Contents
What is essential thrombocythemia
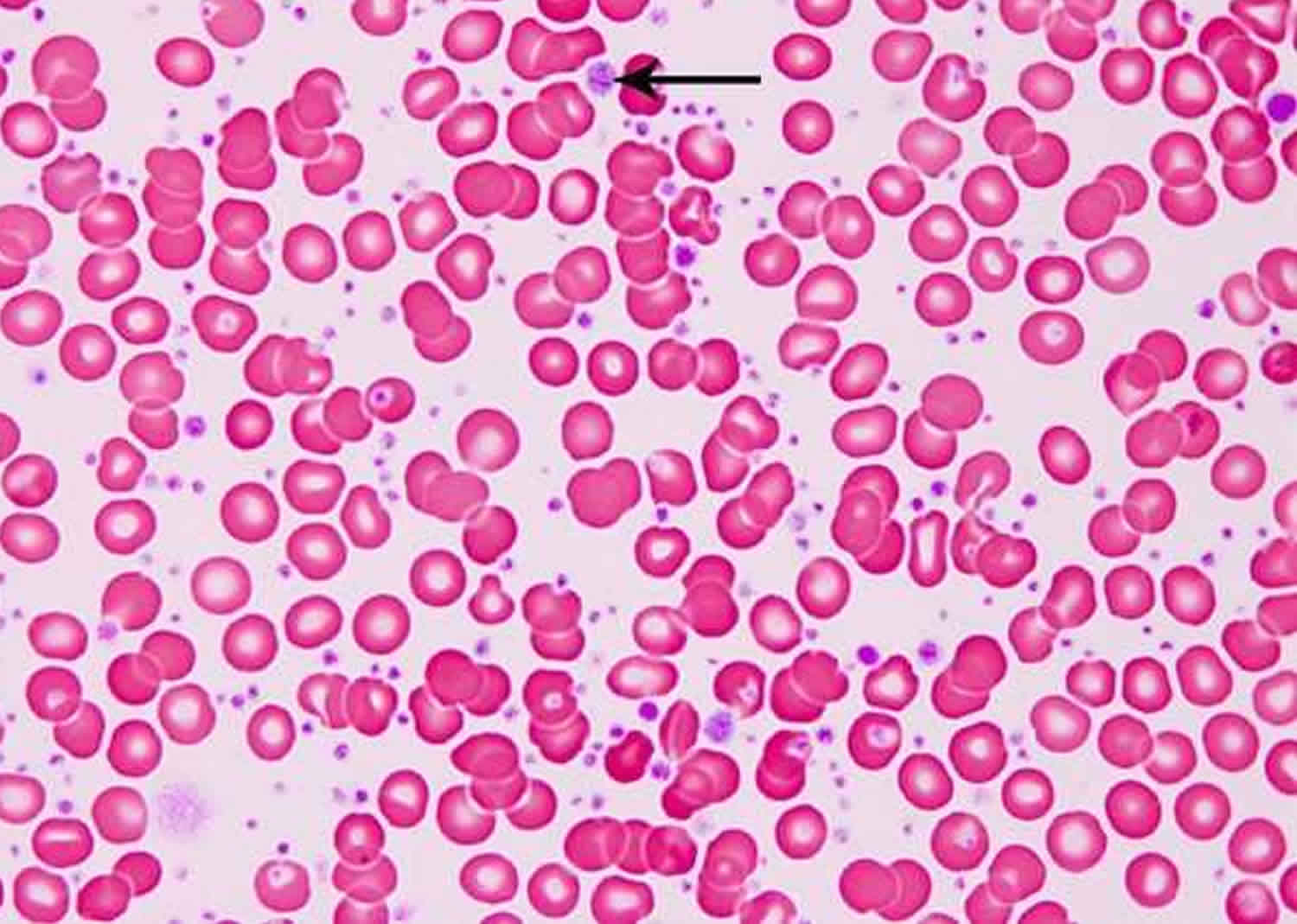
Essential thrombocythemia (also known as essential thrombocytosis or primary thrombocythemia) is a disease in which there are too many platelets (thrombocythemia) are made in the bone marrow. Platelets (thrombocytes) are blood cell fragments involved in blood clotting. Platelets stick together to help form blood clots. Normally, blood clots stop bleeding when you damage a blood vessel, such as when you get a cut. Normally, blood clots stop bleeding when you damage a blood vessel. While some people with this condition have no signs or symptoms, others develop problems associated with the excess platelets leading to abnormal clotting or bleeding. Essential thrombocythemia affects an estimated 1 to 24 per 1 million people worldwide. Essential thrombocythemia is most common in middle aged people. It can also be seen in younger people, especially women under age 40.
