
Contents
- What is Charcot Marie Tooth disease
- The peripheral nervous system
- Charcot Marie Tooth Types
- Charcot Marie Tooth Disease Complications
- Charcot Marie Tooth disease causes
- Charcot Marie Tooth disease symptoms
- Charcot Marie Tooth diagnosis
- Charcot Marie Tooth treatment
What is Charcot Marie Tooth disease
Charcot-Marie-Tooth disease is a group of inherited progressive disorders that affect the peripheral nerves. The peripheral nerves are found outside the main central nervous system (brain and spinal cord). They control the muscles and relay sensory information, such as the sense of touch, pain, heat, and sound from the limbs to the brain. Damage to the peripheral nerves can result in loss of sensation and wasting (atrophy) of muscles in the feet, legs, and hands. Charcot-Marie-Tooth disease is also known as hereditary motor and sensory neuropathy.
Discovered in 1886 by three physicians, Jean-Martin Charcot, Pierre Marie, and Howard Henry Tooth, Charcot Marie Tooth affects an estimated 2.8 million people worldwide.
Charcot-Marie-Tooth syndrome is the most common inherited disorder that involves the peripheral nerves, affecting an estimated 150,000 people in the United States. It occurs in populations worldwide with a prevalence of about 1 in 2,500 individuals.
Charcot-Marie-Tooth disease usually start to appear between the ages of five and 15 or early adulthood, but onset may occur anytime from early childhood through late adulthood. Symptoms of Charcot-Marie-Tooth disease vary in severity, even among members of the same family. Some people never realize they have the disorder, but most have a moderate amount of physical disability. A small percentage of people experience severe weakness or other problems which, in rare cases, can be life-threatening.
Charcot-Marie-Tooth life expectancy
- In most affected individuals, Charcot-Marie-Tooth disease does not affect life expectancy, but can cause severe disability.
People with Charcot-Marie-Tooth syndrome may have:
- muscle weakness in the feet, ankles, legs and hands
- an awkward way of walking (gait)
- highly arched or very flat feet
- numbness in the feet, arms and hands
Typically, the earliest symptoms of Charcot-Marie-Tooth disease involve balance difficulties, clumsiness, and muscle weakness in the feet. Affected individuals may have foot abnormalities such as high arches (pes cavus), flat feet (pes planus), or curled toes (hammer toes). They often have difficulty flexing the foot or walking on the heel of the foot. These difficulties may cause a higher than normal step (or gait) and increase the risk of ankle injuries and tripping.
Charcot-Marie-Tooth syndrome is a progressive condition. This means the symptoms slowly get worse, making everyday tasks increasingly difficult.
As the disease progresses, muscles in the lower legs usually weaken, but leg and foot problems rarely require the use of a wheelchair. Affected individuals may also develop weakness in the hands, causing difficulty with daily activities such as writing, fastening buttons, and turning doorknobs. People with this disorder typically experience a decreased sensitivity to touch, heat, and cold in the feet and lower legs, but occasionally feel aching or burning sensations. In some cases, affected individuals experience gradual hearing loss, deafness, or loss of vision.
There are many different types of Charcot Marie Tooth that are all caused by different mutations (changes) in your genes:
- Type 1 Charcot-Marie-Tooth disease (CMT1) is characterized by abnormalities in myelin, the fatty substance that covers nerve cells, protecting them and helping to conduct nerve impulses. These abnormalities slow the transmission of nerve impulses.
- Type 2 Charcot-Marie-Tooth disease (CMT2) is characterized by abnormalities in the fiber, or axon, that extends from a nerve cell body and transmits nerve impulses. These abnormalities reduce the strength of the nerve impulse.
- Type 3 Charcot-Marie-Tooth disease (Dejerine-Sottas syndrome) – a rare and severe type of Charcot Marie Tooth that affects the myelin sheath, causing severe muscle weakness and sensory problems to begin developing in early childhood
- Type 4 Charcot-Marie-Tooth disease (CMT4) affects either the axon or myelin and is distinguished from the other types by its pattern of inheritance.
- In intermediate forms of Charcot-Marie-Tooth disease, the nerve impulses are both slowed and reduced in strength, probably due to abnormalities in both axons and myelin.
- Type X Charcot-Marie-Tooth disease (CMTX) is caused by mutations in a gene on the X chromosome, one of the two sex chromosomes and it’s more common in men than women.
Within the various types of Charcot-Marie-Tooth disease, subtypes (such as CMT1A, CMT1B, CMT2A, CMT4A, and CMTX1) are distinguished by the specific gene that is altered.
Sometimes other, more historical names are used to describe this disorder. For example, Roussy-Levy syndrome is a form of Charcot-Marie-Tooth disease defined by the additional feature of rhythmic shaking (tremors). Depending on the specific gene that is altered, this severe, early onset form of the disorder may also be classified as CMT1 or CMT4. CMTX5 is also known as Rosenberg-Chutorian syndrome. Some researchers believe that this condition is not actually a form of Charcot-Marie-Tooth disease. Instead, they classify it as a separate disorder characterized by peripheral nerve problems, deafness, and vision loss.
What is Roussy-Lévy Syndrome?
Roussy-Lévy does not describe a specific type of Charcot Marie Tooth, but rather an individual’s symptoms. Roussy- Lévy Syndrome is used to describe a phenotype (or expression of symptoms) that includes high arches, loss of reflexes, distal limb weakness, tremor in the upper limbs, distal sensory loss and gait ataxia (lack of coordination), probably due to the sensory symptoms. This can also be associated with a form of scoliosis called kyphosis. Many people with Charcot Marie Tooth can have this clustering of symptoms: It really isn’t exclusive to any one type, but the key clinical finding is Charcot Marie Tooth with a tremor. It doesn’t help define what type of Charcot Marie Tooth a person has, although it does appear to happen more commonly with demyelinating forms of Charcot Marie Tooth such as Charcot Marie Tooth1A and Charcot Marie Tooth1B. There isn’t a lot of information about Roussy-Lévy Syndrome because it is not a specific disorder and the term isn’t is not really used much anymore (like Dejerine-Sottas Syndrome).
The peripheral nervous system
The peripheral nervous system, the part of the nervous system outside the central nervous system (CNS = brain and spinal cord), consists mainly of the nerves that extend from the brain and spinal cord. Cranial nerves carry signals to and from the brain, whereas spinal nerves carry signals to and from the spinal cord. These peripheral nerves serve as communication lines that link all regions of the body to the central nervous system (CNS = brain and spinal cord). Also included in the peripheral nervous system are ganglia, areas where the cell bodies of neurons are clustered.
The peripheral nervous system receives sensory inputs and dictates motor outputs (Figures 1 and 2). In the sensory or afferent (afferent means “carrying toward”) division, signals are picked up by sensory receptors located throughout the body and carried by nerve fibers of the peripheral nervous system into the CNS (brain and spinal cord). In the motor or efferent (efferent means “carrying away”) division, signals are carried away from the CNS (brain and spinal cord) by nerve fibers of the peripheral nervous system to innervate the muscles and glands, causing these organs either to contract or to secrete. Both the sensory inputs and the motor outputs are further divided according to the body regions they serve: The somatic body region consists of the structures external to the ventral body cavity—in other words, the structures of the outer tube (skin, skeletal musculature, bones). The visceral body region mostly contains the viscera within the ventral body cavity—which means the structures of the body’s inner tube (digestive tube, lungs, heart, bladder, and so on).
This scheme results in the four main subdivisions of the peripheral nervous system:
- Somatic sensory (the sensory innervation of the outer tube: skin, body wall, and limbs);
- Visceral sensory (the sensory innervation of the viscera);
- Somatic motor, or voluntary motor (the motor innervation of the outer tube, specifically skeletal muscles); and
- Visceral motor, also called the autonomic nervous system (ANS) (the involuntary motor innervation of the inner tube, specifically smooth muscle, cardiac muscle, and glands, as well as some outer tube structures: arrector pili muscles, smooth muscle in the vessels, and sweat glands).
