Contents
Aromatase inhibitors
Aromatase inhibitors also called ‘AI drugs’ are a class of medications that work by blocking the activity of an enzyme called aromatase (also known as estrogen synthetase), the enzyme that converts androgens into estrogen to reduce levels of circulating estrogen. By blocking the activity of an enzyme aromatase, the enzyme that converts androgens into estrogen, aromatase inhibitors lower the amount of estrogen made by your body, which may stop the growth of cancer cells that need estrogen to grow. Approximately 67% to 80% of breast cancers in women are estrogen receptor positive (ER positive or ER+) 1, 2. Approximately 90% of breast cancers in men are estrogen receptor positive (ER positive) and approximately 80% are progesterone receptor positive (PR positive) 3. Aromatase inhibitors are used to treat estrogen receptor positive (ER+) breast cancer or to keep it from coming back. Aromatase inhibitors are a type of hormone therapy. There are three aromatase inhibitors approved by the United States Food and Drug Administration (FDA): anastrozole (Arimidex), exemestane (Aromasin), and letrozole (Femara). Anastrozole (Arimidex) and letrozole (Femara), both of which temporarily inactivate aromatase enzyme, and exemestane (Aromasin), permanently inactivates aromatase enzyme. All three aromatase inhibitors are now available in generic forms as well. They are used largely as adjuvant (add-on) therapy in postmenopausal women with estrogen receptor positive (ER+) breast cancer, generally given in daily oral doses for up to 5 years. All three agents are associated with a low rate of serum liver enzyme elevations during therapy and to rare instances of clinically apparent self-limited acute liver injury, most frequently with anastrozole and exemestane.
However, aromatase inhibitors are unable to prevent the ovaries from making estrogen, which means that aromatase inhibitors are only used to treat breast cancer in postmenopausal women (in women who have experienced menopause) because the ovaries in premenopausal women produce too much aromatase for aromatase inhibitors to block effectively. Moreover, aromatase inhibitors can be used in premenopausal women if they are given together with a drug that suppresses ovarian function. Because the ovaries are the main source of estrogen in premenopausal women, estrogen levels in these women can be reduced by eliminating or suppressing ovarian function. Blocking ovarian function is called ovarian ablation. Ovarian ablation can be done surgically in an operation to remove the ovaries called oophorectomy or by treatment with radiation. This type of ovarian ablation is usually permanent. Alternatively, ovarian function can be suppressed temporarily by treatment with drugs called gonadotropin-releasing hormone (GnRH) agonists, which are also known as luteinizing hormone-releasing hormone (LHRH) agonists. By mimicking gonadotropin-releasing hormone (GnRH), these medicines interfere with signals that stimulate the ovaries to produce estrogen.
The most common side effects of aromatase inhibitors are symptoms of menopause, such as hot flashes, night sweats, and vaginal dryness. Aromatase inhibitors can also cause muscle and joint pain. This side effect can be serious enough to cause some women to stop taking the drugs.
Unlike tamoxifen and raloxifene, aromatase inhibitors tend to speed up bone thinning, which can lead to osteoporosis. People with osteoporosis are more likely to have broken bones. Because of this, doctors often recommend checking bone density before starting one of these drugs.
Aromatase inhibitors may also raise your blood cholesterol level. Women with pre-existing heart disease who take an aromatase inhibitor may be at higher risk of having a heart problem.
All patients on aromatase inhibitors should have initial routine lab work, including a complete blood count, serum calcium, vitamin D levels, lipid profile, and liver function tests 4, 5. Patients should also have a baseline bone mineral density test (DEXA scan) before initiating the treatment 6, 7.
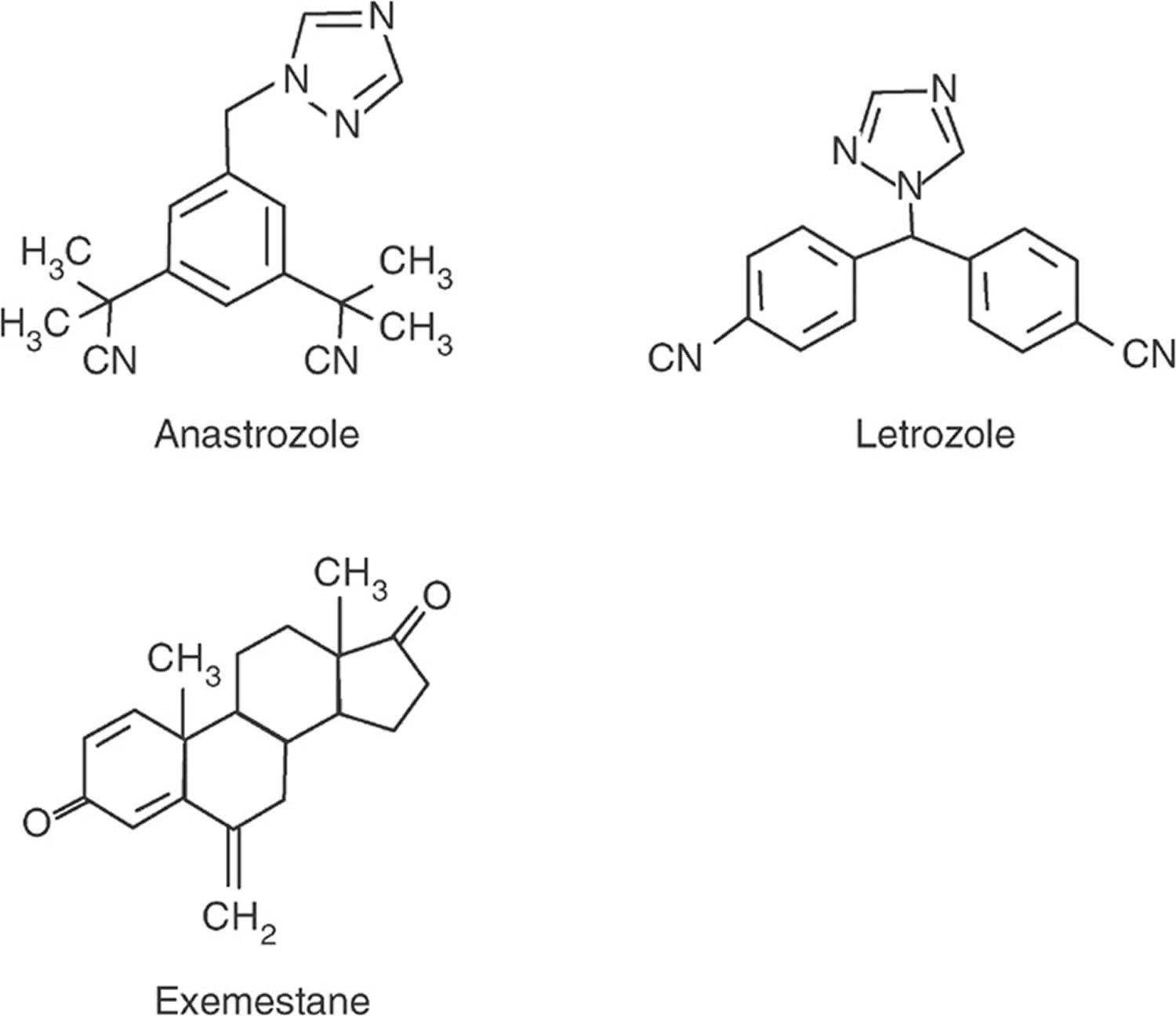
Figure 1. Aromatase inhibitors
What are hormones and hormone receptors?
