, pumpkin, or flax)
- Avocados
- Tofu
The choice of medication or combination of medications depends on various factors, including your personal risk factors, your age, your health and possible drug side effects. Common choices include:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. Choices include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor).
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can be used with a statin drug.
- Bempedoic acid. This newer drug works in much the same way as statins but is less likely to cause muscle pain. Adding bempedoic acid (Nexletol) to a maximum statin dosage can help lower LDL significantly. A combination pill containing both bempedoic acid and ezetimibe (Nexlizet) also is available.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- PCSK9 inhibitors. These drugs can help your liver absorb more LDL cholesterol, which lowers the amount of cholesterol circulating in your blood. Alirocumab (Praluent) and evolocumab (Repatha) might be used for people who have a genetic condition that causes very high levels of LDL or in people with a history of coronary disease who have intolerance to statins or other cholesterol medications. They are injected under the skin every few weeks and are expensive.
If you also have high triglycerides, your doctor might prescribe:
- Fibrates. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Using fibrates with a statin can increase the risk of statin side effects.
- Niacin. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins.
- Omega-3 fatty acid supplements. Omega-3 fatty acid supplements can help lower your triglycerides. They are available by prescription or over-the-counter. If you choose to take over-the-counter supplements, get your doctor’s OK. Omega-3 fatty acid supplements could affect other medications you’re taking.
Some people with familial hypercholesterolemia may benefit from lipoprotein apheresis to lower their blood cholesterol levels. Lipoprotein apheresis uses a filtering machine to remove unwanted substances from the body. The machine removes “bad” LDL cholesterol from the blood, then returns the remainder of the blood to your body.
What is cholesterol?
Cholesterol is a waxy, fat-like substance that’s found in all the cells in your body. Cholesterol is produced by your body and also found in some foods. Your body needs some cholesterol to make hormones, vitamin D and substances that help you digest foods. Cholesterol comes from two sources. Your liver makes all of the cholesterol your body needs to form cell membranes and to make certain hormones. Cholesterol is also found in foods from animal sources, such as egg yolks, meat, and cheese, which is called dietary cholesterol. Although we often blame the cholesterol found in foods that we eat for raising blood cholesterol, the main culprit is actually saturated fat. Foods rich in saturated fat include butter fat in milk products, fat from red meat, and tropical oils such as coconut oil.
Cholesterol travels to cells through your bloodstream in special carriers called lipoproteins. Two of the most important lipoproteins are low-density lipoprotein (LDL) and high-density lipoprotein (HDL).
There are different types of cholesterol:
- HDL stands for high-density lipoprotein or HDL-C (high-density lipoprotein cholesterol). HDL is sometimes called “good cholesterol” because it carries harmful cholesterol from other parts of your body including your arteries back to your liver. Your liver then removes the cholesterol from your body and helps protect you from heart attack and stroke. A healthy HDL-cholesterol level may protect against heart attack and stroke. If you have low HDL levels, you have a greater heart disease risk, even if your total cholesterol is below 200 mg/dL. Your doctor will evaluate your HDL and other cholesterol levels and other factors to assess your risk for heart attack or stroke. People with high blood triglycerides usually also have lower levels of HDL. Genetic factors, Type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do, because the female hormone estrogen raises HDL, but this can change after menopause.
- LDL stands for low-density lipoprotein or LDL-C (low-density lipoprotein cholesterol). LDL is sometimes called “bad cholesterol” because a high LDL level leads to the buildup of plaque in your arteries. LDL is the most important lipid for predicting your heart disease risk. Low-density lipoprotein (LDL or ‘bad’) cholesterol can join with fats and other substances to build up (also known as plaque) in the inner walls of your arteries, which starts a disease process called atherosclerosis. The arteries can become clogged and narrow, and blood flow is reduced. When plaque builds up in your coronary arteries that supply blood to your heart, you are at greater risk of having a heart attack. Since LDL is the bad kind of cholesterol, a low LDL level is considered good for your heart health. A diet high in saturated and trans fat is unhealthy because it tends to raise LDL cholesterol levels. Your LDL levels may be high if you eat a diet with a lot of saturated fat, cholesterol, or both. Sometimes, an under-active thyroid called hypothyroidism may also increase LDL levels.
- VLDL stands for very low-density lipoprotein or VLDL-C (very low-density lipoprotein cholesterol). Some people also call VLDL a “bad cholesterol” because it too contributes to the buildup of plaque in your arteries. But VLDL and LDL are different; VLDL mainly carries triglycerides and LDL mainly carries cholesterol. VLDL particles are released into the blood by the liver and circulate in the bloodstream, ultimately being converted into LDL as they lose triglyceride, having carried it to other parts of the body. According to the National Heart, Lung and Blood Institute’s National Cholesterol Education Program Guidelines ATP III, there is growing evidence that VLDL plays an important role in atherogenesis, in which plaques form on the interior walls of arteries, narrowing these passageways and restricting blood flow, which can lead to heart disease and increase the risk of stroke. Currently, direct measurement of VLDL cholesterol requires specialized testing. However, since VLDL-C contains most of the circulating triglyceride (if a person is fasting) and since the composition of the different particles is relatively constant, it is possible to estimate the amount of VLDL-C based on the triglyceride value. To estimate VLDL-C, divide the triglyceride value by 5 if the value is in mg/dL or divide by 2.2 if the value is in mmol/L. In most cases, this formula provides a good estimate of VLDL-C. However, this formula becomes less accurate with increased triglyceride levels when, for example, a person has not fasted before having blood drawn. The calculation is not valid when the triglyceride level is greater than 400 mg/dl (4.5 mmol/L) because other lipoproteins are usually present. In this situation, VLDL-C may be measured directly using specialized testing.
- Triglycerides. Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. Triglycerides are fats that provide energy for your muscles. If you eat foods with a lot of saturated fat or carbohydrates, you will raise your triglyceride levels. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels. Elevated triglycerides levels are thought to lead to a greater risk of heart disease, but scientists do not agree that high triglycerides alone are a risk factor for heart disease. Normal triglyceride levels vary by age and sex. People with high triglycerides often have a high total cholesterol level, including a high LDL (bad) cholesterol level and a low HDL (good) cholesterol level. Many people with metabolic syndrome or diabetes also have high triglyceride levels. Extremely high triglyceride levels (more than 1000 mg/dL) can lead to abdominal pain and a life-threatening disorder of the pancreas called pancreatitis. Factors that can contribute to elevated triglyceride levels:
- Overweight or obesity
- Insulin resistance or metabolic syndrome
- Diabetes mellitus, especially with poor glucose control
- Alcohol consumption, especially in excess
- Excess sugar intake, especially from processed foods
- High saturated fat intake
- Hypothyroidism
- Chronic kidney disease
- Physical inactivity
- Pregnancy (especially in the third trimester)
- Inflammatory diseases (such as rheumatoid arthritis, systemic lupus erythematosus
- Some medications may also increase triglycerides.
How is my cholesterol tested?
Cholesterol is a fatty substance your body naturally creates to help in digesting food, creating hormones, and cell membranes. The substance is made up of different types of lipoproteins, which are a combination of fats, also known as lipids, and proteins. Lipids connect to proteins (lipoproteins) to be able to move through your blood. Cholesterol testing, including a lipid panel, is performed using a blood sample. Blood is most often taken from a vein in your arm. The blood sample is then analyzed in a laboratory.
When cholesterol tests are performed in a doctor’s office or another health care facility, your doctor may ask you not to eat for the eight to 12 hours leading up to testing. This is known as fasting. Cholesterol testing is often performed in the morning to make it easier for you to fast while you sleep. Usually, drinking water is allowed before your cholesterol test. Your doctor will give you any instructions you need to follow prior to having your cholesterol tested.
Cholesterol testing often measures different substances in the blood:
- High-density (HDL) cholesterol: This carries cholesterol from other parts of your body to your liver for processing and removal and is considered the “good” cholesterol.
- Low-density lipoprotein (LDL) cholesterol: This is known as the “bad” cholesterol because too much of it in your blood can lead to a buildup of plaque in your arteries, putting you at risk of heart disease, diabetes, or stroke.
- Triglycerides: These are fats created by the foods we eat, stored until your body needs energy. Triglycerides are processed by your body when it needs energy. Having high levels of triglycerides can lead to coronary heart disease and other cardiovascular issues.
- Very low-density (VLDL) cholesterol: VLDL is similar to LDL cholesterol but carries triglycerides through the blood. VLDL can contribute to plaque buildup and is considered a “bad” cholesterol.
Knowing about these different components of cholesterol testing is important to understanding the options for checking your LDL level. These levels can be estimated based on the number of other types of cholesterol in the blood or can be measured directly:
- Calculated LDL cholesterol testing: In this test, total cholesterol, HDL cholesterol, and triglycerides are used to estimate LDL cholesterol levels in your blood. Usually, LDL is calculated by subtracting the amount of HDL and VLDL from the total amount of cholesterol. In most cases, LDL cholesterol levels reported by your doctor are calculated rather than measured directly.
- Direct LDL cholesterol testing: Tests that measure only LDL cholesterol levels in your blood are called direct LDL cholesterol tests. Your doctor might use a direct LDL cholesterol test if you have a high level of triglycerides, which can make the formula-based calculation of LDL less accurate.
Most of the time, using a formula to calculate LDL cholesterol is accurate enough to provide your doctor with a useful assessment of your cholesterol levels.
Cholesterol levels
Your cholesterol levels show how much cholesterol is circulating in your blood. Your blood cholesterol levels tell you how much lipid or fat is in your blood and your cholesterol levels are expressed in milligrams per deciliter (mg/dL). High cholesterol usually has no symptoms. You can find out your blood cholesterol levels with a cholesterol or lipid profile blood test. You will need to stop eating for 10 to 12 hours before a cholesterol or lipid profile blood test, and the only liquid you may drink is water.
