Contents
- Spontaneous pneumothorax
- How common is spontaneous pneumothorax?
- What is a small and large pneumothorax?
- How long does it take for a pneumothorax to heal?
- What is the recurrence rate of primary spontaneous pneumothorax?
- Is chest tube drainage superior to conservative strategy?
- Is chest tube drainage superior to needle aspiration?
- Is chest tube drainage superior to surgery?
- Is outpatient superior to inpatient management?
- Chest anatomy
- The Lungs
- Pneumothorax types
- Spontaneous pneumothorax causes
- Risk factors for a pneumothorax
- Spontaneous pneumothorax signs and symptoms
- Spontaneous pneumothorax complications
- Spontaneous pneumothorax diagnosis
- Spontaneous pneumothorax differential diagnosis
- Spontaneous pneumothorax treatment
- Spontaneous pneumothorax prognosis
Spontaneous pneumothorax
Spontaneous pneumothorax is the sudden onset of a collapsed lung with the presence of air or gas in the pleural cavity (the space between your lung and chest wall) without any apparent cause, such as a traumatic injury to the chest or a known lung disease 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18. This buildup of air puts pressure on your lung, so it cannot expand as much as it normally does when you take a breath. In most cases of spontaneous pneumothorax, a small area in the lung that is filled with air, called a bleb, ruptures, causing the air to leak into the space around the lung.
There are 2 types of spontaneous pneumothorax:
- Primary spontaneous pneumothorax. Primary spontaneous pneumothorax is the most common type of pneumothorax (make up about 40% of spontaneous pneumothoraces), has no known cause and develops in otherwise healthy people. Pneumothorax occurs at rest in more than 80% of cases and sports does not seem to be a triggering factor 19. Primary spontaneous pneumothorax is thought to be caused by a tiny tear of an outer part of the lung. This can happen if abnormal air pockets in your lung (blebs) break apart and release air. Primary spontaneous pneumothorax is more common in tall people and mainly affects healthy young adults without lung disease.
- Secondary spontaneous pneumothorax. Secondary spontaneous pneumothorax develops as a complication of existing lung disease, such as chronic obstructive pulmonary disease (COPD), pneumonia, tuberculosis, sarcoidosis or cystic fibrosis. The lung disease weakens the edge of the lung in some way, making the lung more likely to tear and cause air to escape.
In most cases of spontaneous pneumothorax, the cause is unknown. Tall and thin adolescent males are typically at greatest risk, but females can also have spontaneous pneumothorax. Other risk factors include connective tissue disorders, smoking, and activities such as scuba diving, high altitudes and flying.
The signs and symptoms of patients with pneumothorax varies depending on the types of pneumothorax and ranges from completely asymptomatic to life-threatening respiratory distress. A person with spontaneous pneumothorax most commonly complain of sharp, pleuritic chest pain on the same side of the body as the pneumothorax or acute shortness of breath (dyspnea) and increased work of breathing, especially in patients with secondary spontaneous pneumothorax. Fast heart rate (tachycardia) is one of the most common physical exam findings; however, in patients with smaller spontaneous pneumothorax (less than 15% of the hemithorax), the exam may be unremarkable. For patients with larger spontaneous pneumothorax (more than 15%), there may be reduced movement of the chest wall, decreased or absent breath sounds on the same side of the body as the pneumothorax, jugular venous distension, pulsus paradoxus (a condition where your blood pressure drops more than normal when you breathe in), hyperresonance on percussion, and decreased tactile fremitus. Development of a tension pneumothorax is a rare potential complication of spontaneous pneumothorax with the late, ominous findings of low level of oxygen in the blood (hypoxemia), low blood pressure (hypotension), and tracheal deviation.
Spontaneous pneumothorax can be either small or large. A small spontaneous pneumothorax may resolve without treatment, while larger pneumothorax may need surgical intervention.
The goal in treating a pneumothorax is to relieve the pressure on your lung, allowing it to re-expand. Depending on the cause of the pneumothorax, a second goal may be to prevent recurrences. The methods for achieving these goals depend on the severity of your lung collapse, the type of spontaneous pneumothorax you have (i.e., primary spontaneous pneumothorax or secondary spontaneous pneumothorax), size of the pneumothorax and sometimes on your overall health 4, 20, 21, 22, 23.
Treatment options for a pneumothorax may include observation, needle aspiration, chest tube insertion, nonsurgical repair or surgery 24. You may receive supplemental oxygen therapy to speed air reabsorption and lung expansion. Oxygen increases the rate of absorption of the gas from the pleural space up to four-fold compared to the absorption of 1% to 2% of the volume per day without oxygen 25, 26, 27, 28.
Figure 1. Collapsed lung and normal lung
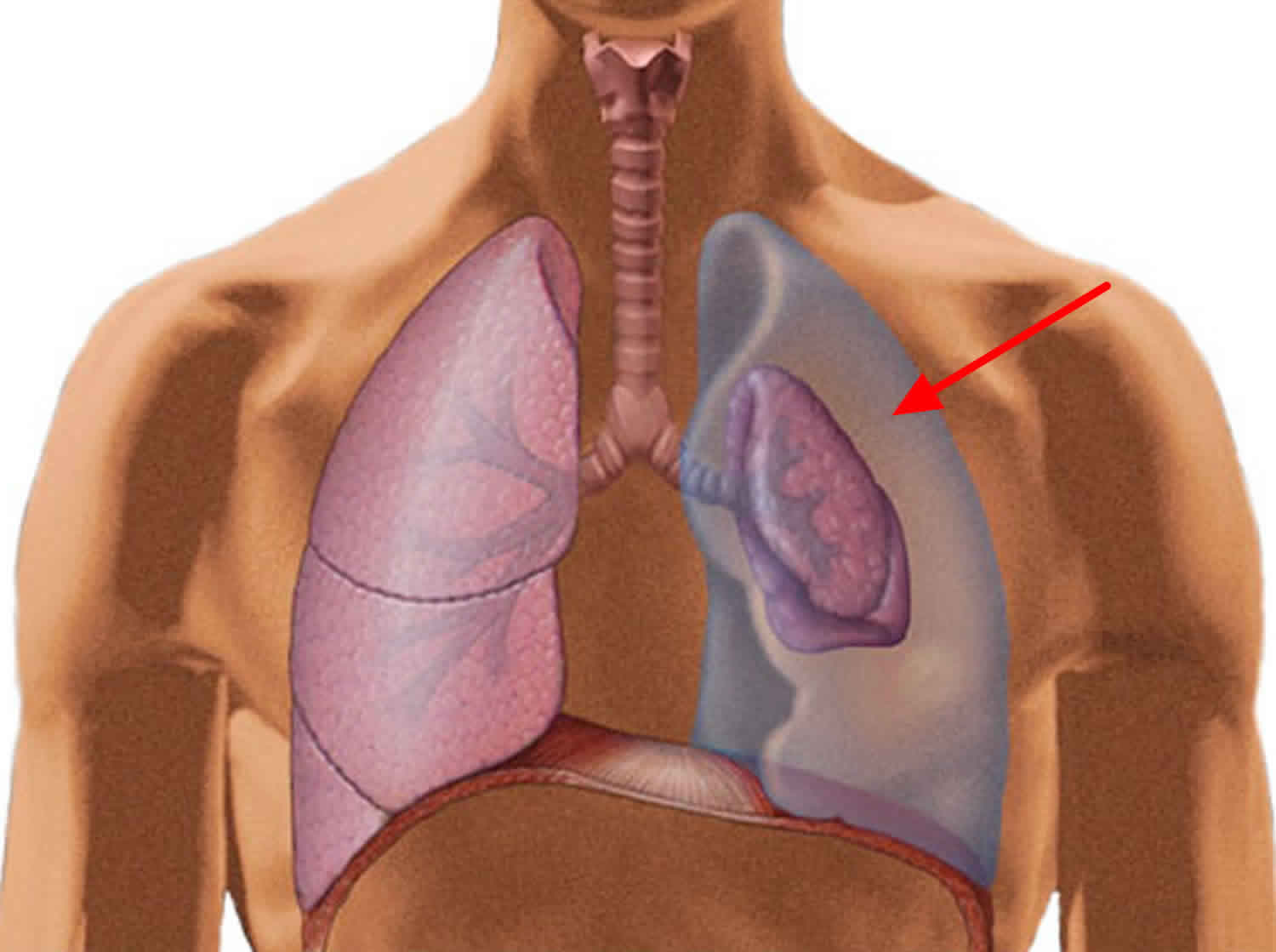
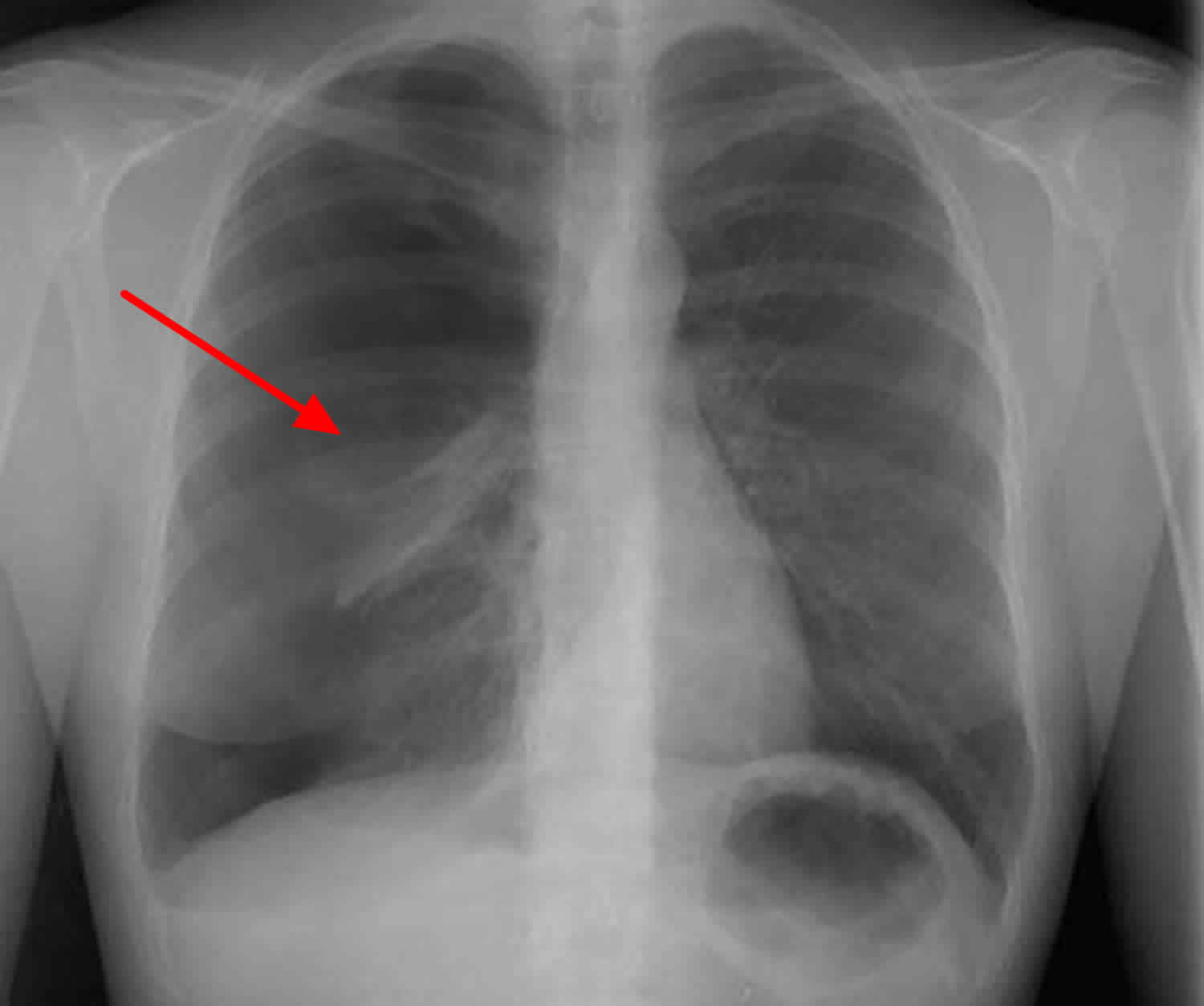
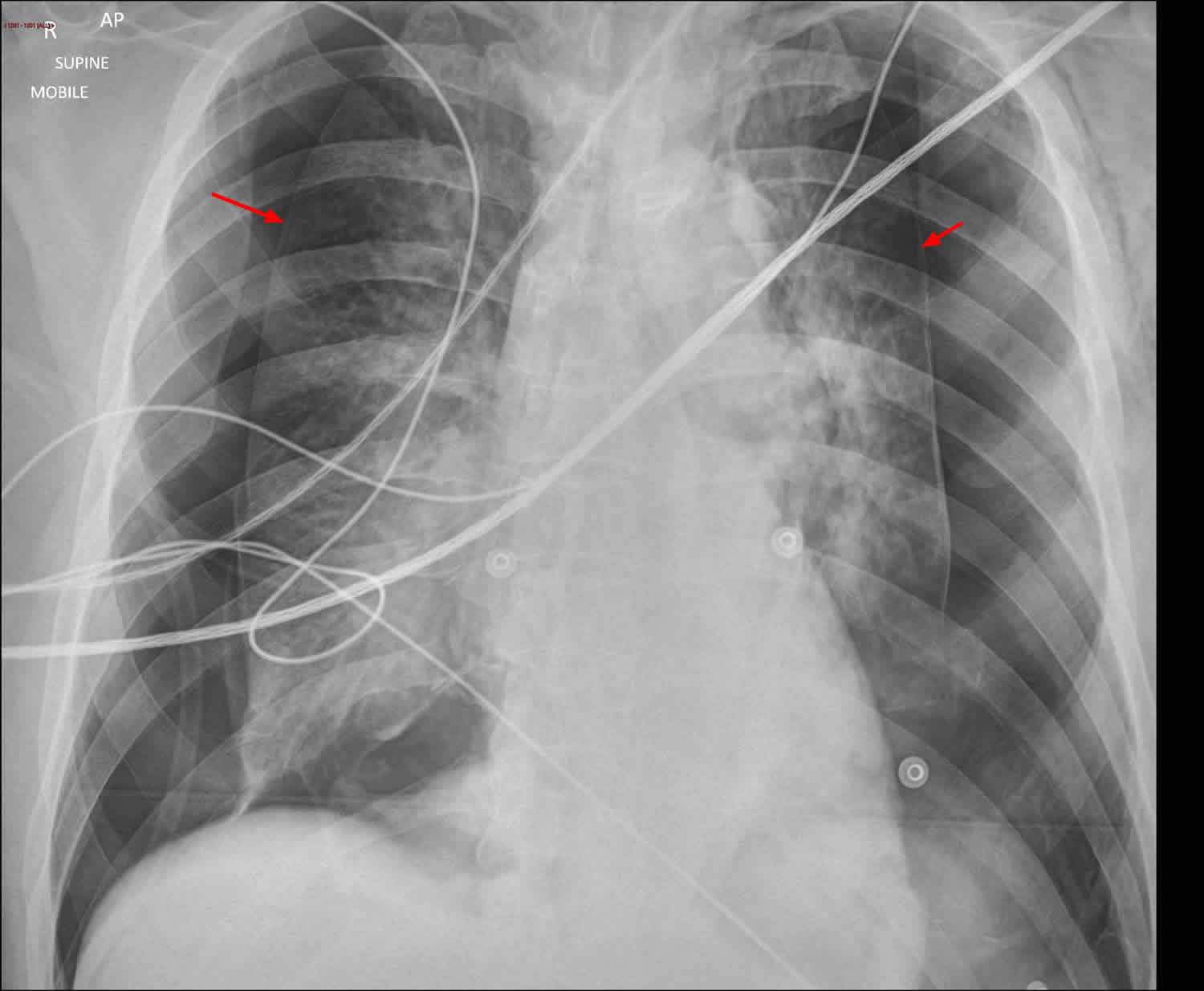
Figure 2. A large, right-sided pneumothorax has occurred from a rupture of a subpleural bleb (chest X-ray).