Hormones are substances that function as chemical messengers in your body. Hormones affect the actions of cells and tissues at various locations in your body, often reaching their targets through the bloodstream. The hormones estrogen and progesterone are produced by the ovaries in premenopausal women and by some other tissues, including fat and skin, in both premenopausal and postmenopausal women and in men. Estrogen promotes the development and maintenance of female sex characteristics and the growth of long bones. Progesterone plays a role in the menstrual cycle and pregnancy.
Estrogen and progesterone also promote the growth of some breast cancers, which are called hormone-sensitive or hormone-dependent breast cancers. Hormone-sensitive breast cancer cells contain proteins called hormone receptors such as estrogen receptors, or ERs, and progesterone receptors, or PRs that become activated when hormones bind to them. The activated hormone receptors cause changes in the expression of specific genes, which can stimulate cell growth.
To determine whether breast cancer cells contain hormone receptors, doctors test samples of tumor tissue that have been removed by surgery. If the tumor cells contain estrogen receptors (ERs), the cancer is called estrogen receptor positive (ER positive or ER+), estrogen sensitive, or estrogen responsive. Similarly, if the tumor cells contain progesterone receptors, the cancer is called progesterone receptor positive (PR positive or PgR positive). Breast tumors that contain estrogen and/or progesterone receptors are sometimes called hormone receptor positive (HR positive). Most estrogen receptor-positive breast cancers are also PR positive.
Breast cancers that lack estrogen receptors are called ER negative, and if they lack both estrogen receptor (ER) and progesterone receptor (PR) they may be called hormone receptor negative (HR negative).
Approximately 67%–80% of breast cancers in women are estrogen receptor positive (ER positive) 1, 2. Approximately 90% of breast cancers in men are estrogen receptor positive (ER positive) and approximately 80% are progesterone receptor positive (PR positive) 3.
What is hormone therapy?
Hormone therapy also called hormonal therapy, hormone treatment, or endocrine therapy slows or stops the growth of hormone-sensitive tumors by blocking the body’s ability to produce hormones or by interfering with effects of hormones on breast cancer cells. Tumors that are hormone insensitive do not have hormone receptors and do not respond to hormone therapy.
Hormone therapy for breast cancer should not be confused with menopausal hormone therapy (MHT), which is treatment with estrogen alone or in combination with progesterone to help relieve symptoms of menopause. These two types of therapy produce opposite effects: hormone therapy for breast cancer blocks the growth of hormone receptor positive (HR positive) breast cancer, whereas menopausal hormone therapy (MHT) can stimulate the growth of HR-positive breast cancer. For this reason, when a woman taking menopausal hormone therapy (MHT) is diagnosed with HR-positive breast cancer she is usually asked to stop that therapy.
Aromatase inhibitors mechanism of action
Aromatase inhibitors (AIs) lower estrogen levels by stopping the aromatase enzyme activity in fat tissue from converting androgens (androstenedione and testosterone) into estrogens (estrone [E1] and estradiol [E2]) with testosterone being converted into estrone (E1) and androstenedione into estradiol (E2) 9. Aromatase also known as estrogen synthetase is a member of the cytochrome P450 superfamily of monooxygenases and catalyzes the demethylation of androgens’ carbon 19, producing phenolic 18-carbon estrogens 10. Highest levels of aromatase are found in the ovary and placenta, which are the major sources of estrogen in premenopausal women 11. However, aromatase is also found in other tissues, such as liver, kidney, adrenals, brain, muscle and subcutaneous fat where it is also active in producing estrogens, although at low levels 11. These tissues are the major source of estrogen after menopause or oopherectomy. Inhibitors of aromatase were developed to block the synthesis of estrogen in the peripheral tissues and, therefore, as antiestrogen therapy of estrogen receptor positive (ER+) breast cancer in postmenopausal women.
Aromatase inhibitors (AIs) don’t stop the ovaries from making estrogen. They only lower estrogen levels in women whose ovaries aren’t making estrogen such as women who have already gone through menopause (post-menopausal women). Because of this, they are used mainly in women who have gone through menopause already.
In postmenopausal women, the conversion of androgens (androstenedione and testosterone) to estrogens (estrone [E1] and estradiol [E2]) occurs primarily in the adrenal glands, the skin, the muscle, and the adipose tissue 12. Aromatase inhibitors block this pathway and consequently suppress estrogen levels in postmenopausal women. The breast cancer cells also demonstrate aromatase activity, a likely source of local estrogen for the tumor cells. The inhibition or inactivation of aromatase suppresses serum estrogen levels, which decrease estrogen-mediated cancer cell proliferation in estrogen receptor positive (ER positive) breast cancer 6.
