Contents
- What is coarctation of the aorta
What is coarctation of the aorta
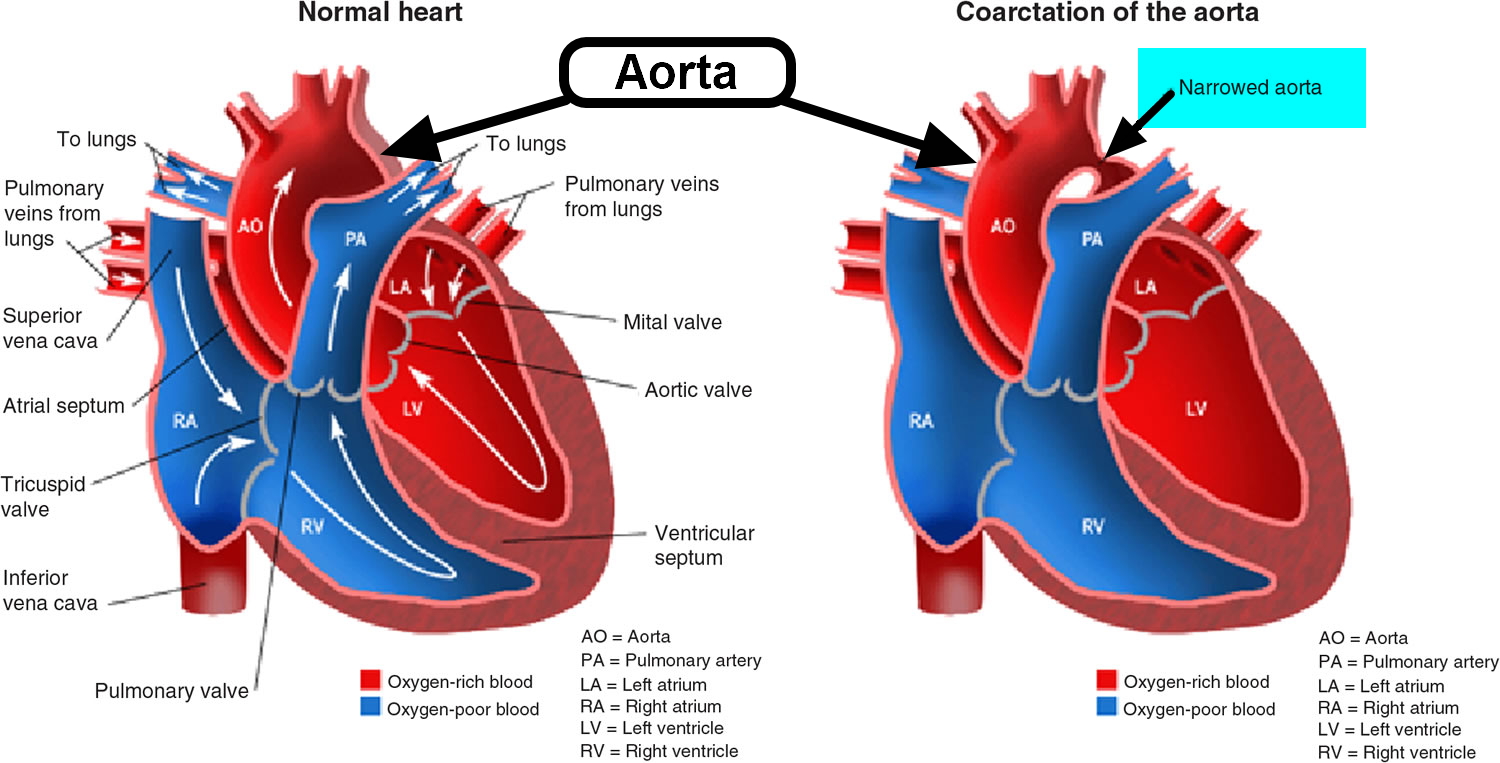
Coarctation of the aorta is a narrowing of part of the aorta, which is the main artery leading out of the heart. The most common site is the arch of the aorta (just after it leaves the heart).