Total blood or serum cholesterol is a composite of different measurements. Your “total blood cholesterol” is calculated by adding your HDL (“good” cholesterol) and LDL (“bad” cholesterol) cholesterol levels, plus 20% of your triglyceride level. Here’s the formula for calculating your “total blood cholesterol”:
Total cholesterol = HDL + LDL + 20% triglycerides.
- “Total cholesterol” is the total amount of cholesterol that’s circulating in your blood. Your “Total cholesterol” should be below 200 milligrams per deciliter of blood (less than 200 mg/dL) or 5.18 mmol/L.
- Your HDL “good” cholesterol is the one number you want to be high, ideally above 60 mg/dL (1.55 mmol/L) or higher.
- Your LDL “bad” cholesterol should be below 100 mg/dL (less than 2.59 mmol/L).
- Your triglycerides should be below 150 mg/dL (less than 1.70 mmol/L). Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels.
- According to the American Heart Association, more than 43% of American adults have cholesterol levels of 200 milligrams (mg) per deciliter (dL) or higher. Talk with your doctor about what your results mean for you and how to manage your cholesterol.
“Normal cholesterol levels” are less important than your overall cardiovascular risk. Like HDL and LDL cholesterol levels, your total blood cholesterol level should be considered in context with your other known risk factors. To determine your cardiovascular risk, your doctor will consider your cholesterol test results in context with your age, sex and family history. Other risk factors, such as smoking, diabetes and high blood pressure, will be considered as well. If your risk remains uncertain, and treatment options are unclear, your doctor may consider other factors and/or request a coronary artery calcium measurement to provide greater insight into your risk and help in decision-making.
In general, you want to have a total cholesterol level below 200 mg/dL or 5.18 mmol/L. Between 200 mg/dL and 239 mg/dL, your cholesterol level is elevated or borderline-high and should be lowered if you can. With a total cholesterol level of 240 mg/dL or above, your cholesterol level is high, and there is a need for action. For example, changing your diet, beginning an exercise program, and taking statins or other cholesterol-lowering medicines are all ways to lower your cholesterol level.
Factors that can increase your risk of bad cholesterol include:
- Poor diet. Eating saturated fat, found in animal products, and trans fats, found in some commercially baked cookies and crackers and microwave popcorn, can raise your cholesterol level. Foods that are high in cholesterol, such as red meat and full-fat dairy products, will also increase your cholesterol.
- Age. Your cholesterol levels tend to rise as you get older. For instance, as you age, your liver becomes less able to remove LDL cholesterol. Even though it is less common, younger people, including children and teens, can also have high cholesterol.
- Sex. Between ages 20 and 39, men have a greater risk for high total cholesterol than women. A woman’s risk goes up after menopause. Menopause lowers levels of female hormones that may protect against high blood cholesterol. After menopause, women’s levels of total and “bad” LDL cholesterol usually go up, while their levels of “good” HDL cholesterol go down.
- Heredity. High blood cholesterol can run in families.
- Weight. Being overweight or having obesity raises your cholesterol level. Having a body mass index (BMI) of 30 or greater puts you at risk of high cholesterol.
- Race. Certain races may have an increased risk of high cholesterol.
- Overall, non-Hispanic White people are more likely than other groups to have high levels of total cholesterol.
- Asian Americans, including those of Indian, Filipino, Japanese, and Vietnamese descent, are more likely to have high levels of “bad” LDL cholesterol than other groups.
- Hispanic Americans are more likely to have lower levels of “good” HDL cholesterol than other groups.
- African Americans are more likely than other groups to have high levels of “good” HDL cholesterol.
- Lack of exercise. Being physically inactive contributes to overweight and can raise LDL and lower HDL. Exercise helps boost your body’s HDL, or “good,” cholesterol while increasing the size of the particles that make up your LDL, or “bad,” cholesterol, which makes it less harmful.
- Smoking. Cigarette smoking damages the walls of your blood vessels, making them more prone to accumulate fatty deposits. Smoking might also lower your level of HDL, or “good,” cholesterol.
- Diabetes. High blood sugar contributes to higher levels of a dangerous cholesterol called very-low-density lipoprotein (VLDL) and lower HDL cholesterol. High blood sugar also damages the lining of your arteries.
There are usually no signs or symptoms that you have high cholesterol. A blood test is the only way to detect if you have it. The American Heart Association recommends all adults age 20 or older with no other risk factors for heart disease should have their cholesterol (and other traditional risk factors) checked every four to six years. If certain factors put you at high risk, or if you already have heart disease, your doctor may ask you to check it more often. Work with your doctor to determine your risk for cardiovascular disease and stroke and create a plan to reduce your risk.
If you have risk factors or if previous testing showed that you had a high cholesterol level, more frequent testing with a full lipid panel is recommended.
Examples of risk factors other than high LDL include:
- Cigarette smoking
- Being overweight or obese
- Unhealthy diet
- Being physically inactive—not getting enough exercise
- Age (if you are a male 45 years or older or a female 50-55 years or older)
- Hypertension (blood pressure of 140/90 or higher or taking high blood pressure medications)
- Family history of premature heart disease (heart disease in a first-degree male relative under age 55 or a first-degree female relative under age 65)
- Pre-existing heart disease or already having had a heart attack
- Diabetes or prediabetes
For people who are age 20 or older:
- Younger adults should have the test every 5 years
- Men ages 45 to 65 and women ages 55 to 65 should have it every 1 to 2 years.
Children, teens, and young adults (ages 2 to 24 years old) with no risk factors should have a lipid panel once between the ages of 9 and 11 and again between 17 and 21, according to the American Academy of Pediatrics.
For people who are age 19 or younger:
- The first test should be between ages 9 to 11
- Children should have the test again every 5 years
- Some children may have this test starting at age 2 if there is a family history of high blood cholesterol, heart attack, or stroke.
Children, teens, and young adults with an increased risk of developing heart disease as adults should have earlier and more frequent screening with lipid panels. Some of the risk factors are similar to those in adults and include a family history of heart disease or health problems such as diabetes, high blood pressure, or being overweight. High-risk children should be tested between 2 and 8 years old with a fasting lipid panel, according to the American Academy of Pediatrics.
Children younger than 2 years old are too young to be tested.
Table 5. Normal Cholesterol Levels
| Age | Total cholesterol | Non-HDL cholesterol | LDL (“bad” cholesterol) | HDL (“good” cholesterol) |
|---|---|---|---|---|
| 19 and younger | Below 170 milligrams per deciliter of blood (mg/dL) | Below 120 mg/dL | Below 110 mg/dL | Above 45 mg/dL |
| 20 and older Male | 125 to 200 milligrams per deciliter of blood (mg/dL) | Below 130 mg/dL | Below 100 mg/dL | 40 mg/dL or higher |
| 20 and older Female | 125 to 200 milligrams per deciliter of blood (mg/dL) | Below 130 mg/dL | Below 100 mg/dL | 50 mg/dL or higher |
Footnotes: As you review your results, remember that you want your LDL to be low and your HDL to be high. Ideally, your HDL should be above 60 mg/dL (1.55 mmol/L). It’s the helpful cholesterol. An HDL above 60 mg/dL (greater than 1.55 mmol/L) offers you protection against heart disease.
Table 6. High Cholesterol Levels
| Age | Total cholesterol | Non-HDL cholesterol | LDL (“bad” cholesterol) |
|---|---|---|---|
| 19 and younger | Borderline high: 170-199 mg/dL High: 200 mg/dL or higher | Borderline high: 120-144 mg/dL High: 145 mg/dL or higher | Borderline high: 110-129 mg/dL High: 130 mg/dL or higher |
| 20 and older | Borderline high: 200-239 mg/dL High: 240 mg/dL or higher | High: 130 mg/dL or higher | Near-optimal: 100-129 mg/dL Borderline high: 130-159 mg/dL High: 160-189 mg/dL Very high: 190 mg/dL or higher |
Footnotes: High cholesterol generally means your total cholesterol is 200 mg/dL (greater than 5.18 mmol/L) or higher. But doctors use additional categories like “borderline high” and “near optimal” to break down your results. If your numbers are close to normal levels, they may be easier to manage through lifestyle and dietary changes.
Table 7. Desirable Cholesterol Levels
| Desirable Cholesterol Levels | |
|---|---|
| Total cholesterol | Less than 200 milligrams per deciliter of blood (mg/dL) or 5.18 mmol/L |
| LDL (“bad” cholesterol) | Less than 100 mg/dL (2.59 mmol/L) |
| HDL (“good” cholesterol) | 60 mg/dL (1.55 mmol/L) or higher |
| Triglycerides | Less than 150 mg/dL (1.70 mmol/L) |
What is HDL cholesterol?
HDL stands for high density lipoprotein or HDL-C (high-density lipoprotein cholesterol). HDL is sometimes called “good cholesterol” because it carries harmful cholesterol from other parts of your body including your arteries back to your liver. Your liver then removes the cholesterol from your body and helps protect you from heart attack and stroke. A healthy HDL-cholesterol level may protect against heart attack and stroke. If you have low HDL levels, you have a greater heart disease risk, even if your total cholesterol is below 200 mg/dL. Your doctor will evaluate your HDL and other cholesterol levels and other factors to assess your risk for heart attack or stroke. People with high blood triglycerides usually also have lower levels of HDL. Genetic factors, type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do, because the female hormone estrogen raises HDL, but this can change after menopause.
Experts believe HDL cholesterol may act in a variety of helpful ways that tend to reduce the risk for heart disease 11:
- High HDL cholesterol 60 mg/dL or higher is Protective against heart disease.
- HDL cholesterol scavenges and removes LDL or “bad” cholesterol.
- HDL reduces, reuses, and recycles LDL cholesterol by transporting it to the liver where it can be reprocessed.
