
Contents
Broken arm
A broken or fractured arm or upper arm needs to be treated as soon as possible. It typically takes 6 weeks or 8 weeks to heal. And forearm bones typically take 3 to 6 months to fully heal. The more severe your injury, however, the longer your recovery may be.
When the bone breaks there is bleeding from the ends as bone has a very good blood supply. The blood forms clots in between the two ends of the bone and is used by the body to start to build new bone.
In order for a fracture to heal, the bones must be held in the correct position and protected.
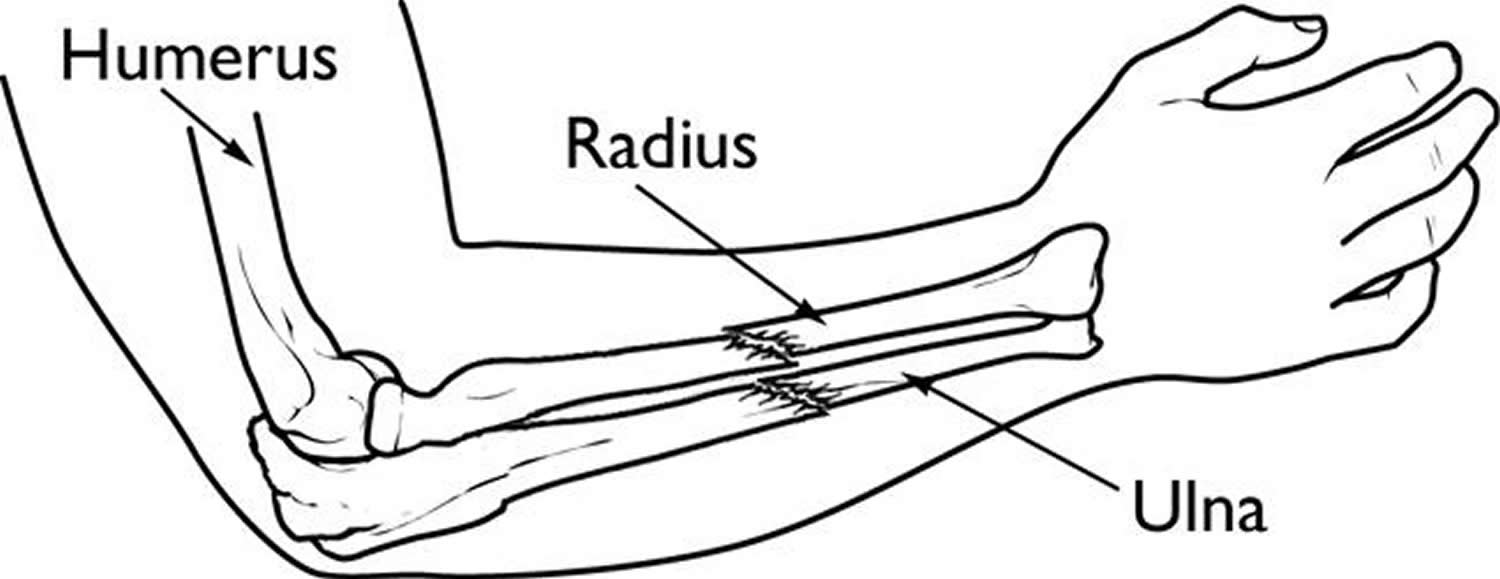
Treatment of broken bones follows one basic rule: the broken pieces must be put back into position and prevented from moving out of place until they are healed. Because the radius and ulna rely on each other for support, it is important that they are properly stabilized. If the bones are not accurately aligned during healing, it may result in future problems with wrist and elbow movement.
It is very important to control the movement of a broken bone. Moving a broken bone can cause additional damage to the bone, nearby blood vessels, and nerves or other tissues surrounding the bone.
Additional immediate treatment will include applying ice to help reduce swelling, and providing you with pain medicine.
Soon after a fracture occurs, the body acts to protect the injured area, and forms a callus (new bone) around the fracture.
- Many new cells enter the damaged area causing inflammation at the site of the injury and new blood vessels are built to carry oxygen. Oxygen is needed for all body functions, including healing.
- New “threads” of bone cells start to grow on both sides of the fracture line. These threads grow toward each other.
- The fracture closes and the callus is absorbed. Depending upon the type of fracture, this healing process may take up to a year.
Bone fractures can be caused by a trauma, such as a sporting injury, motor vehicle accident, or a fall. One of the most common causes of a broken arm is falling onto an outstretched hand.
Bone fractures can also be caused by minor injuries in conditions that weaken the bones and allow them to fracture more easily (osteoporosis and some types of cancer are examples).
Figure 1. Fractured arm
Symptoms of a bone fracture may include:
- pain
- swelling
- deformity
- bruising
- loss of function of the limb.
Fractured bones require medical attention.
It’s important to treat a fracture as soon as possible for proper healing.
If you think you or someone else has a broken arm or wrist:
- go to your nearest accident and emergency (A&E) department or call for an ambulance if it’s a bad break – minor fractures can often be treated at a local minor injuries unit;
- avoid moving the affected arm as much as possible – it may help to support it in a sling that goes under the arm and around the neck;
- stop any bleeding by applying pressure to the wound with a clean pad or dressing if possible;
- apply an ice pack (such as a bag of frozen peas wrapped in a tea towel) to the injured area if one is easily available;
- don’t eat or drink anything in case you need surgery to fix the bone when you get to hospital
If your child has injured their arm or wrist, try to get someone else to drive so you can support and comfort them.
Treatment depends on the site and severity of the injury. A simple break might be treated with a sling, ice and rest. However, the bone may require realignment (reduction) in the emergency room.
A more complicated break might require surgery to realign the broken bone and to implant wires, plates, nails or screws to keep the bone in place during healing.
Complications of a broken arm
The prognosis for most arm fractures is very good if treated early. But complications can include:
- Uneven growth. Because a child’s arm bones are still growing, a fracture in the area where growth occurs near each end of a long bone (growth plate) can interfere with that bone’s growth.
- Osteoarthritis. Fractures that extend into a joint can cause arthritis there years later.
- Stiffness. The immobilization required to heal a fracture in the upper arm bone can sometimes result in painfully limited range of motion of the elbow or shoulder.
- Bone infection. If a part of your broken bone protrudes through your skin, it can be exposed to germs that can cause infection. Prompt treatment of this type of fracture is critical.
