Contents
What is Bell’s palsy
Bell’s palsy is a sudden weakness or paralysis of the facial muscles that usually affects just one side of the face. This produces a strange, lop-sided appearance of the face. The corner of the mouth droops and the eye on the affected side may not close properly. Bilateral idiopathic facial palsy occurs less frequently than unilateral involvement. About 7% of patients with history of Bell’s palsy may experience recurrence. The mean interval to first recurrence is reported at 9.8 years after the first episode 1.
Bell’s palsy is caused by inflammation or damage to the facial nerve (cranial nerve 7 or CN VII). It is usually temporary – most people recover fully. The facial nerve (cranial nerve 7 or CN VII) innervates the muscles of facial expression as well as other structures (see Figures 1 and 2).
- Bell’s palsy is NOT caused by a stroke.
- Bell’s palsy is NOT contagious.
The exact cause of Bell’s is unknown, although viral (especially herpes simplex virus), inflammatory, autoimmune, and ischemic (lack of blood supply) factors have been suggested. There is inflammation and swelling of the facial nerve where it travels through the bones of the skull. The infection inflames or puts pressure on the facial nerve that controls your facial muscles. Bell’s palsy can be mild, or it can be severe.
The incidence of Bell’s palsy is 20-30 cases for 100,000 2 and accounts for 60-70% of all cases of unilateral peripheral facial palsy 3. Either sex is affected equally and may occur at any age, the median age is 40 years. Left and right sides are affected equally 4.
Bell’s palsy appears to occur worldwide, equally in all races and both genders. However, an increased risk in the third trimester of pregnancy and the first week after delivery has been noted. The incidence is lowest under 10 years of age. There are peaks of incidence in the 30 to 50 and 60 to 70 year old age groups with highest in people over the age of 70 5
- Bell’s palsy can occur at any age, but risk increases with age. It is also more common in pregnant women and people with diabetes.
- Bell’s palsy is rare in children.
Bell’s palsy usually gets better on its own, but this can take several weeks. Most people recover without treatment in 3 to 9 months. Sometimes it can take up to a year for recovery. Unfortunately, 20-30 per cent of people are left with residual weakness which may be cosmetically apparent. Older people and those with a more complete paralysis have less chance of full recovery.
The Copenhagen Facial Nerve Study found that around 71% of patients recover normal function without treatment. Around 13% are left with slight weakness and around 4% with severe weakness resulting in major facial dysfunction. Contracture of the facial muscles on the affected side was found in 17% and associated movements were found in 16% 6. Scoring systems such as the House–Brackmann scale used in randomized controlled trials and systematic reviews may be helpful to monitor progress 7.
Symptoms of Bell’s palsy may come on very suddenly over a few hours and include:
- Weakness or paralysis on one side of the face;