The aorta is the main artery leaving the left side of the heart and carrying blood to the body (see Figure 1). It starts as an arch (like an umbrella handle) rising from the heart toward the upper chest, and then descending along the left side of the spine in the chest and to the abdomen. The curving part of the arch (before the artery “descends”) gives off branches to supply blood to the head and arms.
Coarctation of the aorta usually occurs at the proximal thoracic aorta just beyond the left subclavian artery and before the opening of the ductus arteriosus — after the blood reaches the head and neck vessels and right arm artery and in the vicinity of where the left arm artery (left subclavian artery) begins. Coarctation rarely involves the abdominal aorta, the blood vessels that lead to your lower body. This can often lead to high blood pressure in your arms but low blood pressure in your legs and ankles.
Depending on the degree of narrowing, there will be a variable amount of increased work for heart, and increased blood pressure above (upstream) of the narrowing, which can do damage to the heart over time. The degree of narrowing influences how much of a problem this can be. The condition varies from very mild with virtually no ill effect to the heart and circulation, to very severe creating significant load for, and dysfunction of, the heart. With coarctation of the aorta, pressure overload causes the lower left heart chamber (left ventricle) of your heart to work harder to pump blood through the narrowed aorta and blood pressure increases in the left ventricle. This may cause the wall of the left ventricle to thicken (hypertrophy) and hypertension in the upper part of the body including the brain. This is a condition where there are rarely any symptoms, except in some newborns (who may remain well for a few days before becoming sick) and very rare older children.
Hypoperfusion affects the abdominal organs and lower extremities. Malperfusion of the intestine increases the risk of sepsis due to enteric organisms.
Ultimately, the pressure gradient increases collateral circulation to the abdomen and lower extremities via intercostal, internal mammary, scapular, and other arteries.
Untreated coarctation of the aorta may result in left ventricular hypertrophy, heart failure, collateral vessel formation, bacterial endocarditis, intracranial hemorrhage, hypertensive encephalopathy, and hypertensive cardiovascular disease during adulthood. Patients with untreated aortic coarctation are at increased risk of aortic dissection or rupture later in life or in association with pregnancy. The ascending aorta is the area most frequently involved in dissection or rupture. Current data suggest that this risk is less likely a direct consequence of the coarctation and more likely related to a bicuspid aortic valve and associated aortopathy.
Coarctation may occur alone or with various other congenital anomalies (eg, bicuspid aortic valve, ventricular septal defect, aortic stenosis, patent ductus arteriosus, mitral valve disorders, intracerebral aneurysms). The most frequently associated lesions include bicuspid aortic valve (up to 85% of the cases), different levels of aortic stenosis, mitral valve stenosis (parachute mitral valve, a complex known as Shone syndrome) 1.
- The Centers for Disease Control and Prevention (CDC) estimates that about 4 out of every 10,000 babies are born each year in the United States with coarctation of the aorta 2.
- Coarctation of the aorta accounts for 6 to 8% of congenital heart anomalies.
- Coarctation of the aorta occurs in 10 to 20% of patients with Turner syndrome. The male:female ratio is 2:1.
Severe coarctation of the aorta can lead to hypertension. There is usually high blood pressures to the upper limbs (arms) and head, coupled with low blood pressures in the legs (below the block in the aorta).
Depending on the severity of the narrowing, heart failure occurs earlier or later in the disease.
Treatment involves enlargement or removal of the narrowed segment. In most cases this will involve surgery (a “closed heart” procedure carried out from near the shoulder blade at the back of the chest). Sometimes balloon dilation with a special catheter (tube) introduced from an artery in the groin and passed internally is possible, although this is most often reserved for re-coarctation (re-narrowing occurring after surgery, and due to scarring around the original repair). In some older patients balloon dilation and stent (small, tubular wire cage) implantation can improve the outcome of catheter procedures.
Most patients have an excellent outcome with complete return to normal function. Some ongoing checking is important, and this will be explained to you by your cardiologist.
Coarctation of the aorta prognosis
Coarctation of the aorta can be cured with surgery. Symptoms quickly get better after surgery. However, there is an increased risk for death due to heart problems among those who have had their aorta repaired.
Severe heart failure early in life has a poor prognosis without corrective surgery. Without treatment, most people die before age 40. For this reason, doctors usually recommend that the patient has surgery before age 10. Most of the time, surgery to fix the coarctation is done during infancy.