- Nerve or blood vessel injury. If the upper arm bone (humerus) fractures into two or more pieces, the jagged ends can injure nearby nerves and blood vessels. Seek immediate medical attention if you notice numbness or circulation problems.
- Excessive bleeding and swelling right after the injury may lead to acute compartment syndrome, a condition in which the swelling cuts off blood supply to the hand and forearm. It typically occurs within 24 to 48 hours of the injury and causes severe pain when moving the fingers. Compartment syndrome can result in loss of sensation and function, and requires emergency surgery once it is diagnosed. In such cases, the skin and muscle coverings are opened and left open to relieve pressure and allow blood to return.
- Compartment syndrome. Excessive swelling of the injured arm can cut off the blood supply to part of the arm, causing pain and numbness. Typically occurring 24 to 48 hours after the injury, compartment syndrome is a medical emergency that requires surgery.
- Open fractures expose the bone to the outside environment. Even with good surgical cleaning of the bone and muscle, the bone can become infected. Bone infection is difficult to treat and often requires multiple surgeries and long-term antibiotics.
Structure of Bone
A typical long bone consists of the following parts:
- The diaphysis is the bone’s shaft or body—the long, cylindrical, main portion of the bone.
- The epiphyses (singular is epiphysis) are the proximal and distal ends of the bone.
- The metaphyses (singular is metaphysis) are the regions between the diaphysis and the epiphyses. In a growing bone, each metaphysis contains an epiphyseal (growth) plate, a layer of hyaline cartilage that allows the diaphysis of the bone to grow in length. When a bone ceases to grow in length at about ages 14–24, the cartilage in the epiphyseal plate is replaced by bone; the resulting bony structure is known as the epiphyseal line.
- The articular cartilage is a thin layer of hyaline cartilage covering the part of the epiphysis where the bone forms an articulation (joint) with another bone. Articular cartilage reduces friction and absorbs shock at freely movable joints. Because articular cartilage lacks a perichondrium and lacks blood vessels, repair of damage is limited.
- The periosteum is a tough connective tissue sheath and its associated blood supply that surrounds the bone surface wherever it is not covered by articular cartilage. It is composed of an outer fibrous layer of dense irregular connective tissue and an inner osteogenic layer that consists of cells. Some of the cells enable bone to grow in thickness, but not in length. The periosteum also protects the bone, assists in fracture repair, helps nourish bone tissue, and serves as an attachment point for ligaments and tendons. The periosteum is attached to the underlying bone by perforating fibers or Sharpey’s fibers, thick bundles of collagen that extend from the periosteum into the bone extracellular matrix.
- The medullary cavity or marrow cavity, is a hollow, cylindrical space within the diaphysis that contains fatty yellow bone marrow and numerous blood vessels in adults. This cavity minimizes the weight of the bone by reducing the dense bony material where it is least needed. The long bones’ tubular design provides maximum strength with minimum weight.
- The endosteum is a thin membrane that lines the medullary cavity. It contains a single layer of bone-forming cells and a small amount of connective tissue.
Figure 2. Parts of a long bone
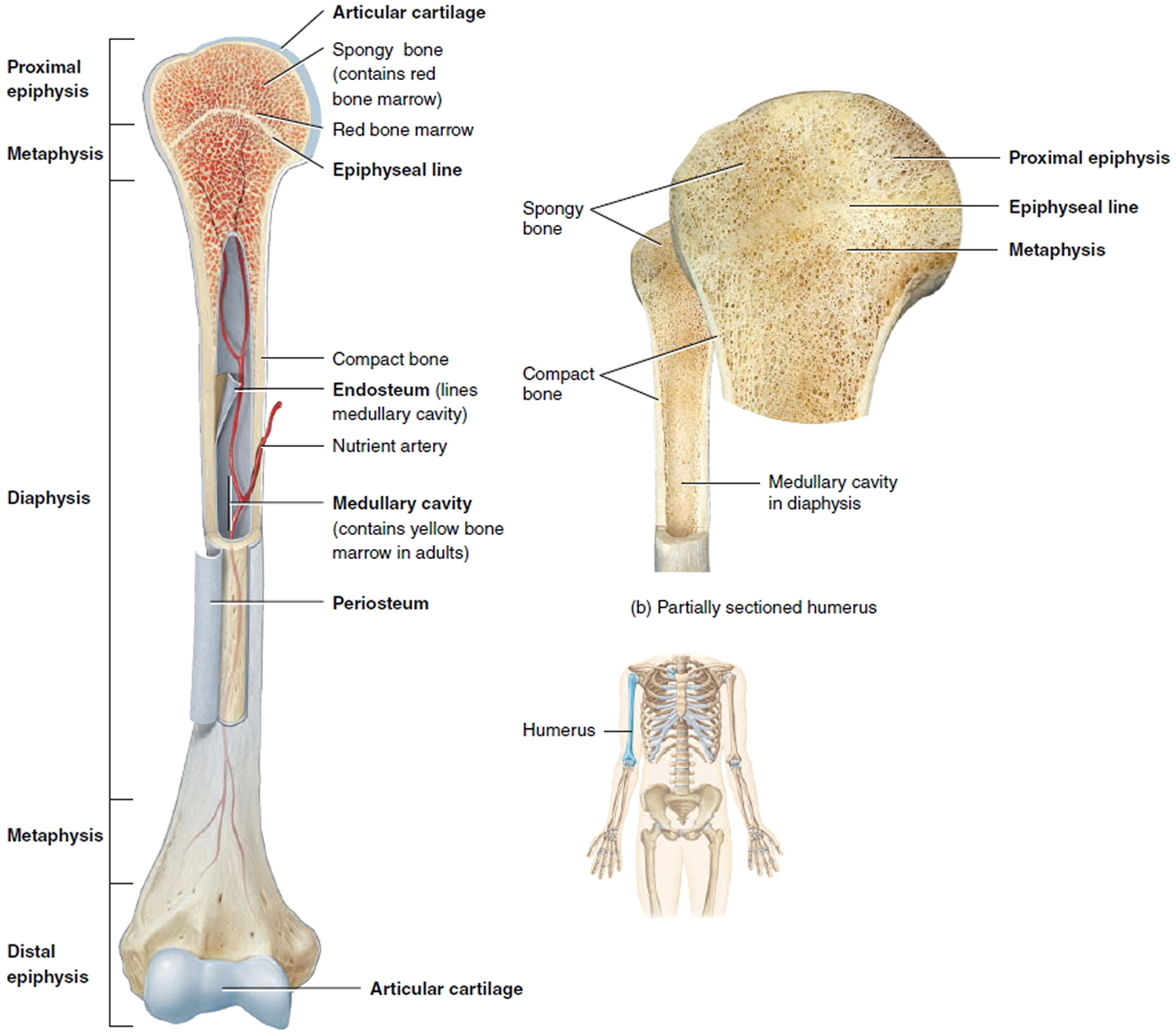
Note: The spongy bone tissue of the epiphyses and metaphyses contains red bone marrow, and the medullary cavity of the diaphysis contains yellow bone marrow (in adults).