- Drooping at the corner of the mouth;
- Drooling;
- Difficulty eating, with food escaping your mouth;
- Being unable to smile with that side of your face;
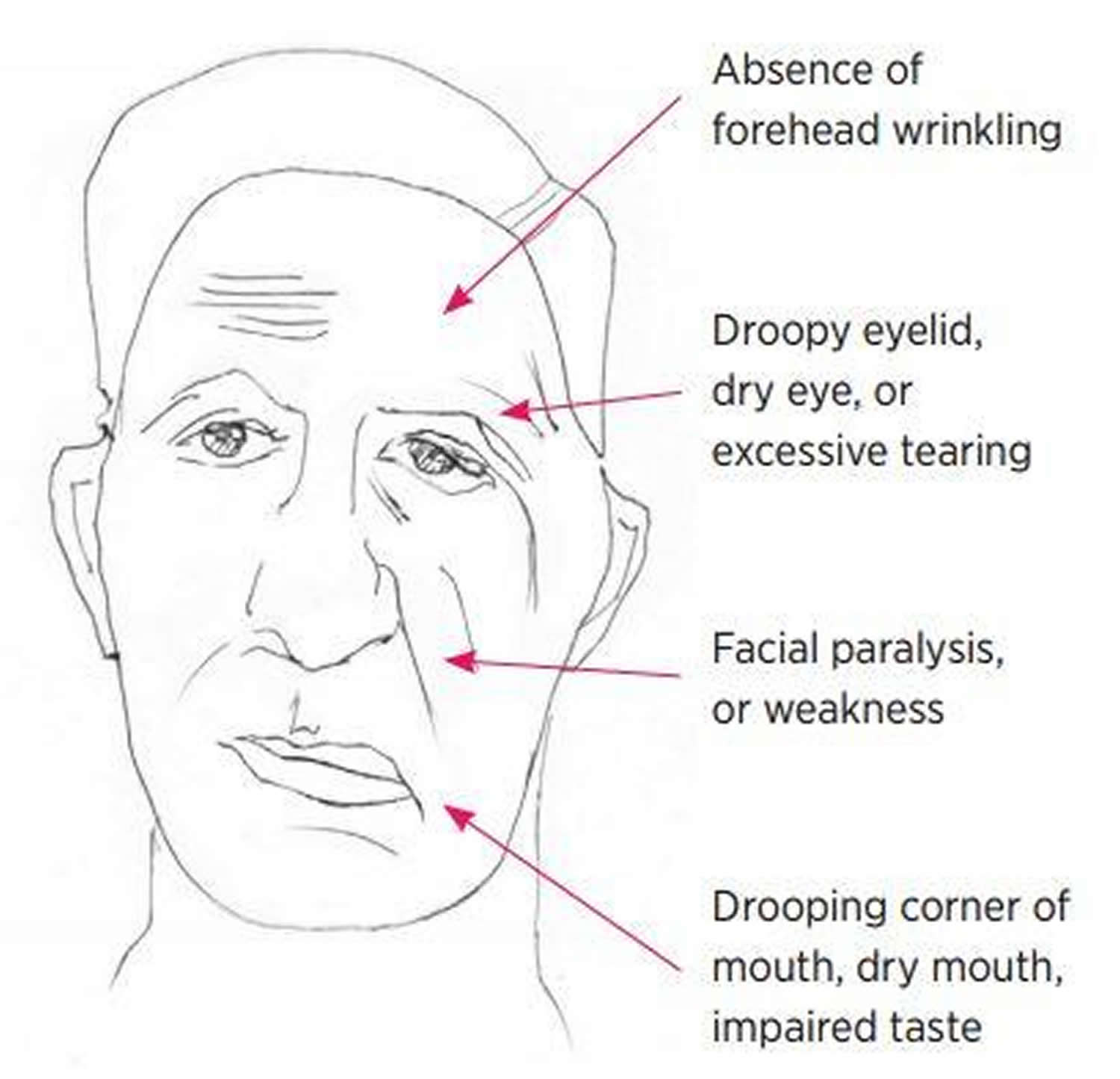
- Not being able to wrinkle your forehead (this can help distinguish Bell’s palsy from a stroke – because in a stroke the forehead muscles are not affected);
- Not being able to close one eye. It may become dry or watery;
- Difficulty with some words; and
- Pain behind the ear or around the jaw.
Corticosteroids, when started within 72 hours of the onset of weakness, may improve the chances of full recovery. There may be a slight added benefit from also taking an antiviral medicine at the same time as the steroid. If your eye doesn’t close properly, the eye needs to be protected from drying out and injury with eye ointment and patches.
- Always seek immediate medical help if you have symptoms of paralysis, as you may be having a stroke.
- If your face droops on one side (the mouth or eye may have drooped)
- If you can’t lift up both arms and keep them there
- If you have difficulty speaking (speech may be slurred or garbled)
These can be signs of a more serious condition, like a stroke. Unlike Bell’s palsy, the symptoms of a stroke usually come on suddenly.
See your doctor if you experience facial weakness or drooping to determine the underlying cause and severity of the illness.
Bell’s palsy vs Stroke
A stroke is a serious life-threatening medical condition that occurs when the blood supply to part of the brain is cut off.
- A stroke is a medical emergency and urgent treatment is essential.
- The sooner a person receives treatment for a stroke, the less damage is likely to happen.
Strokes happen when blood flow to your brain stops. Within minutes, brain cells begin to die. There are two kinds of stroke. The more common kind, called ischemic stroke, is caused by a blood clot that blocks or plugs a blood vessel in the brain. The other kind, called hemorrhagic stroke, is caused by a blood vessel that breaks and bleeds into the brain. “Mini-strokes” or transient ischemic attacks (TIAs), occur when the blood supply to the brain is briefly interrupted.
The main symptoms of stroke can be remembered with the word F.A.S.T.:
- Face – the face may have dropped on one side, the person may not be able to smile, or their mouth or eye may have dropped.
- Arms – the person with suspected stroke may not be able to lift both arms and keep them there because of weakness or numbness in one arm.
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake.
- Time – it’s time to dial your local emergency number for an ambulance immediately if you see any of these signs or symptoms.
If you have any of these symptoms, you must get to a hospital quickly to begin treatment. Acute stroke therapies try to stop a stroke while it is happening by quickly dissolving the blood clot or by stopping the bleeding.
The Facial Nerve
The facial nerve is a mixed nerve — it is the main somatic motor nerve to the facial muscles; parasympathetic innervation to glands; special sensory taste from the tongue.
