
Contents
- What is complex regional pain syndrome
- Complex regional pain syndrome prognosis
- Complex regional pain syndrome pictures
- Complex regional pain syndrome stages
- Complex regional pain syndrome complications
- Complex regional pain syndrome causes
- Complex regional pain syndrome pathophysiology
- Complex regional pain syndrome prevention
- Complex regional pain syndrome symptoms
- Complex regional pain syndrome diagnosis
- Complex regional pain syndrome treatment
- Rehabilitation and physical therapy and occupational therapy
- Psychotherapy
- Medications
- Sympathetic nerve block
- Surgical sympathectomy
- Spinal cord stimulation
- Dorsal root ganglion stimulation
- Other types of neural stimulation
- Epidural infusion
- Intrathecal drug pumps
- Topical Treatments
- Emerging treatments
- Amputation
- Coping and support
What is complex regional pain syndrome
Complex regional pain syndrome (CRPS), also known as reflex sympathetic dystrophy or causalgia, is a chronic (lasting greater than 3 months) pain condition that is regional pain (not in a specific nerve territory or dermatome) most often affects one limb (arm, leg, hand, or foot) usually after an injury, a surgery, a stroke or a heart attack 1, 2, 3, 4, 5, 6, 7, 8, 9, 10. The pain is out of proportion to the severity or duration to the usual course of pain after such tissue trauma 11. For example, complex regional pain syndrome is a syndrome that can occur after simple injuries such as a sprained ankle or a broken arm. Complex regional pain syndrome (CRPS) is characterized by signs indicating autonomic and neuro-inflammatory changes in the affected body region varying between patients and over time. Complex regional pain syndrome is characterized by prolonged or excessive pain and changes in skin color, temperature, stiffness, weakness and/or swelling in the affected area. Often, complex regional pain syndrome (CRPS) is accompanied by significant emotional distress or functional disability. Complex regional pain syndrome is believed to be caused by damage to or malfunction of, the peripheral nervous system (nerves that are located outside of your brain and spinal cord) and central nervous system (brain and spinal cord) 12, 13, 4, 14. Complex regional pain syndrome is almost three or four times more common in women than in men, and peaks in onset between the ages of 50 and 70 years 15. Given the changes in diagnostic criteria and the evolving understanding of complex regional pain syndrome process, studies vary on the actual incidence of complex regional pain syndrome. The overall incidence rates of complex regional pain syndrome can range anywhere from approximately 5 to 29 per 100,000 people each year, with the highest incidence typically occurring in females between 61 and 70 years of age 16, 17, 18. Based on the epidemiological studies available, complex regional pain syndrome appears to be more common in patients of North European ancestry, although it does appear to occur frequently in those of South Korean ancestry as well 17, 18. In the United States, it is estimated that there are at least 50,000 cases of complex regional pain syndrome type 1 each year 19. Similarly, with the variation in complex regional pain syndrome diagnostic criteria over the years the incidence among patients with fractures is anywhere from 0.05% to 0.2% in older studies and 3% to 7% in more recent studies 20. The upper extremity is affected more frequently than the lower extremity 17.
Signs and symptoms of complex regional pain syndrome include:
- Continuous burning or throbbing pain, usually in your arm, leg, hand or foot
- Sensitivity to touch or cold
- Swelling of the painful area
- Changes in skin temperature — alternating between sweaty and cold
- Changes in skin color, ranging from white and mottled to red or blue
- Changes in skin texture, which may become tender, thin or shiny in the affected area
- Changes in hair and nail growth
- Joint stiffness, swelling and damage
- Muscle spasms, tremors, weakness and loss (atrophy)
- Decreased ability to move the affected body part
Symptoms may change over time and vary from person to person. Pain, swelling, redness, noticeable changes in temperature and hypersensitivity particularly to cold and touch usually occur first.
Over time, the affected limb can become cold and pale. It may undergo skin and nail changes as well as muscle spasms and tightening. Once these changes occur, the condition is often irreversible.
Complex regional pain syndrome occasionally may spread from its source to elsewhere in your body, such as the opposite limb.
In some people, signs and symptoms of complex regional pain syndrome go away on their own. In others, signs and symptoms may persist for months to years. Treatment is likely to be most effective when started early in the course of the illness.
Complex regional pain syndrome is divided into two types 21:
- Complex regional pain syndrome type 1: Individuals without a confirmed nerve injury are classified as having Complex regional pain syndrome type 1 (previously known as reflex sympathetic dystrophy syndrome).
- Complex regional pain syndrome type 2: Complex regional pain syndrome type 2 (previously known as causalgia) is when there is an associated, confirmed nerve injury.
As some research has identified evidence of nerve injury in complex regional pain syndrome type 1, it is unclear if this disorder will always be divided into two types 22, 23, 24, 25, 26. Nonetheless, the treatment is similar. Both subtypes of complex regional pain syndrome are characterized by severe pain that is disproportionate to the inciting event, most commonly affecting the hand or foot but which can spread to other body regions 27. Additionally complex regional pain syndrome presents with some or all of the following symptoms in the affected body parts: sensory disturbances, temperature changes, abnormal patterns of sweating, swelling and edema, reduced joint range of motion, movement abnormalities such as weakness, tremor or dystonia, trophic changes such as skin atrophy or altered hair and nail growth, and localized osteoporotic changes 28; and alterations in body perception or schema 29.
Complex regional pain syndrome is often described in terms of “warm” changes and “cold” changes, although they are not separate diagnostic categories. Warm complex regional pain syndrome is associated with a warm, redness of the skin, swelling of extremity and tends to be correlated with inflammatory changes earlier in the disease course; one study described these changes within the first eight months 30. Cold complex regional pain syndrome is associated with a cold, dusky, sweaty extremity and is more often associated with chronic complex regional pain syndrome; in one study, cold symptoms lasted for more than nine months 30. The same extremity can have both warm and cold symptoms, and the disease pattern and clinical course vary among patients 31, 32, 33.
Complex regional pain syndrome symptoms vary in severity and duration, although some cases are mild and eventually go away. In more severe cases, individuals may not recover and may have long-term disability.
Although it is more common in women, complex regional pain syndrome can occur in anyone at any age, with a peak at age 40. Complex regional pain syndrome is rare in the elderly. Complex regional pain syndrome is uncommon in children under age 10.
At the consensus meeting of the International Association for the Study of Pain (IASP) in Budapest in 2004, the Budapest criteria for the diagnosis of complex regional pain syndrome were developed 34, 32. In an effort to enhance specificity, the Budapest clinical diagnostic criteria for complex regional pain syndrome included both symptoms and signs of the disease. The Budapest criteria is 99% sensitive and 68% specific for complex regional pain syndrome, with increased sensitivity as other diagnoses are ruled out 34, 35. The Budapest criteria were formally accepted by the International Association for the Study of Pain (IASP) in 2012 after more robust validation testing 36. It should be noted that a 4 of 4 symptom decision rule is recommended when applying the Budapest criteria for research purposes 35. The Budapest criteria, are listed in Table 1 below.
Additional clinical findings in complex regional pain syndrome 37:
- Allodynia
- pain on light movement/touch/pressure
(e.g., draught, brush, finger [pressure less than 100 g/cm² or load less than 500 g]) - pain from vibration (e.g. tuning fork on a bony prominence), cold, heat
- pain on light movement/touch/pressure
- Hyperalgesia
- periarticular pressure hyperalgesia distal to the site of injury/surgery
- solitary sharp stimulus (pinprick) is felt stronger/longer
- Disturbance of body perception/interoception
- attention: exerted, hypervigilant focussing or disregarding (neglect-like/dissociation)
- shape, size, weight, position, posture, laterality, symmetry, ownership, e.g., as if limbs were detached, foreign, dead (“as if wooden”, “like part of a dead body”)
- attribution of meaning or affective evaluation, e.g., threatening, disgusting, or hated limb; caution: desire for amputation
- Functional disturbances of voluntary motor function
- protective posture, slowed, reduced or non-movement
- reduced experience of motor action, control, intention (agency)
- weakness, disturbances of fine motor skills, coordination or movement
- sometimes several types of disturbance inone and the same limb, e.g.
- myoclonus or tremor (with “entrainment”, i.e. unconscious synchronization with rhythmic movements of the unaffected limb)
- dystonia (usually in fixed flexion/supination)
- increase during manipulation, decrease when distracted, no decrease with sensory tricks
- Trophic, vasomotor and sudomotor disturbances
- non-pitting edema (circumference measurements where possible)
- skin color usually reddish-blue, with time more waxy-pale
- skin temperature about 1–2 degrees difference to the contralateral side
- hair growth: usually increased, thick, dark, sometimes reduced, finer hair
- nail growth: usually harder, brittle, faster or slower nail growth
- increased, with time reduced, sweating
- trophic skin lesions or pressure lesions
- Tendency to spread and become generalized
- at times tendency to spread proximally or to other limbs
- other pain sites; contralateral and generalized reduced pain threshold/body image disturbance
- sensitivity to noise, light, smell, touch, at times with autonomic arousal
- cardiovascular dysregulation, increased heart rate, reduced heart rate variability
- micturition and digestive problems
- Affective, cognitive, general signs and symptoms; behavioral changes
- fear, particularly of touch, movement, and disease progression
- avoidance of sensory stimuli from clothes, wind, movement, other people, etc.
- signs and symptoms of trauma-related disorders (helplessness, flashbacks, dissociation, depersonalization, avoidance, hypervigilance/hyperarousal)
- mood fluctuations, depressiveness, alexithymia (reduced awareness of one’s own emotions and those of others), withdrawal
- fatigue, sleeping problems, and cognitive disturbances
Table 1. The Budapest clinical diagnostic criteria for complex regional pain syndrome
| 1. Continuing pain, which is disproportionate to any inciting event |
2. Must report at least one symptom in all four following categories
|
3. Must display at least one sign at time of evaluation in two or more of the following categories
|
| 4. There is no other diagnosis that better explains the signs and symptoms |
Complex regional pain syndrome type 1 (Sudeck’s atrophy or Reflex sympathetic dystrophy)
Reflex sympathetic dystrophy syndrome or Sudeck’s atrophy involves a disturbance in the sympathetic nervous system. The latter is the the network of nerves that controls many bodily functions and in the skin it is responsible for opening and closing blood vessels, and controlling sweat glands. In complex regional pain syndrome type 1 there is pain, as well as swelling and disability (often after injury) associated with other signs of sympatethic nerve dysfunction (initially warm and dry, and later cold and moist skin) in the affected area. It primarily affects the hands and feet.
Complex regional pain syndrome type 1 (Sudeck’s atrophy) is reasonably common – it may occur after as many as 5% of traumatic injuries. Complex regional pain syndrome type 1 frequently occurs between the ages of 40 and 60 but also can occur in children and the elderly. Complex regional pain syndrome type 1 is more common among women.
- The condition may follow weeks or months after the initial cause – whether it be trauma, myocardial infarct or other.
- It classically is said to go through 3 stages
- Early on there is throbbing, burning pain with the site red, warm and swollen;
- After weeks or months the overlying skin may become cold, mottled, and shiny with stiffness and often underlying osteoporosis.
- Later the pain continues, with associated muscle atrophy and there may also be contractures.
Risk Factors for Complex regional pain syndrome 1 (Sudeck’s atrophy, Reflex sympathetic dystrophy)
- It may occur spontaneously (i.e. without any cause) -but more commonly it follows trauma (fractures, ligament and muscle strains, nerve or soft tissue injuries) which may seem trivial.
- It is believed to be due to prolonged immobilization following the injury.
- It can also be associated with medical conditions – diabetes, stroke/heart attack, thyroid disease, cancer, infections.
Complex regional pain syndrome type 2 (Causalgia)
Complex regional pain syndrome type 2 (causalgia) is a chronic pain condition seen after the section (damage, cutting) of a nerve. It is characterized by a chronic burning pain and hypersensitivity in the area supplied by that nerve.
The sympathetic nerve supply of the involved area is believed to be important in the cause of complex regional pain syndrome type 2 (causalgia). The sympathetic nervous system is a network of nerves (separate from the set of nerves controlling voluntary activities) which controls a lot of bodily functions (like our heart rate, intestinal activity) as well as being important in pain perception and skin blood supply.
- Complex regional pain syndrome type 2 most commonly follows trauma.
- Complex regional pain syndrome type 2 is seen occasionally following amputation.
In the majority of people onset of the pain is within 24 hours of injury.
This condition is most common in people between the ages of 40-60, but has been seen in younger people also.
Medical therapy is usually ineffective.
Sympathetic block: 18-25% of patients have satisfactory long-lasting relief after a series of nerve blocks using a local anesthetic injection.
Surgical sympathectomy: This involves cutting the sympathetic nerves to that area of the body, and it relieves pain in more than 90% of patients. Sympathectomy has been reported to provide complete relief in over 80% and significant relief in 95% of patients with causalgia. The risk of significant complication is approximately 5%. These include a pneumothorax (punctured lung), intercostal nerve pain, spinal cord injury, and Horner’s syndrome (droopy eyelid due to nerve damage).
Complex regional pain syndrome prognosis
The outcome of complex regional pain syndrome is highly variable. Younger persons, children, and teenagers tend to have better outcomes. While older people can have good outcomes, there are some individuals who experience severe pain and disability despite treatment. Anecdotal evidence suggests early treatment, particularly rehabilitation, is helpful in limiting the disorder, a concept that has not yet been proven in clinical studies.
Retrospective chart reviews document a variety of outcomes in patients with complex regional pain syndrome, from full resolution of symptoms to persistent, chronic pain that lasts for years. One study suggests that complex regional pain syndrome usually resolves spontaneously without treatment, although the time frame is not specified 39. Two studies showed that only a minority of patients develop chronic and severely disabling symptoms. A Dutch study showed severe progression of symptoms in 16% of patients, and 54% of patients were stable. Of the 54 out of 102 patients who were working before the complex regional pain syndrome diagnosis, 41% returned to work without restrictions, 28% returned to work with some restrictions, and 31% were not able to return to work 17. A population-based study in the United States showed resolution of symptoms in 74% of patients 39. Worse outcomes are associated with upper extremity limb involvement and cold complex regional pain syndrome symptoms 17.
Worsening psychological distress in conjunction with physical injury has been demonstrated to increase the risk of complex regional pain syndrome and the severity of complex regional pain syndrome symptoms at six- and 12-month intervals 40. Disuse of the painful extremity, a learned behavior for avoiding pain, is also predictive of severe complex regional pain syndrome symptoms, including joint pain with movement, hyperalgesia, hair growth changes, and changes in skin temperature 30.
Complex regional pain syndrome pictures
Figure 1. Acute complex regional pain syndrome with hyperemia, swelling and glossy skin

Figure 2. Complex regional pain syndrome – chronic, cold type complex regional pain syndrome with blue discoloration of the fingers, glossy skin, and increased hair and nail growth.

Figure 3. Complex regional pain syndrome – related dystonia of the left ankle and foot with plantar flexion and inversion of the ankle, and flexion of the toes; edema and increased hair growth are also clearly visible.

Complex regional pain syndrome stages
The staging of complex regional pain syndrome is a concept that is no longer used in clinical practice. The course of the disease seems to be so unpredictable between various patients that staging is NOT helpful in the diagnosis and treatment of complex regional pain syndrome. The following stages are presented in these guidelines merely for historical significance.
Stage 1
- Onset of severe, pain limited to the site of injury
- Increased sensitivity of skin to touch and light pressure (hyperasthesia).
- Localized swelling
- Muscle cramps
- Stiffness and limited mobility
- At onset, skin is usually warm, red and dry and then it may change to a blue (cyanotic) in appearance and become cold and sweaty.
- Increased sweating (hyperhydrosis).
- In mild cases this stage lasts a few weeks, then subsides spontaneously or responds rapidly to treatment.
Stage 2
- Pain becomes even more severe and more diffuse
- Swelling tends to spread and it may change from a soft to hard (brawny) type
- Hair may become coarse then scant, nails may grow faster then grow slower and become brittle, cracked and heavily grooved
- Spotty wasting of bone (osteoporosis) occurs early but may become severe and diffuse
- Muscle wasting begins
Stage 3
- Marked wasting of tissue (atrophic) eventually become irreversible.
- For many patients the pain becomes intractable and may involve the entire limb.
- A small percentage of patients have developed generalized complex regional pain syndrome affecting the entire body.