Narrowing or coarctation of the artery can return after surgery. This is more likely in persons who had surgery as a newborn.
Other mortality is associated with cerebrovascular accidents (strokes) due to the high blood pressures, and endocarditis and emboli associated with turbulent flow.
Coarctation of the aorta complications
Untreated coarctation of the aorta frequently leads to complications. Some complications may be a result of long-standing high blood pressure caused by the aortic coarctation. Complications are also possible after treatment for coarctation of the aorta.
Complications of coarctation of the aorta may include:
- Narrowing of the aortic valve (aortic stenosis)
- High blood pressure
- Stroke
- Enlargement in a section of the wall of the aorta (aneurysm)
- Aortic rupture or tear (dissection)
- Premature coronary artery disease — narrowing of the blood vessels that supply the heart
- Heart failure
- A weakened or bulging artery in the brain (brain aneurysm) or bleeding in the brain (hemorrhage)
In addition, if the coarctation of the aorta is severe, your heart might not be able to pump enough blood to your other organs. This can cause damage to your heart and also can result in kidney failure or other organ failure.
If your coarctation of the aorta was treated when you were young, you have a risk of the aorta re-narrowing (re-coarctation) over time. You also have a higher risk of developing high blood pressure. You will need lifelong follow-up for coarctation of the aorta, and you may require additional treatments.
Complications that may occur before, during, or soon after surgery include:
- Aortic aneurysm
- Aortic dissection
- Aortic rupture
- Bleeding in the brain
- Early development of coronary artery disease (CAD)
- Endocarditis (infection in the heart)
- Heart failure
- Hoarseness
- Kidney problems
- Paralysis of the lower half of the body (a rare complication of surgery to repair coarctation)
- Severe high blood pressure
- Stroke
Long-term complications include:
- Continued or repeated narrowing of the aorta
- Endocarditis
- High blood pressure
Figure 1. The anatomy of the heart
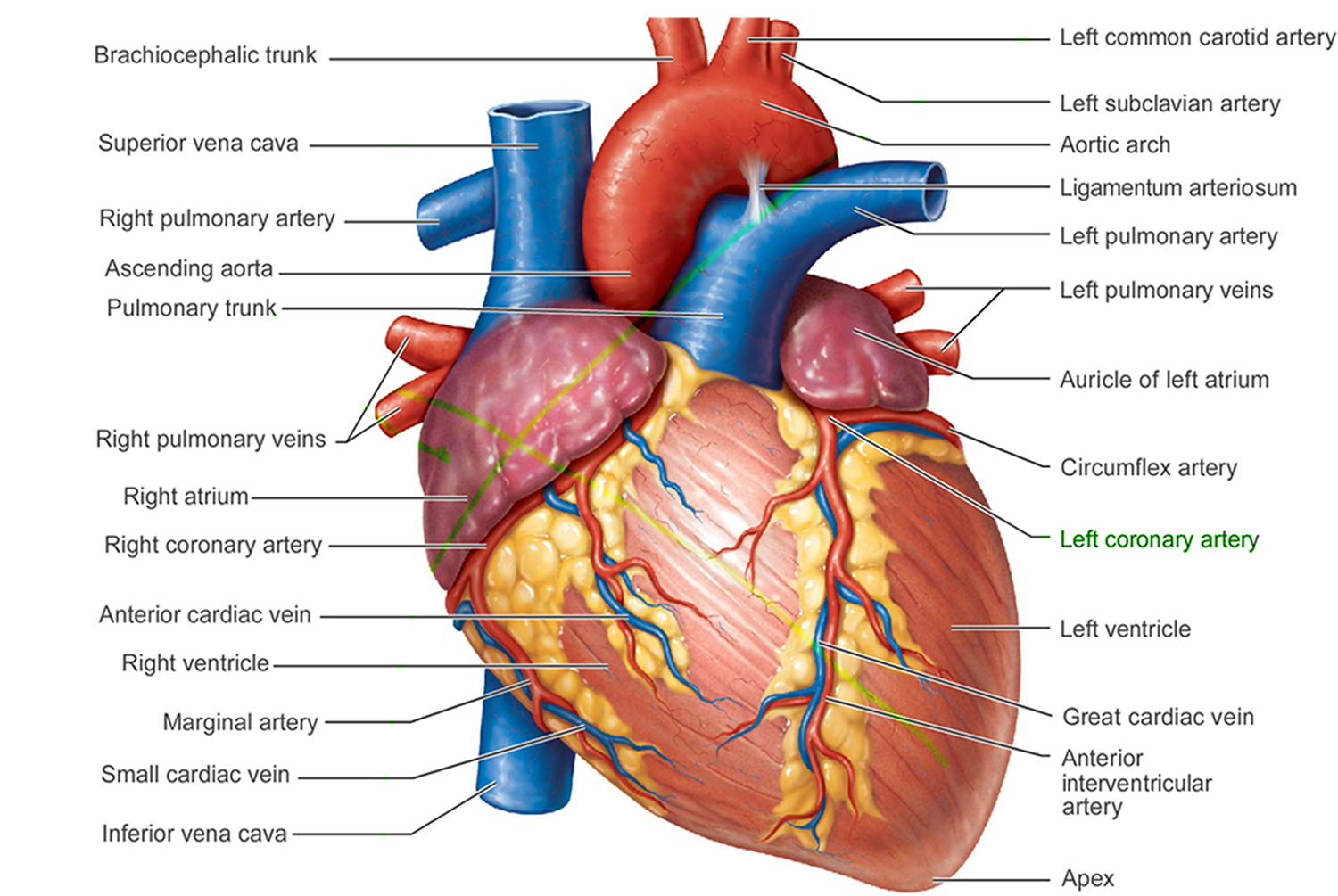
Figure 2. Coarctation of aorta
Coarctation of the aorta causes
Doctors aren’t certain what causes coarctation of the aorta (aortic coarctation). For unknown reasons, mild to severe narrowing develops in part of the aorta. Although aortic coarctation can occur anywhere along the aorta, the coarctation is most often located near a blood vessel called the ductus arteriosus. The condition generally begins before birth (congenital). Congenital heart defects are the most common of all birth defects.
