
Contents
What is drop foot
Foot drop describes the inability to raise the front part of the foot due to weakness or paralysis of the muscles that lift your foot and toes. As a result, individuals with foot drop scuff their toes along the ground or bend their knees to lift their foot higher than usual to avoid the scuffing. Foot drop is also sometimes called drop foot, and can cause you to drag your foot on the ground when you walk.
If you have foot drop, you’ll find it difficult to lift the front part of your foot off the ground. This means you’ll have a tendency to scuff your toes along the ground, increasing your risk of falls. To prevent this, you may lift your foot higher than usual when walking, which causes what is called a “steppage” gait.
Foot drop is a sign of an underlying problem rather than a condition itself. This could be muscular, caused by nerve damage in the leg, or the result of a brain or spinal injury.
Foot drop can be unilateral (affecting one foot) or bilateral (affecting both feet), depending on the cause. Foot drop is a symptom of an underlying problem and is either temporary or permanent, depending on the cause.
Foot drop can be temporary or permanent. If you have foot drop, you might need to wear a brace on your ankle and foot to hold your foot in a normal position.
Foot drop causes include:
- Neurodegenerative disorders of the brain that cause muscular problems, such as multiple sclerosis, stroke, and cerebral palsy;
- Motor neuron disorders such as polio, some forms of spinal muscular atrophy and amyotrophic lateral sclerosis (commonly known as Lou Gehrig’s disease);
- Injury to the nerve roots, such as in spinal stenosis; peripheral nerve disorders such as Charcot-Marie-Tooth disease or acquired peripheral neuropathy;
- Local compression or damage to the superficial fibular nerve (peroneal nerve) as it passes across the fibular bone below the knee; and
- Muscle disorders, such as muscular dystrophy or myositis.
All muscles of the anterior compartment of the leg are dorsiflexors of the ankle and have a common innervation, the common fibular nerve (also called common peroneal nerve) (see Figures 1 to 3). Paralysis of the anterior muscle group causes foot drop, which requires that one lift the leg unusually high during walking to prevent tripping over one’s toes.
Foot drop nerve – Common Fibular Nerve
The common fibular nerve part of the sciatic nerve innervates the short head of the biceps femoris in the posterior compartment of the thigh and then continues into the lateral and anterior compartments of the leg and onto the foot (Figures 1 and 2) .
The common fibular nerve innervates :
- All muscles in the anterior and lateral compartments of the leg,
- One muscle (extensor digitorum brevis) on the dorsal aspect of the foot,
- The first two dorsal interossei muscles in the sole of the foot, and
- Skin over the lateral aspect of the leg, and ankle, and over the dorsal aspect of the foot and toes.
Common fibular nerve divides into superficial fibular and deep fibular branch. The deep fibular nerve supplies all the muscles in the anterior compartment of the leg. The anterior compartment of the leg consists of muscles that dorsiflex the foot. Within the anterior compartment, the tibialis anterior is a long, thick muscle against the lateral surface of the tibia. The extensor hallucis longus is a thin muscle between and partly deep to the tibialis anterior and extensor digitorum longus muscles. This featherlike muscle is lateral to the tibialis anterior muscle, where it can also be palpated easily. The fibularis (peroneus) tertius muscle is part of the extensor digitorum longus, with which it shares a common origin.
The superficial fibular nerve supplies all the muscles in the lateral (fibular) compartment of the leg contains two muscles that plantar flex and evert the foot: the fibularis (peroneus) longus and fibularis (peroneus) brevis.