Complex regional pain syndrome complications
If complex regional pain syndrome isn’t diagnosed and treated early, the disease may progress to more-disabling signs and symptoms. These may include:
- Tissue wasting (atrophy). Your skin, bones and muscles may begin to deteriorate and weaken if you avoid or have trouble moving an arm or a leg because of pain or stiffness.
- Muscle tightening (contracture). You also may experience tightening of your muscles. This may lead to a condition in which your hand and fingers or your foot and toes contract into a fixed position.
Complex regional pain syndrome causes
It is unclear why some individuals develop complex regional pain syndrome while others with similar trauma do not 41, 42, 43. In more than 90 percent of cases, complex regional pain syndrome is triggered by a clear history of trauma or injury 44, 45, 46. The most common triggers are fractures, sprains/strains, soft tissue injury (such as burns, cuts, or bruises), limb immobilization (such as being in a cast), surgery, or even minor medical procedures such as needle stick. Although complex regional pain syndrome can develop after any injury, the most common initiating events are fractures, surgery, crush injuries, and sprains 47. Complex regional pain syndrome represents an abnormal response that magnifies the effects of the injury. Some people respond excessively to a trigger that causes no problem for other people, such as what is observed in people who have food allergies.
Peripheral nerve abnormalities found in individuals with complex regional pain syndrome usually involve the small unmyelinated and thinly myelinated sensory nerve fibers (axons) that carry pain messages and signals to blood vessels. Myelin is a mixture of proteins and fat-like substances that surround and insulate some nerve fibers. Because small fibers in the nerves communicate with blood vessels, injuries to the fibers may trigger the many different symptoms of complex regional pain syndrome. Molecules secreted from the ends of hyperactive small nerve fibers are thought to contribute to inflammation and blood vessel abnormalities. These peripheral nerve abnormalities in turn trigger damage in the spinal cord and brain.
Blood vessels in the affected limb may dilate (open wider) or leak fluid into the surrounding tissue, causing red, swollen skin. The dilation and constriction of small blood vessels is controlled by small nerve fiber axons as well as chemical messengers in the blood. The underlying muscles and deeper tissues can become starved of oxygen and nutrients, which causes muscle and joint pain as well as damage. The blood vessels may over-constrict (clamp down), causing cold, white, or bluish skin.
Complex regional pain syndrome also affects the immune system. High levels of inflammatory chemicals (cytokines) have been found in the tissues of people with complex regional pain syndrome. These contribute to the redness, swelling, and warmth reported by many affected individuals. Complex regional pain syndrome is more common in individuals with other inflammatory and autoimmune conditions such as asthma.
Limited data suggest that complex regional pain syndrome also may be influenced by genetics. Rare family clusters of complex regional pain syndrome have been reported. Familial complex regional pain syndrome may be more severe with earlier onset, greater dystonia, and more than one limb being affected. When comparing patients with sporadic complex regional pain syndrome to families where two or more patients are affected, familial complex regional pain syndrome patients had a younger age at onset and more often had multiple affected extremities and dystonia 48. A recent study demonstrated that a single nucleotide polymorphism in four genes, ANO10, P2RX7, PRKAG1, and SLC12A9, is associated with developing complex regional pain syndrome type 1 with males typically expressing these rare alleles 49. Other genetic studies have demonstrated associations between complex regional pain syndrome and several major histocompatibility complex alleles, including human leukocyte antigen (HLA)-DR6, HLA-DR13, HLA-DR2, HLA-DQ1, HLA-B62, and HLA-DQ8 50. Genome-wide expression profiling of the whole blood has shown that HLA-A29.1, matrix metallopeptidase 9 (MMP9), alanyl aminopeptidase (AAP), histidine decarboxylase (HDC), granulocyte colony-stimulating factor 3 receptor (G-CSF3-R), and signal transducer and activator of transcription 3 genes (STAT-3) were highly expressed when compared to unaffected controls 51. Further genetic and transcriptomic studies hold the promise to predict patient predispositions to complex regional pain syndrome, unravel the molecular mechanisms of complex regional pain syndrome pathogenesis, and discover novel therapeutic targets for complex regional pain syndrome 52.
Occasionally complex regional pain syndrome develops without any known injury. In these cases, an infection, a blood vessel problem, or entrapment of the nerves may have caused an internal injury. A physician will perform a thorough examination in order to identify a cause.
In many cases, complex regional pain syndrome results from a variety of causes. In such instances, treatments are directed at all of the contributing factors.
Risk factors for developing complex regional pain syndrome
Potential risk factors for developing complex regional pain syndrome 37:
- Female sex, in particular postmenopausal women (women of middle age also sustain fractures three times more often than men)
- Severe injuries, in particular crush injuries, displaced, juxta-articular or intra-articular fractures (especially distal radius fractures); ankle injuries; nerve injuries; prolonged anesthesia/ischemia, manipulation procedures such as secondary fracture reductions; restricted range of motion and functional impairment, prolonged immobilization
- High pain intensity initially or directly after surgery, sensory disturbances and low skin temperature (for example, persistent pain ≥5 on a numerical rating scale of 10 points for more than a week after conservative treatment of a distal radius fracture)
- Chronic or widespread pain and hypersensitivity, such as migraine, fibromyalgia, back/period pain, neuropathies, osteoporosis, osteoarthritis, rheumatoid arthritis; also, asthma/allergies
- High anxiety level, depressiveness, passivity, avoidance tendency, pain catastrophizing, or manifest disorders associated with anxiety and trauma/stress; previous critical life events; desire for compensation and litigation.
Extremity injuries, such as fractures or sprains, surgery, and carpal tunnel syndrome have been the most commonly reported inciting events leading to complex regional pain syndrome 44, 46, 53. In a recent analysis of 1043 patients with complex regional pain syndrome, the most common primary causes were fractures (42%), blunt traumatic injuries excluding fractures (e.g., sprains) (21%), surgery (12%), and carpal tunnel syndrome (7%), while 7% had no clear precipitating event 44. However, the overall prevalence of complex regional pain syndrome associated with these inciting events remains relatively low. Crijns et al. 54 found that out of 59,765 patients treated for distal radius fractures, 0.19% were diagnosed with complex regional pain syndrome. A similar more recent study noted a 0.64% incidence of complex regional pain syndrome after 172,194 patients receiving surgical treatment for distal radius fractures 46. Complex regional pain syndrome had previously been reported as a common complication of Dupuytren contracture, but a very recent analysis of a nationwide database found the overall incidence to be 0.31% 55.
Multiple studies have demonstrated complex regional pain syndrome to be much more prevalent in women, with estimates of 2–4 times the rate in men 44, 46, 56, 57, 58. Van Velzen et al. 58 further investigated these sex-related differences, finding that male complex regional pain syndrome patients were more likely to suffer from depression and kinesiophobia, and use passive pain coping strategies. Fibromyalgia is strongly and independently associated with a diagnosis of complex regional pain syndrome, increasing the risk up to 2.5 times that of controls 54, 59. Other musculoskeletal conditions, such as rheumatoid arthritis, may also increase the risk 60. Although complex regional pain syndrome and other autonomic disorders have been anecdotally reported as adverse events after human papillomavirus (HPV) vaccination, review of published reports and a small population-based case series found no statistically significant correlation 61, 62, 63.
Complex regional pain syndrome pathophysiology
Despite being studied for over two decades, the pathogenesis of complex regional pain syndrome remains obscure 64, 65. Complex regional pain syndrome is considered a multifactorial condition with several contributors: classic inflammation, neurogenic inflammation, impairment of the autonomic nervous system and changes of the central nervous system (CNS) 21. Experts believe that complex regional pain syndrome develops when persistent noxious stimuli from an injured body region leads to peripheral and central sensitization, whereby primary afferent nociceptive mechanisms demonstrate abnormally heightened sensation, including spontaneous pain and hyperalgesia 66. Allodynia (a condition where a stimulus that normally wouldn’t cause pain results in pain, for example, a light touch from a feather might cause pain instead of just a sensation) and hyperalgesia (an abnormally increased sensitivity to feeling pain and an extreme response to pain) occur when central nervous system (brain and spinal cord) somatosensory processing misinterprets normal nonpainful mechanical stimuli, such as light touching of the skin, as painful. Therefore, skin in the injured area becomes more sensitive to all stimuli, even nonpainful stimuli. In addition, the sensitization can extend beyond the originally injured area, thus enlarging the region of aberrant pain perception.
A similar impairment of central nervous system (brain and spinal cord) processing leads to motor abnormalities, such as weakness or tremor in the affected area. The peripheral and central sensitization associated with impaired central nervous system (brain and spinal cord) processing is linked to proposed disturbances within the sympathetic nervous system that lead to sympathetic hyperactivity adversely affecting the injured area. Studies suggest that an augmented inflammatory response coupled with impaired healing further contribute to the refractory nature of malevolent complex regional pain syndrome 67, 68, 69, 70, 71, 72.
Figure 4. Complex regional pain syndrome pathophysiology
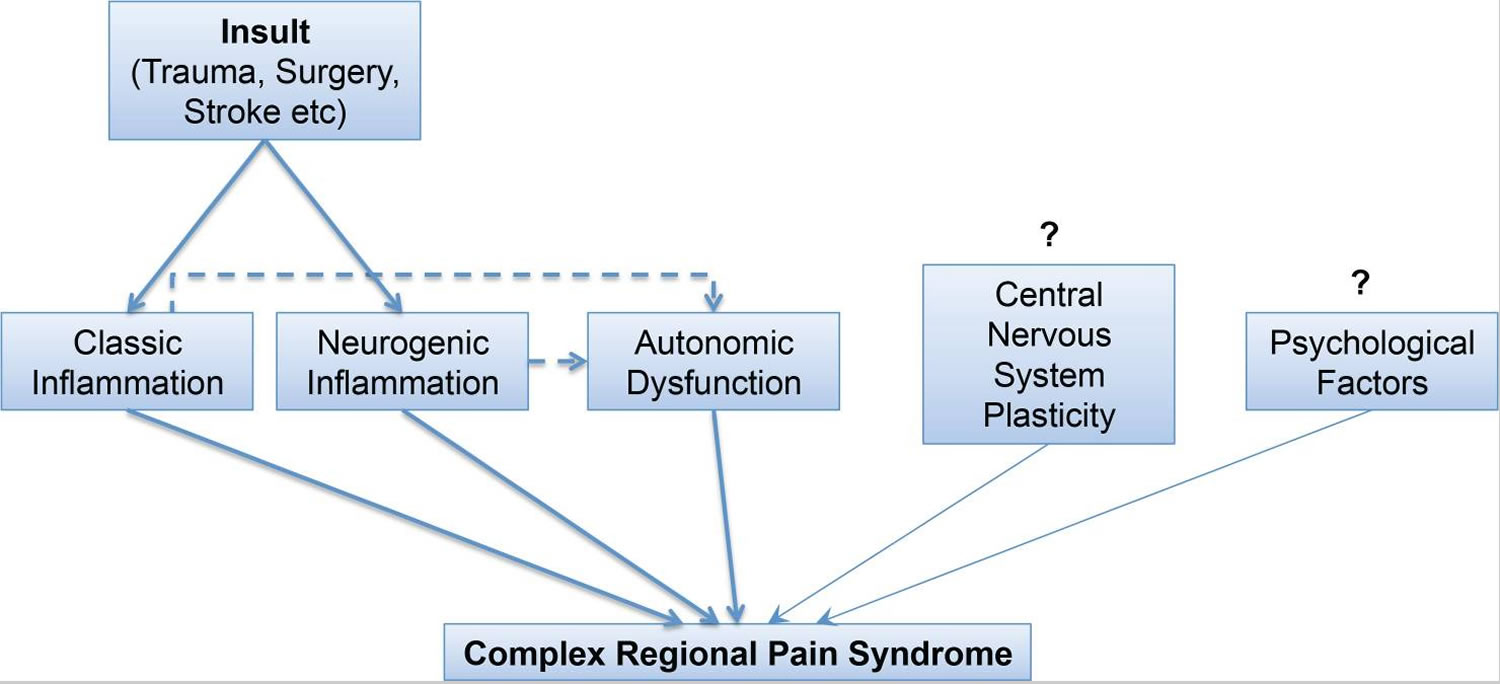
Footnotes: Pathophysiological connections in the complex regional pain syndrome. An insulting event triggers classic and neurogenic inflammation, which are responsible for the inflammatory signs at least of the warm phase and, perhaps, contribute to the autonomic dysfunction. Autonomic dysfunction is also responsible for several aspects of the syndrome, while interventions targeting it have been beneficial, mainly in case series. Central nervous system (brain and spinal cord) plasticity and psychological factors likely complete the process. However, the exact mechanisms eliciting the central nervous system (brain and spinal cord) changes, linking to the psychological factors and ultimately implicating both of these factors to the clinical presentation of the syndrome are still obscure.
[Source 21 ]Neurogenic inflammation
Neurogenic inflammation probably plays a central part in the development of complex regional pain syndrome 21, 73. It begins with the stimulation of the peripheral endings of the nociceptive C-fibres, which, subsequently, conduct the stimulus not only afferently to the dorsal ganglia, but also efferently through branches extending back into the afflicted tissue. This backward firing results in the release of several pro-inflammatory neuropeptides the most important being substance P, calcitonin gene-related peptide (CGRP) and neurokinin A, as well as others including adrenomedullin, neurokinin B, vasoactive intestinal peptide, neuropeptide Y and gastrin-releasing peptide 74. Calcitonin gene-related peptide (CGRP) activates CGRP1 receptor in smooth muscles and endothelial cells inducing vasodilation of arterioles, while substance P and neurokinin A promote vascular permeability by activating neurokinin A1 receptors in endothelial cells 75, 74. These changes result in hyperemia, tissue edema and exudation of leukocytes. Besides, calcitonin gene-related peptide (CGRP) and substance P activate resident cells, such as mast and dendritic cells. These, in turn, release inflammatory mediators including histamine, serotonin, TNFα that attract inflammatory cells and further promote inflammation, but also act upon local nociceptive Aδ-fibers inducing peripheral nerve sensitization 74, 76. Finally, CGRP promotes sweat gland function, as well as hair growth 75, 74.
Central Nervous System-Brain Plasticity
Some studies suggest maladaptive neuroplasticity of the motor and somatosensory cortex. In 2000 Birklein et al. 77 published an analysis of 145 cases studying the neurological findings in complex regional pain syndrome. Ninety-seven percent of patients manifested motor dysfunction such as tremor, exaggerated reflexes, dystonia and myoclonic jerks 77. The brain areas that seem to participate in the motor dysfunction are the primary motor cortex, supplementary motor cortices and posterior parietal cortices. The reorganization of the central motor circuits is thought to lead to an increased activation of the motor cortex and to motor dysfunction of the affected extremity 78. However, a systematic review published in 2013 concluded that there was no significant impairment in the representation of the affected limb on the motor cortex 79.
Changes in the somatosensory cortex have been investigated by several researchers in order to explain hyperalgesia. The affected body part seems to be represented on a smaller area on the primary somatosensory cortex 80. Sensory stimuli on the affected extremity trigger a complex cortical network, including areas of nociceptive, cognitive and motor processing different than the pattern triggered by similar stimuli on the unaffected side. Consequently, the patient does not only feel pain during the movement of the hand or leg, but also with the thought of movement 81. Furthermore, it is hypothesized that the continuous nociceptive stimulation induces plastic changes in the motor and somatosensory networks, so that hyperalgesia and chronic pain is not only the consequence of changes in the central nervous system, but also the cause 82.
Peripheral sensitization
In peripheral sensitization, repetitive noxious stimulation of C fibers results in heightened sensitivity, coupled with reduced stimulus thresholds and prolonged activation of dorsal horn cells, particularly those with excitatory glutamine receptors. The resultant excitation is largely due to a myriad of inflammatory mediated processes that includes actions by substance P, calcitonin gene-related peptide (CRGP), leukotrienes, prostaglandins, histamine, bradykinin, and serotonin, all of which have versatile ligand properties that further compound the inflammatory process and algogenic states 83.
It is known that tissue trauma can cause the release of cytokines and nerve growth factor which further activate nociceptors by stimulating the release of inflammatory or excitatory amino acids and neuropeptides in primary afferent neurons as previously noted thus contributing to long-term peripheral sensitization 84.