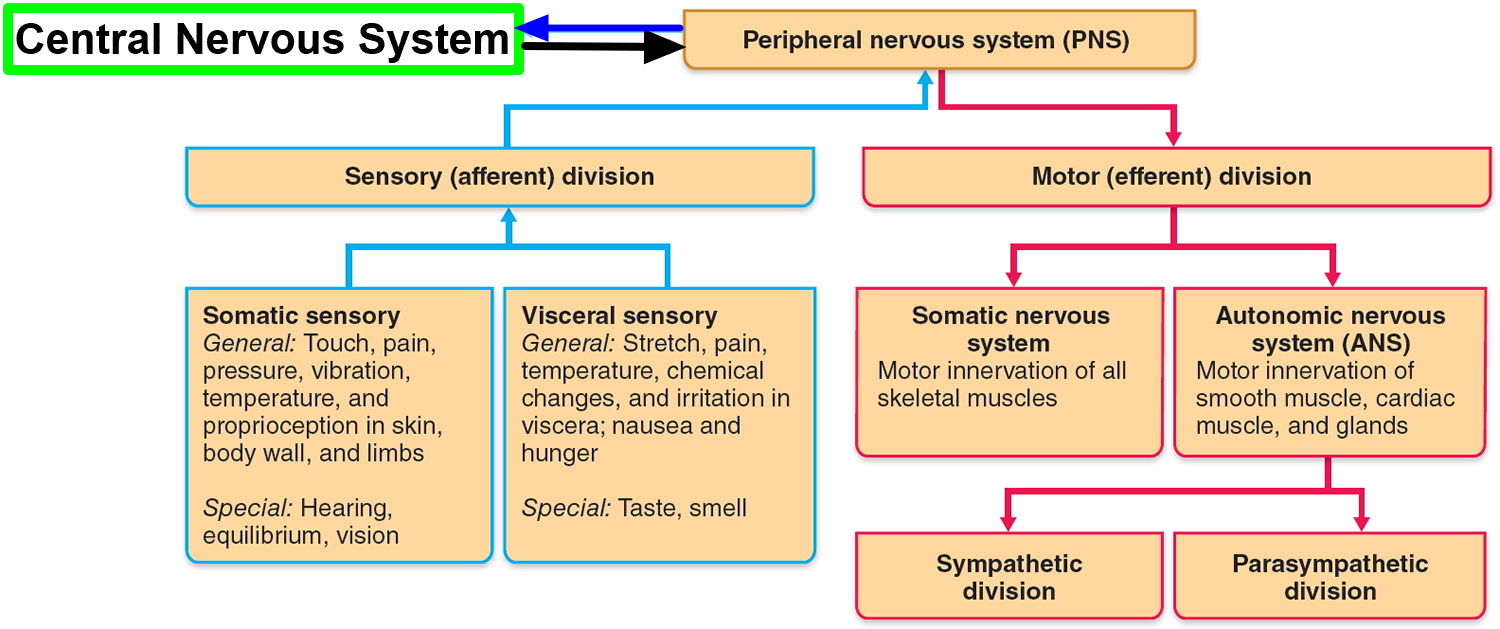
The peripheral nervous system is functionally divided into sensory and motor divisions, and each of these is further divided into somatic and visceral subdivisions.
The sensory (afferent) division carries signals from various receptors (sense organs and simple sensory nerve endings) to the central nervous system (CNS). This pathway informs the central nervous system (CNS) of stimuli within and around the body.
- The somatic sensory division carries signals from receptors in the skin, muscles, bones, and joints.
- The visceral sensory division carries signals mainly from the viscera of the thoracic and abdominal cavities, such as the heart, lungs, stomach, and urinary bladder.
The motor (efferent) division carries signals from the CNS (the brain and the spinal cord) mainly to gland and muscle cells that carry out the body’s responses. Cells and organs that respond to these signals are called effectors.
- The somatic motor division carries signals to the skeletal muscles. This produces voluntary muscle contractions as well as involuntary somatic reflexes.
- The visceral motor division (autonomic nervous system) carries signals to glands, cardiac muscle, and smooth muscle. We usually have no voluntary control over these effectors, and the autonomic nervous system operates at an unconscious level. The responses of the autonomic nervous system and its effectors are visceral reflexes. The autonomic nervous system has two further divisions:
+ The sympathetic division tends to arouse the body for action—for example, by accelerating the heartbeat and increasing respiratory airflow—but it inhibits digestion.
+ The parasympathetic division tends to have a calming effect—slowing the heartbeat, for example—but it stimulates digestion.
Figure 1. Peripheral nervous system (CNS = central nervous system and PNS = peripheral nervous system)
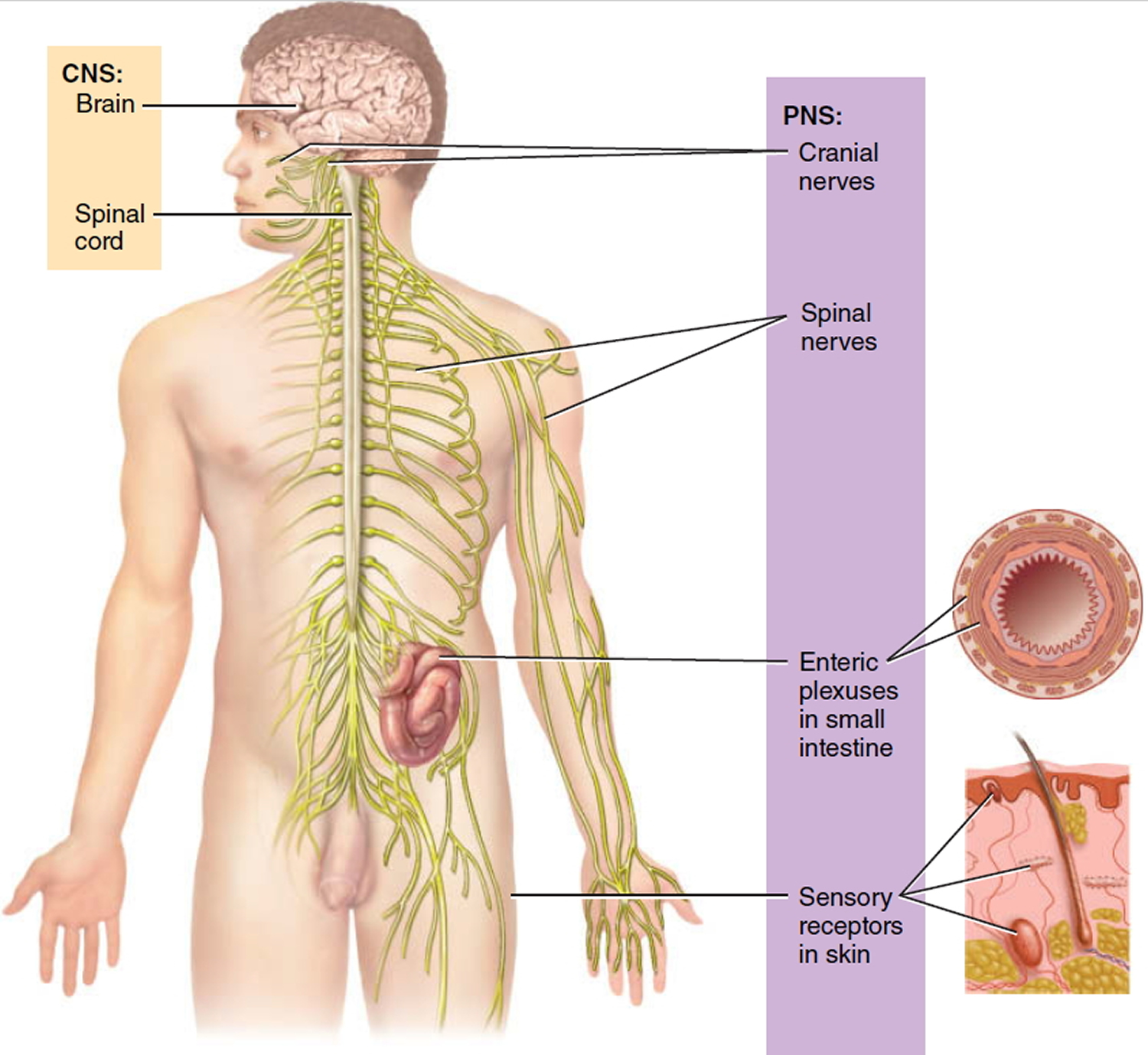
Figure 2. Nervous system and its parts
 Charcot Marie Tooth Types
Charcot Marie Tooth Types
There are over 80+ causative genes behind Charcot Marie Tooth. This sctions aims to describe briefly the current understanding of the genetic classification of the commoner types of the Charcot Marie Tooth disease.