- HDL cholesterol acts as a maintenance crew for the inner walls (endothelium) of blood vessels. Damage to the inner walls is the first step in the process of atherosclerosis, which causes heart attacks and strokes. HDL scrubs the wall clean and keeps it healthy.
People with high blood triglycerides usually also have lower HDL cholesterol. Genetic factors, type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do.
A healthy HDL cholesterol level may protect against heart attack and stroke. Studies show low levels of HDL cholesterol increase the risk of heart disease. HDL cholesterol does not completely eliminate LDL cholesterol. Only one-fourth to one-third of blood cholesterol is carried by HDL.
HDL levels should be around 50 mg/dL. Some people can raise HDL by::
- Exercising for at least 30 minutes 5 times a week
- Quitting smoking
- Avoiding saturated fats
- Losing weight
Others may need medicine to get HDL to a beneficial level, and should work with your doctor on a treatment plan.
What can you do if your HDL cholesterol is Low?
If your HDL levels is low, you can take several steps to boost your HDL level and reduce your heart disease risk 12:
- Get physically active or exercise – Aerobic exercise for 30 to 60 minutes on most days of the week can help pump up your HDL levels. Some studies suggest that physical activity can raise HDL cholesterol. The American Heart Association recommends three to four 40-minute sessions of moderate- to vigorous-intensity aerobic activity per week for adults trying to lower their LDL cholesterol or blood pressure.
- Eat better fats. The monounsaturated and polyunsaturated fats described above can raise HDL cholesterol levels.
- Cut out trans fats. Not only do they increase LDL cholesterol, they decrease HDL cholesterol too.
- Quit smoking – Tobacco smoke lowers HDL, and quitting can increase HDL levels.
- Keep a healthy weight – Being overweight increases LDL cholesterol and reduces HDL cholesterol levels. Losing even a few pounds will increase your HDL-C and lower your LDL-C and blood pressure. Avoiding obesity besides improving HDL levels, reduces risk for heart disease and multiple other health conditions.
Symptoms for high cholesterol
There are usually no signs or symptoms that you have high cholesterol. A blood test is the only way to detect if you have it. Most people do not know they have high blood cholesterol until they have a blood test during a routine healthcare visit.
If your cholesterol levels are very high, you may notice the following signs:
- Fatty bumps also called xanthomas on your skin, especially on the elbows, joints, knees, hands, ankles, or buttocks.
- Grayish-white rings also called arcus senilis that appear around the cornea in your eye.
These signs develop mostly in people who have very high cholesterol that runs in families or familial hypercholesterolemia.
Undiagnosed or untreated high blood cholesterol can lead to serious problems, such as heart attack and stroke. High cholesterol can cause a dangerous accumulation of cholesterol and other deposits on the walls of your arteries (atherosclerosis). These deposits (plaques) can reduce blood flow through your arteries, which can cause complications, such as:
- Chest pain also known as angina. If the arteries that supply your heart with blood (coronary arteries) are affected, you might have chest pain (angina) and other symptoms of coronary artery disease.
- Heart attack. If plaques tear or rupture, a blood clot can form at the plaque-rupture site — blocking the flow of blood or breaking free and plugging an artery downstream. If blood flow to part of your heart stops, you’ll have a heart attack.
- Stroke. Similar to a heart attack, a stroke occurs when a blood clot blocks blood flow to part of your brain.
Talk to your doctor about your risk and steps you can take to keep your cholesterol levels in a healthy range.
Why is high cholesterol bad?
Too much cholesterol in your blood is bad for you. Cholesterol can enter your artery wall, damage its integrity and lead to the formation of atherosclerotic plaque (hardened deposits). This process of plaque buildup is called atherosclerosis. It can lead to serious problems like:
- Coronary artery disease: Blocked blood flow to your heart.
- Peripheral artery disease: Blocked blood flow to your legs and arms.
- Carotid artery disease: Blocked blood flow to your brain.
Cholesterol travels through your blood on proteins called lipoproteins. One type, LDL (low-density lipoprotein), is sometimes called the “bad” cholesterol. A high LDL level leads to a buildup of cholesterol in your arteries. Another type, HDL (high-density lipoprotein), is sometimes called the “good” cholesterol. HDL carries cholesterol from other parts of your body back to your liver. Then your liver removes the cholesterol from your body.
It’s important to keep your cholesterol in check because high cholesterol levels increase the risk of heart disease and stroke. A stroke occurs when a blood clot blocks blood flow to part of your brain. If you have too much cholesterol in your blood, it can combine with other substances in the blood to form plaque. Plaque sticks to the walls of your arteries. This buildup of plaque is known as atherosclerosis. It can lead to coronary artery disease, where your coronary arteries become narrow or even completely blocked, which can cause a heart attack (myocardial infarction). A heart attack occurs when your heart muscle tissue does not receive vital oxygen and nutrients.
Atherosclerosis (buildup of plaque in arteries) is the process that causes the artery wall to get thick and stiff. The disease process begins when LDL (“bad” cholesterol) deposits cholesterol in the artery wall. Your body has an immune response to protect itself and sends white blood cells called macrophages to engulf the invading cholesterol in the artery wall. When the macrophages are full of cholesterol, they are called foam cells because of their appearance. As more foam cells collect in the artery wall, a fatty streak develops between the intima and the media. If the process is not stopped, the fatty streak becomes a plaque, which pushes the intima into the lumen, narrowing the blood flow.
The plaque develops a fibrous coating on its outer edges. But if cholesterol continues to collect in foam cells inside the plaque, the fibrous outer coating can weaken and eventually rupture. Smaller arteries downstream from the rupture can quickly become blocked. Over time, a clot may develop at the rupture site and completely block the artery.
Evidence shows that the atherosclerotic process begins in childhood and progresses slowly into adulthood. Later in life, this often leads to coronary heart disease, the leading cause of death in the United States.
High cholesterol causes
Your body naturally produces all the LDL (bad) cholesterol it needs. However, the genes you inherit and your lifestyle habits play a major role in your cholesterol levels. The most common cause of high cholesterol is an unhealthy lifestyle. An unhealthy lifestyle makes your body produce more LDL cholesterol than it needs. This can include:
- Unhealthy eating habits or unhealthy diet, such as eating lots of bad fats. One type, saturated fat, is found in some meats, dairy products, chocolate, baked goods, and deep-fried and processed foods. Eating a lot of foods high in saturated fats raises “bad” LDL cholesterol levels. Another type, trans fat, is in some fried and processed foods. Eating these fats can raise your LDL (bad) cholesterol. No more than 10% of your daily calories should come from saturated fats.
- Lack of physical activity, with lots of sitting and little exercise. This lowers your HDL (good) cholesterol.
- Smoking or exposure to tobacco smoke, which lowers HDL cholesterol, especially in women. It also raises your LDL cholesterol.
- Being overweight or obese.
- Stress may raise levels of certain hormones, such as corticosteroids. These can cause your body to make more cholesterol.
- Drinking too much alcohol (more than two drinks a day for men or one drink a day for women) can raise your total cholesterol level.
- Getting little or low-quality sleep has been linked to lower cardiovascular health.
Genetics may also cause people to have high cholesterol. For example, some people inherit genes from their mother, father or even grandparents that cause them to have too much cholesterol. This is called familial hypercholesterolemia (FH). The severity of familial hypercholesterolemia is related to the duration and degree of LDL cholesterol in the blood. Familial hypercholesterolemia is dangerous because it can cause premature atherosclerotic heart disease. If you have a family history of familial hypercholesterolemia or problems related to high cholesterol, get your cholesterol levels checked.
Lipoprotein-a also known as Lp(a) or lipoprotein(a) is a lot like LDL cholesterol (‘bad cholesterol’) but it’s more ‘sticky’ 13. Lipoprotein-a or Lp(a) molecule includes two protein components: apolipoprotein(a) [apo(a)] and apolipoprotein B100 (apo-B100) 14. If you have high levels of lipoprotein-a or Lp(a) in your blood, it can stick to your artery walls and clog them up, leading to heart disease and stroke at a young age 15, 16, 17, 18, 19. Today, about 20-30% of people worldwide are estimated to have elevated levels of Lp(a), which are generally thought to start between 30-50 mg/dL. Currently, if a person has elevated Lipoprotein-a or Lp(a) levels, they would likely work with their cardiologist to create a plan to take steps to support heart-healthy living and minimize any risks, such as having high blood pressure or high cholesterol 20, 21, 22, 23. Some patients may also consider taking LDL cholesterol-lowering treatments, such as statins or PCSK9 inhibitors 24, 25, 26, 27. In some cases, PCSK9 inhibitors have been shown to lower Lp(a) levels by about 20-30%. Lipoprotein apheresis, which removes excess Lp(a) and LDL cholesterol from the body, is another option, but for people with higher risks 28, 29. According to the Food and Drug Administration (FDA), patients qualified for lipoprotein apheresis present with familial hypercholesterolemia, coronary artery disease and LDL-C >100 mg/dL and Lp(a) > 60 mg/dL. Lipoprotein apheresis procedure is typically performed every two weeks (in some countries weekly). During the one course (3–4 hour) the Lp(a) concentration can be lowered by 50% to 85%. Additionally, lipoprotein apheresis reduces LDL levels by 60% to 85% 30. It is expected that such Lipoprotein(a) lowering reduces the risk of atherosclerotic cardiovascular disease events.
Other medical conditions and certain medicines may also cause high cholesterol.
See your doctor about your risk of high cholesterol if you have any of the following:
- Chronic kidney disease
- Diabetes
- HIV/AIDS
- Hypothyroidism
- Lupus erythematosus
- Overweight and obesity
- Polycystic ovary syndrome (PCOS)
- Sleep apnea
For people with conditions such as lupus and HIV, the condition itself and the medicine used to treat it may lead to unhealthy cholesterol levels.