A normal platelet count ranges from 150,000 to 450,000 platelets per microliter of blood. Someone with essential thrombocythemia has more than 450,000 platelets per microliter of blood.
Abnormal blood clotting (thrombosis) is common in people with essential thrombocythemia and causes many signs and symptoms of this condition. Clots that block blood flow to the brain can cause strokes or temporary stroke-like episodes known as transient ischemic attacks. Thrombosis in the legs can cause leg pain, swelling, or both. In addition, clots can travel to the lungs (pulmonary embolism), blocking blood flow in the lungs and causing chest pain and difficulty breathing (dyspnea).
Another problem in essential thrombocythemia is abnormal bleeding, which occurs more often in people with a very high number of platelets. Affected people may have nosebleeds, bleeding gums, or bleeding in the gastrointestinal tract. It is thought that bleeding occurs because a specific protein in the blood that helps with clotting is reduced, although why the protein is reduced is unclear.
Other signs and symptoms of essential thrombocythemia include an enlarged spleen (splenomegaly); weakness; headaches; or a sensation in the skin of burning, tingling, or prickling. Some people with essential thrombocythemia have episodes of severe pain, redness, and swelling (erythromelalgia), which commonly occur in the hands and feet.
Most cases of essential thrombocythemia are not inherited. Instead, the condition arises from gene mutations that occur in early blood-forming cells after conception. These alterations are called somatic mutations.
Less commonly, essential thrombocythemia is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. When it is inherited, the condition is called familial essential thrombocythemia.
Essential thrombocythemia is a chronic disease with no cure. If you have a mild form of the disease, you may not need treatment. If you have a severe condition, you may need medicine that lowers your platelet count, blood thinners or both.
The main symptoms of stroke can be remembered with the word F.A.S.T.:
- Face – the face may have dropped on one side, the person may not be able to smile, or their mouth or eye may have dropped.
- Arms – the person with suspected stroke may not be able to lift both arms and keep them there because of weakness or numbness in one arm.
- Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake.
- Time – it’s time to dial your local emergency number immediately if you see any of these signs or symptoms.
If you have any of these symptoms or if you suspect someone else is having a stroke, you must get to a hospital quickly to begin treatment. Acute stroke therapies try to stop a stroke while it is happening by quickly dissolving the blood clot or by stopping the bleeding.
Post-stroke rehabilitation helps individuals overcome disabilities that result from stroke damage. Drug therapy with blood thinners is the most common treatment for stroke.
Seek medical attention immediately:
- If you develop signs or symptoms of a heart attack, such as pressure, fullness or a squeezing pain in the center of your chest lasting more than a few minutes; pain extending to your shoulder, arm, back, teeth or jaw; shortness of breath; and sweating or clammy skin.
Heart attack treatment works best when it’s given right after symptoms occur.
- Don’t Wait–Get Help Quickly
- Quick Action Can Save Your Life
- If you think you or someone else is having a heart attack, even if you’re not sure, don’t feel embarrassed to call your local emergency number right away !
- Do not drive to the hospital or let someone else drive you. Call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room. Take a nitroglycerin pill if your doctor has prescribed this type of treatment.
Is essential thrombocythemia cancer
Yes. Essential thrombocythemia is part of a group of conditions known as myeloproliferative disorders or myeloproliferative cancers. Myeloproliferative disorders cause platelets, white blood cells and red blood cells to grow abnormally in the bone marrow (the soft tissue inside the hollow part of bones that helps form blood cells).
