




Running for beginners weight loss
Physical activity including running is an important part of your weight management program. Running can be a fun and flexible way to exercise – it can help keep you in shape and help you lose weight too. However, most weight loss occurs because of decreased calorie intake. That’s because it’s easier to cut 500 calories a day from your diet than it is to burn 500 extra calories through running. You’d have to run about five miles a day for a week to lose one pound of fat! Jogging uses roughly 100 calories per mile. Precisely how many calories you’ll burn depends on a number of things, including your weight and how fast you run. So you’d lose about one pound for every extra 35 miles you run — provided you don’t change anything about your current food intake or other activities. To lose one pound by running, you need to burn approximately 3,500 calories. If you run slowly (at a pace of 4 miles per hour) for 30 minutes on five out of seven days, you’ll log 10 miles a week. That means it would take three-and-a-half weeks to lose one pound if the number of calories you consume stays the same. On the other hand if you simply altered your diet and cut back by 250 calories a day (e.g., ½ cup of ice cream or two sugar-sweetened sodas), you’d lose a pound in two weeks. If you ate 250 fewer calories a day and run for 30 minutes a day, it would take just over a week to lose one pound. Reducing calorie intake even more and exercising more would further speed the process. Therefore, a better strategy for weight loss involves a two-pronged approach: exercising and cutting calories.
Weight stability requires a balance between calories consumed (calories IN) and calories expended (calories Out). Managing calorie intake is fundamental to achieving and maintaining calorie balance—the balance between the calories intake from foods and the calories expended from metabolic processes and physical activity. The best way to determine whether your eating pattern is at an appropriate number of calories is to monitor your body weight and adjust your calorie intake and energy expenditure in physical activity based on changes in your body weight over time.
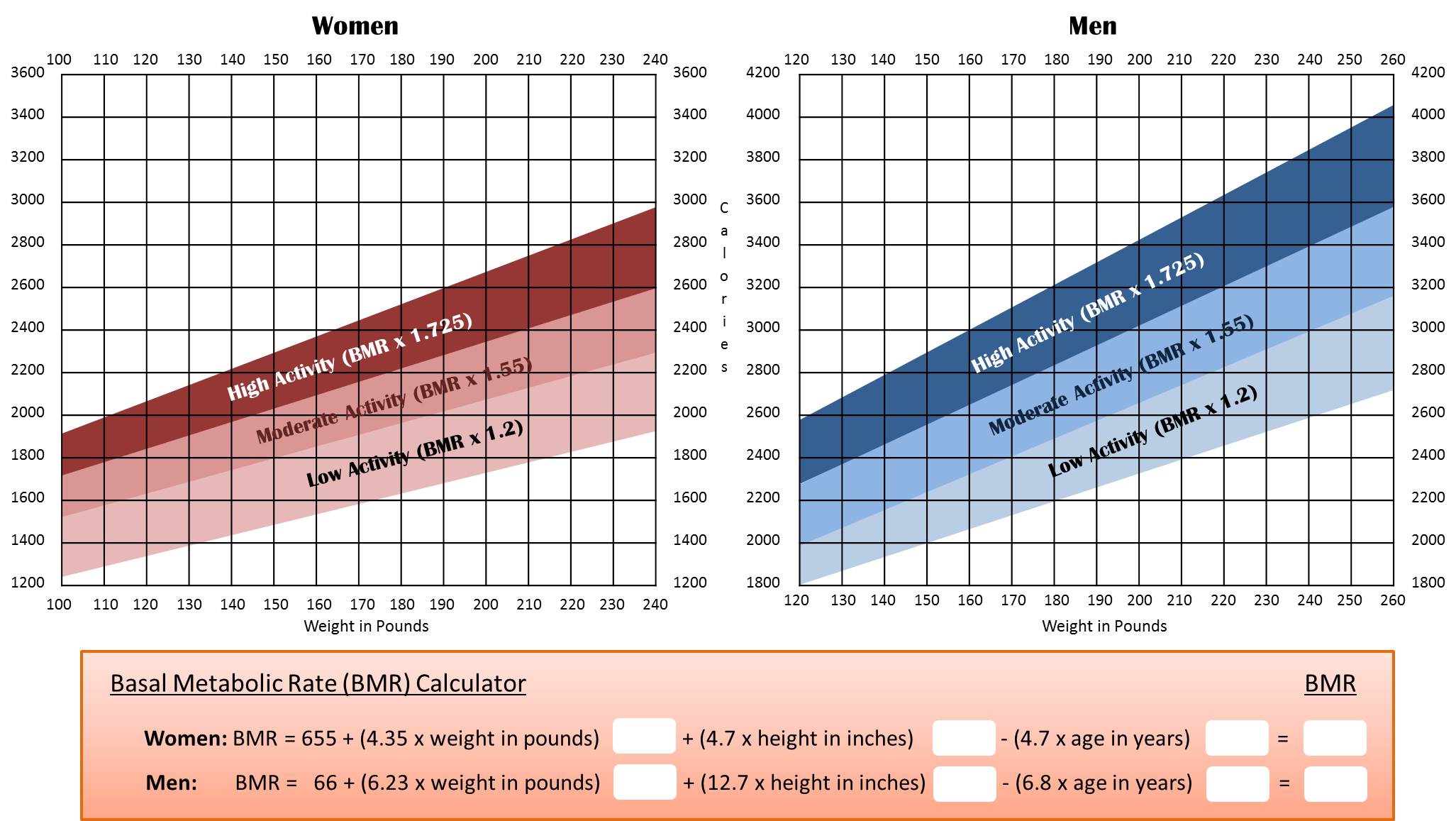
All foods and many beverages contain calories, and the total number of calories varies depending on the macronutrients in a food. On average, carbohydrates and protein contain 4 calories per gram (17 kJ/g), fats contain 9 calories per gram (37 kJ/g) and alcohol (ethanol) has 7 calories per gram (29 kJ/g) and organic acid 3 calories per gram (13 kJ/g). The total number of calories you need each day varies depending on a number of factors, including the your age, sex, height, weight, your build (muscular or athletic or average or overweight) and level of physical activity. In addition, a need to lose, maintain, or gain weight and other factors affect how many calories should be consuming.
The Department of Health and Human Services recommends that healthy adults include aerobic exercise and strength training in their fitness plans, specifically:
- At least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity a week, or an equivalent combination of moderate and vigorous aerobic activity
- Strength training exercises of all the major muscle groups at least twice a week
Sustained physical activity is most helpful in the prevention of weight regain. In addition, exercise has a benefit of reducing risks of cardiovascular disease and diabetes, beyond that produced by weight reduction alone.
- Regular exercise has been proven to help you to reduce the risk of chronic illnesses such as heart disease, certain cancers, type 2 diabetes and stroke.
- Regular exercise can help strengthen your bones and muscles.
- Research shows that physical activity can also boost self-esteem, mood, sleep quality and energy.
Start exercising slowly, and gradually increase the intensity. Trying too hard at first can lead to injury.
How Much Activity Do People Need to Prevent Weight Gain?
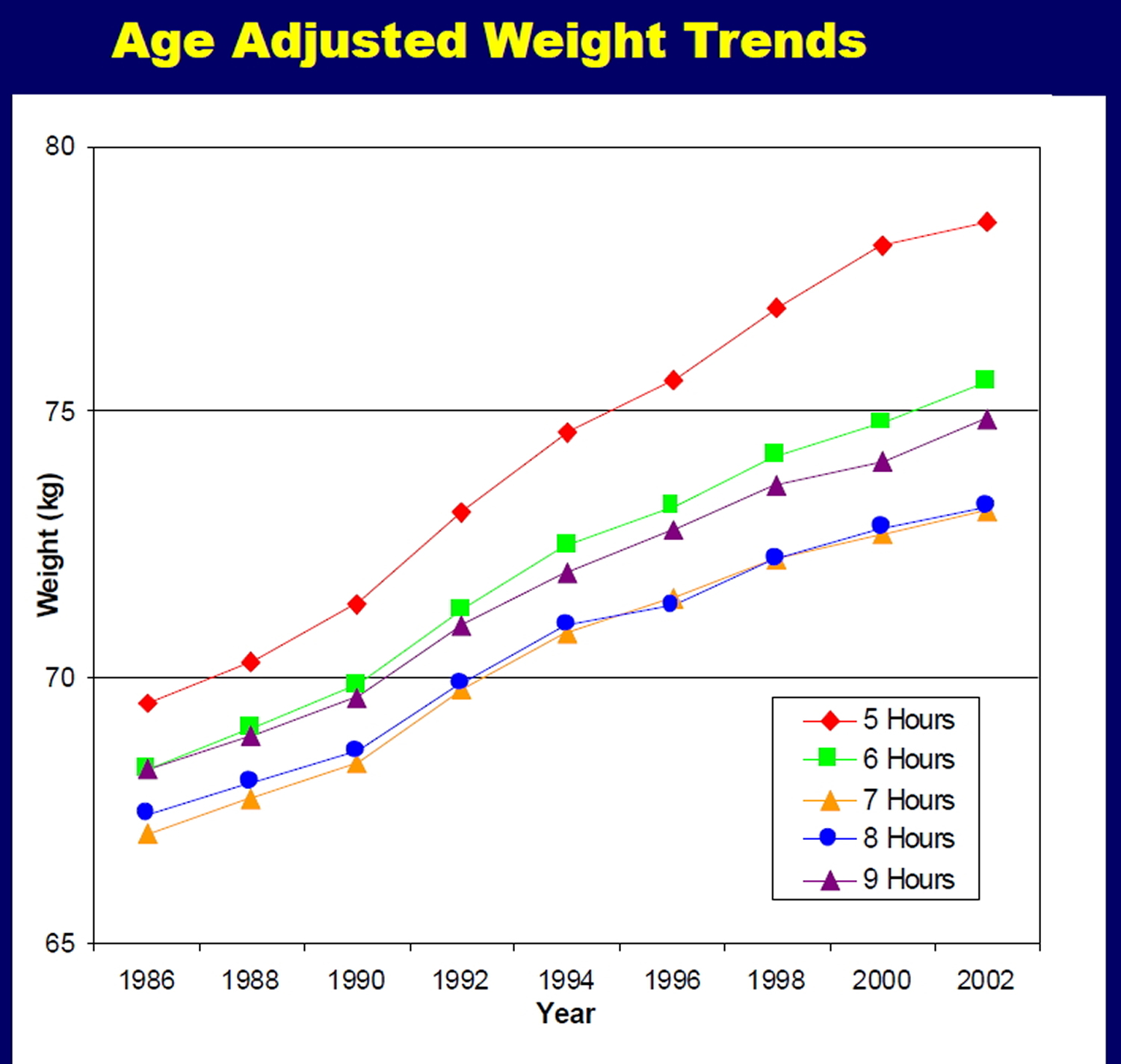
Weight gain during adulthood can increase the risk of heart disease, diabetes, and other chronic conditions. Since it’s hard for people to lose weight and keep it off, it’s better to prevent weight gain in the first place. Encouragingly, there’s strong evidence that staying active can help people slow down or stave off “middle-age spread” 1. The more active people are, the more likely they are to keep their weight steady 2; the more sedentary, the more likely they are to gain weight over time 3. But it’s still a matter of debate exactly how much activity people need to avoid gaining weight. The latest evidence suggests that the recommended two and a half hours a week may not be enough.