Sir Charles Bell described the anatomy and physiology of the facial nerve in the 1800s. The facial nerve is a mixed nerve, containing:
- Motor output fibers to the facial muscles (which control movement of muscles of the face);
- Parasympathetic fibers to the lacrimal, submandibular, and sublingual salivary glands (which control tearing and salivation);
- Afferent fibers for taste from the anterior two thirds of the tongue (which control taste of the front part of the tongue);
- Somatic afferents from the external auditory canal and pinna (which control the outer ear).
These functions may be affected in Bell’s palsy.
Figure 1. Facial nerve (Cranial nerve 7)
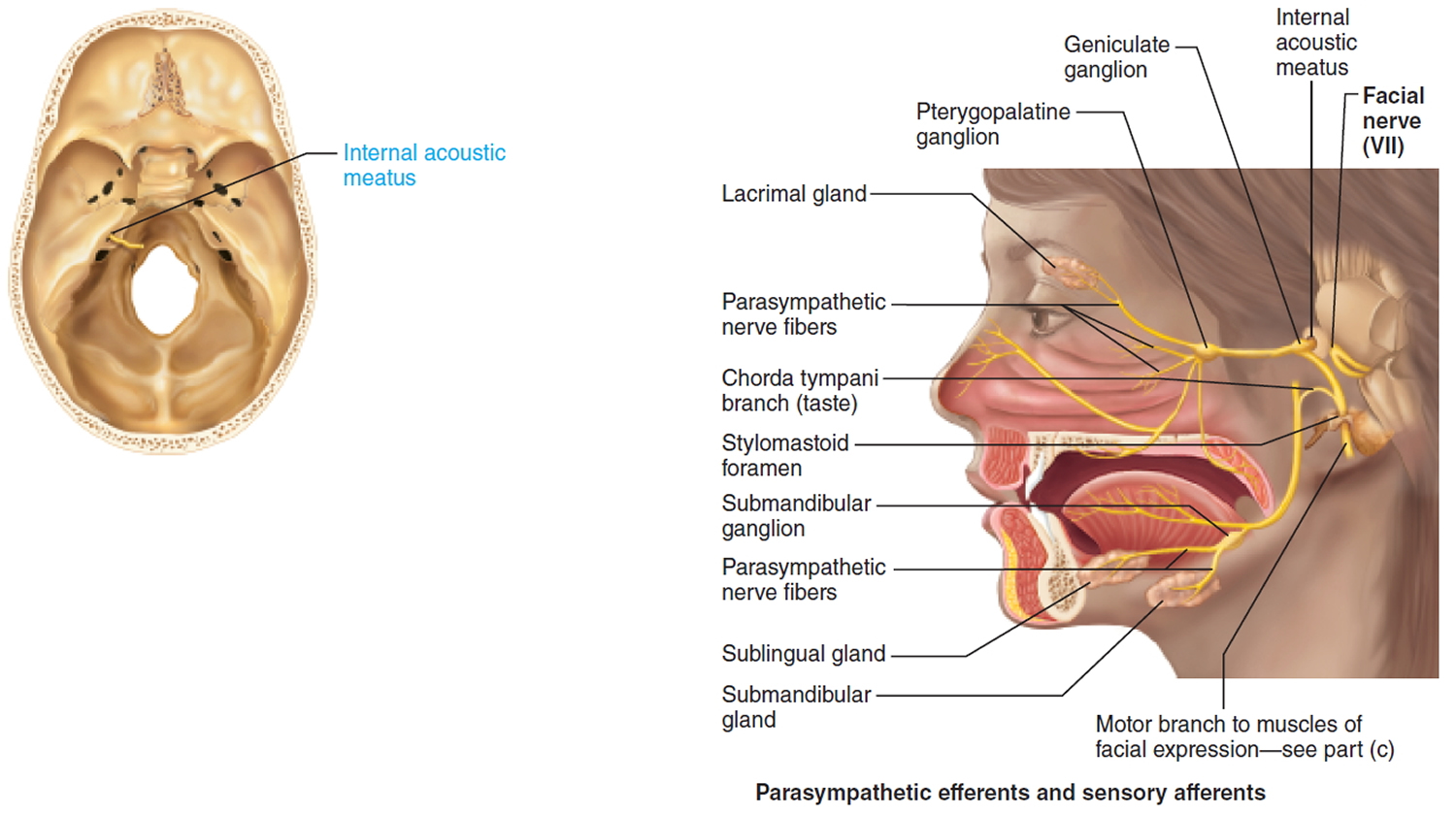 Figure 2. Facial nerve (Cranial nerve 7) – 5 branches
Figure 2. Facial nerve (Cranial nerve 7) – 5 branches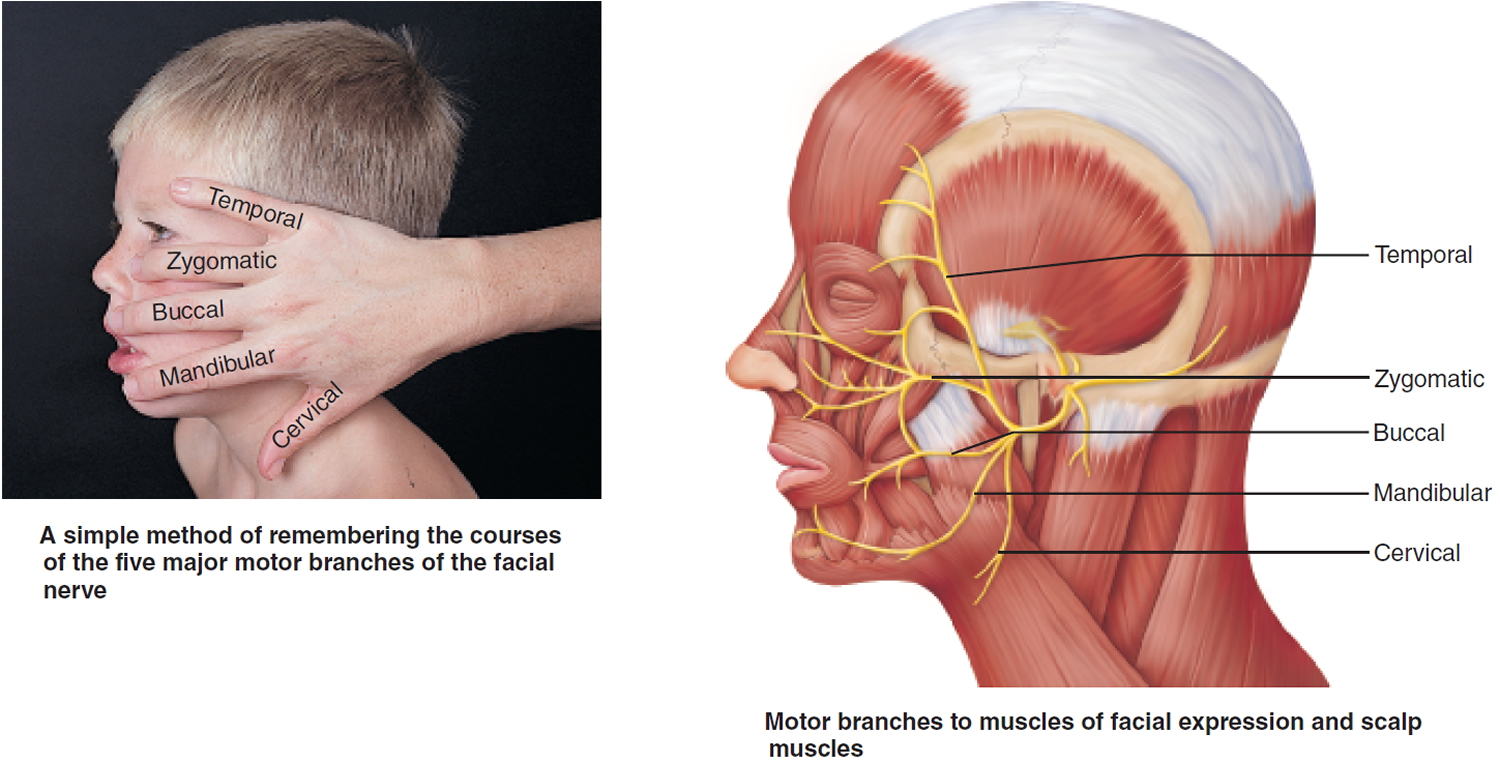 Bell’s palsy recovery
Bell’s palsy recovery
Bell’s palsy will usually begin to improve by itself within days to weeks after onset. Approximately 80-90% of cases will recover completely although this may take 6-12 months. Most people begin improving within two weeks and recover within 3 to 9 months.
According to Peitersen 8, complete recovery was observed in 71% of all patients. Ninety-four per cent of patients with incomplete and 61% with complete paralysis made a complete recovery, but it is unknown if intervention with physical therapies improves outcome.
A few people don’t recover fully and are left with some weakness or paralysis of the muscles in their face. About 23% of people with Bell’s palsy are left with either moderate to severe symptoms, such as hemifacial spasm, partial motor recovery, crocodile tears (tears upon salivation), contracture or synkinesis (involuntary twitching of the face or blinking).