Rarely, coarctation of the aorta develops later in life. Traumatic injury might lead to coarctation of the aorta. Rarely, severe hardening of the arteries (atherosclerosis) or a condition causing inflamed arteries (Takayasu’s arteritis) can narrow the aorta, leading to aortic coarctation.
Coarctation of the aorta is also more common in persons with certain genetic disorders, such as Turner syndrome.
Coarctation of the aorta is one of the more common heart conditions that are present at birth (congenital heart conditions). It is usually diagnosed in children or adults under age 40.
This condition may be related to cerebral aneurysms, which can increase the risk for stroke.
Coarctation of the aorta may be seen with other congenital heart defects, such as:
- Bicuspid aortic valve
- Defects in which only one ventricle is present
- Ventricular septal defect
Risk Factors for coarctation of the aorta
The causes and origins of congenital heart defects is not understood but several factors are known to be associated:
- 1) Maternal drug abuse, alcohol abuse and radiation exposure.
- 2) Maternal infection, particularly rubella.
- 3) Genetic abnormalities.
- 4) Chromosomal abnormalities (septal defects are associated with Trisomy 21- Down’s syndrome, and Turners Syndrome). Women and girls with Turner syndrome have 45 chromosomes, with one missing or incomplete X chromosome, instead of 46. About 10 percent of women and girls with Turner syndrome have aortic coarctation.
Coarctation of the aorta often occurs along with other congenital heart defects, although doctors don’t know what causes multiple heart defects to form together. The condition is more common in males than in females. You or your child may be more likely to have aortic coarctation if certain heart conditions exist, including:
- Bicuspid aortic valve. The aortic valve separates the lower left chamber (left ventricle) of the heart from the aorta. A bicuspid aortic valve has two flaps (cusps) instead of the usual three. Many people with coarctation of the aorta have a bicuspid aortic valve.
- Patent ductus arteriosus. Before birth, the ductus arteriosus is a blood vessel connecting the left pulmonary artery to the aorta — allowing blood to bypass the lungs. Shortly after birth, the ductus arteriosus usually closes. If it remains open, it’s called a patent ductus arteriosus.