Sympathetically maintained pain
Several factors indicate the role of the sympathetic nervous system (SNS) in the appearance of complex regional pain syndrome. Those include changes in skin color, hyper- or hypohidrosis and changes in the extremity skin temperature 85. Systemic manifestations of sympathetic dysfunction have even been observed, such as increased heart rate, reduced heart rate variability and impaired orthostatic response 86. Surgical and chemical sympathectomy can relieve pain in some cases. However, under normal physiological circumstances, there is no interaction between the sympathetic and peripheral afferent nociceptive neurons 67, 87, 88, 89, 33. Furthermore, multiple discrepancies undermine the possibility of sympathetic nervous system involvement. These discrepancies include the following: (1) plasma catecholamine concentrations are lower in complex regional pain syndrome-affected limbs 33, 90, (2) most complex regional pain syndrome patients do not obtain significant or lasting pain relief from sympathetic blocks 91, 92 and (3) skin temperature does not correlate with the activity of sympathetic vasoconstrictor neurons 93.
To explain these incongruities, the pathophysiology of sympathetically maintained pain was hypothesized to involve an abnormal coupling between sympathetic efferent and nociceptive afferent neurons 94. Two possible conditions may lead to pathological coupling: interactions between sympathetic efferents and intact or regenerating peripheral nociceptive C-fiber neurons, or between sympathetic vasoconstrictor neurons and afferent somata within the dorsal root ganglion (DRG) 95.
This coupling is mediated by norepinephrine, which is released from newly expressed sympathetic terminals and adrenoreceptors onto afferent nociceptive neurons. Increased mRNA for alpha-2-adrenoreceptors has been demonstrated in dorsal root ganglion neurons following a nerve injury 96. Therefore, an increased number of targeted and functionally upregulated adrenoreceptors on lesioned nociceptive afferents, which has been demonstrated, would explain how reduced sympathetic nervous system activity in complex regional pain syndrome is capable of maintaining pain 89, 67.
Evidence suggests that early autonomic symptoms and signs of complex regional pain syndrome are indicative of central nervous system dysfunction 97. Wasner et al 33 suggest that warmth of the affected extremity in the early stages of complex regional pain syndrome type 1 is caused by the functional inhibition of central cutaneous vasoconstrictor activity, leading to cutaneous vasodilation. However, over time, this inhibition may lead to adrenergic hypersensitivity from peripheral denervation and/or sympathetic denervation.
In complex regional pain syndrome type 1, the early inhibition of central cutaneous vasoconstrictor activity leads to vasodilation in the denervated area causing it to feel warm. The later increased sensitivity to circulating catecholamines due to upregulation of cutaneous adrenoreceptors causes vasoconstriction and coolness. Interestingly, studies of direct nerve injuries in complex regional pain syndrome type 2 show the same results. Initially, vasodilation is present within the denervated area, causing the skin adjacent and on the same side to become abnormally warm at first and then change to a chronically cold status. Other mechanisms include an increased density of cutaneous α-adrenoreceptors and a pathological upregulation of α-adrenergic receptors 95, 96, 97.
Based on recent clinical studies, patients with neuropathic pain presenting with similar clinical signs and symptoms can be clearly divided into 2 groups by the positive and negative effects of selective sympathetic blockade, selective activation of sympathetic activity, and antagonism of α-adrenergic receptor mechanisms 98. Pain relieved by sympatholytic procedures is considered to be sympathetically maintained pain. sympathetically maintained pain is now defined as a symptom or underlying mechanism in a subset of patients with neuropathic disorders. complex regional pain syndrome is one such neuropathic disorder. However, sympathetically maintained pain is not a clinical entity per se. Nor is it a sine qua non for complex regional pain syndrome as was previously believed. Therefore, the positive effect of sympathetic blockade is not essential for the diagnosis of complex regional pain syndrome. On the other hand, the only way to differentiate between sympathetically maintained pain and sympathetically independent pain is to test the efficacy of a correctly applied sympatholytic intervention 99.
In the warm phase of complex regional pain syndrome, local norepinephrine release from sympathetic fibers is decreased leading to increased cutaneous blood flow. However, in the chronic cold phase, α-adrenoreceptors are more sensitive to circulating catecholamines leading to vasoconstriction and decreased blood flow 92, 100. Expression of adrenoreceptors on nociceptive fibers leads to sympatho-afferent coupling producing sympathetically mediated pain. Under conditions of sympathetic activation, there is a considerable increase of pain intensity in patients with complex regional pain syndrome 93, 94, 72.
Psychological Factors
A cross-sectional study comparing psychological factors between patients with complex regional pain syndrome or low back pain showed that in the complex regional pain syndrome group pain intensity correlated with anxiety 101. Moreover, pain and, particularly, depression were the couple of factors that significantly predicted disability 101. Another prospective multicentre study investigated the effect of various psychological factors (agoraphobia, depression, somatization, insufficiency, sensitivity, insomnia, life events) on the risk of complex regional pain syndrome development in 596 patients with a single fracture 102. Although 7% of patients eventually developed complex regional pain syndrome type 1, none of the psychological scores were significantly different from those of the general population, nor could any psychological factor be identified as a predictor of complex regional pain syndrome 102. Similarly, in a systematic review no association between psychological factors and the occurrence of complex regional pain syndrome could be demonstrated, except that patients with more life events were found to carry a higher risk of developing complex regional pain syndrome 103.
Autoimmune factor
There is evidence that complex regional pain syndrome might involve an autoimmune component, as well. Goebel and Blaes suggested that complex regional pain syndrome can be considered an autoantibody-mediated autoimmune syndrome that has a regionally confined course 104. In autoimmune diseases, the innate immune system stimulates an immune response by the adaptive immune system against its own tissues 105. In complex regional pain syndrome, Dirckx et al. 106 showed that significantly more complex regional pain syndrome patients have positive antinuclear antibody test results than healthy blood bank donors. In addition, immunoglobulin (Ig) G autoantibodies against surface antigens on autonomic neurons on the β2-adrenergic, muscarinic-2 receptor and α-1a adrenoreceptors were demonstrated in complex regional pain syndrome patients but not in healthy controls 107, 108, 109.
Another study by Kohr 110 showed that 30–40% of patients who suffered from complex regional pain syndrome had surface-binding autoantibodies against an autonomic nervous system autoantigen. The autoimmune nature of complex regional pain syndrome was further upheld by Goebel and his colleagues 111 who performed a randomized, double-blind, placebo-controlled crossover trial of intravenous immunoglobulin (IVIG) including 13 patients with moderate to severe pain due to complex regional pain syndrome. The average pain intensity significantly reduced following IVIG treatment compared to placebo 111. However, this result was not replicated in a larger study 112.
In theory, by sensitising these neurons, autoantibodies may be able to produce the painful hypersensitivity observed in complex regional pain syndrome patients 113.
Complex regional pain syndrome prevention
These steps might help you reduce the risk of developing complex regional pain syndrome:
- Taking vitamin C after a wrist fracture. Studies have shown that people who took a daily minimum dose of 500 milligrams (mg) of vitamin C after a wrist fracture had a lower risk of complex regional pain syndrome compared with those who didn’t take vitamin C.
- Early mobilization after a stroke. Some research suggests that people who get out of bed and walk around soon after a stroke (early mobilization) lower their risk of complex regional pain syndrome.
Complex regional pain syndrome symptoms
The key symptom of complex regional pain syndrome is prolonged severe pain that may be constant. It has been described as “burning,” “pins and needles” sensation, or as if someone were squeezing the affected limb. The pain may spread to the entire arm or leg, even though the injury might have only involved a finger or toe. In rare cases, pain can sometimes even travel to the opposite extremity. There is often increased sensitivity in the affected area, known as allodynia, in which normal contact with the skin is experienced as very painful.
People with complex regional pain syndrome also experience changes in skin temperature, skin color, or swelling of the affected limb. This is due to abnormal microcirculation caused by damage to the nerves controlling blood flow and temperature. As a result, an affected arm or leg may feel warmer or cooler compared to the opposite limb. The skin on the affected limb may change color, becoming blotchy, blue, purple, pale, or red.
Other common features of Complex regional pain syndrome include:
- changes in skin texture on the affected area; it may appear shiny and thin
- abnormal sweating pattern in the affected area or surrounding areas
- changes in nail and hair growth patterns
- stiffness in affected joints
- problems coordinating muscle movement, with decreased ability to move the affected body part
- abnormal movement in the affected limb, most often fixed abnormal posture (called dystonia), but also tremors in or jerking of the limb.
Complex regional pain syndrome diagnosis
Currently there is no specific test that can confirm complex regional pain syndrome and complex regional pain syndrome remains a clinical diagnosis of exclusion based on the history, symptoms and signs assisted with the application of the Budapest criteria 4, 21, 1. Complex regional pain syndrome diagnosis is based on a person’s medical history, and signs and symptoms that match the definition. Since other conditions can cause similar symptoms, careful examination is important. As most people improve gradually over time, the diagnosis may be more difficult later in the course of the disorder.
Testing also may be used to help rule out other conditions, such as arthritis, Lyme disease, generalized muscle diseases, a clotted vein, or small fiber polyneuropathies, because these require different treatment. The distinguishing feature of complex regional pain syndrome is that of an injury to the affected area. Such individuals should be carefully assessed so that an alternative treatable disorder is not overlooked.
Magnetic resonance imaging (MRI) or triplephase bone scans may be requested to help confirm a diagnosis. While complex regional pain syndrome is often associated with excess bone resorption, a process in which certain cells break down the bone and release calcium into the blood, this finding may be observed in other illnesses as well.
- Bone scan with technetium Tc 99m. This procedure might help find bone changes. A radioactive substance injected into one of your veins allows your bones to be seen with a special camera.
- Sympathetic nervous system tests. These tests look for disturbances in your sympathetic nervous system. For example, thermography measures the skin temperature and blood flow of your affected and unaffected limbs. Other tests can measure the amount of sweat on both limbs. Uneven results can indicate complex regional pain syndrome.
- Infrared thermometry or thermography has the highest specificity of any objective test for complex regional pain syndrome 35. In earlier phases of the disease, the affected limb typically shows higher temperatures compared to the opposite limb 114. This observation has been shown to reverse with disease progression. Sensitivity for complex regional pain syndrome has been reported as low as 45% 115. Thermography requires specialized equipment and accuracy depends on the ability to maintain thermoregulation during measurements 35, 116. The utility of other autonomic function tests including, quantitative sudomotor axon reflex testing and thermoregulatory sweat testing, have similar limitations in that they require specialized equipment, knowledgeable operators, and they have a lower specificity for complex regional pain syndrome 35, 115.
- X-rays. Loss of minerals from your bones may show up on an X-ray in later stages of the disease. However, X-ray has low reported sensitivity and specificity for complex regional pain syndrome 117, 115. X-ray greatest utility is exclusion of other musculoskeletal injuries, particularly in early diagnosis of a unilateral extremity presentation of the disease.
- Magnetic resonance imaging (MRI). Images captured by an MRI test may show a number of tissue changes. Magnetic resonance imaging (MRI) is especially useful in the exclusion of musculoskeletal disorders, particularly osteonecrosis 115. MRI has been shown to be less sensitive for complex regional pain syndrome diagnosis than bone scan in comparative studies 118.
- Doppler flow studies. Doppler flow studies have been suggested to assess vascular reflexes, especially in patients with symptom duration of four months or less 35. Doppler flow study can also be used for exclusion of contributing vascular pathologies, particularly venous thrombosis.
Complex regional pain syndrome treatment
There is some evidence that early (within the first few months of symptom onset) aggressive treatment of complex regional pain syndrome may prevent complex regional pain syndrome symptoms 119. Currently there are not enough high quality studies to guide clear treatment decisions in complex regional pain syndrome 120. Clinical guidelines, which represent the available evidence and the views of clinical experts in complex regional pain syndrome suggest a number of treatments that may be helpful 121. Treatment options include referral for physical and occupational therapy, a short course of oral corticosteroids, bisphosphonates, and transdermal lidocaine patches 122. Evidence suggests that bisphosphonates used for the first six months of symptoms and a short course (two to four weeks) of oral corticosteroids significantly improve pain in patients with complex regional pain syndrome 32. Often, a combination of different treatments, tailored to your specific case, is necessary 123.
The goal of treatment is to improve function and decrease pain. Complex regional pain syndrome is most likely to respond to a comprehensive, integrated, multi-disciplinary treatment approach that involves medical, psychological, and physical and occupational therapy components 32.
Rehabilitation and physical therapy and occupational therapy
An exercise program to keep the painful limb or body part moving can improve blood flow and lessen the circulatory symptoms 124. Additionally, exercise can help improve the affected limb’s flexibility, strength, and function. Rehabilitating the affected limb also can help to prevent or reverse the secondary brain changes that are associated with chronic pain. Occupational therapy can help the individual learn new ways to work and perform daily tasks.
The challenge with implementing physical and occupational therapy is the broad range of interventions available to therapists and the persistent lack of understanding regarding the underlying pathophysiology of complex regional pain syndrome 1. Regardless, a number of case reports have been published showing efficacy in a wide range of interventions, ranging from strain-counterstrain (SCS), neural mobilization techniques, and thrust manipulation 125, 126, 127. These techniques often rely on some form of neuromodulation, either through decrease in proprioceptive hyperactivity as seen in strain-counterstrain (SCS) or activation of descending pain pathways and inhibitory mechanisms in spinal manual therapy. Additionally, there is evidence of analgesic effects achieved through the release of neurotensin and oxytocin, providing patients with short-term analgesia that may subsequently enhance their ability to participate in other therapeutic modalities they may previously not have tolerated 128, 129. Additionally, there is likely a role involving catecholamines in the pathophysiological pathway of complex regional pain syndrome.
Psychotherapy
Complex regional pain syndrome and other painful and disabling conditions often are associated with profound psychological symptoms for affected individuals and their families. People with complex regional pain syndrome may develop depression, anxiety, or post-traumatic stress disorder, all of which heighten the perception of pain and make rehabilitation efforts more difficult. Treating these secondary conditions is important for helping people cope and recover from complex regional pain syndrome. Furthermore, complex regional pain syndrome patient population carries significant risk factors for suicidal ideation, including: severe pain, depressive symptoms and functional impairment. The link between chronic pain and suicidal ideation has been well established, and given the additional autonomic dysfunction associated with complex regional pain syndrome, these patients carry a significant risk for suicidality 130, 131, 132, 133.
Although the evidence is lacking in clinical trial evidence, case series have shown promise in the benefits of various forms of psychotherapy intervention, especially when combined with other non-invasive modalities 1. Additionally, adaptation of the treatment regimen to the evolution of a patient’s symptoms is critical 134. Of particular interest is the study conducted by Fialka et al. 135 who found a decrease in limb temperature in the psychotherapy arm compared to the physical therapy only group. Although the study was limited by its lack of power, it lends further support to the role psychological stress can play in the progression of complex regional pain syndrome 136, 135.
Medications
Several different classes of medication have been reported to be effective in treating complex regional pain syndrome, particularly when used early in the course of the disease. However, no drug is approved by the U.S. Food and Drug Administration specifically for complex regional pain syndrome, and no single drug or combination of drugs is guaranteed to be effective in every person.
Drugs to treat complex regional pain syndrome include:
- bisphosphonates, such as high dose alendronate or intravenous pamidronate
- non-steroidal anti-inflammatory drugs (NSAIDs) to treat moderate pain, including over-the-counter aspirin, ibuprofen, and naproxin
- corticosteroids that treat inflammation/swelling and edema, such as prednisolone and methylprednisolone (used mostly in the early stages of complex regional pain syndrome)
- drugs initially developed to treat seizures or depression but now shown to be effective for neuropathic pain, such as gabapentin, pregabalin, amitriptyline, nortriptyline, and duloxetine
- botulinum toxin injections
- opioids such as oxycontin, morphine, hydrocodone, fentanyl, and Vicodin. These drugs must be prescribed and monitored under close supervision of a physician, as these drugs may be addictive.
- N-methyl-D-aspartate (NMDA) receptor antagonists such as dextromethorphan and ketamine, and
- topical local anesthetic creams and patches containing numbing agents such as lidocaine.
All drugs or combination of drugs can have various side effects such as drowsiness, dizziness, increased heartbeat, and impaired memory. Inform a healthcare professional of any changes once drug therapy begins.