Recurrence occurs in about 8-10% of patients, either on the same side or opposite side of the face 9. If this happens, alternative causes should be excluded such as diabetes, tumors or infection.
You can help your recovery by:
- use prescribed eye drops and ointment regularly
- wear glasses or goggles during the day
- use an eye patch or tape your eye shut if recommended
If the pain is bothering you, place a warm, damp washcloth over your face several times a day and take over-the-counter pain medication.
Bell’s Palsy Prognosis (Outlook)
The outcome of Bell’s palsy varies. 80-90% of patients will make a gradual recovery although this may take up to 12 months to be complete. A small number of cases result in a permanent facial weakness.
The prognosis depends to a great extent on the time at which recovery begins. Early commencement of recovery is associated with a good prognosis and late recovery a bad prognosis. If recovery begins within one week, 88% obtain full recovery, within one to two weeks 83% and within two to three weeks 61%. Normal taste, stapedius reflex and tearing are also associated with a significantly better prognosis than if these functions are impaired. Recovery is less likely to be satisfactory with complete rather than incomplete paralysis, with pain behind the ear and in older people 10. Other poor prognostic factors include hypertension and diabetes mellitus 8.
Bell’s palsy complications
A mild case of Bell’s palsy normally disappears within a month, but recovery from a more severe case involving total paralysis varies. Complications may include:
- Irreversible damage to your facial nerve
- Misdirected regrowth of nerve fibers, resulting in involuntary contraction of certain muscles when you’re trying to move others (synkinesis) — for example, when you smile, the eye on the affected side may close
- Partial or complete blindness of the eye that won’t close due to excessive dryness and scratching of the cornea, the clear protective covering of the eye
Bell’s palsy causes
Bell’s palsy is due to a problem with the nerve supplying the face — the facial nerve. On its way from the brain to the muscles of the face the facial nerve passes through a tiny hole in the skull. Swelling of the nerve due to inflammation can cause it to get trapped in this hole, causing paralysis of the muscles it supplies. Why this should happen is uncertain but it may be due to a virus infection. Several viral infections have been linked to Bell’s palsy, including cold sore infections, chickenpox and shingles, Epstein-Barr virus, mumps, and hand, foot and mouth disease.
Although the exact reason Bell’s palsy occurs isn’t clear, it’s often linked to exposure to a viral infection. Viruses that have been linked to Bell’s palsy include the virus that causes:
- Cold sores and genital herpes (herpes simplex)
- Chickenpox and shingles (herpes zoster)
- Mononucleosis (Epstein-Barr)
- Cytomegalovirus infections
- Respiratory illnesses (adenovirus)
- German measles (rubella)
- Mumps (mumps virus)
- Flu (influenza B)
- Hand-foot-and-mouth disease (coxsackievirus)
The underlying pathophysiology observed in post mortem cases of Bell’s palsy is vascular distension, inflammation and oedema with ischaemia of the facial nerve. The cause remains unclear. However, reactivation of herpes simplex virus or herpes zoster virus from the geniculate ganglion is suspected to be the most likely cause 11, 12. How the virus damages the facial nerve is uncertain 5. Despite advances in neuroimaging, the diagnosis of Bell’s palsy is mainly clinical 13.
Risk Factors for Bells Palsy (Idiopathic Facial Paralysis)
Bell’s palsy occurs more often in people who:
- Are pregnant, especially during the third trimester, or who are in the first week after giving birth
- Have an upper respiratory infection, such as the flu or a cold
- Have diabetes
Also, some people who have recurrent attacks of Bell’s palsy, which are rare, have a family history of recurrent attacks. In those cases, there may be a genetic predisposition to Bell’s palsy.
Bell’s palsy symptoms
The main symptom is weakness or paralysis of one side of the face. It usually is at its worst within 2 to 3 days of starting. It can also cause:
- Pain: Behind or in front of ear. May precede weakness of facial muscles by 1-2 days
- Drooping eyelid or difficulty closing one eye
- Difficulty smiling and making facial expressions
- Drooping of one side of the mouth
- Difficulty eating and drinking
- Drooling
- Pain or sensitivity around the affected area
- Headache
- Loss of taste
- Sensitivity to sound (hyperacusis) on the affected side
- Changes in the amount of tears or saliva
- Blurred vision
- Tingling or numbness of the cheek/mouth
If you develop these symptoms, see your doctor immediately or go to your nearest emergency department.
Figure 3. Bell’s palsy (possible) signs and symptoms
Bell’s palsy diagnosis
There is no specific test for Bell’s palsy, but it is important to make sure you don’t have a more serious condition like a stroke or a tumor.