Some medicines that you take for other health problems can raise your level of “bad” LDL cholesterol or lower your level of “good” HDL cholesterol, including:
- Arrhythmia medicines, such as amiodarone
- Beta-blockers for relieving angina chest pain or treating high blood pressure
- Chemotherapy medicines used to treat cancer
- Diuretics, such as thiazide, to treat high blood pressure
- Immunosuppressive medicines, such as cyclosporine, to treat inflammatory diseases or to prevent rejection after organ transplant
- Retinoids to treat acne
- Steroids, such as prednisone, to treat inflammatory diseases such as lupus, rheumatoid arthritis, and psoriasis
Risk factors for developing high cholesterol
Factors that can increase your risk of bad cholesterol include:
- Poor diet. Eating saturated fat, found in animal products, and trans fats, found in some commercially baked cookies and crackers and microwave popcorn, can raise your cholesterol level. Foods that are high in cholesterol, such as red meat and full-fat dairy products, will also increase your cholesterol.
- Age. Your cholesterol levels tend to rise as you get older. For instance, as you age, your liver becomes less able to remove LDL cholesterol. Even though it is less common, younger people, including children and teens, can also have high cholesterol.
- Sex. Between ages 20 and 39, men have a greater risk for high total cholesterol than women. A woman’s risk goes up after menopause. Menopause lowers levels of female hormones that may protect against high blood cholesterol. After menopause, women’s levels of total and “bad” LDL cholesterol usually go up, while their levels of “good” HDL cholesterol go down.
- Heredity. High blood cholesterol can run in families.
- Weight. Being overweight or having obesity raises your cholesterol level. Having a body mass index (BMI) of 30 or greater puts you at risk of high cholesterol.
- Race. Certain races may have an increased risk of high cholesterol.
- Overall, non-Hispanic White people are more likely than other groups to have high levels of total cholesterol.
- Asian Americans, including those of Indian, Filipino, Japanese, and Vietnamese descent, are more likely to have high levels of “bad” LDL cholesterol than other groups.
- Hispanic Americans are more likely to have lower levels of “good” HDL cholesterol than other groups.
- African Americans are more likely than other groups to have high levels of “good” HDL cholesterol.
- Lack of exercise. Being physically inactive contributes to overweight and can raise LDL and lower HDL. Exercise helps boost your body’s HDL, or “good,” cholesterol while increasing the size of the particles that make up your LDL, or “bad,” cholesterol, which makes it less harmful.
- Smoking. Cigarette smoking damages the walls of your blood vessels, making them more prone to accumulate fatty deposits. Smoking might also lower your level of HDL, or “good,” cholesterol.
- Diabetes. High blood sugar contributes to higher levels of a dangerous cholesterol called very-low-density lipoprotein (VLDL) and lower HDL cholesterol. High blood sugar also damages the lining of your arteries.
Foods not to eat with high cholesterol
If you have high cholesterol you should maintain a diet that emphasizes fruits, vegetables, whole grains, low-fat dairy products, poultry, fish and nuts. Also limit your intake of red meat and sugar-sweetened foods and beverages. You should also limit both total fat and saturated fat. No more than 25 to 35 percent of your daily calories should come from dietary fats, and less than 7 percent of your daily calories should come from saturated fat. Depending upon how many calories you eat per day, here are the maximum amounts of fats that you should eat:
Table 8. Maximum amounts of total fat and saturated fat in your diet, based on calories
| Calories per Day | Total Fat | Saturated Fat |
| 1500 | 42-58 grams | 10 grams |
| 2000 | 56-78 grams | 13 grams |
| 2500 | 69-97 grams | 17 grams |
Table 9. Good and bad fats
| CHOLESTEROL-RAISING FATS | HEALTHIER FATS | ||
| Saturated Fats | Trans Fats | Monounsaturated Fats | Polyunsaturated Fats |
| Animal Sources: butter, cheese, cream, fatty cuts of meat and processed meats (hot dog, bacon, bologna, salami, sausage), ice cream, lard, poultry skin, sour cream, whole milk Plant Sources: coconut, palm, palm kerne | Foods with a high probability of containing partially hydrogenated oils: Baked Goods biscuits, cakes, cookies, doughnuts, muffins, pancake mix, pastries, pie crust, pizza dough Fried Foods French fries, breaded chicken or breaded fish Snack Foods – crackers, microwave popcorn, stick margarine, shortening and non- dairy creamer | Nuts, seeds and natural nut butters: almonds, hazelnuts, pecans, peanuts, pine nuts, pistachios, pumpkin and sesame seeds Avocados, olives Oils: canola, extra virgin olive, peanut, sesame | High omega-3 seafood: Arctic char, Atlantic mackerel, black cod (sablefish), herring, mussels, wild salmon, sardines, trout Nuts and seeds: chia, ground flaxseeds, hemp seeds, soy nuts, sunflower seeds, walnuts Oils: soybean, safflower, corn |
Saturated fat
Saturated fat is a bad fat because it raises your LDL (bad cholesterol) level more than anything else in your diet. Saturated fat is usually solid at room and refrigerator temperatures. Saturated fat is found in some meats, dairy products, cheese, chocolate, baked goods, butter, lard, and coconut and palm oils and deep-fried and processed foods. Saturated fat should make up less than 10% of your daily calories. Read food labels and choose foods that are lower in saturated fats and higher in unsaturated fats. Unsaturated fats are also known as “good” fats and are found in vegetable oils and nuts. The American Heart Association recommends a diet that emphasizes fish and poultry and limits red meat.
Foods that are high in saturated fat include:
- meat pies
- sausages and fatty cuts of meat
- butter
- lard
- cream
- hard cheese
- cakes and biscuits
- foods that contain coconut or palm oil
The amount of saturated fat in meats can vary widely, depending on the cut and how it’s prepared.
Limit saturated fats by:
- Eating leaner, lower-fat, and skinless meats instead of fatty cuts of meat and chicken with skin.
- Consuming lower-fat dairy products instead of whole-milk.
- Using certain vegetable oils (such as olive and canola oil) instead of butter, lard, and coconut and palm oils.
Here are some ways to reduce the saturated fat in meat:
- Select lean cuts of meat with minimal visible fat. Lean beef cuts include the round, chuck, sirloin or loin. Lean pork cuts include the tenderloin or loin chop. Lean lamb cuts come from the leg, arm and loin.
- Buy “choice” or “select” grades rather than “prime.” Select lean or extra lean ground beef.
- Trim all visible fat from meat before cooking.
- Broil rather than pan-fry meats such as hamburger, lamb chops, pork chops and steak.
- Use a rack to drain off fat when broiling, roasting or baking. Instead of basting with drippings, keep meat moist with wine, fruit juices or a heart-healthy oil-based marinade.
- Cook a day ahead of time. Stews, boiled meat, soup stock or other dishes in which fat cooks into the liquid can be refrigerated. Later, remove the hardened fat from the top.
- When a recipe calls for browning the meat first, try browning it under the broiler instead of in a pan.
- Eat chicken and turkey rather than duck and goose, which are usually higher in fat. Choose white meat most often when eating poultry.
- Remove the skin from chicken or turkey before cooking. If your poultry dries out too much, first try basting with wine, fruit juices or a heart-healthy oil-based marinade. Or leave the skin on for cooking and then remove it before eating.
- Limit processed meats such as sausage, bologna, salami and hot dogs. Many processed meats – even those with “reduced fat” labels – are high in calories and saturated fat. Such foods are often high in sodium, too. Read labels carefully and eat processed meats only occasionally.
- Doughnuts, cookies, crackers, muffins, pies and cakes are examples of foods high in trans fat. Don’t eat them often.
- Limit commercially fried foods and baked goods made with shortening or partially hydrogenated vegetable oils. These foods are very high in fat, and it’s likely to be trans fat.
- Limit fried fast food. Commercial shortening and deep-frying fats are still made by hydrogenation and contain saturated and trans fats.
- Opt for naturally occurring unhydrogenated vegetable oils such as canola, safflower, sunflower or olive oil.
- Look for processed foods made with unhydrogenated oil rather than saturated fat or hydrogenated (or partially hydrogenated) vegetable oils.
- Use soft margarine as a substitute for butter and choose soft margarines (liquid or tub varieties) over harder stick forms. Look for “0 g trans fat” on the Nutrition Facts label.
Try to replace foods containing saturated fats with foods that are high in unsaturated fats, such as:
- avocados or olives
- oily fish (for example, mackerel and salmon)
- nuts (for example, almonds and cashews)
- seeds (for example, sunflower and pumpkin)
- vegetable oils and spreads (for example, sunflower, olive, corn, walnut and rapeseed oils)
Trans fat
Trans fat also known as trans fatty acids or “partially hydrogenated oils” is another bad fat; it can raise your LDL (bad cholesterol) and lower your HDL (good cholesterol). Trans fat is mostly in foods made with hydrogenated oils and fats, such as stick margarine, crackers, and french fries. Trans fats are created in an industrial process that adds hydrogen to liquid vegetable oils to make them more solid. Instead of these bad fats, try healthier fats, such as lean meat, nuts, and unsaturated oils like canola, olive, and safflower oils.
Limit trans fats as much as possible by:
- Limiting foods high in trans fats. This includes foods made with partially hydrogenated oils such as some desserts, microwave popcorn, frozen pizza, stick margarines, and coffee creamers.
- Reading the nutrition labels and choosing foods that do not contain trans fats.
Dairy products and meats naturally contain very small amounts of trans fats. You do not need to avoid these foods because they have other important nutrients.
Limit foods with cholesterol
If you are trying to lower your cholesterol, you should have less than 200 mg a day of cholesterol. Cholesterol is in foods of animal origin, such as liver and other organ meats, egg yolks, shrimp, and whole milk dairy products. Choose reduced fat dairy foods such as milk (preferably unflavored), yogurt (preferably unflavored) and cheese. You can eat smaller amounts of eggs and lean poultry but limit red meat to 1-3 times a week.