The Women’s Health Study, for example, followed 34,000 middle-age women for 13 years to see how much physical activity they needed to stay within 5 pounds of their weight at the start of the study. Researchers found that women in the normal weight range at the start needed the equivalent of an hour a day of moderate-to-vigorous physical activity to maintain a steady weight 4.
Vigorous activities seem to be more effective for weight control than slow walking 5, 6. The Nurses’ Health Study II 7, for example, followed more than 18,000 women for 16 years to study the relationship between changes in physical activity and weight. Although women gained, on average, about 20 pounds over the course of the study, those who increased their physical activity by 30 minutes per day gained less weight than women whose activity levels stayed steady. And the type of activity made a difference: Bicycling and brisk walking helped women avoid weight gain, but slow walking did not.
How Much Activity Do People Need to Lose Weight?
Exercise can help promote weight loss, but it seems to work best when combined with a lower calorie eating plan 8. If people don’t curb their calories, however, they likely need to exercise for long periods of time-or at a high intensity-to lose weight 9, 10.
In one study 9, for example, researchers randomly assigned 175 overweight, inactive adults to either a control group that did not receive any exercise instruction or to one of three exercise regimens-low intensity (equivalent to walking 12 miles/week), medium intensity (equivalent to jogging 12 miles/week), or high intensity (equivalent to jogging 20 miles per week). All study volunteers were asked to stick to their usual diets. After six months, those assigned to the high-intensity regimen lost abdominal fat, whereas those assigned to the low- and medium-intensity exercise regimens had no change in abdominal fat 9.
More recently, researchers conducted a similar trial with 320 post-menopausal women 11, randomly assigning them to either 45 minutes of moderate-to-vigorous aerobic activity, five days a week, or to a control group. Most of the women were overweight or obese at the start of the study. After one year, the exercisers had significant decreases in body weight, body fat, and abdominal fat, compared to the non-exercisers 11.
The Bottom Line
- For Weight Control, Aim for an Hour of Activity a Day
Being moderately active for at least 30 minutes a day on most days of the week can help lower the risk of chronic disease. But to stay at a healthy weight, or to lose weight, most people will need more physical activity-at least an hour a day-to counteract the effects of increasingly sedentary lifestyles, as well as the strong societal influences that encourage overeating.
Keep in mind that staying active is not purely an individual choice: The so-called “built environment”-buildings, neighborhoods, transportation systems, and other human-made elements of the landscape-influences how active people are 12. People are more prone to be active, for example, if they live near parks or playgrounds, in neighborhoods with sidewalks or bike paths, or close enough to work, school, or shopping to safely travel by bike or on foot. People are less likely to be active if they live in sprawling suburbs designed for driving or in neighborhoods without recreation opportunities.
Local and state governments wield several policy tools for shaping people’s physical surroundings, such as planning, zoning, and other regulations, as well as setting budget priorities for transportation and infrastructure. Strategies to create safe, active environments include curbing traffic to make walking and cycling safer, building schools and shops within walking distance of neighborhoods, and improving public transportation, to name a few. Such changes are essential to make physical activity an integral and natural part of people’s everyday lives-and ultimately, to turn around the obesity epidemic.
How much exercise do you need for general good health?
For general good health, the 2008 Physical Activity Guidelines for Americans 13 recommends that adults get a minimum of 2-1/2 hours per week of moderate-intensity aerobic activity. Yet many people may need more than 2-1/2 hours of moderate intensity activity a week to stay at a stable weight 13.
The Women’s Health Study 14, for example, followed 34,000 middle-aged women for 13 years to see just how much physical activity they needed to stay within 5 pounds of their weight at the start of the study. Researchers found that women who were in the normal weight range at the start of the study needed the equivalent of an hour a day of physical activity to stay at a steady weight 14.
If you are exercising mainly to lose weight, 60 minutes or so a day may be effective in conjunction with a healthy diet 15.
If you currently don’t exercise and aren’t very active during the day, any increase in exercise or physical activity is good for you.
Aerobic physical activity—any activity that causes a noticeable increase in your heart rate—is especially beneficial for disease prevention.
Some studies show that walking briskly for even one to two hours a week (15 to 20 minutes a day) starts to decrease the chances of having a heart attack or stroke, developing diabetes, or dying prematurely.
You can combine moderate and vigorous exercise over the course of the week, and it’s fine to break up your activity into smaller bursts as long as you sustain the activity for at least 10 minutes.
Exercise Intensity:
Moderate-intensity aerobic activity is any activity that causes a slight but noticeable increase in breathing and heart rate. One way to gauge moderate activity is with the “talk test”—exercising hard enough to break a sweat but not so hard you can’t comfortably carry on a conversation.
Vigorous-intensity aerobic activity causes more rapid breathing and a greater increase in heart rate, but you should still be able to carry on a conversation—with shorter sentences.
Here is a summary of the 2008 Physical Activity Guidelines for Americans 13
Children and adolescents should get at least 1 hour or more a day of physical activity in age-appropriate activities, spending most of that engaged in moderate- or vigorous–intensity aerobic activities. They should partake in vigorous-intensity aerobic activity on at least three days of the week, and include muscle-strengthening and bone strengthening activities on at least three days of the week.
Healthy adults should get a minimum of 2-1/2 hours per week of moderate-intensity aerobic activity, or a minimum of 1-1/4 hours per week of vigorous-intensity aerobic activity, or a combination of the two. That could mean a brisk walk for 30 minutes a day, five days a week; a high-intensity spinning class one day for 45 minutes, plus a half hour jog another day; or some other combination of moderate and vigorous activity. Doubling the amount of activity (5 hours moderate- or 2-1/2 hours vigorous-intensity aerobic activity) provides even more health benefits. Adults should also aim to do muscle-strengthening activities at least two days a week.
Healthy older Adults should follow the guidelines for healthy adults. Older adults who cannot meet the guidelines for healthy adults because of chronic conditions should be as physically active as their abilities and conditions allow. People who have chronic conditions such as arthritis and type 2 diabetes should talk to a healthcare provider about the amount and type of activity that is best. Physical activity can help people manage chronic conditions, as long as the activities that individuals choose match their fitness level and abilities. Even just an hour a week of activity has health benefits. Older adults who are at risk of falling should include activities that promote balance.