The term myeloproliferative neoplasms typically refers to essential thrombocythemia, polycythemia vera and primary myelofibrosis 1; in addition, some patients with essential thrombocythemia or polycythemia vera might in time progress into a primary myelofibrosis-like post-essential thrombocythemia or post-PV myelofibrosis2. As a group, essential thrombocythemia, polycythemia vera and primary myelofibrosis share three mutually exclusive “driver” mutations, including JAK2, CALR, and MPL3. The most frequent driver mutation is JAK2V617F, found in ~99% of patients with polycythemia vera, 55% essential thrombocythemia, and 65% primary myelofibrosis 2. The driver mutation distributions in essential thrombocythemia and primary myelofibrosis are similar with 50–65% of the patients being JAK2V617F mutated, 15–30% being CALR mutated, and 4–8% being MPL mutated 2, while 10–20% of the patients might not express any one of the three mutations (i.e., are triple-negative) 2.
Table 1. WHO classification of myeloid neoplasms and acute leukemia
| WHO myeloid neoplasm and acute leukemia classification |
|---|
| Myeloproliferative neoplasms (MPN) |
| Chronic myeloid leukemia (CML), BCR-ABL1+ |
| Chronic neutrophilic leukemia (CNL) |
| Polycythemia vera (PV) |
| Primary myelofibrosis (PMF) |
| PMF, prefibrotic/early stage |
| PMF, overt fibrotic stage |
| Essential thrombocythemia |
| Chronic eosinophilic leukemia, not otherwise specified (NOS) |
| MPN, unclassifiable |
| Mastocytosis |
| Myeloid/lymphoid neoplasms with eosinophilia and rearrangement of PDGFRA, PDGFRB, or FGFR1, or with PCM1-JAK2 |
| Myeloid/lymphoid neoplasms with PDGFRA rearrangement |
| Myeloid/lymphoid neoplasms with PDGFRB rearrangement |
| Myeloid/lymphoid neoplasms with FGFR1 rearrangement |
| Provisional entity: Myeloid/lymphoid neoplasms with PCM1-JAK2 |
| Myelodysplastic/myeloproliferative neoplasms (MDS/MPN) |
| Chronic myelomonocytic leukemia (CMML) |
| Atypical chronic myeloid leukemia (aCML), BCR-ABL1− |
| Juvenile myelomonocytic leukemia (JMML) |
| MDS/MPN with ring sideroblasts and thrombocytosis (MDS/MPN-RS-T) |
| MDS/MPN, unclassifiable |
| Myelodysplastic syndromes (MDS) |
| MDS with single lineage dysplasia |
| MDS with ring sideroblasts (MDS-RS) |
| MDS-RS and single lineage dysplasia |
| MDS-RS and multilineage dysplasia |
| MDS with multilineage dysplasia |
| MDS with excess blasts |
| MDS with isolated del(5q) |
| MDS, unclassifiable |
| Provisional entity: Refractory cytopenia of childhood |
| Myeloid neoplasms with germ line predisposition |
| Acute myeloid leukemia (AML) and related neoplasms |
| AML with recurrent genetic abnormalities |
| AML with t(8;21)(q22;q22.1);RUNX1-RUNX1T1 |
| AML with inv(16)(p13.1q22) or t(16;16)(p13.1;q22);CBFB-MYH11 |
| APL with PML-RARA |
| AML with t(9;11)(p21.3;q23.3);MLLT3-KMT2A |
| AML with t(6;9)(p23;q34.1);DEK-NUP214 |
| AML with inv(3)(q21.3q26.2) or t(3;3)(q21.3;q26.2); GATA2, MECOM |
| AML (megakaryoblastic) with t(1;22)(p13.3;q13.3);RBM15-MKL1 |
| Provisional entity: AML with BCR-ABL1 |
| AML with mutated NPM1 |
| AML with biallelic mutations of CEBPA |
| Provisional entity: AML with mutated RUNX1 |
| AML with myelodysplasia-related changes |
| Therapy-related myeloid neoplasms |
| AML, NOS |
| AML with minimal differentiation |
| AML without maturation |
| AML with maturation |
| Acute myelomonocytic leukemia |
| Acute monoblastic/monocytic leukemia |
| Pure erythroid leukemia |