Figure 1. Common fibular nerve (L4-S2)
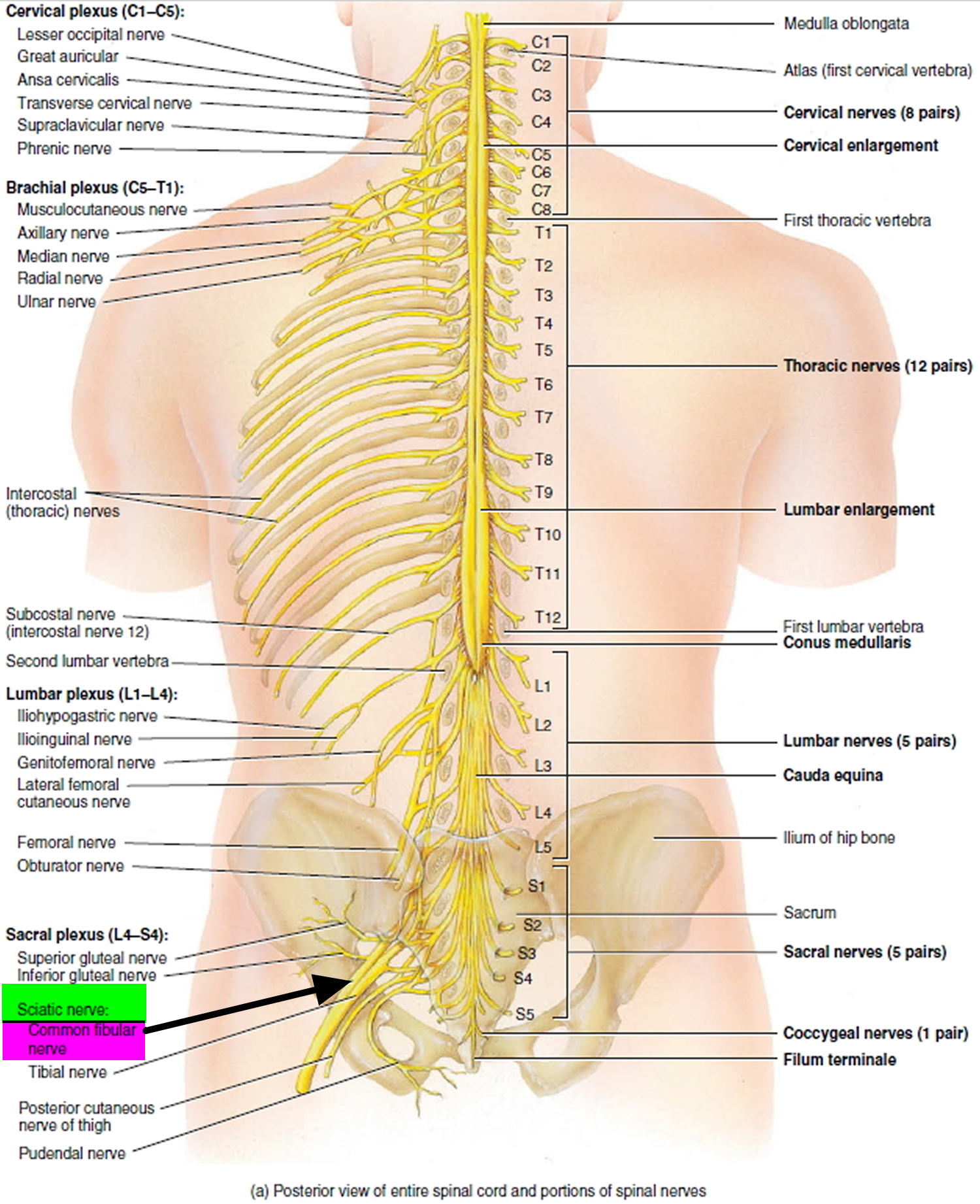
Figure 2. Common fibular nerve (branches)