In premenopausal women, aromatase inhibitors induce an increase in gonadotropin secretion secondary to the reduced negative feedback of estrogen to the pituitary, resulting in ovarian stimulation. Clinicians can use aromatase inhibitors to induce ovulation in the treatment of infertility 6, 13. Aromatase activity increases in endometriosis with extrauterine endometrial tissue acting as a source of estrogens. Estrogen stimulates the synthesis of prostaglandin E2 (PGE2), which causes increased aromatase activity in the endometrium. This vicious cycle leads to the growth of ectopic endometrial tissue, which is blocked by aromatase inhibitors by inhibiting the synthesis of estrogen in extrauterine endometrial tissue 14, 15.
In men, estrogen excess shows an association with premature closure of the epiphyses (growth plates at end part of a long bone). Aromatase inhibitors decrease estrogen by inhibiting the conversion of testosterone to estrogen and have therefore been used in patients with short stature and/or constitutional delay of puberty 12. Lowering estrogen levels is associated with an increase in luteinizing hormone (LH), follicle-stimulating hormone (FSH), and testosterone. Therefore aromatase inhibitors have also been used in age related hypogonadism or partial androgen deficiency. In obese men, there is an increased conversion of androgens to estrogen in the fatty tissue, leading to increased estrogen levels. Aromatase inhibitors also decrease this conversion causing decreased estrogen and increased testosterone and FSH in men with obesity-related hypogonadotropic hypogonadism and male subfertility 16.
Current aromatase inhibitors (AIs) are considered 3rd generation aromatase inhibitors. These inhibitors include anastrozole and letrozole which are nonsteroidal, and exemestane which is a steroidal aromatase inhibitor. These agents have little or no effect on adrenal glucocorticoid or mineralocorticoid synthesis.
Can aromatase inhibitors lower the risk of breast cancer?
In large studies, both anastrozole and exemestane have been shown to lower breast cancer risk in postmenopausal women who are at increased risk 17, 18, 19, 20, 21. While these drugs are not FDA approved to lower breast cancer risk, some expert groups include them as options along with tamoxifen and raloxifene to reduce breast cancer risk in post-menopausal women at increased risk 22. For example, they might be a reasonable option for women who have an increased risk of blood clots and therefore should not take tamoxifen or raloxifene 22.
Anastrozole (Arimidex)
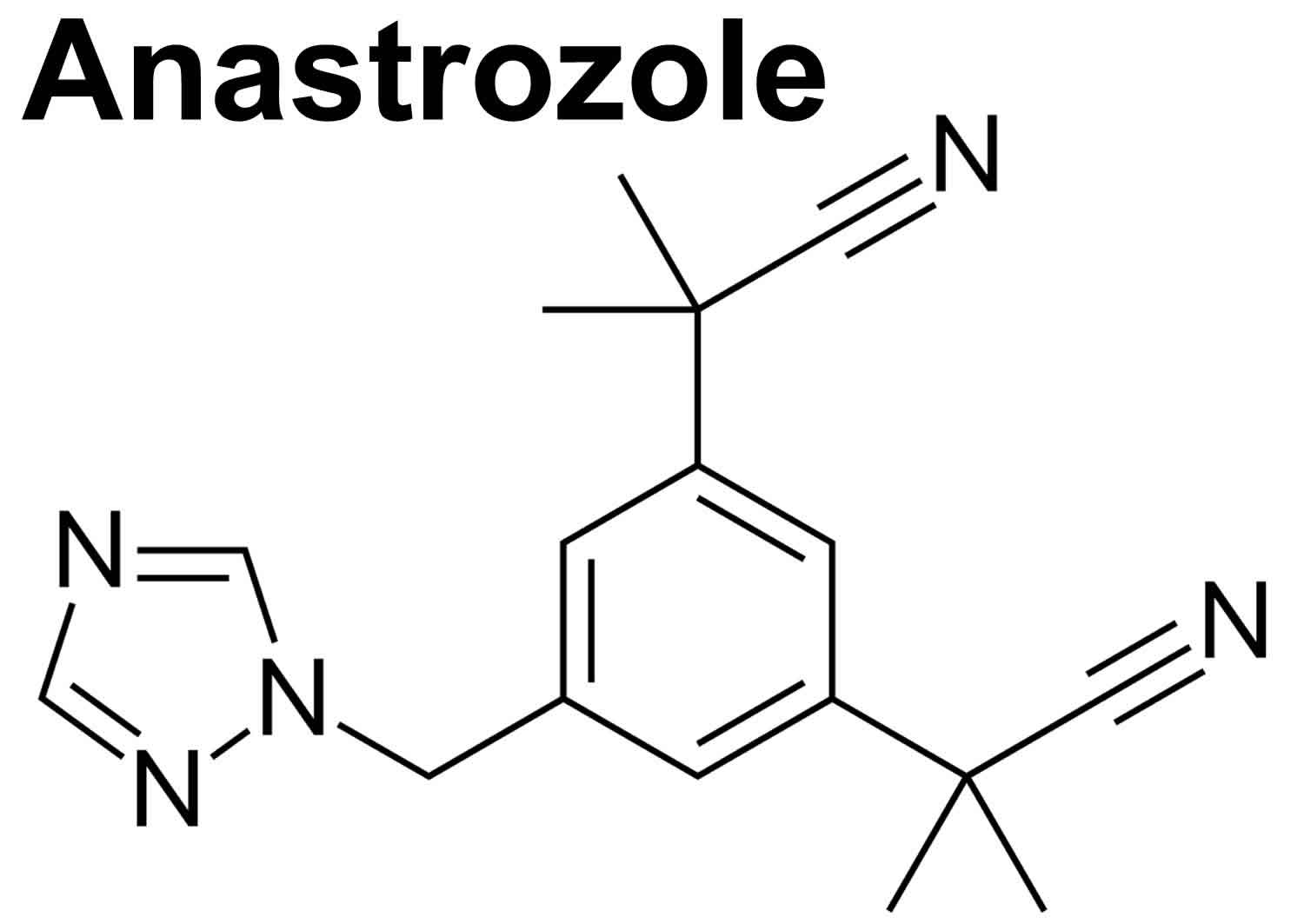
Anastrozole comes as a tablet to take by mouth. Anastrozole is typically given in single oral doses of 1 mg daily for up to five years. But you may need to take anastrozole for several years or longer. Anastrozole is usually taken once a day with or without food. Take anastrozole at around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take anastrozole exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor. Continue to take anastrozole even if you feel well. Do not stop taking anastrozole without talking to your doctor.