Classification of Charcot Marie Tooth
The key point to remember is that there are two main forms of Charcot Marie Tooth:
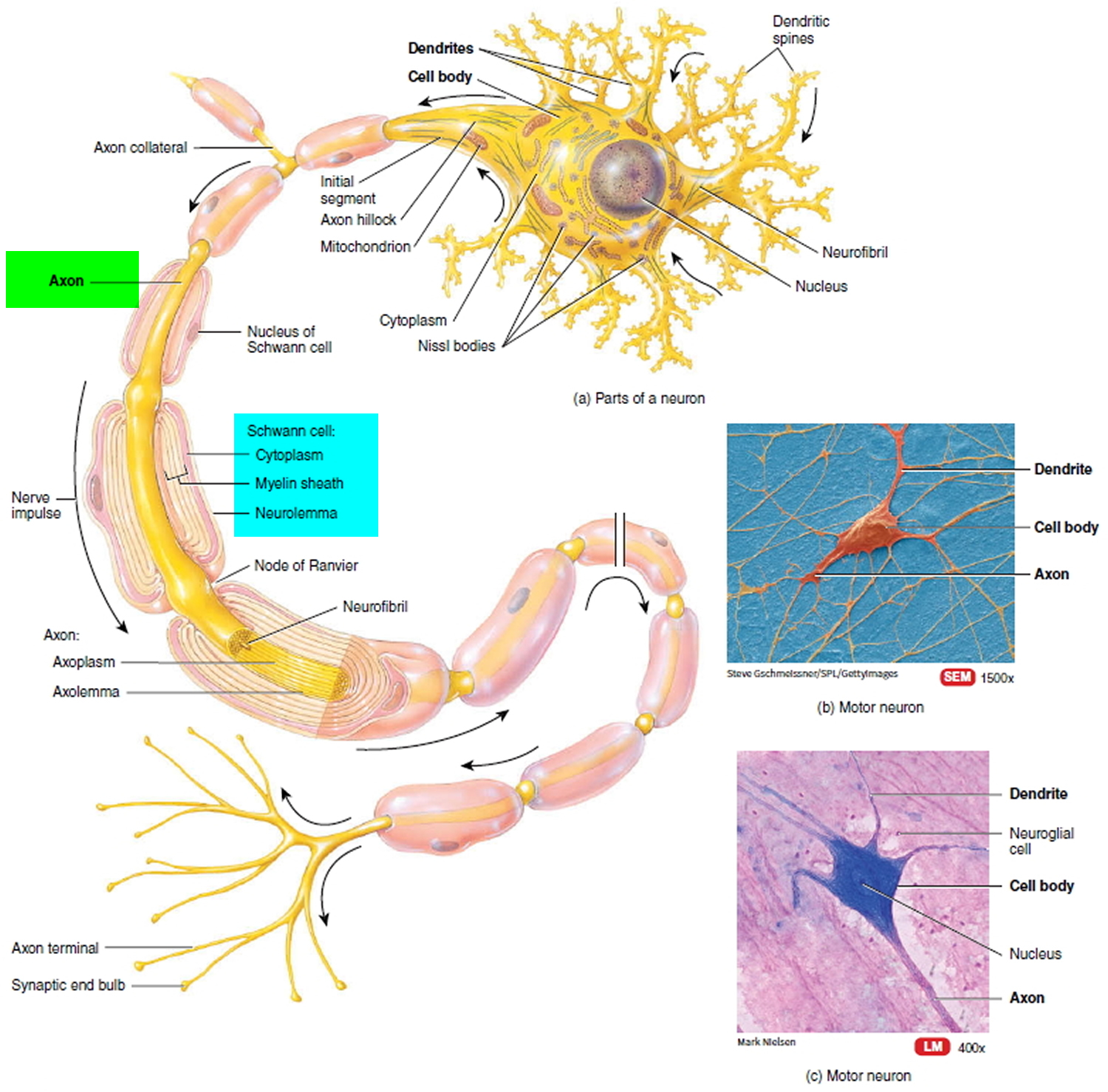
- Demyelinating (Charcot Marie Tooth 1) – affects the myelin sheath insulating and nourishing the nerve’s axon.
- Axonal (Charcot Marie Tooth 2) – directly affects the axon.
Figure 3. Structure of a neuron
Demyelinating Charcot Marie Tooth (Charcot Marie Tooth 1)
Charcot Marie Tooth1 is the most common form of Charcot Marie Tooth (six out of ten people with Charcot Marie Tooth will have Charcot Marie Tooth 1A), affecting the nerve’s insulating myelin sheath. Some forms of Charcot Marie Tooth1 have an earlier age of onset and these forms used to be called HMSN3 in the old classification but are now more commonly referred to as severe Charcot Marie Tooth 1. Two of these forms are sometimes referred to as Dejerine Sottas disease and Congenital Hypomyelinating Neuropathy but these are both forms of Charcot Marie Tooth 1. Autosomal dominant Charcot Marie Tooth 1 (AD Charcot Marie Tooth 1) is much more common than autosomal recessive Charcot Marie Tooth 1 (AR Charcot Marie Tooth 1, more commonly called Charcot Marie Tooth 4). Generally, people with AR Charcot Marie Tooth1 / Charcot Marie Tooth4 have an earlier onset and more severe form of Charcot Marie Tooth.
Autosomal dominant Charcot Marie Tooth 1
Charcot Marie Tooth 1A
This is the most common form of Charcot Marie Tooth, comprising at least 55 percent of all patients with Charcot Marie Tooth Type 1. The disorder is caused by a duplication of the PMP22 gene on Chromosome 17. Instead of having two copies of the gene (one of each paired chromosome), there are three copies, two on one chromosome and one on the other. PMP22 is a peripheral myelin protein, but its exact function in causing Charcot Marie Tooth is still not known. It is inherited in an autosomal dominant fashion. A deletion of the same part of chromosome 17 causes hereditary neuropathy with liability to pressure palsies. Mutations in PMP-22 can also cause a more severe form of Charcot Marie Tooth 1 (Dejerine Sottas disease and Congenital Hypomyelinating Neuropathy in old literature).
Charcot Marie Tooth 1A is the ‘classical’ form of Charcot Marie Tooth. People usually develop symptoms in the first 20 years of life, have a very slowly progressive condition and a normal lifespan. Charcot Marie Tooth 1A usually presents with a typical Charcot Marie Tooth phenotype (clinical presentation). Patients are slow runners in childhood, develop high arches, hammertoes and often require orthotics (braces) for ankle support. Varying degrees of hand weakness occur, often appearing as much as ten years after foot and leg problems. Problems with balance because of ankle weakness and loss of proprioception are common. Most patients remain ambulatory throughout life and life expectancy is normal.
Charcot Marie Tooth 1B
Mutations in MPZ (myelin protein zero) gene on chromosome 1 are responsible for Charcot Marie Tooth 1B. This form of Charcot Marie Tooth is the second commonest form of autosomal dominant Charcot Marie Tooth 1. It can be just like ‘classical’ Charcot Marie Tooth but onset is sometimes earlier and the condition more severe. Mutations in MPZ (myelin protein zero) can also cause a late-onset mild form of Charcot Marie Tooth 2. MPZ (myelin protein zero) is peripheral myelin protein, but its role is not known.
Patients with 1B have a somewhat typical phenotype, but often with more pronounced calf wasting. There is a wide range of severity within Type 1B, from very severe forms such as Dejerine-Sottas (infantile onset) to milder cases with onset much later in life. (More than one type of Charcot Marie Tooth may be referred to as Dejerine-Sottas since the term refers to an age of onset of less than three years rather than to a unique genetic defect.)
Charcot Marie Tooth Type 1C
Researchers at the University of Washington have recently identified the locus of Type 1C as Chromosome 16, the LITAF/SIMPLE gene. Type 1C is also autosomal dominant in inheritance. There is limited clinical information on patients with 1C, but they develop distal weakness, atrophy, and sensory loss and have slow nerve conduction velocity scores.