| Acute megakaryoblastic leukemia |
| Acute basophilic leukemia |
| Acute panmyelosis with myelofibrosis |
| Myeloid sarcoma |
| Myeloid proliferations related to Down syndrome |
| Transient abnormal myelopoiesis (TAM) |
| Myeloid leukemia associated with Down syndrome |
| Blastic plasmacytoid dendritic cell neoplasm |
| Acute leukemias of ambiguous lineage |
| Acute undifferentiated leukemia |
| Mixed phenotype acute leukemia (MPAL) with t(9;22)(q34.1;q11.2); BCR-ABL1 |
| MPAL with t(v;11q23.3); KMT2A rearranged |
| MPAL, B/myeloid, NOS |
| MPAL, T/myeloid, NOS |
| B-lymphoblastic leukemia/lymphoma |
| B-lymphoblastic leukemia/lymphoma, NOS |
| B-lymphoblastic leukemia/lymphoma with recurrent genetic abnormalities |
| B-lymphoblastic leukemia/lymphoma with t(9;22)(q34.1;q11.2);BCR-ABL1 |
| B-lymphoblastic leukemia/lymphoma with t(v;11q23.3);KMT2A rearranged |
| B-lymphoblastic leukemia/lymphoma with t(12;21)(p13.2;q22.1); ETV6-RUNX1 |
| B-lymphoblastic leukemia/lymphoma with hyperdiploidy |
| B-lymphoblastic leukemia/lymphoma with hypodiploidy |
| B-lymphoblastic leukemia/lymphoma with t(5;14)(q31.1;q32.3) IL3-IGH |
| B-lymphoblastic leukemia/lymphoma with t(1;19)(q23;p13.3);TCF3-PBX1 |
| Provisional entity: B-lymphoblastic leukemia/lymphoma, BCR-ABL1–like |
| Provisional entity: B-lymphoblastic leukemia/lymphoma with iAMP21 |
| T-lymphoblastic leukemia/lymphoma |
| Provisional entity: Early T-cell precursor lymphoblastic leukemia |
| Provisional entity: Natural killer (NK) cell lymphoblastic leukemia/lymphoma |
Note: WHO = World Health Organization
[Source 1]Essential thrombocythemia prognosis
While outcomes can vary, most people can go for long periods without complications and have a normal lifespan. In a small number of people, complications from bleeding and blood clots can cause serious problems.
In rare cases, the disease can change into acute myelogenous leukemia or myelofibrosis.
Essential thrombocythemia complications
Older people with essential thrombocythemia are at risk of complications. People who’ve had prior blood clots or bleeding problems related to the disease are also at risk of complications.
The abnormal blood clotting of essential thrombocythemia can lead to a variety of potentially serious complications, including:
- Stroke. A clot that blocks blood flow to your brain can cause a stroke. If you develop signs and symptoms of a stroke, get immediate medical attention.
- Heart attack. Blood clots that obstruct blood flow to your heart cause heart attacks. Get immediate attention if you develop signs and symptoms of a heart attack.
- Excessive bleeding. This may appear as nosebleeds, bleeding gums or bruising.
Rarely, essential thrombocythemia may progress to these potentially life-threatening diseases:
- Acute myelogenous leukemia. This is a type of white blood cell and bone marrow cancer that progresses rapidly.
- Myelofibrosis. This progressive disorder results in bone marrow scarring, leading to severe anemia and enlargement of your liver and spleen.
Pregnancy complications
Pregnant women with essential thrombocythemia have a higher risk of complications than women without the condition. But most women who have thrombocythemia have normal, healthy pregnancies.
However, uncontrolled thrombocythemia can lead to miscarriage and other complications. Your risk of complications may be reduced with regular checkups and medication, so be sure to have your doctor regularly monitor your condition.