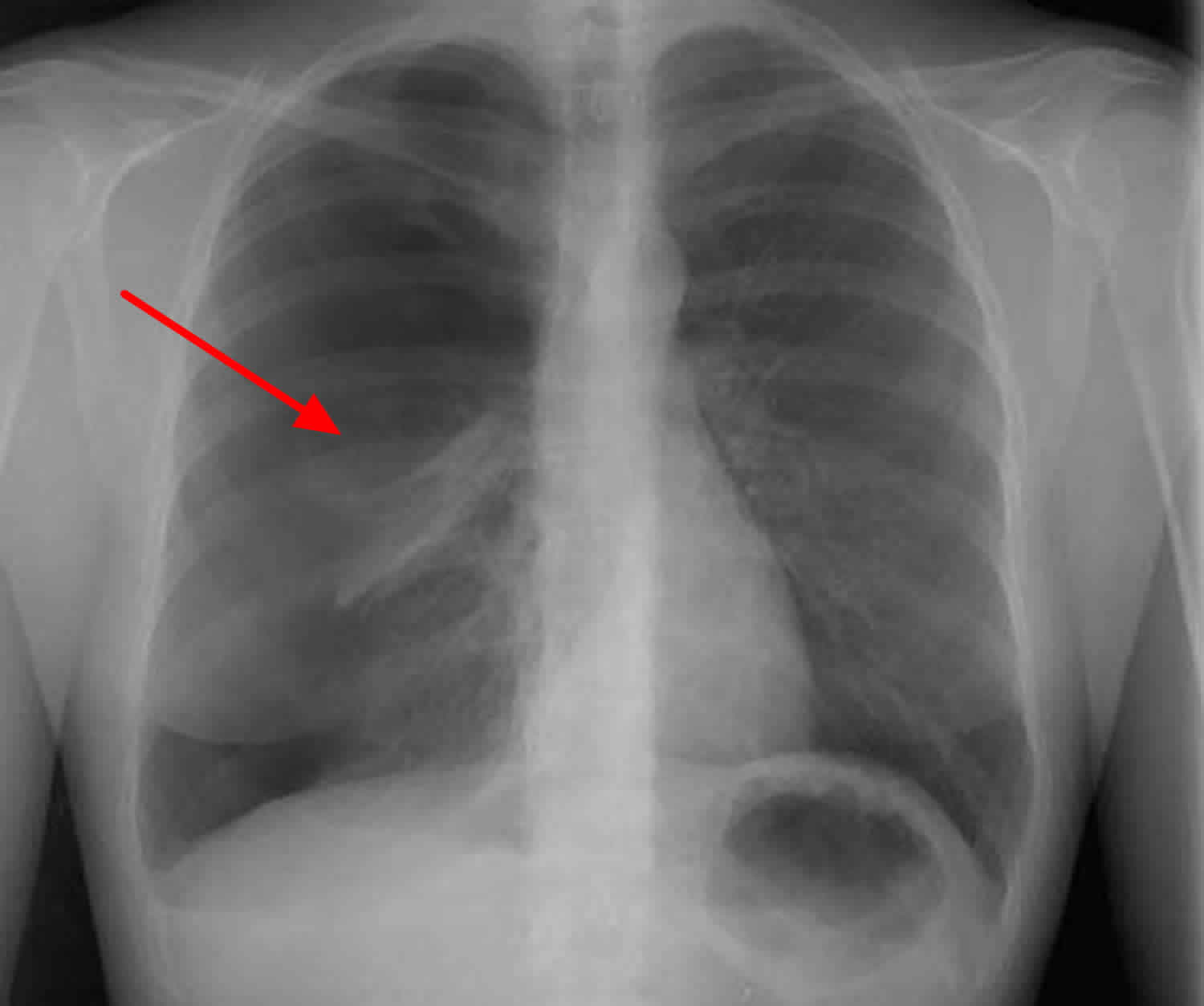
Figure 3. Large spontaneous pneumothorax
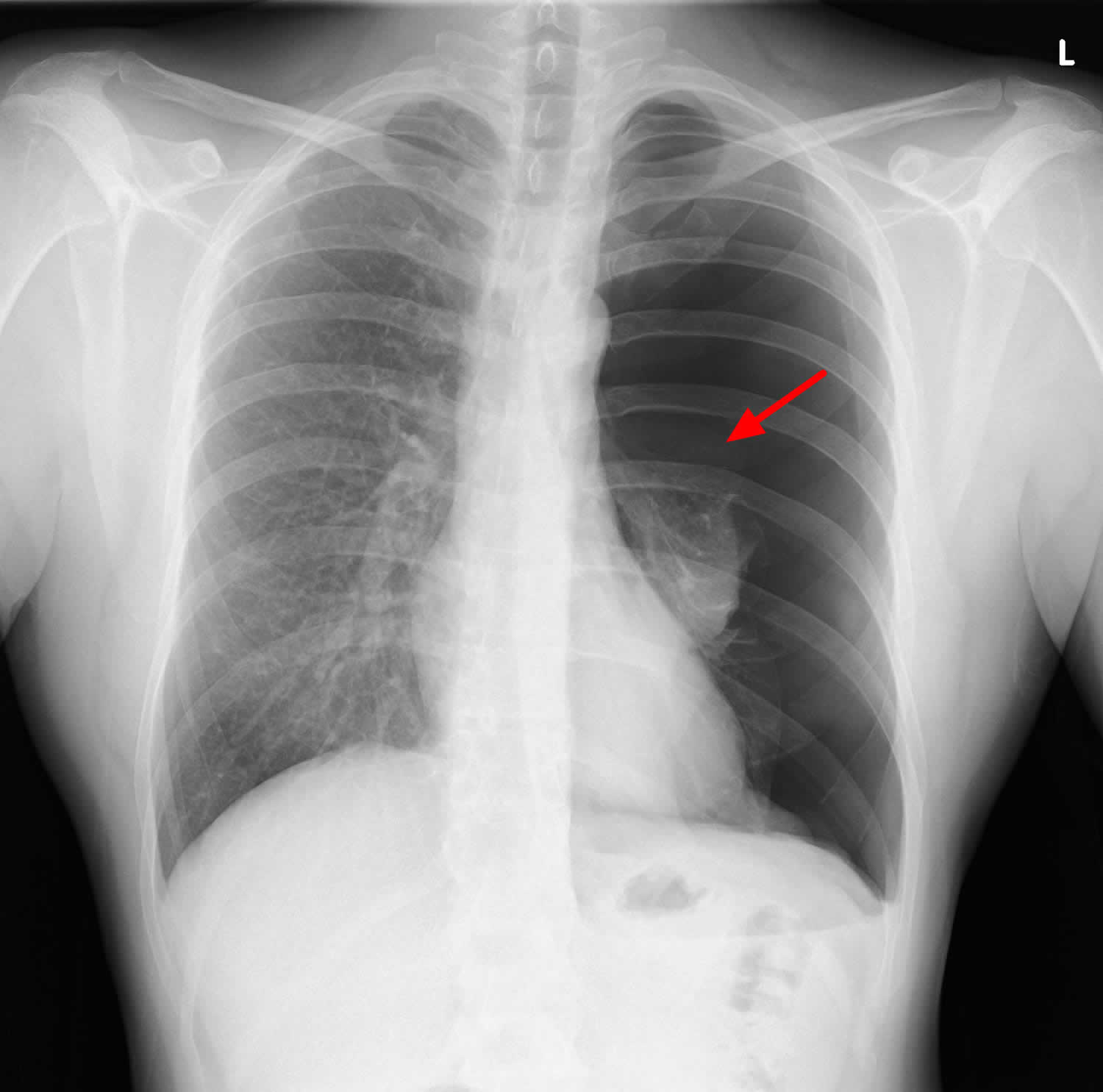
Footnotes: 35 year old male with symptoms of breathlessness on exertion and fatigue. On exam noted to have diminished air entry in the left lower lung base. Oxygen levels 97% at rest. Odd episodes of cough, lateral flow test negative. Chest X-ray showed large left sided pneumothorax with total collapse of the left lung. Minor mediastinal shift. Heart size normal. Right lung clear.
[Source 29 ]Figure 4. Bilateral pneumothoraces
Footnotes: 40 year old male with acute severe shortness of breath. No history of trauma. Chest X-ray large bilateral pneumothoraces. Although the costophrenic angles are excluded from the image, the deep sulcus sign is evident bilaterally.
[Source 30 ]Figure 5. Spontaneous pneumothorax due to ruptured apical bullae
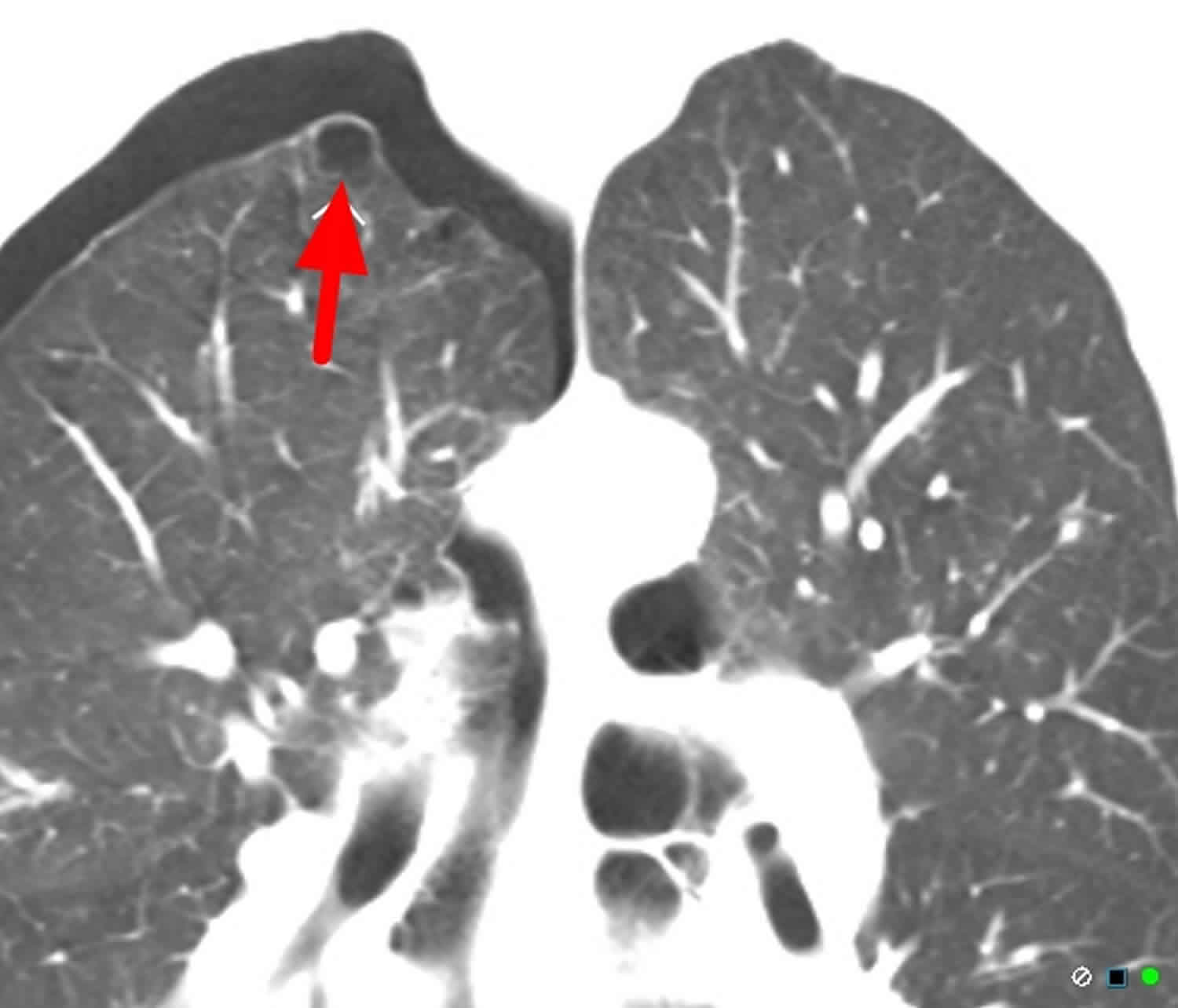
Footnotes: 55 year old male with sudden severe breathlessness and right-sided pleuritic chest pain. Chest CT showed loculated pneumothorax due to pleural adhesions. Apical lung bullae or blebs that predispose to spontaneous pneumothorax. These blebs are not on the background of bullous emphysema.
[Source 31 ]How common is spontaneous pneumothorax?
Spontaneous pneumothorax occurs more frequently in adults than children and more frequently in males than females 4. Spontaneous pneumothorax is a common clinical presentation, with 14.1 admissions per 100 000 people per year aged ≥15 years 32. In the United States, the adult incidence of primary spontaneous pneumothorax is estimated to be 7.4 per 100,000 to 18 per 100,000 people per year in males and 1.2 per 100,000 to 6.0 per 100,000 people per year in females, with similar rates of secondary spontaneous pneumothorax in males and females, 6.3 and 2.0 per 100,000 people per year, respectively 4. In children, the combined incidence of spontaneous pneumothorax is estimated to be 4.0 per 100,000 children per year in males and 1.1 per 100,000 children per year in females. Other risk factors include a history of smoking, and a tall, thin body habitus 10, 33.
What is a small and large pneumothorax?
Estimating the size of pneumothorax is somewhat controversial with no international consensus. Chest CT scan is considered more accurate than plain chest X-ray.
British Thoracic Society (BTS) guidelines (2010) measured from chest wall to lung edge at the level of the hilum 34:
- <2 cm: Small
- ≥2 cm: Large
American College of Chest Physicians guidelines (ACCP) measured from thoracic cupola to lung apex 35:
- <3 cm: Small
- ≥3 cm: Large
Expert group considers a pneumothorax as large when there is a visible rim along the entire axillary line, ≥ 2 cm between the lung margin and the chest wall at the hilum level 2.
Figure 6. Large pneumothorax size
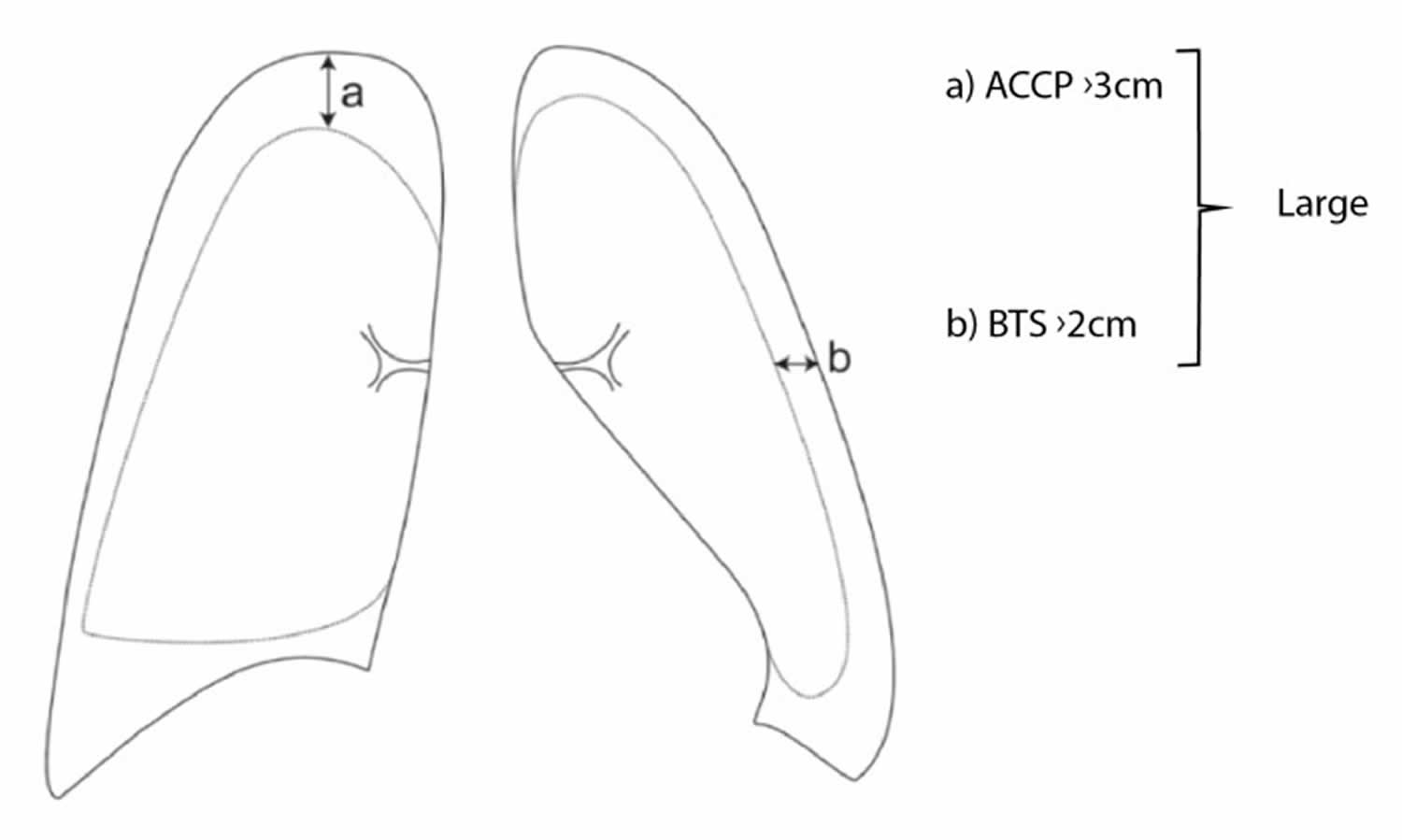
Footnotes: Estimation of size of a pneumothorax based on routine chest X-ray. (a) The American College of Chest Physicians (ACCP) generally use the intrapleural distance from the apex to the cupola of the lung, whereas the British Thoracic Society (BTS) uses the intrapleural distance at the hilum (b).