Charcot Marie Tooth Type 1D
This type is caused by an early growth response protein 2, known as ERG2, found on Chromosome 10. Inheritance is autosomal dominant. Most cases of 1D are severe, such as Dejerine-Sottas, while a few have milder phenotypes presenting later in life.
Charcot Marie Tooth Type 1F
Type 1F accounts for a very small percentage of cases. It is an autosomal dominant form of Charcot Marie Tooth in which the defect is on Chromosome 8 and the neurofilament light chain protein.
Charcot Marie Tooth Type 1X
This second most common of form of Charcot Marie Tooth, accounting for 10-16 percent of all cases is found on the X Chromosome, one of sex chromosomes. The flaw is caused by a gap junction beta 1 protein connected to connexin 32. Typically, this form has onset in adolescence or childhood and often affects males more severely than females. An affected male with Charcot Marie Tooth1X cannot pass the defect to his son, but will pass it to all his daughters. An affected female has a 50% chance of passing the mutation to either her sons or her daughters.
Axonal Charcot Marie Tooth (Charcot Marie Tooth 2)
Charcot Marie Tooth 2 is not as common as Charcot Marie Tooth 1, but has similar symptoms. Rather than damaging the nerves’ insulating myelin sheath, Charcot Marie Tooth2 affects the axon. Because of this Charcot Marie Tooth 2 is also known as ‘axonal Charcot Marie Tooth’. Symptoms are often first noticed between the ages of 10 and 20 but Charcot Marie Tooth 2 can start earlier or later. Like Charcot Marie Tooth 1, autosomal dominant Charcot Marie Tooth 2 (autosomal dominant Charcot Marie Tooth 2) is much more common than autosomal recessive Charcot Marie Tooth2 (autosomal recessive Charcot Marie Tooth 2), which is very rare.
Autosomal dominant Charcot Marie Tooth 2
Charcot Marie Tooth 2A
Mutations in Mitofusin 2 (MFN2) on chromosome 1p36 are responsible for about one in five cases of autosomal dominant Charcot Marie Tooth 2. This gene is mutated and is involved in the fusion of mitochondria, the metabolic engines of the cells. This type of Charcot Marie Tooth is often severe and can include optic atrophy. This usually presents in a more severe form than the ‘classical’ Charcot Marie Tooth, commonly in the first decade of life.
People with Charcot Marie Tooth 2A can be severely affected – with some needing wheelchairs – while others are more mildly affected. There is therefore a wide spectrum of disease severity in Charcot Marie Tooth2A.
Charcot Marie Tooth Type 2B
Type 2B is characterized by severe ulceration problems and the defect is located on chromosome 3, the RAB 7 protein. Charcot Marie Tooth 2B is predominantly a sensory disorder and there is some thought that it is not really Charcot Marie Tooth, but a pure sensory neuropathy.
Charcot Marie Tooth Type 2C
This type is a very rare form in which patients may have diaphragm or vocal cord paresis in addition to the other problems of Charcot Marie Tooth. Linkage to chromosome 12 has been found.
Charcot Marie Tooth Type 2D
The Charcot Marie Tooth 2D locus is on chromosome 7p14 and the genetic cause has been identified as mutations in the glycyl RNA synthetase gene. Charcot Marie Tooth 2D is a confusing disorder because some patients have sensorimotor neuropathies, while others have only motor symptoms.
Charcot Marie Tooth Type 2E
Charcot Marie Tooth type 2E has been established with linkage to chromosome 8p21 and studies have identified mutations in the neurofilament light gene.
Autosomal recessive Charcot Marie Tooth 2
The gene mutations that cause autosomal recessive Charcot Marie Tooth 2 are all very rare.
X-Linked Charcot Marie Tooth
Charcot Marie Tooth X is a variation of Charcot Marie Tooth 1 and Charcot Marie Tooth 2. It is called ‘X’ because the genes that cause this form of Charcot Marie Tooth are carried on the X chromosome. It usually affects men much more severely than women because a man has only one X chromosome and women have two.
Charcot Marie Tooth X1
Mutations in GJB1 (the protein from this gene is connexin 32) cause the commonest form of x-linked Charcot Marie Tooth. This is the second-commonest form of Charcot Marie Tooth, affecting about 10% of all people with the condition. This form usually affects males more severely than females. Males usually present in the first decade of life and on average have a more severe form of Charcot Marie Tooth than the ‘classical’ form. They still have a normal lifespan and rarely need a wheelchair. Their nerve conduction studies look like Charcot Marie Tooth 1. Females may have no symptoms (but often have subtle signs when examined) or they may be mildly affected. The nerve conduction studies in females look like Charcot Marie Tooth 2.
DI-Charcot Marie Tooth
DI stands for ‘dominant intermediate’. This form of Charcot Marie Tooth is rare and usually has similar symptoms to the common versions of autosomal dominant Charcot Marie Tooth 1 and autosomal dominant Charcot Marie Tooth 2. The reason it is called intermediate is that both the myelin sheath and the axon are damaged equally.
For both Charcot Marie Tooth 1 and Charcot Marie Tooth 2 there are many different subtypes and you may hear about Charcot Marie Tooth 1A or Charcot Marie Tooth 2A, for example. These are all different genetic variations of the main types.
Charcot Marie Tooth Type 3
Type 3 is a particularly severe variant. The term Dejerine-Sottas syndrome (DSS) is used to describe patients who are severely disabled and develop Charcot Marie Tooth in infancy. This term was coined before the genetic causes of Charcot Marie Tooth were identified. As a result, the usage of this term is somewhat confusing. Dejerine-Sottas was originally thought to be a severe and disabling neuropathy beginning in infancy with an autosomal recessive inheritance pattern. Recently, it has been shown that DSS patients also have autosomal dominant mutations of PMP22, MPZ, EGR2 and even PRX and GDAP. Most patients with DSS have extremely slow nerve conduction velocities. Most children with DSN have severe demyelination while others show predominantly axonal loss when sural nerve biopsies are done. Currently, the term Dejerine-Sottas is used to define patients who have onset by 3 years of age, delayed motor milestones, and severe motor, sensory and skeletal defects.
Congenital hypomyelination (CH) is a term originally used to describe peripheral nerves that were so abnormal that they suggested a developmental failure of the peripheral nervous system myelination. Patients with CH were hypotonic within the first year of life, had developmental delays in walking and had swallowing or respiratory difficulties. Some patients with CH were considered “floppy” infants. It is difficult to distinguish between DSS and CH since both have severe pathological changes on sural nerve biopsies and both have very slow nerve conduction velocities.
Charcot Marie Tooth Type 4
All Type 4 instances of Charcot Marie Tooth are inherited in an autosomal recessive pattern and are rare in the United States (~5% of cases). They have various phenotypical presentations but are more severe than autosomal dominantly inherited disorders. These disorders often have systemic symptoms, such as cataracts and deafness. Charcot Marie Tooth 4A and B are demyelinating and 4C is axonal.
Charcot Marie Tooth Type 4A
Charcot Marie Tooth Type 4 is linked to Chromosome 8 and is caused by mutations in the GDAP 1 protein, of unknown function. This form was first described in four families in Tunisia who were highly inbred. Clincial onset began at age 2 with delayed developmental milestones of sitting or walking. Many patients are wheelchair dependent by the end of the first decade of life. Hoarse voice and vocal cord paresis have been reported.
Charcot Marie Tooth Type 4B
The genetic location for the defect causing Type 4B is on chromosome 11 and presents with focally folded myelin sheaths in nerve biopsies. Affected patients become symptomatic early in life, with an average age of onset at 34 months. Unlike most types of Charcot Marie Tooth, both proximal and distal weakness is common.
Charcot Marie Tooth Type 4C
Type 4C is a childhood onset form of hereditary motor and sensory neuropathy (HSMN) with early onset scoliosis. The protein defect defines a new family of unknown function.