The Cells of Mature Bone
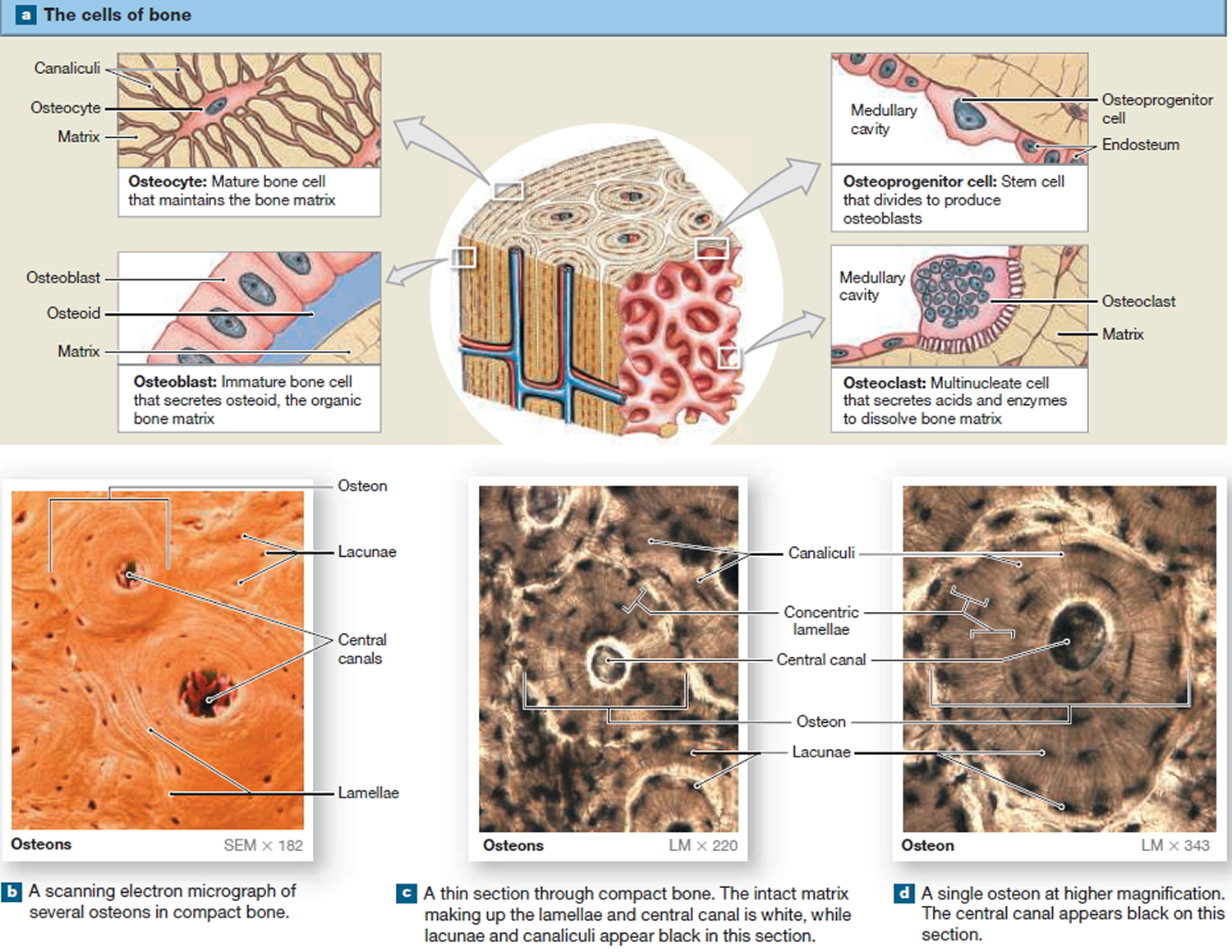
Bone contains four cell types: osteoblasts, osteocytes, osteoprogenitor cells, and osteoclasts.
Osteocytes
Mature bone cells are osteocytes. They maintain and monitor the protein and mineral content of the surrounding matrix. The minerals in the matrix are continually recycled. Each osteocyte directs the release of calcium from bone into blood and the deposition of calcium salts into the surrounding matrix. Osteocytes occupy small chambers, called lacunae, that are sandwiched between layers of calcified matrix. These matrix layers are called lamellae (singular, lamella) (Figure 3 b–d). Channels called canaliculi (“little canals”) radiate through the matrix from lacuna to lacuna and toward free surfaces and adjacent blood vessels. The canaliculi connect adjacent lacunae and bring the processes of neighboring osteocytes into close contact. Tight junctions interconnect these processes and provide a route for the diffusion of nutrients and waste products from one osteocyte to another across gap junctions.
Osteoblasts
Cuboidal cells found in a single layer on the inner or outer surfaces of a bone are called osteoblasts (precursor). These cells secrete the organic components of the bone matrix. This material, called osteoid, later becomes mineralized through a complicated, multistep mechanism. Osteoblasts are responsible for the production of new bone—a process called osteogenesis. It is thought that osteoblasts respond to a variety of different stimuli, including mechanical and hormonal, to initiate osteogenesis. If an osteoblast becomes surrounded by matrix, it differentiates into an osteocyte.
Osteoprogenitor Cells
Bone tissue also contains small numbers of stem cells termed osteoprogenitor cells (ancestor). Osteoprogenitor cells differentiate from mesenchyme and are found in numerous locations, including the innermost layer of the periosteum and the endosteum lining the medullary cavities. Osteoprogenitor cells divide to produce daughter cells that differentiate into osteoblasts. The ability to produce additional osteoblasts becomes extremely important after a bone is cracked or broken.