Common anastrozole side effects include hot flashes, night sweats, fatigue, dizziness, headache, somnolence, abdominal discomfort, nausea, arthralgias, weight gain and rash 23. Uncommon, but potentially severe side effects of anastrozole include decrease in bone mineral density, increase in serum cholesterol and increased rate of cardiovascular events.
Figure 2. Anastrozole
Exemestane (Aromasin)
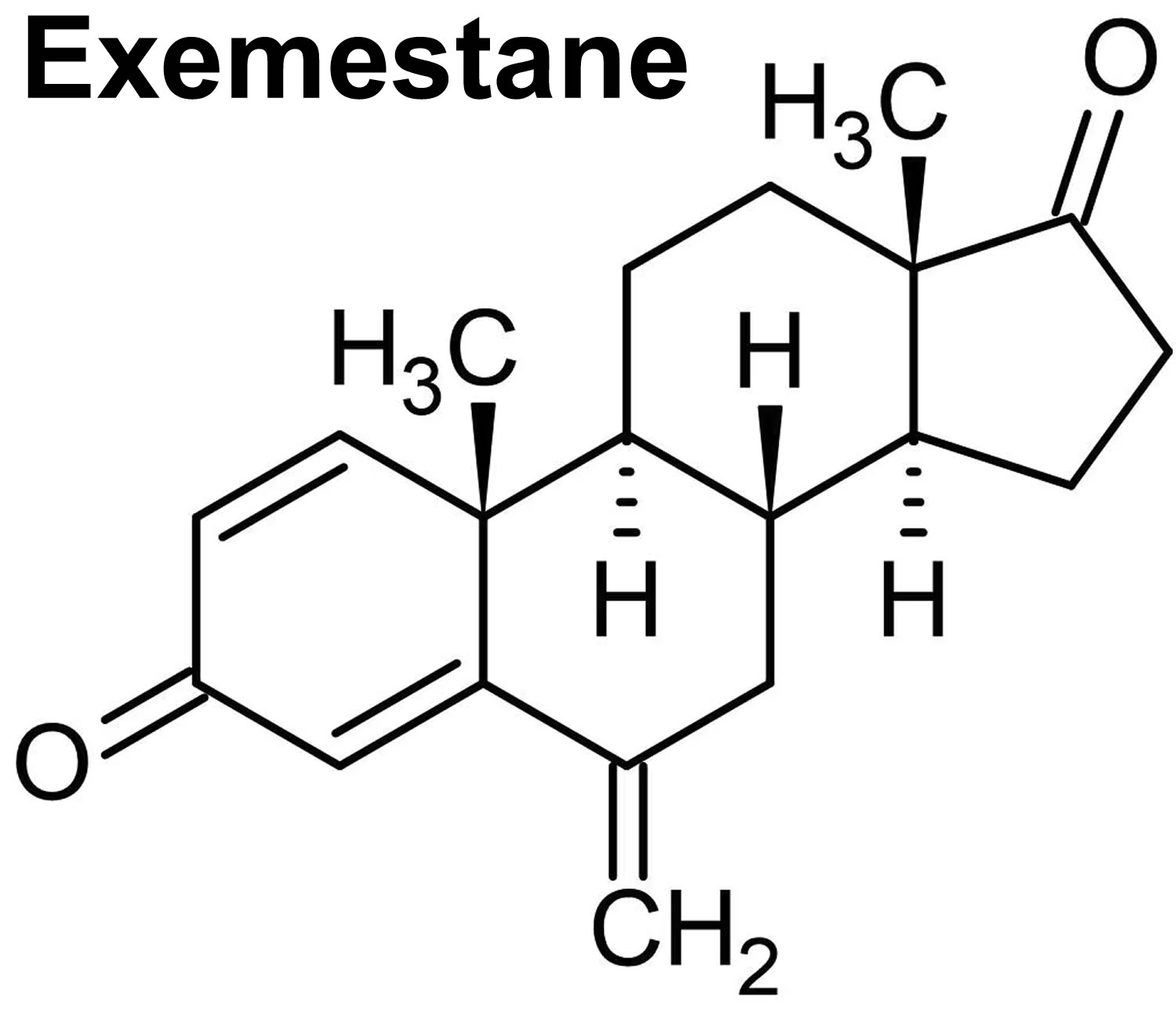
Exemestane (Aromasin) is in a class of medications called aromatase inhibitors. Exemestane (Aromasin) works by decreasing the amount of estrogen produced by the body. This can slow or stop the growth of some types of breast cancer cells that need estrogen to grow. Exemestane (Aromasin) is used as adjuvant (add-on) therapy to treat early breast cancer in women who have experienced menopause and who have already been treated with a medication called tamoxifen (Nolvadex) for 2 to 3 years. Exemestane (Aromasin) is also used to treat estrogen sensitive breast cancer in women who have experienced menopause whose breast cancer has worsened while they were taking tamoxifen.
Exemestane comes in 25 mg tablets in generic forms and under the brand name Aromasin. Exemestane is given in doses of 25 mg once daily by mouth for up to five years. Exemestane is usually taken once a day after a meal. Take exemestane at around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take exemestane exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor. Continue to take exemestane even if you feel well. Do not stop taking exemestane without talking to your doctor.