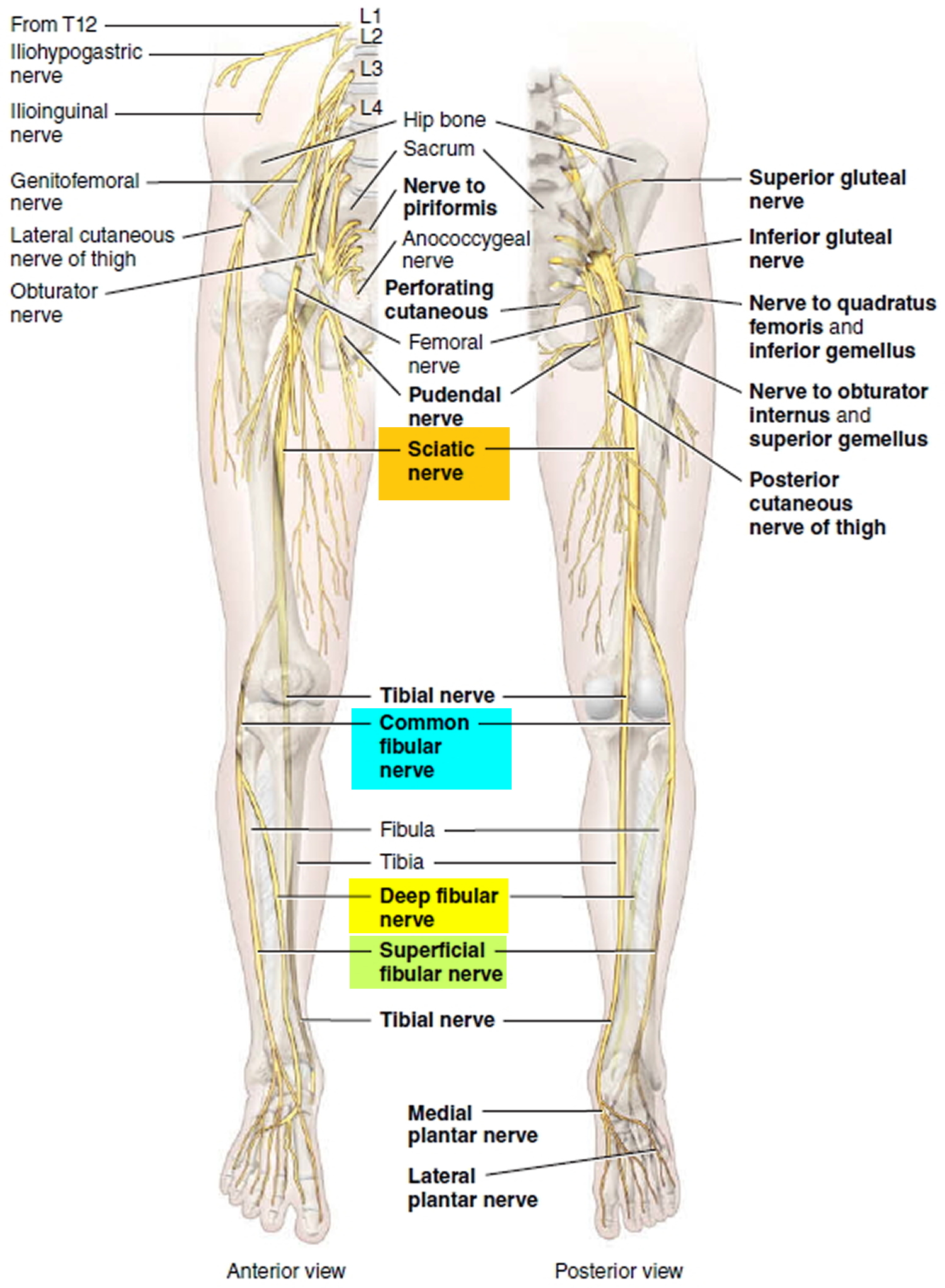
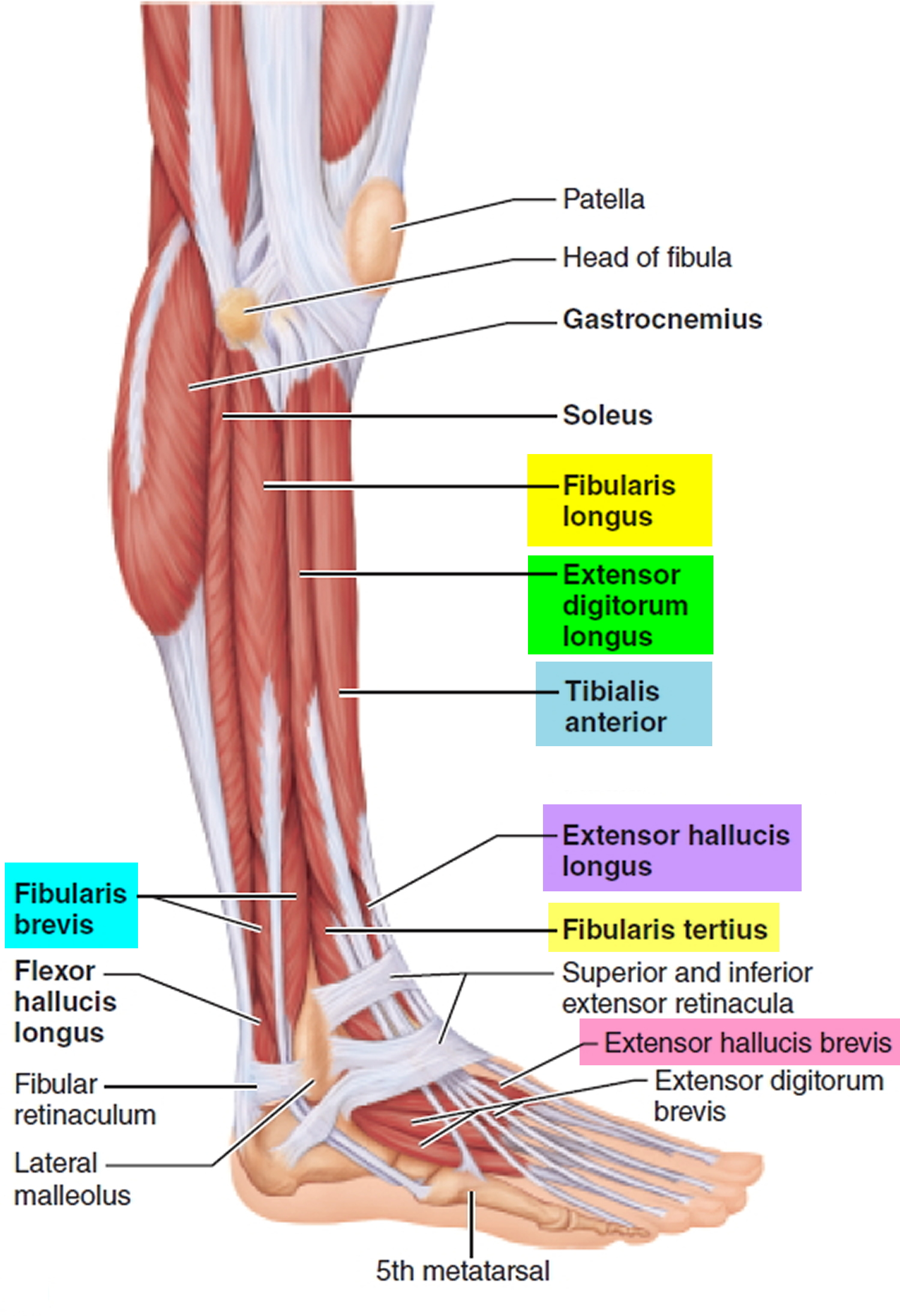
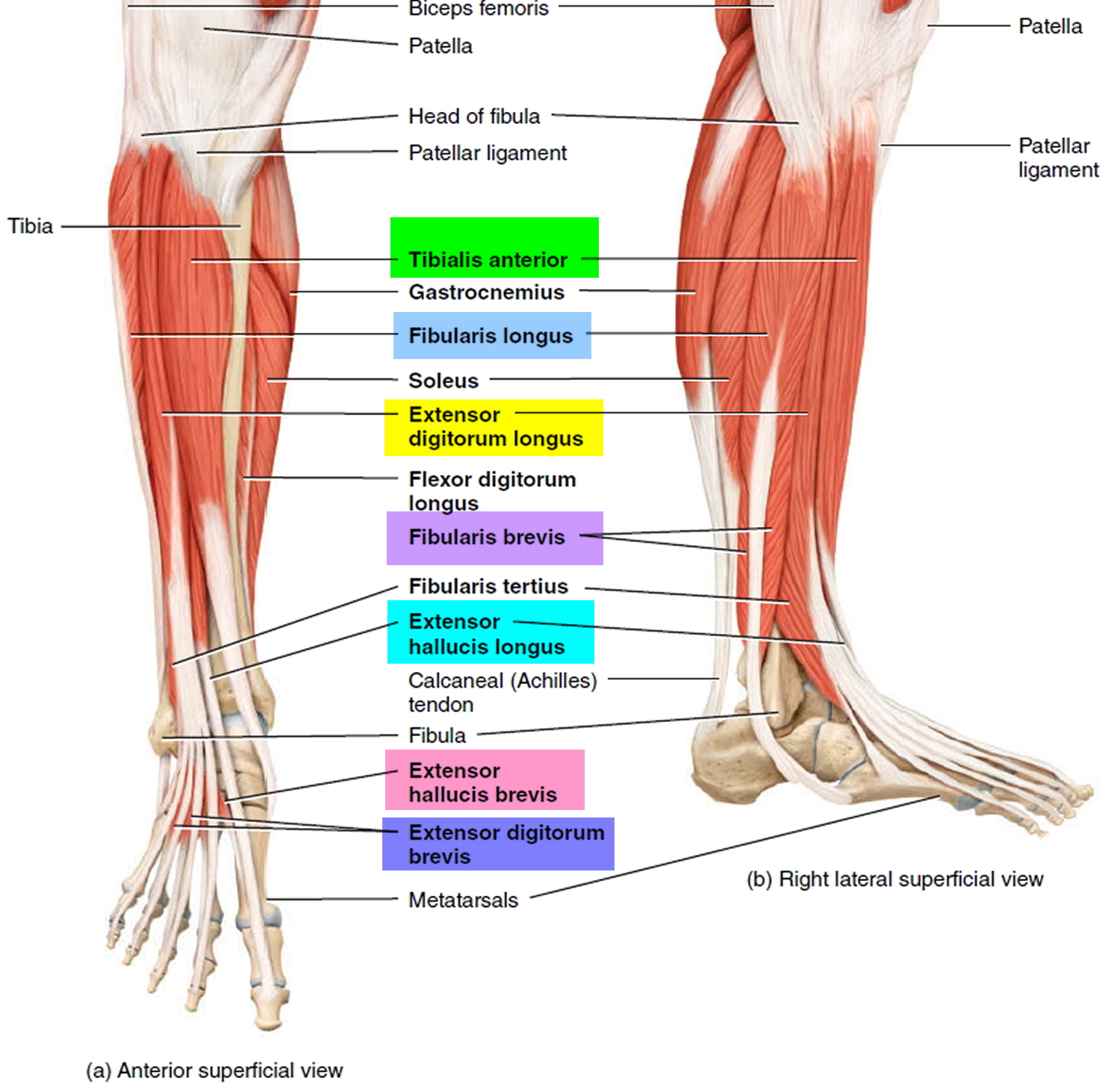
Figure 3. Leg muscles
Foot drop causes
What causes drop foot
Foot drop is the result of weakness or paralysis of the muscles that lift the front part of your foot. This can be caused by a number of underlying problems, which are described below.