Charcot Marie Tooth Type 4D
This form was first described as a separate disorder with linkage to Chromosome 8 in a Gypsy population with autosomal recessive inheritance. The clinical features included distal weakness, muscle wasting and sensory loss, foot and hand deformities and loss of deep tendon reflexes. Deafness is always found in these patients and occurs by the third decade. Nerve conduction is severely reduced in younger patients and completely unattainable after age 15.
Charcot Marie Tooth Type 4F
Charcot Marie Tooth type 4F is a severe form of recessive Charcot Marie Tooth that has been defined in a large Lebanese family with mutations in the PRX gene on Chromosome 19. Nerve conduction studies are markedly slow and onion bulb formations are observed in nerve biopsies.
Charcot Marie Tooth Disease Complications
Complications of Charcot-Marie-Tooth disease vary in severity from person to person. Foot abnormalities and difficulty walking are usually the most serious problems. Muscles may get weaker, and you may injure areas of the body that experience decreased sensation.
You may also experience difficulty breathing, swallowing or speaking if the muscles that control these functions are affected by Charcot-Marie-Tooth disease.
Charcot Marie Tooth disease causes
Charcot Marie Tooth is caused by an inherited mutations (faults) in one of the many genes responsible for the development of the peripheral nerves. This fault means the peripheral nerves become damaged over time.
The peripheral nerves are a network of nerves that run from the brain and spinal cord (the central nervous system). They carry impulses to and from the rest of the body, such as the limbs and organs, and are responsible for the body’s senses and movements (see Figures 1 and 2 above).
A peripheral nerve is similar to an electrical cable, and is made up of two parts:
- the Axon – which transmits electrical information between your brain and limbs, similar to the wiring in an electrical cable
- the Myelin sheath – which is wrapped around the axon to protect it and ensure the electrical signal isn’t broken, similar to the insulation around electrical cable
In some types of Charcot Marie Tooth, faulty genes cause the myelin sheath to disintegrate. The axons become damaged without this protection, which affects the transmission of messages between the brain and the muscles and senses. This leads to muscle weakness and numbness.
In other types of Charcot Marie Tooth, the axons are directly affected and don’t transmit electrical signals at the normal strength. This means muscles and senses are understimulated, leading to symptoms of muscle weakness and numbness.
A child with Charcot Marie Tooth may have inherited the genetic fault responsible for the disease from one or both of their parents.
There’s no single faulty gene that causes Charcot Marie Tooth. There are many varieties of Charcot Marie Tooth that are caused by different genetic faults and these can be inherited in several different ways.
The chances of passing Charcot Marie Tooth to your child depend on the specific genetic faults you and your partner carry.
How Charcot Marie Tooth is inherited
A child with Charcot Marie Tooth may have inherited the genetic fault responsible for the disease from just one or both of their parents.
There’s no single faulty gene that causes Charcot Marie Tooth. The many varieties of Charcot Marie Tooth are caused by different genetic mutations and the faulty genes can be inherited in several different ways.
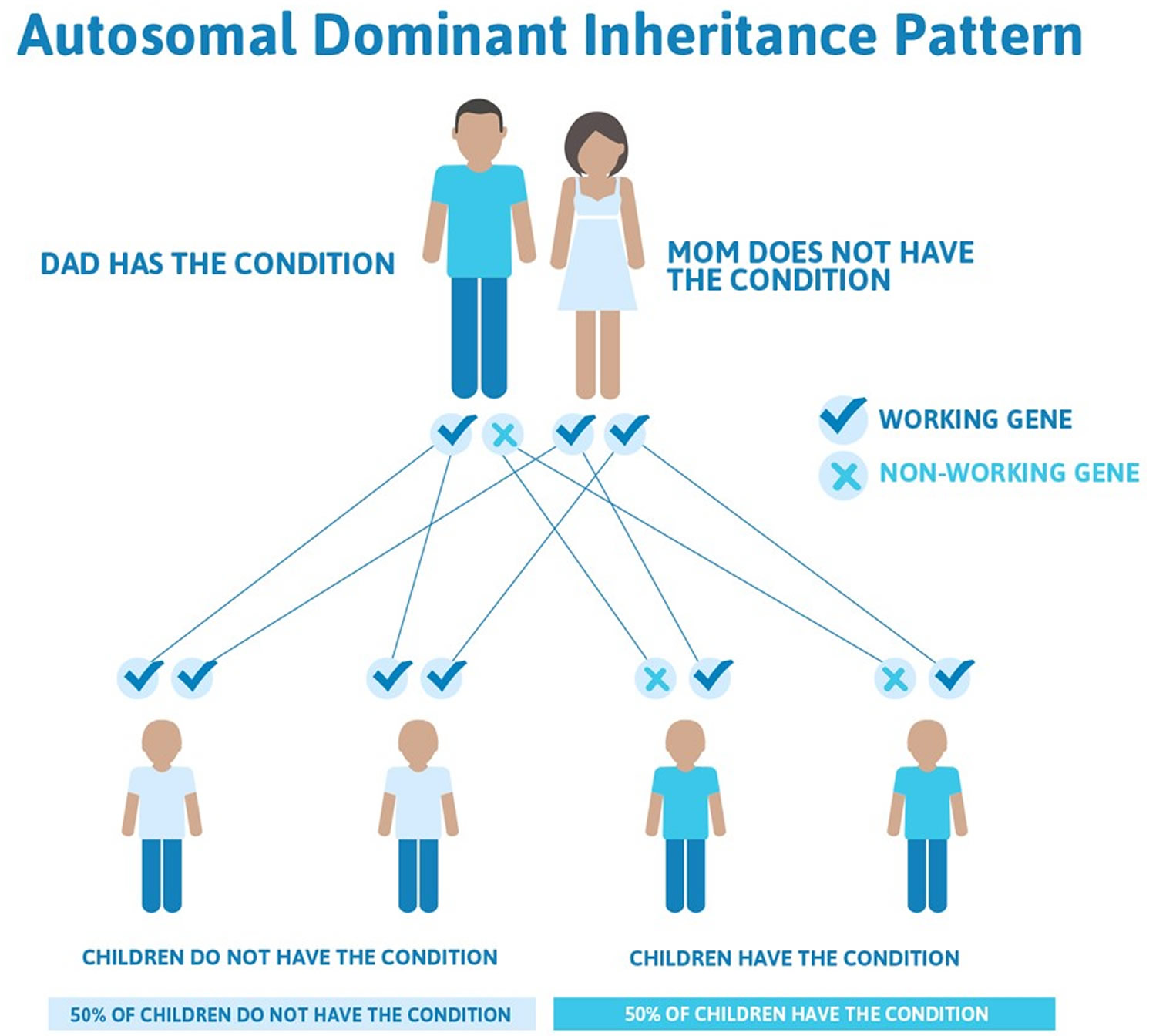
Autosomal dominant
Autosomal dominant inheritance of Charcot Marie Tooth occurs when one copy of a mutated gene is enough to cause the condition. If either parent carries a faulty gene, there’s a 50% chance the condition will be passed on to each child they have.
Figure 4. Autosomal dominant inheritance of Charcot Marie Tooth
Autosomal recessive
Autosomal recessive inheritance of Charcot Marie Tooth occurs when two copies of the defective gene are needed to cause the condition. You inherit one copy from each parent. As your parents only have one copy of the gene, they don’t develop Charcot Marie Tooth themselves.