Non-steroidal anti-inflammatory drugs (NSAIDs)
Non-steroidal anti-inflammatory drugs (NSAIDs) are cyclooxygenase-2 (COX-2) inhibitors, preventing the synthesis of prostaglandins. Prostaglandins are inflammatory mediators and induce hyperalgesia; therefore, downregulating these molecules may disrupt the process of spinal transmission of nociceptive signals and reduce the acute-pain stage of complex regional pain syndrome 137. However, the evidence remains poor regarding the efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) although there are case reports showing potential benefits 138, 139.
Steroids
Steroids are used to target the inflammatory component of the proposed complex regional pain syndrome pathophysiology mechanism. There have been several studies assessing the efficacy of steroids, at various doses, various time-intervals and in patients with varying degrees of complex regional pain syndrome duration (acute vs chronic) 140, 141, 142. Given the noteworthy and potentially significant side effects associated with prolonged steroid use, care needs to be exercised by the clinician when considering these medications. One trial in particular was notable for the significant benefits of a tapered prednisone regimen in patients with an average duration of 1.9 months since onset of complex regional pain syndrome in reducing Visual Analogue Scale (VAS) pain scores 143.
Gabapentin
Gabapentin, originally used as a muscle relaxer and anti-spasmodic medication, has been found to be an effective adjunct anticonvulsant with neural pain control potential 144. Van de Vusse et al. 145 performed a randomized double blind placebo controlled crossover study and found that while gabapentin only had a mild effect on pain in complex regional pain syndrome 1, it had a significant impact on reducing the sensory deficit in the affected limb. These results were similar in the pediatric population, as Brown et al. 146 found that gabapentin significantly reduced pain intensity scores while improving sleep. This study found that both the antidepressant amitriptyline and the anticonvulsant gabapentin were analogous in their effectiveness in reducing pain in complex regional pain syndrome 1. A limitation of these trials was the low number of participants in the trials. While commonly utilized in the treatment of complex regional pain syndrome, there are ultimately few randomized control trials with solid evidence to prove the efficacy of gabapentin, suggesting that there needs to be further research into gabapentin with respect to complex regional pain syndrome 124.
Bisphosphonates
Bisphosphonates inhibit osteoclastic bone resorption by to hydroxyapatite sites, especially at sites undergoing active bone resorption. The exact mechanism for how bisphosphonates provide pain relieve in complex regional pain syndrome remains unclear, although there are a number of potential mechanisms that have been proposed and the true mechanism is likely multifactorial in nature given the limited degree of bone turnover noted in complex regional pain syndrome 147. Regardless, there appears to be a degree of evidence indicating the benefit of bisphosphonates in reducing pain scores in comparison to placebo; however, many of the early trials were often lacking in power. In addition, a lack of true understanding behind the mechanism of action for therapeutic benefit with bisphosphonates limits the ability to identify ideal drug and dosing regimens 148, 124. However, a randomized, double-blind, placebo-controlled study comparing four doses of intravenous (IV) neridronate to placebo found statistically significant decreases in Visual Analogue Scale (VAS) pain scores in the study of 82 patients. The authors posit that these results may be linked to bisphosphonate reduction of the increased bone turnover and subsequent marrow edema seen in complex regional pain syndrome that may contribute to chronic pain. Additionally, locally accumulated drug may interfere with the inflammatory pathways and subsequent pain generation by decreasing lactate concentration and acidosis. Interestingly, some patients also experienced permanent remission of their disease; however, it should be noted that these patients were identified early in their clinical course, an important caveat to the efficacy of bisphosphonates in treating complex regional pain syndrome. Regardless, the significant efficacy and limited adverse effects of the medications suggest an importance in incorporation of bisphosphonates as standard of care when initiating treatment for complex regional pain syndrome patients 147.
Ketamine
Ketamine is a strong anesthetic with an N-methyl-D-aspartate (NMDA) receptor antagonist has a notable role in the modulation of the wind-up response to noxious stimuli that results in central sensitization classically seen in chronic pain conditions. There is also evidence of a role in immunomodulation resulting in the down-regulation of neuroinflammatory markers; therefore, it remains unclear if the potential role of ketamine in complex regional pain syndrome treatment is relegated solely to the effects of NMDA antagonism resulting in down-regulation of central sensitization or if there are additional factors involved 149, 150. Investigators are using low doses of ketamine given intravenously for several days to either reduce substantially or eliminate the chronic pain of complex regional pain syndrome. In certain clinical settings, ketamine has been shown to be useful in treating pain that does not respond well to other treatments. Regardless, the current body of evidence is lacking in supporting the efficacy of ketamine in the treatment of complex regional pain syndrome with the majority of studies lacking in power or utilizing different modes of administration, making it difficult to determine the level of evidence supporting ketamine 151, 85, 149.
Botulinum Toxin A
The use of Botulinum Toxins A and B have been an emerging add-on (adjunct) to local anesthetics for sympathectomies and treatment of dystonia or spasticity in the treatment of complex regional pain syndrome, with most studies published starting in 2008. The mechanism of this therapy was hypothesized to be slightly different depending on the use for treating dystonia and spasticity or for a sympathectomy. In dystonia, the role of botulinum toxin in therapy is due to its function in disrupting the SNARE complex and inhibition of exocytosis. It prevents the release of acetylcholine and causes flaccid paralysis, effectively relieving the pain from muscle dystonia and spastic contractility 152, 153. A retrospective case review of the use of Botulinum Toxin A (Botox) in patients with neck or upper limb girdle muscles with dystonia and spasm showed that there was significant pain relief in 97% of the patients over the first 4 weeks after treatment. Given the efficacy of botulinum toxin in inhibition of cholinergic circuitry, several studies have expanded its use to blocking cholinergic signaling at the sympathetic ganglia in complex regional pain syndrome patients. The majority of studies have been small case-control or retrospective studies regarding the efficacy of Botulinum Toxin A (Botox) and Botulinum Toxin B (BTX-B), either by themselves or in conjunction with local anesthetic. While these studies range from retrospective studies to prospective randomized controlled trials, they all show moderate improvements in pain scores over the short term with either botulinum toxin alone or with local anesthetic. They also reliably show that the use of botulinum toxin has a greater duration of efficacy than the use of local anesthetic alone 154. A meta-analysis performed in 2020 which evaluated randomized controlled trials provided good evidence for the efficacy of Botulinum Toxin A (Botox) for pain relief across neuropathic and muscle based pain syndromes 155. There are numerous other studies that suggest the use of Botulinum Toxin A (Botox) and Botulinum Toxin B (BTX-B) depending on the location of the sympathectomy, but there is not yet strong evidence for the use of one or the other purely based on the site of complex regional pain syndrome being treated 156, 157. There is currently a study underway with very similar parameters looking at the impact to quality of life and disability scores in complex regional pain syndrome patients 158. While Botulinum Toxin A (Botox) has significant therapeutic potential, there are concerns about possible extravasation into surrounding ganglia which could lead to neurologic complications as well as discrepancies between industry and non-industry-sponsored studies 159.
Antioxidants
In the search for improved pharmacological treatments for complex regional pain syndrome, the use of antioxidants has been increasingly studied over the past ten years, spanning the fields of rheumatology, anesthesiology and orthopedics. This is primarily regarding complex regional pain syndrome Type 1, with an established injury or trauma, in many cases from surgery. Eisenberg et al. 160 in 2008 demonstrated that when comparing complex regional pain syndrome 1 and control patients, the patients with complex regional pain syndrome had significantly elevated salivary peroxidase, superoxide dismutase activity, uric acid and total antioxidant status compared to controls. In 2014 Baykal et al. 161 had similar findings, showing that superoxide dismutase, glutathione peroxidase and glutathione s-transferase activity were all significantly elevated in patients who developed complex regional pain syndrome Type 1 when compared to patients who did not. Several studies have been done regarding the prophylactic treatment of surgical patients with Vitamin C post-operatively. These have found that prophylaxis with 500 mg to 1 g of Vitamin C daily post operatively from total knee arthroplasty, foot and ankle surgery, and subacromial shoulder surgery had a statistically significant effect on the development of complex regional pain syndrome 1 162, 163, 164. Patients who received Vitamin C were less likely to develop complex regional pain syndrome, considered to be through the role of Vitamin C in stabilizing reactive oxygen species and in turn reducing inflammation. A meta-analysis of randomized controlled trials using vitamin C for complex regional pain syndrome prophylaxis found a similar reduction in the risk of complex regional pain syndrome development 165. In all, it is safe to say that Vitamin C perioperatively could be a valuable tool in the prevention of complex regional pain syndrome Type 1, especially in the elective surgical setting, ultimately reducing the incidence of this often-debilitating disease.
Sympathetic nerve block
Some individuals report temporary pain relief from sympathetic nerve blocks, but there is no published evidence of long-term benefit. Sympathetic blocks involve injecting an anesthetic next to the spine to directly block the activity of sympathetic nerves and improve blood flow.
It is thought that one of the underlying pathophysiologic mechanisms of complex regional pain syndrome is sympathetic hyperactivity. The most common sympathetic blocks for complex regional pain syndrome are the stellate ganglion sympathetic blocks used to treat upper extremity symptoms while lumbar sympathetic nerve blocks are used to treat lower extremity symptoms 21. Although the quality of the evidence was low, a 2013 Cochrane review found that sympathetic blocks combined with local anesthetic were ineffective at reducing complex regional pain syndrome-related pain 166. A more recent Cochrane review in 2016 was unable to make any firm judgments regarding the effectiveness of this type of treatment for complex regional pain syndrome 166. In 2019 a study looked at the relationship between sympathetic blocks and spinal cord stimulation and found that the effects of a sympathetic block did not predict the success of a spinal cord stimulator 167.
Surgical sympathectomy
A surgical sympathectomy is a procedure that cuts or clamps the sympathetic nerve chain to treat conditions such as excessive sweating, facial blushing, some chronic pain conditions, and Raynaud phenomenon. A surgeon cuts or clamps the sympathetic nerve chain, which runs along the spine in the chest and controls the body’s fight-or-flight response. Sympathectomy is a last resort when other treatments, such as medicines or antiperspirants, have not worked. The use of this operation that destroys some of the nerves is controversial. Some experts think it is unwarranted and makes complex regional pain syndrome worse, whereas others report a favorable outcome. Sympathectomy should be used only in individuals whose pain is dramatically relieved (although temporarily) by sympathetic nerve blocks.
Spinal cord stimulation
Placing stimulating electrodes through a needle into the epidural space to deliver electric stimulation to the spinal cord’s dorsal column provides a tingling sensation in the painful area. Electrodes may be placed temporarily for a few days in order to assess whether spinal cord stimulation (SCS) is likely to be helpful. Minor surgery is required to implant all the parts of the stimulator, battery, and electrodes under the skin on the torso. Some spinal cord stimulation (SCS) devices use an external pulse generator, but typically the electrodes are connected to an implanted pulse generator. Several mechanisms of action for spinal cord stimulation (SCS) have been proposed, including vasodilation, reversal of cortical maladaptive neuroplastic changes, adrenergic inhibition, and inhibition of nociceptive neural conduction in the spinal cord. A comprehensive outcome specific review of the use of spinal cord stimulation specifically for complex regional pain syndrome was published in 2017 168. High-level evidence continues to support spinal cord stimulation (SCS) beneficial and successful role in the treatment of complex regional pain syndrome patients’ perceived pain relief, pain score, and quality of life 168. Functional improvements were noted with less evidence for complex regional pain syndrome resolution, sleep hygiene improvement, positive psychological impact, and analgesic sparing effects 168. A 2021 study looking at the long-term outcome of spinal cord stimulation (SCS) in complex regional pain syndrome did not find statistical functional improvement or a reduction in opioid or neuropathic pain medication use 169. However, they did note that 70% of the patients continued to use their spinal cord stimulation (SCS) devices at the eight-year follow-up 169. Approximately 25 percent of individuals develop equipment problems that may require additional surgeries.
Dorsal root ganglion stimulation
The dorsal root ganglion serves as an ideal target given its role in processing and transmitting sensory information from the periphery to the central nervous system. In animal models of chronic pain, pathophysiologic changes in the dorsal root ganglion have been noted, including altered expression of various genes that may play a role in the hyperexcitability of neurons involved in the nociceptive pathway. An innovative neuromodulation technique for the treatment of chronic pain targets the dorsal root ganglion (DRG) rather than the spinal cord. The exact mechanism of how dorsal root ganglion stimulation exerts its beneficial effects remains unknown, although it may be related to the modulation of a variety of cells housed within the The dorsal root ganglion serves as an ideal target given its role in processing and transmitting sensory information from the periphery to the central nervous system. In animal models of chronic pain, pathophysiologic changes in the dorsal root ganglion have been noted, including altered expression of various genes that may play a role in the hyperexcitability of neurons involved in the nociceptive pathway 170, 171, 172, 173.
As opposed to conventional spinal cord stimulation (SCS), dorsal root ganglion stimulation enables a more targeted application of neurostimulation due to the dorsal root ganglion’s more peripheral location and ease of access. For the treatment of lower extremity pain in complex regional pain syndrome, dorsal root ganglion stimulation received approval from the US Food and Drug Administration (FDA) in 2016. According to a recent pooled analysis study, dorsal root ganglion stimulation was safe and effective for complex regional pain syndrome, resulting in a 4.9-point mean decrease in complex regional pain syndrome type 1 pain intensity 174. In 2017 the ACCURATE study compared spinal cord stimulation (SCS) and dorsal root ganglion stimulation in 152 patients with complex regional pain syndrome 172. Dorsal root ganglion stimulation was found to be more efficient than conventional spinal cord stimulation (SCS) in this multicenter randomized trial for reducing pain and enhancing quality of life in complex regional pain syndrome patients 172.
Other types of neural stimulation
Neurostimulation can be delivered at other locations along the pain pathway, not only at the spinal cord. These include near injured nerves (peripheral nerve stimulators), outside the membranes of the brain (motor cortex stimulation with dural electrodes), and within the parts of the brain that control pain (deep brain stimulation). A recent option involves the use of magnetic currents applied externally to the brain (known as repetitive Transcranial Magnetic Stimulation, or rTMS). A similar method that uses transcranial direct electrical stimulation is also being investigated. These stimulation methods have the advantage of being non-invasive, with the disadvantage that repeated treatment sessions are needed.
Epidural infusion
Epidural infusion is an alternative therapy to provide pain control, by allowing one to vary local anesthetic concentration and infusion dose to be titrated to the desired effect 4. Adjuvant (add-on) medications, such as clonidine with the addition of opioids, can be added to provide additional spinal analgesia and to potentiate the degree of relief 4. The most commonly used combination of epidural medications today includes clonidine with bupivacaine 4. Opioids can be added to the mixture if the pain relief is inadequate or if the local anesthetic concentration required to produce pain relief also prohibits ambulation or full participation in the physiotherapy program 4.
The primary benefit of continuous regional analgesia is that one is able to effectively titrate to the necessary degree of relief and promote active physical therapy as tolerated 4. Furthermore, with patient-activated bolus programming, these continuous regional techniques allow patients to self-administer small boluses for optimal analgesia as the pain levels fluctuate 4. Either before or after a strenuous exercise program, patients may experience elevations in pain, swelling, or allodynia. The ability for patients to readily self-administer extra doses of medication within certain pre-programmed parameters will improve patient satisfaction and optimize pain control 4. Rauck et al. 175 performed a randomized, blinded, placebo-controlled trial utilizing epidural clonidine. They randomized 26 patients with complex regional pain syndrome to receive daily epidural infusions (for 3 consecutive days) of clonidine 300 or 600 mcg, or placebo 175 If patients responded to the clonidine with analgesia and did not respond to placebo, they were placed on an open label infusion for a mean of 32 days at a mean dose of 32 mcg/hour 175. All patients had substantial relief with both the 300 and 700 microgram doses. Of the 26 patients, 19 elected to receive continuous infusions of clonidine for an average of 43 days with an average dose 32 ± 6 micrograms per hour 175. Seventeen of nineteen patients had statistically significant improvement in pain. Side effects were dizziness, dry mouth, mouth sores, and nausea. Six of 19 patients developed catheter related infection, and one developed meningitis 175.