Limit salt (sodium)
You should try to limit the amount of sodium (salt) that you eat to no more than 2,300 milligrams (about 1 teaspoon of salt) a day. If you have high blood pressure, you may need to limit sodium (salt) even more. Children younger than age 14 may need to eat even less sodium (salt) each day based on their sex and age. That includes all the sodium you eat, whether it was added in cooking or at the table, or already present in food products. Limiting salt won’t lower your cholesterol, but it can lower your risk of heart diseases by helping to lower your blood pressure. You can reduce your sodium by instead choosing low-salt and “no added salt” foods and seasonings at the table or while cooking. Flavor your foods with herbs and spices rather than salt, and avoid processed foods, prepackaged foods, sauces and canned foods as these contain a lot of salt too.
Try these shopping and cooking tips to help you choose and prepare foods that are lower in sodium:
- Read food labels and choose products that have less sodium for the same serving size.
- Choose low-sodium, reduced-sodium, or no-salt-added products.
- Choose fresh, frozen, or no-salt-added foods instead of pre-seasoned, sauce-marinated, brined, or processed meats, poultry, and vegetables.
- Eat at home more often so you can cook food from scratch, which will allow you to control the amount of sodium in your meals.
- Flavor foods with herbs and spices instead of salt.
- When cooking, limit your use of premade sauces, mixes, and instant products such as rice, noodles, and ready-made pasta.
Avoid added sugar
You should limit the amount of calories you get each day from added sugars. Sweetened drinks, snacks, and sweet treats are the main source of added sugars in the United States. These include sodas, sweetened coffee and tea, energy drinks, cakes, pies, ice cream, candy, syrups, and jellies. Limit these types of foods and drinks.
Reading the Nutrition labels on foods you buy and eat can help you figure out how much fat, saturated fat, cholesterol, fiber, added sugar and sodium is in the foods that you buy.
Some foods, such as fruit, contain natural sugars. Added sugars do not occur naturally in foods but instead are used to sweeten foods and drinks. They include brown sugar, corn syrup, dextrose, fructose, glucose, high-fructose corn syrup, raw sugar, and sucrose.
In the United States, sweetened drinks, snacks, and sweets are the major sources of added sugars.
- Sweetened drinks include soft drinks or sodas, fruit drinks, sweetened coffee and tea, energy drinks, alcoholic drinks, and favored waters. Sweetened drinks account for about half of all added sugars consumed.
- Snacks and sweets include grain-based desserts such as cakes, pies, cookies, brownies, doughnuts; dairy desserts such as ice cream, frozen desserts, and pudding; candies; sugars; jams; syrups; and sweet toppings.
Lower how much sugar you eat or drink by:
- Choosing drinks without added sugar such as water, low-fat or fat-free milk, or 100% vegetable juice.
- Choosing unsweetened foods for snacks or dessert.
- Eating sweetened drinks, snacks, and desserts less often and in smaller amounts.
Foods to avoid with high cholesterol
You can lower cholesterol over time by eating fewer of the foods that cause high cholesterol and more of the foods that lower cholesterol.
Saturated fats are found in all animal foods and some plant sources. You can reduce the amount of saturated fat in your food and have a healthy diet.
The following foods may be high in saturated fats. Many of them are also low in nutrients and have extra calories from sugar:
- Baked goods (cake, doughnuts, Danish)
- Fried foods (fried chicken, fried seafood, French fries)
- Fatty cuts of meat or processed meats (bacon, sausage, chicken with skin, cheeseburger, steak)
- Whole-fat dairy products (butter, ice cream, pudding, cheese, whole milk)
- Solid fats such as coconut oil, palm, and palm kernel oils (found in packaged foods)
Here are some examples of popular food items with the saturated fat content in a typical serving:
- 12 ounces (oz) or 340 g, steak — 20 g
- Cheeseburger — 10 g
- Vanilla shake — 8 g
- 1 tbsp (15 mL) butter — 7 g
It is fine to treat yourself to these types of foods once in a while. But, it is best to limit how often you eat them and limit portion sizes when you do.
You can cut how much saturated fat you eat by substituting healthier foods for less healthy options. Replace foods high in saturated fats with foods that have polyunsaturated and monounsaturated fats. Here is how to get started:
- Replace red meats with skinless chicken or fish a few days a week.
- Use canola or olive oil instead of butter and other solid fats.
- Replace whole-fat dairy with low-fat or nonfat milk, yogurt, and cheese.
- Eat more fruits, vegetables, whole grains, and other foods with low or no saturated fat.
Trans fats are made when food makers turn liquid oils into solid fats, like shortening or margarine. Trans fats can be found in many fried, “fast” packaged, or processed foods, including:
- Anything fried and battered
- Shortening and stick margarine
- Cakes, cake mixes, pies, pie crust, and doughnuts
Animal foods, such as red meats and dairy, have small amounts of trans fats. But most trans fats come from processed foods.
Trans fats are found in many processed and packaged foods. Note that these foods are often low in nutrients and have extra calories from sugar:
- Cookies, pies, cakes, biscuits, sweet rolls, and donuts
- Breads and crackers
- Frozen foods, such as frozen dinners, pizza, ice cream, frozen yogurt, milk shakes, and pudding
- Snack foods
- Fast food
- Solid fats, such as shortening and margarine
- Nondairy creamer
Not all packaged foods have trans fats. It depends on the ingredients that were used. That is why it is important to read labels.
While it is fine to treat yourself to sweets and other high-fat foods once in a while, it is best to avoid food with trans fats completely.
You can cut how much trans fat you eat by substituting healthier foods for less healthy options. Replace foods high in trans and saturated fats with foods that have polyunsaturated and monounsaturated fats. Here is how to get started:
- Use safflower or olive oil instead of butter, shortening, and other solid fats.
- Switch from solid margarine to soft margarine.
- Ask what type of fats foods are cooked in when you eat out at restaurants.
- Avoid fried, packaged, and processed foods.
- Replace meats with skinless chicken or fish a few days a week.
- Replace whole-fat diary with low-fat or nonfat milk, yogurt, and cheese.
Limit alcohol
Alcohol adds extra calories, which can lead to weight gain. Being overweight can raise your LDL level and lower your HDL level. Too much alcohol can also increase your risk of heart diseases because it can raise your blood pressure and triglyceride level. One drink is a glass of wine, beer, or a small amount of hard liquor, and the recommendation is that:
- Men should have no more than two drinks containing alcohol a day
- Women should have no more than one drink containing alcohol a day.
Your doctor may recommend that you reduce the amount of alcohol you drink or that you stop drinking alcohol. Alcohol can:
- Add calories to your daily diet and possibly cause you to gain weight.
- Raise your blood pressure and levels of triglyceride fats in your blood.
- Contribute to or worsen heart failure in some people, such as some people who have cardiomyopathy.
- Raise your risk of other diseases such as cancer.
If you do not drink, you should not start. You should not drink if you are pregnant, are under the age of 21, taking certain medicines, or if you have certain medical conditions, including heart failure.
How to lower LDL cholesterol
You can lower your LDL cholesterol level by adopting a heart-healthy lifestyle changes. They include eating a healthy diet, weight management, and regular physical activity.
- Choose heart-healthy foods. The DASH eating plans can help you lower your “bad” LDL cholesterol. These plans encourage:
- Limiting saturated fats found in fatty cuts of meats, dairy products, and desserts
- Eating whole grains, fruits, and vegetables rather than refined carbohydrates such as sweets and other high-sugar foods
- Eating a variety of nuts
- Preparing foods with little or no salt
- Get regular physical activity. Studies have shown that physical activity can lower LDL “bad” cholesterol and triglycerides and raise your “good” HDL cholesterol. For example, resistance training among postmenopausal women may decrease total cholesterol, LDL cholesterol, and triglycerides. Before starting any exercise program, ask your provider what level of physical activity is right for you.
- Aim for a healthy weight. Research has shown that adults with overweight and obesity can lower “bad” LDL cholesterol and raise “good” HDL cholesterol by losing only 3% to 5% of their weight.
- Manage stress. Research has shown that chronic stress can sometimes increase LDL cholesterol levels and decrease HDL cholesterol levels.
- Quit smoking. If you smoke, quit. Smoking can raise your risk of heart disease and heart attack and worsen other heart disease risk factors. Talk with your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke.
- Get enough good quality sleep. Getting 7 to 9 hours of sleep a day lowers your risk for high “bad” cholesterol (LDL) and total cholesterol.
- Limit alcohol. Visit the National Institute on Alcohol Abuse and Alcoholism for resources on support and treatment to stop drinking.
If your healthy lifestyle changes alone do not lower your cholesterol enough, you may also need to take medicines. There are several types of cholesterol-lowering drugs available, including statins. If you take medicines to lower your cholesterol, you still should continue with the lifestyle changes.
Some people with familial hypercholesterolemia (FH) may receive a treatment called lipoprotein apheresis. This treatment uses a filtering machine to remove LDL cholesterol from the blood. Then the machine returns the rest of the blood back to the person.
Eating a heart-healthy diet
From a dietary standpoint, the best way to lower your cholesterol is reduce your intake of saturated fat, trans fat and cholesterol. The American Heart Association recommends limiting saturated fat to less than 6% of daily calories and minimizing the amount of trans fat you eat.
Reducing these fats means limiting your intake of red meat and dairy products made with whole milk. Choose skim milk, low-fat or fat-free dairy products instead. It also means limiting fried food and cooking with healthy oils, such as vegetable oil.
A heart-healthy diet emphasizes fruits, vegetables, whole grains, poultry, fish, nuts and nontropical vegetable oils, while limiting red and processed meats, sodium and sugar-sweetened foods and beverages.