Your doctor will diagnose the condition by examining you carefully. You may be referred to a specialist or have tests such as X-rays or CT scans to rule out other causes.
Definable causes of facial paralysis must be ruled out by a thorough examination of the ears, nose, throat, and cranial nerves
Examination findings can include:
- Change in facial appearance:
- Facial droop, sagging of eyebrow;
- Difficulty with facial expressions, grimacing;
- Facial paralysis of one side of the face
- Difficulty closing one eye;
- Difficulty with fine facial movements;
- Drawing of mouth to the non-affected side;
- Drooling due to inability to control facial muscles;
- Difficulty with eating and drinking
- Dry eye secondary to being unable to close eye properly because of facial weakness.
Tests which may be done include:
- Tests for viruses which might be the causative organism;
- Spinal fluid analysis;
- MRI scans of the head;
- Hearing tests to assess the status of the hearing (auditory) nerve which travels with the facial nerve.
Electromyography (EMG)
During this test, the nerve is stimulated by an electrical current applied to the skin overlying the nerve. Function is graded by the amount of current required to cause excitation of the nerve and contraction of the facial muscles. This test is often repeated several times to determine extent of injury and progression of the disease. For example, if testing indicates equal muscle response on both sides of the face, the patient can be expected to have complete return of facial function in 3-6 weeks without significant deformity.
Bell’s palsy treatment
In many cases, no treatment is necessary – 3 out of 4 people recover, with or without treatment. The goal of any treatment given in Bell’s plasy is to relieve the symptoms. However, your doctor may prescribe oral steroids, or an antiviral medicine in the first few days of the onset of Bell’s palsy, as this can improve the chances of full recovery.
Corticosteroids, when started within 72 hours of the onset of weakness (preferably within 24 hours of the onset of paralysis), may improve the chances of full recovery. Corticosteroids or antiviral medications may reduce swelling and relieve pressure on the facial nerve. There may be a slight added benefit from also taking an antiviral medicine at the same time as the steroid. The definite efficacy and benefit of these drugs are still under research.
If your eye doesn’t close properly, the eye needs to be protected from drying out and injury with eye ointment and patches. Your doctor may also prescribe lubricating eye drops and an eye ointment to protect the affected eye and recommend physiotherapy or face massage.
Surgical procedures to decompress the facial nerve have not been shown to routinely benefit people with Bell’s palsy.
Drug therapy
The treatments considered for Bell’s palsy include oral corticosteroids (prednisolone) and antiviral drugs. Although the cause of Bell’s palsy is uncertain, it is known that inflammation and edema of the facial nerve are responsible for the symptoms. Corticosteroids have therefore been used for their anti-inflammatory effect.
Corticosteroids
The maximum benefit is seen when steroids are commenced within 72 hours of the onset of symptoms. There is no optimum regimen, but in adults 50–60 mg prednisolone daily for 10 days has been commonly used 7. Prednisolone has been used at a dose of 1 mg/kg/day up to a maximum of 80 mg in some studies. Doses of more than 120 mg/day have been used safely in patients with diabetes 14.
In a randomized controlled trial the recovery rate at nine months with prednisolone was 94%. It was 81.6% in patients who did not receive prednisolone 7.
A systematic review of trials that used prednisolone showed that at six months 17% of patients had incomplete recovery compared with 28% of patients who received no treatment. There was also a significant reduction in motor synkinesis in those who received prednisolone. There was no significant reduction in cosmetically disabling sequelae 15.
Antiviral drugs
The antiviral drugs used in trials were aciclovir (400 mg five times daily for five days) or valaciclovir (1000 mg/day for five days) 16. There is currently no evidence to support the use of either antiviral drug on its own 17 and there is uncertainty regarding the benefit of adding them to corticosteroids.
Combination therapy
A randomised controlled trial found that at nine months of diagnosis, facial function had recovered in 94.4% of patients who took prednisolone alone, 85.4% of those who took aciclovir alone and 92.7% of those who received both. There were no serious adverse effects in any group. The study concluded that early treatment with prednisolone alone increases the likelihood of complete recovery and there was no additional benefit of treatment with aciclovir alone or combining with prednisolone.7 However, a systematic review also found that treatment with prednisolone reduced the chances of incomplete recovery but using an antiviral drug had an additional benefit 18.
There have been several studies looking at the benefit of antiviral drugs with or without prednisolone. A randomised prospective study found that a combination of an antiviral and a steroid was more effective in treating severe to complete Bell’s palsy than steroid alone 19. A guideline development group found that there was low-quality evidence of benefit from adding antivirals. Patients who are offered them in addition to corticosteroids should be counselled that the increase in recovery is less than 7% 20.