Cooper et al. 176 studied 14 patients in a prospective open label trial and demonstrated improved pain relief and range of motion in patients receiving an epidural bupivacaine-opioid mixture for an average of 4 days. Thirteen of fourteen patients had significant improvement, with 11 of the 14 achieving “resolution of their complex regional pain syndrome” by the end of the trial with no activity restrictions 176. Konig et al. 177 studied 26 patients by using continuous cervical epidural analgesia of bupivacaine (0.25%) for seven days coupled with physical therapy. Eighty-three percent of patients had “improvement in pain”. Edema, sweating abnormalities, and dysfunction of the hand responded particularly well. Sixty-three percent of patients considered their condition to be acceptable whereas only 8% were completely pain free. Reduction in pain medications usage was also noted. Finally, Bucheit and Crews 178 described a single case report where continuous epidural infusion markedly improved range of motion.
The reported rates of infection in epidural catheters used to treat complex regional pain syndrome are as high as 31% 175. Therefore, epidural catheters meant for longer-term use should be performed as minor surgical procedures that require standard surgical sterility techniques. Catheters should be tunneled under the skin and away from the midline entrance point to the spine to minimize the colonization by bacteria that is inherently a greater risk with extended duration infusions. Standard catheter dressings, such as those required for extended central venous catheters, should be followed and dressings should be changed weekly. The hallmarks of an epidural abscess include the triad of back pain, sensorimotor loss, and loss of bowel and bladder function. Epidural abscesses may have earlier prodromal symptoms such as fever, neck pain, or photophobia 179. Careful attention to early symptoms is paramount for early diagnosis. A previous study has demonstrated a catheter related infection rate of 19 out of 350 patients. All of these patients were treated with antibiotics and catheter removal, and none required surgical intervention 179.
Intrathecal drug pumps
An intrathecal drug pump, also known as a pain pump, is a surgically implanted device that delivers painrelieving medications directly into the spinal fluid to treat chronic pain and spasticity. These medication may include opioids, local anesthetic agents, clonidine, and baclofen. The pump is about the size of a hockey puck and is implanted under the skin in the abdomen, flank, or axilla. A catheter is then inserted into the spinal cord and connected to the pump. Intrathecal pumps are often used to treat chronic pain caused by conditions such as cancer, neuropathic pain, failed back surgery, cerebral palsy, multiple sclerosis, stroke, brain injury, and spinal cord injury. Intrathecal pumps can provide more effective pain relief with fewer side effects than oral medication.
Intrathecal analgesia has been studied to a lesser extent when compared to epidural analgesia. Lundborg 180 reported a series of three patients with refractory complex regional pain syndrome, who did not have a favorable clinical response to intrathecal bupivacaine. In spite of initial analgesia, all patients demonstrated a progression of their complex regional pain syndrome 180. In a small subset of patients (n = 7) with refractory complex regional pain syndrome and severe dystonia, van Hilten et al. 181 demonstrated analgesia and functional restoration after a bolus of intrathecal baclofen injected in a double-blind fashion followed by intrathecal infusion. But van Hilten et al 181 stopped using intrathecal baclofen infusions due to what they deemed as unacceptable side effects. Intrathecal infusion for complex regional pain syndrome without dystonia has only limited supporting literature 181.
The major risk associated with these infusion techniques is the rate of infection, which remains to be defined by further prospective study on infusion techniques in complex regional pain syndrome patients.
Topical Treatments
Topical treatments must be distinguished from transdermal formulations such as the fentanyl or clonidine patches that deliver systemic medication through the skin. Topical medications remain local, reaching dermal nerve endings, blood vessels, and other cells in the skin. Topical medications are appealing by virtue of their relative lack of systemic effects; rashes and allergies are their only major adverse effect. Topical options to consider for complex regional pain syndrome include the 5% lidocaine impregnated patch, the capsaicin and dimethylsulfoxide (DMSO 4.
Some clinicians endorse the use Eutectic Mixture of Local Anesthetics (EMLA) for patients with complex regional pain syndrome 182, but it must be applied under an occlusive cover (e.g., plastic food wrap) to maximize penetration. The 5% lidocaine patch is FDA-approved for treating postherpetic neuralgia (PHN), and is available in generic formulation 183. It may have efficacy in some local or focal complex regional pain syndrome phenomena such as allodynia 184.
Capsaicin, the vanilloid compound in chili peppers, is a highly selective agonist for the Transient Receptor Potential channel, Vanilloid-receptor type 1 (TRPV1) that is expressed on central and peripheral terminals of nociceptive primary sensory neurons 185. Topical capsaicin causes activation followed by dying-back of nociceptive nerve endings by allowing unchecked cation influx 185. Capsaicin use is limited by the painful burning sensation it evokes at the site of application until the site becomes denervated. In a randomized controlled trial, topical capsaicin showed modest efficacy for post herpetic neuralgia 186. A preliminary study of high-dose topical capsaicin plus regional anesthesia for complex regional pain syndrome demonstrated partial efficacy 187. Some doctors have found topical capsaicin to be intolerably painful, somewhat messy, and unacceptable to most patients 188, 189, 190, 191, 192. In 2009, the FDA approved a high concentration 8% capsaicin patch for treating post herpetic neuralgia once every 3 months 193. Capsaicin is applied to the painful area for 1 hour after topical local anesthesia. Two additional well-powered randomized controlled trials were positive for high-versus low-dose capsaicin in peripheral neuropathic pain, including in HIV-associated distal sensory polyneuropathy 194, 195. However, in complex regional pain syndrome, exacerbated pain may render this treatment unsuitable 196.
Dimethyl sulfoxide (DMSO) is a free radical-scavenging agent. In a systematic review DMSO (50% cream for 2 months) provided significant complex regional pain syndrome symptom reduction when compared with placebo 197, however pain intensity was not improved 198.
Emerging treatments
Emerging treatments for complex regional pain syndrome include:
- Intravenous immunoglobulin (IVIG)
Researchers in United Kingdom report low-dose IVIG reduced pain intensity in a small trial of 13 patients with complex regional pain syndrome for 6 to 30 months who did not respond well to other treatments. Those who received intravenous immunoglobulin (IVIG) had a greater decrease in pain scores than those receiving saline during the following 14 days after infusion.
A randomized controlled trial of low-dose (0.5 g/kg) intravenous immunoglobulin (IVIG) treatment for persistent complex regional pain syndrome indicated efficacy 111. However, a subsequent larger trial was negative 112. Although there is some anecdotal evidence for the efficacy of high-dose IVIG this has not been formally tested.
- Plasma exchange therapy
Plasma exchange has been reported effective in several case series 199 and consequently complex regional pain syndrome has been added to the list of possible indications by the international plasma exchange society (ASFA) 200. Plasma exchange treatment, although providing pain improvement in some cases, requires use of long repeat-exchange cycles (e.g., eight exchange treatments over 4 weeks) and is unfortunately complicated regularly by pain increase at the venous access site.
- Graded Motor imagery
Several studies have demonstrated the benefits of graded motor imagery therapy for complex regional pain syndrome pain. Individuals do mental exercises including identifying left and right painful body parts while looking into a mirror and visualizing moving those painful body parts without actually moving them.
Several alternative therapies have been used to treat other painful conditions. Options include behavior modification, acupuncture, relaxation techniques (such as biofeedback, progressive muscle relaxation, and guided motion therapy), and chiropractic treatment.
Amputation
The role of amputation in chronic complex regional pain syndrome type 1 is a potentially viable one, specifically for those patients who suffer from intractable and refractory symptoms despite numerous multi-modal therapeutic interventions 1. Although not without their own risks as well as the potential for recurrence of complex regional pain syndrome in the remaining limb or other limbs, several studies have noted patient satisfaction with the benefits of amputation 1. These retrospective reviews are relatively limited in power; however, they suggest a potential role of amputation for those patients who have exhausted alternative options 201, 202, 203. There may be additional benefit in selecting potential amputation candidates for their resilience, as a study conducted by Bodde et al. 132 found that patients with higher resilience scores correlated with higher quality of life and lower psychological distress status post limb amputation. Regardless of the potential benefits, the decision to pursue amputation should be taken in the context of the patient overall, recognizing and acknowledging the associated complications of amputation as well as the risk for minimal relief to recurrence of complex regional pain syndrome 1.
Coping and support
Living with a chronic, painful condition can be challenging, especially when — as is often the case with complex regional pain syndrome — your friends and family don’t believe you could be feeling as much pain as you describe. Share information from reliable sources about complex regional pain syndrome with those close to you to help them understand what you’re experiencing.
Follow these suggestions to take care of your physical and mental health:
- Maintain normal daily activities as best you can.
- Pace yourself and be sure to get the rest that you need.
- Stay connected with friends and family.
- Continue to pursue hobbies that you enjoy and are able to do.
If complex regional pain syndrome makes it difficult for you to do things you enjoy, ask your doctor about ways to get around the obstacles.
Keep in mind that your physical health can directly affect your mental health. Denial, anger and frustration are common with chronic illnesses.
At times, you may need more tools to deal with your emotions. A therapist, behavioral psychologist or other professional may be able to help you put things in perspective. He or she may also be able to teach you coping skills, such as relaxation or meditation techniques.
Sometimes joining a support group, where you can share experiences and feelings with other people, is a good approach. Ask your doctor what support groups are available in your community.
- Abd-Elsayed A, Stark CW, Topoluk N, Isaamullah M, Uzodinma P, Viswanath O, Gyorfi MJ, Fattouh O, Schlidt KC, Dyara O. A brief review of complex regional pain syndrome and current management. Ann Med. 2024 Dec;56(1):2334398. doi: 10.1080/07853890.2024.2334398[↩][↩][↩][↩][↩][↩][↩]
- Mangnus TJP, Bharwani KD, Dirckx M, Huygen FJPM. From a Symptom-Based to a Mechanism-Based Pharmacotherapeutic Treatment in Complex Regional Pain Syndrome. Drugs. 2022 Apr;82(5):511-531. doi: 10.1007/s40265-022-01685-4[↩]
- MG30.04 Complex regional pain syndrome. https://icd.who.int/browse/2024-01/mms/en#1834504950[↩]
- Harden RN, McCabe CS, Goebel A, Massey M, Suvar T, Grieve S, Bruehl S. Complex Regional Pain Syndrome: Practical Diagnostic and Treatment Guidelines, 5th Edition. Pain Med. 2022 Jun 10;23(Suppl 1):S1-S53. doi: 10.1093/pm/pnac046[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Veldman PH, Reynen HM, Arntz IE, Goris RJ. Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet. 1993;342(8878):1012–1016. doi: 10.1016/0140-6736(93)92877-v[↩]
- Finnerup NB, Haroutounian S, Kamerman P, Baron R, Bennett DLH, Bouhassira D, Cruccu G, Freeman R, Hansson P, Nurmikko T, Raja SN, Rice ASC, Serra J, Smith BH, Treede RD, Jensen TS. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016 Aug;157(8):1599-1606. doi: 10.1097/j.pain.0000000000000492[↩]
- Marinus J, Moseley GL, Birklein F, Baron R, Maihöfner C, Kingery WS, et al. Clinical features and pathophysiology of complex regional pain syndrome. Lancet Neurology 2011;10(7):637-48. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5511749/[↩]
- Stanton-Hicks M, Baron R, Boas R, Gordh T, Harden N, Hendler N, Koltzenburg M, Raj P, Wilder R. Complex Regional Pain Syndromes: guidelines for therapy. Clin J Pain. 1998 Jun;14(2):155-66. doi: 10.1097/00002508-199806000-00012[↩]
- Perez RS, Zollinger PE, Dijkstra PU, Thomassen-Hilgersom IL, Zuurmond WW, Rosenbrand KC, Geertzen JH; CRPS I task force. Evidence based guidelines for complex regional pain syndrome type 1. BMC Neurol. 2010 Mar 31;10:20. doi: 10.1186/1471-2377-10-20[↩]
- Merskey H, Bogduk N. Classification of Chronic Pain. 2nd (Revised) ed. IASP Task Force on Taxonomy, IASP Press, 2011; 4–7[↩]
- Taylor SS, Noor N, Urits I, Paladini A, Sadhu MS, Gibb C, Carlson T, Myrcik D, Varrassi G, Viswanath O. Complex Regional Pain Syndrome: A Comprehensive Review. Pain Ther. 2021 Dec;10(2):875-892. doi: 10.1007/s40122-021-00279-4. Epub 2021 Jun 24. Erratum in: Pain Ther. 2021 Dec;10(2):893-894. doi: 10.1007/s40122-021-00291-8[↩]
- Bruehl S. Complex regional pain syndrome. BMJ. 2015 Jul 29;351:h2730. https://www.bmj.com/content/351/bmj.h2730.long[↩]