Strength training for all ages
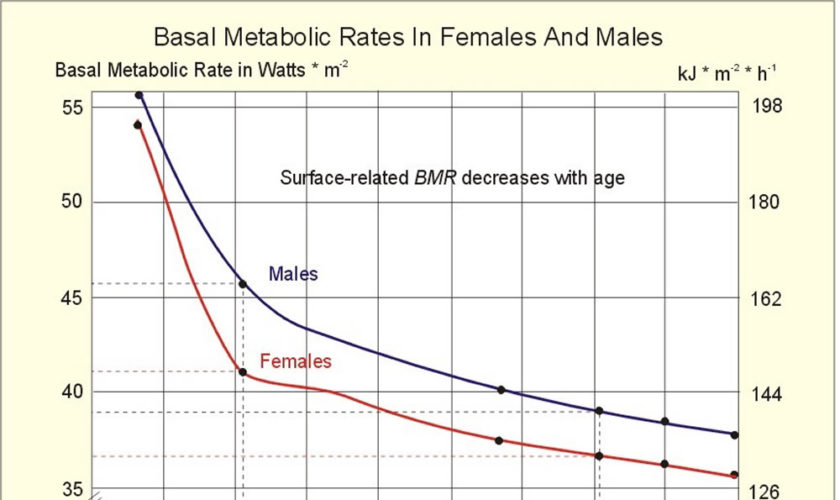
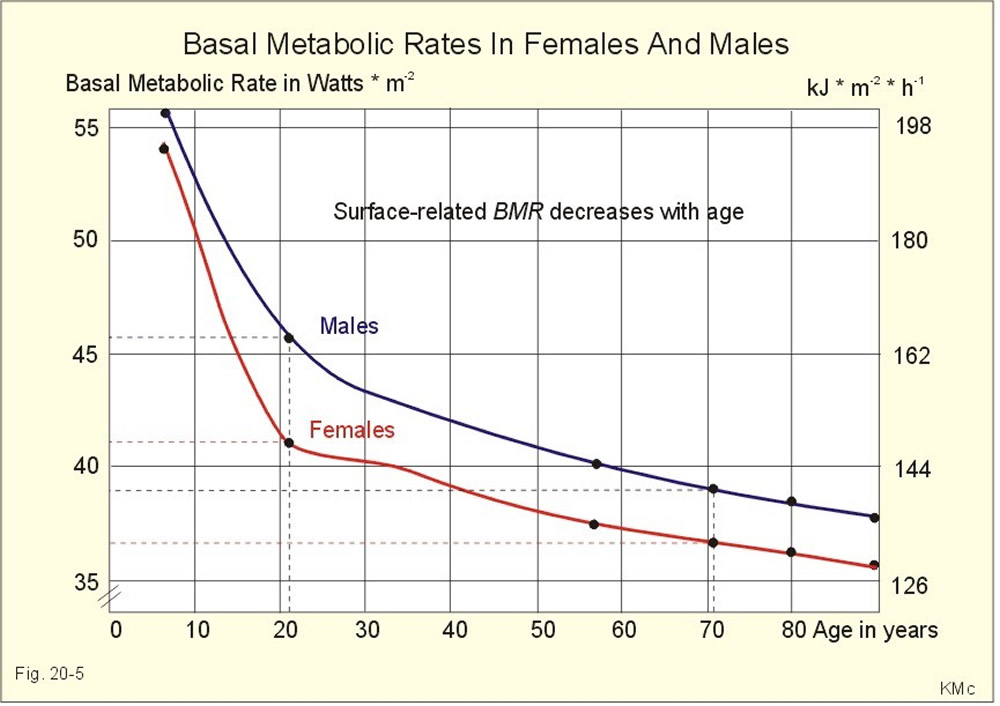
Studies have shown strength training to increase lean body mass, decrease fat mass, and increase resting metabolic rate (a measurement of the amount of calories burned per day) in adults 16. While strength training on its own typically does not lead to weight loss 13, its beneficial effects on body composition may make it easier to manage one’s weight and ultimately reduce the risk of disease, by slowing the gain of fat—especially abdominal fat 17.
- Muscle is metabolically active tissue; it utilizes calories to work, repair, and refuel itself. Fat, on the other hand, doesn’t use as much energy. We slowly lose muscle as part of the natural aging process, which means that the amount of calories we need each day starts to decrease, and it becomes easier to gain weight.
- Strength training regularly helps preserve lean muscle tissue and can even rebuild some that has been lost already.
- Weight training has also been shown to help fight osteoporosis. For example, a study in postmenopausal women examined whether regular strength training and high-impact aerobics sessions would help prevent osteoporosis. Researchers found that the women who participated in at least two sessions a week for three years were able to preserve bone mineral density at the spine and hip; over the same time period, a sedentary control group showed bone mineral density losses of 2 to 8 percent 18.
- In older populations, resistance training can help maintain the ability to perform functional tasks such as walking, rising from a chair, climbing stairs, and even carrying one’s own groceries. An emerging area of research suggests that muscular strength and fitness may also be important to reducing the risk of chronic disease and mortality, but more research is needed 19, 20.
- A systematic review of 8 studies 21 examining the effects of weight-bearing and resistance-based exercises on the bone mineral density in older men found resistance training to be an effective strategy for preventing osteoporosis in this population. Resistance training was found to have more positive effects on bone mineral density than walking, which has a lower impact 21.
The Physical Activity Guidelines for Americans recommends that muscle strengthening activities be done at least two days a week 13. Different types of strength training activities are best for different age groups.
- When talking about the benefits of exercise, keeping the heart and blood vessels healthy usually gets most of the attention. For many individuals, though, stretching and strength training exercises may be just as important.
- Strength training, also known as resistance training, weight training, or muscle-strengthening activity, is one of the most beneficial components of a fitness program.
Children and Adolescents: Choose unstructured activities rather than weight lifting exercises 13.
Examples:
- Playing on playground equipment
- Climbing trees
- Playing tug-of-war
Active Adults: Weight training is a familiar example, but there are other options 13:
- Calisthenics that use body weight for resistance (such as push-ups, pull-ups, and sit-ups)
- Carrying heavy loads
- Heavy gardening (such as digging or hoeing)
Older Adults: The guidelines for older adults are similar to those for adults; older adults who have chronic conditions should consult with a health care provider to set their activity goals. Muscle strengthening activities in this age group include the following 13:
- Digging, lifting, and carrying as part of gardening
- Carrying groceries
- Some yoga and tai chi exercises
- Strength exercises done as part of a rehab program or physical therapy
Flexibility training
Flexibility training or stretching exercise is another important part of overall fitness. It may help older adults preserve the range of motion they need to perform daily tasks and other physical activities 22.
- The American Heart Association 16 recommends that healthy adults engage in flexibility training two to three days per week, stretching major muscle and tendon groups.
- For older adults, the American Heart Association and American College of Sports Medicine recommend two days a week of flexibility training, in sessions at least 10 minutes long 22. Older adults who are at risk of falling should also do exercises to improve their balance.
Running tips for beginners
Running is free, you can do it anywhere, and it burns more calories than any other mainstream exercise. Regular running can reduce your risk of chronic illnesses, such as heart disease, type 2 diabetes and stroke. It can also boost your mood and keep your weight under control.
However, if you feel out of shape, or you’re recovering from injury or worried about an existing condition, see your doctor before you start running.
Before you start
If you’ve not been active for a while, you may want to build your fitness levels gently with walking before you move on to running. Sometimes overlooked as the easiest ways to get more active, walking briskly can help you build stamina, burn excess calories, lose weight and make your heart healthier. Plus walking is simple, free, and walking is also less stressful on your knees, hips and back than is running. You don’t have to walk for hours. A brisk 10-45 minute daily walk has lots of health benefits and counts towards your recommended 150 minutes of weekly exercise.
Running requires little equipment, but a good pair of running shoes that suit your foot type may help improve comfort.
There are many types of trainers on the market, so get advice from a specialist running retailer who will assess your foot and find the right shoe for you.
The shoe’s structure weakens over time, especially with regular use. Running experts advise replacing running shoes every 300 miles (482km).
Choosing running shoes and trainers
Running shoes are probably the most important piece of fitness equipment you’ll buy, so it’s vital to pick the right pair.
There are big differences in the way various running shoes support your feet. This means it’s not good for your feet if you play football or tennis in the same trainers you use for jogging, for example.
Running shoes are great for running and only running. They’re very flexible, allowing the foot to bend and flex through each step, but they’re not suitable for sports such as tennis that involve sideways stepping.
There are many types of trainers on the market, so try to find a specialist retailer who will assess your foot and find the right shoe for you. Good specialist running shoe retailers will offer gait analysis to get you in the right type of running shoe.
There are a number of companies that make ‘functional footwear’ for running rather than fashion-based footwear. There is also a multitude of trainers with differing amounts of support to suit different foot types. Find a specialist retailer who can assess your foot properly and fit the correct type of runner for your foot type.
It’s a good idea to get your running shoes properly fitted to suit your foot type. If they’re too small, they can cause blisters and black toenails.
Serious back, knee and hip pain, Achilles tendonitis, shin splints (leg pain), traumatized toes and painful blisters are some of the conditions people wearing ill-fitting running shoes may face.
Unfortunately, 65% of the US’s recreational sportsmen and women wear the wrong shoes for their chosen sport. Running shoes and trainers are the most important piece of fitness equipment you’ll ever buy, and changing what you wear on your feet can prevent injuries.
Specialist retailers should also be able to advise you on specialist socks that have improved fit, wick sweat away from the foot, prevent blisters and some even have silver threads to reduce smell and prevent athlete’s foot infections.
Quick tips to remember when shoe shopping
- Make sure you can wiggle your toes a little.
- Try on both shoes and walk a few steps to see if they pinch or rub.
- Leave 1cm of room from the top of your longest toe to end of the shoe.
- Feet are usually biggest in the late afternoon/evening.
Quick tips on socks
Good socks will not only help keep your feet comfortable within your shoes but will also keep them dry by drawing moisture away from the feet. Whatever you do, don’t wear 100% cotton socks – they hold the moisture against the skin, causing painful blistering. Wool and silk are often found blended with the latest generation of synthetic materials. If you find wool too warm or irritating, you could try an acrylic blended sock.
How running impacts on the foot
Whether you are running for fun, weight loss or running a marathon, you put yourself and your feet under great stress. On average, you put six times your body weight through each foot when running, which can emphasize any minor or major potential problems significantly.
Maintaining healthy feet for running
Keep your feet clean and dry to prevent blisters. Ensure you shower and dry your feet thoroughly after you have been for a run, to prevent athlete’s foot. Change your trainers every 300-500 miles, to prevent general pain from lack of cushioning or reduction of support. Trainers do not last forever.
Choosing well-fitted sports bra
How a well-fitted sports bra can reduce breast pain
Women should also consider using a sports bra, which is sturdier than a regular bra and provides additional support. The movement of a woman’s breasts during exercise can range from 4cm during a walk to 15cm when running, researchers have found. The exact mechanics are not entirely understood, but it’s thought exercise, especially high-impact exercise like running or jumping, places tension on the supporting structures of the breast, this multi-directional movement can cause breast pain. Not only can exercising with poorly supported breasts cause pain and sagging, it can cause embarrassment and put women off physical activity. A survey by the University of Portsmouth – Research Group in Breast Health 23 found breasts were the fourth biggest barrier to exercise for women after lack of motivation, time and poor health. Exercising with a well-fitted sports bra is just as important as running in the right type of trainers!
What’s the problem with bras?