[Source 3 ]How long does it take for a pneumothorax to heal?
If the pneumothorax is small, the leak usually heals itself and the trapped air is gradually absorbed by your body. This normally takes 1 to 2 weeks. You can use over-the-counter painkillers to manage your pain and you might also be given oxygen.
What is the recurrence rate of primary spontaneous pneumothorax?
Primary spontaneous pneumothorax recurrence rates vary widely in the published literature, with limited data describing the factors that influence recurrence. This systematic review showed a 32% recurrence rate in primary spontaneous pneumothorax, with greatest risk in the first year 36. There are no established factors that predict pneumothorax recurrence and consequently no method for risk-stratifying patients. Female sex, low body weight (lower BMI), smoking and height in males have all been postulated as risk factors for higher risk of pneumothorax recurrence 37, 38, 39, 40. Certain radiographic features have also been suggested to confer additional risk, including bullae on computed tomography (CT) and pleural thickening on chest radiography 41, 42, 43. Importantly, there is no consensus on which treatment offers the greatest reduction in risk of pneumothorax recurrence 23, 44, 45, 46.
Is chest tube drainage superior to conservative strategy?
A single study has assessed the conservative strategy in patients with a first episode of a large unilateral primary spontaneous pneumothorax 47. This multicenter, open-label, randomized controlled trial included 316 patients aged 14 to 50 years: 154 in the chest tube drainage and hospitalization (“standard”) arm and 162 in the conservative strategy arm.
The conservative management was non-inferior to the “standard” management on the primary endpoint (eight weeks radiographic resolution) 47. The risk of ipsilateral recurrence at one year was lower in the conservative arm (8.8% vs 16.8%) 47, 23. However, these data should be considered with caution as 1-year recurrence rate was lower than usual in both arms, 29% in the meta-analysis by Walker et al 48. The conservative strategy allowed reducing the number of procedures (percutaneous pleural procedures, need for surgery, imaging), the hospital length of stay, the rate of adverse events and the number of days out of work 47. The failure rate of the conservative strategy (defined as the need for chest tube drainage) ranged between 15 and 21% 47, 49.
However, some biases limit its conclusions, rending questionable and hardly generalizable these results:
- In sensitivity analyzes, if all lost to follow-up patients are considered as “failures”, the difference in success at eight weeks exceeds the non-inferiority limit and the study is negative, with conservative management less effective than chest tube drainage;
- There might be an inclusion bias, as only 316 patients out of the 2637 screened were included;
- The type of included patients seems unusual: the duration of primary spontaneous pneumothorax evolution was about of 40 hours, the patients being barely asymptomatic (median dyspnea and pain visual analog scale scores respectively of 1 and 2 on 10-points scales).
Further studies are needed to assess the safety and better define the profile of patients who could benefit from a conservative strategy.
Is chest tube drainage superior to needle aspiration?
Needle aspiration requires a transient pleural approach, performed until bubbling stops 50, 51, until aspiration is no longer possible 52, 53, until a fixed volume is aspirated 54, 53, 55 or for a maximal time 50, 51, 52. If needle aspiration is not sufficient, studies suggest either switching to chest tube drainage 56, 51, 57, 58, 59 or to attempt a second (or a third) needle aspiration 50, 51, 52, 60, although not recommended 61, 62. Needle aspiration failure is defined as an attempted needle aspiration followed by a chest tube drainage 50, 57, 58, 59, 60.
Chest tube drainage shows a higher “immediate success” rate compared to needle aspiration 50, 63, 53, 64, 65. A later success rate (at day 7 or later), appears similar between chest tube drainage and needle aspiration 52, 66, 63, 55, 67. The overall immediate success rate is 51% for needle aspiration (after 1 − 3 procedures) and about 68% for chest tube drainage 50, 52, 54, 66, 55, 60, 68.
Needle aspiration reduces the hospital length of stay compared chest tube drainage (i.e. with hospitalization) 50, 52, 54, 66, 55, 60, 68, 69, 65.
Needle aspiration allowed decreasing drainage duration compared to chest tube drainage in an randomized controlled trial 55.
The risk of complications is rarely reported and lower during needle aspiration than chest tube drainage 52, 53, 67. One study found similar complication rates between needle aspiration and chest tube drainage 60.
Conflicting data exist in pain. Although some report less pain with needle aspiration 52, 67 and higher analgesic use in chest tube drainage 52, older studies did not report any difference between techniques 50, 60.
Treatment satisfaction did not differ between needle aspiration and chest tube drainage 60.
Surgery rate did not differ between needle aspiration and chest tube drainage 60, 55. A single old study, of low level of evidence, reported a more frequent need for pleurectomy in chest tube drainage as compared to needle aspiration 54.
Costs had not been analyzed in these studies. The 2017 Cochrane Database considered that no conclusion was possible 70. However, as needle aspiration reduces the hospital length of stay as compared to chest tube drainage, the cost of such management would be lower. Dedicated medico-economic studies are needed.
One-year (and sometimes 3 months) recurrence rates did not differ between needle aspiration and chest tube drainage 50, 52, 54, 66, 63, 64, 67, 68.
Based on these findings, needle aspiration might appear superior to chest tube drainage. Given the possibility of an outpatient management with a chest tube drainage, these two approaches were kept as first-line management of large primary spontaneous pneumothorax.
Is chest tube drainage superior to surgery?
Seventy percent of patients with a first primary spontaneous pneumothorax will never relapse. Therefore, performing surgery at first episode of primary spontaneous pneumothorax seems too invasive 48. However, several studies compared surgical treatment (pleurodesis and bleb removal) following chest tube drainage or needle aspiration to a conventional chest tube drainage strategy without surgery during a first episode of large primary spontaneous pneumothorax. These studies reported a reduced one-year risk of recurrence, a shorter length of stay, a lower cost and no difference in analgesic for surgically treated patients compared to conventional chest tube drainage 71, 72, 73, 74, 75, 76. These studies had several biases drawing the conclusion was not easy.
Is outpatient superior to inpatient management?
No high-quality study has directly compared the outpatient management with needle aspiration versus mini-chest tube drainage with one-way valve. At least one such study is ongoing (PNEUM-AMBU, NCT03691480) 77.
Exclusive outpatient management is feasible in 4 out of 5 patients treated with needle aspiration or chest tube drainage with a one-way valve 78, 79, 80.
Compared with inpatient care, outpatient management reduces the hospital length of stay, as reported in a study comparing a drainage system with an integrated one-way valve versus a standard management with needle aspiration in most cases (68% of patients in the control arm) 80. In most other publications, outpatient needle aspiration has been compared to drainage with hospital-based monitoring. Series reporting outpatient management have also suggested a reduced hospital length of stay but without control arm 81, 79, 78, 82.
Use of surgery was not assessed specifically in study reporting outpatient strategy.
Outpatient management could increase the complications rates as compared to inpatient management 80. However, the design of this prospective study explains most of the severe complications, as adverse events were defined as the need for hospitalization, which could only concern patients of the outpatient arm.
On the other hand, in observational studies, no serious adverse events were reported, but mainly bent or displaced catheters (ranging from 1.5% to 22.6%) 81, 79, 78, 82.
Outpatient management was associated with a similar 1-year recurrence rate as inpatient management, ranging from 12% to 33.1% 81, 79, 78, 82, 78.
Indirect evidence suggest a lower overall health care costs of outpatient management 81, 79.
Expert group recommends outpatient management in patients with large primary spontaneous pneumothorax without signs of immediate severity 2.
The expert group recommends an outpatient management based on needle aspiration or on mini-chest tube with one-way valve, if the following criteria are met 2:
- the patient is stable after intrapleural air removal,
- and a dedicated outpatient care system is previously organized
- and a consultation with chest ultrasound or chest X-ray is scheduled at 24−72 hour to assess the evolution.
The expert group proposes outpatient management of primary spontaneous pneumothorax only if all of the following conditions are met 2:
- A patient information leaflet providing guidance on the way to behave in case of problem and phone numbers available 24/7, is given to the patient before hospital discharge,
- Patient’s comprehension of discharge instructions has been checked
- The patient should not stay alone for the first 24 − 48 hour after being discharged home,
- The patient should be able to access a medical facility within 1 hour, regardless of the means of transportation, in the event of deterioration,
- The time of discharge does not matter if all of the above criteria are met (nighttime discharge is possible).
Chest anatomy
Your chest cavity also called the thoracic cavity is formed by the ribs, the muscles of the chest, the sternum (breastbone), and the thoracic portion of the vertebral column. Within your thoracic cavity are 3 smaller cavities: (a) 2 pleural cavities (fluid-filled spaces one around each lung), your left pleural cavity (holds your left lung) and your right pleural cavity (holds your right lung) and (b) a central portion of your thoracic cavity between your lungs called the mediastinum (media- = middle; -stinum = partition). The mediastinum is the central portion of your thoracic cavity between your lungs, extending from the base of your neck (from your first rib and sternum) to the diaphragm. The mediastinum contains your heart (pericardial cavity, peri- = around; -cardial = heart, a fluid-filled space that surrounds your heart), the major blood vessels connected to your heart and lungs, the trachea (windpipe) and bronchi, the esophagus (foodpipe), the thymus, and lymph nodes but not your lungs. Your right and left lungs are on either side of the mediastinum. The diaphragm is a dome-shaped muscle that separates the thoracic cavity from the abdominopelvic cavity.
Your mediastinum is divided into several parts, which researchers call compartments. The traditional or classical model divides your mediastinum into four parts:
- Superior mediastinum: The top part, located superior to (above) your heart.
- Anterior mediastinum: The part anterior to (in front of) your heart, between your heart and your sternum (breastbone).
- Middle mediastinum: The part that contains your heart.
- Posterior mediastinum: The part posterior to (behind) your heart.
A membrane is a thin, pliable tissue that covers, lines, partitions, or connects internal organs (viscera). One example is a slippery, double-layered membrane associated with body cavities that does not open directly to the exterior called a serous membrane. Serous membrane covers your internal organs (viscera) within the thoracic and abdominal cavities and also lines the walls of the thorax and abdomen. The parts of a serous membrane are (1) the parietal layer (outer layer), a thin epithelium that lines the walls of the cavities, and (2) the visceral layer (inner layer), a thin epithelium that covers and adheres to the viscera within the cavities. Between the two layers is a potential space that contains a small amount of lubricating fluid (serous fluid). The fluid allows the internal organs (viscera) to slide somewhat during movements, such as when the lungs inflate and deflate during breathing.
Within the right and left sides of your thoracic cavity (chest cavity), the compartments that contain your lungs, on either side of the mediastinum, are lined with a membrane called the parietal pleura (outer serous membrane) lining the inside of your rib cage (parietal pleura lines the chest wall) and covering the superior surface of the diaphragm. A similar membrane, called the visceral pleura (inner serous membrane), clings to the surface of your lungs forming the external surface of your lung. The visceral (inner) and parietal (outer) pleural membranes are separated only by a thin film of watery fluid called serous fluid, which is secreted by the parietal and visceral pleural membranes. Although no actual space normally exists between the parietal (outer) and visceral (inner) pleural membranes, the potential space between them is called the pleural cavity. The parietal pleura (outer membrane) and visceral pleura (inner membrane) slide with little friction across the cavity walls as your lungs move, expand and collapse during respiration.
Your heart, which is located in the broadest portion of the mediastinum, is surrounded by pericardial membranes called the pericardium. Your pericardium is a protective, fluid-filled sac that surrounds your heart and helps it function properly.
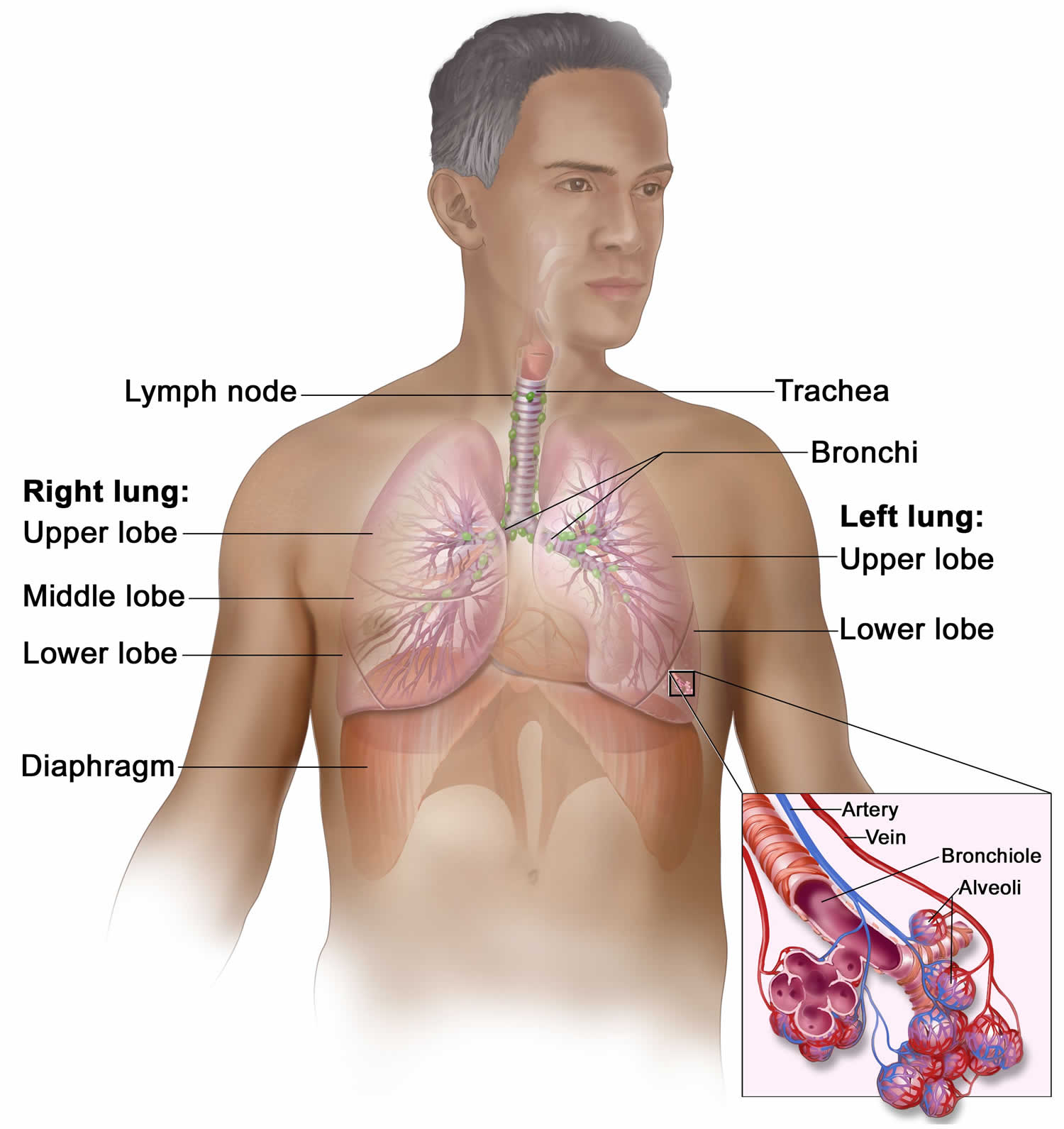
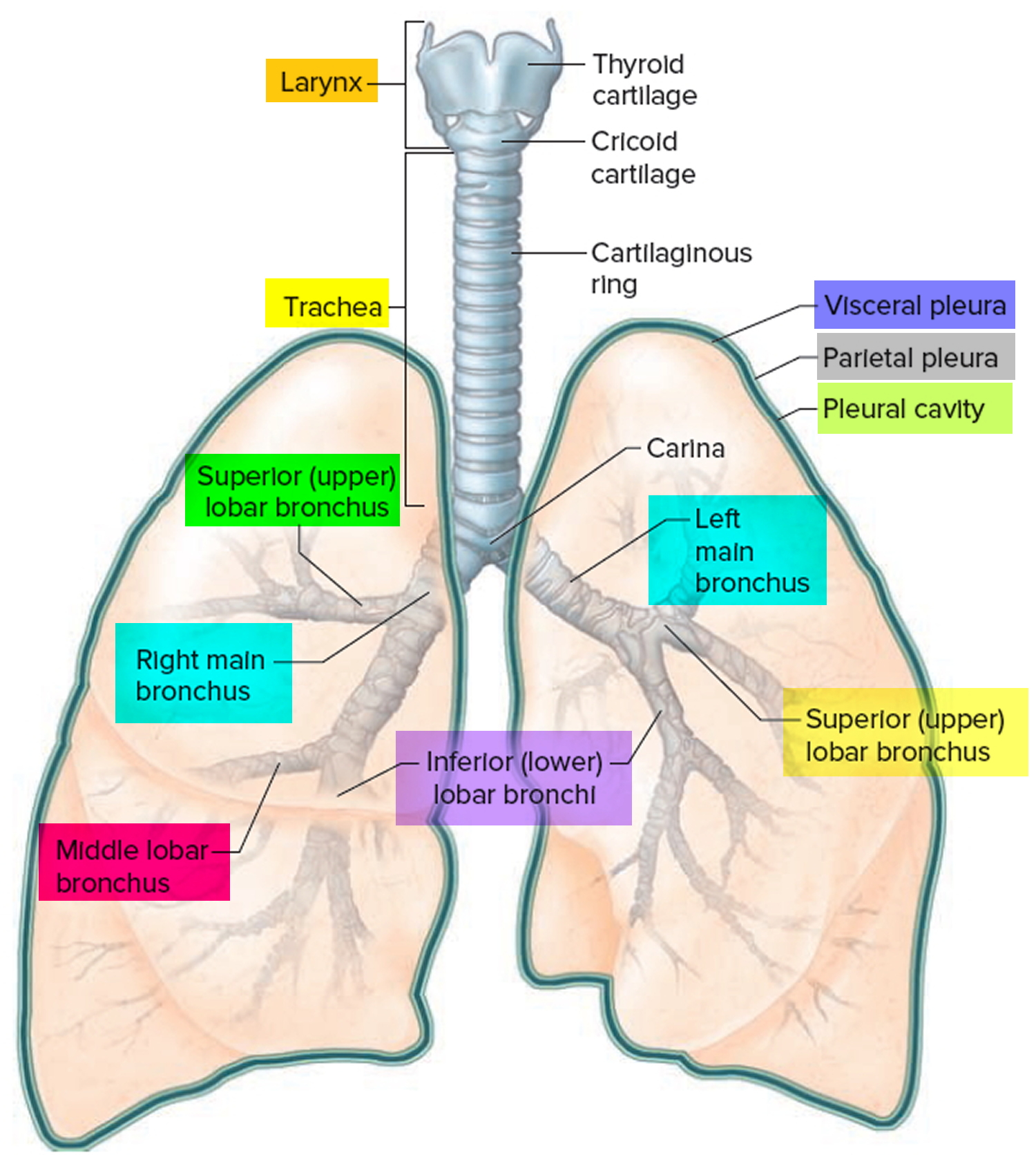
Your respiratory system includes the trachea, the right and left lungs and their lobes, and the bronchi. Oxygen (O2) is inhaled into your lungs and passes through the alveoli (the tiny air sacs at the end of the bronchioles) and into your bloodstream, where it travels to the tissues throughout the body.