A Cochrane review in 2015 17 found that antivirals combined with corticosteroids improved rates of incomplete recovery compared with corticosteroids alone, but this was not significant and the evidence was low quality. There was moderate-quality evidence that the combination reduced long-term sequelae such as excessive tear production and synkinesis. The outcome for patients who received corticosteroids alone was significantly better than for those who received antivirals alone. Antiviral drugs alone had no benefit over placebo. None of the treatments had significant differences in adverse effects, but the evidence was again of low quality.
The optimum management of children with Bell’s palsy is also unknown. A major trial (BellPIC) in Australia is addressing this question 21.
Adverse effects of treatment
Treatment courses are short, but can cause adverse effects.
Prednisolone should be used with caution in immunosuppression and sepsis. It may lead to:
- induction or worsening of peptic ulcer disease
- hyperglycemia especially in diabetics, however higher doses may be required in diabetes
- malignant hypertension
- hepatic and renal dysfunction.
Antiviral drugs may cause:
- nausea and vomiting
- abdominal pain
- diarrhea
- neurological reactions – dizziness, convulsions (more common with higher doses)
- very rarely, hepatitis and jaundice.
Bell’s palsy exercises
Paralyzed muscles can shrink and shorten, causing permanent contractures. A physical therapist can teach you how to massage and exercise your facial muscles to help prevent this from occurring.
Physical therapies including tailored facial exercises, acupuncture to affected muscles, massage, thermotherapy and electrical stimulation have been used to hasten recovery. However, there is no evidence for any significant benefit. A Cochrane review 22 concluded from poor-quality evidence that tailored facial exercises can help improve facial function, mainly for moderate paralysis and chronic cases. Early facial exercise may reduce recovery time, long-term paralysis and number of chronic cases.
Surgery
Surgical treatment to free the facial nerve has been considered. However the evidence for this procedure is of very low quality 23.
Today, decompression surgery isn’t recommended. Facial nerve injury and permanent hearing loss are possible risks associated with this surgery.
In rare cases, plastic surgery may be needed to correct lasting facial nerve problems.
Lifestyle and home remedies
Home treatment may include:
- Protecting the eye you can’t close. Using lubricating eyedrops during the day and an eye ointment at night will help keep your eye moist. Wearing glasses or goggles during the day and an eye patch at night can protect your eye from getting poked or scratched.
- Taking over-the-counter pain relievers. Aspirin, ibuprofen (Advil, Motrin IB, others) or acetaminophen (Tylenol, others) may help ease your pain.
- Applying moist heat. Putting a washcloth soaked in warm water on your face several times a day may help relieve pain.
- Doing your physical therapy exercises. Massaging and exercising your face according to your physical therapist’s advice may help relax your facial muscles.
Alternative medicine
Although there’s little scientific evidence to support the use of alternative medicine for people with Bell’s palsy, some people with the condition may benefit from the following:
- Relaxation techniques. Relaxing by using techniques such as meditation and yoga may relieve muscle tension and chronic pain.
- Acupuncture. Placing thin needles into a specific point in your skin helps stimulate nerves and muscles, which may offer some relief.
- Biofeedback training. By teaching you to use your thoughts to control your body, you may help gain better control over your facial muscles.
- Vitamin therapy. Vitamins B-12, B-6 and zinc may help nerve growth.