Research suggests most women – perhaps more than 70% – wear the wrong bra size. This may result in pain, discomfort and irreversible sagging.
A researcher from the University of Portsmouth – Research Group in Breast Health 23, says women need better advice on getting the right fit. “The most common mistake is to wear the underband too loose and the cup size too small.” It’s important women find the best fit sports bra, rather than using a tape measure to dictate their bra size.
Why do breasts sag?
There are no muscles in the breast. The only supporting structures are the skin and the Cooper’s ligaments – thin, paper-like tissues that weave throughout the breast and attach to the chest wall. It’s thought sagging, which is irreversible, occurs when these ligaments are overstretched.
How do breasts move during exercise?
The breast has limited natural support, and any unsupported movement causes the breasts to move: up-down, in-out, and side-to-side. This multi-directional movement has been shown to increase from 4cm during walking to 15cm during running in a study of women exercising without a bra. And breast motion is not just an issue for larger-breasted women.
Which sports bra is right for me?
There are three types of sports bra:
- Compression (pushing the breast against the chest),
- Encapsulation (lifting and separating each breast) or
- A combination of both.
Not every sports bra suits every person, and wearing the wrong size or style can reduce support. You should always try on a sports bra before you buy it. Jump around in the fitting room to make sure it is giving you the support you need for your chosen activity.
- It’s essential that a sports bra fits properly for it to be effective.
Whether it’s for exercise or not, a correctly fitting and supportive bra can alleviate breast pain and help prevent back and neck pain, as well as irreversible breast sag.
The University of Portsmouth – Research Group in Breast Health 23 recommends these simple steps for choosing the right sports bra:
- Underband: the band should fit firmly around the chest. It shouldn’t slide around as you move, but it shouldn’t be too tight as to be uncomfortable, affect your breathing, or make flesh bulge over the band. The band should be level all the way around the chest.
- Cup: the breasts should be enclosed within the cups, with no bulging or gaping at the top or sides. If the cup material is puckering, then the cup size is probably too big.
- Shoulder straps: the shoulder straps should be adjusted to comfortably provide breast support without being too tight (digging into the skin). The main support for the breast should come from a firm band, not tight shoulder straps.
- Underwire: for sports bras that are underwired, the underwire should follow the natural crease of the breasts and not rest on any breast tissue. If the underwire is resting too far down the ribcage (where the rib cage gets slightly narrower), the band size is probably too small.
When should I wear a sports bra?
A well-fitted, supportive sports bra is just as important for occasional exercise as it is for regular exercise. It’s also important for all types of physical activity, including both low- and high-impact activities, and exercise of short and long duration.
How often should I replace my sports bra?
It’s important to replace your sports bra regularly to make sure it’s still giving you the best support it can. How often you need to replace your bra will depend on a number of factors, including how often you wear it and how often you wash it. The University of Portsmouth – Research Group in Breast Health 23 recommends you replace your sports bra when you replace your running shoes.
How to run correctly
Good running technique can help reduce your risk of injury and make your runs feel less tiring and more enjoyable.
To avoid injury and enjoy the experience, it’s essential to ease yourself into running slowly and increase your pace and distance gradually over several outings.
Start each run with a gentle warm-up of at least five minutes. This can include quick walking, marching on the spot, knee lifts, side stepping and climbing stairs.
Start walking for an amount of time that feels comfortable.
When you first start out, try alternating between running and walking during your session.
As time goes on, make the running intervals longer until you no longer feel the need to walk.
Regular running for beginners means getting out at least twice a week. Your running will improve as your body adapts to the consistent training stimulus.
It’s better to run twice a week, every week, than to run six times one week and then do no running for the next three weeks.
Stretching and flexibility
As a general rule, stretch your major muscle groups after you exercise. In some studies, stretching right before an athletic event has been shown to decrease athletic performance, especially before activities requiring ballistic movements, jumping or running.
Overall, however, stretching after exercise can help you to optimize your joint range of motion. If you don’t exercise regularly, you may want to stretch a few times a week after a brief warmup to maintain flexibility.
When you’re stretching, keep it gentle. Breathe freely as you hold each stretch for around 30 seconds. Try not to hold your breath. Don’t bounce or hold a painful stretch. Expect to feel tension while you’re stretching. If you feel pain, you’ve gone too far.
Keep your head straight
Look straight ahead of you, about 30 to 40 meters out in front, and avoid looking down at your feet. Looking down will create tension in your neck and shoulders. Keep your jaw and neck relaxed.
Don’t hunch your shoulders
Your shoulders should be back and down. Keep them relaxed and avoid tensing them. Don’t hunch over as this restricts breathing, allowing less oxygen to get to the muscles.
Keep your hands relaxed
Your hands should be relaxed, but don’t let them flop. Tight hands can cause tension all the way up to the back and shoulders.
Keep your arms at 90 degrees
Your arms should be bent at a 90-degree angle. Try to swing them forward and back, not across your body. The arm movement helps to propel you forward, so swinging them sideways is a waste of energy.
Lean forward while running
Don’t bend forward or backward from the waist as this places pressure on the hips. Some experts advise running in an upright position, but Phillips believes using your body weight to lean forward a bit while running can reduce heel strike and help you land on the middle of your foot.
Keep your hips stable
Your hips should remain stable and forward-facing. Don’t stick your bottom out or rock your hips from side to side. Keeping this position in your hips can help prevent low back and hip pain.
Don’t lift your knees too high
Land with a slight bend in the knee. This helps to absorb the impact of running on hard surfaces. Don’t lift your knees too high and avoid bouncing up and down. Your knees should be lifting forwards rather than upwards.
Aim for a mid-foot strike
Landing on the middle of your foot is the safest way to land for most recreational runners. Avoid striking the ground with your heel or your forefoot first. Your foot should land below your hips – not out in front of you.
Don’t strike the ground heavily
Aim for short light steps. Good running is light and quiet. Whatever your weight, your feet should not slap loudly as they hit the ground. Light steps are more efficient and cause less stress to the body.
Breathe deeply and rhythmically
Whether you breathe through your nose or mouth, try to breathe deeply and rhythmically. Avoid shallow and quick breaths. Try to aim for one breath for every two strides, but don’t be afraid to try longer breathing.
What if I’m not very active?
If you’re not very active but are able to walk, increase your walking distance gradually.
If your joints are a problem, check whether your local swimming pool holds exercise classes.
The water helps to support your joints while you move, and once you lose a bit of weight, the pressure on your joints will reduce.
If you’re not active because of a medical condition, get advice on exercising with a disability.
How to stretch after a run
Give yourself a few minutes to cool down after each run by walking and a doing few stretches.
Performing stretching exercises after a run will help you cool down gradually and improve your flexibility.
These stretches are best done after exercising, when your muscles are warm and more elastic.
Breathe deeply and regularly during the stretches. Aim to stretch to the point of feeling tightness or slight discomfort.
You shouldn’t feel any pain when doing these exercises. If you do, stop and seek medical advice.