Many diets fit this general description. For example, the DASH (Dietary Approaches to Stop Hypertension) eating plan promoted by the National Heart, Lung, and Blood Institute as well as diets suggested by the U.S. Department of Agriculture and the American Heart Association are heart-healthy approaches. Such diets can be adapted based on your cultural and food preferences.
Becoming more physically active
A sedentary lifestyle lowers HDL cholesterol. Less HDL means there’s less good cholesterol to remove bad cholesterol from your arteries.
Physical activity is important. At least 150 minutes of moderate-intensity aerobic exercise a week is enough to lower both cholesterol and high blood pressure. And you have lots of options: brisk walking, swimming, bicycling or even yard work can fit the bill.
Quitting smoking
Smoking and vaping lowers HDL cholesterol.
Worse still, when a person with unhealthy cholesterol levels also smokes, risk of coronary heart disease increases more than it otherwise would. Smoking also compounds the risk from other risk factors for heart disease, such as high blood pressure and diabetes.
By quitting, smokers can lower their LDL cholesterol and increase their HDL cholesterol levels. It can also help protect their arteries. Nonsmokers should avoid exposure to secondhand smoke.
Losing weight
Being overweight or obese tends to raise bad cholesterol and lower good cholesterol. But a weight loss of as little as 5% to 10% can help improve cholesterol numbers. Losing even 5 to 10 pounds can help lower cholesterol levels.
Manage stress
Research has shown that chronic stress can sometimes raise your LDL cholesterol and lower your HDL cholesterol. Try to reduce your stress. You can do that by deep breathing and relaxation techniques. Examples include meditation and gentle exercise (such as walking or yoga). Also talking with a friend, family member, or health care professional may be helpful.
Medications for high cholesterol
Your doctor might suggest medication to help keep your cholesterol in the healthy range. The choice of medication or combination of medications depends on various factors, including your personal risk factors, your age, your health and possible drug side effects. Common choices include:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. Statins can also help your body reabsorb cholesterol from built-up deposits on your artery walls, potentially reversing coronary artery disease. Choices include atorvastatin (Lipitor), fluvastatin (Lescol XL), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor). The common side effects of statins are muscle pains and muscle damage, reversible memory loss and confusion, and elevated blood sugar.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can be used with a statin drug.
- Bempedoic acid. This newer drug works in much the same way as statins but is less likely to cause muscle pain. Adding bempedoic acid (Nexletol) to a maximum statin dosage can help lower LDL significantly. A combination pill containing both bempedoic acid and ezetimibe (Nexlizet) also is available.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- Injectable medications. A newer class of drugs, known as PCSK9 inhibitors, can help the liver absorb more LDL cholesterol — which lowers the amount of cholesterol circulating in your blood. Alirocumab (Praluent) and evolocumab (Repatha) might be used for people who have a genetic condition that causes very high levels of LDL or in people with a history of coronary disease who have intolerance to statins or other cholesterol medications. PCSK9 inhibitors are injected under the skin every few weeks and are expensive.
If you also have high triglycerides, your doctor might prescribe:
- Fibrates. Fibrates mostly lower triglycerides and, to a lesser degree, raise HDL levels. Fibrates are less effective in lowering LDL levels. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Using fibrates with a statin can increase the risk of statin side effects.
- Nicotinic acid also called niacin or vitamin B3. Niacin is the generic name for nicotinic acid (pyridine-3-carboxylic acid), nicotinamide (niacinamide or pyridine-3-carboxamide), and related derivatives, such as nicotinamide riboside 31. Niacin is a water-soluble B3 vitamin that should be taken only under physician supervision. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. It improves all lipoproteins—total cholesterol, LDL, triglycerides, and HDL—when taken in doses well abovethe vitamin requirement. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins.
- Omega-3 fatty acid supplements. Omega-3 fatty acid supplements can help lower your triglycerides. They are available by prescription or over-the-counter. If you choose to take over-the-counter supplements, get your doctor’s OK. Omega-3 fatty acid supplements could affect other medications you’re taking.
If you are on such medication, you might need regular cholesterol tests to check that they are working well and that you are taking the right dose. If you decide to take cholesterol medication, your doctor might recommend liver function tests to monitor the medication’s effect on your liver.
Experts from the National Cholesterol Education Program (NCEP) say that more aggressive cholesterol treatment is needed for people at high risk of dying from a heart attack or cardiovascular disease. The basic message of the group’s recommendations is the lower the better when it comes to levels of low-density lipoprotein (LDL) or “bad cholesterol”. The updated recommendations say that almost all high-risk patients with LDL cholesterol levels of 100 mg/dL or higher should begin taking cholesterol-lowering medicine.
Lipoprotein apheresis
Some people with familial hypercholesterolemia may benefit from lipoprotein apheresis to lower their blood cholesterol levels. Lipoprotein apheresis uses a filtering machine to remove unwanted substances from the body. The machine removes “bad” LDL cholesterol from the blood, then returns the remainder of the blood to your body.
Alternative medicine
Few natural products have been proved to reduce cholesterol, but some might be helpful. With your doctor’s OK, consider these cholesterol-lowering supplements and products:
- Barley
- Plant sterols and stanols, found in oral supplements, some fortified orange juices and some margarines, such as Promise Activ
- Blond psyllium, found in seed husk and products such as Metamucil
- Oat bran, found in oatmeal and whole oats
Another popular cholesterol-lowering supplement is red yeast rice. There is evidence that red yeast rice can help lower your LDL cholesterol. Some red yeast rice products contain substances called monacolins, which are produced by the yeast. However, the U.S. Food and Drug Administration (FDA) has said that red yeast rice products that contain monacolin K, a naturally occurring form of the prescription cholesterol-lowering drug lovastatin and can cause the same types of side effects and drug interactions as lovastatin, cannot be sold legally as dietary supplements in the United States. Other red yeast rice products contain little or no monacolin K, and it is not known whether these products have any effect on cholesterol levels. Unfortunately, there is no way to know how much monacolin K is present in most red yeast rice products.
If you buy red yeast rice supplements in the United States, there’s no way to know whether you’re getting enough monacolin K to lower your LDL cholesterol. In other countries, lovastatin in red yeast rice products is potentially dangerous because there’s no way to know how much might be in a particular product or what the quality of the lovastatin is.
- Flaxseed. Studies of flaxseed preparations to lower cholesterol levels report mixed results. A 2009 review of the scientific research of flaxseed for lowering cholesterol found modest improvements in cholesterol, seen more often in postmenopausal women and in people with high initial cholesterol concentrations.
- Garlic. Some evidence indicates that taking garlic supplements can slightly lower blood cholesterol levels. A recent review of the research on garlic supplements concluded that they can lower cholesterol if taken for more than 2 months, but their effect is modest in comparison with the effects of cholesterol-lowering drugs. However, a National Center for Complementary and Integrative Health-funded study on the safety and effectiveness of three garlic preparations (fresh garlic, dried powdered garlic tablets, and aged garlic extract tablets) for lowering blood cholesterol levels found no effect. Although garlic supplements appear to be safe for most adults, they can thin the blood in a manner similar to aspirin, so use caution if you are planning to have surgery or dental work. Garlic supplements have also been found to interfere with the effectiveness of saquinavir, a drug used to treat HIV infection.
- Some soy products can have a small cholesterol-lowering effect. An analysis of data from 35 studies indicated that soy foods were more effective in lowering cholesterol than soy protein supplements and that isoflavones (substances in soy that have a weak estrogenic effect) did not lower cholesterol. The effect of soy is much smaller than that of cholesterol-lowering drugs.
- Limited evidence indicates that green tea may have a cholesterol-lowering effect. The evidence on black tea is less consistent.
- Chromium, vitamin C, artichoke extract, the herb Hibiscus sabdariffa, coenzyme Q10, and selenium have been studied for cholesterol but have not been found to be effective. Research findings don’t show clear evidence regarding the cholesterol-lowering effects of policosanol (derived from sugar cane) and guggulipid (from the mukul mirth tree in western India).
Even if you take cholesterol-lowering supplements, remember the importance of a healthy lifestyle, and take medication to reduce your cholesterol as directed. Tell your doctor which supplements you take.
Foods to lower cholesterol
You can lower cholesterol over time by eating fewer of the foods that cause high cholesterol and more of the foods that lower cholesterol. The DASH eating plan is one example. DASH stands for Dietary Approaches to Stop Hypertension. DASH diet is an eating plan that is based on research studies sponsored by the National Heart, Lung, and Blood Institute. Clinical studies have shown that DASH diet lowers high blood pressure and improves levels of cholesterol. This reduces your risk of getting heart disease. Other lifestyle changes can help lower your blood pressure. They include staying at a healthy weight, exercising, and not smoking.
The DASH eating plan:
- Emphasizes vegetables, fruits, and whole-grains
- Includes fat-free or low-fat dairy products, fish, poultry, beans, nuts, and vegetable oils
- Limits foods that are high in saturated fat. These foods include fatty meats, full-fat dairy products, and tropical oils such as coconut, palm kernel, and palm oils.
- Limits sugar-sweetened beverages and sweets
Another example of a heart-healthy diet is the Mediterranean diet. The Mediterranean diet is similar to other heart-healthy diets. It promotes foods such as fish, fruits, vegetables, beans, and whole grains. It does not include many meats, dairy products, or sweets. In other ways, the Mediterranean diet is different. For example, it allows for more calories from fats, like olive oil. The Mediterranean diet also allows for moderate intake of wine.
Studies show that the Mediterranean diet has many health benefits. These are greater when combined with exercise. The Mediterranean diet can help you lose or maintain weight. It also helps to manage your blood pressure, blood sugar, and cholesterol levels. In older adults, it can improve your brain function. Following the Mediterranean diet may also protect against some chronic diseases, such as:
- heart disease
- cancer
- type 2 diabetes
- Alzheimer’s disease
- Parkinson’s disease
You can integrate the Mediterranean diet into your lifestyle.