Muscle weakness
Muscular dystrophy is a group of inherited genetic conditions that cause gradual muscle weakness and can sometimes lead to foot drop.
Foot drop can also be caused by other muscle wasting conditions, such as spinal muscular atrophy or motor neurone disease.
Peripheral nerve problems or neuropathy
Foot drop is often caused by compression (squashing) of the nerve that controls the muscles that lift the foot.
Sometimes, nerves around the knee or lower spine can become trapped. The nerves in the leg can also be injured or damaged during hip replacement or knee replacement surgery.
Foot drop can sometimes be caused by nerve damage linked to diabetes (known as a neuropathy).
Inherited conditions that cause peripheral nerve damage and muscle weakness, such as Charcot-Marie-Tooth disease, can also sometimes lead to foot drop.
Brain and spinal cord disorders
Foot drop can also be caused by conditions that affect the brain or spinal cord, such as:
- stroke
- cerebral palsy
- multiple sclerosis (MS)
- amyotrophic lateral sclerosis (ALS)
Risk factors for foot drop
The common fibular nerve (common peroneal nerve) controls the muscles that lift your foot (see Figures 1 to 3 above). This superficial fibular nerve (superficial peroneal nerve) runs near the surface of your skin on the outer side of your knee close to the head of the fibula (see Figure 2). Activities that compress this nerve can increase your risk of foot drop. Examples include:
- Crossing your legs. People who habitually cross their legs can compress the superficial peroneal nerve on their uppermost leg.
- Prolonged kneeling. Occupations that involve prolonged squatting or kneeling — such as picking strawberries or laying floor tile — can result in foot drop.
- Wearing a leg cast. Plaster casts that enclose the ankle and end just below the knee can exert pressure on the superficial peroneal nerve.
Foot drop symptoms
Foot drop makes it difficult to lift the front part of your foot, so it might drag on the floor when you walk. This can cause you to raise your thigh when you walk, as though climbing stairs (steppage gait), to help your foot clear the floor. This unusual gait might cause you to slap your foot down onto the floor with each step. In some cases, the skin on the top of your foot and toes feels numb.
Depending on the cause, foot drop can affect one or both feet.
Foot drop diagnosis
Foot drop is often diagnosed during a physical examination. Your doctor will look at the way you walk and examine your leg muscles.
He or she may also check for numbness on your shin and on the top of your foot and toes.
In some cases, imaging tests, such as an X-ray, ultrasound scan or computerised tomography (CT) scan, may be required.
Nerve conduction tests may be recommended to help locate where the affected nerve is damaged.
Imaging tests
Foot drop is sometimes caused by an overgrowth of bone in the spinal canal or by a tumor or cyst pressing on the nerve in the knee or spine. Imaging tests can help pinpoint these types of problems.
- X-rays. Plain X-rays use a low level of radiation to visualize a soft tissue mass or a bone lesion that might be causing your symptoms.
- Ultrasound. This technology, which uses sound waves to create images of internal structures, can check for cysts or tumors on the nerve or show swelling on the nerve from compression.
- CT scan. This combines X-ray images taken from many different angles to form cross-sectional views of structures within the body.
- Magnetic resonance imaging (MRI). This test uses radio waves and a strong magnetic field to create detailed images. MRI is particularly useful in visualizing soft tissue lesions that may be compressing a nerve.
Nerve tests
Electromyography (EMG) and nerve conduction studies measure electrical activity in the muscles and nerves. These tests can be uncomfortable, but they’re useful in determining the location of the damage along the affected nerve.
Electromyography, where electrodes are inserted into the muscle fibres to record the muscles’ electrical activity, may also be carried out at the same time.
Foot drop treatment
Treatment for foot drop depends on the cause. If the cause is successfully treated, foot drop might improve or even disappear. If the cause can’t be treated, foot drop can be permanent.
Treatment for foot drop might include:
- Braces or splints. A brace on your ankle and foot or splint that fits into your shoe can help hold your foot in a normal position.