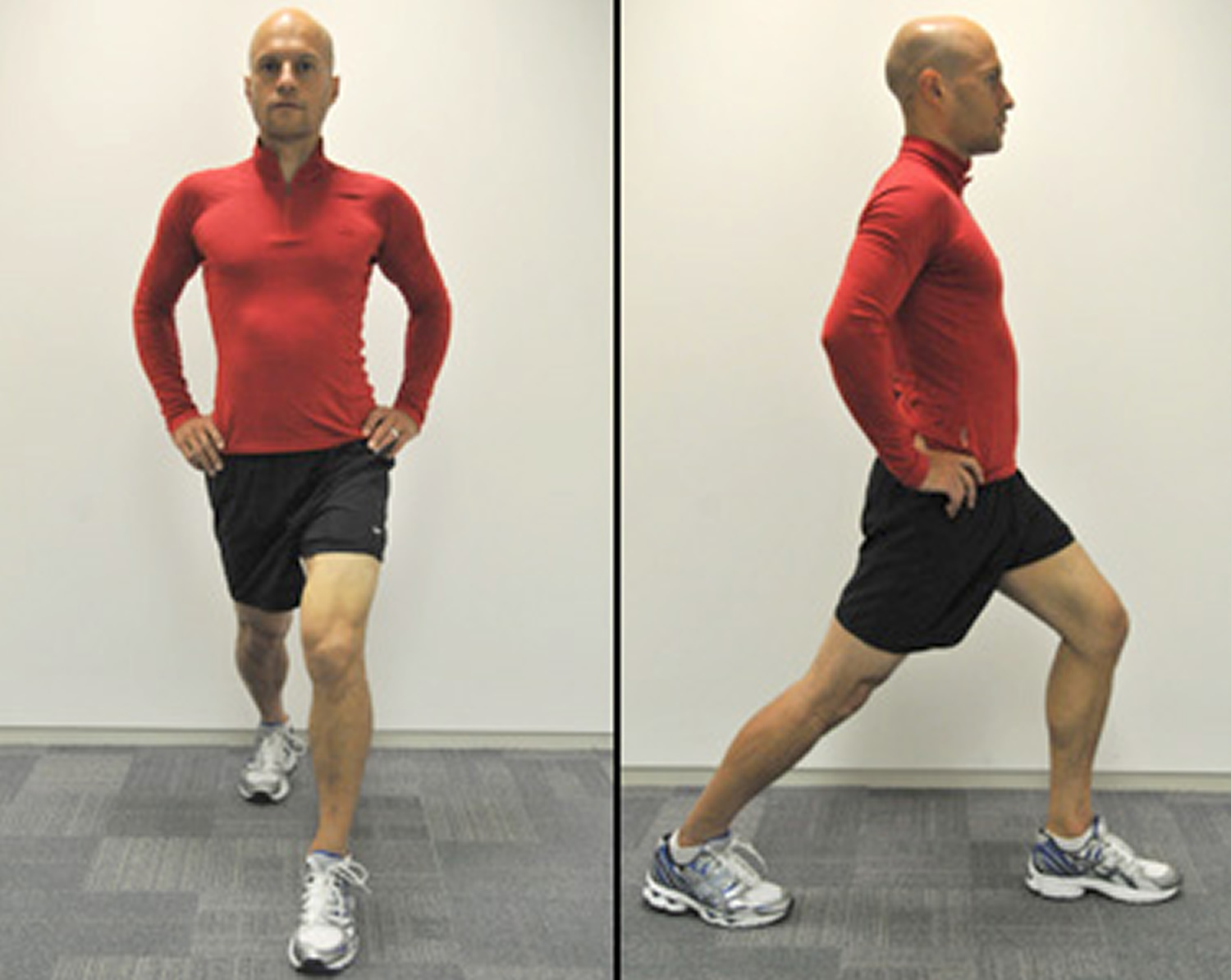
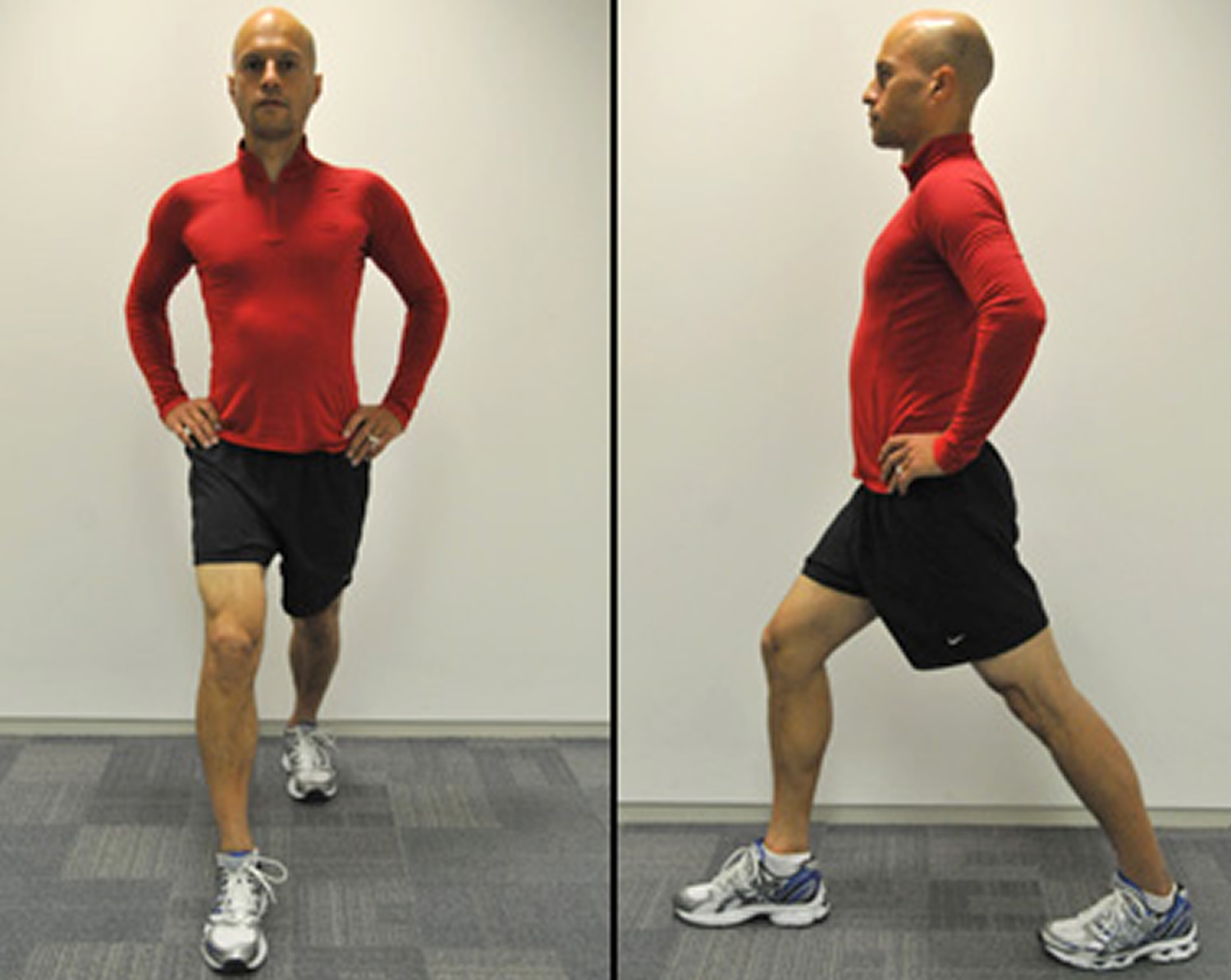
Hip flexor stretch
Step your left leg forward, keeping both feet pointing straight ahead. Keeping your back leg straight and avoiding sticking your buttock out and arching your back, slowly bend your front leg and push your right buttock forward until you feel a stretch across the front of your right hip joint – hold for 15 seconds. Repeat with the other leg.
Figure 1. Hip flexor stretch
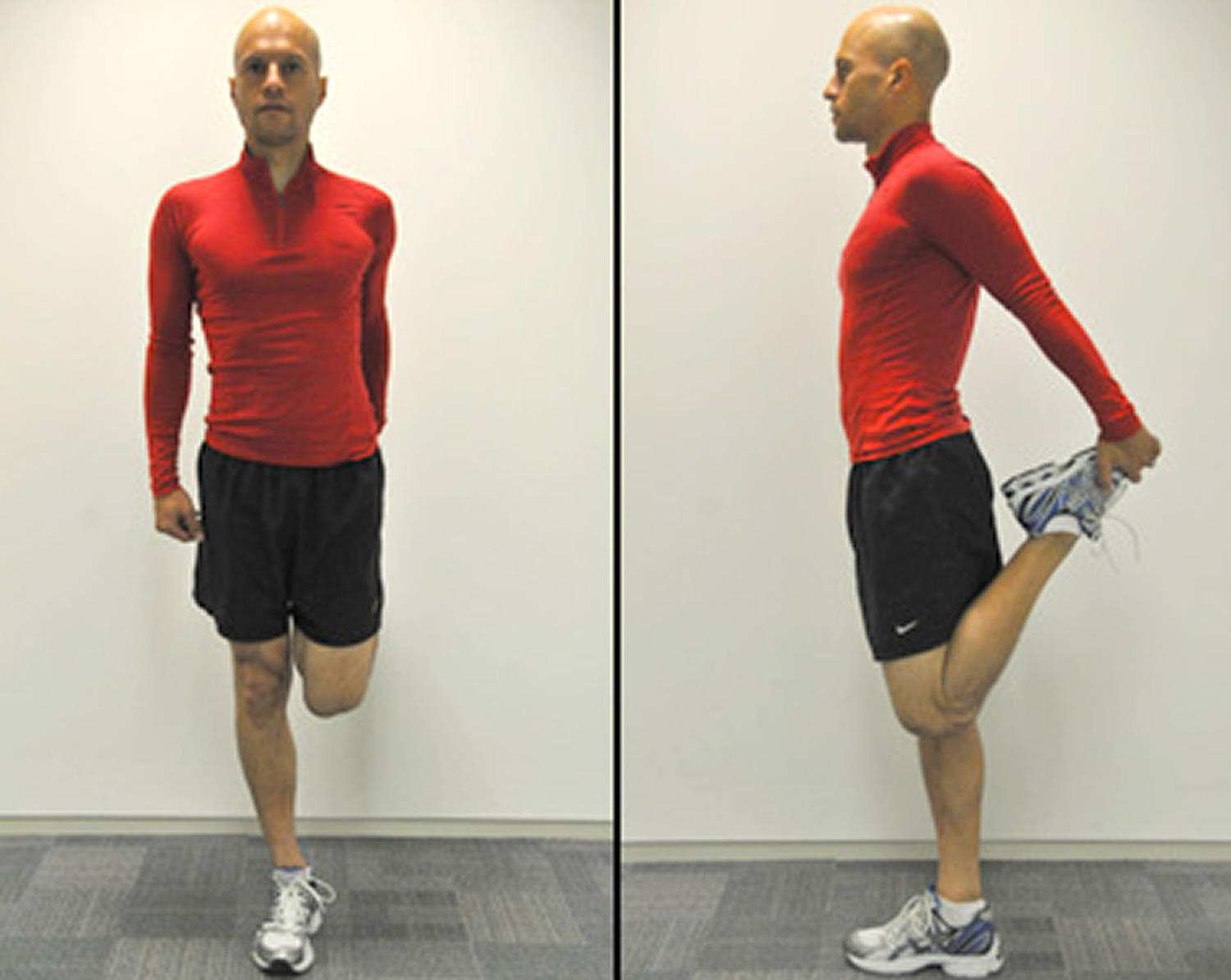
Thigh stretch
Grab the top of your left foot behind you and gently pull your heel towards your left buttock to stretch the front of the thigh, keeping the knees touching – hold for 15 seconds. Avoid leaning forwards or to the side. Repeat with the other leg.
Tip: place a hand on a wall or bench for balance
Figure 2. Thigh stretch
Hamstring stretch
Stand with your right leg just in front of the other and your hands on your hips. Keeping your right leg straight and toes pointing up, bend your left leg. Bend towards your right leg, keeping your back straight – hold for 15 seconds. Repeat with the other leg.
Figure 3. Hamstring stretch

Iliotibial band stretch
To stretch your right iliotibial band, cross your right leg behind your left leg. Keeping both feet on the ground, lean to your left side and push your right hip outwards – hold for 15 seconds. Don’t bend forward or stick your buttocks out. You should feel the stretch along your outer right thigh and hip. Repeat with the other leg.