- Giannotti S, Bottai V, Dell’Osso G, Bugelli G, Celli F, Cazzella N, Guido G. Algodystrophy: complex regional pain syndrome and incomplete forms. Clin Cases Miner Bone Metab. 2016 Jan-Apr;13(1):11-4. doi: 10.11138/ccmbm/2016.13.1.011[↩]
- Russo M, Georgius P, Santarelli DM. A new hypothesis for the pathophysiology of complex regional pain syndrome. Med Hypotheses. 2018 Oct;119:41-53. doi: 10.1016/j.mehy.2018.07.026[↩]
- Lloyd ECO, Dempsey B, Romero L. Complex Regional Pain Syndrome. Am Fam Physician. 2021 Jul 1;104(1):49-55. https://www.aafp.org/pubs/afp/issues/2021/0700/p49.html[↩]
- Kessler A, Yoo M, Calisoff R. Complex regional pain syndrome: An updated comprehensive review. NeuroRehabilitation. 2020;47(3):253-264. doi: 10.3233/NRE-208001[↩]
- de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, Stricker BH, Sturkenboom MC. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007 May;129(1-2):12-20. doi: 10.1016/j.pain.2006.09.008[↩][↩][↩][↩][↩]
- Lewis JS, Kashif M, Maan A, Ciampi de Andrade D, Casey M, Moon JY, Lin CP, Danielsson L, Quek T, Díez Tafur R, Aloweidi A, Birklein F, Knudsen L, Goebel A. Global series: Complex regional pain syndrome: abstracts from the International Association for the Study of Pain complex regional pain syndrome SIG virtual symposia 2021. Pain Rep. 2023 Jan 16;8(1):e1056. doi: 10.1097/PR9.0000000000001056[↩][↩]
- Bruehl S, Chung OY. How common is complex regional pain syndrome-Type I? Pain. 2007 May;129(1-2):1-2. doi: 10.1016/j.pain.2007.02.017[↩]
- Beerthuizen A, Stronks DL, Van’t Spijker A, Yaksh A, Hanraets BM, Klein J, Huygen FJPM. Demographic and medical parameters in the development of complex regional pain syndrome type 1 (CRPS1): prospective study on 596 patients with a fracture. Pain. 2012 Jun;153(6):1187-1192. doi: 10.1016/j.pain.2012.01.026[↩]
- Misidou C, Papagoras C. Complex Regional Pain Syndrome: An update. Mediterr J Rheumatol. 2019 Mar 28;30(1):16-25. doi: 10.31138/mjr.30.1.16[↩][↩][↩][↩][↩][↩]
- Goebel A, Birklein F, Brunner F, et al. The valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain. 2021;162:2346–2348. doi: 10.1097/j.pain.0000000000002245[↩]
- Bruehl S. Complex regional pain syndrome. BMJ. 2015;351 doi: 10.1136/bmj.h2730. h2730[↩]
- Goebel A, Barker C, Birklein F, et al. Standards for the diagnosis and management of complex regional pain syndrome: results of a European Pain Federation task force. Eur J Pain. 2019;23:641–651. doi: 10.1002/ejp.1362[↩]
- Harden RN, McCabe CS, Goebel A, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 5th edition. Pain Med. 2022;23:1–53. doi: 10.1093/pm/pnac046[↩]
- Complex regional pain syndrome in adults (2nd edition). UK guidelines for diagnosis, referral and management in primary and secondary care 2018. https://www.rcp.ac.uk/media/4uijppdz/complex-regional-pain-syndrome-in-adults-second-edition_0.pdf[↩]
- Stanton-Hicks MD, Burton AW, Bruehl SP, Carr DB, Harden RN, Hassenbusch SJ, et al. An updated interdisciplinary clinical pathway for CRPS: report of an expert panel. Pain Practice 2002;2(1):1-16. https://www.ncbi.nlm.nih.gov/pubmed/17134466[↩]
- Bruehl S. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology 2010;113(3):713-25. https://www.ncbi.nlm.nih.gov/pubmed/20693883[↩]
- Lewis JS, Kersten P, Mccabe CS, McPherson KM, Blake DR. Body perception disturbance: a contribution to pain in complex regional pain syndrome (CRPS). Pain 2007;133(1-3):111-9. https://www.ncbi.nlm.nih.gov/pubmed/17509761[↩]
- Ott S, Maihöfner C. Signs and Symptoms in 1,043 Patients with Complex Regional Pain Syndrome. J Pain. 2018 Jun;19(6):599-611. doi: 10.1016/j.jpain.2018.01.004[↩][↩][↩]
- Fukushima FB, Bezerra DM, Villas Boas PJ, Valle AP, Vidal EI. Complex regional pain syndrome. BMJ. 2014 Jun 25;348:g3683. doi: 10.1136/bmj.g3683[↩]
- Harden RN, Oaklander AL, Burton AW, Perez RS, Richardson K, Swan M, Barthel J, Costa B, Graciosa JR, Bruehl S; Reflex Sympathetic Dystrophy Syndrome Association. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Med. 2013 Feb;14(2):180-229. doi: 10.1111/pme.12033[↩][↩][↩][↩]
- Wasner G, Schattschneider J, Heckmann K, Maier C, Baron R. Vascular abnormalities in reflex sympathetic dystrophy (CRPS I): mechanisms and diagnostic value. Brain. 2001 Mar;124(Pt 3):587-99. doi: 10.1093/brain/124.3.587[↩][↩][↩][↩]
- Harden RN, Bruehl S, Stanton-Hicks M, Wilson PR. Proposed new diagnostic criteria for complex regional pain syndrome. Pain Med. 2007 May-Jun;8(4):326-31. doi: 10.1111/j.1526-4637.2006.00169.x[↩][↩]
- Williams K, Guarino A, Raja SN.. Chapter 27 – Complex regional pain syndrome. In: Benzon HT, Raja SN, Liu SS, et al., eds. Essentials of pain medicine. 4th ed. Philadelphia: Elsevier; 2018:223.e2–232.e2. doi: 10.1016/B978-0-323-40196-8.00027-9[↩][↩][↩][↩][↩][↩]
- Harden NR, Bruehl S, Perez RSGM, Birklein F, Marinus J, Maihofner C, Lubenow T, Buvanendran A, Mackey S, Graciosa J, Mogilevski M, Ramsden C, Chont M, Vatine JJ. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain. 2010 Aug;150(2):268-274. doi: 10.1016/j.pain.2010.04.030[↩]
- Melf-Marzi A, Böhringer B, Wiehle M, Hausteiner-Wiehle C. Modern Principles of Diagnosis and Treatment in Complex Regional Pain Syndrome. Dtsch Arztebl Int. 2022 Dec 27;119(51-52):879-886. doi: 10.3238/arztebl.m2022.0358[↩][↩]
- Harden RN, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain. 2010;150:268–74. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2914601/[↩]
- Sandroni P, Benrud-Larson LM, McClelland RL, Low PA. Complex regional pain syndrome type I: incidence and prevalence in Olmsted county, a population-based study. Pain. 2003 May;103(1-2):199-207. doi: 10.1016/s0304-3959(03)00065-4[↩][↩]
- Finnern MM, Kleinböhl D, Flor H, Benrath J, Hölzl R. Deconstructing chronicity of musculoskeletal pain: intensity-duration relations, minimal dimensions and clusters of chronicity. Scand J Pain. 2018 Jul 26;18(3):363-377. doi: 10.1515/sjpain-2018-0021[↩]
- Devarajan J, Mena S, Cheng J. Mechanisms of complex regional pain syndrome. Front Pain Res (Lausanne). 2024 May 17;5:1385889. doi: 10.3389/fpain.2024.1385889[↩]
- Shim H, et al. Complex regional pain syndrome: a narrative review for the practising clinician. Br J Anaesth. 2019;123(2):e424–e433. doi: 10.1016/j.bja.2019.03.030[↩]
- Li TS, Wang R, Su X, Wang XQ. Effect and mechanisms of exercise for complex regional pain syndrome. Front Mol Neurosci. 2023 May 3;16:1167166. doi: 10.3389/fnmol.2023.1167166[↩]
- Ott S, Maihöfner C. Signs and symptoms in 1,043 patients with complex regional pain syndrome. J Pain. 2018;19(6):599–611. doi: 10.1016/j.jpain.2018.01.004[↩][↩][↩][↩]
- Mertz K, Trunzter J, Wu E, Barnes J, Eppler SL, Kamal RN. National trends in the diagnosis of CRPS after open and endoscopic carpal tunnel release. J Wrist Surg. 2019;08(03):209–214. doi: 10.1055/s-0039-1678674[↩]
- Jo Y-H, Kim K, Lee B-G, Kim J-H, Lee C-H, Lee K-H. Incidence of and risk factors for complex regional pain syndrome type 1 after surgery for distal radius fractures: a population-based study. Sci Rep. 2019 doi: 10.1038/S41598-019-41152-X[↩][↩][↩][↩]
- Bruehl S. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology. 2010 Sep;113(3):713-25. doi: 10.1097/ALN.0b013e3181e3db38[↩]
- de Rooij AM, de Mos M, Sturkenboom MC, Marinus J, van den Maagdenberg AM, van Hilten JJ. Familial occurrence of complex regional pain syndrome. Eur J Pain. 2009 Feb;13(2):171-7. doi: 10.1016/j.ejpain.2008.04.004[↩]
- Shaikh SS, Goebel A, Lee MC, Nahorski MS, Shenker N, Pamela Y, Drissi I, Brown C, Ison G, Shaikh MF, Kuttikat A, Woods WA, Dixit A, Stouffer K, Clarke MC, Menon DK, Woods CG. Evidence of a genetic background predisposing to complex regional pain syndrome type 1. J Med Genet. 2024 Jan 19;61(2):163-170. doi: 10.1136/jmg-2023-109236[↩]
- Modarresi S, Aref-Eshghi E, Walton DM, MacDermid JC. Does a familial subtype of complex regional pain syndrome exist? Results of a systematic review. Can J Pain. 2019 Aug 1;3(1):157-166. doi: 10.1080/24740527.2019.1637249[↩]
- Jin EH, Zhang E, Ko Y, Sim WS, Moon DE, Yoon KJ, Hong JH, Lee WH. Genome-wide expression profiling of complex regional pain syndrome. PLoS One. 2013 Nov 14;8(11):e79435. doi: 10.1371/journal.pone.0079435[↩]
- Pohóczky K, Kun J, Szentes N, Aczél T, Urbán P, Gyenesei A, Bölcskei K, Szőke É, Sensi S, Dénes Á, Goebel A, Tékus V, Helyes Z. Discovery of novel targets in a complex regional pain syndrome mouse model by transcriptomics: TNF and JAK-STAT pathways. Pharmacol Res. 2022 Aug;182:106347. doi: 10.1016/j.phrs.2022.106347[↩]
- Wiper A, Amoroso G, Rao S, Nolan J. Complex regional pain syndrome: a rare but potentially disabling complication of transradial cardiac catheterization. Catheter Cardiovasc Interv. 2020;95(5):E140–E143. doi: 10.1002/ccd.28357[↩]
- Crijns TJ, Van Der Gronde BATD, Ring D, Leung N. Complex regional pain syndrome after distal radius fracture is uncommon and is often associated with fibromyalgia. Clin Orthop Relat Res. 2018;476(4):744–750. doi: 10.1007/s11999.0000000000000070[↩][↩]
- Rochlin DH, Sheckter CC, Satteson ES, Swan CC, Fox PM, Curtin C. Separating fact from fiction: a nationwide longitudinal examination of complex regional pain syndrome following treatment of Dupuytren contracture. Hand. 2020 doi: 10.1177/1558944720963915[↩]
- Elsharydah A, Loo NH, Minhajuddin A, Kandil ES. Complex regional pain syndrome type 1 predictors—epidemiological perspective from a national database analysis. J Clin Anesth. 2017 doi: 10.1016/j.jclinane.2017.03.027[↩]
- Elsamadicy AA, Yang S, Sergesketter AR, et al. Prevalence and cost analysis of complex regional pain syndrome (CRPS): a role for neuromodulation. Neuromodulation. 2018;21(5):423–430. doi: 10.1111/ner.12691[↩]
- van Velzen GAJ, Huygen FJPM, van Kleef M, van Eijs FV, Marinus J, van Hilten JJ. Sex matters in complex regional pain syndrome. Eur J Pain (United Kingdom) 2019;23(6):1108–1116. doi: 10.1002/ejp.1375[↩][↩]
- Lipman MD, Hess DE, Werner BC, Deal DN. Fibromyalgia as a predictor of complex regional pain syndrome after distal radius fracture. Hand. 2019;14(4):516–522. doi: 10.1177/1558944717735949[↩]
- Birklein F, Ajit SK, Goebel A, Perez RSGM, Sommer C. Complex regional pain syndrome-phenotypic characteristics and potential biomarkers. Nat Rev Neurol. 2018;14(5):272–284. doi: 10.1038/nrneurol.2018.20[↩]
- Ward D, Thorsen NM, Frisch M, Valentiner-Branth P, Mølbak K, Hviid A. A cluster analysis of serious adverse event reports after human papillomavirus (HPV) vaccination in Danish girls and young women, September 2009 to August 2017. Euro Surveill. 2019;24(19):1. doi: 10.2807/1560-7917.ES.2019.24.19.1800380[↩]
- Hviid A, Thorsen NM, Valentiner-Branth P, Frisch M, Mølbak K. Association between quadrivalent human papillomavirus vaccination and selected syndromes with autonomic dysfunction in Danish females: population based, self-controlled, case series analysis. BMJ. 2020 doi: 10.1136/bmj.m2930[↩]
- Barboi A, Gibbons CH, Axelrod F, et al. Human papillomavirus (HPV) vaccine and autonomic disorders: a position statement from the American Autonomic Society. Auton Neurosci Basic Clin. 2020;223(1):13–18. doi: 10.1016/j.autneu.2019.05.002[↩]
- Misidou C, Papagoras C. Complex regional pain syndrome: an update. Mediterr J Rheumatol. 2019;30(1):16–25. doi: 10.31138/mjr.30.1.16[↩]
- Baronio M, Sadia H, Paolacci S, et al. Molecular aspects of regional pain syndrome. Pain Res Manag. 2020 doi: 10.1155/2020/7697214[↩]
- Complex Regional Pain Syndromes Pathophysiology. https://emedicine.medscape.com/article/1145318-overview#a5[↩]
- Galer BS, Schwartz L, Allen RJ. Loeser JD, Butler SH, Chapman RC, Turk DC,(eds). Complex regional pain syndromes– Type I: reflex sympathetic dystrophy, and type II: causalgia, in: Bonica’s management of pain. Philadelphia: Lippincott Williams & Wilkins; 2001. 388- 411.[↩][↩][↩]
- Baron R, Levine JD, Fields HL. Causalgia and reflex sympathetic dystrophy: does the sympathetic nervous system contribute to the generation of pain? Muscle Nerve. 1999 Jun;22(6):678-95. doi: 10.1002/(sici)1097-4598(199906)22:6<678::aid-mus4>3.0.co;2-p[↩]
- Giordano J, Boswell MV. Neurobiology of nociceptive and anti-nociceptive systems. Manchikanti L, Singh V(eds). Interventional techniques in chronic spinal pain. Paducah, Kentucky: ASSIP publishing; 2007. 17-32.[↩]
- Kawakami, Chatenia K, Weinstein JN. AH, Schofferman JA (ed.). Anatomy, biochemistry, and physiology of low back pain, in White Spine Care: diagnosis and conservative treatment. St. Louis: Mosby Press; 1995. pp 84-103.[↩]
- Wheeler AH, Murrey DB. Spinal pain: pathogenesis, evolutionary mechanisms and management. Pappagallo M, ed. The Neurologic Basis of Pain. New York: McGraw-Hill; 2003. 421-52.[↩]
- Rockett M. Diagnosis, mechanisms and treatment of complex regional pain syndrome. Curr Opin Anaesthesiol. 2014 Oct;27(5):494-500. doi: 10.1097/ACO.0000000000000114[↩][↩]
- Baronio M, Sadia H, Paolacci S, Prestamburgo D, Miotti D, Guardamagna VA, Natalini G, Sullivan SGB, Bertelli M. Molecular Aspects of Regional Pain Syndrome. Pain Res Manag. 2020 Apr 11;2020:7697214. doi: 10.1155/2020/7697214[↩]
- Littlejohn G. Neurogenic neuroinflammation in fibromyalgia and complex regional pain syndrome. Nat Rev Rheumatol. 2015 Nov;11(11):639-48. doi: 10.1038/nrrheum.2015.100[↩][↩][↩][↩]
- Bussa M, Mascaro A, Cuffaro L, Rinaldi S. Adult Complex Regional Pain Syndrome Type I: A Narrative Review. PM R. 2017 Jul;9(7):707-719. doi: 10.1016/j.pmrj.2016.11.006[↩][↩]
- Li WW, Guo TZ, Liang DY, Sun Y, Kingery WS, Clark JD. Substance P signaling controls mast cell activation, degranulation, and nociceptive sensitization in a rat fracture model of complex regional pain syndrome. Anesthesiology. 2012 Apr;116(4):882-95. doi: 10.1097/ALN.0b013e31824bb303[↩]
- Birklein F, Riedl B, Sieweke N, Weber M, Neundörfer B. Neurological findings in complex regional pain syndromes-analysis of 145 cases. Acta Neurol Scand 2000;101:262–9. https://doi.org/10.1034/j.1600-0404.2000.09008.x[↩][↩]
- Maihöfner C, Baron R, DeCol R, Binder A, Birklein F, Deuschl G, Handwerker HO, Schattschneider J. The motor system shows adaptive changes in complex regional pain syndrome. Brain. 2007 Oct;130(Pt 10):2671-87. doi: 10.1093/brain/awm131[↩]