Osteoclasts
Large, multinucleate cells found at sites where bone is being removed are termed osteoclasts. They are derived from the same stem cells that produce monocytes and neutrophils. They secrete acids through a process involving the exocytosis of lysosomes. The acids dissolve the bony matrix and release amino acids and the stored calcium and phosphate. This erosion process, called osteolysis, increases the calcium and phosphate concentrations in body fluids. Osteoclasts are always removing matrix and releasing minerals, and osteoblasts are always producing matrix that quickly binds minerals. The balance between the activities of osteoblasts and osteoclasts is very important; when osteoclasts remove calcium salts faster than osteoblasts deposit them, bones become weaker. When osteoblasts are more active than osteoclasts, bones become stronger and more massive. New research indicates that osteoclasts may also be involved in osteoblast
differentiation, immune system activation, and the proliferation of tumor cells in bone.
Figure 3. Microscopic Structure of a Typical Bone
Organization of Mature Bone
The Matrix of Bone
Calcium phosphate, accounts for almost two-thirds of the weight of bone. It interacts with calcium hydroxide to form crystals of hydroxyapatite. As these crystals form, they incorporate other calcium salts, such as calcium carbonate, and ions such as sodium, magnesium, and fluoride. This process, called calcification is initiated by bone-building cells called osteoblasts. Calcification requires the presence of collagen fibers. Mineral salts first begin to crystallize in the microscopic spaces between collagen fibers. After the spaces are filled, mineral crystals accumulate around the collagen fibers. The combination of crystallized salts and collagen fibers is responsible for the characteristics of bone. These inorganic components enable bone to resist compression. Roughly one-third of the weight of bone is from collagen fibers and other noncollagenous proteins, which give bone considerable tensile strength.
Osteocytes and other cell types account for only 2 percent of the mass of a typical bone. Calcium phosphate crystals are very strong, but relatively inflexible. They with stand compression, but the crystals shatter when exposed to bending, twisting, or sudden impacts. Collagen fibers are tough and flexible. They easily tolerate stretching, twisting, and bending but, when compressed, they simply bend out of the way. In bone, the collagen fibers and other noncollagenous proteins provide an organic framework for the formation of mineral crystals. The hydroxyapatite crystals form small plates that lie alongside these ground substance proteins. The result is a protein–crystal combination with properties intermediate between those of collagen and those of pure mineral crystals.
Compact and Spongy Bone
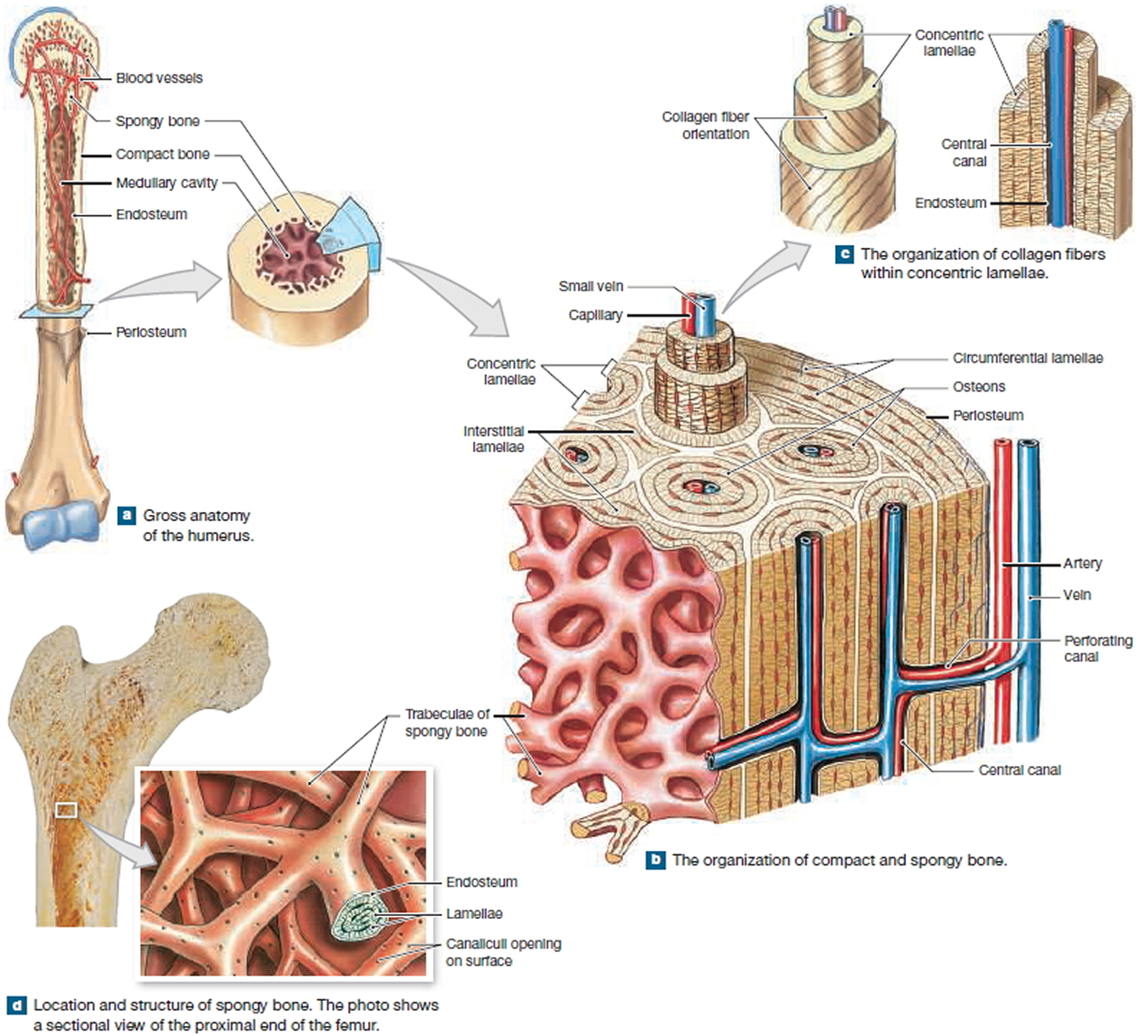
There are two types of osseous tissue: compact bone and spongy bone. Compact bone is relatively dense and solid, whereas spongy bone, also termed trabecular bone or cancellous bone, forms an open network of struts and plates. Both are found in typical bones of the skeleton, such as the humerus, the proximal bone of the upper limb, and the femur, the proximal bone of the lower limb. Compact bone forms the walls, and an internal layer of spongy bone surrounds the medullary
(marrow) cavity. The medullary cavity contains bone marrow, a loose connective tissue that is dominated by either adipocytes (yellow marrow) or a mixture of mature and immature red and white blood cells and the stem cells that produce them (red marrow). Yellow marrow, often found in the medullary cavity of the shaft, is an important energy reserve. Extensive areas of red marrow, such as in the spongy bone of the femur, are important sites of blood cell formation.