Figure 7. Chest anatomy

Figure 8. Thoracic cavity
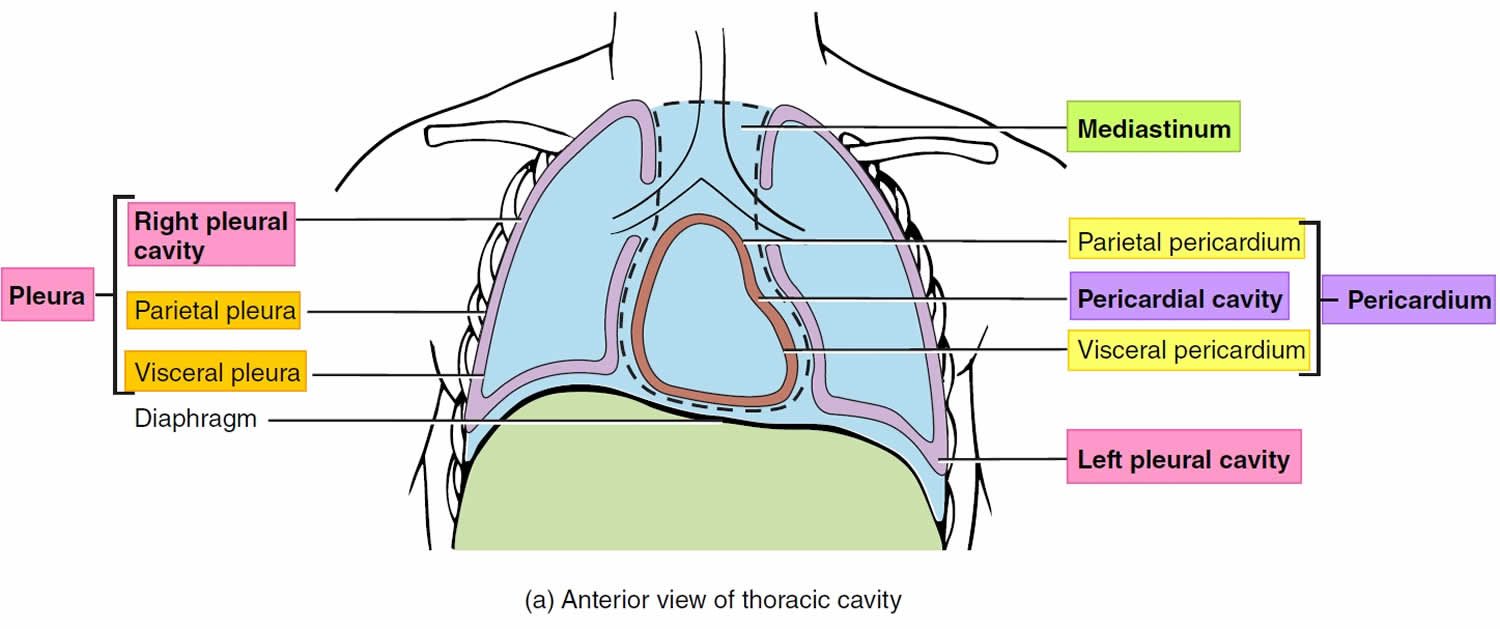
Footnote: The black dashed lines indicate the borders of the mediastinum.
Figure 9. Thoracic cavity transverse section
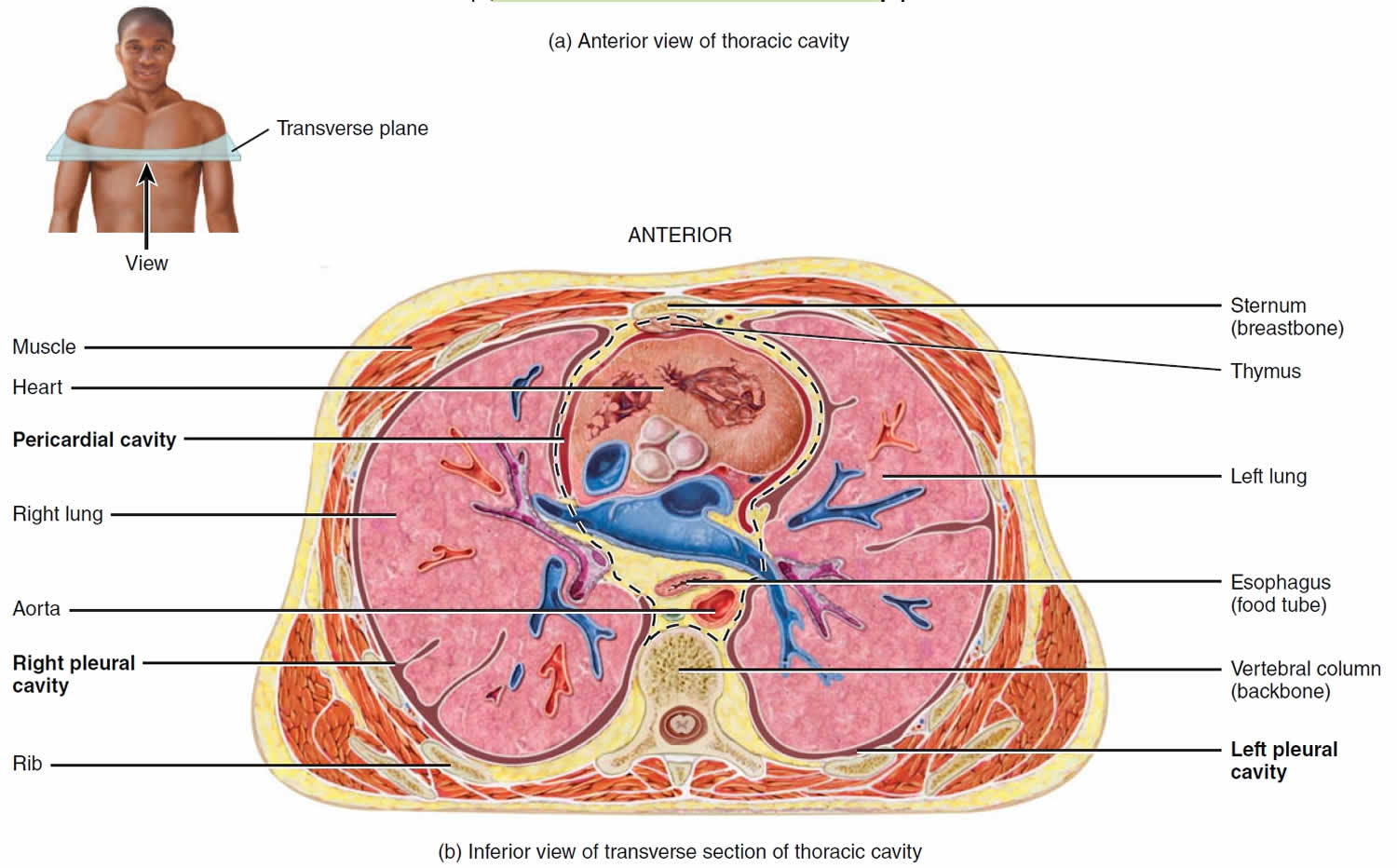
Figure 10. Mediastinum
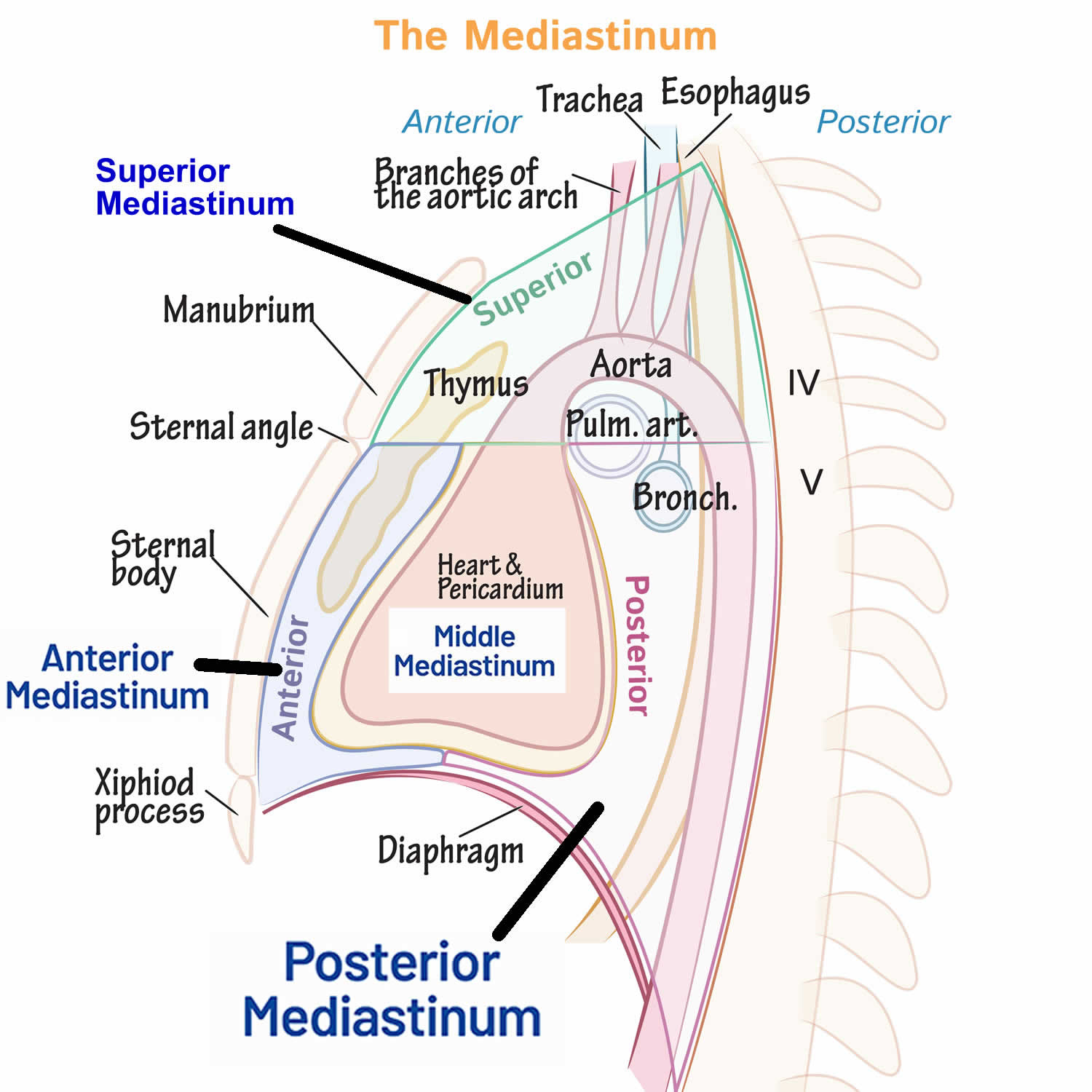
Figure 11. Respiratory system
The Lungs
The lungs (= lightweights, because they float) are paired cone-shaped, soft, spongy organs in the thoracic (chest) cavity (Figure 1). The lungs consist largely of air tubes and spaces. The balance of the lung tissue, its stroma, is a framework of connective tissue containing many elastic fibers. As a result, the lungs are light, soft, spongy, elastic organs that each weigh only about 0.6 kg (1.25 pounds). The elasticity of healthy lungs helps to reduce the effort of breathing. The lungs are separated from each other by the heart and other structures of the mediastinum, which divides the thoracic cavity into two anatomically distinct chambers. As a result, if trauma causes one lung to collapse, the other may remain expanded.
Each lung is enclosed and protected by a double-layered serous membrane called the pleural membrane or pleura. The superficial layer, called the parietal pleura, lines the wall of the thoracic cavity; the deep layer, the visceral pleura, covers the lungs themselves (Figures 2 and 3). Between the visceral and parietal pleurae is a small space, the pleural cavity, which contains a small amount of lubricating fluid secreted by the membranes. This pleural fluid reduces friction between the membranes, allowing them to slide easily over one another during breathing. Pleural fluid also causes the two membranes to adhere to one another just as a film of water causes two glass microscope slides to stick together, a phenomenon called surface tension. Separate pleural cavities surround the left and right lungs. The left and right lungs are situated in the left and right pleural cavities inside the thoracic cavity.
A lung will collapse if air enters the pleural cavity, a condition called pneumothorax. The air breaks the seal of pleural fluid that holds the lung to the thoracic wall, allowing the elastic lung to collapse like a deflating balloon.
Inflammation of the pleural membrane, called pleurisy or pleuritis, may in its early stages cause pain due to friction between the parietal and visceral layers of the pleura. If the inflammation persists, excess fluid accumulates in the pleural space, a condition known as pleural effusion.
Below the lungs, a thin, dome-shaped muscle called the diaphragm separates the chest from the abdomen. When you breathe, the diaphragm moves up and down, forcing air in and out of the lungs. The thoracic cage encloses the rest of the lungs.