- Di Pietro F, McAuley JH, Parkitny L, Lotze M, Wand BM, Moseley GL, Stanton TR. Primary motor cortex function in complex regional pain syndrome: a systematic review and meta-analysis. J Pain. 2013 Nov;14(11):1270-88. doi: 10.1016/j.jpain.2013.07.004[↩]
- Di Pietro F, McAuley JH, Parkitny L, Lotze M, Wand BM, Moseley GL, Stanton TR. Primary somatosensory cortex function in complex regional pain syndrome: a systematic review and meta-analysis. J Pain. 2013 Oct;14(10):1001-18. doi: 10.1016/j.jpain.2013.04.001[↩]
- Maihöfner C, Forster C, Birklein F, Neundörfer B, Handwerker HO. Brain processing during mechanical hyperalgesia in complex regional pain syndrome: a functional MRI study. Pain. 2005 Mar;114(1-2):93-103. doi: 10.1016/j.pain.2004.12.001[↩]
- Schwenkreis P, Maier C, Tegenthoff M. Functional imaging of central nervous system involvement in complex regional pain syndrome. AJNR Am J Neuroradiol. 2009 Aug;30(7):1279-84. doi: 10.3174/ajnr.A1630[↩]
- Shokouhi M, Clarke C, Morley-Forster P, Moulin DE, Davis KD, St Lawrence K. Structural and Functional Brain Changes at Early and Late Stages of Complex Regional Pain Syndrome. J Pain. 2018 Feb;19(2):146-157. doi: 10.1016/j.jpain.2017.09.007[↩]
- Galer BS, Butler S, Jensen MP. Case reports and hypothesis: a neglect-like syndrome may be responsible for the motor disturbance in reflex sympathetic dystrophy (Complex Regional Pain Syndrome-1). J Pain Symptom Manage. 1995 Jul;10(5):385-91. doi: 10.1016/0885-3924(95)00061-3[↩]
- Urits I, Shen AH, Jones MR, Viswanath O, Kaye AD. Complex Regional Pain Syndrome, Current Concepts and Treatment Options. Curr Pain Headache Rep. 2018 Feb 5;22(2):10. doi: 10.1007/s11916-018-0667-7[↩][↩]
- Terkelsen AJ, Mølgaard H, Hansen J, Finnerup NB, Krøner K, Jensen TS. Heart rate variability in complex regional pain syndrome during rest and mental and orthostatic stress. Anesthesiology. 2012 Jan;116(1):133-46. doi: 10.1097/ALN.0b013e31823bbfb0[↩]
- Baron R, Binder A. Pappagallo M (ed). complex regional pain syndromes, in The neurological basis of pain. New York: McGraw-Hill; 2005:. 359-378.[↩]
- Janig W, Koltzendbrg M. Bond MR, Charlton EJ, Woolf CJ (eds). sympathetic reflex activity and neuro- factor transmission change after chronic nerve lesions in Proceedings of the VIth world Congress on pain. Amsterdam: Elsevier Science; 1991. 365-371.[↩]
- Baron R, Wasner G, Borgstedt R, Hastedt E, Schulte H, Binder A, Kopper F, Rowbotham M, Levine JD, Fields HL. Effect of sympathetic activity on capsaicin-evoked pain, hyperalgesia, and vasodilatation. Neurology. 1999 Mar 23;52(5):923-32. doi: 10.1212/wnl.52.5.923[↩][↩]
- Harden RN, Duc TA, Williams TR, Coley D, Cate JC, Gracely RH. Norepinephrine and epinephrine levels in affected versus unaffected limbs in sympathetically maintained pain. Clin J Pain. 1994 Dec;10(4):324-30. doi: 10.1097/00002508-199412000-00014[↩]
- Treede RD, Davis KD, Campbell JN, Raja SN. The plasticity of cutaneous hyperalgesia during sympathetic ganglion blockade in patients with neuropathic pain. Brain. 1992 Apr;115 ( Pt 2):607-21. doi: 10.1093/brain/115.2.607[↩]
- Chelimsky TC, Low PA, Naessens JM, Wilson PR, Amadio PC, O’Brien PC. Value of autonomic testing in reflex sympathetic dystrophy. Mayo Clin Proc. 1995 Nov;70(11):1029-40. doi: 10.4065/70.11.1029[↩][↩]
- Jänig W. Experimental approach to reflex sympathetic dystrophy and related syndromes. Pain. 1991 Sep;46(3):241-245. doi: 10.1016/0304-3959(91)90107-9[↩][↩]
- Jänig W, Levine JD, Michaelis M. Interactions of sympathetic and primary afferent neurons following nerve injury and tissue trauma. Prog Brain Res. 1996;113:161-84. doi: 10.1016/s0079-6123(08)61087-0[↩][↩]
- McLachlan EM, Jänig W, Devor M, Michaelis M. Peripheral nerve injury triggers noradrenergic sprouting within dorsal root ganglia. Nature. 1993 Jun 10;363(6429):543-6. doi: 10.1038/363543a0[↩][↩]
- Shi TS, Winzer-Serhan U, Leslie F, Hökfelt T. Distribution and regulation of alpha(2)-adrenoceptors in rat dorsal root ganglia. Pain. 2000 Feb;84(2-3):319-30. doi: 10.1016/s0304-3959(99)00224-9[↩][↩]
- Jänig W, Baron R. Complex regional pain syndrome is a disease of the central nervous system. Clin Auton Res. 2002 Jun;12(3):150-64. doi: 10.1007/s10286-002-0022-1[↩][↩]
- Raja SN, Treede RD, Davis KD, Campbell JN. Systemic alpha-adrenergic blockade with phentolamine: a diagnostic test for sympathetically maintained pain. Anesthesiology. 1991 Apr;74(4):691-8. doi: 10.1097/00000542-199104000-00012[↩]
- Stanton-Hicks M, Jänig W, Hassenbusch S, Haddox JD, Boas R, Wilson P. Reflex sympathetic dystrophy: changing concepts and taxonomy. Pain. 1995 Oct;63(1):127-133. doi: 10.1016/0304-3959(95)00110-E[↩]
- van Velzen GA, Rombouts SA, van Buchem MA, Marinus J, van Hilten JJ. Is the brain of complex regional pain syndrome patients truly different? Eur J Pain. 2016 Nov;20(10):1622-1633. doi: 10.1002/ejp.882[↩]
- Bean DJ, Johnson MH, Kydd RR. Relationships between psychological factors, pain, and disability in complex regional pain syndrome and low back pain. Clin J Pain. 2014 Aug;30(8):647-53. doi: 10.1097/AJP.0000000000000007[↩][↩]
- Beerthuizen A, Stronks DL, Huygen FJ, Passchier J, Klein J, Spijker AV. The association between psychological factors and the development of complex regional pain syndrome type 1 (CRPS1)–a prospective multicenter study. Eur J Pain. 2011 Oct;15(9):971-5. doi: 10.1016/j.ejpain.2011.02.008[↩][↩]
- Beerthuizen A, van ‘t Spijker A, Huygen FJ, Klein J, de Wit R. Is there an association between psychological factors and the Complex Regional Pain Syndrome type 1 (CRPS1) in adults? A systematic review. Pain. 2009 Sep;145(1-2):52-9. doi: 10.1016/j.pain.2009.05.003[↩]
- Goebel A, Blaes F. Complex regional pain syndrome, prototype of a novel kind of autoimmune disease. Autoimmun Rev. 2013;12(6):682–686. doi: 10.1016/j.autrev.2012.10.015[↩]
- Doria A, Zen M, Bettio S, Gatto M, Bassi N, Nalotto L, et al. Autoinflammation and autoimmunity: bridging the divide. Autoimmun Rev. 2012;12(1):22–30. doi: 10.1016/j.autrev.2012.07.018[↩]
- Dirckx M, Schreurs MW, de Mos M, Stronks DL, Huygen FJ. The prevalence of autoantibodies in complex regional pain syndrome type I. Mediat Inflamm. 2015;2015:718201. doi: 10.1155/2015/718201[↩]
- Kohr D, Singh P, Tschernatsch M, Kaps M, Pouokam E, Diener M, Kummer W, Birklein F, Vincent A, Goebel A, Wallukat G, Blaes F. Autoimmunity against the β2 adrenergic receptor and muscarinic-2 receptor in complex regional pain syndrome. Pain. 2011 Dec;152(12):2690-2700. doi: 10.1016/j.pain.2011.06.012[↩]
- Kohr D, Tschernatsch M, Schmitz K, Singh P, Kaps M, Schafer KH, et al. Autoantibodies in complex regional pain syndrome bind to a differentiation-dependent neuronal surface autoantigen. Pain. 2009;143(3):246–251. doi: 10.1016/j.pain.2009.03.009[↩]
- Dubuis E, Thompson V, Leite MI, Blaes F, Maihöfner C, Greensmith D, et al. Longstanding complex regional pain syndrome is associated with activating autoantibodies against alpha-1a adrenoceptors. Pain. 2014;155(11):2408–2417. doi: 10.1016/j.pain.2014.09.022[↩]
- Kohr D, Tschernatsch M, Schmitz K, Singh P, Kaps M, Schäfer KH, Diener M, Mathies J, Matz O, Kummer W, Maihöfner C, Fritz T, Birklein F, Blaes F. Autoantibodies in complex regional pain syndrome bind to a differentiation-dependent neuronal surface autoantigen. Pain. 2009 Jun;143(3):246-251. doi: 10.1016/j.pain.2009.03.009[↩]
- Goebel A, Baranowski A, Maurer K, Ghiai A, McCabe C, Ambler G. Intravenous immunoglobulin treatment of the complex regional pain syndrome: a randomized trial. Ann Intern Med. 2010 Feb 2;152(3):152-8. doi: 10.7326/0003-4819-152-3-201002020-00006[↩][↩][↩]
- Goebel A, Bisla J, Carganillo R, Frank B, Gupta R, Kelly J, McCabe C, Murphy C, Padfield N, Phillips C, Sanders M, Serpell M, Shenker N, Shoukrey K, Wyatt L, Ambler G. Low-Dose Intravenous Immunoglobulin Treatment for Long-Standing Complex Regional Pain Syndrome: A Randomized Trial. Ann Intern Med. 2017 Oct 3;167(7):476-483. doi: 10.7326/M17-0509[↩][↩]
- Cuhadar U, Gentry C, Vastani N, Sensi S, Bevan S, Goebel A, et al. Autoantibodies produce pain in complex regional pain syndrome by sensitizing nociceptors. Pain. 2019;160(12):2855–2865. doi: 10.1097/j.pain.0000000000001662[↩]
- Pérez-Concha T, Tijero B, Acera M, et al. . Usefulness of thermography in the diagnosis and classification of complex regional pain syndrome. Neurología. 2020;38(5):342–349. doi: 10.1016/j.nrl.2020.10.011[↩]
- Castillo-Guzmán S, Nava-Obregón TA, Palacios-Ríos D, et al. . Complex regional pain syndrome (CRPS), a review. Medicina Universitaria. 2015;17(67):114–121. doi: 10.1016/j.rmu.2015.03.003[↩][↩][↩][↩]
- Lubkowska A, Pluta W.. Infrared thermography as a Non-Invasive tool in musculoskeletal disease rehabilitation–The control variables in applicability–A systematic review. Appl Sci. 2022;12(9):4302. doi: 10.3390/app12094302[↩]
- Kessler A, Yoo M, Calisoff R, et al. . Complex regional pain syndrome: an updated comprehensive review. NeuroRehabilitation. 2020;47(3):253–264. doi: 10.3233/NRE-208001[↩]
- Bruehl S, Harden RN, Galer BS, et al. . Complex regional pain syndrome: are there distinct subtypes and sequential stages of the syndrome? Pain. 2002;95(1-2):119–124. doi: 10.1016/s0304-3959(01)00387-6[↩]
- Bussa M, Guttilla D, Lucia M, Mascaro A, Rinaldi S. Complex regional pain syndrome type I: a comprehensive review. Acta Anaesthesiol Scand. 2015 Jul;59(6):685-97. doi: 10.1111/aas.12489[↩]
- Goebel A. Complex regional pain syndrome in adults. Rheumatology. 2011;50(10):1739-50. https://www.ncbi.nlm.nih.gov/pubmed/21712368[↩]
- O’Connell NE, Wand BM, McAuley J, Marston L, Moseley GL. Interventions for treating pain and disability in adults with complex regional pain syndrome. Cochrane Database Syst Rev. 2013 Apr 30;2013(4):CD009416. doi: 10.1002/14651858.CD009416.pub2. Update in: Cochrane Database Syst Rev. 2023 Jun 12;6:CD009416. doi: 10.1002/14651858.CD009416.pub3[↩]
- Duong S, Bravo D, Todd KJ, Finlayson RJ, Tran Q. Treatment of complex regional pain syndrome: an updated systematic review and narrative synthesis. Can J Anaesth. 2018 Jun;65(6):658-684. English. doi: 10.1007/s12630-018-1091-5[↩]
- Mangnus TJP, Dirckx M, Huygen FJPM. Different Types of Pain in Complex Regional Pain Syndrome Require a Personalized Treatment Strategy. J Pain Res. 2023 Dec 27;16:4379-4391. doi: 10.2147/JPR.S432209[↩]
- Shim H, Rose J, Halle S, et al. . Complex regional pain syndrome: a narrative review for the practising clinician. Br J Anaesth. 2019;123(2):e424–e433. doi: 10.1016/J.BJA.2019.03.03.0[↩][↩][↩]
- Collins CK. Physical therapy management of complex regional pain syndrome I in a 14-year-old patient using strain counterstrain: a case report. J Man Manip Ther. 2007;15(1):25–41 doi: 10.1179/106698107791090150[↩]
- Menck JY, Requejo SM, Kulig K.. Thoracic spine dysfunction in upper extremity complex regional pain syndrome type I. J Orthop Sports Phys Ther. 2000;30(7):401–409. doi: 10.2519/JOSPT.2000.30.7.401[↩]
- Cleland J, McRae M.. Complex regional pain syndrome I: management through the use of vertebral and sympathetic trunk mobilization. J Man Manip Ther. 2002;10(4):188–199. doi: 10.1179/106698102790819067[↩]
- Gutiérrez-Espinoza H, Tabach-Apraiz A, Oyanadel-Maldonado M.. Physical therapy in patients with complex regional pain syndrome type I after distal radius fracture: a case series. J Phys Ther Sci. 2019;31(4):403–407. doi: 10.1589/JPTS.31.40.3[↩]
- Walston Z, Hernandez L, Yake D.. Utilization of manual therapy to the lumbar spine in conjunction with traditional conservative care for individuals with bilateral lower extremity complex regional pain syndrome: A case series. Physiother Theory Pract. 2018;36(1):241–248. doi: 10.1080/09593985.2018.1482392[↩]
- Lohnberg JA, Altmaier EM.. A review of psychosocial factors in complex regional pain syndrome. J Clin Psychol Med Settings. 2013;20(2):247–254. doi: 10.1007/S10880-012-9322-3[↩]
- Edwards RR, Smith MT, Kudel I, et al. . Pain-related catastrophizing as a risk factor for suicidal ideation in chronic pain. Pain. 2006;126(1-3):272–279. doi: 10.1016/J.PAIN.2006.07.004[↩]
- Bodde MI, Schrier E, Krans HK, et al. . Resilience in patients with amputation because of complex regional pain syndrome type I. Disabil Rehabil. 2014;36(10):838–843. doi: 10.3109/09638288.2013.822023[↩][↩]
- Tang NKY, Crane C.. Suicidality in chronic pain: a review of the prevalence, risk factors and psychological links. Psychol Med. 2006;36(5):575–586. doi: 10.1017/S0033291705006859[↩]
- Ryskalin L, Ghelarducci G, Marinelli C, et al. . Effectiveness of decision support to treat complex regional pain syndrome. Appl Sci. 2022;12(18):8979. doi: 10.3390/app12188979[↩]
- Fialka V, Korpan M, Saradeth T, et al. . Autogenic training for reflex sympathetic dystrophy: a pilot study. Complement Ther Med. 1996;4(2):103–105. doi: 10.1016/S0965-2299(96)80026-4[↩][↩]
- Albazaz R, Wong YT, Homer-Vanniasinkam S.. Complex regional pain syndrome: a review. Ann Vasc Surg. 2008;22(2):297–306. doi: 10.1016/J.AVSG.2007.10.006[↩]
- Mackey S, Feinberg S.. Pharmacologic therapies for complex regional pain syndrome. Curr Pain Headache Rep. 2007;11(1):38–43. doi: 10.1007/S11916-007-0020-Z[↩]
- Nazir SST, Ivan N, Antonella U, et al. . Complex regional pain syndrome: a comprehensive review. Pain Ther. 2021;10(2):875–892. doi: 10.1007/S40122-021-00279-4[↩]
- Resmini G, Ratti C, Canton G, et al. . Treatment of complex regional pain syndrome. Clin Cases Miner Bone Metab. 2015;12(Suppl 1):26–30. doi: 10.11138/CCMBM/2015.12.3S.026[↩]
- Kalita J, Vajpayee A, Misra UK.. Comparison of prednisolone with piroxicam in complex regional pain syndrome following stroke: a randomized controlled trial. QJM. 2006;99(2):89–95. doi: 10.1093/QJMED/HCL004[↩]
- Atalay N, Ercidogan O, Akkaya N, et al. . Prednisolone in complex regional pain syndrome. Pain Phys. 2014;2;17(2;3):179–185. doi: 10.36076/ppj.2014/17/179[↩]