Structural Differences between Compact and Spongy Bone
Compact and spongy bone have the same matrix composition, but they differ in the three-dimensional arrangement of the osteocytes, canaliculi, and lamellae.
Figure 4. Internal organization of bones
Compact Bone
Compact bone tissue contains few spaces and is the strongest form of bone tissue. It is found beneath the periosteum of all bones and makes up the bulk of the diaphyses of long bones. Compact bone tissue provides protection and support and resists the stresses produced by weight and movement.
Compact bone tissue is composed of repeating structural units called osteons, or haversian systems. Each osteon consists of concentric lamellae arranged around an osteonic (haversian or central) canal. Resembling the growth rings of a tree, the concentric lamellae are circular plates of mineralized extracellular matrix of increasing diameter, surrounding a small network of blood vessels and nerves located in the central canal. These tubelike units of bone generally form a series of parallel cylinders that, in long bones, tend to run parallel to the long axis of the bone. Between the concentric lamellae are small spaces called lacunae (little lakes; singular is lacuna), which contain osteocytes. Radiating in all directions from the lacunae are tiny canaliculi (small channels), which are filled with extracellular fluid. Inside the canaliculi are slender fingerlike processes of osteocytes.
Neighboring osteocytes communicate via gap junctions. The canaliculi connect lacunae with one another and with the central canals, forming an intricate, miniature system of interconnected canals throughout the bone. This system provides many routes for nutrients and oxygen to reach the osteocytes and for the removal of wastes.
Osteons in compact bone tissue are aligned in the same direction and are parallel to the length of the diaphysis. As a result, the shaft of a long bone resists bending or fracturing even when considerable force is applied from either end. Compact bone tissue tends to be thickest in those parts of a bone where stresses are applied in relatively few directions. The lines of stress in a bone are not static. They change as a person learns to walk and in response to repeated strenuous physical activity, such as weight training. The lines of stress in a bone also can change because of fractures or physical deformity. Thus, the organization of osteons is not static but changes over time in response to the physical demands placed on the skeleton.
The areas between neighboring osteons contain lamellae called interstitial lamellae, which also have lacunae with osteocytes and canaliculi. Interstitial lamellae are fragments of older osteons that have been partially destroyed during bone rebuilding or growth. Blood vessels and nerves from the periosteum penetrate the compact bone through transverse interosteonic (Volkmann’s or perforating) canals. The vessels and nerves of the interosteonic canals connect with those of the medullary cavity, periosteum, and central canals. Arranged around the entire outer and inner circumference of the shaft of a long bone are lamellae called circumferential lamellae. They develop during initial bone formation. The circumferential lamellae directly deep to the periosteum are called external circumferential lamellae. They are connected to the periosteum by perforating (Sharpey’s) fibers. The circumferential lamellae that line the medullary cavity are called internal circumferential lamellae.
Spongy Bone
The major difference between compact and spongy bone is the arrangement of spongy bone into parallel struts or thick, branching plates called trabeculae (also termed spicules). Numerous interconnecting spaces occur between the trabeculae in spongy bone. Spongy bone possesses lamellae, and if the trabeculae are thick enough, osteons will be present. In terms of the associated cells and the structure and composition of the lamellae, spongy bone is no different from compact bone. Spongy bone forms an open framework and as a result it is much lighter than compact bone. However, the branching trabeculae give spongy bone considerable strength despite its relatively light weight. Thus, the presence of spongy bone reduces the weight of the skeleton and makes it easier for muscles to move the bones. Spongy bone is found wherever bones are not stressed heavily or where stresses arrive from many directions.
Functional Differences between Compact and Spongy Bone
A layer of compact bone covers the surface of all bones. The thickness of this layer varies from region to region and from one bone to another, but compact bone is thickest where stresses arrive from a limited number of directions. This superficial layer of compact bone is in turn covered by the periosteum, a connective tissue wrapping that is connected to the deep fascia. The periosteum is complete everywhere except within a joint, where the edges or ends of two bones contact one another.
The shaft of compact bone transfers stresses from one epiphysis to another. For example, when you are standing, the shaft of the femur transfers your body weight from your hip to your knee. The osteons within the shaft are parallel to its long axis, and as a result the femur is very strong when stressed along that axis. Imagine a single osteon as a drinking straw with very thick walls. When you push the ends of a straw together, it seems quite strong. However, when you hold the ends and push the side of the straw, it breaks easily. Similarly, a long bone does not bend when forces are applied to either end, but an impact to the side of the shaft can easily cause a break, or fracture.
Spongy bone is not as massive as compact bone, but it is much more capable of resisting stresses applied from many different directions. The epiphyses of the femur are filled with spongy bone, and the alignment of the trabeculae within the proximal epiphysis. The trabeculae are oriented along the stress lines, but with extensive cross-bracing. At the proximal epiphysis, the trabeculae transfer forces from the hip across the metaphysis to the femoral shaft; at the distal epiphysis, the trabeculae transfer the forces across the knee joint to the leg. In addition to reducing weight and handling stress from many directions, the open trabecular framework supports and protects the cells of the bone marrow.
How does the bone reform?
The cells put fibrous (stringy) tissues and cartilage down in a lump called callus. This callus can be felt as a hard lump under the skin and seen on x-ray. The callus forms a weak type of bone, connecting the two ends. At this stage you will no longer feel pain and the bone feels stronger. However, the bone is not as strong as normal and can easily re-break or bend at this early stage if you’re not careful. This stage is around three to six weeks after the break.
The weaker bone is slowly replaced by your normal bone and the bone looks and works as it did before the break. An increase in strength occurs between six weeks to three months after the break. In children, the bone can even slowly straighten itself if it has healed in a slightly bent position. This process is called remodelling and occurs until your child stops growing as a teenager.