Figure 12. Lung anatomy
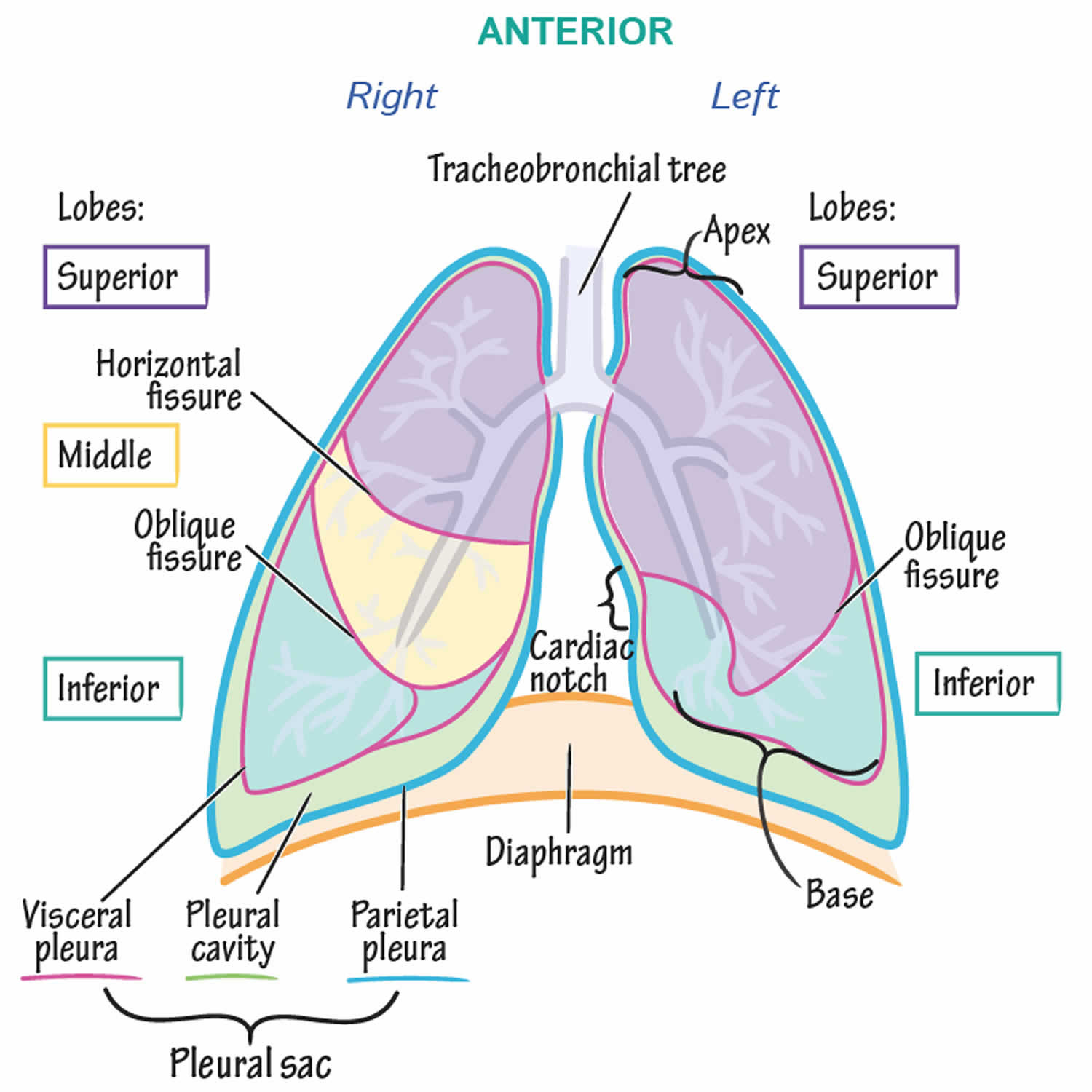
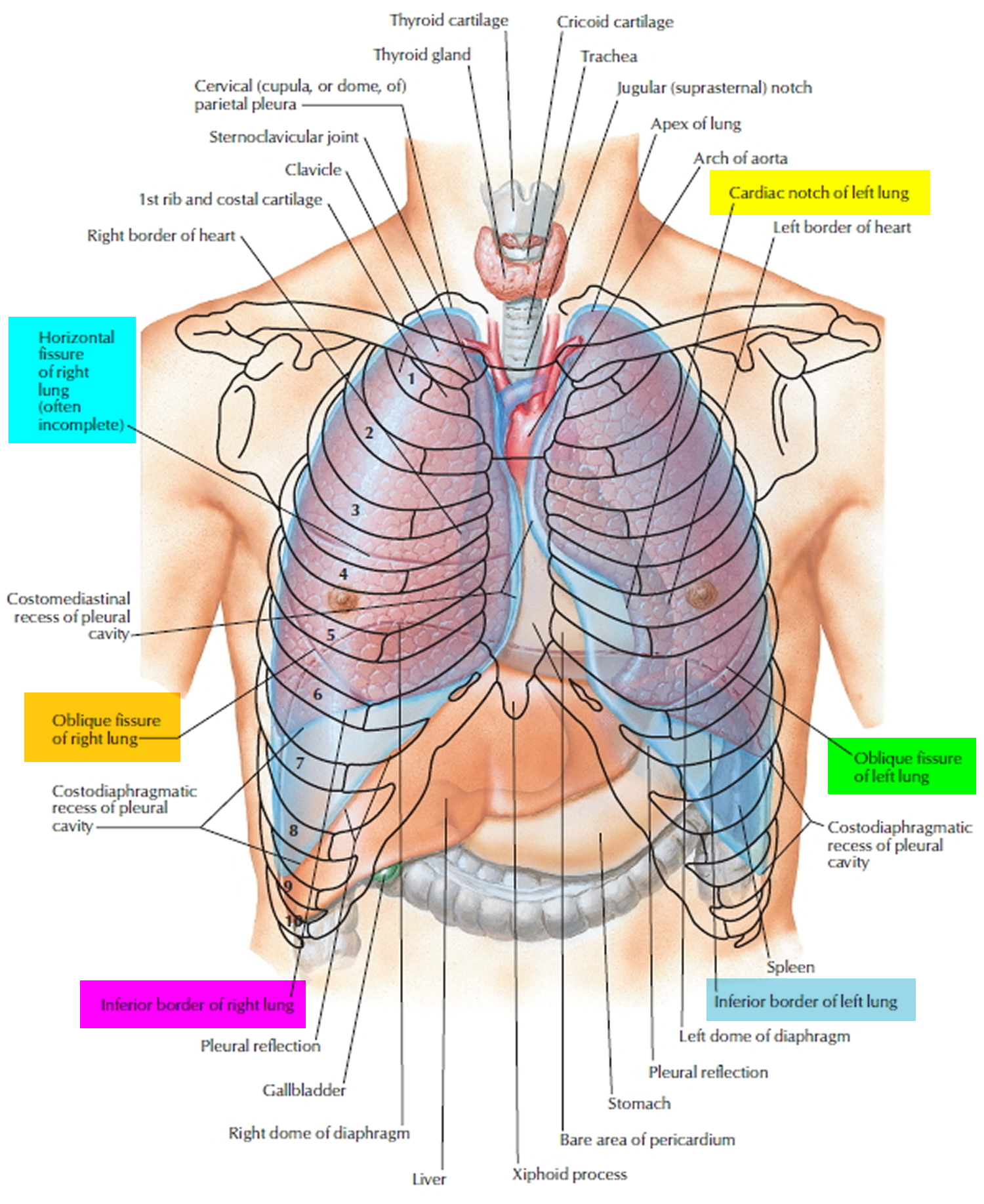
Figure 13. Lungs pleural cavity
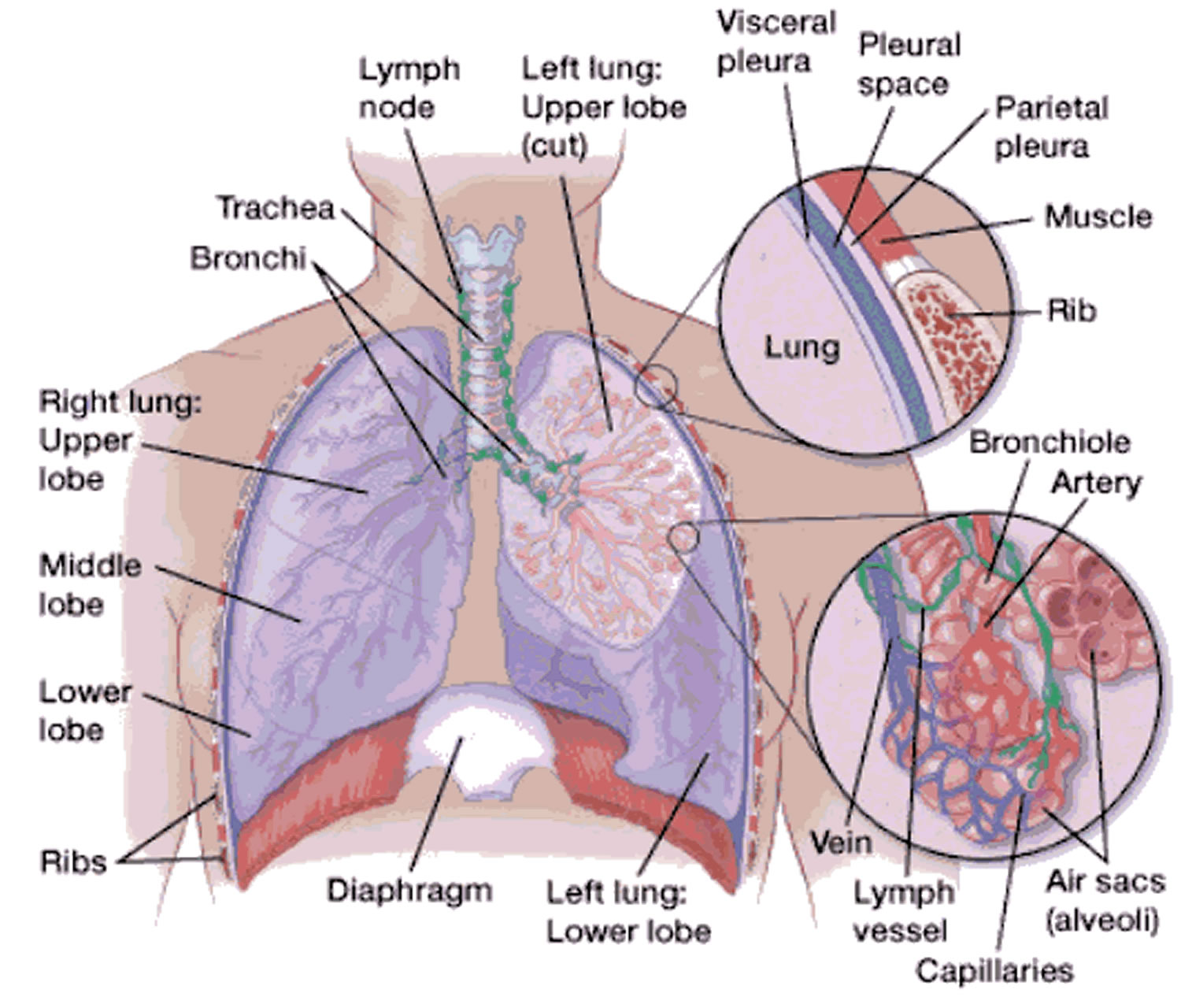
Figure 14. Bronchial tree of the lungs
Pneumothorax types
There are different types of pneumothorax:
Spontaneous pneumothorax
Spontaneous pneumothorax is a collapsed lung that happens without an injury. Spontaneous pneumothorax types include:
Primary spontaneous pneumothorax
Primary spontaneous pneumothorax is the most common type of pneumothorax, has no known cause and develops in otherwise healthy people. Primary spontaneous pneumothorax is thought to be caused by a tiny tear of an outer part of the lung. This can happen if abnormal air pockets in your lung (blebs) break apart and release air. Primary spontaneous pneumothorax is more common in tall people and mainly affects healthy young adults without lung disease.
Secondary spontaneous pneumothorax
Secondary spontaneous pneumothorax develops as a complication of existing lung disease, such as chronic obstructive pulmonary disease (COPD), pneumonia, tuberculosis, sarcoidosis or cystic fibrosis. The lung disease weakens the edge of the lung in some way, making the lung more likely to tear and cause air to escape.
Catamenial pneumothorax
Catamenial pneumothorax is a pneumothorax occurring during the perimenstrual period that affect women with endometriosis 83. “Perimenstrual period” encompasses the period of 72 – 96 hours before and after menstrual bleeding. Endometrial tissue growing outside of your uterus can form cysts that can bleed into the pleural space, causing your lung to collapse.
The broadest definitions of catamenial pneumothorax describe it as pneumothorax occurring from 7 days before the start of monthly bleeding to 7 days after its completion 84. The additional criteria include: characteristic pleural lesions, right-sided location of the pneumothorax, and concomitant endometriosis 85, 86. Concomitance of catamenial pneumothorax and endometriosis was described in a woman in the 8th week of pregnancy 87. Thoracic endometriosis is defined as the presence of ectopic endometrium within the chest, the symptoms of which appear during ovulation 88. Symptoms of pelvic endometriosis, secondary or primary infertility, and previous gynecological procedures 85 may suggest the diagnosis of catamenial pneumothorax in the course of endometriosis. A review of the treatment results of 110 patients with thoracic endometriosis revealed that pneumothorax occurred in 72% of the women, hemoptysis in 14%, pleural hematomas in 12%, and lung nodules in 2% 88. Pelvic endometriosis may precede the development of thoracic endometriosis by 5 years 89. Despite the fact that the most common manifestation of thoracic endometriosis is pneumothorax 88, in some cases of catamenial pneumothorax, endometrial character of the disease cannot be confirmed histologically 84. Abnormal fenestrations in the tendinous part of the diaphragm can be observed during surgical procedures performed on patients suffering from catamenial pneumothorax concomitant with endometriosis. Furthermore, the patients’ pleurae feature spots and nodules which are endometrial implants. The lesions are most often located on the diaphragmatic pleura.
3% to 6% of spontaneous pneumothorax cases meet the definition of catamenial pneumothorax, constituting an indication for surgical treatment in 1/3 of the affected women. The mean age of onset is 32-35 years 90. The condition may develop as late as at 39 years of age 91. Catamenial pneumothorax is most often (85-95%) unilateral, occurring on the right side of the chest, but it may also occur on the left side or bilaterally 91.
The cause and subsequent development of catamenial pneumothorax is explained by the following theories: physiological, migrational, microembolic-metastatic, and the diaphragmatic theory of air “passage” (Table 1).
Catamenial pneumothorax is associated with the following findings: single or multiple fenestrations in the tendinous part of the diaphragm; red/brown spots or nodules located on the diaphragmatic or visceral pleura. Histopathological analysis of these nodules (spots) reveals glandular cells, endometrial stroma, and macrophages filled with hemosiderin, whereas immunohistochemical testing may demonstrate the presence of estrogen and progesterone receptors 92. These findings are observed if pneumothorax is accompanied by endometriosis, especially within the pelvis, as occurs in 30-51% of cases.
Table 1. Theories for the development of thoracic foci of endometriosis in the development of catamenial pneumothorax
| Physiological | High concentration of prostaglandin F2 during menses may cause blood vessels and bronchioles to contract, which leads to alveolar rupture and development of pneumothorax. |
| Migrational | Endometrial cells may migrate from the uterus, through the fallopian tubes, into the lesser pelvis and further, into the area of the diaphragm. The cyclical proliferation and necrosis of endometrial cells may injure the diaphragm, enabling the cells to migrate further into the chest and the visceral pleura, which may lead to pulmonary alveolar injury and pneumothorax. |
| Microembolic-metastatic | Metastatic spread or pulmonary microembolization from endometrial cells through blood or lymph vessels. Necrosis of subpleural interstitial endometriotic foci leads to pneumothorax; foci located more centrally cause hemoptysis. |
| Diaphragmatic theory of air “passage” | Air passes through the uterus and fallopian tubes into the peritoneal cavity and, through diaphragmatic fenestrations, into the pleural cavity. |
Traumatic pneumothorax
Traumatic pneumothorax is a type of pneumothorax is caused by an incident such as a car accident, broken ribs or a stab wound.
Iatrogenic pneumothorax
Iatrogenic pneumothorax is a pneumothorax that occurs as a result of mechanical ventilation, which causes an imbalance in the air pressure around the lungs.
Tension pneumothorax
Tension pneumothorax is a pneumothorax (of any type) that leads to the heart and lungs not working properly. It is a medical emergency.
Spontaneous pneumothorax causes
Spontaneous means the pneumothorax was not caused by an injury such as a rib fracture. Primary spontaneous pneumothorax is likely due to the formation of small sacs of air (blebs) in lung tissue that rupture, causing air to leak into the pleural space. Air in the pleural space creates pressure on the lung and can lead to its collapse. A person with this condition may feel chest pain on the side of the collapsed lung and shortness of breath.
Blebs may be present on an individual’s lung (or lungs) for a long time before they rupture. Many things can cause a bleb to rupture, such as changes in air pressure or a very sudden deep breath. Often, people who experience a primary spontaneous pneumothorax have no prior sign of illness; the blebs themselves typically do not cause any symptoms and are visible only on medical imaging. Affected individuals may have one bleb to more than thirty blebs. Once a bleb ruptures and causes a pneumothorax, there is an estimated 13 to 60 percent chance that the condition will recur.
There are 2 types of spontaneous pneumothorax:
Primary spontaneous pneumothorax
Primary spontaneous pneumothorax is the most common type of pneumothorax making up about 40% of spontaneous pneumothoraces has no known cause and develops in otherwise healthy people. Primary spontaneous pneumothorax is thought to be caused by a tiny tear of an outer part of the lung. This can happen if abnormal air pockets in your lung (blebs) break apart and release air. Primary spontaneous pneumothorax is more common in tall people and mainly affects healthy young adults without lung disease.
Secondary spontaneous pneumothorax
Secondary spontaneous pneumothorax develops as a complication of existing lung disease. The lung disease weakens the edge of the lung in some way, making the lung more likely to tear and cause air to escape.