- Holes in the wall between the left and right sides of the heart. You may have a hole in the wall (septum) between the upper chambers of the heart (atrial septal defect) or the lower chambers of the heart (ventricular septal defect) when you’re born. This causes oxygen-rich blood from the left side of the heart to mix with oxygen-poor blood in the right side of the heart.
- Aortic valve stenosis. This is a narrowing of the valve that separates the left ventricle of the heart from the aorta (aortic valve). This means your heart has to pump harder to get adequate blood flow to your body. Over time, this can cause your heart muscle to thicken and lead to symptoms such as chest pain, fainting spells and breathlessness, or heart failure.
- Aortic valve regurgitation. This occurs when the aortic valve doesn’t close tightly, causing blood to leak backward into the left ventricle.
- Mitral valve stenosis. This is a narrowing of the valve (mitral valve) between the upper left heart chamber (left atrium) and the left ventricle that lets blood flow through the left side of your heart. In this condition, blood may back up into your lungs, causing shortness of breath or lung congestion. Like aortic valve stenosis, this condition can also lead to heart failure.
- Mitral valve regurgitation. This occurs when the mitral valve doesn’t close tightly, causing blood to leak backward into the left atrium.
Coarctation of aorta prevention
Coarctation of the aorta can’t be prevented, because it’s usually present at birth (congenital). However, if you or your child has a condition that increases the risk of aortic coarctation, such as Turner syndrome, bicuspid aortic valve or another heart defect, or a family history of congenital heart disease, early detection can help. Discuss the risk of aortic coarctation with your doctor.
Coarctation of aorta symptoms
Coarctation of the aorta symptoms depend on the severity of the condition. Most people don’t have symptoms.
Symptoms depend on how much blood can flow through the artery. Other heart defects may also play a role.
Around half of newborns with this problem will have symptoms in the first few days of life.
Infants with severe coarctation of the aorta may begin having signs and symptoms shortly after birth. These include:
- Pale skin
- Irritability
- Heavy sweating
- Difficulty breathing
- Difficulty feeding
If aortic coarctation is significant, circulatory shock with renal insufficiency (oliguria or anuria) and metabolic acidosis may develop in the first 7 to 10 days of life and may mimic findings of other systemic disorders such as sepsis. Infants with critical (severe) coarctation of the aorta are likely to become acutely ill as soon as the ductus arteriosus constricts or closes. Left untreated, aortic coarctation in infants might lead to heart failure or death.
Less severe coarctation may be asymptomatic during infancy. Subtle symptoms (eg, headache; chest pain, fatigue, and leg claudication during physical activities) may be present as children age. Upper-extremity hypertension is often present, but heart failure rarely develops after the neonatal period. Rarely, intracerebral aneurysms rupture, resulting in subarachnoid or intracerebral hemorrhage.
In milder cases, symptoms may not develop until the child has reached adolescence. Symptoms include:
- Chest pain
- Cold feet or legs
- Dizziness or fainting
- Decreased ability to exercise
- Failure to thrive
- Leg cramps with exercise
- Nosebleed
- Poor growth
- Pounding headache
- Shortness of breath.
Older children and adults with coarctation of the aorta often don’t have symptoms because their narrowing may be less severe. If you have signs or symptoms that appear after infancy, you most commonly will have high blood pressure (hypertension) measured in your arms. However, your blood pressure is likely to be lower in your legs. Signs and symptoms might include:
- High blood pressure
- Headache
- Muscle weakness
- Leg cramps or cold feet
- Nosebleeds
- Chest pain
How is coarctation of the aorta diagnosed?
The age at which coarctation of the aorta is diagnosed depends on the severity of the condition. If the aortic coarctation is severe, it’s usually diagnosed during infancy. Testing for coarctation of the aorta before birth often isn’t possible.
The health care provider will perform a physical exam and take the blood pressure and pulse in the arms and legs.
- The pulse in the groin (femoral) area or feet will be weaker than the pulse in the arms or neck (carotid). Sometimes, the femoral pulse may not be felt at all.