Vitamin C and calcium found in a healthy, well-balanced diet are all that are required to assist in your bone healing . Medication has not been shown to help heal bones in children. Speak to your doctor or dietician for advice.
How long does a broken arm take to heal
Your doctor will decide on the length of time a plaster cast is required. It is dependent on which bone was broken and how quickly your bone heals. As a general guide, a broken arm can be out of the cast by about six weeks, but a leg may require longer. Each person is different and some may heal quicker or slower than others. After the cast is removed, you are likely to have a stiff joint but this usually resolves over a few days to several weeks without any need for treatment. You will need to be advised by your doctor when you will be able to take part in activities like contact sport.
Note: This video provides information about how fractures heal and factors that can slow or even stop the bone healing process.
Broken arm signs and symptoms
Symptoms of a broken arm or wrist
Signs of a broken arm or wrist include:
- severe pain and tenderness
- bruising and swelling
- difficulty moving the hand or arm
- the wrist or arm being an odd shape
- a snap or grinding noise at the time of injury
- bleeding (if the bone has damaged the skin) – sometimes the bone may poke through the skin
- tingling and numbness
Because of the shock and pain of breaking your arm, you may also feel faint, dizzy or sick.
It can be hard to tell the difference between a minor break and a sprain. It’s best to assume it’s a fracture until it has been checked by a doctor or nurse.
Causes of broken arm or fractured arm
Common causes for a broken arm include:
- Falls. Falling onto an outstretched hand or elbow is the most common cause of a broken arm.
- Sports injuries. Direct blows and injuries on the field or court cause all types of arm fractures.
- Significant trauma. Any of your arm bones can break during a car accident, bike accident or other direct trauma.
- Child abuse. In children, a broken arm might be the result of child abuse.
Risk factors for broken arm
Certain medical conditions or physical activities can increase the risk of a broken arm.
Certain sports
Any sport that involves physical contact or increases your risk of falling — including football, soccer, gymnastics, skiing and skateboarding — also increases the risk of a broken arm.
Bone abnormalities
Conditions that weaken bones, such as osteoporosis and bone tumors, increase your risk of a broken arm. This type of break is known as a pathological fracture.
Prevention of fractured arm
Although it’s impossible to prevent an accident, these tips might offer some protection against bone breakage.
- Eat for bone strength. Eat a healthy diet that includes calcium-rich foods, such as milk, yogurt and cheese, and vitamin D, which helps your body absorb calcium. You can get vitamin D from fatty fish, such as salmon; from fortified foods, such as milk and orange juice; and from sun exposure.
- Exercise for bone strength. Weight-bearing physical activity and exercises that improve balance and posture can strengthen bones and reduce the chance of a fracture. The more active and fit you are as you age, the less likely you are to fall and break a bone.
- Prevent falls. To prevent falling, wear sensible shoes. Remove home hazards that can cause you to trip, such as area rugs. Make sure your living space is well lit. Install grab bars in your bathroom and handrails on your stairways, if necessary.
- Use protective gear. Wear wrist guards for high-risk activities, such as in-line skating, snowboarding, rugby and football.
- Don’t smoke. Smoking can increase your risk of a broken arm by reducing bone mass. It also hampers healing of fractures.
Diagnosis of a broken arm
It is important that your doctor knows the circumstances of your injury. For example, if you fell from a ladder, how far did you fall? It is just as important for your doctor to know if you sustained any other injuries and if you have any other medical problems, such as diabetes. Your doctor also needs to know if you take any medications.
After discussing your symptoms and medical history, your doctor will do a careful examination. Your doctor will:
- Examine your skin to see if there are any cuts from the injury. Bone fragments can break through the skin and create lacerations. This leads to an increased risk for infection.
- Palpate (feel) all around your arm to determine if there are any other areas of tenderness. This can indicate other broken bones or injuries.
- Check your pulse at the wrist to be sure that good blood flow is getting through your forearm to your hand.
- Check to see if you can move your fingers and wrist, and can feel things with your fingers. Sometimes, nerves may be injured at the same time that the bone is broken, which can result in hand and wrist weakness and numbness.
- The doctor may examine your shoulder, upper arm, elbow, wrist, and hand, even if you only complain of arm pain.
X-rays
X-rays are the most common and widely available diagnostic imaging technique. X-rays can show if the bone is broken and whether there is displacement (the gap between broken bones). They can also show how many pieces of broken bone there are.
Your doctor will occasionally, another scan, such as an MRI, might be used to get more-detailed images.
Broken arm treatment
When you arrive at the hospital, you’ll be given painkillers and a support (splint) may be fixed to your arm to secure it in position.
An X-ray will be carried out to check whether your arm or wrist is broken and how severe the break is.
Treatment of a broken arm depends on the type of break. The time needed for healing depends on a variety of factors, including severity of the injury; other conditions, such as diabetes; your age; nutrition; and tobacco and alcohol use.
Fractures are classified into one or more of the following categories:
- Open (compound) fracture. The broken bone pierces the skin, a serious condition that requires immediate, aggressive treatment to decrease the risk of infection.
- Closed fracture. The skin remains unbroken.
- Displaced fracture. The bone fragments on each side of the break aren’t aligned. Surgery might be required to realign the fragments.
- Comminuted fracture. The bone is broken into pieces, so it might require surgery.
- Greenstick fracture. The bone cracks but doesn’t break all the way — like what happens when you bend a green stick of wood. Most broken bones in children are greenstick fractures because children’s bones are softer and more flexible than are those of adults.
- Buckle (torus) fracture. One side of the bone is compressed, which causes the other side to bend (buckle). This type of fracture is also more common in children.
For a minor fracture:
- a plaster cast or removable splint will usually be applied – sometimes this may be done a few days later, to allow any swelling to go down first (a splint can be left on until a cast is fitted)
- you may be given a sling to support your arm
- you’ll be given painkillers to take home and told how to look after your cast
- you’ll probably be asked to attend follow-up appointments to check how your arm or wrist is healing
Figure 5. Broken arm treatment

For more serious fractures:
- a doctor may try to realign the broken bones with their hands – this will usually be done while you’re awake, but your arm will be numbed and you may be given medicine to relax you
- surgery may be carried out to realign the bones – this will often involve putting wires, plates, screws or rods inside your arm, but sometimes a temporary external frame may be used
- a plaster cast will usually be applied to your arm before you go home
- you’ll be asked to attend follow-up appointments to check how your arm or wrist is healing.