- Physical therapy. Exercises that strengthen your leg muscles and help you maintain the range of motion in your knee and ankle might improve gait problems associated with foot drop. Stretching exercises are particularly important to prevent the stiffness in the heel.
- Electrical nerve stimulation. Sometimes stimulating the nerve that lifts the foot improves foot drop.
- Surgery. Depending upon the cause, and if your foot drop is relatively new, nerve surgery might be helpful. If foot drop is long-standing, your doctor might suggest surgery that fuses ankle or foot bones or a procedure that transfers a working tendon and attached muscle to a different part of the foot.
Some of these treatments are discussed in more detail below.
Drop foot brace
A drop foot brace or ankle-foot orthosis is worn on the lower part of the leg to help control the ankle and foot. It holds your foot and ankle in a straightened position to improve your walking.
If your doctor thinks an drop foot brace will help, they’ll refer you for an assessment with an orthotist (a specialist who measures and prescribes orthoses).
Wearing a close-fitting sock between your skin and the drop foot brace will ensure comfort and help prevent rubbing. Your footwear should be fitted around the orthosis.
Figure 4. Drop foot brace

Lace-up shoes or those with Velcro fastenings are recommended for use with drop foot braces because they’re easy to adjust. Shoes with a removable inlay are also useful because they provide extra room. High-heeled shoes should be avoided.
It’s important to break your orthosis in slowly. Once broken in, wear it as much as possible while walking because it will help you walk more efficiently and keep you stable.
Electrical nerve stimulation
In some cases, an electrical stimulation device, similar to a TENS (transcutaneous electrical nerve stimulation) machine, can be used to improve walking ability. It can help you walk faster, with less effort and more confidence.
Two self-adhesive electrode patches are placed on the skin. One is placed close to the nerve supplying the muscle and the other over the center of the muscle. Leads connect the electrodes to a battery-operated stimulator, which is the size of a pack of cards and is worn on a belt or kept in a pocket.
The stimulator produces electrical impulses that stimulate the nerves to contract (shorten) the affected muscles. The stimulator is triggered by a sensor in the shoe and is activated every time your heel leaves the ground as you walk.
If your doctor or consultant thinks you’ll benefit from using an electrical stimulation device, you’ll be referred to an orthopedic foot and ankle surgeon for an assessment. You may then be referred to a specialist unit to try the device and assess its suitability.
For long-term use, it may be possible to have an operation to implant the electrodes under your skin. The procedure involves positioning the electrodes over the affected nerve while you’re under general anesthetic.
The National Institute for Health and Care Excellence 1 advises that electrical stimulation can be used to treat people with foot drop caused by damage to the brain or spinal cord, provided:
- the person understands what’s involved and agrees to the treatment
- the results of the procedure are closely monitored
Foot drop surgery
Surgery may be an option in severe or long-term cases of foot drop that have caused permanent movement loss from muscle paralysis.
The procedure usually involves transferring a tendon from the stronger leg muscles to the muscle that should be pulling your ankle upwards.
Another type of surgery involves fusing the foot or ankle bones to help stabilize the ankle.
Speak to your doctor or orthopedic foot and ankle specialist if you’re thinking about having surgery for foot drop. They’ll be able to give you more information about the available procedures and any associated pros and cons.
Lifestyle and home remedies
Making small changes in your home, such as removing clutter and using non-slip rugs and mats, can help prevent falls.
Because foot drop can increase your risk of tripping and falling, consider taking these precautions around your house:
- Keep all floors clear of clutter.
- Avoid the use of throw rugs.
- Move electrical cords away from walkways.
- Make sure rooms and stairways are well-lit.
- Place fluorescent tape on the top and bottom steps of stairways.
- Functional electrical stimulation for drop foot of central neurological origin. https://www.nice.org.uk/Guidance/IPG278[↩]