Secondary spontaneous pneumothorax is associated with, but not limited to, the following:
- asthma,
- chronic obstructive pulmonary disease (COPD),
- pneumonia,
- tuberculosis,
- sarcoidosis
- cystic fibrosis
- alpha-1 antitrypsin deficiency
- lung abscess
- lung cancer
- interstitial lung disease (e.g., idiopathic pulmonary fibrosis, sarcoidosis, lymphangioleiomyomatosis)
- connective tissue disease (e.g., Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome, homocysteinuria, rheumatoid arthritis)
- pulmonary infarction also called lung infarction, is when part of the lung dies due to a blocked artery. It’s usually caused by a pulmonary embolism (PE).
- foreign body aspiration
- catamenial pneumothorax is as spontaneous pneumothorax occurring within 72 hours before or after onset of menstruation (i.e., associated with menses secondary to thoracic endometriosis)
- Birt-Hogg-Dube syndrome
Risk factors for a pneumothorax
Pneumothorax in those over 40 years of age is commonly seen in the background of emphysema or chronic bronchitis. Occasionally, asthma, and other lung disease can cause a pneumothorax.
In younger patients, pneumothorax may occur spontaneously or due to chest trauma. Spontaneous pneumothorax commonly occurs in tall, thin young men (sex ratio: 6:1), due to rupture of small subpleural ‘blebs’. Trauma such as a rib fracture, or penetrating chest wall injury, may also cause pneumothorax.
Risk factors for a pneumothorax include:
- Your sex. In general, men are far more likely to have a pneumothorax than are women.
- Smoking. The risk increases with the length of time and the number of cigarettes smoked, even without emphysema.
- Age. The type of pneumothorax caused by ruptured air blisters is most likely to occur in people between 20 and 40 years old, especially if the person is a very tall and underweight.
- Genetics. Certain types of pneumothorax appear to run in families.
- Lung disease. Having an underlying lung disease — especially chronic obstructive pulmonary disease (COPD) — makes a collapsed lung more likely.
- Mechanical ventilation. People who need mechanical ventilation to assist their breathing are at higher risk of pneumothorax.
- Previous pneumothorax. Anyone who has had one pneumothorax is at increased risk of another, usually within one to two years of the first.
- Pregnancy
- Have a tall, thin body type, especially if you are a man.
- Marfan syndrome.
- Endometriosis.
Spontaneous pneumothorax signs and symptoms
Spontaneous pneumothorax most commonly presents without severe symptoms.
Patients with a collapsed lung may experience a sudden onset of the following symptoms:
- Sharp chest pain, made worse by a deep breath or a cough
- Shortness of breath
A larger pneumothorax will cause more severe symptoms, including:
- Chest tightness
- Easy fatigue
- Rapid heart rate
- Bluish color of the skin caused by lack of oxygen
- Nasal flaring
- Chest wall retractions.
Until a bleb ruptures and causes pneumothorax, no clinical signs or symptoms are present in primary spontaneous pneumothorax. Young and otherwise healthy patients can tolerate the main physiologic consequences of a decrease in vital capacity and partial pressure of oxygen fairly well, with minimal changes in vital signs and symptoms, but those with underlying lung disease may have respiratory distress.
In one series, acute onset of chest pain and shortness of breath were present in all patients in one series; typically, both symptoms are present in 64-85% of patients. The chest pain is described as severe and/or stabbing, radiates to the ipsilateral (same side) shoulder and increases with inspiration (pleuritic).
In primary spontaneous pneumothorax, chest often improves over the first 24 hours, even without resolution of the underlying air accumulation. Well-tolerated primary spontaneous pneumothorax can take 12 weeks to resolve. In secondary spontaneous pneumothorax, the chest pain is more likely to persist with more significant clinical symptoms.
Shortness of breath/dyspnea in primary spontaneous pneumothorax is generally of sudden onset and tends to be more severe with secondary spontaneous pneumothorax because of decreased lung reserve. Anxiety, cough, and vague presenting symptoms (e.g, general malaise, fatigue) are less commonly observed. The most common underlying abnormality in secondary spontaneous pneumothorax is chronic obstructive pulmonary disease (COPD), and cystic fibrosis carries one of the highest associations, with more than 20% reporting spontaneous pneumothorax.
Despite descriptions of Valsalva maneuvers and increased intrathoracic pressures as inciting factors, spontaneous pneumothorax usually develops at rest without a history of an exertional component. By definition, spontaneous pneumothorax is not associated with trauma or stress. Symptoms of iatrogenic pneumothorax are similar to those of a spontaneous pneumothorax and depend on the age of the patient, the presence of underlying lung disease, and the extent of the pneumothorax.
A history of previous pneumothorax is important, as recurrence is common, with rates reported between 15% and 40%. Up to 15% of recurrences can be on the contralateral (opposite) side. Secondary pneumothoraces are often more likely to recur, with cystic fibrosis carrying the highest recurrence rates at 68-90%. No study has shown that the number or size of blebs and bullae found in the lung can be used to predict recurrence.
Spontaneous pneumothorax complications
Many people who have had one pneumothorax can have another, usually within one to two years of the first. Air may sometimes continue to leak if the opening in the lung won’t close. Surgery may eventually be needed to close the air leak.
Although most collapsed lungs heal without issues, some people have serious complications. These can include:
- Re-expansion pulmonary edema.
- Damage or infection caused by the treatment.
- Respiratory failure.
- Heart failure.
Spontaneous pneumothorax diagnosis
If you have a sudden onset of shortness of breath or sharp chest pain that is worsened by breathing, go to the Emergency Room to be evaluated or call your local emergency number. In order to make an accurate diagnosis, the medical team will evaluate your symptoms and perform a physical exam, including the following:
- History: Your physician will obtain your full medical history, in addition to assessing the symptoms you’re currently experiencing. You may be asked questions about when the symptoms started, the severity of the pain or shortness of breath, and length of time you waited prior to arriving to the Emergency Room.
- Physical exam: Using a stethoscope, your doctor will listen for decreased or no breath sounds on the affected side.
- Chest X-ray: This radiologic test will show a pneumothorax if it is present. Perform frontal chest X-ray in inspiration, without expiratory films, in case of suspected spontaneous pneumothorax to diagnose it and assess its size.
- In some cases, a chest computerized tomography (CT) scan (low-dose chest CT-scan) may be needed to provide more-detailed images. The chest CT-scan is superior to the chest X-ray for assessing the size of a pneumothorax and to determine secondary pneumothorax causes 93. However, the cost, time and radiation exposure do not support its use as a first-line examination.
- Chest ultrasound imaging also may be used to identify a pneumothorax. The added value of chest ultrasound is currently for chest trauma patients or the diagnosis of iatrogenic pneumothorax, with a high pretest probability 94, 95.
Physical Examination
The presentation of a patient with pneumothorax may range from completely asymptomatic to life-threatening respiratory distress. Symptoms may include sweating (diaphoresis), splinting chest wall to relieve pleuritic pain, and cyanosis (in the case of tension pneumothorax). Findings on lung auscultation also vary depending on the extent of the pneumothorax. Affected patients may also reveal altered mental status changes, including decreased alertness and/or consciousness (a rare finding).
Respiratory findings may include the following:
- Respiratory distress (considered a universal finding) or respiratory arrest
- Tachypnea (or bradypnea as a preterminal event)
- Asymmetric lung expansion – A mediastinal and tracheal shift to the contralateral side can occur with a large tension pneumothorax
- Distant or absent breath sounds – Unilaterally decreased or absent lung sounds is a common finding, but decreased air entry may be absent even in an advanced state of the disease
- Lung sounds transmitted from the unaffected hemithorax are minimal with auscultation at the midaxillary line
- Hyperresonance on percussion – This is a rare finding and may be absent even in an advanced state of the disease
- Decreased tactile fremitus
- Adventitious lung sounds (crackles, wheeze; an ipsilateral finding)
Cardiovascular findings may include the following:
- Tachycardia – This is the most common finding. If the heart rate is faster than 135 beats/min, tension pneumothorax is likely
- Pulsus paradoxus is a condition where your blood pressure drops more than normal when you breathe in. It’s a sign of impaired cardiac function or pericardial involvement.
- Hypotension – This should be considered as an inconsistently present finding; although hypotension is typically considered a key sign of a tension pneumothorax, studies suggest that hypotension can be delayed until its appearance immediately precedes cardiovascular collapse
- Jugular venous distention – This is generally seen in tension pneumothorax, although it may be absent if hypotension is severe
- Cardiac apical displacement – This is a rare finding.
Tension pneumothorax
Although tension pneumothorax may be a difficult diagnosis to make and may present with considerable variability in signs, respiratory distress and chest pain are generally accepted as being universally present, and tachycardia and ipsilateral air entry on auscultation are also common findings. Sometimes, reliance on history alone may be warranted.
Findings may be affected by the volume status of the patient. In hypovolemic trauma patients with ongoing hemorrhage, the physical findings may lag behind the presentation of shock and cardiopulmonary collapse. Increased pulmonary artery pressures and decreased cardiac output or cardiac index are evidence of tension pneumothorax in patients with Swan-Ganz catheters.
When examining a patient for suspected tension pneumothorax, any clue may be helpful, as subtle thoracic size and thoracic mobility differences may be elicited by performing careful visual inspection along the line of the thorax. In a supine patient, the examiner should lower themselves to be on a level with the patient.
Tracheal deviation is an inconsistent finding. Although historic emphasis has been placed on tracheal deviation in the setting of tension pneumothorax, tracheal deviation is a relatively late finding caused by midline shift.
Abdominal distention may occur from increased pressure in the thoracic cavity producing caudal deviation of the diaphragm and from secondary pneumoperitoneum produced as air dissects across the diaphragm through the pores of Kohn.
If patients who are mechanically ventilated are difficult to ventilate during resuscitation, high peak airway pressures are clues to pneumothorax. A tension pneumothorax causes progressive difficulty with ventilation as the normal lung is compressed. On volume-control ventilation, this is indicated by marked increase in both peak and plateau pressures, with relatively preserved peak and plateau pressure difference. On pressure control ventilation, tension pneumothorax causes sudden drop in tidal volume. However, these observations are neither sensitive nor specific for making the diagnosis of pneumothorax or ruling out the possibility of pneumothorax.
The development of tension pneumothorax in patients who are ventilated will generally be of faster onset with immediate, progressive arterial and mixed venous oxyhemoglobin saturation decline and immediate decline in cardiac output. Cardiac arrest associated with asystole or pulseless electrical activity (PEA) may ultimately result. Occasionally, the tension pneumothorax may be tolerated and its diagnosis delayed for hours to days after the initial insult. The diagnosis may become evident only if the patient is receiving positive-pressure ventilation. Tension pneumothorax has been reported during surgery with both single- and double-lumen tubes.
Spontaneous pneumothorax differential diagnosis
Spontaneous pneumothorax differential diagnosis may include:
- Heart attack (myocardial infarction)
- Aortic dissection
- Acute pericarditis
- Pulmonary embolism (PE)
- Rib and chest trauma
Spontaneous pneumothorax treatment
Treatment of spontaneous pneumothorax depends on the duration, severity of your symptoms, size of your pneumothorax, the type of spontaneous pneumothorax you have (i.e., primary spontaneous pneumothorax or secondary spontaneous pneumothorax) and sometimes on your overall health 4, 20, 21, 8, 96, 97, 18, 98, 61, 99, 36.
Patients who seek treatment for minimal or resolving symptoms after more than 24 hours will receive a chest X-ray to determine treatment. If the imaging reveals only a small pneumothorax, the patient may only require oxygen supplementation and observation in the hospital for a brief period of time.
Patients with large pneumothorax who seek treatment within a short time of the onset and present more severe symptoms may require placement of a chest tube (inserted between the ribs) to release the tension. In most cases, the placement of the chest tube allows the lung to re-expand fully and quickly.
The chest tube can be left in place for several days. During that time, your child must stay in the hospital for continued evaluation. She will undergo a series of chest X-rays to monitor the pneumothorax and determine if it is improving or worsening.
Some patients with a pneumothorax may also receive supplemental oxygen, which may improve symptoms and can help the air around the lung be reabsorbed more quickly.
Patients with a persistent air leak from the chest tube for more than five days or those with recurrent or bilateral spontaneous pneumothorax may be candidates for surgery.
A tension pneumothorax should be treated with immediate chest decompression with a needle through an anterior (mid-clavicular line in the 2nd intercostal space between the second and third rib at the front) or axillary (mid-axillary line in the 4th intercostal space) approach. This is then followed by a formal intercostal tube insertion as above.
Figure 15. Primary spontaneous pneumothorax treatment algorithm
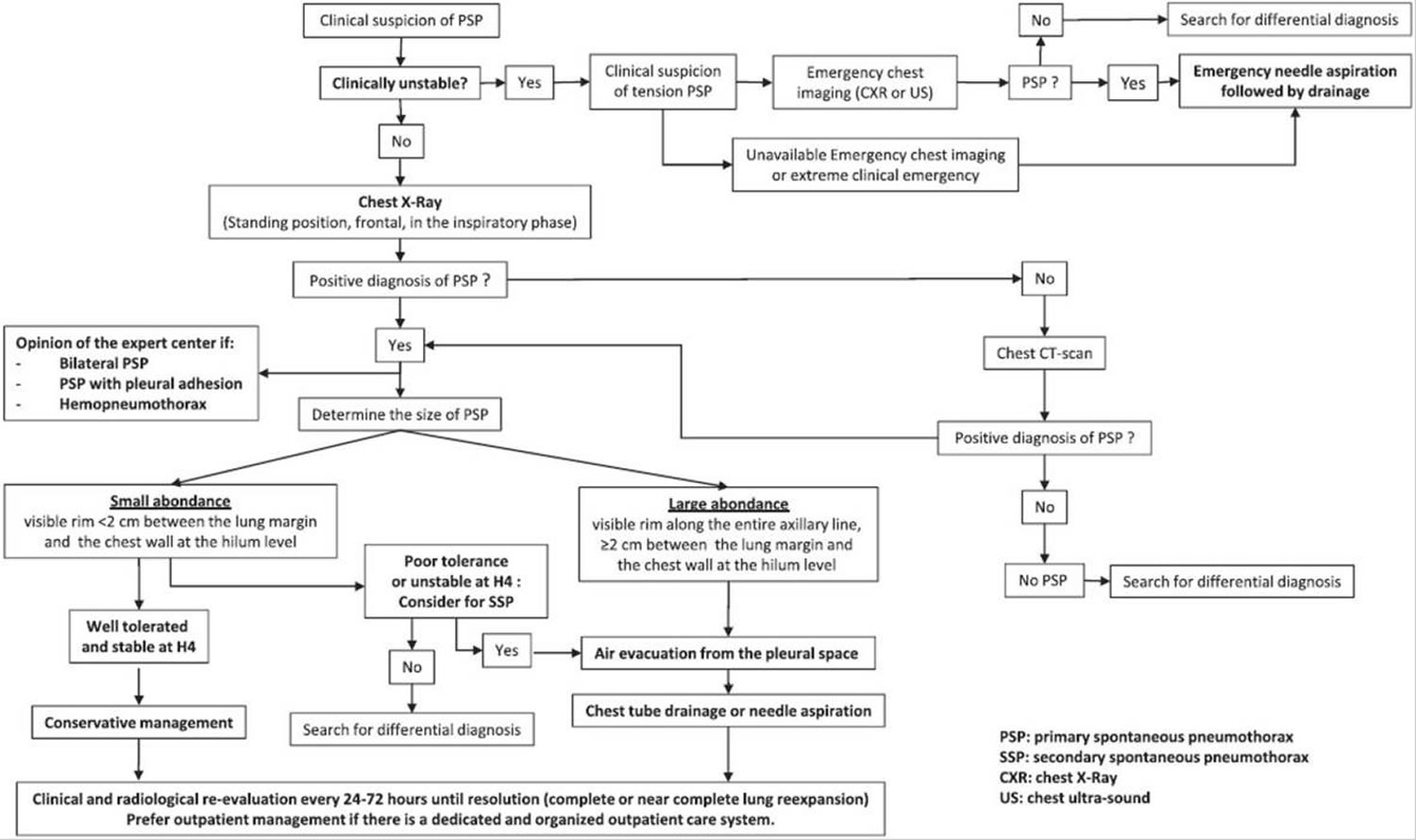
Abbreviation: PSP = primary spontaneous pneumothorax; SSP = secondary spontaneous pneumothorax
[Source 2 ]Observation
If only a small portion of your lung is collapsed, your doctor may simply monitor your condition with a series of chest X-rays until the excess air is completely absorbed and your lung has re-expanded. This may take several weeks.
Needle aspiration or chest tube insertion
If a larger area of your lung has collapsed, it’s likely that a needle or chest tube will be used to remove the excess air.