Setting the bone
While you are in the emergency room, if you have a displaced fracture, your doctor may try to temporarily realign the bones, depending upon how far out of place the pieces are. “Reduction” is the technical term for this process in which the doctor moves the pieces back into position (reduction). This is not a surgical procedure. Your pain will be controlled with medication. Depending on the amount of pain and swelling you have, you might need a muscle relaxant, a sedative or even a general anesthetic before this procedure. Afterward, your doctor will apply a splint (like a cast) to your forearm and provide a sling to keep your arm in position. Unlike a full cast, a splint can be tightened or loosened, and allows swelling to occur safely.
Immobilization
Restricting movement of a broken bone, which requires a splint, sling, brace or cast, is critical to healing. Before applying a cast, your doctor will likely wait until the swelling goes down, usually five to seven days after injury. In the meantime, you’ll likely wear a splint.
Your doctor might ask you to return for X-rays during the healing process to make sure the bones haven’t shifted.
Pain Management
Pain after an injury or surgery is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover faster.
Medications are often prescribed for short-term pain relief after surgery or an injury. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics.
To reduce pain and inflammation, your doctor might recommend an over-the-counter pain reliever. If your pain is severe, you may need a prescription medication that contains a narcotic for a few days.
- Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery or an injury, they are a narcotic and can be addictive. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your treatment.
Nonsteroidal anti-inflammatory drugs can help with pain but might also hamper bone healing, especially if used long term. Ask your doctor if you can take them for pain relief.
If you have an open fracture, in which you have a wound or break in the skin near the wound site, you’ll likely be given an antibiotic to prevent infection that could reach the bone.
Physical Therapy
Rehabilitation begins soon after initial treatment. In most cases, it’s important, if possible, to begin some motion to minimize stiffness in your arm, hand and shoulder while you’re wearing your cast or sling.
After your cast or sling is removed, your doctor might recommend additional rehabilitation exercises or physical therapy to restore muscle strength, joint motion and flexibility.
Recovering from a broken arm or wrist
Your cast will need to stay on until the broken bone has healed. This usually takes a month or two, but can take longer if the break was severe.
While your arm is in a cast:
- avoid putting weight or strain on the arm – don’t stop moving it completely, but avoid activities such as carrying anything heavy, driving and sports
- keep the cast dry and keep your arm raised (for example, on pillows) whenever possible – read more about how to care for a plaster cast
- do some gentle exercises and stretches to reduce stiffness – your doctor or a physiotherapist will advise you about this
- get medical advice if you notice changes in your skin colour, unusual sensations in your arm or wrist, signs of infection (redness, swelling or smelly discharge), severe or continuous pain, or problems with your cast (it’s too loose, too tight or cracked)
Speak to your doctor about when you can return to work and normal activities. They will probably suggest gradually increasing how much you use your arm and hand over a few weeks or months.
Your arm or wrist may be stiff and weak after the cast is removed. A physiotherapist can help with these problems, although sometimes they can last several months or more.
Getting your hand moving after a wrist fracture
It is normal to feel some pain after the plaster has been removed and as your hand hasn’t moved for some weeks, it will feel vulnerable too.
If your pain becomes severe or continuous, you should contact your doctor.
When you get home
Unless you have had an operation on your wrist, soak your hand and forearm in warm, soapy water, allowing your hand to float and move. Pat it dry with a towel and then moisturise thoroughly. Do this 2 – 3 times a day until the skin feels normal. Do not pick or rub at the skin as this can make it sore. If you have had a wound, do this as soon as the skin is fully healed and the scabs are off and the wound is dry.
- Pain
Pain, especially on the little finger side of your wrist, can last for up to a year after a fracture and should subside gradually. This is normal and does not mean your wrist is not healing properly.
- Hypersensitivity
Sometimes the wrist and hand can be overly sensitive to touch, making it difficult to tolerate clothing and making you less confident in using your hand. This will settle with regular, firm massage, but should not be ignored as it will not settle on its own. Please speak to your physiotherapist if you experience this.
The best way to massage is fairly firmly, with straight fingers of your other hand, several times a day, with hand cream.
Reducing swelling
Swelling is common and will get in the way of normal movement.
Reduce this more quickly by:
- high elevation – rest with your elbow up at shoulder height, with your hand upright, as often as possible;
- pump your fingers open and closed, then apart and together to boost the circulation; and
- massage the whole of your forearm and hand from the tips of your fingers to your elbow 2 – 3 times a day. Take your time over this.
The shape of your wrist
This is often a worry as your wrist may look larger and a different shape. As the bone heals, the lump formed may be prominent and will take 12 – 18 months to settle fully. Please be aware that your wrist may never return to its previous shape.
Improving movement
It is important to get as much movement back as soon as you can, so you can start to use your hand normally. Doing your exercises throughout the day will help this to happen more quickly.
Using gentle heat and / or pain relief will make this easier. You can do this with warm water soaks, a hot water bottle wrapped in a towel or a wheat bag. Do not use heat on a swollen wrist or if reduced sensation makes it difficult for you to know when it is too hot.
You will need to do your exercises for several weeks. To start with they will focus on your range of movement and dexterity. From about 10 weeks after the fracture you can usually start to gradually introduce some resistance. Your physiotherapist will advise you when to introduce this.
Exercises
These exercises should be carried out several times a day – work at gradually increasing your range of movement. Exercise within your pain limits, but expect some discomfort. This should settle through the day.
- Shoulder
- Lift your arm above your head as close to your ear as you can and then reach out to the side.
- Elbow
- Bend and then straighten your arm fully.
- Forearm
- With your elbow tucked into your side, turn your palm up and down.
- Wrist
- Place your forearm on a block
and: - a) lift and lower your hand as far as you can;
- b) tilt your wrist from side to side;
- c) circle your hand clockwise and then anticlockwise.
- Place your forearm on a block
- Thumb
- a) Stretch your thumb as far away from your hand as possible, then reach across to the base of your little finger.
- b) Run your thumb up and down each of your fingers.
- Fingers
- Make a full fist and then stretch your fingers out. A soak and stretch in warm water will help if your fingers are stiff.
- Dexterity
- Button box – feel for different shapes and sizes. You could also use pasta, lentils or paper clips, or try turning playing cards over and then back again.
- Prayer stretch
- Place your palms together and move your elbows apart.
- Palm up and down
- Turn your palm up and down holding a plastic bottle at the neck. Make it heavier by gradually filling the bottle with water.