Current treatment recommendations in young women wishing to be pregnant or are pregnant include once-daily aspirin for “very low-risk” or “low-risk” disease and pegylated IFN-α for high-risk disease 3. Both aspirin and IFN-α therapy have been shown to be safe for use during pregnancy and might be associated with lower miscarriage rates in women with essential thrombocythemia 4. The additional value of other measures, including platelet pheresis or low molecular weight heparin, is unclear and not recommended 5.
Essential thrombocythemia life expectancy
Essential thrombocythemia results from an overproduction of platelets. Untreated, essential thrombocythemia worsens over time. Because these platelets do not work normally, blood clots and bleeding are common problems.
Survival in patients with any one of the three JAK2 mutation-enriched myeloproliferative cancers is significantly shorter than that of the sex- and age-adjusted control population, with median estimates of 20 years for essential thrombocythemia, 14 years for polycythemia vera and 6 years for primary myelofibrosis 6.
Most patients with World Health Organization-defined essential thrombocythemia can expect a normal life expectancy with very low risk of leukemic transformation or fibrotic progression and a diagnosis of essential thrombocythemia should not deter one from continuing with normal life activities, including sports, air travel, and pregnancy. Patients with essential thrombocythemia should be informed about their driver mutational status and its prognostic and therapeutic implications. In this regard, aspirin therapy is very important for JAK2-mutated patients, because of their increased risk for arterial thrombosis. MPL mutations are infrequent in essential thrombocythemia (~3%) and their presence raises the possibility of occult prefibrotic primary myelofibrosis or an increased risk of fibrotic progression. Observation alone remains a viable treatment option for “very low-risk” patients with essential thrombocythemia while all other patients might benefit from aspirin therapy, in a once- or twice-daily schedule. In addition, cytoreductive treatment is strongly encouraged in patients with thrombosis history, and our first- and second-line drugs of choice in this regard are hydroxyurea and pegylated IFN-α, respectively.
Certain factors affect prognosis (chance of recovery) and treatment options for essential thrombocythemia.
Prognosis (chance of recovery) and treatment options depend on the following:
- The age of the patient.
- Whether the patient has signs or symptoms or other problems related to essential thrombocythemia.
Essential thrombocythemia causes
Essential thrombocythemia is a type of chronic myeloproliferative disorder. That means the bone marrow, the spongy tissue inside your bones, makes too many of a certain type of cell. In the case of essential thrombocythemia, the bone marrow makes too many cells that create platelets.
It’s not clear what causes this to happen. About 90 percent of people with the disorder have an acquired gene mutation contributing to the disease.
If an underlying condition such as an infection or iron deficiency causes a high platelet count, it’s called reactive, or secondary, thrombocythemia. Secondary thrombocythemia causes less risk of blood clots and bleeding than does essential thrombocythemia.
Many people with essential thrombocythemia have a mutation of a gene (JAK2, CALR, or MPL).
The JAK2 and CALR genes are the most commonly mutated genes in essential thrombocythemia. The MPL, THPO, and TET2 genes can also be altered in this condition. The JAK2, MPL, and THPO genes provide instructions for making proteins that promote the growth and division (proliferation) of blood cells. The CALR gene provides instructions for making a protein with multiple functions, including ensuring the proper folding of newly formed proteins and maintaining the correct levels of stored calcium in cells. The TET2 gene provides instructions for making a protein whose function is unknown.
The proteins produced from the JAK2, MPL, and THPO genes are part of a signaling pathway called the JAK/STAT pathway, which transmits chemical signals from outside the cell to the cell’s nucleus. These proteins work together to turn on (activate) the JAK/STAT pathway, which promotes the proliferation of blood cells, particularly platelets and their precursor cells, megakaryocytes.
Mutations in the JAK2, MPL, and THPO genes that are associated with essential thrombocythemia lead to overactivation of the JAK/STAT pathway. The abnormal activation of JAK/STAT signaling leads to overproduction of megakaryocytes, which results in an increased number of platelets. Excess platelets can cause thrombosis, which leads to many signs and symptoms of essential thrombocythemia.