Figure 5. Autosomal recessive inheritance of Charcot Marie Tooth
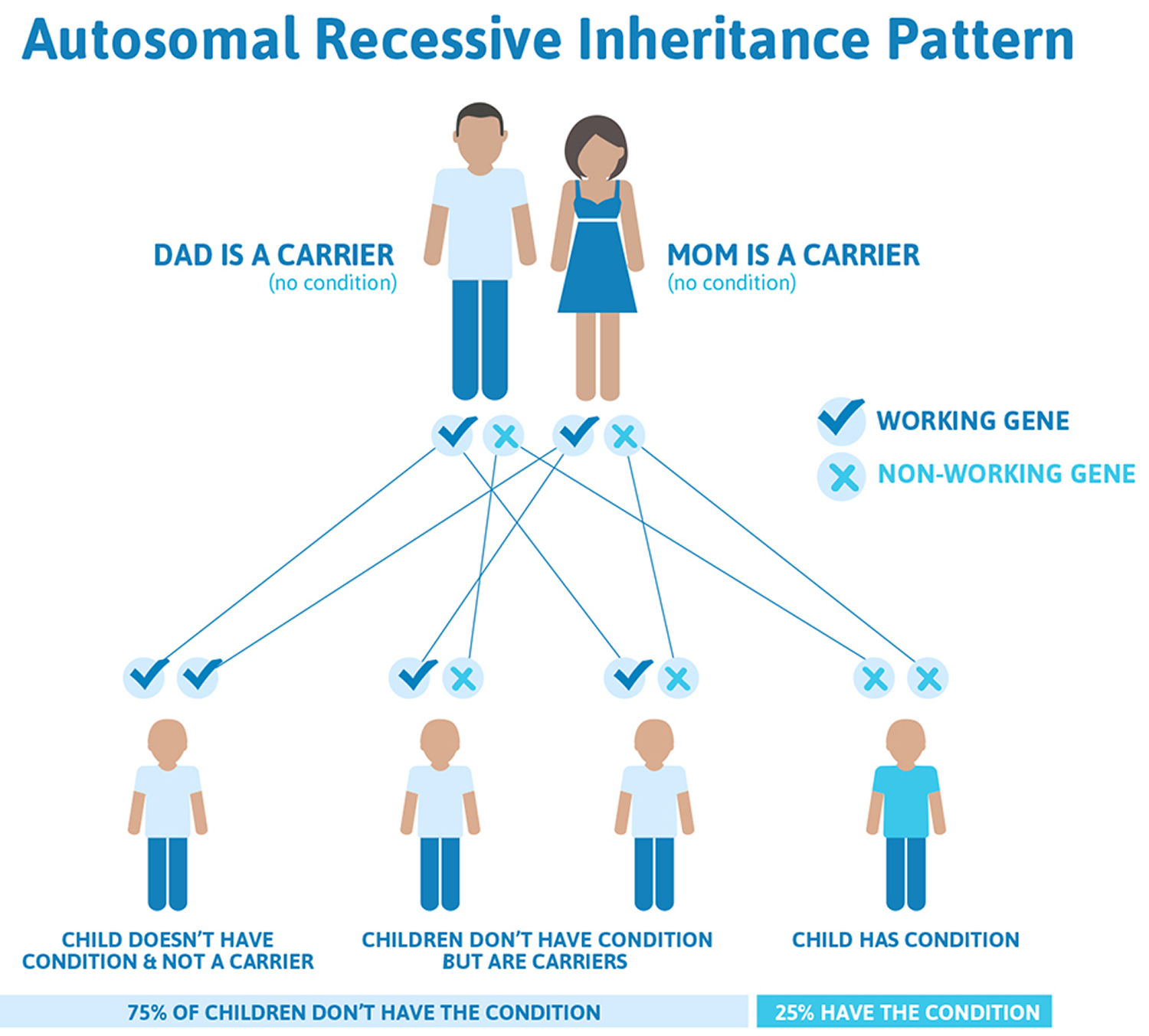
If both you and your partner are carriers of the autosomal recessive Charcot Marie Tooth gene, there’s a:
- 25% chance each child you have will develop Charcot Marie Tooth
- 50% chance each child you have will inherit one of the defective genes and be able to pass the condition to any children they have (known as being a ‘carrier’) – although they won’t have any of the symptoms of Charcot Marie Tooth themselves
- 25% chance each child you have will receive a pair of healthy genes and won’t develop Charcot Marie Tooth
If only one parent has the autosomal recessive gene, your children won’t develop Charcot Marie Tooth. However, there’s a 50% chance each child will be a carrier.
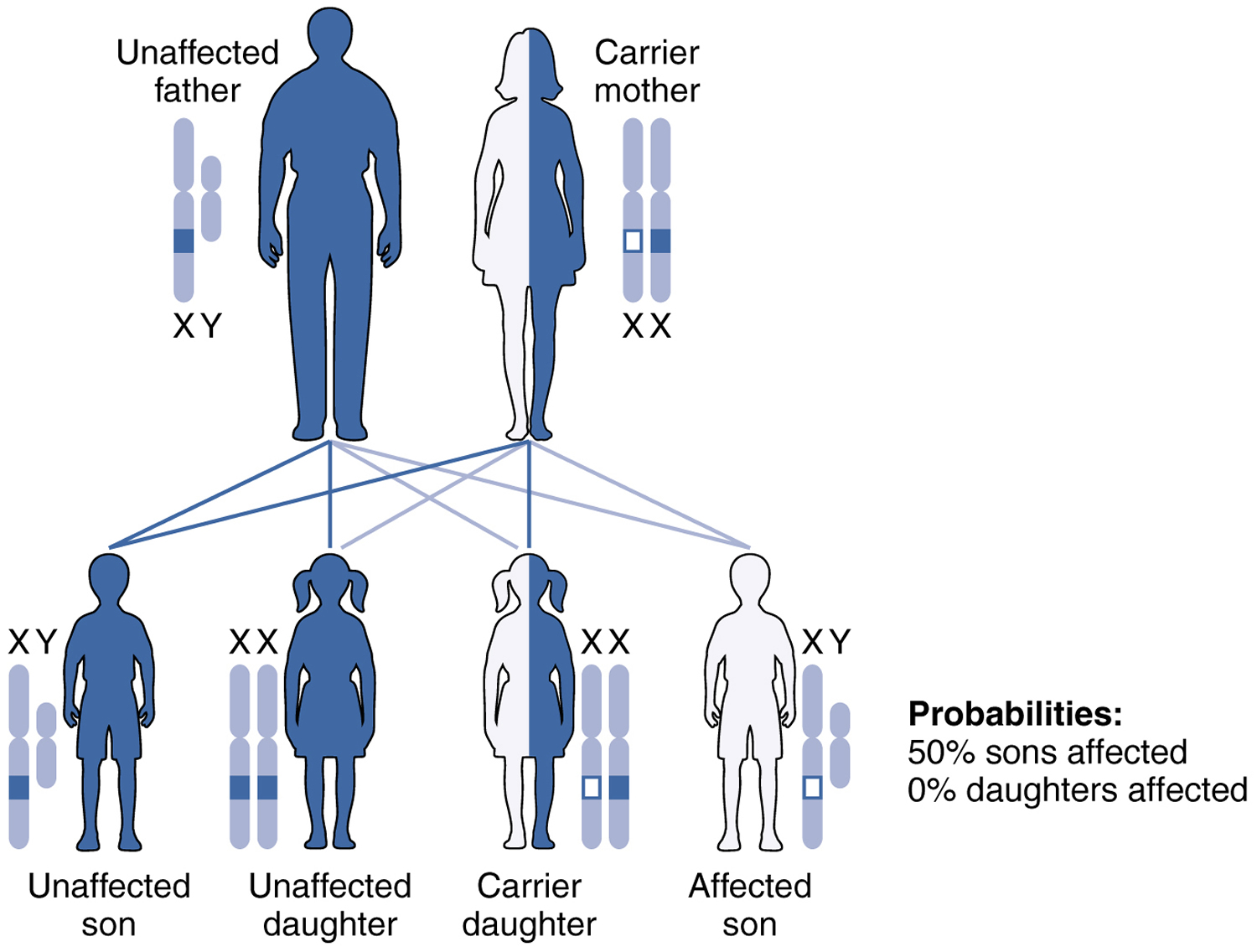
X-linked inheritance
In X-linked inheritance, the mutated gene is located on the X chromosome and passed from mother to son. Chromosomes are the parts of cells that carry your genes.
Men have XY sex chromosomes. They receive the X chromosome from their mother and the Y chromosome from their father. Women have XX chromosomes. They receive one X chromosome from their mother and the other X chromosome from their father.
A woman with the defective X chromosome will usually have no or very mild symptoms because the other healthy X chromosome counters the effect of the defective one. However, there’s a 50% chance she’ll pass on the defective gene to her son and that he’ll develop Charcot Marie Tooth.
If a woman with the defective X chromosome only has daughters, Charcot Marie Tooth can skip a generation until one of her grandsons inherits it.