Here are some foods to improve your cholesterol and protect your heart. Consider using a food diary to keep track of what you eat. It’s a handy way to evaluate the healthy, not-so-healthy and unhealthy foods you’re making a part of your everyday diet.
Oatmeal, oat bran and high-fiber foods
Oatmeal contains soluble fiber, which reduces your low-density lipoprotein (LDL) cholesterol, the “bad” cholesterol. Soluble fiber is also found in such foods as kidney beans, Brussels sprouts, apples and pears.
Soluble fiber can reduce the absorption of cholesterol into your bloodstream. Five to 10 grams or more of soluble fiber a day decreases your LDL cholesterol. One serving of a breakfast cereal with oatmeal or oat bran provides 3 to 4 grams of fiber. If you add fruit, such as a banana or berries, you’ll get even more fiber.
Vegetables
A growing body of scientific evidence indicates that wholesome vegetarian diets offer distinct advantages compared to diets containing meat and other foods of animal origin. The benefits arise from lower intakes of saturated fat, cholesterol and animal protein as well as higher intakes of complex carbohydrates, dietary fiber, magnesium, folic acid, vitamin C and E, carotenoids and other phytochemicals.
Try cooking vegetables in a tiny bit of vegetable oil and add a little water during cooking, if needed. Or use a vegetable oil spray. Just one or two teaspoons of oil is enough for a package of plain frozen vegetables that serves four. Place the vegetables in a skillet with a tight cover and cook them over very low heat until done.
Add herbs and spices to make vegetables even tastier. It’s a healthier choice than opting for pre-packaged vegetables with heavy sauce or seasonings. For example, these combinations add subtle and surprising flavors:
- Rosemary with peas, cauliflower and squash
- Oregano with zucchini
- Dill with green beans
- Marjoram with Brussels sprouts, carrots and spinach
- Basil with tomatoes
Start with a small quantity of herbs and spices (1/8 to 1/2 teaspoon for a package of frozen vegetables), then let your family’s feedback be your guide. Chopped parsley and chives, sprinkled on just before serving, can also enhance the flavor of many vegetables.
Fish and omega-3 fatty acids
Fatty fish has high levels of omega-3 fatty acids, which can reduce your triglycerides — a type of fat found in blood — as well as reduce your blood pressure and risk of developing blood clots. In people who have already had heart attacks, omega-3 fatty acids may reduce the risk of sudden death. Research has shown the health benefits of eating seafood rich in omega-3 fatty acids, especially when it replaces less healthy proteins that are high in saturated fat and low in unsaturated fat. Including seafood high in omega-3 fatty acids as part of a heart-healthy diet can help reduce the risk of heart failure, coronary heart disease, cardiac arrest and the most common type of stroke (ischemic stroke).
Omega-3 fatty acids don’t affect LDL cholesterol levels. But because of omega-3 fatty acids’ other heart benefits, the American Heart Association recommends eating at least two servings of fish a week or at least 8 ounces of non-fried fish each week. Baking or grilling the fish avoids adding unhealthy fats. Prepare fish baked, broiled, grilled or boiled rather than breaded and fried, and without added salt, saturated fat or trans fat. Non-fried fish and shellfish, such as shrimp, crab and lobster, are low in saturated fat and are a healthy alternative to many cuts of meat and poultry.
The highest levels of omega-3 fatty acids are in:
- Mackerel
- Herring
- Tuna
- Salmon
- Trout
Foods such as walnuts, flaxseed and canola oil also have small amounts of omega-3 fatty acids.
Omega-3 and fish oil supplements are available. Talk to your doctor before taking any supplements.
Increase fiber and whole grains
Fiber is a substance found in plants. Dietary fiber, the kind you eat, is found in fruits, vegetables, and grains. Your body cannot digest fiber, so it passes through your intestines without being absorbed much.
Dietary fiber adds bulk to your diet. Because it makes you feel full faster and for longer, it can help you with weight loss efforts or to maintain a healthy weight.
High fiber diets can also help with constipation.
Slowly increase the amount of fiber in your diet. If you have bloating or gas, you have probably eaten too much and need to reduce the amount of fiber you eat for a few days. Drink plenty of fluids. When you increase fiber in your diet, you also need to get enough fluids. Not getting enough fluids may make constipation worse instead of better. Ask your health care provider or a dietitian how much fluid you should be getting each day.
The daily recommended intake (DRI) of fiber for adults 19 to 50 years old is 38 grams a day for men and 25 grams a day for women. To get more fiber into your diet, eat different types of foods, such as:
- Fruits
- Vegetables
- Whole grains
Vegetables, Legumes, and Nuts
Vegetables are a good source of fiber. Eat more:
- Lettuce, Swiss chard, raw carrots, and spinach
- Tender cooked vegetables, such as asparagus, beets, mushrooms, turnips, and pumpkin
- Baked potatoes and sweet potatoes with skin
- Broccoli, artichokes, squashes, and string beans
You can also get more fiber by eating:
- Legumes, such as lentils, black beans, split peas, kidney beans, lima beans, and chickpeas
- Nuts and seeds, such as sunflower seeds, almonds, pistachios, and pecans
Fruits
Fruits are another good source of fiber. Eat more:
- Apples and bananas
- Peaches and pears
- Tangerines, prunes, and berries
- Figs and other dried fruits
Grains
Grains are another important source of dietary fiber. Eat more:
- Hot cereals, such as oatmeal and farina
- Whole-grain breads
- Brown rice
- Popcorn
- High-fiber cereals, such as bran, shredded wheat, and puffed wheat
- Whole-wheat pastas
- Bran muffins
Consider these heart-smart choices:
- Toast and crush (or cube) fiber-rich whole-grain bread to make breadcrumbs, stuffing or croutons.
- Replace the breadcrumbs in your meatloaf with uncooked oatmeal.
- Serve whole fruit at breakfast in place of juice.
- Use brown rice instead of white rice and try whole grain pasta.
- Add lots of colorful veggies to your salad – carrots, broccoli and cauliflower are high in fiber and give your salad a delicious crunch.
Almonds and other nuts
Almonds, peanuts and other tree nuts can improve blood cholesterol. Walnuts are especially high in omega-3 fatty acids, the same heart-healthy fat found in oily fish, but are a lot easier to stash in your pocket or purse. A recent study concluded that a diet supplemented with walnuts can lower the risk of heart complications in people with history of a heart attack. All nuts are high in calories, so a handful added to a salad or eaten as a snack will do.
All nuts will go bad (rancid) in time so keep them in the fridge. The same goes for nut oils and nut butters in jars after you’ve opened them. Rancid nuts have an unpleasant smell and bitter taste.
Avocados
Avocados are a potent source of nutrients as well as monounsaturated fatty acids (MUFAs). Research suggests that adding an avocado a day to a heart-healthy diet can help improve LDL cholesterol levels in people who are overweight or obese.
People tend to be most familiar with avocados in guacamole, which usually is eaten with high-fat corn chips. Try adding avocado slices to salads and sandwiches or eating them as a side dish. Also try guacamole with raw cut vegetables, such as cucumber slices.
Replacing saturated fats, such as those found in meats, with MUFAs are part of what makes the Mediterranean diet heart healthy.
Olive oil
Try using olive oil in place of other fats in your diet. You can saute vegetables in olive oil, add it to a marinade or mix it with vinegar as a salad dressing. You can also use olive oil as a substitute for butter when basting meat or as a dip for bread.
Foods with added plant sterols or stanols
There is evidence that foods that contain certain added ingredients, such as plant sterols and stanols, can reduce levels of cholesterol in the blood. Sterols and stanols are substances found in plants that help block the absorption of cholesterol. Plant sterols and stanols are found in nuts, seeds and legumes, vegetable oils, breads and cereals, and fruits and vegetables. You need to eat 2 to 3 grams a day of plant sterols and stanols to assist in reducing high cholesterol. Eating more is not harmful, but you won’t get any additional benefits.
Foods that have been fortified with sterols or stanols are available.
Margarines, low-fat milks, low-fat yogurts and breakfast cereals, lower fat cheese, processed cheese and orange juice with added plant sterols can help reduce LDL cholesterol. Adding 2 grams of sterol to your diet every day can lower your LDL cholesterol by 5 to 15 percent. People who do not have high cholesterol should not eat these products regularly, particularly children and pregnant or breastfeeding women.
If you do eat foods that are designed to lower cholesterol, read the label carefully to avoid eating too much.
You should not eat foods fortified with plant sterols as a substitute for medication. You can use plant sterol-enriched foods while taking cholesterol medication, but check with your doctor first.
However, it’s not clear whether food with plant sterols or stanols reduces your risk of heart attack or stroke — although experts assume that foods that reduce cholesterol do reduce the risk. Plant sterols or stanols don’t appear to affect levels of triglycerides or of high-density lipoprotein (HDL) cholesterol, the “good” cholesterol.
Whey protein
Whey protein, which is found in dairy products, may account for many of the health benefits attributed to dairy. Studies have shown that whey protein given as a supplement lowers both LDL and total cholesterol as well as blood pressure. You can find whey protein powders in health food stores and some grocery stores.
Use liquid vegetable oils in place of solid fats
Liquid vegetable oils such as canola, safflower, sunflower, soybean and olive oil can often be used instead of solid fats, such as butter, lard or shortening. If you must use margarine, try the soft or liquid kind.
Use a little liquid oil to:
- Pan-fry fish and poultry.
- Sauté vegetables.
- Make cream sauces and soups using low-fat or fat-free milk.
- Add to whipped or scalloped potatoes using low-fat or fat-free milk.
- Brown rice for Spanish, curried or stir-fried rice.