- The blood pressure in the legs is usually weaker than in the arms. Blood pressure is usually higher in the arms after infancy.
- Typical physical examination findings include strong pulses and hypertension in the upper extremities, diminished or delayed femoral pulses, and a BP gradient, with low or unobtainable arterial BP in the lower extremities.
- A grade 2 to 3/6 ejection systolic murmur is often present at the upper left sternal border, left axilla, and sometimes most prominently in the left interscapular area. An apical systolic ejection click is present if a bicuspid aortic valve is also present. Dilated intercostal collateral arteries may cause a continuous murmur in the intercostal spaces.
- Affected females may have Turner syndrome, a congenital disorder causing lymphedema of the feet, webbed neck, squarely shaped chest, cubitus valgus, and widely spaced nipples.
The doctor will use a stethoscope to listen to the heart and check for murmurs. People with aortic coarctation have a harsh-sounding murmur that can be heard from the back. Other types of murmurs may also be present.
Coarctation of the aorta is often discovered during a newborn’s first examination or well-baby exam. Taking the pulse in an infant is an important part of the examination, because there may not be any other symptoms until the child is older.
Tests to diagnose this condition may include:
- Chest x-ray: May show the indentation of the coarctation with dilatation near the lesion. Evidence of heart failure may be seen. There may be evidence of rib erosion secondary to collaterals in adults.
- Electrocardiogram (ECG): An ECG records the electrical activity in your heart each time it contracts. During this procedure, you will have patches with wires (electrodes) placed on your chest, wrists and ankles. The electrodes measure electrical activity, which is recorded on paper or a computer monitor. If the coarctation of the aorta is severe, the ECG may show that the walls of the lower heart chambers are thickened (ventricular hypertrophy).
- Cardiac catheterization and aortography
- Echocardiography is the most common test to diagnose this condition, and it may also be used to monitor the patient after surgery. Echocardiograms use high-pitched sound waves to produce an image of your heart. Sound waves bounce off your heart and produce moving images that can be viewed on a video screen. An echocardiogram can often detect the location and severity of the aortic coarctation and show other heart defects, such as a bicuspid aortic valve. Doctors often use echocardiograms to diagnose coarctation of the aorta and determine the most appropriate treatment options for you.
- Heart CT may be needed in older children. A CT scan uses a series of X-rays to create detailed cross-sectional images of your body. In a CT angiogram, your doctor injects a dye into a blood vessel to highlight blood flow in your arteries and veins. A CT angiogram allows your doctor to see the location and severity of the coarctation of the aorta, determine whether it affects other blood vessels in your body, and detect other heart defects. Your doctor may also use this test to determine your treatment options.
- MRI or MR angiography of the chest may be needed in older children. An MRI uses a powerful magnetic field and radio waves to produce detailed images of your heart and blood vessels. An MRI can reveal the location and severity of the coarctation of the aorta, determine whether it affects other blood vessels in your body, and detect whether you have other heart defects. Doctors may also use this test to determine your treatment options.
- Both Doppler ultrasound and cardiac catheterization can be used to see if there are any differences in blood pressure in different areas of the aorta. During cardiac catheterization, your doctor inserts a long, thin tube (catheter) into an artery or vein in your groin, arm or neck and threads it to your heart using X-ray imaging. Your doctor may inject a dye through the catheter to make your heart structures visible on X-ray pictures. The dye can also measure pressures and oxygen levels in the chambers of the heart and in the blood vessels. Cardiac catheterization can help determine the severity of the aortic coarctation. This test isn’t often used to diagnose coarctation of the aorta, but your doctor may use it to help plan surgery or other treatment, if you need it. Catheter procedures may be used to perform certain treatments for coarctation of the aorta.
Coarctation of the aorta treatment
Treatment options for coarctation of the aorta depend on your age at the time of diagnosis and the severity of your condition. Other heart defects might be repaired at the same time as aortic coarctation.
Treatment approaches usually consist of surgery or a procedure called balloon angioplasty or stent placement. A doctor trained in congenital heart conditions will evaluate you and determine the most appropriate treatment for your condition.