Figure 4. Iliotibial band stretch

Calf stretch
Step your right leg forward. Bend your front leg and keep your back leg straight. Both feet should point forwards. Push your left heel into the ground, keeping your left leg straight. You should feel the stretch at the back of your left leg, below the knee – hold for 15 seconds. Repeat with the other leg.
Figure 5. Calf stretch
Lower back stretch
Lie on your back with both feet flat. Pull your right knee to your chest until you feel a stretch in your lower back. Hold for up to 15 seconds and repeat with the left leg. Then pull both knees to your chest and hold for up to 15 seconds.
Figure 6. Lower back stretch

Buttock stretch
Lie on your back with your knees bent and both feet flat on the floor. Cross your right leg over your left thigh. Grasp the back of your left thigh with both hands and pull the left leg toward your chest – hold for 15 seconds. Repeat with the other leg.
Figure 7. Buttock stretch

Running potential problems and when to seek the help
Pain is the body’s way of letting you know something is wrong. Listen to your body and act on it.
Running can cause normal aches and pains. Something called Delayed Onset Muscle Soreness (DOMS) is a normal response from muscles repairing themselves after running. This typically occurs one to two days after a running session, and only lasts a couple of days. An injury is typically something that does not go away and causes you to stop or reduce your training.
The most common injuries for runners are listed below:
Pain at the front of the knee
Referrered to as Patellofemoral pain syndrome this is pain in and/or around the front of the knee or knee cap. This typically is worse with repeated bending of the knee (i.e., running) and going up or down stairs. The knee pain is typically non-specific with little or no swelling.
Pain typically on the outside of the knee
Referred to as Iliotibial band friction syndrome (ITBFS), this is typically an overuse injury with a tightening of the band of tissue which runs down the outside of the thigh and inserts into the outside of the knee. Pain typically occurs as the foot hits the ground when running, due to the increased angle of the leg.
Achilles Tendon pain
Achilles Tendinopathy is another overuse injury, involving the tendon at the back of the leg and foot. This can either have a gradual onset or become painful after a particularly gruelling session. Early treatment is ideal with Ice, Compression and Elevation (ICE), addressing any mechanical abnormalities that are present, leading on to a strengthening programme.
Shin splints
Known as Medial Tibial Stress Syndrome (MTSS), this a pain that occurs either in the front or inside of the shin which typically improves once you have warmed up and then is painful the following morning after exercise. A mechanical cause in relation to lower leg alignment can be a big influence in shin pain, and this should be addressed.
Heel pain
Otherwise known as Plantar fasciitis, this usually happens on standing up first thing in the morning or after a period of rest. This improves as you warm up but then gets worse the more activity you do. Podiatrists are in an ideal position to treat this, as orthoses can reduce the stress on the band of tissue under the foot.
Foot Blisters
Foot blisters are painful, fluid-filled lesions produced by friction and pressure. They can be caused by the following:
- Ill-fitting shoes.
- Stiff shoes.
- Wrinkled socks against the skin.
- Excessive moisture.
- Foot deformities.
How to prevent foot blisters
- Keep your feet dry.
- Always wear socks as a cushion between your feet and shoes.
- Wear properly fitting shoes.
If a blister does occur, do not pop it. Cut a hole in a 1.5”piece of foam or felt, forming a ‘doughnut’ over the blister; tape the foam or felt in place or cover with a soft gel-type dressing. Treat an open blister with mild soap and water; cover it with an antiseptic ointment and protective soft gel dressing to prevent infection and speed up the healing process
All of the above injuries need treatment
If you think you have one of the above problems you should consult a podiatrist or an orthopedic surgeon. The podiatrist can also assess your ‘mechanics’ – the way you run or walk and offer advice, stretches or exercises to aid performance and prevent injury in the future. They will also assess the need for orthoses, which are special inserts that go inside your shoe to address abnormalities in the way your foot works.
Staying motivated
Set yourself a goal
Whatever your level, setting challenges is useful to stay motivated. Training for a race, such as a 5K, or a charity run is a good way to keep going.
Run with a friend
It really helps to have someone about the same level of ability as you to run with. You’ll encourage each other when you’re not so keen to run. You’ll feel you don’t want to let your running partner down, and this will help motivate you.
Mix it up
Keep your running interesting by adding variety. Running the same route over and over again can become boring. Vary your distances, pace and routes.
Join a club
A running club is the perfect way to commit to running regularly. Most clubs have running groups for different levels, including beginners. Clubs are also a great way to find running partners to run with outside of club sessions.
Interval running for weight loss
An interval training workout involves alternating periods of high-intensity effort with periods of low-intensity effort, which is called the recovery. For runners, this would typically involve interspersing bouts of fast running with slower running.
The long-term health benefits from interval training are similar to those achieved from most types of longer-duration, moderate-intensity aerobic exercise, namely a lower risk of many chronic diseases, such as heart disease, type 2 diabetes, stroke and some cancers.
Interval training is also one of the best techniques for runners to improve their speed. Alternating bursts of fast running with a recovery period trains your muscles to work more efficiently and economically at higher speeds. Another benefit is that your routine moderately paced runs will feel easier.
Can interval training help me lose weight?
During the high-intensity phase, your body burns mainly carbs for energy, but during the recovery, your body burns mainly fat to produce the energy needed to help your body recover from the intense effort. This process can continue for hours after training, which can help you lose weight, as long as you’re also eating healthily.
There is growing evidence to support the notion that interval training might be as effective, if not more so, than longer, moderate-intensity aerobic workouts.
Researchers at McMaster University in Canada found that three 20-minute sessions of interval training a week provided the same benefits as 10 hours of steady exercise over a two-week period.
How often should I do interval training?
You shouldn’t be doing interval training every day. Intervals are hard work and you need to give your body time to recover. If you don’t, you’re likely to lose motivation, tire yourself out and possibly injure yourself.
The recovery phase is a really important part of interval training. The stop-and-start pattern trains your body to recover quickly between bursts of faster running, which, over time, will gradually increase your ability to run faster for longer.
If you’re used to running three days a week, you could set aside one of those runs for an interval training session.
Is interval training safe?
Interval training is hard work on the whole body, but particularly the heart, lungs and muscles. If you’re out of shape or you’ve not exercised for a while, you should get the all-clear from your doctor before starting.
It is generally advisable to have a good level of overall aerobic fitness before performing high-intensity training of any kind.
Running in winter
With the shorter and colder days, lacing up for a run might be the last thing you feel like doing. But don’t let the winter weather stop you from being physically active and keeping fit.
Try the following tips to help you stay safe and motivated when you’re running in colder weather.
What to wear
Dressing appropriately for the weather conditions will help ensure you enjoy your run.
Consider wearing lightweight layers of breathable clothing, known as the layer system.
The layer system works well for keeping you warm and any layer can be removed as conditions change during your run.
When choosing your layers, remember your body heats up during exercise. You should be slightly cool when you start your run.
For example, depending on the weather, a layer system could consist of:
- A base layer: the first layer, such as a breathable synthetic fabric to draw the sweat away from your skin.
- A mid layer: such as a fleece to keep the warmth in and remove any moisture from the base layer.
- An outer layer: such as a light water-resistant jacket: to expel moisture and protect you from the wind and rain.
Use any zips and air vents to help regulate your body temperature to stay comfortable during your run.
Avoid running in cotton tops. Cotton soaks up moisture and takes time to dry and may make you feel cold.
A pair of leggings or running tights underneath a pair of shorts, or some tracksuit bottoms will keep your legs warm.
A pair of gloves and a hat or fleece headband are a good idea to stop you losing heat from your head and hands.
Stay safe – be seen
If you go running before or after work during the winter, it’s likely you’ll be running in the dark.
When running after dark, it’s essential that you’re visible to other people, particularly motorists.
Your clothes should be reflective or a bright, light color, such as white or fluorescent yellow. Don’t wear dark clothes as drivers may not see you.
Most good running brands make clothes that feature reflective strips.
A fluorescent bib that can be worn over your running clothes is also perfect for running after dark.
Stick to well-lit areas and avoid running anywhere you don’t feel completely safe.
Warm up and cool down
Easing into your run is a good way to warm-up, especially in cold weather.
Start slowly with some very gentle running or even walking to ready the muscles for exercise.
Gradually increase your pace until, after around 10 minutes, you get to the pace you’re going to maintain for most of the run.
Don’t stop after your warm-up to stretch. That will cool your muscles down again.
To cool down, reduce your pace or walk for five to ten minutes. This will help your body recover after your run.
Don’t stop and stretch outside or you could get too cold. Do some stretches indoors instead.
Running with a cold or asthma
Colds are more common in winter, but you don’t necessarily have to stop running if you’re feeling under the weather.
Use common sense and listen to your body. If your symptoms are not severe and you generally feel OK, then you can go running. If you feel absolutely rotten, then it’s best not to go.
However, it’s important not to run if you have a fever. A fever is when your body’s temperature is 38 °C (100.4 °F) or above and is rarely a symptom of a cold. If you run with a fever, it’ll make you feel worse. In very rare cases, running with a fever can lead to the virus affecting your heart, which can be dangerous.
If you have asthma, take extra care when running in winter as cold air can trigger symptoms. Doctors recommend using your inhaler before you go running and taking it with you when you run.
Running schedule for weight loss
When you’re designing your personal running schedule, it’s very important that you consider your fitness and weight loss goals, because without a goal you’ll never have a target and you’ll never know when you’ve achieved those goals. By planning carefully and pacing yourself, you can make fitness a healthy habit that lasts a lifetime.