- Strength work
- a) Play-doh – rolling, pinching, gripping, pulling, making a flower / dog etc.
- b) Pinching clothes pegs.
- c) Undoing bottles and jars.
- d) Turning keys in locks.
Driving
You can return to driving when you have enough movement and strength to grip the steering wheel and control a car – usually some weeks after the removal of the plaster cast.
Returning to housework
Light housework will help get your hand and wrist moving, but avoid lifting the kettle and heavy pots early on to allow the fracture to heal. Gradually increase as you feel able to.
Broken arm surgery
Surgery is required to stabilize some fractures. If the fracture didn’t break the skin, your doctor might wait to do surgery until the swelling has gone down. Keeping your arm from moving and elevating it will decrease swelling.
Fixation devices — such as wires, plates, nails or screws — might be needed to hold your bones in place during healing. Complications are rare, but can include infection and lack of bone healing.
Surgical Treatment
When both forearm bones are broken, or if the bones have punctured the skin (open fracture), surgery is usually required.
Because of the increased risk for infection, open fractures are usually scheduled for surgery immediately. Patients are typically given antibiotics by vein (intravenous) in the emergency room, and may receive a tetanus shot. During surgery, the cuts from the injury will be thoroughly cleaned out. The broken bones are typically fixed during the same surgery.
If the skin around your fracture has not been broken, your doctor may recommend waiting until swelling has gone down before having surgery. Keeping your arm immobilized and elevated for several days will decrease swelling. It also gives skin that has been stretched a chance to recover.
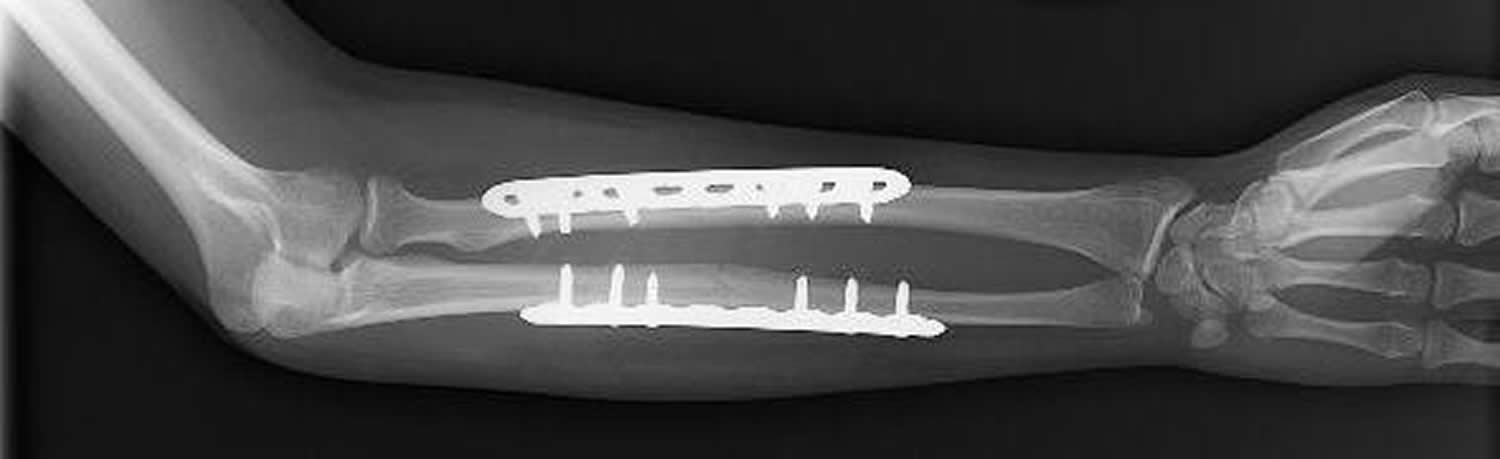
- Open reduction and internal fixation with plates and screws
This is the most common type of surgical repair for forearm fractures. During this type of procedure, the bone fragments are first repositioned (reduced) into their normal alignment. They are held together with special screws and metal plates attached to the outer surface of the bone.
- Open reduction and internal fixation with rods
During this procedure, a specially designed metal rod is inserted through the marrow space in the center of the bone.
- External fixation
If the skin and bone are severely damaged, using plates and screws and large incisions may injure the skin further. This may result in infection. In this case, you may be treated with an external fixator. In this type of operation, metal pins or screws are placed into the bone above and below the fracture site. The pins and screws are attached to a bar outside the skin. This device is a stabilizing frame that holds the bones in the proper position so they can heal.
Figure 6. Broken arm surgery
Complications from Surgery
There are risks associated with all surgery. If your doctor recommends surgery, he or she thinks that the possible benefits of surgery outweigh the risks.
- Infection. There is a risk of infection with any surgery, whether it is for a forearm fracture or another purpose.
- Damage to nerves and blood vessels. There is a minor risk of injury to nerves and blood vessels around the forearm. Although some temporary numbness is common right after your injury, if you experience persistent numbness or tingling in your fingers, contact your doctor.
- Synostosis. Another rare complication is healing between the two bones of the forearm with a bridge of bone known as synostosis. This can decrease the rotation of the bones and prevent full movement.
- Nonunion. Surgery does not guarantee healing of the fracture. A fracture may pull apart, or the screws, plates, or rods may shift or break. This can occur for a variety of reasons, including:
- The patient does not follow directions after surgery.
- The patient has other health issues that slow healing. Some diseases, like diabetes, slow healing. Smoking or using other tobacco products also slow healing.
- If the fracture was associated with a cut in the skin (an open fracture), healing is often slower.
- Infections can also slow or prevent healing.
If the fracture fails to heal, further surgery may be needed.
Rehabilitation
Nonsurgical treatment. Rehabilitation typically begins after a few weeks of keeping the arm still by using a cast or brace. In many cases, a physical therapist will help with rehabilitation, beginning with gentle exercises to increase range of motion, and gradually adding exercises to strengthen the arm.
Surgical treatment. Depending on the complexity of the fracture and the stability of the repair, a cast or brace may be necessary for 2 to 6 weeks after surgery. Motion exercises for the forearm, elbow, and wrist usually begin shortly after surgery. This early motion is important to prevent stiffness. Your doctor may also prescribe visits to a physical or occupational therapist, depending on how long your arm was immobilized.





{kind=link}