- For symptomatic neonates, prostaglandin E1 infusion
- For hypertension, beta-blockers
- Surgical correction or balloon angioplasty (sometimes with stent placement)
- Symptomatic neonates are treated promptly. In infants who do not have symptoms, the condition is monitored until definitive repair is done.
Medical management of coarctation of the aorta
Medication isn’t used to repair coarctation of the aorta, but it might be used to control blood pressure before and after stent or surgery. Although repairing aortic coarctation improves blood pressure, many people still need to take blood pressure medication, even after a successful surgery or stenting.
Babies with severe coarctation of the aorta often are given a medication that keeps the ductus arteriosus open. This provides a bypass for blood flow around the constriction until the coarctation is repaired.
Symptomatic neonates require cardiopulmonary stabilization with infusion of prostaglandin E1 (0.01 to 0.10 mcg/kg/min—titrate to the lowest effective dose) to reopen the constricted ductus arteriosus. Opening the ductus and its aortic ampulla provides some relief by allowing pulmonary artery blood to bypass the aortic obstruction via the ductus and increase perfusion of the descending aorta, improving systemic perfusion and reversing metabolic acidosis.
Diuretics can help treat heart failure symptoms. IV cardioactive drugs (eg, milrinone, dopamine, dobutamine) can be useful in select circumstances (eg, infants with heart failure and significant left ventricle dysfunction).
In nonemergent situations, patients with hypertension may be treated with beta-blockers; ACE inhibitors may adversely affect renal function. After repair of the coarctation, hypertension may persist or develop years after repair and can be treated with beta-blockers, ACE inhibitors, angiotensin II receptor blockers, or calcium channel blockers.
Supplemental oxygen should be used with caution in neonates because the resulting decrease in pulmonary vascular resistance may increase pulmonary blood flow at the expense of systemic blood flow.
Coarctation of aorta surgery
Most newborns with symptoms will have surgery either right after birth or soon afterward. First they will receive medications to stabilize them.
Children who are diagnosed when they are older will also need surgery. Usually, the symptoms are not as severe, and more time will be taken to plan for surgery.
Surgical options include:
- Resection with end-to-end anastomosis. This method involves removing the narrowed segment of the aorta (resection) followed by connecting the two ends of the aorta together (anastomosis).
- Subclavian flap aortoplasty. A portion of the blood vessel that delivers blood to your left arm (left subclavian artery), might be used to expand the narrowed area of the aorta.
- Bypass graft repair. This technique involves bypassing the narrowed area by inserting a plastic tube called a graft between the portions of the aorta.
- Patch aortoplasty. Your doctor might treat your coarctation by cutting across the narrowed area of the aorta and then attaching a patch of synthetic material to widen the blood vessel. Patch aortoplasty is useful if the coarctation involves a long segment of the aorta.
- Balloon angioplasty, often with stenting, is an option for initially treating aortic coarctation or for treating re-narrowing (re-coarctation) that has occurred after surgery. During this procedure, your doctor inserts a thin, flexible tube (catheter) into an artery in your groin and threads it through your blood vessels to your heart using X-ray imaging. Your doctor places an uninflated balloon through the opening of the narrowed aorta. When the balloon is inflated, the aorta widens and blood flows more easily. In some cases, your doctor may insert a mesh-covered hollow tube (stent) in the aorta to keep the narrowed part of the aorta open.
The preferred definitive treatment is controversial. Some centers prefer balloon angioplasty with or without stent placement, but most prefer surgical correction and reserve the balloon procedure for re-coarctation after surgical correction or for primary treatment of discrete coarctation in older children or adolescents. Initial success rate after balloon angioplasty is about 73% in patients with native coarctation and about 80% in patients with recurrent coarctation. Subsequent catheterization can dilate the stent as children grow.
Surgical options include resection and end-to-end anastomosis, patch aortoplasty, and left subclavian flap aortoplasty. In severe coarctation manifesting early in life, the transverse aorta and isthmus are often hypoplastic, and this region of the aorta may need to be surgically enlarged.
Choice of surgical technique depends on anatomy and center preference. Surgical mortality rate is < 5% for symptomatic infants and <1% for older children. Residual coarctation is common (6 to 33%). Rarely, paraplegia results from cross-clamping of the aorta during surgery.