Common exemestane side effects include hot flashes, night sweats, joint pain (arthralgias), fatigue, dizziness, nervousness, insomnia, nausea, weight gain and headache 24. Uncommon, but potentially severe adverse reactions of exemestane include reduction in body mineral density and embryo-fetal toxicity 24.
Figure 3. Exemestane (Aromasin)
Letrozole (Femara)
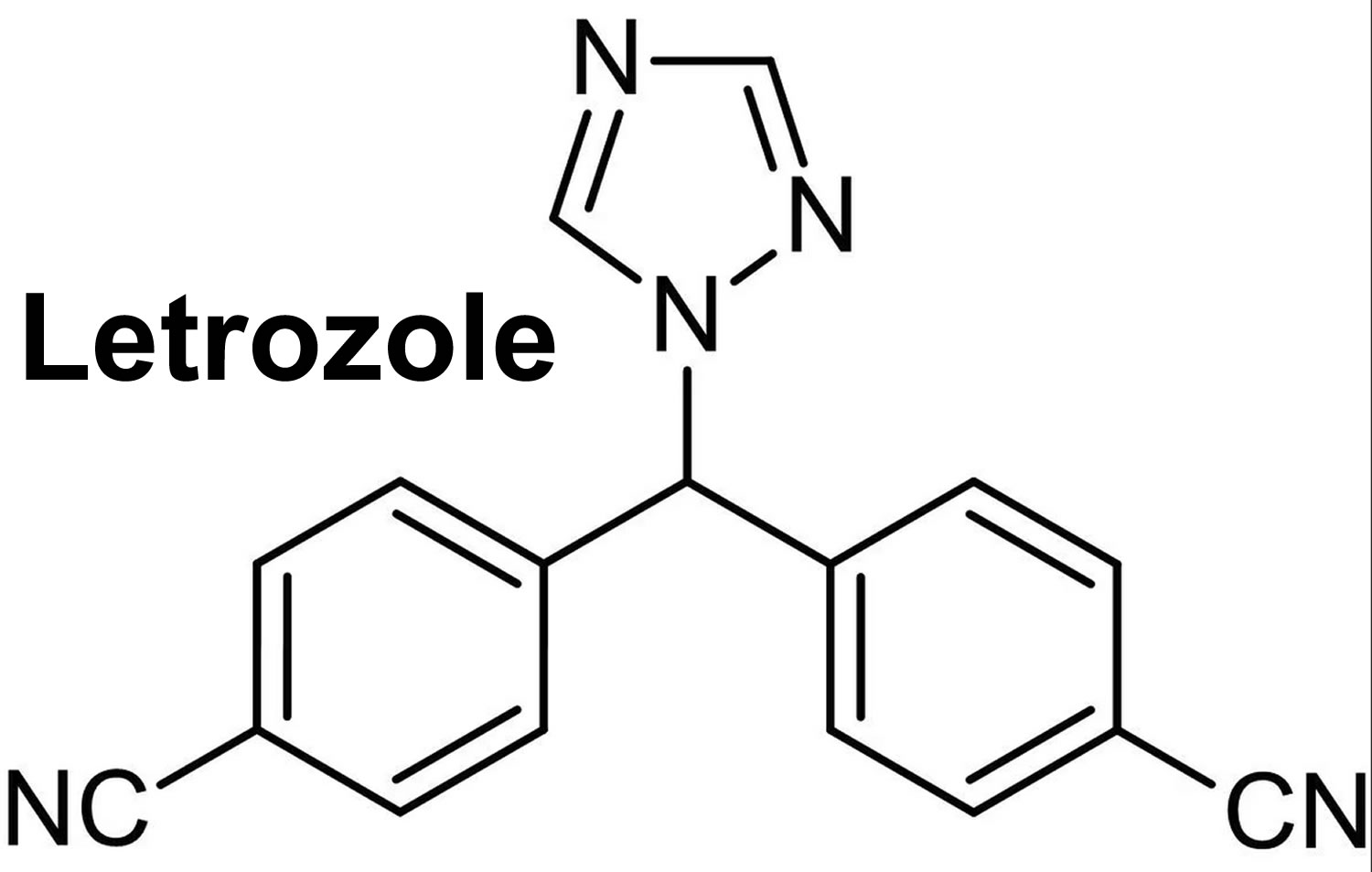
Letrozole (Femara) is in a class of medications called aromatase inhibitors. Letrozole (Femara) works by decreasing the amount of estrogen produced by the body. This can slow or stop the growth of some types of breast cancer cells that need estrogen to grow. Letrozole (Femara) is used treat early breast cancer in women who have experienced menopause and who have had other treatments, such as radiation or surgery to remove the tumor. Letrozole (Femara) is also used to treat early breast cancer in women who have experienced menopause and who have already been treated with a medication called tamoxifen (Nolvadex) for 5 years. Letrozole is also used in women who have experienced menopause as a first treatment of breast cancer that has spread within the breast or to other areas of the body or in women whose breast cancer has worsened while they were taking tamoxifen.
Letrozole was approved for use in postmenopausal women with estrogen receptor positive (ER+) breast cancer in the United States in 1997. Current indications are as adjuvant (add-on) therapy in postmenopausal women with estrogen receptor positive (ER+) breast cancer, given in daily oral doses for up to 5 years 25. Letrozole is also indicated as a first line treatment of estrogen receptor positive or unknown, locally advanced or metastatic breast cancer in postmenopausal women 25.
Letrozole is available in 2.5 mg tablets in generic forms and under the brand name Femara. The recommended dose is one tablet daily by mouth once a day with or without food. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take letrozole exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor. Continue to take letrozole even if you feel well. Do not stop taking letrozole without talking to your doctor.
Common side effects of Letrozole include hot flashes, night sweats, fatigue, dizziness, headache, somnolence, abdominal discomfort, nausea, arthralgias, weight gain and rash 25. Uncommon, but potentially severe side effects of Letrozole include decrease in bone mineral density, increases in serum cholesterol levels and embryo-fetal toxicity 25.