- Bianchi C, Rossi S, Turi S, Brambilla A, Felisari G, Mascheri D. Long-term functional outcome measures in corticosteroid-treated complex regional pain syndrome. Eura Medicophys. 2006 Jun;42(2):103-11. https://www.minervamedica.it/en/journals/europa-medicophysica/article.php?cod=R33Y2006N02A0103[↩]
- Jamroz A, Berger M, Winston P.. Prednisone for acute complex regional pain syndrome: a retrospective cohort study. Pain Res Manag. 2020;2020:8182569. doi: 10.1155/2020/8182569[↩]
- Gelman B, Hsu ES.. Gabapentin. In: Sinatra RS, Jahr JS, J. Watkins-Pitchford M (editors). The essence of analgesia and analgesics. Cambridge: Cambridge University Press; 2022. p. 294–297. doi: 10.1017/CBO9780511841378.071[↩]
- van de Vusse AC, Stomp-van den Berg SGM, Kessels AHF, et al. . Randomised controlled trial of gabapentin in complex regional pain syndrome type 1 [ISRCTN84121379]. BMC Neurol. 2004;4(1):13. doi: 10.1186/1471-2377-4-13[↩]
- Brown S, Johnston B, Amaria K, et al. . A randomized controlled trial of amitriptyline versus gabapentin for complex regional pain syndrome type I and neuropathic pain in children. Scand J Pain. 2016;13(1):156–163. doi: 10.1016/J.SJPAIN.2016.05.039[↩]
- Varenna M, Adami S, Sinigaglia L. Bisphosphonates in Complex Regional Pain syndrome type I: how do they work? Clin Exp Rheumatol. 2014 Jul-Aug;32(4):451-4. https://www.clinexprheumatol.org/abstract.asp?a=8025[↩][↩]
- Chevreau M, Romand X, Gaudin P, et al. . Bisphosphonates for treatment of complex regional pain syndrome type 1: a systematic literature review and meta-analysis of randomized controlled trials versus placebo. Joint Bone Spine. 2017;84(4):393–399. doi: 10.1016/J.JBSPIN.2017.03.009[↩]
- Connolly SB, Prager JP, Harden RN.. A systematic review of ketamine for complex regional pain syndrome. Pain Med. 2015;16(5):943–969. doi: 10.1111/PME.12675[↩][↩]
- Rosenbaum SB, Gupta V, Patel P, et al. Ketamine. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470357[↩]
- Azari P, Lindsay DR, Briones D, et al. . Efficacy and safety of ketamine in patients with complex regional pain syndrome. CNS Drugs. 2012;26(3):215–228. doi: 10.2165/11595200-000000000-00000[↩]
- Wissel J, Müller J, Dressnandt J, et al. . Management of spasticity associated pain with botulinum toxin A. J Pain Symptom Manage. 2000;20(1):44–49. doi: 10.1016/S0885-3924(00)00146-9[↩]
- Schilder JC, van Dijk JG, Dressler D, Koelman JH, Marinus J, van Hilten JJ. Responsiveness to botulinum toxin type A in muscles of complex regional pain patients with tonic dystonia. J Neural Transm (Vienna). 2014 Jul;121(7):761-7. doi: 10.1007/s00702-014-1172-8[↩]
- Carroll I, Clark JD, Mackey S.. Sympathetic block with botulinum toxin to treat complex regional pain syndrome. Ann Neurol. 2009;65(3):348–351. doi: 10.1002/ANA.21601[↩]
- Siongco PRL, Rosales RL, Moore AP, Freynhagen R, Arimura K, Kanovsky P, Kaji R, Fernandez HH, Dressler D. Botulinum neurotoxin injections for muscle-based (dystonia and spasticity) and non-muscle-based (neuropathic pain) pain disorders: a meta-analytic study. J Neural Transm (Vienna). 2020 Jun;127(6):935-951. doi: 10.1007/s00702-020-02163-5[↩]
- Lee Y, Lee CJ, Choi E, et al. . Lumbar sympathetic block with botulinum toxin type a and type B for the complex regional pain syndrome. Toxins. 2018;10(4):164. doi: 10.3390/TOXINS10040164[↩]
- Comella CL, Jankovic J, Shannon KM, et al. . Comparison of botulinum toxin serotypes a and B for the treatment of cervical dystonia. Neurology. 2005;65(9):1423–1429. doi: 10.1212/01.WNL.0000183055.81056.5C[↩]
- Tokuno H. Efficacy of Botulinum toxin injection in reducing limb pain in patients with complex regional pain syndrome. https://clinicaltrials.gov/study/NCT03616262[↩]
- Singh V, Cohen SP.. Prolonging sympathetic blockade for complex regional pain syndrome: is botulinum toxin the answer? Anesthesiology. 2022;136(2):261–264. doi: 10.1097/ALN.0000000000004093[↩]
- Eisenberg E, Shtahl S, Geller R, et al. . Serum and salivary oxidative analysis in complex regional pain syndrome. Pain. 2008;138(1):226–232. doi: 10.1016/J.PAIN.2008.04.019[↩]
- Baykal T, Seferoglu B, Karsan O, et al. . Antioxidant profile in patients with complex regional pain syndrome type I. Int J Rheum Dis. 2014;17(2):156–158. doi: 10.1111/1756-185X.12140[↩]
- Hernigou J, Labadens A, Ghistelinck B, Bui Quoc E, Maes R, Bhogal H, Callewier A, Bath O, Chahidi E, Safar A. Vitamin C prevention of complex regional pain syndrome after foot and ankle surgery: a prospective randomized study of three hundred and twenty nine patients. Int Orthop. 2021 Sep;45(9):2453-2459. doi: 10.1007/s00264-021-05159-2[↩]
- Jacques H, Jérôme V, Antoine C, Lucile S, Valérie D, Amandine L, Theofylaktos K, Olivier B. Prospective randomized study of the vitamin C effect on pain and complex pain regional syndrome after total knee arthroplasty. Int Orthop. 2021 May;45(5):1155-1162. doi: 10.1007/s00264-020-04936-9[↩]
- Laumonerie P, Martel M, Tibbo ME, Azoulay V, Mansat P, Bonnevialle N. Influence of vitamin C on the incidence of CRPS-I after subacromial shoulder surgery. Eur J Orthop Surg Traumatol. 2020 Feb;30(2):221-226. doi: 10.1007/s00590-019-02542-z[↩]
- Aïm F, Klouche S, Frison A, et al. . Efficacy of vitamin C in preventing complex regional pain syndrome after wrist fracture: a systematic review and meta-analysis. Orthop Traumatol Surg Res. 2017;103(3):465–470. doi: 10.1016/J.OTSR.2016.12.021[↩]
- O’Connell NE, Wand BM, Gibson W, Carr DB, Birklein F, Stanton TR. Local anaesthetic sympathetic blockade for complex regional pain syndrome. Cochrane Database Syst Rev. 2016 Jul 28;7(7):CD004598. doi: 10.1002/14651858.CD004598.pub4[↩][↩]
- Cheng J, Salmasi V, You J, et al. . Outcomes of sympathetic blocks in the management of complex regional pain syndrome: a retrospective cohort study. Anesthesiology. 2019;131(4):883–893. doi: 10.1097/ALN.0000000000002899[↩]
- Visnjevac O, Costandi S, Patel BA, Azer G, Agarwal P, Bolash R, Mekhail NA. A Comprehensive Outcome-Specific Review of the Use of Spinal Cord Stimulation for Complex Regional Pain Syndrome. Pain Pract. 2017 Apr;17(4):533-545. doi: 10.1111/papr.12513[↩][↩][↩]
- Hoikkanen T, Nissen M, Ikäheimo TM, Jyrkkänen HK, Huttunen J, von Und Zu Fraunberg M. Long-Term Outcome of Spinal Cord Stimulation in Complex Regional Pain Syndrome. Neurosurgery. 2021 Sep 15;89(4):597-609. doi: 10.1093/neuros/nyab239[↩][↩]
- Graham RD, Sankarasubramanian V, Lempka SF.. Dorsal root ganglion stimulation for chronic pain: hypothesized mechanisms of action. J Pain. 2022;23(2):196–211. doi: 10.1016/J.JPAIN.2021.07.008[↩]
- Koetsier E, Franken G, Debets J, et al. . Mechanism of dorsal root ganglion stimulation for pain relief in painful diabetic polyneuropathy is not dependent on GABA release in the dorsal horn of the spinal cord. CNS Neurosci Ther. 2020;26(1):136–143. doi: 10.1111/CNS.13192[↩]
- Deer TR, Levy RM, Kramer J, et al. . Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158(4):669–681. doi: 10.1097/J.PAIN.0000000000000814[↩][↩][↩]
- Koopmeiners AS, Mueller S, Kramer J, et al. . Effect of electrical field stimulation on dorsal root ganglion neuronal function. Neuromodulation. 2013;16(4):304–311. doi: 10.1111/NER.12028[↩]
- Huygen FJPM, Liem L, Nijhuis H, et al. . Evaluating dorsal root ganglion stimulation in a prospective Dutch cohort. Neuromodulation. 2019;22(1):80–86. doi: 10.1111/NER.12798[↩]
- Rauck RL, Eisenach JC, Jackson K, Young LD, Southern J. Epidural clonidine treatment for refractory reflex sympathetic dystrophy. Anesthesiology. 1993 Dec;79(6):1163-9; discussion 27A.[↩][↩][↩][↩][↩][↩]
- Cooper DE, DeLee JC, Ramamurthy S. Reflex sympathetic dystrophy of the knee. Treatment using continuous epidural anesthesia. J Bone Joint Surg Am. 1989 Mar;71(3):365-9. https://journals.lww.com/jbjsjournal/abstract/1989/71030/reflex_sympathetic_dystrophy_of_the_knee_.9.aspx[↩][↩]
- Koning H, Christiaans C, Overdijk G, Mackie D.. Cervical epidural blockade and reflex sympathetic dystrophy. Pain Clinic 1995;8:239–44.[↩]
- Buchheit T, Crews JC. Lateral cervical epidural catheter placement for continuous unilateral upper extremity analgesia and sympathetic block. Reg Anesth Pain Med. 2000 May-Jun;25(3):313-7. doi: 10.1016/s1098-7339(00)90019-1[↩]
- Du Pen SL, Peterson DG, Williams A, Bogosian AJ. Infection during chronic epidural catheterization: diagnosis and treatment. Anesthesiology. 1990 Nov;73(5):905-9. doi: 10.1097/00000542-199011000-00018[↩][↩]
- Lundborg C, Dahm P, Nitescu P, Appelgren L, Curelaru I. Clinical experience using intrathecal (IT) bupivacaine infusion in three patients with complex regional pain syndrome type I (CRPS-I). Acta Anaesthesiol Scand. 1999 Jul;43(6):667-78. doi: 10.1034/j.1399-6576.1999.430613.x[↩][↩]
- van Hilten BJ, van de Beek WJ, Hoff JI, Voormolen JH, Delhaas EM. Intrathecal baclofen for the treatment of dystonia in patients with reflex sympathetic dystrophy. N Engl J Med. 2000 Aug 31;343(9):625-30. doi: 10.1056/NEJM200008313430905[↩][↩][↩]
- Attal N, Brasseur L, Chauvin M, Bouhassira D. Effects of single and repeated applications of a eutectic mixture of local anaesthetics (EMLA) cream on spontaneous and evoked pain in post-herpetic neuralgia. Pain. 1999 May;81(1-2):203-9. doi: 10.1016/s0304-3959(99)00014-7[↩]
- Galer BS, Rowbotham MC, Perander J, Friedman E. Topical lidocaine patch relieves postherpetic neuralgia more effectively than a vehicle topical patch: results of an enriched enrollment study. Pain. 1999 Apr;80(3):533-538. doi: 10.1016/S0304-3959(98)00244-9[↩]
- Rowbotham MC, Davies PS, Verkempinck C, Galer BS. Lidocaine patch: double-blind controlled study of a new treatment method for post-herpetic neuralgia. Pain. 1996 Apr;65(1):39-44. doi: 10.1016/0304-3959(95)00146-8[↩]
- Chang A, Rosani A, Quick J. Capsaicin. [Updated 2023 May 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459168[↩][↩]
- Watson CP, Tyler KL, Bickers DR, Millikan LE, Smith S, Coleman E. A randomized vehicle-controlled trial of topical capsaicin in the treatment of postherpetic neuralgia. Clin Ther. 1993 May-Jun;15(3):510-26.[↩]
- Robbins WR, Staats PS, Levine J, Fields HL, Allen RW, Campbell JN, Pappagallo M. Treatment of intractable pain with topical large-dose capsaicin: preliminary report. Anesth Analg. 1998 Mar;86(3):579-83. doi: 10.1097/00000539-199803000-00027[↩]
- Bernstein JE, Korman NJ, Bickers DR, Dahl MV, Millikan LE. Topical capsaicin treatment of chronic postherpetic neuralgia. J Am Acad Dermatol. 1989 Aug;21(2 Pt 1):265-70. doi: 10.1016/s0190-9622(89)70171-7[↩]
- Treatment of painful diabetic neuropathy with topical capsaicin. A multicenter, double-blind, vehicle-controlled study. The Capsaicin Study Group. Arch Intern Med. 1991 Nov;151(11):2225-9. doi: 10.1001/archinte.151.11.2225[↩]
- Peikert A, Hentrich M, Ochs G. Topical 0.025% capsaicin in chronic post-herpetic neuralgia: efficacy, predictors of response and long-term course. J Neurol. 1991 Dec;238(8):452-6. doi: 10.1007/BF00314653[↩]
- Simone DA, Ochoa J. Early and late effects of prolonged topical capsaicin on cutaneous sensibility and neurogenic vasodilatation in humans. Pain. 1991 Dec;47(3):285-294. doi: 10.1016/0304-3959(91)90217-L[↩]
- Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain. 1992 May;49(2):221-230. doi: 10.1016/0304-3959(92)90145-2[↩]
- Backonja M, Wallace MS, Blonsky ER, Cutler BJ, Malan P Jr, Rauck R, Tobias J; NGX-4010 C116 Study Group. NGX-4010, a high-concentration capsaicin patch, for the treatment of postherpetic neuralgia: a randomised, double-blind study. Lancet Neurol. 2008 Dec;7(12):1106-12. doi: 10.1016/S1474-4422(08)70228-X Erratum in: Lancet Neurol. 2009 Jan;8(1):31.[↩]
- Simpson DM, Brown S, Tobias J; NGX-4010 C107 Study Group. Controlled trial of high-concentration capsaicin patch for treatment of painful HIV neuropathy. Neurology. 2008 Jun 10;70(24):2305-13. doi: 10.1212/01.wnl.0000314647.35825.9c[↩]
- Simpson DM, Gazda S, Brown S, Webster LR, Lu SP, Tobias JK, Vanhove GF; NGX-4010 C118 Study Group. Long-term safety of NGX-4010, a high-concentration capsaicin patch, in patients with peripheral neuropathic pain. J Pain Symptom Manage. 2010 Jun;39(6):1053-64. doi: 10.1016/j.jpainsymman.2009.11.316[↩]
- Girtler R, Kloimstein H, Gustorff B. Ausgeprägte Symptomverschlechterung bei CRPS Typ II nach einmaliger Applikation eines hochprozentigen Capsaicinpflasters. Ein Fallbericht [Pronounced symptom deterioration in complex regional pain syndrome type II after isolated application of a highly concentrated capsaicin patch. A case report]. Schmerz. 2013 Feb;27(1):67-71. German. doi: 10.1007/s00482-012-1268-8[↩]
- Zuurmond WW, Langendijk PN, Bezemer PD, Brink HE, de Lange JJ, van loenen AC. Treatment of acute reflex sympathetic dystrophy with DMSO 50% in a fatty cream. Acta Anaesthesiol Scand. 1996 Mar;40(3):364-7. doi: 10.1111/j.1399-6576.1996.tb04446.x[↩]
- Forouzanfar T, Köke AJ, van Kleef M, Weber WE. Treatment of complex regional pain syndrome type I. Eur J Pain. 2002;6(2):105-22. doi: 10.1053/eujp.2001.0304[↩]
- Aradillas E, Schwartzman RJ, Grothusen JR, Goebel A, Alexander GM. Plasma Exchange Therapy in Patients with Complex Regional Pain Syndrome. Pain Physician. 2015 Jul-Aug;18(4):383-94. https://www.painphysicianjournal.com/linkout?issn=&vol=18&page=383[↩]
- Schwartz J, Padmanabhan A, Aqui N, Balogun RA, Connelly-Smith L, Delaney M, Dunbar NM, Witt V, Wu Y, Shaz BH. Guidelines on the Use of Therapeutic Apheresis in Clinical Practice-Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Seventh Special Issue. J Clin Apher. 2016 Jun;31(3):149-62. doi: 10.1002/jca.21470[↩]
- Krans-Schreuder HK, Bodde MI, Schrier E, et al. . Amputation for long-standing, therapy-resistant type-I complex regional pain syndrome. J Bone Joint Surg Am. 2012;94(24):2263–2268. doi: 10.2106/JBJS.L.00532[↩]
- Honkamp N, Amendola A, Hurwitz S, et al. . Retrospective review of eighteen patients who underwent transtibial amputation for intractable pain. J Bone Joint Surg Am. 2001;83(10):1479–1483. doi: 10.2106/00004623-200110000-00003[↩]
- Kashy BK, Abd-Elsayed AA, Farag E, et al. . Amputation as an unusual treatment for Therapy-Resistant complex regional pain syndrome, type 1. Ochsner J. 2015;15(4):441–442. doi: 10.1043/TOJ-14-0074[↩]





{kind=link}