Endocarditis prophylaxis is not needed preoperatively and is required only for the first 6 mo after repair.
During surgery, the narrowed part of the aorta will be removed or opened. If the problem area is small, the two free ends of the aorta may be re-connected. This is called an end-to-end anastomosis. This usually resolves the hypertension unless renal damage has occurred.
If a large part of the aorta is removed, a Dacron graft (a man-made material) or one of the patient’s own arteries may be used to fill the gap. A tube graft connecting two parts of the aorta may also be used.
Sometimes, doctors will try to stretch open the narrowed part of the aorta by using a balloon that is widened inside the blood vessel. This type of procedure is called a balloon angioplasty. It may be done instead of surgery, but it has a higher rate of failure.
Older children usually need medicines to treat high blood pressure after surgery. Some will need lifelong treatment for this problem.
Medical management of heart failure should be dictated by the clinical picture.
After treatment
The American College of Cardiology/American Heart Association 3 guidelines recommend that patients who have had surgical repair or percutaneous intervention for coarctation of the aorta should have at least a yearly follow–up and, the evaluation of the coarctation repair site by MRI/CT, should be performed at intervals of 5 years or less, depending on the specific anatomic findings before and after repair. Even if the coarctation repair appears to be satisfactory, late postoperative thoracic aortic imaging should be performed to assess for aortic dilatation or aneurysm formation. Magnetic resonance imaging has a limited role in CoA after stent placement since the metallic artifact (or noise) prevents detailed evaluation of the aortic segment within the stent, despite adequate visualization of the aorta proximal and distal to the stent.
The most common long-term complication of coarctation of the aorta is high blood pressure. Although your blood pressure usually falls after the aortic coarctation has been repaired, it might still remain higher than normal.
Occasionally, the segment of the aorta that has been repaired will become weak and enlarge (aortic aneurysm) and might eventually rupture. In some cases, the coarctation can recur, possibly even years after treatment. It’s possible to have additional surgeries or procedures to correct the re-narrowing or treat other complications.
Lifestyle and home remedies
Although coarctation of the aorta may be repaired, you’ll need careful follow-up throughout life in order for doctors to monitor you for complications and recurrences.
Your doctor may suggest that you have regular follow-up appointments with a doctor who specializes in congenital heart disease. In follow-up appointments, your doctor may evaluate you and order imaging tests to monitor your condition. Your doctor will also check your blood pressure and treat it as needed.
Here are a few tips for managing your condition:
- Get regular exercise. Regular exercise helps lower blood pressure. Talk to your doctor about whether you need to restrict certain physical activities, such as weightlifting, which can temporarily raise your blood pressure. Your doctor may evaluate you and conduct exercise tests prior to deciding if you should participate in competitive sports or weightlifting.
- Consider pregnancy carefully. Before becoming pregnant, talk to your doctor to determine if you can undergo pregnancy safely. Women with coarctation of the aorta, even after repair, may have a higher risk of aortic rupture, aortic dissection or other complications during pregnancy and delivery. Doctors will also evaluate whether your blood pressure is controlled. If you have had aortic coarctation repair and are considering becoming pregnant, careful management of your blood pressure is important to help keep you and your baby healthy.
- Prevent endocarditis. Endocarditis is an inflammation of the inner lining of the heart or of its structures, caused by a bacterial infection. You generally won’t need to take antibiotics before certain dental procedures to prevent endocarditis. However, if you’ve had endocarditis in the past, or if you had a stent placed or had valve replacement surgery, then your doctor may recommend antibiotics.
- Jurcut R, Daraban A, Lorber A, et al. Coarctation of the aorta in adults: what is the best treatment? Case report and literature review . Journal of Medicine and Life. 2011;4(2):189-195. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3124275[↩]
- Bjornard, K., Riehle-Colarusso, T., Gilboa, S. M. and Correa, A. Patterns in the prevalence of congenital heart defects, metropolitan Atlanta, 1978 to 2005. Birth Defects Res Part A: Clin Mol Teratol. 2013;97:87–94.[↩]
- Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: a reportof the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease) . Circulation. 2008;118:714–833. http://circ.ahajournals.org/content/118/23/e714.long[↩]





{kind=link}