- Cook dehydrated potatoes and other prepared foods that call for fat to be added.
- Make pancakes or waffles.
Unsaturated fat
The two kinds of unsaturated fats are: monounsaturated and polyunsaturated. Monounsaturated fats have one (“mono”) unsaturated carbon bond in the molecule. Polyunsaturated fats have more than one (“poly,” for many) unsaturated carbon bonds. Both of these unsaturated fats are typically liquid at room temperature.
Eaten in moderation, both kinds of unsaturated fats may help improve your blood cholesterol when used in place of saturated and trans fats.
Unsaturated fats are in fish, such as salmon, trout and herring, and plant-based foods such as avocados, olives and walnuts. Liquid vegetable oils, such as soybean, corn, safflower, canola, olive and sunflower, also contain unsaturated fats.
Puree fruits and veggies for baking
Pureed fruits or vegetables can be used in place of oil in muffin, cookie, cake and snack bar recipes to give your treats an extra healthy boost. For many recipes, use the specified amount of puree instead of oil. Check the mix’s package or your cookbook’s substitutions page for other conversions. You can:
- Use applesauce in spice muffins or oatmeal cookies.
- Include bananas in breads and muffins.
- Try zucchini in brownies.
Lower dairy fats
Low-fat (1%) or fat-free (skim) milk can be used in many recipes in place of whole milk or half-and-half. (Some dishes, such as puddings, may result in a softer set.)
When it comes to cheeses used in recipes, you can substitute low-fat, low-sodium cottage cheese, part-skim milk mozzarella (or ricotta) cheese, and other low-fat, low-sodium cheeses with little or no change in consistency.
- Chávez-Sánchez, Luis & Chávez-Rueda, Karina & Legorreta, Victoria & Montoya-Díaz, Eduardo & Blanco-Favela, Francisco. (2012). The Innate Immune Response Mediated by TLRs in Atherosclerosis. https://www.researchgate.net/publication/221927810_The_Innate_Immune_Response_Mediated_by_TLRs_in_Atherosclerosis[↩][↩]
- Feingold KR. Introduction to Lipids and Lipoproteins. [Updated 2024 Jan 14]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK305896[↩]
- Berneis KK, Krauss RM. Metabolic origins and clinical significance of LDL heterogeneity. J Lipid Res. 2002 Sep;43(9):1363-79. doi: 10.1194/jlr.r200004-jlr200[↩]
- Warden BA, Fazio S, Shapiro MD. Familial Hypercholesterolemia: Genes and Beyond. [Updated 2024 Sep 23]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK343488[↩]
- Familial hypercholesterolemia. https://medlineplus.gov/ency/article/000392.htm[↩]
- Familial hypercholesterolemia. https://medlineplus.gov/genetics/condition/familial-hypercholesterolemia[↩]
- Vaezi Z, Amini A. Familial Hypercholesterolemia. [Updated 2022 Sep 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556009[↩]
- Blood Cholesterol Diagnosis. https://www.nhlbi.nih.gov/health/blood-cholesterol/diagnosis[↩][↩]
- High cholesterol. https://www.mayoclinic.org/diseases-conditions/high-blood-cholesterol/diagnosis-treatment/drc-20350806[↩][↩][↩][↩]
- National Cholesterol Education Program. Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. https://www.nhlbi.nih.gov/files/docs/guidelines/atp3xsum.pdf[↩]
- Centers for Heart Disease and Stroke Prevention. State Heart Disease and Stroke Prevention Programs Address High Blood Cholesterol. https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_state_cholesterol.htm[↩]
- American Heart Association. Why Cholesterol Matters. http://heartinsight.heart.org/Summer-2017/Why-Cholesterol-Matters/[↩]
- Pasławska A, Tomasik PJ. Lipoprotein(a)—60 Years Later—What Do We Know? Cells. 2023; 12(20):2472. https://doi.org/10.3390/cells12202472[↩]
- Peripheral Vascular Disease; Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2022, 42, e48–e60.[↩]
- Paré, G.; Çaku, A.; McQueen, M.; Anand, S.S.; Enas, E.; Clarke, R.; Boffa, M.B.; Koschinsky, M.; Wang, X.; Yusuf, S.; et al. Lipoprotein(a) Levels and the Risk of Myocardial Infarction Among 7 Ethnic Groups. Circulation 2019, 139, 1472–1482.[↩]
- Langsted A, Kamstrup PR, Nordestgaard BG. High lipoprotein(a) and high risk of mortality. Eur Heart J. 2019 Sep 1;40(33):2760-2770. doi: 10.1093/eurheartj/ehy902[↩]
- Burgess S, Ference BA, Staley JR, et al. European Prospective Investigation Into Cancer and Nutrition–Cardiovascular Disease (EPIC-CVD) Consortium. Association of LPA Variants With Risk of Coronary Disease and the Implications for Lipoprotein(a)-Lowering Therapies: A Mendelian Randomization Analysis. JAMA Cardiol. 2018 Jul 1;3(7):619-627. doi: 10.1001/jamacardio.2018.1470[↩]
- Pavanello, C.; Pirazzi, C.; Bjorkman, K.; Sandstedt, J.; Tarlarini, C.; Mosca, L.; Romeo, S.; Calabresi, L.; Mancina, R.M. Individuals with familial hypercholesterolemia and cardiovascular events have higher circulating Lp(a) levels. J. Clin. Lipidol. 2019, 13, 778–787.[↩]
- Patel AP, Wang (汪敏先) M, Pirruccello JP, Ellinor PT, Ng K, Kathiresan S, Khera AV. Lp(a) (Lipoprotein[a]) Concentrations and Incident Atherosclerotic Cardiovascular Disease: New Insights From a Large National Biobank. Arterioscler Thromb Vasc Biol. 2021 Jan;41(1):465-474. doi: 10.1161/ATVBAHA.120.315291[↩]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188.[↩]
- Wilson, D.P.; Jacobson, T.A.; Jones, P.H.; Koschinsky, M.L.; McNeal, C.J.; Nordestgaard, B.G.; Orringer, C.E. Use of Lipoprotein(a) in clinical practice: A biomarker whose time has come. A scientific statement from the National Lipid Association. J. Clin. Lipidol. 2019, 13, 374–392.[↩]
- Stone NJ, Smith SC Jr, Orringer CE, Rigotti NA, Navar AM, Khan SS, Jones DW, Goldberg R, Mora S, Blaha M, Pencina MJ, Grundy SM. Managing Atherosclerotic Cardiovascular Risk in Young Adults: JACC State-of-the-Art Review. J Am Coll Cardiol. 2022 Mar 1;79(8):819-836. doi: 10.1016/j.jacc.2021.12.016[↩]
- Kronenberg F, Mora S, Stroes ESG, Ference BA, Arsenault BJ, Berglund L, Dweck MR, Koschinsky M, Lambert G, Mach F, McNeal CJ, Moriarty PM, Natarajan P, Nordestgaard BG, Parhofer KG, Virani SS, von Eckardstein A, Watts GF, Stock JK, Ray KK, Tokgözoğlu LS, Catapano AL. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022 Oct 14;43(39):3925-3946. doi: 10.1093/eurheartj/ehac361[↩]
- Verbeek, R.; Hoogevee, R.M.; Langste, A.; Stiekema, L.; Verweij, S.; Hoving, G.K.; Wareham, N.J.; Khav, K.; Boekholdt, S.M.; Nordestgaard, B.; et al. Cardiovascular disease risk associated with elevated lipoprotein(a) attenuates at low low-density lipoprotein cholesterol levels in a primary prevention setting. Eur. Heart J. 2018, 39, 2589–2596.[↩]
- Madsen CM, Kamstrup PR, Langsted A, Varbo A, Nordestgaard BG. Lipoprotein(a)-Lowering by 50 mg/dL (105 nmol/L) May Be Needed to Reduce Cardiovascular Disease 20% in Secondary Prevention: A Population-Based Study. Arterioscler Thromb Vasc Biol. 2020 Jan;40(1):255-266. doi: 10.1161/ATVBAHA.119.312951[↩]
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Chapman MJ, De Backer GG, Delgado V, Ference BA, Graham IM, Halliday A, Landmesser U, Mihaylova B, Pedersen TR, Riccardi G, Richter DJ, Sabatine MS, Taskinen MR, Tokgozoglu L, Wiklund O; ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020 Jan 1;41(1):111-188. doi: 10.1093/eurheartj/ehz455. Erratum in: Eur Heart J. 2020 Nov 21;41(44):4255. doi: 10.1093/eurheartj/ehz826[↩]
- Pearson GJ, Thanassoulis G, Anderson TJ, Barry AR, Couture P, Dayan N, Francis GA, Genest J, Grégoire J, Grover SA, Gupta M, Hegele RA, Lau D, Leiter LA, Leung AA, Lonn E, Mancini GBJ, Manjoo P, McPherson R, Ngui D, Piché ME, Poirier P, Sievenpiper J, Stone J, Ward R, Wray W. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Can J Cardiol. 2021 Aug;37(8):1129-1150. doi: 10.1016/j.cjca.2021.03.016[↩]
- Waldmann, E.; Parhofer, K.G. Apheresis for severe hypercholesterolaemia and elevated lipoprotein(a). Pathology 2019, 51, 227–232.[↩]
- Sachais, B.S.; Shaz, B.H. Apheresis to mitigate atherosclerotic vascular disease. Am. J. Hypertens. 2018, 31, 945–949.[↩]
- Pokrovsky, S.N.; Afanasieva, O.I.; Ezhov, M.V. Therapeutic apheresis for management of Lp(a) hyperlipoproteinemia. Curr. Atheroscler. Rep. 2020, 22, 68.[↩]
- Kirkland JB. Niacin. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease, 11th ed. Baltimore, MD: Williams & Wilkins; 2014:331-40.[↩]





{kind=link}