Figure 4. Letrozole (Femara)
Aromatase inhibitors contraindications
There are two major contraindications to aromatase inhibitors.
- Hypersensitivity: Aromatase inhibitors are contraindicated in patients with hypersensitivity reactions to aromatase inhibitor. Hypersensitivity can present as anaphylaxis, angioedema, and urticaria.
- Pregnancy and Premenopausal women: Aromatase inhibitors can harm the fetus or cause loss of pregnancy in pregnant patients 26. Due to their mechanism of action, aromatase inhibitors have no clinical benefit in breast cancer patients who are premenopausal.
Aromatase inhibitors uses
Aromatase inhibitors block estrogen synthesis and are used as therapy of estrogen receptor positive (ER+) breast cancer in postmenopausal women, usually after surgery to remove the cancer and as a first line treatment or after failure of tamoxifen (Nolvadex). Studies have shown that aromatase inhibitors are effective when used as adjuvant (add-on) therapy to chemotherapy and surgery in metastatic estrogen-dependent breast cancer. Aromatase inhibitors use in preventative and adjuvant therapies for other conditions is currently under investigation 27, 28.
Aromatase inhibitors FDA Approved Indications
- Adjuvant treatment of postmenopausal women with estrogen receptor positive (ER+) early breast cancer 29.
- First-line treatment of postmenopausal women with estrogen receptor positive (ER+) or hormone receptor unknown locally advanced or metastatic breast cancer 30.
- Second-line treatment of advanced breast cancer that has progressed on Tamoxifen therapy 31.
- Treatment of male gynecomastia 32
- Second-line treatment for the prevention of estrogen receptor positive (ER+) breast cancer in postmenopausal women 33.
Aromatase inhibitors FDA Non-approved Indications
- Treatment of benign conditions like cyclical breast pain and recurrent fibrocystic disease 32
- Treatment of symptomatic uterine fibroids (smooth, non-cancerous tumors that may develop in or around the uterus) and endometriosis as an alternative to surgical intervention 34
- Ovulation induction in the treatment of infertility 35
- Treatment of male breast cancer 36
- Treatment of prostate cancer 32
- Treatment of age related hypogonadism or partial androgen deficiency, obesity-related hypogonadotropic hypogonadism, and male subfertility 37
- Treatment of rare pediatric conditions associated with sex steroid excess 38
- Treatment of boys with short stature and constitutional delay of puberty 38
- Prevention of the initial estrogen flare effect of gonadotropin-releasing hormone (GnRH) agonist treatment 34
Aromatase inhibitors dosage
Anastrozole (Arimidex), a selective aromatase inhibitor, is available as a 1 mg tablet, which is to be taken orally once a day, with or without food. No dose adjustment is necessary for patients with kidney or liver impairment or elderly patients. The American Society of Clinical Oncology recommends the use of aromatase inhibitors as a component of adjuvant (add-on) hormonal therapy after surgery for ten years in postmenopausal patients who have a diagnosis of early-stage, node-positive, and hormone receptive breast cancer.
Letrozole (Femara) is also a selective aromatase inhibitor. It is manufactured in 2.5 mg tablets. For postmenopausal breast cancer, dosing is 2.5 mg daily. As an agent to induce ovulation, dosing is 2.5 mg to 5 mg daily for 5 days starting on day 3 of the menstrual cycle. Kidney adjustment is unnecessary if creatinine clearance is above 10. In patients with cirrhosis of the liver, CHild-Pugh Class C, increase the dosing interval to every 48 hours.
Exemestane (Aromasin), another selective aromatase inhibitor, comes in 25 mg tablets, and for postmenopausal breast cancer, dosing is 25 mg daily for 2 to 3 years. No kidney or liver dose adjustments are necessary.
Monitoring
All patients on aromatase inhibitors should have initial routine lab work, including a complete blood count, serum calcium, vitamin D levels, lipid profile, and liver function tests 4, 5. Patients should also have a baseline bone mineral density test (DEXA scan) before initiating the treatment 6, 7.
Aromatase inhibitors side effects
Various adverse reactions can happen with aromatase inhibitors. Seen in less than 1 in 10,000 patients. Some of them are as follows:
- Ulcers and blisters are the common skin side effects;
- Allergic reactions, such as swelling of the face along with lips and tongue and occasionally throat; these reactions can result in difficulty swallowing and/or breathing;
- Liver function abnormality with or without jaundice due to inflammation of the liver;
- Bone loss due to estrogen deficiency with long-term use.
Common adverse reactions (10% incidence) include the following 6, 39, 40, 41, 42:
- hot flashes,
- generalized physical weakness and/or a lack of energy and strength (asthenia),
- joint disorders such as arthritis or arthralgia,
- osteoporosis,
- fractures,
- bone pain,
- back pain,
- vaginal dryness,
- painful sexual intercourse (dyspareunia),
- sexual dysfunction,
- uterine atrophy,
- hypertension,
- hyperlipidemia,
- hypercholesterolemia,
- thromboembolic disease,
- cardiac and cerebrovascular events,
- insomnia,
- nausea.
The most common reason for discontinuing aromatase inhibitor therapy is the development of arthralgias (joint pain), known as aromatase inhibitor-associated arthralgia syndrome 43. Patients will present with joint pain (arthralgia) and mild swelling in the absence of other systemic diseases or other causes. The deficiency of estrogen causes a decrease in bone mineral density, which contributes to joint pain (arthralgia). Estrogen also shows links to the regulation of cytokine activity as well as the modulation of pain reception in the nervous system 43.