Plan your runs. Work out when and where (the exact route and time) you’re going to run and put it in your diary. That way, it won’t slip your mind.
7-week training schedule for running beginners
Doing a 5K (3.1 miles) run can add a new level of challenge and interest to your exercise program. Don’t be daunted by the distance. A 5K run is a great distance for a beginner. You can prepare for a 5K run in just two months.
Consider using this seven-week 5K run training schedule as your guide. This 5K run training schedule was created by Olympian Jeff Galloway 24. It’s tailored for beginners or anyone who wants to complete a 5K race. You don’t have to use this training schedule only for a 5K run. You can also adapt it for a 5K walk.
How to use the 5K training schedule
This 5K training schedule incorporates a mix of running, walking and resting. This combination helps reduce the risk of injury, stress and fatigue while boosting your enjoyment of physical activity. Remember, you can run or walk slowly to help your body adjust to this 5K training schedule.
Under this 5K run training schedule, you’ll spend a portion of your time walking. For instance, during week one on run/walk days, you’ll run for 15 seconds and then walk for 45 seconds, repeating that cycle for 30 minutes.
As the weeks progress, you’ll gradually increase the amount of time running and reduce the amount of time walking. If you’re adapting the training for a 5K walk, then you always walk, even on run/walk days.
One day a week, which is Friday on this 5K schedule, is a day of rest from exercise, giving your muscles time to recover. On Sunday, you can either take a second day of rest, or you can enjoy a walk at your choice of distance. On this 5K run training schedule, race day falls on Saturday of your seventh week.
Figure 8. Running schedule for weight loss
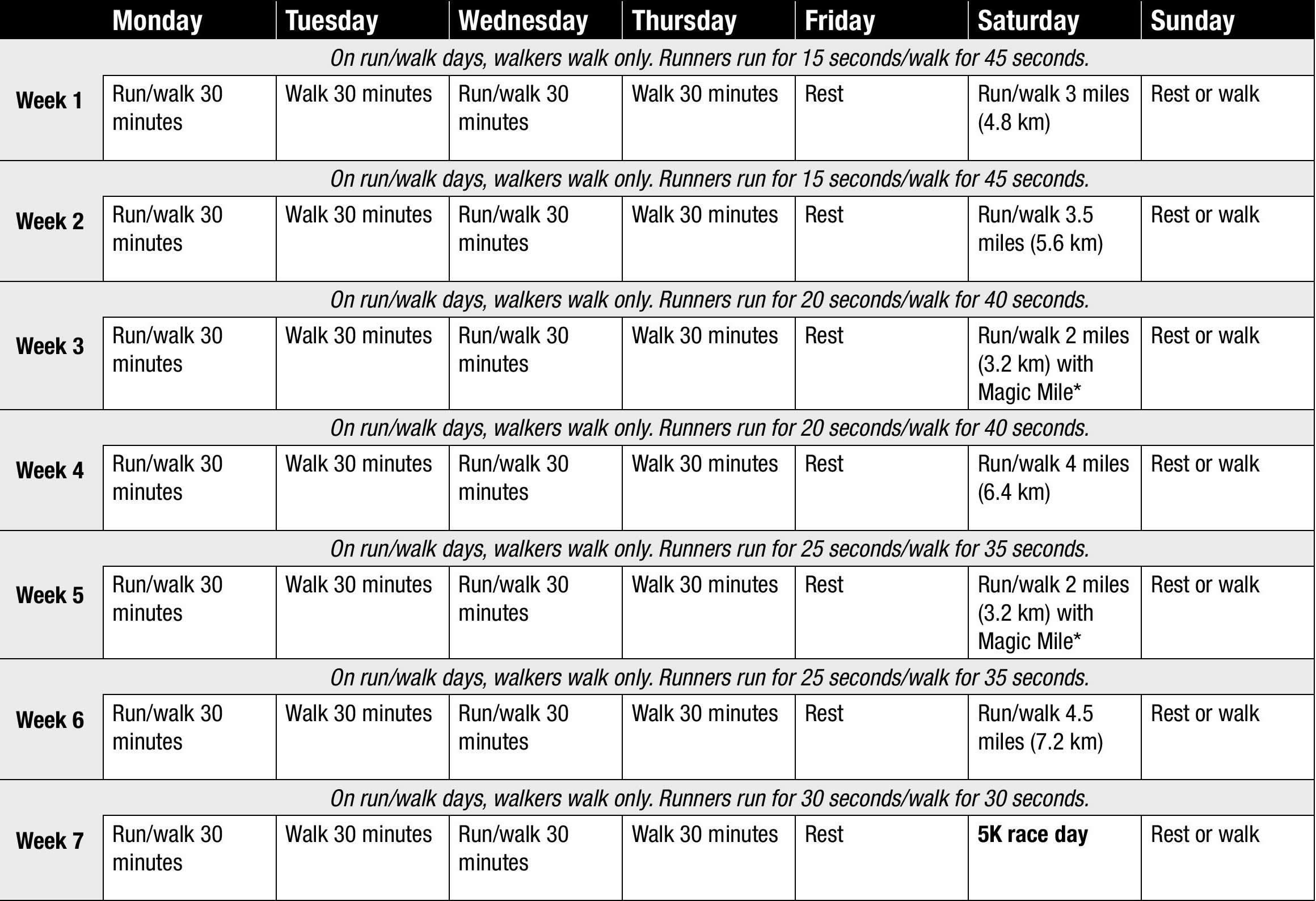
Note: *The Magic Mile is a training tool designed to help you find a realistic race pace. On the first Magic Mile, warm up as usual and then run or walk one mile (1.6 km) slightly faster than your normal pace. Time your one-mile run/walk with a stopwatch. Run or walk easily the rest of the distance assigned for the day. On each successive Magic Mile, warm up as usual and then try to beat your previous one-mile run/walk time. Your 5K race pace should be one to two minutes slower than your fastest Magic Mile time.
Week 1 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 15 seconds/walk for 45 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | Run/walk 3 miles (4.8 km) |
| Sunday | Rest or walk |
Week 2 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 15 seconds/walk for 45 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | Run/walk 3.5 miles (5.6 km) |
| Sunday | Rest or walk |
Week 3 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 20 seconds/walk for 40 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | Run/walk 2 miles (3.2 km) with Magic Mile* |
| Sunday | Rest or walk |
Week 4 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 20 seconds/walk for 40 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | Run/walk 4 miles (6.4 km) |
| Sunday | Rest or walk |
Week 5 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 25 seconds/walk for 35 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | Run/walk 2 miles (3.2 km) with Magic Mile* |
| Sunday | Rest or walk |
Week 6 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 25 seconds/walk for 35 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | Run/walk 4.5 miles (7.2 km) |
| Sunday | Rest or walk |
Week 7 – Running schedule for weight loss
On run/walk days, walkers walk only. Runners run for 30 seconds/walk for 30 seconds.
| Monday | Run/walk 30 minutes |
| Tuesday | Walk 30 minutes |
| Wednesday | Run/walk 30 minutes |
| Thursday | Walk 30 minutes |
| Friday | Rest |
| Saturday | 5K race day |
| Sunday | Rest or walk |
9-week training schedule for running beginners
Couch to 5K
Couch to 5K is a running plan for absolute beginners. It was developed by a new runner, Josh Clark, who wanted to help his fifty-something mum get off the couch and start running, too.
The plan involves 3 runs a week, with a day of rest in between, and a different schedule for each of the 9 weeks.
Couch to 5K is for everyone. Whether you’ve never run before or if you just want to get more active, Couch to 5K is a free and easy way of getting fitter and healthier.
If you have any health concerns about beginning an exercise regime like Couch to 5K, make an appointment to see your doctor and discuss it with them first.
How does Couch to 5K work?
Probably the biggest challenge a new runner faces is not knowing how or where to start.
Often when trying to get into exercise, we can overdo it, feel defeated and give up when we’re just getting started.
Couch to 5K works because it starts with a mix of running and walking to gradually build up your fitness and stamina.
Week 1 involves running for just a minute at a time, creating realistic expectations and making the challenge feel achievable right from the start.
How do I get started on the Couch to 5K?
1. Download the free Couch to 5K podcasts to your mobile device or computer. If downloading to a computer, you’ll then need to copy the podcast on to your mobile device.
The podcasts feature a narrator, Laura, who guides you through the session, explaining when you need to run and when it’s time to walk.
Download the Couch to 5K Podcasts (get your free copy here https://www.nhs.uk/LiveWell/c25k/Pages/couch-to-5k.aspx or at iTunes https://itunes.apple.com/gb/podcast/nhs-couch-to-5k/id394384987)
Week 1 Podcast:
For the runs in Week 1, you will begin with a brisk 5-minute warm-up walk, then you will alternate 60 seconds of running, with 90 seconds of walking, for a total of 20 minutes.
Week 2 Podcast:
For the runs in Week 2, you will begin with a brisk 5-minute warm-up walk then you will alternate 90 seconds of running, with 2 minutes of walking, for a total of 20 minutes.
Week 3 Podcast:
For the runs in Week 3, you will begin with brisk 5-minute warm-up walk followed by 2 repetitions of the following; 90 seconds of running, 90 seconds of walking, 3 minutes of running, 3 minutes of walking.
Week 4 Podcast:
For the runs in Week 4, you will begin with a brisk 5-minute warm-up walk then 3 minutes of running, 90 seconds walking, 5 minutes running, 2 ½ minutes walking, 3 minutes running, 90 seconds walking, 5 minutes running.
Week 5 Podcast:
There are three different workouts for this week. They are as follows:
- Run 1: brisk 5-minute warm-up walk, then 5 minutes running, 3 minutes walking, 5 minutes running, 3 minutes walking, 5 minutes running.