- Murthy JMK, Saxena AB. Bell’s palsy: Treatment guidelines. Annals of Indian Academy of Neurology. 2011;14(Suppl1):S70-S72. doi:10.4103/0972-2327.83092. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3152161/[↩]
- Hauser WA, Karnes WE, Annis J, Kurland LT. Incidence and prognosis of Bell’s palsy in the population of Rochester, Minnesota. Mayo Clin Proc. 1971;46:258–64. https://www.ncbi.nlm.nih.gov/pubmed/5573820[↩]
- Adour KK, Byl FM, Hilsinger RL, Jr, Kahn ZM, Sheldon MI. The true nature of Bell’s palsy: Analysis of 1,000 consecutive patients. Laryngoscope. 1978;88:787–801. https://www.ncbi.nlm.nih.gov/pubmed/642672[↩]
- Katusic SK, Beard CM, Wiederholt WC, Bergstralh EJ, Kurland LT. Incidence, clinical features, and prognosis in Bell’s palsy, Rochester, Minnesota 1968-1982. Ann Neurol. 1986;20:622–7. https://www.ncbi.nlm.nih.gov/pubmed/3789675[↩]
- Gilden DH. Clinical Practice. Bell’s palsy. The New England Journal of Medicine 2004;351(13):1323-31. http://www.nejm.org/doi/full/10.1056/NEJMcp041120[↩][↩]
- Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl 2002;549:4-30.[↩]
- Sullivan FM, Swan IR, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med 2007;357:1598-607. http://www.nejm.org/doi/full/10.1056/NEJMoa072006[↩][↩][↩]
- Peitersen E. Bell’s Palsy: the spontaneous course of 2500 peripheral facial nerve palsies of different etiologies. Acta Oto-Laryngologica. Supplementum 2002;549:4-30. https://www.ncbi.nlm.nih.gov/pubmed/12482166[↩][↩]
- Valença MM, Valença LP, Lima MC. Idiopathic facial paralysis (Bell’s palsy): a study of 180 patients [Paralisia facial periférica idiopática de Bell]. Arquivos de Neuro-Psiquiatria 2001;59(3-B):733-9. https://www.ncbi.nlm.nih.gov/pubmed/11593275[↩]
- Danielidis V, Skevas A, Van Cauwenberge P, Vinck B. A comparative study of age and degree of facial nerve recovery in patients with Bell’s palsy. European Archives of Otorhinolaryngology 1999;256(10):520-2. https://www.ncbi.nlm.nih.gov/pubmed/10638361[↩]
- Holland NJ, Weiner GM. Recent developments in Bell’s palsy. BMJ 2004;329(7465):553-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC516110/[↩]
- Linder T, Bossart W, Bodmer D. Bell’s palsy and Herpes simplex virus: fact or mystery? Otol Neurotol 2005;26:109-13.[↩]
- Seok JI, Lee DK, Kim KJ. The usefulness of clinical findings in localising lesions in Bell’s palsy: comparison with MRI. J Neurol Neurosurg Psychiatry 2008;79:418-20. http://jnnp.bmj.com/content/79/4/418[↩]
- Saito O, Aoyagi M, Tojima H, Koike Y. Diagnosis and treatment for Bell’s palsy associated with diabetes mellitus. Acta Otolaryngol Suppl 1994;511:153-5. https://www.ncbi.nlm.nih.gov/pubmed/7515552[↩]
- Madhok VB, Gagyor I, Daly F, Somasundara D, Sullivan M, Gammie F, Sullivan F. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews 2016, Issue 7. Art. No.: CD001942. DOI: 10.1002/14651858.CD001942.pub5. http://onlinelibrary.wiley.com/enhanced/exportCitation/doi/10.1002/14651858.CD001942.pub5[↩]
- Hato N, Yamada H, Kohno H, Matsumoto S, Honda N, Gyo K, et al. Valacyclovir and prednisolone treatment for Bell’s palsy: a multicentre, randomized, placebo-controlled study. Otol Neurotol 2007;28:408-13.[↩]
- Gagyor I, Madhok VB, Daly F, Somasundara D, Sullivan M, Gammie F, Sullivan F. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews 2015, Issue 11. Art. No.: CD001869. DOI: 10.1002/14651858.CD001869.pub8. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001869.pub8/full[↩][↩]
- de Almeida JR, Al Khabori M, Guyatt GH, Witterick IJ, Lin VY, Nedzelski JM, et al. Combined corticosteroid and antiviral treatment for Bell palsy: a systematic review and meta-analysis. JAMA 2009;302:985-93. https://jamanetwork.com/journals/jama/fullarticle/184482[↩]
- Lee HY, Byun JY, Park MS, Yeo SG. Steroid-antiviral treatment improves the recovery rate in patients with severe Bell’s palsy. Am J Med 2013;126:336-41. http://www.amjmed.com/article/S0002-9343(12)00907-2/fulltext[↩]
- Gronseth GS, Paduga R; American Academy of Neurology. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2012;79:2209-13. http://n.neurology.org/content/79/22/2209[↩]
- https://researchdata.ands.org.au/bells-palsy-children-bellpic/518554[↩]
- Teixeira LJ, Valbuza JS, Prado GF. Physical therapy for Bell’s palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews 2011, Issue 12. Art. No.: CD006283. DOI: 10.1002/14651858.CD006283.pub3. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006283.pub3/full[↩]
- de Almeida JR, Guyatt GH, Sud S, Dorion J, Hill MD, Kolber MR, et al.; Bell Palsy Working Group, Canadian Society of Otolaryngology – Head and Neck Surgery and Canadian Neurological Sciences Federation. Management of Bell palsy: clinical practice guideline. CMAJ 2014;186:917-22. http://www.cmaj.ca/content/186/12/917[↩]





{kind=link}