Figure 6. X-linked inheritance of Charcot Marie Tooth
Charcot Marie Tooth disease symptoms
Charcot Marie Tooth is a progressive condition, which means the symptoms gradually get worse over time. Therefore, it may be difficult to spot any symptoms in young children who have Charcot Marie Tooth.
Signs that a young child may have Charcot Marie Tooth include:
- appearing unusually clumsy and accident-prone for their age
- finding it difficult to walk because they may have problems lifting their feet from the ground
- their toes dropping forward as they lift their feet (known as ‘foot drop’)
The main symptoms of Charcot Marie Tooth usually appear between the ages of five and 15, although they sometimes don’t develop until well into middle age or later.
Main signs and symptoms of Charcot-Marie-Tooth disease may include:
- First signs include frequent tripping, ankle sprains, clumsiness and “burning” or pins-and-needles sensations in the feet or hands.
- Structural foot deformities such as high foot arches or having very flat feet and curled toes (hammertoes) are common.
- Muscle wasting in the lower legs and feet may lead to foot drop, poor balance and other gait problems.
- Weakness in your legs, ankles and feet
- Decreased ability to run
- Difficulty lifting your foot at the ankle (footdrop)
- Awkward or higher than normal step (gait)
- Frequent tripping or falling
- Decreased sensation or a loss of feeling in your legs and feet
As Charcot-Marie-Tooth disease progresses, symptoms may spread from the feet and legs to the hands and arms. The severity of symptoms can vary greatly from person to person, even among family members.
- Muscular atrophy in the hands often causes people to have difficulty with tasks involving manual dexterity, such as writing and manipulating zippers and buttons.
- Abnormal sensation in the extremities and an inability to sense where one’s body is in space are also common, and many people experience neuropathy, muscle or joint pain.
- Poor tolerance for cool or cold temperatures is typical and many people have chronically cold hands and feet.
- Additional symptoms may include fatigue, sleep apnea, breathing difficulties, scoliosis, kyphosis and hearing loss.
Some people also develop additional problems such as:
- tremor (uncontrollable shaking)
- scoliosis (abnormal curvature of the spine)
- problems speaking, breathing or swallowing (dysphagia) – but these symptoms are rare in Charcot Marie Tooth.
Later symptoms of Charcot Marie Tooth
As Charcot Marie Tooth progresses, the muscle weakness and lack of sensation worsens and starts to affect your hands and arms more. This can lead to problems with both manual dexterity and hand strength, making tasks such as doing up the buttons of a shirt very difficult.
Persistent problems with walking and posture can put excessive strain on your body, which often leads to muscle and joint pain. Less commonly, damaged nerves may also cause pain, known as neuropathic pain.
Problems with mobility and walking tend to get worse with age. It’s uncommon to lose the ability to walk completely, but older people with Charcot Marie Tooth often need a walking aid to get around.
Charcot Marie Tooth diagnosis
A visit to a neurologist will start with a physical exam to look for further signs of distal weakness and sensory loss. To identify weakness, the patient may be asked to walk on his heels or to move part of his leg against an opposing force. Sensory loss is often identified when the doctor tests for deep tendon reflexes, such as the knee-jerk, which are reduced or absent in Charcot Marie Tooth patients.
During the physical exam, your doctor may check for:
- Signs of muscle weakness in your arms, legs, hands and feet
- Decreased muscle bulk in your lower legs, resulting in an inverted champagne bottle appearance
- Reduced reflexes
- Sensory loss in your feet and hands
- Foot deformities, such as high arches or hammertoes
- Other orthopedic problems, such as mild scoliosis or hip dysplasia
Further tests
If Charcot Marie Tooth is suspected, you may be referred to a neurologist (a doctor who specialises in treating conditions of the nervous system) for further testing. Tests you may have are described below.
Nerve conduction test
A nerve conduction test measures the strength and speed of signals transmitted through your peripheral nerves (network of nerves that run from the brain and spinal cord to and from the rest of the body, such as the limbs and organs).
Electrodes (small metal discs) are placed on your skin, which release a small electric shock that stimulates the nerves. The speed and strength of the nerve signal is then measured. An unusually slow or weak signal could indicate Charcot Marie Tooth.
Electromyography (EMG)
Electromyography (EMG) uses a small needle-shaped electrode placed in your skin to measure the electrical activity of your muscles. Some types of Charcot Marie Tooth cause a distinctive change in the pattern of electrical activity that can be detected by an EMG.
Genetic testing
Genetic testing involves taking your blood sample and testing it for defective genes known to cause Charcot Marie Tooth. So far, many of these genes have been found, but there may be more not yet identified.
Most people with Charcot Marie Tooth should be able to have their diagnosis confirmed by genetic testing and find out exactly which type of Charcot Marie Tooth they have. For others, genetic testing may prove inconclusive because an unidentified gene may be involved in their Charcot Marie Tooth.
Nerve biopsy
In a small number of cases where other tests have been inconclusive, a test called a nerve biopsy may be carried out.
This is a minor surgical procedure where a sample of a peripheral nerve is removed from your leg for testing. Charcot Marie Tooth can cause physical changes to the shape of the nerve, which can be seen under a microscope. The biopsy is carried out under a local anaesthetic, so you’ll be awake, but unable to feel pain.
Tests before and during pregnancy
Couples with a family history of Charcot Marie Tooth who are thinking of having a baby can be referred to a genetics specialist for advice.
A genetic counselor can help couples work through the decision-making process and explain possible tests that can be carried out and any alternatives you may want to consider, such as adoption.
The main tests that can be carried out during pregnancy to check if a baby will develop certain types of Charcot Marie Tooth are:
- chorionic villus sampling (CVS) – where a small sample of placenta is removed from the womb and tested for known Charcot Marie Tooth genes, usually during weeks 11 to 14 of pregnancy
- amniocentesis – where a sample of amniotic fluid is taken for testing, usually during weeks 15 to 20 of pregnancy
If these tests show that your child is likely to have Charcot Marie Tooth, you can discuss with your genetic counselor whether you want to continue the pregnancy or have a termination (abortion).
However, it’s important to be aware that the results of these tests won’t indicate how serious your child’s Charcot Marie Tooth will be. This is because the symptoms and progression of the condition can vary widely, even among family members with the same type of Charcot Marie Tooth.
It’s also important to bear in mind that both these tests can slightly increase your chances of having a miscarriage.
Pre-implantation genetic diagnosis
For some couples at risk of having a child with Charcot Marie Tooth, pre-implantation genetic diagnosis may be an option.
Pre-implantation genetic diagnosis involves using in vitro fertilisation (IVF), where eggs are removed from a woman’s ovaries before being fertilized with sperm in a laboratory. After a few days, the resulting embryos can be tested for certain types of Charcot Marie Tooth and a maximum of two unaffected embryos are transferred into the womb.
Charcot Marie Tooth treatment
There’s no cure nor drug treatment for Charcot-Marie-Tooth disease, but physical therapies are available to help reduce your symptoms and enable you to live as independently as possible.
As Charcot Marie Tooth gets worse over time, you’ll need to be assessed regularly to check for any new developments in your condition. How often you’re assessed depends on the type of Charcot Marie Tooth you have and the severity of your symptoms.
Your treatment programme may involve a number of healthcare professionals working together in a multidisciplinary team. You’ll usually have a doctor who co-ordinates your treatment program and makes sure every aspect of your condition is closely monitored and treated if necessary. Ask your multidisciplinary team if they have specific lifestyle advice for you, as risks may vary from person to person.
Physical therapy and moderate activity (but not overexertion) can help maintain muscle strength, endurance and flexibility. Mechanical supports like ankle-foot orthoses and custom-made shoes can improve gait and balance. When medically indicated, orthopedic surgery can correct deformity and help maintain mobility and function. Occupational therapy and adaptive devices can help people perform activities of daily living.
Physiotherapy
Physiotherapy is one of the most important therapies for improving the symptoms of Charcot Marie Tooth and reducing the risk of muscle contractures (where muscles shorten and lose their normal range of movement).
Physiotherapy uses physical methods, such as massage and manipulation, to promote healing and wellbeing. It usually involves low-impact exercises such as stretching, swimming and moderate weight-training.