- Needle aspiration. A hollow needle with a small flexible tube (catheter) is inserted between the ribs into the air-filled space that’s pressing on the collapsed lung. Then the doctor removes the needle, attaches a syringe to the catheter and pulls out the excess air. The catheter may be left in for a few hours to ensure the lung is re-expanded and the pneumothorax does not recur.
- Chest tube insertion. A flexible chest tube is inserted into the air-filled space and may be attached to a one-way valve device that continuously removes air from the chest cavity until your lung is re-expanded and healed.
Nonsurgical repair
If a chest tube doesn’t re-expand your lung, nonsurgical options to close the air leak may include:
- Chemical pleurodesis: Using a substance (such as doxycycline or talcum powder to irritate the tissues around your lung so that they’ll stick together and seal any leaks. This can be done through the chest tube, but it may be done during surgery.
- Drawing blood from your arm and placing it into the chest tube. The blood creates a fibrinous patch on the lung (autologous blood patch), sealing the air leak.
- Passing a thin tube (bronchoscope) down your throat and into your lungs to look at your lungs and air passages and placing a one-way valve. The valve allows the lung to re-expand and the air leak to heal.
Surgery
Patients with a persistent air leak from the chest tube for more than five days or those with recurrent or bilateral spontaneous pneumothorax may be candidates for surgery. In most cases, the surgery can be performed through small incisions, using a tiny fiber-optic camera and narrow, long-handled surgical tools. The surgeon will look for the leaking area or ruptured air blister and close it off. Rarely, the surgeon will have to make a larger incision between the ribs to get better access to multiple or larger air leaks.
Goals of surgery:
- Identify bullae (blebs) responsible for the air leak and remove them if they are present.
- Obliterate the pleural space and minimize the chances for future lung collapse.
The operation is usually performed using a video-assisted thoracic surgery (VATS), with two to four small incisions.
After surgery
After your child has surgery to treat spontaneous pneumothorax, she will spend an hour or so recovering in the post-acute care unit before returning to a room in the hospital. She will likely have a chest tube after the operation, which may need to remain in place for a number of days.
Your child will experience some pain and will receive pain medications throughout the stay. Some patients will initially require IV pain medications and then transition to oral pain medications. The pain management team will work with the surgical team and your child to provide adequate pain control.
Your child may have chest incisions with a clear adhesive glue dressing or gauze covering the site. The clear adhesive will dissolve and peel off naturally; the gauze dressings will be removed 48-72 hours after surgery.
Follow-up care
If your child has an operation or receives inpatient treatment with a chest tube or oxygen therapy to treat spontaneous pneumothorax, you will need to make an appointment to see the surgeon for follow-up three to four weeks after discharge. After your child has been treated for spontaneous pneumothorax, it is important that you carefully monitor her health.
After you or your child has been treated for spontaneous pneumothorax, it is important that you carefully monitor her health. See your doctor if you or your child experiences any of the following symptoms:
- Fever greater than 101 °F (> 38.3 °C)
- Signs of infection of incision sites, including: redness, yellow or green discharge, tenderness, warmth or foul odor
- Any other concerns
If your child suffers any of the following signs or symptoms, she must be brought to the Emergency Department as quickly as possible to receive proper treatment:
- Sudden onset of chest pain
- Shortness of breath or difficulty breathing
Ongoing care
You may need to avoid certain activities that put extra pressure on your lungs for a time after your pneumothorax heals. Examples include flying, scuba diving or playing a wind instrument. Expert group proposes to strongly avoid scuba diving in patients with a history of primary spontaneous pneumothorax, even if the patient has undergone pleurodesis, due to the risk of fatal barotrauma 2. Talk to your doctor about the type and length of your activity restrictions. Keep follow-up appointments with your doctor to monitor your healing.
Spontaneous pneumothorax prognosis
Tension pneumothorax is a potentially life-threatening condition, due to restriction of venous return, and respiratroy and cardiac shock. Otherwise, pneumothorax tends to slowly resolve, such that a pneumothorax causing 50% collapse of the lung will take 40 days to heal.
- MacDuff A, Arnold A, Harvey J. Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline 2010. Thorax 2010; 65: Suppl. 2, ii18–ii31. doi: 10.1136/thx.2010.136986[↩]
- Jouneau S, Ricard JD, Seguin-Givelet A, Bigé N, Contou D, Desmettre T, Hugenschmitt D, Kepka S, Le Gloan K, Maitre B, Mangiapan G, Marchand-Adam S, Mariolo A, Marx T, Messika J, Noël-Savina E, Oberlin M, Palmier L, Perruez M, Pichereau C, Roche N, Garnier M, Martinez M. SPLF/SMFU/SRLF/SFAR/SFCTCV Guidelines for the management of patients with primary spontaneous pneumothorax. Ann Intensive Care. 2023 Sep 19;13(1):88. doi: 10.1186/s13613-023-01181-2[↩][↩][↩][↩][↩][↩][↩]
- Louw EH, Shaw JA, Koegelenberg CFN. New insights into spontaneous pneumothorax: A review. Afr J Thorac Crit Care Med. 2021 Mar 9;27(1):10.7196/AJTCCM.2021.v27i1.054. doi: 10.7196/AJTCCM.2021.v27i1.054[↩][↩]
- Costumbrado J, Ghassemzadeh S. Spontaneous Pneumothorax. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459302[↩][↩][↩][↩][↩]
- Shorthose M, Barton E, Walker S. The contemporary management of spontaneous pneumothorax in adults. Breathe (Sheff). 2023 Dec;19(4):230135. doi: 10.1183/20734735.0135-2023[↩]
- Nava GW, Walker SP. Management of the Secondary Spontaneous Pneumothorax: Current Guidance, Controversies, and Recent Advances. J Clin Med. 2022 Feb 22;11(5):1173. doi: 10.3390/jcm11051173[↩]
- Wilson PM, Rymeski B, Xu X, Hardie W. An evidence-based review of primary spontaneous pneumothorax in the adolescent population. J Am Coll Emerg Physicians Open. 2021 Jun 18;2(3):e12449[↩]
- Skaarup SH, Laursen CB, Hallifax RJ, Iqbal B, Bødtger U. National survey on management of spontaneous pneumothorax from emergency department to specialised treatment: room for improvement. Eur Clin Respir J. 2024 Jan 31;11(1):2307648. doi: 10.1080/20018525.2024.2307648[↩][↩]
- Farag GAI, Zineldin MAI, Al Awady RSAA, Abd El Salam AB, Elkahely MA. Comparative Analysis of Demographic Characteristics, Management, and Outcomes in Primary Versus Secondary Spontaneous Pneumothorax. Cureus. 2024 Jul 23;16(7):e65216. doi: 10.7759/cureus.65216[↩]
- Hallifax RJ, Goldacre R, Landray MJ, Rahman NM, Goldacre MJ. Trends in the Incidence and Recurrence of Inpatient-Treated Spontaneous Pneumothorax, 1968-2016. JAMA. 2018 Oct 9;320(14):1471-1480. doi: 10.1001/jama.2018.14299[↩][↩]
- Fujiwara T, Tanaka K, Toyoda T, Inage T, Sakairi Y, Ishibashi F, Suzuki H, Nakajima T, Yoshino I. Risk factors of postoperative recurrence of primary spontaneous pneumothorax. J Thorac Dis. 2020 Nov;12(11):6458-6465. doi: 10.21037/jtd-20-2436[↩]
- Baldemir R, Ülger G. A holistic investigation of the global outcomes of spontaneous pneumothorax during 1980-2021, including the COVID-19 pandemic A bibliometric approach. Medicine (Baltimore). 2022 Mar 18;101(11):e29113. doi: 10.1097/MD.0000000000029113[↩]
- Huang N, He S, Chen S, Zhang G, Ruan L, Huang J. Incidence and risk factors for recurrent primary spontaneous pneumothorax after video-assisted thoracoscopic surgery: a systematic review and meta-analysis. J Thorac Dis. 2024 Jun 30;16(6):3696-3710. doi: 10.21037/jtd-24-175[↩]
- van Steenwijk QCA, Spaans LN, Heineman DJ, van den Broek FJC, Dickhoff C. Population-based study on surgical care for primary spontaneous pneumothorax. Eur J Cardiothorac Surg. 2024 Mar 29;65(4):ezae104. doi: 10.1093/ejcts/ezae104[↩]
- Miró Ò, Llorens P, Jiménez S, Piñera P, Burillo-Putze G, Martín A, Martín-Sánchez FJ, García-Lamberetchs EJ, Jacob J, Alquézar-Arbé A, Mòdol JM, López-Díez MP, Guardiola JM, Cardozo C, Lucas Imbernón FJ, Aguirre Tejedo A, García García Á, Ruiz Grinspan M, Llopis Roca F, González Del Castillo J; Spanish Investigators on Emergency Situations Team (SIESTA) Network. Frequency, Risk Factors, Clinical Characteristics, and Outcomes of Spontaneous Pneumothorax in Patients With Coronavirus Disease 2019: A Case-Control, Emergency Medicine-Based Multicenter Study. Chest. 2021 Mar;159(3):1241-1255. doi: 10.1016/j.chest.2020.11.013[↩]
- Noppen M. Spontaneous pneumothorax: epidemiology, pathophysiology and cause. Eur Respir Rev. 2010 Sep;19(117):217-9. doi: 10.1183/09059180.00005310[↩]
- Porcel JM, Lee P. Thoracoscopy for Spontaneous Pneumothorax. J Clin Med. 2021 Aug 26;10(17):3835. doi: 10.3390/jcm10173835[↩]
- Gariépy M, Beaunoyer M, Miron MC, Gravel J. Management and recurrence of spontaneous pneumothorax in children. Paediatr Child Health. 2020 Mar;25(2):86-92. doi: 10.1093/pch/pxz032[↩][↩]
- Bense L, Wiman LG, Hedenstierna G. Onset of symptoms in spontaneous pneumothorax: correlations to physical activity. Eur J Respir Dis. 1987 Sep;71(3):181-6.[↩]
- Baig MA, Majeed MB, Attar BM, Khan Z, Demetria M, Gandhi SR. Efficacy and Safety of Indwelling Pleural Catheters in Management of Hepatic Hydrothorax: A Systematic Review of Literature. Cureus. 2018 Aug 6;10(8):e3110. doi: 10.7759/cureus.3110[↩][↩]
- Ojeda Rodriguez JA, Hipskind JE. Iatrogenic Pneumothorax. [Updated 2024 Mar 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526057[↩][↩]
- Kepka S, Dalphin JC, Pretalli JB, Parmentier AL, Lauque D, Trebes G, et al. How spontaneous pneumothorax is managed in emergency departments: a French multicentre descriptive study. BMC Emerg Med. 2019;19(1):4. doi: 10.1186/s12873-018-0213-2[↩]
- Brown SG, Ball EL, Macdonald SP, Wright C, McD Taylor D. Spontaneous pneumothorax; a multicentre retrospective analysis of emergency treatment, complications and outcomes. Intern Med J. 2014 May;44(5):450-7. doi: 10.1111/imj.12398[↩][↩][↩]
- Eamer G, Povolo CA, Petropoulos JA, Ohinmaa A, Vanhouwelingen L. Observation, Aspiration, or Tube Thoracostomy for Primary Spontaneous Pneumothorax: A Systematic Review, Meta-Analysis, and Cost-Utility Analysis. Chest. 2023 Oct;164(4):1007-1018. doi: 10.1016/j.chest.2023.05.017[↩]
- Harris M, Rocker J. Pneumothorax In Pediatric Patients: Management Strategies To Improve Patient Outcomes. Pediatr Emerg Med Pract. 2017 Mar;14(3):1-28. https://www.ebmedicine.net/topics/cardiovascular/pediatric-pneumothorax[↩]
- Wong A, Galiabovitch E, Bhagwat K. Management of primary spontaneous pneumothorax: a review. ANZ J Surg. 2019 Apr;89(4):303-308. doi: 10.1111/ans.14713[↩]
- Schnell J, Beer M, Eggeling S, Gesierich W, Gottlieb J, Herth FJF, Hofmann HS, Jany B, Kreuter M, Ley-Zaporozhan J, Scheubel R, Walles T, Wiesemann S, Worth H, Stoelben E. Management of Spontaneous Pneumothorax and Post-Interventional Pneumothorax: German S3 Guideline. Respiration. 2019;97(4):370-402. doi: 10.1159/000490179[↩]
- Santos C, Gupta S, Baraket M, Collett PJ, Xuan W, Williamson JP. Outcomes of an initiative to improve inpatient safety of small bore thoracostomy tube insertion. Intern Med J. 2019 May;49(5):644-649. doi: 10.1111/imj.14110[↩]
- Large spontaneous pneumothorax. https://radiopaedia.org/cases/large-spontaneous-pneumothorax#image-54418964[↩]
- Bilateral pneumothoraces with deep sulcus sign. https://radiopaedia.org/cases/bilateral-pneumothoraces-with-deep-sulcus-sign#image-51875702[↩]
- Spontaneous pneumothorax due to ruptured apical bullae. https://radiopaedia.org/cases/spontaneous-pneumothorax-due-to-ruptured-apical-bullae-1#image-2441527 [↩]
- Hallifax RJ, Goldacre R, Landray MJ, et al. Trends in the incidence and recurrence of inpatient-treated spontaneous pneumothorax, 1968–2016. JAMA 2018; 320: 1471–1480. doi: 10.1001/jama.2018.14299[↩]
- Savitsky E, Oh SS, Lee JM. The Evolving Epidemiology and Management of Spontaneous Pneumothorax. JAMA. 2018 Oct 9;320(14):1441-1443. doi: 10.1001/jama.2018.12878[↩]
- MacDuff A, Arnold A, Harvey J; BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010 Aug;65 Suppl 2:ii18-31. doi: 10.1136/thx.2010.136986[↩]
- Baumann MH, Strange C, Heffner JE, Light R, Kirby TJ, Klein J, Luketich JD, Panacek EA, Sahn SA; AACP Pneumothorax Consensus Group. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest. 2001 Feb;119(2):590-602. doi: 10.1378/chest.119.2.590[↩]
- Walker SP, Bibby AC, Halford P, Stadon L, White P, Maskell NA. Recurrence rates in primary spontaneous pneumothorax: a systematic review and meta-analysis. Eur Respir J. 2018 Sep 6;52(3):1800864. doi: 10.1183/13993003.00864-2018[↩][↩]
- Tan J, Yang Y, Zhong J, Zuo C, Tang H, Zhao H, Zeng G, Zhang J, Guo J, Yang N. Association Between BMI and Recurrence of Primary Spontaneous Pneumothorax. World J Surg. 2017 May;41(5):1274-1280. doi: 10.1007/s00268-016-3848-8[↩]
- Sadikot RT, Greene T, Meadows K, Arnold AG. Recurrence of primary spontaneous pneumothorax. Thorax. 1997 Sep;52(9):805-9. doi: 10.1136/thx.52.9.805[↩]
- Olesen WH, Lindahl-Jacobsen R, Katballe N, Sindby JE, Titlestad IL, Andersen PE, Licht PB. Recurrent Primary Spontaneous Pneumothorax is Common Following Chest Tube and Conservative Treatment. World J Surg. 2016 Sep;40(9):2163-70. doi: 10.1007/s00268-016-3508-z[↩]
- Guo Y, Xie C, Rodriguez RM, Light RW. Factors related to recurrence of spontaneous pneumothorax. Respirology. 2005 Jun;10(3):378-84. doi: 10.1111/j.1440-1843.2005.00715.x[↩]
- Primavesi F, Jäger T, Meissnitzer T, Buchner S, Reich-Weinberger S, Öfner D, Hutter J, Aspalter M. First Episode of Spontaneous Pneumothorax: CT-based Scoring to Select Patients for Early Surgery. World J Surg. 2016 May;40(5):1112-20. doi: 10.1007/s00268-015-3371-3[↩]
- Ganesalingam R, O’Neil RA, Shadbolt B, Tharion J. Radiological predictors of recurrent primary spontaneous pneumothorax following non-surgical management. Heart Lung Circ. 2010 Oct;19(10):606-10. doi: 10.1016/j.hlc.2010.06.663[↩]