Although mutations in the CALR and TET2 genes have been found in people with essential thrombocythemia, it is unclear how these gene mutations are involved in development of the condition.
Some people with essential thrombocythemia do not have a mutation in any of the known genes associated with this condition. Researchers are working to identify other genes that may be involved in the condition.
Essential thrombocythemia is part of a group of conditions known as myeloproliferative disorders. Myeloproliferative disorders cause platelets, white blood cells and red blood cells to grow abnormally in the bone marrow (the soft tissue inside the hollow part of bones that helps form blood cells).
Other myeloproliferative disorders include:
- Chronic myelogenous leukemia (cancer that starts in the bone marrow)
- Polycythemia vera (bone marrow disease that leads to an abnormal increase in the number of blood cells)
- Primary myelofibrosis (disorder of the bone marrow in which the marrow is replaced by fibrous scar tissue)
Essential thrombocythemia symptoms
Patients with essential thrombocythemia may have no signs or symptoms.
Essential thrombocythemia often does not cause early signs or symptoms. It may be found during a routine blood test. Signs and symptoms may be caused by essential thrombocytopenia or by other conditions. Check with your doctor if you have any of the following:
- Headache (most common).
- Tingling, coldness, burning, numbness or blueness in the hands and feet.
- Redness and warmth of the hands or feet.
- Feeling dizzy or lightheaded.
- Vision or hearing problems.
- Mini-strokes (transient ischemic attacks) or stroke.
Platelets are sticky. When there are too many platelets, they may clump together and make it hard for the blood to flow. Clots may form in blood vessels and there may also be increased bleeding. These can cause serious health problems such as stroke or heart attack.
If a blood clot occurs in the arteries that supply the brain, it may cause a transient ischemic attack (TIA) or stroke. A TIA, or ministroke, is a temporary interruption of blood flow to part of the brain. Signs and symptoms of a stroke or TIA develop suddenly and include:
- Weakness or numbness of your face, arm or leg, usually on one side of your body
- Difficulty speaking or understanding speech (aphasia)
- Blurred, double or decreased vision
Less commonly, essential thrombocythemia may cause bleeding, especially if your platelet count is extremely high (more than 1 million platelets per microliter of blood). If bleeding is a problem, symptoms may include any of the following:
- Easy bruising and nosebleeds
- Bleeding from the gastrointestinal tract, respiratory system, urinary tract, or skin
- Bleeding from the gums
- Prolonged bleeding from surgical procedures or tooth removal
Essential thrombocythemia diagnosis
Most of the time, essential thrombocythemia is found through blood tests done for other health problems before symptoms appear. If your blood count is above 450,000 platelets per microliter of blood, your doctor will look for an underlying condition.
Your health care provider may notice an enlarged liver or spleen on physical examination. You may also have abnormal blood flow in the toes or feet that causes skin damage in these areas.
Your doctor will rule out all other causes of high platelet counts to confirm a diagnosis of essential thrombocythemia.
Blood tests
Samples of your blood will be checked for:
- The number of platelets
- The size of your platelets
- The activity of your platelets
- Specific genetic flaws, such as the JAK2, CALR or MPL gene mutation
- Iron levels
- Markers of inflammation
Bone marrow tests
Your doctor may also suggest two bone marrow tests:
- Bone marrow aspiration. Your doctor extracts a small amount of your liquid bone marrow through a needle. The sample is examined under a microscope for abnormal cells.
- Bone marrow biopsy. Your doctor takes a sample of solid bone marrow tissue through a needle. The sample is examined under a microscope to determine whether your bone marrow has a higher than normal number of the large cells that make platelets (megakaryocytes).
Essential thrombocythemia treatment
Although there’s no cure for essential thrombocythemia, there are treatments available. And, lifespan is expected to be normal despite the disease.
Treatment of essential thrombocythemia depends on your risk of blood-clotting or bleeding episodes. If you’re younger than 60 and have had no signs or symptoms, you may simply need periodic medical checkups.