There’s a lack of good quality medical research into the benefits of exercise for people with Charcot Marie Tooth. However, it’s possible that some types of exercise are beneficial. For example:
- strengthening exercises that focus on improving muscle strength, such lifting weights, may help improve overall strength and reduce ‘foot drop’
- aerobic exercise, such as walking or swimming, which raises your heart rate and makes you breathe harder, may improve your fitness and your ability to function on a day-to-day basis
- posture and balance exercises, such as yoga, may also have benefits
Any exercise needs to be carefully planned as part of a personalized exercise programme. A certain level of exercise may be safe, but you risk making symptoms worse if you don’t follow proper instructions or if you over-exert yourself.
Speak to your doctor or physiotherapist about arranging a suitable exercise programme that will allow you to pace yourself. Read more information about the benefits of exercise.
Occupational therapy
Occupational therapy involves identifying problem areas in your everyday life, such as dressing yourself, then working out practical solutions.
Occupational therapy will be useful if muscle weakness in your arms and hands makes it difficult for you to do day-to-day tasks, such as dressing or writing.
An occupational therapist will teach you how to use adaptive aids to compensate for your difficulties, such as clothing with clasps instead of buttons, and magnetic tubes that allow you to pick up objects.
Orthoses and walking aids
Orthoses are devices worn inside your shoes or on your legs to improve the strength and functionality of your limbs, or to correct your gait (the way you walk).
There are several different types of orthoses, including:
- insoles in your shoes
- custom-made shoes that support your ankles
- ankle or leg braces
- thumb splints that can improve your hand strength
It’s unusual to completely lose the ability to walk, but you may benefit from using a wheelchair occasionally. Moving around can be difficult if you have Charcot Marie Tooth and using a wheelchair every now and again can give you a chance to rest.
Controlling pain
There are two types of pain associated with Charcot Marie Tooth:
- joint and muscle pain – caused by the stresses that Charcot Marie Tooth places on your body
- neuropathic pain – caused by damage to your nerves (this is less common)
Joint and muscle pain can usually be controlled by taking non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen.
Neuropathic pain may be treated with tricyclic antidepressants (TCAs) or an anti-convulsant medication (a medicine often used to prevent seizures). These medications weren’t originally designed to be painkillers, but there’s evidence to suggest they’re effective in treating long-term nerve pain in some people.
Surgery
If Charcot Marie Tooth causes significant deformities, surgery may be needed to correct them. Some of the types of surgery that may be carried out are described below.
Osteotomy
An osteotomy is a surgical procedure used to correct severe flatness of the feet. An incision (cut) is made in your foot and the surgeon removes or repositions the bones in your foot to correct its shape.
After surgery, your foot (or feet) will need to be kept in plaster for several weeks until the bones have healed.
Arthrodesis
Arthrodesis can also be used to correct flat feet, as well as relieve joint pain and correct heel deformities. It involves fusing the three main joints in the back of your feet to strengthen your feet, correct their shape and relieve pain.
After surgery, your foot (or feet) will be placed in plaster, and you won’t be able to place any weight on them for six weeks. During this time, you’ll need to use crutches or a wheelchair.
Once you can put weight on your feet, you’ll need to wear the cast for another six weeks (12 weeks in total). However, it may take up to 10 months for you to fully recover from the operation.
Plantar fascia release
Plantar fascia release is a surgical procedure used to relieve persistent heel pain caused by inflamed tendons. Tendons are the fibrous cords that join bones to muscle.
During the procedure, part of the tendon is removed and the remaining tendon repositioned and allowed to heal. Afterwards, you’ll need to wear a cast for three weeks and won’t be able to put any weight on your feet during this time.
Spinal surgery
Although abnormal curvature of the spine (scoliosis) can often be treated using a back brace, corrective surgery may be required.
Research into treatments
There’s some promising research that may provide new ways of treating people with Charcot Marie Tooth. This research includes:
- using stem cells (cells at an early stage of development) to repair nerve damage
- using hormones (powerful chemicals) and gene therapy to slow progression of the condition
Research looking into whether ascorbic acid (vitamin C) could help people with Charcot Marie Tooth has recently been carried out, but unfortunately no evidence of a benefit was found.
Speak to your care team if you’re interested in taking part in a clinical research trial. You can also search for Charcot Marie Tooth clinical trials to see what research is currently being carried out.
Taking care of yourself
In addition to the treatment you receive, there are some general precautions you can take to avoid further problems. These may include:
- try to maintain a healthy weight – being overweight can make moving around more difficult and put more strain on your body
- take good care of your feet – make sure you check and clean your feet regularly, as there’s a risk of injury and infection if you have reduced sensation in your feet
- avoid drinking too much alcohol – as this has many health risks, which may be worse if you have Charcot Marie Tooth
- avoid caffeine (found in tea, coffee, cola and energy drinks) and nicotine (found in tobacco) if you have tremors (shaking), as they can make this worse
- avoid medicines that can cause nerve damage.
Any medications people with Charcot Marie Tooth should avoid?
YES! Some medications are potentially toxic to people with Charcot Marie Tooth (https://www.cmtausa.org/resource-center/treatment-management/neurotoxic-medications).
- Vincristine has been proven hazardous and should be avoided by all Charcot Marie Tooth patients.
- Taxols (paclitaxel, docetaxel, cabazitaxel) also pose a high risk to people with Charcot Marie Tooth.
The complete list of potentially neurotoxic medications can be viewed here 1. Before taking any medication or changing medications, be sure your physician is fully aware of your medical condition, and discuss any possible side effects they may have on Charcot Marie Tooth.
Alcohol was removed from the neurotoxic drug list in July 2004 1. While people with Charcot Marie Tooth generally suffer no ill effects from the moderate consumption of alcohol, they should be particularly mindful of the fact that alcohol affects balance and coordination, and that overconsumption of alcohol is generally not recommend under any circumstances. If you have questions about alcohol and your health, consult your physician.
Lifestyle and home remedies
Some habits may prevent complications caused by Charcot-Marie-Tooth disease and help you manage its effects.
Started early and followed regularly, at-home activities can provide protection and relief:
- Stretch regularly. Stretching can help improve or maintain the range of motion of your joints and reduce the risk of injury. It’s also helpful in improving your flexibility, balance and coordination. If you have Charcot-Marie-Tooth disease, regular stretching can prevent or reduce joint deformities that may result from uneven pulling of muscle on your bones.
- Exercise daily. Regular exercise keeps your bones and muscles strong. Low-impact exercises, such as biking and swimming, are less stressful on fragile muscles and joints. By strengthening your muscles and bones, you can improve your balance and coordination, reducing your risk of falls.
- Improve your stability. Muscle weakness associated with Charcot-Marie-Tooth disease may cause you to be unsteady on your feet, resulting in falls and serious injury. Walking with a cane or a walker can increase your stability. Good lighting at night can help you avoid stumbling and falling.
Foot care is important
Because of foot deformities and loss of sensation, regular foot care is important to help relieve symptoms and to prevent complications:
- Inspect your feet. Check them daily to prevent calluses, ulcers, wounds and infections.
- Take care of your nails. Cut your nails regularly. To avoid ingrown toenails and infections, cut straight across and avoid cutting into the nailbed edges. A podiatrist can trim toenails for you if you have problems with circulation, sensation, and damage to the nerves in your feet. Your podiatrist also may be able to recommend a salon to safely trim your toenails.
- Wear the right shoes. Choose properly fitting, protective shoes. Consider wearing boots or high-top shoes for ankle support. If you have foot deformities, such as a hammertoe, explore having shoes custom made.
Living with Charcot Marie Tooth
Living with Charcot Marie Tooth can be challenging and the condition can have an impact on many aspects of your life, including:
- driving and getting around
- employment and finances
- holidays and leisure activities
- your emotional health
The Charcot-Marie-Tooth Association can also offer help and support. You can contact Charcot-Marie-Tooth Association here: https://www.cmtausa.org/index.php
Coping and support
Support groups, in conjunction with your doctor’s advice, can be valuable in dealing with Charcot-Marie-Tooth disease. Support groups bring together people who are coping with the same kinds of challenges, and offer a setting in which people can share common problems.
Ask your doctor about support groups in your community. The Internet and your local health department, public library and telephone book also may be good sources to find a support group in your area.





{kind=link}