- Casali C, Stefani A, Ligabue G, Natali P, Aramini B, Torricelli P, Morandi U. Role of blebs and bullae detected by high-resolution computed tomography and recurrent spontaneous pneumothorax. Ann Thorac Surg. 2013 Jan;95(1):249-55. doi: 10.1016/j.athoracsur.2012.05.073[↩]
- Chan SS, Rainer TH. Primary spontaneous pneumothorax: 1-year recurrence rate after simple aspiration. Eur J Emerg Med. 2006 Apr;13(2):88-91. doi: 10.1097/01.mej.0000192047.97105.59[↩]
- Ouanes-Besbes L, Golli M, Knani J, Dachraoui F, Nciri N, El Atrous S, Gannouni A, Abroug F. Prediction of recurrent spontaneous pneumothorax: CT scan findings versus management features. Respir Med. 2007 Feb;101(2):230-6. doi: 10.1016/j.rmed.2006.05.016[↩]
- Noppen M, Alexander P, Driesen P, Slabbynck H, Verstraeten A. Manual aspiration versus chest tube drainage in first episodes of primary spontaneous pneumothorax: a multicenter, prospective, randomized pilot study. Am J Respir Crit Care Med. 2002 May 1;165(9):1240-4. doi: 10.1164/rccm.200111-078OC[↩]
- Brown SGA, Ball EL, Perrin K, Asha SE, Braithwaite I, Egerton-Warburton D, et al. Conservative versus interventional treatment for spontaneous pneumothorax. N Engl J Med. 2020;382(5):405–415. doi: 10.1056/NEJMoa1910775[↩][↩][↩][↩][↩]
- Walker SP, Bibby AC, Halford P, Stadon L, White P, Maskell NA. Recurrence rates in primary spontaneous pneumothorax: a systematic review and meta-analysis. Eur Respir J. 2018;52(3):1800864. doi: 10.1183/13993003.00864-2018[↩][↩]
- Kelly AM, Kerr D, Clooney M. Outcomes of emergency department patients treated for primary spontaneous pneumothorax. Chest. 2008;134(5):1033–1036. doi: 10.1378/chest.08-0910[↩]
- Andrivet P, Djedaini K, Teboul JL, Brochard L, Dreyfuss D. Spontaneous pneumothorax. Comparison of thoracic drainage vs immediate or delayed needle aspiration. Chest. 1995;108(2):335–339. doi: 10.1378/chest.108.2.335[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Vuillard C, Dib F, Achamlal J, Gaudry S, Roux D, Chemouny M, et al. Longer symptom onset to aspiration time predicts success of needle aspiration in primary spontaneous pneumothorax. Thorax. 2019;74(8):780–786. doi: 10.1136/thoraxjnl-2019-213168[↩][↩][↩][↩]
- Ayed AK, Chandrasekaran C, Sukumar M. Aspiration versus tube drainage in primary spontaneous pneumothorax: a randomised study. Eur Respir J. 2006;27(3):477–482. doi: 10.1183/09031936.06.00091505[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Thelle A, Gjerdevik M, SueChu M, Hagen OM, Bakke P. Randomised comparison of needle aspiration and chest tube drainage in spontaneous pneumothorax. Eur Respir J. 2017;49(4):1601296. doi: 10.1183/13993003.01296-2016[↩][↩][↩][↩]
- Harvey J, Prescott RJ. Simple aspiration versus intercostal tube drainage for spontaneous pneumothorax in patients with normal lungs. British thoracic society research committee. BMJ. 1994;309(6965):1338–1339. doi: 10.1136/bmj.309.6965.1338[↩][↩][↩][↩][↩]
- Korczynski P, Gorska K, Nasilowski J, Chazan R, Krenke R. Comparison of small bore catheter aspiration and chest tube drainage in the management of spontaneous pneumothorax. Adv Exp Med Biol. 2015;866:15–23. doi: 10.1007/5584_2015_146[↩][↩][↩][↩][↩][↩]
- Camuset J, Laganier J, Brugiere O, Dauriat G, Jebrak G, Thabut G, et al. Needle aspiration as first-line management of primary spontaneous pneumothorax. Presse Med. 2006;35(5 Pt 1):765–768. doi: 10.1016/s0755-4982(06)74687-5[↩]
- Chen JS, Tsai KT, Hsu HH, Yuan A, Chen WJ, Lee YC. Intrapleural minocycline following simple aspiration for initial treatment of primary spontaneous pneumothorax. Respir Med. 2008;102(7):1004–1010. doi: 10.1016/j.rmed.2008.02.006[↩][↩]
- Nishiuma T, Ohnishi H, Katsurada N, Yamamoto S, Yoshimura S, Kinami S. Evaluation of simple aspiration therapy in the initial treatment for primary spontaneous pneumothorax. Intern Med. 2012;51(11):1329–1333. doi: 10.2169/internalmedicine.51.6919[↩][↩]
- Chan SS, Lam PK. Simple aspiration as initial treatment for primary spontaneous pneumothorax: results of 91 consecutive cases. J Emerg Med. 2005;28(2):133–138. doi: 10.1016/j.jemermed.2004.11.001[↩][↩]
- Ho KK, Ong ME, Koh MS, Wong E, Raghuram J. A randomized controlled trial comparing minichest tube and needle aspiration in outpatient management of primary spontaneous pneumothorax. Am J Emerg Med. 2011;29(9):1152–1157. doi: 10.1016/j.ajem.2010.05.017[↩][↩][↩][↩][↩][↩][↩][↩]
- MacDuff A, Arnold A, Harvey J, Group BTSPDG Management of spontaneous pneumothorax: British thoracic society pleural disease guideline 2010. Thorax. 2010;65(Suppl 2):18–31. doi: 10.1136/thx.2010.136986[↩][↩]
- Tschopp JM, Bintcliffe O, Astoul P, Canalis E, Driesen P, Janssen J, et al. ERS task force statement: diagnosis and treatment of primary spontaneous pneumothorax. Eur Respir J. 2015;46(2):321–335. doi: 10.1183/09031936.00219214[↩]
- Parlak M, Uil SM, van den Berg JW. A prospective, randomised trial of pneumothorax therapy: manual aspiration versus conventional chest tube drainage. Respir Med. 2012;106(11):1600–1605. doi: 10.1016/j.rmed.2012.08.005[↩][↩][↩]
- Ganaie MB, Maqsood U, Lea S, Bankart MJ, Bikmalla S, Afridi MA, et al. How should complete lung collapse secondary to primary spontaneous pneumothorax be managed? Clin Med (Lond) 2019;19(2):163–168. doi: 10.7861/clinmedicine.19-2-163[↩][↩]
- Chan JW, Ko FW, Ng CK, Yeung AW, Yee WK, So LK, Lam B, Wong MM, Choo KL, Ho AS, Tse PY, Fung SL, Lo CK, Yu WC. Management of patients admitted with pneumothorax: a multi-centre study of the practice and outcomes in Hong Kong. Hong Kong Med J. 2009 Dec;15(6):427-33. https://www.hkmj.org/system/files/hkm0912p427.pdf[↩][↩]
- Noppen M, Alexander P, Driesen P, Slabbynck H, Verstraeten A. Manual aspiration versus chest tube drainage in first episodes of primary spontaneous pneumothorax: a multicenter, prospective, randomized pilot study. Am J Respir Crit Care Med. 2002;165(9):1240–1244. doi: 10.1164/rccm.200111-078OC[↩][↩][↩][↩]
- Ramouz A, Lashkari MH, Fakour S, Rasihashemi SZ. Randomized controlled trial on the comparison of chest tube drainage and needle aspiration in the treatment of primary spontaneous pneumothorax. Pak J Med Sci. 2018;34(6):1369–1374. doi: 10.12669/pjms.346.16126[↩][↩][↩][↩]
- Kim IH, Kang DK, Min HK, Hwang YH. A prospective randomized trial comparing manual needle aspiration to closed thoracostomy as an initial treatment for the first episode of primary spontaneous pneumothorax. Korean J Thorac Cardiovasc Surg. 2019;52(2):85–90. doi: 10.5090/kjtcs.2019.52.2.85[↩][↩][↩]
- Contou D, Razazi K, Katsahian S, Maitre B, Mekontso-Dessap A, Brun-Buisson C, et al. Small-bore catheter versus chest tube drainage for pneumothorax. Am J Emerg Med. 2012;30(8):1407–1413. doi: 10.1016/j.ajem.2011.10.014[↩]
- Carson-Chahhoud KV, Wakai A, van Agteren JE, Smith BJ, McCabe G, Brinn MP, et al. Simple aspiration versus intercostal tube drainage for primary spontaneous pneumothorax in adults. Cochrane Database Syst Rev. 2017;9:CD004479. doi: 10.1002/14651858.CD004479.pub3[↩]
- Olesen WH, Katballe N, Sindby JE, Titlestad IL, Andersen PE, Lindahl-Jacobsen R, et al. Surgical treatment versus conventional chest tube drainage in primary spontaneous pneumothorax: a randomized controlled trial. Eur J Cardiothorac Surg. 2018;54(1):113–121. doi: 10.1093/ejcts/ezy003[↩]
- Hofmann HS, Suttner T, Neu R, Potzger T, Szoke T, Grosser C, et al. Burden between undersupply and overtreatment in the care of primary spontaneous pneumothorax. Thorac Cardiovasc Surg. 2018;66(7):575–582. doi: 10.1055/s-0037-1609011[↩]
- Divisi D, Di Leonardo G, Crisci R. Video-assisted thoracic surgery versus pleural drainage in the management of the first episode of primary spontaneous pneumothorax. Am J Surg. 2015;210(1):68–73. doi: 10.1016/j.amjsurg.2014.10.025[↩]
- Torresini G, Vaccarili M, Divisi D, Crisci R. Is video-assisted thoracic surgery justified at first spontaneous pneumothorax? Eur J Cardiothorac Surg. 2001;20(1):42–45. doi: 10.1016/s1010-7940(01)00679-0[↩]
- Chen JS, Hsu HH, Tsai KT, Yuan A, Chen WJ, Lee YC. Salvage for unsuccessful aspiration of primary pneumothorax: thoracoscopic surgery or chest tube drainage? Ann Thorac Surg. 2008;85(6):1908–1913. doi: 10.1016/j.athoracsur.2008.02.038[↩]
- Al-Mourgi M, Alshehri F. Video-Assisted Thoracoscopic Surgery for the Treatment of First-Time Spontaneous Pneumothorax versus Conservative Treatment. Int J Health Sci (Qassim). 2015 Oct;9(4):428-32. https://pmc.ncbi.nlm.nih.gov/articles/PMC4682597[↩]
- Outpatient Management of Primary Spontaneous Pneumothorax: Pigtail Catheter With Unidirectional Valve vs. Exsufflation, Randomized Prospective Study (PNEUM-AMBU). https://clinicaltrials.gov/study/NCT03691480[↩]
- Sale A, Sohier L, Campion M, Le Ho R, Bazin Y, Gangloff C, et al. Exclusive ambulatory management of spontaneous pneumothorax with pigtail catheters, a prospective multicentric study. Respir Med. 2020;166:105931. doi: 10.1016/j.rmed.2020.105931[↩][↩][↩][↩][↩]
- Voisin F, Sohier L, Rochas Y, Kerjouan M, Ricordel C, Belleguic C, et al. Ambulatory management of large spontaneous pneumothorax with pigtail catheters. Ann Emerg Med. 2014;64(3):222–228. doi: 10.1016/j.annemergmed.2013.12.017[↩][↩][↩][↩][↩]
- Hallifax RJ, McKeown E, Sivakumar P, Fairbairn I, Peter C, Leitch A, et al. Ambulatory management of primary spontaneous pneumothorax: an open-label, randomised controlled trial. Lancet. 2020;396(10243):39–49. doi: 10.1016/S0140-6736(20)31043-6[↩][↩][↩]
- Massongo M, Leroy S, Scherpereel A, Vaniet F, Dhalluin X, Chahine B, et al. Outpatient management of primary spontaneous pneumothorax: a prospective study. Eur Respir J. 2014;43(2):582–590. doi: 10.1183/09031936.00179112[↩][↩][↩][↩]
- Hassani B, Foote J, Borgundvaag B. Outpatient management of primary spontaneous pneumothorax in the emergency department of a community hospital using a small-bore catheter and a Heimlich valve. Acad Emerg Med. 2009;16(6):513–518. doi: 10.1111/j.1553-2712.2009.00402.x[↩][↩][↩]
- Marjański T, Sowa K, Czapla A, Rzyman W. Catamenial pneumothorax – a review of the literature. Kardiochirurgia i Torakochirurgia Polska = Polish Journal of Cardio-Thoracic Surgery. 2016;13(2):117-121. doi:10.5114/kitp.2016.61044. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4971265/[↩][↩]
- Rousset-Jablonski C, Alifano M, Plu-Bureau G, Camilleri-Broet S, Rousset P, Regnard JF, Gompel A. Catamenial pneumothorax endometriosis-related pneumothorax: clinical features and risk factors. Hum Repord. 2011;26:2322–2329. https://www.ncbi.nlm.nih.gov/pubmed/21685141[↩][↩]
- Alifano M, Legras A, Rousset-Jablonski C, Bobbio A, Magdeleinat P, Damotte D, Roche N, Regnard JF. Pneumothorax recurrence after surgery in women: clinicopathologic characteristic and management. Ann Thorac Surg. 2011;92:322–326. https://www.ncbi.nlm.nih.gov/pubmed/21718864[↩][↩]
- Majak P, Langebrekke A, Hagen OM, Qviqstad E. Catamenial pneumothorax, clinical manifestations – a multidisciplinary challenge. Pneumonol Alergol Pol. 2011;79:347–350. https://www.ncbi.nlm.nih.gov/pubmed/21861259[↩]
- Yoshioka H, Fukui T, Mori S, Usami N, Nagasaka T, Yokoi K. Catamenial pneumothorax in a pregnant patient. Jpn J Thorac Cardiovasc Surg. 2005;53:280–282. https://www.ncbi.nlm.nih.gov/pubmed/15952324[↩]
- Channabasavaiah AD, Joseph JV. Thoracic endometriosis: revisiting the association between clinical presentation and thoracic pathology based on thoracoscopic findings in 110 patients. Medicine (Baltimore) 2010;89:183–188. https://www.ncbi.nlm.nih.gov/pubmed/20453605[↩][↩][↩]
- Joseph J, Sahn SA. Thoracic endometriosis syndrome: new observation from an analysis of 110 cases. Am J Med. 1996;100:164–170. https://www.ncbi.nlm.nih.gov/pubmed/8629650[↩]
- Attaran S, Bille A, Karenovics W, Lang-Lazdunski L. Videothoracoscopic repair of diaphragm and pleurectomy/abrasion in patients with catamenial pneumothorax: a 9-year experience. Chest. 2013;143:1066–1069. https://www.ncbi.nlm.nih.gov/pubmed/23117231[↩]
- Haga T, Kurihara M, Kataoka H, Ebana H. Clinical-pathological findings of catamenial pneumothorax: comparison between recurrent cases and non-recurrent cases. Ann Thorac Cardiovasc Surg. 2014;20:202–206. https://www.jstage.jst.go.jp/article/atcs/20/3/20_oa.12.02227/_pdf/-char/en[↩][↩]
- Visouli AN, Darwiche K, Mpakas A, Zarogoulidis P, Papagiannis A, Tsakiridis K, Machairiotis N, Stylianaki A, Katsikogiannis N, Courcoutsakis N, Zarogoulidis K. Catamenial pneumothorax: a rare entity? Report of 5 cases and review of the literature. J Thorac Dis. 2012;4(Suppl 1):17–31. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3537379/[↩]
- Hilliard NJ, Marciniak SJ, Babar JL, Balan A. Evaluation of secondary spontaneous pneumothorax with multidetector CT. Clin Radiol. 2013;68(5):521–528. doi: 10.1016/j.crad.2012.10.008[↩]
- Frankel HL, Kirkpatrick AW, Elbarbary M, Blaivas M, Desai H, Evans D, et al. Guidelines for the appropriate use of bedside general and cardiac ultrasonography in the evaluation of critically Ill patients-Part I: general ultrasonography. Crit Care Med. 2015;43(11):2479–2502. doi: 10.1097/CCM.0000000000001216[↩]
- Tasci O, Hatipoglu ON, Cagli B, Ermis V. Sonography of the chest using linear-array versus sector transducers: correlation with auscultation, chest radiography, and computed tomography. J Clin Ultrasound. 2016;44(6):383–389. doi: 10.1002/jcu.22331[↩]
- Aguinagalde B, Aranda JL, Busca P, Martinez I, Royo I, Zabaleta J, et al. SECT Clinical practice guideline on the management of patients with spontaneous pneumothorax. Cir Esp. 2018;96(1):3–11. doi: 10.1016/j.ciresp.2017.11.005[↩]
- Baumann MH, Strange C, Heffner JE, Light R, Kirby TJ, Klein J, et al. Management of spontaneous pneumothorax: an American college of chest physicians Delphi consensus statement. Chest. 2001;119(2):590–602. doi: 10.1378/chest.119.2.590[↩]
- De Leyn P, Lismonde M, Ninane V, Noppen M, Slabbynck H, Van Meerhaeghe A, et al. Guidelines belgian society of pneumology guidelines on the management of spontaneous pneumothorax. Acta Chir Belg. 2005;105(3):265–267. doi: 10.1080/00015458.2005.11679714[↩]
- Collins CD, Lopez A, Mathie A, Wood V, Jackson JE, Roddie ME. Quantification of pneumothorax size on chest radiographs using interpleural distances: regression analysis based on volume measurements from helical CT. AJR Am J Roentgenol. 1995;165(5):1127–1130. doi: 10.2214/ajr.165.5.7572489[↩]





{kind=link}