- Run 2: brisk 5-minute warm-up walk, then 8 minutes running, 5 minutes walking, 8 minutes running.
- Run 3: brisk 5-minute warm-up walk, then 20 minutes running, with no walking.
Week 6 Podcast:
As with Week 5, there are three different runs for this week.
- Run 1: brisk 5-minute warm-up walk, then 5 minutes running, 3 minutes walking, 8 minutes running, 3 minutes walking, 5 minutes running.
- Run 2: brisk 5-minute warm-up walk, then 10 minutes running, 3 minutes walking, 10 minutes running
- Run 3: brisk 5-minute warm-up walk, then 25 minutes with no walking.
Week 7 Podcast:
For the runs in Week 7, you will begin with a brisk 5-minute warm-up walk then 25 minutes of running.
From now on, the plan gets you used to running for solid blocks of time, without the distraction of walking intervals.
Week 8 Podcast:
For the runs in Week 8, you will begin with a brisk 5-minute warm-up walk then 28 minutes of running.
By now, you should be getting comfortable with the longer runs but you still need to concentrate on completing the 28 minutes without going too fast.
Week 9 Podcast:
For the runs in Week 9, you will begin with a brisk 5-minute warm-up walk then 30 minutes of running.
You’ve nearly reached the end of your programme and you’ve made some great progress. This is the week when you can reach your goal. Well done!
2. When will you run? The best way to ensure you stick with your running plan is to carefully work out how to fit Couch to 5K into your day.
3. Plan your route. You may want to look at a map to plan your route first so you can focus on running. There are lots of great websites out there to help you with this.
4. Think about safety. If you’re planning to run outdoors, bear in mind that you may be less aware of your surroundings if you’re wearing headphones. Watch out for other pedestrians, cyclists and vehicles. When running in the dark, make sure you can see where you’re going and that other road users can see you. Consider running along routes with adequate lighting or wearing reflective clothing.
5. What gear? The most essential piece of kit is a pair of running trainers.
Tips on progression
The Couch to 5K running plan for beginners is designed for beginners to gradually build up their running ability so they can eventually run 5km without stopping.
The pace of the nine-week running plan has been tried and tested by thousands of new runners.
You can, however, repeat any one of the weeks until you feel physically ready to move on to the next podcast.
Structure is important for motivation, so try to allocate specific days of the week for your runs and stick to them.
Rest days
Rest days are critical. Having one between each week’s runs will reduce your chance of injury and also make you a stronger, better runner.
Resting allows your joints to recover from what is a high-impact exercise, and your running muscles to repair and strengthen.
Alternatively, you could do Strength and Flex on your rest days. This is a five-week plan designed to improve your strength and flexibility, which will help your running.
Strength and Flex exercise plan
The Strength and Flex five-week plan consists of a series of equipment-free exercises designed to improve your strength and flexibility.
The workout instructions and pace are easy to follow to ensure you perform each exercise correctly and in time.
You can easily combine Strength and Flex with your Couch to 5K running plan, by following the plans on alternate days of the week.
Strength and Flex will help you achieve your recommended two weekly sessions of strength exercises.
Strength and Flex features:
- Equipment-free
- Easy to follow
- Full body workout
- How-to video clips
- Use anywhere, anytime
- Can be used with Couch to 5K
Starting with Strength and Flex Week 1, your goal is to work your way up to Week 5 in five weeks. To achieve this, you need to do each podcast at least three times in a week.
By Week 5, you’ll be doing back, arm and leg stretches along with press-ups and squats with ease. You’ll be feeling stronger, more flexible and full of energy to go about your daily life.
You can do these full body workouts anywhere and any time you choose. They can be done indoors or out in the park or garden, on your own or with a friend.
All you need is enough space to walk about freely, a fixed bench, a wall and either some shoulder-height railings or a shoulder-height horizontal bar.
Week 1 of Strength and Flex
A gentle workout starting with a warm-up followed by a series of strength and flexibility exercises, finishing off with a cool down. Duration: 35:28
Week 2 of Strength and Flex
In week 2 some of the podcast week 1 exercises have been made a bit more challenging and the duration of your workout increased. Duration: 36:31
Week 3 of Strength and Flex
In week 3 some new moves have been added and the difficulty level of some of the podcast week 2 exercises increased. Duration: 35:32
Week 4 of Strength and Flex
In week 4 some new exercises have been added and the intensity stepped up as well as the length of your workout. Duration: 45:12
Week 5 of Strength and Flex
Week 5 exercises are more challenging than previous week to give you the definitive strength and flexibility workout. Duration: 43:32
Beyond week 5 of Strength and Flex
Once you’ve completed week 5, download the ‘without intro’ version for ongoing use, beyond the end of the programme. Duration: 41:38
- Wareham NJ, van Sluijs EM, Ekelund U. Physical activity and obesity prevention: a review of the current evidence. Proc Nutr Soc. 2005; 64:229-47. https://www.ncbi.nlm.nih.gov/pubmed/15960868[↩]
- Seo DC, Li K. Leisure-time physical activity dose-response effects on obesity among US adults: results from the 1999-2006 National Health and Nutrition Examination Survey. J Epidemiol Community Health. 2010; 64:426-31. http://jech.bmj.com/content/64/5/426.long[↩]
- Lewis CE, Smith DE, Wallace DD, Williams OD, Bild DE, Jacobs DR, Jr. Seven-year trends in body weight and associations with lifestyle and behavioral characteristics in black and white young adults: the CARDIA study. Am J Public Health. 1997; 87:635-42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1380845/pdf/amjph00503-0109.pdf[↩]
- Lee IM, Djousse L, Sesso HD, Wang L, Buring JE. Physical activity and weight gain prevention. JAMA. 2010; 303:1173-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2846540/[↩]
- Lusk AC, Mekary RA, Feskanich D, Willett WC. Bicycle riding, walking, and weight gain in premenopausal women. Arch Intern Med. 2010; 170:1050-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3119355/[↩]
- Mekary RA, Feskanich D, Malspeis S, Hu FB, Willett WC, Field AE. Physical activity patterns and prevention of weight gain in premenopausal women. Int J Obes (Lond). 2009; 33:1039-47. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2746452/[↩]
- Mekary RA, Feskanich D, Hu FB, Willett WC, Field AE. Physical activity in relation to long-term maintenance after intentional weight loss in premenopausal women. Obesity (Silver Spring, Md). 2010;18(1):167-174. doi:10.1038/oby.2009.170. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2798010/[↩]
- U.S. Dept. of Health and Human Services. 2008 Physical Activity Guidelines for Americans; 2008. https://health.gov/paguidelines/[↩]
- Slentz CA, Aiken LB, Houmard JA, et al. Inactivity, exercise, and visceral fat. STRRIDE: a randomized, controlled study of exercise intensity and amount. J Appl Physiol. 2005; 99:1613-8. https://www.physiology.org/doi/pdf/10.1152/japplphysiol.00124.2005[↩][↩][↩]
- McTiernan A, Sorensen B, Irwin ML, et al. Exercise effect on weight and body fat in men and women. Obesity (Silver Spring). 2007; 15:1496-512. https://onlinelibrary.wiley.com/doi/pdf/10.1038/oby.2007.178[↩]
- Friedenreich CM, Woolcott CG, McTiernan A, et al. Adiposity changes after a 1-year aerobic exercise intervention among postmenopausal women: a randomized controlled trial. Int J Obes (Lond). 2010. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3061001/[↩][↩]
- Sallis JF, Glanz K. Physical activity and food environments: solutions to the obesity epidemic. Milbank Q. 2009; 87:123-54. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2879180/[↩]
- Physical Activity Guidelines for Americans. https://health.gov/paguidelines/[↩][↩][↩][↩][↩][↩][↩][↩]
- Lee, I.M., et al., Physical activity and weight gain prevention. JAMA, 2010. 303(12): p. 1173-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2846540/[↩][↩]
- Jakicic, J.M., et al., Effect of exercise duration and intensity on weight loss in overweight, sedentary women: a randomized trial. JAMA, 2003. 290(10): p. 1323-30. https://www.ncbi.nlm.nih.gov/pubmed/12966123[↩]
- Williams, M.A., et al., Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation, 2007. 116(5): p. 572-84. http://circ.ahajournals.org/content/116/5/572.long[↩][↩]
- Schmitz, K.H., et al., Strength training and adiposity in premenopausal women: strong, healthy, and empowered study. Am J Clin Nutr, 2007. 86(3): p. 566-72. https://www.ncbi.nlm.nih.gov/pubmed/17823418[↩]
- Engelke, K., et al., Exercise maintains bone density at spine and hip EFOPS: a 3-year longitudinal study in early postmenopausal women. Osteoporos Int, 2006. 17(1): p. 133-42.[↩]
- Ling, C.H., et al., Handgrip strength and mortality in the oldest old population: the Leiden 85-plus study. CMAJ, 2010. 182(5): p. 429-35. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2842834[↩]
- Ruiz, J.R., et al., Association between muscular strength and mortality in men: prospective cohort study. BMJ, 2008. 337: p. a439. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2453303/[↩]
- Bolam, K.A., J.G. van Uffelen, and D.R. Taaffe, The effect of physical exercise on bone density in middle-aged and older men: A systematic review. Osteoporos Int, 2013. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0055053/[↩][↩]
- Nelson, M.E., et al., Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation, 2007. 116(9): p. 1094-105. http://circ.ahajournals.org/content/116/9/1094.long[↩][↩]
- The Research Group in Breast Health. http://www.port.ac.uk/department-of-sport-and-exercise-science/research/breast-health/[↩][↩][↩][↩]
- Galloway J. Galloway’s 5K/10K Running. 2nd. ed. Aachen, Germany: Meyer & Meyer Sport; 2008.[↩]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}