- Kohler BA, Sherman RL, Howlader N, Jemal A, Ryerson AB, Henry KA, Boscoe FP, Cronin KA, Lake A, Noone AM, Henley SJ, Eheman CR, Anderson RN, Penberthy L. Annual Report to the Nation on the Status of Cancer, 1975-2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State. J Natl Cancer Inst. 2015 Mar 30;107(6):djv048. doi: 10.1093/jnci/djv048. Erratum in: J Natl Cancer Inst. 2015 Apr 13;107(5):djv121. doi: 10.1093/jnci/djv121. Erratum in: J Natl Cancer Inst. 2015 Jun 04;107(7):djv177. doi: 10.1093/jnci/djv177[↩][↩]
- Joe BN. Clinical features, diagnosis, and staging of newly diagnosed breast cancer. In: UpToDate. Burstein HJ, Vora SR (eds.). Waltham, MA: UpToDate, 2019.[↩][↩]
- Rudlowski C. Male Breast Cancer. Breast Care (Basel). 2008;3(3):183-189. doi: 10.1159/000136825[↩][↩]
- Van Poznak C, Makris A, Clack G, Barlow DH, Eastell R. Lipid profiles within the SABRE trial of anastrozole with and without risedronate. Breast Cancer Res Treat. 2012 Aug;134(3):1141-7. doi: 10.1007/s10549-012-2147-9[↩][↩]
- Gonnelli S, Petrioli R. Aromatase inhibitors, efficacy and metabolic risk in the treatment of postmenopausal women with early breast cancer. Clin Interv Aging. 2008;3(4):647-57. doi: 10.2147/cia.s3466[↩][↩]
- Nabholtz JM. Long-term safety of aromatase inhibitors in the treatment of breast cancer. Ther Clin Risk Manag. 2008 Feb;4(1):189-204. doi: 10.2147/tcrm.s1566[↩][↩][↩][↩][↩]
- Jonat W, Howell A, Blomqvist C, Eiermann W, Winblad G, Tyrrell C, Mauriac L, Roche H, Lundgren S, Hellmund R, Azab M. A randomised trial comparing two doses of the new selective aromatase inhibitor anastrozole (Arimidex) with megestrol acetate in postmenopausal patients with advanced breast cancer. Eur J Cancer. 1996 Mar;32A(3):404-12. doi: 10.1016/0959-8049(95)00014-3[↩][↩]
- Sainsbury, R. Aromatase inhibition in the treatment of advanced breast cancer: is there a relationship between potency and clinical efficacy?. Br J Cancer 90, 1733–1739 (2004). https://doi.org/10.1038/sj.bjc.6601731[↩]
- Hong Y, Chen S. Aromatase, estrone sulfatase, and 17β-hydroxysteroid dehydrogenase: structure-function studies and inhibitor development. Mol Cell Endocrinol. 2011 Jul 4;340(2):120-6. doi: 10.1016/j.mce.2010.09.012[↩]
- Blakemore J, Naftolin F. Aromatase: Contributions to Physiology and Disease in Women and Men. Physiology (Bethesda). 2016 Jul;31(4):258-69. doi: 10.1152/physiol.00054.2015[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Aromatase Inhibitors. [Updated 2017 Jul 27]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548490[↩][↩]
- Peters A, Tadi P. Aromatase Inhibitors. [Updated 2023 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557856[↩][↩]
- Forbes JF. The use of early adjuvant aromatase inhibitor therapy: contributions from the BIG 1-98 letrozole trial. Semin Oncol. 2006 Apr;33(2 Suppl 7):S2-7. doi: 10.1053/j.seminoncol.2006.03.026[↩]
- Słopień R, Męczekalski B. Aromatase inhibitors in the treatment of endometriosis. Prz Menopauzalny. 2016 Mar;15(1):43-7. doi: 10.5114/pm.2016.58773[↩]
- Abu Hashim H. Potential role of aromatase inhibitors in the treatment of endometriosis. Int J Womens Health. 2014 Jul 21;6:671-80. doi: 10.2147/IJWH.S34684[↩]
- de Ronde W, de Jong FH. Aromatase inhibitors in men: effects and therapeutic options. Reprod Biol Endocrinol. 2011 Jun 21;9:93. doi: 10.1186/1477-7827-9-93[↩]
- Cuzick J, Sestak I, Forbes JF, Dowsett M, Knox J, Cawthorn S, Saunders C, Roche N, Mansel RE, von Minckwitz G, Bonanni B, Palva T, Howell A; IBIS-II investigators. Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled trial. Lancet. 2014 Mar 22;383(9922):1041-8. doi: 10.1016/S0140-6736(13)62292-8. Epub 2013 Dec 12. Erratum in: Lancet. 2014 Mar 22;383(9922):1040. Erratum in: Lancet. 2017 Mar 11;389(10073):1010. doi: 10.1016/S0140-6736(17)30654-2[↩]
- Goss PE, Ingle JN, Alés-Martínez JE, Cheung AM, Chlebowski RT, Wactawski-Wende J, McTiernan A, Robbins J, Johnson KC, Martin LW, Winquist E, Sarto GE, Garber JE, Fabian CJ, Pujol P, Maunsell E, Farmer P, Gelmon KA, Tu D, Richardson H; NCIC CTG MAP.3 Study Investigators. Exemestane for breast-cancer prevention in postmenopausal women. N Engl J Med. 2011 Jun 23;364(25):2381-91. doi: 10.1056/NEJMoa1103507. Epub 2011 Jun 4. Erratum in: N Engl J Med. 2011 Oct 6;365(14):1361.[↩]
- Nelson HD, Fu R, Zakher B, Pappas M, McDonagh M. Medication Use for the Risk Reduction of Primary Breast Cancer in Women: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2019 Sep 3;322(9):868-886. doi: 10.1001/jama.2019.5780[↩]
- US Preventive Services Task Force; Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, Caughey AB, Doubeni CA, Epling JW Jr, Kubik M, Landefeld CS, Mangione CM, Pbert L, Silverstein M, Tseng CW, Wong JB. Medication Use to Reduce Risk of Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2019 Sep 3;322(9):857-867. doi: 10.1001/jama.2019.11885[↩]