Your doctor may prescribe medication if:
- You’re older than 60 and have had previous blood clots or transient ischemic attacks (TIAs)
- You have cardiovascular risk factors, such as high cholesterol, high blood pressure and diabetes
Medication
Your doctor may suggest one of the following prescription drugs, perhaps along with low-dose aspirin (81 to 100 mg per day), to reduce your platelet count or clotting risk. Aspirin makes platelets less sticky and your blood less likely to form clots. It’s often used in pregnancy because it has a low risk of causing side effects to the fetus.
- Hydroxyurea (Droxia, Hydrea). This drug suppresses bone marrow production of blood cells, including platelets. Its side effects are usually mild, and may include nausea, hair loss, discolored nails and ulcers in the mouth or on the legs. Your doctor will monitor your blood counts and liver function. There’s some concern that long-term use may slightly increase the risk of developing acute myelogenous leukemia.
- Anagrelide (Agrylin). Unlike hydroxyurea, anagrelide isn’t associated with an increased risk of leukemia, but it’s not considered as effective. Side effects may include fluid retention, heart problems, headaches, dizziness, nausea and diarrhea.
- Interferon alfa (Intron A) or peginterferon alpha-2a (Pegasys). This drug is given by injection, and may cause worse side effects than hydroxyurea or anagrelide does. But it’s the best choice for some people. Side effects may include flu-like symptoms, confusion, nausea, depression, diarrhea, seizures, irritability and sleepiness.
Emergency procedure
A medical procedure called platelet pheresis is used only in emergencies, such as after a stroke or other dangerous blood clotting. It temporarily lowers your platelet count. A needle connected to a tube allows your blood to flow into a device that removes platelets, after which your blood is returned to your body.
Essential thrombocythemia diet
Eat healthy foods. Choose a varied diet rich in whole grains, vegetables and fruits, and low in saturated fats. Try to avoid trans fats. Learn about portion control to maintain a normal weight.
Also try to choose healthy lifestyle habits to lower your risk of developing conditions that may contribute to blood clotting. These include diabetes, high blood pressure and high blood cholesterol. Take steps to:
- Increase your physical activity. Aim for at least 30 minutes of moderate physical activity a day. Take a brisk daily walk, ride your bike or swim laps.
- Achieve or maintain normal weight. Being overweight or obese increases the risk of blood clots.
- Stop smoking. If you smoke, take steps to try to stop.
- Arber DA, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–2405. doi: 10.1182/blood-2016-03-643544. http://www.bloodjournal.org/content/127/20/2391.long[↩][↩]
- Tefferi A, Pardanani A. Myeloproliferative neoplasms: a contemporary review. JAMA Oncol. 2015;1:97–105. doi: 10.1001/jamaoncol.2015.89. https://www.ncbi.nlm.nih.gov/pubmed/26182311[↩][↩][↩]
- Tefferi A, Passamonti F. Essential thrombocythemia and pregnancy: Observations from recent studies and management recommendations. Am. J. Hematol. 2009;84:629–630. doi: 10.1002/ajh.21508. https://www.ncbi.nlm.nih.gov/pubmed/19731306[↩]
- Beauverd Y, et al. Pegylated interferon alpha-2a for essential thrombocythemia during pregnancy: outcome and safety. A case series. Haematologica. 2016;101:e182–e184. doi: 10.3324/haematol.2015.139691 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5004380/[↩]
- Valera MC, Parant O, Vayssiere C, Arnal JF, Payrastre B. Essential thrombocythemia and pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011;158:141–147. doi: 10.1016/j.ejogrb.2011.04.040. https://www.ncbi.nlm.nih.gov/pubmed/21640467[↩]
- Tefferi A, et al. Long-term survival and blast transformation in molecularly annotated essential thrombocythemia, polycythemia vera, and myelofibrosis. Blood. 2014;124:2507–2513. doi: 10.1182/blood-2014-05-579136. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4199952/[↩]





{kind=link}