- Visvanathan K, Fabian CJ, Bantug E, Brewster AM, Davidson NE, DeCensi A, Floyd JD, Garber JE, Hofstatter EW, Khan SA, Katapodi MC, Pruthi S, Raab R, Runowicz CD, Somerfield MR. Use of Endocrine Therapy for Breast Cancer Risk Reduction: ASCO Clinical Practice Guideline Update. J Clin Oncol. 2019 Nov 20;37(33):3152-3165. doi: 10.1200/JCO.19.01472[↩]
- Aromatase Inhibitors for Lowering Breast Cancer Risk. https://www.cancer.org/cancer/types/breast-cancer/risk-and-prevention/aromatase-inhibitors-for-lowering-breast-cancer-risk.html[↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Anastrozole. [Updated 2017 Jul 25]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548189[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Exemestane. [Updated 2017 Jul 25]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548926[↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Letrozole. [Updated 2017 Jul 25]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548381[↩][↩][↩][↩]
- Tiboni GM, Ponzano A. Fetal safety profile of aromatase inhibitors: Animal data. Reprod Toxicol. 2016 Dec;66:84-92. doi: 10.1016/j.reprotox.2016.09.016[↩]
- Arora A, Potter JF. Aromatase inhibitors: current indications and future prospects for treatment of postmenopausal breast cancer. J Am Geriatr Soc. 2004 Apr;52(4):611-6. doi: 10.1111/j.1532-5415.2004.52171.x[↩]
- Brueggemeier RW, Hackett JC, Diaz-Cruz ES. Aromatase inhibitors in the treatment of breast cancer. Endocr Rev. 2005 May;26(3):331-45. doi: 10.1210/er.2004-0015[↩]
- Burstein HJ, Temin S, Anderson H, Buchholz TA, Davidson NE, Gelmon KE, Giordano SH, Hudis CA, Rowden D, Solky AJ, Stearns V, Winer EP, Griggs JJ. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: american society of clinical oncology clinical practice guideline focused update. J Clin Oncol. 2014 Jul 20;32(21):2255-69. doi: 10.1200/JCO.2013.54.2258[↩]
- Paridaens RJ, Dirix LY, Beex LV, Nooij M, Cameron DA, Cufer T, Piccart MJ, Bogaerts J, Therasse P. Phase III study comparing exemestane with tamoxifen as first-line hormonal treatment of metastatic breast cancer in postmenopausal women: the European Organisation for Research and Treatment of Cancer Breast Cancer Cooperative Group. J Clin Oncol. 2008 Oct 20;26(30):4883-90. doi: 10.1200/JCO.2007.14.4659[↩]
- Simpson D, Curran MP, Perry CM. Letrozole: a review of its use in postmenopausal women with breast cancer. Drugs. 2004;64(11):1213-30. doi: 10.2165/00003495-200464110-00006[↩]
- Miller WR, Jackson J. The therapeutic potential of aromatase inhibitors. Expert Opin Investig Drugs. 2003 Mar;12(3):337-51. doi: 10.1517/13543784.12.3.337[↩][↩][↩]
- Behan LA, Amir E, Casper RF. Aromatase inhibitors for prevention of breast cancer in postmenopausal women: a narrative review. Menopause. 2015 Mar;22(3):342-50. doi: 10.1097/GME.0000000000000426[↩]
- Bedaiwy MA, Mousa NA, Casper RF. Aromatase inhibitors: potential reproductive implications. J Minim Invasive Gynecol. 2009 Sep-Oct;16(5):533-9. doi: 10.1016/j.jmig.2009.05.009[↩][↩]
- Santen RJ. Inhibition of aromatase: insights from recent studies. Steroids. 2003 Sep;68(7-8):559-67. doi: 10.1016/s0039-128x(03)00096-5[↩]
- Zagouri F, Sergentanis TN, Azim HA Jr, Chrysikos D, Dimopoulos MA, Psaltopoulou T. Aromatase inhibitors in male breast cancer: a pooled analysis. Breast Cancer Res Treat. 2015 May;151(1):141-7. doi: 10.1007/s10549-015-3356-9[↩]
- Tan RB, Guay AT, Hellstrom WJ. Clinical Use of Aromatase Inhibitors in Adult Males. Sex Med Rev. 2014 Apr;2(2):79-90. doi: 10.1002/smrj.23[↩]
- Hero M. Aromatase Inhibitors in the Treatment of Short Stature. Endocr Dev. 2016;30:130-40. doi: 10.1159/000439338[↩][↩]
- Cuzick J, Sestak I, Baum M, Buzdar A, Howell A, Dowsett M, Forbes JF; ATAC/LATTE investigators. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol. 2010 Dec;11(12):1135-41. doi: 10.1016/S1470-2045(10)70257-6[↩]
- Sini V, Botticelli A, Lunardi G, Gori S, Marchetti P. Pharmacogenetics and aromatase inhibitor induced side effects in breast cancer patients. Pharmacogenomics. 2017 Jun;18(8):821-830. doi: 10.2217/pgs-2017-0006[↩]
- Foglietta J, Inno A, de Iuliis F, Sini V, Duranti S, Turazza M, Tarantini L, Gori S. Cardiotoxicity of Aromatase Inhibitors in Breast Cancer Patients. Clin Breast Cancer. 2017 Feb;17(1):11-17. doi: 10.1016/j.clbc.2016.07.003[↩]
- Krásenská M. Léčba inhibitory aromatázy u postmenopauzálních pacientek s karcinomem prsu a možnosti ovlivnění nežádoucích účinků [Treatment with Aromatase Inhibitors in Postmenopausal Women with Breast Cancer and the Possibility of Influencing Side Effects]. Klin Onkol. 2016 Fall;29 Suppl 3:S39-49. Czech. doi: 10.14735/amko20163S39[↩]
- Burstein HJ. Aromatase inhibitor-associated arthralgia syndrome. Breast. 2007 Jun;16(3):223-34. doi: 10.1016/j.breast.2007.01.011[↩][↩]





, Exemestane (Aromasin) and Letrozole (Femara). What are uses and side effects of aromatase inhibitors){kind=link}